儿童失语症的干预措施
Abstract
研究背景
儿童失语症(apraxia of speech, CAS)影响了儿童精确一致地发出声音和音节的能力,并且影响他们用精准正确的节奏说出单词和句子的能力。这是一种罕见的情况,只影响到总人口的0.1%。目前已达成共识,三个核心特征具有诊断效力:(1)在重复的音节和单词产生的过程中,辅音和元音会出现不一致的错误;(2)声音和音节之间的协同发音转换延长或受损;(3)不恰当的韵律(ASHA 2007)。运动规划或计划的不足被认为是这种疾病的基础。这意味着孩子们知道他们想说什么,但是规划出良好迅速的精确言语运动的能力被破坏了。CAS患儿在以下一个或多个领域也可能有损伤:非言语的口语运动功能,构音障碍,语言,语音生产障碍,音位意识或元语言技能和识字,或这些的组合。关于对CAS干预的随机对照试验的高质量证据不足。
研究目的
本综述的目的是言语和语言病理学家/治疗师对患CAS的儿童和青少年的言语和语言干预的效果。
检索策略
我们检索了CENTRAL,MEDLINE,Embase,八个其他数据库和七个试验注册库,检索截止至2017年4月。我们检索了纳入报告的参考文献列表,并且要求获取已发表研究作者、其他专家、言语语言治疗/病理及语言学领域信息小组的未发表试验的信息。
标准/纳入排除标准
我们纳入了经言语和语言病理学家/治疗师诊断的3至16岁儿童的RCTs和半RCTs研究,并按治疗类型分组。
数据收集与分析
两位综述作者(FL,AM)独立评价从检索中确定的题目和摘要并获取所有可能相关文章的全文报告,评价它们是否符合标准。同样两位作者提取资料并进行“偏倚风险”和GRADE评价。一位综述作者(EM)将排除的观察性研究的结果制成表格(表格1)。
主要结果
本综述只纳入一项RCT,这项RCT由澳大利亚研究理事会、悉尼大学国际发展基金、道格拉斯&洛拉道格拉斯儿童和青少年健康奖学金、纳迪亚维罗尔纪念奖学金和詹姆斯肯特利纪念奖学金提供资金支持。本研究招募了26名4至12岁的患不明原因轻度至中度CAS的儿童,并对比了两种干预措施:纳菲尔德运动障碍项目‐3(Nuffield Dyspraxia Programme‐3, NDP‐3)和快速音节转换治疗(Rapid Syllable Transitions Treatment, ReST)。患儿被随机分为两组接受不同的处理措施。治疗在澳大利亚的一所医学院门诊中集中进行,每周3天,每次一小时,持续三周。语言病理学学生用英语进行治疗。在治疗前,治疗结束时,治疗结束后一个月、四个月分别对结局进行评价。我们的综述只针对治疗后一个月的结局。每个队列中都有一些病例在治疗后一至四个月间重新开始接受语言病理学家的常规治疗(NDP‐3:9/13受试者;ReST:9/13受试者)。因此,如果没有明显的潜在偏倚,就无法分析治疗四个月后的疗效。所以这个时间点未被纳入本综述的进一步分析中。
我们判断所有核心结局的偏倚风险较低。考虑到只有一项RCT是确定的,由于不精确性,我们把证据等级降低一级降至中等。
NDP‐3和ReST疗法均在治疗后一个月使症状改善。对于三种结果,NDP‐3的影响略大于其他疗法:处理过的文字的准确性(NDP‐3平均差(mean difference,MD)=36.0,ReST MD=33.9;两组间绝对MD=2.1);语音生产一致性, 使用发音和音系的诊断评估(Diagnostic Evaluation of Articulation and Phonology, DEAP)中的不一致性子评估检测25个真实词汇并重复三次(NDP‐3 MD=11.1,ReST MD=10.9;两组间绝对MD=0.2);和连接词的准确性,通过至少三个词组合的连接词的模仿词的准确性来评估(NDP‐3 MD=14.3,ReST MD=11.5;两组间绝对MD=2.8).ReST(MD=18.3)对治疗后1个月未处理单词的生产准确性的影响略大于NDP‐3(MD=18.2)(组间绝对MD=0.1)。这项研究没有评价功能沟通的结果。
作者结论
有限的证据表明,集中进行治疗时,NDP‐3和ReST疗法都会影响4到12岁CAS患儿单词准确度的改善。单词准确度的改善可以通过治疗和未经治疗单词的表达准确性、语言表达的一致性和连续发音的准确性来衡量。本研究没有测量功能性交流。原研究作者没有进行正式的分析来对比NDP‐3和ReST疗法,因此提倡一种疗法比另一种疗法更好并不可靠。我们也无法说明这两种疗法之一是否优于不治疗或常规治疗。目前尚无证据表明针对4到12岁无其他神经发育异常的先天性CAS患儿的其他疗法有效。进一步开展随机对照试验重复该研究将增强证据基础。同样地,对于其他干预措施、其他年龄范围和患有CAS同时并发其他障碍的患者都需要进一步开展随机对照试验。
PICO
Plain language summary
一项对照良好的研究为两种干预措施治疗儿童失语症(apraxia of speech, CAS)的影响提供了证据。
系统综述问题
什么治疗有助于改善患有失语症(apraxia of speech, CAS)的儿童及青少年的言语和语言能力。
研究背景
患有CAS的儿童很难连贯准确地发出声音与音节,以清晰正确地语音节奏说出单词句子。因此,患有CAS的儿童很难被理解,可能会对学业成绩和同伴友谊产生负面影响。CAS会影响到约1%的普通人。本综述整理了研究证据以确定治疗CAS患儿的最有效的方法。
检索日期
证据检索截止到2017年4月6日。
研究特点
我们发现了一项针对26名4到12岁CAS儿的研究。这些儿童患有不明病因的轻度到中度的CAS。患儿被随机分配(使用掷硬币等方法)至2种治疗之一:纳菲尔德运动障碍项目‐第三版(Nuffield Dyspraxia Programme ‐ Third Edition, NDP‐3)和快速音节过渡治疗(Rapid Syllable Transition treatment, ReST)。两种疗法均在一小时内密集进行,每周四天,持续三周。由临床医学院里的语言病理学学生进行治疗。在治疗前,治疗结束时,治疗结束后一个月、四个月分别对结局进行评价。我们的综述只针对治疗后一个月的结局。
研究资金来源
纳入的研究资金来源为澳大利亚研究理事会,悉尼大学国际发展基金,道格拉斯&洛拉道格拉斯儿童和青少年健康奖学金,纳迪亚维罗尔纪念奖学金和詹姆斯肯特利纪念奖学金。
主要结局
重复这些发现的进一步研究将加强现有可获得的证据。
该研究提供的有限证据表明NDP‐3可以提高治疗项目的准确性和连接语音的准确性。有限的证据表明NDP‐3对发音一致性的影响微乎其微,ReST对未处理的词语生成的准确性影响也非常小。本研究没有测量功能性交流。
证据质量
纳入的研究为随机对照试验,并且总体偏倚风险低。考虑到只有一项RCT是确定的,由于不精确性,我们把证据等级降低一级降至中等。
建议
有限的证据表明,NDP‐3或ReST可能对4‐12岁的没有其他共同情况发生的患有不明病因CAS的患儿有帮助。我们无法确定这两种治疗中的某一种是否比另一种更好,也无法确定这两种治疗中的任意一种是否优于无治疗或常规治疗。目前还没有关于其他治疗的证据。
进一步的随机对照试验应关注于加强证据基础,包括将治疗与无治疗(等待名单)对照组进行比较的研究。还需要进一步研究 CAS 和其他疾病或诊断的患儿。
Authors' conclusions
Summary of findings
| Nuffield Dyspraxia Programme ‐ Third Edition (NDP‐3) versus Rapid Syllable Transition Treatment (ReST) for Childhood Apraxia of Speech | |||||
| Patient or population: children aged 4 to 12 years with CAS of unknown cause Settings: University of Sydney Communication Disorders Treatment and Research Clinic Intervention: NDP‐3 Comparison: ReST | |||||
| Outcomes | Summary of MD findings | Absolute MD | Number of participants (studies) | Quality of the evidence | Comments |
| Primary outcomes | |||||
| Accuracy of production on treated items Measured by: counting the number of real words produced correctly (/x) Follow‐up: pre‐intervention to 1 month post‐intervention | NDP‐3 MD of 36.0 was greater than the ReST MD of 33.9 | 2.1 | 26 (1 trial) | ⊕⊕⊕⊝ | — |
| Accuracy of production on non‐treated items Measured by: counting the number of real words produced correctly (/x) Follow‐up: pre‐intervention to 1 month post‐intervention | ReST MD of 18.3 was minimally greater than the NDP‐3 MD of 18.2 | 0.1 | 26 (1 trial) | ⊕⊕⊕⊝ | — |
| Secondary outcomes | |||||
| Speech production consistency Measured by: calculating the number of inconsistent productions of 25 words produced 3 times using the DEAP inconsistency subtestb Follow‐up: pre‐intervention to 1 month post‐intervention | NDP‐3 MD of 11.1 was greater than the ReST MD of 10.9 | 0.2 | 26 (1 trial) | ⊕⊕⊕⊝ | — |
| Accuracy of connected speech Measured by: counting the number of correct imitations of 3 word phrases (/x) Follow‐up: pre‐intervention to 1 month post‐intervention | NDP‐3 MD of 14.3 was greater than the ReST MD of 11.5 | 2.8 | 26 (1 trial) | ⊕⊕⊕⊝ | — |
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. | |||||
| CAS: childhood apraxia of speech; DEAP: Diagnostic Evaluation of Articulation and Phonology; MD: mean difference; NDP‐3: Nuffield Dyspraxia Programme ‐ Third Edition;ReST: Rapid Syllable Transition Treatment (ReST) for Childhood Apraxia of Speech | |||||
| aWe downgraded the quality of evidence by one level, to moderate, for imprecision, as there was only one study for comparison. | |||||
Background
Description of the condition
Childhood apraxia of speech (CAS) affects a child's ability to produce speech sounds and syllables in the right order, and to speak words and sentences with accuracy and correct speech rhythm. Over sixty years ago, Morley 1954 provided a seminal paper documenting a series of speech characteristics in children that resembled the speech production disorder of adults with acquired apraxia of speech, and the diagnosis of CAS was born. CAS is a rare condition, affecting only around 0.1% of the general population (Morley 1972; Yoss 1975). CAS is more prevalent within particular medical subgroups, however, and particularly penetrant in certain genetic syndromes (e.g. Fedorenko 2016; Mei 2017).
Historically, synonyms such as verbal dyspraxia and developmental apraxia of speech have been used. The most commonly used terms today are CAS and developmental verbal dyspraxia (DVD), with the latter used largely in the UK context (RCSLT 2011). We use the term CAS consistently throughout this review.
A deficit in motor programming or planning is thought to underlie CAS; that is, children know what they would like to say but there is a breakdown in the ability to programme or plan the required movements to accurately produce speech. The current approach to diagnosis of CAS is expert‐based perception of speech symptoms (Maas 2012a). There is consensus amongst speech and language pathologists (SLPs), also known as speech and language therapists (SLTs), that three core features of CAS have diagnostic validity: (1) inconsistent error production on both consonants and vowels across repeated productions of syllables or words; (2) lengthened and impaired coarticulatory transitions between sounds and syllables; and (3) inappropriate prosody (ASHA 2007).
In addition to the core features of CAS, children may also have co‐occurring impairments affecting non‐speech oral motor function, language, phonemic awareness/meta‐linguistics and literacy (ASHA 2007). Younger children typically present with more severe forms of the disorder, with improvement noted over time for both idiopathic CAS (Davis 2005; Jacks 2006) and individuals with CAS associated with genetic syndromes (Morgan 2017; Morgan 2018). It is not currently known how age, severity or underlying aetiology impact upon CAS treatment response or outcome.
There are no epidemiological data on the prevalence of CAS, although it occurs infrequently in comparison with other forms of developmental speech disorder such as articulation disorder and phonological disorder, which occur in around 3.5% of preschool children (Eadie 2015). A population‐based estimate suggests that CAS occurs in one child per 1000 (0.1%) (Morley 1972; Yoss 1975), and is found in 3.4% to 4.3% of the children referred to clinics for speech disorder management (Delaney 2004). The diagnosis of CAS can apply to children who have a specific impairment in speech with other neurodevelopmental functions relatively more preserved (e.g. borderline or typical non‐verbal cognition). Historically most cases were referred to as 'idiopathic', given limited aetiological knowledge of the condition (Morgan 2008). In recent times, however, novel insights have been gained into the genetic and neurobiological bases of CAS (Eising 2018). Variations in an increasing number of single genes have been associated with CAS (Eising 2018; Turner 2015), with the most replicated finding being disruption of the Forkhead box protein P2 or FOXP2 (Lai 2001; Morgan 2017; Vargha‐Khadem 2005). Beyond single gene causes, CAS has also been associated with copy number variant syndromes, such as 16p11.2 deletion syndrome (Fedorenko 2016; Mei 2017), Koolen de Vries Syndrome (Morgan 2018), 6q25.3 deletion syndrome (Peter 2017), 7q11.23 duplication syndrome (Velleman 2011), and other genetic conditions such as Floating Harbour syndrome (White 2010). Further to genetic causes, other medical conditions associated with CAS include metabolic disorders (e.g. galactosaemia; Shriberg 2011) or epilepsy disorders (e.g. Liégeois 2012). In relation to neurobiology or brain function, there is inconsistency as regards the key brain regions and networks disrupted in CAS, with neuroimaging studies reporting both cortical and subcortical anomalies (Liégeois 2012; Liégeois 2014; Liégeois 2016).
Description of the intervention
A range of CAS treatment approaches with differing theoretical standpoints have been reported. These studies are almost exclusively in the form of uncontrolled case studies or case series. Therapeutic approaches for CAS can be grouped into the following three areas.
-
Motor‐based approaches. These therapies are based on principles of motor learning (see Maas 2008 for a review); for example, traditional articulation‐based drill therapy (Velleman 1994), the Nuffield Dyspraxia Programme (Williams 2004), the Rapid Syllable Transitions Treatment (Ballard 2010), rate control therapy (Rosenthal 1994), the PROMPT System (Prompts for Restructuring Oral MuscularPhonetic Targets) (Chumpelik 1984; Dale 2013), melodic intonation therapy (Helfrich‐Miller 1994), adapted cueing technique (Klick 1985), and integral stimulation or dynamic temporal and tactile cueing (Maas 2012a; Strand 2006). Motor‐based therapy can also include non‐speech oro‐motor techniques; for example, oral form recognition training (Kingston 1987) and orofacial myofunctional therapy (Ray 2003). Motor‐based therapy can also be instrumentally based, such as delayed auditory feedback (Lozano 1978), electropalatography (Carter 2004; Lundeborg 2007), and ultrasound (Preston 2013).
-
Linguistic approaches. Linguistic therapies address language impairments that can co‐occur in children with CAS. Examples of linguistic approaches include programmes to address phonological speech production or awareness (McNeill 2009).
-
Multi‐modal communication approaches. These approaches seek to support verbal communication. Methods can address specific communication messages or features, such as Aided AAC (augmentative and alternative communication) Modelling (Binger 2007), or use of technological devices (Bornman 2001; Cumley 1999).
How the intervention might work
Below, we describe the ways in which the aforementioned approaches (described under Description of the intervention) might work.
-
Motor‐based approaches. These methods use principles of motor learning, such as emphasizing a high number of successful repetitions of a task, using stimuli with high complexity, and a period of teaching followed by practice where cues and feedback are faded. Such approaches are reported to facilitate maintenance and generalisation in children with CAS (Maas 2008; Maas 2014).
-
Linguistic approaches. These methods are focused on the semantics, phonology or grammar of language, and not on motor speech production per se. For example, a linguistic approach may include phonological contrast therapy, where children are taught how to abstract speech sound rules for the specific language(s) they speak (Dodd 2008). Another example of a linguistic approach is core vocabulary therapy, which focuses on shaping children's word approximations whilst expanding their expressive and receptive vocabulary (Crosbie 2005).
-
Multi‐modal communication approaches. These methods are used for children who are minimally verbal to help them communicate and reduce the frustration associated with their speech disability. Devices may include a computer, phone or tablet with applications to help children produce words, phrases and sentences. Other methods involve gesture, sign language or use of visual picture boards.
Why it is important to do this review
There is a need for clinicians and parents to be aware of the most efficacious treatments for children with CAS. To date, studies in the field are largely non‐RCT (randomised controlled trials), single case series or case‐control studies that are generally positive in stating improvements in speech post‐therapy across motor (e.g. Baas 2008; Ballard 2010; Edeal 2011; Hall 1989; Kadis 2014; McCabe 2014; Strand 2000; Strand 2006), linguistic (e.g. McNeill 2009a; McNeill 2009b; McNeill 2010; Stokes 2010; Zaretsky 2010), and multi‐modal communication approaches (e.g. Harris 1996; King 2013; Tierney 2016). Yet these non‐RCT studies are inherently biased in nature and there is a need in the field for a systematic evaluation of available evidence. This review identifies best available treatments for CAS. This is an update of a Cochrane Review first published in 2008 (Morgan 2008). The previous review revealed no available RCTs for review. The first RCT in this field was published in 2015, hence it was timely to provide an updated review.
Objectives
To assess the efficacy of interventions targeting speech and language in children and adolescents with CAS as delivered by speech and language pathologists/therapists.
Methods
Criteria for considering studies for this review
Types of studies
RCTs and quasi‐RCTs (e.g. studies in which participants are allocated to intervention groups on alternate days).
Types of participants
Children aged 3 to 16 years with a diagnosis of CAS made by a speech and language pathologist/therapist.
Types of interventions
See Description of the intervention section above.
Eligible control groups were no treatment control (e.g. wait‐list control), treatment as usual, or other treatment controls.
Types of outcome measures
Primary outcomes
-
Accuracy of production on treated or non‐treated* items (may be associated with motor‐based, linguistic or multi‐modal communication approaches noted under How the intervention might work)
A desirable outcome would have been an improvement in accuracy of speech or multi‐modal communication, while an undesirable outcome would have been deterioration from baseline.
*Non‐treated items are stimuli (e.g. syllables, words, phrases) that have not been practised by children during intervention sessions. They are a form of control whereby we are able to measure children's performance on 'treated' items (e.g. syllables, words, phrases the child has practised during speech sessions) and compare it with performance on 'non‐treated' items. In this way, we can quantify whether the child has 'generalised' their newly acquired speech skills, or improvement in speech, to non‐treated stimuli, or whether they have only improved on speech items practised during therapy.
Secondary outcomes
-
Speech production consistency across repeated words and syllables (may be associated with motor‐based, linguistic or multi‐modal communication approaches noted under How the intervention might work)
-
Accuracy of connected speech, including co‐articulation accuracy (e.g. syllable segregation, voice onset time; most commonly associated with motor‐based or linguistic approaches noted under How the intervention might work)
-
Functional communication (e.g. child‐ or parent‐based questionnaire; may be associated with motor‐based, linguistic or multi‐modal communication approaches noted under How the intervention might work)
A desirable outcome would have been an improvement on outcomes one to three, whilst an undesirable outcome would have been deterioration from baseline on outcomes one to three.
Outcome measurements were recorded before, immediately after and at longer‐term follow‐up.
Search methods for identification of studies
Electronic searches
Margaret Anderson, Cochrane Information Specialist for the Developmental, Psychosocial and Learning Problems Group, conducted the searches for this update in August 2011, June 2014 and April 2017. We searched the following list of sources which includes bibliographic databases, and international and national trials registers. We did not apply any date restrictions, but we only examined articles written in the English language. We report the search strategies for this update in Appendix 1. Earlier search strategies are in Appendix 2.
-
Cochrane Central Register of Controlled Trials (CENTRAL; 2017, Issue 3) in the Cochrane Library, and which includes the Cochrane Developmental, Psychosocial and Learning Problems Specialized Register (searched 6 April 2017)
-
Ovid MEDLINE (1946 to March week 5 2017)
-
Ovid MEDLINE E‐Pub Ahead of Print (searched 6 April 2017)
-
Ovid MEDLINE In Process & Other Non‐indexed Citations (searched 6 April 2017)
-
Embase Ovid (1980 to 2017 week 15)
-
CINAHL EBSCOhost (Cumulative Index to Nursing and Allied Health Literature; 1937 to 10 April 2017)
-
PsycINFO Ovid (1806 to April week 1 2017)
-
PsycINFO EBSCOhost (1887 to 4 August 2011)
-
ERIC EBSCOhost (Education Resources Information Center; 1966 to 10 April 2017)
-
ERIC Proquest (Education Resources Information Center; 1966 to 6 June 2014)
-
Cochrane Database of Systematic Reviews (CDSR; 2017, Issue 4) part of the Cochrane Library
-
Database of Abstracts of Reviews of Effect (DARE; 2015, Issue 2) part of the Cochrane Library (not searched in previous version of review (Morgan 2008). Final issue published in 2015)
-
SpeechBITE (speechbite.com; searched 10 April 2017)
-
Australian New Zealand Clinical Trials Registry (ANZCTR; www.anzctr.org.au/BasicSearch.aspx; searched 12 April 2017)
-
Chinese Clinical Trial Registry (ChiCTR; www.chictr.org.cn; searched 10 April 2017)
-
ClinicalTrials.gov (clinicaltrials.gov; searched 10 April 2017)
-
EU Clinical Trials Register (clinicaltrialsregister.eu; searched 10 April 2017)
-
ISRCTN Registry (www.isrctn.com; searched 10 April 2017)
-
Nederlands Trial Register (trialregister.nl/trialreg/admin; searched 10 April 2017)
-
World Health Organization International Clinical Trials Registry Platform (WHO ICTRP; www.who.int/ictrp/en; searched 10 April 2017)
Searching other resources
We searched the reference lists of included reports, and requested information on unpublished trials from authors of published studies and other experts, as well as information groups in the areas of speech and language therapy/pathology and linguistics.
Data collection and analysis
We were unable to use many of our preplanned methods (Morgan 2006), as only one study met the inclusion criteria (Criteria for considering studies for this review). This study was published in a peer‐reviewed journal and there are no other completed RCTs or quasi‐RCTs at this time, published or unpublished. See Appendix 3 and Morgan 2006.
Selection of studies
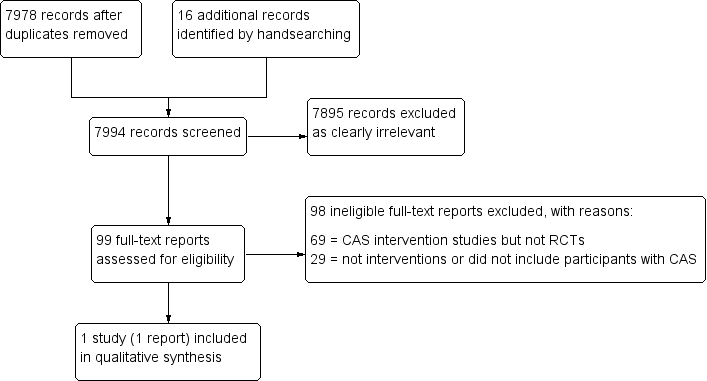
Two review authors (FL and AM) independently screened all titles and abstracts yielded by the search for eligibility. In cases of uncertainty over whether an abstract met the inclusion criteria, we obtained the full‐text report. Next, the same two reviewers independently evaluated each full‐text report against the inclusion criteria (Criteria for considering studies for this review). In the event of disagreement over inclusion of a particular paper, FL and AM reached consensus by re‐assessing the study against the inclusion criteria together. We present the results of our selection process in a PRISMA diagram; see Figure 1 (Moher 2009).
Study flow diagram
Data extraction and management
In addition to outcome data, we documented the following information using a data management form: participant details; setting (e.g. community clinic, school); type of intervention; length and frequency of intervention; professions involved; duration of impairment; level of severity; co‐morbidity; and assessment tools employed. We requested any information that was missing or unclear from the corresponding author (Dealing with missing data). AM independently extracted and entered the outcome data into Review Manager 5 (Review Manager 2014), and FL then independently evaluated the data and entries. AM and FL discussed any disagreements until they reached a consensus. EM entered further details of excluded studies into Table 1.
| Study | Participants | Methodology/paper type | Intervention | Intervention approach | Intervention intensity and duration | Outcome measures | Treatment outcomes | Timing of outcome measures | Methodological considerations |
| 1 male aged 12.8 years with CAS and charge syndrome | Not quasi‐/RCT (Single case (AB) design) | Dynamic Temporal and Tactile Cueing | Motor | Phase I and II: sessions 4 × per week; Phase III: weekly therapy. Study over 25 months. Home practice not reported | Articulation accuracy on 2‐item scale for treated items; speech rate | Phase I (core vocabulary): change on 4/6 targets. Maintained at last probe. Phase II (core vocabulary): reached 100% accuracy for 3/5 words. Reduction of stereotypies. Phase III: decreased speech rate from 94 to 71 SPM | Baseline and during treatment. No longer‐term follow‐up data | Lack of experimental control, multiple baselines, control, longer‐term follow‐up or generalisation data. Clinical file data used. No replication across participants. Assessors, participants, therapists not blinded | |
| 3 siblings (2 males, 1 female) aged 7.8 and 10.10 years with CAS | Not quasi‐/RCT (Single subject multiple baseline design across behaviours and participants) | Rapid Syllable Transition Treatment (ReST) | Motor | 60‐minute sessions (100‐120 trials per session), 4 × per week for 12 sessions. Home practice not reported | Reading aloud 10 treated and 10 non‐treated non‐word strings; real word generalisation data; perceptual analysis of prosodic pattern and acoustic analysis using pairwise variability index | 3/3 had significant gains in treated items and generalisation to same level of treated complexity. 2/3 generalised to lower and higher complexity non‐word items. Minimal generalisation to real words | Baseline data taken at beginning of every 4th session and at 4 weeks post‐treatment | No long‐term follow‐up data. Limited participants for generalisation of outcomes. No blinding of assessors, participants or therapists. No stimulus generalisation measures | |
| 1 female aged 3 years with CAS | Not quasi‐/RCT (Case description) | Music therapy | Other (alternative interventions) | 30‐minute sessions over 9 months. 24 sessions in total | Descriptive data only | Commenced non‐verbal. At end, had 11 phonemes in inventory | Pre‐treatment and post‐treatment. No follow‐up data | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No replicable outcome measures. No statistical analysis. No blinding of assessors, participants or therapists. No follow‐up or generalisation data. Unclear which aspect of treatment provided outcomes or affect of maturation, schooling, etc. No replication across participants. No long‐term follow‐up data | |
| 2 males aged 4.2 and 4.4 years with CAS and language disorder | Not quasi‐/RCT (Single case multiple baseline across participants) | Aided AAC Modeling | Augmentative and alternative communication | 15‐minute sessions, 1 to 3 × per week for 10 to 15 sessions | Frequency of use of multi‐symbol messages in play scenarios | Significantly more frequent use of multi‐symbol messages using aided AAC as well as different types of messages. Maintained and generalised gains. Increased participation | Baseline × 3, every 2nd treatment session, and at 2, 4 and 8 weeks post‐treatment | CAS diagnosis unclear and not replicable. Limited outcome measures. No blinding of assessors. No response generalisation data taken (only stimulus generalisation) | |
| 1 female (Latino) aged 3.4 years with CAS and suspected velocardiofacial syndrome | Not quasi‐/RCT (Single case multiple baseline across participants) | Aided AAC Modeling | Augmentative and alternative communication | 10‐minute sessions, 1 to 3 × per week for 10 to 15 sessions | Frequency of use of multi‐symbol messages in play scenarios | Significantly more frequent use of multi‐symbol messages using aided AAC. Parental response to training excellent. Maintained and generalised gains | Baseline × 3, every 2nd treatment session, and at 2, 4 and 8 weeks post‐treatment | CAS diagnosis unclear and not replicable. No blinding of assessors. No response generalisation data taken (only stimulus generalisation) | |
| 1 female aged 6 years with CAS and language disorder | Not quasi‐/RCT (Single case multiple baseline across behaviours) | Aided AAC Modeling | Augmentative and alternative communication | 15‐minute sessions, 1 to 3 × per week for 10 to 15 sessions | Frequency of use of grammatical morphemes | Significantly more frequent use of grammatical morphemes using aided AAC. 2nd intervention period needed for 2/3 targets. Maintained gains | Baseline × 3, every treatment session, and 2, 4 and 8 weeks post‐treatment | CAS diagnosis unclear and not replicable. No blinding of assessors. No response generalisation data taken (only stimulus generalisation) | |
| 1 male aged 6.6 years with CAS, hemiplegia and seizures | Not quasi‐/RCT (Single case (ABA) design) | Voice output devices (Macaw) | Augmentative and alternative communication | 60‐minute sessions for 2 sessions (training). Home practice focus | Frequency of appropriate responses to questions in structured discourse | Mother provided greater frequency and type of questions. Frequency of appropriate responses increased | 2 × baseline, 2 × practice period, 1 × post‐treatment, and 4 weeks post‐treatment | Lack of experimental control, multiple baselines or control data. | |
| 1 male and 1 female aged 12 and 8 years respectively diagnosed with CAS. Additional 8 children (7 males) aged 4 to 7 years with persistent articulation errors | Not quasi‐/RCT (Case series ‐ single group study) | Electropalatography (EPG) on /t, d, k, g, s, z/ | Motor | 30‐minute sessions, 1 × per week for 10 weeks | Per cent consonants correct (PCC) and Probe Scoring System (PSS) on probe of 43 words | Significant difference noted for PSS for whole group. PCC scores improved in percentage | Pre‐treatment (baseline first session) and post‐treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No follow‐up or generalisation data. No blinding of assessors | |
| 1 female aged 8 years with CAS and intellectual disability | Not quasi‐/RCT (Single case (ABA) design) | Partners in Augmentative Communication Training (PACT) | Augmentative and alternative communication | 30 to 90‐minute sessions daily after 3 days of intensive training. Home practice focus | Ratio of parent vs participant messages; ratio of successful/intelligible messages from child | Participant had greater frequency of messages compared to parent, and slightly higher frequency of successful measures (high baseline accuracy). Increased participation | Pre‐treatment and 2 months post‐treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 2 females and 1 male aged 3.4, 8 and 12.9 years respectively, with CAS (2 with intellectual disability and 1 with submucous cleft) | Not quasi‐/RCT (3 case studies/reports) | Combined communication boards and voice output devices | Augmentative and alternative communication | 3.4‐year‐old: 2 to 3 × per week for 12 weeks 8‐year‐old: daily for 6 months 12‐year‐old: not reported | 3.4‐year‐old: MLU. 8‐year‐old: assessment of phonological processes; communication repairs. 12‐year‐old: description of functional communication | 3.4‐year old: minimal speech improvement, MLU increased to WNL 8‐year old: no change in speech, parent report of greater communication repairs, and less frustration 12‐year old: supplemented natural speech to initiate, maintain and repair communication | Pre‐assessment and treatment descriptions | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 3 males and 1 female aged 3.6 to 6 years diagnosed with CAS | Not quasi‐/RCT (Single subject (ABB or ABC) design) | Prompts for Restructuring Oral Muscular Phonetic Targets (PROMPT) ‐ full programme (FP) for 8 weeks versus PROMPT without tactile‐kinaesthetic‐proprioceptive cueing for 4 weeks and FP for 4 weeks | Motor | 50‐minute session, 2 × per week for 8 weeks | Trained words on probe, untrained words. Pre‐post testing on the DEAP, TOCS+, VMPAC focal motor and sequencing subtests and Vineland socialization scales | 2/4 improved on DEAP. 4/4 improved on TOCS+, VMPAC subtests and Vineland. All 4 showed greater improvement on easier targets and majority maintained to 3 months post‐treatment. Generalisation to untrained items noted | Probe words: baseline × 3, treatment × 4, post‐treatment, and 3 months post‐treatment | Lack of experimental control as control data changed and interpreted as generalisation but no other control used (e.g. multiple baselines). CAS diagnosis concerning prosody unclear. Blinded assessors for only some outcomes. No withdrawal period between treatment phases and participant differences made comparison between conditions difficult. All measures not taken at consistent times | |
| 2 males aged 6.2 and 3.4 years with CAS (1 case with repaired cleft lip and palate and language disorder) | Not quasi‐/RCT (Single case (AB) design) | Integral Stimulation (Dynamic Temporal and Tactile Cueing) | Motor | Varied across participants. 40‐minute sessions (15 minutes each condition plus probes). 1 case: 3 × per week for 11 weeks. | Probe data on targeted phonemes (articulation) in words for each participant. 1 phoneme targeted with high production frequency = 100 trials and another with moderate production frequency = 60 trials. Articulation and language sample taken at 2 weeks post‐treatment | Large effect sizes for high production frequency and moderate for moderate production frequency. Improvement in PCC and phoneme inventory post‐treatment. Some generalisation | Baseline × 3, each treatment session, and 1 probe post‐treatment | Lack of experimental control, multiple baselines or control data. No long‐term follow‐up data. No blinding of assessors. Accuracy based on if target phoneme was correct (including cognate pair substitution) not if whole word was correct | |
| 1 female aged 9 years with mild CAS (followed until 12 years) | Not quasi‐/RCT (Case study/report) | Articulation therapy, motor‐programming remedial model | Motor | 5 school semesters | Templin‐Darley Tests of Articulation | Remediation of all 31 items for /r/, /ɝ/ and /ɚ/ | Test completed each semester | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 1 male aged 5 years with CAS and language disorder | Not quasi‐/RCT (Multiple baseline across discourse contexts) | Computer‐based AAC | Augmentative and alternative communication | 4‐minute sessions, 2 × per week for 22 sessions over 4 months | Frequency of noun/verb phrases in reciprocal book reading and structured discourse | Improvement in both contexts but more so in book reading than discourse. Some generalisation | Baseline, treatment, and withdrawal probes | CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. No follow‐up data. No blinding of assessors. No replication across participants | |
| 3 children (2 males, 1 female) aged 2.9 to 8 years with CAS | Not quasi‐/RCT (Case study series) | Melodic Intonation therapy (MIT) | Linguistic and motor | Varied. 37 to 71 sessions | Varied. Description of skills, consonant inventories, sequencing error rates and intelligibility compared to typical development | Child 1: all consonants in inventory Child 2: spoke in complex sentences, poor intelligibility, and articulation errors present. Child 3: sequencing error rate dropped from 75% to 22%. 13/18 consonant sounds improved | Pre‐ and post‐treatment | No experimental control. Lack of information on diagnosis of CAS. Primarily descriptive measures ‒ not reliable or tested using statistics. No control, maintenance or generalisation data | |
| 4 children (2 males, 2 females) aged 3.7 to 6.10 years with CAS | Not quasi‐/RCT (Single case design) | Stimulability (STP) and modified Core Vocabulary (mCVT) used concurrently | Linguistic and motor | 55‐minute sessions (10 minutes STP, 45 minutes mCVT), 2 × per week for 20 sessions. No home practice | Per cent phonemes correct, phonetic inventory and inconsistency | PCC increased on average 20% after combined therapy (range 9% to 32%). Inventory gained 5 phones on average (range 1 to 10). 3/4 had greater consistency on CSIP and ISP after therapy; 1 had greater inconsistency | Pre‐ and post‐ treatment | Poor experimental control as stable baseline not established, lack of control data. CAS diagnosis unclear and not replicable. No statistical analysis. No blinding of assessors. No immediate post‐treatment data or generalisation data | |
| 1 male aged 5.5 years with "some dyspraxic features" (CAS diagnosis not explicit) | Not quasi‐/RCT (Case study) | Sensory integrative therapy and speech therapy | Motor | Daily sessions for 2 months | (SP only) Illinois Test of Psycholinguistic Abilities | Test not completed post‐treatment. Observation of greater self‐monitoring and correction of speech | Pre‐treatment only | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures and no post‐treatment data. | |
| 14 children (9 males, 5 females) aged 3 to 6 years with diagnosed CAS (compared to 14 age‐matched controls) | Not quasi‐/RCT (Case series pre‐post design) | Prompts for Restructuring Oral Muscular Phonetic Targets (PROMPT) | Motor | 2 × per week for 8 weeks (16 sessions in total) | GFTA2, HCAPP, VMPAC, MRI | Significant gains as a group for all speech measures | 1‐week pre‐treatment (baseline), 1‐week post‐treatment | CAS diagnosis unclear and not replicable. Age‐matched control group older than CAS group. Limited information on PROMPT targets selected for replication. No blinding of assessors. No stimulus generalisation measures | |
| 3 males aged 4.1, 5.8 and 8.6 years diagnosed with CAS. 1 of the 3 diagnosed with Opitz FG syndrome and another with PDD‐NOS | Not quasi‐/RCT (Single subject multiple baseline across participants design) | Integrated Multimodal Intervention (structured book reading, drill and play activities with AAC devices present and speech encouraged) | Augmentative and alternative communication | 1‐hour sessions, 2 × per week for 3 to 6 weeks | Category (e.g. vocalisation, AAC or both), type of word and accuracy targets. Case 1: final consonants. Case 2: initial /s/ clusters then /f/. Case 3: initial /s/ clusters | Increases in vocalisations/spoken speech noted for 3/3. Speech accuracy improved on targets for 1/3 cases but all showed some generalisation to more accurate everyday speech | Baseline probes, probes every 2nd treatment session, 1‐month post‐treatment | Poor experimental control for case 1 and some change on control data noted. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 1 female aged 5.6 years with CAS | Not quasi‐/RCT (Case description) | Adapted Cueing Technique | Motor | 30 minutes of therapy per day for 6 months | Number of single words/utterances | From 2 to 4 words to 12 words and several carrier phrases. After 6 months began to produce novel sentences | Description of progress during treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 2 males aged 5 and 6 years diagnosed with CAS | Not quasi‐/RCT (Single case (ABAA) design) | Concurrent Melodic Intonation Therapy (MIT) and traditional therapy (20% and 80% of sessions respectively) | Linguistic and motor | 2 × per week over 2‐month period | Pre‐ and post‐treatment gains on word‐morpheme usage, auditory comprehension, naming, describing function, sentence completion, imitation of word phrases and articulation. Tested using language sampling and Porch Index of Communicative Ability in Children | Significant gains were found in phrase length (MLU), picture naming, and verbal imitation tasks. Little change in articulation | Pre‐treatment, post‐traditional therapy, and post‐MIT therapy | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. | |
| 2 males aged 5 and 6 years with suspected CAS | Not quasi‐/RCT (Single case (AB) design) | Melodic Intonation Therapy (MIT) compared to 'traditional speech‐language therapy' | Linguistic and motor | Ongoing 1 × per week speech therapy (traditional articulation sessions) and 40‐minute MIT music sessions over 4 weeks (both treatments concurrent) | GFTA2; KLPA2 and speech production on stimulable sounds in 1‐ or 2‐syllable words | Case 1 made greater gains in MIT sessions (but only 2% gain). Case 2 made greater gains on traditional articulation therapy (15% gain) | Pre‐ and post‐ treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 1 German‐speaking male aged 2.7 years with severe CAS | Single case design (A‐B design with 3 follow‐up assessments post‐treatment with some treatment sessions between assessments) | Speech Generating Devices ‒ fixed display (Gotalk 20+) and dynamic display (DynaVox V) | Augmentative and alternative communication | 45‐minute sessions × 50 treatment sessions. Treatment sessions 2 to 28 days apart | Means of communication (oral versus SGD), intelligibility of speech productions, consistency of speech productions, lexical development, and grammatical development | Significantly more communication initially with SGD than speech; significant increase in speech intelligibility; consistency (however reduced data in baseline period); amount of words used; and increased MLU and inflections after 8 to 9 sessions | Baseline × 3, every 2nd treatment session, and 2, 4 and 8 weeks post‐treatment | Lack of baseline data for consistency. CAS diagnosis unclear and not replicable. No blinding of assessors. No clear withdrawal phase after treatment with SGDs for control and no generalisation data | |
| 1 female aged 5.1 years with CAS | Not quasi‐/RCT (Single case cross‐over design) | Intra‐oral stimulation and electropalatography | Motor | 25‐minute sessions (5 minutes intra‐oral stim, 20 minutes EPG); daily at home, total of 195 sessions in 12 months | Per cent consonants correct, per cent phonemes correct, per cent words correct, intelligibility, visual deviancy | Significant treatment outcomes on all measures | Pre‐testing, A1 (baseline), B (intervention: oral stimulation therapy), A2 (withdrawal for 3 months), B (intervention: EPG), and A3 (follow‐up) | Cross‐over design, no control group or data taken to control for maturation. No replication across participants. No long‐term follow‐up or generalisation data taken | |
| 4 children (2 males, 2 females) aged 5.4 to 8.4 years with CAS (2 also with dysarthria and a third with language disorder); 3 also in Maas 2012b, as below | Not quasi‐/RCT (Single case alternating treatments design with multiple baselines across behaviours over | Dynamic Temporal and Tactile Cueing (high versus moderate feedback frequency in cross‐over design) | Motor | 50‐minute sessions 3 × per week for 3 participants but 1 had 60‐minute sessions 2 × per week | Per cent accuracy on 2‐point scale of segmental and suprasegmental aspects of target words and phrases with 2 words | 2 responded better to low frequency feedback, 1 to high frequency feedback, and 1 to no condition. No generalisation effects | Weekly probes: 3 to 4 × baseline, 4 × treatment. Phase 1: 4 to 5 × withdrawal, 4 × treatment. Phase 2: 2 × withdrawal and 1 month post‐treatment | Small sample size with heterogeneity. Cross‐over conditions made comparison difficult regarding targets chosen. No control group. Effect sizes used not interpretable or comparable to others. Different doses across all participants. Treatment fidelity < 80%. No stimulus generalisation measures | |
| 4 children (2 males and 2 females) aged 5.0 to 7.9 years with CAS. 2 cases had additional dysarthria diagnoses. 1 other case had multiple co‐occurring disorders | Not quasi‐/RCT (Single case alternating treatments design with multiple baselines across behaviours over | Dynamic Temporal and Tactile Cueing (random versus blocked practice compared in cross‐over design) | Motor | 2 × 4 week blocks of therapy | Per cent accuracy on 2‐point scale of segmental and suprasegmental aspects of entire target words and phrases with 2 words | 3/4 responded to both conditions. 2 responded relatively better to blocked practice, 1 to random practice, and 1 to no condition. 2/4 demonstrated generalization | Weekly probes: 3 to 4 × baseline, 4 × treatment. Phase 1: 4 to 5 × withdrawal, 4 × treatment. Phase 2: 2 × withdrawal and 1 month post‐treatment | Small sample size with heterogeneity. Cross‐over conditions made comparison difficult regarding targets chosen. No control group. Effect sizes used not interpretable or comparable to others. Treatment fidelity < 80%. No stimulus generalisation measures | |
| 1 female aged 4.7 years with CAS | Not quasi‐/RCT (Multiple baseline across behaviours ‐ cross‐over treatment design) | Combined Melodic Intonation Therapy (MIT) and Touch Cue Method (TCM) | Motor and linguistic | 3 sessions for 6 weeks for 18 sessions for MIT. 6 weeks no therapy. 3 sessions for 6 weeks for 18 sessions for TCM | Articulation accuracy: PVC, PCC. Also, overall word accuracy scores: PMLU, PWP, PWC. All calculated from responses to 46 picture cards | 1/5 measures significant post‐MIT (per cent vowels correct). Per cent consonants correct also reduced. 3/5 significant post‐TCM (PVC, PCC, PMLU). PVC, PCC and PMLU maintained. Greater changes for both therapies after withdrawal. PCC and PMLU only significant after MIT withdrawn | Beginning and end of 6‐week baseline, beginning and end of both treatment phases, 12 weeks after TCM withdrawn | Lack of experimental control of other factors. Cross‐over design makes comparison of both treatments difficult as many changes only noted after withdrawal of MIT (accumulation effects). Limited outcome data. Lack of generalisation data No blinded assessors. No replication across participants | |
| 12 children (sex unknown) aged 3 to 10 years with CAS (11 with co‐occurring conditions) | Case series (pre and post design) | DuBard Association Method®. It is a multimodal, phonetic therapy which works from accurate sounds in isolation | Motor | Daily in small groups in a school programme for an 11‐month period | Articulation, mean length of utterance (MLU), and intelligibility on Arizona Articulation Proficiency | Significant changes in articulation, intelligibility and MLU, and some resilience measures over 2‐year period | Pre‐ and post‐ treatment | Lack of experimental control regarding maturation effects (despite using the Intervention Efficiency Index and Proportional Change Index) and lack of control of covariate, including other potential intervention over the same period. No control group. No follow‐up or generalisation data | |
| 4 males aged 5.5 to 8.6 years with CAS. 2 children had additional auditory processing impairments | Not quasi‐/RCT (Single case (AB) design with 1 month follow‐up) | Rapid Syllable Transition Treatment (ReST) | Motor | 60‐minute session, 4 × per week for 3 weeks (12 sessions in total). Minimum of 1200 trials per session | Articulation, prosodic and simultaneous articulation and prosodic accuracy on trained and untrained probe pseudo words; PCC, PVC and per cent lexical stress matches from connected speech; PPVT‐4 as control data | All 4 participants increased perceptual accuracy. 1/4 participants showed change in untreated items. All participants showed change in prosody (average prosody gain 58%, 3/4 in PVC and 2/4 in PCC; average gain 79%). Control data (receptive vocabulary on PPVT‐IV) changed minimally | Baseline × 2, probes in treatment × 2, 1 month follow‐up | There was no immediate post‐treatment data taken to determine treatment effects, the follow‐up data was 1 month post‐treatment and included a withdrawal phase. There was no statistical analysis of connected speech data. 1 participant reached ceiling. No blinding of assessors. No stimulus generalisation measures | |
| 12 children (9 males, 3 females) aged 4.2 to 7.6 years with CAS | Not quasi‐/RCT (Case series design) | Integrated Phonological Awareness Intervention | Linguistic | 45‐minute session; 2 × per week for 6 weeks in 2 blocks with 6‐week withdrawal between blocks. Total of 245 sessions | Trained speech accuracy and phonological awareness accuracy on a probe. Generalisation‐ BTOPP and first trial of DEAP inconsistency subtest for PVC, PVC and inconsistency score. PIPA for 4‐year‐olds. TOPA for 5 to 7‐year‐olds. Burt Word Reading Test for non‐word reading and informal non‐word reading probe (Gillon 2000). Per cent grapheme correct score in spelling 10 words from DEAP inconsistency subtest | Speech: 9/12 children improved on trained items. Phonological awareness: 8/12 children improved in 1 or both intervention blocks. Generalisation for 8/12 on all measures except Burt Word Reading Test | Pre‐ and post‐treatment | Lack of experimental control, control group or control data. CAS diagnosis unclear regarding prosody. Limited information provided on each participant. Limited treatment phase data. No maintenance data. No blinding of assessors | |
| 2 male identical twins aged 4.5 years with CAS (deletion at 10q21.2‐22.1) | Not quasi‐/RCT (Single case design) | Integrated Phonological Awareness intervention | Linguistic | 45‐minute session; 2 × per week for 6 weeks in 2 blocks with 6‐week withdrawal between blocks. Total of 245 sessions | PPC, PVC on BTOPP, and DEAP inconsistency percentage. PIPA, PhonRep, Burt Word Reading, Non‐word Reading, Neale accuracy and comprehension | PCC and PVC improved at post‐treatment and follow‐up. Reduced inconsistency. Sound‐letter knowledge increased from 0 to 7 at post‐treatment. Reading WNL and spelling demonstrated use of strategies at final follow‐up | Pre‐ and post‐ treatment, and 6‐month follow‐up | Lack of experimental control, control group or control data. CAS diagnosis unclear regarding prosody. Limited information provided on each participant. Limited treatment phase data. No maintenance data. No blinding of assessors. No stimulus generalisation measures | |
| 12 children (9 males, 3 females) aged 4.2 to 7.6 years diagnosed with CAS | Not quasi‐/RCT (12‐month follow‐up to 2009 case series) | Integrated Phonological Awareness intervention | Linguistic | As per McNeill 2009a | BBTOP and 1st trial of DEAP yielding PPC. PIPA for 4‐year‐olds & TOPA for 5 to 7‐year‐olds. Decoding measures (Burt Word Reading Test and Non‐word Reading Task) and spelling measures (probe of 10 words from the DEAP inconsistency subtest) were completed for participants at least 6 years of age at the beginning of the study. The NARA was administered for participants aged 5 years, 6 months and up | Significant difference for CAS group from pre‐ to post‐treatment on letter knowledge, non‐word reading probe, spelling, PCC, TOPA and Burt Non‐Word Reading. 3/7 improved on NARA to age‐appropriate level | 1‐year follow‐up to McNeill 2009a | 7/12 of original participants followed up. Whole group data ‒ case series. No control group or control data for experimental control or maturation effects | |
| 3 children (2 males, 1 female) aged 6.3, 6.10 and 7.3 years with CAS | Not quasi‐/RCT (Single case multiple baseline design across behaviours) | Integrated Phonological Awareness Intervention | Linguistic | 45‐minute sessions 3 × per week for 3 weeks | PPC on probe, phoneme segmentation probe, phoneme manipulation probes, initial sound identification probes, letter‒sound knowledge subtest from the PIPA, non‐word reading tasks | 2/3 significantly increased PPC, 2/3 significantly improved phonological awareness skills on probes, letter‒sound knowledge, and non‐word reading. Limited transfer to untreated words | Baseline and post‐treatment (3 probes each) | Lack of control group and control data. CAS diagnosis unclear regarding prosody. Lack of multiple baseline data throughout treatment. No long‐term follow‐up. No blinding of assessors | |
| 12 children (9 males, 3 females) aged 3 to 6 years with speech sound disorders | Not quasi‐/RCT (Case series pre‐post design) | Prompts for Restructuring Oral Muscular Phonetic Targets (PROMPT) | Motor | 45‐minute session 2 × per week for 8 weeks | GFTA2, HCAPP, VMPAC focal motor and sequencing subtests, Children's Speech Intelligibility Measure | Significant gains as a group for all speech measures | Baseline 1 week prior to treatment, and 1 week post‐treatment | Lack of experimental control, control group, multiple baseline or control data. No blinding of assessors. No blinding of assessors. No long‐term follow‐up | |
| 37 children (28 males, 9 females) aged 2.6 to 4.5 years with CAS | Not quasi‐/RCT (pre‐postgroup design) | Motor Speech Treatment Protocol (MSTP) | Motor | Intense treatment group: 45‐minute session, 2 × per week × 10 weeks = 20 sessions. Less intense group: 45‐minute session, 1 × per week × 10 weeks = 10 sessions | GFTA‐2 sounds in words subtest; speech intelligibility using Children's Speech Intelligibility Measure (CSIM) at word level, and Beginner's Intelligibility Test (BIT) at sentence level. Functional Outcomes for Children Under Six (FOCUS) scale | Intense group had greater changes in articulation and functional communication compared to the less intense group with large effect sizes. Mixed results were found for intelligibility: at word‐level (CSIM), both the less intense and 1/2 intense groups made a significant and large change. At sentence level, 1/2 intense groups made a significant change | Pre‐ and post‐ treatment | No control group or control data. Participants were not directly randomised; however, no between‐group differences were found at baseline. There were missing data (dealt with using intention‐to‐treat analysis). No information on session trials was obtained, which is important for intensity calculations | |
| 6 males aged 9 to 15 years with CAS. 1 child had additional ADHD and another child had additional dysarthria | Not quasi‐/RCT (Single case multiple baseline across behaviours across participants) | Ultrasound biofeedback (targeting articulation on clusters and CV or VC sequences of inaccurate phones) | Motor (instrumentally based) | 60 minute sessions, 2 × per week × 18 sessions (at least 150 trials per session) | Probe of whole‐word accuracy of treated and untreated items | U002 and U007 had significant gains on 2/4 treated combinations, U005 for 3/4, and U008, U009 and U012 had significant gains on all treated combinations. All exhibited some generalisation (target‐dependant). U005, U007, U008, U009, U012 demonstrated maintenance above pre‐treatment levels | Probes at baseline × 3, every treatment session, post‐treatment, and 2 months post‐treatment | No control group or comparison treatment. No blinding of assessors. Untreated items were not clearly selected as control or generalisation data with some showing change and others not | |
| 3 male children aged 11 to 13 years diagnosed with CAS and poor expressive language and phonological processing. 1 participant had additional flaccid dysarthria, ADHD, language and learning difficulties | Not quasi‐/RCT (Single case multiple baseline across behaviours (syllable positions)) | Ultrasound biofeedback (using structured chaining and principles of motor learning) | Motor (instrumentally based) | 1 hour sessions × 14 sessions. Sessions 1 to 7 addressed target 1 and sessions 8 to 14 addressed target 2 with randomly assigned prosody or no prosody conditions | Treatment acquisition data, generalisation probe of untreated words, maintenance to 2 months post‐treatment | 2/3 participants acquired accurate articulation. 0/3 demonstrated generalisation or maintenance | 3 × baseline probes, midway therapy probe, post‐therapy probe (within 1 week after treatment), and 2‐month follow‐up | No control group. Greater within‐treatment probes and post‐treatment probes would have allowed for greater statistical analysis. No control data. No blinding of assessors. No stimulus generalisation measures | |
| 3 males aged 11 to 14 years with CAS | Not quasi/RCT (Single case (ABA) design) | Ultrasound biofeedback (using structured chaining and principles of motor learning.) | Motor (Instrumentally based) | 2 × 1‐hour articulation treatment a day for 2 weeks. 16 hours of therapy in total. Over 100 trials per session | Treatment acquisition of /ɹ/, /s/ or /ʧ/. Generalisation to untrained items using a probe and sentence imitation task, and maintenance 1 to 3 weeks post‐treatment (audio‐samples submitted) | Case 1 had acquisition, generalisation, and maintenance of targets. Case 2 had some acquisition in the 2nd week of therapy and no generalisation and maintenance. Case 3 showed acquisition, limited generalisation to words and not phrases, and no maintenance | Probe conducted 1 × before treatment, at the end of the first week, and at the end of the second week (post‐treatment) | Lack of experimental control, multiple baselines or control data. No blinding of assessors. No long‐term follow‐up data. No stimulus generalisation measures | |
| 1 adult with CAS and class III malocclusion. Another 5 adults aged 18 to 23 years with persistent articulation disorders | Not quasi‐/RCT (Case series) | Orofacial myofunctional therapy | Motor (Instrumentally based) | 45‐minute session, 1 × per week for 6 weeks | Dworkin‐Culatta Oral Mechanism Examination for oral postures and intelligibility in single words, sentences, and spontaneous speech | All improved lips and tongue postures. 5/6 participants increased intelligibility. No improvement in intelligibility for person with DVD | Pre‐ and post‐treatment | Lack of experimental control, multiple baselines or control data. No treatment data or follow‐up reported. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 1 female aged 9 years with CAS | Not quasi‐/RCT (Case study) | Intensive, systematic drill motor therapy | Motor | 22 sessions over 3 months | 20‐item probe of /r/ (target), ineligibility in spontaneous speech | /r/ improved from 0 to 20 correct in probe. Intelligibility judged by unfamilar listeners improved | Treatment sessions | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No follow‐up data. Only ancedotal generalisation data. No statistical analysis. No reliability of judgments reported. No replication across participants | |
| 4 children (3 males, 1 female) aged 10‐14 years diagnosed with CAS | Not quasi‐/RCT (Single subject (ABAB) design) | Rate Control Therapy | Linguistic and motor | 20‐minute session per reading passage. No further information available | Articulation accuracy (words read correctly) | Improved to 85% accuracy at 50% habitual rate and maintained in therapy as rate was slowly increased. Limited generalisation to conversation ‐ therapy implemented | Reading rate in 5‐minute intervals | Lack of control and follow‐up data. CAS diagnosis unclear and not replicable. No statistical analysis. No blinding of assessors. No stimulus generalisation measures. No report of data reliability | |
| 3 children (2 males, 1 female) aged 4 to 6 years diagnosed with CAS | Not quasi‐/RCT (Single case multiple baseline design across participants) | Concurrent treatment (using randomised variable practice) | Motor | Therapy until target sounds reached 80% accuracy. P1 had 26, P2 had 12 and P3 had 28 sessions. 2 × per week, 30 minutes per session and on average 100 to 115 trials per session | Per cent correct productions on /s, z, f, v/ trained targets during baseline and treatment; generalisation probes to untrained words and 3‐word phrases | All children reached 80% accuracy on target sounds. Moderate to large generalisation effects at word and 3‐word phrases levels (70% to 100% accuracy) | 3 × baseline probes, probes every 5 therapy sessions | No post‐treatment or follow‐up/maintenance data. No blinded assessors. No stimulus generalisation data. P3 continued regular school therapy during the study so could be a confounding factor. No stimulus generalisation measures | |
| 1 male aged 7 years with residual CAS | Not quasi‐/RCT (Single case (ABA) design) | Articulation with facilitative vowel contexts | Linguistic | 45‐ to 55‐minute session, 3 × per week for 3 weeks. 60+ trials per session. Home practice provided | Accuracy on 'sh' sound in word initial probe, 'tr' as control | Significant improvement in 'sh' articulation accuracy in trained and untrained words. No change in control words with 'tr' initial | Pre‐treatment, mid‐therapy × 2 (after sessions 3 and 6), post‐treatment, and maintenance (2 weeks post‐treatment) | Participant did not meet current CAS criteria. Lack of generalisation data beyond 'sh' sound. No blinded assessors. No replication across participants. No long‐term follow‐up data. No reliability of data reported | |
| 1 female aged 5 years with "severe motor planning deficits but no dysarthria" (CAS) | Not quasi‐/RCT (Single case multiple baseline design) | Integral stimulation | Motor | 30‐ to 50‐minute session, 3 to 5 × per week (1 to 2 × per day) for 10 to 16 sessions. No home practice | Articulation accuracy ratings on a 2‐point scale | Improvement from 0.25 to 0.80 on 2‐point scale. 4/5 treatment stimuli achieved rating of 2/2 by end of therapy | Treated stimuli at start of each session, control stimuli twice a week | No statistical analysis. Limited outcome measures. | |
| 4 males aged 5.5 to 6.1 years with CAS (2 with dysarthria and 1 with mild intellectual disability) | Not quasi‐/RCT (Single case multiple baseline across participants) | Dynamic Temporal and Tactile Cueing | Motor | 30‐minute sessions, 2 × per day for 5 days a week for 38 to 50 sessions | Articulation accuracy on a 3‐point scale | Treatment gains for 3/4 participants maintained by 2/4 | Baseline × 4 (or more, staggered baseline), 20+ treatment probes | No follow‐up or generalisation data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures | |
| 4 children (2 males, 2 females) aged 4.8 to 8 years with CAS | Not quasi‐/RCT (Single case multiple baseline across participants and behaviours) | Rapid Syllable Transition Treatment (ReST) | Motor | 50 minute sessions 2 × per week for 6 weeks. 100 trials per session | Accuracy on imitated (a) treated words, (b) untreated pseudo words, (c) untreated real words and control words | Significant improvement on treated words and untreated real words. Significant improvement for 2/4 participants on untreated pseudo words. No change in control items | Baseline × 3 to 6, treatment × 3, and 1 day, 1 month and 4 months post‐treatment | Use of GFTA2 for control items. No stimulus generalisation data | |
| 5 children (4 males, 1 female) aged 5 to 11 years with CAS (3 with mild or moderate receptive language disorder) | Not quasi‐/RCT | Rapid Syllable Transition Treatment (ReST) | Motor (instrumentally based ‐ telehealth) | 60‐minute session, 4 times a week for 3 weeks (12 sessions in total). Minimum of 1200 trials per session | Accuracy on treated pseud‐word items, generalisation to untreated non‐words and real words, and control items (articulation of rhotics) on a probe; client/family satisfaction with telehealth treatment | 5/5 participants demonstrated significant change in treated items. 4/5 maintained gains to 4 months post‐treatment. 4/5 had significant generalisation to untrained non‐words and real words, and 1/5 demonstrated change in control data (articulation errors of rhotics or /s/). Families very satisfied and motivated by telehealth treatment | At least 3 baseline probes, 3 therapy probes (sessions 5, 9 and 1 day post‐treatment). Follow‐up at 1 week, 4 weeks & 4 months post‐treatment | Missing data for some participants at certain time points in Table 3. Problems with change in control data. Some internet issues (dropouts, port sound quality, etc.) were observed in 61% of sessions; however, significant outcomes were found. No stimulus generalisation data | |
| 1 male aged 3 years with CAS and fine motor delay | Not quasi‐/RCT (Single case design; descriptive) | Multimodal therapy: Signed Exact English sign language, Sarah Rosenfeld Johnson's oro‐motor programme and Kaufman Speech Praxis Program | Augmentative and alternative communication | Clinic‐based sessions 45 minutes 1 to 2 × per week and home‐based sessions for 60 minutes 1 × per week | Language assessment; observations and Kaufman Speech Praxis Test; Verbal Motor | Receptive and expressive language consistently in average range but receptive relatively better than expressive language. By 3.6 years of age receptive and expressive language same level. Marked drooling and limited inventory and sequencing at 18 months, yet skills on Kaufman & VMPAC in average range at 3 years, 9 months. Discharged from therapy | Language assessment at 1.1 year, 3 years and 3.6 years. Kaufman test or observations at 1.6, 3 and 3.9 years. VMPAC at 3 years, 9 months | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable regarding prosody and drooling. No statistical analysis. | |
| 1 male aged 14 years with severe CAS and limb/motor apraxia and obsessive compulsive disorder | Not quasi‐/RCT (Case study) | Verbal Motor Learning (with Dynamic Distal Stabilization Technique (DDST)) | Motor | 1 × 30‐minute clinic session and 6 × home practice sessions a week for 4 weeks | (1) Producing highest pitch using /I/ sound with and without DDST, to determine minimum and maximum frequency and length using Speech Analyser 1.5 (2) Imitation of 18 words to analyse word length, maximum loudness, maximum and minimum frequency | Significant t‐test results for (1) increase in maximum frequency and length of pitch after DDST, no change in minimum frequency, and (2) decrease in word length (word said faster), maximum loudness, and maximum frequency | Pre‐ and post‐ treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 1 female aged 10 years with CAS and ASD | Not quasi‐/RCT (Case study) | Verbal Motor Learning (Initial Phoneme Cue (IPC) technique) | Motor | 2 × 1 hour sessions, 2 weeks apart (participant had initial therapy: 1‐hour session weekly for 1 year prior to this study) | Imitation accuracy of CVCV treated words either (a) with IPC or (b) without IPC | Imitation of CVCV was 0% to 22% accuracy and imitation with IPC was 96% to 100% accuracy | Pre‐ and post‐ treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. No statistical analysis. No blinding of assessors. No follow‐up or generalisation data. No replication across participants | |
| 10 children (no information on gender reported) aged 6 to 11 years with moderate to severe DAS | Not quasi‐/RCT (Case descriptions/file audit) | School‐based intervention | Motor | 25 to 307 hours of therapy | Articulation, polysyllable words and connected speech in speech samples. Intelligibility rated on a 9‐point scale | Significant improvement on articulation. Minimal generalisation to polysyllable words and connected speech. Intelligibility improved by at least 0.5 points | Pre‐ and post‐ treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. | |
| 1 female aged 11.6 years with CAS, intellectual disability and language disorder | Not quasi‐/RCT (Single case design) | Phonological awareness (phoneme‒grapheme mapping, reading comprehension, 'Basics' programme). Speech ‐ PROMPT and Moving Across Syllables | Linguistic | Between 6.0 and 11.6 ongoing weekly treatments ‐ 1 hour × 1:1 sessions and PROMPT institute over summer | Per cent accuracy on phonological awareness and decoding | Improvement seen in phoneme‒grapheme mapping, segmentation and short vowel identification. Some improvement in decoding | Ongoing 1 × per week sessions from 6.0 to 11.6 years | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. |
Participants: All participants are English speakers unless otherwise reported.
AOS: apraxia of speech; BBTOP: Bankson‐Bernthal Test of Phonology; CAS: childhood apraxia of speech; CSIP: consonant substitute inconsistency percentage; DAS: developmental apraxia of speech; DEAP: Diagnostic Evaluation of Articulation and Phonology; DVD: developmental verbal dyspraxia; GDD: global developmental delay; GFTA‐2: Goldman Fristoe Test of Articulation 2; HCAPP: Hodson Computerized Analysis of Phonological Patterns; ISP: inconsistency severity percentage; KLPA‐2: Khan‐Lewis Phonological Analysis, Second Edition; NARA: Neale Analysis of Reading Ability; PCC: percentage consonants correct; PDD‐NOS: pervasive developmental disorder ‐ not otherwise specified; PMLU: phonological mean length of utterance; PVC: percentage vowels correct; PWC: percentage words correct; PWP: proportion of whole‐word proximity; PIPA: Preschool and Primary Inventory of Phonological Awareness; RCT: randomised control trial; SSD: speech sound disorder; TOCS+: Test of Children's Speech Plus; TOPA: Test of Phonological Awareness; VMPAC: Verbal Motor Production Assessment for Children
Assessment of risk of bias in included studies
Two review authors (FL and AM) independently assessed the risk of bias within the one included study, using Cochrane's 'Risk of bias' tool (Higgins 2011a). Both review authors rated the risk of bias as low, high or unclear (uncertain), across each of the domains listed below. There were no cases of disagreement.
-
Sequence generation. Did the study describe the method used to generate the allocation sequence in sufficient detail to determine whether it produced comparable groups? In the review authors' judgment, was the sequence adequately generated?
-
Allocation concealment. Did the study describe the method used to conceal the allocation sequence in sufficient detail to assess whether intervention schedules could have been foreseen in advance of, or during, recruitment? In the review authors' judgment, was allocation adequately concealed?
-
Blinding of participants and personnel. Did the study describe any measures used to blind participants and personnel from knowledge of which intervention a given participant might have received? In the review authors' judgment, was knowledge of the allocated interventions adequately concealed from participants and relevant personnel during the study?
-
Blinding of outcome assessment. Did the study describe any measures used to blind outcome assessors from knowledge of which intervention a given participant might have received? In the review authors' judgment, was knowledge of the allocated interventions adequately concealed from all outcome assessors during the study?
-
Incomplete outcome data. Did the study report data on attrition and exclusions as well as the numbers involved (compared with total randomised), reasons for attrition/exclusion, and any re‐inclusions in analyses performed. In the review authors' judgment, did the study authors deal adequately with incomplete data?
-
Selective outcome reporting. Did the study make attempts to assess the possibility of selective outcome reporting? In the review authors' judgment, are reports of the study free of suggestion of selective outcome reporting determined by comparing the outcomes listed in the original study protocol with the final RCT publication?
-
Other sources of bias. Was the study apparently free of other problems that could put it at a high risk of bias? In the review authors' judgement, was the study free of other problems not covered by the domains above?
Measures of treatment effect
We were unable to conduct a meta‐analysis due to there being only one included study. We have archived our methods for use in future updates of this review (see Appendix 3; Morgan 2006).
Unit of analysis issues
For each outcome measure, we averaged the accuracy of production (e.g. number of correct items from total items elicited) across the group. Units were mean accuracy scores for each intervention group. See Appendix 3 for additional methods archived for use in future updates of this review.
Dealing with missing data
There were missing data for 1/26 participants in the Murray 2015 RCT, due to a participant withdrawing in the middle of treatment (see Appendix 3 and Morgan 2006).
Assessment of heterogeneity
We were unable to assess heterogeneity as only one study met the inclusion criteria (see Appendix 3 and Morgan 2006).
Assessment of reporting biases
We were unable to assess reporting biases due to there being only one included study (see Appendix 3 and Morgan 2006).
Data synthesis
We could not undertake a meta‐analysis as we included only one study in the review (see Appendix 3 and Morgan 2006).
Summary of findings
Using GRADEpro GDT (GRADEpro GDT 2015), we created a 'Summary of findings' table for the comparison: Nuffield Dyspraxia Programme ‐ Third Edition (NDP‐3) versus Rapid Syllable Transition Treatment (ReST) for Childhood Apraxia of Speech. In this table we report our primary (accuracy of production on treated and non‐treated items) and secondary (speech production consistency and accuracy of connected speech) outcomes for one month post‐treatment. We chose this time point as it is the most clinically salient time point. The time point immediately after therapy is not sufficient to determine whether the treatment effect was sustained. We did not examine the time point of four months post‐therapy because the number of participants in each group (NDP‐3: 9/13 participants; ReST: 9/13 participants) had returned to community SLP/SLT treatment between the one‐month and four‐month post‐therapy period and, as such, it would be difficult to delineate between a sustained treatment effect of the RCT versus the usual therapy re‐introduced. We also report in this table the quality ratings for each outcome as assessed by two review authors (AM and FL) using the GRADE approach (Schünemann 2017). They assigned ratings of high, moderate, low or very low quality, according to the presence of risk of bias (Risk of bias in included studies), indirectness of evidence, unexplained heterogeneity or inconsistency in results, imprecision of results and high probability of publication bias; they discussed any disagreements over the quality ratings until a consensus was reached.
Please see 'summary of findings Table for the main comparison' for an overview of treatment effects for each outcome measure and GRADE assessment of the quality of the evidence.
Subgroup analysis and investigation of heterogeneity
We were unable to perform any subgroup analyses as we included only one study in the review. See Appendix 3 and Morgan 2006.
Sensitivity analysis
We were unable to perform a sensitivity analysis as we included only one study in the review. See Appendix 3 and Morgan 2006.
Results
Description of studies
Results of the search
We identified a total of 7978 records once duplicates were discarded. EM identified a further 16 records through handsearching. Of these 7994 titles and abstracts, we excluded 7895 as clearly irrelevant, and assessed the full texts of the remaining 99 reports against our inclusion criteria (Criteria for considering studies for this review). From these 99 reports, only one study met our inclusion criteria for this review (Included studies); we excluded the remaining 98 reports as irrelevant (see Excluded studies). We did not identify any non‐English abstracts for inclusion. Please see Figure 1.
Included studies
The one included study, Murray 2015, was an RCT that compared treatment effects for two interventions, each delivered intensively (one hour for four days a week for three weeks): the Nuffield Dyspraxia Programme ‐ Third Edition (NDP‐3; Williams 2004) and the Rapid Syllable Transition treatment (ReST; Ballard 2010). Twenty‐six children (13 allocated to each therapy group), aged 4 to 12 years (18 males) with CAS diagnosed by a SLP/SLT participated in the study, which took place at the University of Sydney Communication Disorders Treatment and Research Clinic. The primary outcomes were per cent accuracy on treated and untreated pseudo‐words and real words and phrases.
The research was funded (as published in the article) by: Douglas and Lola Douglas Scholarship on Child and Adolescent Health; Nadia Verrall Memorial 2010; and Postgraduate Student Scholarship 2011 through Speech Pathology Australia, James Kentley Memorial Scholarship, Postgraduate Research Support Schemes and Faculty of Health Sciences; University of Sydney International Development Program Fund, and the Australian Research Council Future Fellowship.
Please see the Characteristics of included studies table for further detail of the nature of these interventions.
Excluded studies
We excluded 98 full‐text reports. Of these, 29 studies were either not interventions (e.g. diagnostic studies), or did not include participants with CAS (e.g. focused on other speech disorders or adult‐acquired apraxia of speech). The remaining 69 excluded papers were CAS intervention studies but were not RCTs, and are tabulated in Characteristics of excluded studies tables. Further detail on the excluded CAS studies is provided in Table 1.
Risk of bias in included studies
We examined the one included study, Murray 2015, for risk of bias. We judged the study to be at low risk of bias for all domains except 'other sources of bias', which we judged to be at unclear risk of bias. Please see the 'Risk of bias' table (beneath the Characteristics of included studies table) for further detail on the basis of our decisions, and Figure 2 for a summary of ratings.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Effects of interventions
See: Summary of findings for the main comparison
We downgraded the quality of the evidence by one level to moderate due to imprecision, given that only one RCT was identified.
Primary outcome: accuracy of production
The Murray 2015 study compared the number of real words produced correctly (out of the total elicited words) at pre‐treatment with one month post‐treatment for treated and non‐treated items.
Treated items
The study authors reported that, compared to pre‐treatment baseline, the NDP‐3 MD of 36.0 was greater than the ReST MD of 33.9 at one month post‐treatment, with an absolute mean difference of 2.1 between groups.
Non‐treated items
The study authors reported that, compared to pre‐treatment baseline, the ReST MD of 18.3 was minimally greater than the NDP‐3 MD of 18.2 at one month post‐treatment with an absolute mean difference of 0.1 between groups.
Secondary outcomes
Speech production consistency
The Murray 2015 study compared treatment gains in speech production consistency (measured by 25 real words repeated three times using the inconsistency subtest of the Diagnostic Evaluation of Articulation and Phonology (DEAP) test (Dodd 2006)), at pre‐treatment with one month post‐treatment for treated items. The study authors reported that, compared to pre‐treatment baseline, the NDP‐3 MD of 11.1 was minimally greater than the ReST MD of 10.9 at one month post‐treatment, with an absolute mean difference of 0.2 between groups.
Accuracy of connected speech
The Murray 2015 study compared treatment gains in the accuracy of connected speech (as assessed by imitated word accuracy in connected speech of at least three word combinations), at pre‐treatment with one month post‐treatment for treated items. The study authors reported that, compared to pre‐treatment baseline, the NDP‐3 MD of 14.3 was greater than the ReST MD of 11.5 at one month post‐treatment, with an absolute mean difference of 2.8 between groups.
The study did not measure functional communication.
Discussion
Summary of main results
We sought to investigate the effectiveness of targeted speech and language interventions for children and young people, aged 3 to 16 years of age, with a diagnosis of CAS made by a speech and language pathologist/therapist. We found only one study, Murray 2015, which met our inclusion criteria (Criteria for considering studies for this review). This RCT recruited 26 children aged 4 to 12 years, and compared two interventions: the Nuffield Dyspraxia Programme‐3 (NDP‐3); and the Rapid Syllable Transitions Treatment (ReST). Treatments were delivered intensively in one‐hour sessions, four days a week for three weeks, in a university clinic in Australia. Speech pathology students delivered the treatments in the English language.
We considered all core domains to be at low risk of bias. Both the NDP‐3 and ReST therapies demonstrated improvement at one month post‐treatment. A number of cases in each cohort had recommenced usual treatment by their speech and language pathologist between one month and four months post‐treatment (NDP‐3: 9/13 participants; ReST: 9/13 participants). Hence we could not analyse maintenance of treatment effects to four months post‐treatment without significant potential bias, and so we did not include this time point for further analysis in this review.
Overall there is limited evidence that, when delivered intensively, both the NDP‐3 and ReST may effect improvement in word accuracy in 4‐ to 12‐year‐old children with CAS, measured by the accuracy of production on treated and non‐treated words, speech production consistency and the accuracy of connected speech. The study did not assess functional communication. We are unable to say whether either treatment is better than the other, or better than no treatment or treatment as usual. No evidence currently exists to support the effectiveness of other treatments for children aged 4 to 12 years with idiopathic CAS, without other comorbid neurodevelopmental disorders. No formal analyses were conducted to compare NDP‐3 and ReST by the original study authors, hence one treatment cannot be reliably advocated over the other. Further RCTs replicating this study would strengthen the evidence, which we currently rate as low using the GRADE evidence rating system (i.e. that 'further research is very likely to have an important impact on our confidence in the estimate and is likely to change the estimate').
Further well‐controlled studies investigating the effectiveness of other treatments for CAS are also needed across other motor‐based therapies, and also across linguistic and multi‐modal approaches. As noted earlier in the Why it is important to do this review section, non‐RCT case series or case‐control studies examining motor, linguistic and multi‐modal interventions for CAS have described positive effects of intervention, but RCTs are required to strengthen the evidence base for these approaches. Further, there is also a need for trials that examine interventions for CAS compared to no treatment (e.g. wait‐list control group). A no‐treatment comparison is arguably difficult to achieve in this field however, given the typically severe presentation of speech disorder and reticence of parents or clinicians (or both) to withhold treatment from children. Finally, RCTs are also needed on populations with CAS and co‐occurring neurodevelopmental or medical disorders.
Cochrane Reviews are often criticised in the SLP/SLT field because they do not allow consideration of lower levels of evidence, such as case studies or case series, which are more commonly performed in the field. Recognising these concerns we have provided a summary of the observational studies of CAS interventions excluded from this review (see Table 1), to encourage future, rigorous and controlled investigation of the efficacy of these methods. The lack of RCT intervention data in the CAS field to date is reinforced by challenges of: (1) the low incidence of the disorder; (2) the lack of a universally applied diagnostic classification system; (3) a lack of understanding of the aetiology of CAS; and (4) the challenge of designing trials for children with co‐occurring clinical features (e.g. non‐verbal cognitive impairment) or disorders (e.g. intellectual disability, autism spectrum disorder).
Overall completeness and applicability of evidence
We identified only one small RCT for inclusion in this review, indicating that there is an urgent need for further RCTs in this field. The interventions examined are currently in use and therefore results are applicable to clinical practice.
Quality of the evidence
We considered the overall quality of the evidence to be moderate using the GRADE approach; see summary of findings Table for the main comparison. We downgraded the quality of the evidence by one level to moderate, due to imprecision, given that only one RCT was identified.
Potential biases in the review process
We carefully managed potential conflicts of interest, as described below under Contributions of authors and Declarations of interest. There is a possible risk of language bias given that we only included studies written in English.
Agreements and disagreements with other studies or reviews
There are no other systematic reviews examining only RCT and quasi‐RCT evidence for efficacy of treatment for CAS.

Study flow diagram
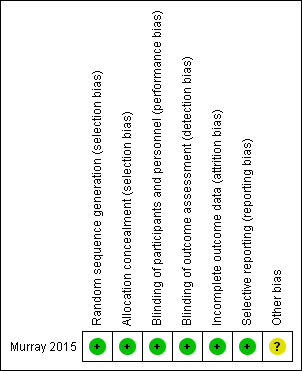
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
| Nuffield Dyspraxia Programme ‐ Third Edition (NDP‐3) versus Rapid Syllable Transition Treatment (ReST) for Childhood Apraxia of Speech | |||||
| Patient or population: children aged 4 to 12 years with CAS of unknown cause Settings: University of Sydney Communication Disorders Treatment and Research Clinic Intervention: NDP‐3 Comparison: ReST | |||||
| Outcomes | Summary of MD findings | Absolute MD | Number of participants (studies) | Quality of the evidence | Comments |
| Primary outcomes | |||||
| Accuracy of production on treated items Measured by: counting the number of real words produced correctly (/x) Follow‐up: pre‐intervention to 1 month post‐intervention | NDP‐3 MD of 36.0 was greater than the ReST MD of 33.9 | 2.1 | 26 (1 trial) | ⊕⊕⊕⊝ | — |
| Accuracy of production on non‐treated items Measured by: counting the number of real words produced correctly (/x) Follow‐up: pre‐intervention to 1 month post‐intervention | ReST MD of 18.3 was minimally greater than the NDP‐3 MD of 18.2 | 0.1 | 26 (1 trial) | ⊕⊕⊕⊝ | — |
| Secondary outcomes | |||||
| Speech production consistency Measured by: calculating the number of inconsistent productions of 25 words produced 3 times using the DEAP inconsistency subtestb Follow‐up: pre‐intervention to 1 month post‐intervention | NDP‐3 MD of 11.1 was greater than the ReST MD of 10.9 | 0.2 | 26 (1 trial) | ⊕⊕⊕⊝ | — |
| Accuracy of connected speech Measured by: counting the number of correct imitations of 3 word phrases (/x) Follow‐up: pre‐intervention to 1 month post‐intervention | NDP‐3 MD of 14.3 was greater than the ReST MD of 11.5 | 2.8 | 26 (1 trial) | ⊕⊕⊕⊝ | — |
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. | |||||
| CAS: childhood apraxia of speech; DEAP: Diagnostic Evaluation of Articulation and Phonology; MD: mean difference; NDP‐3: Nuffield Dyspraxia Programme ‐ Third Edition;ReST: Rapid Syllable Transition Treatment (ReST) for Childhood Apraxia of Speech | |||||
| aWe downgraded the quality of evidence by one level, to moderate, for imprecision, as there was only one study for comparison. | |||||
| Study | Participants | Methodology/paper type | Intervention | Intervention approach | Intervention intensity and duration | Outcome measures | Treatment outcomes | Timing of outcome measures | Methodological considerations |
| 1 male aged 12.8 years with CAS and charge syndrome | Not quasi‐/RCT (Single case (AB) design) | Dynamic Temporal and Tactile Cueing | Motor | Phase I and II: sessions 4 × per week; Phase III: weekly therapy. Study over 25 months. Home practice not reported | Articulation accuracy on 2‐item scale for treated items; speech rate | Phase I (core vocabulary): change on 4/6 targets. Maintained at last probe. Phase II (core vocabulary): reached 100% accuracy for 3/5 words. Reduction of stereotypies. Phase III: decreased speech rate from 94 to 71 SPM | Baseline and during treatment. No longer‐term follow‐up data | Lack of experimental control, multiple baselines, control, longer‐term follow‐up or generalisation data. Clinical file data used. No replication across participants. Assessors, participants, therapists not blinded | |
| 3 siblings (2 males, 1 female) aged 7.8 and 10.10 years with CAS | Not quasi‐/RCT (Single subject multiple baseline design across behaviours and participants) | Rapid Syllable Transition Treatment (ReST) | Motor | 60‐minute sessions (100‐120 trials per session), 4 × per week for 12 sessions. Home practice not reported | Reading aloud 10 treated and 10 non‐treated non‐word strings; real word generalisation data; perceptual analysis of prosodic pattern and acoustic analysis using pairwise variability index | 3/3 had significant gains in treated items and generalisation to same level of treated complexity. 2/3 generalised to lower and higher complexity non‐word items. Minimal generalisation to real words | Baseline data taken at beginning of every 4th session and at 4 weeks post‐treatment | No long‐term follow‐up data. Limited participants for generalisation of outcomes. No blinding of assessors, participants or therapists. No stimulus generalisation measures | |
| 1 female aged 3 years with CAS | Not quasi‐/RCT (Case description) | Music therapy | Other (alternative interventions) | 30‐minute sessions over 9 months. 24 sessions in total | Descriptive data only | Commenced non‐verbal. At end, had 11 phonemes in inventory | Pre‐treatment and post‐treatment. No follow‐up data | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No replicable outcome measures. No statistical analysis. No blinding of assessors, participants or therapists. No follow‐up or generalisation data. Unclear which aspect of treatment provided outcomes or affect of maturation, schooling, etc. No replication across participants. No long‐term follow‐up data | |
| 2 males aged 4.2 and 4.4 years with CAS and language disorder | Not quasi‐/RCT (Single case multiple baseline across participants) | Aided AAC Modeling | Augmentative and alternative communication | 15‐minute sessions, 1 to 3 × per week for 10 to 15 sessions | Frequency of use of multi‐symbol messages in play scenarios | Significantly more frequent use of multi‐symbol messages using aided AAC as well as different types of messages. Maintained and generalised gains. Increased participation | Baseline × 3, every 2nd treatment session, and at 2, 4 and 8 weeks post‐treatment | CAS diagnosis unclear and not replicable. Limited outcome measures. No blinding of assessors. No response generalisation data taken (only stimulus generalisation) | |
| 1 female (Latino) aged 3.4 years with CAS and suspected velocardiofacial syndrome | Not quasi‐/RCT (Single case multiple baseline across participants) | Aided AAC Modeling | Augmentative and alternative communication | 10‐minute sessions, 1 to 3 × per week for 10 to 15 sessions | Frequency of use of multi‐symbol messages in play scenarios | Significantly more frequent use of multi‐symbol messages using aided AAC. Parental response to training excellent. Maintained and generalised gains | Baseline × 3, every 2nd treatment session, and at 2, 4 and 8 weeks post‐treatment | CAS diagnosis unclear and not replicable. No blinding of assessors. No response generalisation data taken (only stimulus generalisation) | |
| 1 female aged 6 years with CAS and language disorder | Not quasi‐/RCT (Single case multiple baseline across behaviours) | Aided AAC Modeling | Augmentative and alternative communication | 15‐minute sessions, 1 to 3 × per week for 10 to 15 sessions | Frequency of use of grammatical morphemes | Significantly more frequent use of grammatical morphemes using aided AAC. 2nd intervention period needed for 2/3 targets. Maintained gains | Baseline × 3, every treatment session, and 2, 4 and 8 weeks post‐treatment | CAS diagnosis unclear and not replicable. No blinding of assessors. No response generalisation data taken (only stimulus generalisation) | |
| 1 male aged 6.6 years with CAS, hemiplegia and seizures | Not quasi‐/RCT (Single case (ABA) design) | Voice output devices (Macaw) | Augmentative and alternative communication | 60‐minute sessions for 2 sessions (training). Home practice focus | Frequency of appropriate responses to questions in structured discourse | Mother provided greater frequency and type of questions. Frequency of appropriate responses increased | 2 × baseline, 2 × practice period, 1 × post‐treatment, and 4 weeks post‐treatment | Lack of experimental control, multiple baselines or control data. | |
| 1 male and 1 female aged 12 and 8 years respectively diagnosed with CAS. Additional 8 children (7 males) aged 4 to 7 years with persistent articulation errors | Not quasi‐/RCT (Case series ‐ single group study) | Electropalatography (EPG) on /t, d, k, g, s, z/ | Motor | 30‐minute sessions, 1 × per week for 10 weeks | Per cent consonants correct (PCC) and Probe Scoring System (PSS) on probe of 43 words | Significant difference noted for PSS for whole group. PCC scores improved in percentage | Pre‐treatment (baseline first session) and post‐treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No follow‐up or generalisation data. No blinding of assessors | |
| 1 female aged 8 years with CAS and intellectual disability | Not quasi‐/RCT (Single case (ABA) design) | Partners in Augmentative Communication Training (PACT) | Augmentative and alternative communication | 30 to 90‐minute sessions daily after 3 days of intensive training. Home practice focus | Ratio of parent vs participant messages; ratio of successful/intelligible messages from child | Participant had greater frequency of messages compared to parent, and slightly higher frequency of successful measures (high baseline accuracy). Increased participation | Pre‐treatment and 2 months post‐treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 2 females and 1 male aged 3.4, 8 and 12.9 years respectively, with CAS (2 with intellectual disability and 1 with submucous cleft) | Not quasi‐/RCT (3 case studies/reports) | Combined communication boards and voice output devices | Augmentative and alternative communication | 3.4‐year‐old: 2 to 3 × per week for 12 weeks 8‐year‐old: daily for 6 months 12‐year‐old: not reported | 3.4‐year‐old: MLU. 8‐year‐old: assessment of phonological processes; communication repairs. 12‐year‐old: description of functional communication | 3.4‐year old: minimal speech improvement, MLU increased to WNL 8‐year old: no change in speech, parent report of greater communication repairs, and less frustration 12‐year old: supplemented natural speech to initiate, maintain and repair communication | Pre‐assessment and treatment descriptions | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 3 males and 1 female aged 3.6 to 6 years diagnosed with CAS | Not quasi‐/RCT (Single subject (ABB or ABC) design) | Prompts for Restructuring Oral Muscular Phonetic Targets (PROMPT) ‐ full programme (FP) for 8 weeks versus PROMPT without tactile‐kinaesthetic‐proprioceptive cueing for 4 weeks and FP for 4 weeks | Motor | 50‐minute session, 2 × per week for 8 weeks | Trained words on probe, untrained words. Pre‐post testing on the DEAP, TOCS+, VMPAC focal motor and sequencing subtests and Vineland socialization scales | 2/4 improved on DEAP. 4/4 improved on TOCS+, VMPAC subtests and Vineland. All 4 showed greater improvement on easier targets and majority maintained to 3 months post‐treatment. Generalisation to untrained items noted | Probe words: baseline × 3, treatment × 4, post‐treatment, and 3 months post‐treatment | Lack of experimental control as control data changed and interpreted as generalisation but no other control used (e.g. multiple baselines). CAS diagnosis concerning prosody unclear. Blinded assessors for only some outcomes. No withdrawal period between treatment phases and participant differences made comparison between conditions difficult. All measures not taken at consistent times | |
| 2 males aged 6.2 and 3.4 years with CAS (1 case with repaired cleft lip and palate and language disorder) | Not quasi‐/RCT (Single case (AB) design) | Integral Stimulation (Dynamic Temporal and Tactile Cueing) | Motor | Varied across participants. 40‐minute sessions (15 minutes each condition plus probes). 1 case: 3 × per week for 11 weeks. | Probe data on targeted phonemes (articulation) in words for each participant. 1 phoneme targeted with high production frequency = 100 trials and another with moderate production frequency = 60 trials. Articulation and language sample taken at 2 weeks post‐treatment | Large effect sizes for high production frequency and moderate for moderate production frequency. Improvement in PCC and phoneme inventory post‐treatment. Some generalisation | Baseline × 3, each treatment session, and 1 probe post‐treatment | Lack of experimental control, multiple baselines or control data. No long‐term follow‐up data. No blinding of assessors. Accuracy based on if target phoneme was correct (including cognate pair substitution) not if whole word was correct | |
| 1 female aged 9 years with mild CAS (followed until 12 years) | Not quasi‐/RCT (Case study/report) | Articulation therapy, motor‐programming remedial model | Motor | 5 school semesters | Templin‐Darley Tests of Articulation | Remediation of all 31 items for /r/, /ɝ/ and /ɚ/ | Test completed each semester | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 1 male aged 5 years with CAS and language disorder | Not quasi‐/RCT (Multiple baseline across discourse contexts) | Computer‐based AAC | Augmentative and alternative communication | 4‐minute sessions, 2 × per week for 22 sessions over 4 months | Frequency of noun/verb phrases in reciprocal book reading and structured discourse | Improvement in both contexts but more so in book reading than discourse. Some generalisation | Baseline, treatment, and withdrawal probes | CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. No follow‐up data. No blinding of assessors. No replication across participants | |
| 3 children (2 males, 1 female) aged 2.9 to 8 years with CAS | Not quasi‐/RCT (Case study series) | Melodic Intonation therapy (MIT) | Linguistic and motor | Varied. 37 to 71 sessions | Varied. Description of skills, consonant inventories, sequencing error rates and intelligibility compared to typical development | Child 1: all consonants in inventory Child 2: spoke in complex sentences, poor intelligibility, and articulation errors present. Child 3: sequencing error rate dropped from 75% to 22%. 13/18 consonant sounds improved | Pre‐ and post‐treatment | No experimental control. Lack of information on diagnosis of CAS. Primarily descriptive measures ‒ not reliable or tested using statistics. No control, maintenance or generalisation data | |
| 4 children (2 males, 2 females) aged 3.7 to 6.10 years with CAS | Not quasi‐/RCT (Single case design) | Stimulability (STP) and modified Core Vocabulary (mCVT) used concurrently | Linguistic and motor | 55‐minute sessions (10 minutes STP, 45 minutes mCVT), 2 × per week for 20 sessions. No home practice | Per cent phonemes correct, phonetic inventory and inconsistency | PCC increased on average 20% after combined therapy (range 9% to 32%). Inventory gained 5 phones on average (range 1 to 10). 3/4 had greater consistency on CSIP and ISP after therapy; 1 had greater inconsistency | Pre‐ and post‐ treatment | Poor experimental control as stable baseline not established, lack of control data. CAS diagnosis unclear and not replicable. No statistical analysis. No blinding of assessors. No immediate post‐treatment data or generalisation data | |
| 1 male aged 5.5 years with "some dyspraxic features" (CAS diagnosis not explicit) | Not quasi‐/RCT (Case study) | Sensory integrative therapy and speech therapy | Motor | Daily sessions for 2 months | (SP only) Illinois Test of Psycholinguistic Abilities | Test not completed post‐treatment. Observation of greater self‐monitoring and correction of speech | Pre‐treatment only | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures and no post‐treatment data. | |
| 14 children (9 males, 5 females) aged 3 to 6 years with diagnosed CAS (compared to 14 age‐matched controls) | Not quasi‐/RCT (Case series pre‐post design) | Prompts for Restructuring Oral Muscular Phonetic Targets (PROMPT) | Motor | 2 × per week for 8 weeks (16 sessions in total) | GFTA2, HCAPP, VMPAC, MRI | Significant gains as a group for all speech measures | 1‐week pre‐treatment (baseline), 1‐week post‐treatment | CAS diagnosis unclear and not replicable. Age‐matched control group older than CAS group. Limited information on PROMPT targets selected for replication. No blinding of assessors. No stimulus generalisation measures | |
| 3 males aged 4.1, 5.8 and 8.6 years diagnosed with CAS. 1 of the 3 diagnosed with Opitz FG syndrome and another with PDD‐NOS | Not quasi‐/RCT (Single subject multiple baseline across participants design) | Integrated Multimodal Intervention (structured book reading, drill and play activities with AAC devices present and speech encouraged) | Augmentative and alternative communication | 1‐hour sessions, 2 × per week for 3 to 6 weeks | Category (e.g. vocalisation, AAC or both), type of word and accuracy targets. Case 1: final consonants. Case 2: initial /s/ clusters then /f/. Case 3: initial /s/ clusters | Increases in vocalisations/spoken speech noted for 3/3. Speech accuracy improved on targets for 1/3 cases but all showed some generalisation to more accurate everyday speech | Baseline probes, probes every 2nd treatment session, 1‐month post‐treatment | Poor experimental control for case 1 and some change on control data noted. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 1 female aged 5.6 years with CAS | Not quasi‐/RCT (Case description) | Adapted Cueing Technique | Motor | 30 minutes of therapy per day for 6 months | Number of single words/utterances | From 2 to 4 words to 12 words and several carrier phrases. After 6 months began to produce novel sentences | Description of progress during treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 2 males aged 5 and 6 years diagnosed with CAS | Not quasi‐/RCT (Single case (ABAA) design) | Concurrent Melodic Intonation Therapy (MIT) and traditional therapy (20% and 80% of sessions respectively) | Linguistic and motor | 2 × per week over 2‐month period | Pre‐ and post‐treatment gains on word‐morpheme usage, auditory comprehension, naming, describing function, sentence completion, imitation of word phrases and articulation. Tested using language sampling and Porch Index of Communicative Ability in Children | Significant gains were found in phrase length (MLU), picture naming, and verbal imitation tasks. Little change in articulation | Pre‐treatment, post‐traditional therapy, and post‐MIT therapy | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. | |
| 2 males aged 5 and 6 years with suspected CAS | Not quasi‐/RCT (Single case (AB) design) | Melodic Intonation Therapy (MIT) compared to 'traditional speech‐language therapy' | Linguistic and motor | Ongoing 1 × per week speech therapy (traditional articulation sessions) and 40‐minute MIT music sessions over 4 weeks (both treatments concurrent) | GFTA2; KLPA2 and speech production on stimulable sounds in 1‐ or 2‐syllable words | Case 1 made greater gains in MIT sessions (but only 2% gain). Case 2 made greater gains on traditional articulation therapy (15% gain) | Pre‐ and post‐ treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 1 German‐speaking male aged 2.7 years with severe CAS | Single case design (A‐B design with 3 follow‐up assessments post‐treatment with some treatment sessions between assessments) | Speech Generating Devices ‒ fixed display (Gotalk 20+) and dynamic display (DynaVox V) | Augmentative and alternative communication | 45‐minute sessions × 50 treatment sessions. Treatment sessions 2 to 28 days apart | Means of communication (oral versus SGD), intelligibility of speech productions, consistency of speech productions, lexical development, and grammatical development | Significantly more communication initially with SGD than speech; significant increase in speech intelligibility; consistency (however reduced data in baseline period); amount of words used; and increased MLU and inflections after 8 to 9 sessions | Baseline × 3, every 2nd treatment session, and 2, 4 and 8 weeks post‐treatment | Lack of baseline data for consistency. CAS diagnosis unclear and not replicable. No blinding of assessors. No clear withdrawal phase after treatment with SGDs for control and no generalisation data | |
| 1 female aged 5.1 years with CAS | Not quasi‐/RCT (Single case cross‐over design) | Intra‐oral stimulation and electropalatography | Motor | 25‐minute sessions (5 minutes intra‐oral stim, 20 minutes EPG); daily at home, total of 195 sessions in 12 months | Per cent consonants correct, per cent phonemes correct, per cent words correct, intelligibility, visual deviancy | Significant treatment outcomes on all measures | Pre‐testing, A1 (baseline), B (intervention: oral stimulation therapy), A2 (withdrawal for 3 months), B (intervention: EPG), and A3 (follow‐up) | Cross‐over design, no control group or data taken to control for maturation. No replication across participants. No long‐term follow‐up or generalisation data taken | |
| 4 children (2 males, 2 females) aged 5.4 to 8.4 years with CAS (2 also with dysarthria and a third with language disorder); 3 also in Maas 2012b, as below | Not quasi‐/RCT (Single case alternating treatments design with multiple baselines across behaviours over | Dynamic Temporal and Tactile Cueing (high versus moderate feedback frequency in cross‐over design) | Motor | 50‐minute sessions 3 × per week for 3 participants but 1 had 60‐minute sessions 2 × per week | Per cent accuracy on 2‐point scale of segmental and suprasegmental aspects of target words and phrases with 2 words | 2 responded better to low frequency feedback, 1 to high frequency feedback, and 1 to no condition. No generalisation effects | Weekly probes: 3 to 4 × baseline, 4 × treatment. Phase 1: 4 to 5 × withdrawal, 4 × treatment. Phase 2: 2 × withdrawal and 1 month post‐treatment | Small sample size with heterogeneity. Cross‐over conditions made comparison difficult regarding targets chosen. No control group. Effect sizes used not interpretable or comparable to others. Different doses across all participants. Treatment fidelity < 80%. No stimulus generalisation measures | |
| 4 children (2 males and 2 females) aged 5.0 to 7.9 years with CAS. 2 cases had additional dysarthria diagnoses. 1 other case had multiple co‐occurring disorders | Not quasi‐/RCT (Single case alternating treatments design with multiple baselines across behaviours over | Dynamic Temporal and Tactile Cueing (random versus blocked practice compared in cross‐over design) | Motor | 2 × 4 week blocks of therapy | Per cent accuracy on 2‐point scale of segmental and suprasegmental aspects of entire target words and phrases with 2 words | 3/4 responded to both conditions. 2 responded relatively better to blocked practice, 1 to random practice, and 1 to no condition. 2/4 demonstrated generalization | Weekly probes: 3 to 4 × baseline, 4 × treatment. Phase 1: 4 to 5 × withdrawal, 4 × treatment. Phase 2: 2 × withdrawal and 1 month post‐treatment | Small sample size with heterogeneity. Cross‐over conditions made comparison difficult regarding targets chosen. No control group. Effect sizes used not interpretable or comparable to others. Treatment fidelity < 80%. No stimulus generalisation measures | |
| 1 female aged 4.7 years with CAS | Not quasi‐/RCT (Multiple baseline across behaviours ‐ cross‐over treatment design) | Combined Melodic Intonation Therapy (MIT) and Touch Cue Method (TCM) | Motor and linguistic | 3 sessions for 6 weeks for 18 sessions for MIT. 6 weeks no therapy. 3 sessions for 6 weeks for 18 sessions for TCM | Articulation accuracy: PVC, PCC. Also, overall word accuracy scores: PMLU, PWP, PWC. All calculated from responses to 46 picture cards | 1/5 measures significant post‐MIT (per cent vowels correct). Per cent consonants correct also reduced. 3/5 significant post‐TCM (PVC, PCC, PMLU). PVC, PCC and PMLU maintained. Greater changes for both therapies after withdrawal. PCC and PMLU only significant after MIT withdrawn | Beginning and end of 6‐week baseline, beginning and end of both treatment phases, 12 weeks after TCM withdrawn | Lack of experimental control of other factors. Cross‐over design makes comparison of both treatments difficult as many changes only noted after withdrawal of MIT (accumulation effects). Limited outcome data. Lack of generalisation data No blinded assessors. No replication across participants | |
| 12 children (sex unknown) aged 3 to 10 years with CAS (11 with co‐occurring conditions) | Case series (pre and post design) | DuBard Association Method®. It is a multimodal, phonetic therapy which works from accurate sounds in isolation | Motor | Daily in small groups in a school programme for an 11‐month period | Articulation, mean length of utterance (MLU), and intelligibility on Arizona Articulation Proficiency | Significant changes in articulation, intelligibility and MLU, and some resilience measures over 2‐year period | Pre‐ and post‐ treatment | Lack of experimental control regarding maturation effects (despite using the Intervention Efficiency Index and Proportional Change Index) and lack of control of covariate, including other potential intervention over the same period. No control group. No follow‐up or generalisation data | |
| 4 males aged 5.5 to 8.6 years with CAS. 2 children had additional auditory processing impairments | Not quasi‐/RCT (Single case (AB) design with 1 month follow‐up) | Rapid Syllable Transition Treatment (ReST) | Motor | 60‐minute session, 4 × per week for 3 weeks (12 sessions in total). Minimum of 1200 trials per session | Articulation, prosodic and simultaneous articulation and prosodic accuracy on trained and untrained probe pseudo words; PCC, PVC and per cent lexical stress matches from connected speech; PPVT‐4 as control data | All 4 participants increased perceptual accuracy. 1/4 participants showed change in untreated items. All participants showed change in prosody (average prosody gain 58%, 3/4 in PVC and 2/4 in PCC; average gain 79%). Control data (receptive vocabulary on PPVT‐IV) changed minimally | Baseline × 2, probes in treatment × 2, 1 month follow‐up | There was no immediate post‐treatment data taken to determine treatment effects, the follow‐up data was 1 month post‐treatment and included a withdrawal phase. There was no statistical analysis of connected speech data. 1 participant reached ceiling. No blinding of assessors. No stimulus generalisation measures | |
| 12 children (9 males, 3 females) aged 4.2 to 7.6 years with CAS | Not quasi‐/RCT (Case series design) | Integrated Phonological Awareness Intervention | Linguistic | 45‐minute session; 2 × per week for 6 weeks in 2 blocks with 6‐week withdrawal between blocks. Total of 245 sessions | Trained speech accuracy and phonological awareness accuracy on a probe. Generalisation‐ BTOPP and first trial of DEAP inconsistency subtest for PVC, PVC and inconsistency score. PIPA for 4‐year‐olds. TOPA for 5 to 7‐year‐olds. Burt Word Reading Test for non‐word reading and informal non‐word reading probe (Gillon 2000). Per cent grapheme correct score in spelling 10 words from DEAP inconsistency subtest | Speech: 9/12 children improved on trained items. Phonological awareness: 8/12 children improved in 1 or both intervention blocks. Generalisation for 8/12 on all measures except Burt Word Reading Test | Pre‐ and post‐treatment | Lack of experimental control, control group or control data. CAS diagnosis unclear regarding prosody. Limited information provided on each participant. Limited treatment phase data. No maintenance data. No blinding of assessors | |
| 2 male identical twins aged 4.5 years with CAS (deletion at 10q21.2‐22.1) | Not quasi‐/RCT (Single case design) | Integrated Phonological Awareness intervention | Linguistic | 45‐minute session; 2 × per week for 6 weeks in 2 blocks with 6‐week withdrawal between blocks. Total of 245 sessions | PPC, PVC on BTOPP, and DEAP inconsistency percentage. PIPA, PhonRep, Burt Word Reading, Non‐word Reading, Neale accuracy and comprehension | PCC and PVC improved at post‐treatment and follow‐up. Reduced inconsistency. Sound‐letter knowledge increased from 0 to 7 at post‐treatment. Reading WNL and spelling demonstrated use of strategies at final follow‐up | Pre‐ and post‐ treatment, and 6‐month follow‐up | Lack of experimental control, control group or control data. CAS diagnosis unclear regarding prosody. Limited information provided on each participant. Limited treatment phase data. No maintenance data. No blinding of assessors. No stimulus generalisation measures | |
| 12 children (9 males, 3 females) aged 4.2 to 7.6 years diagnosed with CAS | Not quasi‐/RCT (12‐month follow‐up to 2009 case series) | Integrated Phonological Awareness intervention | Linguistic | As per McNeill 2009a | BBTOP and 1st trial of DEAP yielding PPC. PIPA for 4‐year‐olds & TOPA for 5 to 7‐year‐olds. Decoding measures (Burt Word Reading Test and Non‐word Reading Task) and spelling measures (probe of 10 words from the DEAP inconsistency subtest) were completed for participants at least 6 years of age at the beginning of the study. The NARA was administered for participants aged 5 years, 6 months and up | Significant difference for CAS group from pre‐ to post‐treatment on letter knowledge, non‐word reading probe, spelling, PCC, TOPA and Burt Non‐Word Reading. 3/7 improved on NARA to age‐appropriate level | 1‐year follow‐up to McNeill 2009a | 7/12 of original participants followed up. Whole group data ‒ case series. No control group or control data for experimental control or maturation effects | |
| 3 children (2 males, 1 female) aged 6.3, 6.10 and 7.3 years with CAS | Not quasi‐/RCT (Single case multiple baseline design across behaviours) | Integrated Phonological Awareness Intervention | Linguistic | 45‐minute sessions 3 × per week for 3 weeks | PPC on probe, phoneme segmentation probe, phoneme manipulation probes, initial sound identification probes, letter‒sound knowledge subtest from the PIPA, non‐word reading tasks | 2/3 significantly increased PPC, 2/3 significantly improved phonological awareness skills on probes, letter‒sound knowledge, and non‐word reading. Limited transfer to untreated words | Baseline and post‐treatment (3 probes each) | Lack of control group and control data. CAS diagnosis unclear regarding prosody. Lack of multiple baseline data throughout treatment. No long‐term follow‐up. No blinding of assessors | |
| 12 children (9 males, 3 females) aged 3 to 6 years with speech sound disorders | Not quasi‐/RCT (Case series pre‐post design) | Prompts for Restructuring Oral Muscular Phonetic Targets (PROMPT) | Motor | 45‐minute session 2 × per week for 8 weeks | GFTA2, HCAPP, VMPAC focal motor and sequencing subtests, Children's Speech Intelligibility Measure | Significant gains as a group for all speech measures | Baseline 1 week prior to treatment, and 1 week post‐treatment | Lack of experimental control, control group, multiple baseline or control data. No blinding of assessors. No blinding of assessors. No long‐term follow‐up | |
| 37 children (28 males, 9 females) aged 2.6 to 4.5 years with CAS | Not quasi‐/RCT (pre‐postgroup design) | Motor Speech Treatment Protocol (MSTP) | Motor | Intense treatment group: 45‐minute session, 2 × per week × 10 weeks = 20 sessions. Less intense group: 45‐minute session, 1 × per week × 10 weeks = 10 sessions | GFTA‐2 sounds in words subtest; speech intelligibility using Children's Speech Intelligibility Measure (CSIM) at word level, and Beginner's Intelligibility Test (BIT) at sentence level. Functional Outcomes for Children Under Six (FOCUS) scale | Intense group had greater changes in articulation and functional communication compared to the less intense group with large effect sizes. Mixed results were found for intelligibility: at word‐level (CSIM), both the less intense and 1/2 intense groups made a significant and large change. At sentence level, 1/2 intense groups made a significant change | Pre‐ and post‐ treatment | No control group or control data. Participants were not directly randomised; however, no between‐group differences were found at baseline. There were missing data (dealt with using intention‐to‐treat analysis). No information on session trials was obtained, which is important for intensity calculations | |
| 6 males aged 9 to 15 years with CAS. 1 child had additional ADHD and another child had additional dysarthria | Not quasi‐/RCT (Single case multiple baseline across behaviours across participants) | Ultrasound biofeedback (targeting articulation on clusters and CV or VC sequences of inaccurate phones) | Motor (instrumentally based) | 60 minute sessions, 2 × per week × 18 sessions (at least 150 trials per session) | Probe of whole‐word accuracy of treated and untreated items | U002 and U007 had significant gains on 2/4 treated combinations, U005 for 3/4, and U008, U009 and U012 had significant gains on all treated combinations. All exhibited some generalisation (target‐dependant). U005, U007, U008, U009, U012 demonstrated maintenance above pre‐treatment levels | Probes at baseline × 3, every treatment session, post‐treatment, and 2 months post‐treatment | No control group or comparison treatment. No blinding of assessors. Untreated items were not clearly selected as control or generalisation data with some showing change and others not | |
| 3 male children aged 11 to 13 years diagnosed with CAS and poor expressive language and phonological processing. 1 participant had additional flaccid dysarthria, ADHD, language and learning difficulties | Not quasi‐/RCT (Single case multiple baseline across behaviours (syllable positions)) | Ultrasound biofeedback (using structured chaining and principles of motor learning) | Motor (instrumentally based) | 1 hour sessions × 14 sessions. Sessions 1 to 7 addressed target 1 and sessions 8 to 14 addressed target 2 with randomly assigned prosody or no prosody conditions | Treatment acquisition data, generalisation probe of untreated words, maintenance to 2 months post‐treatment | 2/3 participants acquired accurate articulation. 0/3 demonstrated generalisation or maintenance | 3 × baseline probes, midway therapy probe, post‐therapy probe (within 1 week after treatment), and 2‐month follow‐up | No control group. Greater within‐treatment probes and post‐treatment probes would have allowed for greater statistical analysis. No control data. No blinding of assessors. No stimulus generalisation measures | |
| 3 males aged 11 to 14 years with CAS | Not quasi/RCT (Single case (ABA) design) | Ultrasound biofeedback (using structured chaining and principles of motor learning.) | Motor (Instrumentally based) | 2 × 1‐hour articulation treatment a day for 2 weeks. 16 hours of therapy in total. Over 100 trials per session | Treatment acquisition of /ɹ/, /s/ or /ʧ/. Generalisation to untrained items using a probe and sentence imitation task, and maintenance 1 to 3 weeks post‐treatment (audio‐samples submitted) | Case 1 had acquisition, generalisation, and maintenance of targets. Case 2 had some acquisition in the 2nd week of therapy and no generalisation and maintenance. Case 3 showed acquisition, limited generalisation to words and not phrases, and no maintenance | Probe conducted 1 × before treatment, at the end of the first week, and at the end of the second week (post‐treatment) | Lack of experimental control, multiple baselines or control data. No blinding of assessors. No long‐term follow‐up data. No stimulus generalisation measures | |
| 1 adult with CAS and class III malocclusion. Another 5 adults aged 18 to 23 years with persistent articulation disorders | Not quasi‐/RCT (Case series) | Orofacial myofunctional therapy | Motor (Instrumentally based) | 45‐minute session, 1 × per week for 6 weeks | Dworkin‐Culatta Oral Mechanism Examination for oral postures and intelligibility in single words, sentences, and spontaneous speech | All improved lips and tongue postures. 5/6 participants increased intelligibility. No improvement in intelligibility for person with DVD | Pre‐ and post‐treatment | Lack of experimental control, multiple baselines or control data. No treatment data or follow‐up reported. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 1 female aged 9 years with CAS | Not quasi‐/RCT (Case study) | Intensive, systematic drill motor therapy | Motor | 22 sessions over 3 months | 20‐item probe of /r/ (target), ineligibility in spontaneous speech | /r/ improved from 0 to 20 correct in probe. Intelligibility judged by unfamilar listeners improved | Treatment sessions | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No follow‐up data. Only ancedotal generalisation data. No statistical analysis. No reliability of judgments reported. No replication across participants | |
| 4 children (3 males, 1 female) aged 10‐14 years diagnosed with CAS | Not quasi‐/RCT (Single subject (ABAB) design) | Rate Control Therapy | Linguistic and motor | 20‐minute session per reading passage. No further information available | Articulation accuracy (words read correctly) | Improved to 85% accuracy at 50% habitual rate and maintained in therapy as rate was slowly increased. Limited generalisation to conversation ‐ therapy implemented | Reading rate in 5‐minute intervals | Lack of control and follow‐up data. CAS diagnosis unclear and not replicable. No statistical analysis. No blinding of assessors. No stimulus generalisation measures. No report of data reliability | |
| 3 children (2 males, 1 female) aged 4 to 6 years diagnosed with CAS | Not quasi‐/RCT (Single case multiple baseline design across participants) | Concurrent treatment (using randomised variable practice) | Motor | Therapy until target sounds reached 80% accuracy. P1 had 26, P2 had 12 and P3 had 28 sessions. 2 × per week, 30 minutes per session and on average 100 to 115 trials per session | Per cent correct productions on /s, z, f, v/ trained targets during baseline and treatment; generalisation probes to untrained words and 3‐word phrases | All children reached 80% accuracy on target sounds. Moderate to large generalisation effects at word and 3‐word phrases levels (70% to 100% accuracy) | 3 × baseline probes, probes every 5 therapy sessions | No post‐treatment or follow‐up/maintenance data. No blinded assessors. No stimulus generalisation data. P3 continued regular school therapy during the study so could be a confounding factor. No stimulus generalisation measures | |
| 1 male aged 7 years with residual CAS | Not quasi‐/RCT (Single case (ABA) design) | Articulation with facilitative vowel contexts | Linguistic | 45‐ to 55‐minute session, 3 × per week for 3 weeks. 60+ trials per session. Home practice provided | Accuracy on 'sh' sound in word initial probe, 'tr' as control | Significant improvement in 'sh' articulation accuracy in trained and untrained words. No change in control words with 'tr' initial | Pre‐treatment, mid‐therapy × 2 (after sessions 3 and 6), post‐treatment, and maintenance (2 weeks post‐treatment) | Participant did not meet current CAS criteria. Lack of generalisation data beyond 'sh' sound. No blinded assessors. No replication across participants. No long‐term follow‐up data. No reliability of data reported | |
| 1 female aged 5 years with "severe motor planning deficits but no dysarthria" (CAS) | Not quasi‐/RCT (Single case multiple baseline design) | Integral stimulation | Motor | 30‐ to 50‐minute session, 3 to 5 × per week (1 to 2 × per day) for 10 to 16 sessions. No home practice | Articulation accuracy ratings on a 2‐point scale | Improvement from 0.25 to 0.80 on 2‐point scale. 4/5 treatment stimuli achieved rating of 2/2 by end of therapy | Treated stimuli at start of each session, control stimuli twice a week | No statistical analysis. Limited outcome measures. | |
| 4 males aged 5.5 to 6.1 years with CAS (2 with dysarthria and 1 with mild intellectual disability) | Not quasi‐/RCT (Single case multiple baseline across participants) | Dynamic Temporal and Tactile Cueing | Motor | 30‐minute sessions, 2 × per day for 5 days a week for 38 to 50 sessions | Articulation accuracy on a 3‐point scale | Treatment gains for 3/4 participants maintained by 2/4 | Baseline × 4 (or more, staggered baseline), 20+ treatment probes | No follow‐up or generalisation data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures | |
| 4 children (2 males, 2 females) aged 4.8 to 8 years with CAS | Not quasi‐/RCT (Single case multiple baseline across participants and behaviours) | Rapid Syllable Transition Treatment (ReST) | Motor | 50 minute sessions 2 × per week for 6 weeks. 100 trials per session | Accuracy on imitated (a) treated words, (b) untreated pseudo words, (c) untreated real words and control words | Significant improvement on treated words and untreated real words. Significant improvement for 2/4 participants on untreated pseudo words. No change in control items | Baseline × 3 to 6, treatment × 3, and 1 day, 1 month and 4 months post‐treatment | Use of GFTA2 for control items. No stimulus generalisation data | |
| 5 children (4 males, 1 female) aged 5 to 11 years with CAS (3 with mild or moderate receptive language disorder) | Not quasi‐/RCT | Rapid Syllable Transition Treatment (ReST) | Motor (instrumentally based ‐ telehealth) | 60‐minute session, 4 times a week for 3 weeks (12 sessions in total). Minimum of 1200 trials per session | Accuracy on treated pseud‐word items, generalisation to untreated non‐words and real words, and control items (articulation of rhotics) on a probe; client/family satisfaction with telehealth treatment | 5/5 participants demonstrated significant change in treated items. 4/5 maintained gains to 4 months post‐treatment. 4/5 had significant generalisation to untrained non‐words and real words, and 1/5 demonstrated change in control data (articulation errors of rhotics or /s/). Families very satisfied and motivated by telehealth treatment | At least 3 baseline probes, 3 therapy probes (sessions 5, 9 and 1 day post‐treatment). Follow‐up at 1 week, 4 weeks & 4 months post‐treatment | Missing data for some participants at certain time points in Table 3. Problems with change in control data. Some internet issues (dropouts, port sound quality, etc.) were observed in 61% of sessions; however, significant outcomes were found. No stimulus generalisation data | |
| 1 male aged 3 years with CAS and fine motor delay | Not quasi‐/RCT (Single case design; descriptive) | Multimodal therapy: Signed Exact English sign language, Sarah Rosenfeld Johnson's oro‐motor programme and Kaufman Speech Praxis Program | Augmentative and alternative communication | Clinic‐based sessions 45 minutes 1 to 2 × per week and home‐based sessions for 60 minutes 1 × per week | Language assessment; observations and Kaufman Speech Praxis Test; Verbal Motor | Receptive and expressive language consistently in average range but receptive relatively better than expressive language. By 3.6 years of age receptive and expressive language same level. Marked drooling and limited inventory and sequencing at 18 months, yet skills on Kaufman & VMPAC in average range at 3 years, 9 months. Discharged from therapy | Language assessment at 1.1 year, 3 years and 3.6 years. Kaufman test or observations at 1.6, 3 and 3.9 years. VMPAC at 3 years, 9 months | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable regarding prosody and drooling. No statistical analysis. | |
| 1 male aged 14 years with severe CAS and limb/motor apraxia and obsessive compulsive disorder | Not quasi‐/RCT (Case study) | Verbal Motor Learning (with Dynamic Distal Stabilization Technique (DDST)) | Motor | 1 × 30‐minute clinic session and 6 × home practice sessions a week for 4 weeks | (1) Producing highest pitch using /I/ sound with and without DDST, to determine minimum and maximum frequency and length using Speech Analyser 1.5 (2) Imitation of 18 words to analyse word length, maximum loudness, maximum and minimum frequency | Significant t‐test results for (1) increase in maximum frequency and length of pitch after DDST, no change in minimum frequency, and (2) decrease in word length (word said faster), maximum loudness, and maximum frequency | Pre‐ and post‐ treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| 1 female aged 10 years with CAS and ASD | Not quasi‐/RCT (Case study) | Verbal Motor Learning (Initial Phoneme Cue (IPC) technique) | Motor | 2 × 1 hour sessions, 2 weeks apart (participant had initial therapy: 1‐hour session weekly for 1 year prior to this study) | Imitation accuracy of CVCV treated words either (a) with IPC or (b) without IPC | Imitation of CVCV was 0% to 22% accuracy and imitation with IPC was 96% to 100% accuracy | Pre‐ and post‐ treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. No statistical analysis. No blinding of assessors. No follow‐up or generalisation data. No replication across participants | |
| 10 children (no information on gender reported) aged 6 to 11 years with moderate to severe DAS | Not quasi‐/RCT (Case descriptions/file audit) | School‐based intervention | Motor | 25 to 307 hours of therapy | Articulation, polysyllable words and connected speech in speech samples. Intelligibility rated on a 9‐point scale | Significant improvement on articulation. Minimal generalisation to polysyllable words and connected speech. Intelligibility improved by at least 0.5 points | Pre‐ and post‐ treatment | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. | |
| 1 female aged 11.6 years with CAS, intellectual disability and language disorder | Not quasi‐/RCT (Single case design) | Phonological awareness (phoneme‒grapheme mapping, reading comprehension, 'Basics' programme). Speech ‐ PROMPT and Moving Across Syllables | Linguistic | Between 6.0 and 11.6 ongoing weekly treatments ‐ 1 hour × 1:1 sessions and PROMPT institute over summer | Per cent accuracy on phonological awareness and decoding | Improvement seen in phoneme‒grapheme mapping, segmentation and short vowel identification. Some improvement in decoding | Ongoing 1 × per week sessions from 6.0 to 11.6 years | Lack of experimental control, multiple baselines or control data. CAS diagnosis unclear and not replicable. No statistical analysis. Limited outcome measures. | |
| Participants: All participants are English speakers unless otherwise reported. AOS: apraxia of speech; BBTOP: Bankson‐Bernthal Test of Phonology; CAS: childhood apraxia of speech; CSIP: consonant substitute inconsistency percentage; DAS: developmental apraxia of speech; DEAP: Diagnostic Evaluation of Articulation and Phonology; DVD: developmental verbal dyspraxia; GDD: global developmental delay; GFTA‐2: Goldman Fristoe Test of Articulation 2; HCAPP: Hodson Computerized Analysis of Phonological Patterns; ISP: inconsistency severity percentage; KLPA‐2: Khan‐Lewis Phonological Analysis, Second Edition; NARA: Neale Analysis of Reading Ability; PCC: percentage consonants correct; PDD‐NOS: pervasive developmental disorder ‐ not otherwise specified; PMLU: phonological mean length of utterance; PVC: percentage vowels correct; PWC: percentage words correct; PWP: proportion of whole‐word proximity; PIPA: Preschool and Primary Inventory of Phonological Awareness; RCT: randomised control trial; SSD: speech sound disorder; TOCS+: Test of Children's Speech Plus; TOPA: Test of Phonological Awareness; VMPAC: Verbal Motor Production Assessment for Children | |||||||||