Corticosteroides y agonistas beta2 de acción prolongada combinados en un solo inhalador versus placebo para la enfermedad pulmonar obstructiva crónica
Resumen
Antecedentes
Los agonistas beta 2 de acción prolongada (ABAP) y los corticosteroides inhalados (CSI) se han recomendado en las guías de tratamiento de la enfermedad pulmonar obstructiva crónica (EPOC). Su administración concurrente en un inhalador combinado puede facilitar el cumplimiento con los regímenes de medicación y mejorar su eficacia.
Objetivos
Determinar la eficacia y la seguridad de la combinación de CSI y ABAP para la EPOC estable, en comparación con placebo.
Métodos de búsqueda
Se realizaron búsquedas en el registro especializado de ensayos del Grupo Cochrane de Vías Respiratorias (Cochrane Airways Group), las listas de referencias de los estudios incluidos y los registros de ensayos de los fabricantes. La fecha de la búsqueda más reciente fue junio 2013.
Criterios de selección
Se incluyeron estudios aleatorizados y doble ciego, con una duración de al menos cuatro semanas. Los estudios elegibles compararon preparados combinados de CSI y ABAP con placebo.
Obtención y análisis de los datos
Dos autores de la revisión, de forma independiente, evaluaron el riesgo de sesgo de los estudios y extrajeron los datos. Los datos dicotómicos se analizaron como odds ratios (OR) de efectos fijos o cocientes de tasas (CT) con intervalos de confianza (IC) del 95%, y los datos continuos como diferencias de medias con intervalos de confianza del 95%.
Resultados principales
Diecinueve estudios cumplieron los criterios de inclusión (con 10 400 participantes asignados al azar y una duración de entre cuatro y 156 semanas, media 42 semanas). Los estudios utilizaron tres preparados combinados diferentes (fluticasona/salmeterol, budesonida/formoterol o mometasona/formoterol). Los estudios en general presentaron riesgo bajo de sesgo en cuanto al cegamiento, aunque hubo riesgo incierto o alto de sesgo de desgaste debido a los abandonos de los participantes. En comparación con placebo, la fluticasona/salmeterol y la budesonida/formoterol redujeron la tasa de exacerbaciones. La combinación mometasona/formoterol redujo el número de participantes que experimentaron una o más exacerbaciones. El análisis agrupado de los tratamientos combinados indicó que las exacerbaciones fueron menos frecuentes en comparación con placebo (cociente de tasas 0,73; IC del 95%: 0,69 a 0,78; siete estudios, 7495 participantes). La calidad de la evidencia cuando se aplicaron los criterios GRADE se calificó como moderada. Los participantes incluidos en estos ensayos tuvieron como promedio una o dos exacerbaciones por año, lo que significa que el tratamiento combinado daría lugar a una reducción de una exacerbación cada dos a cuatro años en estos individuos. Se observó una reducción general de la mortalidad, aunque este resultado fue dominado por los resultados de un estudio (TORCH) de fluticasona/salmeterol. En general, las muertes en los estudios más pequeños y más cortos fueron demasiado pocas para contribuir al cálculo general. Se necesitan estudios adicionales más largos sobre budesonida/formoterol y mometasona/formoterol para aclarar si lo anterior se observa de forma más general. Cuando se utilizó un riesgo inicial de muerte del 15,2% del brazo placebo de TORCH, el número necesario a tratar para lograr un resultado beneficioso adicional (NNTB) en tres años con fluticasona/salmeterol con objeto de evitar una muerte extra fue 42 (IC del 95%: 24 a 775). Los tres tratamientos combinados dieron lugar a una mejora estadísticamente significativa en las mediciones del estado de salud, aunque las diferencias de medias observadas son relativamente pequeñas con relación a la diferencia mínima clínicamente importante. Además, los síntomas y las evaluaciones de la función pulmonar favorecieron a los tratamientos combinados. Se observó un aumento del riesgo de neumonía con los inhaladores combinados en comparación con el tratamiento placebo (OR 1,62; IC del 95%: 1,36 a 1,94), y la calidad de esta evidencia se calificó como moderada, aunque no se observó un efecto de la dosis. El NNTD en tres años para un caso extra de neumonía fue 17, sobre la base de un riesgo del 12,3% de neumonía en el brazo de placebo del TORCH. Menos participantes se retiraron de los brazos de tratamiento combinado a causa de los eventos adversos o la falta de eficacia.
Conclusiones de los autores
El tratamiento con una inhalador combinado redujo en alrededor de un cuarto las exacerbaciones de la EPOC, en comparación con las observadas con placebo. Se observó una reducción significativa de la mortalidad por todas las causas, aunque este resultado fue dominado por un ensayo (TORCH), lo que recalca la necesidad de ensayos adicionales de mayor duración. Además, se señala que ha habido cierto debate sobre la idoneidad del análisis realizado en el ensayo de TORCH (véase Retroalimentación). El aumento del riesgo de neumonía es motivo de preocupación; sin embargo, no se tradujo en un aumento de las exacerbaciones, las hospitalizaciones o las muertes. La evidencia actual no indica diferencias importantes entre los inhaladores en cuanto a los efectos, aunque tampoco hay evidencia suficientemente sólida como para demostrar que todos son equivalentes. Es importante señalar que no es posible comentar sobre la contribución relativa de los componentes individuales de la terapia combinada a los efectos identificados, ya que esta revisión solo presenta la comparación pareada entre la terapia combinada y placebo. Para permitir conclusiones más firmes acerca de los efectos del tratamiento combinado se necesitan más datos, en particular relacionados con el perfil de eventos adversos y los efectos beneficiosos en cuanto a las diferentes formulaciones y dosis de CSI inhalados. Se necesitan comparaciones directas para determinar si un inhalador combinado es mejor que los otros.
PICO
Resumen en términos sencillos
Inhaladores combinados versus placebo para el tratamiento de la enfermedad pulmonar obstructiva crónica (EPOC)
Pregunta de la revisión
Se examinó la evidencia sobre los efectos de los inhaladores combinados en pacientes con EPOC, en comparación con placebo. El interés se centró especialmente en si los inhaladores combinados son un tratamiento efectivo y seguro para los adultos con EPOC.
Antecedentes
La EPOC es un trastorno respiratorio grave que afecta a millones de personas en todo el mundo. En la mayoría de los casos es causada por el hábito de fumar. El tratamiento de la EPOC a menudo incluye inhaladores. Actualmente, tres tipos de inhaladores combinan un esteroide y un “agonista beta2 de acción prolongada” (ABAP). Los esteroides funcionan al reducir la inflamación de las vías respiratorias y los ABAP funcionan al relajar los músculos de las vías respiratorias y abrirlas. El uso de inhaladores combinados es más conveniente que la administración de los dos fármacos por separado, aunque también es más costoso. Se buscó la evidencia sobre si la administración de un inhalador combinado es mejor o peor que placebo (inhalador simulado).
Características de los estudios
Se incluyeron en esta revisión 19 estudios con 10 400 pacientes. Los estudios duraron entre cuatro y 156 semanas. Todos los pacientes incluidos en los estudios presentaban EPOC de diferente gravedad. Se incluyeron hombres y mujeres, y en la mayoría de los estudios solo participaron adultos de 45 años de edad o más.
Todos los estudios compararon un inhalador combinado con un placebo idéntico en apariencia al inhalador combinado, de manera que los pacientes de los ensayos no sabían si recibían el fármaco o el inhalador simulado. Algunos de los estudios incluyeron dos grupos tratados con el inhalador combinado; un grupo recibió una dosis más alta y un grupo recibió una dosis más baja.
La evidencia presentada aquí está actualizada hasta junio 2013.
La mayoría de los estudios fueron patrocinados por la industria farmacéutica.
Resultados clave
Se encontró que los pacientes que recibieron un inhalador combinado presentaron menos probabilidades de sufrir una crisis (exacerbación) de la EPOC. Las posibilidades de presentar una exacerbación se redujeron en alrededor de la cuarta parte.
Se observó una reducción pequeña del riesgo de muerte a los tres años, aunque la mayor parte de la evidencia sobre la muerte proviene de un ensayo grande y de gran duración denominado TORCH. Según TORCH, aproximadamente 42 pacientes necesitarían ser tratados con un inhalador combinado durante tres años para evitar una muerte.
También se encontró que los pacientes que recibieron inhaladores combinados presentaron mejoras pequeñas en la calidad de vida, los síntomas relacionados con la EPOC y las pruebas respiratorias. Sin embargo, estas mejoras pueden no haber sido muy notorias para los pacientes.
Los pacientes tratados con inhaladores combinados presentaron mayores probabilidades de sufrir una infección pulmonar llamada neumonía. Nuevamente, la mayor parte de la evidencia acerca de la neumonía proviene del ensayo TORCH. Según TORCH, en comparación con placebo, aproximadamente de cada 17 pacientes tratados con un inhalador combinado, un paciente extra desarrollará neumonía.
Los pacientes tratados con inhaladores combinados no presentaron más o menos probabilidades de experimentar eventos graves no deseados, incluso efectos secundarios, durante el tratamiento.
No se encontraron diferencias consistentes entre los tres tipos diferentes de inhaladores incluidos en esta revisión.
Sin embargo, es importante señalar que no es posible determinar a partir de esta revisión si lo importante es la combinación o si uno de los dos medicamentos del inhalador combinado puede haber tenido el impacto real.
Calidad de la evidencia
En general, se considera que la evidencia presentada en esta revisión es de calidad moderada. La mayoría de los estudios no explicaron claramente la forma en la que decidieron qué pacientes recibirían el inhalador combinado y quiénes recibirían placebo, que es una parte importante de un estudio bien realizado. Además, más pacientes que recibieron placebo abandonaron los ensayos, en comparación con los que recibieron un inhalador combinado. Este hecho ocurrió a menudo debido a las exacerbaciones de la EPOC. Lo anterior significa que, al final del ensayo, los grupos podrían haber estado desequilibrados, lo que podría afectar la exactitud de los resultados.
Authors' conclusions
Summary of findings
| Combined inhalers versus placebo (primary outcomes) for chronic obstructive pulmonary disease (COPD) | ||||||
| Patient or population: patients with COPD Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Combined inhalers versus placebo (primary outcomes) | |||||
| Annual exacerbation rates | 1.35 | 0.99 (0.93 to 1.05) | Rate ratio 0.73 (0.69 to 0.78) | 7473 (seven studies) | ⊕⊕⊕⊝ | |
| Participants with at least one exacerbation Duration of six months3 | 301 per 1000 | 251 per 1000 (221 to 286) | OR 0.78 | 3141 (eight studies) | ⊕⊕⊕⊝ | |
| Mortality Duration of 18 months3 | 60 per 1000 | 50 per 1000 | OR 0.82 | 10129 | ⊕⊕⊕⊝ | |
| Pneumonia Duration of 18 months3 | 55 per 1000 | 85 per 1000 | OR 1.62 | 9620 | ⊕⊕⊕⊝ | |
| Hospitalisations due to COPD exacerbations Duration of 18 months3 | 115 per 1000 | 108 per 1000 | OR 0.93 | 9492 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| 1Downgraded because of risk of attrition bias. 2Concerns have been raised about the analysis of the largest study, TORCH. We note that the protocol was published after the trial had recruited (See Feedback 1, Feedback 2). No downgrade. 3Weighted mean duration. 4Downgraded because of imprecision. 5Downgraded because of risk of attrition bias and imprecision. | ||||||
| Fluticasone/salmeterol (FPS) versus placebo for COPD | ||||||
| Patient or population: patients with COPD Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Fluticasone/salmeterol (FPS) versus placebo (PLA) | |||||
| Adverse events—any Duration of two years1 | 780 per 1000 | 794 per 1000 | OR 1.09 | 5574 | ⊕⊕⊝⊝ | |
| Adverse events—'serious' Duration of two years1 | 271 per 1000 | 287 per 1000 | OR 1.08 | 5531 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| 1Weighted mean duration. 2Downgraded because of risk of attrition bias and imprecision. 3Concerns have been raised about the analysis of the largest study, TORCH. We note that the protocol was published after the trial had recruited (See Feedback 1, Feedback 2). | ||||||
| Budesonide/formoterol (BDF) versus placebo for COPD | ||||||
| Patient or population: patients with COPD Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Budesonide/formoterol (BDF) versus placebo | |||||
| Adverse event—any—320/94 Duration of nine months 3 | 538 per 1000 | 623 per 1000 | OR 1.42 | 1552 | ⊕⊕⊝⊝ | |
| Adverse event—any—160/94 Duration of nine months 3 | 538 per 1000 | 606 per 1000 | OR 1.32 | 1556 | ⊕⊕⊝⊝ | |
| Adverse events—'serious'—320/94 Duration of 10 months3 | 162 per 1000 | 184 per 1000 | OR 1.17 | 2476 | ⊕⊕⊝⊝ | |
| Adverse events—'serious'—160/94 Duration of nine months 3 | 113 per 1000 | 132 per 1000 | OR 1.2 | 1556 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| 1Downgraded because of risk of attrition bias and imprecision and heterogeneity. 3Weighted mean duration. 4Delivered dose. | ||||||
| Mometasone/formoterol (MF/F) versus placebo for COPD | ||||||
| Patient or population: patients with chronic obstructive pulmonary disease Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Mometasone/formoterol (MF/F) versus placebo | |||||
| Adverse event—any—400/103 Duration of six months | 362 per 1000 | 357 per 1000 | OR 0.98 | 890 | ⊕⊕⊝⊝ | |
| Adverse event—any—200/103 Duration of six months | 362 per 1000 | 317 per 1000 | OR 0.82 | 894 | ⊕⊕⊝⊝ | |
| Adverse events—serious—400/103 Duration of six months | 74 per 1000 | 80 per 1000 | OR 1.09 | 890 | ⊕⊕⊝⊝ | |
| Adverse events—serious—200/103 Duration of six months | 74 per 1000 | 53 per 1000 | OR 0.71 | 894 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| 1Downgraded because of risk of attrition bias, imprecision and heterogeneity. 3Delivered dose. | ||||||
Background
Description of the condition
Chronic obstructive pulmonary disease (COPD) is the fourth leading cause of death in most industrialised countries, and it is projected to be the third leading cause of death worldwide by 2020 (GOLD 2012). The disease is predominantly caused by smoking. An estimated three million people are affected by COPD in the UK (NCGC2010). COPD is a heterogeneous syndrome that is characterised by reduced post‐bronchodilator lung function (forced expiratory volume in one second/forced vital capacity (FEV1/FVC)) < 0.7 in all patients (GOLD 2012). Acute bronchodilator reversibility has traditionally been regarded as a characteristic of asthma, and only in the past few years has it been generally acknowledged that this clinical feature is also present in COPD (Hanania 2011), as it was found in the UPLIFT study (UPLIFT 2008), in which 53% of participants had an increase of at least 200 mL in FEV1 post‐salbutamol. In TORCH, an increase in predicted FEV1 of 10% was an exclusion criterion (TORCH). Patients with COPD generally show progressive lung function loss, accompanied by worsening respiratory symptoms (e.g. dyspnoea, cough and sputum) and health status (GOLD 2012). These clinical features are a result of persisting and progressive airway inflammation (i.e. bronchial infiltration of neutrophils, macrophages, lymphocytes and mast cells) and increasing evidence of autoimmunity (Cosio 2009). Furthermore, it has been suggested that some phenotypes of COPD involve chronic systemic inflammation that has an impact on co‐morbidities, such as cardiovascular disease (Garcia‐Aymerich 2011).
Description of the intervention
This review focusses on combined inhalers that contain both an inhaled corticosteroid (ICS) and a long‐acting beta2‐agonist (LABA).
ICS, LABA and long‐acting antimuscarinic agents (LAMA) have been shown to be effective in a range of outcomes in COPD. ICS have not been shown to reduce the rate of decline in FEV1, although short‐term increases in FEV1 and significant reductions in exacerbations have been reported (Yang 2012). LABA and LAMA reduce exacerbation frequency and symptoms and improve quality of life. On the basis of the evidence, GOLD 2012 recommends that inhaled steroids should be used in patients with an FEV1 < 50% predicted (GOLD stages 3 and 4 or quadrant C and D in the 2012 update of the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria) and a history of exacerbations (GOLD 2012). National Institute for Health and Care Excellence (NICE) guidelines recommend either a LABA with an ICS in a combined inhaler, or with a LAMA, if FEV1 is less than 50% predicted. Furthermore, the guidelines recommended combined ICS/LABA In people with stable COPD with an FEV1 ≥ 50% who remain breathless or have exacerbations despite maintenance therapy with a LABA (NCGC2010).
How the intervention might work
The evidence base for the addition of long‐acting beta2‐agonists to inhaled steroids in asthma is well established (Ducharme 2010; Ni Chroinin 2009). In asthma, the scientific rationale for combining LABA and ICS in a single inhaler relates to synergy of action. At a molecular level, ICS up‐regulate the expression of beta2‐agonist receptors in bronchial smooth muscle. At the same time, LABA increase the genomic actions of ICS by promoting passage to the cellular nuclei. Thus, beta2‐agonists and ICS may interact in a beneficial way, with ICS preventing the loss of function of beta2‐agonists with long‐term use, whereas beta2‐agonists may potentiate the local anti‐inflammatory actions of ICS in people with asthma (Barnes 2002).
Some of these mechanisms may also be important in COPD. Several possible advantages associated with a combination of therapies have already been shown to improve outcomes. In particular, ICS in combination with LABA may have a greater effect than either treatment alone on the number of exacerbations, or on other outcomes such as quality of life (Nannini 2012; Nannini 2013). One clinical rationale is based on patient convenience, with the expectation that a simplified inhaler regimen may lead to greater treatment adherence (Barnes 2002).
Why it is important to do this review
This is an update of a previous review, which considered the effect of combined therapy compared with placebo, as well as both monocomponents separately, in people with COPD (Nannini 2004). The availability of several new studies has prompted us to split the review between comparisons with placebo and those with monocomponents. This review summarises the evidence from clinical trials comparing combined ICS and LABA with placebo. Reviews of the comparison between combined therapy and ICS (Nannini 2013) or long‐acting beta2‐agonists (Nannini 2012) are published separately.
Concerns have been raised recently regarding the safety of LABA in asthma (Walters 2007). Moreover, questions have surrounded the validity of summary estimates from clinical trials that assessed exacerbation rates without accounting for follow‐up time or adjustment for between‐participant variability (Suissa 2006). Two well‐known COPD guidelines (GOLD 2012; NCGC2010) had issued a strong recommendation regarding ICS/LABA combined therapy. But others are more guarded: "Recommendation 5: ACP, ACCP, ATS, and ERS suggest that clinicians may administer combination inhaled therapies (long‐acting inhaled anticholinergics, long‐acting inhaled beta2‐agonists, or inhaled corticosteroids) for symptomatic patients with stable COPD and FEV1 < 60% predicted (Grade: weak recommendation, moderate‐quality evidence)" (ACP 2011). Finally, the largest randomised controlled trial (RCT) of combined therapy (TORCH) demonstrated a significant reduction in mortality versus placebo (P = 0.052). We wished to see whether other combined inhalers had a similar effect.
Objectives
To determine the efficacy and safety of combined ICS and LABA for stable COPD in comparison with placebo.
Methods
Criteria for considering studies for this review
Types of studies
Randomised, double‐blind, parallel‐group clinical trials of at least four weeks' duration.
Types of participants
Adult patients (age > 40 years) with known, stable COPD fulfilling American Thoracic Society (ATS), European Respiratory Society (ERS) or Global Initiative for Chronic Obstructive Lung Disease (GOLD) diagnostic criteria. Patients were to be clinically stable with no evidence of an exacerbation for one month before study entry. Patients with significant diseases other than COPD (e.g. with a diagnosis of asthma, cystic fibrosis, bronchiectasis or other lung diseases) were excluded. However, patients with partial reversibility on pulmonary function testing were included.
Types of interventions
-
Fluticasone propionate/salmeterol versus placebo (FPS).
-
Budesonide/formoterol versus placebo (BDF).
-
Mometasone furoate/formoterol versus placebo (MF/F).
Concomitant therapy was permitted, as long as no systematic difference was noted between treatment groups; however, trials in which participants were randomly assigned to tiotropium and combined ICS/LABA therapy versus tiotropium and placebo were excluded from the review, as this comparison is already considered in Karner 2011.
Types of outcome measures
Primary outcomes
-
Exacerbations, measured as rate or number of participants experiencing an exacerbation.
-
All‐cause mortality.
-
Pneumonia.
-
Hospitalisations due to COPD exacerbation (note that we accepted COPD reported as a serious adverse event as a surrogate marker for this outcome; the internationally recognised definition of a serious adverse event includes a life‐threatening event or one that results in hospitalisation or prolonged hospitalisation).
Secondary outcomes
-
Change in forced expiratory volume in 1 second (FEV1) and change in forced vital capacity (FVC): trough, peak and average and other measures of pulmonary function.
-
Exercise performance: six‐minute walk and other measures.
-
Quality of life scales: St George's Respiratory Questionnaire (SGRQ), Chronic Respiratory Disease Questionnaire (CRDQ).
-
Symptoms.
-
Inhaled rescue medication used during the treatment period and other concomitant medications used, including antibiotics and steroids.
-
Adverse events: palpitations, tremor, hoarseness/dysphonia, oral candidiasis, cataracts, skin bruising, bone fracture, bone density, plasma cortisol level.
-
Rate of withdrawal due to lack of efficacy or COPD deterioration.
-
Withdrawal due to adverse events.
Search methods for identification of studies
Electronic searches
We identified trials using the Cochrane Airways Group Specialised Register of trials, which is derived from systematic searches of bibliographic databases including the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE, CINAHL, AMED and PsycINFO; we also handsearched respiratory journals and meeting abstracts (see Appendix 1 for more details). All records in the Specialised Register coded as 'COPD' were searched using the following terms:
(((beta* and agonist*) and long*) or ((beta* and adrenergic*) and long*) and (*steroid or steroid* or corticosteroid*)) or (fluticasone and salmeterol) or Seretide or Advair or (formoterol and budesonide) or Symbicort.
The most recent search was done in June 2013. We applied no restrictions on language of publication or publication type.
Searching other resources
We reviewed reference lists of all primary studies and review articles for additional references, and we contacted authors of identified randomised trials about other published and unpublished studies. In addition, we consulted the online trial registries of GlaxoSmithKline and AstraZeneca, manufacturers of FPS and BDF, respectively (www.ctr.gsk.co.uk; www.astrazenecaclinicaltrials.com).
Data collection and analysis
Selection of studies
Two review authors (LJN and PP) independently identified abstracts of trials that appeared potentially relevant. Using the full text of each study, these review authors independently selected trials for inclusion in the review. Consensus was by simple agreement, with third party adjudication used to resolve differences.
Data extraction and management
Two review authors (RN and RH) independently extracted data from included trials. RN entered the data into Review Manager, and this work was checked by RH. In some cases, we estimated information regarding outcomes from graphs. This was performed independently. Data extraction included the following items.
-
Design: method of randomisation, presence and type of run‐in period, study design (parallel, cross‐over).
-
Population: age, gender, smoking status, study setting (country, practice setting), inclusion and exclusion criteria.
-
Intervention: dose, delivery device, duration.
-
Control: concurrent treatments (ipratropium, beta2‐agonist, inhaled and systemic corticosteroids).
-
Outcomes: as above.
Assessment of risk of bias in included studies
The risk of bias of included studies was assessed using The Cochrane Collaboration's risk of bias tool (Higgins 2011). Two review authors (RN and RH) assessed the risk of bias of all included studies with regard to random sequence generation, allocation concealment, blinding, incomplete outcome data and selective outcome reporting. Each item was assessed as having high, low or unclear risk of bias on the basis of relevant information reported in the randomised controlled trial.
Measures of treatment effect
For dichotomous variables, data are expressed as odds ratios (OR) with 95% confidence intervals (CI). Data for continuous variables were reported as mean differences (MD) with 95% CI.
Unit of analysis issues
The unit of analysis was the participant.
Dealing with missing data
We contacted study sponsors and primary investigators to obtain information that we could not verify by reviewing the study reports.
We used reported confidence intervals or P values to calculate standard deviations, or standard errors, when necessary.
Assessment of heterogeneity
For pooled effects, heterogeneity was assessed by using the I2 measurement. This estimates the degree of variation between studies not attributable to the play of chance. I2 was interpreted in relation to the following guidance (Higgins 2011).
-
0% to 40%: may not be important.
-
30% to 60%: may represent moderate heterogeneity.
-
50% to 90%: may represent substantial heterogeneity.
-
75% to 100%: may represent considerable heterogeneity (Higgins 2011).
We also considered the Chi2 test (P value < 0.10). We regarded I2 as our primary measure of heterogeneity.
Assessment of reporting biases
We evaluated publication bias by using visual inspection of funnel plots when an adequate number of trials were aggregated in the analyses (more than ten). We recognised that an asymmetrical funnel plot can reflect heterogeneity, outcome reporting bias and small study effects and therefore is not necessarily a reflection of publication bias.
Data synthesis
For continuous variables, we used a fixed‐effect mean difference (MD) for outcomes measured on the same metric. A standardised mean difference (SMD) with 95% confidence interval (95% CI) was calculated for outcomes when data were combined from studies using different metrics. All similar studies were pooled using fixed‐effect MD/SMD and 95% CI.
For dichotomous variables, we calculated a fixed‐effect odds ratio (OR) with 95% CI. All similar studies were pooled using a fixed‐effect OR and 95% CI.
When mean treatment differences were reported, data were entered as generic inverse variance (GIV), provided a standard error for the difference could be extracted or imputed. When this method was used, the effect size was reported from the original papers, for example, as a Rate Ratio (RR). This method (GIV) was not available when the protocol was written for the review, so it was not prespecified.
We used pooled OR with 95% CI to calculate numbers needed to treat for an additional beneficial outcome (NNTB) or harm (NNTH) using Visual Rx. Control event rates were taken from the event rates in the individual trials and are reported with the corresponding duration of the trial because NNTs are time dependent (Cates 2012).
Subgroup analysis and investigation of heterogeneity
We separated the types of steroids and long‐acting beta2‐agonists, and for the new studies included in this update, we also separated differing dosages of the same drug. We planned the following a priori subgroups.
-
Disease severity (related to baseline FEV1 and placebo group exacerbation rate) according to GOLD staging of IIA or IIB (moderate COPD, characterised by deteriorating lung function (IIA = FEV1 ≤ 80% predicted; IIB = ≤ 50% predicted) with progression of symptoms) and III (severe COPD, characterised by severe airflow limitation (FEV1 < 30% predicted) and the presence of respiratory failure or clinical signs of right heart failure (GOLD 2012).
-
Prior inhaled corticosteroid plus long‐acting beta2‐agonist use (dichotomised as yes/no).
-
Concurrent therapy with routine beta2‐agonist (short‐ or long‐acting), corticosteroid (systemic or inhaled) or theophylline (dichotomised as yes/no).
-
Reversibility of airflow obstruction with beta2‐agonist therapy (dichotomised as partial/none). Definition: > 12% and > 200 mL from baseline FEV1 or > 12% post‐bronchodilator (metered‐dose inhaler (MDI) salbutamol 200 to 400 mcg).
-
Dose, duration and delivery method of therapy.
Sensitivity analysis
For pooled effects, heterogeneity was to be tested by using the I2 measurement of the degree of variation between studies, not attributable to the play of chance. If heterogeneity was found (I2 statistic > 30%), a random‐effects model was used to determine the impact of heterogeneity on the overall pooled effect. In addition, the robustness of the results was tested using a sensitivity analysis based on the quality of the trials when possible.
Results
Description of studies
Results of the search
For details of the search history, see Table 1.
| Version | Detail |
| First published version—Issue 4, 2003 (all years to April 2002) | References identified: 34 |
| Second published version—Issue 3, 2004 (April 2003 to April 2004) | References identified: 12 |
| Third published version—Issue 3, 2005 (April 2004 to April 2005) | References identified: 52 |
| Fourth published version (April 2005 to April 2007) | References identified: 66 |
| Fifth published version (April 2007 to June 2013) | References identified: 129 New unique studies identified: eight (ongoing studies: zero) New studies included: eight Total studies included: 19 |
Included studies
Nineteen studies are included in this review. A previous ongoing study, Morgan 2004, has now been linked to the TRISTAN trial. For a full description of baseline characteristics, methods used and inclusion and exclusion entry criteria for the individual studies, see Characteristics of included studies.
Design
All trials had a randomised, double‐blind, parallel‐group design and were of at least four weeks' duration. Methods of randomisation were described in six studies (Bourbeau 2007; Lapperre 2009; Mahler 2002; Sin 2008; Tashkin 2008; Tashkin 2012). The method of blinding was not fully described in all studies. Through correspondence from GlaxoSmithKline, trial methodology was confirmed for TRISTAN, and AstraZeneca confirmed the methodology for Szafranski 2003. Study characteristics were sufficiently described in two data sets without journal publication to justify their inclusion in the review (SFCT01 and SCO104925).
Participants
A total of 10,400 participants were randomly assigned to interventions within studies included in this review. Participants suffered from COPD, with variable definitions of COPD and reversibility. COPD was defined by national or international criteria as follows: ATS (Hanania 2003; Mahler 2002); ERS (TORCH; TRISTAN); or GOLD (Barnes 2006; Bourbeau 2007; Calverley 2003; Dal Negro 2003; Lapperre 2009; Sin 2008; Szafranski 2003; Zheng 2006). In seven studies, definitions were not specified or were based on lung function tests and smoking history (Doherty 2012; O'Donnell 2006; Rennard 2009; SCO104925; SFCT01; Tashkin 2008; Tashkin 2012). Participant populations in the studies suffered from moderate to very severe COPD, with the exception of Bourbeau 2007, in which participants with mild COPD were also enrolled, and Sin 2008, in which enrolled participants had FEV1 < 80% predicted. Two studies enrolled participants with reversible or non‐reversible COPD (Hanania 2003; Mahler 2002). In TORCH, participants were not required to have had previous exacerbations requiring oral steroids or antibiotics to be included in the study. All participants were required to have a smoking history, with the exception of those enrolled in Zheng 2006, which included both smokers and never smokers.
Interventions
All 19 studies compared combination therapy with placebo, but the therapies varied. Thirteen studies compared FPS with placebo, four compared BDF and two compared MF/F. In three of the FPS studies, the combination of ICS/LABA was 250 mcg/50 mcg twice daily (Dal Negro 2003; Hanania 2003; O'Donnell 2006). In the remainder of the FPS studies, the dose was 500 mcg/50 mcg twice daily. Previous versions of this review did not consider these dosage groups separately, and as the participant numbers are small, this has not been changed in the current update. In Calverley 2003 and Szafranski 2003, the combination ICS/LABA was BDF 320 mcg/9 mcg twice daily, whereas both Rennard 2009 and Tashkin 2008 included two combined inhaler active treatment arms: BDF 320 mcg/9 mcg twice daily and 160 mcg/9 mcg twice daily. The two studies of MF/F, Doherty 2012 and Tashkin 2012, also included two combined inhaler active treatment arms: 400/10 twice daily and 200/10 twice daily.
The nature of the run‐in period varied between studies, but studies generally included a two‐ to four‐week washout period from inhaled long‐acting medication. In one study, all participants had a two‐week run‐in treatment with oral corticosteroids, inhaled formoterol and as required a short acting beta2‐agonist (SABA) (Calverley 2003). Full details are given in the tables of included studies.
Concomitant therapy was as‐needed SABA, short‐acting muscarinic antagonists (SAMA) and, in some studies, tiotropium. In five studies, theophylline was also used. Eleven per cent of participants in Hanania 2003 and all 18 participants in Dal Negro 2003 received theophylline, in addition to the study drugs. One participant in the FPS group in Bourbeau 2007 used theophylline. The exact proportion of participants in TRISTAN who were taking theophylline was not reported. In Zheng 2006, 2.7% of the active treatment group used theophylline compared with 7.4% of the placebo group. Oral steroids and/or antibiotics were used in all studies in the case of exacerbations.
Duration
-
13 weeks or less: Barnes 2006; Bourbeau 2007; O'Donnell 2006; Sin 2008; SCO104925.
-
24 to 26 weeks: Doherty 2012; Hanania 2003; Mahler 2002; Tashkin 2008; Tashkin 2012; Zheng 2006.
-
52 weeks: Calverley 2003; Dal Negro 2003; SFCT01; Szafranski 2003; Rennard 2009; TRISTAN.
-
130 weeks: Lapperre 2009.
-
156 weeks: TORCH.
Outcomes
The definition of an exacerbation varied between the included studies, and all definitions are summarised in Appendix 2. Hanania 2003 and Mahler 2002 withdrew participants whose condition was exacerbated. Lung function, if reported, was measured as FEV1 or peak expiratory flow (PEF). Quality of life assessment by SGRQ or CRDQ was available for Calverley 2003; Doherty 2012; Hanania 2003; Mahler 2002; Rennard 2009; SFCT01; Szafranski 2003; Tashkin 2008; Tashkin 2012; TORCH; TRISTAN; and Zheng 2006. In addition, breathlessness, cough and sputum score (BCSS) was reported by Rennard 2009 and Tashkin 2008. All‐cause mortality was reported by TORCH.
Excluded studies
Studies that did not meet the entry criteria of this review are listed in Characteristics of excluded studies, together with a reason for exclusion.
Risk of bias in included studies
A summary of the risk of bias assessment for each trial is provided in Figure 1.

Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
Allocation
Most of our judgements on allocation procedures were unclear because of the paucity of information provided in the trial reports. We were able to ascertain a low risk of bias in four large studies (Szafranski 2003; Tashkin 2012; TORCH; TRISTAN) and in one smaller study (Sin 2008). However, as most included studies are industry‐sponsored, they are extremely likely to have followed gold standards for both random sequence generation and concealment of allocation and therefore to be at low risk of bias.
Blinding
All studies were 'double‐blinded', and the authors stated that identical inhaler devices were used to deliver active treatment and placebo; they therefore are likely to be at low risk of performance and detection bias. However, in all trials, further details of participant and assessor blinding were not given.
Incomplete outcome data
Most studies had high attrition rates and therefore were deemed to be at unclear or high risk of bias for all outcomes, including mortality. The TORCH trial, however, attempted to follow up all participants for their vital status and therefore was deemed to be at low risk of bias for this outcome. It should be noted that attrition rates reported in the included studies are in keeping with, if not lower than, those expected in COPD trials; therefore these studies are at low risk of bias when compared with similar trials in this field.
Selective reporting
Most included studies reported all prespecified outcomes and were deemed to be at low risk of reporting bias. However, as pointed out in feedback received, the trial protocol of the largest included study, TORCH, was submitted and published after recruitment of participants (Vestbo 2004).
Other potential sources of bias
Both SCO104925 and SFCT01 are pharmaceutical company reports that have not been published in the peer‐reviewed literature. However, the trials were sufficiently described to warrant their inclusion and are likely to be at low risk of bias.
Effects of interventions
See: Summary of findings for the main comparison Combined inhalers versus placebo (primary outcomes) for chronic obstructive pulmonary disease; Summary of findings 2 Fluticasone/salmeterol (FPS) versus placebo for COPD; Summary of findings 3 Budesonide/formoterol (BDF) versus placebo for COPD; Summary of findings 4 Mometasone/formoterol (MF/F) versus placebo for COPD
Primary outcomes
Rate of exacerbations
Pooled results of all combined inhalers versus placebo
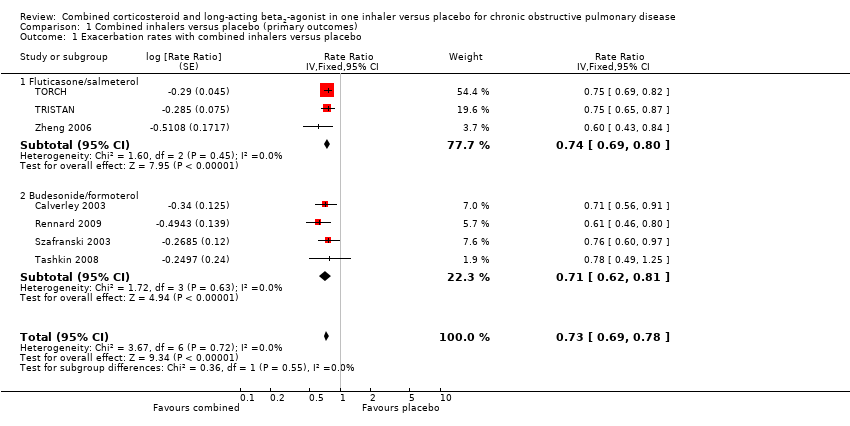
When data from seven trials (N = 7495) were pooled, the overall reduction in the rate of exacerbations when FPS or BDF was used was 0.73 (95% CI 0.69 to 0.78; Analysis 1.1); the quality of this evidence when GRADE criteria were used was rated as moderate (summary of findings Table for the main comparison).
FPS versus placebo
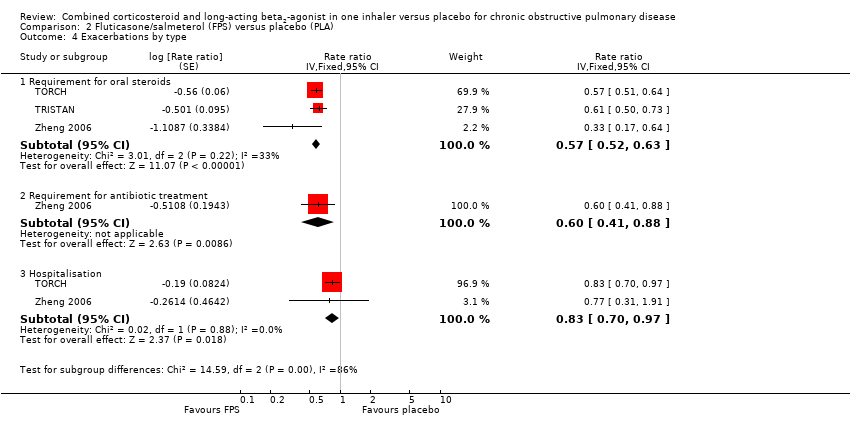
A significant reduction was noted in the rate of exacerbations with combination therapy when compared with placebo (RR 0.74, 95% CI 0.69 to 0.80, three studies, 4255 participants; Analysis 2.1). This result was not altered by removing TRISTAN, a study for which the summary estimate may have been biased by inadequate adjustment for between‐participant variability (Suissa 2006); see Figure 2. Additional analyses were performed on exacerbations with specific definitions. Compared with placebo, FPS led to fewer exacerbations requiring oral steroids (RR 0.57, 95% CI 0.52 to 0.63, three studies), less requirement for antibiotics (RR 0.60, 95% CI 0.41 to 0.88) and fewer hospitalisations (RR 0.83, 95% CI 0.7 to 0.97, two studies).

Forest plot of comparison: 1 Combined inhalers versus placebo (primary outcomes), outcome: 1.1 Exacerbation rates with combined inhalers versus placebo.
BDF versus placebo
A significant effect on pooled exacerbation rates favoured BDF compared with placebo (RR 0.71, 95% CI 0.62 to 0.81); see Figure 2. These results are based on data on 3240 participants from four trials (Szafranski 2003; Calverley 2003; Rennard 2009 and Tashkin 2008).
Number of people experiencing at least one exacerbation
FPS versus placebo
No significant difference was noted between FPS and placebo in terms of the number of participants experiencing at least one exacerbation (OR 0.83, 95% CI 0.64 to 1.07, seven studies, 1817 participants; Analysis 2.2)
MF/F versus placebo
The odds ratio for the numbers of participants experiencing at least one exacerbation for the 400/10 strength inhaler was 0.72 (95% CI 0.54 to 0.95, 882 participants; Doherty 2012; Tashkin 2012) and 0.76 (95% CI 0.58 to 1.01) for the 200/10 strength inhaler (886 participants; Doherty 2012; Tashkin 2012).
The point estimates are very similar, and the test for subgroup differences is negative. Thus it cannot be inferred from these results that one strength inhaler is significantly different from another (Chi² = 0.10, df = 1, P = 0.75, I2 = 0%).
Of interest, a post hoc observation was made that the treatment effect is more pronounced when only participants with moderate or severe exacerbations are considered, that is, those requiring antibiotics and/or systemic steroids, emergency treatment or hospitalisation (OR 0.57, 95% CI 0.38 to 0.86 for 400/10; and OR 0.62, 95% CI 0.42 to 0.92 for 200/10; Analysis 4.2).
Mortality
Pooled results of all combined inhalers versus placebo
When results were pooled, the overall reduction in mortality with FPS, BDF or MF/F compared with placebo was 0.82 (95% CI 0.68 to 0.99, 16 studies, N = 10,129); the quality of this evidence was rated as moderate (summary of findings Table for the main comparison). Most of the weight for mortality comes from the TORCH trial, which is the only included trial that collected mortality as a primary outcome (Figure 3).
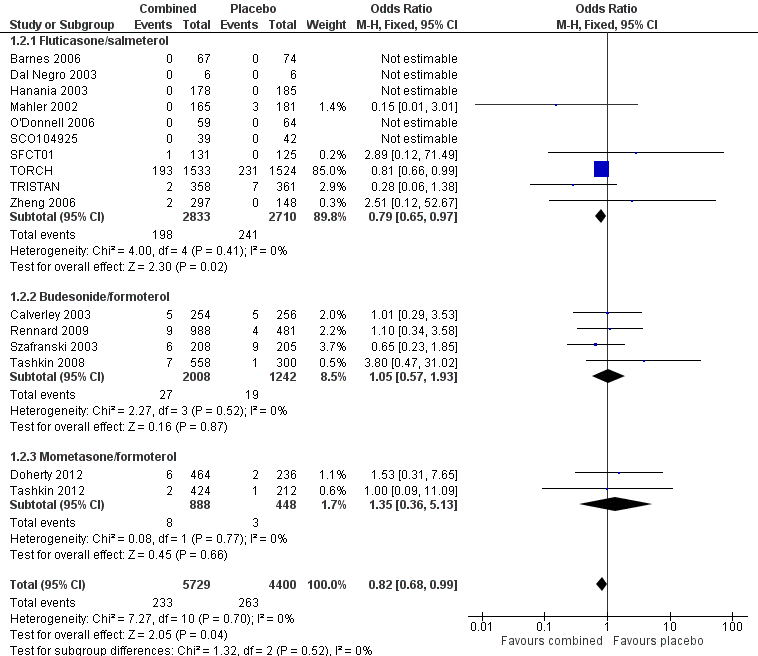
Forest plot of comparison: 1 Combined inhalers versus placebo (primary outcomes), outcome: 1.2 Mortality.
Because differing length of follow‐up across studies hinders the calculation of a pooled NNTB, we have tabulated this for each study individually (see Table 2). The three‐year NNTB (using the baseline risk of 15.2% in the placebo arm of TORCH) to prevent one extra death is 42 (95% CI 24 to 775).
| Study ID | Study duration | Placebo rate (%) mortality | NNTB for mortality | Placebo rate (%) pneumonia | NNTH for pneumonia |
| 156 weeks | 15.2 | 42 (24 to 775) | 12.3 | 17 (27 to 12) | |
| 52 weeks | 1.94 | 292 (164 to 5256) | 0.83 | 197 (339 to 131) | |
| 52 weeks | 1.95 | 249 (149 to 1307) | 3.6 | 48 (82 to 32) | |
| 52 weeks | 4.5 | 110 (66 to 581) | 0 | N/A | |
| 52 weeks | 0.83 | 674 (379 to 12,149) | 4.78 | 37 (63 to 25) | |
| 26 weeks | 0.33 | 1689 (950 to 30,403) | 1 | 164 (282 to 109) | |
| 26 weeks | 0.85 | 659 (370 to 11,865) | 0.85 | 193 (331 to 128) | |
| 26 weeks | 0.47 | 1187 (668 to 21,377) | 0.47 | 346 (595 to 229) | |
| 24 weeks | 1.66 | 340 (191 to 6125) | 0 | N/A | |
| 8 weeks | 0 | N/A | 1.56 | 107 (182 to 71) |
FPS versus placebo
The adjusted hazard ratio (HR) from TORCH did not identify a significant effect of FPS over placebo (HR 0.825, 95% CI 0.681 to 1.002, P = 0.052; TORCH). When the number of deaths in each treatment group was analysed by odds ratio and was combined with data from four other studies, a significant reduction in the odds of death favoured FPS versus placebo (OR 0.79, 95% CI 0.65 to 0.97, N = 5543, 10 studies; Analysis 2.5). Data were separated according to the time point and were subgrouped for data reported at three years, data at one to three years, data at one year and data at six months.
BDF versus placebo
The four studies with duration of six months to one year involving 3250 participants did not detect a significant difference in mortality between BDF and placebo (OR 1.05, 95% CI 0.57 to 1.93; Analysis 3.3).
MF/F versus placebo
Neither of two very similar studies (Doherty 2012; Tashkin 2012) of 26 weeks' duration and including 1336 participants detected a significant difference between MF/F and placebo (OR 1.35, 95% CI 0.36 to 5.13; Analysis 4.3).
However, it should be noted that the confidence intervals for both MF/F and BDF are wide and overlap with those of FPS, so a decrease in mortality with MF/F or BDF cannot be excluded.
Pneumonia
Pooled results of all combined inhalers versus placebo
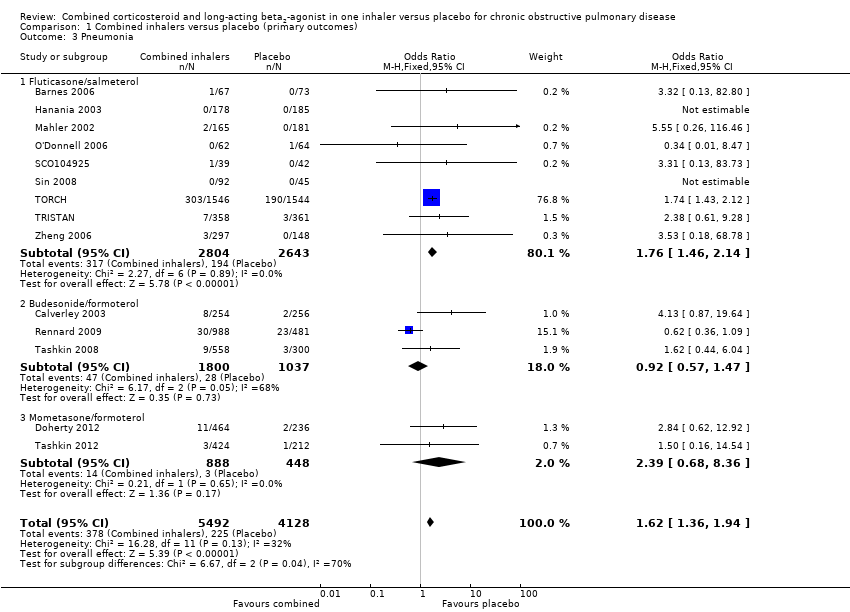
For combined inhalers, the pooled OR for pneumonia is 1.62 (95% CI 1.36 to 1.94, N = 9620, fixed‐effect model) with a moderate level of heterogeneity (I2 = 32%); the quality of this evidence was rated as moderate (summary of findings Table for the main comparison). When a random‐effects model of analysis is used, the effect size is reduced but remains significant (OR 1.57, 95% CI 1.01 to 2.42). Most of the weight for this combined result again comes from the TORCH trial, which tested the FPS inhaler.
FPS versus placebo
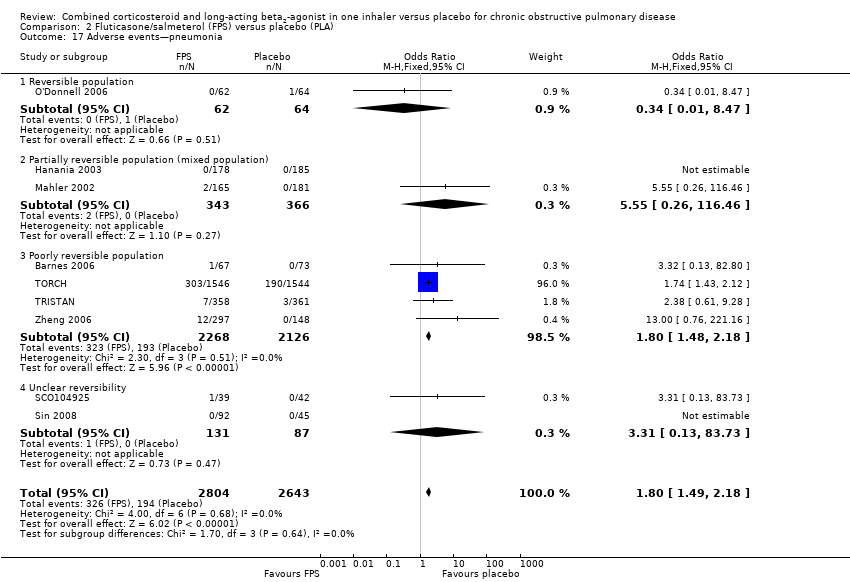
Pooled data from nine FPS trials (N = 5447) show a significant increase in pneumonia among participants treated with FPS in comparison with placebo (OR 1.76, 95% CI 1.46 to 2.14; Figure 4).
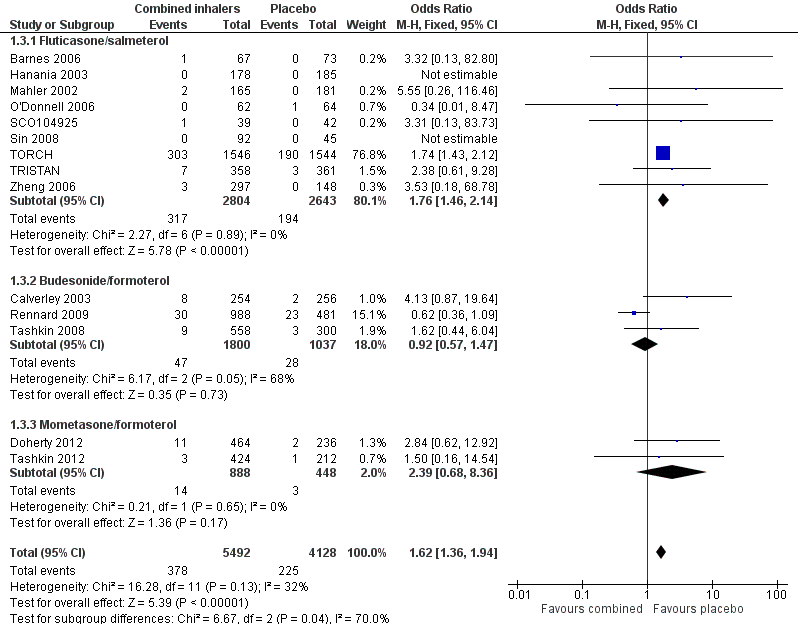
Forest plot of comparison: 1 Combined inhalers versus placebo (primary outcomes), outcome: 1.3 Pneumonia.
BDF versus placebo
Calverley 2003, Rennard 2009 and Tashkin 2008 reported data on pneumonia; no significant difference was detected between BDF and placebo (OR 0.92, 95% CI 0.57 to 1.47). The test for subgroup differences between BDF and FPS was significant (P = 0.01) when a fixed‐effect model was used. However, when a random‐effects model was applied, no significant difference between subgroups was found (P = 0.65).
MF/F versus placebo
Data from Doherty 2012 and Tashkin 2012 suggest no significant difference between treatments in diagnoses of pneumonia (OR 2.39, 95% CI 0.68 to 8.36, N = 1336), but the test for a subgroup difference between MF/F and FPS was negative for both fixed‐effect and random‐effects models (P = 0.64 and 0.66, respectively).
Table 2 gives the range of numbers needed to treat for an additional harmful outcome (NNTH) across the studies for pneumonia. A pooled NNTH was not calculated because of the wide differences in duration and the likely impact this would have on the calculation of a pooled event rate. The three‐year NNTH (when the baseline risk of 12.3% was used in the combination therapy arm of TORCH) for one extra participant to suffer from pneumonia was 17 (95% CI 27 to 12).
Hospitalisations due to COPD
Pooled results of combined inhalers versus placebo
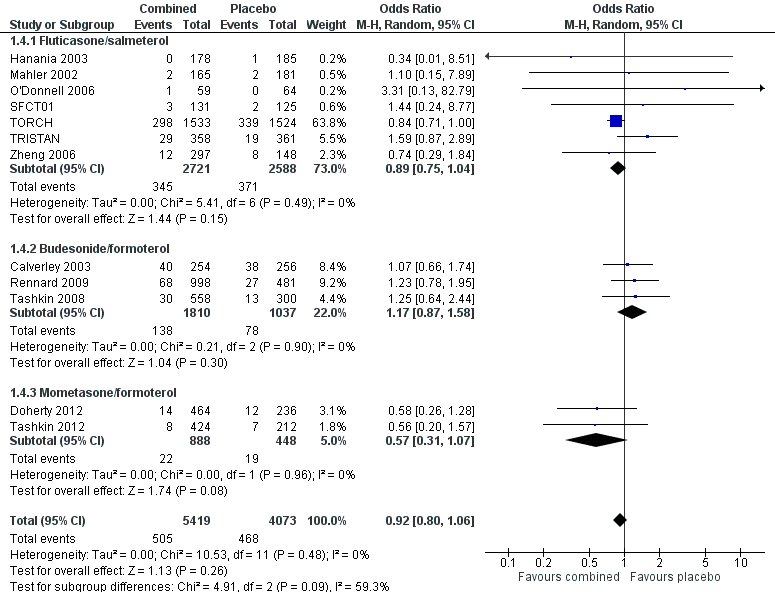
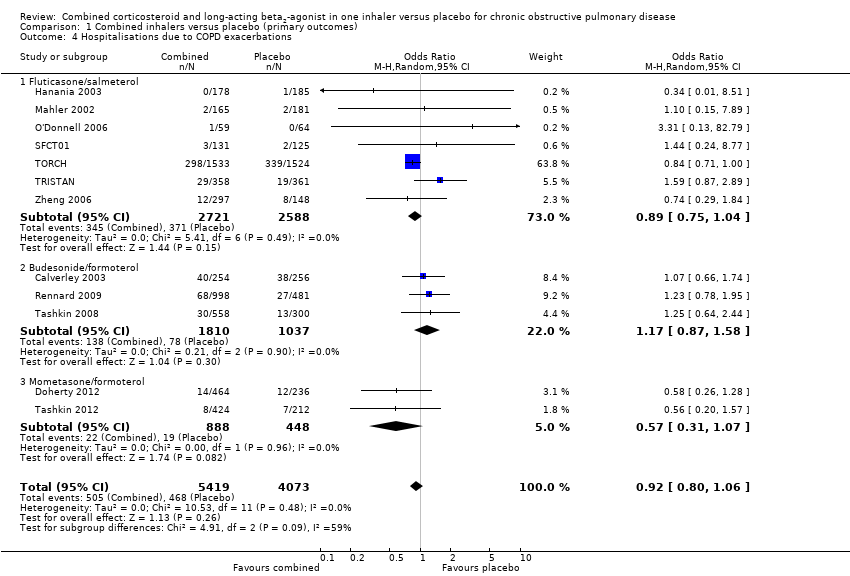
No significant difference was observed between active treatment and placebo for hospitalisation (OR 0.93, 95% CI 0.81 to 1.06, N = 9492; Figure 5); the quality of this evidence was rated as low (summary of findings Table for the main comparison).
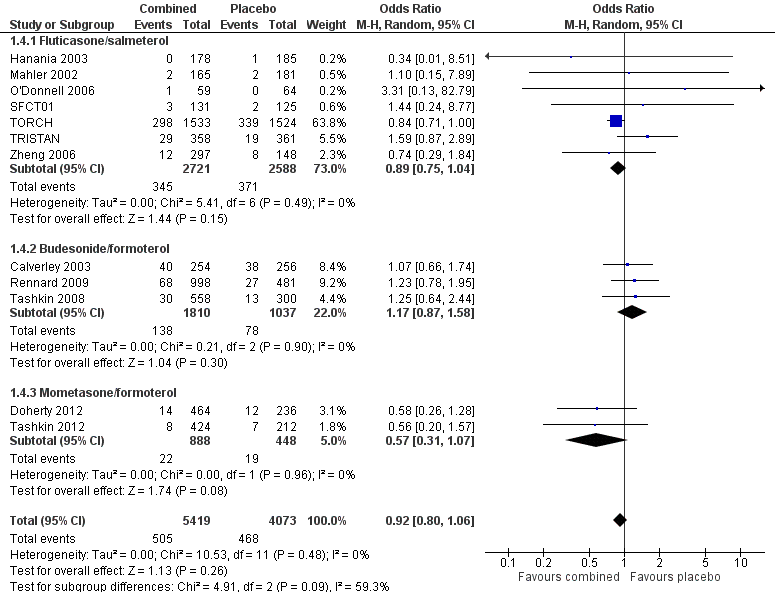
Forest plot of comparison: 1 Combined inhalers versus placebo (primary outcomes), outcome: 1.4 Hospitalisations due to COPD exacerbations.
Secondary outcomes
Quality of life
FPS versus placebo
Treatment with FPS improved SGRQ scores by an average of ‐2.9 units versus placebo (95% CI ‐3.61 to ‐2.18, four studies, N = 3346). Pooled data from Mahler 2002 and Hanania 2003 indicated a statistically significant improvement in CRDQ for those treated with FPS compared with placebo (5 units, 95% CI 2.48 to 7.52).
BDF versus placebo
A significant effect favoured BDF compared with placebo: ‐3.29 units on the SGRQ (95% CI ‐4.45 to ‐2.13) for the 320/9 strength inhaler, and ‐3.39 units (95% CI ‐4.70 to ‐2.07) for the 160/9 strength inhaler. A high level of heterogeneity was noted when these data were pooled (I2 = 70%). Random‐effects modelling also generated a significant effect (MD ‐4.11, 95% CI ‐6.18 to ‐2.04 for 320/9; and MD ‐3.39, 95% CI ‐4.70 to ‐2.07 for 160/9). The magnitude of improvement in the Szafranski 2003 BDF group was 3.9 units from baseline and was not dissimilar from the change scores from post run‐in treatment in Calverley 2003 (see graphical presentation of data in the published article, page 916). However, the placebo group deteriorated more in Calverley 2003, which possibly reflects the withdrawal of active treatment, with the subsequent loss of predosing effects achieved with high‐dose oral corticosteroids and LABA. In comparison, BDF may have maintained the predosing treatment effects of quality of life more successfully.
MF/F versus placebo
Treatment with MF/F resulted in a significant improvement in SGRQ scores when compared with placebo. This was true for both 400/10 (MD ‐3.80, 95% CI ‐5.75 to ‐1.86) and 200/10 (MD ‐3.91, 95% CI ‐6.01 to ‐1.81) inhalers.
Symptom score
FPS versus placebo
FPS led to improved symptom scores (transitional dyspnoea index) when compared with placebo (MD 1.04, 95% CI 0.56 to 1.53).
BDF versus placebo
Data were pooled for Calverley 2003 and Szafranski 2003. There was a significant effect in favour of BDF when compared with placebo (MD ‐0.63, 95% CI ‐0.90 to ‐0.37).
Rennard 2009 and Tashkin 2008 reported change from baseline in the breathlessness, cough and sputum score. Both trials described a significant improvement in average score over the treatment period for both strengths of combined inhalers (MD ‐0.43, 95% CI ‐0.59 to ‐0.26 for 320/9; and MD ‐0.44, 95% CI ‐0.60 to ‐0.28 for 160/9).
Lung function
FPS versus placebo
Pooled analysis of data was conducted without findings from the Dal Negro 2003 study. Owing to the small size of this study, we were concerned that the standard deviation (SD) represented an inaccurate estimate for the SD of the population, and that the small variance increased the weight of the study out of all proportion to its size. Data pooled from seven studies revealed an MD in predose FEV1 of 0.16 L (95% CI 0.14 to 0.19, N = 1408). Pooled data from Zheng 2006 and TORCH for postdose FEV1 indicated a significant improvement in favour of FPS over placebo of 0.09 L (95% CI 0.07 to 0.11). Results from Rennard 2009 demonstrate a clear improvement in average 0‐ to 12‐hour FEV1 for inhalers of both strengths.
BDF versus placebo
FEV1 data for mean percentage change from baseline were reported by two trials (Calverley 2003; Szafranski 2003). There was a significant increase in FEV1 in favour of BDF versus placebo (MD 14.40% 95%CI 11.91 to 16.90).
Predose FEV1 and one hour postdose FEV1 data were reported by one study, which included 858 participants (Tashkin 2008). A significant improvement was noted for both outcomes for combined inhalers of both strengths compared with placebo. Rennard 2009 reported average 12‐hour FEV1 and FEV1 at 12 hours compared with baseline. Again, a significant improvement was noted for both outcomes and for inhalers of both strengths when compared with placebo.
Both Rennard 2009 and Tashkin 2008 reported change from baseline morning and evening PEF, with significant benefit over placebo noted for inhalers of both strengths.
MF/F versus placebo
Both Doherty 2012 and Tashkin 2012 reported mean change from baseline in predose FEV1 at 13 weeks and demonstrated a significant improvement for both 400/10 (MD 114.64, 95% CI 77.79 to 151.50) and 200/10 (MD 66.00, 95% CI 14.37 to 117.63) inhalers when compared with placebo. It should be noted that no significant difference was seen between the 400/10 and 200/10 groups (test for subgroup differences: Chi2 = 2.77, df = 1, P = 0.10).
Mean change from baseline FEV1 area under the curve (AUC) 0 to 12 hours is also reported by Doherty 2012 and Tashkin 2012 and shows significant improvement in favour of active treatment for inhalers of both strengths (MD 162.04, 95% CI 126.54 to 197.53 for 400/10; and MD 122.01, 95% CI 86.64 to 157.39 for 200/10).
Rescue medication
FPS versus placebo
Pooled data from Mahler 2002 and Hanania 2003 indicated a significant reduction in mean puffs per day of short‐acting beta2‐agonist usage for FPS versus placebo (MD ‐1.19 puffs/d, 95% CI ‐1.83 to ‐0.55).
Mahler 2002 reported significant increases in the percentage of nights with no awakenings requiring short‐acting beta2‐agonist in favour of FPS versus placebo (5.7% vs ‐4.3%, respectively; P < 0.031).
TRISTAN reported a significant difference in median percentage of days without use of relief medication (FPS 14% vs placebo 0%, P < 0.001).
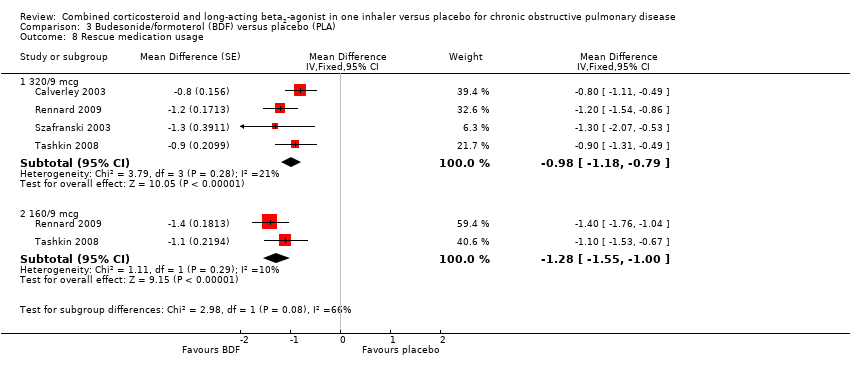
BDF versus placebo
BDF treatment reduced the requirement for reliever medication when compared with placebo. Combined results of Szafranski 2003; Calverley 2003; Rennard 2009 and Tashkin 2008 for the 320/9 strength inhaler show a reduction in use of rescue medication when compared with placebo (‐0.98 puffs/d, 95% CI ‐1.18 to ‐0.79). Pooled results from Rennard 2009 and Tashkin 2008 compare the 160/9 strength inhaler with placebo and also reveal a reduction in the use of rescue medication (‐1.28 puffs/d, 95% CI ‐1.55 to ‐1.00)
Safety and tolerability
FPS versus placebo
No significant difference was noted between FPS and placebo in the occurrence of overall reported adverse events (OR 1.09, 95% CI 0.95 to 1.25) or serious adverse events (OR 1.08, 95% CI 0.95 to 1.23, N = 5574, nine studies). In both cases, the quality of evidence was rated as low (summary of findings Table 2).
Pneumonia, candidiasis, nasopharyngitis, hoarseness and upper respiratory tract infection (URTI) occurred more frequently among FPS‐treated participants.
-
Pneumonia: OR 1.80, 95% CI 1.49 to 2.18, nine studies, N = 5447.
-
Candidiasis: OR 5.73, 95% CI 3.07 to 10.67, seven studies, N = 2039.
-
Hoarseness: OR 8.79, 95% CI 1.11 to 69.62, two studies, N = 585.
-
Nasopharyngitis: OR 1.28, 95% CI 1.05 to 1.56, two studies, N = 3535.
-
URTI: OR 1.23, 95% CI 1.04 to 1.47, five studies, N = 4963.
BDF
Rennard 2009 and Tashkin 2008 report overall adverse event data and demonstrate a significant difference favouring placebo for inhalers of both 320/9 and 160/9 strength (OR 1.42, 95% CI 1.16 to 1.74 for 320/9; and OR 1.32, 95% CI 1.08 to 1.61 for 160/9). In both cases, the quality of this evidence was rated as low (summary of findings Table 3).
When only serious adverse events were considered, the odds ratios were 1.17 (95% CI 0.95 to 1.45) for the 320/9 strength inhaler and 1.20 (95% CI 0.89 to 1.63) for the 160/9 strength inhaler; again, the quality of this evidence was rated as low (summary of findings Table 3).
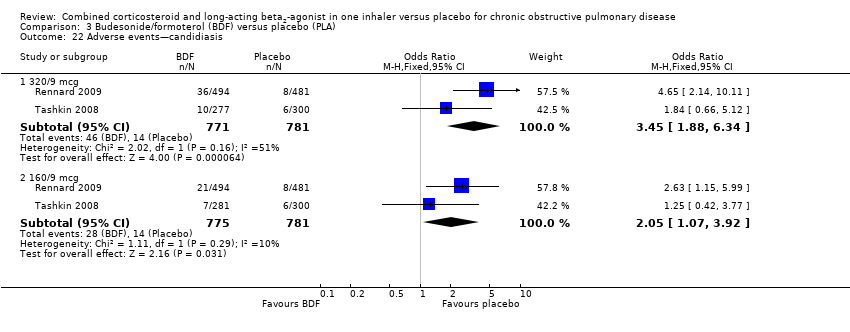
No difference was noted between active treatment and placebo for specific adverse events associated with ICS use, with the exception of reported episodes of candidiasis, which were noted to be significantly higher among those receiving active treatment. In addition, more cases of dysphonia were reported in the active treatment group receiving the higher‐dose inhaler, but not in the lower‐dose group. However, the test for subgroup differences was negative, so we cannot be certain of a dose effect.
MF/F
No significant difference in the occurrence of overall reported adverse events was reported between either strength of MF/F inhaler and placebo (OR 0.98, 95% CI 0.75 to 1.30 for 400/10; and OR 0.82, 95% CI 0.62 to 1.09 for 200/10). This finding was consistent when only serious adverse events were considered. The quality of this evidence was rated as low in both cases (summary of findings Table 4).
Also, no significant differences were noted between the groups when specific adverse events associated with ICS use were considered, although the overall numbers of events were small.
Withdrawals
FPS versus placebo
Significantly fewer withdrawals from treatment were seen with FPS than with placebo (OR 0.69, 95% CI 0.62 to 0.78). Withdrawals due to adverse events and lack of efficacy also occurred less frequently on treatment with FPS than with placebo (withdrawal due to adverse event: OR 0.74, 95% CI 0.64 to 0.86, twelve studies, 5491 participants; withdrawal due to lack of efficacy: OR 0.30, 95% CI 0.22 to 0.41, eight studies, 5115 participants).
BDF versus placebo
Data were pooled from Calverley 2003; Rennard 2009; Szafranski 2003; and Tashkin 2008 for withdrawals due to adverse events, and from Calverley 2003; Rennard 2009 and Szafranski 2003 for withdrawals due to lack of efficacy or worsening COPD.
A significant difference favoured active treatment in withdrawals due to worsening of COPD symptoms when BDF was compared with placebo (OR 0.56, 95% CI 0.43 to 0.74, three studies, 2392 participants).
No significant difference was noted between BDF and placebo in the likelihood of withdrawal due to any adverse event (OR 0.85, 95% CI 0.70 to 1.03).
MF/F versus placebo
Significantly fewer withdrawals from treatment were seen with MF/F than with placebo for inhalers of both strengths (OR 0.56, 95% CI 0.40 to 0.77 for 400/10; and OR 0.55, 95% CI 0.40 to 0.76 for 200/10).
Of note, a significant difference favoured MF/F when withdrawals due to lack of efficacy of treatment or worsening of COPD symptoms were considered. This was true for inhalers of both strengths (OR 0.24, 95% CI 0.08 to 0.74 for 400/10; and OR 0.31, 95% CI 0.11 to 0.84 for 200/10).
Discussion
Summary of main results
We reviewed data from 19 randomised controlled trials (10,400 participants) assessing the efficacy and safety of combined inhaled corticosteroids and long‐acting beta2‐agonists versus placebo for the treatment of COPD. Thirteen studies involved a combined inhaler of fluticasone and salmeterol, four involved budesonide and formoterol and two involved mometasone and formoterol. The findings of this review complement those of two others assessing the effects of combination inhalers with their components, that is, LABA or ICS (Nannini 2012; Nannini 2013). Despite the addition of eight new studies for this update, most of the weight is still coming from the TORCH study, which is the largest trial of combined therapy (FPS) in COPD.
Primary outcomes
The main findings related to the primary outcomes of exacerbations, mortality, pneumonia and hospitalisations appear in the summary of findings Table for the main comparison. All eligible studies addressed at least one of the primary outcomes.
Combined therapy reduced the rate of moderate exacerbations compared with placebo by about a quarter (Analysis 1.1). But, as was found in the Cochrane reviews comparing combined inhalers with LABA alone or ICS alone (Nannini 2013), this did not translate to a statistically significant reduction in COPD hospitalisation rates. One explanation is that those receiving combined treatment who respond may have fewer and/or milder exacerbations, but equally the smaller number of hospitalisations means that less statistical power was present to show a significant difference. On the other hand, adverse effects were more common with combined treatment than with placebo, particularly the development of pneumonia. The NNTH for this outcome in studies of at least 52 weeks' duration varied from 17 to 197. Concern about pneumonia as an adverse event associated with ICS treatment has persisted ever since TORCH was published in 2006. Indeed our analysis shows that the excess of pneumonia is seen only with FPS, not with the other combined inhalers. If the TORCH study was not included, the significant OR disappeared, but heterogeneity among trials is still evident (Analysis 1.3), making it difficult to decide whether this effect is a true one. This may suggest ongoing difficulties with the accurate identification of pneumonia, or variations in participant populations, actions of medicines or the nature of lower respiratory tract infections and their treatment over the time course of a study. It is also possible that the heterogeneity in the pneumonia outcome is due to differential withdrawal rates. Withdrawal due to lack of efficacy in the FPS subgroup was greater in the placebo arm (Analysis 2.14), as was seen with BDF (Analysis 3.18) and MF/F studies (Analysis 4.8). It is interesting to note that withdrawals due to adverse events were not different between arms in BDF (Analysis 3.17), whereas for MF/F studies, withdrawals due to adverse events were greater in the placebo arm (Analysis 4.9). These findings suggest something different about the three‐year TORCH study compared with the others. Whatever the case, it is reassuring that this apparent excess of pneumonia cases did not translate into greater numbers of hospitalisations or exacerbations, or greater mortality rates. In fact, quite the opposite was noted—exacerbation rates and mortality were reduced with combined treatment.
We found that treatment with a combined inhaler led to a significant reduction in mortality compared with placebo when data from all studies were pooled. As with other outcomes, TORCH had a major influence on mortality; however, it should be noted that the TORCH investigators did not claim a significant reduction in mortality with FPS over placebo (P = 0.052). The difference between the study report and the OR reported in this Cochrane review may be due to variations in statistical methods. TORCH used a hazard ratio that was adjusted for repeated measurement. This analysis has been the subject of some debate as the study adopted a factorial design but did not report a factorial analysis (see Feedback 1, Feedback 2). Furthermore, although mortality was recorded in many of the studies, it was a primary outcome in TORCH. In that study, cause‐specific mortality was also reported, but the definition of a primary cause of death continues to pose challenges in a population of patients who may suffer from co‐morbidities such as lung cancer (McGarvey 2007).
Secondary outcomes
We were unable to pool secondary outcomes and reported results for each type of combined inhaler separately. Although the only way to test whether one product is better than another is a head‐to‐head comparison, we found that the results for all secondary outcomes, except adverse events, were relatively similar, that is, each combined inhaler showed a small benefit over placebo in effects on health‐related quality of life, symptoms, lung function, use of rescue medication and withdrawal rates. In some cases, the benefits reached accepted levels of clinical significance, but only just. Minimal clinical important differences (MCID) are sometimes used to help clinicians interpret trial findings in a meaningful way. The MCID for predose FEV1 is thought to be approximately 100 mL (Donohue 2005). Leidy 2003 suggests that changes of 1.0 in the BCSS represent substantial symptomatic improvement, changes of approximately 0.6 can be interpreted as moderate and changes of 0.3 can be considered small. A four‐unit difference is the generally accepted MCID for SGRQ score (Jones 2005). Mean differences reflect an unknown range of results from individual participants, and although an MCID may be achieved on average, this neither confirms nor rules out meaningful improvement over placebo for all. Furthermore, for some of these outcomes, a high degree of heterogeneity was noted, some of which may be due to differences in study protocols.
Overall completeness and applicability of evidence
Participants and outcomes reported were typical of those described for COPD patients. The most abundant evidence comes from studies on the FPS combination, which was the only one to show a mortality benefit. Fewer data are available for the MF/F combination, but nothing has been discovered to suggest that it behaves differently from the other inhalers.
This review addresses the efficacy and safety of combined ICS and LABA in one inhaler versus placebo as a pair‐wise comparison. We did not seek to address the efficacy of the individual components (LABA and ICS) versus combined treatment, although such comparisons were included in some of studies in this review, notably the TORCH trial. In this large trial, it appears that the mortality benefit, while not reaching statistical significance, is driven largely by the LABA component of combined therapy. The efficacy of the individual components versus combined therapy is addressed in two linked Cochrane reviews (Nannini 2012; Nannini 2013) and will be included in a forthcoming network meta‐analysis (Oba 2017).
Quality of the evidence
Most trials were industry‐sponsored. The risk of bias in blinding was considered low for all trials. The risk of bias from attrition was considered higher because of the number of participants withdrawn (over 20% in most trials), especially as this group may represent a more severely involved subgroup (Kesten 2007). In addition, we found significantly greater participant withdrawal in the placebo arm across all three combined inhalers (Analysis 2.12, Analysis 3.16 and Analysis 4.7). However, the completion rate in the included trials was generally equal to, or better than, that of other trials involving participants with COPD. Selective reporting was generally considered to be of low risk.
Intention‐to‐treat analyses were conducted in all studies, but for outcomes such as mean exacerbation rates, withdrawal of severe frequent exacerbators from the studies may have distorted study findings because of the lower exacerbation rates seen with active treatment. Loss of participants with more frequent exacerbations from the studies may thus limit the accuracy of mean event rates. The question of exacerbations and the appropriate statistical analysis of rate ratios cast some doubt regarding the validity of some of the findings in this review. In particular, the large long‐term studies (i.e. those in excess of six months), which are adequately powered to detect statistically significant findings, may overestimate the treatment effects of this therapy (Suissa 2006). The method of weighting counts of exacerbations as described by Suissa 2006 (using duration of person follow‐up time as a denominator in calculating the mean group rate of exacerbations rather than an unweighted approach) was undertaken in Calverley 2003; Szafranski 2003;and TORCH. In these studies, the effects were consistent and significantly favoured combination therapy over placebo. However, the major primary outcome after mortality rate was hospitalisation due to COPD exacerbation, and this did not show any difference between treatments.
Visual inspection of a funnel plot for the mortality outcome does not suggest publication bias (Figure 6).

Funnel plot of comparison: 1 Combined inhalers versus placebo (primary outcomes), outcome: 1.2 Mortality.
Potential biases in the review process
The Cochrane Airways Group provided an excellent level of support in the identification of potentially relevant trials. To minimise the risk of selection and publication bias, an exhaustive search of the published literature and the unpublished literature, with no language restrictions, for potentially relevant clinical trials was underpinned by a systematic search strategy. Trial selection and data extraction followed a prespecified protocol, and the process was independently conducted by two review authors. Nevertheless, we acknowledge that additional unidentified trials may exist.
Agreements and disagreements with other studies or reviews
This Cochrane review confirms and builds upon an earlier one (Nannini 2004) and upon related reviews (Nannini 2012; Nannini 2013). For this update, we checked all previous data and added hospital admissions using COPD‐related serious adverse events as a surrogate marker. To enhance clarity, several outcomes in the FPS subgroup with few contributing studies have been deleted from the current update. We have added data for MF/F versus placebo, as these studies took place after the previous review.
Our finding that combined inhaler therapy reduced death is concordant with that of another review of all inhaled medications in COPD, which concluded that ICS/LABA was associated with the lowest risk of death among all treatments (Dong 2013).

Methodological quality summary: review authors' judgements about each methodological quality item for each included study.

Forest plot of comparison: 1 Combined inhalers versus placebo (primary outcomes), outcome: 1.1 Exacerbation rates with combined inhalers versus placebo.

Forest plot of comparison: 1 Combined inhalers versus placebo (primary outcomes), outcome: 1.2 Mortality.

Forest plot of comparison: 1 Combined inhalers versus placebo (primary outcomes), outcome: 1.3 Pneumonia.
Forest plot of comparison: 1 Combined inhalers versus placebo (primary outcomes), outcome: 1.4 Hospitalisations due to COPD exacerbations.

Funnel plot of comparison: 1 Combined inhalers versus placebo (primary outcomes), outcome: 1.2 Mortality.
Comparison 1 Combined inhalers versus placebo (primary outcomes), Outcome 1 Exacerbation rates with combined inhalers versus placebo.

Comparison 1 Combined inhalers versus placebo (primary outcomes), Outcome 2 Mortality.
Comparison 1 Combined inhalers versus placebo (primary outcomes), Outcome 3 Pneumonia.
Comparison 1 Combined inhalers versus placebo (primary outcomes), Outcome 4 Hospitalisations due to COPD exacerbations.

Comparison 1 Combined inhalers versus placebo (primary outcomes), Outcome 5 Number of participants with at least one exacerbation.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 1 Exacerbations.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 2 Number of participants with at least one exacerbation.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 3 Participants with at least one exacerbation by type.
Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 4 Exacerbations by type.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 5 Mortality.
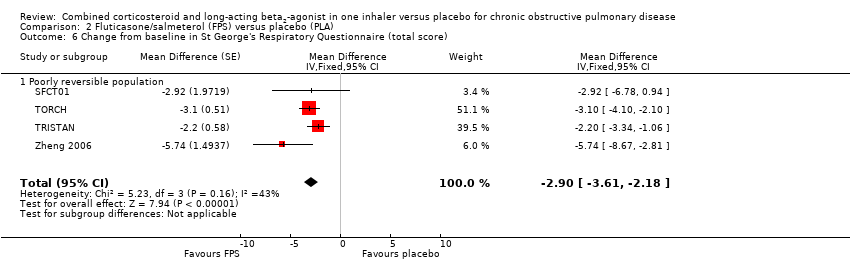
Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 6 Change from baseline in St George's Respiratory Questionnaire (total score).

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 7 Change from baseline in Chronic Respiratory Disease Questionnaire scores.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 8 Change from baseline in Transitional Dyspnoea Index (TDI) scores.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 9 Change from baseline in predose FEV1.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 10 Change from baseline in postdose FEV1.
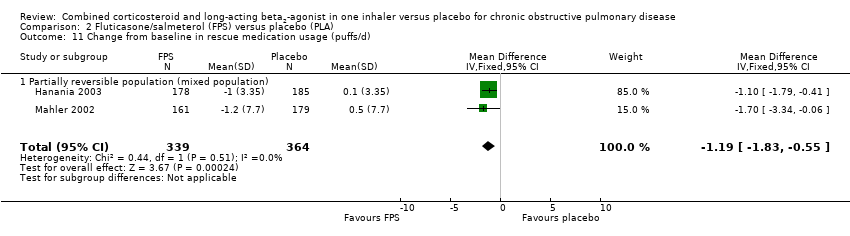
Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 11 Change from baseline in rescue medication usage (puffs/d).
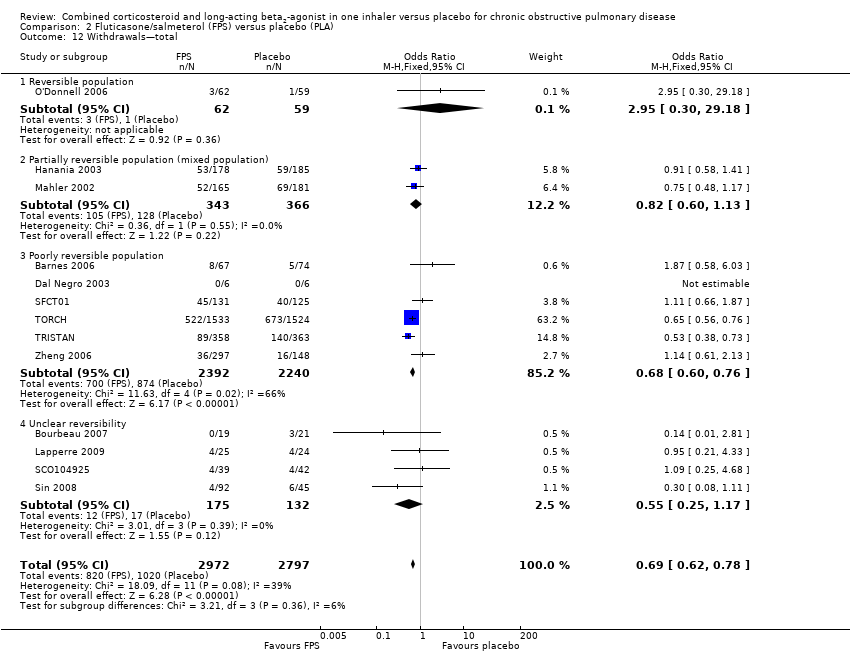
Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 12 Withdrawals—total.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 13 Withdrawals due to adverse events.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 14 Withdrawals due to lack of efficacy.
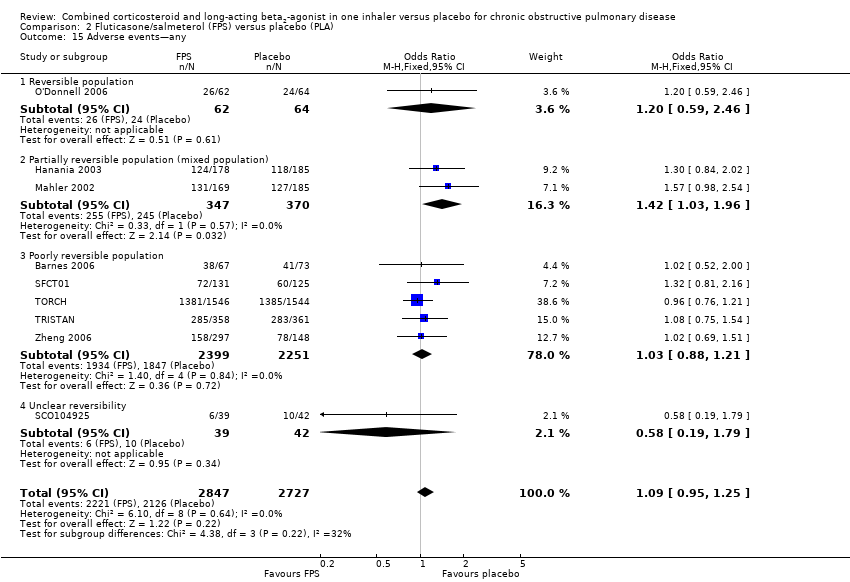
Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 15 Adverse events—any.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 16 Adverse events—'serious'.
Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 17 Adverse events—pneumonia.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 18 Adverse events—candidiasis.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 19 Adverse events—hoarseness.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 20 Adverse events—palpitations.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 21 Adverse events—blood glucose increased.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 22 Adverse event—skin bruising.
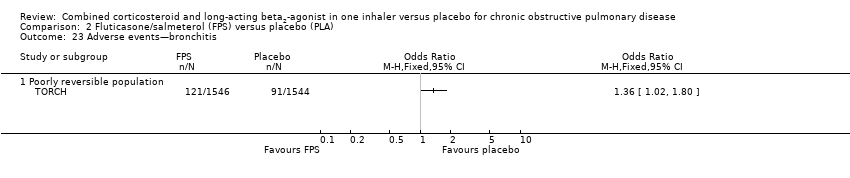
Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 23 Adverse events—bronchitis.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 24 Adverse events—upper respiratory tract infection.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 25 Adverse events—nasopharyngitis.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 26 Adverse events—cough.

Comparison 2 Fluticasone/salmeterol (FPS) versus placebo (PLA), Outcome 27 Adverse events—headache.

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 1 Severe exacerbations.

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 2 Mean severe exacerbation rates per participant per year.
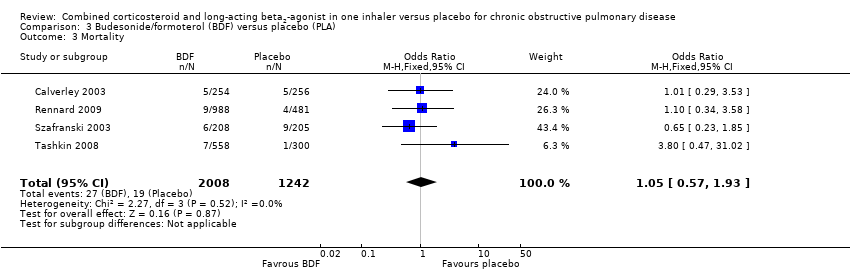
Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 3 Mortality.
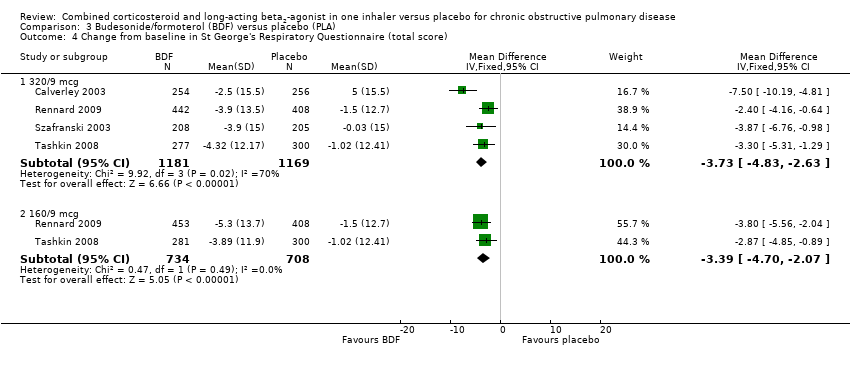
Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 4 Change from baseline in St George's Respiratory Questionnaire (total score).

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 5 Quality of life—change scores.

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 6 Symptoms (change scores).

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 7 Breathlessness, cough and sputum score (BCSS) change from baseline—average over treatment period.
Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 8 Rescue medication usage.

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 9 Mean FEV1 (% change from baseline).

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 10 Average 12‐hour FEV1 change from baseline—end of treatment (L).
![Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 11 Predose FEV1 [L] change from baseline to the average over the randomised treatment period.](/es/cdsr/doi/10.1002/14651858.CD003794.pub4/media/CDSR/CD003794/image_n/nCD003794-CMP-003-11.png)
Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 11 Predose FEV1 [L] change from baseline to the average over the randomised treatment period.
![Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 12 1 Hour postdose FEV1 [L] change from baseline to the average over the randomised treatment period.](/es/cdsr/doi/10.1002/14651858.CD003794.pub4/media/CDSR/CD003794/image_n/nCD003794-CMP-003-12.png)
Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 12 1 Hour postdose FEV1 [L] change from baseline to the average over the randomised treatment period.

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 13 FEV1 at 12‐hour change from baseline—end of treatment (L).

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 14 Morning PEFR change from baseline, average over treatment period (L/min).

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 15 Evening PEFR mean change from baseline, average over treatment period (L/min).

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 16 Withdrawals—total.

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 17 Withdrawals due to adverse events.
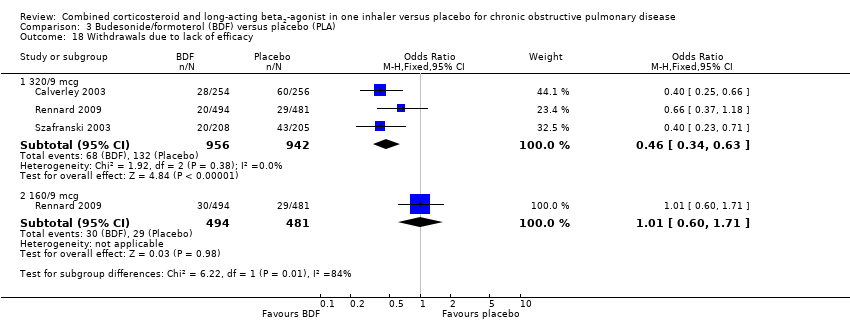
Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 18 Withdrawals due to lack of efficacy.

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 19 Adverse event—any.

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 20 Adverse events—'serious'.

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 21 Adverse events—pneumonia.
Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 22 Adverse events—candidiasis.

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 23 Adverse events—dysphonia.

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 24 Adverse events—cataracts.

Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 25 Adverse events—COPD.
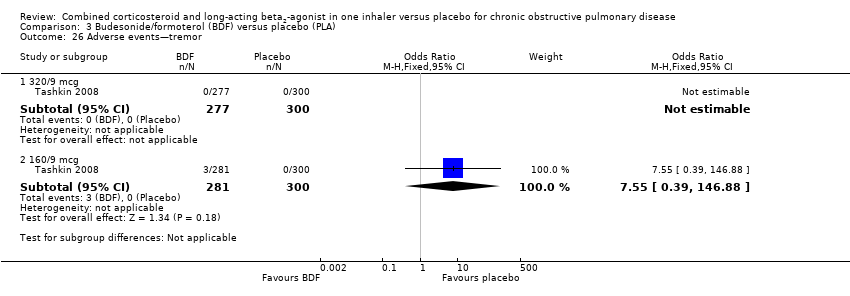
Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 26 Adverse events—tremor.
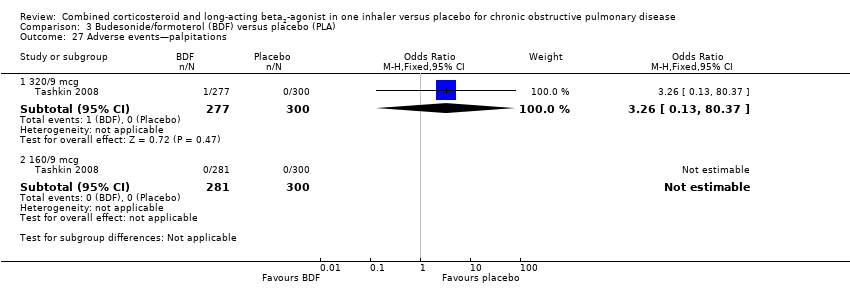
Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 27 Adverse events—palpitations.
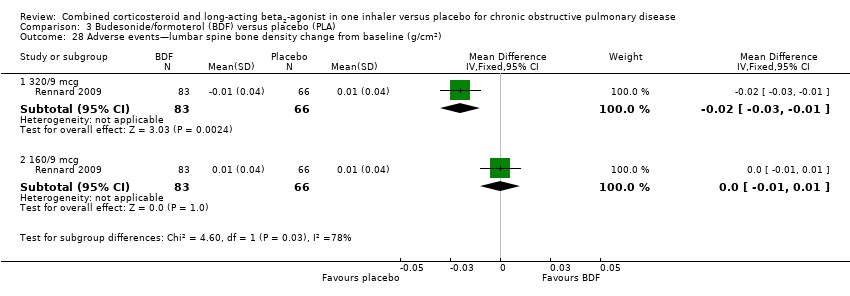
Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 28 Adverse events—lumbar spine bone density change from baseline (g/cm2).
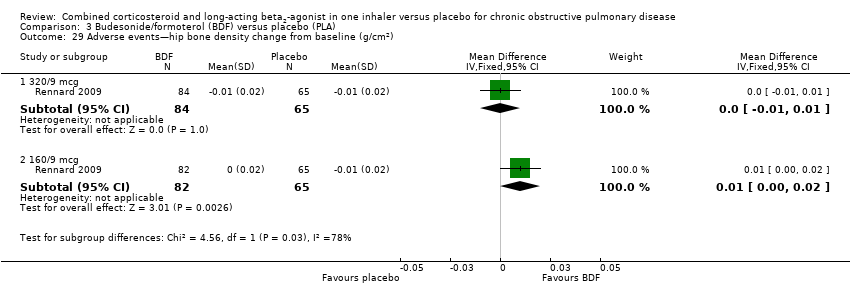
Comparison 3 Budesonide/formoterol (BDF) versus placebo (PLA), Outcome 29 Adverse events—hip bone density change from baseline (g/cm2).

Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 1 Number of participants with at least one exacerbation.

Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 2 Number of participants having at least one moderate or severe exacerbation.

Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 3 Mortality.

Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 4 Change from baseline in St George's Respiratory Questionnaire (total score).
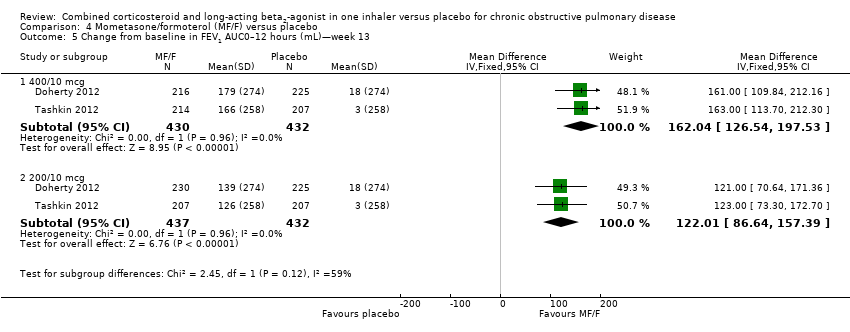
Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 5 Change from baseline in FEV1 AUC0–12 hours (mL)—week 13.

Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 6 Mean change from baseline AM predose FEV1 at 13 weeks (mL).
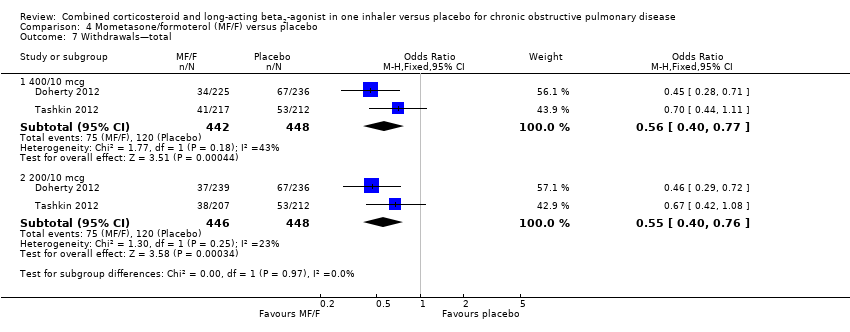
Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 7 Withdrawals—total.
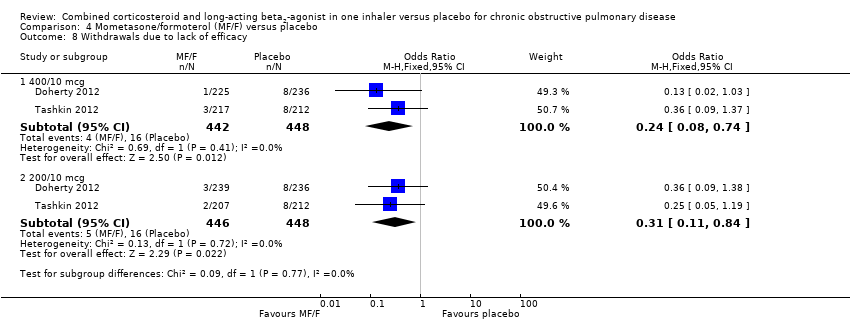
Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 8 Withdrawals due to lack of efficacy.
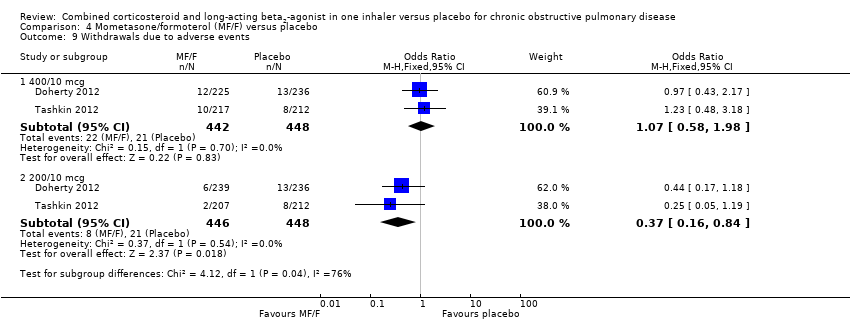
Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 9 Withdrawals due to adverse events.

Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 10 Adverse events—any.
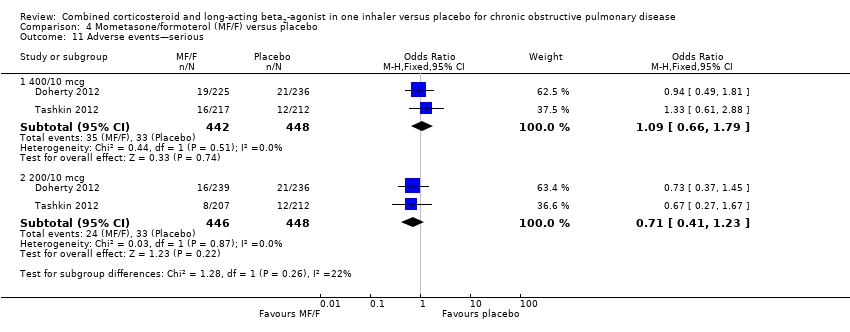
Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 11 Adverse events—serious.

Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 12 Adverse events—pneumonia.
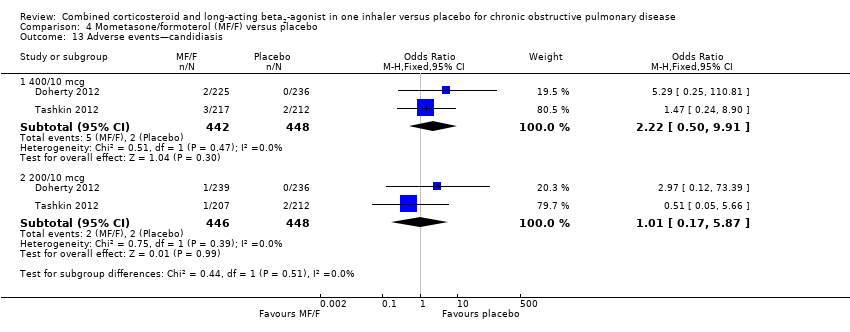
Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 13 Adverse events—candidiasis.

Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 14 Adverse events—dysphonia.

Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 15 Adverse events—cataract.

Comparison 4 Mometasone/formoterol (MF/F) versus placebo, Outcome 16 Adverse events—COPD requiring hospitalisation.
| Combined inhalers versus placebo (primary outcomes) for chronic obstructive pulmonary disease (COPD) | ||||||
| Patient or population: patients with COPD Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Combined inhalers versus placebo (primary outcomes) | |||||
| Annual exacerbation rates | 1.35 | 0.99 (0.93 to 1.05) | Rate ratio 0.73 (0.69 to 0.78) | 7473 (seven studies) | ⊕⊕⊕⊝ | |
| Participants with at least one exacerbation Duration of six months3 | 301 per 1000 | 251 per 1000 (221 to 286) | OR 0.78 | 3141 (eight studies) | ⊕⊕⊕⊝ | |
| Mortality Duration of 18 months3 | 60 per 1000 | 50 per 1000 | OR 0.82 | 10129 | ⊕⊕⊕⊝ | |
| Pneumonia Duration of 18 months3 | 55 per 1000 | 85 per 1000 | OR 1.62 | 9620 | ⊕⊕⊕⊝ | |
| Hospitalisations due to COPD exacerbations Duration of 18 months3 | 115 per 1000 | 108 per 1000 | OR 0.93 | 9492 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| 1Downgraded because of risk of attrition bias. 2Concerns have been raised about the analysis of the largest study, TORCH. We note that the protocol was published after the trial had recruited (See Feedback 1, Feedback 2). No downgrade. 3Weighted mean duration. 4Downgraded because of imprecision. 5Downgraded because of risk of attrition bias and imprecision. | ||||||
| Fluticasone/salmeterol (FPS) versus placebo for COPD | ||||||
| Patient or population: patients with COPD Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Fluticasone/salmeterol (FPS) versus placebo (PLA) | |||||
| Adverse events—any Duration of two years1 | 780 per 1000 | 794 per 1000 | OR 1.09 | 5574 | ⊕⊕⊝⊝ | |
| Adverse events—'serious' Duration of two years1 | 271 per 1000 | 287 per 1000 | OR 1.08 | 5531 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| 1Weighted mean duration. 2Downgraded because of risk of attrition bias and imprecision. 3Concerns have been raised about the analysis of the largest study, TORCH. We note that the protocol was published after the trial had recruited (See Feedback 1, Feedback 2). | ||||||
| Budesonide/formoterol (BDF) versus placebo for COPD | ||||||
| Patient or population: patients with COPD Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Budesonide/formoterol (BDF) versus placebo | |||||
| Adverse event—any—320/94 Duration of nine months 3 | 538 per 1000 | 623 per 1000 | OR 1.42 | 1552 | ⊕⊕⊝⊝ | |
| Adverse event—any—160/94 Duration of nine months 3 | 538 per 1000 | 606 per 1000 | OR 1.32 | 1556 | ⊕⊕⊝⊝ | |
| Adverse events—'serious'—320/94 Duration of 10 months3 | 162 per 1000 | 184 per 1000 | OR 1.17 | 2476 | ⊕⊕⊝⊝ | |
| Adverse events—'serious'—160/94 Duration of nine months 3 | 113 per 1000 | 132 per 1000 | OR 1.2 | 1556 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| 1Downgraded because of risk of attrition bias and imprecision and heterogeneity. 3Weighted mean duration. 4Delivered dose. | ||||||
| Mometasone/formoterol (MF/F) versus placebo for COPD | ||||||
| Patient or population: patients with chronic obstructive pulmonary disease Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Mometasone/formoterol (MF/F) versus placebo | |||||
| Adverse event—any—400/103 Duration of six months | 362 per 1000 | 357 per 1000 | OR 0.98 | 890 | ⊕⊕⊝⊝ | |
| Adverse event—any—200/103 Duration of six months | 362 per 1000 | 317 per 1000 | OR 0.82 | 894 | ⊕⊕⊝⊝ | |
| Adverse events—serious—400/103 Duration of six months | 74 per 1000 | 80 per 1000 | OR 1.09 | 890 | ⊕⊕⊝⊝ | |
| Adverse events—serious—200/103 Duration of six months | 74 per 1000 | 53 per 1000 | OR 0.71 | 894 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| 1Downgraded because of risk of attrition bias, imprecision and heterogeneity. 3Delivered dose. | ||||||
| Version | Detail |
| First published version—Issue 4, 2003 (all years to April 2002) | References identified: 34 |
| Second published version—Issue 3, 2004 (April 2003 to April 2004) | References identified: 12 |
| Third published version—Issue 3, 2005 (April 2004 to April 2005) | References identified: 52 |
| Fourth published version (April 2005 to April 2007) | References identified: 66 |
| Fifth published version (April 2007 to June 2013) | References identified: 129 New unique studies identified: eight (ongoing studies: zero) New studies included: eight Total studies included: 19 |
| Study ID | Study duration | Placebo rate (%) mortality | NNTB for mortality | Placebo rate (%) pneumonia | NNTH for pneumonia |
| 156 weeks | 15.2 | 42 (24 to 775) | 12.3 | 17 (27 to 12) | |
| 52 weeks | 1.94 | 292 (164 to 5256) | 0.83 | 197 (339 to 131) | |
| 52 weeks | 1.95 | 249 (149 to 1307) | 3.6 | 48 (82 to 32) | |
| 52 weeks | 4.5 | 110 (66 to 581) | 0 | N/A | |
| 52 weeks | 0.83 | 674 (379 to 12,149) | 4.78 | 37 (63 to 25) | |
| 26 weeks | 0.33 | 1689 (950 to 30,403) | 1 | 164 (282 to 109) | |
| 26 weeks | 0.85 | 659 (370 to 11,865) | 0.85 | 193 (331 to 128) | |
| 26 weeks | 0.47 | 1187 (668 to 21,377) | 0.47 | 346 (595 to 229) | |
| 24 weeks | 1.66 | 340 (191 to 6125) | 0 | N/A | |
| 8 weeks | 0 | N/A | 1.56 | 107 (182 to 71) |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Exacerbation rates with combined inhalers versus placebo Show forest plot | 7 | Rate Ratio (Fixed, 95% CI) | 0.73 [0.69, 0.78] | |
| 1.1 Fluticasone/salmeterol | 3 | Rate Ratio (Fixed, 95% CI) | 0.74 [0.69, 0.80] | |
| 1.2 Budesonide/formoterol | 4 | Rate Ratio (Fixed, 95% CI) | 0.71 [0.62, 0.81] | |
| 2 Mortality Show forest plot | 16 | 10129 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.68, 0.99] |
| 2.1 Fluticasone/salmeterol | 10 | 5543 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.79 [0.65, 0.97] |
| 2.2 Budesonide/formoterol | 4 | 3250 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.57, 1.93] |
| 2.3 Mometasone/formoterol | 2 | 1336 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.35 [0.36, 5.13] |
| 3 Pneumonia Show forest plot | 14 | 9620 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.62 [1.36, 1.94] |
| 3.1 Fluticasone/salmeterol | 9 | 5447 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.76 [1.46, 2.14] |
| 3.2 Budesonide/formoterol | 3 | 2837 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.57, 1.47] |
| 3.3 Mometasone/formoterol | 2 | 1336 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.39 [0.68, 8.36] |
| 4 Hospitalisations due to COPD exacerbations Show forest plot | 12 | 9492 | Odds Ratio (M‐H, Random, 95% CI) | 0.92 [0.80, 1.06] |
| 4.1 Fluticasone/salmeterol | 7 | 5309 | Odds Ratio (M‐H, Random, 95% CI) | 0.89 [0.75, 1.04] |
| 4.2 Budesonide/formoterol | 3 | 2847 | Odds Ratio (M‐H, Random, 95% CI) | 1.17 [0.87, 1.58] |
| 4.3 Mometasone/formoterol | 2 | 1336 | Odds Ratio (M‐H, Random, 95% CI) | 0.57 [0.31, 1.07] |
| 5 Number of participants with at least one exacerbation Show forest plot | 9 | 3141 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.78 [0.66, 0.93] |
| 5.1 Fluticasone/salmeterol | 7 | 1817 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.64, 1.07] |
| 5.2 Mometasone/formoterol | 2 | 1324 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.74 [0.58, 0.94] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Exacerbations Show forest plot | 3 | 3777 | Rate ratio (Fixed, 95% CI) | 0.74 [0.69, 0.80] |
| 1.1 Poorly reversible population | 3 | 3777 | Rate ratio (Fixed, 95% CI) | 0.74 [0.69, 0.80] |
| 2 Number of participants with at least one exacerbation Show forest plot | 7 | 1817 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.64, 1.07] |
| 2.1 Reversible population | 1 | 126 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.32 [0.06, 1.66] |
| 2.2 Partially reversible population (mixed population) | 2 | 713 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.69, 1.44] |
| 2.3 Poorly reversible population | 3 | 841 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.79 [0.54, 1.15] |
| 2.4 Unclear reversibility | 1 | 137 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.31 [0.09, 1.05] |
| 3 Participants with at least one exacerbation by type Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.1 Requirement for oral steroids | 2 | 417 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.61, 1.68] |
| 3.2 Requirement for antibiotic treatment | 1 | 140 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.26, 2.44] |
| 3.3 Requirement for oral steroid or antibiotic treatment | 1 | 140 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.32 [0.13, 82.80] |
| 3.4 Hospitalisation | 1 | 140 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.32 [0.13, 82.80] |
| 4 Exacerbations by type Show forest plot | 3 | Rate ratio (Fixed, 95% CI) | Subtotals only | |
| 4.1 Requirement for oral steroids | 3 | Rate ratio (Fixed, 95% CI) | 0.57 [0.52, 0.63] | |
| 4.2 Requirement for antibiotic treatment | 1 | Rate ratio (Fixed, 95% CI) | 0.60 [0.41, 0.88] | |
| 4.3 Hospitalisation | 2 | Rate ratio (Fixed, 95% CI) | 0.83 [0.70, 0.97] | |
| 5 Mortality Show forest plot | 10 | 5543 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.79 [0.65, 0.97] |
| 5.1 Mortality: three‐year data | 1 | 3057 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.81 [0.66, 0.99] |
| 5.2 Mortality: one‐year data | 3 | 987 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.46 [0.13, 1.65] |
| 5.3 Mortality: six‐month data | 3 | 1154 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.54 [0.11, 2.75] |
| 5.4 Mortality: three‐month data | 3 | 345 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Change from baseline in St George's Respiratory Questionnaire (total score) Show forest plot | 4 | Mean Difference (Fixed, 95% CI) | ‐2.90 [‐3.61, ‐2.18] | |
| 6.1 Poorly reversible population | 4 | Mean Difference (Fixed, 95% CI) | ‐2.90 [‐3.61, ‐2.18] | |
| 7 Change from baseline in Chronic Respiratory Disease Questionnaire scores Show forest plot | 2 | 712 | Mean Difference (IV, Fixed, 95% CI) | 5.0 [2.48, 7.52] |
| 7.1 Partially reversible population (mixed population) | 2 | 712 | Mean Difference (IV, Fixed, 95% CI) | 5.0 [2.48, 7.52] |
| 8 Change from baseline in Transitional Dyspnoea Index (TDI) scores Show forest plot | 2 | 707 | Mean Difference (IV, Fixed, 95% CI) | 1.04 [0.56, 1.53] |
| 8.1 Partially reversible population (mixed population) | 2 | 707 | Mean Difference (IV, Fixed, 95% CI) | 1.04 [0.56, 1.53] |
| 9 Change from baseline in predose FEV1 Show forest plot | 5 | Mean Difference (Fixed, 95% CI) | 0.16 [0.14, 0.19] | |
| 9.1 Reversible population | 3 | Mean Difference (Fixed, 95% CI) | 0.19 [0.15, 0.24] | |
| 9.2 Poorly reversible population | 4 | Mean Difference (Fixed, 95% CI) | 0.15 [0.11, 0.18] | |
| 10 Change from baseline in postdose FEV1 Show forest plot | 2 | Mean Difference (Fixed, 95% CI) | 0.09 [0.07, 0.11] | |
| 10.1 Poorly reversible population | 2 | Mean Difference (Fixed, 95% CI) | 0.09 [0.07, 0.11] | |
| 11 Change from baseline in rescue medication usage (puffs/d) Show forest plot | 2 | 703 | Mean Difference (IV, Fixed, 95% CI) | ‐1.19 [‐1.83, ‐0.55] |
| 11.1 Partially reversible population (mixed population) | 2 | 703 | Mean Difference (IV, Fixed, 95% CI) | ‐1.19 [‐1.83, ‐0.55] |
| 12 Withdrawals—total Show forest plot | 13 | 5769 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.69 [0.62, 0.78] |
| 12.1 Reversible population | 1 | 121 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.95 [0.30, 29.18] |
| 12.2 Partially reversible population (mixed population) | 2 | 709 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.60, 1.13] |
| 12.3 Poorly reversible population | 6 | 4632 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.68 [0.60, 0.76] |
| 12.4 Unclear reversibility | 4 | 307 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.55 [0.25, 1.17] |
| 13 Withdrawals due to adverse events Show forest plot | 11 | 5491 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.74 [0.64, 0.86] |
| 13.1 Reversible population | 1 | 123 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.36 [0.01, 8.90] |
| 13.2 Partially reversible population (mixed population) | 1 | 354 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.69 [0.31, 1.51] |
| 13.3 Poorly reversible population | 6 | 4630 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.65, 0.89] |
| 13.4 Unclear reversibility | 4 | 384 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.31 [0.11, 0.93] |
| 14 Withdrawals due to lack of efficacy Show forest plot | 8 | 5115 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.30 [0.22, 0.41] |
| 14.1 Partially reversible population (mixed population) | 1 | 346 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.29 [0.08, 1.04] |
| 14.2 Poorly reversible population | 6 | 4632 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.30 [0.21, 0.42] |
| 14.3 Unclear reversibility | 1 | 137 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.30 [0.08, 1.11] |
| 15 Adverse events—any Show forest plot | 9 | 5574 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.09 [0.95, 1.25] |
| 15.1 Reversible population | 1 | 126 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.20 [0.59, 2.46] |
| 15.2 Partially reversible population (mixed population) | 2 | 717 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.42 [1.03, 1.96] |
| 15.3 Poorly reversible population | 5 | 4650 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.88, 1.21] |
| 15.4 Unclear reversibility | 1 | 81 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.58 [0.19, 1.79] |
| 16 Adverse events—'serious' Show forest plot | 9 | 5531 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.95, 1.23] |
| 16.1 Reversible population | 1 | 123 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.53 [0.05, 6.05] |
| 16.2 Partially reversible population | 2 | 709 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.38, 1.35] |
| 16.3 Poorly reversible population | 6 | 4699 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.97, 1.26] |
| 17 Adverse events—pneumonia Show forest plot | 9 | 5447 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.80 [1.49, 2.18] |
| 17.1 Reversible population | 1 | 126 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.34 [0.01, 8.47] |
| 17.2 Partially reversible population (mixed population) | 2 | 709 | Odds Ratio (M‐H, Fixed, 95% CI) | 5.55 [0.26, 116.46] |
| 17.3 Poorly reversible population | 4 | 4394 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.80 [1.48, 2.18] |
| 17.4 Unclear reversibility | 2 | 218 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.31 [0.13, 83.73] |
| 18 Adverse events—candidiasis Show forest plot | 7 | 2039 | Odds Ratio (M‐H, Fixed, 95% CI) | 5.73 [3.07, 10.67] |
| 18.1 Reversible population | 1 | 126 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.06, 16.88] |
| 18.2 Partially reversible population (mixed population) | 2 | 717 | Odds Ratio (M‐H, Fixed, 95% CI) | 11.13 [3.36, 36.90] |
| 18.3 Poorly reversible population | 3 | 1115 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.40 [2.01, 9.62] |
| 18.4 Unclear reversibility | 1 | 81 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 19 Adverse events—hoarseness Show forest plot | 2 | 585 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.61 [0.61, 4.26] |
| 19.1 Poorly reversible population | 2 | 585 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.61 [0.61, 4.26] |
| 20 Adverse events—palpitations Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 20.1 Poorly reversible population | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 21 Adverse events—blood glucose increased Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 21.1 Poorly reversible population | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 22 Adverse event—skin bruising Show forest plot | 1 | 445 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 22.1 Poorly reversible population | 1 | 445 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 23 Adverse events—bronchitis Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 23.1 Poorly reversible population | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 24 Adverse events—upper respiratory tract infection Show forest plot | 5 | 4963 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.23 [1.04, 1.47] |
| 24.1 Partially reversible population (mixed population) | 2 | 709 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.25 [0.81, 1.92] |
| 24.2 Poorly reversible population | 3 | 4254 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.23 [1.02, 1.48] |
| 25 Adverse events—nasopharyngitis Show forest plot | 2 | 3535 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.28 [1.05, 1.56] |
| 25.1 Poorly reversible population | 2 | 3535 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.28 [1.05, 1.56] |
| 26 Adverse events—cough Show forest plot | 3 | 612 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.55 [0.23, 1.27] |
| 26.1 Reversible population | 1 | 126 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.15 [0.13, 78.72] |
| 26.2 Partially reversible population (mixed population) | 1 | 346 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.49 [0.18, 1.31] |
| 26.3 Poorly reversible population | 1 | 140 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.35 [0.04, 3.48] |
| 27 Adverse events—headache Show forest plot | 4 | 3922 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.84, 1.31] |
| 27.1 Reversible population | 1 | 123 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.22 [0.02, 2.01] |
| 27.2 Partially reversible population (mixed population) | 2 | 709 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.38 [0.91, 2.10] |
| 27.3 Poorly reversible population | 1 | 3090 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.73, 1.26] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Severe exacerbations Show forest plot | 2 | Rate ratio (Fixed, 95% CI) | 0.74 [0.62, 0.88] | |
| 1.1 Poorly reversible | 2 | Rate ratio (Fixed, 95% CI) | 0.74 [0.62, 0.88] | |
| 2 Mean severe exacerbation rates per participant per year Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2.1 Poorly reversible population | 2 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Mortality Show forest plot | 4 | 3250 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.57, 1.93] |
| 4 Change from baseline in St George's Respiratory Questionnaire (total score) Show forest plot | 4 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 4.1 320/9 mcg | 4 | 2350 | Mean Difference (IV, Fixed, 95% CI) | ‐3.73 [‐4.83, ‐2.63] |
| 4.2 160/9 mcg | 2 | 1442 | Mean Difference (IV, Fixed, 95% CI) | ‐3.39 [‐4.70, ‐2.07] |
| 5 Quality of life—change scores Show forest plot | 2 | SGRQ (Fixed, 95% CI) | ‐6.06 [‐7.90, ‐4.22] | |
| 5.1 Poorly reversible | 2 | SGRQ (Fixed, 95% CI) | ‐6.06 [‐7.90, ‐4.22] | |
| 6 Symptoms (change scores) Show forest plot | 2 | Symptom scale (Fixed, 95% CI) | ‐0.63 [‐0.90, ‐0.37] | |
| 6.1 Poorly reversible | 2 | Symptom scale (Fixed, 95% CI) | ‐0.63 [‐0.90, ‐0.37] | |
| 7 Breathlessness, cough and sputum score (BCSS) change from baseline—average over treatment period Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 7.1 320/9 mcg | 2 | 1533 | Mean Difference (IV, Fixed, 95% CI) | ‐0.43 [‐0.59, ‐0.26] |
| 7.2 160/9 mcg | 2 | 1536 | Mean Difference (IV, Fixed, 95% CI) | ‐0.44 [‐0.60, ‐0.28] |
| 8 Rescue medication usage Show forest plot | 4 | Mean Difference (Fixed, 95% CI) | Subtotals only | |
| 8.1 320/9 mcg | 4 | Mean Difference (Fixed, 95% CI) | ‐0.98 [‐1.18, ‐0.79] | |
| 8.2 160/9 mcg | 2 | Mean Difference (Fixed, 95% CI) | ‐1.28 [‐1.55, ‐1.00] | |
| 9 Mean FEV1 (% change from baseline) Show forest plot | 2 | Mean Difference (Fixed, 95% CI) | 14.40 [11.91, 16.90] | |
| 9.1 Poorly reversible | 2 | Mean Difference (Fixed, 95% CI) | 14.40 [11.91, 16.90] | |
| 10 Average 12‐hour FEV1 change from baseline—end of treatment (L) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 10.1 320/9 mcg | 1 | 246 | Mean Difference (IV, Fixed, 95% CI) | 0.19 [0.12, 0.26] |
| 10.2 160/9 mcg | 1 | 245 | Mean Difference (IV, Fixed, 95% CI) | 0.16 [0.10, 0.22] |
| 11 Predose FEV1 [L] change from baseline to the average over the randomised treatment period Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 11.1 320/9 mcg | 1 | 577 | Mean Difference (IV, Fixed, 95% CI) | 0.08 [0.04, 0.12] |
| 11.2 160/9 mcg | 1 | 581 | Mean Difference (IV, Fixed, 95% CI) | 0.06 [0.03, 0.09] |
| 12 1 Hour postdose FEV1 [L] change from baseline to the average over the randomised treatment period Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 12.1 320/9 mcg | 1 | 577 | Mean Difference (IV, Fixed, 95% CI) | 0.17 [0.14, 0.20] |
| 12.2 160/9 mcg | 1 | 581 | Mean Difference (IV, Fixed, 95% CI) | 0.16 [0.13, 0.19] |
| 13 FEV1 at 12‐hour change from baseline—end of treatment (L) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 13.1 320/9 mcg | 1 | 246 | Mean Difference (IV, Fixed, 95% CI) | 0.1 [0.03, 0.17] |
| 13.2 160/9 mcg | 1 | 245 | Mean Difference (IV, Fixed, 95% CI) | 0.07 [0.00, 0.14] |
| 14 Morning PEFR change from baseline, average over treatment period (L/min) Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 14.1 320/9 mcg | 2 | 1530 | Mean Difference (IV, Fixed, 95% CI) | 19.12 [15.69, 22.55] |
| 14.2 160/9 mcg | 2 | 1535 | Mean Difference (IV, Fixed, 95% CI) | 14.63 [11.47, 17.80] |
| 15 Evening PEFR mean change from baseline, average over treatment period (L/min) Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 15.1 320/9 mcg | 2 | 1529 | Mean Difference (IV, Fixed, 95% CI) | 16.09 [12.61, 19.57] |
| 15.2 160/9 mcg | 2 | 1531 | Mean Difference (IV, Fixed, 95% CI) | 12.74 [9.56, 15.91] |
| 16 Withdrawals—total Show forest plot | 4 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 16.1 320/9 mcg | 4 | 2475 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.57 [0.48, 0.68] |
| 16.2 160/9 mcg | 2 | 1556 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.62 [0.50, 0.78] |
| 17 Withdrawals due to adverse events Show forest plot | 4 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 17.1 320/9 mcg | 4 | 2475 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.79 [0.61, 1.01] |
| 17.2 160/9 mcg | 2 | 1556 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.70, 1.30] |
| 18 Withdrawals due to lack of efficacy Show forest plot | 3 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 18.1 320/9 mcg | 3 | 1898 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.46 [0.34, 0.63] |
| 18.2 160/9 mcg | 1 | 975 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.60, 1.71] |
| 19 Adverse event—any Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 19.1 320/9 mcg | 2 | 1552 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.42 [1.16, 1.74] |
| 19.2 160/9 mcg | 2 | 1556 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.32 [1.08, 1.61] |
| 20 Adverse events—'serious' Show forest plot | 4 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 20.1 320/9 mcg | 4 | 2476 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.17 [0.95, 1.45] |
| 20.2 160/9 mcg | 2 | 1556 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.20 [0.89, 1.63] |
| 21 Adverse events—pneumonia Show forest plot | 3 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 21.1 320/9 mcg | 3 | 2062 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.89 [0.52, 1.52] |
| 21.2 160/9 mcg | 2 | 1556 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.45, 1.42] |
| 22 Adverse events—candidiasis Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 22.1 320/9 mcg | 2 | 1552 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.45 [1.88, 6.34] |
| 22.2 160/9 mcg | 2 | 1556 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.05 [1.07, 3.92] |
| 23 Adverse events—dysphonia Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 23.1 320/9 mcg | 2 | 1552 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.07 [1.52, 10.90] |
| 23.2 160/9 mcg | 2 | 1556 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.17 [0.37, 3.67] |
| 24 Adverse events—cataracts Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 24.1 320/9 mcg | 1 | 975 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.32 [0.01, 7.97] |
| 24.2 160/9 mcg | 1 | 975 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.95 [0.18, 21.59] |
| 25 Adverse events—COPD Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 25.1 320/9 mcg | 2 | 1552 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.69, 1.22] |
| 25.2 160/9 mcg | 2 | 1556 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.16 [0.88, 1.53] |
| 26 Adverse events—tremor Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 26.1 320/9 mcg | 1 | 577 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 26.2 160/9 mcg | 1 | 581 | Odds Ratio (M‐H, Fixed, 95% CI) | 7.55 [0.39, 146.88] |
| 27 Adverse events—palpitations Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 27.1 320/9 mcg | 1 | 577 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.26 [0.13, 80.37] |
| 27.2 160/9 mcg | 1 | 581 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 28 Adverse events—lumbar spine bone density change from baseline (g/cm2) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 28.1 320/9 mcg | 1 | 149 | Mean Difference (IV, Fixed, 95% CI) | ‐0.02 [‐0.03, ‐0.01] |
| 28.2 160/9 mcg | 1 | 149 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [‐0.01, 0.01] |
| 29 Adverse events—hip bone density change from baseline (g/cm2) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 29.1 320/9 mcg | 1 | 149 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [‐0.01, 0.01] |
| 29.2 160/9 mcg | 1 | 147 | Mean Difference (IV, Fixed, 95% CI) | 0.01 [0.00, 0.02] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Number of participants with at least one exacerbation Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 400/10 mcg | 2 | 882 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.54, 0.95] |
| 1.2 200/10 mcg | 2 | 886 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.58, 1.01] |
| 2 Number of participants having at least one moderate or severe exacerbation Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 400/10 mcg | 2 | 882 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.57 [0.38, 0.86] |
| 2.2 200/10 mcg | 2 | 886 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.62 [0.42, 0.92] |
| 3 Mortality Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.1 400/10 mcg | 2 | 890 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.72 [0.41, 7.25] |
| 3.2 200/10 mcg | 2 | 894 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.20, 4.98] |
| 4 Change from baseline in St George's Respiratory Questionnaire (total score) Show forest plot | 2 | Mean Difference (Fixed, 95% CI) | Subtotals only | |
| 4.1 400/10 mcg | 2 | 866 | Mean Difference (Fixed, 95% CI) | ‐3.80 [‐5.75, ‐1.86] |
| 4.2 200/10 mcg | 2 | 869 | Mean Difference (Fixed, 95% CI) | ‐3.91 [‐6.01, ‐1.81] |
| 5 Change from baseline in FEV1 AUC0–12 hours (mL)—week 13 Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 5.1 400/10 mcg | 2 | 862 | Mean Difference (IV, Fixed, 95% CI) | 162.04 [126.54, 197.53] |
| 5.2 200/10 mcg | 2 | 869 | Mean Difference (IV, Fixed, 95% CI) | 122.01 [86.64, 157.39] |
| 6 Mean change from baseline AM predose FEV1 at 13 weeks (mL) Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 6.1 400/10 mcg | 2 | 856 | Mean Difference (IV, Fixed, 95% CI) | 114.64 [77.79, 151.50] |
| 6.2 200/10 mcg | 2 | 859 | Mean Difference (IV, Fixed, 95% CI) | 70.43 [33.63, 107.23] |
| 7 Withdrawals—total Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 7.1 400/10 mcg | 2 | 890 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.56 [0.40, 0.77] |
| 7.2 200/10 mcg | 2 | 894 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.55 [0.40, 0.76] |
| 8 Withdrawals due to lack of efficacy Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 8.1 400/10 mcg | 2 | 890 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.24 [0.08, 0.74] |
| 8.2 200/10 mcg | 2 | 894 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.31 [0.11, 0.84] |
| 9 Withdrawals due to adverse events Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 9.1 400/10 mcg | 2 | 890 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.07 [0.58, 1.98] |
| 9.2 200/10 mcg | 2 | 894 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.37 [0.16, 0.84] |
| 10 Adverse events—any Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 10.1 400/10 mcg | 2 | 890 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.75, 1.30] |
| 10.2 200/10 mcg | 2 | 894 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.62, 1.09] |
| 11 Adverse events—serious Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 11.1 400/10 mcg | 2 | 890 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.09 [0.66, 1.79] |
| 11.2 200/10 mcg | 2 | 894 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.41, 1.23] |
| 12 Adverse events—pneumonia Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 12.1 400/10 mcg | 2 | 890 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.14 [0.84, 11.65] |
| 12.2 200/10 mcg | 2 | 894 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.67 [0.40, 7.04] |
| 13 Adverse events—candidiasis Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 13.1 400/10 mcg | 2 | 890 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.22 [0.50, 9.91] |
| 13.2 200/10 mcg | 2 | 894 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.17, 5.87] |
| 14 Adverse events—dysphonia Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 14.1 400/10 mcg | 1 | 461 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.11 [0.19, 23.41] |
| 14.2 200/10 mcg | 1 | 475 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.98 [0.18, 22.02] |
| 15 Adverse events—cataract Show forest plot | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 15.1 400/10 mcg | 1 | 429 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.06, 15.72] |
| 15.2 200/10 mcg | 1 | 419 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.06, 16.48] |
| 16 Adverse events—COPD requiring hospitalisation Show forest plot | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 16.1 400/10 mcg | 2 | 890 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.40, 1.60] |
| 16.2 200/10 mcg | 2 | 894 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.36 [0.15, 0.86] |