Terapia medicamentosa para sintomas associados à ansiedade em pacientes adultos em cuidados paliativos.
Resumo
Introdução
Esta é a atualização de uma revisão Cochrane publicada originalmente em 2004 (Issue 1) e que já foi atualizada em 2012 (Issue 10). A ansiedade é comum em pacientes em cuidados paliativos. Ela pode ser uma resposta natural diante da incerteza que cerca o diagnóstico de uma doença terminal ou da morte iminente. Entretanto, a ansiedade por si só pode se tornar um problema clínico significativo.
Objetivos
Avaliar a efetividade da terapia medicamentosa para tratar sintomas de ansiedade em adultos com doença terminal progressiva, que estão no último ano de vida.
Métodos de busca
Para esta atualização, rodamos a busca em maio de 2016. Pesquisamos as seguintes bases de dados: CENTRAL, MEDLINE (Ovid), Embase (Ovid), CINAHL (EBSCO), PsychLIT (Silver Platter) e PsycINFO (Ovid). Fizemos buscas em sete plataformas de registros de ensaios clínicos e em outras sete plataformas de registros de ensaios clínicos da industria farmacêutica. Fizemos buscas manuais nos livros de resumos das conferências da European Association of Palliative Care.
Critério de seleção
Selecionamos ensaios clínicos randomizados que avaliaram o efeito da terapia medicamentosa para o tratamento de sintomas de ansiedade em adultos em cuidados paliativos, ou seja, pessoas com uma doença progressiva terminal que não respondia mais a tratamento curativo de longo prazo. Os participantes podiam também ter doença cardíaca respiratória e neurológica avançadas (e até demência). O grupo de comparação podia ser um placebo, outra terapia medicamentosa, diferentes doses do mesmo remédio, ou uma intervenção não medicamentosa, como aconselhamento, terapia cognitivo‐comportamental ou terapias de relaxamento.
Coleta dos dados e análises
Dois revisores independentes selecionaram os títulos e resumos para identificar artigos potencialmente relevantes para inclusão na revisão. Dois revisores independentes leram esses artigos e avaliaram se preenchiam os critérios de inclusão da revisão. Pretendíamos extrair os dados dos artigos relevantes, incluindo informações sobre eventos adversos, e fazer a avaliação da qualidade metodológica (risco de viés) desses estudos. Pretendíamos avaliar a qualidade da evidência usando o GRADE e criar uma tabela de “sumário dos achados”.
Principais resultados
Nesta atualização, identificamos 707 citações potencialmente relevantes e selecionamos 10 artigos para leitura na íntegra. Após avaliarmos esses textos completos, excluímos oito estudos, e dois (em andamento) estão aguardando classificação, pois não oferecem informações suficientes para tomarmos uma decisão. Portanto, nessa atualização, não encontramos nenhum estudo que preenchesse nossos critérios de inclusão. Na versão original da revisão, identificamos seis estudos potencialmente relevantes. Porém, após a leitura na íntegra desses estudos, todos foram excluídos. Na atualização de 2012, selecionamos dois estudos potencialmente relevantes para leitura na íntegra, porém ambos foram excluídos. Portanto, não encontramos estudos sobre a efetividade de medicamentos para tratar ansiedade em pacientes sob cuidados paliativos.
Conclusão dos autores
Existe uma carência de evidências para se chegar a uma conclusão sobre a efetividade da terapia medicamentosa para o tratamento da ansiedade em adultos em cuidados paliativos. Até esta data, não encontramos estudos que preencham os critérios de inclusão desta revisão. Estamos aguardando mais informações de dois estudos que poderão ser incluídos em uma futura atualização da revisão. Estudos randomizados controlados que avaliem o manejo da ansiedade como desfecho primário são necessários para estabelecer os benefícios e riscos da terapia medicamentosa para o tratamento da ansiedade em pacientes em cuidados paliativos.
PICO
Resumo para leigos
Medicamentos para ajudar a reduzir a ansiedade em pessoas próximas ao fim da vida devido a doenças
Pergunta da revisão
Queríamos responder à seguinte pergunta: "qual é a eficácia dos remédios que controlam a ansiedade para pessoas que estão no último ano de sua vida devido a uma doença terminal?"
Contexto
É comum as pessoas que sofrem com uma doença terminal e que estão no último ano de suas vidas ficaram ansiosas ou preocupadas. Existem muitas razões para essa ansiedade. Por exemplo, as pessoas podem ficar preocupadas com a dor e com o tratamento, com o fato de terem que depender de outras pessoas e de terem que enfrentar a morte. A ansiedade pode dificultar a forma como as pessoas lidam com sua doença. A ansiedade pode piorar outros problemas e dificultar o manejo da dor ou da sensação de falta de ar. Por isso, se possível, é importante tentar reduzir as preocupações das pessoas que estão na fase final de suas vidas devido a uma doença. Alguns medicamentos podem ajudar a reduzir a ansiedade. No entanto, há poucos estudos sobre a ansiedade que acomete as pessoas que se aproximam do fim da vida. Muitas vezes, o tratamento oferecido para as pessoas que sofrem de ansiedade não é adequado.
Procuramos encontrar estudos que tivessem avaliado qual era a eficácia dos remédios para reduzir a ansiedade de adultos na fase final de suas vidas. Estávamos interessados em estudos que comparassem o uso de um remédio para ansiedade versus qualquer dos seguintes: não usar nenhum remédio, usar outro tipo de remédio, usar uma dosagem diferente do mesmo remédio, fazer terapia de relaxamento ou terapias que envolviam conversar com alguém. Procuramos por estudos que tivessem medido a ansiedade dos participantes. Queríamos achar pesquisas projetadas para garantir que os participantes tivessem a mesma chance de cair em um dos grupos de tratamento testados em cada estudo. Esta revisão foi feita pela primeira vez em 2004 e atualizada em 2012. Esta é a segunda atualização. Incluímos nesta revisão todos estudos que tivessem sido publicados até maio de 2016.
Principais resultados
Não encontramos nenhum estudo que pudesse ser incluído nesta revisão. Não havíamos encontrado estudos para incluir na revisão original de 2004 ou na atualização de 2012. Existe uma carência de estudos que avaliem o efeito dos remédios para reduzir a ansiedade dos adultos que estão na fase final de suas vidas. Encontramos dois estudos relevantes que talvez possam ser incluídos em uma futura atualização dessa revisão. Porém, precisamos ter mais informações sobre esses estudos para tomarmos essa decisão. A ansiedade pode ter um grande impacto sobre como uma pessoa lida com sua doença. Portanto, precisamos saber como reduzir esta ansiedade. Estudos de boa qualidade sobre esse tema são necessários.
Authors' conclusions
Background
Description of the condition
This is the second update of the review "Drug therapy for anxiety in adult palliative care patients" originally published in Issue 1, 2004 (Jackson 2004) of the Cochrane Library and published as a first update in Issue 10, 2012 (Candy 2012).
Anxiety can be an intractable and crippling condition. It impacts on the person's ability to cope emotionally and to function socially, and may make physical symptoms more difficult to manage (Spencer 2010). In the advanced stages of a progressive, life‐limiting illness it may also manifest with concomitant depression and result in the person experiencing even greater difficulties (Mitchell 2011; Wilson 2007). The symptoms of anxiety include feelings of apprehension, fear, irritability and tension. Cognitively, anxiety manifests itself as excessive worry or difficulty concentrating. Behavioural symptoms involve avoidant or compulsive tendencies, and physical and somatic symptoms include diarrhoea, sweating, restlessness, fatigue, and insomnia. People may also present with more acute symptoms including palpitations, tachycardia, and shortness of breath (Thielking 2003). Anxiety is a term for a number of disorders, specifically generalised anxiety disorders (GAD), substance‐induced anxiety, adjustment disorders, obsessive‐compulsive disorders, specific phobias such as in response to medical interventions, panic disorders and post‐traumatic stress disorder (DSM‐5 2013). GAD and panic disorder were found in one study to be the most common anxiety disorders in advanced disease (Wilson 2007). The importance of a holistic approach to managing all symptoms including anxiety has been reaffirmed by frameworks around palliative and end of life care including Ambitions for Palliative and End of Life Care (National Palliative and End of Care 2015) and National Institute for Health and Care Excellence (NICE) guidance on end of life care (NICE 2011a).
In people with a progressive life‐limiting illness, anxiety can be a natural reaction to the extraordinary psychological and physical challenges to be faced including the prognostic and treatment uncertainties often associated with the situation. The prevalence of symptoms of excessive anxiety is under researched, but it is one of the most common reasons for a psychiatric consultation in this patient group (Roth 2007). Anxiety can increase because of a broad range of concerns faced, such as how well symptoms will be managed, increasing dependency on other people, increased social isolation, confrontation with existential issues, and a growing inability to support and be with family and friends. Anxiety may also occur as the result of poorly controlled symptoms, such as pain, or the use of medications. Despite these known risks, anxiety in terminally ill people is underdiagnosed and undertreated, and is less extensively researched than depression (Kolva 2011; Wilson 2007).
One of the challenges in palliative care is to distinguish between excessive or maladaptive anxiety, and normal distress. There are numerous causes; in particular, it has been highly correlated with uncontrolled pain (Payne 1995). In addition, many studies looking at psychiatric states in people with a life‐limiting diagnosis do not clearly separate their assessments of depression and anxiety states or define clearly their study populations with respect to where a person is on their illness journey. This makes it more difficult to identify if anxiety is associated with specific stages in an illness journey, such as the palliative phase.
Anxiety may be a manifestation of a change in metabolic state such as hypoxia or hypoglycaemia, or in the dying phase (last 48 hours of life) as part of the result of multiple organ failure. Certain medications commonly used in caring for people near the end of life may produce symptoms that can be confused with anxiety, for example, akathisia or motor restlessness. These include phenothiazines (e.g. prochlorperazine), butyrophenones (e.g. haloperidol), methotrimeprazine and metoclopramide. Abrupt discontinuation of certain substances can also lead to withdrawal and precipitate an anxiety state, for instance alcohol, nicotine, anticonvulsants, benzodiazepines, clonidine, corticosteroids, opioids and sedative‐hypnotics (Maguire 1993). Numerous other medications and substances have been associated with anxiety symptoms and, therefore, a thorough medication history should always precede changes in a drug therapy regimen (Jackson 2000).
Description of the intervention
While there are clinical guidelines for the treatment of clinically significant anxiety (Baldwin 2005; NICE 2011b; NICE 2015), few are specific to palliative care where treatments may need to be different because of the added psychological and physical burden of living with a terminal disease (National Consensus Project 2009; NICE 2004; NICE 2015). Treatment in palliative care can include behavioural techniques, such as cognitive behavioural therapy (CBT) (Moorey 2009), and drug therapy. In deciding on treatment options, the clinician has to consider whether a person has both sufficient energy to engage with non‐pharmacological interventions and the time needed to establish the benefit of such interventions. In deciding whether a pharmacological approach may be useful, the severity of the person's symptoms and the degree to which they interfere with overall function and well‐being are important factors to consider. In addition, the clinician needs to assess whether the person has compromised hepatic and renal function, and must also consider the potential adverse effects of the drug therapy. Short‐acting benzodiazepines, such as lorazepam and oxazepam, are often the drugs of choice in terminally ill people (Breitbart 1996; Henderson 2006; Noyes 1998; Roth 2007). However, they may not be suitable for everyone because of adverse effects such as excessive sedation and confusion, which are associated with an increased risk of falls. Furthermore, if benzodiazepines are given for longer than a few weeks, there is the potential risk of physical dependency. The palliative care literature lists a variety of other potentially useful agents in the management of anxiety including antidepressants, buspirone, chlorpromazine, haloperidol, hydroxyzine, levomepromazine, ketamine and atypical antipsychotic drugs (e.g. olanzapine, risperidone) (Khojainova 2002; Mintzer 2001).
How the intervention might work
This review explores the evidence for the effectiveness of drugs to treat anxiety in palliative care patients. These medications have a variety of mechanisms of action, including some drugs where the exact mechanism is unknown. Drug therapy for treatment of anxiety can be considered to work from two distinct approaches. The first is related to the mechanism of action at the level of neurotransmitters in the central nervous system. These include dopamine, gamma amino butyric acid (GABA), noradrenaline and serotonin.
The second approach is aimed at reducing the physical symptoms of anxiety that result from autonomic hyperactivity, such as tremors and palpitations. In some instances, it is these physical manifestations that worsen the cognitive aspects of anxiety, such as an inability to concentrate or sense of foreboding. The use of drugs such as beta‐blockers, which slow the heart rate, may reduce or eliminate these physical manifestations and so reduce the overall impact of anxiety. The use of agents to treat physical manifestations may reduce or possibly eliminate the need for agents aimed at altering neurotransmitter systems.
Why it is important to do this review
Anxiety is a distressing condition that is particularly common and troublesome for people dealing with the advanced stages of a life‐limiting condition. Excessive anxiety can manifest itself as both physical and emotional symptoms and can reduce a person's ability to cope physically and mentally with the life‐limiting condition. Drugs represent one way of allaying a person's anxiety, but choosing the most appropriate drug is dependent on the clinician having access to evidence reviewing the effectiveness of drugs for anxiety in people with life‐limiting conditions. To our knowledge prior to the original review in 2004 there had been no systematic search of the international literature for evidence regarding the effectiveness of drug therapy for anxiety disorders in palliative care patients.
Objectives
To assess the effectiveness of drug therapy for treating symptoms of anxiety in adults with a progressive life‐limiting illness who are thought to be in their last year of life.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs).
Types of participants
Adult palliative care patients (aged 18 years or older) whose symptoms of anxiety were described by the trial authors as beyond what could be seen as normal in this patient group. This could be captured as a score equivalent to clinically significant symptoms on a validated scale, such as the Hamilton Anxiety Rating Scale (HAM‐A) (Hamilton 1959).
We included trials where anxiety was described as a disorder such as adjustment disorder, obsessive‐compulsive disorder, phobia, panic disorder, post‐traumatic stress disorder or GAD. We sought to verify that symptoms reported as clinically significant were measured using validated scales, and if the population was described as having an anxiety disorder (specifically GAD, substance‐induced anxiety, adjustment disorders, obsessive‐compulsive disorders, specific phobias such as in response to medical interventions, panic disorders and post‐traumatic stress disorder) that it was defined using the International Classification of Disease (ICD) (ICD‐10 2010) or the Diagnostic and Statistical Manual of Mental Disorders (DSM‐III 1980; DSM‐R 1987; DSM‐IV 1994; DSM‐IV‐TR 2000; DSM‐5 2013).
For the purposes of the review, we defined palliative care patients as people with a progressive, life‐limiting illness, no longer responsive to disease‐modifying treatments who were thought to be in the last year (or so) of life and were, or would be, eligible to receive palliative care. We did not include studies in which participants were in the last 24 to 48 hours of life. At this time, symptoms of anxiety may also be in part a manifestation of irreversible processes such as multiple organ failure, and treatment may differ from that considered in earlier phases of the disorder.
Types of interventions
Interventions for anxiety included any type of drug therapy, for example, 5‐HT3 receptor antagonists, anxiolytic agents, antidepressive agents, antipsychotic and atypical antipsychotic agents, benzodiazepines, butyrophenones, phenothiazines, antihistamines, barbiturates, sedative hypnotics, antiepileptic drugs, ketamine and beta‐blockers. We did not include any non‐conventional drugs, such as herbal medicines.
Comparator treatments included placebo; another drug therapy or different dose schedule; or a non‐drug intervention such as counselling, CBT or relaxation therapies.
Types of outcome measures
Primary outcomes
-
Anxiety: studies were eligible for inclusion if they reported anxiety measured using a validated scale which measures either anxiety alone or as a subscale. Examples of validated instruments include the following:
-
-
Hamilton Anxiety Rating Scale (HAM‐A) (Hamilton 1959);
-
Symptom Check List‐90 (SCL‐90) anxiety sub scale (Derogatis 1983);
-
Diagnostic Interview Schedule (DIS) (Robins 1981);
-
Affects Balance Scale (ABS) (Bradburn 1969);
-
Hospital Anxiety and Depression Scale (HADS) (Zigmond 1983);
-
Edmonton Symptom Assessment System (ESAS) (Bruera 1991);
-
Profile of Mood States (Pollock 1979);
-
Rotterdam Symptoms Checklist (de Haes 1996);
-
Palliative care Outcome Scale (or Patient Outcome Scale) (Hearn 1999);
-
Support Team Assessment Schedule (STAS) (Higginson 1993);
-
Beck Anxiety Inventory (BAI) (Beck 1988);
-
State‐Trait Anxiety Inventory (STAI) (Spielberger 1983).
-
We reported anxiety outcomes assessed at one week.
Secondary outcomes
-
Depression measured using any validated scale either alone or as a subscale. Examples of validated instruments include:
-
Hospital Anxiety and Depression Scale (HADS) (Zigmond 1983);
-
Beck Depression Inventory (BDI) (Beck 1961).
-
-
Breathlessness measured using a validated scale. An example includes:
-
St George's Respiratory Questionnaire (Jones 1991).
-
-
Insomnia measured using any validated scale. Examples include:
-
Insomnia Severity Index (Bastien 2001);
-
Pittsburgh Sleep Quality Index (Buysse 1989);
-
Athens Insomnia Scale (Soldatos 2000).
-
-
Participants experiencing any adverse events, such as sedation or failure of treatment.
-
Withdrawals due to lack of efficacy, adverse events or any cause.
Search methods for identification of studies
Electronic searches
To identify studies for inclusion in this review, we developed detailed search strategies for each electronic database searched. These were based on the search strategy developed for MEDLINE but revised appropriately for each database. The search strategy used in the original review run in 2003 is reported in Appendix 1 and the search strategies used in the first update of 2012 are presented in Appendix 2, Appendix 3, Appendix 4, Appendix 5, Appendix 6, and Appendix 7. The search strategies used in 2016 for the second update of this review are reported in Appendix 8. We also updated the list of drugs included in the search and re‐ran the search for these for all years to May 2016 (see Appendix 9).
Databases searched
-
The Cochrane Central Register of Controlled Trials (CENTRAL; 2016, Issue 4) (Cochrane Register of Studies Online) (18 May 2016).
-
MEDLINE (OVID) (1966 to May week 1 2016).
-
Embase (OVID) (1980 to 16 May 2016).
-
CINAHL (EBSCO) (1982 to 18 May 2016).
-
PsychLIT (Silver Platter) (1974 to 2000).
-
PsycINFO (OVID) (1990 to May week 2 2016).
For the original review, the Cochrane Pain, Palliative & Supportive Care Register was searched to July 2003 but its contents are now captured by CENTRAL and so we did not search it for this update.
Searching other resources
We searched the following trials and pharmaceutical industry trials registers.
Trials registers searched
-
ClinicalTrials.gov (clinicaltrials.gov/) (to May 2016).
-
metaRegister of controlled trials (www.isrctn.com/page/mrct) (to May 2016).
-
ISRCTN Trials Register (www.controlled‐trials.com/isrctn) (to 2012).
-
Netherlands Trial Register (www.trialregister.nl/trialreg/index.asp) (to May 2016).
-
NIHR Clinical Research Portfolio Database (public.ukcrn.org.uk/search/) (to May 2016).
-
UMIN Japan Trial Register (www.umin.ac.jp/ctr) (to May 2016).
-
UK Clinical Trials Gateway (www.ukctg.nihr.ac.uk/default.aspx) (to May 2016).
-
World Health Organization (WHO) Portal (covers ClinicalTrials.gov; ISRCTN; Australian and New Zealand Clinical Trial Registry; Chinese Clinical Trial Register; India Clinical Trials Registry; German Clinical Trials Register; Iranian Registry of Clinical Trials; Sri Lanka Clinical Trials Registry; The Netherlands National trial Register) (www.who.int/trialsearch) (to May 2016).
For the original review and the first update, we searched the ISRCTN Trials Register (www.controlled‐trials.com/isrctn) to 2012, but its contents are captured by the WHO Portal and so we did not search it for this second update in 2017.
Pharmaceutical industry trials registers searched
-
AstraZeneca Clinical Trials (www.astrazenecaclinicaltrials.com) (to May 2016).
-
Daiichi Sankyo (www.daiichisankyo.com) (to May 2016).
-
Eisai (www.eisai.com/) (to May 2016).
-
GlaxoSmithKline Clinical Trial Register (www.gsk‐clinicalstudyregister.com) (to May 2016).
-
Lundbeck (www.lunbeck.com) (to May 2016).
-
NovartisClinicalTrials.com (www.novartis.com/) (to May 2016).
-
Roche Clinical Trial Protocol Registry (www.roche‐trials.com/main.action) (to May 2016).
Conference abstracts
For this second update of the review, we handsearched the following conference abstracts:
-
World Research Congress EAPC (2012 and 2014);
-
World Congress EAPC (2013 and 2015).
We did not search the EAPC 2016 conference abstracts as the conference was not held until June 2016.
Reference lists
We searched the reference lists of review articles.
Unpublished data
We did not seek unpublished studies.
Language
The search was not restricted by language of publication.
Data collection and analysis
Selection of studies
In this update, two review authors (SS and CM) independently assessed titles and abstracts for eligibility for inclusion in the review. We sought full‐text reports of all potentially relevant studies remaining after the initial assessment and two review authors (SS and CM) independently assessed these against our predefined inclusion criteria. We resolved any disagreements between the review authors by consulting a third review author (NP). Where we identified posters or conference abstracts which we considered potentially relevant, we sought full‐text reports of the study and, if unsuccessful, we contacted study authors to seek further information. Where English translations for studies published in another language were not available at the screening stage, we obtained full‐text reports and translated these initially using an electronic translator. We reported reasons for excluding full‐text reports. See Characteristics of excluded studies table.
Data extraction and management
We designed a data extraction form to collect the following data:
-
publication details;
-
study eligibility criteria;
-
study details (e.g. aim, start and end date, ethics approval);
-
participant characteristics (e.g. number of participants, age, sex, diagnosis of anxiety, study setting);
-
description of intervention and comparator (e.g. duration of treatment, timing, delivery, number randomised to groups);
-
outcome details (e.g. instrument used to evaluate anxiety, time points when outcomes were assessed, withdrawals).
Assessment of risk of bias in included studies
We planned for two review authors (SS and CM) to independently assess risk of bias for each study, using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), with any disagreements resolved by discussion. We planned to complete a 'Risk of bias' table for each included study using the 'Risk of bias' tool in Review Manager 5 (RevMan 2014).
We aimed to assess the following for each study.
-
Random sequence generation (checking for possible selection bias). We planned to assess the method used to generate the allocation sequence as: low risk of bias (any truly random process, e.g. random number table; computer random number generator); unclear risk of bias (method used to generate sequence not clearly stated). We planned to exclude studies using a non‐random process (e.g. odd or even date of birth; hospital or clinic record number).
-
Allocation concealment (checking for possible selection bias). The method used to conceal allocation to interventions prior to assignment determines whether intervention allocation could have been foreseen in advance of, or during, recruitment, or changed after assignment. We planned to assess the methods as: low risk of bias (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes); unclear risk of bias (method not clearly stated). We aimed to exclude studies that did not conceal allocation (e.g. open list).
-
Blinding of participants and personnel (checking for possible performance bias). We planned to assess the methods used to blind study participants and personnel from knowledge of which intervention a participant received. We aimed to assess methods as: low risk of bias (study stated that it was blinded and described the method used to achieve blinding, such as identical tablets matched in appearance or smell, or a double‐dummy technique); unclear risk of bias (study stated that it was blinded but did not provide an adequate description of how it was achieved). Studies that were not double‐blind were considered to have high risk of bias.
-
Blinding of outcome assessment (checking for possible detection bias). We aimed to assess the methods used to blind study participants and outcome assessors from knowledge of which intervention a participant received. We planned to assess the methods as: low risk of bias (study had a clear statement that outcome assessors were unaware of treatment allocation, and ideally described how this was achieved); unclear risk of bias (study stated that outcome assessors were blind to treatment allocation but lacked a clear statement on how it was achieved). We considered studies where outcome assessment was not blinded as having a high risk of bias.
-
Selective reporting (checking for reporting bias). We aimed to assess whether primary and secondary outcome measures were prespecified and whether these were consistent with those reported. We aimed to assess selective reporting as: low risk of bias (studies reported primary and secondary outcomes); high risk of bias (not all prespecified outcomes reported or only for certain data collection time points).
-
Incomplete outcome data (checking for possible attrition bias due to the amount, nature and handling of incomplete outcome data). We planned to assess the methods used to deal with incomplete data as: low risk of bias (less than 10% of participants did not complete the study or used 'baseline observation carried forward' analysis), or both; unclear risk of bias (used 'last observation carried forward' analysis); high risk of bias (used 'completer' analysis).
-
Size of study (checking for possible biases confounded by small size). We aimed to assess studies as being at low risk of bias (200 participants or greater per treatment arm); unclear risk of bias (50 to 199 participants per treatment arm); high risk of bias (fewer than 50 participants per treatment arm)
Measures of treatment effect
We planned to analyse dichotomous data as odds ratios and 95% confidence intervals (CI) and continuous data as mean difference and 95% CI.
Unit of analysis issues
For any RCTs using a cross‐over design, we planned to use only data from the first comparative phase prior to cross‐over. This decision was based on the possibility of a carry‐over of treatment effect from the drug evaluation or a comparative treatment.
Dealing with missing data
For this review, we expected a significant loss to follow‐up due to participants' declining health. We planned to report trial attrition rates in the 'Risk of bias' table. This would have included, if available, reasons for attrition per treatment arm. Where study data were missing but might have been available, we planned to contact the authors to obtain missing outcome data where possible. We planned not to exclude trials on the basis of missing data.
Assessment of heterogeneity
If meta‐analysis had been possible, we planned to use the I² statistic to assess heterogeneity among the trials in each analysis. If we identified substantial heterogeneity (i.e. I² greater than 50%), we aimed to report it and explore possible causes by performing prespecified subgroup analysis.
Assessment of reporting biases
If meta‐analysis had been possible using 10 or more studies, we planned to explore publication bias using Egger's test and by inspection of funnel plots for symmetry.
Data synthesis
We planned to combine study data to provide a pooled effect estimate using a fixed‐effect model. If we had found no substantial heterogeneity, we planned to use a random‐effects model to check the robustness of the fixed‐effect model. If substantial statistical heterogeneity had been observed, we would have used the random‐effects model a priori.
If we had found studies that reported a mixture of change‐from‐baseline and final value scores, we would have only combined data if the studies reported the outcome using the same measurement scale.
Where there were insufficient studies to undertake a meta‐analysis, we planned to combine individual studies in a narrative review.
Quality of the evidence
We planned that two review authors (SS and CM) would independently rate the quality of the outcomes. We planned to use the GRADE system to rank the quality of the evidence using the GRADEprofiler Guideline Development Tool software (GRADEpro GDT 2015), and the guidelines provided in Section 12.2 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
The GRADE approach uses five considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the quality of the body of evidence for each outcome. The GRADE system uses the following criteria for assigning grade of evidence:
-
high: we are very confident that the true effect lies close to that of the estimate of the effect;
-
moderate: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of effect, but there is a possibility that it is substantially different;
-
low: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect;
-
very low: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect.
We planned to decrease the grade rating by one (‐1) or two (‐2) if we identified:
-
serious (‐1) or very serious (‐2) limitation to study quality;
-
important inconsistency (‐1);
-
some (‐1) or major (‐2) uncertainty about directness;
-
imprecise or sparse data (‐1);
-
high probability of reporting bias (‐1).
'Summary of findings' table
We planned to include six 'Summary of findings' tables to present the main findings for the primary outcome (anxiety) and five secondary outcomes (depression, breathlessness, insomnia, adverse events and withdrawals) in a transparent and simple tabular format. In particular, we planned to include key information concerning the quality of evidence, the magnitude of effect of the interventions examined, and the sum of available data.
Subgroup analysis and investigation of heterogeneity
If three or more studies reported relevant data, we planned to perform the following subgroup analyses:
-
men versus women;
-
mild or moderate anxiety versus severe anxiety;
-
follow‐up no greater than one month versus follow‐up greater than one month.
Sensitivity analysis
We planned to perform sensitivity analyses to explore the influence of the following factors:
-
excluding unpublished studies;
-
excluding studies considered at high risk of selection bias in terms of adequate allocation concealment, detection bias in terms of blinded outcome assessment and attrition bias due to follow‐up of less than 80% of participants in each arm;
-
excluding studies using the following filters:
-
industry funded;
-
non‐validated scales used for measuring effect;
-
non‐validated diagnostic criteria.
-
Results
Description of studies
Results of the search
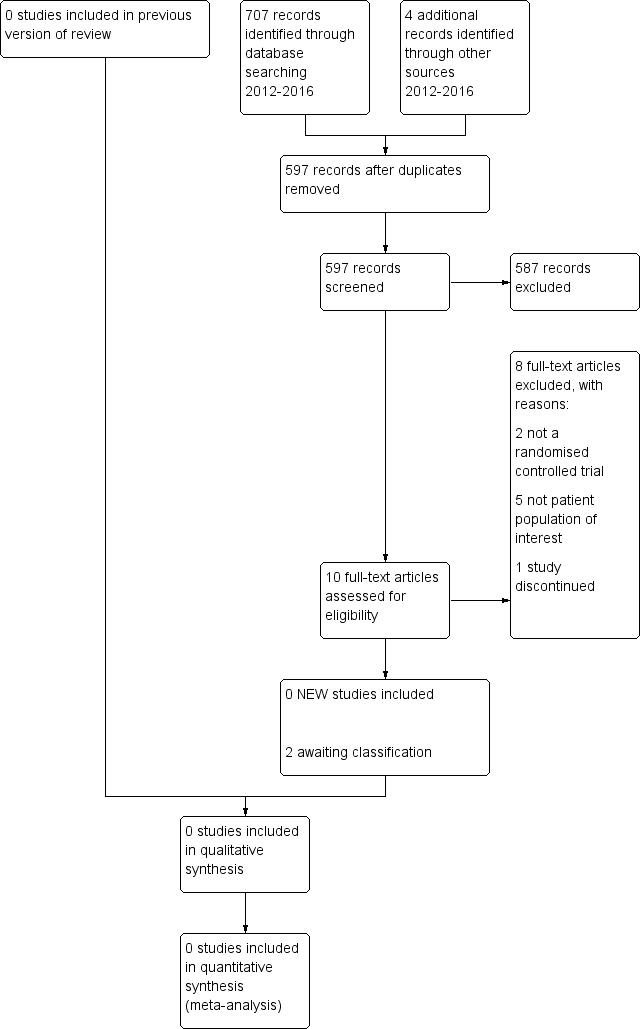
We retrieved 707 potentially relevant studies from the electronic searches and four from other sources for this second update. After removing duplicates, we screened 597 articles for inclusion in the review. We assessed full‐text reports of 10 articles. Figure 1 shows the results of the search.

Study flow diagram.
Included studies
Of the 10 full‐text reports we assessed for inclusion in this update, we did not identify any studies fulfilling our criteria.
Excluded studies
In this update, we excluded eight reports for the following reasons: five did not include a patient population of interest, specifically it was considered that three included participants with depression and not anxiety (Centeno 2012; Dauchy 2015; Ng 2014), and two included participants not considered at a palliative stage of disease (Kronish 2012; Yazici 2012); two were not an RCT (Grob 2011; Irwin 2013), and one study was discontinued (Daubert 2014). See Characteristics of excluded studies table. Overall, there are 16 excluded studies.
Studies awaiting classification
Two studies provided insufficient information on which to make a decision regarding inclusion, despite attempts to contact the authors for further information (Hart 2012; Usmani 2013).
Ongoing studies
We did not identify any ongoing studies.
Risk of bias in included studies
We did not identify any relevant studies.
Effects of interventions
We did not identify any relevant studies.
Discussion
Summary of main results
We found no studies assessing the effectiveness of drug therapy for treating symptoms of anxiety in adults with a progressive life‐limiting illness and who were thought to be in their last year of life. There was a lack of RCTs; while we identified five RCTs, three studies assessed depression rather than anxiety and were thus excluded. There are two studies awaiting classification which may be included in a future update.
Overall completeness and applicability of evidence
We were unable to find any evidence of the effectiveness of drug therapy in the treatment of adult palliative care patients experiencing symptoms of anxiety.
Quality of the evidence
We did not identify any studies to include in the review and thus we are unable to assess the quality of the evidence.
Potential biases in the review process
We undertook a comprehensive search for studies, including searching trials registers and handsearching of conference abstracts with no restrictions on language of study reports. One potential problem we encountered with identifying papers for inclusion was that when first reading a paper the title and abstract might suggest that the study participants were experiencing with anxiety but, on closer inspection, participants were assessed using scales which predominantly measured depression and thus studies did not meet our inclusion criteria.
Agreements and disagreements with other studies or reviews
One systematic review of anxiety therapy for palliative care patients with cancer was undertaken at a similar time to the first update of this Cochrane Review (Nübling 2012). Nübling 2012 included four RCTs in their review but stated that they did not make recommendations for pharmacological treatments based on the findings of these four studies because of "deficiencies in the studies or the analyses." All four studies were excluded from the original Cochrane Review of 2004 as study participants were not considered those of interest for this review. Traeger 2012 examined the evidence for treatment of anxiety in people with cancer and identified two of the studies included in the Nübling 2012 review. Traeger 2012 concluded that finding evidence for effective treatments of anxiety in people with cancer is challenging as anxiety is a complex problem, thus making a diagnosis of anxiety and assessing the effects of treatment is difficult.
Study flow diagram.