Intervenciones para la prevención de embarazos no deseados en adolescentes
Resumen
Antecedentes
Los embarazos no deseados entre las adolescentes representan un importante problema de salud pública en los países de altos ingresos, así como en los de ingresos medios y bajos. Para abordar este problema se han utilizado numerosas estrategias de prevención en diferentes países del mundo como la educación sanitaria, el desarrollo de habilidades y la mejora de la accesibilidad a métodos anticonceptivos. Sin embargo, existe incertidumbre con respecto a los efectos de estas intervenciones, por lo que se necesita examinar su base de evidencia.
Objetivos
Evaluar los efectos de las intervenciones de prevención primaria (realizadas en la escuela, la comunidad/el domicilio, de carácter clínico y de carácter religioso) sobre los embarazos no deseados en adolescentes.
Métodos de búsqueda
Se buscaron todos los estudios pertinentes, independientemente del idioma o el estado de publicación, hasta noviembre 2015. Se realizaron búsquedas en el registro de ensayos especializados del Grupo Cochrane de Regulación de la Fertilidad (Cochrane Fertility Regulation Group), en el Registro Cochrane Central de Ensayos Controlados (Cochrane Central Register of Controlled Trials) (CENTRAL) (The Cochrane Library 2015, Número 11), MEDLINE, EMBASE, LILACS, Social Science Citation Index y Science Citation Index, Dissertations Abstracts Online, The Gray Literature Network, HealthStar, PsycINFO, CINAHL y POPLINE y en las listas de referencias de los artículos.
Criterios de selección
Se incluyeron los ensayos controlados aleatorizados (ECA) y los ensayos controlados aleatorizados grupales que evaluaron alguna intervención destinada a mejorar el conocimiento y las actitudes en relación con el riesgo de embarazo no deseado, a promover el retraso en el comienzo de las relaciones sexuales y a estimular el uso constante de los métodos de regulación de la natalidad para reducir los embarazos no deseados en adolescentes de entre diez y 19 años de edad.
Obtención y análisis de los datos
Dos autores de la revisión de forma independiente evaluaron la eligibilidad y el riesgo de sesgo de los ensayos y extrajeron los datos. Cuando fue apropiado, los resultados binarios se agruparon mediante un modelo de efectos aleatorios, con intervalos de confianza (IC) del 95%. Cuando fue apropiado, los datos se combinaron en metanálisis y la calidad de la evidencia se evaluó mediante los criterios GRADE.
Resultados principales
Se incluyeron 53 ECA en los que participaron 105 368 adolescentes. Las participantes fueron de diversas etnias. Dieciocho estudios asignaron al azar a individuos, 32 fueron estudios aleatorizados grupales (escuelas [20], aulas [6], y comunidades/vecindarios [6]). Tres estudios fueron mixtos (asignaron al azar individuos y grupos). La duración del seguimiento varió de tres meses a siete años; la duración mayor de 12 meses fue la más frecuente. Cuatro ensayos se realizaron en países de ingresos bajos y medios, y el resto se realizó en países de ingresos altos.
Intervenciones múltiples
Los resultados mostraron que las intervenciones múltiples (combinación de intervenciones educativas y de promoción de la anticoncepción) redujeron significativamente el riesgo de embarazos no deseados entre las adolescentes (RR 0,66; IC del 95%: 0,50 a 0,87; cuatro ECA individuales, 1905 participantes, evidencia de calidad moderada. Sin embargo, esta reducción no fue estadísticamente significativa en los ECA grupales. La evidencia de los posibles efectos de las intervenciones sobre los resultados secundarios (comienzo de las relaciones sexuales, uso de métodos de regulación de la natalidad, aborto, parto, enfermedades de transmisión sexual) no es definitiva.
Los puntos fuertes de la metodología incluyeron un tamaño de las muestras relativamente grande y el control estadístico de las diferencias iniciales, mientras que las limitaciones incluyeron la falta de resultados biológicos, el posible sesgo de autoinforme, análisis que ignoraron la asignación al azar grupal y el uso de pruebas estadísticas diferentes para informar los resultados.
Intervenciones educativas
Fue poco probable que las intervenciones educativas retrasaran significativamente el inicio de las relaciones sexuales entre las adolescentes, en comparación con los controles (RR 0,95; IC del 95%: 0,71 a 1,27; dos estudios, 672 participantes, evidencia de calidad baja).
Las intervenciones educativas aumentaron significativamente el uso de preservativos informado en la última relación sexual en las adolescentes, en comparación con los controles que no recibieron la intervención (RR 1,18; IC del 95%: 1,06 a 1,32; dos estudios, 1431 participantes, evidencia de calidad moderada).
Sin embargo, no está claro si las intervenciones educativas tuvieron algún efecto sobre los embarazos no deseados, ya que ninguno de los estudios incluidos informó este resultado.
Intervenciones de promoción de la anticoncepción
En el caso de las adolescentes que recibieron intervenciones de promoción de la anticoncepción, hubo poca o ninguna diferencia en el riesgo de un primer embarazo no deseado, en comparación con los controles (RR 1,01; IC del 95%: 0,81 a 1,26; dos estudios, 3440 participantes, evidencia de calidad moderada).
El uso de anticonceptivos hormonales fue significativamente mayor en las adolescentes del grupo de intervención, en comparación con las del grupo de control (RR 2,22; IC del 95%: 1,07 a 4,62; dos estudios, 3091 participantes, evidencia de alta calidad)
Conclusiones de los autores
La combinación de las intervenciones educacionales y anticonceptivas parece reducir el embarazo no deseado en las adolescentes. La evidencia sobre los efectos del programa en las medidas biológicas es limitada. La variabilidad en las poblaciones de estudio, las intervenciones y los resultados de los ensayos incluidos, así como la escasez de estudios que comparen diferentes intervenciones directamente, impiden establecer una conclusión definitiva con respecto a qué tipo de intervención es más efectiva
PICO
Resumen en términos sencillos
Intervenciones para la prevención de embarazos no deseados en adolescentes
Las intervenciones para prevenir los embarazos no deseados incluyen cualquier actividad (solo educación o asesoramiento en materia de salud, educación en materia de salud y desarrollo de aptitudes, educación en materia de salud y educación sobre anticonceptivos, educación y distribución de anticonceptivos, asesoramiento individual o grupo basados en la fe) destinada a aumentar los conocimientos y las actitudes de los adolescentes en relación con el riesgo de embarazos no deseados; promover el retraso en el inicio de las relaciones sexuales; fomentar el uso sistemático de métodos de control de la natalidad y reducir los embarazos no deseados.
Esta revisión incluyó 53 ensayos controlados aleatorizados que compararon estas intervenciones con varios grupos control (en su mayoría, educación sexual estándar habitual ofrecida por las escuelas). La búsqueda de ensayos no se limitó por país, aunque la mayoría de los ensayos incluidos se realizaron en países de altos ingresos; solo cuatro ensayos se realizaron en países de ingresos medios y bajos y representaron principalmente a los grupos socioeconómicos más bajos. Las intervenciones se administraron en escuelas, centros comunitarios, establecimientos de asistencia sanitaria y domicilios. Se realizó un metanálisis para los estudios en los que fue posible extraer los datos.
Se observó que solo las intervenciones que incluyeron una combinación de educación y promoción de la anticoncepción (intervenciones múltiples) redujeron de manera significativa los embarazos no deseados en el período de seguimiento a medio y largo plazo. Los resultados para las medidas de resultado conductuales (secundarias) no fueron consistentes entre los ensayos.
Las limitaciones de esta revisión incluyen que dependen de la fiabilidad con la que las participantes del programa informen con exactitud sobre su comportamiento y de las deficiencias metodológicas de los ensayos.
Authors' conclusions
Summary of findings
| Contraceptive‐promoting interventions (individual RCTs) | |||||
| Patient or population: Male and female adolescents aged 10 years to 19 years | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | |
| Risk with No intervention/standard curriculum | Risk with Contraception Intervention | ||||
| Unintended pregnancy | Study population | RR 1.01 | 3440 | ⊕⊕⊕⊝ | |
| 83 per 1000 | 84 per 1000 | ||||
| Moderate | |||||
| 85 per 1000 | 86 per 1000 | ||||
| Use of birth control methods (condom use in last sex) | Study population | RR 0.95 | 3091 | ⊕⊕⊕⊕ | |
| 367 per 1000 | 348 per 1000 | ||||
| Moderate | |||||
| 312 per 1000 | 296 per 1000 | ||||
| Use of birth control methods (hormonal contraceptives) | Study population | RR 2.22 | 3091 | ⊕⊕⊕⊕ | |
| 165 per 1000 | 365 per 1000 | ||||
| Moderate | |||||
| 131 per 1000 | 292 per 1000 | ||||
| Sexually Transmitted Diseases | Study population | RR 0.92 | 3440 | ⊕⊕⊕⊕ | |
| 103 per 1000 | 95 per 1000 | ||||
| Moderate | |||||
| 98 per 1000 | 90 per 1000 | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| 1 Downgraded by 1 for imprecision: confidence interval fail to appreciable harm and included the null value | |||||
| Educational interventions (cluster RCTs) | |||||
| Patient or population: Male and female adolescents aged 10 years to 19 years | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | |
| Risk with No intervention/Standard curriculum | Risk with Educational intervention | ||||
| Use of birth control methods (condom use at last sex) | Study population | RR 1.18 | 1431 | ⊕⊕⊕⊝ | |
| 261 per 1000 | 308 per 1000 | ||||
| Moderate | |||||
| 534 per 1000 | 630 per 1000 | ||||
| Initiation of sexual intercourse (mixed gender) | Study population | RR 0.95 | 672 | ⊕⊕⊝⊝ | |
| 227 per 1000 | 215 per 1000 | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| 1 Several risk of bias assessment were unclear (not provided in the text) 2 Low number of events and confidence interval includes the null value | |||||
| Multiple interventions (cluster RCTs) | |||||
| Patient or population: Male and female adolescents aged 10 years to 19 years | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | |
| Risk with No Intervention/Standard curriculum | Risk with Multiple interventions | ||||
| Unintended pregnancy | Study population | RR 0.50 | 3149 | ⊕⊕⊝⊝ | |
| 67 per 1000 | 33 per 1000 | ||||
| Moderate | |||||
| 25 per 1000 | 13 per 1000 | ||||
| Initiation of sexual intercourse (mixed gender) | Study population | RR 0.84 | 8608 | ⊕⊝⊝⊝ | |
| 253 per 1000 | 212 per 1000 | ||||
| Moderate | |||||
| 212 per 1000 | 178 per 1000 | ||||
| Use of birth control methods (condom use at last sex) | Study population | RR 1.01 | 2620 | ⊕⊕⊕⊝ | |
| 585 per 1000 | 591 per 1000 | ||||
| Moderate | |||||
| 565 per 1000 | 570 per 1000 | ||||
| Use of birth control methods (consistent condom use) | Study population | RR 1.95 | 826 | ⊕⊕⊝⊝ | |
| 353 per 1000 | 689 per 1000 | ||||
| Moderate | |||||
| 133 per 1000 | 259 per 1000 | ||||
| Use of birth control methods (hormonal contraceptives) | Study population | RR 1.01 | 3987 | ⊕⊝⊝⊝ | |
| 244 per 1000 | 246 per 1000 | ||||
| Moderate | |||||
| 251 per 1000 | 254 per 1000 | ||||
| Sexually Transmitted Diseases | Study population | RR 0.76 | 420 | ⊕⊕⊝⊝ | |
| 37 per 1000 | 28 per 1000 | ||||
| Moderate | |||||
| 31 per 1000 | 24 per 1000 | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| 1 Downgraded by 1 for risk of bias; several assessments were unclear due to no information provided. Such potential limitations are likely to lower confidence in the estimate of effect 2 Downgraded by 1 for imprecision; low number of events, confidence interval includes appreciable benefit and null value 3 Heterogeneity could be explained (difference in comparison intervention and length of follow up) 4 Downgraded by 1 for imprecision: confidence interval includes appreciable benefit 5 Downgraded by 1 for inconsistency: unexplained large variations in effect 6 Confidence interval includes the null value, however, the sample size and number of events are fairly large and confidence interval is relatively narrow 7 Downgraded by 1 for imprecision: confidence interval includes appreciable benefit and harm 8 Downgraded by 1 for imprecision; low number of events, confidence interval includes appreciable benefit and harm | |||||
| Multiple interventions ( individual RCTs) | |||||
| Patient or population: Male and female adolescents aged 10 years to 9 years | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | |
| Risk with No Intervention/Standard curriculum | Risk with Multiple interventions | ||||
| Unintended pregnancy | Study population | RR 0.66 | 1905 | ⊕⊕⊕⊝ | |
| 116 per 1000 | 76 per 1000 | ||||
| Moderate | |||||
| 149 per 1000 | 98 per 1000 | ||||
| Initiation of sexual intercourse (mixed gender) | Study population | RR 0.99 | 1796 | ⊕⊕⊕⊝ | |
| 410 per 1000 | 406 per 1000 | ||||
| Moderate | |||||
| 236 per 1000 | 234 per 1000 | ||||
| Use of birth control methods (condom use in last sex) | Study population | RR 1.00 | 796 | ⊕⊕⊕⊝ | |
| 840 per 1000 | 840 per 1000 | ||||
| Moderate | |||||
| 837 per 1000 | 837 per 1000 | ||||
| Use of birth control methods (consistent condom use) | Study population | RR 1.21 | 1681 | ⊕⊕⊝⊝ | |
| 353 per 1000 | 427 per 1000 | ||||
| Moderate | |||||
| 476 per 1000 | 575 per 1000 | ||||
| Sexually Transmitted Diseases | Study population | RR 0.89 | 699 | ⊕⊝⊝⊝ | |
| 191 per 1000 | 170 per 1000 | ||||
| Moderate | |||||
| 270 per 1000 | 241 per 1000 | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| 1 Downgraded by 1 for risk of bias; several assessments were unclear due to no information provided. Such potential limitations are likely to lower confidence in the estimate of effect 2 Downgraded by 1 for imprecision; low number of events, confidence interval includes appreciable benefit and null value 3 Heterogeneity could be explained (difference in comparison intervention and length of follow up) 4 Downgraded by 1 for imprecision: confidence interval includes appreciable benefit 5 Downgraded by 1 for inconsistency: unexplained large variations in effect 6 Confidence interval includes the null value, however, the sample size and number of events are fairly large and confidence interval is relatively narrow 7 Downgraded by 1 for imprecision: confidence interval includes appreciable benefit and harm 8 Downgraded by 1 for imprecision; low number of events, confidence interval includes appreciable benefit and harm | |||||
Background
The World Health Organization defines adolescents as individuals between 10 years and 19 years of age (WHO 1980). Adolescence is a period of transition, growth, exploration and opportunities. During this phase of life, adolescents experience physical and sexual maturation and tend to develop an increased interest in sex, with attendant risks of unintended pregnancies, health risks associated with early childbearing, abortion outcomes, and sexually transmitted infections, including HIV/AIDS.
Adolescents who have an unintended pregnancy face a number of challenges, including abandonment by their partners, inability to complete school education (which ultimately limits their future social and economic opportunities), and increased adverse pregnancy outcomes (Henshaw 2000; Koniak‐Griffin 2001; Kosunen 2002; Moore 1993; Phipps 2002;, Upchurch 1990).
Description of the condition
Unintended pregnancy among adolescents is a common public health problem in industrialised, middle‐ or low‐income countries (WHO 1995). The number of unintended pregnancies is reported to be on the decline in the US, with the Office of Adolescent Health reporting a 10% drop from 2012 to 2013, and more than a 50% drop between 1991 and 2013 (Hamilton 2014). The same decline was seen across all racial groups but some disparities remain: Black and Hispanic teens make up a large proportion of teen births in the US (Hamilton 2014). The same trend is reported in most countries (World Bank 2014): in sub‐Saharan Africa, there was a decline in the fertility rate among adolescents from 134 live births per 1000 in 2000 to 115 live births per 1000 in 2010, although these rates are still high when compared to the world standard; in India, adolescent pregnancies constitute 19% of total fertility (Mehra 2004) but this rate has been declining with 77 live births per 1000 in 2010 as compared to 109 live births per 1000 in 2000; and an Israeli study estimated the incidence of teenage pregnancy in Israel to be 32 live births per 1000 adolescent girls (Sikron 2003).
Repeat pregnancies among adolescents are also common and are associated with increased risks of adverse maternal and child health outcomes (Nelson 1990). Unintended pregnancy is not only costly to the teenagers and their families, it is also a huge financial burden to the state, borne by taxpayers in high‐income nations. It was estimated that spending on medicaid‐subsidised medical care related to unintended pregnancy totals more than USD 12 billion annually (Thomas 2009). These costs include welfare support for mothers experiencing financial difficulties, implementation of programmes (educational and skills training) to empower mothers to gain financial independence, and lost tax revenues arising from reduced employability and earnings (Burt 1986; Haveman 1997; Maynard 1996; Rich‐Edwards 2002 ).
Adolescent mothers are more likely to perform poorly in school, come from low socio‐economic homes and a less advantageous environment; and be themselves children of mothers with limited school education and a history of unintended teenage pregnancies (Elfebein 2003). Children born to adolescent mothers are more likely to have low birth weight, and become victims of physical neglect and abuse (Elfebein 2003), more likely to end up as school‐dropouts like their mothers, or engage in delinquent behaviours (Monea 2011).
Description of the intervention
On account of the short‐ and long‐term consequences of unintended pregnancies for the adolescent, their families and society at large (Burt 1990; Trussell 1997), government public health programmes, bilateral agencies and non‐governmental organisations (NGOs) have implemented (and continue to implement) various interventions to address the problem, using a variety of approaches.
Such interventions include:
-
curriculum‐based sex and STD/HIV education programmes (Safer Choices (Coyle 2001), Becoming a Responsible Teen (St. Lawrence 2005), All for You (Coyle 2006));
-
abstinence‐alone programmes (Postponing Sexual Involvement (Kirby 1997b), Sex can Wait (Denny 2006));
-
comprehensive programmes ‐ a combination of multiple components (Sexual Health and Relationships (SHARE) (Henderson 2007), RIPPLE (Stephenson 2004), Children's Aid Society‐Carrera program (Philliber 2002));
-
sex and STD/HIV education programmes for parents and teens (Keepin' it R.E.A.L (Dilorio 2006), REAL Men (Dilorio 2007));
-
interactive video‐based and computer‐based interventions (DeLamater 2000, Downs 2004);
-
clinical protocol and one‐on‐one programmes, which include advance promotion and provision of emergency contraceptives (Raine 2000; Raymond 2006);
-
clinic‐based programmes (Lindberg 2006), promotion of clinic appointments and supportive activities (Danielson 1990, Orr 1996);
-
youth development programmes (service learning such as the Reach for health service learning program (O'Donnell 2003), Teen Outreach Program (TOP) (Philliber 1992); and
-
vocational education (Summer Training and Education Program (STEP) (Grossman 1992).
How the intervention might work
Interventions that are designed to reduce teen pregnancy appear to be most effective when a multifaceted approach is used, as the problem is multiple determined and multidimensional. The interventions should not only focus on sexual factors and related consequences, they should also include non‐sexual factors such as skills training, and personal development. Further, stakeholders including pregnant teens, parents, the health sector, schools and churches should work together to devise programmes that are practical, evidence based, culturally appropriate and acceptable to the target population.
Some interventions focus primarily on changing the psychosocial risk and protective factors that involve sexuality. One such is Safer Choices (Coyle 2001) which improves teens’ knowledge about the risks and consequences of pregnancy and STDs, values and attitudes regarding sex, perceptions of peer norms about sex and contraception, self‐efficacy (ability to say ‘no’ to unwanted sex), consistent use of contraception including condoms, and their intentions regarding sexual behaviours. Some interventions promote abstinence only (Denny 2006), and others add a comprehensive, health‐education approach wherein safer sexual practices are also included (Jemmott 1998). Sex and STD/HIV education programmes for parents and teens seek to improve parent/child communication regarding sexual health and sexuality, and promote connectedness (Dilorio 2006). Clinic protocols and one‐on‐one programmes promote practices that provide advance supplies of emergency contraceptives to high risk adolescents (Lindberg 2006; Orr 1996), as well as providing health counselling for young men (Danielson 1990).
Other interventions, such as youth development endeavours, focus on non‐sexual factors, which aim to engender positive values in adolescents, inspire hope for the future, improve performance in school and bolster family relationships. They also aim to reduce risky behaviours such substance abuse and violence; promote service‐learning programmes which provide supervised voluntary community‐service opportunities, as well as mentoring opportunities on skills‐building (O'Donnell 2003, Philliber 1992). Some make use of trained peer educators to conduct the health‐education sessions serving as mentors or role models in achieving sustained behavioural changes (Borgia 2005).
Experts suggest that in order to reduce teenage pregnancies, interventions should be designed to address multiple sexual and non‐sexual antecedents that correlate with adolescent sexuality, and which may be related to the adolescents, their families, schools, communities and cultural factors ‐ notably religion (Kirby 2002a). Interventions should also include publicly‐financed mass media campaigns and expanding government‐subsidised family‐planning services (Thomas 2012).
With regard to cultural factors, while one Israeli study showed that the incidence of pregnancy was three times higher among Muslims than among Jews (Sikron 2003), another showed that women with no religious affiliation had the highest unintended pregnancy rate compared to women with religious affiliation, and that these women were also most likely to end the pregnancy by abortion (Finer 2006). This raises questions about the possible impact of faith‐based interventions, which tend to start early and are often sustained for long periods at the home and community levels. In some communities, premarital or extra‐marital sex, whether in young or older people, is seen by the larger society as a violation of morality. Most moral codes and laws that prescribe acceptable conducts of sexual relationships have their origin in major religions.
Why it is important to do this review
Evaluation studies of specific interventions as well as reviews and meta‐analyses of the effects of current strategies show discrepant evidence of effectiveness (DiCenso 2002, Fullerton 1997, Maness 2013). For example, a review of 73 studies reported that four intervention programmes resulted in delay in initiation of sexual intercourse, increased condom and contraceptive use, and reduced unintended teenage pregnancy (Kirby 2002b). The interventions identified as being effective in that review were sex and HIV education curricula; one‐on‐one clinician‐patient protocols in healthcare settings; service learning programmes; and intensive youth development programmes (Kirby 2002b).
Another systematic review of randomised controlled trials showed that several primary prevention measures did not delay the initiation of sexual intercourse nor reduce the number of pregnancies among adolescents (DiCenso 2002, Maness 2013). As this review demonstrated, a small number of programmes actually led to an increase in the number of pregnancies among partners of male participants of abstinence programmes (DiCenso 2002). One author had attributed the small decline in the level of adolescent pregnancy in the US to a decrease in sexual activity and an increase in contraceptive use, especially long‐term contraceptive injectables and implants (Pettinato 2003), fear of contracting HIV/AIDS, health education programmes, a changing moral climate, new contraceptives, and improved economic climate (Klerman 2002).
It is possible that discrepancies in results of existing reviews and meta‐analyses may partly be explained by design flaws in the evaluation of studies and reviews. For example, most reviews included non‐randomised and observational studies; most were limited in scope through their exclusion of unpublished studies; very few included rigorous statistical analysis, and some were based on surveys (Franklin 1997).
This calls for rigorous reviews to more clearly elucidate the effects of these interventions, taking cognizance of the complex and multi‐factorial nature of adolescent sexuality and pregnancy.
Moreover, most of the reviews were limited to industrialised nations (DiCenso 2002), and thus could not account for any influences of social, cultural, and economic factors in diverse populations. Such reviews have limited value to bilateral agencies and international NGOs working in the field of adolescent health promotion. In light of this, the Cochrane systematic approach was used to limit bias (systematic errors) and reduce chance effects, thereby providing more reliable results upon which to draw conclusions and make rational and evidence‐based recommendations (Antman 1992; Oxman 1993). This review draws from the expertise and resources already developed within Cochrane in general and Cochrane Fertility Regulation in particular.
In this review, we assessed and summarised the effects that adolescent pregnancy prevention interventions have on: [i] adolescents' knowledge and attitudes relating to risks of unintended pregnancies, [ii] delay in initiation of sexual intercourse, [iii] consistent use of birth control methods, and [iv] reduction in unintended pregnancies. To reduce publication bias (Cook 1993, Dickersin 1990), we considered all published and unpublished randomised controlled studies that assessed the effectiveness of interventions to reduce unintended pregnancy among adolescents, written in any language. Studies conducted in both high‐income and middle‐ and low‐income countries were also considered (WHO 1995). This body of evidence will help to elucidate what works, and what does not in the efforts to reduce unintended pregnancies among adolescents, and thus help to justify the use of scarce resources, train public health professionals, and facilitate the design of interventions that are effective.
Objectives
To assess the effects of primary prevention interventions (school‐based, community/home‐based, clinic‐based, and faith‐based) on unintended pregnancies among adolescents.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials, including cluster randomised trials where the unit of randomisation is the household, community, youth centre, school, classroom, health facility, or faith‐based institution.
Types of participants
Male and female adolescents aged 10 years to 19 years
Types of interventions
Any activity (either health education or counselling only, health education plus skills‐building, health education plus contraception‐education, contraception education and distribution, faith‐based group or individual counselling) designed to increase adolescents' knowledge and attitudes about the risk of unintended pregnancies, promote delay in initiation of sexual intercourse, encourage consistent use of birth control methods, and reduce unintended pregnancies. Where our search strategy identified studies that were not specifically designed to influence adolescent pregnancy, but were later reported to influence any of our primary or secondary outcomes, we included such studies if they met the other eligibility criteria.
We categorised interventions as follows.
-
Educational interventions: health education, HIV/STD education, community services, counselling only, health education plus skills‐building, faith‐based group or individual counselling.
-
Contraceptive‐promoting interventions: contraception‐education with or without contraceptive distribution.
-
Multiple interventions: combination of educational interventions with contraceptive‐promotion interventions.
Control: no additional activity/intervention to existing conventional population‐wide activities.
Types of outcome measures
Primary outcomes
-
Unintended pregnancy.
Secondary outcomes
-
Reported changes in knowledge and attitudes about the risk of unintended pregnancies.
-
Initiation of sexual intercourse.
-
Use of birth control methods
-
Abortion.
-
Childbirth.
-
Morbidity related to pregnancy, abortion or childbirth.
-
Mortality related to pregnancy, abortion or childbirth.
-
Sexually transmitted infections (including HIV).
Search methods for identification of studies
See: Cochrane Fertility Regulation methods used in reviews.
We did not impose any language restrictions, and sought translations where necessary. We did not impose any restrictions on journal of publication and used no country names or other geographical terms in the search. Full search strategies are shown below (Appendix 1).
Electronic searches
We searched all relevant studies regardless of language or publication status (published, unpublished, in press, and in progress).
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library) online; Issue 11 November 2015.
The Cochrane Fertility Regulation Trials Search Co‐ordinator helped us to search the Group's specialised trial register (Code: SR‐FERTILREG).
We searched the following electronic databases: MEDLINE (1966 to November 2015), EMBASE (1980 to November 2015), Dissertations Abstracts Online (http://library.dialog.com/bluesheets/html/bl0035.html), The Gray Literature Network (http://www.osti.gov/graylit/), HealthStar, PsycINFO, CINAHL and POPLINE for randomised controlled trials using the Cochrane Fertility Regulation search strategy (Helmerhorst 2004).
We searched LILACS (La Literatura Latinoamericana y del Caribe de Informacion en Ciencias de la Salud) database 2015 (www.bireme.br; accessed November 2015) and the Social Science Citation Index and Science Citation Index (1981 to November 2015).
We searched the Specialist Health Promotion Register (Social Science Research Unit (SSRU), Institute of Education, University of London at: http://eppi.ioe.ac.uk; June 2005)
For search terms, see Appendix 1.
Searching other resources
In addition, we contacted individual researchers, national and international research institutes/centres and organisations (including non‐governmental organisations) working in the field of adolescent reproductive health in order to obtain information on unpublished and on‐going trials. To ensure that no relevant studies were left out, we read through the list of references in each identified study in order to follow up on articles that may have qualified for inclusion in the review.
Data collection and analysis
One hundred and forty‐two (142) potentially relevant studies were identified of which 53 studies met the inclusion criteria and two are awaiting data extraction (Studies awaiting classification) pending the collection of complete data from the study authors.
Selection of studies
Two authors (CO and EE) independently applied the inclusion criteria to all identified studies and made decisions on which studies to include. The studies were initially checked for duplicates and relevance to the review by looking at the titles and abstracts. Where it was not possible to exclude a publication by looking at the title or the abstract, the full paper was retrieved. Differences were resolved by discussion and consultation with a third author (MM, HE or JE) when in doubt. The results section of each publication was blinded during screening to minimise bias. There were no language preferences in the search or the selection of articles.
Data extraction and management
Two authors (CO and EE) undertook data extraction using a standard data extraction form. We extracted the following data from each study that qualified for inclusion in the review.
Methods: the nature of concealment of allocation to study or control group (whether adequate, unclear, inadequate, or not done), study duration, type of trial, provider and outcome assessor blinding, extent of drop‐outs and cross‐overs, co‐interventions, other potential confounders, and any validity criteria that were used.
Participants: study setting (including country, state, region, community) and unit of randomisation (schools, households, communities, faith‐based institutions), age, gender, race/ethnicity, and other socio‐demographic characteristics of participants.
Interventions: nature of the intervention delivered to the study and control groups, and how it was delivered; timing and duration, and length of follow‐up.
Outcome measures and results: differences between intervention and control groups in terms of unintended pregnancy (first pregnancy), reported knowledge and attitudes about the risk of unintended pregnancies, initiation of sexual intercourse, use of birth control methods, abortion, childbirth, morbidity related to pregnancy, abortion or childbirth, and mortality related to pregnancy, abortion or childbirth.
Missing data: missing data arose from two sources, participant attrition and missing statistics.
Assessment of risk of bias in included studies
We assessed the methodological quality of included studies using standard methods for randomised controlled trials as described in the Cochrane Handbook for Systematic Reviews of Interventions Version 5.1 (Higgins 2011a).
We considered six parameters: generation of allocation sequence, concealment of allocation sequence, blinding, incomplete outcome data, selective outcome reporting and other sources of bias.
-
Generation of allocation sequence:
-
Yes ‐ if the method described was suitable to prevent selection bias (such as computer‐generated random numbers, table of random numbers or drawing lots);
-
Unclear ‐ if the method was not described but trial was described as "randomised"; and
-
No ‐ if sequences could be related to prognosis (case record number, date of birth, day, month, or year of admission).
-
-
Concealment of allocation:
-
Yes ‐ if there was evidence that the authors took proper measures to conceal allocation through, for example, centralised randomisation or use of serially‐numbered, opaque, sealed envelopes;
-
Unclear ‐ if the authors either did not report an allocation concealment scheme at all, or reported an approach that is unclear;
-
No ‐ if concealment of allocation was inadequate (such as alternation or reference to participant identification numbers or dates of birth).
-
-
Blinding:
-
Yes ‐ if there was evidence of no blinding and outcomes were unlikely to be influenced by lack of blinding, or blinding of participants and key study personnel was ensured and unlikely that blinding was broken, or outcome assessment was blinded and the non‐blinding of others was unlikely to introduce bias;
-
Unclear ‐ insufficient information or outcome not addressed;
-
No ‐ no blinding and outcome likely to be influenced by lack of blinding or blinding carried out but likely to be broken.
-
-
Incomplete outcome data:
-
Yes ‐ if there is evidence that there are no missing outcome data, or reason for missing outcome data unlikely to be related to true outcome, or missing outcome data balanced in numbers across intervention groups and with similar reasons across groups, or for dichotomous outcome data, the proportion of missing outcomes compared with observed event risk not enough to have a clinically‐relevant impact on the intervention effect estimate, or for continuous outcome data, plausible effect size (difference in means or standardised difference in means) among missing outcomes not enough to have a clinically‐relevant impact on observed effect size, or missing data have been imputed using appropriate methods;
-
Unclear ‐ insufficient reporting of attrition/exclusions to permit judgement of ‘Yes’ or ‘No’ (e.g. number randomised not stated, no reasons for missing data provided) or outcome not addressed;
-
No ‐ reason for missing outcome data likely to be related to true outcome, with either imbalance in numbers or reasons for missing data across intervention groups or for dichotomous outcome data, the proportion of missing outcomes compared with observed event risk enough to induce clinically‐relevant bias in intervention effect estimate, or for continuous outcome data, plausible effect size (difference in means or standardised difference in means) among missing outcomes enough to induce clinically relevant bias in observed effect size, or ‘as‐treated’ analysis done with substantial departure of the intervention received from that assigned at randomisation, or potentially inappropriate application of simple imputation.
-
-
Selective outcome reporting:
-
Yes ‐ if there is evidence that all of the study’s pre‐specified (primary and secondary) outcomes that are of interest in the review have been reported as stated in the protocol, or it is clear that the published reports include all expected outcomes, including those that were pre‐specified in the absence of the protocol;
-
Unclear ‐ insufficient information to permit judgement of ‘Yes’ or ‘No’;
-
No ‐ not all of the study’s pre‐specified primary outcomes have been reported; or one or more primary outcomes is reported using measurements, analysis methods or subsets of the data (e.g. sub scales) that were not pre‐specified, or one or more reported primary outcomes were not pre‐specified, or one or more outcomes of interest in the review are reported incompletely so that they cannot be entered in a meta‐analysis, or the study report fails to include results for a key outcome that would be expected to have been reported for such a study.
-
-
Other sources of bias:
-
Yes ‐ if study is free of other sources of bias;
-
Unclear ‐ insufficient information to assess if an important risk of bias exists or insufficient rationale or evidence that an identified problem will introduce bias;
-
No ‐ has extreme baseline imbalance or claimed to have been fraudulent or stopped early due to some data‐dependent process (including a formal ‐ stopping rule) or potential source of bias related to the specific study design used.
-
Measures of treatment effect
We performed data entry and analysis in Review Manager (RevMan) version 5.3 (RevMan 2014). For meta‐analysis of categorical variables we calculated Relative Risk (RR) or Peto's Odds Ratio (OR) with 95% confidence interval (Cl). For meta‐analysis of continuous variables we calculated mean differences (MD).
Unit of analysis issues
Cluster randomised trials
Only cluster‐randomised trials for which adjustment had been made for design effect were included in the meta‐analyses. Where possible, we corrected for design effects using standard procedures (Rao 1992). Before entering the results of cluster‐randomised studies into RevMan, we transformed outcome data according to the procedure in the Cochrane Handbook for Systematic Reviews of Interventions ( Adam 2004; Deeks 2011), dividing the number of events and number of participants by the design effect [1 + (1 ‐ m) * r]. We used the details provided by each study (total n and number of clusters) to calculate the average cluster size (m). Since most of the trials did not provide the intra cluster correlation coefficient, we adopted a fairly reliable intra cluster correlation coefficient of 0.02 which had been used in a similar systematic review (DiCenso 2002).
Trials with multiple groups
Eleven studies had multiple groups ( Dilorio 2006; Downs 2004; Herceg‐Brown 1986; Jemmott 1998; Jemmott 2005; Markham 2012; Morberg 1998;, Norton 2012; O'Donnell 1999; Raine 2005, Walker 2006, ). For studies included in the meta‐analyses (Dilorio 2006; Herceg‐Brown 1986; Jemmott 1998; Morberg 1998; Raine 2005), we combined all relevant experimental intervention groups in the studies into a single group. The same was done for the control groups as recommended by the Cochrane Handbook for Systematic Reviews of Interventions, Section 16.5.4 .(Higgins 2011b) For studies with multiple follow‐up points, we used data from the last time points.
Dealing with missing data
Missing data arose from participant attrition and missing statistics.
Where possible, we extracted data by allocation intervention, irrespective of compliance with the allocated intervention, in order to allow an 'intention‐to‐treat' analysis, as this minimizes bias (Hollis, 1999); otherwise we performed an 'as‐treated' analysis. We included these variables in a meta‐analysis using Review Manager (RevMan) 5.3 for the outcomes selected above (RevMan 2014). We conducted sensitivity analyses to investigate attrition as a source of heterogeneity and possible bias.
Where statistics were missing (numbers of participants per group, attrition rates, percentage affected for each outcome), we contacted primary study authors to supply the information. Where the information was unavailable due to data loss or non‐response, we reported the available results as stated in the trial report in the Additional table (Table 1).
| Intervention | Outcome | Study ID | Number Assessed | Case affected | Control affected | Test Statistics | 95% CI | p‐value |
| Educational intervention | Pregnancy | 1701 | ‐ | ‐ | OR: 0.97 | 0.93 to 1.0 | 0.04 | |
| Initiation of intercourse | 156 | ‐ | ‐ | Beta: 1.604 and SE: 1.00 | ‐ | < 0.11 | ||
| Aarons 2000 (females) | 139 | Adj. OR: 1.88 | 1.02 to 3.47 | 0.04 | ||||
| Aarons 2000 (males) | 123 | Adj. OR: 1.18 | 0.61 to 2.29 | 0.62 | ||||
| 1079 | ‐ | ‐ | OR: 1.00 | 0.70 to 1.41 | ||||
| Changes in knowledge and attitudes about the risk of unintended pregnancy | 351 | 92.9% | 91.8% | ns | ||||
| Use of birth control at last sex | Mitchell‐DiCenso 1997 (females) | 109 | 42.2% | 46.7% | OR: 1.03 | 1.00 to 1.07 | 0.03 | |
| Mitchell‐DiCenso 1997 (males) | 214 | 39.3% | 35.9% | OR: 1.06 | 1.02 to 1.77 | 0.005 | ||
| Aarons 2000 (females) | 135 | Adj. OR: 3.39 | 1.16 to 9.95 | 0.025 | ||||
| Aarons 2000 (males) | 125 | Adj. OR: 1.53 | 0.55 yo 4.26 | 0.42 | ||||
| Use of condom at last sex | 1896 | 39.1% | 31.9% | OR: 1.41 | 1.12 to 1.77 | ‐ | ||
| 221 | 77% | 73% | ||||||
| Unprotected intercourse in the past 3 monthsa | 502 | Beta: ‐0.375 and SE: 0.32 | >0.05 | |||||
| Ever had sex without condoms | Mean: 0.23 | Mean: 0.57 | ‐0.61 to ‐0.06 | 0.03 | ||||
| Multiple interventions | Pregnancy | 308 | ‐ | ‐ | OR; 0.84 | ‐ | 0.61 | |
| 460 | ‐ | ‐ | OR: 0.53 | 0.27 to 1.03 | 0.06 | |||
| 1172 | 2.3% | 3.3% | ‐ | ‐ | 0.07 | |||
| 2145 | ‐ | ‐ | OR: 1.34 | 0.98 to 1.84 | 0.07 | |||
| 417 | ‐ | ‐ | OR: 0.77 | 0.49 to 1.23 | 0.28 | |||
| 95 | ‐ | ‐ | ‐ | ‐ | < 0.05 | |||
| 195 | 6.8% | 18.5% | ||||||
| 323 | B=‐.823 OR: 0.44 | 0.009 | ||||||
| 560 | ‐ | ‐ | OR: 0.41 | ‐ | ‐ | |||
| Initiation of sexual intercourse (mixed gender) | 94 | ‐ | ‐ | OR: 1.23 | 0.51 to 2.97 | 0.65 | ||
| 95 | .Mean: 1.19 | .Mean: 2.74 | ||||||
| 8326 | ‐ | ‐ | OR: 1.03 | 0.88 to 1.21 | 0.69 | |||
| 627 | AOR:0.65 | 0.54,0.77 | <.01 | |||||
| 195 | 40.1% | 66.1% | OR: 0.39 | 0.20 to 0.76 | 0.005 | |||
| 735 | AOR:0.82 | 0.51,1.34 | >0.05 | |||||
| 2565 | OR:1.13 SE: 0.24 | 0.71 to 1.82 | 0.60 | |||||
| Initiation of sexual intercourse (male) | 1412 | 19.3% | 27.7% | model R2: 0.118 | ‐ | 0.02 | ||
| 809 | ‐ | ‐ | OR: 1.08 | 0.80 to 1.46 | 0.63 | |||
| 8156 | 32.7% | 31.1% | OR: 0.90 | 0.65 to 1.23 | 0.35 | |||
| 408 | 36% | 44% | ‐ | ‐ | ‐ | |||
| Initiation of sexual intercourse (female) | 1417 | 20.3% | 22.1% | model R2: 0.145 | ‐ | 0.53 | ||
| 1220 | ‐ | ‐ | OR: 0.88 | 0.59 to 1.31 | 0.54 | |||
| 8156 | 34.7% | 40.8% | OR: 0.80 | 0.66 to 0.97 | 0.008 | |||
| 480 | 27% | 22% | ‐ | ‐ | ‐ | |||
| Use of condoms at last sex | 2145 | ‐ | ‐ | OR: 1.38 | 1.06 to 1.79 | 0.02 | ||
| 359 | ‐ | ‐ | OR: 1.00 | 0.49 to 1.23 | 0.99 | |||
| 460 | ‐ | ‐ | OR: 3.94 | 2.58 to 6.03 | < .001 | |||
| 258 | ‐ | ‐ | OR: 2.13 | ‐ | 0.15 | |||
| 198 | OR: 0.93 | ‐0.75,0.62 | 0.85 | |||||
| 1018 | OR:191 SE:0.27 | 1.13 to 3.21 | 0.02 | |||||
| Childbirth | 4196 | 300/1000 | 274/1000 | OR: 14.6 | 0.32 | |||
| Abortion | 4196 | 127/1000 | 112/1000 | OR: 26.4 | 0.40 | |||
| Consistent condom use at 12 months | 253 | Mean: 0.96 (116/126) | Mean: 0.66 (81/127) | ARR:145 | 1.26 to 1.67 | 0.00 | ||
| Consistent condom use at 24 months | 204 | Mean:1.53 | Mean: 0.93 | ARR: 1.57 | 1.28,1.94 | |||
| Consistent hormonal contraceptive use at 12 months | 253 | Mean: 4.27 (74/126) | Mean: 2.91 (51/127) | ARR:1.46 | 1.13 to 1.89 | 0.00 | ||
| Consistent hormonal contraceptive use at 24 months | 203 | Mean: 3.29 | Mean: 2.34 | ARR: 1.30 | 1.06,1.58 | |||
| 162 | OR:0.42 | 0.12 | ||||||
| Use of condoms at first sex | 285 | OR:0.68 SE:0.48 | 0.26 to 1.75 | 0.42 | ||||
| Protected against pregnancy at last sex | 998 | OR:1.62 SE:0.22 | 1.05 to 2.50 | 0.03 | ||||
| Sexually Transmitted Infections | 323 | B=‐0.067 OR: ‐0.94 | 0.77 | |||||
| Mean:10.5 SE: 2.9 | Mean:18.2 SE:2.8 | 0.05 | ||||||
| Baird 2010: The following listed outcomes were reported. However, the method of reporting made difficult to extract correct estimates. 1. Pregnancy School girls and dropouts among the treatment group are 1.1 percentage points less likely to have become pregnant over the past year. Not statistically significant. | ||||||||
a ‐ Binary outcome (did unprotected intercourse occur or not?)
b ‐ Study (Stephenson 2008) same as Stephenson 2004, but with an extended follow up (7yrs)
c ‐ Data comparing skills‐based intervention versus health‐promotion intervention
Analyses assessing impact on delay of sexual initiation excluded individuals who reported any type of sexual intercourse at baseline
Analyses assessing impact on other on sexual behaviours are limited to individuals that are sexually active
ns ‐ non‐significant
Assessment of heterogeneity
We assessed data sets for heterogeneity by visual assessment of forest plots and chi2 tests for heterogeneity with a 10% level of statistical significance, and applied the I2 statistic with a value of 50% or higher denoting significant levels of heterogeneity.
Assessment of reporting biases
Since asymmetry of funnel plots may result from publication bias, heterogeneity, or poor methodological quality (Sterne 2011), we planned to examine funnel plots using Review Manager 5.3 but found an insufficient number of trials to do this.
Data synthesis
We used a fixed‐effects model (FEM) for data synthesis and a random‐effects model (REM) for cases where we detected heterogeneity, and considered it appropriate to still perform meta‐analysis.
Subgroup analysis and investigation of heterogeneity
We sub‐grouped the use of birth control into 'condom use at last sex', 'consistent condom use', 'contraceptive use at last sex', 'consistent contraceptive use' and 'use of hormonal contraceptive'. We found insufficient data to conduct sub‐group analysis of homosexual and heterosexual intercourse. We excluded quasi‐experimental studies (controlled before‐and‐after, and interrupted time series) as this was cumbersome and would have delayed the update of this review.
Sensitivity analysis
We conducted sensitivity analysis of the primary outcome (unintended pregnancy) including and excluding trials with high attrition rates (> 20%). The number of trials that used adequate allocation concealment was insufficient to allow for sensitivity analysis to assess the possible influence of high risk of bias in trials that did not apply allocation concealment.
Results
Description of studies
Results of the search
We found 142 studies, of which we included 53 and excluded 87 , with two awaiting assessment (Characteristics of studies awaiting classification); we have approached the primary authors of these papers for relevant additional information.
Included studies
All the studies were randomised controlled trials. Eighteen of the studies randomised individuals, 32 randomised clusters (schools (20), classrooms (6), and communities/neighbourhoods such as community‐based organisations and social networks (6). Three studies were mixed (individually and cluster randomised) (Allen 1997; Eisen 1990; Kirby 1997b). The length of follow up varied from three months to seven years, with greater than 12 months being the most common duration.
Participants
A total of 105,368 participants were included in all the included studies. The number of participants per study varied greatly (Characteristics of included studies). Most of the studies confined inclusion of participants to specific age requirements, others restricted inclusion based on specific school grade levels (varying between 6th grade to 12th grade). The age of participants in the included studies ranged from 9 years to 19 years, except for seven studies which included participants aged 9 years to 24 years: Baird 2010, 13 years to 22 years; Mba 2007, 10 years to 20 years; Minnis 2014, 16 years to 21 years; Okonofua 2003, 14 years to 20 years; Raine 2005, 15 years to 24 years (mean 19.9); Raymond 2006, 14 years to 24 years; and Shrier 2001, 13 years to 22 years (median 17). For these studies, more than 75% of the participants were within the stipulated age limit of 10 years to 19 years. Sixteen studies included participants who were sexually active (Baird 2010; Bonell 2013; Diclemente 2004; Downs 2004; Jemmott 2005, Jemmott 2010; Kogan 2012; Markham 2012; Mba 2007; Minnis 2014; Morrison‐Beedy 2013; Norton 2012; O'Donnell 1999; Raine 2005; Raymond 2006; Sieving 2011); one study recruited adolescent mothers < 18 years at time of delivery living with their mothers (Black 2006); three studies recruited dyads (adolescents and their guardian) (Dilorio 2006; Dilorio 2007; Guilamo‐Ramos 2011b). Most studies included male and female participants. Eighteen studies included female participants only (Allen 1997; Baird 2010; Black 2006; Bonell 2013; Cabezon 2005; Diclemente 2004; Downs 2004; Ferguson 1998; Guilamo‐Ramos 2011b; Henderson 2007; Herceg‐Brown 1986; Howard 1990; Jemmott 2005; Morrison‐Beedy 2013; Raine 2005; Raymond 2006; , Shrier 2001; Sieving 2011) and one, male participants only (Dilorio 2007).
Setting
Four trials were conducted in low‐ and middle‐income countries (Baird 2010; Fawole 1999; Mba 2007; Okonofua 2003), and all others were conducted in high‐income countries: United States of America (41), England (2), Scotland (2), Canada (1), Italy (1) and Mexico (2). Most of the studies were conducted in schools. Other sites included hospitals or family planning health agencies, neighbourhoods/communities and clubs.
Interventions
Educational interventions
Six studies compared an educational interventions to a standard school curriculum (control): Aarons 2000; Blake 2001; Clark 2005; Dilorio 2007 (parent‐based educational intervention); Mitchell‐DiCenso 1997; and Perskin 2015 (computer‐based sexual health education). Three studies compared the intervention to regular health promotion classes or no control intervention (Kogan 2012; Mba 2007; Okonofua 2003). One study offered the same intervention to the two groups but with different instructors (peers or teachers) (Borgia 2005). Another study compared a parent‐based intervention based on social cognitive theory (intervention 1) and a life skills programme based on problem behaviour theory (intervention 2) versus a one‐hour HIV‐prevention session (control) (Dilorio 2006);
Contraceptive‐promoting interventions
Two studies compared the effect of improving access to contraception. Raine 2005 had two intervention groups (pharmacy access and advance provision of contraceptives) and a control (clinic access, as needed); Raymond 2006 compared increased access to contraceptives (unlimited free supply) versus standard access (as needed, at usual cost). Another study compared contraception education to usual school sex education (Graham 2002).
Multiple interventions (educational and contraceptive‐promoting interventions)
Twelve studies compared a combination of educational interventions and contraceptive‐promoting interventions with standard school curriculum (sex or HIV/AIDS education) (Basen‐Engquist 2001; Coyle 1999; Coyle 2004; Coyle 2006; Eisen 1990; Fawole 1999; Henderson 2007; Howard 1990; Kirby 1997a; Kirby 2004; Shrier 2001; Wight 2002). Sieving 2011 compared multiple interventions linked to clinical services versus usual clinical service only for 17 months and 24 months, and Bonell 2013 compared weekly three‐hour sessions over 18 weeks to 20 weeks in pre‐school nurseries developing parenting, self‐awareness and confidence versus health promotion only . Three studies added community youth services to their intervention versus the following control groups: regular health curriculum (Allen 1997) and standard class curriculum (O'Donnell 1999; O'Donnell 2002).
Four studies compared multiple interventions with health promotional interventions unrelated to sexual behaviour, or no intervention for the control groups (Cabezon 2005; Diclemente 2004; Morrison‐Beedy 2013; Villarruel 2006 ). One study offered written materials on the lessons covered in the intervention programme to the control group (Smith 1994).
Nine studies compared more than one intervention (multiple intervention groups). Jemmott 1998 had two interventions, one with an emphasis on abstinence versus one with an emphasis on the use of contraceptives, compared to a health promotion control. Jemmott 2005 compared the same intervention (informative versus skills‐based (practical) versus health promotion (control). Kirby 1997b compared an adult‐led intervention versus a youth‐led intervention (each with the same contents) compared to the standard sex curriculum. Markham 2012 compared risk avoidance (abstinence until marriage) versus risk reduction (with the emphasis on abstinence until older) versus a control of regular health classes. Morberg 1998 compared a four‐week intervention over three years in one intervention group and a 12‐week intervention over one year in the other, versus the usual school curriculum. Walker 2006 used the same intervention for both intervention groups but one emphasised the use of condoms and the other emphasised access to condoms and emergency contraceptives, versus biology‐based sex education.. . . Two studies compared three intervention groups with different aims. Jemmott 2010 compared three different levels of training: enhanced training (intervention package, two days' training plus hands‐on training/practice); standard training (intervention package plus two days' training); and manual only (intervention package provided to participants but no training) compared to non‐sexual‐related health promotion intervention (control). Norton 2012 compared the promotion of condom use to prevent an unplanned pregnancy (pregnancy intervention), STI (STI intervention), and HIV (HIV intervention), versus standard health services received by students. . Herceg‐Brown 1986 had two intervention groups, regular clinic services plus 50 minutes of family or individualised counselling services on sex and contraceptive education for six weeks known as the 'Family support group', versus regular clinic services plus staff support through two to six telephone calls four to six weeks after the initial clinic visit, known as the 'Periodic support group', versus regular clinic services.
One study, Downs 2004 had one intervention and two control groups. The same information was provided to the control groups as to the intervention group, however they differed in their mode of administration (interactive video versus book form or brochure for the controls). Another study, Guilamo‐Ramos 2011b evaluated a parent‐based intervention (health education and skills‐building); parents and their adolescent children participated in the intervention, versus standard health promotion for nine months.
Two studies offered some form of incentive to the intervention group; Minnis 2014 combined conditional cash transfers (CCT) as an incentive for completing educational, reproductive health and life skills sessions; while Baird 2010 provided CCT (an incentive for schoolgirls and dropouts to stay in school or return to school respectively), with the aim of reducing certain sexual behaviours.
One study offered peer‐led multiple interventions versus usual teacher‐led sex education (Stephenson 2004), while another compared same intervention administered by peer counsellors compared to adult staff (Ferguson 1998).
One study compared the intervention with an alternative youth programme (recreational activities, art & crafts) (Philliber 2002).
Black 2006 aimed to prevent a second unintended pregnancy. The intervention involved a home‐mentoring programme (home visits every week until the infant's first birthday, approximately 19 visits) compared to a no‐intervention control ().
Outcomes
Twenty studies assessed and reported on unintended pregnancy (Allen 1997; Bonell 2013; Cabezon 2005; Coyle 2006; Diclemente 2004; Ferguson 1998; Herceg‐Brown 1986; Howard 1990; , Kirby 1997a; Kirby 1997b; Kirby 2004; Mitchell‐DiCenso 1997; Morrison‐Beedy 2013; O'Donnell 2002; Philliber 2002; , Raine 2005; Raymond 2006; Smith 1994; Stephenson 2004; Wight 2002 , , , , ) and one study reported second unintended pregnancy (Black 2006). Other outcomes reported were initiation of intercourse, consistent use of contraceptives or condoms, use of contraceptives or condoms at last sex, use of hormonal contraceptives, knowledge about the risk of pregnancy, abstinence, sexually transmitted diseases, childbirth and abortion.
Most studies reported outcomes on the change in knowledge of STD, HIV, AIDS, condom and contraceptive use, as well as intentions to use condoms, contraceptives or have sex. However, these were not part of the outcomes assessed in this review and therefore were not reported.
Excluded studies
Eighty‐four studies were excluded; forty‐six studies, though randomised studies were excluded for one or more of the following reasons: none of the desired outcomes was measured, participants were either pregnant or couples, more than 25% of the participants were above the required age range, the study did not use the desired intervention, there was no formal control group, had no protocol, and the stated method of randomisation was not adequate. The remaining studies (38) were not randomised controlled studies (Characteristics of excluded studies).
No ongoing studies were found.
Risk of bias in included studies

Risk of bias summary: review authors' judgments about each risk of bias item for each included study.
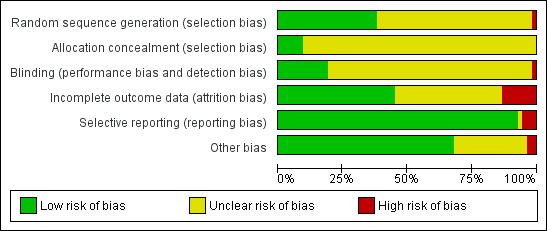
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
Generation of allocation sequence: ten studies used a computer‐generated allocation sequence (Bonell 2013; Dilorio 2006; Graham 2002; Jemmott 1998; Jemmott 2005; Jemmott 2010; Raine 2005; Raymond 2006; Stephenson 2004; Villarruel 2006), four used a table of random numbers (Diclemente 2004; Downs 2004; Mitchell‐DiCenso 1997, Shrier 2001), one used simple balloting (Cabezon 2005), two used coin toss technique (Allen 1997; Ferguson 1998). Two trials used restricted randomisation involving multiple steps (Coyle 2004, Coyle 2006), and two other studies used block randomisation (Morberg 1998; Philliber 2002,). One trial reported use of "balanced randomisation" (Wight 2002) but gave no details to explain the procedure, and another one used quarterly marking period within school (Blake 2001). One study used a modified "multi‐attribute randomization method", providing no further details (Perskin 2015). The remaining studies (29) had insufficient or no information on the randomisation generation method, and used terms such as "assigned at random" or "randomly assigned", leaving us uncertain whether the trial results were vulnerable to selection bias.
Allocation concealment: four studies reported adequate allocation concealment that used sealed, opaque envelopes (Diclemente 2004; Philliber 2002; Raine 2005; Raymond 2006). The remaining studies did not provide information on concealment of allocation.
Baseline differences can be increased by inadequate and clustered randomisation sequences. Out of the 53 trials, 17 reported at least one significant group difference at baseline (Aarons 2000; Allen 1997; Basen‐Engquist 2001; Coyle 2004; Coyle 2006; Dilorio 2006; Jemmott 1998; Jemmott 2005; Jemmott 2010; Kirby 1997b; Markham 2012; Mitchell‐DiCenso 1997; Morberg 1998; Okonofua 2003; Raymond 2006; Smith 1994 ) and each one of these trials controlled for baseline differences in analyses. One study Mba 2007, did not test for baseline differences between groups.
Three trials did not report a clear statement of baseline differences between groups (Dilorio 2007; Ferguson 1998; Henderson 2007) but controlled for these differences in their analyses. One trial used a significance level of P < 0.01 for these calculations (Kirby 1997a), and two reported baseline differences only for sexual behaviours (Clark 2005; O'Donnell 2002).
Blinding
For most of the trials, staff (assessors and administrators) were not blinded to group assignment, as every trial utilised written self‐reported questionnaires, although assessor blinding was reported in eight studies (Black 2006; Bonell 2013; Diclemente 2004; Jemmott 1998; Raine 2005; Shrier 2001; Stephenson 2004; Wight 2002 ). Two studies blinded participants and interviewers (Jemmott 2010; Minnis 2014). For one study, the condition was unknown to participant and facilitators until groups were filled and facilitators assigned (Morrison‐Beedy 2013) and for another, the condition was unknown only to participants until after baseline assessment (Perskin 2015). Blinding was not reported in the remaining 42 studies. The impossibility of blinding intervention staff may have given rise to performance bias.
Contamination or 'exchange of information' of the control group might have occurred as the intervention and control groups sometimes attended different programmes at the same site. This is more likely to be present in trials that randomised participants by individual or classroom, rather than by entire community centre, school or neighbourhood. This, however, leads to bias in the findings in the direction of no effect rather than in the direction of significance.
Incomplete outcome data
Attrition rates at final follow‐up ranged from 0.5% (Henderson 2007) to 58% (Coyle 2006). Five studies did not clearly explain/state the numbers of individuals lost to follow up (Baird 2010; Basen‐Engquist 2001; Blake 2001; Howard 1990; Norton 2012). Eighteen trials reported overall attrition rates that exceeded 20% at final follow up (Borgia 2005; Clark 2005; Coyle 2004; Coyle 2006; Dilorio 2007; Eisen 1990; Jemmott 2010; Kirby 1997a; Kirby 2004; Markham 2012; Mitchell‐DiCenso 1997; Morberg 1998; O'Donnell 2002; Philliber 2002; Shrier 2001; ,Smith 1994; Stephenson 2004; Walker 2006 , . ).
Most trials conducted a modified intention‐to‐treat analysis (whereby all students were included in the analysis regardless of number of sessions attended as long as they provided baseline and follow‐up data). Outcomes such as pregnancy, use of condoms, contraceptive and sexually transmitted diseases were analysed using the number who initiated sex or were already sexually active as the sample size (denominator). Coyle 2004 made use of a rich‐imputation model based on baseline peer norms, group, time, ethnicity, and group‐by‐time interaction to account for dropouts. O'Donnell 2002 conducted several sets of analyses according to different principles: not reporting results according to original dropouts.
Studies with outcomes that could not be included in the meta analysis are reported in Table 1.
Selective reporting
Apart from the primary outcome, most included studies reported a range of outcomes (sexual behaviour), using different recall periods and grouping outcomes such as initiation of intercourse at three months and six months, and use of condoms at last sex, thus suggesting no standard set of outcomes for evaluation, preventing a comprehensive meta‐analysis.
Results were also analysed based on subgroups of participants, for example, measuring initiation of intercourse among virgins and non‐virgins at baseline. However, more often, sexual initiation was often assessed only among participants who reported never having had sexual intercourse at baseline.
Few studies reported at least one outcome separately by gender without providing overall summaries of effect (Aarons 2000; Coyle 2004; O'Donnell 2002).
Due to missing information such as numbers of participants per trial arm and percentages for dichotomous outcomes, meta‐analysis could not be carried out for some studies (data presented in Table 1).
The lack of statistical controls for cluster‐randomised data, is a limitation for this study. While most cluster randomised studies controlled for clustering in their analyses, some did not (Aarons 2000; Allen 1997; Fawole 1999; Kirby 1997a), suggesting that studies which did not report statistical methods for dealing with clustered data analysed their results on an individual level.
Few studies attempted to control for the occurrence of a Type I error which is likely to occur when different outcomes are analysed; Allen 1997 and Raine 2005 used a Bonferroni correction when considering the significance of statistical tests, and Coyle 2004 stated it use though the method was not specified.
Other potential sources of bias
Limitations of self‐report and behavioural outcome data
Most of the studies made use of self‐reported data which is an inevitable source of bias for studies evaluating sexual behaviours (as there is the tendency for respondents to agree with statements associated with healthier behaviours or attitudes). However, the veracity of the self‐reported behaviours was improved by privacy and confidentiality in most studies.
Heterogeneity in programme design and implementation across trials
A major source of bias in this review is a high degree of heterogeneity in the ways programmes were designed and implemented across trials. This can be seen in some of the meta‐analyses carried out. Our inclusion criteria specified that we would accept interventions that aimed to prevent unintended pregnancy while promoting safer‐sex strategies such as condom use or contraceptive use but it is unclear how much emphasis was put on these goals. An example is Eisen 1990 that offered almost the same intervention to both groups differing only in the level of emphasis and duration of the intervention, or studies offering same intervention but administered differently such as peer‐counsellor facilitators versus adult staff (Ferguson 1998) and Downs 2004, interactive video versus book form or brochure of the same intervention.
Finding relevant trials
Though the search for relevant trials was comprehensive, it is likely that relevant trials may have been omitted from this review, if the specified search terms were not mentioned in the title and abstracts but most likely due to inability to assess all unpublished trials.
Underreporting of implementation data
Inadequate description of programme design and implementation made the assessment of heterogeneity challenging. Differences in the way that programmes were designed, delivered, and taken up may have made the studies too heterogeneous to permit comparisons across trials; however, these differences are difficult to determine from the available data and could have influenced the meta‐analyses. Few studies reported strategies to monitor and promote the extent to which programmes were delivered by facilitators and taken up by participants as planned. Such strategies include take‐home assignments, keeping attendance records, conducting interviews with programme staff and participants, bringing in independent raters (Morrison‐Beedy 2013), conducting exit interviews with participants, and communication with participants by phone (Herceg‐Brown 1986, Dilorio 2006). One study regularly trained all programme staff, visiting each site regularly (Philliber 2002). Though these strategies were put in place, most trials rarely stated the extent of implementation fidelity. One study Morberg 1998, reported difficulties for community‐based programme activities to convey programme messages related to sexual behaviour due to vocal opposition; at one programme site, a member of the community opposition group attended every programme session related to sexual behaviour, potentially affecting programme delivery.
Effects of interventions
See: Summary of findings for the main comparison ; Summary of findings 2 ; Summary of findings 3 ; Summary of findings 4
MULTIPLE INTERVENTIONS
Unintended pregnancy
Four individually randomised trials (Bonell 2013; Herceg‐Brown 1986; Morrison‐Beedy 2013; Philliber 2002), showed that risk of unintended pregnancy was significantly lower among participants that received multiple interventions compared with the control group; (RR 0.66, 95% CI 0.50 to 0.87; 4 studies; 1905 participants, Analysis 1.1).
Five cluster trials (Cabezon 2005; Ferguson 1998; Howard 1990; Kirby 1997b; Wight 2002) that adjusted for design effect showed a 50% reduction in the risk of unintended pregnancy in the intervention group compared to the control group, although the difference was not statistically significant ((RR 0.50, 95% CI 0.23 to 1.09; 5 studies, 3149 participants, Analysis 1.2). However sensitivity analysis excluding trials with high attrition rates showed that the risk of unintended pregnancy was significantly lower in the intervention than control groups ((RR 0.20, 95% CI 0.10 to 0.39; 2 studies, 497 participants, Analysis 2.1). In addition, an analysis that combined cluster‐randomized trials (adjusted for design effect) with individually randomised trials (Bonell 2013; Cabezon 2005; Ferguson 1998; Herceg‐Brown 1986; Morrison‐Beedy 2013 ) showed significantly lower risk of unintended pregnancy in the intervention group compared to control (RR 0.53, 95% CI 0.39 to 0.72; 5 studies,1918 participants,Analysis 2.3 ). This sensitivity analysis showed a persistence of statistical heterogeneity with I2 statistic of 77% (Analysis 2.3).
Table 1 shows trials with insufficient data for inclusion in meta‐analyses. Based on trial authors' conclusions, two of the trials reported results in favour of the intervention groups suggesting that the intervention reduced the risk of unintended pregnancy (Morrison‐Beedy 2013; Smith 1994).
Initiation of sexual intercourse
Four individually randomised trials (Guilamo‐Ramos 2011b; Jemmott 1998Philliber 2002; Villarruel 2006) reporting initiation of intercourse among a mixed gender sample showed no significant difference between participants in the intervention and control groups with respect to time of initiation of sexual intercourse (during the intervention or in the follow up period) (RR 0.99, 95% CI 0.74 to 1.32; 4 studies, 1796 participants, Analysis 1.3).
Seven cluster randomised studies (Fawole 1999; Ferguson 1998; Howard 1990; Kirby 1997a; Morberg 1998; O'Donnell 1999; Wight 2002) that merged male and female participants showed no statistically significant difference in effects between intervention and control groups (RR 0.84, 95% CI 0.68 to 1.04; 7 studies, 8608 participants, Analysis 1.4).
Sensitivity analysis excluding trials with high attrition rates also showed no statistically significant difference in effects in three individual randomised trials (Guilamo‐Ramos 2011b; Jemmott 1998; Villarruel 2006) (RR: 1.18, 95% Cl 0.67 to 2.09) and four cluster randomised trials (Fawole 1999; Ferguson 1998; Morberg 1998; O'Donnell 1999) (RR 0.84, 95% CI 0.57 to 1.25). Meta‐analysis including cluster‐randomized trials (adjusted for design effects) and individually randomised trials also showed no statistically significant difference in effects between intervention and control groups (RR 0.88, 95% CI 0.74 to 1.05, Analysis 3.3).
The summary of results of 8 trials (Basen‐Engquist 2001; Coyle 2004; Coyle 2006; Eisen 1990; Kirby 2004; Markham 2012; Smith 1994; Stephenson 2004) that reported this outcome but had insufficient data to meta‐analyse has been presented in Table 1. One trial (Markham 2012) with mixed gender participants, reported significantly lower risk of initiation of sexual intercourse in the intervention group compared to the control group.Two trials reporting effects among male participants (Coyle 2004; Eisen 1990) concluded that participants who had multiple interventions were less likely to initiate intercourse during the period of follow‐up in comparison to the control arm. One trial (Stephenson 2004) which reported initiation of sexual intercourse in female participants, also showed significant effects in favour of the intervention.
Use of birth control methods
a) Condom use at last sex
Three individually randomised trials (Bonell 2013; Philliber 2002; Shrier 2001) showed no difference between intervention and control groups with respect to condom use at last sex (RR 1.00, 95% CI 0.95 to 1.06; 3 studies, 796 participants, Analysis 1.5)
Four cluster‐randomised trials (Fawole 1999; Jemmott 2010; Kirby 1997a; Walker 2006) reported condom use at last sex showed no statistically significant differences between intervention and control groups (RR: 1.01, 95% CI 0.93 to 1.09; 4 studies, 2620 participants, Analysis 1.6).
b) Consistent condom use (in prior 90 days and more)
Five individually randomised trials (Herceg‐Brown 1986; Jemmott 1998; Morrison‐Beedy 2013; Sieving 2011; Villarruel 2006) which reported consistent condom use, similarly showed no statistically significant differences between intervention and control groups (RR 1.21, 95% CI 0.95 to 1.54; 5 studies, 1681 participants, Analysis 1.5)
Three cluster‐randomised trials (Ferguson 1998; Jemmott 2010; Morberg 1998) reported consistent condom use in at least the preceding 90 days. There however was no statistically significant difference between intervention and control groups (RR 1.95, 95% CI 0.70 to 5.44; 3 studies, 826 participants, Analysis 1.6). There was also a significantly high level of heterogeneity (I2= 93%).
c) Contraceptive use at last sex
One individually randomised trial (Bonell 2013) reported no significant difference in the risk of contraceptive use at the last sex between intervention and control groups (RR 0.99, 95% CI 0.95 to 1.03; 1 study, 408 participants, Analysis 1.5).
d) Consistent contraceptive use at 24 months
Another individually randomised trial (Sieving 2011) reported consistent contraceptive use up to 24 months post‐intervention. However, there was no significant difference between the intervention and control groups (RR 1.29, 95% CI 1.06 to 1.59; 1 study, 253 participants, Analysis 1.5).
e) Hormonal contraceptive use
Three cluster‐randomised trials (Kirby 1997a; Walker 2006; Wight 2002) which reported hormonal contraceptive use showed no difference between intervention and control groups (RR 1.01, 95% CI 0.72 to 1.43; 3 studies, 3987 participants, I2= 85%, Analysis 1.6)
Sexually Transmitted Diseases (STD)
Two individually randomised controlled trials (Morrison‐Beedy 2013; Shrier 2001) measured STD reporting in the intervention group (61/359) compared with the control group (65/340) (RR 0.89, 95% CI 0.65 to 1.22; 2 studies, 699 participants, Analysis 1.7).
Two cluster RCTs (Fawole 1999; Kirby 1997b) measured STD reporting in the intervention group (6/205) compared with the control group (8/215) (RR 0.72, 95% Cl 0.26 to 2.02, Analysis 1.8). Neither the individual nor cluster randomised trials showed statistically significant effects.
Childbirth
One cluster randomised trial (Stephenson 2004) reported that relatively fewer participants in the intervention group (178/2529) than in the control group (237/2247) had experienced childbirth during the period of observation; the difference was statistically significant (RR 0.64, 95% CI 0.52 to 0.79; 1 study, 4776 participants, Analysis 1.9)
One individually randomised study (Philliber 2002) reported that relatively fewer participants in the intervention group (10/242) than in the control group (15/242) had experienced childbirth during the period of observation; the difference was, however, not statistically significant (RR 0.67, 95% Cl 0.31 to 1.45, 1 study, 484 participants, Analysis 1.10).
Second unintended pregnancy
One study (Black 2006) reported a lower risk of second unintended pregnancy in the intervention group (8/70) compared to the control group; the difference in effect approached statistical significance (19/79) (RR: 0.48, 95% Cl 0.22 to 1.02; 1 study, 149 participants, Analysis 1.11).
Abortion
One cluster randomised trial (Stephenson 2004) reported no statistically significant difference in the incidence of abortion between participants in the intervention group and the control group (RR 0.93, 95% CI 0.72 to 1.21; 1 study, 4776 participants, Analysis 1.12)
EDUCATIONAL INTERVENTIONS
Initiation of sexual intercourse
Two cluster RCTs (Clark 2005; Dilorio 2006) of an educational intervention showed no statistically significant difference in the proportion of participants that initiated sexual intercourse during follow‐up in the intervention group and control (RR 0.95, 95% Cl 0.71 to 1.27, Analysis 4.1).
Condom use at last sex
Two cluster RCTs (Borgia 2005, Dilorio 2006) showed that condom use at last sex was statistically significantly higher in the intervention group (258/704) than control group (190/727) (RR 1.18, Cl 1.06 to 1.32, Analysis 4.2).
Use of contraceptives
One study (Mba 2007) reported a significant increase in the use of contraceptives in the intervention group (35/180) compared to control group (14/180) (RR 2.50, 95% CI 1.39 to 4.48; 1 study, 360 participants, Analysis 4.3).
Changes in knowledge and attitudes about the risk of unintended pregnancies
Only one study (Blake 2001) clearly reported the above outcome by assessing change in knowledge on the risks of pregnancy at first intercourse and found no significant difference between intervention and control groups (see Table 1).
CONTRACEPTIVE‐PROMOTING INTERVENTIONS
Unintended pregnancy
Two individually randomised trials (Raine 2005, Raymond 2006) (3440 participants) showed no statistically significant difference in risk of unintended pregnancy between the intervention group (133/1572) and control (155/1868) (RR 1.01, 95% CI 0.81 to 1.26, Analysis 5.1).
Initiation of Sexual Intercourse
One cluster RCT (Graham 2002) measured initiation of sexual intercourse. The result showed no statistically significant difference in effect between intervention and control, neither for male participants (RR 1.02, 95% Cl 0.87 to 1.21; 1560 participants) nor female (RR 0.89, 95% Cl 0.76 to 1.04; 1446 participants, Analysis 5.2).
Use of birth control
See Analysis 5.3 and Analysis 5.4
a) Condom use at last sex
Two individual RCTs (Raine 2005, Raymond 2006) of contraceptive‐promoting interventions showed no statistically significant difference in condom use at last sex between intervention group (457/1395) and control group (622/1696) (RR 0.94, 95% Cl 0.87 to 1.04).
b) Consistent condom use
One individual RCT (Raine 2005) measured the consistent use of condoms in sexual intercourse; the result showed no statistically significant difference between intervention group (99/826) and control group (149/1124) (RR 0.90, 95% Cl 0.71 to 1.15).
c) Hormonal contraceptive use
Two individual RCTs (Raine 2005, Raymond 2006) showed that the rate of hormonal contraceptive use was significantly higher in the intervention group (366/1395) than in the control group (279/1696) (RR 2.22, 95% Cl 1.07 to 4.62). The analysis showed a statistically significant heterogeneity (I2 = 86%).
One cluster RCT (Graham 2002) found no statistically significant difference in use of emergency contraceptives between the intervention group (63/195) and control (79/220) (RR 0.90, 95% Cl 0.69 to 1.18, Analysis 5.3).
Sexually Transmitted Diseases (STD)
Two individual RCTs (Raine 2005, Raymond 2006) of contraceptive‐promoting interventions showed no statistically significant difference in risk of sexually transmitted diseases between the intervention group (143/1572) and control group (193/1868) (RR: 0.92, 95% Cl 0.75 to 1.13, Analysis 5.5).
Discussion
Summary of main results
Limited information suggests that programmes that involve concurrent application of multiple interventions (educational, skill building and contraception promotion) can reduce rates of unintended pregnancies in adolescents. Reviews done by Kirby 2002c; Manlove 2002; National Research Council (NRC 1987) have also highlighted the need for multiple strategies to address this public health challenge. Sensitivity analyses including trials with lower risk of bias showed that more cases of unintended pregnancy were reported in the control group than those that received multiple preventive interventions. Promoting the use of contraceptive measures alone did not appear to reduce the risk of unintended pregnancy. There was insufficient data to show whether education as a single intervention would reduce the risk of unintended pregnancy.
The possible effects of these preventive interventions on secondary outcomes such as time of initiation of sexual intercourse, risk of sexually transmitted infections and use of contraceptive measures like condoms and pills were not conclusively determined because of insufficient data and variation in methods of reporting.
Overall completeness and applicability of evidence
External validity
Some of the limitations of this review include the relatively small data sets available for the main outcomes of interest, and the likelihood of incomplete reporting of such outcomes as abortion, which have the potential to affect the rate of unintended pregnancy reported.
Furthermore, most of the trials were conducted in high‐income countries, thus this may limit the applicability of the results in middle‐ or low‐income countries.
Another limitation is the small number of studies with a true control group (without any intervention capable of reducing the incidence of unintended pregnancy). Because most of the trial settings already had community‐wide interventions (primarily in schools) aimed at improving adolescent sexual behaviours, it was difficult to find trials that had a control arm that was totally devoid of any form of educational intervention. The situation is likely to be different in low‐income countries, where such interventions may not be as widespread, making it more feasible to set up trials with true control arms.
Evidence in the practice context
The evidence provided in this review shows that concurrent application of preventive interventions such as education, skills‐building and contraception promotion could lower the incidence of unintended pregnancies in adolescents but the fact that most of the trials were conducted in industrialised countries (especially the USA) and among the lower socio‐economic populations, raises issues about applicability. The socio‐cultural context as well as cost implications of these interventions should be considered in efforts to introduce such measures in low‐income countries. Many low‐ and middle‐income countries may lack the infrastructure and resources to successfully implement these interventions. Trials in such resource‐poor settings would be needed to address some of these contextual and location‐specific issues.
Summaries for stakeholders
Application of the findings of this review should be approached with caution given the methodological deficiencies of included trials, the substantial heterogeneity across trials in the ways programmes were delivered and the frequent omission of methodological details and implementation information from primary trial reports.
Quality of the evidence
We assessed the quality of the evidence using the GRADE approach (Schünemann 2011) and have presented it in four ’Summary of findings’ tables (summary of findings Table for the main comparison; summary of findings Table 2; summary of findings Table 3; summary of findings Table 4). We assessed the evidence for the following outcomes: reduction of unintended pregnancy; reduction in the initiation of sexual intercourse; and increase in the use of birth controls (condoms or hormonal contraceptives, or both) for the different groups of interventions.
Unintended Pregnancy
We considered the evidence for a reduction in unintended pregnancies to be moderate quality, and low quality for both the contraceptive‐promoting interventions (downgraded for imprecision) and for multiple interventions (downgraded for risk of bias (ROB), imprecision and inconsistency) (summary of findings Table for the main comparison; summary of findings Table 3).
Contraceptive‐promoting intervention
The evidence for the following outcomes, condom use at last sex, use of hormonal contraceptives and reduction in sexually transmitted diseases was considered high quality (summary of findings Table for the main comparison).
Educational interventions
Evidence for the reduction in the initiation of intercourse was considered low quality (downgraded for ROB and imprecision); while evidence for use of condom at last sex was considered moderate quality (downgraded for ROB only). (summary of findings Table 2)
Multiple interventions
Evidence for studies that employed multiple interventions was grouped into individual and cluster randomised controlled trials (summary of findings Table 3; summary of findings Table 4). For Individual RCTs, evidence for reduction in initiation of intercourse and condom use at last sex was considered moderate quality (downgraded for ROB only); evidence for consistent use of condoms and reduction in sexually transmitted diseases was considered low quality (downgraded for ROB and inconsistency) and very low quality (downgraded for ROB, inconsistency and imprecision) respectively. Evidence from cluster RCTs was considered moderate quality (downgraded for ROB only) for condom use at last sex, low quality (downgraded for ROB and imprecision) for consistent condom use and reduction in sexually transmitted diseases; and very low quality (downgraded for ROB, imprecision and inconsistency) for reduction in initiation of intercourse and use of hormonal contraception.
Overall, the studies had several important strengths: most had large sample sizes, long‐term follow‐up, described the development of data collection instruments, used techniques to promote the validity of self‐reported data, controlled for baseline differences in statistical analyses, and reported the causes and possible impacts of attrition.
Methodological quality was sometimes difficult to judge due to incomplete reporting of key methodological features and it was often difficult to obtain additional information by contacting the trial authors due to data loss and non‐response. Weaknesses include the underreporting of key methodological features; few of the trials specified the procedures used for assigning participants, or concealed allocation, blinded outcome assessors or separated programme facilitators between the intervention and control groups.
Five studies reported adequate allocation concealment using sealed, opaque envelopes (Diclemente 2004; Jemmott 2010; Raine 2005; Raymond 2006; Philliber 2002 ). The remaining studies did not provide information on concealment of allocation.
Assessor blinding was reported in 11 studies (Black 2006; Bonell 2013; Diclemente 2004; Jemmott 1998; Jemmott 2010; Minnis 2014; Morrison‐Beedy 2013; Raine 2005; Shrier 2001; Wight 2002, ) and not in the remaining 42 studies.
Thirty‐four studies had insufficient or no information on randomisation generation method and used terms such as "assigned at random" or "randomly assigned".
Attrition at last follow‐up
Sixteen studies included more than 90% of randomised participants in the analysis (defined in the review methods as adequate), thirty‐seven had greater than 10% attrition and accounted for less than 90% of randomised participants in the data analysis (inadequate), and two studies did not mention number of participants lost to follow up. The percentage loss to follow up ranged from 0.5% to 48%.
Missing data
Commonly missing data across studies included the number of participants per trial arm at baseline and follow‐up, means and standard deviations for continuous outcomes, percentages for dichotomous outcomes, effect sizes, and attrition analyses.
Unit of analysis problems
Of the thirty‐four trials that used cluster randomisation, 26 controlled for clustering in analyses and eight did not (Aarons 2000; Allen 1997; Cabezon 2005; Fawole 1999; Ferguson 1998, Howard 1990; Kirby 1997a; Morberg 1998). While one study (Kirby 1997a) explained that using individuals as the unit of analysis gave no significant results thus no need for adjusting for clusters. These studies are potentially vulnerable to bias due to incorrect analysis and could result in one or more statistically significant effect occurring by chance.
Limitations of outcome measures:
All outcome data in this review are vulnerable to self‐report bias except for pregnancy and STDs in the following studies: Jemmott 1998; Raine 2005; Raymond 2006. These studies used biological outcomes which are better indicators for pregnancy and STDs. Self‐reported behavioural outcomes unavoidably introduce self‐report bias. Most behavioural outcomes were reported in subgroups and varied greatly such as initiation of intercourse ("last sex", "sex in the last three months", "sex among virgins"). Follow‐up periods also varied greatly. Likewise the use of contraceptives; while some studies used the term "contraceptive", others differentiated it into condom use, hormonal contraceptives, pills. The reporting of sub‐groups also varied. The results of this review highlight the need for a standardised set of outcome measures with explicit definitions, consistent follow‐up times and recall periods to enable comparisons across primary trials. Long‐term follow‐up data are also particularly relevant for studies of unintended pregnancy and sexual behaviour, although these studies tend to lose large numbers of study participants to follow up. One study (Guilamo‐Ramos 2011b), reported "had vaginal intercourse" as one of its outcomes but did not indicate if individuals analysed excluded those who reported any sexual intercourse.
Potential biases in the review process
There are several potential biases in the review process. Our search strategy, though exhaustive may have not been enough to identify all potentially important unpublished data, thus the review is not without publication bias. Several randomised controlled trials that we included did not measure unintended pregnancy which is the primary outcome in this review.
While assessing trials for inclusion, we might have omitted trials that aimed at preventing unintended pregnancy as they may not have included any of the search terms in their title or abstract. We hope to correct this in future updates.
Another source of bias is our inability to obtain relevant missing data, including methodological characteristics and outcome data leading to the exclusion of a number of trials from the meta‐analysis. Twenty studies were included in the meta‐analysis, of which the majority had various methodological limitations capable of increasing the risk of bias and definitely compromising the strength of evidence.
We encountered some difficulty finding a reliable intra‐class correlation coefficient (ICC) when computing the design effect for cluster randomised trials. Using the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011c), we were able to run a sensitivity analysis for some of the data that provided enough information to calculate average cluster size using a range of possible ICC values. This could have affected the significance of results for isolated pair‐wise comparisons in the direction of insignificance.
Agreements and disagreements with other studies or reviews
Evidence about the prevention of unintended pregnancy in adolescence differed from a previous systematic review carried out (DiCenso 2002) as this reported that the interventions had no effect on the incidence of unintended pregnancy. The review did not include the recent trials, which reported a reduction in the incidence of unintended pregnancy in the intervention group (Cabezon 2005; Philliber 2002). Outcomes such as the initiation of sexual intercourse and contraceptive use showed no significant difference between intervention and control irrespective of intervention, a finding consistent with the previous review.

Risk of bias summary: review authors' judgments about each risk of bias item for each included study.
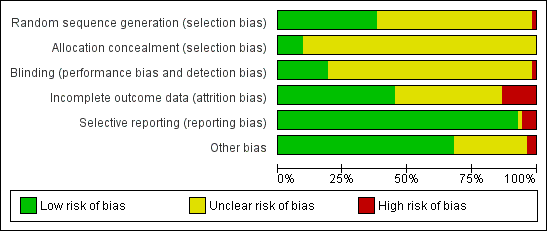
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
![Comparison 1 Multiple interventions, Outcome 1 Unintended pregnancy [individually randomised trials].](/es/cdsr/doi/10.1002/14651858.CD005215.pub3/media/CDSR/CD005215/image_n/nCD005215-CMP-001-01.png)
Comparison 1 Multiple interventions, Outcome 1 Unintended pregnancy [individually randomised trials].
![Comparison 1 Multiple interventions, Outcome 2 Unintended pregnancy [cluster‐randomised trials].](/es/cdsr/doi/10.1002/14651858.CD005215.pub3/media/CDSR/CD005215/image_n/nCD005215-CMP-001-02.png)
Comparison 1 Multiple interventions, Outcome 2 Unintended pregnancy [cluster‐randomised trials].
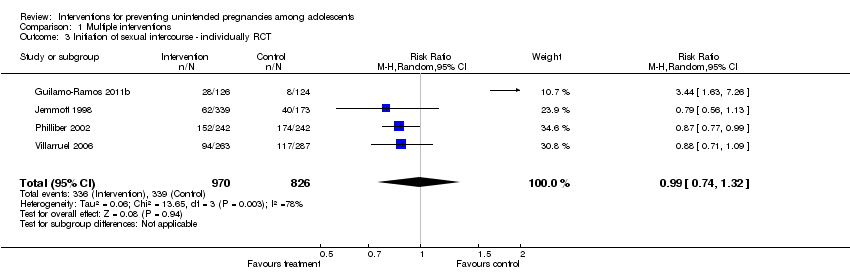
Comparison 1 Multiple interventions, Outcome 3 Initiation of sexual intercourse ‐ individually RCT.

Comparison 1 Multiple interventions, Outcome 4 Initiation of sexual intercourse ‐ cluster RCT.

Comparison 1 Multiple interventions, Outcome 5 Use of birth control methods ‐ individually RCT.

Comparison 1 Multiple interventions, Outcome 6 Use of birth control methods ‐ cluster RCT.

Comparison 1 Multiple interventions, Outcome 7 Sexually Transmitted Diseases ‐ individually RCT.
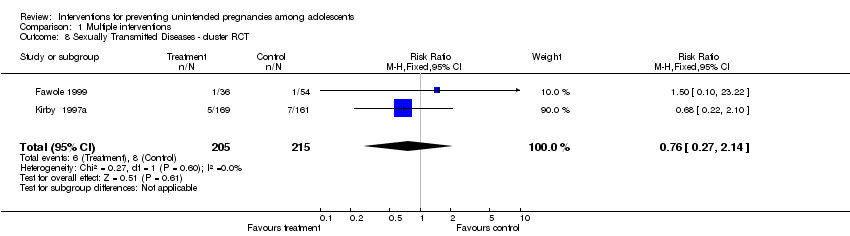
Comparison 1 Multiple interventions, Outcome 8 Sexually Transmitted Diseases ‐ cluster RCT.

Comparison 1 Multiple interventions, Outcome 9 Childbirth ‐ cluster RCT.

Comparison 1 Multiple interventions, Outcome 10 Childbirth ‐ individually RCT.

Comparison 1 Multiple interventions, Outcome 11 Second unintended pregnancy ‐ individually RCT.
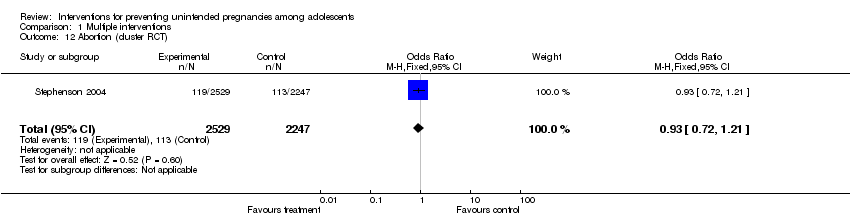
Comparison 1 Multiple interventions, Outcome 12 Abortion (cluster RCT).
![Comparison 2 Sensitivity analysis [Multiple interventions]: Unintended pregnancy, Outcome 1 Unintended pregnancy ‐ cluster‐randomi sed trials .](/es/cdsr/doi/10.1002/14651858.CD005215.pub3/media/CDSR/CD005215/image_n/nCD005215-CMP-002-01.png)
Comparison 2 Sensitivity analysis [Multiple interventions]: Unintended pregnancy, Outcome 1 Unintended pregnancy ‐ cluster‐randomi sed trials .
![Comparison 2 Sensitivity analysis [Multiple interventions]: Unintended pregnancy, Outcome 2 Unintended pregnancy ‐ individually‐randomi sed trials .](/es/cdsr/doi/10.1002/14651858.CD005215.pub3/media/CDSR/CD005215/image_n/nCD005215-CMP-002-02.png)
Comparison 2 Sensitivity analysis [Multiple interventions]: Unintended pregnancy, Outcome 2 Unintended pregnancy ‐ individually‐randomi sed trials .
![Comparison 2 Sensitivity analysis [Multiple interventions]: Unintended pregnancy, Outcome 3 Unintended pregnancy ‐ cluster‐adjusted + individual .](/es/cdsr/doi/10.1002/14651858.CD005215.pub3/media/CDSR/CD005215/image_n/nCD005215-CMP-002-03.png)
Comparison 2 Sensitivity analysis [Multiple interventions]: Unintended pregnancy, Outcome 3 Unintended pregnancy ‐ cluster‐adjusted + individual .
![Comparison 3 Sensitivity analysis [Multiple interventions]: Initiation of intercourse, Outcome 1 Initiation of sexual intercourse ‐ individually RCT.](/es/cdsr/doi/10.1002/14651858.CD005215.pub3/media/CDSR/CD005215/image_n/nCD005215-CMP-003-01.png)
Comparison 3 Sensitivity analysis [Multiple interventions]: Initiation of intercourse, Outcome 1 Initiation of sexual intercourse ‐ individually RCT.
![Comparison 3 Sensitivity analysis [Multiple interventions]: Initiation of intercourse, Outcome 2 Initiation of sexual intercourse ‐ cluster RCT.](/es/cdsr/doi/10.1002/14651858.CD005215.pub3/media/CDSR/CD005215/image_n/nCD005215-CMP-003-02.png)
Comparison 3 Sensitivity analysis [Multiple interventions]: Initiation of intercourse, Outcome 2 Initiation of sexual intercourse ‐ cluster RCT.
![Comparison 3 Sensitivity analysis [Multiple interventions]: Initiation of intercourse, Outcome 3 Initiation of sexual intercourse ‐ cluster‐adjusted + individual.](/es/cdsr/doi/10.1002/14651858.CD005215.pub3/media/CDSR/CD005215/image_n/nCD005215-CMP-003-03.png)
Comparison 3 Sensitivity analysis [Multiple interventions]: Initiation of intercourse, Outcome 3 Initiation of sexual intercourse ‐ cluster‐adjusted + individual.
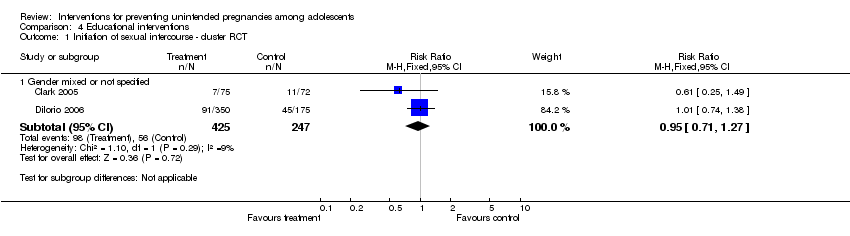
Comparison 4 Educational interventions , Outcome 1 Initiation of sexual intercourse ‐ cluster RCT.

Comparison 4 Educational interventions , Outcome 2 Use of birth control methods ‐ cluster RCT.

Comparison 4 Educational interventions , Outcome 3 Use of contraceptives ‐ individually RCT.

Comparison 5 Contraceptive‐promoting interventions, Outcome 1 Unintended pregnancy ‐ individually RCT.
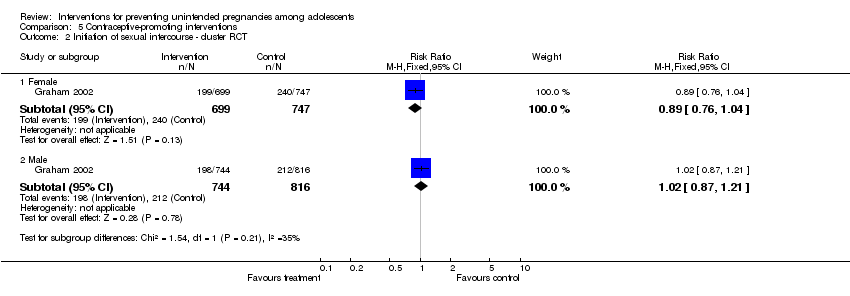
Comparison 5 Contraceptive‐promoting interventions, Outcome 2 Initiation of sexual intercourse ‐ cluster RCT.
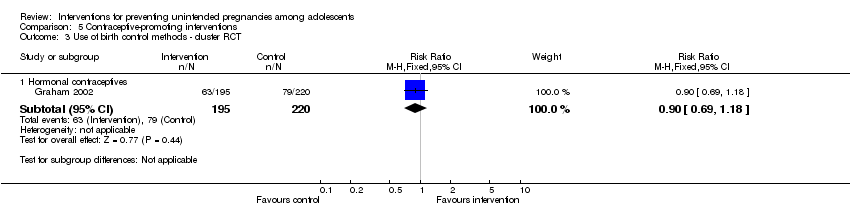
Comparison 5 Contraceptive‐promoting interventions, Outcome 3 Use of birth control methods ‐ cluster RCT.
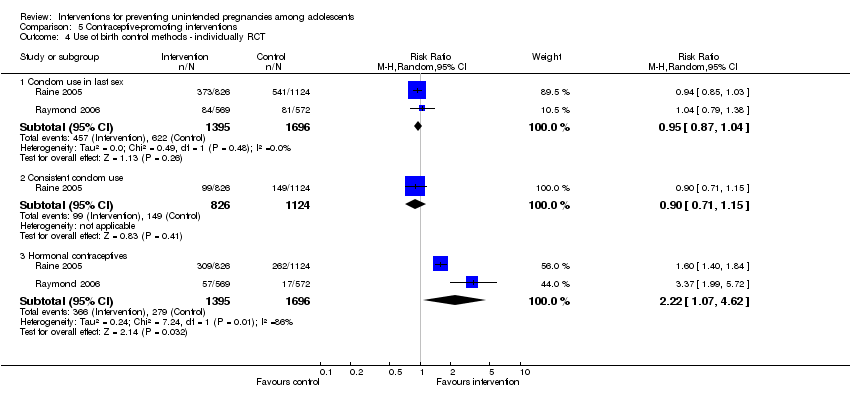
Comparison 5 Contraceptive‐promoting interventions, Outcome 4 Use of birth control methods ‐ individually RCT.
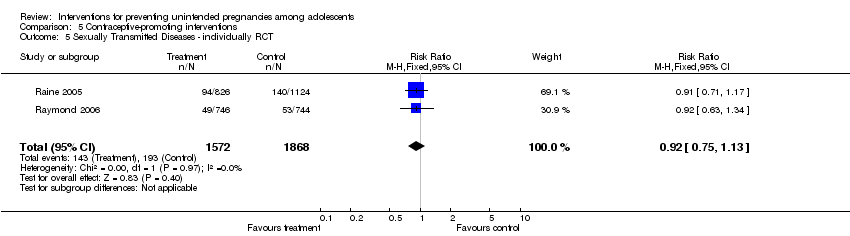
Comparison 5 Contraceptive‐promoting interventions, Outcome 5 Sexually Transmitted Diseases ‐ individually RCT.
| Contraceptive‐promoting interventions (individual RCTs) | |||||
| Patient or population: Male and female adolescents aged 10 years to 19 years | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | |
| Risk with No intervention/standard curriculum | Risk with Contraception Intervention | ||||
| Unintended pregnancy | Study population | RR 1.01 | 3440 | ⊕⊕⊕⊝ | |
| 83 per 1000 | 84 per 1000 | ||||
| Moderate | |||||
| 85 per 1000 | 86 per 1000 | ||||
| Use of birth control methods (condom use in last sex) | Study population | RR 0.95 | 3091 | ⊕⊕⊕⊕ | |
| 367 per 1000 | 348 per 1000 | ||||
| Moderate | |||||
| 312 per 1000 | 296 per 1000 | ||||
| Use of birth control methods (hormonal contraceptives) | Study population | RR 2.22 | 3091 | ⊕⊕⊕⊕ | |
| 165 per 1000 | 365 per 1000 | ||||
| Moderate | |||||
| 131 per 1000 | 292 per 1000 | ||||
| Sexually Transmitted Diseases | Study population | RR 0.92 | 3440 | ⊕⊕⊕⊕ | |
| 103 per 1000 | 95 per 1000 | ||||
| Moderate | |||||
| 98 per 1000 | 90 per 1000 | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| 1 Downgraded by 1 for imprecision: confidence interval fail to appreciable harm and included the null value | |||||
| Educational interventions (cluster RCTs) | |||||
| Patient or population: Male and female adolescents aged 10 years to 19 years | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | |
| Risk with No intervention/Standard curriculum | Risk with Educational intervention | ||||
| Use of birth control methods (condom use at last sex) | Study population | RR 1.18 | 1431 | ⊕⊕⊕⊝ | |
| 261 per 1000 | 308 per 1000 | ||||
| Moderate | |||||
| 534 per 1000 | 630 per 1000 | ||||
| Initiation of sexual intercourse (mixed gender) | Study population | RR 0.95 | 672 | ⊕⊕⊝⊝ | |
| 227 per 1000 | 215 per 1000 | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| 1 Several risk of bias assessment were unclear (not provided in the text) 2 Low number of events and confidence interval includes the null value | |||||
| Multiple interventions (cluster RCTs) | |||||
| Patient or population: Male and female adolescents aged 10 years to 19 years | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | |
| Risk with No Intervention/Standard curriculum | Risk with Multiple interventions | ||||
| Unintended pregnancy | Study population | RR 0.50 | 3149 | ⊕⊕⊝⊝ | |
| 67 per 1000 | 33 per 1000 | ||||
| Moderate | |||||
| 25 per 1000 | 13 per 1000 | ||||
| Initiation of sexual intercourse (mixed gender) | Study population | RR 0.84 | 8608 | ⊕⊝⊝⊝ | |
| 253 per 1000 | 212 per 1000 | ||||
| Moderate | |||||
| 212 per 1000 | 178 per 1000 | ||||
| Use of birth control methods (condom use at last sex) | Study population | RR 1.01 | 2620 | ⊕⊕⊕⊝ | |
| 585 per 1000 | 591 per 1000 | ||||
| Moderate | |||||
| 565 per 1000 | 570 per 1000 | ||||
| Use of birth control methods (consistent condom use) | Study population | RR 1.95 | 826 | ⊕⊕⊝⊝ | |
| 353 per 1000 | 689 per 1000 | ||||
| Moderate | |||||
| 133 per 1000 | 259 per 1000 | ||||
| Use of birth control methods (hormonal contraceptives) | Study population | RR 1.01 | 3987 | ⊕⊝⊝⊝ | |
| 244 per 1000 | 246 per 1000 | ||||
| Moderate | |||||
| 251 per 1000 | 254 per 1000 | ||||
| Sexually Transmitted Diseases | Study population | RR 0.76 | 420 | ⊕⊕⊝⊝ | |
| 37 per 1000 | 28 per 1000 | ||||
| Moderate | |||||
| 31 per 1000 | 24 per 1000 | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| 1 Downgraded by 1 for risk of bias; several assessments were unclear due to no information provided. Such potential limitations are likely to lower confidence in the estimate of effect 2 Downgraded by 1 for imprecision; low number of events, confidence interval includes appreciable benefit and null value 3 Heterogeneity could be explained (difference in comparison intervention and length of follow up) 4 Downgraded by 1 for imprecision: confidence interval includes appreciable benefit 5 Downgraded by 1 for inconsistency: unexplained large variations in effect 6 Confidence interval includes the null value, however, the sample size and number of events are fairly large and confidence interval is relatively narrow 7 Downgraded by 1 for imprecision: confidence interval includes appreciable benefit and harm 8 Downgraded by 1 for imprecision; low number of events, confidence interval includes appreciable benefit and harm | |||||
| Multiple interventions ( individual RCTs) | |||||
| Patient or population: Male and female adolescents aged 10 years to 9 years | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | |
| Risk with No Intervention/Standard curriculum | Risk with Multiple interventions | ||||
| Unintended pregnancy | Study population | RR 0.66 | 1905 | ⊕⊕⊕⊝ | |
| 116 per 1000 | 76 per 1000 | ||||
| Moderate | |||||
| 149 per 1000 | 98 per 1000 | ||||
| Initiation of sexual intercourse (mixed gender) | Study population | RR 0.99 | 1796 | ⊕⊕⊕⊝ | |
| 410 per 1000 | 406 per 1000 | ||||
| Moderate | |||||
| 236 per 1000 | 234 per 1000 | ||||
| Use of birth control methods (condom use in last sex) | Study population | RR 1.00 | 796 | ⊕⊕⊕⊝ | |
| 840 per 1000 | 840 per 1000 | ||||
| Moderate | |||||
| 837 per 1000 | 837 per 1000 | ||||
| Use of birth control methods (consistent condom use) | Study population | RR 1.21 | 1681 | ⊕⊕⊝⊝ | |
| 353 per 1000 | 427 per 1000 | ||||
| Moderate | |||||
| 476 per 1000 | 575 per 1000 | ||||
| Sexually Transmitted Diseases | Study population | RR 0.89 | 699 | ⊕⊝⊝⊝ | |
| 191 per 1000 | 170 per 1000 | ||||
| Moderate | |||||
| 270 per 1000 | 241 per 1000 | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| 1 Downgraded by 1 for risk of bias; several assessments were unclear due to no information provided. Such potential limitations are likely to lower confidence in the estimate of effect 2 Downgraded by 1 for imprecision; low number of events, confidence interval includes appreciable benefit and null value 3 Heterogeneity could be explained (difference in comparison intervention and length of follow up) 4 Downgraded by 1 for imprecision: confidence interval includes appreciable benefit 5 Downgraded by 1 for inconsistency: unexplained large variations in effect 6 Confidence interval includes the null value, however, the sample size and number of events are fairly large and confidence interval is relatively narrow 7 Downgraded by 1 for imprecision: confidence interval includes appreciable benefit and harm 8 Downgraded by 1 for imprecision; low number of events, confidence interval includes appreciable benefit and harm | |||||
| Intervention | Outcome | Study ID | Number Assessed | Case affected | Control affected | Test Statistics | 95% CI | p‐value |
| Educational intervention | Pregnancy | 1701 | ‐ | ‐ | OR: 0.97 | 0.93 to 1.0 | 0.04 | |
| Initiation of intercourse | 156 | ‐ | ‐ | Beta: 1.604 and SE: 1.00 | ‐ | < 0.11 | ||
| Aarons 2000 (females) | 139 | Adj. OR: 1.88 | 1.02 to 3.47 | 0.04 | ||||
| Aarons 2000 (males) | 123 | Adj. OR: 1.18 | 0.61 to 2.29 | 0.62 | ||||
| 1079 | ‐ | ‐ | OR: 1.00 | 0.70 to 1.41 | ||||
| Changes in knowledge and attitudes about the risk of unintended pregnancy | 351 | 92.9% | 91.8% | ns | ||||
| Use of birth control at last sex | Mitchell‐DiCenso 1997 (females) | 109 | 42.2% | 46.7% | OR: 1.03 | 1.00 to 1.07 | 0.03 | |
| Mitchell‐DiCenso 1997 (males) | 214 | 39.3% | 35.9% | OR: 1.06 | 1.02 to 1.77 | 0.005 | ||
| Aarons 2000 (females) | 135 | Adj. OR: 3.39 | 1.16 to 9.95 | 0.025 | ||||
| Aarons 2000 (males) | 125 | Adj. OR: 1.53 | 0.55 yo 4.26 | 0.42 | ||||
| Use of condom at last sex | 1896 | 39.1% | 31.9% | OR: 1.41 | 1.12 to 1.77 | ‐ | ||
| 221 | 77% | 73% | ||||||
| Unprotected intercourse in the past 3 monthsa | 502 | Beta: ‐0.375 and SE: 0.32 | >0.05 | |||||
| Ever had sex without condoms | Mean: 0.23 | Mean: 0.57 | ‐0.61 to ‐0.06 | 0.03 | ||||
| Multiple interventions | Pregnancy | 308 | ‐ | ‐ | OR; 0.84 | ‐ | 0.61 | |
| 460 | ‐ | ‐ | OR: 0.53 | 0.27 to 1.03 | 0.06 | |||
| 1172 | 2.3% | 3.3% | ‐ | ‐ | 0.07 | |||
| 2145 | ‐ | ‐ | OR: 1.34 | 0.98 to 1.84 | 0.07 | |||
| 417 | ‐ | ‐ | OR: 0.77 | 0.49 to 1.23 | 0.28 | |||
| 95 | ‐ | ‐ | ‐ | ‐ | < 0.05 | |||
| 195 | 6.8% | 18.5% | ||||||
| 323 | B=‐.823 OR: 0.44 | 0.009 | ||||||
| 560 | ‐ | ‐ | OR: 0.41 | ‐ | ‐ | |||
| Initiation of sexual intercourse (mixed gender) | 94 | ‐ | ‐ | OR: 1.23 | 0.51 to 2.97 | 0.65 | ||
| 95 | .Mean: 1.19 | .Mean: 2.74 | ||||||
| 8326 | ‐ | ‐ | OR: 1.03 | 0.88 to 1.21 | 0.69 | |||
| 627 | AOR:0.65 | 0.54,0.77 | <.01 | |||||
| 195 | 40.1% | 66.1% | OR: 0.39 | 0.20 to 0.76 | 0.005 | |||
| 735 | AOR:0.82 | 0.51,1.34 | >0.05 | |||||
| 2565 | OR:1.13 SE: 0.24 | 0.71 to 1.82 | 0.60 | |||||
| Initiation of sexual intercourse (male) | 1412 | 19.3% | 27.7% | model R2: 0.118 | ‐ | 0.02 | ||
| 809 | ‐ | ‐ | OR: 1.08 | 0.80 to 1.46 | 0.63 | |||
| 8156 | 32.7% | 31.1% | OR: 0.90 | 0.65 to 1.23 | 0.35 | |||
| 408 | 36% | 44% | ‐ | ‐ | ‐ | |||
| Initiation of sexual intercourse (female) | 1417 | 20.3% | 22.1% | model R2: 0.145 | ‐ | 0.53 | ||
| 1220 | ‐ | ‐ | OR: 0.88 | 0.59 to 1.31 | 0.54 | |||
| 8156 | 34.7% | 40.8% | OR: 0.80 | 0.66 to 0.97 | 0.008 | |||
| 480 | 27% | 22% | ‐ | ‐ | ‐ | |||
| Use of condoms at last sex | 2145 | ‐ | ‐ | OR: 1.38 | 1.06 to 1.79 | 0.02 | ||
| 359 | ‐ | ‐ | OR: 1.00 | 0.49 to 1.23 | 0.99 | |||
| 460 | ‐ | ‐ | OR: 3.94 | 2.58 to 6.03 | < .001 | |||
| 258 | ‐ | ‐ | OR: 2.13 | ‐ | 0.15 | |||
| 198 | OR: 0.93 | ‐0.75,0.62 | 0.85 | |||||
| 1018 | OR:191 SE:0.27 | 1.13 to 3.21 | 0.02 | |||||
| Childbirth | 4196 | 300/1000 | 274/1000 | OR: 14.6 | 0.32 | |||
| Abortion | 4196 | 127/1000 | 112/1000 | OR: 26.4 | 0.40 | |||
| Consistent condom use at 12 months | 253 | Mean: 0.96 (116/126) | Mean: 0.66 (81/127) | ARR:145 | 1.26 to 1.67 | 0.00 | ||
| Consistent condom use at 24 months | 204 | Mean:1.53 | Mean: 0.93 | ARR: 1.57 | 1.28,1.94 | |||
| Consistent hormonal contraceptive use at 12 months | 253 | Mean: 4.27 (74/126) | Mean: 2.91 (51/127) | ARR:1.46 | 1.13 to 1.89 | 0.00 | ||
| Consistent hormonal contraceptive use at 24 months | 203 | Mean: 3.29 | Mean: 2.34 | ARR: 1.30 | 1.06,1.58 | |||
| 162 | OR:0.42 | 0.12 | ||||||
| Use of condoms at first sex | 285 | OR:0.68 SE:0.48 | 0.26 to 1.75 | 0.42 | ||||
| Protected against pregnancy at last sex | 998 | OR:1.62 SE:0.22 | 1.05 to 2.50 | 0.03 | ||||
| Sexually Transmitted Infections | 323 | B=‐0.067 OR: ‐0.94 | 0.77 | |||||
| Mean:10.5 SE: 2.9 | Mean:18.2 SE:2.8 | 0.05 | ||||||
| Baird 2010: The following listed outcomes were reported. However, the method of reporting made difficult to extract correct estimates. 1. Pregnancy School girls and dropouts among the treatment group are 1.1 percentage points less likely to have become pregnant over the past year. Not statistically significant. | ||||||||
| a ‐ Binary outcome (did unprotected intercourse occur or not?) b ‐ Study (Stephenson 2008) same as Stephenson 2004, but with an extended follow up (7yrs) c ‐ Data comparing skills‐based intervention versus health‐promotion intervention Analyses assessing impact on delay of sexual initiation excluded individuals who reported any type of sexual intercourse at baseline Analyses assessing impact on other on sexual behaviours are limited to individuals that are sexually active ns ‐ non‐significant | ||||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Unintended pregnancy [individually randomised trials] Show forest plot | 4 | 1905 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.66 [0.50, 0.87] |
| 2 Unintended pregnancy [cluster‐randomised trials] Show forest plot | 5 | 3149 | Risk Ratio (M‐H, Random, 95% CI) | 0.50 [0.23, 1.09] |
| 3 Initiation of sexual intercourse ‐ individually RCT Show forest plot | 4 | 1796 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.74, 1.32] |
| 4 Initiation of sexual intercourse ‐ cluster RCT Show forest plot | 7 | 8608 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.68, 1.04] |
| 5 Use of birth control methods ‐ individually RCT Show forest plot | 8 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 5.1 Condom use in last sex | 3 | 796 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.95, 1.06] |
| 5.2 Consistent condom use | 5 | 1681 | Risk Ratio (M‐H, Random, 95% CI) | 1.21 [0.95, 1.54] |
| 5.3 Contraceptive use at last sex | 1 | 408 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.95, 1.03] |
| 5.4 Consistent contraceptive use | 1 | 253 | Risk Ratio (M‐H, Random, 95% CI) | 1.29 [1.06, 1.59] |
| 6 Use of birth control methods ‐ cluster RCT Show forest plot | 6 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 6.1 Condom use at last sex | 4 | 2620 | Risk Ratio (M‐H, Random, 95% CI) | 1.01 [0.93, 1.09] |
| 6.2 Consistent condom use | 3 | 826 | Risk Ratio (M‐H, Random, 95% CI) | 1.95 [0.70, 5.44] |
| 6.3 Hormonal contraceptives | 3 | 3987 | Risk Ratio (M‐H, Random, 95% CI) | 1.01 [0.72, 1.43] |
| 7 Sexually Transmitted Diseases ‐ individually RCT Show forest plot | 2 | 699 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.89 [0.65, 1.22] |
| 8 Sexually Transmitted Diseases ‐ cluster RCT Show forest plot | 2 | 420 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.27, 2.14] |
| 9 Childbirth ‐ cluster RCT Show forest plot | 1 | 4776 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.64 [0.52, 0.79] |
| 10 Childbirth ‐ individually RCT Show forest plot | 1 | 484 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.31, 1.45] |
| 11 Second unintended pregnancy ‐ individually RCT Show forest plot | 1 | 149 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.48 [0.22, 1.02] |
| 12 Abortion (cluster RCT) Show forest plot | 1 | 4776 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.72, 1.21] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Unintended pregnancy ‐ cluster‐randomi sed trials Show forest plot | 2 | 497 | Risk Ratio (M‐H, Random, 95% CI) | 0.20 [0.10, 0.39] |
| 2 Unintended pregnancy ‐ individually‐randomi sed trials Show forest plot | 3 | 1421 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.68 [0.46, 1.00] |
| 3 Unintended pregnancy ‐ cluster‐adjusted + individual Show forest plot | 5 | 1918 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.53 [0.39, 0.72] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Initiation of sexual intercourse ‐ individually RCT Show forest plot | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.1 Gender mixed or not specified | 3 | 1312 | Risk Ratio (M‐H, Random, 95% CI) | 1.18 [0.67, 2.09] |
| 2 Initiation of sexual intercourse ‐ cluster RCT Show forest plot | 4 | 1687 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.57, 1.25] |
| 2.1 Gender mixed or not specified | 4 | 1687 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.57, 1.25] |
| 3 Initiation of sexual intercourse ‐ cluster‐adjusted + individual Show forest plot | 7 | 2999 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.74, 1.05] |
| 3.1 Gender mixed or not specified | 7 | 2999 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.74, 1.05] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Initiation of sexual intercourse ‐ cluster RCT Show forest plot | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 Gender mixed or not specified | 2 | 672 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.71, 1.27] |
| 2 Use of birth control methods ‐ cluster RCT Show forest plot | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 2.1 condom use at last sex | 2 | 1431 | Risk Ratio (M‐H, Random, 95% CI) | 1.18 [1.06, 1.32] |
| 3 Use of contraceptives ‐ individually RCT Show forest plot | 1 | 360 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.5 [1.39, 4.48] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Unintended pregnancy ‐ individually RCT Show forest plot | 2 | 3440 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.81, 1.26] |
| 2 Initiation of sexual intercourse ‐ cluster RCT Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 Female | 1 | 1446 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.89 [0.76, 1.04] |
| 2.2 Male | 1 | 1560 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.87, 1.21] |
| 3 Use of birth control methods ‐ cluster RCT Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.1 Hormonal contraceptives | 1 | 415 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.69, 1.18] |
| 4 Use of birth control methods ‐ individually RCT Show forest plot | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 4.1 Condom use in last sex | 2 | 3091 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.87, 1.04] |
| 4.2 Consistent condom use | 1 | 1950 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.71, 1.15] |
| 4.3 Hormonal contraceptives | 2 | 3091 | Risk Ratio (M‐H, Random, 95% CI) | 2.22 [1.07, 4.62] |
| 5 Sexually Transmitted Diseases ‐ individually RCT Show forest plot | 2 | 3440 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.75, 1.13] |