Intervenciones por los medios masivos de comunicación para el abandono del hábito de fumar en adultos
Información
- DOI:
- https://doi.org/10.1002/14651858.CD004704.pub4Copiar DOI

- Base de datos:
-
- Cochrane Database of Systematic Reviews
- Versión publicada:
-
- 21 noviembre 2017see what's new
- Tipo:
-
- Intervention
- Etapa:
-
- Review
- Grupo Editorial Cochrane:
-
Grupo Cochrane de Tabaquismo
- Copyright:
-
- Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cifras del artículo
Altmetric:
Citado por:
Autores
Contributions of authors
MB developed the concept for the project, formulated the search strategy and carried out searches, prescreened the abstracts, assessed relevant studies for inclusion, extracted the data and wrote the text of the review.
LS assessed relevant studies for inclusion, checked data extraction, and proofread the text of the review. RTM assessed relevant studies for inclusion and proofread the text of the review.
Sources of support
Internal sources
-
Jagiellonian University Medical College, Poland.
-
Medycyna Praktyczna, Poland.
-
Department of Primary Care Health Sciences, University of Oxford, UK.
-
National School for Health Research, School for Primary Care Research, UK.
External sources
-
State Committee for Scientific Research, Poland.
(2008 version of this review)
-
National Institute for Health Research, UK.
Declarations of interest
MB: none known.
LS: none known
RTM: none known
Acknowledgements
We thank Dr Paul Aveyard for comments and suggestions at the draft stage of this review; and Kate Cahill, who was an author on the previous version of the review.
Version history
| Published | Title | Stage | Authors | Version |
| 2017 Nov 21 | Mass media interventions for smoking cessation in adults | Review | Malgorzata M Bala, Lukasz Strzeszynski, Roman Topor‐Madry | |
| 2013 Jun 06 | Mass media interventions for smoking cessation in adults | Review | Malgorzata M Bala, Lukasz Strzeszynski, Roman Topor‐Madry, Kate Cahill | |
| 2008 Jan 23 | Mass media interventions for smoking cessation in adults | Review | Malgorzata M Bala, Lukasz Strzeszynski, Kate Cahill | |
| 2004 Apr 19 | Mass media interventions for smoking cessation in adults | Protocol | Malgorzata Bala, Lukasz Strzeszynski, Kate Hey | |
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
Medical Subject Headings Check Words
Adult; Female; Humans; Male;

Prisma flow diagram of search results
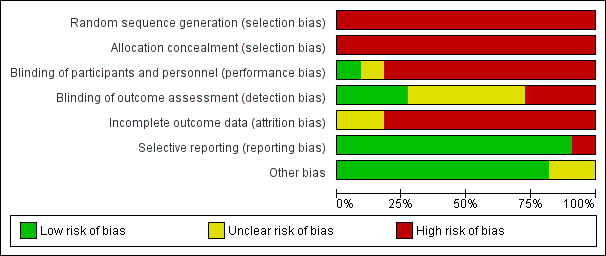
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
| Study | Design | Intervention | Control |
| California TCP 2003 | Nested cross‐sectional | 1990‐1 75.1%1 (CA only) | NHIS, BRFSS and CPS rates apply. |
| CORIS 1997 | Nested cross‐sectional | 69.5% at baseline, 67.5% at resurvey | 64% at baseline, 63% at resurvey |
| Jenkins 1997 | Nested cross‐sectional | Pretest: 84%, post‐test: 94% | Pretest: 82%, post‐test: 88% |
| Massachusetts 2003 | Nested cross‐sectional | Median (1995): 60.4%, median (1999): 42.7%6 | Median (1995): 68.4%, median (1999): 55.2% |
| McAlister 2004 | Nested cross‐sectional | Baseline survey 9407, 7m follow‐up 8974; response rate approximately 60%. | Not reported separately |
| McPhee 1995 | Nested cross‐sectional | Pretest: 81%, post‐test: 82% | Pretest: 85%, post‐test: 88% |
| McVey 2000 | Nested cohort | Smokers: 6m: 73%, 18m: 70% | Smokers: 6m: 74%, 18m: 66% |
| Mogielnicki 1986 | Randomized cohort | Mail: Yr2 follow‐up: 17% | Mail: Yr2 follow‐up: 15% |
| North Coast QFL 1983 | Nested cross‐sectional | Baseline: 71% | Baseline: 72% |
| Stanford 3 City 1977 | Nested cross‐sectional | Gilroy 116 at baseline. | Tracy 115 at baseline. |
| Sydney QFL 1986 | Nested cross‐sectional | Sydney: 66% | Australia‐wide: 60% |
Comparison 1 Mass media versus no mass media, Outcome 1 Response and retention rates.
| Study | Intermediate measure | Process measures |
| California TCP 2003 | Between 1996 and 1999 slight increases in agreements that smoking causes cancer (82.2% and 83.3%) and that passive smoking harms children's health (93.2% and 94%). Between 1992 and 2002 increases in agreement that passive smoking causes cancer in nonsmokers (1992: 62.4%, 1996: 66.8%, 1999: 68.9%, 2002: 72.1%) and that smoking harms children's health (1992: 85.5%, 1996: 87.7%, 1999: 90.1%, 2002: 90.9%). In 2008, 67.2% of daily smokers, 80.2% of non‐daily smokers, and 85.8% of nonsmokers perceived secondhand smoke (SHS) as a cause of cancer and 88.6% of daily smokers, 94.1% of non‐daily smokers and 94.7% of non‐smokers believed that SHS can harm the health of children and babies. Further increase in % of smokers thinking about quitting between 1994 and 2005, in the next 30 days (1994: 30.9, 2000:37.8%, 2005: 43.9%) and in the next 6 months (1994: 65.6%, 2000: 74%, 2005: 75%). In 2008, 95.2% of smokers and 96.6% of nonsmokers report having a completely smoke‐free workplace. Between 1992 and 2008 increase in % of homes with smoking ban (1992: 48.1, 1993: 50.9%, 1996: 64.5%, 1999: 72.8%, 2002: 76.9%, 2005: 78.4%, 2008: 80.8%). Between 1992 and 2008 increase in % of smokers with a total home ban on smoking (1992: 19.4 ± 1.6%, 2008: 59.3 ± 2.6%; increase of 204.9%). Between 1990 and 2008 decrease in % of nonsmokers exposed to ETS at work (1990: 29%, 1993: 22.4%, 1996: 11.8%, 1999: 15.6%, 2002: 12.0%, 2005: 13.9%, 2008: 13.5%). Increases in: support for further increase in tax on tobacco (1992: 74%, 1993: 78%; 2008: 78%), support for ban on tobacco advertising (1990: 52%, 1996: 65% [read from the graph]), support for ban on tobacco sponsorships (1998: 56%, 2000: 60%), % of adults preferring non‐smoking bars (1996: 75%, 2000: 81%), support for banning smoking outside the entrance of buildings (2002: 62.8%, 2008: 72.1%) and in restaurant outdoor patios (2002: 62.4%, 2008: 75%), outdoor public places (2002: 52.3%, 2008: 60.4%), Indian casinos (2002: 59.9%, 2008: 66.5%), inside cars when children are in them (2005: 92.3%, 2008: 95.2%). | Systematic monitoring of the campaign and independent evaluations of the programme. Media weight: 1990/1: 50+ TV spots, 50 radio spots (69 radio stations), 20 outdoor ads (775 outdoor venues), 40 newspaper ads (130 newspapers); 1992/3: 40 spots (20 TV, 12 radio, 8 in outdoor locations), 44% focused on reducing ETS, 34% on countering pro‐tobacco influences, 20% smoking cessation and 2% on reducing youth access. 1990/4: local health departments conducted 10,000+ multi‐session programmes focusing on prevention (61%), cessation (37%) and ETS (2%). July 1995 ‐ Dec 1996: 19 ads (11 TV, 4 radio, 4 outdoor); 1997 ‐ 1998: 40 general audience ads for distribution (20 TV, 12 radio, 8 outdoor); July 1998 ‐ Aug 1999: 50 general audience anti‐tobacco ads (22 TV, 13 radio, 15 print ‐ mostly billboards). In 1996, 67% of adults reported seeing antismoking message on TV, 44% hearing on radio, 41% seeing antismoking billboard. In 1998 80% of adults were exposed to tobacco control programme through two or more components. In 2011 in CSC 28% to 61% recalled anti‐tobacco commercials. 2011 recall of any of anti‐tobacco spots was not related to quitting 1 yr later, recall of one specific spot ("Stages") was associated with higher quit attempts rate and quitting for more than 1 month, after 1 yr. The analysis on the basis of per capita consumption of cigarettes and average per capita media expenditures gave estimates of a fall of 3.9 packs per capita per year for each per capita USD spent on the media campaign. |
| CORIS 1997 | At baseline, knowledge scores higher in Swellenden than in Riversdale (both cross‐sectional and cohort surveys; no statistical comparisons given); at 4 yrs more increase in women in Swellenden (both cross‐sectional and cohort surveys; in cohort survey net change statistically significant); at 12 yrs increase in both communities and no difference. | Participation and reach of activities recorded in mass media and community intervention town (not included in this analysis). Media weight: Limited data. 1st yr: 6 different billboards, 6 posters, 8 mailings, frequent news items, health messages on electricity accounts, 1 special supplement in local newspaper. 2nd and 3rd yr frequency of billboards, posters and mailings about half of the initial rate, but news items frequent and annual special supplement in a local newspaper was added. Intervention costs: per capita costs given (USD 5 over 4 yrs in intervention community). |
| Jenkins 1997 | At baseline no differences in motivation to quit and self efficacy (SF/Houston: 29%/23%; 29%/25%). At follow‐up significant increase in motivation in both communities, but no difference (SF/Houston: 45%/ 44%), no significant change in self efficacy (SF/Houston: 33%/26%). | A 15‐month uncontrolled pilot anti‐tobacco campaign. Maintenance: no evidence found. Intervention costs: no evidence found. |
| Massachusetts 2003 | 1993 ‐ 2000: the majority of non‐smokers believed that second‐hand smoke (SHS) can harm children (96%) and can cause lung cancer (89%); increase in % of smokers believing that environmental tobacco smoke (ETS) can harm their children (1993: 78%, 1999: 91%, 2000: 93%) and can cause cancer (1993: 58%, 1999: 72%, 2000: 74%); 2007 ‐ 94.5% believe ETS is harmful. Decrease in: ETS exposure at work (1993: 44%, 2000: 29%), at home (1993: 28%, 2000: 18%) and in restaurants (1995: 64%, 2000: 39%, 2002: 37%), mean hours of ETS exposure during prior week at work (1993: 4.2, 1995: 2.3, P < 0.05, 1997: 2.2, 2001: 1.4), and at home (1993: 4.7, 2000: 3.3). Increase in: % of population covered by smoking restrictions in restaurants (1995: 26%, 2000: 69%, 2001: 78%); % of population living in a town with some form of smoking restrictions in public places (1993: 22%, 2000: 78%, 2001: 85%); % of smokers reporting that fewer than half their friends and relatives smoke (1993: 40.8%, 2000: 46.9%; P for trend = 0.03); most non‐smokers reported so both in 1993 and 2000 (1993: 90.1, 2000: 89.9). 2008 ‐ 80.7% voluntary tobacco‐free homes (vs 81.5% in 2007). 2009‐ 57% of schools with comprehensive smoking policies 2014 ‐ based BRFSS exposure for ETS decreased to 10% (vs 32% in 2002); only 16.4% of houses allow smoking. and exposure to ETS >1 hr/last wk decreased to 11% (vs 32% in 2002; 14.5% in 2008). Increase in support smoking ban in all personal spaces ‐ of people living in smoke‐free houses 87% and of those living in non smoke‐free houses 52%. | Messages were developed through formative research including focus groups. Systematic evaluation of the programme. Media weight: Oct 1993 ‐ Dec 1996: 66 spots aired; 35 TV ads (14,901 total gross rating points [GRP]), 27 radio spots (13,644 total GRP) on smoking cessation in adults; 38 TV (17,800 total GRP) and 22 radio (13,950 total GRP) ads targeted youth; 6 TV (17,727 total GRP) and 2 radio spots (6,308 total GRP) on ETS. Awareness/reach: 88% respondents saw any TV ads, among quitters ‐ 97%. On average 4.48 ads recognised. In 1995, 65% of the adult population were aware of the statewide anti‐tobacco campaign, and 76% recognised the tag line of the media campaign "It's time we made smoking history". Around 89% of adult smokers reported having heard, read or seen information about quitting smoking within the past year. Dose‐response: no evidence found. Maintenance: The campaign is ongoing. Intervention costs: On average USD13 million per year spent on anti‐tobacco advertising. About 48% expenditure (up to Dec 1996) spent on TV time (much prime time viewing hours). MTCP activities expenditures: 1st yr ‐ USD 43 million, 3rd yr ‐ USD 35 million. Mean per capita cost for media campaign was USD 2.42. |
| McAlister 2004 | Knowledge, attitudes, beliefs, intentions, brand preferences were assessed at baseline. Process of change variables were measured by rating by responders how much they agree or disagree (1 = strongly disagree, 5 = strongly agree) with the statements regarding attitudes to smoking and occurrence of behaviours associated with smoking cessation. At follow‐up, mean level of agreement was significantly higher among those who reported daily smoking cessation compared to those who maintained daily smoking with regard to having support for quitting and behaviours associated with smoking cessation and dealing with tension. Participants still smoking at follow‐up were significantly more likely to agree with the statements about attitudes and ability to quit . There are no follow‐up results in comparison with control group. | In message development community forums, focus groups and pre‐testing were used. No information regarding ongoing monitoring of media campaign was provided. Media weight: no evidence found. Awareness/reach: At follow‐up correlations between media exposures and process variables were calculated for all groups. No separate result for mass media were given. Dose‐response: Not given for mass media campaigns without community programmes separately. Maintenance: no evidence found. Intervention costs: per capita media spending reported, high level and low level media represented about USD 0.25 versus USD 1.00 per capita for media spending during the year of the campaign. |
| McPhee 1995 | Motivation to quit and self efficacy significantly more common in Santa Clara (SC) at baseline (SC/Houston: 36%/23%; 34%/ 25%). At follow‐up motivation to quit increased significantly in both communities, but did not differ (SC/Houston: 44%/ 44%), self efficacy did not change significantly and did not differ at follow‐up (SC/Houston: 32%/ 26%). 'Any household member smokes' responses similar at baseline (SC/Houston: 31%/29%) fell significantly in both communities (SC/Houston: 26%/24%). 'No friend smokes' responses not different at baseline (SC/Houston: 4%/3%) increased significantly in both communities (SC/Houston: 15%/13%). 'All or most friends smoke' responses similar at baseline (SC/Houston: 43%/46%) increased in Houston (SC/H: 44%/51%). Never‐smokers or former smokers advising family or friends to quit smoking increased from baseline in both communities (SC vs Houston: from 51% to 62% (P < 0.05) vs from 34% to 66% (P < 0.05)). Current or former smokers being advised to quit by family or friends increased from baseline in both communities (SC vs Houston: from 53% to 63% (P < 0.05) vs from 51% to 62% (P< 0.05)). | Media weight: newspaper articles ‐ 562,000 print media exposures, videotape copies distributed to 60+ Vietnamese doctors' offices and 20 community agencies in SC; nearly 42,000 brochures at 500+ location in SC, nearly 6000 self‐help quit kit copies at 250+ locations; 1140 signs with adhesive backings saying "Please do not smoke" in Vietnamese distributed; 50 copies of 3 billboards posted each month and printed in newspapers and magazines (8,000,000 print media exposures). Paid TV ads ‐13,000 secs of air time; short anti‐tobacco presentations at 30 community events. CME courses on smoking cessation ‐ 68 Vietnamese physicians. Awareness/reach: Participants were asked if they had ever read article or seen advertisement in Vietnamese language newspaper or seen television programme or billboard in Vietnamese or heard a speech at a Vietnamese community meeting. Significantly more respondents from SC reported exposure to anti‐smoking activities in Vietnamese language (except for newspaper articles and public speaking). Smokers and non‐smokers in SC recalled significantly more intervention elements (SC vs Houston: out of a possible 5: 3.0 vs 1.6, P < 0.01 and 2.8 vs 1.4, P < 0.01). In SC significantly more physicians reported using antismoking brochures in Vietnamese, providing self‐help quit kits and referring patients to smoking cessation programmes (SC vs Houston: 86.4% vs 32.5%, P = 0.001; 66.7% vs 43.2%, P = 0.03; 35.9% vs 13.5%, P = 0.02). Quality of health education materials assessed: at follow‐up 96.4% of physicians reported they were helpful. Dose‐response: no evidence found. Maintenance: no evidence found. Intervention costs: no evidence found. |
| McVey 2000 | Smoking and health‐related attitudes assessed at baseline, no follow‐up data given. | Qualitative pilot research studies using focus groups and in‐depth interviews with smokers and ex‐smokers were conducted before and during the campaign. Media weight: It was estimated that over the course of the campaign in the double‐weight regions each viewer could see at least 20 screenings, and in single‐weight regions about 15. Awareness/reach: no evidence found. Dose‐response: nearly 20,000 calls to the quit line during the campaign. No evidence of an effect of intensity of ads measured at 6 month follow‐up found. Maintenance: After study completion the TV advertisements were shown nationally in all TV regions in England. Intervention costs: evidence not found. |
| Mogielnicki 1986 | Attitudes and beliefs regarding cigarette smoking were assessed on enrolment on a 5‐point rating scale (1 = disagree strongly, 5 = agree strongly). No separate results for 2nd yr follow‐up (mass media) given. | Surveys, interviews, copy tests among patients fulfilling study inclusion criteria but not included in the final study group. Media weight: One 60‐sec main commercial and 2 x 30‐sec variants used. A series of 3‐week 'flights'; main spot on TV was broadcast 40 times, and variants 106 times, radio spot ‐ 90 times. Each flight lasted 2 ‐ 3 weeks. Awareness/reach: Participants were asked about the recall of advertising campaign, clinic participants in media group (White River Jct): 61% did and 39% did not recall the advertising campaign at 6 month follow‐up. Dose‐response: Among those who recalled, 43.5% were abstinent at 6 months, while among those who did not 26.7% abstinent. Maintenance: no evidence found. Intervention costs: total costs of commercials development and production: USD 7480, broadcast time cost: USD15,150. |
| North Coast QFL 1983 | Attitudes to smoking and knowledge of the effects of smoking assessed in a questionnaire (6 questions each). No significant differences were found. Influences in decision to quit smoking reported ‐ the most common: health concerns (Coffs Harbour/Tamworth: 53%/ 59%), the least common: social pressure and media advertisement (Coffs Harbour/Tamworth: 1%/1%, 2%/1%), other were friends/family (Coffs Harbour/Tamworth: 15%/ 13%) and doctor's advice (Coffs Harbour/Tamworth: 7%/5%). Technique of quitting: most common ‐ 'cold turkey' (87% in both towns), quitting with help was rare (Coffs Harbour: self‐help kits 2%, group programme 1%, hypnosis 2%). | Focus groups and spot surveys were used to assess the effectiveness of the intervention techniques used. Media weight: Information collected only on community programme exposure. Awareness/reach: no evidence found. Dose‐response: no evidence found. Maintenance: no evidence found. Intervention costs: no evidence found. |
| Stanford 3 City 1977 | 25‐item behavioural interview on participants' knowledge about risk factors (diet, weight, exercise and smoking ‐ 3 items). Significant increases in knowledge scores in intervention cities compared to control city after 2 yrs. | Mass media campaign was monitored and revised; instructional content, development, pretesting, application and reformulation co‐ordinated by study staff. Media weight: limited data; TV programming ‐ 3 hours, 50 TV spots, 100 radio spots, several hours of radio programming, weekly newspaper columns, no details about newspaper and ads stories, billboards, printed materials sent via direct mail to participants, posters in buses, stores and work sites. Awareness/reach: no evidence found. Dose‐response: increases in risk factor knowledge related to increases in intervention intensity, even in Watsonville‐reconstituted group (mass media only, but a group in community received intensive face‐to‐face counselling) the gains were bigger than in Gilroy (mass media only group) and in both intervention communities the gains were bigger than in Tracy. Maintenance: After intensive 2 yrs, 1 yr reduced level campaign. Intervention costs: no evidence found. |
| Sydney QFL 1986 | Additional random samples of Sydney and Melbourne smoker populations surveyed in 1983 and 1986 (Sydney/Melbourne: 1983: 271/217; 1986: 557/ 550). Health beliefs and social influences increased between 1983 and 1986 (Sydney/Melbourne: 40+ years old: males 10% to 29%/21% to 29%; females 12% to 27%/22% to 32%; < 40: males 34% to 53%/30% to 43%, females 30% to 44%/31% to 41%). | Formative research on messages' effectiveness among target audience. Media weight: 1983: 389 primetime ads spots (3 commercials used) ‐ the intensity alternated in 2‐wk phases: between heavy and nothing for 1st 3 months, follow‐up ad campaign of half the intensity after 5 months. After 1st year spots during prime or fringe time for approx 4 wks at the start of the campaign yr ‐ each yr nearly 40 spots/wk. Awareness/reach: During 1st yr each month 750 people in Sydney and 200 in Melbourne interviewed on recall of campaign messages and response to the question on likelihood of giving up smoking in the next 12 months. The recall rates for the commercial most frequently shown were 87% in smokers, 82% in non‐smokers and 85% in ex‐smokers, the second in the frequency: 73%, 69% and 67% respectively. The third commercial recall rates were: smokers: 39%, non‐smokers: 31%, ex‐smokers: 33%. During campaign more smokers in Sydney indicated they were likely to quit smoking, especially after 4 months (difference: 18.6%); the difference disappeared by the end of the campaign. Long‐term assessment: TV ads recall measured each yr in separate random samples of the population of at least 1000 persons higher in Sydney (Sydney/Melbourne: 1984: males: 72%/70%, females: 80%/67%; 1986: males: 92%/68, females: 94%/67%). Dose‐response: number of calls to quitline was measured as a direct relationship to the number of TV spots aired (presented on the graph); peak response ‐ 11,000 calls in wk 8; 50,000+ calls to the quitline in the 1st 3 months. 'Quit centre' stop smoking programmes enrolments: almost 3000 in 1983 (previous yr 500); in wk 8 with peak quitline calls number ‐ 352. 19,196 quit kits sold. Maintenance: Since 1984 the campaigns continued in both Sydney and Melbourne till 1986, ads shown on primetime TV for 6 ‐ 8 weeks during winter months. Intervention costs: The budget for the campaign given (AUD 620,000), most of which was used for purchase of newspaper space and radio and TV time (AUD 500,000). |
Comparison 1 Mass media versus no mass media, Outcome 2 Intermediate measures.
| Study | Study population | Smoking prevalence | Tobacco consumption | Other outcomes |
| California TCP 2003 | Selection: population‐based surveys conducted nationally and in California (CA): National Health Interview Surveys (NHIS) 1978 ‐ 1994: household survey of a stratified, multistage, probability sample of the US population administered to all adults 18+ yrs; Behavioral Risk Factor Surveillance System (BRFSS) 1984 ‐ 1994: state surveillance of behavioural risk factors among adults, data collected through random digit dial telephone interviews (with multistage cluster sampling method); with California Adult Tobacco Survey from 1994, data up to 2008. Current Population Surveys (CPS) 1985, 1989, 1992/3 ‐ 1996: national survey of the US household population 15+ yrs, interviews in person; data up to 2008 California Tobacco Survey 1990‐2008 response rate 79.5% to 87.8%; CA, rest of US: from 1112 to 5747, from 9205 to 39,203; BRFSS 1984 ‐ 1994, response rate from 77% to 84%: from 1081 to 3959; with CATS from 1994 over 10,000 in CA and 80,000 to 400,000 in the rest of US. CPS 1985 ‐ 1996: response rate from 86% to 89%: CA, rest of US: from 4076 to 8272, from 70,164 to 97,856; CPS 1992/3 to 2006/7, CA, rest of US: from 16,000 to 24,000, from 210,000 to 290,000; CTS, CA only between 44,000 and 93,000 respondents per survey. | Final data (From 1990 programme start to 2008): All surveys (CTS, CPS and BRFSS pooled analysis years 1990 ‐ 2008, decline of smoking prevalence: CA 0.32% points per year, rest of US 0.24% points per year. 2008 smoking prevalence: CA 13.1%, rest of US: 19% Interim reported data: According to the analysis of the results of NHIS, adult smoking prevalence decreased more rapidly from 1985 to 1990 than from 1978 to 1985 in CA and in the rest of USA . Increase in rate of decline between 2 periods in CA was 0.62% points per year (95% CI ‐1.27 to ‐0.03), and in rest of USA 0.43 (‐0.70 to ‐0.16). Adult smoking prevalence decreased less rapidly from 1990 to 1994 than from 1985 to 1990 in CA (0.39% points per year) and in the rest of USA (0.05%, non‐sig different from zero). Between 1978 and 1994 adult smoking prevalence was 2 ‐ 5 percentage points lower in CA than in the rest of USA, but the estimated rate of decline in smoking prevalence was no‐sig different from that of the rest of USA during any of the 3 time periods. ‐0.6 (95% CI ‐0.79 to ‐0.40) vs ‐0.5 (‐0.67 to ‐0.33); All surveys combined analysis: CA, rest of US rate of decline % (SE) ‐ smoking prevalence %: | Final data (1970 ‐ 2008), per capita taxable sales: 1970 per capita sales similar in CA and rest of US. In 1989, CA sales 26.1% lower than sales for the rest of the US (108.8 versus 147.2 packs per year). Faster rate of decline in CA vs rest of the US. 2002 CA vs rest of the US lower sales (48 versus 101 packs per capita per year). From 2002 slower rate of decline in CA vs rest of the US (from 44.6 to 40.4 packs per year, a decline of 9.4%), but still lower sales than in the rest of the US. 2008: 40 versus 77 packs per capita per year, or 3.37 versus 6.42 packs per capita per month). 1989/90 to 2006/7, per capita consumption greater decline in CA vs rest of the US: 60.8% vs 41.0% (40 vs 92 packs per person per year). Per capita consumption based on aggregated sales data declined faster in CA in the early period of the campaign than before it started, and the decline was significantly greater than in the rest of USA. During late programme the decline slowed but remained greater than in the rest of USA. In another analysis presenting the results up to 1999 the rate of decline of tobacco consumption (tobacco consumption pack/month), CA/rest of US: Baseline 1/1983 ‐ 12/1988: ‐0.46 (9.5)/ ‐0.35 (12.4); In analysis presenting the results for tobacco consumption up to 2002, CA,/rest of US packs/month * CA vs rest of US P < 0.01. | Quit ratio, defined as % of ever‐smokers (current and former) who were former smokers in a given year, accelerated non‐sig in CA and in the rest of US between 1985 and 1990. 1990 to 1994, rate of increase in quit ratio decreased, with no significant changes in CA and in the rest of US compared to the period of 1985 to 1990. % of smokers who are currently quit for 3+ months did not change significantly (1990: 8.5 ± 1.0%, 1999: 5.4 ± 0.5%, 2008: 8.0 ± 2.5%) % of recent smokers currently in a quit attempt of 6+ months did not change significantly (1990: 5.6 ± 0.7%, 1999: 4.2 ± 0.5%, 2008: 6.4 ± 2.5%) |
| CORIS 1997 | Selection: Total population included in baseline and 4‐yr follow‐up surveys (15 ‐ 64 yrs at baseline and 15 ‐ 68 at 4‐yr follow‐up). | In total population % of smokers was lower in men and women in intervention compared to control city (non‐sig difference). | In total population tobacco consumption was lower in men and women in intervention compared to control city (non‐sig difference). | In women quit rates were significantly lower in intervention compared to control city. *significant difference compared to control; **significant compared with heavy smokers. |
| Jenkins 1997 | Selection: Phone surveys of randomly selected Vietnamese men, with numbers chosen randomly from 23 most common Vietnamese surnames listed in area phone books. After enumerating all men aged 18+ living in the household and speaking Vietnamese, subjects for interview were selected according to random age rankings in the household. | Smoking prevalence did not differ significantly at baseline. Post‐intervention, smoking prevalence fell significantly (P = 0.004) in SF and increased in Houston. Current smokers % among Vietnamese men: SF/Houston: | Significant difference in cpd at baseline (Houston higher), significant decrease in Houston, but not in SF. At follow‐up mean cpd was significantly higher in Houston. | Significant increase in quit rate in SF compared to Houston (P = 0.017). |
| Massachusetts 2003 | Selection: population‐based survey in Massachusetts (MA) and in the rest of USA (excluding CA) ‐ Behavioral Risk Factor Surveillance System (BRFSS): annual, state‐based, standardised, random digit dialled telephone survey of non‐institutionalised US adults aged 18+; 42 states including MA and CA participated consistently in BRFSS between 1989 and 1998; MA tobacco surveys conducted since 1993‐4 (baseline) in adults, and every month since March 1995, estimates of adult smoking prevalence are derived from household screening interviews with an adult informant who reported on smoking status for all adult members of the household. | According to the analysis based on BRFSS 1989 to 1998 and MA Tobacco Surveys 1993 to 1999 the slope of smoking prevalence after 1992 was significantly different from zero and from the slope for the rest of USA. Based only on BRFSS 1990 ‐ 1999 controlling for age, sex, race, and education there was a greater decline in current smoking between 1990 and 1999 among MA men than among MA women, and the decline was greater in MA than in the rest of the USA for men and for both sexes combined. | Annual per capita tobacco consumption based on aggregated sales data: | Quit ratio: not reported. |
| McAlister 2004 | Selection: telephone surveys of randomly selected (random digit dialing) adults from Texas (including individuals not resident in treatment areas); respondent in each household with the most recent birthday aged 18+ selected. Cohort of smokers identified in baseline cross‐sectional sample was followed. | Not reported ‐ only levels of daily smoking given (15.7 at baseline, 17.5 at follow up).. | Not reported. | Complete cessation achieved by approx 2% of panel of daily smokers. |
| McPhee 1995 | Selection: Phone surveys of randomly selected Vietnamese men, chosen randomly from 23 most common Vietnamese surnames in area telephone books. After enumerating all men aged 18+ living in the household and speaking Vietnamese, subjects for interview were selected according to modified Kish procedure. | At baseline smoking prevalence in SC differed significantly from Houston (control community). It slightly increased in control area and remained unchanged in intervention area ‐ there was no intervention effect. Current smokers among Vietnamese men, SC/ Houston: Baseline 1990: 36%/40%; | At baseline SC cig consumption differed significantly from Houston. It fell significantly in the control area , but there was no significant intervention effect. Mean cpd among smokers: SC/Houston: Baseline 1990: 9.9/13.2; | Quit rates in past 2 yrs differed significantly at baseline, but there was no significant intervention effect. |
| McVey 2000 | Selection: In each TV region a random sample of enumeration districts were selected (1 in 40) and within each district a random sample of households (1 in 20) using computer‐generated lists. Selected households were visited by interviewers and a resident member was selected for the sample with the use of pseudo‐random Kish‐grid method. Only adults at least 16 yrs were sampled. Only smokers and ex‐smokers were included in the study. Attempts were made to re‐interview the same respondents 6m and 18m later with similar structured questionnaire. | Not reported other than varying in different target regions. | Not reported. | By 18m, more successfully followed smokers in TV media group gave up smoking than in control group (non‐sig). Quit rates in smokers (TV media/control): 9.7%/8.7%; OR: 1.27 (95% CI 0.77 to 2.08), adjusted for predictors of giving up cigarettes: sex, age, manual/non‐manual job, daily cig consumption, "want to reduce smoking" and sex by manual/non‐manual work interaction. More ex‐smokers not relapsing were observed in TV media than in control group (significant): 96.3% vs 94.5%, adjusted OR: 2.21 (95% CI 1.11 to 4.40, P = 0.025); adjusted for predictors of remaining off cigs: number of cpd before stopping, length of time since stopping, whether persuaded to stop smoking by somebody else. TV media compared to no intervention was estimated to have increased the odds of not smoking. |
| Mogielnicki 1986 | Selection: reception clerks asked all patients registering for clinic visits about smoking and interest in stopping. | Not reported. | Not reported. | In clinic participants, number abstinent was higher in group receiving mass media compared to group not receiving mass media (calculated for all participants included in the study at baseline). In the mailing group in both media and no‐media groups no participant was abstinent and no number of participants included in the study at baseline was given. |
| North Coast QFL 1983 | Selection: systematic random sample of men and women 18+ from each town, up to 2 adults per household. | Significant effect of the intervention was found. | Not reported. | Quit rates not reported. |
| Stanford 3 City 1977 | Selection: in each city random multistage probability sample of men and women 35 ‐ 59 yrs old. | Reported only for high‐risk group (baseline/1st /2nd /3rd year follow‐ups): | Per capita cig consumption for adults 35 ‐ 59 yrs (baseline/% change 1973/1974): | Quit rates not reported. |
| Sydney QFL 1986 | Selection: random weekly selection from list of all Australian electoral subdivisions. Selected 10 separate households starting from randomly selected address from each electoral subdivision (clockwise direction around the residential block). Within household youngest person 14+ or 16+ interviewed. | At 1st cross‐sectional surveys prevalence decreased in Sydney compared to the rest of Australia (non‐sig). | Cross‐sectional studies after 1st issue of the campaign found decrease in cpd in Sydney compared to the rest of Australia (non‐sig). | Significantly larger proportion of Sydney smokers compared to Melbourne smokers quit smoking or cut down on cigs. Relapse rate and initiation rate were similar in both cities. * P < 0.05. |
Comparison 1 Mass media versus no mass media, Outcome 3 Primary measures of smoking behaviour.
| Study | Type of outcome | Orientation | Cost | Effect |
| California TCP 2003 | Prevalence | Social diffusion theory, with social marketing and social policy change | April 1990 ‐ June 1993 USD 26m for media campaign. | Pre‐programme prevalence 23.3 in CA vs 26.2 in rest of USA. By 1993 down to 18.0 in CA, 23.3 rest of USA; By 1996, prevalence still 18.0 in CA vs 22.4 in rest of USA. Final data (2008): CA 13.1%, rest of US: 19% Rate of decline % (SE): CA: Pre‐TCP: ‐0.74 (0.12) > early period : ‐1.06 (0.17) [P < 0.05 CA vs USA, P < 0.001 change from pre‐TCP] > late period 0.01 (0.21) P < 0.05 CA vs USA. Final data (up to 2008): CA 0.32% points per year, rest of US 0.24% points per year. Media campaign alone (without other Prop 99 components) led to decline in cig consumption of 12.2% between April 1990 and March 1991. Final data (1970 ‐ 2008), per capita taxable sales: CA sales 26.1% lower than sales for the rest of the US (108.8 versus 147.2 packs per year). Faster decline in CA vs rest of the US. 2002 48 versus 101 pc per yr 2008: 40 versus 77 pc per yr, |
| CORIS 1997 | Prevalence | Not reported | pc cost of USD 5 over 4 yrs in media‐only intervention town. | After 4 yrs, Intervention (Control) prevalence in men dropped from 49.5 (45.7) to 40.4 (38.1) , and in women from 17.6 (16.1) to 14.0 (15.6) . Data contains paired and unpaired observations, in total population. |
| Jenkins 1997 | Prevalence | Not reported | Not reported | At 2 yrs, San Francisco (int) prevalence down from 36.1 to 33.9 (P ≤ 0.01), and Houston (control) up from 39.6 to 40.9. Net change was ‐3.5 % points (P = 0.004). |
| Massachusetts 2003 | Prevalence | Social diffusion theory, with social marketing and social policy change | USD 39m pa for whole programme. | 1990 ‐ 9: MA prevalence declined from 23.5 (CI 21.0 to 26.1) to 19.4 (CI 18.0 to 20.8). |
| McAlister 2004 | Prevalence | Social learning theory, transtheoretical model. using modelling, social reinforcement for behaviour change, and emotional arousal. | USD 9m pa | Prevalence of daily smoking increased from 15.7 to 17.5. |
| McPhee 1995 | Prevalence | Not reported | Not reported | No change in prevalence in Intervention community from baseline to 2 yrs: 36.0, while controls increased (non‐sig) from 40 to 41. |
| McVey 2000 | Quit and relapse rates. | No formal attributing, but 'morbid humour' used. | Not reported | At 18m, 9.8% of intervention smokers vs 8.7% of control had quit, and 4.3% of intervention ex‐smokers vs 3.7% controls had relapsed. Pooled OR of not smoking was 1.53 (CI 1.02 to 2.29, P = 0.04). |
| Mogielnicki 1986 | Cessation rates | Mass marketing techniques (situation analysis, objective definition, copy development, media plan, campaign launch) combined with traditional clinical trial approach. | Copy development and production: USD 7480, Air time: USD 15,150 (1980 USD) | Per protocol clinic cessation at 2nd year: |
| North Coast QFL 1983 | Prevalence | Social marketing and communication theory | Not reported | Mean declines in prevalence in Intervention community of 9.5% from baseline to Yr 3, and in controls of 4.4%. |
| Stanford 3 City 1977 | Prevalence | Social marketing, social learning and communication theory | Not reported | All participants: Baseline: Intervention 65.5, Control 55.6. |
Comparison 1 Mass media versus no mass media, Outcome 4 Study summary by type of outcome.
| Study | Differences | Possible confounders | Adjusted effects |
| Jenkins 1997 | San Francisco (Int) respondents significantly less proficient in English, of lower education, lower income, less likely to be employed and more recent year of immigration than Houston (control) respondents. | All these factors were included in multivariate analyses. | Unadjusted ORs not reported. Strongest predictor of quitting was being a student (adjusted OR 2.19, 95% CI 1.45 to 3.33); at least high school education (OR 1.33: CI 1.04 to 1.70); more recent year of immigration (OR 1.03: CI 1.00 to 1.05); each + yr of age (OR 1.03: CI 1.02 to 1.04). |
| Massachusetts 2003 | MA respondents were more likely to be white non‐Hispanic and more likely to be college graduates than the respondents from the rest of USA. | Age, sex, race and education were treated as confounders. | Unadjusted OR for current smoking in MA in 1999 vs 1990 was 0.78 (CI 0.66 to 0.92, P trend 0.01). |
| McAlister 2004 | Responders and non‐responders to follow‐up survey differed significantly by age, race and gender. | Daily smoking rate "adjusted for age, gender and educational level". No OR reported. | |
| McPhee 1995 | Small but significant differences in mean age, educational level, English language proficiency, mean year of immigration, between SC and Houston and/or between pre‐ and post‐test samples. Larger differences in employment (8% unemployed in SC vs 6% in Houston pre‐test) and income (32% below poverty level in SC vs 26% in Houston post‐test). | Analyses controlled for site, time, (pre‐, post‐test), intervention term (site x time), age, education, English language proficiency, year of immigration, employment status, income. | Differences in prevalence between SC and Houston did not persist after controlling for sociodemographic characteristics. Strongest predictor of current non‐smoking was age 65+. Age 18 ‐ 24, immigration before 1977, college education and English fluency all predicted non‐smoking, but employment and income did not. Adjusted OR for intervention term was 1.1 (95% CI 0.9 to 1.4). Adjusted OR for recent quitting 1.1 (95% CI 0.7 to 1.7). |
| North Coast QFL 1983 | Age and sex differences across towns and years. | To counter known confounding, an AGE*SEX*TOWN term was constructed for the regression model, and a TOWN*YEAR factor. | |
| Sydney QFL 1986 | Location of interview (Sydney vs Melbourne) was significant predictor of quitting (P < 0.05). | Sex, age, education, marital status, SES did not predict quitting or act as confounders. | No ORs reported. |
Comparison 1 Mass media versus no mass media, Outcome 5 Baseline differences and possible confounding.
| Mass media smoking cessation intervention compared with no intervention for smoking cessation | ||||
| Patient or population: Adults who smoke Settings: Community Intervention: Mass media Comparison: No mass media | ||||
| Outcomes | Impact | No of | Quality of the evidence | Comments |
| Smoking prevalence (follow up from 6 months to 18 years) | The 2 state‐wide programmes, in which mass media campaigns were part of comprehensive tobacco control programmes, observed greater declines in smoking prevalence than in the rest of the USA. Of the 5 community‐based studies, 2 found significant decreases in smoking prevalence, 1 did not detect a significant effect, and of 2 studies conducted among Vietnamese‐American men, one detected a statistically significant decrease in smoking prevalence at 2 years, while the other did not. | 7 (n = 1,965,478)1 | ⊕⊝⊝⊝ | 2 studies were interrupted time series; and 5 were quasi experimental |
| Tobacco consumption (follow up from 2 to 18 years) | In the 2 state‐wide campaigns cigarette consumption was measured on the basis of aggregated sales data. In 1, a statistically significant decline was observed compared with the rest of the USA. In the other, declines in consumption were reported, but without statistical comparisons. Of the five community‐based studies, 1 study detected a significant reduction in cigarette or tobacco consumption for a high‐risk group, who also received counselling, but not in the media‐only intervention community compared with controls. The remaining 4 studies did not detect significant differences. | 7 (n = 1,964,292)1 | ⊕⊝⊝⊝ | 2 studies were interrupted time series and 5 were quasi experimental |
| Abstinence or quit rates (follow up from 6 months to 18 years) | Among the 8 studies presenting abstinence or quit rates, 4 showed some positive effect. 1 state‐wide campaign presented the quit ratio (i.e. the percentage of ever‐smokers (current and former) who were ex‐smokers in a given year), finding a statistically significant difference in favour of the intervention. The other 7 studies were community based; of these, 4 detected a statistically significant effect in favour of the intervention across the study population, 1 found statistically significant differences only in women, 1 study reported a non‐statistically significant difference in point prevalence of daily smoking, and 1 detected no significant differences. | 8 (n = 987,800)1 | ⊕⊝⊝⊝ | 1 study was quasi RCT and 7 were quasi experimental |
| Quit attempts (follow‐up from 7 months to 18 years) | Of the 5 studies that assessed quit attempts, 3 were community‐based studies, and 2 were state‐wide campaigns. 2 community‐based studies among Vietnamese‐American men found no significant differences between the intervention and control communities. A third study only assessed quit attempts among participants still smoking at follow‐up, of whom 27.3% had made quit attempt. 2 state‐wide campaigns assessed quit attempts only in the intervention community. In 1 they increased in line with campaign duration but not to a statistically significant extent, in the other the percentage of smokers with a quit attempt in the last year increased over the duration of the study, but without statistical comparisons. | 5 (n=1,947,674)1 | ⊕⊝⊝⊝ | 2 studies were interrupted time series and 3 studies were quasi experimental |
| GRADE Working Group grades of evidence | ||||
| 1 Estimated participant numbers based on the number of respondents to surveys and the number of participants at follow up in the quasi‐experimental studies. 2 GRADE rating started at 'low': none of the studies were RCTs. One was a quasi‐RCT, two were interrupted time series and eight were quasi‐experimental. 3 Downgraded one level for inconsistency: included studies varied in design, intervention, comparator and population, and results were not homogenous. | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Response and retention rates Show forest plot | Other data | No numeric data | ||
| 2 Intermediate measures Show forest plot | Other data | No numeric data | ||
| 3 Primary measures of smoking behaviour Show forest plot | Other data | No numeric data | ||
| 4 Study summary by type of outcome Show forest plot | Other data | No numeric data | ||
| 5 Baseline differences and possible confounding Show forest plot | Other data | No numeric data | ||