Systemische antimykotische Therapie bei Kindern mit Tinea capitis
Abstract
Background
Tinea capitis is a common contagious fungal infection of the scalp in children. Systemic therapy is required for treatment and to prevent spread. This is an update of the original Cochrane review.
Objectives
To assess the effects of systemic antifungal drugs for tinea capitis in children.
Search methods
We updated our searches of the following databases to November 2015: the Cochrane Skin Group Specialised Register, CENTRAL (2015, Issue 10), MEDLINE (from 1946), EMBASE (from 1974), LILACS (from 1982), and CINAHL (from 1981). We searched five trial registers and checked the reference lists of studies for references to relevant randomised controlled trials (RCTs). We obtained unpublished, ongoing trials and grey literature via correspondence with experts in the field and from pharmaceutical companies.
Selection criteria
RCTs of systemic antifungal therapy in children with normal immunity under the age of 18 with tinea capitis confirmed by microscopy, growth of fungi (dermatophytes) in culture or both.
Data collection and analysis
We used standard methodological procedures expected by Cochrane.
Main results
We included 25 studies (N = 4449); 4 studies (N = 2637) were new to this update.
Terbinafine for four weeks and griseofulvin for eight weeks showed similar efficacy for the primary outcome of complete (i.e. clinical and mycological) cure in three studies involving 328 participants with Trichophyton species infections (84.2% versus 79.0%; risk ratio (RR) 1.06, 95% confidence interval (CI) 0.98 to 1.15; low quality evidence).
Complete cure with itraconazole (two to six weeks) and griseofulvin (six weeks) was similar in two studies (83.6% versus 91.0%; RR 0.92, 95% CI 0.81 to 1.05; N = 134; very low quality evidence). In two studies, there was no difference between itraconazole and terbinafine for two to three weeks treatment (73.8% versus 78.8%; RR 0.93, 95% CI 0.72 to 1.19; N = 160; low quality evidence). In three studies, there was a similar proportion achieving complete cured with two to four weeks of fluconazole or six weeks of griseofulvin (41.4% versus 52.7%; RR 0.92, 95% CI 0.81 to 1.05; N = 615; moderate quality evidence). Current evidence for ketoconazole versus griseofulvin was limited. One study favoured griseofulvin (12 weeks) because ketoconazole (12 weeks) appeared less effective for complete cure (RR 0.76, 95% CI 0.62 to 0.94; low quality evidence). However, their effects appeared to be similar when the treatment lasted 26 weeks (RR 0.95, 95% CI 0.83 to 1.07; low quality evidence). Another study indicated that complete cure was similar for ketoconazole (12 weeks) and griseofulvin (12 weeks) (RR 0.89, 95% CI 0.57 to 1.39; low quality evidence). For one trial, there was no significant difference for complete cure between fluconazole (for two to three weeks) and terbinafine (for two to three weeks) (82.0% versus 94.0%; RR 0.87, 95% CI 0.75 to 1.01; N = 100; low quality evidence). For complete cure, we did not find a significant difference between fluconazole (for two to three weeks) and itraconazole (for two to three weeks) (82.0% versus 82.0%; RR 1.00, 95% CI 0.83 to 1.20; low quality evidence).
This update provides new data: in children with Microsporum infections, a meta‐analysis of two studies found that the complete cure was lower for terbinafine (6 weeks) than for griseofulvin (6‐12 weeks) (34.7% versus 50.9%; RR 0.68, 95% CI 0.53 to 0.86; N = 334; moderate quality evidence). In the original review, there was no significant difference in complete cure between terbinafine (four weeks) and griseofulvin (eight weeks) in children with Microsporum infections in one small study (27.2% versus 60.0%; RR 0.45, 95% CI 0.15 to 1.35; N = 21; low quality evidence).
One study provides new evidence that terbinafine and griseofulvin for six weeks show similar efficacy (49.5% versus 37.8%; RR 1.18, 95% CI 0.74 to 1.88; N = 1006; low quality evidence). However, in children infected with T. tonsurans, terbinafine was better than griseofulvin (52.1% versus 35.4%; RR 1.47, 95% CI 1.22 to 1.77; moderate quality evidence). For children infected with T. violaceum, these two regimens have similar effects (41.3% versus 45.1%; RR 0.91, 95% CI 0.68 to 1.24; low quality evidence). Additionally, three weeks of fluconazole was similar to six weeks of fluconazole in one study in 491 participants infected with T. tonsurans and M. canis (30.2% versus 34.1%; RR 0.88, 95% CI 0.68 to 1.14; low quality evidence).
The frequency of adverse events attributed to the study drugs was similar for terbinafine and griseofulvin (9.2% versus 8.3%; RR 1.11, 95% CI 0.79 to 1.57; moderate quality evidence), and severe adverse events were rare (0.6% versus 0.6%; RR 0.97, 95% CI 0.24 to 3.88; moderate quality evidence). Adverse events for terbinafine, griseofulvin, itraconazole, ketoconazole, and fluconazole were all mild and reversible.
All of the included studies were at either high or unclear risk of bias in at least one domain. Using GRADE to rate the overall quality of the evidence, lower quality evidence resulted in lower confidence in the estimate of effect.
Authors' conclusions
Newer treatments including terbinafine, itraconazole and fluconazole are at least similar to griseofulvin in children with tinea capitis caused by Trichophyton species. Limited evidence suggests that terbinafine, itraconazole and fluconazole have similar effects, whereas ketoconazole may be less effective than griseofulvin in children infected with Trichophyton. With some interventions the proportion achieving complete clinical cure was in excess of 90% (e.g. one study of terbinafine or griseofulvin for Trichophyton infections), but in many of the comparisons tested, the proportion cured was much lower.
New evidence from this update suggests that terbinafine is more effective than griseofulvin in children with T. tonsurans infection.
However, in children with Microsporum infections, new evidence suggests that the effect of griseofulvin is better than terbinafine. We did not find any evidence to support a difference in terms of adherence between four weeks of terbinafine versus eight weeks of griseofulvin. Not all treatments for tinea capitis are available in paediatric formulations but all have reasonable safety profiles.
PICOs
Laienverständliche Zusammenfassung
Antimykotische Medikamente für die Behandlung von Kindern mit Scherpilzflechte
Hintergrund
Tinea capitis oder Scherpilzflechte ist eine Pilzerkrankung der Kopfhaut, die hauptsächlich von den zwei Pilzgattungen Trichophyton und Microsporum hervorgerufen wird. Sie kommt häufig bei Kindern vor. Die meisten Pilzerkrankungen lassen sich mit antimykotischen Cremes (Antipilzmittel) behandeln, die auf die Haut aufgetragen werden (Lokaltherapie). Da die Pilzerkrankung jedoch an den Wurzeln der Haarbälge auftritt, die durch die Lokaltherapie nicht erreicht werden, muss Tinea capitis immer mit oral (d.h. durch den Mund) verabreichten Arzneimitteln behandelt werden, damit diese sich im ganzen Körper verteilen können (systemische Behandlung). Mehrere verschiedene Arten von antimykotischen Arzneimitteln stehen zur Verfügung.
Reviewfrage
Welches antimykotische Arzneimittel eignet sich am besten um Scherpilzflechte auf der Kopfhaut von Kindern zu behandeln?
Studienmerkmale
Im November 2015 suchten wir nach Studien zu oral verabreichten antimykotischen Arzneimitteln, die in ihrem Studiendesign dem Goldstandard für klinische Studien (randomisierte kontrollierte Studien) entsprachen. Wir fanden 25 Studien an denen 4.449 Kinder unter 18 Jahren teilgenommen hatten (4 Studien mit 2.637 Kindern gingen neu in die vorliegende Aktualisierung mit ein).
Hauptergebnisse
Hinsichtlich einer vollständigen Genesung (sowohl der Infektion (Mykose) als auch der sichtbaren Schäden auf der Kopfhaut) weist Evidenz niedriger und moderater Qualität darauf hin, dass neuere Arzneimittel wie Terbinafin, Itraconazol und Fluconazol mindestens so gut für die Behandlung von Kindern mit Tinea capitis, die durch eine Trichophyton ‐Infektion verursacht wurde, geeignet sind wie das herkömmliche Arzneimittel Griseofluvin. Neue Evidenz in dieser Aktualisierung deutet jedoch darauf hin, dass Terbinafin besser für eine vollständige Genesung von Kindern mit Trichophyton tonsurans ‐Infektion geeignet ist, als Griseofulvin. Im Gegensatz scheint neue Evidenz zu zeigen, dass bei Kindern mit Microsporum ‐Infektion Griseofulvin wirksamer ist als Terbinafin.
Terbinafin, Itraconazol und Fluconazol haben anscheinend eine ähnliche Wirkung was den Anteil an Studienteilnehmern betrifft, die vollständig geheilt wurden. Ketoconazol dagegen ist anscheinend weniger wirksam bei Kindern mit Tinea capitis die durch Trichophyton ‐Arten hervorgerufen wurde, als Griseofulvin. Die Qualität dieser Evidenz ist jedoch niedrig. Bei einigen Interventionen lag der Anteil an vollständigen klinischen Genesungen über 90% (z.B. eine Studie über Terbinafin im Vergleich zu Griseofulvin gegen Trichophyton ‐Infektionen). Allerdings lag in vielen der durchgeführten Vergleiche der Anteil an Geheilten weit niedriger.
Die eingeschlossenen Studien berichteten von unerwünschten Nebenwirkungen, die für Terbinafin, Griseofulvin, Itraconazol, Ketoconazol und Fluconazol gleichermaßen mild und umkehrbar waren. Sie beinhalteten Haut‐spezifische Nebenwirkungen wie Juckreiz sowie abdominale Beschwerden, Kopfschmerzen und Übelkeit.
Qualität der Evidenz
Die Qualität der Evidenz in diesem Review war im Allgemeinen niedrig bis moderat, weshalb weitere Forschung sich wahrscheinlich stark auf unser Vertrauen in diese Ergebnisse auswirken wird. Teilweise war die Evidenz sogar von sehr niedriger Qualität. Wir brauchen nach wie vor mehr und bessere Evidenz, die uns hilft die Alltagswirksamkeit und die unerwünschten Ereignisse der systemischen antimykotischen Arzneimittel gegen Tinea capitis bei Kindern zu verstehen.
Authors' conclusions
Summary of findings
| Terbinafine versus griseofulvin for children with tinea capitis | ||||||
| Patient or population: children with tinea capitis | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Griseofulvin | Terbinafine | |||||
| Proportion of participants with complete cure | 790 per 1000 | 837 per 1000 | RR 1.06 | 328 | ⊕⊕⊝⊝ | This outcome was for children infected with Trichophyton, terbinafine (2‐4 weeks) versus griseofulvin (6‐8 weeks); short treatment duration |
| Proportion of participants with complete cure | 378 per 1000 | 446 per 1000 | RR 1.18 | 1006 | ⊕⊕⊕⊝ | This outcome was for children infected with Trichophyton (T. tonsurans and T. violaceum) Terbinafine (6 weeks) versus griseofulvin (6 weeks) in Trichophyton infections; medium treatment duration |
| Proportion of participants with complete cure | 354 per 1000 | 521 per 1000 | RR 1.47 | 764 | ⊕⊕⊕⊝ | This outcome was for children infected with T. tonsurans Terbinafine (6 weeks) versus griseofulvin (6 weeks) in Trichophyton infections; medium treatment duration |
| Proportion of participants with complete cure | 451 per 1000 | 411 per 1000 | RR 0.91 | 242 | ⊕⊕⊝⊝ | This outcome was for children infected with T. violaceum Terbinafine (6 weeks) versus griseofulvin (6 weeks) in Trichophyton infections; medium treatment duration |
| Proportion of participants with complete cure | 509 per 1000 | 346 per 1000 | RR 0.68 | 334 | ⊕⊕⊕⊝ | This outcome was for children infected with Microsporum. Terbinafine medium‐ (6 to 8 weeks) and long‐term (10 to 12 weeks) treatment versus griseofulvin |
| Proportion of participants with complete cure | 600 per 1000 | 270 per 1000 (90 to 810) | RR 0.45 (0.15 to 1.35) | 21 (1 study) | ⊕⊝⊝⊝ | This outcome was for children infected with Microsporum. Terbinafine short‐term (4 weeks) versus griseofulvin |
| Adverse events attributed to the study drugs | 83 per 1000 | 92 per 1000 | RR 1.11 | 1549 | ⊕⊕⊕⊝ | This outcome was for children infected with Trichophyton and Microsporum Terbinafine (6 weeks) versus griseofulvin (6 weeks), medium treatment duration |
| Severe adverse events | 6 per 1000 | 6 per 1000 | RR 0.97 | 1549 | ⊕⊕⊕⊝ | This outcome was for children infected with Trichophyton and Microsporum Terbinafine (6 weeks) versus griseofulvin (6 weeks), medium treatment duration |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aDowngraded one level because 1 of the 3 studies was at high risk of bias, the other two studies were at unclear risk of bias. | ||||||
| Itraconazole versus griseofulvin for children infected with Trichophyton and Microsporum | |||||
| Patient or population: children infected with Trichophyton and Microsporum | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Griseofulvin | Itraconazole | ||||
| Proportion of participants with complete cure | 910 per 1000 | 838 per 1000 | RR 0.92 | 134 | ⊕⊝⊝⊝ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| aDowngraded one level because both studies were at unclear risk of bias. | |||||
| Itraconazole versus terbinafine in children infected with Trichophyton | |||||
| Patient or population: children infected with Trichophyton | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Terbinafine | Itraconazole | ||||
| Proportion of participants with complete cure | 788 per 1000 | 732 per 1000 | RR 0.93 | 160 | ⊕⊕⊝⊝ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| aDowngraded one level because both studies were at unclear risk to bias. | |||||
| Ketoconazole versus griseofulvin in children infected with Trichophyton | ||||||
| Patient or population: children infected with Trichophyton | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Griseofulvin | Ketoconazole | |||||
| Proportion of participants with complete cure Follow‐up: 12 weeks | 964 per 1000 | 733 per 1000 (598 to 906) | RR 0.76 (0.62 to 0.94) | 62 | ⊕⊕⊝⊝ | Ketoconazole (12 weeks) versus griseofulvin (12 weeks) |
| Proportion of participants with complete cure Follow‐up: 26 weeks | 1000 per 1000 | 920 per 1000 (810 to 1000) | RR 0.92 (0.81 to 1.03) | 62 (1 study) | ⊕⊕⊝⊝ | Ketoconazole (up to 26 weeks) versus griseofulvin (up to 26 weeks) |
| Proportion of participants with complete cure Follow‐up: 12 weeks | 543 per 1000 | 484 per 1000 (310 to 755) | RR 0.89 (0.57 to 1.39) | 79 (1 study) | ⊕⊕⊝⊝ | Ketoconazole (12 weeks) versus griseofulvin (12 weeks) |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aDowngraded one level because the study was at high risk of bias. | ||||||
| Fluconazole versus griseofulvin in children with tinea capitis | |||||
| Patient or population: children with tinea capitis | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Griseofulvin | Fluconazole | ||||
| Proportion of participants with complete cure | 449 per 1000 | 413 per 1000 | RR 0.92 | 615 | ⊕⊕⊕⊝ |
| Proportion of participants with complete cure | 322 per 1000 | 341 per 1000 | RR 1.06 | 361 | ⊕⊕⊝⊝ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| aDowngraded one level because one of the three studies was at high risk of bias, the other two were at unclear risk of bias. | |||||
| Fluconazole versus terbinafine for children infected with Trichophyton | |||||
| Patient or population: children infected with Trichophyton | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Terbinafine | Fluconazole | ||||
| The proportion of participants with complete cure | 940 per 1000 | 818 per 1000 | RR 0.87 | 100 | ⊕⊕⊝⊝ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| a Downgraded one level because the study was at unclear risk of bias. | |||||
| Fluconazole versus itraconazole in children infected with Trichophyton | |||||
| Patient or population: children infected with Trichophyton | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Itraconazole | Fluconazole | ||||
| Proportion of participants with complete cure Follow‐up:12 weeks | 820 per 1000 | 820 per 1000 | RR 1.00 | 100 | ⊕⊕⊝⊝ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| a Downgraded one level because the study was at unclear risk of bias. | |||||
| Different durations of fluconazole in children infected with T. tonsurans and M. canis | |||||
| Patient or population: children infected with T. tonsurans and M. canis Comparison: fluconazole (6 weeks duration) | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Fluconazole ( 6 weeks duration) | Fluconazole ( 3 weeks duration) | ||||
| Proportion of participants with complete cure Follow‐up: 8‐12 weeks | 341 per 1000 | 300 per 1000 | RR 0.88 | 491 | ⊕⊕⊝⊝ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| a Downgraded one level because the study was at unclear risk of bias. | |||||
Background
This is an updated version of an original Cochrane review (Gonzalez 2007).
Description of the condition
Tinea capitis is the medical term for an infection of the scalp (also known as scalp ringworm) involving the skin and the hair (Higgins 2000). It is caused by fungi (dermatophytes), mainly by Trichophyton or Microsporum species that invade the hair shaft (Higgins 2000). The clinical hallmark is one or more patches of hair loss, sometimes with a black dot pattern (studded with broken‐off hairs), which may be accompanied by inflammation, scaling, pustules and itching (Chan 2004; Higgins 2000).
Tinea capitis is uncommon in adults and is mostly seen in preteen children from disadvantaged communities in countries of all income levels (Chan 2004; Ginter‐Hanselmayer 2007). Over the past 30 years, the reported incidence of tinea capitis has increased significantly, as travel and migration have been associated with changes in epidemiology and in distribution of the species of fungi that are likely to cause tinea capitis (Aly 1999).
There are several species of dermatophytes characteristically associated with tinea capitis. Trichophyton infections are most common in Central America, the United States and in parts of Western Europe. Cases of Microsporum infections are mainly seen in South America, Southern and Central Europe, Africa and the Middle East (Havlickova 2008).
Tinea capitis is contagious and can be transmitted by humans, animals or objects carrying the fungus (Yu 2005). Carrier states also exist where the fungus is present on the scalp but there is no clinical infection (Pomeranz 1999). Although it is not life‐threatening in people with normal immunity, if left untreated there may be persistent symptoms (Elewski 2000). The inflammatory form, kerion, can result in scarring alopaecia (hair loss), or permanent baldness (Elewski 2000).
Physicians should confirm the clinical diagnosis by identifying the presence of fungi within the hair shaft in hair samples viewed under the microscope, by growing the fungus from such samples in laboratory conditions (mycological diagnosis) or both (Higgins 2000). The main methods of collecting samples for microbiological diagnosis involve either scraping or brushing the scalp and plucking the affected hairs (Fuller 2003). Looking at the sample under a microscope is the fastest way to diagnose the infection, and if the result is positive, treatment can commence immediately (Fuller 2003). However, sometimes this method indicates someone does not have the condition even if they actually do. Culturing the scrapings is more sensitive and allows accurate identification of the organism involved; however, this method may take up to four weeks to provide a result (Fuller 2003; Gupta 1999). A Wood's light (filtered ultraviolet light) can be used to detect infections that fluoresce under this type of light such as M. canis and M. audouinii, but it is not helpful in diagnosing T. tonsurans tinea capitis (Elewski 2000).
Description of the intervention
The primary aim of treatment for tinea capitis is to achieve complete clinical (signs and symptoms) and mycological cure (culture negative) as quickly as possible with minimal adverse events. Most superficial fungal infections can be treated topically (treatment applied directly to the skin), but tinea capitis always requires systemic medication (which spreads throughout the entire body) because the fungal infection is found at the root of the hair follicles, where topical agents cannot reach (Higgins 2000). Topical medications are only used as adjuvant therapy alongside systemic treatments (Higgins 2000).
Tinea capitis mainly occurs in children, and there are potential problems with persuading them to take their medicine (Hay 2006). Factors enhancing adherence include an acceptable taste and a short course of therapy. The latter factor may be important in reducing the risk of adverse events.
Griseofulvin has traditionally been the most widely prescribed and commonly used antifungal treatment for tinea capitis in clinical practice (Bennett 2000; Friedlander 2000). The paediatric dosage of griseofulvin is 10 to 25 mg/kg/d for six to eight weeks (Blumer 1999). It is still a relatively inexpensive drug and has been used as the standard to evaluate many newer agents (Blumer 1999). However, it has a bitter, unpleasant taste and should be taken with meals for one to two months, which may affect adherence in children (Bennett 2000). The liquid form is not always available.
Physicians increasingly consider treating tinea capitis with newer antifungal agents, such as ketoconazole, itraconazole, terbinafine or fluconazole (Friedlander 2000; Gonzalez 2007), but there is concern regarding the use of these drugs in children because of the possibility of rare but potentially serious side effects, such as liver toxicity or drug interaction (Blumer 1999). These newer agents are also expensive, which is an important consideration given that tinea capitis is endemic in some of the poorest communities in the world.
How the intervention might work
The main mechanism of action of griseofulvin is binding and inactivating the microtubular proteins that are essential for mitosis (cell division), thus arresting cell division of the fungal cell. Griseofulvin also inhibits nucleic acid synthesis and impairs synthesis of the fungal cell wall (Fuller 2014).
The mechanism of action of terbinafine involves inhibition of squalene epoxidase, which is a key enzyme in sterol biosynthesis in the fungal cell. This causes a deficiency in ergosterol within the fungal cell membrane, which results in damage to the fungi cell membrane (Abdel‐Rahman 2005).
The mechanism of action of the azole antifungals (e.g. itraconazole and fluconazole) is inhibition of the cytochrome P450‐dependent enzyme lanosterol 14‐alpha‐demethylase, which is essential for the conversion of lanosterol to ergosterol. Disruptions in the synthesis of ergosterol lead to damage in the cell membrane of fungi and damage to the fungal cell (Zonios 2008).
Why it is important to do this review
There is a choice between several systemic antifungal drugs for treating children with tinea capitis.
We wish to determine the comparative efficacy and safety profiles for these drugs. Furthermore, because of the worldwide distribution of this infection and the responsiveness of fungal species to different drugs, the cost implications may also be very important. We are also interested in comparing different lengths of treatment, because shorter courses of treatment, if effective, would be preferable to prolonged therapy, which may increase the risk of adverse events and the likelihood of non‐adherence.
Objectives
To assess the effects of systemic antifungal drugs for tinea capitis in children.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs).
Types of participants
Children with normal immunity under the age of 18 years with tinea capitis confirmed by microscopy, growth of dermatophytes in culture or both.
Types of interventions
We considered studies of all regimens of any systemic antifungal drug interventions for tinea capitis using the following comparisons.
-
Any systemic treatment versus no treatment or placebo.
-
Comparison of two or more systemic therapies.
-
Comparison of different doses and regimens of the same systemic therapy.
-
Comparison of systemic versus topical therapies.
We anticipated that studies would not focus on some systemic antifungal agents, such as amphotericin B, flucytosine, caspofungin or miconazole, because of either a lack of antifungal spectrum of activity or a lack of acceptable toxicity in this population.
Types of outcome measures
Primary outcomes
-
The proportion of participants with complete cure, i.e., clinical and mycological cure. We defined complete clinical cure as resolution of itching and clinical signs, such as redness, scaling, and oedema. We defined complete mycological cure as negative results on microscopy, no growth in culture or both.
-
The frequency and type of adverse events.
Secondary outcomes
-
The proportion of participants with clinical cure only.
-
Measurement of recurrence of the condition after the end of the intervention period.
-
Percentage of drop‐outs as a surrogate for participant adherence.
-
The time taken to cure.
Search methods for identification of studies
We aimed to identify all relevant RCTs regardless of language or publication status (published, unpublished, in press, or in progress).
Electronic searches
For this update, we revised all our search strategies in line with current Skin Group practices. We searched the following databases up to 23rd November 2015:
-
The Cochrane Skin Group Specialised Register using the search strategy in Appendix 1.
-
The Cochrane Central Register of Controlled Trials (CENTRAL) 2015, Issue 10, in The Cochrane Library using the strategy in Appendix 2.
-
MEDLINE via Ovid (from 1946) using the strategy in Appendix 3.
-
EMBASE via Ovid (from 1974) using the strategy in Appendix 4.
-
LILACS (Latin American and Caribbean Health Science Information database, from 1982) using the strategy in Appendix 5.
-
CINAHL via EBSCO (Cumulative Index to Nursing and Allied Health Literature, from 1981) using the strategy in Appendix 6.
Trial registers
We searched the following trial registers up to 30th November 2015 using the strategy in Appendix 7.
-
The ISRCTN registry (www.controlled‐trials.com).
-
The US National Institutes of Health Ongoing Trials Register (www.clinicaltrials.gov).
-
The Australian New Zealand Clinical Trials Registry (www.anzctr.org.au).
-
The World Health Organization International Clinical Trials Registry platform (www.who.int/trialsearch).
-
The EU Clinical Trials Register (https://www.clinicaltrialsregister.eu/).
Searching other resources
References from included studies
We handsearched the bibliographies of included and excluded studies for further references to relevant trials.
Unpublished literature
We sought information on unpublished and ongoing trials as well as grey literature via correspondence with authors of published studies and pharmaceutical companies. We consulted the Ringworm Committee of the European Confederation of Medical Mycology with regard to unpublished data.
Conference proceedings
We stated in the protocol that we would search the conference proceedings from major dermatology and mycology meetings. We were unable to search proceedings from mycology meetings, and we understand that the Cochrane Skin Group is searching some of the major dermatology meetings. We will search mycology meeting abstracts for an update of this review.
Adverse events
We asked pharmaceutical companies for surveillance data on adverse events.
Data collection and analysis
Some parts of the 'Methods' section of this review use text that was originally published in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We included 'Summary of findings' tables in our review to summarise the primary outcomes and assessed the quality of the body of evidence using the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias).
Selection of studies
For the original review, two authors (GB and UG) checked titles and abstracts identified from the searches. If study design was not clear from the abstract, then two authors (GB and UG) independently reviewed the full text of the study. The authors also decided which trials met the inclusion criteria and resolved any disagreement by discussion between the authors or referred to a third author (JT) when necessary. We listed the excluded studies and reasons for exclusion in the 'Characteristics of excluded studies' tables.
In this update, two authors (XC and MY) independently selected the studies using the same methods as before. We resolved discrepancies between XC and MY through discussion with XH.
Data extraction and management
For the previously published version of the review, at least two authors (TS and UG) extracted data independently using a pre‐designed data extraction form. We extracted reported data for cure rates for all evaluated drugs, paying particular attention to the doses and frequencies of treatment administration (including 'pulsed' regimens: administering the drug in waves with drug‐free intervals). We used the extracted data to populate the Characteristics of included studies table. We resolved disagreements by discussion, and we attempted to obtain missing information from authors whenever possible.
In this update, two authors (XC and MY) independently extracted the information from the newly included studies, and another author (MZ) checked and compared the data extraction forms.
Assessment of risk of bias in included studies
Two authors (MY and XC) independently assessed the quality of included studies according to the methods recommended in Sections 8.9 to 8.15 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We resolved discrepancies between MY and XC by consulting another author (MZ).
In addition, we considered the following factors in order to address other potential biases: reporting of sample size calculation, definition of inclusion and exclusion criteria, reporting of type of fungi involved, baseline comparability and statement of funding resources.
-
Low risk of bias: study appears to be free of other sources of bias.
-
High risk of bias: had extreme baseline imbalance; has been claimed to have been fraudulent.
-
Unclear risk of bias: insufficient information to permit judgement of 'high' or 'low'; had some drawbacks in either of the items listed above except for extreme baseline imbalance.
Measures of treatment effect
We expressed dichotomous data, such as proportion of participants achieving complete cure, as risk ratios (RR). We analysed these in Review Manager (RevMan) using the Mantel‐Haenszel test, unless stated otherwise (Revman 2014). We reported all outcomes with 95% confidence intervals (CIs) if possible.
We reported data that could not be combined by meta‐analyses narratively. We expressed the time taken to cure as a mean.
Unit of analysis issues
We did not consider internally controlled trials, such as those with cross‐over and within‐participant designs, because even with a washout period, they are inappropriate designs for systemic treatment (because effects of antifungal therapy may endure over the washout period, as most participants would experience a cure or at least some improvement in the first period of a cross‐over study).
For RCTs with multiple intervention groups, we combined groups to a single pair‐wise comparison or split the shared group into two or more groups and included two or more independent comparisons, as recommended by Cochrane (Higgins 2011).
Dealing with missing data
We contacted the trial authors of Elewski 2008 and Foster 2005 by email on 9 January 2015 to ask for for missing data; however, we did not receive any response. For the previous version of the review, we sent an email (when an email address was available) to authors of published studies asking for unpublished, ongoing trials and grey literature. We also consulted the Ringworm Committee of the European Confederation of Medical Mycology about unpublished data. We did not receive any positive response.
Assessment of heterogeneity
We assessed statistical heterogeneity in the analyses results by inspecting the forest plots to detect non‐overlapping CIs, and by implementing the I2 statistic (with a value of at least 50% being interpreted as moderate to high levels of heterogeneity (Higgins 2011).
Assessment of reporting biases
We planned to perform funnel plots for publication bias if 10 or more studies contributed data. However, we could not carry this out because of the small number of included studies for each outcome.
Data synthesis
We used Revman 2014 to combine some outcomes. To estimate differences between treatments, we pooled trials that evaluated similar interventions using meta‐analysis based on a random‐effects model (Mantel‐Haenszel method), if possible, to calculate a weighted treatment effect across trials.
For each trial, we calculated complete cure at follow‐up based on the reported mycological and clinical results. Although we failed to specify the acceptable window for the timing in the primary outcome assessment in the original protocol, we decided during the course of the review to combine studies that recorded primary outcomes at 12 to 20 weeks on the basis that these are the range of time periods that best reflect clinical decision‐making in practice.
When necessary, we categorised the duration of treatment into three groups.
-
Short term (closest to 2 weeks, but between 1 and 4 weeks).
-
Medium term (closest to 6 weeks, but between 5 and 8 weeks).
-
Long term (closest to 12 weeks, but between 9 and 14 weeks).
Subgroup analysis and investigation of heterogeneity
In the original protocol we planned to perform subgroup analyses where adequate information was given for severity of infection, geographical setting of the trial, and dermatophyte species, whose variation may play an important role in the response to treatment. To explore reasons for heterogeneity in the review, we performed subgroup analyses where the trial report gave adequate information, based on dermatophyte species variation and duration of treatment.
Sensitivity analysis
In the original protocol we planned to exclude some studies or subgroups in sensitivity analyses, but we did not perform any sensitivity analyses in this review.
Results
Description of studies
Results of the search
The electronic database searches for this update yielded 85 studies after duplicates were removed. We discarded 79 studies after screening titles and abstract and examined the full text of the remaining 6 records. We excluded two further studies (Koumantaki‐Mathioudaki 2005; Shemer 2013; see 'Characteristics of excluded studies'), and we identified four new studies for inclusion in this update (Deng 2011; Elewski 2008; Foster 2005; Khan 2011; see 'Characteristics of included studies'). We did not identify any other studies in our searches of ongoing trial registers or from other resources.
The original review identified 21 trials of systemic treatments for tinea capitis (Gonzalez 2007).
Please see Figure 1 for the study flow diagram.
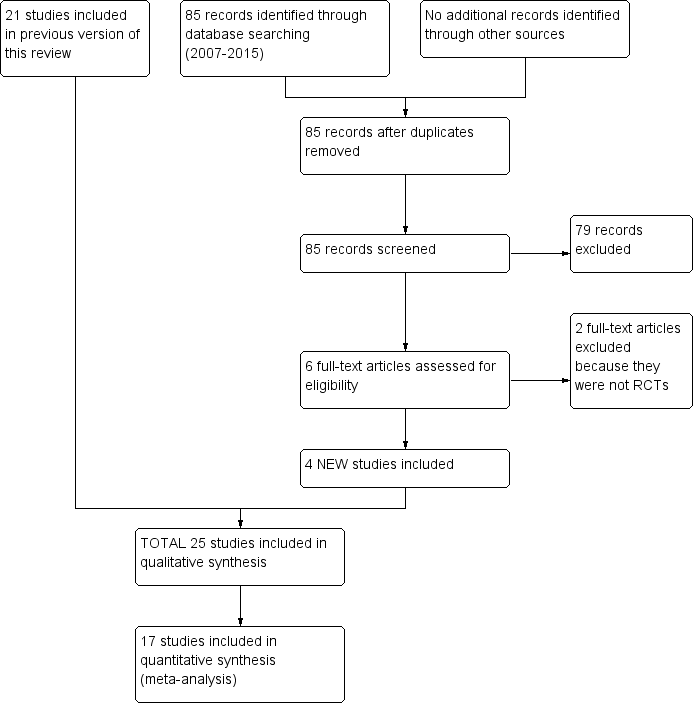
Study flow diagram.
Included studies
In total, we included 25 studies that randomised 4449 participants (Characteristics of included studies). We found no other trials that compared an active treatment to placebo. The trials compared different active treatments: either different drugs or different regimens of the same drug.
Design
All included studies were parallel group RCTs. Ten of them had a multi‐arm design (Deng 2011; Foster 2005; Friedlander 2002; Gupta 2001; Haroon 1996; Kullavanijaya 1997; Lipozencic 2002; Memisoglu 1999; Solomon 1997; Talarico Filho 1998).
Sample size
Only six studies reported a sample size calculation (Elewski 2008; Foster 2005; Fuller 2001, Khan 2011; Lipozencic 2002; Ungpakorn 2004).
Regarding the sample size, we organised the studies into three distinct groups.
-
Nine studies were small (N < 50) (Cáceres‐Ríos 2000; Dastghaib 2005; Hamm 1999; López‐Gómez 1994; Martínez‐Roig 1988; Rademaker 1998; Solomon 1997; Tanz 1985; Ungpakorn 2004).
-
Eight studies were medium (N = 51 to 150) (Deng 2011; Gan 1987; Jahangir 1998; Khan 2011; Kullavanijaya 1997; Memisoglu 1999; Talarico Filho 1998; Tanz 1988).
-
Eight studies were large (N > 150) (Elewski 2008; Foster 2005; Friedlander 2002; Fuller 2001; Gupta 2001; Haroon 1995; Haroon 1996; Lipozencic 2002).
Settings
The studies included in this review took place in many parts of the world.
Eight took place in Asia: four in Pakistan (Haroon 1995; Haroon 1996; Jahangir 1998; Khan 2011); two in Thailand (Kullavanijaya 1997; Ungpakorn 2004); one in China (Deng 2011); and one in Iran (Dastghaib 2005).
Five studies were carried out in Europe: one in Germany (Hamm 1999); one in Turkey (Memisoglu 1999); two in Spain (López‐Gómez 1994; Martínez‐Roig 1988); and one in the UK (Fuller 2001).
Two studies were from South America (Cáceres‐Ríos 2000; Talarico Filho 1998), five were completed in North America (Friedlander 2002; Gan 1987; Solomon 1997; Tanz 1985; Tanz 1988), and one study took place in New Zealand (Rademaker 1998).
Four of the studies were conducted in several locations: Gupta 2001 took place in the United States and South Africa; Lipozencic 2002, in Europe and South America; Elewski 2008 in the United States, Peru, the United Kingdom, Egypt, Russia and South Africa; and Foster 2005, in the United States, Guatemala, Chile, Costa Rica and India.
Participants
With regard to age, most of the participants of included studies were older than two years. Cáceres‐Ríos 2000 and Talarico Filho 1998 included participants as young as one year. Another study involved participants as young as six months of age (Gupta 2001). The upper age limit in the majority of the trials was 16 years, although Haroon 1995 included participants ranging in age from 2 to 65 years. In that trial, 94 of the 105 participants were under 12 years of age, so we assumed all the participants were under 16 years of age and therefore analysed the whole population. Three other studies reported a total of four adults in their samples (Kullavanijaya 1997; Lipozencic 2002; López‐Gómez 1994).
Fungal type
Each of the 25 studies reported the types of fungi cultured; some provided general percentages and reported exact proportions of the types of fungi within each arm. The Trichophyton species predominated over Microsporum species. T. tonsurans and M. canis were responsible for causing infection in the highest proportion of participants. T. tonsurans was the most commonly identified fungus in 11 studies (Cáceres‐Ríos 2000; Elewski 2008; Foster 2005; Friedlander 2002; Fuller 2001; Gan 1987; Ginsburg 1987; Khan 2011; Solomon 1997; Tanz 1985; Tanz 1988); T. violaceum was the predominant fungus in four studies (Deng 2011; Haroon 1995; Haroon 1996; Jahangir 1998); in one study, the proportions of M. canis and T. tonsurans were the same (Hamm 1999); and M. canis was the main fungus in five trials (Lipozencic 2002; López‐Gómez 1994; Memisoglu 1999; Rademaker 1998; Talarico Filho 1998). Three trials identified the causative fungi, but their relative frequencies were not provided so it was impossible to determine the frequencies: T. tonsurans and M. ferrugineum were identified in one study (Kullavanijaya 1997), T. tonsurans and T. violaceum in another (Gupta 2001), and T. mentagrophytes and M. canis in a third study (Martínez‐Roig 1988). In addition, one study failed to classify the causative species of fungi (Memisoglu 1999).
Interventions
The standard dose for griseofulvin used in trials is generally 10 to 20 mg/kg/d or 125 mg/d in participants weighing 10 to 20 kg; 250 mg/d in those weighing from 20 to 40 kg and 500 mg/d for those over 40 kg. Unless otherwise stated, the standard dosing for terbinafine studies was 62.5 mg/d in participants weighing from 10 to 20 kg; 125 mg/d from 20 to 40 kg, and 250 mg/d over 40 kg.
In total, we studied five different antifungal agents: griseofulvin, terbinafine, itraconazole, fluconazole and ketoconazole.
Comparisons
We evaluated a variety of regimens, including between‐drug and within‐drug comparisons. We considered griseofulvin to be the standard because it is the oldest agent, and 17 studies used it as a control. Of the 25 included studies, 17 compared griseofulvin as standard therapy with terbinafine (Cáceres‐Ríos 2000; Deng 2011; Elewski 2008; Fuller 2001; Gupta 2001; Haroon 1995; Khan 2011; Lipozencic 2002; Memisoglu 1999; Rademaker 1998), itraconazole (Gupta 2001; López‐Gómez 1994; Memisoglu 1999), ketoconazole (Gan 1987; Martínez‐Roig 1988; Tanz 1985; Tanz 1988), or fluconazole (Dastghaib 2005; Foster 2005; Gupta 2001; Memisoglu 1999). Gupta 2001 and Memisoglu 1999 compared griseofulvin, itraconazole and fluconazole.
Ten studies compared terbinafine versus griseofulvin (Cáceres‐Ríos 2000; Deng 2011; Elewski 2008; Fuller 2001; Gupta 2001;Haroon 1995; Khan 2011; Lipozencic 2002; Memisoglu 1999; Rademaker 1998), two versus itraconazole (Gupta 2001; Memisoglu 1999) and two versus fluconazole (Gupta 2001; Memisoglu 1999). Seven studies compared different treatment duration regimens for terbinafine (Deng 2011; Friedlander 2002; Hamm 1999; Haroon 1996; Kullavanijaya 1997; Lipozencic 2002; Talarico Filho 1998), and one compared different doses (Ungpakorn 2004).
Three studies (Gupta 2001; López‐Gómez 1994; Memisoglu 1999) compared itraconazole with other antifungals: three with griseofulvin (Gupta 2001; López‐Gómez 1994; Memisoglu 1999), two with terbinafine (Gupta 2001; Memisoglu 1999) and two with fluconazole (Gupta 2001; Memisoglu 1999). Ketoconazole was compared with griseofulvin in four trials (Gan 1987; Martínez‐Roig 1988; Tanz 1985; Tanz 1988).
Five trials studied fluconazole (Dastghaib 2005; Foster 2005; Gupta 2001; Memisoglu 1999; Solomon 1997); four with griseofulvin (Dastghaib 2005; Foster 2005; Gupta 2001; Memisoglu 1999), two with terbinafine (Gupta 2001; Memisoglu 1999), two with itraconazole (Gupta 2001; Memisoglu 1999), one by itself with varying doses (Solomon 1997), and one by itself with different durations of treatment (Foster 2005).
Outcomes
Primary outcomes
All but three studies reported the proportion of participants with complete cure, which was our pre‐specified primary outcome (Martínez‐Roig 1988; Rademaker 1998; Tanz 1985). Most of the studies reported complete cure at 12 to 16 weeks but three reported at 8 weeks (Dastghaib 2005; Deng 2011; Gan 1987), one at 10 weeks (Elewski 2008), one at 2 weeks, 4 weeks, 8 weeks and one year (Deng 2011), one at 3, 6 and 10 weeks (Foster 2005), one at 2, 4 and 6 weeks (Khan 2011), and two at 20 to 24 weeks (Fuller 2001; Ungpakorn 2004).
Three studies failed to report our other primary outcome: adverse events (Gan 1987; Kullavanijaya 1997; Solomon 1997).
Secondary outcomes
Fourteen studies reported the proportion of participants with clinical cure only, which was our first pre‐specified secondary outcome (Cáceres‐Ríos 2000; Elewski 2008; Friedlander 2002; Gupta 2001; Hamm 1999; Haroon 1996; Lipozencic 2002; López‐Gómez 1994; Martínez‐Roig 1988; Memisoglu 1999; Rademaker 1998; Solomon 1997; Talarico Filho 1998; Tanz 1988).
Only three studies reported recurrence of the condition after the end of the intervention period, which was our second pre‐specified secondary outcome (Martínez‐Roig 1988; Rademaker 1998; Solomon 1997).
Twelve studies reported the percentage of drop‐outs as a surrogate for participant adherence, our third pre‐specified secondary outcome (Deng 2011; Friedlander 2002; Fuller 2001; Gan 1987; Gupta 2001; Hamm 1999; Lipozencic 2002; López‐Gómez 1994; Memisoglu 1999; Talarico Filho 1998; Tanz 1985; Tanz 1988).
Four studies reported the time taken to cure, our fourth pre‐specified secondary outcome (Friedlander 2002; Gan 1987; Lipozencic 2002; Martínez‐Roig 1988).
Follow‐up
The follow‐up period ranged from six weeks in Martínez‐Roig 1988, Khan 2011 and Tanz 1985 to one year in Deng 2011. Although most studies had a 12‐week follow‐up period, five trials had longer follow‐up periods ranging from 16 to 24 weeks (Fuller 2001; Kullavanijaya 1997; Lipozencic 2002; Solomon 1997; Ungpakorn 2004). In addition, two trials had a 10‐week follow‐up period (Elewski 2008; Foster 2005).
Other
Some of the studies did not provide detailed information on the clinical setting or baseline characteristics of sex, age and infection severity, or they did not report the comparability between arms or the duration of symptoms or signs. Rademaker 1998 did not compare the baseline characteristics at all, and two trials did not report the information on comparability (Martínez‐Roig 1988; Solomon 1997). Finally, only five trials reported information about the severity of the infection (Cáceres‐Ríos 2000; Deng 2011; Elewski 2008; Gupta 2001; Tanz 1985). For the 25 studies, the most common reason for excluding a participant from the trial was treatment with any antifungal agent within one month prior to entering the trial.
Excluded studies
We provide details of the excluded studies in the 'Characteristics of excluded studies' table.
In this update, we excluded Koumantaki‐Mathioudaki 2005 and Shemer 2013 because we found that neither of them were RCTs after reading the full texts.
The original review excluded 3 of the initial 24 trials of systemic treatments for tinea capitis because they evaluated the therapy for the inflammatory component (kerion) caused by tinea capitis infection (Ginsburg 1987; Honig 1994; Hussain 1999).
Studies awaiting classification
One trial reported in a conference paper appeared to meet the inclusion criteria, but as we could not obtain further information, we could neither include or exclude it (Pather 2006). See Characteristics of studies awaiting classification.
Risk of bias in included studies
Please see Figure 2 for our judgements about each 'Risk of bias' item presented as percentages across all included studies and Figure 3 for the judgements about each domain for all the included studies.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Randomisation
All included studies stated or implied that treatment allocation was randomised; however, there were only four studies that reported an adequate generation method of randomisation: two used a computer‐generated random number table (Fuller 2001; Martínez‐Roig 1988), and two used a table of random numbers (Elewski 2008; Gan 1987).
Allocation concealment
Only two studies reported adequate allocation concealment (Elewski 2008; Foster 2005).
Blinding
Performance bias
Five included studies reported that participants or personnel were not blinded; therefore, we judged these studies to be at high risk of performance bias (Dastghaib 2005; Fuller 2001; Gan 1987; Rademaker 1998; Talarico Filho 1998).
We judged the other 20 studies as being at unclear risk of performance bias, either because they did not report blinding of participants or personnel (Hamm 1999; Haroon 1995; Jahangir 1998; Khan 2011), or because they did not describe the method of blinding (Deng 2011; Elewski 2008; Foster 2005; Friedlander 2002; Gupta 2001; Haroon 1995; Haroon 1996; Kullavanijaya 1997; Lipozencic 2002; López‐Gómez 1994; Martínez‐Roig 1988; Memisoglu 1999; Solomon 1997; Tanz 1985; Tanz 1988; Ungpakorn 2004).
Detection bias
Five included studies reported that outcome assessors were not blinded; therefore, we judged these studies to be at high risk of detection bias (Deng 2011; Fuller 2001; Gan 1987; Rademaker 1998; Talarico Filho 1998).
We deemed the other 20 studies to be at unclear risk of detection bias, either because they did not report blinding of outcome assessors (Cáceres‐Ríos 2000; Hamm 1999; Jahangir 1998; Khan 2011), or because they did not describe the method of blinding (Dastghaib 2005; Elewski 2008; Foster 2005; Friedlander 2002; Gupta 2001; Haroon 1995; Haroon 1996; Kullavanijaya 1997; Lipozencic 2002; López‐Gómez 1994; Martínez‐Roig 1988; Memisoglu 1999; Solomon 1997; Tanz 1985; Tanz 1988; Ungpakorn 2004).
Incomplete outcome data
Overall, after randomising 4449 people, 471 participants (10.6%) were lost. Only six studies performed intention‐to‐treat (ITT) analyses (Elewski 2008; Foster 2005; Friedlander 2002; Fuller 2001; Lipozencic 2002; Talarico Filho 1998).
We considered 14 studies to be at low risk of attrition bias because either less than 10% of participants dropped out, or because the drop‐outs were between 10% and 20% but balanced in numbers across intervention groups (Cáceres‐Ríos 2000; Elewski 2008; Foster 2005; Gupta 2001; Hamm 1999; Haroon 1995; Haroon 1996; Jahangir 1998; Khan 2011; Kullavanijaya 1997; López‐Gómez 1994; Martínez‐Roig 1988; Talarico Filho 1998; Ungpakorn 2004).
We judged 10 studies to be at high risk of attrition bias because either more than 20% of participants dropped out, whether ITT analysis was performed or not (Friedlander 2002; Fuller 2001; Gan 1987; Lipozencic 2002; Solomon 1997; Tanz 1985; Tanz 1988), or the drop‐outs were between 10% and 20% but ITT analysis was not performed (Dastghaib 2005; Deng 2011; Memisoglu 1999).
Rademaker 1998 was at unclear risk of attrition bias, as it did not provide sufficient information on drop‐outs to make a judgement.
Selective reporting
All included studies reported findings on all outcomes listed in the 'Methods' section; therefore, we judged all included studies as being at low risk of reporting bias. However, we did not have access to the original study protocols in any of the included studies.
Other potential sources of bias
Ninteen of the 25 included studies did not report the method of sample size calculation (Cáceres‐Ríos 2000; Dastghaib 2005; Deng 2011; Friedlander 2002; Gan 1987; Gupta 2001; Hamm 1999; Haroon 1995; Haroon 1996; Jahangir 1998; Kullavanijaya 1997; López‐Gómez 1994; Martínez‐Roig 1988; Memisoglu 1999; Rademaker 1998; Solomon 1997; Talarico Filho 1998; Tanz 1985; Tanz 1988).
Nine studies did not report the funding sources (Dastghaib 2005; Friedlander 2002; Gan 1987; Gupta 2001; Jahangir 1998; Khan 2011; Memisoglu 1999; Rademaker 1998; Solomon 1997).
Three studies did not report their inclusion or exclusion criteria (Hamm 1999; Kullavanijaya 1997; Rademaker 1998); two other studies did not report baseline comparability (Khan 2011; Tanz 1988). However, whether these factors introduced bias to the results remained unclear. We therefore judged these studies as being at unclear risk of other bias.
In addition, all but two of the included studies reported the proportion of different types of fungi (Kullavanijaya 1997; Martínez‐Roig 1988). Most included studies recruited children infected with both Trichophyton and Microsporum.Lipozencic 2002 and Ungpakorn 2004 only recruited children infected with Microsporum, while Friedlander 2002, Gupta 2001, Jahangir 1998 and Solomon 1997 only recruited children infected with Trichophyton.Tanz 1985 recruited children infected with Trichophyton,Scopulariopsis,Penicillium and unidentified fungus. We list the details of type of fungi in each study in the 'Characteristics of included studies' tables.
Effects of interventions
See: Summary of findings for the main comparison Complete cure and adverse events for terbinafine versus griseofulvin in children with tinea capitis; Summary of findings 2 Complete cure for itraconazole versus griseofulvin in children infected with Trichophyton and Microsporum ; Summary of findings 3 Complete cure for itraconazole versus terbinafine in children infected with Trichophyton ; Summary of findings 4 Complete cure for ketoconazole versus griseofulvin in children infected with Trichophyton ; Summary of findings 5 Complete cure for fluconazole versus griseofulvin in children with tinea capitis; Summary of findings 6 Complete cure for fluconazole versus terbinafine in children infected with Trichophyton ; Summary of findings 7 Complete cure for fluconazole versus itraconazole in children infected with Trichophyton ; Summary of findings 8 Complete cure for different durations of fluconazole in children infected with T. tonsurans and M. canis
Numbers given show the total numbers of participants included in the analysis. When it was possible to calculate an effect size, we reported this with the 95% confidence interval (CI). We used the P value of 0.05 as the cutoff value to determine statistical significance; when P values were below this threshold, we stated whether the result favoured the intervention group or the control condition. In the text below, we report an I² statistical value for heterogeneity as moderate or high if it exceeds 50%.
We have presented the results for our pre‐specified outcomes below under the following 13 comparisons.
-
Terbinafine versus griseofulvin (short treatment duration).
-
Terbinafine versus griseofulvin in Trichophyton infections (medium treatment duration).
-
Terbinafine (medium‐ and long‐term treatment) versus griseofulvin in Microsporum infections.
-
Terbinafine short‐ versus long‐term.
-
Terbinafine standard dose compared to terbinafine double dose.
-
Itraconazole versus griseofulvin.
-
Itraconazole versus terbinafine.
-
Ketoconazole versus griseofulvin.
-
Fluconazole versus griseofulvin.
-
Fluconazole versus terbinafine.
-
Fluconazole versus itraconazole.
-
Fluconazole dosages (1.5, 3.0 and 6.0 mg/kg/d).
-
Treatment durations of fluconazole (short‐term versus medium‐term).
We have summarised the results of included studies that we could not combine in meta‐analyses because of differences between studies in terms of design. We present the results of studies that could not be pooled in meta‐analyses using data and information derived from the reports of individual studies.
We produced eight 'Summary of findings' tables for the first primary outcome of complete clinical cure (summary of findings Table for the main comparison; summary of findings Table 2; summary of findings Table 3; summary of findings Table 4; summary of findings Table 5; summary of findings Table 6; summary of findings Table 7; summary of findings Table 8). In summary of findings Table for the main comparison we also reported our primary outcome of adverse events.
1. Terbinafine (2 to 4 weeks) versus griseofulvin (6 to 8 weeks); short treatment duration; 6 to 24 weeks follow‐up
Eight studies assessed the efficacy of terbinafine used in the short‐term for 2 to 4 weeks as compared to griseofulvin (used for 8 weeks) (Cáceres‐Ríos 2000; Deng 2011; Fuller 2001; Gupta 2001; Haroon 1995; Khan 2011; Memisoglu 1999; Rademaker 1998).
Primary outcomes
Complete cure, i.e. clinical and mycological cure, at 12 to 24 weeks follow‐up
Five studies reported on complete cure (Cáceres‐Ríos 2000; Fuller 2001; Gupta 2001; Haroon 1995; Memisoglu 1999). This update did not identify any new studies addressing this outcome.
A pooled analysis of the five studies found that the difference in the proportion of participants with complete cure between four weeks of terbinafine and eight weeks of griseofulvin was not statistically significant (73.6% versus 68.4%; RR 1.08, 95% CI 0.94 to 1.24; Analysis 1.1).
Trichophyton infections
Three studies included participants with Trichophyton infections (Fuller 2001; Gupta 2001; Haroon 1995). Haroon 1995 compared terbinafine for 4 weeks with 10 mg/kg/d of griseofulvin for 8 weeks in 105 participants, of whom 87.6% had T. violaceum tinea capitis. The proportion of participants with complete cure at week 12 was 93% (52/56) in the terbinafine group and 80% (39/49) in the griseofulvin group (RR 1.17, 95% CI 0.99 to 1.37; Analysis 1.1).
Fuller 2001 recruited 210 participants and included 147 in the ITT analyses. Trichophyton infection accounted for 84.4% of the terbinafine group (N = 65) and 82.9% of the griseofulvin group (N = 58). At 24 weeks, the proportion of participants with complete cure was 69.2% (45/65) in the terbinafine group and 67.2% (39/58) in the griseofulvin group (RR 1.03, 95% 0.81 to 1.31; Analysis 1.1)
Gupta 2001 compared 50 participants in each treatment group with infections caused by T. tonsurans and T. violaceum. In this trial, administration of terbinafine for 2 to 3 weeks was compared with microsize griseofulvin 20 mg/kg for 6 weeks. The proportion of participants with complete cure at week 12 was 94% (47/50) for the terbinafine group and 92% (46/50) for the griseofulvin treated group (RR 1.02, 95% CI 0.92 to 1.14; Analysis 1.1).
In the pooled analysis of 328 participants with a confirmed Trichophyton infection, terbinafine for four weeks and griseofulvin for 8 weeks showed similar efficacy in three studies (84.2% versus 79.0%; RR 1.06 95% CI 0.98 to 1.15; low quality evidence; Analysis 1.1; Fuller 2001; Gupta 2001; Haroon 1995; summary of findings Table for the main comparison).
Microsporum infections
In Fuller 2001, the proportion of the 21 children with Microsporum infections who achieved complete cure in the terbinafine (for four weeks) group and the griseofulvin (for eight weeks) group were 27.2% (3/11) and 60.0% (6/10), respectively (RR 0.45, 95% CI 0.15 to 1.35; N = 21; low quality evidence; Analysis 1.1; summary of findings Table for the main comparison).
Mixed Trichophyton and Microsporum infections
Cáceres‐Ríos 2000 and Memisoglu 1999 included participants with Trichophyton and Microsporum infections but did not report results separately. In Memisoglu 1999, complete cure at the final follow‐up visit (week 12) was 39% (15/39) for the group treated with four weeks of terbinafine compared with 44% (17/39) in the group treated with eight weeks of ultra microsized griseofulvin (RR 0.88, 95% CI 0.52 to 1.50; Analysis 1.1). There was a similar proportion of participants with complete cure within the subgroups infected with M. canis (48% of participants) and Trichophyton species according to the principal investigators of that study. The other study, Cáceres‐Ríos 2000, evaluated terbinafine for four weeks versus microsized griseofulvin for 8 weeks in 50 participants from Peru and found a significant increase in complete cure with terbinafine (76%; 19/25) compared to griseofulvin (44%; 11/25) measured at 12 weeks (RR 1.73, 95% CI 1.05 to 2.83; Analysis 1.1). The causative organisms were T. tonsurans and M. canis, at 74% and 26%, respectively.
A pooled analysis of the two studies showed no significant difference between the groups (53.1% versus 43.8%; RR 1.24, 95% CI 0.64 to 2.42; Analysis 1.1).
Adverse events
Seven studies reported this outcome (Cáceres‐Ríos 2000; Deng 2011; Fuller 2001; Gupta 2001; Haroon 1995; Khan 2011; Memisoglu 1999), of which two were new studies added in this update (Deng 2011; Khan 2011).
Khan 2011 reported that the incidence of adverse events was comparable between the two groups, with none of participants showing serious side effects, except for nausea and mild abdominal discomfort. Deng 2011 reported one case of vomiting in the griseofulvin group and no side effects in the terbinafine group.
Drug‐related adverse events
In the open study (Fuller 2001), 36 participants in the terbinafine group reported 57 adverse events (pruritus, urticaria, skin scaling), and 4 participants withdrew from the study due to adverse events (vomiting, dizziness, urticaria and weight loss). A total of 52 adverse events, predominantly abdominal discomfort and vomiting, were detected in 27 participants in the griseofulvin group, and 1 participant withdrew from the study due to abdominal pain, headache and vomiting. There was no significant difference regarding adverse events that might be attributed to either of the study drugs in the terbinafine (26/77) or griseofulvin (17/70) group (33.8% versus 24.3%, RR 1.39, 95% CI 0.83 to 2.34; Analysis 1.2).
Some studies reported good tolerability for terbinafine because there were no or few adverse events, and these had either an uncertain or no relationship to the treatment (Cáceres‐Ríos 2000; Haroon 1995). Haroon 1995 reported tonsillitis, cutaneous infestations, raised hepatic enzymes, raised triglycerides and eosinophilia, and Memisoglu 1999 reported mild elevated triglycerides, with an uncertain relationship to the drug. The following adverse events were reported less commonly and may not have been caused by griseofulvin: skin infections, skin infestations, elevated hepatic enzymes, elevated serum triglycerides, elevated serum uric acid, anaemia, eosinophilia, leucocytosis and granulocytopenia (Haroon 1995; Memisoglu 1999). Gupta 2001 reported three gastric problems and three cases of nausea in the griseofulvin group. Griseofulvin was associated with a small number of adverse events in other trials.
Secondary outcomes
None of the included studies reported measurement of recurrence of the condition after the end of the intervention period or the time taken to cure.
Proportion of participants with clinical cure only
Three studies reported the proportion of patients achieving only a clinical cure (Deng 2011; Gupta 2001; Khan 2011); two were new studies added in this update (Deng 2011; Khan 2011). We did not pool the data from these studies because of significant clinical heterogeneity, especially due to the various fungal types in different studies.
Deng 2011 compared the effects of terbinafine for two weeks, terbinafine for four weeks, and griseofulvin for treating participants infected with T. violaceum (55.1%), A. vanbreuseghemi (30.6%) and T. tonsurans (14.3%). Investigators found that the clinical cure in week 8 was 85.2% (23/27) in the 2‐week terbinafine group and 84.2% (16/19) in the griseofulvin group (RR 1.01, 95% CI 0.79 to 1.30; Analysis 1.3). The corresponding rate was 78.3% (18/23) in the 4‐week terbinafine group and 84.2% (16/19) in the griseofulvin group (RR 0.93, 95% CI 0.70 to 1.24; Analysis 1.3). When the follow‐up was extended to one year, all participants in the three groups achieved clinical cure.
Gupta 2001 reported that the proportion of participants with clinical cure was determined at the end of treatment (week four for terbinafine and week six for griseofulvin) showing better results in the griseofulvin group (70%, 35/50) than in the terbinafine group (40%, 20/50) (RR 0.57, 95% CI 0.39 to 0.84; Analysis 1.3).
Khan 2011 compared the effects of terbinafine for four weeks and griseofulvin for treating patients infected with T. tonsurans (75%) and M. canis (22%). The proportion of participants with clinical cure only at week six seemed to be higher in the terbinafine group than in the griseofulvin group, but the difference was not statistically significant (70% versus 55%; RR 1.27, 95% CI 0.96 to 1.69; Analysis 1.3).
Percentage of drop‐outs as a surrogate for participant adherence
Four studies reported on the percentage of drop‐outs as a surrogate for participant adherence (Deng 2011; Fuller 2001; Gupta 2001; Memisoglu 1999), including one new study added to this update (Deng 2011). Deng 2011 reported no drop‐outs in the terbinafine group and one in the griseofulvin group (5.3%, 1/19) (RR 0.13, 95% CI 0.01 to 3.08; Analysis 1.4).
The percentage of drop‐outs was 35.9% (37/103) versus 24.2% (26/107) (RR 1.48, 95% CI 0.97 to 2.26 Fuller 2001); 4.0% (2/50) versus 8.0% (4/50) (RR 0.50, 95% CI 0.10 to 2.61 Gupta 2001); 10.2% (4/39) versus 17.9% (7/39) (RR 0.57, 95% CI 0.18 to 1.80; Memisoglu 1999) in the terbinafine and griseofulvin groups, respectively (see Analysis 1.4). Only one study reported no drop‐outs from either treatment arm (Haroon 1995).
2. Terbinafine (6 weeks) versus griseofulvin (6 weeks) in Trichophyton infections; medium treatment duration; 10 weeks follow‐up
Primary outcomes
Complete cure, i.e. clinical and mycological cure
Two studies reported on complete cure (Elewski 2008; Lipozencic 2002), including one new study added to this update (Elewski 2008). This study included 1549 participants and compared terbinafine (5 to 8 mg/kg for 6 weeks) with griseofulvin (10 to 20 mg/kg for 6 weeks) in children with tinea capitis. In this study, 49.3% of the participants were infected with T. tonsurans, 15.6% were infected with T. violaceum, and 15.1% were infected with M. canis.
Trichopyton tonsurans infections
In those infected with T. tonsurans, 52.1% (264/507) of participants in the terbinafine group versus 35.4% (91/257) in the griseofulvin group achieved a complete cure (RR 1.47, 95% CI 1.22 to 1.77; N = 764; moderate quality evidence; Analysis 2.1; summary of findings Table for the main comparison).
Trichopyton violaceum infections
In those infected with T. violaceum, 41.3% (66/160) of participants in the terbinafine group versus 45.1% (37/82) in the griseofulvin group achieved a complete cure (RR 0.91, 95% CI 0.68 to 1.24; N = 242; low quality evidence; Analysis 2.1; summary of findings Table for the main comparison).
The pooled data of participants infected with Trichophyton indicated that there was no significant difference between the terbinafine group and the griseofulvin group (49.5% versus 37.8%; RR 1.18, 95% CI 0.74 to 1.88; N = 1006; low quality evidence; Analysis 2.1; summary of findings Table for the main comparison).
Adverse events
Drug‐related adverse events
Both Elewski 2008 and Lipozencic 2002 reported this outcome. New evidence from Elewski 2008 indicated that 51.9% (541/1042) of participants in the terbinafine group and 49.1% (249/507) in the griseofulvin group reported an adverse effect during the study (RR 1.06, 95% CI 0.95 to 1.18). A total of 9.2% (96/1042) of participants in the terbinafine group and 8.3% (42/507) in the griseofulvin group had adverse events attributed to the study drugs (RR 1.11, 95% CI 0.79 to 1.57; N = 1549; moderate quality evidence; Analysis 2.2; summary of findings Table for the main comparison). The most frequent adverse events, accounting for more than 5% in any group, were nasopharyngitis, headache, pyrexia, cough, and vomiting. These individual adverse events were also similar between the two groups.
In addition, Lipozencic 2002 reported "adverse events from 18.4% to 42.4% for the terbinafine treatment groups and 16.7% for the griseofulvin group". The most common adverse events, accounting for approximately 5% in any group, were fever, pharyngitis, infections (parasitic, viral and upper respiratory tract) and influenza‐like symptoms. Terbinafine was well tolerated in all treatment groups, although two participants prematurely discontinued treatment. One suffering from urticaria was in the terbinafine 6‐week group; and the other, suffering from asymptomatic and reversible neutropaenia, was in the terbinafine 10‐week group. Both events resolved without sequelae. Somnolence and gastrointestinal disorders were also reported.
Severe adverse events
Severe adverse events were rare (0.6% in both groups; RR 0.97, 95% CI 0.24 to 3.88; N = 1549; moderate quality evidence; Analysis 2.3; summary of findings Table for the main comparison).
Secondary outcomes
None of the studies comparing terbinafine (six weeks) to griseofulvin (six weeks) for Trichophyton infection reported recurrence of the condition after the end of the intervention period, percentage of drop‐outs as a surrogate for participant adherence or the time taken to cure.
Proportion of participants with clinical cure only
One new study reported the proportion of patients with a clinical cure only (Elewski 2008). In participants infected with T. tonsurans, the proportion of participants with clinical cure only at week 10 was 70% (355/507) in the terbinafine group and 57.2% (147/257) in the griseofulvin group (RR 1.22, 95% CI 1.09 to 1.38; Analysis 2.4). In participants infected with T. violaceum, the corresponding proportion was 65% (104/160) in the terbinafine group and 64.6% (53/82) in the griseofulvin group (RR 1.01, 95% CI 0.83 to 1.22; Analysis 2.4).
3. Terbinafine (medium (6 to 8 weeks) and long term (10 to 12 weeks) treatment versus griseofulvin in Microsporum infections; 10‐16 weeks follow‐up
Primary outcome
Complete cure, i.e. clinical and mycological cure
Microsporum infections
We included two studies that reported data for participants infected with Microsporum (Elewski 2008; Lipozencic 2002). In Elewski 2008, a new study added in this update that included 1549 participants,15.1% were infected with M. canis. Of these, 27% (41/152) of participants in the medium‐term terbinafine group versus 43.9% (36/82) in the griseofulvin group achieved complete cure (Elewski 2008) (RR 0.61, 95% CI 0.43 to 0.88; Analysis 3.1).
Another open study, Lipozencic 2002, assessed medium‐ to long‐term treatment regimens of terbinafine versus griseofulvin. In this study, 98.5% of the 165 included participants were infected with M. canis, and the remainder were infected with M. audouini. A lower proportion of participants treated with medium‐term terbinafine achieved complete cure (51.4%, 36/70) compared to those treated with griseofulvin (70%, 21/30), but the difference was not statistically significant (RR 0.73, 95% CI 0.53 to 1.02; Analysis 3.1). Long‐term duration of treatment (10 or 12 weeks) resulted in the complete cure being higher in those in the griseofulvin group (70%, 21/30) compared to those in the terbinafine group (35%, 23/65) at 4 weeks after the end of treatment (RR 0.51, 95% CI 0.34 to 0.76; Analysis 3.1).
In participants infected with Microsporum, pooling the data from two studies for medium‐term treatment (six or eight weeks) resulted in an increase in complete cure for those in the griseofulvin group compared to those in the terbinafine group at four weeks after the end of treatment (34.7% versus 50.9%; RR 0.68, 95% CI 0.53 to 0.86; N = 334; moderate quality evidence; Analysis 3.1; Elewski 2008; Lipozencic 2002; summary of findings Table for the main comparison).
Adverse events
None of the studies (Elewski 2008; Lipozencic 2002) reported this outcome.
Secondary outcomes
Neither of the included studies comparing short‐ or long‐term treatment with terbinafine versus griseofulvin for Microsporum reported on recurrence of the condition after the end of the intervention period or the time taken to cure.
Proportion of participants with clinical cure only
Two studies reported the proportion of participants with a clinical cure only (Elewski 2008; Lipozencic 2002), including one new study added to this update (Elewski 2008). According to Elewski 2008, in participants infected with M. canis, the proportion of participants with clinical cure only at week 10 was 39.5% (60/152) in the terbinafine group and 57.3% (47/82) in the griseofulvin group (RR 0.69, 95% CI 0.53 to 0.90; Analysis 3.2). In Lipozencic 2002 at 16 weeks, the proportion of participants infected with Microsporum with clinical cure only was 61.1% (22/36) and 70.5% (24/34) in the groups treated with terbinafine for 6 and 8 weeks, respectively, and 60.6% (20/33) and 50% (16/32) in the groups treated with terbinafine for 10 and 12 weeks, respectively, compared to 80% (24/30) in the griseofulvin group. The control treatment (griseofulvin for 12 weeks) resulted in more cures compared with medium‐term terbinafine treatment duration (6 to 8 weeks) (RR 0.82, 95% CI 0.64 to 1.05; Analysis 3.2) and long‐term terbinafine treatment duration (10 to 12 weeks) (RR 0.69, 95% CI 0.52 to 0.92; Analysis 3.2), which was statistically significant in favour of griseofulvin. We pooled data from two studies (Elewski 2008; Lipozencic 2002) in a meta‐analysis. In participants infected with Microsporum, the proportion of participants with clinical cure only was significantly lower in the medium‐term terbinafine treatment group than in the griseofulvin group (RR 0.76, 95% CI 0.63 to 0.91; N = 334; Analysis 3.2).
Percentage of drop‐outs as a surrogate for participant adherence
Lipozencic 2002 reported on drop‐outs as a surrogate to measure adherence. The percentage of drop‐outs was 22.2% (8/36), 14.7% (5/34), 18.18% (6/33), 34.2% (12/32), and 23.3% (7/30), in the groups treated with terbinafine for 6, 8, 10, or 12 weeks and griseofulvin, respectively.
4. Terbinafine short‐term versus long‐term for treating Trichophyton and Microsporum infections; 12 to 20 weeks follow‐up
Primary outcomes
Complete cure, i.e. clinical and mycological cure
One to two weeks versus four weeks
Four studies reported on complete cure (Friedlander 2002; Haroon 1996; Kullavanijaya 1997; Talarico Filho 1998). Meta‐analysis showed that a four‐week treatment duration of terbinafine was significantly better than one to two weeks (65.1% versus 48.6%; RR 0.73, 95% CI 0.62 to 0.86; Analysis 4.1).
Medium term (6 to 8 weeks) versus long‐term (10 to 12 weeks)
Medium‐term (six to eight weeks) treatment duration of terbinafine appeared to be better than long‐term (10 to 12 weeks) treatment duration, but the difference was not statistically significant (51.4% versus 35.3%; RR 1.45, 95% CI 0.97 to 2.17; Lipozencic 2002; Analysis 4.1).
Adverse events
Five studies reported on adverse events (Deng 2011; Friedlander 2002; Hamm 1999; Haroon 1996; Talarico Filho 1998), including one study added to this update (Deng 2011).
Deng 2011 reported that none of the terbinafine treated patients experienced adverse events.
Talarico Filho 1998 reported the following adverse events: mild itching and mild constipation in the one‐week arm; mild headache and nausea in the two‐week arm; mild urticaria, swelling of the lips (labial oedema), mild constipation, moderate loss of appetite, mild diarrhoea, mild nausea and moderate or partial loss of taste (recovered within eight weeks) in the four‐week arm.
Hamm 1999 reported: abdominal pain (mild to moderate), epistaxis (nose bleed), lack of appetite, headache, severe facial swelling, coughing and fever (mild to moderate) in the one‐week arm; abdominal pain, fatigue, nausea, dyspepsia, headache and fever in the two‐week arm. One additional participant had lack of appetite and gastroenteritis only during the additional four‐week treatment period.
In Friedlander 2002, around 44% of the participants experienced mild to moderate adverse events, which were probably not related to treatment. The most frequent adverse events were "upper respiratory tract infections, gastrointestinal upsets and other events common in this patient population". Authors did not report relevant data but stated that the frequency of adverse events was similar between groups.
Haroon 1996 compared three different regimens (at one, two and four weeks), reporting a few adverse events: headache, raised hepatic enzymes, raised triglycerides, eosinophilia and leucocytosis in the one‐week arm; raised hepatic enzymes and eosinophilia in the two‐week arm and raised hepatic enzymes, raised triglycerides, eosinophilia and leucocytosis in the four‐week arm.
Secondary outcomes
None of the studies reported recurrence of the condition after the end of the intervention period.
Proportion of participants with clinical cure only
Four studies reported on the proportion of participants achieving a clinical cure only, all of which were also included in the original review (Friedlander 2002; Haroon 1996; Lipozencic 2002; Talarico Filho 1998).
One to two weeks versus four weeks
Meta‐analysis of three included studies showed that a four‐week treatment duration of terbinafine seemed to be better than one‐ to two‐week treatment duration, but the difference was not statistically significant (75.1% versus 63.9%; RR 0.84, 95% 0.67 to 1.06; Friedlander 2002; Haroon 1996; Talarico Filho 1998; Analysis 4.2).
Medium term (6 to 8 weeks) versus long‐term (10 to 12 weeks)
Data from Lipozencic 2002 showed that medium‐term (6 to 8 weeks) treatment duration of terbinafine appeared to be better than long‐term (10 to 12 weeks), but the difference was also not statistically significant (65.7% versus 55.4%; RR 1.19, 95% CI 0.90 to 1.56; Analysis 4.2).
Percentage of drop‐outs as a surrogate for participant adherence
Two studies reported drop‐outs as a surrogate for adherence (Deng 2011; Friedlander 2002), including one new study added to this update (Deng 2011).
Deng 2011 reported there were no drop‐outs in the two‐week or four‐week terbinafine groups.
In Friedlander 2002, the percentage of drop‐outs in the one‐, two‐ and four‐week arms were reported as 25% (14/56), 25.4%(15/59) and 19.3% (12/62), respectively.
Time taken to cure
One study, also included in the original review, reported on time taken to cure (Hamm 1999). The time taken to cure was about two weeks if the causative organism was a Trichophyton. Participants infected with Microsporum only responded to an additional four‐week treatment course of terbinafine, i.e. two to three weeks after an initial course of one or two weeks.
5. Terbinafine standard dose versus double dose in Microsporum infections; 20 weeks follow‐up
This update did not identify any new studies addressing the outcomes for this comparison. Likewise, we did not find any studies reporting on our primary outcome of adverse events or the secondary outcomes of proportion of participants with clinical cure only; measurement of recurrence of the condition after the end of the intervention period; or percentage of drop‐outs as a surrogate for participant adherence.
Primary outcomes
Complete cure, i.e. clinical and mycological cure
Ungpakorn 2004 reported on complete cure and assessed the efficacy of the standard dose of terbinafine compared to double doses of terbinafine after 20 weeks of follow‐up. Both treatments were given in a pulsed protocol (one week on, three weeks off) for the treatment of tinea capitis caused by Microsporum species. The proportion with complete cure for the standard dose group reached 60.8% (14/23) and was similar to 68.4% (13/19) in the double dose group (RR 1.12, 95% CI 0.72 to 1.76; Analysis 5.1).
Secondary outcomes
Time taken to cure
Ungpakorn 2004 also reported time taken to cure: at week 20 all participants were cured with the exception of one who at the beginning had moderately severe tinea capitis.
6. Itraconazole (six and two weeks) versus griseofulvin (six weeks) in Trichophyton and Microsporum infections
This update did not identify any new studies addressing the outcomes for this comparison.
Primary outcomes
Complete cure, i.e. clinical and mycological cure
Two studies reported complete cure (Gupta 2001; López‐Gómez 1994).
Gupta 2001 compared six weeks of griseofulvin versus two to three weeks of itraconazole in 100 people, with the dose given according to the participant's weight. This study showed complete cure at 82% (41/50) for the itraconazole group and 92% (46/50) for the griseofulvin group (RR 0.89, 95% CI 0.76 to 1.04; Analysis 6.1). The main causative fungi were T. tonsurans and T. violaceum, although investigators did not report the exact percentages. According to this trial, when Trichophyton species are the infecting fungi, both griseofulvin and itraconazole reach high complete cure percentages, although griseofulvin tends to be more effective. However the disadvantage was that griseofulvin was administered for six weeks treatment, while itraconazole was administered only for two to three weeks.
In another study involving 34 participants, in whom M. canis was the most common fungi, complete cure was the same for both drugs at 88% (15/17 and 15/17) (López‐Gómez 1994). This study compared six weeks of treatment with ultra microsize griseofulvin 500 mg/d or itraconazole 100 mg/d with a follow‐up of 14 weeks. According to this trial, in tinea capitis involving Microsporum species, both itraconazole and griseofulvin reached high complete cure percentages within a treatment period of six weeks (RR 1.00, 95% CI 0.78 to 1.28; Analysis 6.1).
We did not see a significant statistical difference between the different doses of itraconazole employed in the two studies and griseofulvin in the pooled analysis (83.6% versus 91.0%; RR 0.92, 95% CI 0.81 to 1.05; N = 134; very low quality evidence; Analysis 6.1; summary of findings Table 2).
Adverse events
Two studies reported adverse events (Gupta 2001; López‐Gómez 1994).
Authors did not report adverse events in the itraconazole group of either of the trials. In those treated with griseofulvin, two participants experienced nausea and intense stomach ache with severe vomiting at weeks two and four of treatment, requiring discontinuation of therapy (López‐Gómez 1994). Gupta 2001 reported three gastric problems and three cases of nausea in the griseofulvin group. One of the participants who experienced nausea dropped out of the study.
Secondary outcomes
None of the studies under this comparison reported recurrence of the condition after the end of the intervention period or the time taken to cure.
Proportion of participants with clinical cure only
Only one study reported this outcome (Gupta 2001). The proportion of participants with clinical cure only at the end of treatment reported in the study were 44% (22/50) and 70% (35/50) in the itraconazole and in the griseofulvin groups, respectively (RR 0.63, 95% CI 0.44 t0 0.90; Analysis 6.2).
Percentage of drop‐outs as a surrogate for participant adherence
Two studies reported on drop‐outs (Gupta 2001; López‐Gómez 1994).
In Gupta 2001, the percentage of drop‐outs was the same for both treatment groups (8% versus 8%; RR 1.00, 95% CI 0.26 to 3.78; Analysis 6.3). In López‐Gómez 1994 the percentage of drop‐outs was 5.5% (1/18) in the itraconazole group and 11.7% (2/17) in the griseofulvin group (RR 0.47, 95% CI 0.05 to 4.74; Analysis 6.3).
7. Itraconazole versus terbinafine (both two weeks) in Trichophyton infections
This update did not identify any new studies addressing the outcomes for this comparison.
Primary outcomes
Complete cure, i.e. clinical and mycological cure
Gupta 2001 and Jahangir 1998 reported on complete cure.
Jahangir 1998 had 60 participants and compared a two‐week course of itraconazole (50 to 200 mg/d based on weight) with two weeks of terbinafine. T. violaceum was the causative fungus in 82% to 89% of the participants. Twelve weeks after the start of treatment, 53% (16/30) and 60% (18/30) of participants were completely cured in the terbinafine and itraconazole groups, respectively (RR 1.13, 95% CI 0.72 to 1.75; Analysis 7.1). Gupta 2001, where Trichophyton was the species of fungus, compared itraconazole and terbinafine with a two‐ to three‐week course of therapy. At 12 weeks, 94% (47/50) in the terbinafine group had a complete cure, compared to 82% (41/50) in the itraconazole group (RR 0.87, 95% CI 0.75 to 1.01; Analysis 7.1).
In the pooled analyses, there was very little difference in the proportion of participants achieving complete cure with itraconazole and terbinafine (as treatment of Trichophyton species) when used for periods of two to three weeks (73.8% versus 78.8%; RR 0.93, 95% CI 0.72 to 1.19; N = 160; low quality evidence; Analysis 7.1; summary of findings Table 3).
Adverse events
Only Jahangir 1998 reported adverse events. Two participants reported urticaria in the itraconazole group. In the terbinafine group, one participant experienced fever, body aches and vertigo, but no participant showed any significant haematological or biochemical change.
Secondary outcomes
No studies for this comparison reported recurrence of the condition after the end of the intervention period or the time taken to cure.
Proportion of participants with clinical cure only
Only Gupta 2001 reported on the proportion of participants achieving clinical cure at the end of the four‐week treatment, with similar results in both terbinafine and itraconazole treatment groups: 40% (20/50) and 44% (22/50), respectively (RR 1.10, 95% CI 0.69 to 1.75; Analysis 7.2).
Percentage of drop‐outs as a surrogate for participant adherence
Gupta 2001 reported that the percentage of drop‐outs was 8% (4/50) for the itraconazole group and 4% (2/50) for the terbinafine group (RR 2.00, 95% CI 0.38 to 10.43, Analysis 7.3).
8. Ketoconazole versus griseofulvin (12 to 26 weeks) in Trichophyton infections; 12 to 26 weeks follow‐up
This update did not identify any new studies addressing the outcomes for this comparison.
Primary outcomes
Complete cure, i.e. clinical and mycological cure
Two studies reported complete cure, but because of the differences in treatment durations between them, we did not pool the results (Gan 1987; Tanz 1988).
Gan 1987 was an open study in 80 participants where Trichophyton species predominated; investigators compared once‐daily ketoconazole 5 mg/kg/d with once‐daily griseofulvin 15 mg/kg/d. The children were examined every two weeks while they were receiving therapy (and at least one follow‐up after the end of therapy). Treatment was stopped when there was either complete cure or after six months had passed. At the end of 12 weeks of therapy, 73.5% (25/34) of participants treated with ketoconazole had complete cure of their infection, compared with 96.4% (27/28) of the participants given griseofulvin (RR 0.76, 95% CI 0.62 to 0.94; N = 62; low quality evidence; Analysis 8.1; summary of findings Table 4 ).
Those who did not achieve a complete clinical cure within 12 weeks continued to take therapy and were assessed between 12 and 26 weeks of therapy, until they exhibited complete resolution of clinical disease and negative hair sample cultures. During this period, the one remaining griseofulvin participant and six of the ketoconazole participants with continuing disease had complete clearance of clinical and mycological disease.
Thus, by the end of 26 weeks, all of the participants in the griseofulvin group were completely cured, and only three ketoconazole‐treated patients remained with persistent clinical disease and positive mycological cultures (i.e. 91.2% (31/34) participants receiving ketoconazole compared with 100% (28/28) in the griseofulvin group (RR 0.95, 95% CI 0.83 to 1.07; N = 62; low quality evidence; Analysis 8.1; summary of findings Table 4).
In Tanz 1988, participants randomly received ketoconazole or griseofulvin for 12 weeks. The proportion of participants with complete cure was similar at 48% (16/33) in the ketoconazole group and 54% (25/46) in the griseofulvin group (RR 0.89, 95% CI 0.57 to 1.39; N = 79; low quality evidence; Analysis 8.1; summary of findings Table 4).
Adverse events
Four studies reported adverse events (Gan 1987; Martínez‐Roig 1988; Tanz 1985; Tanz 1988). Despite reports of liver disease (Lewis 1984), we did not find any studies reporting this adverse effect. Ketoconazole use was associated with two cases of abdominal pain and one case of urticaria (Tanz 1985). Only one participant from the ketoconazole group withdrew from the study and reported to have nausea. Other than this, there were no serious adverse reactions in any of the two groups (Tanz 1988). No adverse events were reported in the ketoconazole group (Gan 1987; Martínez‐Roig 1988). One griseofulvin‐treated participant showed a two‐fold increase in serum alanine aminotransferase and aspartate aminotransferase after three weeks of treatment, but values returned to normal at the following weekly clinic visits (Martínez‐Roig 1988).
Secondary outcomes
Proportion of participants with clinical cure only
Only one study reported this outcome (Martínez‐Roig 1988). The proportion of participants with clinical cure evaluated at the end of treatment were 100% (8/8) and 80% (4/5) in the ketoconazole and griseofulvin groups, respectively (RR 1.26, 95% CI 0.77 to 2.05; Analysis 8.2).
Proportion of participants with recurrence of the condition after the end of the intervention period
Gan 1987 reported (page 48) that "three patients (two treated with ketoconazole and one treated with griseofulvin) had a recurrence of tinea capitis at four weeks (two patients) and at four months (one patient) following discontinuation of therapy".
Percentage of drop‐outs as a surrogate for participant adherence
Two studies reported this outcome (Tanz 1985; Tanz 1988).
In Tanz 1985, the percentage of drop‐outs was 30% (3/10) and 41.6% (5/12) in the ketoconazole and griseofulvin groups, respectively (RR 0.72, 95% CI 0.23 to 2.30, Analysis 8.3).
In Tanz 1988, the percentage of drop‐outs was 66.6% (22/33) and 56.5% (26/46) in the ketoconazole and griseofulvin groups, respectively (RR 1.18, 95% CI 0.83 to 1.67; Analysis 8.3).
Time taken to cure
Two studies reported this outcome (Gan 1987; Martínez‐Roig 1988).
In Gan 1987, the time needed to improve was 60 days and 108 days in the ketoconazole and griseofulvin groups, respectively. Hair sample cultures took significantly longer to become negative (sterile) in the ketoconazole group (median eight weeks) than in the griseofulvin group (four weeks).
Martínez‐Roig 1988 reported the mean time to clinical cure in weeks: 4.2 weeks in the griseofulvin group and 5.0 weeks in the ketoconazole group. They also reported the mean time needed to achieve negative cultures in weeks: 3.6 and 4.7 weeks in the griseofulvin and ketoconazole groups, respectively.
9. Fluconazole (2 to 6 weeks) versus griseofulvin (6 weeks); 8‐12 weeks follow‐up
The study by Foster 2005 was new to this update.
Primary outcomes
Complete cure, i.e. clinical and mycological cure
Three studies reported this outcome (Dastghaib 2005; Foster 2005; Gupta 2001).
Dastghaib 2005 assessed 40 participants: 16 were infected with T. violaceum, 16 with T. verrucosum and 8 with M. canis. The children were treated with 5 mg/kg/d of fluconazole or 15 mg/kg/d griseofulvin for four and six weeks, respectively. Complete cure was reported for 79% (15/19) of the fluconazole arm and 76% (16/21) of the griseofulvin arm (RR 1.04, 95% CI 0.74 to 1.45; Analysis 9.1).
Foster 2005 included 880 participants: 86% were infected with T. tonsurans and 11% with M. canis; 721 of them were included in the analyses: 245 participants on short‐term fluconazole, 246 participants on the medium‐term fluconazole and 230 participants in the griseofulvin group. As we stated in the 'Methods' section, for RCTs with multiple intervention groups, we split the shared griseofulvin group (N = 230) in two (N = 115 each) to avoid double‐counting.
The children were randomly assigned to three groups and treated with a short‐term course of fluconazole (6 mg/kg/d for three weeks; N = 245); medium‐term use of fluconazole (6 mg/kg/d for six weeks; N = 246); or griseofulvin (11 mg/kg/d for six weeks; 230), respectively. Complete cure was not significantly different between the short‐term fluconazole group and the griseofulvin group (30.2% versus 31.3%; RR 0.96, 95% CI 0.69 to 1.34; Analysis 9.1).
Gupta 2001 assessed 100 participants who were infected with T. tonsurans and/or T. violaceum (the exact percentages were not reported). They were treated with either fluconazole 6 mg/kg/d for two to three weeks or with microsize griseofulvin 20 mg/kg/d for six weeks. The proportion of participants with complete cure were 82% (41/50) and 92% (46/50), respectively (RR 0.89, 95% CI 0.76 to 1.04; Analysis 9.1).
Short‐term (2‐4 weeks) fluconazole
Meta‐analysis of the three studies failed to show any significant difference between short‐term use of fluconazole and griseofulvin for proportions of participants with complete cure i.e. clinical and mycological cure (41.4% versus 52.7%; RR 0.92, 95% CI 0.81 to 1.05; N = 615; moderate quality evidence; Analysis 9.1; Dastghaib 2005; Foster 2005; Gupta 2001; summary of findings Table 5).
Medium‐term (6 weeks) fluconazole
There is a single trial in this subgroup (N = 361; Foster 2005). There was no clear difference between between the medium‐term fluconazole group and the griseofulvin group (34.1% versus 32.1%; RR 1.06, 95% CI 0.77 to 1.46; N = 361; low quality evidence; Analysis 9.1; summary of findings Table 5).
Adverse events
Three studies reported this outcome (Dastghaib 2005; Foster 2005; Gupta 2001).
Foster 2005 included 1063 patients for safety evaluation and reported that the most frequent treatment‐related adverse events were abdominal pain (1.3%) and diarrhoea (0.7%) in the short‐term fluconazole group; headache (0.9%) and rash (0.6%) in the medium‐term fluconazole group; and headache (1.7%), abdominal pain (1.4%) and dyspepsia (1.0%) in the griseofulvin group. There were no significant differences between the three groups with regard to all causality and treatment‐related adverse events.
Two studies reported nausea as an adverse effect in the griseofulvin group (Dastghaib 2005; Gupta 2001).
Secondary outcomes
None of the studies in this comparison reported on recurrence of the condition after the end of the intervention period or the time taken to cure.
Proportion of participants with clinical cure only
Two studies reported this outcome (Foster 2005; Gupta 2001).
Foster 2005 reported that the proportions of participants with clinical cure only at week 10 were 40% (98/245), 46% (112/246), and 40% (92/230) in the short‐term fluconazole, medium‐term fluconazole, and griseofulvin groups, respectively.
Gupta 2001 reported the proportions of participants with clinical cure only at the end of treatment (week 4 for fluconazole and week 6 for griseofulvin) were 26% (13/50) and 70% (35/50) in the fluconazole and griseofulvin groups, respectively (RR 0.37, 95% CI 0.22 to 0.61; Analysis 9.2).
Percentage of drop‐outs as a surrogate for participant adherence
Two studies reported this outcome (Foster 2005; Gupta 2001).
Foster 2005 reported that the percentages of drop‐outs were 12% (37/302), 7% (21/286), and 8% (24/292) in the short‐term fluconazole, medium‐term fluconazole and griseofulvin groups, respectively.
The same percentage of drop‐outs was reported for both groups in Gupta 2001 (8% versus 8%, RR 1.00, 95% CI 0.26 to 3.78; Analysis 9.3).
10. Fluconazole (2 to 3 weeks) versus terbinafine (2 to 3 weeks) in Trichophyton infections; 12 weeks follow‐up
This update did not identify any new studies addressing the outcomes for this comparison. Moreover, none of the trials evaluating this comparison reported on adverse events, recurrence of the condition after the end of the intervention period or the time taken to cure.
Primary outcome
Complete cure, i.e. clinical and mycological cure
Only one study reported this outcome (Gupta 2001). The efficacy of fluconazole for two to three weeks was compared with terbinafine, dosed according to weight for two to three weeks in Trichophyton infections. The proportions of participants with complete cure were 82% (41/50) for the fluconazole arm and 94% (47/50) for the terbinafine arm (RR 0.87, 95% CI 0.75 to 1.01; N = 100; low quality evidence; Analysis 10.1; summary of findings Table 6).
Secondary outcomes
Proportion of participants with clinical cure only
Only one study reported this outcome (Gupta 2001). The proportion of participants with clinical cure only at the end of treatment (week 4 for terbinafine and fluconazole) was not significantly different in the terbinafine group compared with the fluconazole group ((40% versus 26%; RR 1.54, 95% CI 0.86 to 2.74).
Percentage of drop‐outs as a surrogate for participant adherence
Only one study reported this outcome (Gupta 2001). The percentage of drop‐outs was 4% (2/50) and 8% (4/50) in the terbinafine and fluconazole groups, respectively (RR 0.50, 95% CI 0.10 to 2.61).
11. Fluconazole (2 to 3 weeks) versus itraconazole (2 to 3 weeks) in Trichophyton infections; 12 weeks follow‐up
This update did not identify any new studies addressing the outcomes for this comparison. Moreover, none of the trials evaluating this comparison reported on adverse events, recurrence of the condition after the end of the intervention period or the time taken to cure.
Primary outcome
Complete cure, i.e. clinical and mycological cure
Only one study reported this outcome (Gupta 2001). When fluconazole treatment was compared with itraconazole in participants with Trichophyton tinea capitis, in doses of 5 mg/kg/d daily for two to three weeks, the proportion of participants with complete cure was 82% (41/50 and 41/50) for both groups (RR 1.00, 95% CI 0.83 to 1.20; N = 100; low quality evidence; Analysis 11.1; summary of findings Table 7).
Secondary outcome:
Proportion of participants with clinical cure only
Only one study reported this outcome (Gupta 2001). The proportion of participants with clinical cure only at the end of treatment (week four in itraconazole and fluconazole groups) was nearly double in the itraconazole group: 44% (22/50) compared with 26% (13/50) in the fluconazole group, but the difference was not statistically significant (RR 1.69, 95% CI 0.96 to 2.97; Analysis 11.2).
Percentage of drop‐outs as a surrogate for participant adherence
Only one study reported this outcome (Gupta 2001). The same percentage of drop‐outs as a surrogate for participant adherence was reported in both treatment groups (8%, 4/50; RR 1.00, 95% CI 0.26 to 3.78; Analysis 11.3).
12. Fluconazole low dose versus higher dose (1.5, 3.0 and 6.0 mg/kg/d) in Trichophyton infections; 4 months follow‐up
This update did not identify any new studies addressing the outcomes for this comparison. In fact, we found a single study for this comparison, and it only reported on one primary outcome (complete cure) and not on any of our secondary outcomes (Solomon 1997). We categorised data into three subgroups comprising 1.5 mg versus 3.0 mg; 1.5 mg versus 6.0 mg; and 3.0 mg versus 6.0 mg.
Primary outcome
Complete cure, i.e. clinical and mycological cure
Solomon 1997 compared different doses of fluconazole: 1.5 mg/kg/d, 3.0 mg/kg/d, and 6.0 mg/kg/d, for 20 days in a group of 41 participants with tinea capitis caused by the Trichophyton species. Authors reported efficacy in only 27 participants and did not provide details on drop‐outs by group. However, they reported the total missing participants (34%) in the study. Thus, we assumed that the same percentage was applied for the missing participants in each group, being originally 12, 15 and 14 participants randomly assigned in the 1.5 mg/kg/d, 3.0 mg/kg/d and 6.0 mg/kg/d groups, respectively. Intention‐to‐treat efficacy rates in the 1.5 mg/kg/d, 3.0 mg/kg/d and 6.0 mg/kg/d groups were 17% (2/12), 40% (6/15) and 57% (8/14), respectively.
Although higher doses resulted in more cures than lower doses, none of the comparisons reached statistical significance (3.0 mg versus 1.5 mg: RR 2.40, 95% CI 0.59 to 9.82; Analysis 12.1; 6.0 mg versus 1.5 mg: RR 3.43, 95% CI 0.89 to 13.15; Analysis 12.1; 6.0 mg versus 3.0 mg: RR 1.43, 95% CI 0.66 to 3.08; Analysis 12.1).
13. Treatment durations of fluconazole (3 weeks versus 6 weeks); 10 weeks follow‐up
One new study added to this update evaluated this comparison, but it did not report on adverse events, recurrence of the condition after the end of the intervention period or the time taken to cure (Foster 2005).
Primary outcome
Complete cure, i.e. clinical and mycological cure
Foster 2005 compared different treatment duration of fluconazole: short‐term use of fluconazole (6 mg/kg/d for three weeks) and medium‐term use of fluconazole (6 mg/kg/d for six weeks). At week 10, there was no significant difference with regard to the proportion of participants with complete cure for the short‐term and medium‐term use of fluconazole in children infected with T. tonsurans and M. canis (30.2%, 74/245 versus 34.1%, 84/246; RR 0.88, 95% CI 0.68 to 1.14; N = 491; low quality evidence; Analysis 13.1; summary of findings Table 8).
Secondary outcomes
Proportion of participants with clinical cure only
Foster 2005 reported that short‐term use of fluconazole and medium‐term use of fluconazole had similar effects on clinical cure (RR 0.88, 95% CI 0.72 to 1.08).
Percentage of drop‐outs as a surrogate for participant adherence
Foster 2005 reported the percentage of drop‐outs was 12% (37/302) and 7% (21/286) in the short‐term and medium‐term fluconazole groups, respectively (RR 1.67, 95% CI 1.00 to 2.78).
Discussion
Summary of main results
In this updated review, we included 25 studies (comprising of 4449 participants), including 4 new studies (2637 participants) added to this update. The data from the included studies produced 13 main comparisons of interventions.
Terbinafine versus griseofulvin
In our meta‐analyses of terbinafine for 4 weeks versus griseofulvin for 8 weeks assessed at 12 to 24 weeks of follow‐up, the result favoured neither terbinafine nor griseofulvin for Trichophyton infections (RR 1.06, 95% CI 0.98 to 1.15; N = 328, 3 RCTs; low quality evidence; summary of findings Table for the main comparison) for our primary outcome of complete cure.This was also the case for mixedTrichophyton and Microsporum infections in two studies and in a single study analysis of Microsporum infections.
New evidence from Elewski 2008 indicated that terbinafine (at standard doses according to the participant's weight for six weeks) achieved a similar proportion with complete cure as griseofulvin (at standard doses according to the participant's weight for six weeks) in children infected with Trichophyton, when followed up for 10 weeks (RR 1.18, 95% CI 0.74 to 1.88; N = 1006; 1 RCT; low quality evidence, summary of findings Table for the main comparison). Sub‐group analysis assessing response to treatment in children infected with T. tonsurans revealed that terbinafine is better than griseofulvin. This new evidence resulted in a change in the conclusions of this review. However, both of the two regimens had similar effects in children with T. violaceum.
There is moderate quality evidence that griseofulvin (6 to 12 weeks) is better than medium‐term (6 to 8 weeks) use of terbinafine with respect to the proportion of participants achieving complete cure (RR 0.68, 95% CI 0.53 to 0.86; N = 334; 2 RCTs; summary of findings Table for the main comparison).This evidence in favour of the efficacy of griseofulvin in Microsporum infection was newly added to this update (Elewski 2008).
Moderate quality evidence also confirmed that the adverse events and severe adverse events are comparable between terbinafine and griseofulvin, the adverse events being mild and reversible in most cases (RR 1.11, 95% CI 0.79 to 1.57; N = 1549; 1 RCT; summary of findings Table for the main comparison).
Different dose regimens of terbinafine
We investigated a possible relationship between dose, duration and response for terbinafine. A meta‐analysis of four studies indicated that a four‐week treatment duration of terbinafine was significantly better than one or two weeks of treatment with respect to complete cure of Trichophyton and Microsporum infections (RR 0.73, 95% CI 0.62 to 0.86; N = 552; 4 RCTs). There were no differences in the proportion of participants who were completely cured, or cured clinically, when comparing medium‐term (6 to 8 weeks) versus long‐term (10 to 12 weeks) terbinafine in a single‐study analysis. Comparisons of adverse events between the different terms of treatment showed that the adverse events were mild and comparable between the groups. A single‐study comparison of the standard dose of terbinafine compared to a double dose in one study of Microsporum infections showed that the effectiveness in completely curing the infection was comparable between regimens when assessed at 20 weeks follow‐up.
Itraconazole versus griseofulvin
A meta‐analysis of two studies found no significant difference between itraconazole and griseofulvin for achieving a complete cure in children with Trichophyton and Microsporum (RR 0.92, CI 0.81 to 1.05; N = 134; 2 RCTs; very low quality evidence; summary of findings Table 2).
Itraconazole versus terbinafine
A meta‐analysis of two studies indicated that there was no significant difference between itraconazole and griseofulvin for achieving a complete cure in children infected with Trichophyton (RR 0.93, CI 0.72 to 1.19; N = 160; 2 RCTs; low quality evidence; summary of findings Table 3).
Ketoconazole versus griseofulvin
Current evidence regarding ketoconazole versus griseofulvin was limited. One study favoured griseofulvin, because ketoconazole (for 12 weeks) appeared to be less effective in terms of complete cure than griseofulvin for the same period (RR 0.76; 95% CI 0.62 to 0.94; Gan 1987). However, by the end of the study, when the treatment duration was extended up to a maximum of 26 weeks in those who had not achieved a cure by 12 weeks, their effects appeared to be similar (RR 0.95, 95% CI 0.83 to 1.07). Another study indicated that the proportion with a complete cure was similar in the ketoconazole (for 12 weeks) and griseofulvin (for 12 weeks) groups (RR 0.89, 95% CI 0.57 to 1.39; summary of findings Table 4).
Fluconazole versus other therapies (griseofulvin or terbinafine or fluconazole)
A meta‐analysis of three studies indicated that fluconazole and griseofulvin had similar effects for achieving complete cure either in the short term of two to four weeks (RR 0.92, 95% CI 0.81 to 1.05; N = 500; 3 RCTs moderate quality evidence) or in the medium term of six weeks (RR 1.06, 95% CI 0.77 to 1.46; N = 361; 1 RCT low quality evidence, summary of findings Table 5).
A single study analysis of one small trial showed no differences between either of the two interventions for the outcome of complete cure when fluconazole was compared with terbinafine, both administered for two to three weeks (RR 0.87 CI 0.75 to 1.01; N = 100; 1 RCT; low quality evidence; summary of findings Table 6), or when fluconazole was compared to itraconazole each administered for two to three weeks, for Trichophyton infections (RR 1.00 CI 0.83 to 1.20; N = 100, 1 RCT low quality evidence, summary of findings Table 7).
Different dosages of fluconazole
The dosage of fluconazole was compared in one small single study analysis, that is, 1.5, 3.0, and 6.0 mg/k/d in Trichophyton infections, with no significant differences between the groups, although higher doses resulted in more cures in each comparison when followed up at 4 months.
Different treatment duration of fluconazole
A further single study analysis of treatment duration of fluconazole treatment comparing short‐term (3‐week) versus medium‐term (6‐week) treatment at 10 weeks follow‐up, showed no significant differences between the groups for children infected with T. tonsurans and M. canis.
Overall completeness and applicability of evidence
This review may help physicians worldwide weigh the advantages and disadvantages of systemic antifungal agents and the options when treating children with tinea capitis. It draws on detailed information derived from clinical trials assessing the efficacy of treatments for tinea capitis. However, caution is warranted when interpreting the data, because the 25 included studies published between 1987 to 2013 were conducted in different countries and included people of different ethnicities. Furthermore, fungal types varied from one trial to another. This means that our results may not be directly clinically applicable to individual participants and their specific situations.
Quality of the evidence
The quality of evidence in this review for each outcome, as presented in the 'Summary of findings' tables, was very low to moderate. The main reasons for downgrading the quality of the evidence for these outcomes were imprecision due to low sample sizes and risk of bias in the included studies.
Limitations in study design, execution, and reporting
The studies included in this review had several methodological limitations: only four studies adequately described the method of randomisation, and only two described adequate allocation concealment. Blinding of participants and personnel and blinding of outcome assessors was not adequate in any of the studies. Ten studies were at high risk of bias from incomplete reporting of outcome data (attrition bias), and although we judged that none was at high risk of selective reporting bias, we did not actually have access to the study protocols for comparison.
We detected other sources of bias, including failure to report disease severity or baseline comparability, but the extent to which these factors may have introduced bias was unclear. It is therefore important to emphasise that any conclusions that we have drawn are reliant on primary studies with varying degrees of bias. Readers should consider risk of bias when interpreting these results (Figure 3) and exercise caution with findings derived from studies with high or unclear risk of bias.
Inconsistency of the results
Inconsistency refers to an unexplained heterogeneity of the results across studies.
In this review, most of the comparisons were assessed in single studies, so assessment of consistency of the results across studies was not necessary. In outcomes for which the data were pooled, inconsistency of effects was only identified for one outcome (complete cure, terbinafine versus griseofulvin, summary of findings Table for the main comparison). In this outcome, we downgraded one level because I2 of the pooled outcome was 85%, which indicated substantial heterogeneity. One source of heterogeneity in this analysis of Trichophyton infections may be that the analysis included bothT. tonsurans and T. violaceum infections; however, the extent to which this clinical heterogeneity contributed to the observed statistical heterogeneity is unclear.
Imprecision of the results
Results are considered imprecise when studies include relatively few patients and few effects. In this review, imprecision was identified in some comparisons, and the reason for imprecision was that total number of effects was less than 300 as recommended by the GRADE handbook (Schünemann 2013).
Indirectness of the evidence
The majority of the 4449 participants with fungal infections in the 25 included studies were aged 2 to 16 years, so the evidence we found directly relates to the disease population of interest. In this review, patient‐reported outcomes (PROs), such as quality of life, were rarely reported in the included studies. PROs are important for evidence‐based clinical decision making and need to be addressed in future studies.
Publication bias
It was impossible to perform a funnel plot analysis to assess potential publication bias for any of our outcomes because of the limited number of trials; there were only one to three studies for each comparison.
Potential biases in the review process
Our assessment of the included studies was based on the published manuscripts; therefore, the results were inevitably influenced by the reporting quality of these studies. Undoubtedly, poor reporting quality influences the accuracy of the assessments, and we were unable to obtain further information from the trial investigators we contacted. Pather 2006 was a conference paper that appeared to meet the inclusion criteria, but as we could not obtain further information, we could not include or exclude it. This may be a source of potential bias, as the conclusions of the review could change once that study has been assessed. We attempted to conduct a comprehensive search for studies, but theoretically, there might be some missing studies because we did not search all local medical databases around the world.
In addition, clinical heterogeneity between included studies is inevitable because each study had participants with different ethnicities, types of fungal infection, severity of disease, dosages of drugs, and durations of treatment and follow‐up. Clinical heterogeneity could introduce bias when we combined the results of different studies by meta‐analysis.
Agreements and disagreements with other studies or reviews
Griseofulvin
In this review, griseofulvin was employed as a standard therapy for the evaluation of any newer treatments for tinea capitis.
An earlier meta‐analysis found that griseofulvin was an effective therapy for tinea capitis (Gupta 2008). This conclusion is supported by the findings of our review: in our meta‐analyses of griseofulvin versus terbinafine (two to four weeks), griseofulvin (six to eight weeks) was at least as effective as terbinafine for Trichophyton, Microsporum and mixedTrichophyton and Microsporum infections for our primary outcome of complete cure.
Tey 2011, another meta‐analysis, concluded that "griseofulvin is more efficacious than terbinafine in treating tinea capitis caused by Microsporum species". Additionally, Gupta 2013 performed a further meta‐analysis of randomised controlled trials and found no differences in the overall efficacy of the two drugs at the doses specified, but differences were observed based on the infectious species, i.e. griseofulvin was superior for Microsporum spp., whereas terbinafine was superior for Trichophyton spp. The recent guideline from the British Association of Dermatologists (BAD) also recommended griseofulvin as the first‐line treatment for tinea capitis in children, especially in those infected with Microsporum spp. (Fuller 2014). This update of the review also provides new, moderate quality evidence that for Microsporum infections, griseofulvin is better than terbinafine with respect to the proportion of participants achieving complete cure (summary of findings Table for the main comparison), which is in agreement with previous reviews and guidelines.
In our other comparisons of griseofulvin with triazole antifungal agents (itraconazole, fluconazole and ketoconazole) we found no evidence that griseofulvin was superior in efficacy for the outcome of complete cure, but these were small trials, and the quality of the evidence was moderate at best.
We found only limited evidence about the most suitable doses, duration and formulations of griseofulvin. Dosage recommendations for griseofulvin vary due to different formulations (Higgins 2000), and taking griseofulvin with fatty food improves its absorption and bioavailability. Some trials recommended higher doses for microsized griseofulvin but not for ultra‐microsized griseofulvin, although up to 25 mg/kg may be necessary (Higgins 2000). We found no evidence that directly compared different formulations of griseofulvin.
The main disadvantage of griseofulvin is perceived to be long duration of treatment required, which may lead to reduced adherence. The European Society for Pediatric Dermatology (ESPD) recommended, "The treatment decision between griseofulvin and newer antifungal agents for children with Trichophyton spp. for tinea capitis can be based on an individual patient on the balance between duration of treatment ⁄ adherence and economic considerations" (Kakourou 2010). It is still unclear if there is a difference in terms of adherence between four weeks of terbinafine versus eight weeks of griseofulvin, as in this review we did not find any evidence to support the hypothesis that adherence improves with shorter courses of treatment. It could be argued, though, that long courses of griseofulvin versus shorter courses of terbinafine for example, already incorporate any reduced adherence simply because of the longer duration of the former.
We included two studies that reported data on duration of treatment for participants infected with Microsporum (Elewski 2008; Lipozencic 2002). A lower proportion of participants treated with six to eight weeks of terbinafine in M. canis and M. audouini infections achieved complete cure compared to those treated with griseofulvin (not statistically significant). Long‐term duration of treatment (10 or 12 weeks) resulted in a higher proportion of participants achieving complete cure in the griseofulvin group than in the terbinafine group (summary of findings Table for the main comparison). However, in the absence of further direct comparisons of duration or formulations, we cannot comment further on the optimal regimens for treating tinea capitis in children with griseofulvin.
Griseofulvin is reported to be a safe drug, although it commonly causes side effects such as headaches and gastrointestinal upsets (Bennassar 2010). Despite the assumption that gastrointestinal disturbance is a major drawback of the older drugs like griseofulvin, we did not find reports of gastrointestinal disturbance associated with use of griseofulvin in our included studies. We acknowledge that while RCTs may not always provide a platform for reporting rare side effects, they are a reasonable method of detecting common ones. We included common adverse events as an outcome in our review; however, the included studies registered some infrequent adverse events that may or may not be related to griseofulvin treatment. We did find evidence that when they occur, severe adverse events are comparable between terbinafine and griseofulvin. In most cases, though, adverse events were mild and reversible. These included elevated serum liver enzymes, triglycerides and uric acid; anaemia, eosinophilia; leucocytosis and granulocytopenia. Although few observed adverse events were labelled as severe, periodic monitoring every month of organ system functions, including hepatic, renal and haematopoietic (blood) systems is advisable in those taking griseofulvin for more than eight weeks (Möhrenschlager 2005).
Griseofulvin has traditionally been the most widely used systemic treatment for tinea capitis, and its advantages are that it is inexpensive, there is extensive experience of its use, the suspension dosage form allows for accurate dosing in children, and it is licensed in most countries. However, griseofulvin is no longer available in New Zealand and other countries including Canada (Bortolussi 2016), as it has been superseded by newer antifungal drugs.
Terbinafine
The original version of this review found that terbinafine was at least as effective as griseofulvin for the treatment of Trichophyton infections of the scalp. In this update, we added some new evidence to support this finding. We found that for T. tonsurans, terbinafine is better than griseofulvin, while the two regimens had similar effects in children with T. violaceum. This finding also agrees with that of a previous meta‐analysis comparing terbinafine against griseofulvin (Fleece 2004).
The efficacy of terbinafine treatment may vary according to the fungal species isolated. New evidence in this update shows that terbinafine has a poorer effect on complete cure in participants with Microsporum infections. This finding correlates with the 2014 BAD guideline (Fuller 2014), which concluded that terbinafine was more effective against Trichophyton species; whereas griseofulvin was more effective against Microsporum species.
We found no evidence about formulations of terbinafine. While tablets may be preferred by some children (age five years and older perhaps), they may not allow for dosage individualisation (generally calculated by body weight, therefore smaller doses may be required than that provided by tablet formations). Drops or syrups are preferable to tablets for dosage individualisation in children, and there is a granule formation of terbinafine to be sprinkled on food (Fuller 2014).
The duration of terbinafine therapy may be important. Limited evidence from observational studies suggests that longer therapeutic regimens of terbinafine may improve complete cure for those infected with Microsporum species (Aste 2004; Commens 2003; Devliotou 2004). In our meta‐analysis of four studies that directly compared two weeks versus four weeks duration of terbinafine, a longer treatment duration was significantly better than a short duration for a complete cure.
Itraconazole
Itraconazole is currently the preferred agent in most European countries, although it is not licensed in some countries (e.g. the United Kingdom) for treating tinea capitis in children aged 12 years or younger (Fuller 2014). However, in this review, we only identified limited evidence based on small trials suggesting that oral itraconazole at weight‐adjusted doses was effective and safe for tinea capitis caused by T. violaceum (two weeks of treatment) and M. canis (six weeks of treatment). More well‐designed RCTs with large sample sizes are needed to confirm the safety, efficacy and optimal treatment regimens of itraconazole for paediatric tinea capitis patients.
Fluconazole
In this update, we included a large RCT that compared short‐term use of fluconazole (6 mg/kg/d for three weeks) with medium‐term use of fluconazole (6 mg/kg/d for six weeks) (Foster 2005). According to this study, short‐term and medium‐term use of fluconazole had a similar effect on complete cure. In the 2014 BAD guideline (Fuller 2014), fluconazole was recommended as an alternative to terbinafine for tinea capitis in children. However, the optimal regimen of fluconazole for treating paediatric tinea capitis remains unclear. Based on Fuller 2014 and the findings of this review, short‐term duration of fluconazole may be a useful treatment regimen.
Ketoconazole
This review identified low quality evidence that indicated that ketoconazole appeared to have similar efficacy with griseofulvin for tinea capitis in children, although it appears to be less effective than griseofulvin for children with tinea capitis caused by Trichophyton species (Gan 1987). However, ketoconazole is not recommended for use in children because of potential adverse events, especially hepatotoxicity (Elewski 2000), and oral ketoconazole was withdrawn from use in the United Kingdom and Europe in 2013 (Fuller 2014).
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Comparison 1 Terbinafine (2‐4 weeks) versus griseofulvin (6‐8 weeks); short treatment duration; 6‐24 weeks follow‐up, Outcome 1 Primary outcome: complete cure, i.e. clinical and mycological cure.

Comparison 1 Terbinafine (2‐4 weeks) versus griseofulvin (6‐8 weeks); short treatment duration; 6‐24 weeks follow‐up, Outcome 2 Primary outcome: adverse events.

Comparison 1 Terbinafine (2‐4 weeks) versus griseofulvin (6‐8 weeks); short treatment duration; 6‐24 weeks follow‐up, Outcome 3 Secondary outcome: proportion of participants with clinical cure only.

Comparison 1 Terbinafine (2‐4 weeks) versus griseofulvin (6‐8 weeks); short treatment duration; 6‐24 weeks follow‐up, Outcome 4 Secondary outcome: percentage of drop‐outs as a surrogate for participant adherence.

Comparison 2 Terbinafine (6 weeks) versus griseofulvin (6 weeks) in Trichophyton infections; medium treatment duration; 10 weeks follow‐up, Outcome 1 Primary outcome: complete cure, i.e. clinical and mycological cure.

Comparison 2 Terbinafine (6 weeks) versus griseofulvin (6 weeks) in Trichophyton infections; medium treatment duration; 10 weeks follow‐up, Outcome 2 Primary outcome: drug‐related adverse events.

Comparison 2 Terbinafine (6 weeks) versus griseofulvin (6 weeks) in Trichophyton infections; medium treatment duration; 10 weeks follow‐up, Outcome 3 Primary outcome: severe adverse events.

Comparison 2 Terbinafine (6 weeks) versus griseofulvin (6 weeks) in Trichophyton infections; medium treatment duration; 10 weeks follow‐up, Outcome 4 Secondary outcomes: proportion of participants with clinical cure only.

Comparison 3 Terbinafine, medium‐ (6‐8 weeks) and long‐term (10‐12 weeks) treatment versus griseofulvin in Microsporum infections; 10‐16 weeks follow‐up, Outcome 1 Primary outcome: complete cure, i.e. clinical and mycological cure.

Comparison 3 Terbinafine, medium‐ (6‐8 weeks) and long‐term (10‐12 weeks) treatment versus griseofulvin in Microsporum infections; 10‐16 weeks follow‐up, Outcome 2 Secondary outcome: clinical cure only.

Comparison 4 Terbinafine, short‐term versus long‐term for treating Trichophyton and Microsporum infections; 12‐20 weeks follow‐up, Outcome 1 Primary outcome: complete cure, i.e. clinical and mycological cure.

Comparison 4 Terbinafine, short‐term versus long‐term for treating Trichophyton and Microsporum infections; 12‐20 weeks follow‐up, Outcome 2 Secondary outcome: clinical cure only.

Comparison 5 Terbinafine standard dose versus double dose in Microsporum infections; 20 weeks follow‐up, Outcome 1 Primary outcome: complete cure, i.e. clinical and mycological cure.

Comparison 6 Itraconazole (6 and 2 weeks) versus griseofulvin (6 weeks) in Trichophyton and Microsporum infections, Outcome 1 Primary outcome: complete cure, i.e. clinical and mycological cure.

Comparison 6 Itraconazole (6 and 2 weeks) versus griseofulvin (6 weeks) in Trichophyton and Microsporum infections, Outcome 2 Secondary outcome: proportion of participants with clinical cure only.

Comparison 6 Itraconazole (6 and 2 weeks) versus griseofulvin (6 weeks) in Trichophyton and Microsporum infections, Outcome 3 Secondary outcome: percentage of drop‐outs as a surrogate for participant adherence.

Comparison 7 Itraconazole versus terbinafine (both 2 weeks) in Trichophyton infections, Outcome 1 Primary outcome: complete cure, i.e. clinical and mycological cure.

Comparison 7 Itraconazole versus terbinafine (both 2 weeks) in Trichophyton infections, Outcome 2 Secondary outcome: clinical cure only.

Comparison 7 Itraconazole versus terbinafine (both 2 weeks) in Trichophyton infections, Outcome 3 Secondary outcome: percentage of drop‐outs as a surrogate for participant adherence.

Comparison 8 Ketoconazole (2‐26 weeks) versus griseofulvin (2 to 26 weeks) in Trichophyton infections; 12‐26 weeks follow‐up, Outcome 1 Primary outcome: complete cure, i.e. clinical and mycological cure.

Comparison 8 Ketoconazole (2‐26 weeks) versus griseofulvin (2 to 26 weeks) in Trichophyton infections; 12‐26 weeks follow‐up, Outcome 2 Secondary outcome: proportion of participants with clinical cure only.

Comparison 8 Ketoconazole (2‐26 weeks) versus griseofulvin (2 to 26 weeks) in Trichophyton infections; 12‐26 weeks follow‐up, Outcome 3 Secondary outcome: percentage of drop‐outs as a surrogate for participant adherence.

Comparison 9 Fluconazole (2‐6 weeks) versus griseofulvin (6 weeks); 8‐12 weeks follow‐up, Outcome 1 Primary outcome: complete cure, i.e. clinical and mycological cure.

Comparison 9 Fluconazole (2‐6 weeks) versus griseofulvin (6 weeks); 8‐12 weeks follow‐up, Outcome 2 Secondary outcome: proportion of participants with clinical cure only.

Comparison 9 Fluconazole (2‐6 weeks) versus griseofulvin (6 weeks); 8‐12 weeks follow‐up, Outcome 3 Secondary outcome: percentage of drop‐outs as a surrogate for participant adherence.

Comparison 10 Fluconazole (2‐3 weeks) versus terbinafine (2‐3 weeks) in Trichophyton infections; 12 weeks follow‐up, Outcome 1 Primary outcome: complete cure, i.e. clinical and mycological cure.

Comparison 11 Fluconazole (2‐3 weeks) versus itraconazole (2‐3 weeks) in Trichophyton infections; 12 weeks follow‐up, Outcome 1 Primary outcome: complete cure, i.e. clinical and mycological cure.

Comparison 11 Fluconazole (2‐3 weeks) versus itraconazole (2‐3 weeks) in Trichophyton infections; 12 weeks follow‐up, Outcome 2 Secondary outcome: proportion of participants with clinical cure only.

Comparison 11 Fluconazole (2‐3 weeks) versus itraconazole (2‐3 weeks) in Trichophyton infections; 12 weeks follow‐up, Outcome 3 Secondary outcome: percentage of drop‐outs as a surrogate for participant adherence.

Comparison 12 Fluconazole low dose versus higher dose (1.5, 3.0 and 6.0 mg/kg/d) in Trichophyton infections; 4 months follow‐up, Outcome 1 Primary outcome: complete cure, i.e. clinical and mycological cure.

Comparison 13 Fluconazole 3 weeks versus 6 weeks; 10 weeks follow‐up, Outcome 1 Primary outcome: complete cure, i.e. clinical and mycological cure.
| Terbinafine versus griseofulvin for children with tinea capitis | ||||||
| Patient or population: children with tinea capitis | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Griseofulvin | Terbinafine | |||||
| Proportion of participants with complete cure | 790 per 1000 | 837 per 1000 | RR 1.06 | 328 | ⊕⊕⊝⊝ | This outcome was for children infected with Trichophyton, terbinafine (2‐4 weeks) versus griseofulvin (6‐8 weeks); short treatment duration |
| Proportion of participants with complete cure | 378 per 1000 | 446 per 1000 | RR 1.18 | 1006 | ⊕⊕⊕⊝ | This outcome was for children infected with Trichophyton (T. tonsurans and T. violaceum) Terbinafine (6 weeks) versus griseofulvin (6 weeks) in Trichophyton infections; medium treatment duration |
| Proportion of participants with complete cure | 354 per 1000 | 521 per 1000 | RR 1.47 | 764 | ⊕⊕⊕⊝ | This outcome was for children infected with T. tonsurans Terbinafine (6 weeks) versus griseofulvin (6 weeks) in Trichophyton infections; medium treatment duration |
| Proportion of participants with complete cure | 451 per 1000 | 411 per 1000 | RR 0.91 | 242 | ⊕⊕⊝⊝ | This outcome was for children infected with T. violaceum Terbinafine (6 weeks) versus griseofulvin (6 weeks) in Trichophyton infections; medium treatment duration |
| Proportion of participants with complete cure | 509 per 1000 | 346 per 1000 | RR 0.68 | 334 | ⊕⊕⊕⊝ | This outcome was for children infected with Microsporum. Terbinafine medium‐ (6 to 8 weeks) and long‐term (10 to 12 weeks) treatment versus griseofulvin |
| Proportion of participants with complete cure | 600 per 1000 | 270 per 1000 (90 to 810) | RR 0.45 (0.15 to 1.35) | 21 (1 study) | ⊕⊝⊝⊝ | This outcome was for children infected with Microsporum. Terbinafine short‐term (4 weeks) versus griseofulvin |
| Adverse events attributed to the study drugs | 83 per 1000 | 92 per 1000 | RR 1.11 | 1549 | ⊕⊕⊕⊝ | This outcome was for children infected with Trichophyton and Microsporum Terbinafine (6 weeks) versus griseofulvin (6 weeks), medium treatment duration |
| Severe adverse events | 6 per 1000 | 6 per 1000 | RR 0.97 | 1549 | ⊕⊕⊕⊝ | This outcome was for children infected with Trichophyton and Microsporum Terbinafine (6 weeks) versus griseofulvin (6 weeks), medium treatment duration |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aDowngraded one level because 1 of the 3 studies was at high risk of bias, the other two studies were at unclear risk of bias. | ||||||
| Itraconazole versus griseofulvin for children infected with Trichophyton and Microsporum | |||||
| Patient or population: children infected with Trichophyton and Microsporum | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Griseofulvin | Itraconazole | ||||
| Proportion of participants with complete cure | 910 per 1000 | 838 per 1000 | RR 0.92 | 134 | ⊕⊝⊝⊝ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| aDowngraded one level because both studies were at unclear risk of bias. | |||||
| Itraconazole versus terbinafine in children infected with Trichophyton | |||||
| Patient or population: children infected with Trichophyton | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Terbinafine | Itraconazole | ||||
| Proportion of participants with complete cure | 788 per 1000 | 732 per 1000 | RR 0.93 | 160 | ⊕⊕⊝⊝ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| aDowngraded one level because both studies were at unclear risk to bias. | |||||
| Ketoconazole versus griseofulvin in children infected with Trichophyton | ||||||
| Patient or population: children infected with Trichophyton | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Griseofulvin | Ketoconazole | |||||
| Proportion of participants with complete cure Follow‐up: 12 weeks | 964 per 1000 | 733 per 1000 (598 to 906) | RR 0.76 (0.62 to 0.94) | 62 | ⊕⊕⊝⊝ | Ketoconazole (12 weeks) versus griseofulvin (12 weeks) |
| Proportion of participants with complete cure Follow‐up: 26 weeks | 1000 per 1000 | 920 per 1000 (810 to 1000) | RR 0.92 (0.81 to 1.03) | 62 (1 study) | ⊕⊕⊝⊝ | Ketoconazole (up to 26 weeks) versus griseofulvin (up to 26 weeks) |
| Proportion of participants with complete cure Follow‐up: 12 weeks | 543 per 1000 | 484 per 1000 (310 to 755) | RR 0.89 (0.57 to 1.39) | 79 (1 study) | ⊕⊕⊝⊝ | Ketoconazole (12 weeks) versus griseofulvin (12 weeks) |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aDowngraded one level because the study was at high risk of bias. | ||||||
| Fluconazole versus griseofulvin in children with tinea capitis | |||||
| Patient or population: children with tinea capitis | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Griseofulvin | Fluconazole | ||||
| Proportion of participants with complete cure | 449 per 1000 | 413 per 1000 | RR 0.92 | 615 | ⊕⊕⊕⊝ |
| Proportion of participants with complete cure | 322 per 1000 | 341 per 1000 | RR 1.06 | 361 | ⊕⊕⊝⊝ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| aDowngraded one level because one of the three studies was at high risk of bias, the other two were at unclear risk of bias. | |||||
| Fluconazole versus terbinafine for children infected with Trichophyton | |||||
| Patient or population: children infected with Trichophyton | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Terbinafine | Fluconazole | ||||
| The proportion of participants with complete cure | 940 per 1000 | 818 per 1000 | RR 0.87 | 100 | ⊕⊕⊝⊝ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| a Downgraded one level because the study was at unclear risk of bias. | |||||
| Fluconazole versus itraconazole in children infected with Trichophyton | |||||
| Patient or population: children infected with Trichophyton | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Itraconazole | Fluconazole | ||||
| Proportion of participants with complete cure Follow‐up:12 weeks | 820 per 1000 | 820 per 1000 | RR 1.00 | 100 | ⊕⊕⊝⊝ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| a Downgraded one level because the study was at unclear risk of bias. | |||||
| Different durations of fluconazole in children infected with T. tonsurans and M. canis | |||||
| Patient or population: children infected with T. tonsurans and M. canis Comparison: fluconazole (6 weeks duration) | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | |
| Assumed risk | Corresponding risk | ||||
| Fluconazole ( 6 weeks duration) | Fluconazole ( 3 weeks duration) | ||||
| Proportion of participants with complete cure Follow‐up: 8‐12 weeks | 341 per 1000 | 300 per 1000 | RR 0.88 | 491 | ⊕⊕⊝⊝ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | |||||
| GRADE Working Group grades of evidence | |||||
| a Downgraded one level because the study was at unclear risk of bias. | |||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Primary outcome: complete cure, i.e. clinical and mycological cure Show forest plot | 5 | 477 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [0.94, 1.24] |
| 1.1 Trichophyton infections | 3 | 328 | Risk Ratio (M‐H, Random, 95% CI) | 1.06 [0.98, 1.15] |
| 1.2 Microsporum infections | 1 | 21 | Risk Ratio (M‐H, Random, 95% CI) | 0.45 [0.15, 1.35] |
| 1.3 Mixed Trichophyton/Microsporum infections | 2 | 128 | Risk Ratio (M‐H, Random, 95% CI) | 1.24 [0.64, 2.42] |
| 2 Primary outcome: adverse events Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2.1 Drug‐related adverse events | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Secondary outcome: proportion of participants with clinical cure only Show forest plot | 3 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3.1 2‐week terbinafine | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 4‐week terbinafine | 3 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Secondary outcome: percentage of drop‐outs as a surrogate for participant adherence Show forest plot | 4 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Primary outcome: complete cure, i.e. clinical and mycological cure Show forest plot | 1 | 1006 | Risk Ratio (M‐H, Random, 95% CI) | 1.18 [0.74, 1.88] |
| 1.1 T. tonsurans infections | 1 | 764 | Risk Ratio (M‐H, Random, 95% CI) | 1.47 [1.22, 1.77] |
| 1.2 T. violaceum infections | 1 | 242 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.68, 1.24] |
| 2 Primary outcome: drug‐related adverse events Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Primary outcome: severe adverse events Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 4 Secondary outcomes: proportion of participants with clinical cure only Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 4.1 T. tonsurans infections | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 T. violaceum infections | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Primary outcome: complete cure, i.e. clinical and mycological cure Show forest plot | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.1 Medium terbinafine treatment duration (6‐8 weeks) | 2 | 334 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.53, 0.86] |
| 1.2 Long terbinafine treatment duration (10‐12 weeks) | 1 | 95 | Risk Ratio (M‐H, Random, 95% CI) | 0.51 [0.34, 0.76] |
| 2 Secondary outcome: clinical cure only Show forest plot | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 2.1 Medium terbinafine treatment duration (6‐8 weeks) | 2 | 334 | Risk Ratio (M‐H, Random, 95% CI) | 0.76 [0.63, 0.91] |
| 2.2 Long terbinafine treatment duration (10‐12 weeks) | 1 | 95 | Risk Ratio (M‐H, Random, 95% CI) | 0.69 [0.52, 0.92] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Primary outcome: complete cure, i.e. clinical and mycological cure Show forest plot | 5 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.1 1‐2 weeks versus 4 weeks | 4 | 552 | Risk Ratio (M‐H, Random, 95% CI) | 0.73 [0.62, 0.86] |
| 1.2 Medium term (6‐8 weeks) versus long term (10‐12 weeks) | 1 | 135 | Risk Ratio (M‐H, Random, 95% CI) | 1.45 [0.97, 2.17] |
| 2 Secondary outcome: clinical cure only Show forest plot | 4 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 2.1 1‐2 weeks versus 4 weeks | 3 | 470 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.67, 1.06] |
| 2.2 Medium term (6‐8 weeks) versus long term (10‐12 weeks) | 1 | 135 | Risk Ratio (M‐H, Random, 95% CI) | 1.19 [0.90, 1.56] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Primary outcome: complete cure, i.e. clinical and mycological cure Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Primary outcome: complete cure, i.e. clinical and mycological cure Show forest plot | 2 | 134 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.81, 1.05] |
| 2 Secondary outcome: proportion of participants with clinical cure only Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Secondary outcome: percentage of drop‐outs as a surrogate for participant adherence Show forest plot | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Primary outcome: complete cure, i.e. clinical and mycological cure Show forest plot | 2 | 160 | Risk Ratio (M‐H, Random, 95% CI) | 0.93 [0.72, 1.19] |
| 2 Secondary outcome: clinical cure only Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Secondary outcome: percentage of drop‐outs as a surrogate for participant adherence Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Primary outcome: complete cure, i.e. clinical and mycological cure Show forest plot | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.1 Ketoconazole (12 weeks) versus griseofulvin (12 weeks) assessed at 12 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Ketoconazole (up to 26 weeks) versus griseofulvin (up to 26 weeks) assessed at 26 weeks | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 Ketoconazole (12 weeks) versus griseofulvin (12 weeks) | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Secondary outcome: proportion of participants with clinical cure only Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Secondary outcome: percentage of drop‐outs as a surrogate for participant adherence Show forest plot | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Primary outcome: complete cure, i.e. clinical and mycological cure Show forest plot | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.1 Short‐term (2‐4 weeks) fluconazole | 3 | 500 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.81, 1.05] |
| 1.2 Medium‐term (6 weeks) fluconazole | 1 | 361 | Risk Ratio (M‐H, Random, 95% CI) | 1.06 [0.77, 1.46] |
| 2 Secondary outcome: proportion of participants with clinical cure only Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Secondary outcome: percentage of drop‐outs as a surrogate for participant adherence Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Primary outcome: complete cure, i.e. clinical and mycological cure Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Primary outcome: complete cure, i.e. clinical and mycological cure Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Secondary outcome: proportion of participants with clinical cure only Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3 Secondary outcome: percentage of drop‐outs as a surrogate for participant adherence Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Primary outcome: complete cure, i.e. clinical and mycological cure Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.1 1.5 mg versus 3.0 mg | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 1.5 mg versus 6.0 mg | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 3.0 mg versus 6.0 mg | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Primary outcome: complete cure, i.e. clinical and mycological cure Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |