Limpieza de la herida en las úlceras por presión
Resumen
Antecedentes
Las úlceras por presión (también denominadas escaras por presión, escaras de decúbito y úlceras de decúbito) son áreas de daño tisular en pacientes de edad avanzada, desnutridos o enfermos agudos, que no pueden cambiar de posición por sus propios medios. Las úlceras por presión representan una carga económica significativa para los sistemas de asistencia sanitaria y afectan de manera negativa la calidad de vida. La limpieza de las heridas se considera un componente importante del cuidado de las úlceras por presión.
Objetivos
Esta revisión sistemática trata de responder a la siguiente pregunta: ¿cuál es el efecto de las soluciones de limpieza de la herida y las técnicas de limpieza de la herida en la tasa de cicatrización de las úlceras por presión?
Métodos de búsqueda
Se hicieron búsquedas en el Registro especializado del Grupo Cochrane de Heridas (Cochrane Wounds Group) (búsqueda 3 de enero 2013), en el Registro Cochrane Central de Ensayos Controlados (Cochrane Central Register of Controlled Trials) (CENTRAL) (The Cochrane Library 2012, Número 12); Ovid MEDLINE (2010 hasta diciembre, semana 3, 2012); Ovid MEDLINE (In‐Process & Other Non‐Indexed Citations, 31 de diciembre 2012); Ovid EMBASE (2010 hasta 2012, semana 52); y en EBSCO CINAHL (2010 hasta el 21 de diciembre 2012).
Criterios de selección
Fueron elegibles para inclusión los ensayos controlados aleatorizados (ECA) que compararon la limpieza de la herida con ninguna limpieza de la herida, las diferentes soluciones de limpieza de la herida, o diferentes técnicas de limpieza, que informaron una medida objetiva de cicatrización de la úlcera por presión.
Obtención y análisis de los datos
Dos autores de la revisión de forma independiente extrajeron los datos y resolvieron los desacuerdos mediante discusión. Se realizó un resumen narrativo estructurado de los estudios incluidos. Para los resultados dicotómicos se calculó el riesgo relativo (RR), más los intervalos de confianza (IC) del 95%; para los resultados continuos, se calculó la diferencia de medias (DM), más los IC del 95%. No se realizó un metanálisis debido al número pequeño de ECA diferentes identificados. Dos autores de la revisión de forma independiente evaluaron cada estudio incluido mediante la herramienta de la Colaboración Cochrane para evaluar el riesgo de sesgo.
Resultados principales
En las búsquedas actualizadas se identificó un estudio elegible adicional, y se agregó un estudio a la tabla de estudios excluidos. Tres estudios (169 participantes) cumplieron los criterios de inclusión para la revisión. Ningún estudio comparó la limpieza con ninguna limpieza. Dos estudios compararon diferentes soluciones de limpieza de la herida. Se produjo una mejora estadísticamente significativa en las puntuaciones de la Pressure Sore Status Tool para las heridas que se limpiaron con un aerosol salino que contenía Aloe vera, cloruro de plata y decil glucósido (Vulnopur), en comparación con la solución salina isotónica (valor p = 0,025), pero no se observaron cambios estadísticamente significativos en la cicatrización cuando se comparó el agua con la solución salina (RR 3,00; IC del 95%: 0,21 a 41,89). Un estudio comparó técnicas de limpieza; en el caso de las úlceras por presión que se limpiaron con un lavado pulsátil, en comparación con el lavado simulado (el flujo de lavado se dirigió a un lavabo situado adyacente a la herida que no era visible para los participantes), hubo una reducción estadísticamente significativa del volumen de la úlcera al final del período de estudio de tres semanas en el grupo de lavado, en comparación con el grupo de lavado simulado (DM ‐6,60; IC del 95%: 11,23; ‐1,97).
Conclusiones de los autores
Solo se identificaron tres estudios que abordaron la limpieza de las úlceras por presión. Uno de ellos informó de una mejora estadísticamente significativa en la cicatrización de las úlceras por presión en las heridas que se limpiaron con un aerosol salino que contenía aloe vera, cloruro de plata y decil glucósido (Vulnopur), en comparación con solución salina isotónica; otro estudio informó que no se observaron cambios estadísticamente significativos en la cicatrización cuando las heridas se limpiaron con agua, en comparación con solución salina. En un estudio final se comparó el lavado pulsátil con el simulado y se encontró una reducción significativamente mayor del volumen de la úlcera al final del período de estudio en el grupo de lavado, en comparación con el grupo simulado. En términos generales, no existen evidencia convincentes de ensayos para apoyar el uso de cualquier solución de limpieza de la herida o técnica para las úlceras por presión.
Resumen en términos sencillos
Limpieza de la herida para ayudar a la cicatrización de las úlceras por presión.
Las úlceras por presión (también denominadas escaras por presión, escaras de decúbito y úlceras de decúbito) son áreas de daño tisular en pacientes de edad avanzada, desnutridos o enfermos agudos, que no pueden cambiar de posición por sus propios medios. Los tres ensayos identificados no encontraron evidencia convincente de que la limpieza de las úlceras por presión (escaras de decúbito) mediante una técnica particular, o la limpieza con una solución particular, ayuden a la cicatrización. Muy pocos estudios de investigación han examinado la limpieza de las úlceras por presión (escaras de decúbito), por lo que no es posible establecer conclusiones firmes.
Authors' conclusions
Background
Description of the condition
Pressure ulcers (also known as pressure sores, bed sores and decubitus ulcers) are localised areas of tissue damage caused by excess pressure, shearing or friction forces, which occur in those who cannot reposition themselves in order to relieve pressure on their bony prominences. This ability is often diminished in the very old, the malnourished and those with acute illness (Robertson 1990). In order to quantify the problem of pressure ulcers, prevalence studies and incidence studies have been conducted (Keelaghan 2008; Moore 2012; Schoonhoven 2006). It should be noted that the terms 'prevalence' and 'incidence' have different meanings and should not be used interchangeably. Prevalence refers to the number of people with a pressure ulcer at a point in time, or during a specific time period, while incidence concerns the rate at which new pressure ulcers develop in a defined population in a specific time period (Beaglehole 1993).
One cross‐sectional European study found that approximately 18% of hospital patients had a pressure ulcer (EPUAP 2002). An number of Irish studies have identified prevalence rates of between 10% ‐ 18.8% in acute and long tern care settings (Gallagher 2008; Moore 2000; Moore 2012). Reported incidence rates of pressure ulcers range from 2.2% to 66% in the UK, to 0% to 65.6% in the USA and Canada (Kaltenthaler 2001). These figures are influenced by the location and condition of the patient group (hospital compared with community setting, general hospital patients compared with those with fractured neck of femur) (Bridel 1996; Hanson 1993; Richardson 1981; Versluysen 1986). Pressure ulcers are more common in patient groups such as the elderly (Whittington 2000), those in orthopaedic settings (Versluysen 1986), and those who cannot reposition themselves (for example, younger patients with injuries to the spinal cord). Other medical conditions can also predispose the development of pressure ulcers (Schoonhoven 2002). Changing population demographics and the rise in the number of elderly patients in the future means that the number of people with pressure ulcers is likely to increase in the years ahead (Haalboom 2000). It is reasonable to suggest, therefore, that anything which improves ulcer healing outcomes will have a positive impact on both the individual and the health service as a whole (Thompson 1999).
The presence of a pressure ulcer impacts on the individual in many ways (Gorecki 2009). Pressure ulcers are painful (Gorecki 2009) and malodorous, especially when there is a large amount of dead tissue combined with anaerobic bacteria in the wound bed (Stotts 2001). Furthermore, pressure ulcers can exude profusely, particularly during the early inflammatory phase (Iocono 1998), and so require frequent changes of dressings (Rolstad 2000). It has been noted that the issues of concern for patients are pain, exudates, body image and worry about healing (Fox 2002), all of which alter an individual's quality of life (Gorecki 2009). In addition, it has been suggested that pressure ulcers also contribute to increased mortality (Kroger 2008; Redelings 2005).
Pressure ulcers are a significant financial burden to health care systems (Posnett 2009). The Touche Ross report (Touche Ross 1993) estimated the annual cost of treatment for pressure ulcers in the UK in 1993, at between £180 and £321 million, with the cost of prevention estimated at £180 to £755 million. More recently, Bennett 2004 explored the cost of pressure ulcer management and suggested that the total annual cost in the UK is £1.4 to 2.1 billion, or 4% of total healthcare expenditure. It is worth noting that costs of litigation or effects on quality of life, in terms of pain, depression and social isolation, were not included in these estimates. Therefore, at present, the precise economic impact of pressure ulcers has yet to be established (Posnett 2009).
Description of the intervention
The management of people with pressure ulcers involves a myriad of different interventions such as nutritional care (EPUAP/NPUAP 2009), pressure reducing/relieving surfaces (McInnes 2011), repositioning (Moore 2011) and skin and wound care (EPUAP/NPUAP 2009). Furthermore, in order to reduce the distress for individuals with pressure ulcers, it is essential that their wounds be managed successfully (Fox 2002). Following assessment of both the patient and the wound, the goal of management is to create the optimum local wound environment for healing (Rolstad 2000).
Selection of appropriate topical therapies (i.e. those applied to the skin) is widely believed to contribute to healing (Rolstad 2000). Available therapies include wound debridement (Ligresti 2007), the application of dressings (Ligresti 2007) and topical antimicrobial agents (O'Meara 2001). However there is little high quality research evidence to support the use of these therapies. Wound cleansing is regarded as an important component of pressure ulcer care (Hellewell 1997). It is assumed to be necessary to remove dead tissue and foreign bodies from wounds, and is usually undertaken before applying a dressing (Flanagan 1998a). However, there is uncertainty about what constitutes best practice (Fernandez 2012) and whether cleansing at all makes a difference. Clinicians and manufacturers recommend different solutions and methods of application, which is confusing (Fernandez 2012; Lawrence 1997; Lindholm 1999). Indeed, it is argued that wound cleansing practice is often based on past experience and ritual rather than the best available evidence (Carr 2006).
Why it is important to do this review
Fernandez 2012 previously conducted a systematic review of the effect of water as a wound cleanser however an exploration of the effect of cleansing technique was not a feature of this review. It is argued that wound cleansing has three elements: namely, the technique, the solution and the equipment (Young 1995). Techniques used include high pressure irrigation, swabbing, low pressure irrigation, showering, bathing, washing the affected area under a running solution, or total immersion in a whirlpool bath (also known as hydrotherapy) (Lawrence 1997; Lindholm 1999). Different cleansing solutions are also used; for example, normal saline, water, and antiseptic solutions (Angeras 1992). Furthermore, wound cleansing requires the use of equipment; for example, syringes, needles, catheters and pressurised canisters (Young 1995). Therefore, it is important to explore all components of the wound cleansing process, as the correct application of the solution may be as relevant as the solution itself (Morison 1989; Singer 1994). Consequently, it was decided to undertake a systematic review of the literature to summarise current evidence that could provide a contribution to relevant clinical guidelines. In addition, the review will inform research in this important area of patient care.
Objectives
To assess the effects of wound cleansing solutions and wound cleansing techniques on the healing rates of pressure ulcers.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) comparing wound cleansing with no wound cleansing, or RCTs comparing different wound cleansing solutions or different wound cleansing techniques, were considered for the review. Controlled clinical trials (CCTs) were to be considered in the absence of RCTs.
Types of participants
Studies involving people of any age, in any health care setting, with existing pressure ulcers (defined as a break in the continuity of the skin, caused by pressure, shearing or friction forces) (Nixon 1999).
Types of interventions
For the purposes of this review, cleansing was defined as the application of fluid to the pressure ulcer to aid removal of exudate, debris and contaminants, but not the use of dressings or mechanical debridement (Towler 2001). Water was included if, within the relevant study, it had been compared with another solution.
Studies investigating the following comparisons were eligible for the review:
-
cleansing compared with no cleansing;
-
one cleansing solution compared with another;
-
one cleansing technique compared with another (e.g. irrigation, swabbing, soaking, immersion).
Types of outcome measures
Primary outcomes
Trials were considered if they reported at least one of the primary outcomes:
-
an objective measure of pressure ulcer healing, such as time to complete healing; absolute or percentage change in pressure ulcer area or volume over time; proportion of pressure ulcers healed at the completion of the trial period; or healing rate.
Secondary outcomes
-
procedural pain (using validated scales where reported);
-
ease of use of the method of cleansing.
Secondary outcomes were only reported from studies that also reported primary outcomes.
Search methods for identification of studies
The search methods section of the second update of this review can be found in Appendix 1.
Electronic searches
For this third review update we searched the following electronic databases:
-
Cochrane Wounds Group Specialised Register (searched 3 January 2013);
-
The Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2012, Issue 12);
-
Ovid MEDLINE (2010 to November Week 3 2012);
-
Ovid MEDLINE (In‐Process & Other Non‐Indexed Citations December 31, 2012);
-
Ovid EMBASE (2010 to 2012 Week 52); EBSCO CINAHL (2010 to December 2012).
The following search strategy was used in The Cochrane Central Register of Controlled Trials (CENTRAL):
#1 MeSH descriptor Sodium Chloride explode all trees
#2 MeSH descriptor Sodium Hypochlorite explode all trees
#3 MeSH descriptor Saline Solution, Hypertonic explode all trees
#4 MeSH descriptor Iodophors explode all trees
#5 MeSH descriptor Chlorhexidine explode all trees
#6 MeSH descriptor Anti‐Infective Agents, Local explode all trees
#7 MeSH descriptor Disinfectants explode all trees
#8 MeSH descriptor Detergents explode all trees
#9 MeSH descriptor Soaps explode all trees
#10 MeSH descriptor Hydrogen Peroxide explode all trees
#11 MeSH descriptor Benzoyl Peroxide explode all trees
#12 MeSH descriptor Gentian Violet explode all trees
#13 MeSH descriptor Water explode all trees
#14 MeSH descriptor Alcohols explode all trees
#15 MeSH descriptor Solutions explode all trees
#16 normal saline or hypochlorit* or iodophor* or povidone or iodine or chlorhexidine or hibitane or betadine or antiseptic* or disinfectant* or antiseptic* or detergent* or soap* or “hydrogen peroxide” or “benzoyl peroxide” or “gentian violet” or eusol or dakin* or permanganate or water or "alcohol" or alcohols or solution*
#17 MeSH descriptor Irrigation explode all trees
#18 MeSH descriptor Baths explode all trees
#19 MeSH descriptor Hydrotherapy explode all trees
#20 (wound NEXT clean*) or (wound NEXT cleans*)
#21 wash* or scrub* or swab* or shower* or bath* or soak* or irrigat* or whirlpool
#22 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21)
#23 MeSH descriptor Pressure Ulcer explode all trees
#24 pressure NEXT (ulcer* or sore*)
#25 decubitus NEXT (ulcer* or sore*)
#26 (bed NEXT sore*) or bedsore*
#27 (#23 OR #24 OR #25 OR #26)
#28 (#22 AND #27)
The search strategies for Ovid MEDLINE, Ovid EMBASE and EBSCO CINAHL can be found in Appendix 2, Appendix 3 and Appendix 4 respectively. The Ovid MEDLINE search was combined with the Cochrane Highly Sensitive Search Strategy for identifying randomised trials in MEDLINE: sensitivity‐ and precision‐maximizing version (2008 revision) (Lefebvre 2011). The Ovid EMBASE and EBSCO CINAHL searches was combined with the trial filters developed by the Scottish Intercollegiate Guidelines Network (SIGN 2013). There were no restrictions on the basis of date or language of publication.
Searching other resources
For the original review, we searched the bibliographies of all retrieved and relevant publications, identified through these strategies. Manufacturers of cleansing solutions, as identified in the British National Formulary (BNF 2003) and experts in the wound care field, namely: council members of the European Pressure Ulcer Advisory Panel, The European Wound Management Association, The National Pressure Ulcer Advisory Panel and the World Union of Wound Healing Societies, were contacted (by ZM) to identify any studies not located through the primary search, or to identify any further researchers involved in pressure ulcer research, whom the authors could contact directly.
Data collection and analysis
Selection of studies
Titles and, where available, abstracts of the studies were assessed by two review authors independently, for their eligibility for inclusion in the review. Full versions of potentially relevant studies were obtained and screened against the inclusion criteria by two review authors independently. Any differences in opinion were resolved by discussion and where necessary with reference to the Cochrane Wounds Group editorial base.
Data extraction and management
Data from included trials were extracted into pre‐prepared data extraction tables. Two review authors conducted data extraction independently and any differences in opinion were resolved by discussion and reference to the Cochrane Wounds Group editorial base. If data were missing from reports, the study authors were contacted to obtain the missing information. The following information was extracted specifically from trial reports:
-
Author; title; source; date of study; geographical location of study.
-
Care setting.
-
Type of wound.
-
Inclusion/exclusion criteria.
-
Sample size.
-
Patient characteristics (by treatment group).
-
Design details; study type; method of group allocation.
-
Intervention details; outcome measures.
-
Analysis; results; conclusions.
Assessment of risk of bias in included studies
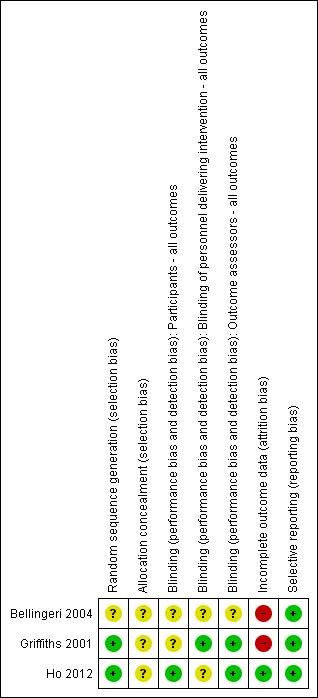
Two review authors independently assessed each included study using the Cochrane Collaboration tool for assessing risk of bias (Higgins 2011). This tool addresses six specific domains: namely, sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting and other issues (e.g. extreme baseline imbalance) (see Appendix 5) for details of criteria on which each judgement was based). Blinding and completeness of outcome data were assessed for each outcome separately. We then completed a risk of bias table for each eligible study, identifying wether we judged each component of the study to be low, unclear or high risk of bias. We have presented an assessment of risk of bias using a 'risk of bias summary figure' (see Figure 1) which presents all of the judgments in a cross‐tabulation of study by entry. This display of internal validity indicates the weight the reader may give to the results of each study.

Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
Data synthesis
Initially, a structured narrative summary of the studies reviewed was conducted. Data were then entered into the Cochrane RevMan software. For dichotomous outcomes, risk ratio (RR), plus 95% confidence intervals (CI) were calculated; for continuous outcomes, mean difference (MD), plus 95% CI were calculated.
Results
Description of studies
The initial search identified 111 titles. In addition, 33 letters were written to wound care experts and drug companies supplying cleansing solutions and 13 replies were received (response rate of 40%). No further trials were identified through this process.
Following independent review of the abstracts by two review authors, 12 papers were judged to be eligible and full papers were obtained. Two review authors independently assessed the papers and applied the inclusion and exclusion criteria. There was complete agreement between the review authors and three papers were identified as meeting the inclusion criteria (see Characteristics of included studies). The Characteristics of excluded studies table summarises the nine studies which did not meet the inclusion criteria and were subsequently excluded from the review (Boykin 1989; Colombo 1983; Della Marchina 1997; Hartman 2002; Hinz 1986; Kucan 1981; Saydak 1990; Toba 1997; Van Der Cammen 1987).
For subsequent updates of this review six studies were identified as excluded studies (Anzai 1989; Bellingeri 2003; Burke 1998; Diekmann 1984; Liu 1999; Wang 1997) (Characteristics of excluded studies) and one additional study was included (Ho 2012). The study by Burke 1998 was excluded at this review stage because the ocutome measures employed were objective not subjective (defined by Burke 1998 as wounds improved or not improved), this is an exclusion criteria as we had previously stated that the we would only include studies reporting an objective measure of pressure ulcer healing, such as time to complete healing; absolute or percentage change in pressure ulcer area or volume over time; proportion of pressure ulcers healed at the completion of the trial period; or healing rate.
Three eligible RCTs were identified, therefore, CCTs were not considered. The trials were published between 2001 and 2012. The first study looked at cleansing of chronic wounds (including pressure ulcers) with saline compared with cleansing with water, in the community care setting (Griffiths 2001). The second study looked at cleansing of pressure ulcers with isotonic saline compared with cleansing with saline spray containing Aloe vera, silver chloride and decyl glucoside (Vulnopur) in the hospital setting (Bellingeri 2004). The final study looked at cleansing of pressure ulcers with low‐pressure pulsatile lavage compared with sham (the lavage flow was directed into a washbasin positioned adjacent to the wound), in a spinal cord injury tertiary care center inpatient unit (Ho 2012). Overall, sample size was generally small which, consequently, is a major limitation of the studies; indeed the mean sample size was 53 (range 8 to 110).
Risk of bias in included studies
All studies detailed participant eligibility criteria and all stated that the participants were randomly allocated to the groups however only two studies reported an adequate method of generating the random sequence (Griffiths 2001; Ho 2012). The extent of allocation concealment was unclear for all three studies due to poor reporting.
Performance bias occurs where the awareness of which group the participant is in, rather than the intervention itself, actually affect the study outcomes. Reducing the risk of performance bias may be achieved through blinding participants and care givers. However, this remains a challenge in wound care, as many of the treatments used look different and are therefore difficult to disguise. None the less, Ho 2012 ensured that the participants were blind to the treatment allocation, however the treatment nurse knew which group each participant was in. Griffiths 2001 ensured that the outcome assessor was blinded to the treatment allocation, in addition the treatment nurse was also blinded (this was relatively easy to do as both solutions (saline and tap water) appeared identical). Bellingeri 2004 does not report whether the participant or the care giver were blinded to treatment allocation.
The risk of detection bias, that is systematic differences in how outcomes are assessed depending on which group the individual is allocated to, is reduced through the use of blinding of outcome assessment. Ho 2012 and Griffiths 2001 ensured that the outcome assessor was blind to the treatment allocation. However, Bellingeri 2004 did not report this information.
There were no drop outs in the study by Ho 2012, all ulcers being assessed at the final outcome assessment. Bellingeri 2004 reported that a per protocol analysis, instead of an intention to treat analysis, was undertaken, because it was not possible to assign a PSST score to patients withdrawn from the trial. Thus, only those who completed the study were included in the final analysis. Griffiths 2001, in their overall study, did not conduct intention to treat analysis as he excluded from the analysis 8 participants who were lost to follow up (four from each group) because they were admitted into hospital, did not adhere to the protocol, or declined to continue to participate.
Data on baseline comparability for prognostic factors were not clearly described in the studies of Griffiths 2001 and Bellingeri 2004. However, Ho 2012 reported that groups were equivalent at baseline.
Effects of interventions
How the results are presented and what the terms mean
Results for dichotomous variables are presented as risk ratio (RR) with 95% CI. Risk ratio is the rate of the event of interest (e.g. pressure ulcers healed) in the experimental group divided by the rate of this event in the control group and indicates the chances of pressure ulcer healing for people on the experimental treatment compared with the control treatment (Higgins 2011). Results for continuous variables are presented as mean difference (MD), with 95% CI. The mean difference measures the absolute difference between the mean value in two groups in a clinical trial (Higgins 2011). It estimates the amount by which the experimental intervention changes the outcome on average (for example, changes in pressure ulcer volume) compared with the control (Higgins 2011). Interpretation of the results is the same as RR except the point of no effect is 0 rather than 1 (Higgins 2011).
Comparison: cleansing compared with no cleansing
No trials were identified for this comparison.
Comparison: different cleansing solutions
Two trials were identified that compared different cleansing solutions (Bellingeri 2004; Griffiths 2001).
Saline Spray with aloe vera, silver chloride and decyl glucoside compared with isotonic saline
One RCT (Bellingeri 2004) enrolled 133 patients with pressure ulcers greater than Grade 1 (National Pressure Ulcer Advisory Panel scale, NPUAP 1989), seven of whom withdrew before the end of the trial because they were put onto antibiotics; use of antibiotics was an exclusion criterion. It is not known to which group or groups these seven participants were allocated and the trial author, in a personal communication, has not been able to obtain this information. Analysis was based on the 126 subjects who completed the trial.
The Pressure Sore Status Tool (PSST), developed in 1992 by Bates‐Jensen and colleagues, was used as an outcome measure in this study (Bates‐Jensen 1992). The tool uses 13 different items to assess pressure ulcer condition. All the items are scored with a Likert scale, giving a final value of between 13 and 65, with 13 indicating a healed ulcer.
There were 46 women and 28 men in the control group, with a median age of 73 years (range 62 to 83 years). Their wounds were cleansed with isotonic saline solution: PSST at baseline was 33 for this group, with a standard deviation (SD) of 10.3, minimum value (min) 15, maximum value (max) 52. There were 36 women and 23 men in the intervention group, with a median age of 74 years (range 56 to 84 years). Their wounds were cleansed with saline spray with Aloe vera, silver chloride and decyl glucoside (Vulnopur): mean PSST at baseline was 34.0, with SD 11.5, min 13.0, max 52.0. (Table 1 data presented in the study report with translated headings).
| Intervention | PSST Baseline | PSST Day 7 | PSST Day 14 | Total % Change |
| Isotonic saline solution (control) | mean 31.6 (SD 10.3, min 15.0, max 52.0) | 28.9 (SD 10.5, min 12.0, max 52.0). | 25.3 (SD 12.2, min 10.0, max 50.0). | ‐20.5 (SD 24.1, min ‐65.8, max 22.7). |
| Saline spray, Aloe vera, silver chloride and decyl glucoside (Vulnopur) (intervention) | mean 31.3 (SD 11.5, min 13.0 max 56.0) | 27.1 (SD 11.1, min 13.0, max 54.0). | 21.6 (SD 11.6, min 10.0, max 51,0). | ‐27.8 (SD 31.3, min ‐69.8, max 123.5). |
The authors did not describe how the cleansing was carried out, or identify the types of dressings used on the wounds after cleansing. The patients were followed up for a period of 14 days.
Primary outcome measure: percentage reduction in pressure sore status
The mean percentage change from baseline to day 14 in the control group was ‐20.5 (SD 24.1, min ‐65.8, max 22.7), while the mean percentage change in the Vulnopur spray group was ‐27.8 (SD 31.3, min 69.8, max 123.5). The data from this study were skewed and the trialists used non‐parametric tests that cannot be reproduced, because the raw data were not reported. As RevMan assumes a normal distribution, data have not been plotted graphically for this study, and we have accepted the trialists' analysis, which found that there was a statistically significant improvement in healing in the intervention group (P value = 0.025). The original author cannot confirm the group(s) from which the seven patients withdrew due to infection, however, the final group sizes are n = 59 in the Vulnopur group and n = 74 in the control group. If more of these patients withdrew from the Vulnopur group, the result would be biased towards that group.
Saline compared with tap water
Whilst the RCT comparing saline with tap water (Griffiths 2001), which enrolled 43 patients with 60 wounds, was intended to be analysed by intention to treat, eight patients were lost to follow up (four from each group) because they were admitted into hospital, did not adhere to the protocol, or declined to continue to participate therefore this was not analysis by intention to treat. Data analysis was, therefore, conducted on 35 patients with 49 wounds, eight of which were pressure ulcers. The data on pressure ulcers alone was made available by the trial authors, and this data forms the basis of what is reported in this review, i.e. 8 individuals with one pressure ulcer each.
The patients had chronic wounds of Grade 2 or 3, using Carville's definition (Carville 1995), and were receiving care in a community setting. According to Carville's definition, Grade 2 wounds have partial‐thickness skin loss (down to the epidermis and/or dermis), while Grade 3 wounds have full‐thickness skin loss (down to, but not through, the fascia) (Carville 1995). For the purpose of this review, data are presented on the eight pressure ulcers.
There were three men and three women in the intervention group (six wounds), with a mean age of 70.5 years (range 40 to 82 years). Their wounds were cleansed with tap water; the mean wound diameter size at baseline was 463 mm (range 59 mm to 826 mm). The control group consisted of one man and one woman (two wounds), with a mean age of 71 years (range 56 to 86 years). Their wounds were cleansed using saline; the mean wound size at baseline was 713 mm; range 535 mm to 790 mm.
Wound cleansing for both groups was conducted in a similar manner. The wounds were irrigated with either saline or water, delivered at room temperature via a 30 ml syringe and a 20 g cannula. The surrounding skin was patted dry and a clean dressing applied. It is not clear from the study how often the wounds were irrigated. A variety of topical dressings were used, including hydrocolloids and gels. A combination of hydrocolloid and gel or hydrocolloid alone was used topically on the intervention group, whereas either a hydrocolloid alone or a hydrocolloid and hydrocolloid paste was used in the control group. The participants were followed up for a period of six weeks.
Primary outcome measure: number of ulcers healed
Three wounds cleansed with tap water healed in the six‐week period, whereas none of the wounds cleansed with saline had healed at six weeks; risk ratio (RR) was 3.00 (95% confidence interval (CI) 0.21 to 41.89) (Analysis 2.1). The sample size was too small to rule out a treatment effect and therefore it is not possible to draw a firm conclusion.
Comparison: different cleansing techniques
One trial was identified that compared different cleansing techniques (Ho 2012).
Pulsatile lavage compared with sham
One small RCT (Ho 2012) recruited inpatients who had spinal cord injury and were receiving standard wound care for Grade 3 and 4 pelvic (coccygeal, ischial, or trochanteric region) pressure ulcers. 28 males were included in the study and randomly allocated, using a computer‐generated randomisation table, to control group (sham; n=14 ) or to the intervention group (pulsatile lavage; n=14 ). The authors report that the two groups were equivalent at baseline.
In the intervention group, low‐pressure pulsatile lavage treatment with 1 litre of normal saline at 11 psi of pressure was applied to the pressure ulcer once daily. In the control group, the pressure ulcers received sham treatment, that is, the lavage flow was directed into a washbasin positioned adjacent to the wound and was not visible to the participants, yet the noise of the machine could be heard by the participant. Following pulsatile lavage or sham treatment, each study participant received standard wound care (moist wound care) and bed rest with regular turning, and use of a low air loss mattress for those with pelvic pressure ulcers.
The participants were followed up for a three week period and improvement in pressure ulcer condition was assessed by measuring changes in ulcer volume, length, width and depth of the pressure ulcers.
Primary outcome measure: improvement in pressure ulcer condition
The wounds in the pulsatile lavage group demonstrated a statistically significantly greater mean reduction in ulcer volume (‐4.9 cm3) than the wounds in the sham group (‐3.7 cm3) (MD ‐6.60, 95% CI ‐11.23 to ‐1.97) (Analysis 1.1). However, this is a small study and these between group differences would need to be confirmed in a larger study.
Discussion
No adequately powered RCT was identified that compared cleansing with no cleansing of pressure ulcers. Three small RCTs were identified, each exploring a different aspect of wound cleansing. This is interesting when one considers that 18% of hospitalised patients have a pressure ulcer (EPUAP 2002) and that wound cleansing, among many other interventions such as repositioning and nutritional support, is a routine component of the management of these wounds (Rolstad 2000).
Saline spray containing Aloe vera, silver chloride and decyl glucoside (Vulnopur) was found to significantly improve PSST scores when used to cleanse pressure ulcers compared with isotonic saline. Furthermore, in one small RCT, cleansing with pulsatile lavage yielded a greater mean reduction in ulcer volume, compared with sham. There was no statistically significant difference in healing of pressure ulcers that had cleansed with saline when compared with those cleansed with water.
Some methodological issues require consideration and limit the conclusions that can be drawn from this review. The existing studies are small and underpowered ‐ indeed the mean sample size was 53 (range 8 to 110) ‐ which restricts the certainty with which differences between groups can be identified as statistically significant.
Risk of bias due to methodological approaches used and potential risk of bias where poor reporting precluded the adequate assessment of bias are important considerations in this review. True allocation concealment prevents the researcher being aware which group, experimental or control, a participant is allocated to, ensuring that the participant is assigned to a specific study group by chance (Higgins 2011). Concealment of group allocation was inadequately described in all of the studies. It has been suggested that lack of a clear description of allocation concealment leads to bias in assessing the outcome of studies (Moher 2001); the size of the effect could be overestimated and so give a false impression of the value of the intervention. Studies without adequate allocation concealment tend to report larger estimates of effect when compared to those who describe adequate allocation concealment (Schulz 2000).
Blinding of the study is said to be complete if the investigators, participants, outcome assessor, and the data analyst do not know which group the participant is allocated to (Higgins 2011). Human behaviour is influenced by prior knowledge, thus, without blinding, there is a risk that the size of the effect may be overestimated, resulting in a bias in favour of the treatment (Day 2000). Therefore, blinding is considered important in the assessment of subjective outcomes, such as ease of use of a treatment, and in ensuring comparability of assessment and diagnostic interventions across all groups within a study (Higgins 2011). Blinding is difficult to achieve in wound care, however blinded outcome assessment was achieved in two trials (Griffiths 2001; Ho 2012), though information on blinding was not reported by Bellingeri 2004.
The rationale for using intention to treat analysis is two‐fold; it maintains treatment groups that are similar (apart from random variation) and therefore validates the use of randomisation, and allows for handling of protocol deviations, further protecting the randomisation process (Hollis 1999). Omitting those who do not complete the study from the final analysis may bias the outcomes of the study, because those who do not complete may do so because of adverse effects of the intervention (Montori 2001). Intention to treat analysis was conducted in one of the studies as there were no reported withdrawals (Ho 2012) and Bellingeri 2004 reported undertaking a per protocol analysis. Greenhalgh 1997 suggests that data should be analysed for all participants originally included in the study, even if they did not complete the trial. Failure to do this can lead to an overestimation of the size of the effect, usually in favour of the intervention. However, although Fergusson 2002 argues that there may be certain circumstances where it is possible to exclude patients from analysis after randomisation (in order to avoid bias and to minimise random error), well designed studies that adhere to a high standard of methodological rigour, should ensure that this rarely happens.
In three of the studies, information regarding prognostic factors was unclear. The CONSORT statement set out to identify the key criteria required of authors when reporting results of studies (Moher 2001). The rationale for the development of this statement is that, to understand the significance of an RCT, the reader must be able to comprehend all components of the study clearly. Therefore, in order to be able to do this, the studies must include all relevant information when they are published. For the reader, the ability to judge the quality of a study is severely hampered by a lack of baseline data. It is evident from the studies included in this review that important pieces of information are either not reported or are not adequately described.
In conclusion, there is little evidence available pertaining to wound cleansing for pressure ulcers. One study demonstrated a statistically significant difference in outcomes for wounds cleansed with saline spray containing Aloe vera, silver chloride and decyl glucoside (Vulnopur) compared to isotonic saline solution (Bellingeri 2004) however this study was poorly reported and at potential risk of bias. A small study demonstrated a statistically significant reduction in ulcer volume reduction in wounds cleansed with pulsatile lavage compared with those cleansed using sham pulsatile lavage (Ho 2012). It appears that there is no evidence supporting the use of water rather than saline as a wound cleansing solution. None of the trials were without some risk of bias.
Well designed, robust studies are required. Such trials need to be sufficiently powered, with all groups comparable at baseline, adequate allocation concealment and blinded outcome assessment, with an intention to treat analysis, before firm conclusions can be drawn.
Methodological quality summary: review authors' judgements about each methodological quality item for each included study.

Comparison 1 Different cleansing techniques, Outcome 1 Pulsatile Lavage versus sham.

Comparison 2 Different cleansing solutions, Outcome 1 Saline versus tap water.
| Intervention | PSST Baseline | PSST Day 7 | PSST Day 14 | Total % Change |
| Isotonic saline solution (control) | mean 31.6 (SD 10.3, min 15.0, max 52.0) | 28.9 (SD 10.5, min 12.0, max 52.0). | 25.3 (SD 12.2, min 10.0, max 50.0). | ‐20.5 (SD 24.1, min ‐65.8, max 22.7). |
| Saline spray, Aloe vera, silver chloride and decyl glucoside (Vulnopur) (intervention) | mean 31.3 (SD 11.5, min 13.0 max 56.0) | 27.1 (SD 11.1, min 13.0, max 54.0). | 21.6 (SD 11.6, min 10.0, max 51,0). | ‐27.8 (SD 31.3, min ‐69.8, max 123.5). |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pulsatile Lavage versus sham Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.1 Changes in Volume | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Saline versus tap water Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.1 Healed wound within 6 weeks | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |