பிரசவத்தின் போது பெண்களுக்கு தொடர் ஆதரவு (ஊக்கம்) தருவது
Abstract
Background
Historically, women have been attended and supported by other women during labour. However, in hospitals worldwide, continuous support during labour has become the exception rather than the routine.
Objectives
Primary: to assess the effects of continuous, one‐to‐one intrapartum support compared with usual care. Secondary: to determine whether the effects of continuous support are influenced by: (1) routine practices and policies; (2) the provider's relationship to the hospital and to the woman; and (3) timing of onset.
Search methods
We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (31 May 2013).
Selection criteria
All published and unpublished randomised controlled trials comparing continuous support during labour with usual care.
Data collection and analysis
We used standard methods of The Cochrane Collaboration Pregnancy and Childbirth Group. Two review authors independently evaluated methodological quality and extracted the data. We sought additional information from the trial authors. We used random‐effects analyses for comparisons in which high heterogeneity was present, and we reported results using the average risk ratio (RR) for categorical data and mean difference (MD) for continuous data.
Main results
Twenty‐two trials involving 15,288 women met inclusion criteria and provided usable outcome data. Results are of random‐effects analyses, unless otherwise noted. Women allocated to continuous support were more likely to have a spontaneous vaginal birth (RR 1.08, 95% confidence interval (CI) 1.04 to 1.12) and less likely to have intrapartum analgesia (RR 0.90, 95% CI 0.84 to 0.96) or to report dissatisfaction (RR 0.69, 95% CI 0.59 to 0.79). In addition, their labours were shorter (MD ‐0.58 hours, 95% CI ‐0.85 to ‐0.31), they were less likely to have a caesarean (RR 0.78, 95% CI 0.67 to 0.91) or instrumental vaginal birth (fixed‐effect, RR 0.90, 95% CI 0.85 to 0.96), regional analgesia (RR 0.93, 95% CI 0.88 to 0.99), or a baby with a low five‐minute Apgar score (fixed‐effect, RR 0.69, 95% CI 0.50 to 0.95). There was no apparent impact on other intrapartum interventions, maternal or neonatal complications, or breastfeeding. Subgroup analyses suggested that continuous support was most effective when the provider was neither part of the hospital staff nor the woman's social network, and in settings in which epidural analgesia was not routinely available. No conclusions could be drawn about the timing of onset of continuous support.
Authors' conclusions
Continuous support during labour has clinically meaningful benefits for women and infants and no known harm. All women should have support throughout labour and birth.
PICO
எளியமொழிச் சுருக்கம்
பிரசவத்தின் போது பெண்களுக்கு தொடர் ஆதரவு (ஊக்கம்) தருவது
பிரசவத்தின் போது தொடர்ந்து ஆதரவு (ஊக்கம்) தருவது, ஒரு தன்னிச்சையான யோனிவழி பிறப்பின் வாய்ப்பை அதிகரித்தது, எந்த தீங்கும் இல்லை, மற்றும் பெண்கள் அதிக திருப்தி அடைந்தார்கள்.
காலம்காலமாக பிரசவத்தின் போது பெண்கள் மற்ற பெண்களால் கவனிக்க பட்டதோடு அவர்களிடமிருந்து ஆதரவும் கிடைக்கபெற்றார்கள். எனினும், பல நாடுகளில், அதிக எண்ணிக்கையில் பெண்கள் வீட்டிற்கு பதிலாக மருத்துவமனையில் குழந்தையை பெற்றெடுக்கிறார்கள். பிரசவத்தின் போது, தொடர் ஆதரவு என்பது விதியாக அல்லாமல் விதிவிலக்காகவே மாறிவிட்டது. இது பெண்களின் பிரசவ அனுபவங்கள் பாலுள்ள மனித நேயத்தை இழக்கும் படி செய்ததற்கு காரணமாக இருக்கலாம். நவீன மகப்பேறு பேணுகை பொதுவாக பெண்களை நிறுவன நடைமுறைகளுக்கு உட்படுத்துகின்றன. அது பிரசவத்தின் முன்னேற்றத்தில் பாதகமான விளைவுகளை உண்டுபண்ணலாம். பிரசவத்தின் போது காட்டும் ஆதரவு உணர்ச்சிபூர்வமான ஆதரவாக, பிரசவத்திற்கான வசதிகளை ஏற்படுத்தல் , தகவல் மற்றும் ஆலோசனை ஆகியவற்றை கொண்டவையாகயிருக்கலாம். இது பிரசவத்தின் உடலியல் செயல்முறைகளை மேம்படுத்துவதுடன் பெண்களின் கட்டுப்பாடு மற்றும் ஆற்றல் உணர்வுகளை அதிகரிக்கலாம். இதனால் மகப்பேறியல் தலையீட்டின் தேவையை குறைக்கலாம். பலதரப்பட்ட அமைப்புகள் மற்றும் சூழ்நிலைகளில், 15,000 க்கும் மேற்பட்ட பெண்கள் கொண்டு, 16 நாடுகளில் மேற்கொண்ட 23 சோதனைகள் (22 ஆய்வுகளின் தரவுகள் கொண்டது) இந்த திறனாய்வில் சேர்க்கப்பட்டுள்ளது. தொடர் ஆதரவு, ஒன்று மருத்துவமனை ஊழியர்கள் (செவிலி அல்லது செவிலித்தாய் போன்றவர்கள்) அல்லது வைத்தியசாலை ஊழியர்கள் அல்லாத மற்றும் பிரசவ பெண்களுக்கு உறவும் அல்லாத பெண்கள் (சுமாரான அளவு வழிகாட்டல் வழங்கப்பட்ட மகப்பேறில் உதவ முறைப்படி கற்ற அல்லது பெண்கள் போன்றவர்கள்) அல்லது பிரசவ பெண்களின் விருப்பப்படி அவர்களின் சமுகத்தில் உள்ள நபித்தோழர்கள் (அவரது கணவர், கூட்டாளி, தாயார், நண்பர் போன்றவர்கள்) போன்றவர்களால் வழங்கப்பட்டுள்ளது. தொடர்ச்சியான பிரசவ ஆதரவு பெற்ற பெண்கள் தன்னிச்சையாக குழந்தையை பெற்றெடுக்க அதாவது, அறுவை வழிப்பேறு (சிசேரியன்) இல்லாமலும் அல்லது வெற்றிடம் அல்லது இடுக்கி இழுவையால் பெறல் (ஃபோர்செப்ஸ்) இல்லாமலும் பெற்றெடுக்க அதிக வாய்ப்பு இருந்தது. மேலும், பெண்களுகள், வலி மருந்துகள் பயன்படுத்துவதற்கான வாய்ப்பு குறைவாகவே இருந்தது, திருப்தி அதிகமாக இருந்தது, மற்றும் பிரசவ நேரம் சற்று குறைவாக இருந்தது. அவர்களின் குழந்தைகள் ஐந்து நிமிட அப்கார் (Apgar) அளவீட்டில் குறைந்த மதிப்பெண்ணுடன் இருக்க வாய்ப்பு குறைவாகவே இருந்தது. இதில் பாதகமான விளைவுகள் ஏதும் அடையாளம் காணப்படவில்லை. நாங்கள் அனைத்து பெண்களுக்கும் பிரசவத்தின் போது, தொடர் ஆதரவு வேண்டும் என்று முடிவுக்கு வந்தோம். தொடர் ஆதரவு அந்த பெண்களின் சமுக வலையில் இல்லாத நபராக, பிரசவத்திற்கு ஆதரவு கொடுப்பதில் அனுபவமுள்ள, மிதமான அளவாவது அதற்கென்றே பயிற்சிபெற்ற நபரால் வழங்கும் போது மிகவும் பயனுள்ளதாக இருக்கும் என்று தோன்றுகிறது. தேர்வு செய்யப்பட்ட குடும்ப உறுப்பினர் அல்லது நண்பர் பிரசவத்தின் போது துணையாக, இருப்பதை அவ்வாறு ஒரு துணை இல்லாததுடன் ஒப்பிடுகையில் பெண்களுக்கு, தங்கள் குழந்தைபேறு அனுபவத்தின் திருப்தியை அதிகரிக்கிறது என தோன்றுகிறது.
Authors' conclusions
Background
The first version of this Cochrane review was published in 1995 (Hodnett 2003), when the first systematic reviews in The Cochrane Collaboration Pregnancy and Childbirth Group Module were converted to the Cochrane review format. Thus, a formal Cochrane protocol was not initially published. Subsequently, the review author, Ellen Hodnett, completed a trial of labour support (Hodnett 2002) with a sample size larger than the entire sample in the prior version of the original review. As a protection against bias, she sought co‐authors who were blind to the results of the new trial and who had special expertise that would enhance the quality of the review. Discussions among the authors led to decisions to modify the background and methods. The authors decided that the best approach would be to write a new protocol for the review. The new protocol was submitted through the peer review process of the Cochrane Pregnancy and Childbirth Group and has subsequently evolved into a review that has been updated.
Historically and cross‐culturally, women have been attended and supported by other women during labour and birth. However, since the middle of the 20th century, in many countries as the majority of women gave birth in hospital rather than at home, continuous support during labour has become the exception rather than the routine. Concerns about dehumanisation of women's birth experiences (in high‐, middle‐, and low‐income countries) have led to calls for a return to continuous, one‐to‐one support by women for women during labour (Klaus 2002). Common elements of this care include emotional support (continuous presence, reassurance and praise), information about labour progress and advice regarding coping techniques, comfort measures (such as comforting touch, massage, warm baths/showers, promoting adequate fluid intake and output) and advocacy (helping the woman articulate her wishes to others).
Two complementary theoretical explanations have been offered for the effects of labour support on childbirth outcomes. Both explanations hypothesise that labour support enhances labour physiology and mothers' feelings of control and competence, reducing reliance on medical interventions. The first theoretical explanation considers possible mechanisms when companionship during labour is used in stressful, threatening and disempowering clinical birth environments (Hofmeyr 1991). During labour, women may be uniquely vulnerable to environmental influences; modern obstetric care frequently subjects women to institutional routines, high rates of intervention, unfamiliar personnel, lack of privacy and other conditions that may be experienced as harsh. These conditions may have an adverse effect on the progress of labour and on the development of feelings of competence and confidence; this may in turn impair adjustment to parenthood and establishment of breastfeeding, and increase the risk of depression. The provision of support and companionship during labour may to some extent buffer such stressors.
The second theoretical explanation does not focus on a particular type of birth environment. Rather, it describes two pathways ‐ enhanced passage of the fetus through the pelvis and soft tissues, as well as decreased stress response ‐ by which labour support may reduce the likelihood of operative birth and subsequent complications, and enhance women's feelings of control and satisfaction with their childbirth experiences (Hodnett 2002a). Enhanced fetopelvic relationships may be accomplished by encouraging mobility and effective use of gravity, supporting women to assume their preferred positions and recommending specific positions for specific situations. Studies of the relationships among fear and anxiety, the stress response and pregnancy complications have shown that anxiety during labour is associated with high levels of the stress hormone epinephrine in the blood, which may in turn lead to abnormal fetal heart rate patterns in labour, decreased uterine contractility, a longer active labour phase with regular well‐established contractions and low Apgar scores (Lederman 1978; Lederman 1981). Emotional support, information and advice, comfort measures and advocacy may reduce anxiety and fear and associated adverse effects during labour.
Continuous support has been viewed by some as a form of pain relief, specifically, as an alternative to epidural analgesia (Dickinson 2002), because of concerns about the deleterious effects of epidural analgesia, including on labour progress (Anim‐Somuah 2011). Many labour and birth interventions routinely involve, or increase the likelihood of, co‐interventions to monitor, prevent or treat adverse effects, in a "cascade of interventions". Continuous, one‐to‐one support has the potential to limit this cascade and therefore, to have a broad range of different effects, in comparison to usual care. For example, if continuous support leads to reduced use of epidural analgesia, it may in turn involve less use of electronic fetal monitoring, intravenous drips, synthetic oxytocin, drugs to combat hypotension, bladder catheterisation, vacuum extraction or forceps, episiotomy and less morbidity associated with these, and may increase mobility during labour and spontaneous birth (Caton 2002).
A systematic review examining factors associated with women's satisfaction with the childbirth experience suggests that continuous support can make a substantial contribution to this satisfaction. When women evaluate their experience, four factors predominate: the amount of support from caregivers, the quality of relationships with caregivers, being involved with decision‐making and having high expectations or having experiences that exceed expectations (Hodnett 2002a).
Clarification of the effects of continuous support during labour, overall and within specific circumstances, is important in light of public and social policies and programs that encourage this type of care. For example, the Congress in Uruguay passed a law in 2001 decreeing that all women have the right to companionship during labour. In several low‐ and middle‐income countries (including China, South Africa, Tanzania and Zimbabwe); the Better Births Initiative promotes labour companionship as a core element of care for improving maternal and infant health (WHO 2010). In many low‐income countries, women are not permitted to have anyone with them during labour and birth. Efforts to change policies in these settings have led to questions about the effectiveness of support from husbands/partners or other support people of the woman's own choosing, particularly in settings where the cost of paid companions would be prohibitive.
In North America, the services of women with special training in labour support have become available. Most commonly known as doula (a Greek word for 'handmaiden'), this new member of the caregiver team may also be called a labour companion, birth companion, labour support specialist, labour assistant or birth assistant. A number of North American organisations offer doula training, certification and professional support; according to one estimate more than 50,000 people have received this training to date (P Simkin, personal communication). Some North American hospitals have begun to sponsor doula services. In recent national surveys of childbearing women in the United States, 3% to 5% of respondents indicated that they had used doula services during their most recent labours (Declercq 2002; Declercq 2006). An association for doulas has been established in the UK (McGinnis 2001). Maternal healthcare systems in dozens of high‐ and low‐ to middle‐income countries throughout the world are developing new traditions for supportive female companionship during labour (Pascali‐Bonaro 2010).
Questions have arisen about the ability of employees (such as nurses or midwives) to provide effective labour support, in the context of modern institutional birth environments (Hodnett 1997). For example, nurses and midwives often have simultaneous responsibility for more than one labouring woman, spend a large proportion of time managing technology and keeping records, and begin or end work shifts in the middle of women's labours. They may lack labour support skills or may work in short‐staffed environments.
Companions from a woman's social network, such as husbands/partners and female relatives, usually have little experience in providing labour support and are themselves in need of support when with a loved one during labour and birth. As they are frequently available to assume the role, often without extra cost to families or health systems, it is important to understand their effectiveness as providers of continuous labour support.
In addition to questions about the impact of the type of provider of labour support, there are other questions about the effectiveness of support, including its impact under a variety of environmental conditions, and whether its effects are mediated by when continuous support begins (early versus active labour).
Childbearing women, policy‐makers, payers of health services, health professionals and facilities and those who provide labour support all need evidence about the effects of continuous support, overall and under specific conditions.
Objectives
The primary objective was to assess the effects, on mothers and their babies, of continuous, one‐to‐one intrapartum support compared with usual care, in any setting. Secondary objectives were to determine whether the effects of continuous support are influenced by the following.
-
Routine practices and policies in the birth environment that may affect a woman's autonomy, freedom of movement and ability to cope with labour, including:
-
policies about the presence of support people of the woman's own choosing;
-
epidural analgesia; and
-
continuous electronic fetal monitoring.
-
-
Whether the provider is:
-
a member of the staff of the institution (and thus has additional loyalties or responsibilities);
-
not a staff member but not part of the woman's social network and present solely for the purpose of providing continuous support; or
-
a person chosen by the woman from family members and friends.
-
-
Whether the continuous support begins early or later in labour.
Methods
Criteria for considering studies for this review
Types of studies
All controlled trials comparing continuous labour support by either a familiar or unfamiliar person (with or without healthcare professional qualifications) with usual care, in which there was random allocation to treatment and control groups, were considered for inclusion in the review.
Types of participants
Pregnant women, in labour.
Types of interventions
The form of care that was evaluated was continuous presence and support during labour and birth. The person providing the support could have qualifications as a healthcare professional (nurse, midwife) or training as a doula or childbirth educator, or be a family member, spouse/partner, friend or stranger with little or no special training in labour support. The control group received usual care, as defined by the trialists. In all cases, 'usual care' did not involve continuous intrapartum support, but it could involve other measures, such as routine epidural analgesia, to help women to cope with labour.
Types of outcome measures
Theoretically, continuous support can have many diverse physiological and psychosocial effects (both short‐ and long‐term), and therefore, a larger than usual number of outcomes were considered.
Primary outcomes
Mother
-
Any analgesia/anaesthesia (pain medication).
-
Synthetic oxytocin during labour.
-
Spontaneous vaginal birth.
-
Postpartum depression (defined using a pre‐specified cutoff score on a validated instrument).
-
Negative rating of/negative feelings about the birth experience.
Baby
-
Admission to special care nursery.
-
Breastfeeding at one to two months postpartum.
Secondary outcomes
Labour events
-
Regional analgesia/anaesthesia.
-
Labour length
-
Severe labour pain (postpartum report).
Birth
-
Caesarean birth.
-
Instrumental vaginal birth.
-
Perineal trauma (defined as episiotomy or laceration requiring suturing).
Newborn
-
Low five‐minute Apgar score (as defined by trial authors).
-
Prolonged newborn hospital stay.
Longer‐term maternal outcomes
-
Difficulty mothering.
-
Low self‐esteem in the postpartum period.
Search methods for identification of studies
Electronic searches
We searched the Cochrane Pregnancy and Childbirth Group’s Trials Register by contacting the Trials Search Co‐ordinator (31 May 2013).
The Cochrane Pregnancy and Childbirth Group’s Trials Register is maintained by the Trials Search Co‐ordinator and contains trials identified from:
-
monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL);
-
weekly searches of MEDLINE;
-
weekly searches of Embase;
-
handsearches of 30 journals and the proceedings of major conferences;
-
weekly current awareness alerts for a further 44 journals plus monthly BioMed Central email alerts.
Details of the search strategies for CENTRAL, MEDLINE and Embase, the list of handsearched journals and conference proceedings, and the list of journals reviewed via the current awareness service can be found in the ‘Specialized Register’ section within the editorial information about the Cochrane Pregnancy and Childbirth Group.
Trials identified through the searching activities described above are each assigned to a review topic (or topics). The Trials Search Co‐ordinator searches the register for each review using the topic list rather than keywords.
We did not apply any language restrictions.
Data collection and analysis
For this update we assessed one new trial (Yuenyong 2012) and added 'postpartum depression' outcome data from one existing trial report (Hofmeyr 1991), using the following methods.
Selection of studies
For the current update, three review authors (E Hodnett, J Hofmeyr, C Sakala) independently assessed for inclusion all potentially eligible studies. Had any disagreement occurred, we would have resolved it through discussion or, if required, we would have consulted a third member of the review team.
Data extraction and management
We designed a form to extract data. For eligible studies, data were independently extracted by two people (either two review authors or an author and an assistant), using the agreed form. We resolved discrepancies through discussion. We entered data into Review Manager software (RevMan 2011) and checked for accuracy.
When information regarding any of the above was unclear, we attempted to contact authors of the original reports to provide further details.
Assessment of risk of bias in included studies
For each study, at least two review authors independently assessed risk of bias, using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We would have resolved any disagreement by discussion or by involving a third assessor.
(1) Sequence generation (checking for possible selection bias)
We described for each included study the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups.
We assessed the method as:
-
low risk of bias (any truly random process, e.g. random number table; computer random number generator);
-
high risk of bias (any non‐random process, e.g. odd or even date of birth; hospital or clinic record number);
-
unclear risk of bias.
(2) Allocation concealment (checking for possible selection bias)
We described for each included study the method used to conceal the allocation sequence, and determined whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment.
We assessed the methods as:
-
low risk of bias (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes);
-
high risk of bias (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth);
-
unclear risk of bias.
(3) Blinding (checking for possible performance and detection bias)
We described for each included study the methods used, if any, to blind personnel from knowledge of which intervention a participant received. Since women and care providers cannot be blinded as to whether continuous support was given, we considered blinding adequate if outcomes were recorded by outcome assessors who had no knowledge of the woman's group assignment. We judged studies at low risk of bias if they were blinded, or if we judged that the lack of blinding could not have affected the results. We assessed blinding separately for different outcomes or classes of outcomes.
(4) Incomplete outcome data (checking for possible attrition bias through withdrawals, dropouts, protocol deviations)
We described for each included study, and for each outcome or class of outcomes, the completeness of data including attrition and exclusions from the analysis. We stated whether attrition and exclusions were reported, the numbers included in the analysis at each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. To be included in the review, data on a given outcome had to be available for at least 80% of those who were originally randomised. For outcomes collected post‐hospital discharge, we recognise that follow‐up, particularly in low‐income countries, can be very difficult. Therefore, we included data if the response rate was higher than 75% and there was no obvious imbalance in groups. Where sufficient information was reported, or could be supplied by the trial authors, we planned to include missing data in the analyses. We assessed methods as:
-
low risk of bias;
-
high risk of bias;
-
unclear risk of bias.
(5) Selective reporting bias
We described for each included study how we investigated the possibility of selective outcome reporting bias and what we found.
We assessed the methods as:
-
low risk of bias (where it is clear that all of the study’s pre‐specified outcomes and all expected outcomes of interest to the review have been reported);
-
high risk of bias (where not all the study’s pre‐specified outcomes have been reported; one or more reported primary outcomes were not pre‐specified; outcomes of interest are reported incompletely and so cannot be used; study fails to include results of a key outcome that would have been expected to have been reported);
-
unclear risk of bias.
(6) Other sources of bias
We planned to describe for each included study any important concerns we had about other possible sources of bias, including, for example, whether the trial was stopped early due to a data‐dependent process, there was evidence of extreme baseline imbalance, or there had been claims of fraud.
We assessed whether each study was free of other problems that could put it at risk of bias:
-
low risk of other bias;
-
high risk of other bias;
-
unclear whether there is risk of other bias.
(7) Overall risk of bias
We made explicit judgements about whether studies are at high risk of bias, according to the criteria given in the Handbook (Higgins 2011). With reference to (1) to (6) above, we assessed the likely magnitude and direction of the bias and whether we considered it is likely to impact on the findings. We explored the impact of the level of bias through undertaking sensitivity analyses ‐ seeSensitivity analysis.
Measures of treatment effect
Dichotomous data
For dichotomous data, we presented results as summary risk ratio with 95% confidence intervals.
Continuous data
All but one pre‐specified outcome involved dichotomous data. For labour length, we used the mean difference because it was measured in the same way in the trials.
Unit of analysis issues
Cluster‐randomised trials
Had we found cluster‐randomised trials, we would have included them in the analyses along with individually‐randomised trials. Our plan was as follows: we would adjust their sample sizes or standard errors using the methods described in the Handbook (Section 16.3.4 or 16.3.6) using an estimate of the intracluster correlation co‐efficient (ICC) derived from the trial (if possible), from a similar trial or from a study of a similar population. If we had used ICCs from other sources, we planned to report this and conduct sensitivity analyses to investigate the effect of variation in the ICC. In future updates of this review, if we identify both cluster‐randomised trials and individually‐randomised trials, we plan to synthesise the relevant information. We will consider it reasonable to combine the results from both if there is little heterogeneity between the study designs and the interaction between the effect of intervention and the choice of randomisation unit is considered to be unlikely. We will also acknowledge heterogeneity in the randomisation unit and perform a separate meta‐analysis.
Dealing with missing data
For included studies, we noted levels of attrition. We included data for a given outcome which occurred prior to hospital discharge only if the data were available for at least 80% of those originally randomised. For outcomes collected post‐hospital discharge we included data if the response rate was higher than 75% and there was no obvious imbalance in groups.
For all outcomes we have carried out analyses, as far as possible, on an intention‐to‐treat basis, i.e. we attempted to include all participants randomised to each group in the analyses. The denominator for each outcome in each trial was the number randomised minus any participants whose outcomes were known to be missing.
Assessment of heterogeneity
We assessed statistical heterogeneity in each meta‐analysis using the T², I² and Chi² statistics. We regarded heterogeneity as substantial if the T² was greater than zero and either the I² was greater than 30% or there was a low P value (less than 0.10) in the Chi² test for heterogeneity. In such cases we took the following steps:
-
a sensitivity analysis, in which methodological weak trials were removed from the analyses and results compared for the primary outcomes;
-
visual inspection of the forest plots for evidence of inconsistency in results; and
-
comparison of the results of fixed‐effect and random‐effects analyses.
Assessment of reporting biases
Had we suspected reporting bias, we would have attempted to contact study authors asking them to provide missing outcome data. If this were not possible, and the missing data were thought to introduce serious bias, we would not have included the outcome data from that trial.
Data synthesis
We carried out statistical analysis using the Review Manager software (RevMan 2011). We used fixed‐effect Mantel‐Haenszel meta‐analysis for combining data in the absence of heterogeneity, and random‐effects analysis if substantial heterogeneity was detected and we considered that combining trials was meaningful. We defined heterogeneity as substantial if a given meta‐analysis resulted in an I² value greater than 30%, and there was inconsistency among trials in the direction or magnitude of effects (judged visually in the forest plot), or a low (less than 0.10) P value in the Chi² test for heterogeneity.
Subgroup analysis and investigation of heterogeneity
We planned the following subgroup analyses.
A) Three subgroup analyses that concern characteristics of the childbirth environment
-
Trials in settings in which women were permitted to be accompanied by one or more support persons of their own choosing compared with trials in which accompaniment was not permitted.
-
Trials conducted in settings in which epidural analgesia was available compared with trials in settings in which it was unavailable.
-
Trials in which there was a policy of routine electronic fetal heart rate monitoring compared with trials in settings in which continuous electronic fetal monitoring was not routine.
(B) One subgroup analysis that concerns characteristics of the providers of labour support
-
Trials in which the caregivers were employees of the institution, compared with trials in which the caregivers were not employees and were not members of the woman's social network, compared with trials in which the providers were not employees and were lay people chosen by the participants (e.g. husband/partner, friend, close relative).
(C) One subgroup analysis that concerns differences in the timing of onset of continuous support
-
Trials in which continuous labour support began prior to or during early labour (as defined by trial authors), compared with trials in which continuous support began in active labour.
Because few of the trial reports contained all of the information needed for the above subgroup analyses, we contacted the trial authors in an attempt to verify the presence/absence of routine electronic fetal monitoring (EFM), the presence/absence of epidural analgesia and timing of onset of continuous support. We excluded some studies included in the primary comparisons from the subgroup analyses concerning the use of EFM because their status regarding EFM use was unknown. For tests of differences between these subgroups, we recalculated the overall analysis by including only the studies in which EFM use was known.
The seven primary outcomes and one secondary outcome were used in the subgroup analyses. While normally, subgroup analyses are restricted to primary outcomes, we also included the outcome of caesarean delivery, because there is widespread concern about escalating caesarean rates worldwide, and subgroup analyses could be helpful to policy makers in decisions about the provision of continuous labour support. Thus the outcomes in the subgroup analyses were: any analgesia/anaesthesia, synthetic oxytocin during labour, spontaneous vaginal birth, caesarean birth, postpartum depression, negative ratings of the birth experience, admission to special care nursery, and breastfeeding at one to two months postpartum.
When I² levels were high but the amount of heterogeneity in treatment effects was low (as happens when there are a large number of big trials and thus the amount of variation due to sampling error is extremely low), we compared the results of random‐effects and fixed‐effect analyses. In instances in which the conclusions were not materially different in both methods of analysis, we reported the results of fixed‐effect, inverse variance meta‐analysis, in order to be able to calculate a Chi² for the purpose of exploring differences based on pre‐specified subgroups. As a consequence the totals in the subgroup analysis tables are sometimes slightly different from those in the main comparison, since the main comparisons used the Mantel‐Haenszel rather than the inverse variance method.
Sensitivity analysis
We performed sensitivity analyses, for the primary outcomes, in instances in which there was a high risk of bias associated with the quality of included trials.
Results
Description of studies
Included studies
Please seeCharacteristics of included studies table. While 23 trials met the inclusion criteria, one trial (Thomassen 2003) provided no usable outcome data. We do not describe it here, but provide details in the Characteristics of included studies table.
All 22 trials (n = 15,288) that provided usable outcome data were conducted in hospitals. The trials were conducted in Australia, Belgium, Botswana, Brazil, Canada, Chile, Finland, France, Greece, Guatemala, Mexico, Nigeria, South Africa, Sweden, Thailand, and the United States, under widely disparate hospital conditions, regulations and routines. There was remarkable consistency in the descriptions of continuous support across all trials. In all instances the intervention included continuous or nearly continuous presence, at least during active labour. Twenty of the 22 trials that provided usable outcome data (all except Cogan 1988 and Dickinson 2002) also included specific mention of comforting touch and words of praise and encouragement.
In 11 trials (Breart ‐ Belgium 1992; Breart ‐ France 1992; Campbell 2006; Cogan 1988; Dickinson 2002; Gagnon 1997; Hemminki 1990a; Hemminki 1990b; Hodnett 1989; Hodnett 2002; McGrath 2008), hospital policy permitted women to be accompanied by their husbands/partners or other family members during labour, while in the other 11 trials, no additional support people were allowed. Epidural analgesia was not routinely available in seven trials (Breart ‐ Greece 1992; Hofmeyr 1991; Kashanian 2010; Klaus 1986; Madi 1999; Morhason‐Bello 2009; Yuenyong 2012). We were unsuccessful in obtaining information about the availability of epidural analgesia in one trial (Cogan 1988). Epidural analgesia was routinely available in the other 14 trials. Electronic fetal heart rate monitoring was not routine in eight trials (Bruggemann 2007; Hofmeyr 1991; Kashanian 2010; Klaus 1986; Langer 1998; Madi 1999; Morhason‐Bello 2009; Yuenyong 2012). In nine trials (Campbell 2006; Dickinson 2002; Gagnon 1997; Hemminki 1990a; Hemminki 1990b; Hodnett 1989; Hodnett 2002; Kennell 1991; McGrath 2008) electronic fetal monitoring was used routinely. We were unsuccessful in obtaining information about the use of electronic fetal monitoring in five trials (Breart ‐ Greece 1992; Breart ‐ Belgium 1992; Breart ‐ France 1992; Cogan 1988; Torres 1999).
It was not possible to categorise most of the trials according to the pre‐specified subgroups of early versus active labour. In four trials (Cogan 1988; Hodnett 1989; Klaus 1986; Madi 1999), the support began in early labour. In the other 17 trials, the timing of onset of support was much more heterogenous, as were definitions of early and active labour, in instances in which these were defined. Women were in varying phases of labour, from elective induction to active labour.
In addition, the persons providing the support intervention varied in their experience, qualifications and relationship to the labouring women. In nine trials (Breart ‐ Belgium 1992; Breart ‐ France 1992; Breart ‐ Greece 1992; Dickinson 2002; Gagnon 1997; Hemminki 1990a; Hemminki 1990b; Hodnett 2002; Kashanian 2010), the support was provided by a member of the hospital staff, for example, a midwife, student midwife or nurse. In seven trials the providers were not members of the hospital staff and were not part of the woman's social network; they were women with or without special training, such as doulas or women who had given birth before (Hodnett 1989; Hofmeyr 1991; Kennell 1991; Klaus 1986; McGrath 1999): a childbirth educator (Cogan 1988), or retired nurses (Langer 1998). In six trials they were companions of the woman's choice from her social network, with or without brief training ‐‐ a female relative or friend or the woman's husband/partner (Bruggemann 2007; Campbell 2006; Madi 1999; Morhason‐Bello 2009; Torres 1999; Yuenyong 2012).
Excluded studies
Sixteen trials were excluded altogether (Bender 1968; Bochain 2000; Brown 2007; Dalal 2006; Gordon 1999; Hemminki 1990c; Lindow 1998; McGrath 1999; Orenstein 1998; Pinheiro 1996; Ran 2005; Scott 1999; Sosa 1980; Trueba 2000; Tryon 1966; Zhang 1996). Seven trials were excluded as they were not randomised trials (Bender 1968; Dalal 2006; Ran 2005; Scott 1999; Sosa 1980; Trueba 2000; Tryon 1966). Five trials were excluded because the intervention was not continuous support (Bochain 2000; Brown 2007; Lindow 1998; Orenstein 1998; Zhang 1996). Two trials reported as abstracts provided insufficient information in order to assess eligibility (McGrath 1999; Pinheiro 1996). Two further trials were excluded because they did not provide any usable data (Gordon 1999; Hemminki 1990c). Please refer to table Characteristics of excluded studies for details.
Risk of bias in included studies
The trials were of generally good quality (Figure 1; Figure 2).

Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
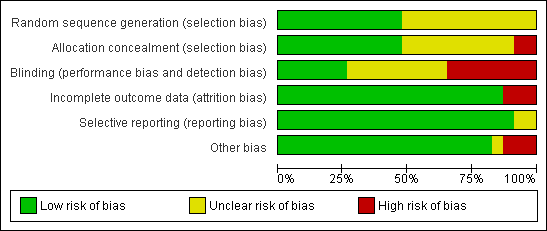
Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies
Allocation
Random sequence generation: Twelve trials were at unclear risk of bias (Breart ‐ Belgium 1992; Breart ‐ France 1992; Breart ‐ Greece 1992; Cogan 1988; Dickinson 2002; Hemminki 1990a; Hemminki 1990b; Kennell 1991; Klaus 1986; Madi 1999; McGrath 2008; Thomassen 2003) because they did not describe the method of random assignment. Eleven trials described using a computer random number generator or referred to a random number table (Bruggemann 2007; Campbell 2006; Gagnon 1997; Hodnett 1989; Hodnett 2002; Hofmeyr 1991; Kashanian 2010; Langer 1998; Morhason‐Bello 2009; Torres 1999; Yuenyong 2012) and were assessed as low risk of bias.
Allocation concealment: The risk of selection bias was high in two small trials (Bruggemann 2007; Kashanian 2010). In Bruggemann 2007, women picked their treatment allocation from an opaque container. In 11 trials (Campbell 2006; Gagnon 1997; Hodnett 1989; Hodnett 2002; Kennell 1991; Klaus 1986; Madi 1999; McGrath 2008; Morhason‐Bello 2009; Torres 1999; Yuenyong 2012), risk of selection bias was low with allocation described as either using central allocation, e.g. Hodnett 2002 used a central, computerised randomisation service accessed by telephone or other trials described using sequentially numbered, opaque, sealed envelopes. In the remaining trials (Breart ‐ Belgium 1992; Breart ‐ France 1992; Breart ‐ Greece 1992; Cogan 1988; Dickinson 2002; Hemminki 1990a; Hemminki 1990b; Hofmeyr 1991; Langer 1998; Thomassen 2003), risk of selection bias was unclear, e.g. one trial used methods that were centrally controlled but not concealed (Cogan 1988).
Blinding
Performance bias: neither those providing nor receiving care could be blinded to the presence/absence of a person providing continuous support. Hodnett 2002 provided evidence to discount contamination and co‐intervention as serious threats to validity. In eight trials group assignment was known and no attempt to blind outcome assessment was apparent and so these were assessed as being at high risk of bias (Bruggemann 2007; Campbell 2006; Gagnon 1997; Hemminki 1990a; Hemminki 1990b; Hofmeyr 1991; Madi 1999; Morhason‐Bello 2009).
Detection bias: in the trials which sought participants' evaluations of their birth experiences, efforts were made to reduce response bias, through use of an interviewer blinded to the woman's group allocation or self‐administered questionnaires. Six trials were assessed as being at low risk of bias because some blinding of outcome assessment was performed (Cogan 1988; Hodnett 1989; Hodnett 2002; Kashanian 2010; Langer 1998; Yuenyong 2012).
In the remaining trials, risk of bias for blinding (performance and detection bias) was unclear (Breart ‐ Belgium 1992; Breart ‐ France 1992; Breart ‐ Greece 1992; Dickinson 2002; Kennell 1991; Klaus 1986; McGrath 2008; Thomassen 2003; Torres 1999).
Incomplete outcome data
Attrition bias: we did not include data for outcomes assessed in hospital in a comparison if there was more than 20% loss to follow‐up; we did not include longer‐term outcome data if there was more than 25% loss to follow‐up. Based on these criteria, one trial (Thomassen 2003) provided no usable outcome data. Two trials further trials were assessed as being at high risk of bias for attrition bias (Campbell 2006; Cogan 1988).
Selective reporting
All outcomes appear to have been reported upon in the majority of trials. In two trials, it was unclear whether selective reporting had taken place (Cogan 1988; Thomassen 2003).
Other potential sources of bias
Three trials were assessed as being at high risk of other bias: in two trials the mothers had been told the purpose of the study differentially (Hemminki 1990a; Hemminki 1990b) and one trial was stopped early for 'a range of largely organizational issues' when only a quarter of the original sample size had been enrolled (Thomassen 2003). Risk of bias was unclear in one study (Campbell 2006) and no other sources of bias were apparent in the remaining trials.
Effects of interventions
Main comparison: continuous support versus usual care ‐ all trials
We considered 17 outcomes. Between one and 22 trials contributed to the analyses of each outcome. Sensitivity analyses, conducted by removing the trials (all of which were small) with a high likelihood of selection bias (Bruggemann 2007; Hodnett 1989; Kashanian 2010) did not alter the conclusions. According to our pre‐specified criteria, there was statistical heterogeneity in all but three outcomes (instrumental vaginal birth, low five‐minute Apgar score, and low postpartum self‐esteem). Inspection of the forest plots did not suggest sources of heterogeneity. For the two outcomes postpartum depression and difficulty mothering, this statistical heterogeneity confirmed our conclusion that based on clinical heterogeneity a summary statistic would not yield meaningful results (discussed further below). In all instances in which summary statistics are reported, the comparisons of fixed‐effect and random‐effects analyses did not yield substantive differences, nor alter conclusions. We report the results of fixed‐effect analyses for instrumental vaginal birth, low five‐minute Apgar score, and low postpartum self‐esteem (the latter only contained one trial), and random‐effects analyses for all other outcomes in which summary statistics were computed.
Primary outcomes
Women who had continuous, one‐to‐one support during labour were:
more likely to have
-
a spontaneous vaginal birth (19 trials, n = 14,119, average risk ratio (RR) 1.08, 95% confidence interval (CI) 1.04 to 1.12, I² 45%, т² 0.00), Analysis 1.5;
less likely to have
-
any intrapartum analgesia/anaesthesia (14 trials, n = 12,283, average RR 0.90, 95% CI 0.84 to 0.96, I² 75%, т² 0.01), Analysis 1.1;
-
reported negative rating of/negative feelings about childbirth experience (11 trials, n = 11,133, average RR 0.69, 95% CI 0.59 to 0.79, I² 63%, т² 0.03), Analysis 1.13;
and there was no apparent impact of continuous support on
-
use of synthetic oxytocin during labour (15 trials, n = 12,620, average RR 0.97, 95% CI 0.91 to 1.04, I² 65%, т² 0.01), Analysis 1.3;
-
admission to the special care nursery (seven trials; n = 8897, average RR 0.97, 95% CI 0.76 to 1.25, I² 37%, т² 0.03), Analysis 1.10;
-
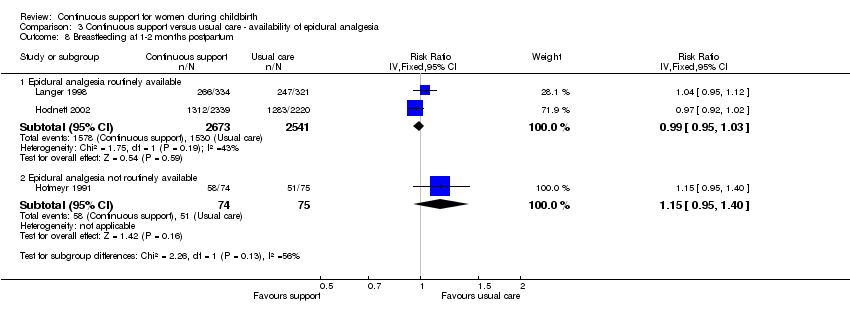
breastfeeding at one to two months postpartum (three trials, n = 5363, average RR 1.01, 95% CI 0.94 to 1.09, I² 52%, т² 0.00), Analysis 1.15; and
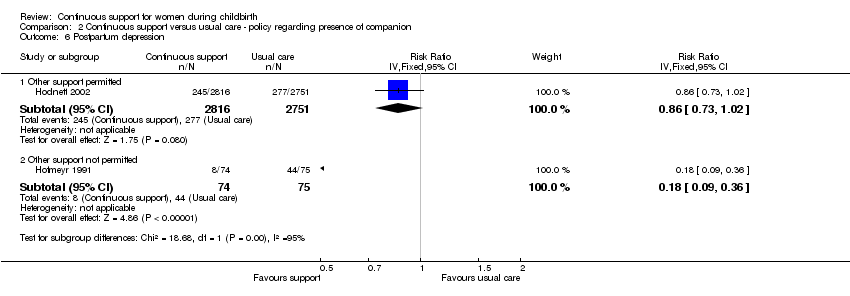
evidence of postpartum depression was a reported outcome in just two trials (Hodnett 2002; Hofmeyr 1991). Hodnett 2002 used the Edinburgh Postnatal Depression Inventory and reported the frequencies of scores greater than 12. Hofmeyr 1991 used the Pitt Depression Inventory and reported scores indicating mild (less than 20), moderate (20 to 34), and severe (greater than 34) depressive symptomatology. We combined the frequencies of moderate and severe depressive symptomatology, since Pitt scores greater than 19 have been considered indicative of postpartum depression (Avan 2010). The two trials were widely disparate in populations, the hospital conditions within which they were conducted, and the type of support provider. We concluded that combining them would not yield meaningful information. In both trials the direction of effect was the same. In Hofmeyr 1991, eight of 74 women in the group receiving continuous support had depressive symptomatology compared to 44 of 75 women in the control group; RR 0.18, 95% CI 0.09 to 0.36. In Hodnett 2002, 245 out of 2816 in the supported group had depressive symptomatology, compared to 277 out of 2751 in the control group; RR 0.86, 95% CI 0.73 to 1.02.
Secondary outcomes
Women who had continuous, one‐to‐one support were:
more likely to have
-
shorter labours (12 trials, n = 5366, mean difference (MD) ‐0.58 hours, 95% CI ‐0.85 to ‐0.31, I² 45%, т² 0.08), Analysis 1.4;
less likely to have
-
regional analgesia/anaesthesia (nine trials, n = 11,444, average RR 0.93, 95% CI 0.88 to 0.99, I² 81%, т² 0.01), Analysis 1.2;
-
an instrumental vaginal birth (19 trials, n = 14,118, RR 0.90, 95% CI 0.85 to 0.96, fixed‐effect), Analysis 1.6;
-
a caesarean birth (22 trials, n = 15,175, average RR 0.78, 95% CI 0.67 to 0.91, I² 53%, т² 0.05), Analysis 1.7;
-
a baby with a low five‐minute Apgar score (13 trials, n = 12,515, RR 0.69, 95% CI 0.50 to 0.95, fixed‐effect), Analysis 1.9;
and there was no apparent impact of continuous labour support on
-
the likelihood of serious perineal trauma (four trials, n = 8120, average RR 0.97, 95% CI 0.92 to 1.01, I² 44%, т² 0.00), Analysis 1.8;
-
severe labour pain (four trials; n = 2456, average RR 1.00, 95% CI 0.83 to 1.21, I² 78%, т² 0.03), Analysis 1.12;
-
low postpartum self‐esteem (one trial, n = 652, RR 1.00, 95% CI 0.77 to 1.30, fixed‐effect), Analysis 1.17; and
-
prolonged neonatal hospital stay (three trials, n = 1098, average RR 0.83, 95% CI 0.42 to 1.65, I² 62%, т² 0.15), Analysis 1.11.
Three trials reported results related to difficulty in mothering (Campbell 2006; Hofmeyr 1991; Hodnett 2002). As was the case with postpartum depression, the trials were widely disparate in populations, the hospital conditions within which they were conducted, and the type of support provider, and the forest plot supported our conclusion that combining them would not yield meaningful information. In Hofmeyr 1991, 41 out of 75 in the continuous support group reported difficulty mothering, compared to 67 out of 75 in the control group; RR 0.61, 95% CI 0.49, 0.76. In Hodnett 2002, 873 out of 2836 in the continuous support group reported difficulty mothering, compared to 853 out of 2765 in the control group; RR 1.00, 95% CI 0.92, 1.08. In Campbell 2006, 11 out of 292 in the continuous support group reported difficulty mothering, compared to 38 out of 265 in the control group; RR 0.26, 95% CI 0.14, 0.50.
Subgroup comparisons
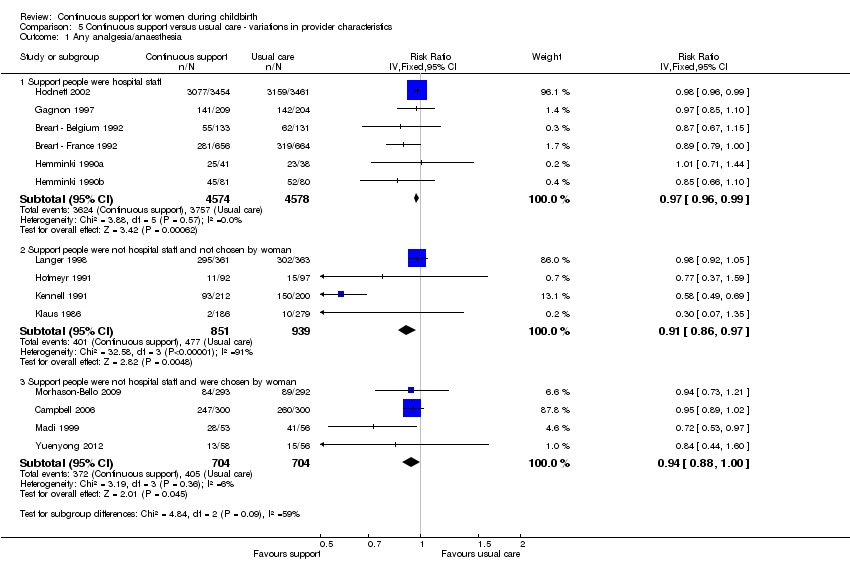
We grouped the trials according to the following provider characteristics: 1) staff members of the hospital; 2) neither hospital employees nor part of the woman's social network; and 3) chosen by the woman from her social network.
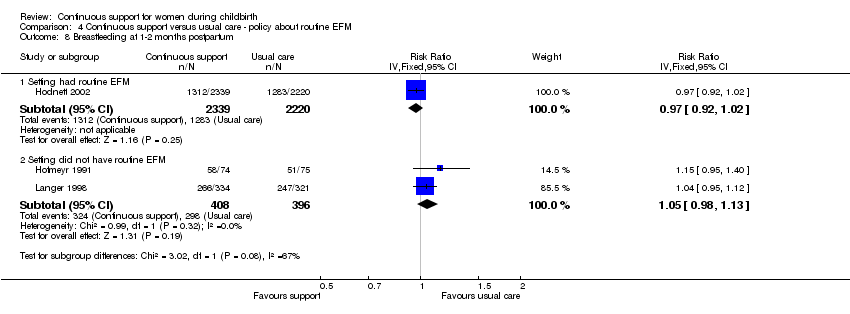
We have presented the results of the subgroup analyses below. While we made every effort to obtain the required information from trial authors, none of the subgroup comparisons are based on the total number of included trials for which usable data were available. Thus results must be interpreted with caution. The text below does not present the results for postpartum depression or breastfeeding at one to two months postpartum, because too few trials provided data. Only two trials contributed data about postpartum depression (Hodnett 2002; Hofmeyr 1991) and three about breastfeeding (Hodnett 2002; Hofmeyr 1991; Langer 1998).
We were unable to conduct the planned subgroup comparison based on timing of onset of labour support. It was not possible to categorise most of the trials according to the pre‐specified subgroups of early versus active labour. In four trials (Cogan 1988; Hodnett 1989; Klaus 1986; Madi 1999), the support began in early labour. In the other 18 trials, both the definitions of early and active labour and the timing of onset of support were much more heterogenous, in instances in which they were defined. Women were in varying phases of labour, from elective induction to active labour.
As noted in Subgroup analysis and investigation of heterogeneity, totals in the subgroup analysis figures may differ slightly from those in the main comparisons, because a different method of analysis had to be used. All subgroup comparisons used fixed‐effect, to allow computation of tests for differences between subgroups.
Outcome: any intrapartum analgesia/anaesthesia
-
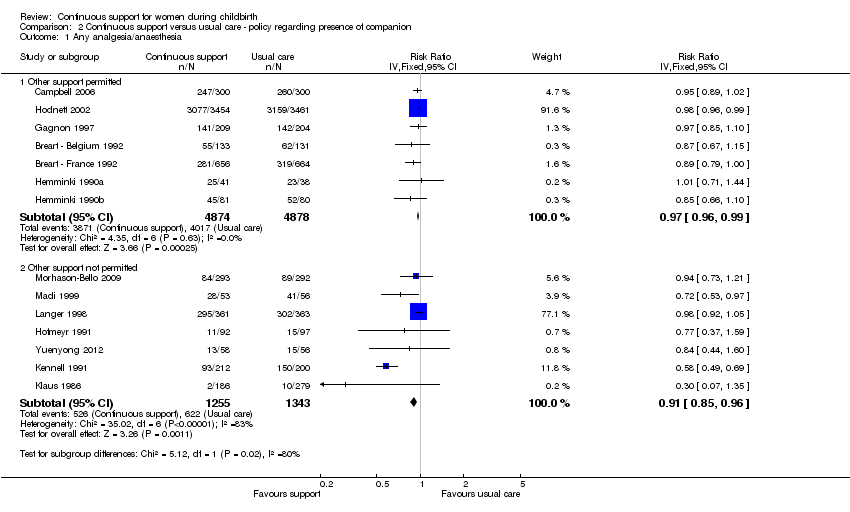
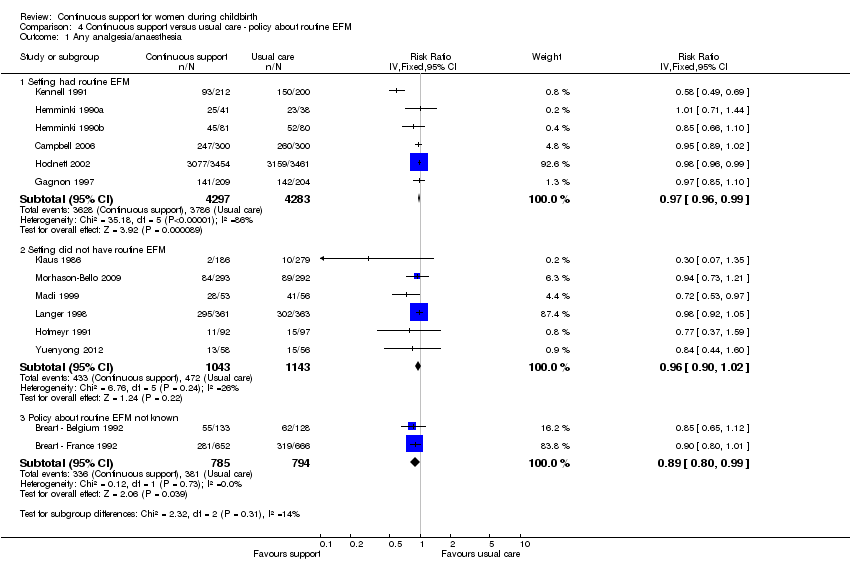
Policies about the presence of companions during labour and birth: In seven trials (n = 9752) companions were permitted; RR 0.97, 95% CI 0.96 to 0.99, while in seven trials (n = 2598) companions were not permitted; RR 0.91, 95% CI 0.85 to 0.96. Chi² for the subgroup comparison = 5.12, P = 0.02, Analysis 2.1.
-
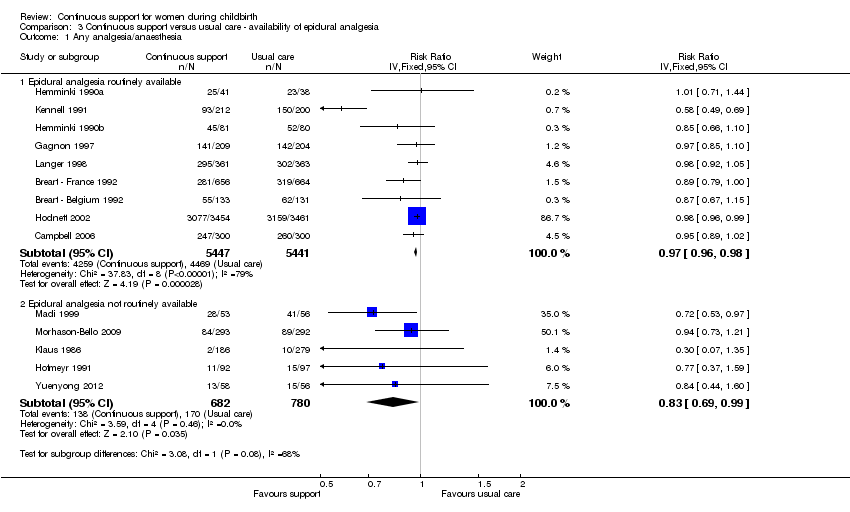
Availability of epidural analgesia: In nine trials (n = 10,888), epidural analgesia was routinely available; RR 0.97, 95% CI 0.96 to 0.98. In five trials (n = 1462) epidural analgesia was not routinely available; RR 0.83, 95% CI 0.69 to 0.99. Chi² for the subgroup comparison = 3.08, P = 0.08, Analysis 3.1.
-
Routine use of electronic fetal monitoring (EFM): in six trials (n = 8580), EFM was routine; RR 0.97, 95% CI 0.96 to 0.99. In six trials (n = 2186), EFM was not routine; RR 0.96, 95% CI 0.90 to 1.02. In two trials (n = 1579), the policy about routine EFM was unknown; RR 0.89, 95% CI 0.80 to 0.99. Chi² for the subgroup comparison = 2.32, P = 0.31, Analysis 4.1.
-
Provider characteristics: in six trials (n = 9152) the support was provided by a member of the hospital staff; RR 0.97, 95% CI 0.96 to 0.99. In four trials (n = 1790), the support was provided by a woman who was not a member of the staff and was not part of the woman's social network; RR 0.91, 95% CI 0.86 to 0.97. In four trials (n = 1408) the support was provided by a member of the woman's social network; RR 0.94, 95% CI 0.88 to 1.00. Chi² for the subgroup comparison = 4.84, P = 0.09, Analysis 5.1.
Thus, the effects of continuous support on use of any intrapartum analgesia/anaesthesia appeared to be stronger in settings where companions were not permitted, but did not appear to be influenced by the availability of epidural analgesia, the use of routine EFM, or provider characteristics.
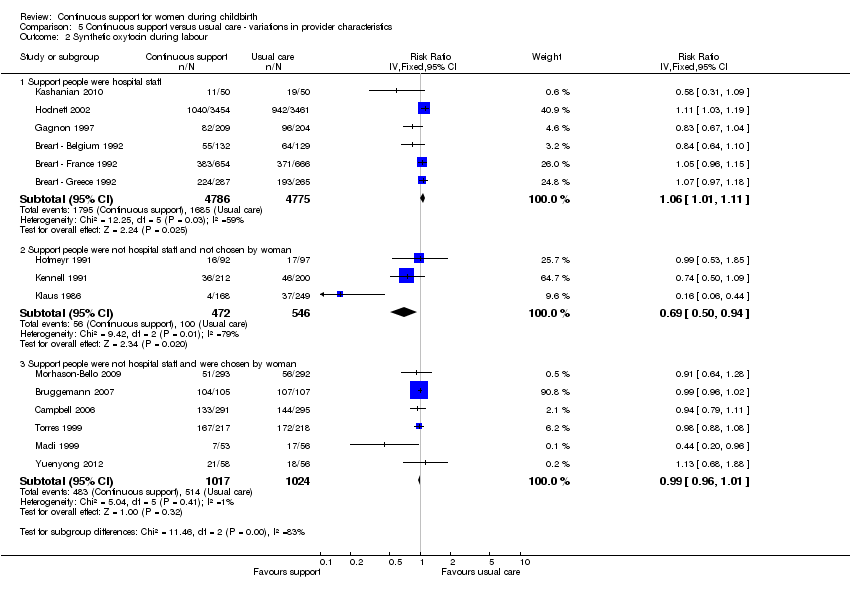
Outcome: synthetic oxytocin during labour
-
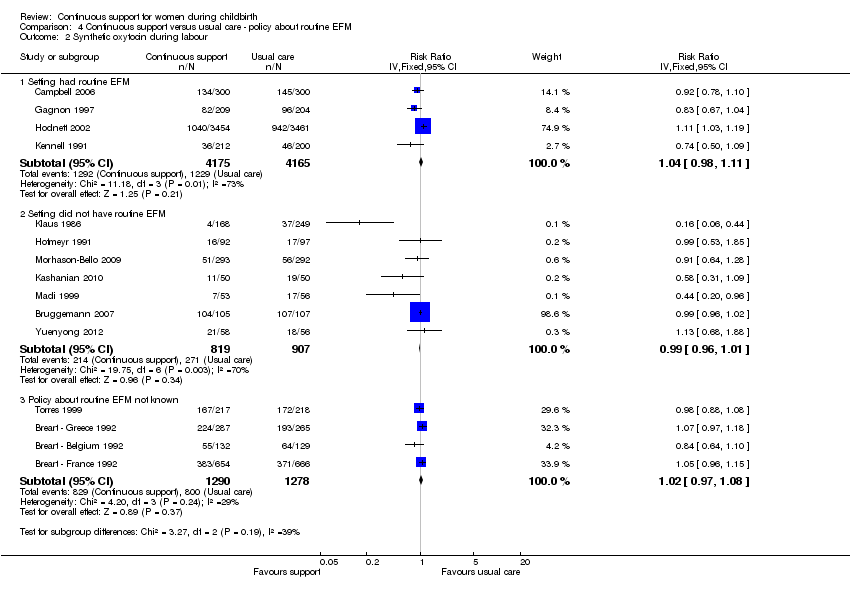
Policies about the presence of companions: in five trials (n = 9495) companions were permitted; RR 1.04, 95% CI 0.99 to 1.10. In 10 trials (n = 3125) companions were not permitted; RR 0.99, 95% CI 0.97 to 1.02. Chi² for the subgroup comparison = 3.13, P = 0.08, Analysis 2.2.
-
Availability of epidural analgesia: in eight trials (n = 10,568) epidural analgesia was routinely available; RR 1.00, 95% CI 0.98 to 1.02. In seven trials (n = 2066), epidural analgesia was not routinely available; RR 1.02, 95% CI 0.93 to 1.11. Chi² for the subgroup comparison = 0.24, P = 0.63, Analysis 3.2.
-
Use of routine EFM: in four trials (n = 8340) EFM was routine; RR 1.04, 95% CI 0.98 to 1.11. In seven trials (n = 1726) EFM was not routine; RR 0.99, 95% CI 0.96 to 1.01. In four trials (n = 2568) it is not known whether EFM was routine; RR 1.02, 95% CI 0.97 to 1.08. Chi² for the subgroup comparison = 3.27, P = 0.19, Analysis 4.2.
-
Provider characteristics: in six trials (n = 9561), the support was provided by a member of the hospital staff; RR 1.06, 95% CI 1.01 to 1.11. In three trials (n = 1018), the support was provided by a woman who was not a member of the staff and was not part of the woman's social network; RR 0.69, 95% CI 0.50 to 0.94. In six trials (n = 2041), the support was provided by a member of the woman's social network; RR 0.99, 95% CI 0.96 to 1.01. Chi² for the subgroup comparison = 11.46, P = 0.003, Analysis 5.2.
Thus the effects of continuous support on use of synthetic oxytocin during labour did not appear to be influenced by policies about the presence of companions, use of routine EFM, or availability of epidural analgesia. The effectiveness of continuous support in reducing the likelihood of intrapartum oxytocin seemed to be strongest when the provider was neither a staff member nor part of the woman's social network.
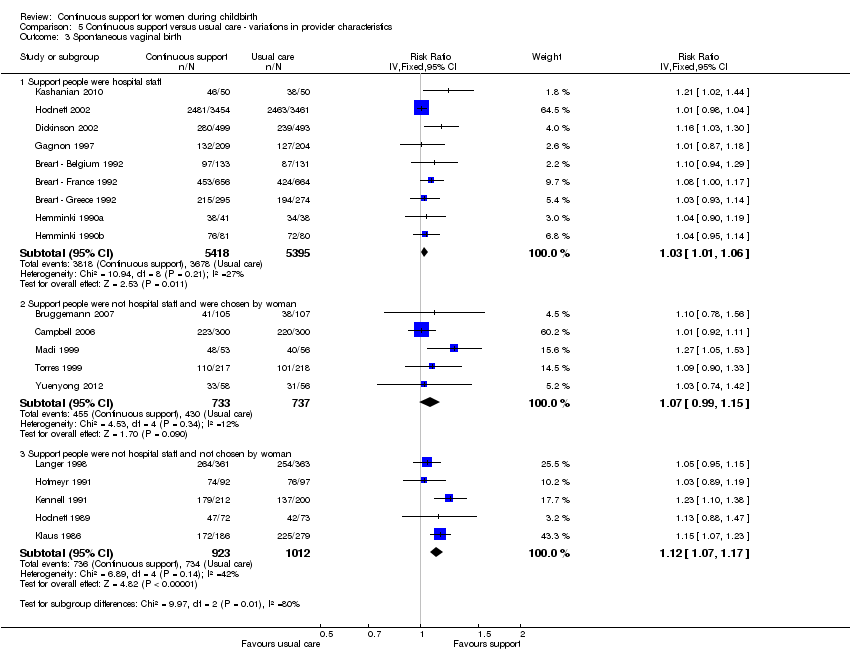
Outcome: spontaneous vaginal birth
-
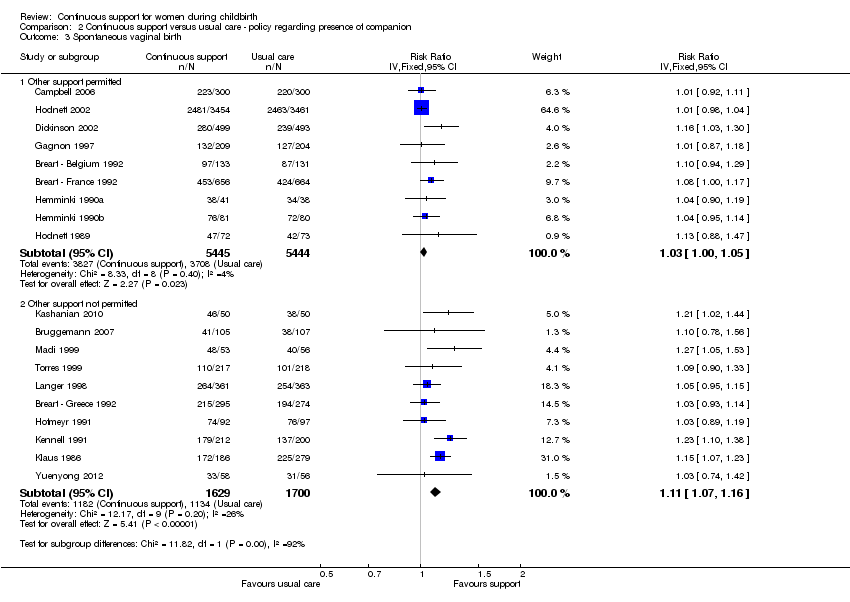
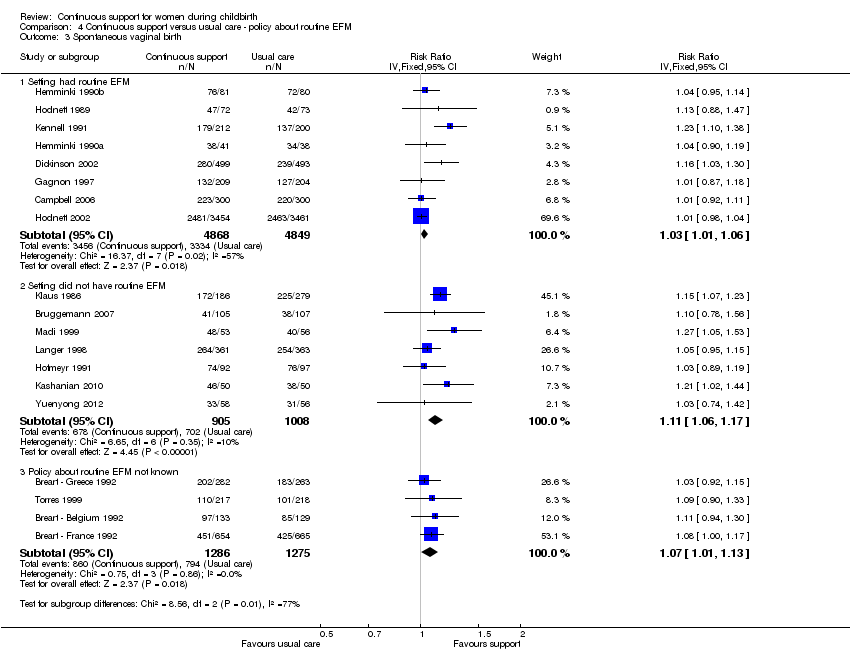
Policies about companions: In nine trials (n = 10,889) companions were permitted; RR 1.03, 95% CI 1.00 to 1.05. In ten trials (n = 3329) companions were not permitted; RR1.11, 95% CI 1.07 to 1.16. Chi² for the subgroup comparison = 11.82, P < 0.001, Analysis 2.3.
-
Availability of epidural analgesia: In 13 trials (n = 12,672), epidural analgesia was routinely available; RR 1.04, 95% CI 1.01 to 1.06). In six trials (n = 1546) epidural analgesia was not routinely available; RR 1.11, 95% CI 1.06 to 1.17. Chi² for the subgroup comparison = 6.59, P = 0.01, Analysis 3.3.
-
Routine use of EFM: In eight trials (n = 9717) EFM was routine; RR 1.03, 95% CI 1.01 to 1.06. In seven trials (n = 1913) EFM was not routine; RR 1.11, 95% CI 1.06 to 1.17. In four trials (n = 2561), the policy about routine EFM is not known; RR 1.07, 95% CI 1.01 to 1.13. Chi² for the subgroup comparison = 8.56, P = 0.01, Analysis 4.3.
-
Provider characteristics: in nine trials (n = 10,813) the support was provided by a member of the hospital staff; RR 1.03, 95% CI 1.01 to 1.06. In five trials (n = 1935) the support was provided by a woman who was not part of the hospital staff nor part of the woman's social network; RR 1.12, 95% CI 1.07 to 1.17. In five trials (n = 1470), the support was provided by a member of the woman's social network; RR 1.07, 95% CI 0.99 to 1.15. Chi² for the subgroup comparison = 9.97, P = 0.007, Analysis 5.3.
Thus the effectiveness of continuous support in increasing the likelihood of spontaneous vaginal birth appeared to be stronger when hospital policies did not permit companions, when epidural analgesia was not available, when EFM was not routine, and when the support provider was neither a staff member nor part of the woman's social network.
Outcome: caesarean birth
-
Policies about companions: in 11 trials (n = 11,326) companions were permitted; RR 0.94, 95% CI 0.85 to 1.03. In 11 trials (n = 3849) companions were not permitted; RR 0.75, 95% CI 0.65 to 0.86. Chi² for the subgroup comparison = 6.46, P = 0.01, Analysis 2.4.
-
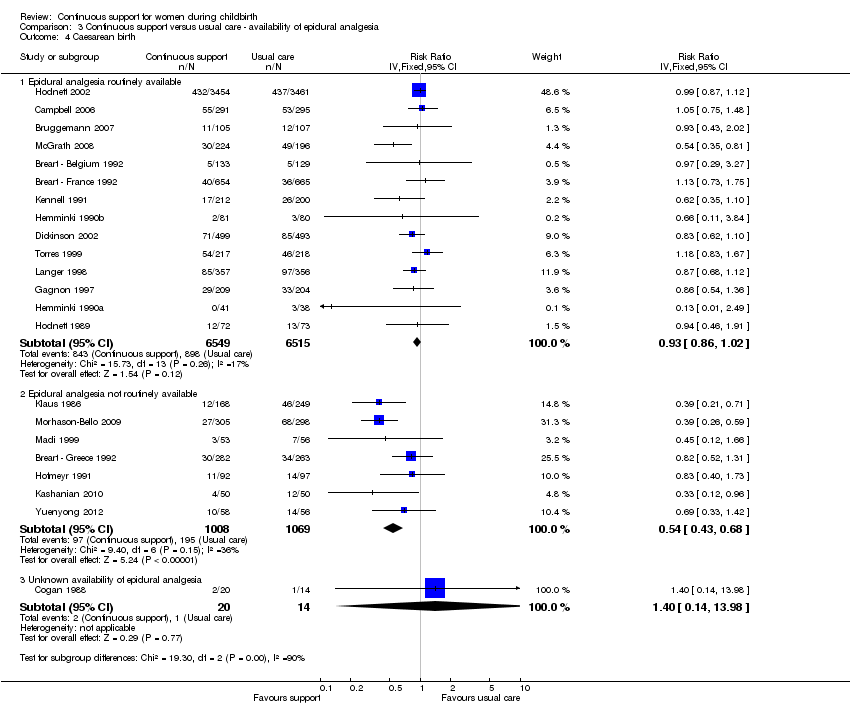
Availability of epidural analgesia: in 14 trials (n = 13,064), epidural analgesia was routinely available; RR 0.93, 95% CI 0.86 to 1.02. In seven trials (n = 2077), epidural analgesia was not routinely available; RR 0.54, 95% CI 0.43 to 0.68. In one very small trial (n = 34), we were unable to determine if epidural analgesia was routinely available; RR 1.40, 95% CI 0.14 to 13.98. Chi² for the subgroup comparison = 19.30, P < 0.0001, Analysis 3.4.
-
Routine use of EFM: in nine trials (n = 10,123), EFM was routine; RR 0.92, 95% CI 0.83 to 1.01. In eight trials (n = 2457) EFM was not routine; RR 0.66, 95% CI 0.55 to 0.79. In five trials (n = 2595), it is not known whether EFM was routine; RR 1.06, 95% CI 0.84 to 1.33. Chi² for the subgroup comparison = 12.78, P = 0.002, Analysis 4.4.
-
Provider characteristics: in nine trials (n = 10,786), the support was provided by a member of the hospital staff; RR 0.95, 95% CI 0.85 to1.05. In seven trials (n = 2330), the support was provided by a woman who was not a member of the hospital staff and not part of the woman's social network; RR 0.72, 95% CI 0.60 to 0.86. In six trials (n = 2059), the support was provided by a member of the woman's social network; RR 0.83, 95% CI 0.69 to 1.01. Chi² for the subgroup comparison = 6.88, P = 0.03, Analysis 5.4.
Thus the effectiveness of continuous support in reducing the likelihood of caesarean birth appeared to be stronger in settings where companions were not permitted, epidural analgesia was not routinely available and EFM was not routine, and when the provider was neither a staff member nor part of the woman's social network.
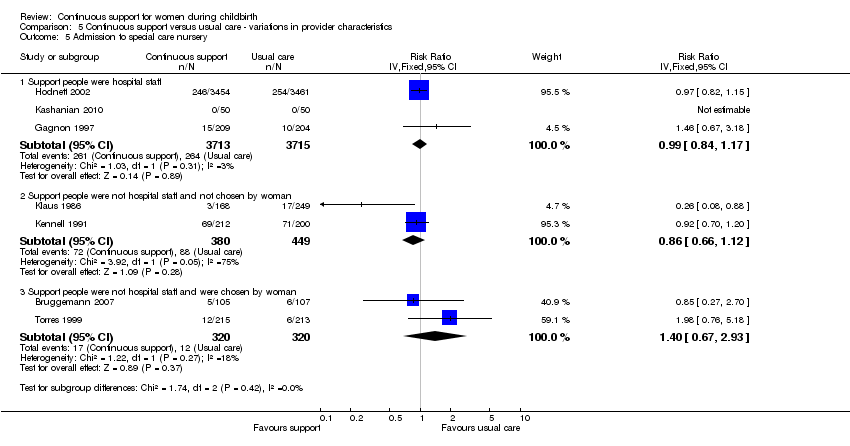
Outcome: admission to special care nursery
-
Policies about companions: in two trials (n = 7328), companions were permitted; RR 0.99, 95% CI 0.84 to 1.17. In five trials (n = 1569), companions were not permitted; RR 0.91, 95% CI 0.71 to 1.17. Chi² for the subgroup comparison = 0.28, P = 0.60, Analysis 2.5.
-
Availability of epidural analgesia: in five trials (n = 8380) epidural analgesia was routinely available; RR 0.98, 95% CI 0.85 to 1.13. In two trials (n = 517) epidural analgesia was not routinely available; RR 0.26, 95% CI 0.08 to 0.88. Chi² for the subgroup comparison = 4.51, P = 0.03, Analysis 3.5.
-
Routine use of EFM: in three trials (n = 7740) EFM was routine; RR 0.97, 95% CI 0.84 to 1.11. In three trials (n = 729) EFM was not routine; RR 0.48, 95% CI 0.21 to 1.12. In one trial (n = 428), it is not known whether EFM was routine; RR 1.98, 95% CI 0.76 to 5.18. Chi² for the subgroup comparison = 4.76, P = 0.09, Analysis 4.5.
-
Provider characteristics: in three trials (n = 7428), the support was provided by a member of the hospital staff; RR 0.99, 95% CI 0.84, 1.17. In two trials (n = 829), the support was provided by a woman who was not a member of the hospital staff and not part of the woman's social network; RR 0.86, 95% CI 0.66 to 1.12. In two trials (n = 640) the support was provided by a member of the woman's social network; RR 1.40, 95% CI 0.67 to 2.93. Chi² for the subgroup comparison = 1.74, P = 0.42, Analysis 5.5.
Thus the effectiveness of continuous support in reducing the likelihood of admission of the newborn to a special care nursery appeared to be stronger in settings in which epidural analgesia was not routinely available, but effectiveness did not appear to be influenced by policies about companions or routine EFM, or by provider characteristics.
Outcome: negatives ratings of/negative views about the birth experience
-
Policies about companions: in five trials (n = 8639) companions were permitted; RR 0.70, 95% CI 0.62 to 0.78. In six trials (n = 2539) companions were not permitted; RR 0.62, 95%CI 0.56 to 0.69. Chi² for the subgroup comparison = 2.03, P = 0.15, Analysis 2.7.
-
Availability of epidural analgesia: in nine trials (n = 10,404) epidural analgesia was routinely available; RR 0.70, 95% CI 0.64 to 0.77. In two trials (n = 774) epidural analgesia was not routinely available; RR 0.55, 95% CI 0.48 to 0.63. Chi² for the subgroup comparison = 7.92, P 0.0005, Analysis 3.7.
-
Routine use of EFM: four trials (n = 7467) were conducted in settings with routine EFM; RR 0.67, 95% CI 0.60 to 0.76. Four trials (n = 1710) were conducted in settings in which EFM was not routine; RR 0.60, 95% CI 0.53 to 0.68. Three trials (n = 1977) were in settings in which the use of routine EFM is not known; RR 0.84, 95% CI 0.65 to 1.08. Chi² for the subgroup comparison = 5.55, P = 0.06, Analysis 4.7.
-
Provider characteristics: in four trials (n = 8145) support providers were hospital staff; RR 0.87, 95% CI 0.73 to 1.03. In three trials (n = 1325) the providers were not hospital staff and not part of the woman's social network; RR 0.66, 95% CI 0.57 to 0.77. In four trials (n = 1708), providers were part of the woman's social network; RR 0.57, 95% CI 0.51 to 0.64. Chi² for the subgroup comparison = 16.47, P = 0.0003, Analysis 5.7.
Thus the effectiveness of continuous support in reducing the likelihood of dissatisfaction with or negative views of the childbirth experience appeared to be stronger in settings in which epidural analgesia was not routinely available, and when the provider was neither a staff member nor part of the woman's social network.
Discussion
This review summarises results of 22 trials involving 15,288 women, conducted in 16 countries under a wide variety of circumstances. Continuous one‐to‐one support was given by providers with a variety of experiences, through having given birth themselves and/or through education and practice as nurses, midwives, doulas or childbirth educators, or by the woman's husband or partner, female relative or close friend. The methodological quality of the trials was generally good to excellent. For all outcomes in which summary statistics were computed, comparisons of fixed‐effect and random‐effects analyses did not yield material differences in the results. Thus neither the risk of bias nor heterogeneity should be of concern when interpreting results.
In the primary comparison, women who were allocated to continuous one‐to‐one support were more likely to have a spontaneous vaginal birth (risk ratio (RR) 1.08, 95% confidence interval (CI) 1.04 to 1.12) and less likely to have intrapartum analgesia (RR 0.90, 95% CI 0.84 to 0.96) or to report dissatisfaction (RR 0.69, 95% CI 0.59 to 0.79). In addition their labours were shorter (mean difference (MD) ‐0.58 hours, 95% CI ‐0.85 to ‐0.31), they were less likely to have a caesarean (RR 0.78, 95% CI 0.67 to 0.91) or instrumental vaginal birth (RR 0.90, 95% CI 0.85 to 0.96), regional analgesia (RR 0.93, 95% CI 0.88 to 0.99), or a baby with a low five‐minute Apgar score (RR 0.69, 95% CI 0.50 to 0.95). The trial reports do not list any adverse effects. This form of care appears to confer important benefits without attendant risks. The results of earlier versions of this review prompted organisations in Canada, the UK and the USA to issue practice guidelines, advocating continuous support (AWHONN 2002; MIDIRS 1999; NICE Intrapartum Care 2007; SOGC 1995). The results of the primary comparison in the current review offer continued justification for such practice guidelines.
The subgroup analyses should be interpreted with caution. Individually each should be considered exploratory and hypothesis‐generating, particularly when the sample size in one subgroup was much smaller than in another. However, taken in their totality, the consistency of the patterns suggests that the effectiveness of continuous intrapartum support may be enhanced or reduced by policies and practices in the birth setting and by the nature of the relationship between the provider and labouring woman.
We chose three aspects of the birth environment ‐ routine use of electronic fetal monitoring (EFM), availability of epidural analgesia and policies about the presence of additional support people of the woman's own choosing ‐ as proxies for environmental conditions that may mediate the effectiveness of labour support. This review cannot answer questions about the mechanisms whereby settings with epidural analgesia limit the effectiveness of labour support. The impact of epidural analgesia may be direct (Anim‐Somuah 2011) or indirect, as part of the 'cascade of interventions' described in the Background. The effects of a policy of routine EFM are less clear, most likely because we were unable to obtain information about EFM policies for several of the trials. However, continuous labour support in settings without routine EFM was associated with greater likelihood of spontaneous vaginal birth and lower likelihood of a caesarean birth. These results raise questions about the ability of labour support to act as a buffer against adverse aspects of routine medical interventions. Labour support appears to be effective in reducing the adverse consequences of the fear and distress associated with labouring alone in an unfamiliar environment. A report of a qualitative component of one of the included trials (Langer 1998), aptly titled "Alone, I wouldn't have known what to do", provides further justification for this argument.
Effects of continuous labour support appear to vary by provider characteristics. Divided loyalties, additional duties besides labour support, self‐selection and the constraints of institutional policies and routine practices may all have played a role in the apparently limited effectiveness of members of the hospital staff. Childbirth environments influence the healthcare professionals who work in them as well as labouring women and their support people. Furthermore, while women want and benefit from the presence of selected members of their social network, the support of partners and others with whom they have a longstanding relationship is qualitatively different and more complex than that of a woman who is experienced and often trained to provide labour support and who has no other role other than to provide it. An early trial of labour support with partners present found that women received more support from their partners when a doula was present to guide them, and the partners themselves reported more support (Hodnett 1989). While continuous labour support appears to be more effective when it is provided by caregivers who are not employees of an institution (and thus have no obligation to anyone other than the labouring woman) and who have an exclusive focus on this task, support from a member of the woman's social network is effective in improving women's satisfaction with their birth experiences.
There remains relatively little information about the effects of continuous intrapartum support on mothers' and babies' health and well‐being in the postpartum period.
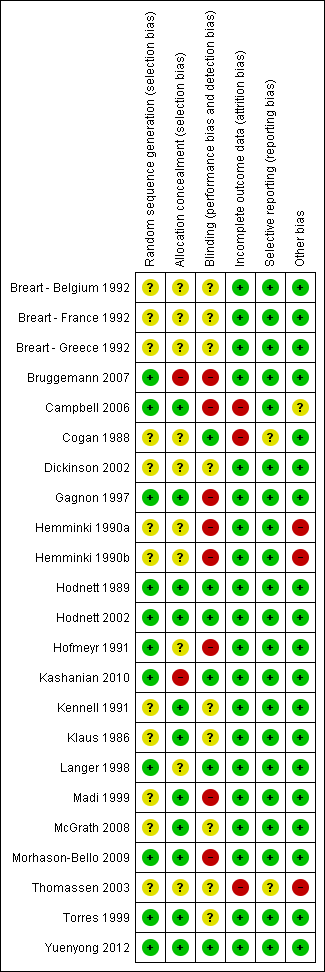
Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
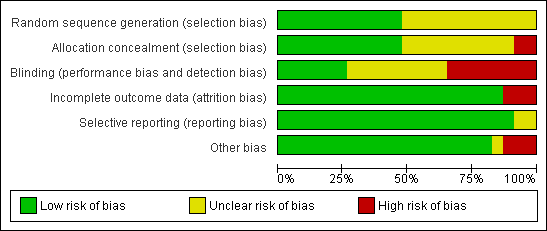
Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies

Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 1 Any analgesia/anaesthesia.
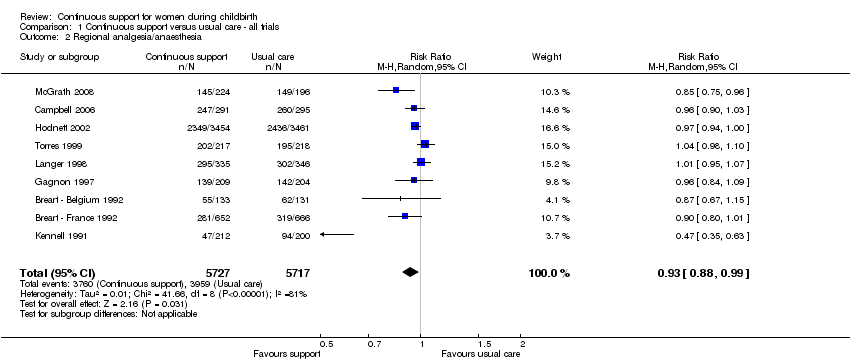
Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 2 Regional analgesia/anaesthesia.
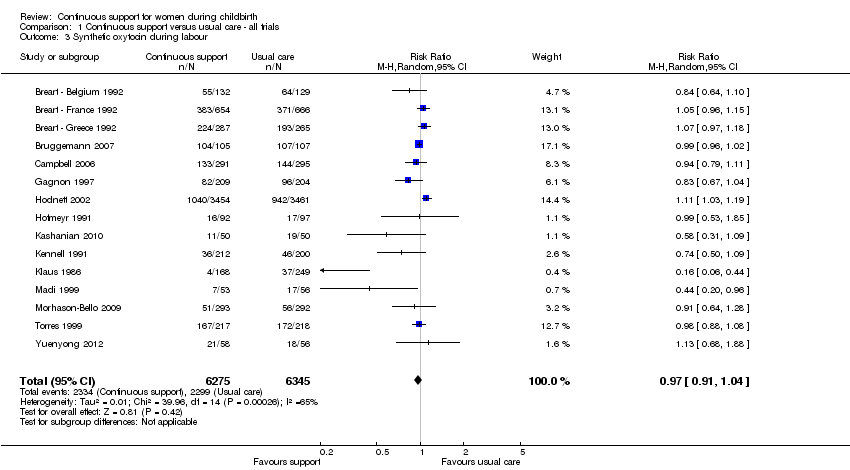
Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 3 Synthetic oxytocin during labour.
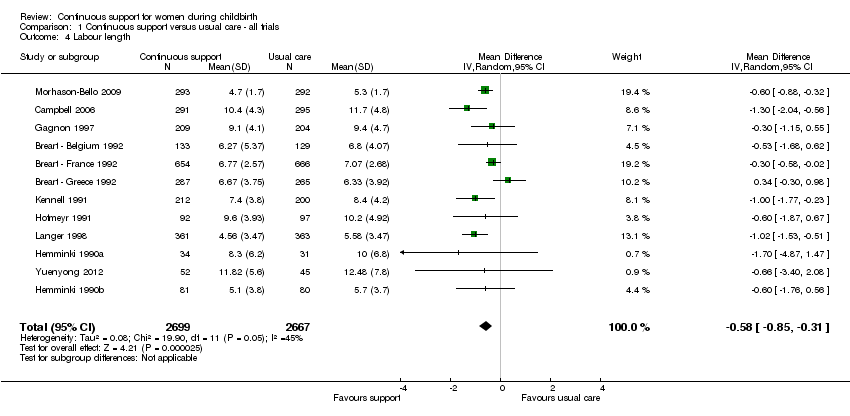
Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 4 Labour length.
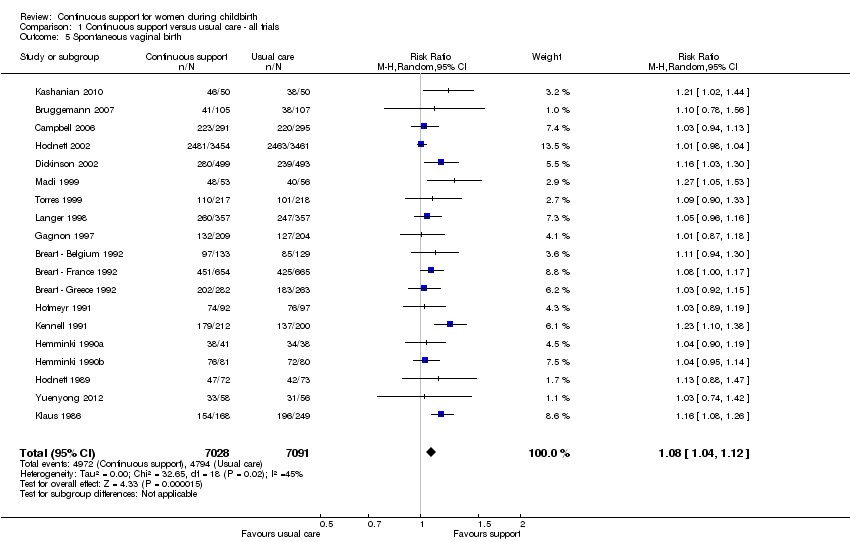
Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 5 Spontaneous vaginal birth.

Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 6 Instrumental vaginal birth.

Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 7 Caesarean birth.
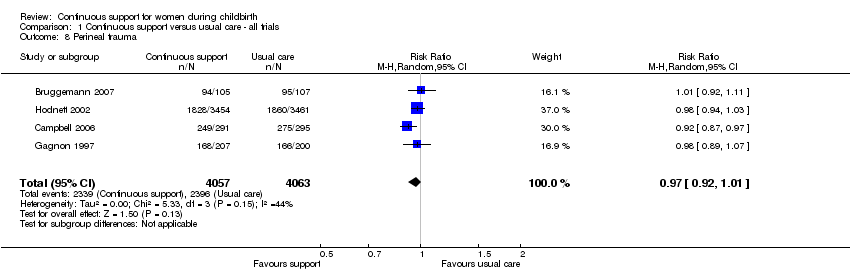
Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 8 Perineal trauma.
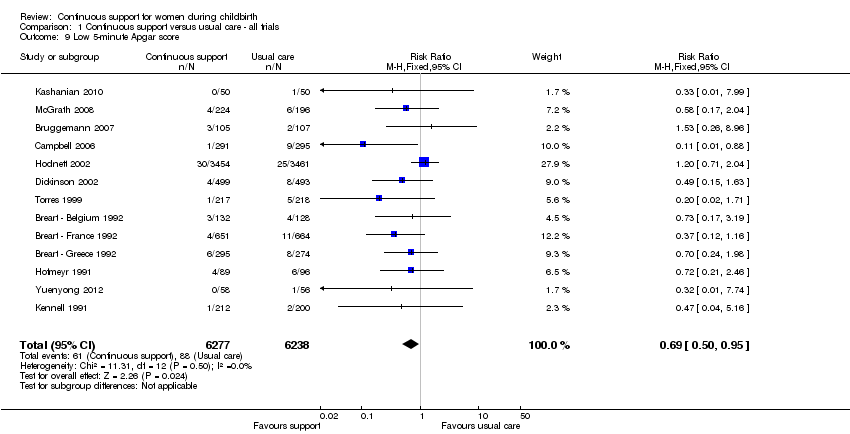
Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 9 Low 5‐minute Apgar score.

Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 10 Admission to special care nursery.
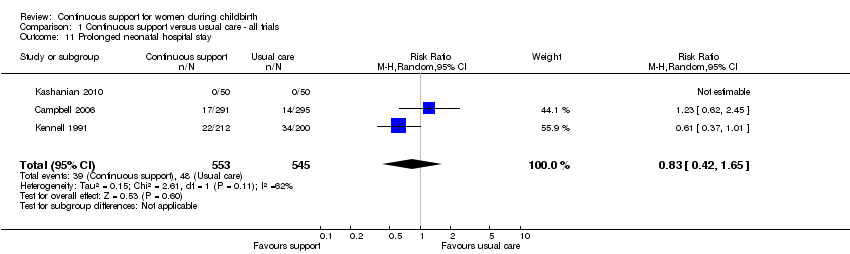
Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 11 Prolonged neonatal hospital stay.
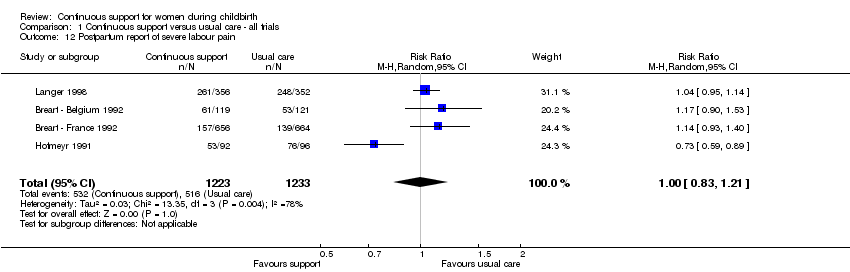
Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 12 Postpartum report of severe labour pain.
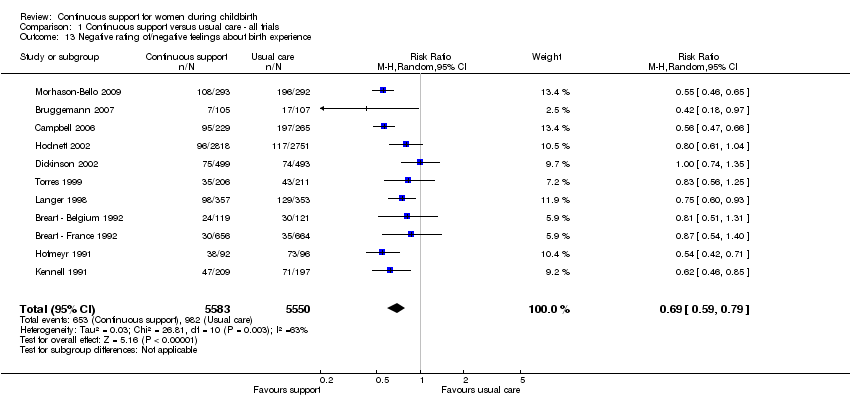
Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 13 Negative rating of/negative feelings about birth experience.

Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 14 Difficulty mothering.
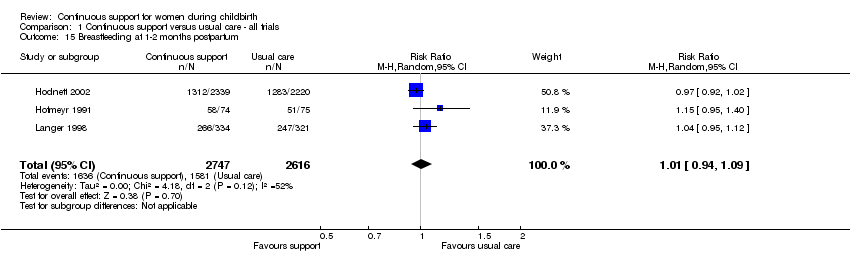
Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 15 Breastfeeding at 1‐2 months postpartum.

Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 16 Postpartum depression.
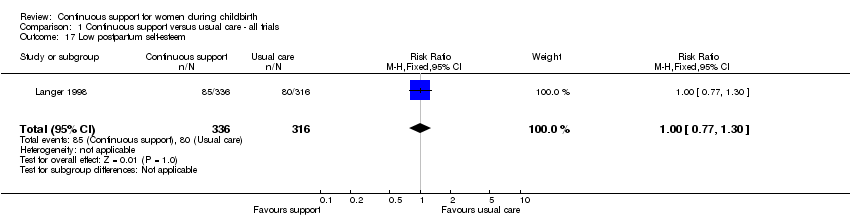
Comparison 1 Continuous support versus usual care ‐ all trials, Outcome 17 Low postpartum self‐esteem.
Comparison 2 Continuous support versus usual care ‐ policy regarding presence of companion, Outcome 1 Any analgesia/anaesthesia.

Comparison 2 Continuous support versus usual care ‐ policy regarding presence of companion, Outcome 2 Synthetic oxytocin during labour.
Comparison 2 Continuous support versus usual care ‐ policy regarding presence of companion, Outcome 3 Spontaneous vaginal birth.

Comparison 2 Continuous support versus usual care ‐ policy regarding presence of companion, Outcome 4 Caesarean birth.

Comparison 2 Continuous support versus usual care ‐ policy regarding presence of companion, Outcome 5 Admission to special care nursery.
Comparison 2 Continuous support versus usual care ‐ policy regarding presence of companion, Outcome 6 Postpartum depression.

Comparison 2 Continuous support versus usual care ‐ policy regarding presence of companion, Outcome 7 Negative rating of/negative feelings about birth experience.

Comparison 2 Continuous support versus usual care ‐ policy regarding presence of companion, Outcome 8 Breastfeeding at 1‐2 months postpartum.
Comparison 3 Continuous support versus usual care ‐ availability of epidural analgesia, Outcome 1 Any analgesia/anaesthesia.

Comparison 3 Continuous support versus usual care ‐ availability of epidural analgesia, Outcome 2 Synthetic oxytocin during labour.

Comparison 3 Continuous support versus usual care ‐ availability of epidural analgesia, Outcome 3 Spontaneous vaginal birth.
Comparison 3 Continuous support versus usual care ‐ availability of epidural analgesia, Outcome 4 Caesarean birth.

Comparison 3 Continuous support versus usual care ‐ availability of epidural analgesia, Outcome 5 Admission to special care nursery.

Comparison 3 Continuous support versus usual care ‐ availability of epidural analgesia, Outcome 6 Postpartum depression.

Comparison 3 Continuous support versus usual care ‐ availability of epidural analgesia, Outcome 7 Negative rating of/negative feelings about birth experience.
Comparison 3 Continuous support versus usual care ‐ availability of epidural analgesia, Outcome 8 Breastfeeding at 1‐2 months postpartum.
Comparison 4 Continuous support versus usual care ‐ policy about routine EFM, Outcome 1 Any analgesia/anaesthesia.
Comparison 4 Continuous support versus usual care ‐ policy about routine EFM, Outcome 2 Synthetic oxytocin during labour.
Comparison 4 Continuous support versus usual care ‐ policy about routine EFM, Outcome 3 Spontaneous vaginal birth.

Comparison 4 Continuous support versus usual care ‐ policy about routine EFM, Outcome 4 Caesarean birth.

Comparison 4 Continuous support versus usual care ‐ policy about routine EFM, Outcome 5 Admission to special care nursery.

Comparison 4 Continuous support versus usual care ‐ policy about routine EFM, Outcome 6 Postpartum depression.

Comparison 4 Continuous support versus usual care ‐ policy about routine EFM, Outcome 7 Negative rating of/negative views about birth experience.
Comparison 4 Continuous support versus usual care ‐ policy about routine EFM, Outcome 8 Breastfeeding at 1‐2 months postpartum.
Comparison 5 Continuous support versus usual care ‐ variations in provider characteristics, Outcome 1 Any analgesia/anaesthesia.
Comparison 5 Continuous support versus usual care ‐ variations in provider characteristics, Outcome 2 Synthetic oxytocin during labour.
Comparison 5 Continuous support versus usual care ‐ variations in provider characteristics, Outcome 3 Spontaneous vaginal birth.

Comparison 5 Continuous support versus usual care ‐ variations in provider characteristics, Outcome 4 Caesarean birth.
Comparison 5 Continuous support versus usual care ‐ variations in provider characteristics, Outcome 5 Admission to special care nursery.

Comparison 5 Continuous support versus usual care ‐ variations in provider characteristics, Outcome 6 Postpartum depression.

Comparison 5 Continuous support versus usual care ‐ variations in provider characteristics, Outcome 7 Negative rating of/negative feelings about birth experience.
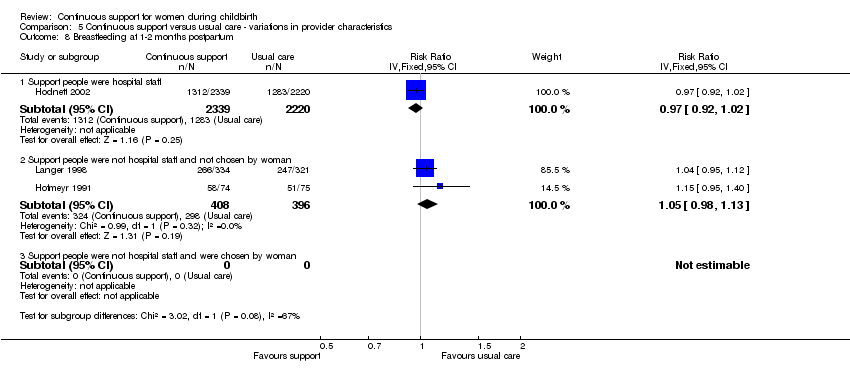
Comparison 5 Continuous support versus usual care ‐ variations in provider characteristics, Outcome 8 Breastfeeding at 1‐2 months postpartum.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Any analgesia/anaesthesia Show forest plot | 14 | 12283 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.84, 0.96] |
| 2 Regional analgesia/anaesthesia Show forest plot | 9 | 11444 | Risk Ratio (M‐H, Random, 95% CI) | 0.93 [0.88, 0.99] |
| 3 Synthetic oxytocin during labour Show forest plot | 15 | 12620 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.91, 1.04] |
| 4 Labour length Show forest plot | 12 | 5366 | Mean Difference (IV, Random, 95% CI) | ‐0.58 [‐0.85, ‐0.31] |
| 5 Spontaneous vaginal birth Show forest plot | 19 | 14119 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [1.04, 1.12] |
| 6 Instrumental vaginal birth Show forest plot | 19 | 14118 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.85, 0.96] |
| 7 Caesarean birth Show forest plot | 22 | 15175 | Risk Ratio (M‐H, Random, 95% CI) | 0.78 [0.67, 0.91] |
| 8 Perineal trauma Show forest plot | 4 | 8120 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.92, 1.01] |
| 9 Low 5‐minute Apgar score Show forest plot | 13 | 12515 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.69 [0.50, 0.95] |
| 10 Admission to special care nursery Show forest plot | 7 | 8897 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.76, 1.25] |
| 11 Prolonged neonatal hospital stay Show forest plot | 3 | 1098 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.42, 1.65] |
| 12 Postpartum report of severe labour pain Show forest plot | 4 | 2456 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.83, 1.21] |
| 13 Negative rating of/negative feelings about birth experience Show forest plot | 11 | 11133 | Risk Ratio (M‐H, Random, 95% CI) | 0.69 [0.59, 0.79] |
| 14 Difficulty mothering Show forest plot | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 15 Breastfeeding at 1‐2 months postpartum Show forest plot | 3 | 5363 | Risk Ratio (M‐H, Random, 95% CI) | 1.01 [0.94, 1.09] |
| 16 Postpartum depression Show forest plot | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 17 Low postpartum self‐esteem Show forest plot | 1 | 652 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.77, 1.30] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Any analgesia/anaesthesia Show forest plot | 14 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1 Other support permitted | 7 | 9752 | Risk Ratio (IV, Fixed, 95% CI) | 0.97 [0.96, 0.99] |
| 1.2 Other support not permitted | 7 | 2598 | Risk Ratio (IV, Fixed, 95% CI) | 0.91 [0.85, 0.96] |
| 2 Synthetic oxytocin during labour Show forest plot | 15 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 2.1 Other support permitted | 5 | 9495 | Risk Ratio (IV, Fixed, 95% CI) | 1.04 [0.99, 1.10] |
| 2.2 Other support not permitted | 10 | 3125 | Risk Ratio (IV, Fixed, 95% CI) | 0.99 [0.97, 1.02] |
| 3 Spontaneous vaginal birth Show forest plot | 19 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 3.1 Other support permitted | 9 | 10889 | Risk Ratio (IV, Fixed, 95% CI) | 1.03 [1.00, 1.05] |
| 3.2 Other support not permitted | 10 | 3329 | Risk Ratio (IV, Fixed, 95% CI) | 1.11 [1.07, 1.16] |
| 4 Caesarean birth Show forest plot | 22 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 4.1 Other support permitted | 11 | 11326 | Risk Ratio (IV, Fixed, 95% CI) | 0.94 [0.85, 1.03] |
| 4.2 Other support not permitted | 11 | 3849 | Risk Ratio (IV, Fixed, 95% CI) | 0.75 [0.65, 0.86] |
| 5 Admission to special care nursery Show forest plot | 7 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 5.1 Other support permitted | 2 | 7328 | Risk Ratio (IV, Fixed, 95% CI) | 0.99 [0.84, 1.17] |
| 5.2 Other support not permitted | 5 | 1569 | Risk Ratio (IV, Fixed, 95% CI) | 0.91 [0.71, 1.17] |
| 6 Postpartum depression Show forest plot | 2 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 6.1 Other support permitted | 1 | 5567 | Risk Ratio (IV, Fixed, 95% CI) | 0.86 [0.73, 1.02] |
| 6.2 Other support not permitted | 1 | 149 | Risk Ratio (IV, Fixed, 95% CI) | 0.18 [0.09, 0.36] |
| 7 Negative rating of/negative feelings about birth experience Show forest plot | 11 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 7.1 Other support permitted | 5 | 8639 | Risk Ratio (IV, Fixed, 95% CI) | 0.70 [0.62, 0.78] |
| 7.2 Other support not permitted | 6 | 2539 | Risk Ratio (IV, Fixed, 95% CI) | 0.62 [0.56, 0.69] |
| 8 Breastfeeding at 1‐2 months postpartum Show forest plot | 3 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 8.1 Other support permitted | 1 | 4559 | Risk Ratio (IV, Fixed, 95% CI) | 0.97 [0.92, 1.02] |
| 8.2 Other support not permitted | 2 | 804 | Risk Ratio (IV, Fixed, 95% CI) | 1.05 [0.98, 1.13] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Any analgesia/anaesthesia Show forest plot | 14 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1 Epidural analgesia routinely available | 9 | 10888 | Risk Ratio (IV, Fixed, 95% CI) | 0.97 [0.96, 0.98] |
| 1.2 Epidural analgesia not routinely available | 5 | 1462 | Risk Ratio (IV, Fixed, 95% CI) | 0.83 [0.69, 0.99] |
| 2 Synthetic oxytocin during labour Show forest plot | 15 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 2.1 Epidural analgesia routinely available | 8 | 10568 | Risk Ratio (IV, Fixed, 95% CI) | 1.00 [0.98, 1.02] |
| 2.2 Epidural analgesia not routinely available | 7 | 2066 | Risk Ratio (IV, Fixed, 95% CI) | 1.02 [0.93, 1.11] |
| 3 Spontaneous vaginal birth Show forest plot | 19 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 3.1 Epidural analgesia routinely available | 13 | 12672 | Risk Ratio (IV, Fixed, 95% CI) | 1.04 [1.01, 1.06] |
| 3.2 Epidural analgesia not routinely available | 6 | 1546 | Risk Ratio (IV, Fixed, 95% CI) | 1.11 [1.06, 1.17] |
| 4 Caesarean birth Show forest plot | 22 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 4.1 Epidural analgesia routinely available | 14 | 13064 | Risk Ratio (IV, Fixed, 95% CI) | 0.93 [0.86, 1.02] |
| 4.2 Epidural analgesia not routinely available | 7 | 2077 | Risk Ratio (IV, Fixed, 95% CI) | 0.54 [0.43, 0.68] |
| 4.3 Unknown availability of epidural analgesia | 1 | 34 | Risk Ratio (IV, Fixed, 95% CI) | 1.4 [0.14, 13.98] |
| 5 Admission to special care nursery Show forest plot | 7 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 5.1 Epidural analgesia routinely available | 5 | 8380 | Risk Ratio (IV, Fixed, 95% CI) | 0.98 [0.85, 1.13] |
| 5.2 Epidural analgesia not routinely available | 2 | 517 | Risk Ratio (IV, Fixed, 95% CI) | 0.26 [0.08, 0.88] |
| 6 Postpartum depression Show forest plot | 2 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 6.1 Epidural analgesia routinely available | 1 | 6915 | Risk Ratio (IV, Fixed, 95% CI) | 0.89 [0.75, 1.05] |
| 6.2 Epidural analgesia not routinely available | 1 | 149 | Risk Ratio (IV, Fixed, 95% CI) | 0.18 [0.09, 0.36] |
| 7 Negative rating of/negative feelings about birth experience Show forest plot | 11 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 7.1 Epidural analgesia routinely available | 9 | 10404 | Risk Ratio (IV, Fixed, 95% CI) | 0.70 [0.64, 0.77] |
| 7.2 Epidural analgesia not routinely available | 2 | 774 | Risk Ratio (IV, Fixed, 95% CI) | 0.55 [0.48, 0.63] |
| 8 Breastfeeding at 1‐2 months postpartum Show forest plot | 3 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 8.1 Epidural analgesia routinely available | 2 | 5214 | Risk Ratio (IV, Fixed, 95% CI) | 0.99 [0.95, 1.03] |
| 8.2 Epidural analgesia not routinely available | 1 | 149 | Risk Ratio (IV, Fixed, 95% CI) | 1.15 [0.95, 1.40] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Any analgesia/anaesthesia Show forest plot | 14 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1 Setting had routine EFM | 6 | 8580 | Risk Ratio (IV, Fixed, 95% CI) | 0.97 [0.96, 0.99] |
| 1.2 Setting did not have routine EFM | 6 | 2186 | Risk Ratio (IV, Fixed, 95% CI) | 0.96 [0.90, 1.02] |
| 1.3 Policy about routine EFM not known | 2 | 1579 | Risk Ratio (IV, Fixed, 95% CI) | 0.89 [0.80, 0.99] |
| 2 Synthetic oxytocin during labour Show forest plot | 15 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 2.1 Setting had routine EFM | 4 | 8340 | Risk Ratio (IV, Fixed, 95% CI) | 1.04 [0.98, 1.11] |
| 2.2 Setting did not have routine EFM | 7 | 1726 | Risk Ratio (IV, Fixed, 95% CI) | 0.99 [0.96, 1.01] |
| 2.3 Policy about routine EFM not known | 4 | 2568 | Risk Ratio (IV, Fixed, 95% CI) | 1.02 [0.97, 1.08] |
| 3 Spontaneous vaginal birth Show forest plot | 19 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 3.1 Setting had routine EFM | 8 | 9717 | Risk Ratio (IV, Fixed, 95% CI) | 1.03 [1.01, 1.06] |
| 3.2 Setting did not have routine EFM | 7 | 1913 | Risk Ratio (IV, Fixed, 95% CI) | 1.11 [1.06, 1.17] |
| 3.3 Policy about routine EFM not known | 4 | 2561 | Risk Ratio (IV, Fixed, 95% CI) | 1.07 [1.01, 1.13] |
| 4 Caesarean birth Show forest plot | 22 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 4.1 Setting had routine EFM | 9 | 10123 | Risk Ratio (IV, Fixed, 95% CI) | 0.92 [0.83, 1.01] |
| 4.2 Setting did not have routine EFM | 8 | 2457 | Risk Ratio (IV, Fixed, 95% CI) | 0.66 [0.55, 0.79] |
| 4.3 Policy about routine EFM not known | 5 | 2595 | Risk Ratio (IV, Fixed, 95% CI) | 1.06 [0.84, 1.33] |
| 5 Admission to special care nursery Show forest plot | 7 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 5.1 Setting had routine EFM | 3 | 7740 | Risk Ratio (IV, Fixed, 95% CI) | 0.97 [0.84, 1.11] |
| 5.2 Setting did not have routine EFM | 3 | 729 | Risk Ratio (IV, Fixed, 95% CI) | 0.48 [0.21, 1.12] |
| 5.3 Policy about routine EFM not known | 1 | 428 | Risk Ratio (IV, Fixed, 95% CI) | 1.98 [0.76, 5.18] |
| 6 Postpartum depression Show forest plot | 2 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 6.1 Setting had routine EFM | 1 | 6915 | Risk Ratio (IV, Fixed, 95% CI) | 0.89 [0.75, 1.05] |
| 6.2 Setting did not have routine EFM | 1 | 149 | Risk Ratio (IV, Fixed, 95% CI) | 0.18 [0.09, 0.36] |
| 7 Negative rating of/negative views about birth experience Show forest plot | 11 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 7.1 Setting had routine EFM | 4 | 7467 | Risk Ratio (IV, Fixed, 95% CI) | 0.67 [0.60, 0.76] |
| 7.2 Setting did not have routine EFM | 4 | 1710 | Risk Ratio (IV, Fixed, 95% CI) | 0.60 [0.53, 0.68] |
| 7.3 Policy about routine EFM not known | 3 | 1977 | Risk Ratio (IV, Fixed, 95% CI) | 0.84 [0.65, 1.08] |
| 8 Breastfeeding at 1‐2 months postpartum Show forest plot | 3 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 8.1 Setting had routine EFM | 1 | 4559 | Risk Ratio (IV, Fixed, 95% CI) | 0.97 [0.92, 1.02] |
| 8.2 Setting did not have routine EFM | 2 | 804 | Risk Ratio (IV, Fixed, 95% CI) | 1.05 [0.98, 1.13] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Any analgesia/anaesthesia Show forest plot | 14 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1 Support people were hospital staff | 6 | 9152 | Risk Ratio (IV, Fixed, 95% CI) | 0.97 [0.96, 0.99] |
| 1.2 Support people were not hospital staff and not chosen by woman | 4 | 1790 | Risk Ratio (IV, Fixed, 95% CI) | 0.91 [0.86, 0.97] |
| 1.3 Support people were not hospital staff and were chosen by woman | 4 | 1408 | Risk Ratio (IV, Fixed, 95% CI) | 0.94 [0.88, 1.00] |
| 2 Synthetic oxytocin during labour Show forest plot | 15 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 2.1 Support people were hospital staff | 6 | 9561 | Risk Ratio (IV, Fixed, 95% CI) | 1.06 [1.01, 1.11] |
| 2.2 Support people were not hospital staff and not chosen by woman | 3 | 1018 | Risk Ratio (IV, Fixed, 95% CI) | 0.69 [0.50, 0.94] |
| 2.3 Support people were not hospital staff and were chosen by woman | 6 | 2041 | Risk Ratio (IV, Fixed, 95% CI) | 0.99 [0.96, 1.01] |
| 3 Spontaneous vaginal birth Show forest plot | 19 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 3.1 Support people were hospital staff | 9 | 10813 | Risk Ratio (IV, Fixed, 95% CI) | 1.03 [1.01, 1.06] |
| 3.2 Support people were not hospital staff and were chosen by woman | 5 | 1470 | Risk Ratio (IV, Fixed, 95% CI) | 1.07 [0.99, 1.15] |
| 3.3 Support people were not hospital staff and not chosen by woman | 5 | 1935 | Risk Ratio (IV, Fixed, 95% CI) | 1.12 [1.07, 1.17] |
| 4 Caesarean birth Show forest plot | 22 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 4.1 Support people were hospital staff | 9 | 10786 | Risk Ratio (IV, Fixed, 95% CI) | 0.95 [0.85, 1.05] |
| 4.2 Support people were not hospital staff and not chosen by woman | 7 | 2330 | Risk Ratio (IV, Fixed, 95% CI) | 0.72 [0.60, 0.86] |
| 4.3 Support people were not hospital staff and were chosen by woman | 6 | 2059 | Risk Ratio (IV, Fixed, 95% CI) | 0.83 [0.69, 1.01] |
| 5 Admission to special care nursery Show forest plot | 7 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 5.1 Support people were hospital staff | 3 | 7428 | Risk Ratio (IV, Fixed, 95% CI) | 0.99 [0.84, 1.17] |
| 5.2 Support people were not hospital staff and not chosen by woman | 2 | 829 | Risk Ratio (IV, Fixed, 95% CI) | 0.86 [0.66, 1.12] |
| 5.3 Support people were not hospital staff and were chosen by woman | 2 | 640 | Risk Ratio (IV, Fixed, 95% CI) | 1.40 [0.67, 2.93] |
| 6 Postpartum depression Show forest plot | 2 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 6.1 Support people were hospital staff | 1 | 5567 | Risk Ratio (IV, Fixed, 95% CI) | 0.86 [0.73, 1.02] |
| 6.2 Support people were not hospital staff and not chosen by woman | 1 | 149 | Risk Ratio (IV, Fixed, 95% CI) | 0.17 [0.09, 0.33] |
| 6.3 Support people were not hospital staff and were chosen by woman | 0 | 0 | Risk Ratio (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 7 Negative rating of/negative feelings about birth experience Show forest plot | 11 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 7.1 Support people were hospital staff | 4 | 8145 | Risk Ratio (IV, Fixed, 95% CI) | 0.87 [0.73, 1.03] |
| 7.2 Support people were not hospital staff and not chosen by woman | 3 | 1325 | Risk Ratio (IV, Fixed, 95% CI) | 0.66 [0.57, 0.77] |
| 7.3 Support people were not hospital staff and were chosen by woman | 4 | 1708 | Risk Ratio (IV, Fixed, 95% CI) | 0.57 [0.51, 0.64] |
| 8 Breastfeeding at 1‐2 months postpartum Show forest plot | 3 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 8.1 Support people were hospital staff | 1 | 4559 | Risk Ratio (IV, Fixed, 95% CI) | 0.97 [0.92, 1.02] |
| 8.2 Support people were not hospital staff and not chosen by woman | 2 | 804 | Risk Ratio (IV, Fixed, 95% CI) | 1.05 [0.98, 1.13] |
| 8.3 Support people were not hospital staff and were chosen by woman | 0 | 0 | Risk Ratio (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |