مقایسه اکسیزیون کامل مزورکتال از طریق لاپاروسکوپی در برابر جراحی باز در مدیریت بالینی سرطان رکتوم
چکیده
پیشینه
سرطان کولورکتال از جمله سرطان رکتوم سومین علت شایع مرگومیرهای ناشی از سرطان در جهان غرب به شمار میآید. برای کارسینوم کولون، جراحی لاپاروسکوپی ثابت شده که منجر به بهبودی سریعتر پس از جراحی، عوارض کمتر و نتایج زیبایی بهتر، با نتایج اونکولوژیکی برابر، میشود. انتظار میرود که این مزایای کوتاهمدت برای جراحی لاپاروسکوپی سرطان رکتوم مشابه باشند. با این حال، بیخطری (safety) اونکولوژیکی جراحی لاپاروسکوپی برای سرطان رکتوم به دلیل عدم نتایج قطعی طولانیمدت مورد بحث باقی مانده است. بنابراین، مزایای کوتاهمدت مورد انتظار فقط زمانی میتوانند مورد توجه قرار گیرند که نتایج اونکولوژیکی حداقل برابر باشند.
اهداف
ارزیابی تفاوت در نتایج کوتاهمدت و طولانیمدت پس از اکسیزیون کامل مزورکتال از طریق لاپاروسکوپی (laparoscopic total mesorectal excision; LTME) الکتیو برای رزکسیون سرطان رکتوم در مقایسه با اکسیزیون کامل مزورکتال از طریق جراحی باز (open total mesorectal excision; OTME).
روشهای جستوجو
پایگاه مرکزی ثبت کارآزماییهای کنترلشده کاکرین (CENTRAL، کتابخانه کاکرین، 2013، شماره 2)؛ MEDLINE (ژانویه 1990 تا فوریه 2013)؛ EMBASE (ژانویه 1990 تا فوریه 2013)؛ ClinicalTrials.gov (فوریه 2013) و Current Controlled Trials (فوریه 2013) را جستوجو کردیم. فهرست منابع مقالات واردشده را برای یافتن مطالعات از دست رفته به صورت دستی جستوجو کردیم.
معیارهای انتخاب
فقط کارآزماییهای تصادفیسازی و کنترلشدهای (randomised controlled trials; RCTs) برای گنجاندن در نظر گرفته شدند که LTME و OTME را با هم مقایسه کرده و حداقل یکی از معیارهای پیامد ما را گزارش دادند.
گردآوری و تجزیهوتحلیل دادهها
دو نویسنده بهطور مستقل از هم کیفیت مطالعه را بر اساس بیانیه CONSORT ارزیابی کرده و اختلاف نظرها را با بحث حلوفصل کردند. کیفیت شواهد را با استفاده از روشهای درجهبندی توصیه، ارزیابی، توسعه و ارزشیابی (Grading of Recommendations Assessment, Development and Evaluation; GRADE) ارزیابی کردیم.
نتایج اصلی
تعداد 45 منبع را از 953 نتیجه جستوجو شناسایی کردیم، 14 مطالعه شامل 3528 بیمار مبتلا به سرطان رکتوم، معیارهای ورود را داشتند. تاثیر خطر سوگیری (bias) مطالعات واردشده را بر کیفیت شواهد در نظر نگرفتیم. دادهها بر اساس اصل قصد درمان (intention‐to‐treat; ITT) با میانگین نرخ تبدیل 14.5% (محدوده 0% تا 35%) در گروه لاپاروسکوپی آنالیز شدند.
شواهدی با کیفیت متوسط نشان داد که TME به روش لاپاروسکوپی و جراحی باز تاثیرات مشابهی بر بقای (survival) بدون بیماری در پنج سال داشتند (OR: 1.02؛ 95% CI؛ 0.76 تا 1.38؛ 4 مطالعه، N = 943). تاثیرات تخمینی TME از طریق لاپاروسکوپی و جراحی باز روی عود موضعی و بقای کلی مشابه بودند، اگرچه فواصل اطمینان گسترده بوده، و هر دو دارای شواهدی با کیفیت متوسط بودند (عود موضعی: OR: 0.89؛ 95% CI؛ 0.57 تا 1.39 و نرخ بقای کلی: OR: 1.15؛ 95% CI؛ 0.87 تا 1.52). شواهدی با کیفیت متوسط تا بالا وجود داشت مبنی بر اینکه تعداد غدد لنفاوی برداشتهشده و حاشیههای جراحی میان دو گروه مشابه بودند.
برای نتایج کوتاهمدت، طول مدت بستری در بیمارستان تا دو روز کاهش یافت (95% CI؛ 3.22‐ تا 1.10‐) (شواهد با کیفیت متوسط)، و زمان سپریشده تا اولین اجابت مزاج (defecation) در گروه LTME کوتاهتر بود (0.86‐ روز؛ 95% CI؛ 1.17‐ تا 0.54‐). شواهدی با کیفیت متوسط وجود داشت مبنی بر اینکه میزان موربیدیتی 30 روزه در هر دو گروه مشابه بود (OR: 0.94؛ 95% CI؛ 0.8 تا 1.1). موارد کمتری از عفونت زخم (OR: 0.68؛ 95% CI؛ 0.50 تا 0.93) و عوارض خونریزیدهنده (OR: 0.30؛ 95% CI؛ 0.10 تا 0.93) در گروه LTME رخ داد.
شواهد بارزی مبنی بر وجود تفاوت در کیفیت زندگی پس از LTME یا OTME در رابطه با بهبود عملکرد، مثانه و عملکرد جنسی وجود نداشت. هزینههای LTME بهطور قابل ملاحظهای بالاتر بود، به طوری که تفاوت در هزینههای مستقیم تا 2000 پوند انگلیس (GBP) گزارش شد.
نتیجهگیریهای نویسندگان
شواهدی را با کیفیت متوسط پیدا کردیم که نشان میدهند اکسیزیون کامل مزورکتال (TME) از طریق لاپاروسکوپی تاثیرات مشابهی با TME به روش جراحی باز بر پیامدهای بقای طولانیمدت در درمان سرطان رکتوم دارد. سطح کیفیت شواهد به دلیل عدم دقت (imprecision) کاهش یافت و انجام پژوهشهای بیشتر میتواند بر اعتماد ما به این نتیجه تاثیر بگذارد. شواهدی با کیفیت متوسط نشان میدهد که این روش منجر به پیامدهای کوتاهمدت پس از جراحی بهتری از نظر بهبود سرطان رکتوم غیرموضعی پیشرفته میشود. نتایج در حال حاضر در نشان دادن بقای بدون بیماری و بقای کلی مشابه بوده، و برای عود پس از حداقل سه سال و تا 10 سال همسو و سازگار است، اگرچه به دلیل عدم دقت نمیتوانیم برتری هر دو روش را منتفی بدانیم. برای انجام یک آنالیز عمیقتر از بقای بدون بیماری در طولانیمدت، بقای کلی و عود موضعی، در انتظار جمعآوری دادههای طولانیمدت از تعدادی از مطالعات در حال انجام و به تازگی تکمیل شده هستیم.
PICO
خلاصه به زبان ساده
جراحی لاپاروسکوپی سوراخ کلید یا جراحی باز در درمان سرطان رکتوم
سرطان کولورکتال (روده بزرگ) از جمله سرطان رکتوم سومین علت شایع مرگومیرهای ناشی از سرطان در جهان غرب است. خطر ابتلا به سرطان رکتوم با افزایش سن افزایش مییابد و در افراد در سنین 70 سال شایعتر است. درمان آن شامل رزکسیون کامل جراحی تومور و بافت اطراف آن با تکنیکی به نام اکسیزیون کامل مزورکتال (total mesorectal excision; TME) است که گاهی با شیمیدرمانی و رادیوتراپی همراه میشود. این جراحی را میتوان با جراحی شکمی باز معمولی از طریق ایجاد یک برش بزرگ یا با جراحی لاپاروسکوپی سوراخ کلید با چندین برش کوچک برای ورود ابزارها و دوربین انجام داد. برای سرطان کولون ثابت شده که جراحی لاپاروسکوپی باعث بهبودی سریعتر پس از جراحی، عوارض کمتر و نتایج زیبایی بهتری میشود. انتظار میرود که این نتایج برای جراحی رکتوم نیز یکسان باشد. با این حال، به دلیل قرارگیری عمیقتر رکتوم در لگن و مجاورت آن با اعصاب مهم، انجام جراحی برای سرطان رکتوم از نظر فنی دشوارتر از سرطان کولون است. بنابراین تضمین رزکسیون کامل و بیخطر تومور حائز اهمیت است، این کار به دلیل کاهش خطر عود تومور مهم است و میتواند با ارزیابی نرخ عود و بقای بیمار در طولانیمدت تست شود.
در این مرور بهروز شده، تمام مطالعات تصادفیسازی شده را درباره TME از طریق لاپاروسکوپی و جراحی باز برای درمان سرطان رکتوم ارزیابی کردهایم تا نتایج آنها را مقایسه و ترکیب کنیم. تعداد 14 کارآزمایی را وارد کردیم که در مجموع نتایج 3528 بیمار تحت جراحی سرطان رکتوم را گزارش کردند. در 14.5% از افرادی که تحت جراحی لاپاروسکوپی قرار گرفتند، به دلیل مشکلات یا مسائل پیش آمده حین پروسیجر، تبدیل روش درمان به جراحی باز با ایجاد یک برش بزرگ در شکم ضرورت داشت.
در حال حاضر، شواهدی با کیفیت متوسط نشان میدهند که اکسیزیون کامل مزورکتال از طریق لاپاروسکوپی (laparoscopic total mesorectal excision; LTME) تاثیرات مشابهی با TME به روش جراحی باز (OTME) بر پیامدهای بقای طولانیمدت در درمان سرطان رکتوم دارد. تاثیر تخمین زده شده غیردقیق بود و انجام پژوهشهای بیشتر میتواند بر اعتماد ما به این نتیجه تاثیر بگذارد. شواهدی با کیفیت متوسط نشان میدهد که از نظر طول مدت بستری در بیمارستان، این روش منجر به پیامدهای کوتاهمدت پس از جراحی بهتری میشود. به این نتیجه رسیدیم که درد در گروه LTME کمتر بود و از سرگیری رژیم غذایی بهتر. شواهد بارزی را مبنی بر تفاوت در کیفیت زندگی میان دو گروه پیدا نکردیم، اما هزینههای انجام LTME بالاتر بود. در انتظار انتشار دادههای طولانیمدت تعدادی از مطالعات در حال انجام و اخیرا تکمیلشده هستیم تا به درک ما از تاثیرات این رویکردهای جراحی بر بقای طولانیمدت بدون بیماری، بقای کلی و عود موضعی بیماری کمک کنند.
Authors' conclusions
Summary of findings
| Laparoscopic versus open total mesorectal excision (TME) for rectal cancer | |||||
| Patient or population: people with Rectal Cancer | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Open TME | Laparoscopic TME | ||||
| Disease‐free survival at 5 years | 718 per 1000 | 722 per 1000 | OR 1.02 | 943 | ⊕⊕⊕⊝ |
| Overall survival at 5 years | 679 per 1000 | 709 per 1000 | OR 1.15 | 987 | ⊕⊕⊕⊝ |
| Local recurrences | 54 per 1000 | 48 per 1000 | OR 0.89 | 1538 | ⊕⊕⊕⊝ |
| Lymph nodes retrieved | The mean number of lymph nodes retrieved in the intervention groups was | 3682 | ⊕⊕⊕⊕ | ||
| CRM positivity | 61 per 1000 | 60 per 1000 | OR 0.99 | 2313 | ⊕⊕⊕⊝ |
| 30‐day morbidity (total) | 275 per 1000 | 263 per 1000 | OR 0.94 | 3397 | ⊕⊕⊕⊝ |
| Hospital stay (days) | The mean length of hospital stay in the intervention groups was | 3084 | ⊕⊕⊕⊝ | ||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| 1Statistical inaccuracy with wide confidence interval at both sides 2Statistical inaccuracy with wide confidence interval at both sides, but a tendency for a higher overall survival for LTME 3Statistical inaccuracy with wide confidence interval at both sides, but a tendency for a lower recurrence rate for LTME 4Only 8 studies provided data on CRM positivity | |||||
Background
Description of the condition
The incidence of rectal cancer in the western world is 28% to 35% of the total colorectal cancer incidence, with 15 to 25/100,000 new patients per year for both men and women. The risk increases with age, with a median age of 70 years at the time of diagnosis; the associated mortality is between 4 and 10 per 100,000 per year (Glimelius 2013). Symptoms suggesting rectal cancer typically include changes in bowel habits, the feeling of incomplete emptying, rectal bleeding, anaemia or weight loss. The diagnosis can be made by tumour biopsy during colonoscopy or sigmoidoscopy. If rectal cancer is confirmed, the extent of the disease is examined by imaging of the chest and liver for signs of metastases, and magnetic resonance imaging (MRI) of the pelvis and/or endorectal ultrasound (ERUS) are done to determine the degree of rectal wall and mesorectal fascia invasion. The majority of rectal carcinomas are adenocarcinoma (95% to 98%), usually arising from an adenoma (Glimelius 2013; Monson 2013).
Description of the intervention
Complete resection of rectal cancer can be achieved by a sphincter‐preserving anterior resection (AR, rectosigmoid resection) or an abdominoperineal resection (APR). Both had high local recurrence rates until the introduction of the total mesorectal excision (TME) (Heald 1986). Total mesorectal excision achieves a complete removal of the rectum together with its draining lymphatics, and results in low rates of recurrence. Despite the successful introduction of laparoscopic and laparoscopic‐assisted procedures for the resection of colonic cancer, surgeons have been more reluctant to introduce laparoscopic TME due to the technically demanding resection plane.
How the intervention might work
Laparoscopic and laparoscopic‐assisted TME offers several theoretical advantages compared to open resection. It may be associated with less blood loss, faster recovery, early feeding and a lower morbidity rate, as shown in laparoscopic colonic surgery (Braga 2002; Pikarsky 2002). The magnified view of the pelvis afforded by the laparoscope may facilitate identification of the autonomic nerves and thus prevent unintentional injury of these nerves. However, these advantages of LTME are only beneficial to people with rectal cancer when local recurrence and disease‐free survival rates are at least similar to those achieved with OTME.
Why it is important to do this review
The introduction of laparoscopy 20 years ago has caused major changes in colorectal surgery. For benign disease, such as diverticulitis and inflammatory bowel disease, laparoscopy has become the surgical technique of choice for its benefits in recovery, complication rate and cosmetic results. Only recently, sufficient evidence has become available showing laparoscopic surgery is safe for the treatment of colonic cancer. Four large randomised trials (472 to 1076 participants) could not show any differences in quality of resection and long‐term recurrence and survival rates between laparoscopic and open surgery for colon cancer (MRC CLASICC a 2005; COST 2007; COLOR 2009; LAPKON II 2009). Although COLOR 2009 was not able to rule out any difference with their non‐inferiority design, the meta‐analysis by Kuhry 2008 did not show any differences.
Despite the larger number of randomised trials on laparoscopic surgery for colon cancer, there is still limited evidence for long‐ and short‐term outcomes after LTME due to the lack of high quality randomised controlled trials with sufficient follow up. Now the results of more well designed large randomised controlled trials (RCTs) become available, there is a need for a updated systematic review of these results.
Objectives
To evaluate the differences in short‐ and long‐term results after elective laparoscopic total mesorectal excision (LTME) for the resection of rectal cancer compared with open total mesorectal excision (OTME).
Methods
Criteria for considering studies for this review
Types of studies
In contrast to the published protocol and previous version of this review, for this update we have only considered RCTs comparing LTME to OTME, since sufficient RCTs have become available since the publication of the original review. We did not apply any language restrictions.
Types of participants
People with rectal cancer undergoing total mesorectal excision were considered for inclusion. Studies including participants with colorectal cancer are only eligible if the results for those with rectal carcinoma were presented separately.
Types of interventions
These include laparoscopic, laparoscopic‐assisted or open total mesorectal excision as (low) anterior resection or abdominoperineal resection. When a primary anastomosis was constructed, it could either be performed intraperitoneally ('double‐stapled' colorectal anastomosis) or extraperitoneally (hand‐sewn or stapled colorectal anastomosis).
Types of outcome measures
We sought the following outcomes in all included studies:
Primary outcomes
‐ Disease‐free and overall survival
Secondary outcomes
‐ Recurrences (local, wound/port site and distant)
‐ Quality of resection (circumferential margin (CRM) positivity and number of lymph nodes)
‐ Surgical data (surgical time, incision length, conversion rate)
‐ Intraoperative complications, blood loss and transfusion requirement
‐ Postoperative morbidity and mortality (overall morbidity, need for reoperation, anastomotic leakage, wound infection, urinary complications, bleeding, chest infection)
‐ Postoperative pain (use of medication and visual analogue scale (VAS) score)
‐ Gastrointestinal recovery and hospital stay (time to first bowel movement, time to normal diet, length of hospital stay)
‐ Long‐term morbidity (incisional herniae and bowel obstruction)
‐ Quality of life (functional recovery, bladder and sexual function)
‐ Immunologic response
‐ Costs
Search methods for identification of studies
Electronic searches
We followed the recommendations of the Cochrane Colorectal Cancer Group and searched the following bibliographic databases with no language restrictions in order to identify relevant primary studies:
Cochrane Central Register of Controlled Trials (CENTRAL) (January 1990 to February 2013);
MEDLINE (January 1990 to February 2013);
EMBASE (January 1990 to February 2013).
We conducted searches using medical subject headings (MeSH) and free‐text words. The search has been adapted for each database search and is shown in Appendix 1 (CENTRAL), Appendix 2 (MEDLINE) and Appendix 3 (EMBASE).
Searching other resources
We handsearched the reference lists of all selected articles for further relevant studies. There was no language restriction. In addition, we searched for ongoing trials in the ClinicalTrials.gov and the Current Controlled Trials databases.
Data collection and analysis
Selection of studies
Two authors (SV and LP) independently reviewed all abstracts. We retrieved full‐text copies of all studies that potentially met the inclusion criteria based on abstract review. If both authors agreed that a study did not meet the eligibility criteria, we excluded it. If we disagreed, we resolved conflicts by discussion and consensus or by consulting a third member of the review team.
Data extraction and management
We collected data according to the outcomes mentioned above. Each author extracted the data independently from each study and compared them, resolving disagreement by discussion. We used Review Manager 5 (RevMan 5.2) software for statistical analysis, provided by the Cochrane Collaboration. Data not suitable for meta‐analysis is discussed in the results section.
Assessment of risk of bias in included studies
Two authors (SV and LP) have assessed all the selected studies for methodological quality according to the CONSORT Statement 2010, and have summarised the information in the 'Risk of bias' figure (Figure 2). In addition, we have used the Cochrane 'Risk of bias' tool as described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Measures of treatment effect
We measured the treatment effect using the mean difference (MD) or standardised mean difference (SMD) for continuous data and the odds ratio (OR) for dichotomous data. Standardised mean differences were only used when the reported units or drugs varied between the studies, for instance the number of doses of analgesia. All outcomes included 95% confidence intervals (CI).
Unit of analysis issues
For randomised controlled trials for this surgical intervention, we would expect only a simple parallel design. The only possible cross‐over would be the conversion of laparoscopy to open surgery. Because worse outcomes for this group can be expected and should be evaluated as a complication of laparoscopic‐intended surgery, all analyses should be performed on the intention‐to‐treat principle.
Dealing with missing data
To avoid missing unpublished studies, we searched clinical trial databases as stated above. We compared reported outcomes to published protocols or to the Methods section of each article. If we found inconsistencies, this is reported in the 'Selective reporting' section of the 'Risk of bias' table. As missing postoperative and follow‐up data are common in surgical studies, we assume a random pattern of missingness.
Assessment of heterogeneity
We used the Cochrane Chi² test (Q‐test) to assess heterogeneity and the I² statistic to estimate the degree of heterogeneity (Higgins 2003). We considered an I² of between 0% and 40% as probably not important, between 30% and 60% as representing moderate heterogeneity, between 50% and 90% as substantial heterogeneity, and between 75% and 100% as considerable heterogeneity (Higgins 2011). We used a fixed‐effect analysis for outcomes with low heterogeneity.
Assessment of reporting biases
We present an overview of all outcomes per study in the table Selective reporting (reporting bias).
Data synthesis
We analysed continuous variables using mean differences with 95% confidence intervals. For dichotomous variables we used odds ratios with 95% confidence intervals. We constructed forest plots, using the Mantel‐Haenszel method (fixed‐ or random‐effects) to combine the outcomes. In case of continuous data presented as median and range, we estimated the mean and standard deviation according to the methods described by Hozo 2005. We generated funnel plots to screen for publication bias. In case of inclusion of an original RCT and the additional publication of a subgroup of participants, we included only the most appropriate subgroup data in the meta‐analyses, to avoid duplication of data.
Subgroup analysis and investigation of heterogeneity
We had planned subgroup analyses for abdominoperineal resection (APR) and anterior resection (AR), and for studies allowing and excluding neoadjuvant therapy. These analyses were not performed because too few studies presented separate data for these groups. However, we plan to explore these subgroups if possible in future updates.
Summary of Findings table
We applied methods developed by the GRADE working group to rate the quality of evidence from RCTs, starting at high quality and downgrading for risk of bias, imprecision, inconsistency, indirectness and publication bias.
We rated the quality of the evidence for the following main outcomes:
-
Disease‐free survival at 5 years
-
Overall survival at 5 years
-
Local recurrences
-
Lymph nodes retrieved
-
CRM positivity
-
30‐day morbidity
-
Hospital stay (days)
Results
Description of studies
See: Characteristics of included studies, Characteristics of excluded studies and Characteristics of ongoing studies.
Results of the search
Our searches of the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE and EMBASE identified 90, 253 and 852 results respectively. In addition we handsearched MEDLINE for any missed publications for the included trials. After exclusion of duplicates, we screened 953 references and identified 45 eligible references, as shown in the flow chart (Figure 1).

Study selection flow diagram.
Included studies
From the 29 references, we identified two ongoing trials and 14 published clinical trials. Most larger trials have published their results at several stages in different papers. Both ongoing trials (ACTRN12609000663257 and NCT00726622) are still recruiting participants and no results have been published yet. Of the 14 published trials, two (Kang 2010; COLOR 2 a 2013) completed participant recruitment but have not yet published long‐term data on survival. The COLOR 2 trial has a second published paper on a local subgroup, referred to as COLOR 2 b 2011 in this review. The Hong Kong trials are divided into the low rectal cancer group in Ng 2008 and the rectosigmoid group in Hong Kong a 2004, with the last subdivided in four papers because results are published for different subgroups as shown in the Characteristics of included studies. Hong Kong a 2004 is the biggest group, presenting upper rectum and sigmoid data, Hong Kong b 2009 is the upper rectal subgroup and reports 10‐year follow‐up data. Hong Kong c 2000 and Hong Kong d 2003 are both small subgroups of Hong Kong a 2004 and present only short‐term data on immunological response.
The UK MRC CLASICC study is presented across nine papers, with six grouped as MRC CLASICC a 2005, giving respectively the short‐term, three‐year, five‐year and 10‐year results, the costs and an analysis of long term complications of the same participant group. MRC CLASICC c 2001 (one) and MRC CLASICC b 2005 (two) include papers for a selected or local participant subgroup and are therefore reported separately. King 2006 also consists of two papers, with the second paper focusing on functional recovery in the same participant group. The remaining eight clinical trials have one reference each, with the note that Zhou 2004 and Zhou 2007 are different trials and different authors despite the coincidence of names.
All 14 clinical trials were published as full papers and involved a total of 3528 rectal cancer patients (range 19 to 1044). The characteristics of these trials are described in 20 separate data sets and thus tables to allow for sufficient details on six additional subgroup papers.
All studies had quite similar exclusion criteria. The most common were: T4 rectal cancer, rectal cancer recurrence, people with synchronous or metachronous colorectal cancer, metastatic disease, emergency surgery, intestinal obstruction or perforation, contraindication for laparoscopy and no informed consent. The majority of the studies described the technique for laparoscopic total mesorectal excision (TME). Perioperative treatment of participants was not described in most of the trials. Six studies had a standardised protocol (Hong Kong a 2004; Braga 2007; Ng 2008; Kang 2010; COLOR 2 b 2011; Liang 2011) and only two had an enhanced recovery protocol (King 2006; Lujan 2009). Data on the type of anaesthesia and analgesia were not given in most studies.
Most studies reported on a range of different outcomes. The most commonly assessed were overall and disease‐free survival rates, local recurrence rates, adequacy of oncological resection (margins and number of lymph nodes removed), duration of surgery, conversion rate, mortality, morbidity, anastomotic leakage, postoperative pain, gastrointestinal recovery rate and hospital stay. Most studies lacked a definition of conversion. The most common causes for conversion to open surgery were tumour invasion of adjacent structures or bulky tumours, dense adhesions and technical failure. Few studies evaluated quality of life (MRC CLASICC a 2005; MRC CLASICC b 2005; King 2006; Braga 2007; Kang 2010), immune response (Hong Kong c 2000; MRC CLASICC c 2001; Hong Kong d 2003; Zhou 2007; COLOR 2 b 2011) or costs (Hong Kong a 2004; MRC CLASICC a 2005; King 2006; Braga 2007; Ng 2008).
Excluded studies
Sixteen papers were excluded for the following reasons: two studies were not completely randomised (Leung 1999; Mirza 2008) and two other studies presented the same data as another included study (Braga 2002; Braga 2005). Two studies included participants with benign disease (Milsom 1998; Polle 2007) and two other studies excluded people treated with TME for low rectal cancer (Schwenk 1998; Liu 2009). Four studies included colorectal cancer patients, but did not report the number of rectal cancer patients or any separate outcomes for rectal cancer (Kim 1998; JCOG 0404 2005; LAPKON II 2009; LaFa 2011). One study presented low‐quality data from a period with a steep learning curve (Pan 2007). Three more studies turned out not to be prospective RCTs, but were a comparison with the national registry (Morris 2011), an economic comparison between UK and USA trials (Stead 2000), and a single‐arm phase II trial (Yamamoto 2008).
Risk of bias in included studies
The risk of bias is described in the Characteristics of included studies section, and a summary is shown in Figure 2. Of the included trials, only one had a low risk of bias on all items and three scored low on six out of seven domains. Five were of unclear or low quality, with a high or unclear risk in at least five out of seven domains.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
The method of randomisation was unclear in four trials, and allocation concealment was not described in seven trials. Only seven trials presented an adequate inclusion and randomisation flow diagram, including a description of the loss to follow‐up.
Blinding
Because of the nature of the interventions, blinding is not an option in these trials. Instead of blinding, we assessed whether operative technique and postoperative care were standardised, and how outcome data and pathological data were registered. We assessed standardisation in three studies as inadequate. Outcome registration was adequate in eight studies and unknown in all other studies.
Incomplete outcome data
We did not detect any attrition bias. Not all studies reported on loss to follow‐up. Questionnaire response rates were reported for both groups when eligible.
Selective reporting
Comparing the described protocols and methods to the reported results of the different studies, we did not find evidence of any selective reporting, although some studies did not report exact data on non‐significant results mentioned in the text sections. An overview of studies and outcomes in Table 1 shows that most studies report on the same outcomes. Five papers reported only one outcome in a subgroup analysis of another trial and one study reported only one outcome for the included participant group.
| Study ID | n | Long‐term survival | 30‐day mortality | 30‐day morbidity | Long‐term morbidity | Lymphnodes | Gastrointestinal recovery | Pain | Bleeding | Length of hospital stay | Immune response | Quality of life | Cost |
| 28 | ‐ | ‐ | + | ‐ | + | ‐ | ‐ | + | + | ‐ | ‐ | ‐ | |
| 168 | 5y/3y | + | + | + | + | + | ‐ | + | + | ‐ | + | + | |
| 1044 | ‐ | + | + | ‐ | + | + | + | + | + | ‐ | ‐ | ‐ | |
| 40 | ‐ | + | + | ‐ | + | ‐ | ‐ | + | + | + | ‐ | ‐ | |
| 403 | 5y | + | + | ‐ | + | + | + | + | + | ‐ | ‐ | + | |
| 153 | 10y | ‐ | ‐ | + | ‐ | + | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | |
| 34 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | + | ‐ | ‐ | |
| 40 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | + | ‐ | ‐ | |
| 340 | ‐ | + | + | ‐ | + | + | + | + | + | ‐ | + | ‐ | |
| 19 | ‐ | + | + | ‐ | ‐ | ‐ | ‐ | + | + | ‐ | + | + | |
| 343 | 3y | + | + | ‐ | + | + | ‐ | + | ‐ | ‐ | ‐ | ‐ | |
| 186 | ‐ | + | + | ‐ | + | ‐ | ‐ | + | + | ‐ | ‐ | ‐ | |
| 204 | 5y | + | + | ‐ | + | + | ‐ | + | + | ‐ | ‐ | ‐ | |
| 381 | 10y/5y/3y | + | + | ‐ | + | + | ‐ | ‐ | + | ‐ | + | ‐ | |
| 148 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | + | ‐ | |
| 236 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | + | ‐ | ‐ | |
| 99 | 5y | + | + | ‐ | + | + | + | + | + | ‐ | ‐ | + | |
| 73 | ‐ | ‐ | ‐ | ‐ | + | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | |
| 171 | ‐ | + | + | ‐ | ‐ | + | ‐ | + | + | ‐ | ‐ | ‐ | |
| 71 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | + | ‐ | ‐ |
Other potential sources of bias
An important source of bias is the experience of the surgeons conducting LTME, because of the known steep learning curve. (Schlachta 2001; Tekkis 2005) When only one experienced surgical team is involved, this bias can be limited, but it can be extensive in large multi centre trials or less experienced teams. Only the MRC CLASICC a 2005 and Kang 2010 defined the experience of their surgeons as based on at least 20 procedures. Four other studies only stated that their surgeons were "well experienced" or "the most experienced" (Hong Kong a 2004; Braga 2007; Pechlivanides 2007; Ng 2008;). The remaining eight did not describe surgeons' experience at all or stated only a single surgeon or team performed the procedures.
Effects of interventions
Disease‐free and overall survival
The disease‐free and overall survival rates have been reported in only six studies including 1494 participants, because of lack of follow‐up in the other eight studies. Two of these are trials that will report on these results in the near future (Kang 2010; COLOR 2 b 2011), while the other six did not mention any long‐term outcomes in their Methods or protocol.
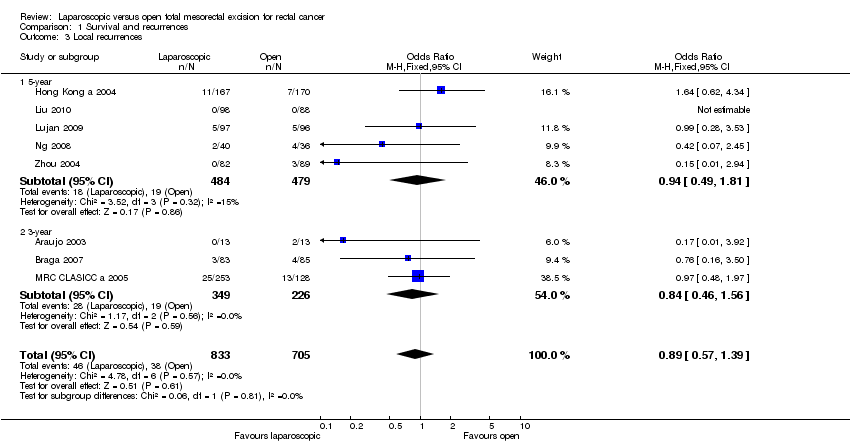
The combined data for these studies do not show statistical significant differences in disease‐free survival at three ((OR 1.08; 95% CI 0.67 to 1.74), five (OR 1.02; 95% CI 0.76 to 1.38) and 10 years ((OR 1.25; 95% CI 0.51 to 3.06) Analysis 1.1) for LTME and OTME. Regarding overall survival at three (OR 1.00; 95% CI 0.70 to 1.42), five (OR 1.15; 95% CI 0.87 to 1.52) or 10 years ((OR 1.15; 95% CI 0.80 to 1.65); Analysis 1.2), again no differences could be found between the groups. Braga 2007 could not be included in the meta‐analysis because data were only shown in a Kaplan‐Meier curve, but did not show any differences between LTME and OTME groups. See Figure 3.

Forest plot of comparison: 2 Survival and recurrences, outcome: 2.1 Disease free survival.
Ng 2012 has reported the combined 10‐year follow‐up of Hong Kong a 2004 and Ng 2008 (n = 278) in a conference abstract, and reported no statistically significant differences in survival and recurrences (disease‐free survival 82.5% versus 77.6%, P = 0.443, overall survival 63.0% versus 61.1%, P = 0.505 and locoregional recurrences 5.5% versus 9.3%, P = 0.296).
Recurrences
There are no statistical significant differences seen in recurrence rates between LTME and OTME (local OR 0.89; 95% CI 0.57 to 1.39; Analysis 1.3, and distant OR 0.96; 95% CI 0.70 to 1.32; Analysis 1.4). As for port site metastases, only 11 participants (0.9%) in the LTME group developed a port site metastasis (Analysis 1.5). Eight were an extraction site recurrence, leaving only one true port site metastasis. The other two recurrences were not specified. Only three studies described the use of a wound protector in LTME, and reported a similar total of two (0.8%) port site recurrences (Hong Kong a 2004; Zhou 2004; Kang 2010).
Quality of resection: CRM positivity and number of lymph nodes retrieved
One of the most important variables for measuring the quality of the oncological resection and predicting recurrence and survival are circumferential margin involvement and number of lymph nodes retrieved. Eleven RCTs describe the number of retrieved lymph nodes, with no difference between both groups (MD ‐0.43; 95% CI ‐1.13 to 0.26; Analysis 2.1). Eight studies reported on circumferential margin positivity, with no difference between LTME and OTME (OR 0.99; 95% CI 0.71 to 1.40; Analysis 2.2).
Duration of surgery, incision length and conversion rate
The duration of surgery was longer for LTME in 11 out of 12 included trials for this analysis, with a difference of 37 minutes (MD 37.48; 95% CI 27.80 to 47.15; Analysis 2.3). Two other studies did not report on surgical time. Four studies reporting on incision length all found a shorter incision length for LTME with a mean difference of 12 centimetres (MD ‐12.83; 95% CI ‐14.87 to ‐10.80; Analysis 2.4).
All studies except two (Zhou 2004; Zhou 2007) describe the conversion rate for the laparoscopic group (Analysis 2.5). The mean conversion rate was 14.5% (0% ‐ 34%), and as described in MRC CLASICC a 2005, is highly dependent on the location of the tumour and the experience of the surgeon. For most studies, the surgeons' experience was not clearly stated and therefore cannot be compared from these results.
Intraoperative morbidity, blood loss and transfusion requirement
Ten studies described less intraoperative blood loss or transfusion requirement for LTME with a mean difference of 102 millilitres (MD ‐101.78; 95% CI ‐147.57 to ‐55.98; Analysis 2.6) and an odds ratio for transfusion requirement of 0.34 (95% CI 0.19 to 0.62; Analysis 2.7). Only King 2006 described a higher transfusion requirement for LTME, but a lower percentage of participants with over 100 millilitres of blood loss during surgery (27% versus 95%, P < 0.001). The overall intraoperative morbidity was described in four studies and was 11.3% for LTME versus 12.0% for OTME (OR 0.86; 95% CI 0.62 to 1.18; Analysis 2.8). There were insufficient data to compare bowel injury, haemorrhage and solid organ injury separately but individual studies did not show any differences.
Postoperative morbidity and mortality
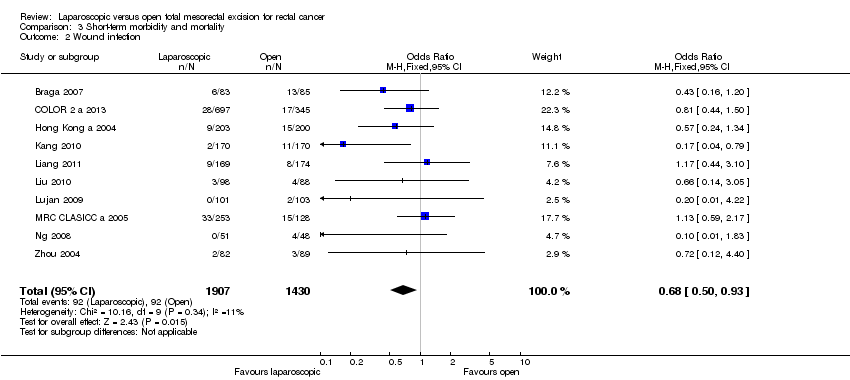
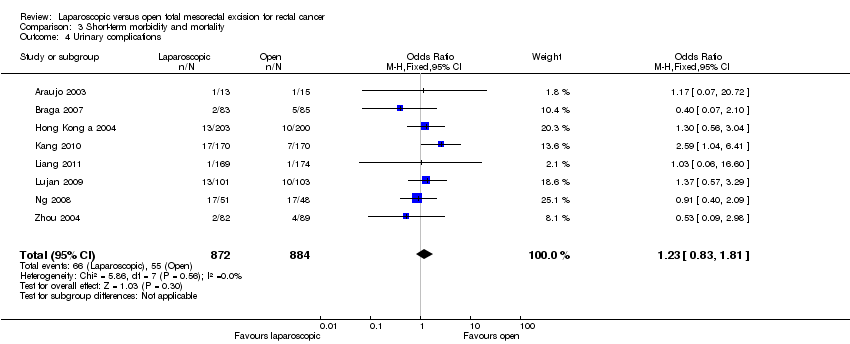
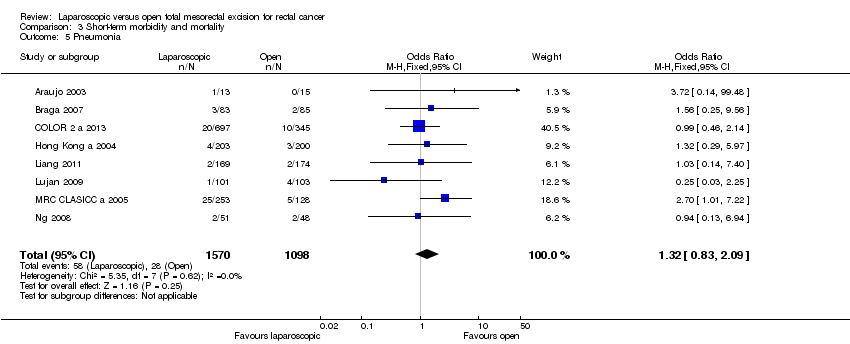
The overall complication rate was 29.3% (LTME) and 27.5% (OTME) (OR 0.94; 95% CI 0.80 to 1.10; Analysis 3.1), with fewer wound infections and less postoperative bleeding in the LTME group (OR 0.68; 95% CI 0.50 to 0.93 (Analysis 3.2) and OR 0.30; 95% CI 0.10 to 0.93 (Analysis 3.3)). We found no differences in urinary bladder infection or retention (OR 1.23; 95% CI 0.83 to 1.81; Analysis 3.4) and pneumonia (OR 1.32; 95% CI 0.83 to 2.09; Analysis 3.5) between both groups. See Figure 4.

Forest plot of comparison: 4 Short term morbidity and mortality, outcome: 4.1 30d morbidity (total).
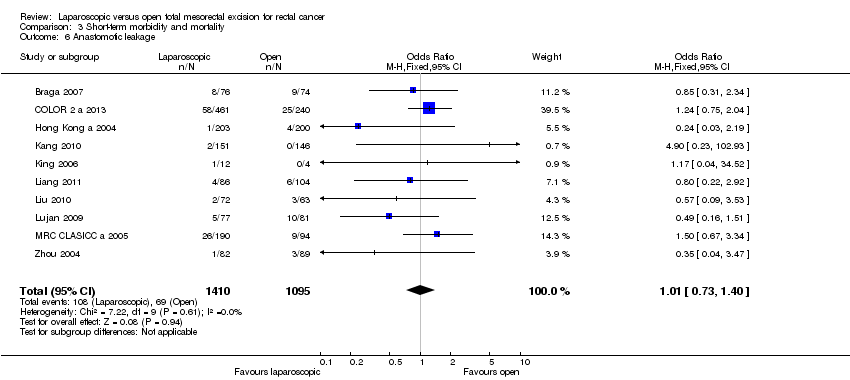
Ten studies described similar anastomotic leakage rate for both groups (7.7% vs 6.3% OR 1.01; 95% CI 0.73 to 1.40; Analysis 3.6), while two other trials only included abdominoperineal resection and did not have anastomotic leakage as an outcome. Consequently, the need for reoperation was 5.1% and 5.8% (OR 0.82; 95% CI 0.57 to 1.20; Analysis 3.7) in the LTME and OTME groups respectively. The anastomotic leakage rate has been corrected for participants without an anastomosis.
Data on postoperative mortality were available for 11 studies, with similar mortality rates for the two treatment groups for individual and grouped data (OR 0.81; 95% CI 0.50 to 1.32; Analysis 3.8). Four of them (Zhou 2004; Kang 2010; Liu 2010; Liang 2011) reported no 30‐day mortality in either group.
Postoperative pain
Postoperative pain can be assessed in many different ways. Common measures are a visual analogical scale (VAS) score, patient‐controlled anaesthesia (PCA) use, days of morphine use and epidural insufficiency requiring opioid use. Six studies reported results for pain score and analgesic use, and all reported lower analgesic use in the LTME group (standardised mean difference (SMD) ‐0.60; 95% CI ‐0.93 to ‐0.27; Analysis 4.1). COLOR 2 a 2013 reported on the percentage of participants using epidural, opioids or other analgesics, with less epidural use in the LTME group.Three trials reported on VAS pain scores, with a lower pain score for LTME at day one (MD ‐0.74; 95% CI ‐1.04 to ‐0.44; Analysis 4.2).
Gastrointestinal recovery and hospital stay
Length of hospital stay was given in 11 studies, and showed a reduction of two days for the LTME group (MD ‐2.16; 95% CI ‐3.22 to ‐1.10; Analysis 4.3). This is reflected in the gastrointestinal recovery rate to a faster resumption of a normal diet (MD ‐0.52; 95% CI ‐0.80 to ‐0.23; Analysis 4.4), and an earlier first bowel movement (MD ‐0.86; 95% CI ‐1.17 to ‐0.54; Analysis 4.5) in the LTME group. See Figure 5.
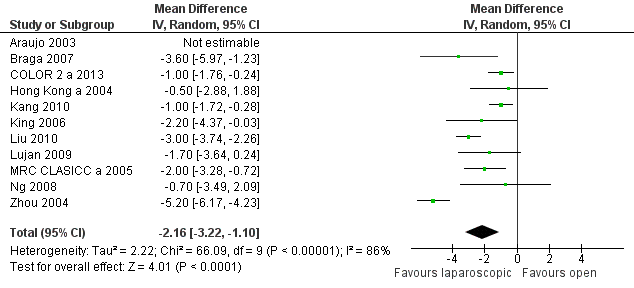
Forest plot of comparison: 5 Post op recovery, outcome: 5.3 Hospital stay.
Long‐term morbidity: Incisional herniae and bowel obstruction
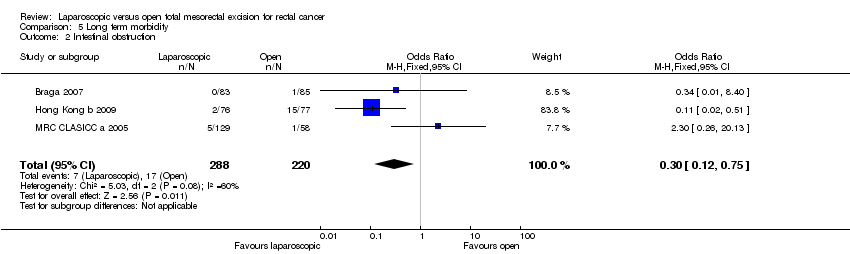
Only three studies reported on long‐term morbidity from incisional hernia and intestinal obstruction (MRC CLASICC a 2005; Braga 2007; Hong Kong b 2009). No statistically significant difference between OTME and LTME was seen (OR 0.84; 95% CI 0.32 to 2.21; Analysis 5.1). Intestinal obstruction occurred less frequently in the LTME group (OR 0.30; 95% CI 0.12 to 0.75; Analysis 5.2).
Quality of life: physical and sexual functioning
Four studies reported on quality of life using questionnaires (MRC CLASICC a 2005; King 2006; Braga 2007; Kang 2010). Only two reported on bladder and sexual functioning (MRC CLASICC a 2005; Kang 2010).
Of the four reporting on physical functioning, three reported significantly better functioning in the LTME group at three, six or 12 months. The MRC CLASICC a 2005 showed return to normal functioning at three months for both groups.
The reports on bladder and sexual functioning suffered from low response rates, varying from 71% overall response rate down to 10% on specific questions about sexual enjoyment and problems. Kang 2010 showed a baseline difference in sexual problems, but better sexual functioning after three months in both groups. In contrast, male sexual problems were worse three months after surgery but there was no difference between both groups. The LTME group had significantly fewer micturition, gastrointestinal and defecation problems at three months after surgery.
MRC CLASICC a 2005 and MRC CLASICC b 2005 both reported on participants in the CLASICC trial, but used different populations, questionnaires and time points. MRC CLASICC b 2005 showed worse sexual functioning after LTME, specifically for erectile dysfunction, but none were statistically significant. No differences in sexual interest, activity and enjoyment were seen at any time point, although for women there was a significant decrease compared to the preoperative baseline for both groups.
Immune response
Five studies described some short‐term differences in immune response (MRC CLASICC c 2001; Hong Kong d 2003; Zhou 2007; Hong Kong c 2000; COLOR 2 b 2011). They all reported different parameters, including C‐reactive protein (CRP), white blood cell count (WBC) and Interleukin‐6 (IL‐6). Two studies reported on B‐cell, T‐cell, cortisol and natural‐killer cell (NK‐cell) levels.
MRC CLASICC c 2001 had the largest population (n = 161), but did not show any differences in T‐cell, B‐cell and NK‐cell levels at day three. Zhou 2007 included 71 participants and the three other studies around 40 participants each. Hong Kong c 2000 showed higher levels of IL‐6 and CRP, with a peak for IL‐6 at two hours (P < 0.001) and CRP at 48 hours (P < 0.01) in the OTME group. The same results were shown by Zhou 2007, but they were measured at one and three days with a difference for IL‐6 at day one and for CRP at day one and three for the OTME group. Cortisol levels and WBC were also higher in the OTME group at day one. COLOR 2 b 2011 expressed results only as ratios compared to preoperative values and showed less increase in IL‐6 level at two hours postoperatively in the LTME group. Cortisol, WBC and CRP did not show any differences at 2, 24 and 72 hours. Finally, Hong Kong d 2003 did not show any differences at days one and three for WBC, NK‐cell, T‐cell and B‐cell levels, but for T‐cell and B‐cell levels there was less suppression in the LTME group at day eight.
Costs
An analysis of costs was included in five studies (Hong Kong a 2004; MRC CLASICC a 2005; King 2006; Braga 2007; Ng 2008). Data were too heterogeneous to be included in a meta‐analysis. Braga 2007 only reported the difference in costs in which the benefits of LTME could not compensate for the additional operating room charges, with a mean difference of USD 351 more for LTME. The four other studies calculated the costs per participant randomised. King 2006 and MRC CLASICC a 2005 reported the median direct and indirect costs for LTME. King 2006 reported the costs at GBP 6344 for LTME and GBP 6786 for OTME resulting in a saving of GBP 353 for LTME while being the only study in this analysis that used a fast‐track programme. MRC CLASICC a 2005 reported the opposite, with GBP 8259 for LTME and GBP 7820 for OTME, resulting in GBP 439 higher costs for LTME. Neither result achieved a statistically significant difference. Hong Kong a 2004 and Ng 2008 reported only the direct costs, with means of USD 9297 and USD 9588 for LTME and USD 7148 and USD 7517 for OTME with a significant difference of about USD 2000 in favour of OTME.
Discussion
Summary of main results
Nine studies (n = 1877) reported on at least one of the long‐term survival or recurrence outcomes and the meta‐analyses as well as the separate studies showed similar long‐term survival and recurrence rates for laparoscopic and open total mesorectal excision.
We found a mean difference in hospital stay of two days, with individual studies reporting a 0.5‐ to 5‐day difference in favour of LTME. Schwenk 2005 found comparable results for colon cancer with a mean difference of 1.5 days in favour of the laparoscopic group. Seven studies standardised their postoperative protocol, but only two implemented an enhanced recovery programme.
Overall completeness and applicability of evidence
Benefits of laparoscopic surgery are attributable to causing less surgical trauma to the patient, which has a positive effect on surgery‐induced immunosuppression. This can be demonstrated by taking measurements after surgery, with different peak moments for several parameters. The included studies in this review did not take measurements at the same time point, which may explain why not all of them could show differences in similar parameters. Reduced immunosuppression could be related to a lower complication rate and to shorter hospital stay, and may reduce development of postoperative metastasis (although this has yet to be shown in a randomised trial (Hogan 2011)).
The included RCTs include studies and subgroups of patients with low, mid and high rectal cancer and both APR and anterior resections with and without anastomosis. These differences can affect outcomes, especially the various techniques for low rectal resections can influence the circumferential margins and therefore local recurrences and survival. Lack of reporting of the CRM is an important issue with only eight out of fourteen studies describing this outcome. The number of retrieved lymph nodes is described by eleven studies but is more dependent on difference in high and low vascular ligations of the mesentery than on open or laparoscopic surgery. (Kessler 2013)
With a mean age between 44 and 72, three studies including T4 carcinoma and six offering neoadjuvant treatment in selected cases and a tumour localisation between 15 cm and the anal verge, there is a fair amount of heterogeneity among the included studies. Especially the early and smaller studies included a younger and healthier study population compared to the average rectal cancer patient. Of the four ongoing trials (n = 470 to 1100 participants), three (Kang 2010; ACTRN12609000663257; NCT00726622) require neoadjuvant treatment for selected stages of rectal cancer and the fourth (COLOR 2 a 2013) stratifies the randomisation for neoadjuvant treatment. This might influence both long term and short term outcomes as only six offered neoadjuvant therapy in this review. All ongoing studies include abdominoperineal resections as well as (low) anterior resections, but the maximum distance from the anal verge varies between 9 cm (Kang 2010), 12 cm (NCT00726622) and 15 cm (ACTRN12609000663257; COLOR 2 a 2013).
Another important difference between the included RCTs and current practise are the fast track recovery programmes such as the enhanced recovery after surgery (ERAS) programme. Only two included studies describe an enhanced recovery programme (King 2006; Lujan 2009). COLOR 2 a 2013 referred to local protocols, whereas the other two ongoing studies do not describe their postoperative protocol in the online summary. The LAFA trial (Vlug 2011) showed laparoscopic surgery in combination with fast track recovery resulted in the fastest recovery and hospital discharge compared to regular care and open surgery.
Quality of the evidence
Since 1998, 14 RCTs have been published to answer the question whether LTME results in better short‐term results and at least equal long‐term oncological results. The quality of these studies varied extensively, as did the number of included participants. Although the total mesorectal excision principle has been established since 1986, treatment protocols have changed. Surgeons gained more experience in laparoscopic colon and rectal cancer surgery, fast‐track protocols were introduced and neoadjuvant treatment became a standard of care in a proportion of cases. All of these factors are able to influence the long‐term results of these trials; however they should influence both the laparoscopic and open groups equally, except for the learning curve for laparoscopic procedures.
The quality of the evidence for the most important outcomes was moderate (summary of findings Table for the main comparison). This means that further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. The main reason is the imprecision of the confidence intervals, they allow for a variability in odds ratios up to 40% on both sides, which contributes to an absolute increase or decrease of 6% in disease free survival, 5% in overall survival, 2% in local recurrences, and 3% in 30‐day morbidity. The COLOR 2 a 2013 trial used a 5% margin for local recurrences for their non‐inferiority design, therefore our results remain within those limits.
Potential biases in the review process
Publication bias is a threat for any systematic review. We believe we have missed no important randomised controlled trials after screening reference lists of included trials and other relevant studies and reviews, in addition to the extensive systematic searching of electronic databases and trials registers. We have described all registered ongoing trials.
In the current literature regarding learning curves in laparoscopic colorectal surgery, a wide range of numbers of procedures is reported until a flat curve is achieve, ranging from 11 to 15 colectomies (Simons 1995), 30 colorectal resections (Schlachta 2001) and 60 to 65 colectomies (Tekkis 2005). For the open total mesorectal excision (OTME) technique, the cut‐off point for percentage of clear resection margins is defined as around 50 procedures (Oh 2011). This suggests that only the surgeons in Kang 2010 are assumed to have had sufficient experience for a good laparoscopic resection and results may further improve over time.
Agreements and disagreements with other studies or reviews
A meta‐analysis of RCTs on laparoscopic and open colorectal surgery (Sammour 2011) has shown a higher intraoperative complication rate for laparoscopic surgery of 6.3% versus 3.9% for open surgery (OR)1.55, 95%CI 1.12 to 2.15). The rate of bowel perforations was 2.1% versus 0.9% (OR 2.28, 95% CI 1.27 to 4.10) across 3018 participants. These differences had limited effect on the outcome, with an average postoperative complication rate of 28%. Compared to the intraoperative complication rate of 11.3% in LTME versus 12.0% in OTME in four included studies in our review (n = 1618), we cannot confirm these previously reported complication rates for LTME.
The results of this review confirm what other colorectal and rectal trials have suggested: short‐term results are similar with faster recovery in the LTME group and no statistically significant differences were found in the long‐term oncological results. For rectal cancer, non‐randomised trials have suggested oncological safe resections as presented in the previous version of this review (Fleshman 1999; Feliciotti 2003; Breukink 2006). Since then, several other reviews have been published describing the same results. Aziz 2006, Gao 2006, Anderson 2008 and Poon 2009 included mainly non‐randomised trials, and Row 2010 was a literature review. Ohtani 2011, Huang 2011 and Trastulli 2012 were the first to include only randomised trials. However, Ohtani 2011 also included three non‐randomised trials, Huang 2011 included only six trials and Trastulli 2012 nine trials, whereas this systematic review was able to identify 14. In addition, the Cochrane review of laparoscopic colorectal cancer (Kuhry 2008) presented separate meta‐analyses for four included rectal cancer RCTs.
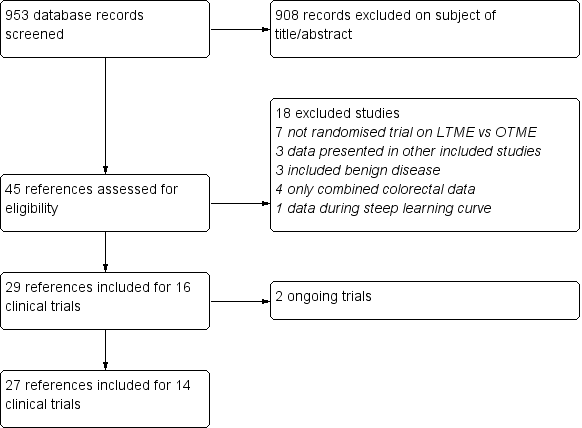
Study selection flow diagram.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Forest plot of comparison: 2 Survival and recurrences, outcome: 2.1 Disease free survival.
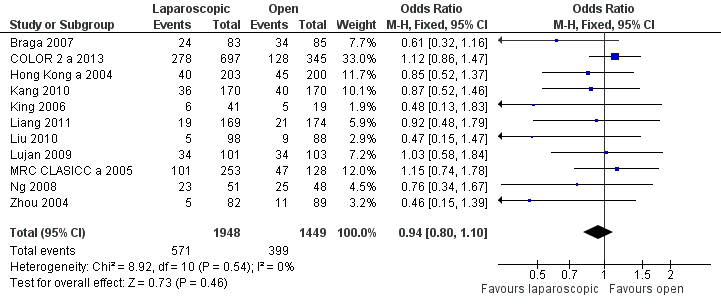
Forest plot of comparison: 4 Short term morbidity and mortality, outcome: 4.1 30d morbidity (total).

Forest plot of comparison: 5 Post op recovery, outcome: 5.3 Hospital stay.

Comparison 1 Survival and recurrences, Outcome 1 Disease‐free survival.

Comparison 1 Survival and recurrences, Outcome 2 Overall survival.
Comparison 1 Survival and recurrences, Outcome 3 Local recurrences.

Comparison 1 Survival and recurrences, Outcome 4 Distant recurrences.

Comparison 1 Survival and recurrences, Outcome 5 Wound/port site metastases.
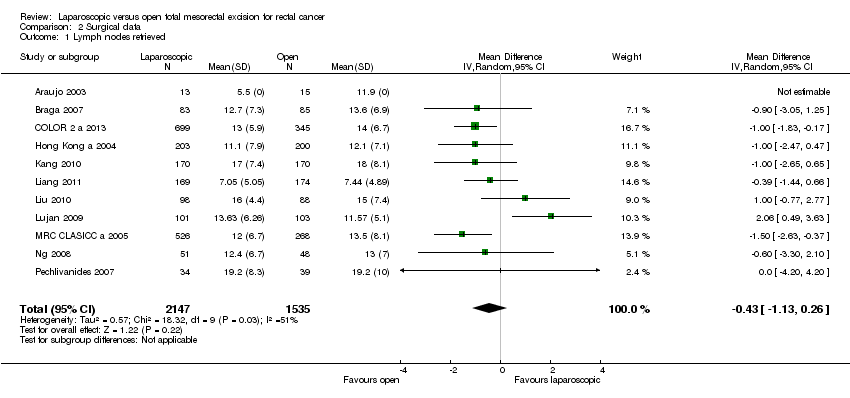
Comparison 2 Surgical data, Outcome 1 Lymph nodes retrieved.

Comparison 2 Surgical data, Outcome 2 CRM positivity.

Comparison 2 Surgical data, Outcome 3 Duration of surgery.

Comparison 2 Surgical data, Outcome 4 Incision length.
| Study | |
| Araujo 2003 | 0 (0/13) |
| Braga 2007 | 7.2 (6/83) |
| COLOR 2 a 2013 | 17 (121/695) |
| Hong Kong a 2004 | 23.2 (47/203) |
| Kang 2010 | 1.2 (2/170) |
| King 2006 | 7.3 (3/41) |
| Liang 2011 | 0.5 (1/169) |
| Liu 2010 | 0 (0/98) |
| Lujan 2009 | 7.9 (8/101) |
| MRC CLASICC a 2005 | 33.9 (82/242) |
| Ng 2008 | 9.8 (5/51) |
| Pechlivanides 2007 | 2.9 (1/34) |
| Zhou 2004 | Unknown |
| Zhou 2007 | Unknown |
Comparison 2 Surgical data, Outcome 5 Conversion rate.
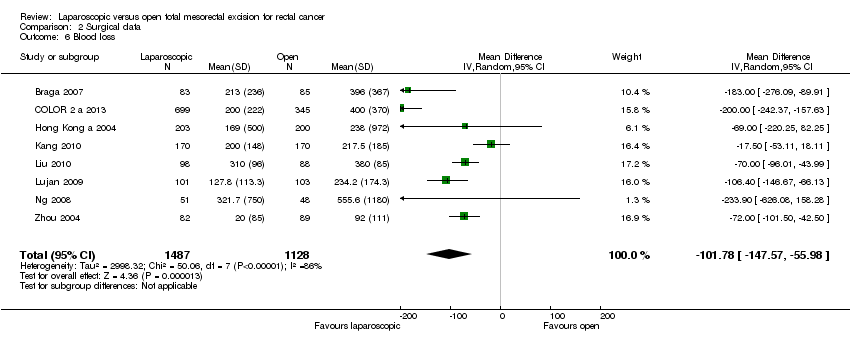
Comparison 2 Surgical data, Outcome 6 Blood loss.
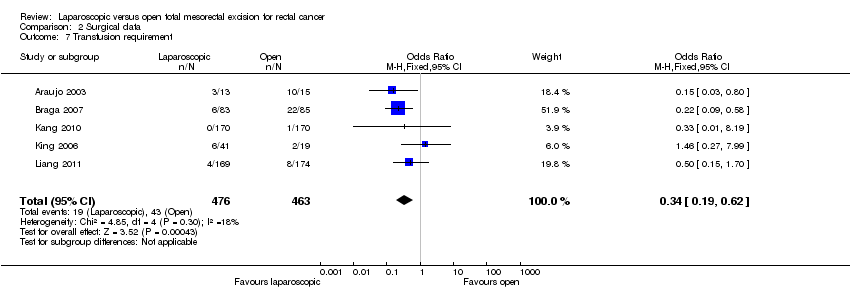
Comparison 2 Surgical data, Outcome 7 Transfusion requirement.

Comparison 2 Surgical data, Outcome 8 Intraoperative morbidity.
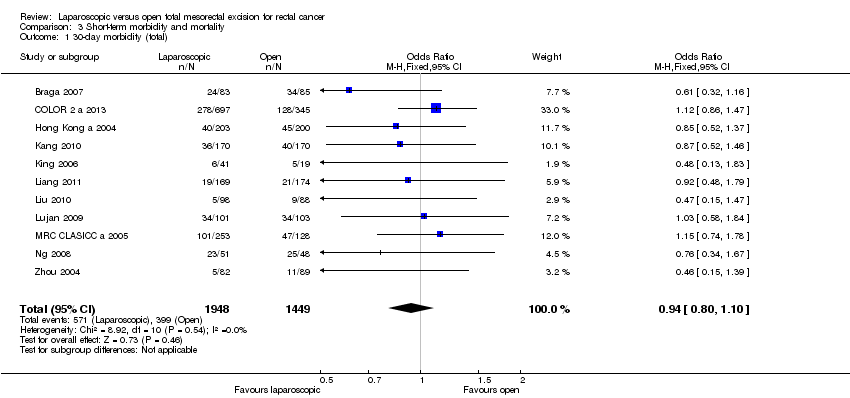
Comparison 3 Short‐term morbidity and mortality, Outcome 1 30‐day morbidity (total).
Comparison 3 Short‐term morbidity and mortality, Outcome 2 Wound infection.

Comparison 3 Short‐term morbidity and mortality, Outcome 3 Bleeding.
Comparison 3 Short‐term morbidity and mortality, Outcome 4 Urinary complications.
Comparison 3 Short‐term morbidity and mortality, Outcome 5 Pneumonia.
Comparison 3 Short‐term morbidity and mortality, Outcome 6 Anastomotic leakage.

Comparison 3 Short‐term morbidity and mortality, Outcome 7 Need for reoperation.

Comparison 3 Short‐term morbidity and mortality, Outcome 8 30‐day mortality.
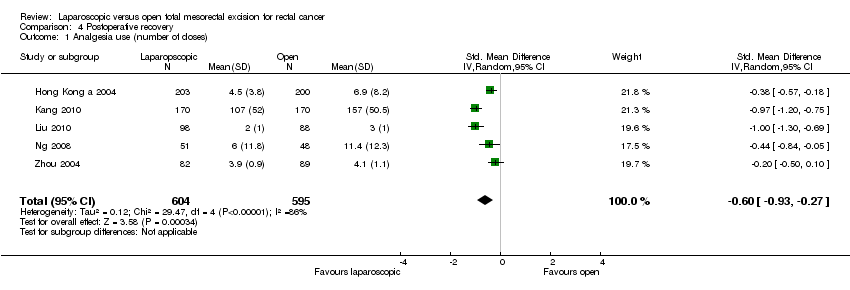
Comparison 4 Postoperative recovery, Outcome 1 Analgesia use (number of doses).
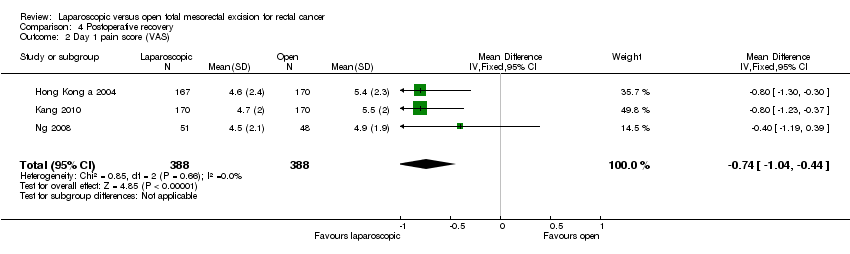
Comparison 4 Postoperative recovery, Outcome 2 Day 1 pain score (VAS).
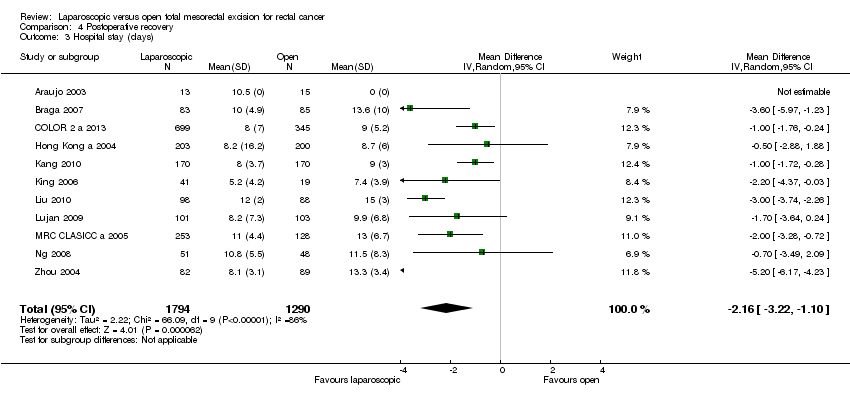
Comparison 4 Postoperative recovery, Outcome 3 Hospital stay (days).
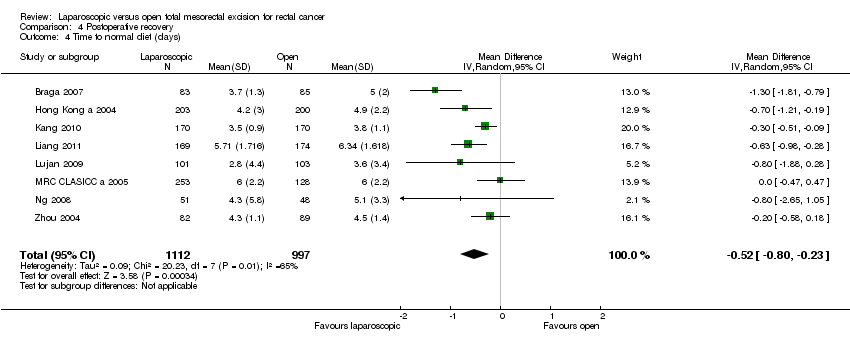
Comparison 4 Postoperative recovery, Outcome 4 Time to normal diet (days).

Comparison 4 Postoperative recovery, Outcome 5 Time to first defecation (days).

Comparison 5 Long term morbidity, Outcome 1 Incisional hernia.
Comparison 5 Long term morbidity, Outcome 2 Intestinal obstruction.
| Laparoscopic versus open total mesorectal excision (TME) for rectal cancer | |||||
| Patient or population: people with Rectal Cancer | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Open TME | Laparoscopic TME | ||||
| Disease‐free survival at 5 years | 718 per 1000 | 722 per 1000 | OR 1.02 | 943 | ⊕⊕⊕⊝ |
| Overall survival at 5 years | 679 per 1000 | 709 per 1000 | OR 1.15 | 987 | ⊕⊕⊕⊝ |
| Local recurrences | 54 per 1000 | 48 per 1000 | OR 0.89 | 1538 | ⊕⊕⊕⊝ |
| Lymph nodes retrieved | The mean number of lymph nodes retrieved in the intervention groups was | 3682 | ⊕⊕⊕⊕ | ||
| CRM positivity | 61 per 1000 | 60 per 1000 | OR 0.99 | 2313 | ⊕⊕⊕⊝ |
| 30‐day morbidity (total) | 275 per 1000 | 263 per 1000 | OR 0.94 | 3397 | ⊕⊕⊕⊝ |
| Hospital stay (days) | The mean length of hospital stay in the intervention groups was | 3084 | ⊕⊕⊕⊝ | ||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| 1Statistical inaccuracy with wide confidence interval at both sides 2Statistical inaccuracy with wide confidence interval at both sides, but a tendency for a higher overall survival for LTME 3Statistical inaccuracy with wide confidence interval at both sides, but a tendency for a lower recurrence rate for LTME 4Only 8 studies provided data on CRM positivity | |||||
| Study ID | n | Long‐term survival | 30‐day mortality | 30‐day morbidity | Long‐term morbidity | Lymphnodes | Gastrointestinal recovery | Pain | Bleeding | Length of hospital stay | Immune response | Quality of life | Cost |
| 28 | ‐ | ‐ | + | ‐ | + | ‐ | ‐ | + | + | ‐ | ‐ | ‐ | |
| 168 | 5y/3y | + | + | + | + | + | ‐ | + | + | ‐ | + | + | |
| 1044 | ‐ | + | + | ‐ | + | + | + | + | + | ‐ | ‐ | ‐ | |
| 40 | ‐ | + | + | ‐ | + | ‐ | ‐ | + | + | + | ‐ | ‐ | |
| 403 | 5y | + | + | ‐ | + | + | + | + | + | ‐ | ‐ | + | |
| 153 | 10y | ‐ | ‐ | + | ‐ | + | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | |
| 34 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | + | ‐ | ‐ | |
| 40 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | + | ‐ | ‐ | |
| 340 | ‐ | + | + | ‐ | + | + | + | + | + | ‐ | + | ‐ | |
| 19 | ‐ | + | + | ‐ | ‐ | ‐ | ‐ | + | + | ‐ | + | + | |
| 343 | 3y | + | + | ‐ | + | + | ‐ | + | ‐ | ‐ | ‐ | ‐ | |
| 186 | ‐ | + | + | ‐ | + | ‐ | ‐ | + | + | ‐ | ‐ | ‐ | |
| 204 | 5y | + | + | ‐ | + | + | ‐ | + | + | ‐ | ‐ | ‐ | |
| 381 | 10y/5y/3y | + | + | ‐ | + | + | ‐ | ‐ | + | ‐ | + | ‐ | |
| 148 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | + | ‐ | |
| 236 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | + | ‐ | ‐ | |
| 99 | 5y | + | + | ‐ | + | + | + | + | + | ‐ | ‐ | + | |
| 73 | ‐ | ‐ | ‐ | ‐ | + | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | |
| 171 | ‐ | + | + | ‐ | ‐ | + | ‐ | + | + | ‐ | ‐ | ‐ | |
| 71 | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | + | ‐ | ‐ |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Disease‐free survival Show forest plot | 5 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 10‐year | 1 | 130 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.25 [0.51, 3.06] |
| 1.2 5‐year | 4 | 943 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.76, 1.38] |
| 1.3 3‐year | 1 | 326 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.67, 1.74] |
| 2 Overall survival Show forest plot | 6 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 10‐year | 2 | 534 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.15 [0.80, 1.65] |
| 2.2 5‐year | 4 | 987 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.15 [0.87, 1.52] |
| 2.3 3‐year | 2 | 682 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.70, 1.42] |
| 3 Local recurrences Show forest plot | 8 | 1538 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.89 [0.57, 1.39] |
| 3.1 5‐year | 5 | 963 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.49, 1.81] |
| 3.2 3‐year | 3 | 575 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.84 [0.46, 1.56] |
| 4 Distant recurrences Show forest plot | 6 | 1341 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.70, 1.32] |
| 5 Wound/port site metastases Show forest plot | 7 | 2130 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.76 [0.75, 10.20] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Lymph nodes retrieved Show forest plot | 11 | 3682 | Mean Difference (IV, Random, 95% CI) | ‐0.43 [‐1.13, 0.26] |
| 2 CRM positivity Show forest plot | 8 | 2313 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.71, 1.40] |
| 3 Duration of surgery Show forest plot | 12 | 3840 | Mean Difference (IV, Random, 95% CI) | 37.48 [27.80, 47.15] |
| 4 Incision length Show forest plot | 4 | 1488 | Mean Difference (IV, Random, 95% CI) | ‐12.83 [‐14.87, ‐10.80] |
| 5 Conversion rate Show forest plot | Other data | No numeric data | ||
| 6 Blood loss Show forest plot | 8 | 2615 | Mean Difference (IV, Random, 95% CI) | ‐101.78 [‐147.57, ‐55.98] |
| 7 Transfusion requirement Show forest plot | 5 | 939 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.34 [0.19, 0.62] |
| 8 Intraoperative morbidity Show forest plot | 4 | 1618 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.62, 1.18] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 30‐day morbidity (total) Show forest plot | 11 | 3397 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.80, 1.10] |
| 2 Wound infection Show forest plot | 10 | 3337 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.68 [0.50, 0.93] |
| 3 Bleeding Show forest plot | 5 | 1181 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.30 [0.10, 0.93] |
| 4 Urinary complications Show forest plot | 8 | 1756 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.83, 1.81] |
| 5 Pneumonia Show forest plot | 8 | 2668 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.32 [0.83, 2.09] |
| 6 Anastomotic leakage Show forest plot | 10 | 2505 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.73, 1.40] |
| 7 Need for reoperation Show forest plot | 7 | 2316 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.57, 1.20] |
| 8 30‐day mortality Show forest plot | 11 | 3812 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.81 [0.50, 1.32] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Analgesia use (number of doses) Show forest plot | 5 | 1199 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.60 [‐0.93, ‐0.27] |
| 2 Day 1 pain score (VAS) Show forest plot | 3 | 776 | Mean Difference (IV, Fixed, 95% CI) | ‐0.74 [‐1.04, ‐0.44] |
| 3 Hospital stay (days) Show forest plot | 11 | 3084 | Mean Difference (IV, Random, 95% CI) | ‐2.16 [‐3.22, ‐1.10] |
| 4 Time to normal diet (days) Show forest plot | 8 | 2109 | Mean Difference (IV, Random, 95% CI) | ‐0.52 [‐0.80, ‐0.23] |
| 5 Time to first defecation (days) Show forest plot | 8 | 2893 | Mean Difference (IV, Random, 95% CI) | ‐0.86 [‐1.17, ‐0.54] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Incisional hernia Show forest plot | 3 | 508 | Odds Ratio (M‐H, Random, 95% CI) | 0.84 [0.32, 2.21] |
| 2 Intestinal obstruction Show forest plot | 3 | 508 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.30 [0.12, 0.75] |