Duboka poprečna masaža trljanjem za liječenje lateralnog tendinitisa lakta ili koljena
Abstract
Background
Deep transverse friction massage, one of several physical therapy interventions suggested for the management of tendinitis pain, was first demonstrated in the 1930s by Dr James Cyriax, a renowned orthopedic surgeon in England. Its goal is to prevent abnormal fibrous adhesions and abnormal scarring. This is an update of a Cochrane review first published in 2001.
Objectives
To assess the benefits and harms of deep transverse friction massage for treating lateral elbow or lateral knee tendinitis.
Search methods
We searched the following electronic databases: the specialized central registry of the Cochrane Field of Physical and Related Therapies, the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Clinicaltrials.gov, and the Physiotherapy Evidence Database (PEDro), up until July 2014. The reference lists of these trials were consulted for additional studies.
Selection criteria
All randomized controlled trials (RCTs) and controlled clinical trials (CCTs) comparing deep transverse friction massage with control or other active interventions for study participants with two eligible types of tendinitis (ie, extensor carpi radialis tendinitis (lateral elbow tendinitis, tennis elbow or lateral epicondylitis or lateralis epicondylitis humeri) and iliotibial band friction syndrome (lateral knee tendinitis)) were selected. Only studies published in English and French languages were included.
Data collection and analysis
Two review authors independently assessed the studies on the basis of inclusion and exclusion criteria. Results of individual trials were extracted from the included study using extraction forms prepared by two independent review authors before the review was begun. Data were cross‐checked by a third review author. Risk of bias of the included studies was assessed using the "Risk of bias" tool of The Cochrane Collaboration. A pooled analysis was performed using mean difference (MD) for continuous outcomes and risk ratio (RR) for dichotomous outcomes with 95% confidence intervals (CIs).
Main results
Two RCTs (no new additional studies in this update) with 57 participants met the inclusion criteria. These studies demonstrated high risk of performance and detection bias, and the risk of selection, attrition, and reporting bias was unclear.
The first study included 40 participants with lateral elbow tendinitis and compared (1) deep transverse friction massage combined with therapeutic ultrasound and placebo ointment (n = 11) versus therapeutic ultrasound and placebo ointment only (n = 9) and (2) deep transverse friction massage combined with phonophoresis (n = 10) versus phonophoresis only (n = 10). No statistically significant differences were reported within five weeks for mean change in pain on a 0 to 100 visual analog scale (VAS) (MD ‐6.60, 95% CI ‐28.60 to 15.40; 7% absolute improvement), grip strength measured in kilograms of force (MD 0.10, 95% CI ‐0.16 to 0.36) and function on a 0 to 100 VAS (MD ‐1.80, 95% CI ‐0.18.64 to 15.04; 2% improvement), pain‐free function index measured as the number of pain‐free items (MD 1.10, 95% CI ‐1.00 to 3.20) and functional status (RR 3.3, 95% CI 0.4 to 24.3) for deep transverse friction massage, and therapeutic ultrasound and placebo ointment compared with therapeutic ultrasound and placebo ointment only. Likewise for deep transverse friction massage and phonophoresis compared with phonophoresis alone, no statistically significant differences were found for pain (MD ‐1.2, 95% CI ‐20.24 to 17.84; 1% improvement), grip strength (MD ‐0.20, 95% CI ‐0.46 to 0.06) and function (MD 3.70, 95% CI ‐14.13 to 21.53; 4% improvement). In addition, the GRADE (Grades of Recommendation, Assessment, Development and Evaluation) approach was used to evaluate the quality of evidence for the pain outcome, which received a score of "very low". Pain relief of 30% or greater, quality of life, patient global assessment, adverse events, and withdrawals due to adverse events were not assessed or reported.
The second study included 17 participants with iliotibial band friction syndrome (knee tendinitis) and compared deep transverse friction massage with physical therapy intervention versus physical therapy intervention alone, at two weeks. Deep transverse friction massage with physical therapy intervention showed no statistically significant differences in the three measures of pain relief on a 0 to 10 VAS when compared with physical therapy alone: daily pain (MD ‐0.40, 95% CI ‐0.80 to ‐0.00; absolute improvement 4%), pain while running (scale from 0 to 150) (MD ‐3.00, 95% CI ‐11.08 to 5.08), and percentage of maximum pain while running (MD ‐0.10, 95% CI ‐3.97 to 3.77). For the pain outcome, absolute improvement showed a 4% reduction in pain. However, the quality of the body of evidence received a grade of “very low.” Pain relief of 30% or greater, function, quality of life, patient global assessment of success, adverse events, and withdrawals due to adverse events were not assessed or reported.
Authors' conclusions
We do not have sufficient evidence to determine the effects of deep transverse friction on pain, improvement in grip strength, and functional status for patients with lateral elbow tendinitis or knee tendinitis, as no evidence of clinically important benefits was found. The confidence intervals of the estimate of effects overlapped the null value for deep transverse friction massage in combination with physical therapy compared with physical therapy alone in the treatment of lateral elbow tendinitis and knee tendinitis. These conclusions are limited by the small sample size of the included randomized controlled trials. Future trials, utilizing specific methods and adequate sample sizes, are needed before conclusions can be drawn regarding the specific effects of deep transverse friction massage on lateral elbow tendinitis.
PICO
Laički sažetak
Duboka poprečna masaža trljanjem za liječenje upale bočne tetive lakta ili koljena
Istraživačko pitanje
Autori su iznova razmotrili učinke duboke poprečne masaže trljanjem (prema engl. deep transverse friction massage) za liječenje osoba s upalom bočne tetive lakta ili koljena. Pronašli su dvije studije (ovaj obnovljeni sustavni pregled ne sadrži nova istraživanja) s ukupno 57 ispitanika.
Pozadina problema: što je tendinitis i što je duboka masaža trljanjem?
Tetive su vlaknaste strukture koje povezuju mišić s kosti. Tendinitis je upala tetive (bolnooticanje). Upalu uzrokuje preveliko opterećenje tetive nastalo ponavljanjem istih pokreta, što dovodi do boli i ukočenosti u zglobovima poput lakta ili koljena.
Duboka poprečna masaža trljanjem metoda je fizikalne terapije koja se često koristi kako bi se smanjili ozljeda i ožiljci uzrokovani upalom. Ona povećava dotok krvi u zglob, što olakšava zacjeljivanje ozlijeđene tetive tako što povećava opskrbu kisikom.
Obilježja istraživanja
Jedna studija u trajanju od pet tjedana proučavala je učinke duboke poprečne masaže trljanjemu kombinaciji s terapijskim ultrazvukom i placebo masti u usporedbi s terapijskim ultrazvukom i placebo masti u 20 osoba s upalom bočne tetive lakta (teniski lakat), kao i učinke duboke poprečne masaže trljanjem u kombinaciji s fonoforezom (uporaba ultrazvukaza pospješivanje upijanj lokalno primijenjenih lijekova) u usporedbi s fonoforezom u 20 osoba s upalom bočne tetive lakta (teniski lakat). Druga studija, koja je trajala dva tjedna, proučavala je učinke duboke poprečne masaže trljanjem s fizikalnom intervencijskom terapijom u usporedbi s fizikalnom intervencijskom terapijom u 17 ljudi s upalom bočne tetive koljena.
Ključni rezultati
Što se događa kod ljudi s upalom bočne tetive lakta (teniski lakat), koje se liječidubokom poprečnom masažom trljanjem?
• Autori nisu sigurni da se dubokom poprečnom masažom s trljanjem smanjuje bol ipoboljšava funkcija (vrlo niska kvaliteta dokaza).
• Nijedna studija nije opisala kod koliko bolesnika je bol ublažena za 30% ili više, kvalitetuživota, procjenu ukupnog stanja pacijenta, nuspojave i povlačenje nuspojava.
Autori često nemaju precizne podatke o nuspojavama i komplikacijama. To posebno vrijedi za rijetke, ali ozbiljne nuspojave.
Što se događa kod ljudi s upalom bočne tetive koljena, koje se liječi dubokompoprečnom masažom trljanjem?
• Autori nisu sigurni da duboka poprečna masaža trljanjem smanjuje bol (vrlo niska kvaliteta dokaza).
• Nijedna studija nije opisala kod koliko bolesnika je bol ublažena za 30% ili više, kvalitetu života, procjenu ukupnog stanja pacijenta, nuspojave i povlačenje nuspojava.
Autori često nemaju precizne podatke o nuspojavama i komplikacijama. To posebno vrijedi za rijetke, ali ozbiljne nuspojave.
Authors' conclusions
Summary of findings
| Massage + therapeutic ultrasound and placebo ointment compared with ultrasound + placebo ointment only (follow‐up 2 weeks) for treating tendinitis | ||||||
| Patient or population: patients with extensor carpi radialis tendinitis | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | Number of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control (US + placebo ointment only) | Massage + US and placebo ointment | |||||
| Pain Scale from 0 to 100 (lower is better) | Mean change in pain in the control groups was | Mean change in pain in the intervention groups was | 20 | ⊕⊝⊝⊝ | MD = ‐6.60 (‐28.60 to 15.40) Absolute improvement = ‐7% (‐29% to ‐15%) Relative percentage change = 8% (‐24% to 37%) Not statistically significant | |
| Proportion reporting pain relief of 30% or greater not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Function Scale from 0 to 100 (higher is better) | Mean function (vas 0 to 100, 0 = worst) in the control groups was | Mean function (VAS 0‐100, 0 = worst) in the intervention groups was | 20 | ⊕⊝⊝⊝ | MD = ‐1.80 (‐18.64 to 15.04) Absolute improvement = 2% (‐19% to 15%) Relative percentage change = ‐3% (‐28% to 23%) Not statistically significant | |
| Quality of life—not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Patient global assessment of success not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Adverse events not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Withdrawals due to adverse events not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| *The basis for the assumed risk (e.g. median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| aAllocation concealment was unclear. Only assessors were blinded. Baseline imbalance was reported. | ||||||
| Massage + phonophoresis compared with control (phonophoresis only) (follow‐up 2 weeks) for treating tendinitis | ||||||
| Patient or population: patients with extensor carpi radialis tendinitis | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | Number of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control (phonophoresis only) (follow‐up 2 weeks) | Massage + phonophoresis | |||||
| Pain Scale from 0 to 100 (lower is better) | Mean change in pain in the control groups was | Mean change in pain in the intervention groups was | 20 | ⊕⊝⊝⊝ | MD = ‐1.2 (‐20.24 to 17.84) Absolute improvement = ‐1% Relative percentage change = 6% (‐86% to 97%) Not statistically significant | |
| Proportion reporting pain relief of 30% or greater not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Function Scale from 0 to 100 (higher is better) | Mean function in the control groups was | Mean function in the intervention groups was | ‐ | 20 | ⊕⊝⊝⊝ | MD = 3.70 (‐14.13 to 21.53) Absolute improvement = 4% (‐14% to 22%) Relative percentage change = 5% (‐18% to 28%) Not statistically significant |
| Quality of life not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Patient global assessment of success not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Adverse events not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Withdrawals due to adverse events not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| *The basis for the assumed risk (e.g. median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| aAllocation concealment was unclear. Only assessors were blinded. Baseline imbalance was reported. | ||||||
| Deep transverse friction massage + physical therapy compared with physical therapy alone | ||||||
| Patient or population: patients with iliotibial band friction syndrome (knee tendinitis) Settings: community sports injury clinic in South Africa Intervention: deep transverse massage and physical therapy Comparison: physical therapy alone | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | Number of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Deep transverse massage | |||||
| Daily pain Follow‐up mean 2 | Mean daily pain | Mean daily pain in the intervention groups was | 17 | ⊕⊝⊝⊝ | MD = ‐0.4 (‐0.8 to 0) Absolute improvement = ‐4% (‐8% to 0%) Relative percentage change = ‐40% (‐80% to 0%) Not statistically significant | |
| Proportion reporting pain relief of 30% or greater not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Function not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Quality of life not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Patient global assessment not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Adverse events not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Withdrawals due to adverse events | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| *The basis for the assumed risk (e.g. median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| aRandomization and allocation concealment were unclear. Only assessors were blinded. No intention‐to‐treat analysis was done, and baseline imbalance was reported. | ||||||
Background
Description of the condition
Extensor carpi radialis tendinitis (ECRT) (ie, lateral elbow tendinitis, tennis elbow or lateral epicondylitis, or lateralis epicondylitis humeri) is a local inflammation near the proximal (upper) attachments of wrist extensor muscles, characterized by pain on palpation of the lateral epicondyle of the humerus and in resisted movements against wrist extension (Struijs 2002). The prevalence of lateral elbow tendinitis (tennis elbow) varies between 1% and 10% of the population; it commonly occurs between the ages of 34 and 74 years (Allander 1974; Roquelaure 2006; Shiri 2006; Walker‐Bone 2004). Stratford 1989 reported that lateral elbow tendinitis (tennis elbow) does not seem to be a degenerative condition, as its prevalence declines after the age of 42 (Allander 1974). It is a syndrome of overuse (eg, use of computer mouse, racquet sports) that can result in considerable socioeconomic costs resulting from prolonged leave of absence from work (Struijs 2002).
Iliotibial band friction syndrome (ITBFS) (lateral knee tendinitis) is an overuse musculoskeletal injury that causes lateral knee pain and is frequently observed in long distance runners, cyclists, football players, and military personnel. The incidence of lateral knee tendinitis varies between 1.6% and 52%, depending upon the population studied (Jordaan 1994; Kirk 2000; Lavine 2010; Pinshaw 1984; Strauss 2011). The mechanism of lateral knee tendinitis appears to be repetitive friction of the iliotibial band moving over the lateral femoral condyle during knee flexion/extension (Schwellnus 1991). The cause of ITBFS (lateral knee tendinitis) is multifactorial (Messier 1988). Three main risk factors play a large role in the development of lateral knee tendinitis, according to the current literature: (1) biomechanical factors such as muscle imbalance causing maximal braking forces required to control body movements depending on velocity and angle of inclination (Messier 1995), (2) anthropometric factors such as abnormalities in leg and/or feet anatomy (Messier 1988), and (3) training factors such as inadequate warm‐up and cool‐down training (Messier 1988; Messier 1995).
Description of the intervention
Treatment of tendinitis consists of medical, physiotherapeutic, and surgical approaches. The medical approach encompasses rest and the prescription of anti‐inflammatory agents combined with anti‐inflammatory or analgesic medication to control pain and inflammation (Kirk 2000). Goals of the physiotherapeutic approach in the treatment of tendinitis include (1) control of pain and inflammation (Cyriax 1975a; Cyriax 1975b; Thaunton 1987; Wilk 2004); (2) correction of biomechanical deficiencies (Johnson 2007; Thaunton 1987); (3) restoration of motion (Hart 1994); (4) increase in strength, endurance, and function (Hart 1994; Reinold 2002; Thaunton 1987; Wilk 2004); (5) prevention of reinjury (Hart 1994; Reinold 2002); and (6) gradual return to training (Reinold 2002; Thaunton 1987). The surgical approach includes resection of the impinging portion of the extensor carpi radialis brevis tendon release (Grewal 2009) or the iliotibial band (Kirk 2000; Martens 1989).
Deep transverse friction massage (DTFM) is a technique popularized by Dr James Cyriax (Cyriax 1975a; Cyriax 1975b) for relief of pain and inflammation in musculoskeletal conditions. Deep friction is given transverse to the fiber direction of involved tissue, and friction massage must be sufficiently deep to impact the affected structure.
How the intervention might work
Deep transverse friction massage is offered in the treatment of various musculoskeletal conditions. This technique attempts to prevent or destroy abnormal fibrous adhesions (cross‐links or cross‐bridges) by imposing stress transversely to the remodeling collagen of the tissue to soften the adhesion. Thus, DTFM also optimizes the quality of the scar tissue by realigning the collagen of normal soft tissue fibers in a longitudinal way (Walker 1984). It has been indicated that DTFM enhances normal healing conditions and prevents abnormal scarring. Its mechanical action causes hyperemia (ie, an increase in blood flow to the affected area).
Why it is important to do this review
No meta‐analyses or literature reviews have reported the efficacy of this type of massage for lateral elbow or knee tendinitis. Clinicians and patients must be provided with evidence that will enable them to make informed decisions regarding treatment options.
Objectives
To assess the benefits and harms of deep transverse friction massage for treating lateral elbow or lateral knee tendinitis.
Methods
Criteria for considering studies for this review
Types of studies
According to an a priori protocol, randomized controlled trials (RCTs) and controlled clinical trials (CCTs) (and CCTs with pseudorandom methods of allocating participants to treatment) were selected because they are defined as comparative controlled trials with the presence of comparison groups, which allow evaluation of DTFM and patients with tendinitis pain compared with other types of interventions and populations. Only articles published in the English language or the French language were included.
Types of participants
Studies were included if study participants were 18 years of age or older and had been diagnosed with tendinitis (lateral elbow tendinitis and knee tendinitis). Participants had to show no signs of psychiatric conditions and had to demonstrate stable physical and medical status. Mixed populations (individuals with multiple conditions other than tendinitis) were not permitted. Inclusion criteria for lateral elbow tendinitis comprised (1) tenderness on palpation over the lateral aspect of the elbow and (2) pain in the lateral aspect of the elbow during resisted wrist extension. For knee tendinitis, inclusion criteria consisted of (1) history of pain on the lateral aspect of the knee during running, (2) tenderness over the lateral femoral condyle at rest, and (3) aggravation of symptoms at 30 degrees of knee flexion. For the complete list of exclusion criteria and the PICOTS (populations, interventions, comparators, outcomes, timing, and setting) framework, see Table 1.
| Inclusion | Exclusion |
| Participants/Population (P)
| Participants/Population (P)
|
| Interventions (I)
| Interventions (I)
|
| Comparisons (C) Studies were included if they compared an intervention group (eg, deep transverse frictions techniques combined with modalities, exercises) with a comparison group (eg, placebo, no treatment, active treatment such as modalities, exercises) | Comparisons (C) Studies were excluded if they did not compare the intervention group with a comparison group (eg, placebo, no treatment, active treatment such as modalities, exercises) |
| Outcomes (O)
| Outcomes (O)
|
| Period of time (P) Studies were included if the intervention period lasted longer than 1 week or 1 treatment session, with or without a follow‐up period | Period of time (P) Studies were excluded if the intervention period lasted less than 1 week or 1 treatment session |
| Study designs (S)
*English and French articles only. | Study designs (S)
|
BMI: Body mass index.
ESR: Erythrocyte sedimentation rate.
PICOTS: Populations, interventions, comparators, outcomes, timing, and setting framework.
SD: Standard deviation.
Types of interventions
Trials comparing deep transverse friction massage versus no therapy or active treatments (such as therapeutic ultrasound, exercise program, or phonophoresis therapy) were accepted, provided they were given equally to all treatment groups. So trials comparing DTFM combined with other physical therapy manipulative interventions were excluded if co‐interventions were not applied to the control group (ie, if investigators wished to assess the effects of deep massage therapy alone).
Types of outcome measures
Major outcomes
-
Mean (or mean change in) pain.
-
Proportion reporting pain relief of 30% or greater.
-
Function.
-
Quality of life.
-
Patient global assessment of success.
-
Total number of withdrawals due to adverse effects.
-
Number of adverse events.
Minor outcomes
In addition to these outcomes, one of the review authors (LB) has developed a theoretical framework for important outcome measures for physical therapy interventions (Morin 1996). These outcomes were considered as secondary measures of effectiveness and include the following.
-
Joint range of motion (ROM).
-
Muscle strength (and grip strength for tendenitis of upper extremities).
-
Endurance.
Outcomes were assessed at end of treatment or at end of follow‐up.
Search methods for identification of studies
Electronic searches
We searched the specialized register of the Cochrane Field of Physical and Related Therapies, the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Clinicaltrials.gov, and the Physiotherapy Evidence Database (PEDro), until July 2014 (Figure 1). The search included deep transverse friction therapy terms and tendinitis pain terms. Full strategies for these databases are provided in Appendix 1 (MEDLINE), Appendix 2 (EMBASE), Appendix 3 (CENTRAL), Appendix 4 (CINAHL), Appendix 5 (PEDro), and Appendix 6 (Clinicaltrials.gov).
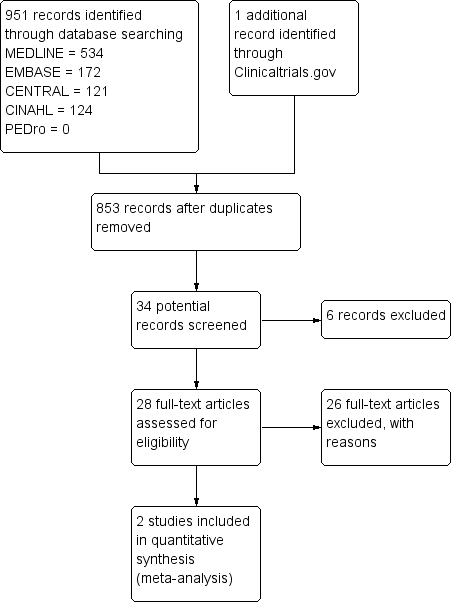
Study flow diagram.
Searching other resources
We searched the reference lists of selected articles.
Data collection and analysis
Selection of studies
Two independent review authors (LB, LML) examined the titles and abstracts of the trials identified by the search strategy to select trials that met the inclusion criteria (see Table 1 for more details). All trials classified as relevant by at least one of the review authors were retrieved as full‐text articles and were assessed for eligibility. Disagreements were resolved by consensus. When selecting studies for inclusion, we did not consider languages other than French and English.
Data extraction and management
The results of the individual trials were extracted from the included study by two independent review authors (LB, LML) using predetermined extraction forms. Data were cross‐checked by a third review author (BS). The extraction forms were developed and pilot‐tested on the basis of other forms used by the Cochrane Musculoskeletal Review Group. The extraction form documented specific information about DTFM, including (1) characteristics of the technique and (2) methods of therapeutic application such as duration, frequency, rhythm, pressure, and total number of sessions. Also, forms were designed to collect information about participant characteristics (eg, age, gender, injury type, injury duration), comparator intervention characteristics, and outcomes (including scale of tool, direction of effect [eg, lower score = worse off]). Final data values were based on consensus of the two review authors. In the event of multiple time points, we would collect the last time point.
Assessment of risk of bias in included studies
Two independent review authors (LB, LML) assessed risk of bias using the "Risk of bias" tool of The Cochrane Collaboration (Higgins 2011); differences were resolved by consensus. This tool assesses seven domains: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and "other issues." For "other issues," we considered baseline imbalance as a potential source of bias. The review authors classified the different items for the two included studies as "high risk," "unclear risk," or "low risk" of bias. A third review author (BS) was consulted when necessary.
Measures of treatment effect
Mean differences (MDs) between experimental and control groups were calculated for continuous data, with the same measurements and standardized mean differences (SMDs) for continuous outcomes with different measurements, and 95% confidence intervals (CIs). For dichotomous data, risk ratios (RRs) and 95% CIs were calculated.
Unit of analysis issues
Individual participants represented the unit of analysis in these studies. No cluster‐randomized controlled trials or cross‐over design trials were selected. In cases of multiple treatment groups, we made multiple pairwise comparisons between all possible pairs of intervention groups to avoid double‐counting of participants in the meta‐analyses.
Dealing with missing data
The procedure was to contact the study authors if only an abstract was provided, or if available results were not sufficient for the data analysis, or to identify additional studies. For this review update, it was not necessary to contact the study authors.
Assessment of heterogeneity
We planned to assess heterogeneity using the I2 statistic when a value of 0% to 40% might "not be important", 30% to 60% may represent "moderate" heterogeneity, 50% to 90% may represent "substantial" heterogeneity, and 75% to 100% represents "considerable" heterogeneity (Higgins 2011).
Assessment of reporting biases
We intended to assess the possibility of publication bias by using funnel plots.
We also planned to assess trial protocols versus published reports. For example, for studies published after July 1, 2005, we would screen the Clinical Trial Register at the International Clinical Trials Registry Platform of the World Health Organization (http://apps.who.int/trialssearch) for the a priori trial protocol. We would evaluate whether selective reporting of outcomes is present (outcome reporting bias).
We planned to compare the fixed‐effect estimate against the random‐effects model to assess the possible presence of small sample bias (ie, in which the intervention effect is more beneficial in smaller studies) in the published literature. In the presence of small sample bias, the random‐effects estimate of the intervention is more beneficial than the fixed‐effect estimate (Higgins 2011).
Data synthesis
We planned to pool the intervention versus a common comparator by using the fixed‐effect model of meta‐analysis if data were homogenous, and the random‐effects model if heterogeneity was substantive (ie, I2 > 50%).
Subgroup analysis and investigation of heterogeneity
No studies were pooled; therefore exploration of heterogeneity and subgroup analyses were not possible.
Sensitivity analysis
We planned sensitivity analyses based on the risk of bias assessment of included studies (allocation concealment, blinding of participants, intention‐to‐treat analysis). However, we could not perform sensitivity analyses for this review.
Grading of the evidence and summary of findings tables
We graded the overall quality of the evidence for each outcome using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach (Guyatt 2008), as recommended by The Cochrane Collaboration (Schünemann 2011a). This approach consists of four levels of quality: high, moderate, low, and very low. Evidence‐based randomized studies start at a high quality rating and could be downgraded on the basis of five factors (study limitations, inconsistency of results, indirectness of evidence, imprecision, and publication bias).
We incorporated grading of evidence into the "Summary of findings" table. We also presented other key results in the "Summary of findings" table, as recommended by The Cochrane Collaboration (Schünemann 2011b), including the absolute and relative magnitude of effect of the interventions examined. Main outcomes in the "Summary of findings" table were mean (or mean change in) pain, proportion reporting pain relief of 30% or greater, function, quality of life, patient global assessment of success, total number of withdrawals due to adverse effects, and number of adverse events.
Results
Description of studies
Results of the search
We retrieved 853 references after deduplication and identified 34 potentially eligible articles through electronic database searches (Figure 1). Two review authors evaluated the studies and screened 28 full‐text articles on deep transverse friction massage and pain of tendinitis for eligibility. Two full‐text articles met our inclusion criteria, and 26 were excluded.
Included studies
Two trials met the inclusion criteria. See the Characteristics of included studies table.
In the first included RCT (Stratford 1989), all participants were 18 years of age or older. Mean participant age was 43.3 years, and symptom duration was 4.25 weeks. This included RCT examined the efficacy of DTFM in the management of extensor carpi radialis tendinitis (lateral elbow tendinitis or tennis elbow) and included the following comparison groups: (1) deep transverse friction massage combined with therapeutic ultrasound and placebo ointment (n = 11) versus therapeutic ultrasound combined with placebo ointment (n = 9) and (2) deep transverse friction massage and phonophoresis (n = 10) versus phonophoresis alone (n = 10). The study consisted of nine treatment sessions within five weeks.
The second RCT (Schwellnus 1992) compared two groups: One received combined physical therapy interventions with DTFM, and the other received combined physical therapy interventions without DTFM. The study consisted of four consecutive treatment sessions in two weeks. A total of 17 participants with iliotibial band friction syndrome (lateral knee tendinitis) were randomly assigned. All participants in this study were prescribed rest, stretching exercises, cryotherapy and therapeutic ultrasound. Mean participant age was 27.6 years, disease duration was 48.5 weeks, years of running experience were 6.6, and the weekly distance in kilometers was 54.5 for both groups. Injury severity was assessed by grading the pain level (ie, grade 1: pain experienced after running; grade 2: pain experienced during running; grade 3: pain experienced during running associated with restriction of distance or velocity; grade 4: severe pain that prevents running). The grade of injury was 3.4 of a maximum possible of 4 for both groups.
Excluded studies
Twenty‐six trials were excluded for the reasons outlined here: (1) healthy participants (Chiarello 1997; Crosman 1984), (2) not tendinitis (Balke 1989; Feehan 1989; Thomee 1997; Zhang 1987), (3) combined modalities (Pellecchia 1994), (4) combination of interventions and co‐interventions not applied to the control group (Baltaci 2001; Bisset 2007; Fernandez 2006; Fernandez 2008; Nagrale 2009; Smidt 2002; Stasinopoulos 2004a; Stasinopoulos 2006; Struijs 2006; Viswas 2012), (5) no control goup (Kohia 2008; Malier 1986; Mayer 2007; Stasinopoulos 2004b; Verhaar 1995), (6) pilot design (Struijs 2003), and (8) not an RCT (Iwatsuki 2001; Joseph 2012; Zheng 2012). See the Characteristics of excluded studies table.
Risk of bias in included studies
We assessed the risk of bias for each included study using the "Risk of bias" tool of The Cochrane Collaboration. The risk of bias graph and summary are presented in Figure 2 and Figure 3, respectively.
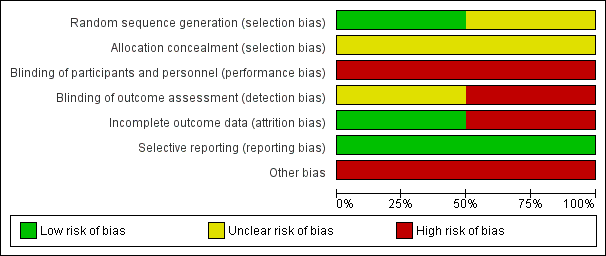
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
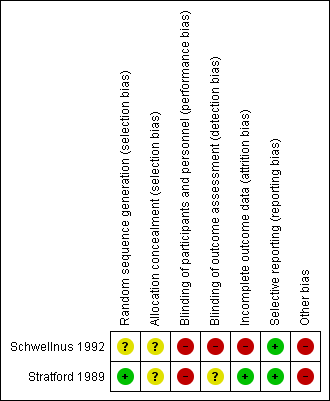
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
In the RCT for extensor carpi radialis tendinitis (lateral elbow tendinitis) (Stratford 1989), the study authors used a 2 × 2 factorial design and created strata on the basis of pain‐free grip strength. Afterward, participants were randomly assigned to one of the four treatment groups using a balanced blocked randomization table. In the second RCT for iliotibial band friction syndrome (lateral knee tendinitis) (Schwellnus 1992), participants were randomly assigned, but the methods of sequence generation and allocation were not described, and so risk was judged as unclear.
Blinding
Participants and personnel were not blinded to treatment. As this is a physical intervention, it is more difficult to blind participants and therapists. Only the outcome assessors were blinded to the treatment groups of participants in both included studies. We did not have enough information to assess the impact on patient‐reported outcomes, but detection bias is more likely "high risk" for self‐reported subjective outcomes (eg, pain).
Incomplete outcome data
One trial (Schwellnus 1992) reported a 15% dropout rate. Duration of follow‐up was mentioned, but investigators did not perform an intention‐to‐treat analysis. In the second trial (Stratford 1989), withdrawals and dropouts were not mentioned. However, all randomly assigned participants were accounted for in the results.
Selective reporting
Both studies reported planned outcomes whether or not findings were significant (Schwellnus 1992; Stratford 1989). No protocols were found.
Other potential sources of bias
Baseline imbalance was noted in both included studies (Schwellnus 1992; Stratford 1989). The duration of symptoms, for example, was different in the intervention group compared with the control group.
Effects of interventions
See: Summary of findings for the main comparison Massage + ultrasound and placebo ointment compared with ultrasound + placebo ointment only for treating lateral elbow tendinitis (tennis elbow); Summary of findings 2 Massage + phonophoresis compared with phonophoresis alone for treating lateral elbow tendinitis (tennis elbow); Summary of findings 3 Deep transverse massage + physical therapy compared with physical therapy alone for treating lateral knee tendinitis
No studies were pooled; therefore assessment of heterogeneity and subgroup analyses were not possible. (See Data and analyses section for additional details.)
Deep transverse friction masssage + therapeutic ultrasound and placebo ointment versus therapeutic ultrasound and placebo ointment
The RCT for extensor carpi radialis tendinitis (tennis elbow) (Stratford 1989) showed no statistically significant differences in pain intensity, grip strength, and functional status after nine consecutive sessions of deep transverse friction massage combined with therapeutic ultrasound and placebo ointment (n = 11) compared with therapeutic ultrasound alone (n = 9). We found the following: mean change in pain on a 0 to 100 visual analog scale (VAS) (MD ‐6.60, 95% CI ‐28.60 to 15.40) (Analysis 1.1), grip strength in kilograms of force (MD 0.10, 95% CI ‐0.16 to 0.36) (Analysis 1.2), function (VAS 0 to 100) (MD ‐1.80, 95% CI ‐18.64 to 15.04) (Analysis 1.3), pain‐free function index measured as the number of pain‐free items (MD 1.10, 95% CI ‐1.00 to 3.20) (Analysis 1.4), and functional status assessed by the physician as the number of successes needed to perform the strengthening program (RR 3.3, 95% CI 0.4 to 24.3) (Analysis 1.5). This difference was not clinically or statistically significant. The quality of the body of evidence was "very low" according to the GRADE approach.
Pain‐free function scores recorded in the two groups at the end of the study were ‐1.8 ± 2.7 for deep transverse friction massage combined with therapeutic ultrasound and placebo ointment and 2.7 ± 2.1 for therapeutic ultrasound and placebo ointment. We found the following values for the other measures, at the end of the study.
-
Pain VAS: 44.8 ± 33.4 for deep transverse friction massage combined with therapeutic ultrasound and placebo ointment and 23.8 ± 17.0 for therapeutic ultrasound alone.
-
Function VAS: 76.3 ± 21.9 for deep transverse friction massage combined with therapeutic ultrasound and placebo ointment and 78.1 ± 16.5 for therapeutic ultrasound alone.
-
Absolute improvement measures demonstrated reduction in pain by 7% and improvement in function by 2%.
-
As a minor outcome, the ratio index of pain‐free grip strength scores was as follows: 0.7 ± 0.3 for deep transverse friction massage combined with therapeutic ultrasound and placebo ointment and 0.6 ± 0.3 for therapeutic ultrasound alone.
-
Quality of life, patient global assessment of success, adverse events, withdrawals due to adverse events, joint range of motion, and endurance were not assessed or reported. (See summary of findings Table for the main comparison.)
Deep transverse friction masssage + phonophoresis versus phonophoresis alone
Mean differences and risk ratios were also calculated for the comparison of deep transverse friction massage and phonophoresis (n = 10) versus phonophoresis alone (n = 10) for pain on a 0 to 100 VAS scale (MD ‐1.2, 95% CI ‐20.24 to 17.84) (Analysis 2.1), grip strength in kilograms of force (MD ‐0.20; 95% CI ‐0.46 to 0.06) (Analysis 2.2), function (VAS 0 to 100) (MD 3.70, 95% CI ‐14.13 to 21.53) (Analysis 2.3), pain‐free function index measured as the number of pain‐free items (MD 0.10, 95% CI ‐2.27 to 2.47) (Analysis 2.4), and functional status assessed by the physician as the number of successes needed to perform the strengthening program (RR 0.67, 95% CI 0.1 to 3.2) (Analysis 2.5) in extensor carpi radialis tendinitis (Stratford 1989). This difference was not clinically or statistically significant. Again, the quality of the body of evidence received a score of "very low" according to the GRADE approach.
The study authors reported different results for the two groups for pain‐free function scores, at the end of the study: 3.7 ± 2.8 for deep transverse friction massage and phonophoresis compared with 3.6 ± 2.6 for phonophoresis alone.
-
Pain VAS: 24.6 ± 20.6 for deep transverse friction massage and phonophoresis compared with 21.8 ± 30.4 for phonophoresis alone.
-
Function VAS: 82.5 ± 16.3 for deep transverse friction massage and phonophoresis compared with 78.8 ± 23.7 for phonophoresis alone.
-
Absolute improvement confirmed reduction in pain by 1% and improvement in function by 4%.
-
As a minor outcome, results for the ratio index of pain‐free grip strength were as follows: 0.5 ± 0.3 for deep transverse friction massage and phonophoresis compared with 0.7 ± 0.3 for phonophoresis alone.
-
Proportion reporting pain relief of 30% or greater, quality of life, patient global assessment of success, adverse events, withdrawals due to adverse events, joint range of motion, and endurance were not assessed or reported. (See summary of findings Table 2.)
Deep transverse friction masssage and physical therapy versus physical therapy alone
Only one small study with 17 participants looked at this comparison in iliotibial band friction syndrome (knee tendinitis) (Schwellnus 1992). Although within‐group reduction in the three types of pain relief measured was significant (overall daily pain, pain while running, and percentage of maximum pain when running) on a 0 to 10 VAS scale, in both treatment groups after two weeks of follow‐up (P value < 0.0005), no statistically significant between‐group differences (mean differences (MDs)) were reported for daily pain (MD ‐0.40, 95% CI ‐0.80 to 0.00), pain while running measured as the total daily pain of all participants while running (scale from 0 to 150) (MD ‐3.00, 95% CI ‐11.08 to 5.08), and percentage of maximum pain while running (MD ‐0.10, 95% CI ‐3.97 to 3.77) (Analysis 3.1). The absolute improvement highlighted a reduction in pain by 4%. It is important to note that the difference in daily pain was significant at P value 0.05 in favor of DTFM, although care in assessing this result must be exercised, as (1) the result is borderline significant and (2) the data are determined from a graph and are subject to interpretation errors. In addition, the quality of the body of evidence according to the GRADE approach received a score of "very low."
-
Mean daily pain scores recorded in the two groups, at the end of the study, were as follows: 0.6 ± 0.3 for the experimental group (combined physiotherapy interventions and DTFM) and 1 ± 0.5 for the control group (physiotherapy interventions only).
-
At the same period, the study authors found different results in the two groups for total pain while running: 20 ± 9 for the experimental group and 23 ± 8 for the control group.
-
Finally, the percentage of maximum pain experienced during running for the two groups was similar at the end of the study: 8 ± 5 for the experimental group and 8.1 ± 3 for the control group.
-
Proportion reporting pain relief of 30% or greater, function, quality of life, patient global assessment of success, number of adverse effects, total number of withdrawals due to adverse effects, joint range of motion, muscle strength, and endurance were not mentioned or reported. (See summary of findings Table 3.)
Discussion
Summary of main results
Evidence was insufficient to demonstrate a consistent clinically important benefit of deep transverse friction massage combined with additional physical therapy modalities when compared with a control in the treatment of extensor carpi radialis tendinitis (lateral elbow tendinitis) (Stratford 1989) and of iliotibial band friction syndrome (knee tendinitis) (Schwellnus 1992). The additional benefit of deep transverse friction massage was not confirmed, as combined interventions were used. The included studies did not report on adverse events.
Overall completeness and applicability of evidence
Only two clinical trials met the inclusion criteria of this review update. Moreover, these two trials were at high risk of bias. Therefore evidence on the specific benefits of deep transverse friction massage is sparse. Further, results of the intervention looking at deep transverse friction massage and physical therapy versus physical therapy alone may not be applicable to general populations, as participants in the trial were experienced runners. The Philadelphia Panel recommends that evidence is insufficient (level 1, grade C for pain) to include or exclude deep transverse friction massage alone as a therapeutic intervention for treating tendinitis (Philadelphia 2001). Evaluation of deep transverse friction massage as a single treatment in comparison with other techniques has not been undertaken, so its efficacy has not yet been demonstrated (Joseph 2012).
Quality of the evidence
For both included RCTs, the two major outcomes (pain and function) received a GRADE score of “very low” for the quality of the body of evidence.
The two RCTs included in this systematic review highlight a common problem among trials of rehabilitation interventions: difficulty or inability to blind participants and personnel, which contributes to the high risk of bias. Although outcome assessors were blinded in both studies, lack of blinding of participants may have an impact on patient‐reported outcomes such as pain, leading to overestimation. Both presented baseline imbalance (mean age and duration of symptoms were different across groups). One of the studies (Schwellnus 1992) demonstrated high risk of incomplete outcome data, as investigators reported a 15% dropout rate, and no intention‐to‐treat analysis was performed. The small sample sizes and wide confidence intervals also contribute to the very low quality rating of the body of evidence for reported outcomes.
Confounding variables such as characteristics of the device, characteristics of the therapeutic application, characteristics of the population, characteristics of the disease, and methodological considerations might have contributed to the lack of effect (Morin 1996). Characteristics of the technique described by Cyriax (Cyriax 1975a; Cyriax 1975b) such as years of experience of the therapist, characteristics of the application (pressure, rhythm and progression, and frequency), duration of treatment sessions and the treatment schedule, characteristics of the population (age, gender), characteristics of the disease (chronic vs acute conditions), and weakness of methodological considerations (comparison groups, sample size, study duration, nonvalidated outcome measures) in both studies (Schwellnus 1992; Stratford 1989) may have contributed to inconclusive results on the effectiveness of deep transverse friction massage for tendinitis. FInally, larger and better powered studies are required to confirm findings because of the small number of studies included in this update of the review and the small sample sizes presented by the included trials.
For both studies, further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. In other words, we obtained very low grades for the main outcomes, principally because of unclear allocation concealment and randomization, single‐blind processes, wide confidence intervals, and small sample size.
Potential biases in the review process
It is important to consider whether all relevant trials were identified (whether or not all pertinent data could be obtained) and if the methods used (search strategy, selection of studies, data collection, analysis) could have introduced potential bias. When selecting studies for inclusion, we did not consider languages other than French and English. This could have limited the number of potentially eligible studies found.
Agreements and disagreements with other studies or reviews
This systematic review of deep transverse friction massage for tendinitis was initially conducted as part of a guideline development project entitled the Philadelphia Panel Guidelines on Rehabilitation Interventions for knee pain (Philadelphia 2001). Other guidelines such as ACR 1996, ACR 2000, Godlee 2000, and Manal 1996 did not evaluate any type of massage as a treatment intervention for knee conditions. To our knowledge, no guidelines on massage for extensor carpi radialis tendinitis are available. The American Physical Therapy Association (APTA) guidelines (APTA 2001) recommend massage for musculoskeletal conditions, although the APTA guidelines do not differentiate between types of massage. However, these guidelines are not based on evidence from comparative controlled trials.
No meta‐analysis or literature reviews have reported the efficacy of this type of massage (Chapman 1991; Furlan 2008; Green 1998; van der Heijden 1997). Evaluation of deep transverse friction massage as a single treatment in comparison with other techniques has not been undertaken, so its efficacy has not been yet demonstrated. Comparison of different studies is difficult to perform because of heterogeneity in terms of (1) types of tendinitis, (2) confounding approaches, and (3) varied outcome measures selected (Joseph 2012).
In the included RCT (Stratford 1989), deep transverse friction massage was performed to reduce symptoms of tendinitis. The inflammation and pain observed in tendinitis are frequently due to three main factors: (1) biomechanical factors), (2) anthropometric factors, and (3) training factors. Pain is an indirect symptom. Based on identified factors, pain could be controlled more effectively through other physical therapy interventions such as strengthening and postural exercises, or changes in functional and sporting activities that correct biomechanical deficiencies (Thaunton 1987), restore motion (Hart 1994), increase strength, endurance, and function (Hart 1994; Thaunton 1987), and permit gradual return to training (Thaunton 1987). One included study (Stratford 1989) found that phonophoresis is not superior to ultrasound and placebo ointment, where similar results were obtained. Antich et al (Antich 1986) mentioned that phonophoresis is as good as ice and ultrasound. Halle and colleagues (Halle 1986) confirmed that ultrasound, transcutaneous electrical nerve stimulation (TENS), and cortisone injections represent comparative therapies in terms of efficacy. The second included RCT (Schwellnus 1992) suggested that the addition of deep transverse friction massage might not appear to aggravate clinical outcomes in iliotibial band friction syndrome (knee tendinitis). Therefore, the included study rejected the findings of the first study author, who examined the biologic rationale of this therapy (Griffin 1963) and reported that the success rate was significantly greater in the phonophoresis group compared with the group given ultrasound therapy. Similar success rates for the phonophoresis groups were shown in the work of Kleinkort et al (Griffin 62% vs Kleinkort 66%) (Stratford 1989). However, it is important to note that those study authors did not consider the presence of potential confounding variables, and neither of them reported their diagnostic criteria and the power of their statistical test (Stratford 1989).
Additional well‐designed RCTs are needed before this specific type of massage can be excluded for treatment of this condition. Clinicians and patients need to be presented with evidence that will enable them to make informed decisions regarding treatment options.

Study flow diagram.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
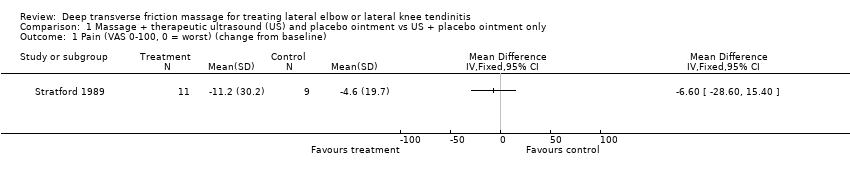
Comparison 1 Massage + therapeutic ultrasound (US) and placebo ointment vs US + placebo ointment only, Outcome 1 Pain (VAS 0‐100, 0 = worst) (change from baseline).

Comparison 1 Massage + therapeutic ultrasound (US) and placebo ointment vs US + placebo ointment only, Outcome 2 Grip strength (ratio index, higher is better).

Comparison 1 Massage + therapeutic ultrasound (US) and placebo ointment vs US + placebo ointment only, Outcome 3 Function (VAS 0‐100, 0 = worst).
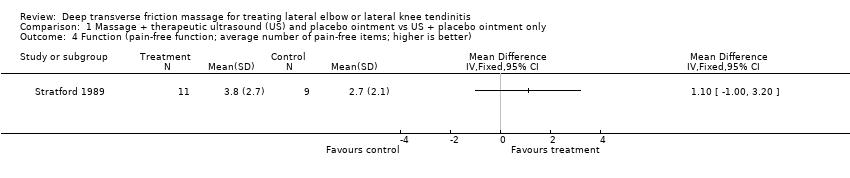
Comparison 1 Massage + therapeutic ultrasound (US) and placebo ointment vs US + placebo ointment only, Outcome 4 Function (pain‐free function; average number of pain‐free items; higher is better).

Comparison 1 Massage + therapeutic ultrasound (US) and placebo ointment vs US + placebo ointment only, Outcome 5 Functional status (number of successes to perform strengthening program).

Comparison 2 Massage + phonophoresis vs phonophoresis only, Outcome 1 Pain (VAS 0‐100, 0 = worst).

Comparison 2 Massage + phonophoresis vs phonophoresis only, Outcome 2 Grip strength (ratio index, higher is better).

Comparison 2 Massage + phonophoresis vs phonophoresis only, Outcome 3 Function (VAS 0‐100, 0 = worst).

Comparison 2 Massage + phonophoresis vs phonophoresis only, Outcome 4 Function (pain‐free function; average number of pain‐free items; higher is better).
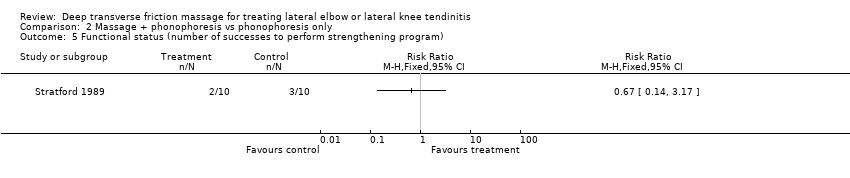
Comparison 2 Massage + phonophoresis vs phonophoresis only, Outcome 5 Functional status (number of successes to perform strengthening program).

Comparison 3 Massage + physical therapy vs physical therapy only, Outcome 1 Pain.
| Massage + therapeutic ultrasound and placebo ointment compared with ultrasound + placebo ointment only (follow‐up 2 weeks) for treating tendinitis | ||||||
| Patient or population: patients with extensor carpi radialis tendinitis | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | Number of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control (US + placebo ointment only) | Massage + US and placebo ointment | |||||
| Pain Scale from 0 to 100 (lower is better) | Mean change in pain in the control groups was | Mean change in pain in the intervention groups was | 20 | ⊕⊝⊝⊝ | MD = ‐6.60 (‐28.60 to 15.40) Absolute improvement = ‐7% (‐29% to ‐15%) Relative percentage change = 8% (‐24% to 37%) Not statistically significant | |
| Proportion reporting pain relief of 30% or greater not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Function Scale from 0 to 100 (higher is better) | Mean function (vas 0 to 100, 0 = worst) in the control groups was | Mean function (VAS 0‐100, 0 = worst) in the intervention groups was | 20 | ⊕⊝⊝⊝ | MD = ‐1.80 (‐18.64 to 15.04) Absolute improvement = 2% (‐19% to 15%) Relative percentage change = ‐3% (‐28% to 23%) Not statistically significant | |
| Quality of life—not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Patient global assessment of success not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Adverse events not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Withdrawals due to adverse events not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| *The basis for the assumed risk (e.g. median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| aAllocation concealment was unclear. Only assessors were blinded. Baseline imbalance was reported. | ||||||
| Massage + phonophoresis compared with control (phonophoresis only) (follow‐up 2 weeks) for treating tendinitis | ||||||
| Patient or population: patients with extensor carpi radialis tendinitis | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | Number of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control (phonophoresis only) (follow‐up 2 weeks) | Massage + phonophoresis | |||||
| Pain Scale from 0 to 100 (lower is better) | Mean change in pain in the control groups was | Mean change in pain in the intervention groups was | 20 | ⊕⊝⊝⊝ | MD = ‐1.2 (‐20.24 to 17.84) Absolute improvement = ‐1% Relative percentage change = 6% (‐86% to 97%) Not statistically significant | |
| Proportion reporting pain relief of 30% or greater not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Function Scale from 0 to 100 (higher is better) | Mean function in the control groups was | Mean function in the intervention groups was | ‐ | 20 | ⊕⊝⊝⊝ | MD = 3.70 (‐14.13 to 21.53) Absolute improvement = 4% (‐14% to 22%) Relative percentage change = 5% (‐18% to 28%) Not statistically significant |
| Quality of life not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Patient global assessment of success not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Adverse events not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Withdrawals due to adverse events not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| *The basis for the assumed risk (e.g. median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| aAllocation concealment was unclear. Only assessors were blinded. Baseline imbalance was reported. | ||||||
| Deep transverse friction massage + physical therapy compared with physical therapy alone | ||||||
| Patient or population: patients with iliotibial band friction syndrome (knee tendinitis) Settings: community sports injury clinic in South Africa Intervention: deep transverse massage and physical therapy Comparison: physical therapy alone | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | Number of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Deep transverse massage | |||||
| Daily pain Follow‐up mean 2 | Mean daily pain | Mean daily pain in the intervention groups was | 17 | ⊕⊝⊝⊝ | MD = ‐0.4 (‐0.8 to 0) Absolute improvement = ‐4% (‐8% to 0%) Relative percentage change = ‐40% (‐80% to 0%) Not statistically significant | |
| Proportion reporting pain relief of 30% or greater not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Function not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Quality of life not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Patient global assessment not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Adverse events not measured | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| Withdrawals due to adverse events | See comment | See comment | Not estimable | ‐ | See comment | Not measured |
| *The basis for the assumed risk (e.g. median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| aRandomization and allocation concealment were unclear. Only assessors were blinded. No intention‐to‐treat analysis was done, and baseline imbalance was reported. | ||||||
| Inclusion | Exclusion |
| Participants/Population (P)
| Participants/Population (P)
|
| Interventions (I)
| Interventions (I)
|
| Comparisons (C) Studies were included if they compared an intervention group (eg, deep transverse frictions techniques combined with modalities, exercises) with a comparison group (eg, placebo, no treatment, active treatment such as modalities, exercises) | Comparisons (C) Studies were excluded if they did not compare the intervention group with a comparison group (eg, placebo, no treatment, active treatment such as modalities, exercises) |
| Outcomes (O)
| Outcomes (O)
|
| Period of time (P) Studies were included if the intervention period lasted longer than 1 week or 1 treatment session, with or without a follow‐up period | Period of time (P) Studies were excluded if the intervention period lasted less than 1 week or 1 treatment session |
| Study designs (S)
*English and French articles only. | Study designs (S)
|
| BMI: Body mass index. | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pain (VAS 0‐100, 0 = worst) (change from baseline) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Grip strength (ratio index, higher is better) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3 Function (VAS 0‐100, 0 = worst) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4 Function (pain‐free function; average number of pain‐free items; higher is better) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5 Functional status (number of successes to perform strengthening program) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pain (VAS 0‐100, 0 = worst) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Grip strength (ratio index, higher is better) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3 Function (VAS 0‐100, 0 = worst) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4 Function (pain‐free function; average number of pain‐free items; higher is better) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5 Functional status (number of successes to perform strengthening program) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pain Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.1 Daily pain | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Pain while running | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 % of maximum pain while running | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |