Le tramadol pour les douleurs neuropathiques chez l'adulte
Appendices
Appendix 1. Methodological considerations for chronic pain
There have been several recent changes in how the efficacy of conventional and unconventional treatments is assessed in chronic painful conditions. The outcomes are now better defined, particularly with new criteria for what constitutes moderate or substantial benefit (Dworkin 2008); older trials may only report participants with 'any improvement'. Newer trials tend to be larger, avoiding problems from the random play of chance. Newer trials also tend to be of longer duration, up to 12 weeks, and longer trials provide a more rigorous and valid assessment of efficacy in chronic conditions. New standards have evolved for assessing efficacy in neuropathic pain, and we are now applying stricter criteria for the inclusion of trials and assessment of outcomes, and are more aware of problems that may affect our overall assessment. To summarise some of the recent insights that must be considered in this new review:
-
Pain results tend to have a U‐shaped distribution rather than a bell‐shaped distribution. This is true in acute pain (Moore 2011a; Moore 2011b), back pain (Moore 2010c), and arthritis (Moore 2010d), as well as in fibromyalgia (Straube 2010); in all cases average results usually describe the experience of almost no‐one in the trial. Data expressed as averages are potentially misleading, unless they can be proven to be suitable.
-
As a consequence, we have to depend on dichotomous results (the individual either has or does not have the outcome) usually from pain changes or patient global assessments. The Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) group has helped with their definitions of minimal, moderate, and substantial improvement (Dworkin 2008). In arthritis, trials of less than 12 weeks' duration, and especially those shorter than eight weeks, overestimate the effect of treatment (Moore 2010c); the effect is particularly strong for less effective analgesics, and this may also be relevant in neuropathic‐type pain.
-
The proportion of patients with at least moderate benefit can be small, even with an effective medicine, falling from 60% with an effective medicine in arthritis to 30% in fibromyalgia (Moore 2009; Moore 2010c; Moore 2010d; Moore 2013b; Moore 2014b; Straube 2008; Sultan 2008). A Cochrane Review of pregabalin in neuropathic pain and fibromyalgia demonstrated different response rates for different types of chronic pain (higher in diabetic neuropathy and postherpetic neuralgia and lower in central pain and fibromyalgia) (Moore 2009). This indicates that different neuropathic pain conditions should be treated separately from one another, and that pooling should not be done unless there are good grounds for doing so.
-
Individual patient analyses indicate that patients who get good pain relief (moderate or better) have major benefits in many other outcomes, affecting quality of life in a significant way (Moore 2010b; Moore 2014a).
-
Imputation methods such as last observation carried forward (LOCF), used when participants withdraw from clinical trials, can overstate drug efficacy especially when adverse event withdrawals with drug are greater than those with placebo (Moore 2012).
Appendix 2. CENTRAL search strategy (via CRSO)
-
MESH DESCRIPTOR Tramadol (757)
-
(tramadol* or tramal* or ultram or zamadol or zydol):TI,AB,KY (2227)
-
1 OR 2 (2227)
-
MESH DESCRIPTOR Neuralgia EXPLODE ALL TREES (718)
-
MESH DESCRIPTOR Peripheral Nervous System Diseases EXPLODE ALL TREES (2963)
-
MESH DESCRIPTOR Somatosensory Disorders EXPLODE ALL TREES (796)
-
((pain* or discomfort*) adj10 (central or complex or nerv* or neuralg* or neuropath*)):TI,AB,KY (3875)
-
((neur* or nerv*) adj6 (compress* or damag*)):TI,AB,KY (721)
-
4 OR 5 OR 6 OR 7 OR 8 (7310)
-
3 AND 9 (151)
Appendix 3. MEDLINE search strategy (via Ovid)
-
Tramadol/ (2637)
-
(tramadol* or tramal* or ultram or zamadol or zydol).mp. (3719)
-
1 or 2 (3719)
-
exp NEURALGIA/ (17673)
-
exp PERIPHERAL NERVOUS SYSTEM DISEASES/ (137699)
-
exp SOMATOSENSORY DISORDERS/ (20383)
-
((pain* or discomfort*) adj10 (central or complex or nerv* or neuralg* or neuropath*)).mp. (49191)
-
((neur* or nerv*) adj6 (compress* or damag*)).mp. (57636)
-
4 or 5 or 6 or 7 or 8 (222483)
-
randomized controlled trial.pt. (469510)
-
randomized.ab. (359272)
-
placebo.ab. (177279)
-
drug therapy.fs. (2035842)
-
randomly.ab. (250055)
-
trial.ab. (379955)
-
groups.ab. (1554754)
-
10 or 11 or 12 or 13 or 14 or 15 or 16 (3875115)
-
3 and 9 and 17 (388)
Appendix 4. Embase search strategy (via Ovid)
-
Tramadol/ (16416)
-
(tramadol* or tramal* or ultram or zamadol or zydol).mp. (16918)
-
1 or 2 (16918)
-
exp neuropathy/ (465954)
-
exp peripheral neuropathy/ (61799)
-
postherpetic neuralgia/ or neuralgia/ or trigeminus neuralgia/ (20978)
-
exp somatosensory disorder/ (82589)
-
((pain* or discomfort*) adj10 (central or complex or nerv* or neuralg* or neuropath*)).mp. (93462)
-
((neur* or nerv*) adj6 (compress* or damag*)).mp. (80148)
-
4 or 5 or 6 or 7 or 8 or 9 (327771)
-
random*.ti,ab. (1153236)
-
factorial*.ti,ab. (29202)
-
(crossover* or cross over* or cross‐over*).ti,ab. (85870)
-
placebo*.ti,ab. (249172)
-
(doubl* adj blind*).ti,ab. (175156)
-
assign*.ti,ab. (302886)
-
allocat*.ti,ab. (111144)
-
Randomized Controlled Trial/ (463655)
-
Double‐blind procedure/ (138148)
-
Crossover Procedure/ (53925)
-
11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 (1623468)
-
3 and 10 and 21 (737)
Appendix 5. Clinical trials registers search strategy
Conditions: neuropathic pain OR neuralgia OR neuropathy OR phantom OR stump
Intervention: tramadol
Limits: Adult and Senior
ClinicalTrials.gov identified 8 studies.
apps.who.int/trialsearch/ identified 3 studies.
Appendix 6. GRADE: criteria for assigning grade of evidence
The GRADE system uses the following criteria for assigning a quality level to a body of evidence (Chapter 12, Schünemann 2011a).
-
High: randomised trials; or double‐upgraded observational studies
-
Moderate: downgraded randomised trials; or upgraded observational studies
-
Low: double‐downgraded randomised trials; or observational studies
-
Very low: triple‐downgraded randomised trials; or downgraded observational studies; or case series/case reports
Factors that may decrease the quality level of a body of evidence are:
-
limitations in the design and implementation of available studies suggesting high likelihood of bias;
-
indirectness of evidence (indirect population, intervention, control, outcomes);
-
unexplained heterogeneity or inconsistency of results (including problems with subgroup analyses);
-
imprecision of results (wide confidence intervals).
-
high probability of publication bias.
Factors that may increase the quality level of a body of evidence are:
-
large magnitude of effect;
-
all plausible confounding would reduce a demonstrated effect or suggest a spurious effect when results show no effect;
-
dose‐response gradient.
Appendix 7. Summary of outcomes in individual studies: efficacy
| Study | Treatment | Pain outcome | Other efficacy outcome |
| Arbaiza 2007 | Tramadol 1 mg/kg bodyweight every 6 h; increased to 1.5 mg/kg every 6 h if relief inadequate, n = 18 | Mean PI at 45 days: | Use of antiepileptic drugs reduced in tramadol group, but not in placebo group |
| Boureau 2003 | Tramadol SR 100 mg taken in evening, n = 64 | ≥ 50% PIR (PP population, LOCF) | Mean PI on day 43 (ITT population, similar for PP population): QoL improved for both groups, but no significant difference |
| Harati 1998 | Tramadol 100 mg to 200 mg daily, titrated from 50 mg daily over maximum 28 days, n = 65 | Mean (SD) PR at end of study (scale ‐1 to 4): Mean PI at end of study (scale 0 to 4): | Subset of participants with severe/extreme pain after washout: |
| Norrbrink 2009 | Tramadol 150 mg to 400 mg daily, n = 23 | PGIC "much improved or very much improved" | Proportion of participants reporting decreased pain intensity larger with tramadol than placebo |
| Sindrup 1999 | Tramadol SR 200 mg to 400 mg daily, titrated over at least one week N = 45 (34 in both periods of cross‐over) | ≥ 50% PIR (participants in both periods) ≥ 30% PIR (participants in both periods) | PI reduced from ≥ 3/10 to < 3/10 by 4th week: |
| Sindrup 2012 | Tramadol SR 200 mg to 400 mg daily, titrated over one week N = 64 (48 completed cross‐over) | PP (completer) population ≥ 50% PIR: PGIC ‐ mean score at end of study: | Full analysis set |
| ADL: activities of daily living; h: hour; ITT: intention to treat; LOCF: last observation carried forward; N: number of participants in study; n: number of participants in treatment arm; PGIC: Patient Global Impression of Change; PI: pain intensity; PIR: pain intensity reduction; PP: per protocol; SD: standard deviation; SR: sustained release. | |||
Appendix 8. Summary of outcomes in individual studies: adverse events, withdrawals
| Study | Treatment | Adverse events | Specific adverse events | Withdrawals |
| Arbaiza 2007 | Tramadol 1 mg/kg bodyweight every 6 h. Increased to 1.5 mg/kg every 6 h if relief inadequate, n = 18 | Any AE: | Events with tramadol: nausea, somnolence, constipation, dry mouth, general malaise, dizziness, tiredness, sweaty hands | All cause: |
| Boureau 2003 | Tramadol SR 100 mg taken in evening, n = 64 | Any AE: | Tramadol: mostly digestive system (11), body as a whole (6), nervous system (6) | AE: (Note: denominators uncertain) |
| Harati 1998 | Tramadol 100 mg to 200 mg daily, titrated from 50 mg daily over maximum 28 days, n = 65 | Participants with any AE not reported | AEs occurring in ≥ 5% reported | All cause: |
| Norrbrink 2009 | Tramadol 150 mg to 400 mg daily, n = 23 | Any AE: | Tiredness: | All cause: All AE, 1 judged unrelated to drug |
| Sindrup 1999 | Tramadol SR 200 mg to 400 mg daily, titrated over at least one week N = 45 (34 in both periods of cross‐over) | Any AE: | Tiredness: | All cause (both periods): LoE: |
| Sindrup 2012 | Tramadol SR 200 mg to 400 mg daily, titrated over one week N = 64 (48 completed cross‐over) | Any AE not reported | Nausea: | All cause: |
| AE: adverse event; hour: h; LoE: lack of efficacy; N: number of participants in study; n: number of participants in treatment arm; SAE: serious adverse event; SR: sustained release. | ||||

Study flow diagram for the updated search

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Forest plot of comparison: 1 Tramadol versus placebo, outcome: 1.1 Participants with ≥ 50% pain intensity reduction.
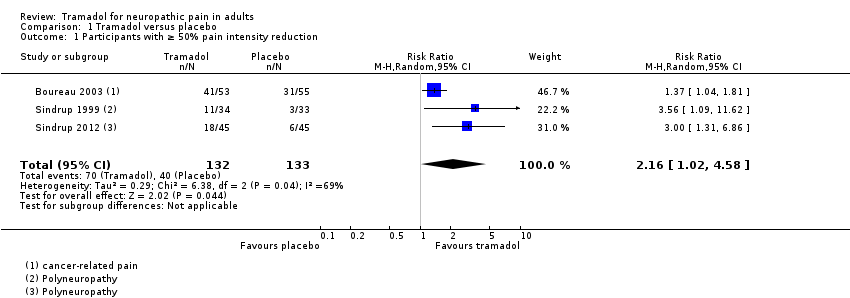
Comparison 1 Tramadol versus placebo, Outcome 1 Participants with ≥ 50% pain intensity reduction.
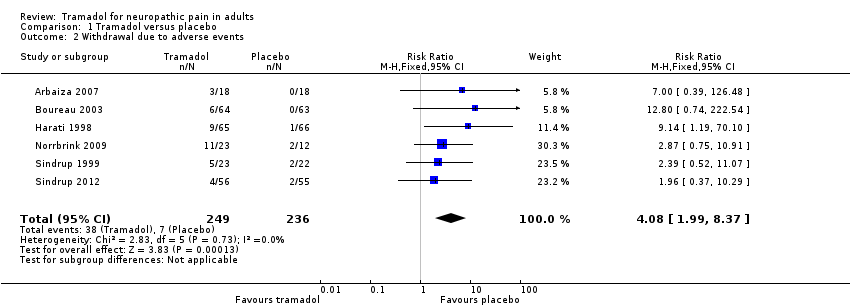
Comparison 1 Tramadol versus placebo, Outcome 2 Withdrawal due to adverse events.
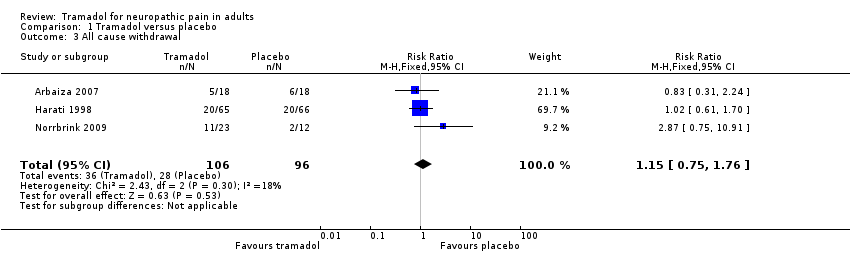
Comparison 1 Tramadol versus placebo, Outcome 3 All cause withdrawal.

Comparison 1 Tramadol versus placebo, Outcome 4 Participants with any adverse event.

Comparison 1 Tramadol versus placebo, Outcome 5 Participants with specific adverse events.
| Tramadol compared with placebo for neuropathic pain | ||||||
| Patient or population: adults with neuropathic pain (any origin) Settings: community Intervention: oral tramadol (typically started at a dose of about 100 mg daily and increased over 1 to 2 weeks to a maximum of 400 mg daily) Comparison: placebo | ||||||
| Outcomes (at trial end) | Probable outcome with | Probable outcome with | Relative effect | No of participants | Quality of the evidence | Comments |
| At least 30% reduction in pain | Not analysed | Not analysed | Not analysed | 157 participants (2 studies) 60 events | Low quality1 | ‐ |
| At least 50% reduction in pain | 530 per 1000 | 300 per 1000 | RR 2.2 (1.02, 4.6) NNT 4.4 (2.9 to 8.8) | 265 participants (3 studies) 110 events | Low quality1 | ‐ |
| PGIC much or very much improved | Not analysed | Not analysed | Not analysed | 35 participants (1 study) 4 events | Very low quality2 | ‐ |
| Withdrawal due to adverse event | 160 per 100 | 30 per 1000 | RR 4.1 (2.0 to 8.4) NNH 8.2 (5.8 to 14) | 485 participants (6 studies) 45 events | Low quality1 | ‐ |
| Participants experiencing any adverse event | 580 per 1000 | 340 per 1000 | RR 1.6 (1.2 to 2.1) NNH 4.2 (2.8 to 8.3) | 266 participants (4 studies) 123 events | Low quality1 | ‐ |
| Serious adverse events | 4 serious adverse events reported in total | Not all studies reported specifically on serious adverse events | Very low quality2 | ‐ | ||
| Death | No data | No data | Not calculated | No data | Very low quality3 | ‐ |
| CI: confidence interval; NNH: number needed to treat for one additional harmful outcome; PGIC: Patient Global Impression of Change; RR: risk ratio | ||||||
| Descriptors for levels of evidence (EPOC 2015): † Substantially different: a large enough difference that it might affect a decision. | ||||||
| 1Downgraded 2 levels due to small number of studies and participants and relatively few events, and several sources of potential bias. | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Participants with ≥ 50% pain intensity reduction Show forest plot | 3 | 265 | Risk Ratio (M‐H, Random, 95% CI) | 2.16 [1.02, 4.58] |
| 2 Withdrawal due to adverse events Show forest plot | 6 | 485 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.08 [1.99, 8.37] |
| 3 All cause withdrawal Show forest plot | 3 | 202 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.15 [0.75, 1.76] |
| 4 Participants with any adverse event Show forest plot | 4 | 266 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.61 [1.22, 2.13] |
| 5 Participants with specific adverse events Show forest plot | 6 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.1 Nausea | 6 | 508 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.62 [2.23, 5.88] |
| 5.2 Constipation | 5 | 381 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.11 [2.36, 7.16] |
| 5.3 Tiredness/fatigue/somnolence | 4 | 345 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.22 [1.93, 5.36] |
| 5.4 Dizziness | 3 | 214 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.72 [1.94, 7.12] |
| 5.5 Dry mouth | 3 | 214 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.44 [1.35, 4.42] |