Laxantes para el tratamiento del estreñimiento en pacientes que reciben cuidados paliativos
Resumen
Antecedentes
Este artículo describe la segunda actualización de una revisión Cochrane sobre la efectividad de los laxantes para el tratamiento del estreñimiento en pacientes que reciben cuidados paliativos. Las versiones anteriores se publicaron en 2006 y 2010, donde también se evaluaron los ensayos de metilnaltrexona. Estos ensayos se han eliminado ya que se incluyen en otra revisión en prensa. En estas versiones anteriores no se establecieron conclusiones sobre la efectividad individual de diferentes laxantes debido al número limitado de evaluaciones. Esta situación ocurre a pesar de que el estreñimiento es frecuente en los cuidados paliativos y genera un sufrimiento considerable debido a los síntomas físicos desagradables y la disponibilidad de una gama amplia de laxantes con diferencias conocidas en cuanto a su efecto en otras poblaciones.
Objetivos
Determinar la efectividad y la eficacia diferencial de los laxantes utilizados para tratar el estreñimiento en pacientes que reciben cuidados paliativos.
Métodos de búsqueda
Se hicieron búsquedas de ensayos en el Registro Cochrane Central de Ensayos Controlados (Cochrane Central Register of Controlled Trials) (CENTRAL; The Cochrane Library), MEDLINE, EMBASE, CINAHL y en Web of Science (SCI & CPCI‐S) hasta septiembre 2014.
Criterios de selección
Ensayos controlados aleatorios (ECA) que evaluaran los laxantes para el estreñimiento en pacientes que reciben cuidados paliativos.
Obtención y análisis de los datos
Dos autores de la revisión evaluaron la calidad de los ensayos y extrajeron los datos. La pertinencia de la combinación de los datos de los estudios dependió de la homogeneidad clínica y de la medida de resultado.
Resultados principales
Se identificaron cinco estudios que incluyeron los laxantes lactulosa, sen, codantrámero, misrakasneham, docusato e hidróxido de magnesio combinado con parafina líquida. En general los resultados de los estudios tuvieron un riesgo incierto de sesgo. Como los cinco estudios compararon diferentes laxantes o combinaciones de laxantes no fue posible realizar un metanálisis. No hubo pruebas sobre si los laxantes individuales fueron más eficaces que otros o causaron menos efectos adversos.
Conclusiones de los autores
Esta segunda actualización encontró que los laxantes tuvieron efectividad similar, pero las pruebas todavía son limitadas debido a que no hay datos suficientes a partir de unos pocos ECA pequeños. Ninguno de los estudios evaluó el polietilenglicol o cualquier intervención administrada por vía rectal. Se necesitan más ensayos para evaluar la efectividad de los laxantes en las poblaciones de cuidados paliativos. Los resultados sobre la efectividad de los laxantes evaluados en otras poblaciones se deben extrapolar con precaución. Lo anterior se debe a las diferencias inherentes en los pacientes que reciben cuidados paliativos que pueden repercutir, probablemente de forma negativa, sobre el efecto del laxante.
PICO
Resumen en términos sencillos
Laxantes para el tratamiento del estreñimiento en pacientes que reciben cuidados paliativos
Antecedentes
Los pacientes con una enfermedad incurable pueden recibir cuidados paliativos que incluyen hacer que el paciente esté tan cómodo como sea posible mediante el control del dolor y de otros síntomas angustiantes. Los pacientes que reciben cuidados paliativos habitualmente presentan estreñimiento. Este hecho es resultado del uso de fármacos (p.ej. morfina) para el control del dolor, y también de factores relacionados con la enfermedad, la dieta y la movilidad. Se dispone de una amplia variedad de laxantes. El objetivo de esta revisión fue determinar lo que se sabe acerca de la efectividad de los laxantes para el tratamiento del estreñimiento en pacientes que reciben cuidados paliativos.
Características de los estudios
Se efectuaron búsquedas en las bases de datos médicas de ensayos clínicos de la administración de laxantes para el estreñimiento en pacientes que reciben cuidados paliativos. Dos autores de la revisión evaluaron la calidad de los estudios y extrajeron los datos.
Resultados clave y calidad de la evidencia
Se identificaron cinco estudios que incluyeron a 370 personas. Los fármacos evaluados fueron: lactulosa, sen, codantrámero combinado con poloxámero, docusato e hidróxido de magnesio combinado con parafina líquida. También se evaluó el Misrakasneham, que es una medicina tradicional india que se utiliza como laxante y contiene aceite de ricino, ghee, leche y 21 tipos de hierbas.
No hubo pruebas sobre qué laxante proporcionó el mejor tratamiento. Sin embargo, la revisión fue limitada ya que las pruebas provinieron solamente de cinco ensayos pequeños y las preferencias de los pacientes y el costo se evaluaron de forma insuficiente. Se necesitan ensayos independientes y rigurosos adicionales para evaluar la efectividad de los laxantes.
Conclusiones de los autores
Antecedentes
Descripción de la afección
Esta es la segunda actualización de una revisión Cochrane publicada por primera vez en 2006 (Miles 2006), y posteriormente en 2010, donde también se evaluaron los ensayos de metilnaltrexona. Estos ensayos se han eliminado ya que se incluyen en otra revisión en prensa (Candy 2011).
Existen muchas definiciones de estreñimiento (Gray 2011). En parte esto refleja diferencias en lo que es normal. Por ejemplo, en las personas sanas el rango de evacuaciones intestinales puede ser de tres veces al día a tres veces a la semana (Thompson 1999). Sin embargo, en general las definiciones de estreñimiento, incluidos los Rome III Criteria (Longstreth 2006), hacen referencia a:
-
evacuación intestinal poco frecuente, difícil o incompleta que puede provocar dolor y malestar;
-
heces que pueden variar desde "rocas" pequeñas y duras, hasta una masa amplia y voluminosa;
-
una sensación de evacuación incompleta.
El estreñimiento puede generar molestias considerables, que incluyen dolor abdominal y distensión, anorexia, náuseas, malestar general y diarrea con rebosamiento por impactación fecal. También puede causar cefaleas, halitosis, inquietud y confusión. Hay consecuencias psicológicas y sociales significativas que pueden contribuir al deterioro de la calidad de vida del paciente. El sufrimiento puede ser tan grave que algunos pacientes con estreñimiento inducido por opiáceos deciden reducir o incluso interrumpir los opiáceos, y de ese modo prefieren experimentar un control inadecuado del dolor en lugar de los síntomas del estreñimiento (Thomas 2008).
Las causas del estreñimiento pueden clasificarse de la siguiente forma:
-
Relacionadas con el estilo de vida, como una dieta baja en fibras y una ingestión deficiente de líquidos. La inactividad física puede producir una reducción de la actividad y de la estimulación de los músculos abdominales dando lugar a un “intestino perezoso” (Winney 1998). En los pacientes tratados en un contexto de asistencia sanitaria, la falta de privacidad o los factores ambientales, o ambos, como tener que utilizar una cuña o una silla con orinal en un área comunal puede inhibir la función intestinal y predisponer al estreñimiento en pacientes que ya están débiles.
-
Las causas mecánicas‐anatómicas relacionadas con la enfermedad, como una fisura anal, colitis, enfermedad diverticular, hemorroides, hernia y rectocele. En los cánceres frecuentes, en particular el cáncer de intestino y ovario, los síntomas digestivos son una complicación frecuente (Droney 2008; Dunlop 1989). También existen consecuencias metabólicas y fisiológicas de diversas afecciones que aumentan la tendencia hacia el estreñimiento, incluida la hipercalcemia paraneoplástica, la hipopotasemia, la obstrucción del flujo venoso con insuficiencia cardíaca derecha y el linfedema intestinal.
-
Inducido por fármacos, pues hay una gama amplia de fármacos que presentan el estreñimiento como un efecto secundario. Estos fármacos incluyen agentes quimioterapéuticos neurotóxicos, antieméticos, anticolinérgicos y diuréticos. Los buenos cuidados paliativos se basan en la necesidad de lograr un control óptimo del dolor; muchos de los fármacos utilizados para lograrlo, como los opiáceos, causan estreñimiento.
El estreñimiento es un problema frecuente en los cuidados paliativos, donde las estimaciones generales de la incidencia varían, según la definición de estreñimiento utilizada, del 18% al 90% de los pacientes (Clark 2012; Laugsand 2009; Sykes 1998). Las causas en esta población suelen ser multifactoriales y están relacionados con una ingesta dietética deficiente, inactividad física, la enfermedad y el tratamiento relacionado. En los pacientes que reciben cuidados paliativos con tratamientos con opiáceos las estimaciones de la incidencia del estreñimiento son incluso mayores: del 72% (Droney 2008) al 87% de las personas (Sykes 1998).
Descripción de la intervención
La prevención y el tratamiento del estreñimiento se relacionan con la causa. Los pacientes que reciben cuidados paliativos están en riesgo de presentar estreñimiento como resultado de los cambios en su estilo de vida. Los mismos son atribuibles a la progresión de la enfermedad y tienen poca probabilidad de resolverse fácilmente. Sin embargo, debido a que en la mayoría de los pacientes que reciben cuidados paliativos es posible que el estreñimiento sea inducido por fármacos, el tratamiento para provocar evacuaciones intestinales satisfactorias habitualmente incluye alguna forma de administración farmacéutica, y la primera línea de tratamiento recomendada generalmente es un laxante (Caraceni 2012; NICE 2012; Scottish Palliative Care Guidelines 2014).
Hay una variedad amplia de laxantes que funcionan al ablandar la materia fecal o mediante la estimulación directa del peristaltismo, o ambos. Los laxantes se clasifican generalmente según su modo de acción: laxantes formadores de masa, laxantes osmóticos, laxantes estimulantes y suavizantes y lubricantes fecales. Los laxantes más utilizados son los preparados estimulantes: entre ellos se encuentran el sen, el bisacodilo, el picosulfato de sodio y el salvado de trigo. En una encuesta en España, el prescrito con más frecuencia fue la lactulosa (Noguera 2010). Los autores indican que se debe a la facilidad de la dosis, el sabor dulce y a que con frecuencia está libremente disponible mediante prescripción y de ese modo exige menor carga económica a la persona.
De qué manera podría funcionar la intervención
Los laxantes funcionan de diversas maneras. Los laxantes formadores de masa incluyen la absorción de grandes cantidades de líquidos. Lo anterior incluye un reflejo de dilatación en la pared intestinal que provoca actividad reflexiva y propulsiva y da lugar a la evacuación intestinal. Este tipo de laxantes no se recomienda generalmente en los pacientes que reciben cuidados paliativos, ya que éstos no pueden mantener una ingestión de líquido adecuada para evitar la obstrucción intestinal o la impactación fecal. Los laxantes osmóticos aumentan el contenido de agua y de ese modo la blandura y el volumen de las heces. Además de la lactulosa, los laxantes osmóticos incluyen polietilenglicol, sorbitol y citrato de magnesio. Los laxantes estimulantes inducen la motilidad propulsiva. Individualmente, dentro de estos grupos de mecanismos de acción, los laxantes funcionan de diferentes maneras.
-
El bisacodilo funciona después de la hidrólisis bacteriana en los intestinos.
-
El picosulfato sódico y el sen solamente después de la hidrólisis en el intestino grueso (colon).
-
La lactulosa se fermenta en el intestino, lo que produce dióxido de carbono e hidrógeno y da lugar a la acidificación de las heces. Debido a la irritación de la pared del colon se promueve el peristaltismo (Droney 2008).
Por qué es importante realizar esta revisión
Los laxantes son un tratamiento aceptado en el estreñimiento. La revisión de la base de pruebas es necesaria para apoyar la administración y para comparar y evaluar los laxantes individuales en cuanto al efecto y los efectos perjudiciales, así como la preferencia de los pacientes y el costo. Las recomendaciones publicadas de prácticas clínicas en los cuidados paliativos han sido informadas por versiones anteriores de esta revisión e incluyen las de la European Palliative Care Association (Caraceni 2012). Es oportuno actualizar esta revisión según la última búsqueda realizada en 2010.
Es importante destacar que hay otras revisiones sobre los laxantes en otras poblaciones que han identificado ensayos múltiples; de renombre es una revisión Cochrane sobre la lactulosa en comparación con polietilenglicol para el estreñimiento crónico (Lee‐Robichaud 2010). Sobre la base de las pruebas de diez ensayos esta revisión concluyó que el polietilenglicol se debe utilizar de preferencia a la lactulosa. Cuando se extrapolan a una población de cuidados paliativos, los resultados se deben analizar con atención ya que provienen de estudios con poblaciones diferentes. Además, es importante evaluar la efectividad de los laxantes en las poblaciones de cuidados paliativos debido a las diferencias inherentes en este grupo que pueden repercutir, probablemente de forma negativa, en el efecto del laxante. En particular, la fisiopatología multifactorial del estreñimiento en los pacientes con enfermedad avanzada. Lo anterior incluye, pero no está limitado a, la repercusión de la progresión de la enfermedad, que ciertas enfermedades terminales tienen un curso rápido, que los pacientes pueden presentar comorbilidades, presentar insuficiencia orgánica múltiple, tener una mayor debilidad, una reducción en la ingesta de líquidos y alimentos y pueden recibir diversos tratamientos que incluyan fármacos múltiples diferentes (Bader 2012; Sanderson 2014). Los pacientes que reciben cuidados paliativos también pueden tener un mayor riesgo que otras poblaciones de experimentar efectos adversos de los laxantes administrados.
Desde mediados de los 2000 se han desarrollado antagonistas mu‐opioides como la metilnaltrexona y se han recomendado como una opción a los laxantes. Generalmente estos fármacos sólo se recomiendan cuando los laxantes tradicionales han fracasado (Caraceni 2012; Scottish Palliative Care Guidelines 2014). Otra revisión Cochrane sobre los antagonistas mu‐opioides en pacientes que reciben cuidados paliativos está en etapa de publicación.
Objetivos
Determinar la efectividad y la eficacia diferencial de los laxantes utilizados para tratar el estreñimiento en pacientes que reciben cuidados paliativos.
Métodos
Criterios de inclusión de estudios para esta revisión
Tipos de estudios
Se incluyeron ensayos controlados con asignación aleatoria (ECA) sobre la eficacia de los laxantes.
No se aplicó restricción de idioma y se permitieron estudios publicados y no publicados.
Tipos de participantes
-
Los estudios elegibles incluyeron adultos que recibían cuidados paliativos y se les administraron laxantes como profilaxis o porque los pacientes presentaban estreñimiento. Estos estudios podían haberse realizado en cualquier ámbito de atención (ambulatorio, hospitalario, atención institucionalizada o en la comunidad).
-
También se incluyeron los estudios en pacientes cuya enfermedad se describió como avanzada o terminal independientemente del ámbito de atención.
-
Se excluyeron los estudios con voluntarios sanos, pacientes con estreñimiento como resultado del consumo de drogas y pacientes con estreñimiento como resultado de una obstrucción intestinal.
Tipos de intervenciones
Todos los laxantes fueron elegibles para su inclusión. Dicha elegibilidad fue independiente de las vías de administración (oral, rectal u otra vía) y de las dosis que se evaluaron en el tratamiento del estreñimiento en los cuidados paliativos por cáncer y otras enfermedades progresivas que limitan la vida. Los laxantes incluyeron, por ejemplo, el sen y la lactulosa. El comparador podría ser placebo, atención habitual u otra intervención activa como un estudio de la comparación entre dos laxantes.
Tipos de medida de resultado
Los estudios reunieron los requisitos cuando las medidas de resultado se informaban en cuanto al alivio del estreñimiento. Las mismas podían incluir:
-
respuesta al laxante, como el cambio en la frecuencia de defecación y la facilidad de la defecación;
-
alivio de los síntomas sistémicos y abdominales relacionados con el estreñimiento, como mejor apetito, reducción del dolor y la distensión abdominal y reducción de la confusión;
-
cambio en la calidad de vida;
-
necesidad de laxantes adicionales, como la administración de laxantes de "rescate" como un supositorio rectal o un enema;
-
aceptabilidad y tolerabilidad que incluyen la preferencia del participante.
También se recopiló información sobre los efectos adversos como:
-
náuseas/vómitos;
-
dolor;
-
flatulencia;
-
diarrea; y
-
incontinencia fecal.
Resultados primarios
-
Respuesta al laxante. La respuesta al laxante se podía medir al informar el tiempo hasta una evacuación intestinal o la frecuencia de tener una evacuación intestinal. Podría ser por la necesidad de administración de un laxante adicional más allá de los que se evaluaron en el ensayo, o medida según si el paciente presentó dificultades o completó la defecación. El tipo de heces evacuadas, como el volumen y la consistencia, también podía ser medido por el Bristol Stool Chart (Lewis 1997).
-
Eventos adversos
Resultados secundarios
-
Preferencia del participante.
-
Alivio de otros síntomas asociados con el estreñimiento como dolor abdominal, náuseas, vómitos y pérdida del apetito.
Métodos de búsqueda para la identificación de los estudios
The aim of the search strategy was to be as comprehensive as possible. We updated our 2014 review search strategy as in earlier versions using three approaches: a literature search for recent reviews, expert consultation and a search of the British National Formulary.
Búsquedas electrónicas
We used both English and American spellings and names. Searches were restricted to human participants. The subject search used a combination of controlled vocabulary and free‐text terms based on a strategy for searching MEDLINE. Appendix 1 details the search strategies used for this current update. We did not seek studies pre‐dating 1966.
For this update, we searched the following databases:
-
Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library), Issue 8 of 12, 2014.
-
MEDLINE (OVID) August 2010 to 9 September 2014.
-
EMBASE (OVID) August 2010 to 9 September 2014.
-
CINAHL (EBSCO) August 2010 to September 2014.
-
Web of Science (SCI & CPCI‐S) 2010 to September 2014.
Previously, for the original review and the first updated version, the following was searched up to 2010 unless otherwise stated:
-
CENTRAL (The Cochrane Library Issue 8, 2010).
-
MEDLINE search from 1966 to January 2005 ‐ (update to August 2010).
-
EMBASE search from 1980 to January 2005 ‐ (update to August 2010).
-
CANCERLIT from 1980 to March 2001.
-
Science Citation Index from 1981 to March 2005.
-
Web of Science March 2005 to August 2010.
-
CINAHL from 1982 to March 2005 (update to August 2010).
-
Databases that provide information on grey literature: SIGLE from 1980 to 2005 (containing British Reports, Translations and Theses), NTIS, DHSS‐DATA and Dissertation Abstracts from 1961 to 2005, and Index to Thesis to October 2010.
-
Conference proceedings from both international and national conferences were handsearched and databases on conference proceedings were accessed ‐ Boston Spa Conferences (containing Index of Conference Proceedings) and Inside Conferences 1996 to 2001, Index to Scientific and Technical Proceedings from 1982 to 2005. In addition, conference proceedings for the European Association of Palliative Care 2007 to 2010 were handsearched.
-
National Health Service National Research Register (containing Medical Research Council Directory) (inception to 2007).
Búsqueda de otros recursos
Reference searching
We searched the MetaRegister of controlled trials (www.controlled‐trials.com/mrct), clinicaltrials.gov (www.clinicaltrials.gov), the World Health Organization (WHO) International Clinical Trials Registry Platform (apps.who.int/trialsearch/) to October 2014. We also searched reference lists and undertook a forward citation check of all included studies. We also searched reference lists from relevant review articles and sought contact with representatives of pharmaceutical companies for further trial evaluations.
Obtención y análisis de los datos
Selección de los estudios
Two review authors (BC/LJ or BC/PL) independently screened citations identified in our searches for eligibility. If it was not possible to accept or reject a study with certainty, we obtained the full text of the study for further evaluation. Two review authors independently assessed studies in accordance with the above inclusion criteria. We resolved any differences in opinion by discussion. We included a PRISMA study flow diagram (Moher 2009), to document the screening process, as recommended in Part 2, Section 11.2.1, of the Cochrane Handbook on Systematic Reviews of Interventions (Higgins 2011).
Extracción y manejo de los datos
We designed a data extraction form specifically for the review. If possible, we obtained the following information for each of the eligible studies:
-
study methods (trial design, duration, allocation method, blinding, setting, study inclusion criteria);
-
participants (number, age, sex, drop‐outs/withdrawals);
-
laxative(s) (type, dose(s), route of delivery, control used);
-
outcome data including laxation response;
-
tolerance and adverse effects.
Evaluación del riesgo de sesgo de los estudios incluidos
Two review authors assessed the quality of included RCTs according to the criteria described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Where differences of opinion existed, we resolved them by consensus with the other review authors. We assessed five main sources of systematic bias for each included study.
-
Randomisation allocation sequence generation.
-
Concealment of allocation sequence.
-
Blinding of participants, personnel and outcome assessors.
-
Level of completeness of outcome data.
-
Selective outcome reporting.
We assessed each domain by whether the criteria for that domain had been met (i.e. low risk of bias), whether they had not (i.e. high risk of bias) or whether it was judged 'unclear' because of insufficient reporting.
Based on these criteria, we categorised a trial as:
-
low risk of bias if all quality criteria met;
-
unclear risk of bias if one or more of the criteria was judged as unclear;
-
high risk of bias if one or more criteria not met.
Medidas del efecto del tratamiento
We report study results organised by type of intervention treatments evaluated.
We measured treatment effects using dichotomous data, an ordinal rating scale or qualitative evidence.
Dichotomous data
Where dichotomous data were reported, we generated odds ratios (ORs) and their 95% confidence intervals (CIs). We also calculated the risk difference (RD), which is the absolute difference in the proportions in each treatment group.
Continuous data
We assessed effects measures for ordinal data as continuous data. We generated the mean difference (MD) for continuous and ordinal data where the data were provided as a mean and standard deviation (SD).
If baseline data were reported pre‐intervention and post‐intervention, we reported means or proportions for both intervention and control groups and calculated the change from baseline. For cross‐over trials, we only generated, as appropriate, an OR or MD for pre‐cross‐over results.
If limitations in the study data prevented reporting an OR, RD or, if continuous data, an MD, we reported the results with caution due to lack of transparency of the evidence.
Qualitative evidence
We planned if there had been any qualitative data reported in the included studies to extract it in consultation with the Cochrane Qualitative Methods Group. Such qualitative data may aim to capture the participant's views on the value of the intervention.
Cuestiones relativas a la unidad de análisis
We planned to seek statistical advice if we had identified trials using a cluster design (in which participants were randomly assigned at group level).
Manejo de los datos faltantes
Given the nature of this field, there was a significant amount of missing data as a result of trial attrition due to the death of the participant.
Where data were not reported we attempted to contact study authors. For studies using continuous outcomes in which SDs were not reported, and no information was available from the authors, we calculated the SDs using the standard error of the mean (SEM).
Evaluación de la heterogeneidad
If meta‐analysis had been possible, we would have assessed statistical heterogeneity between the studies using the Chi2 test and the I2 statistic (we considered a Chi2 P value of less than 0.05 or an I2 value of 50% or more than to indicate substantial heterogeneity).
Evaluación de los sesgos de notificación
We planned to explore publication bias using funnel plots.
Síntesis de los datos
Where study data were of sufficient quality and sufficiently similar (in diagnostic criteria, intervention, outcome measure, length of follow‐up and type of analysis), we planned to combine data in a meta‐analysis to provide a pooled effect estimate. We would have used a fixed‐effect model in the first instance. If there was no statistical heterogeneity, we would have used a random‐effects model to check the robustness of the fixed‐effect model.
Análisis de subgrupos e investigación de la heterogeneidad
If heterogeneity had been identified in a meta‐analysis, we planned to undertake subgroup analysis to investigate its possible sources.
To explore clinical heterogeneity and investigate the effect modification of specific participant characteristics that have been identified in general palliative care populations as effect modifiers, we planned to exclude studies of a higher risk of bias from subgroup analysis.
Análisis de sensibilidad
If sufficient studies were available, we planned to perform, in a meta‐analysis, sensitivity analyses in order to explore the influence of:
-
publication status by excluding unpublished studies;
-
study quality by excluding studies that had a high risk of bias;
-
validated measures of outcome effect by excluding studies that did not use validated measures.
'Summary of findings' tables
We had planned to use the GRADE system to assess the quality of the evidence associated with specific outcomes (e.g. pain reduction, quality of life improvement, adverse effects) (Schünemann 2008), and construct a 'Summary of findings' table using the GRADE software. Although the review authors note that it is possible to create a 'Summary of findings' table despite the lack of meta‐analysis, because the search found of the small cohort of heterogeneous trials comprising of different laxatives and outcomes, we did not construct a 'Summary of findings' table as it would not add any meaning for the reader.
Results
Description of studies
Results of the search
From the searches undertaken for the earlier versions of this review we identified three published trials (Agra 1998; Ramesh 1998; Sykes 1991a). We also identified a fourth relevant, but unpublished, study (Sykes 1991b). We excluded 20 studies that had warranted further consideration. They were mostly excluded as they were evaluating the effect of laxatives in a non‐palliative care population.
The 2014 update search identified 717 unique citations (of MEDLINE, EMBASE, CENTRAL, CINAHL and Web of Science databases) of which one trial was included (Tarumi 2013). We excluded a further study that had warranted further consideration at full text as it was evaluating laxatives in a non‐palliative care population. We also identified two ongoing trials that may fit inclusion criteria when completed (NCT01189409 2014; NCT01416909 2014). In total, we reviewed five RCTs in this update. Figure 1 charts the project progress from screening to inclusion.

Study flow diagram for update search in 2014.
Included studies
The five RCTs analysed 370 participants (Agra 1998; Ramesh 1998; Sykes 1991a; Sykes 1991b; Tarumi 2013). Two studies were of cross‐over design (Sykes 1991a; Sykes 1991b); the others were parallel design. The studies were undertaken in Canadian, British, Spanish and Indian populations. All participants were at an advanced stage of disease and were cared for within a palliative care setting. All participants had a cancer diagnosis, apart from four participants (5% of sample) in one study (Tarumi 2013). The mean age of participants ranged from 61 to 75 years. The laxatives evaluated were all taken orally, they were senna (Agra 1998; Ramesh 1998; Sykes 1991a; Tarumi 2013); lactulose (Agra 1998; Sykes 1991a); co‐danthramer plus poloxamer (Sykes 1991a); magnesium hydroxide plus liquid paraffin (Sykes 1991b), and docusate (Tarumi 2013). One study also evaluated the effect of misrakasneham (Ramesh 1998), a drug used in traditional Indian medicine as a purgative, containing castor oil, ghee, milk and 21 types of herbs. We identified no studies of interventions given rectally.
Study comparisons were mostly between different laxatives, others involved an active control of a placebo plus a common laxative. Two studies used in one or both arms a combination of laxatives; senna plus lactulose (Sykes 1991a; Sykes 1991b), and magnesium hydroxide plus liquid paraffin (Sykes 1991b). Another study used an active control of placebo and senna (Tarumi 2013). All studies measured laxation response and adverse effects. Commonly, laxation response was captured by self report and was assessed at several time points over one or two weeks. Timing of follow‐up was not clear in two studies (Ramesh 1998; Sykes 1991a). None of the studies reported significant baseline differences between the trial arms.
Excluded studies
We excluded 21 studies after assessing full‐text publications, reasons for exclusion included not a trial, outcomes not on laxation or intervention was not a laxative. See table on Characteristics of excluded studies table.
Risk of bias in included studies
All trials under‐reported key design features. Much of the information from the studies was of an unclear risk of bias. See Figure 2 and Figure 3.
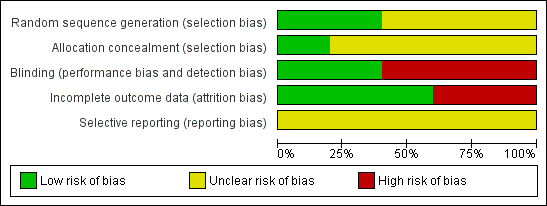
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Two studies described how they generated random allocation (Ramesh 1998; Tarumi 2013), and three studies did not describe how they generated the random allocation to trial arms (Agra 1998; Sykes 1991a; Sykes 1991b). Only one of the studies reported the methods used to conceal random allocation (Tarumi 2013).
Blinding
Owing to differences in the physical characteristics of the intervention laxative and comparison, blinding was not possible in four of the trials, (Agra 1998; Ramesh 1998; Sykes 1991a; Sykes 1991b). Complete details on who was blinded were provided by one study (Tarumi 2013).
Incomplete outcome data
Attrition rates were provided by all studies. Three studies were are a low risk of attrition bias; over three‐quarters of participants completed the studies and the numbers and reasons for dropping out were similar in trial arms (Agra 1998; Ramesh 1998; Tarumi 2013). The other studies were at a higher risk of attrition bias as higher proportions of participants dropped out, 49% in one (Sykes 1991a) and 64% in the other (Sykes 1991b). In these two studies, no participants dropped because of inefficacy and one participant in one trial dropped out because of stomach cramps associated with taking the intervention laxatives of lactulose with senna (Sykes 1991b).
Selective reporting
It is unclear if any of the studies were at risk of reporting bias as there was insufficient information to permit judgement of 'low risk' or 'High risk'.
Other potential sources of bias
The two cross‐over studies did not involve, between the different interventions, a washout period when the participants did not receive any active trial treatment (Sykes 1991a; Sykes 1991b). Washout is intended to prevent continuation of the effects of the trial treatment from one period to another.
Effects of interventions
Co‐danthramer plus poloxamer versus senna plus lactulose
One cross‐over study of 51 participants evaluated the effectiveness of co‐danthramer plus poloxamer versus senna plus lactulose (Sykes 1991a). Both laxatives were in a liquid format. Neither dosage nor details of the data analyses were reported in full. The study analysed laxation response according to opioid use. Table 1 details findings reported.
| Outcome or subgroup | Participants | Effect estimate* |
| Bowel movements in participants receiving strong opioid analgesia (taking ≥ 80 mg) | 17 | "Lactulose plus senna was associated with significantly higher frequency (regardless of which laxative taken first) (P value = < 0.01)" |
| Bowel movements in participants receiving opioid analgesia (< 80 mg) or no opioid analgesia | 21 | "No statistical difference between the trial arms" |
| No bowel movement in treatment week | Unclear | While participants were receiving co‐danthramer plus poloxamer, this occurred 11 times versus once in senna plus lactulose group (P value = 0.01) |
| Suspension of laxative therapy for 24 hours | Unclear | Occurred more frequently with lactulose plus senna (15 cases) than co‐danthramer plus poloxamer (5 cases) (P value = 0.05) |
| Rescue laxatives | Unclear | 14 participants received a rescue laxative only while taking co‐danthramer plus poloxamer but not with senna plus lactulose. 4 participants received rescue laxatives while taking senna plus lactulose but not with co‐danthramer plus poloxamer. 5 participants received rescue laxatives both while taking both trial treatments |
| Participant assessment of bowel function | Unclear | The reported mean change in participant assessment of their bowel function was not significant between drugs at the first week prior to cross‐over or in the week following cross‐over |
| Participant preference | 58 | "While favourable comments about agents effectiveness and flavour were evenly shared, twice as many patients disliked the flavour of co‐danthramer as that of lactulose with senna" |
| Diarrhoea | Unclear | "...diarrhoea resulted in the suspension of laxative therapy occurred more frequently with lactulose and senna compared to co‐danthramer (15 versus 5)" |
| Adverse effects | Unclear | 2 participants reported per‐anal soreness and burning on co‐danthramer plus poloxamer |
| Overall finding | ‐ | Outcomes were mixed on laxation response |
* If data available and appropriate effect estimate was presented as an odds ratio (OR) or a mean difference (MD) with 95% confidence interval (CI). If not available or appropriate then effect was reported as stated in the trial.
Laxation response
The trialists report that the 17 participants receiving 80 mg or more of a strong opioid analgesia (either diamorphine or morphine) "had a significantly higher stool frequency when taking lactulose plus senna than while receiving co‐danthramer, P < 0.01". The study reported no statistical difference for the other participants receiving either a lower dose of opioid or no opioid. For participants' assessments of bowel function, they reported no statistical difference between laxatives.
Need for additional laxatives
Nineteen participants required rescue laxatives in the co‐danthramer plus poloxamer group and nine in the senna plus lactulose group.
Constipation‐associated symptoms
The study did not evaluate constipation‐associated symptoms.
Acceptability and tolerability
Diarrhoea resulted in suspension of laxative therapy for 24 hours for 15 participants while taking senna plus lactulose and for five participants while taking co‐danthramer plus poloxamer. The trialists reported that six instances of diarrhoea occurred at opioid doses of at least 80 mg/day while taking senna plus lactulose and none occurred while taking co‐danthramer plus poloxamer. Two participants reported perianal soreness and burning while taking co‐danthramer plus poloxamer. Participant preference was similar between the trial arms (15 for senna plus lactulose and 14 for co‐danthramer plus poloxamer), although they reported more participants disliked the flavour of co‐danthramer plus poloxamer compared with senna plus lactulose.
Magnesium hydroxide plus liquid paraffin versus senna plus lactulose
One unpublished cross‐over trial involved 118 participants (Sykes 1991b). It evaluated the effectiveness of
-
one week of magnesium hydroxide plus liquid paraffin (mean dose per cross‐over group 45 mL if taken in first week and 49 mL daily if taken in second week), versus
-
one week of senna plus lactulose (mean dose per cross‐over group of 34 mL if taken in the first week and 38 mL daily if taken in the second week).
Forty‐two of the 118 participants completed the trial. Results were not analysed in terms of whether different opioid doses influenced laxative results. Table 2 details findings.
| Magnesium hydroxide plus liquid | Participants | Effect outcome* |
| Laxation response | 35 | "For all patients and for the subgroups who either were or were not receiving strong opioids there was no statistical difference in stool frequency between the two trial treatment groups". At the end of the trial, 19/35 (54%) participants had bowel function they accepted as normal |
| Treatment failure | 29 | 2 participants passed no spontaneous stool with either treatment |
| Loose stools | unclear | There was no significant difference between treatments in the proportion of participants reporting loose stools |
| Rescue laxatives | unclear | "...rectal measures were used on ten occasions during treatment with senna plus lactulose and 23 occasions while magnesium hydroxide plus liquid paraffin was being used" |
| Participant assessment of constipation | 35 | OR 1.10; 95% CI 0.28 to 4.26** |
| Participant assessment of diarrhoea | 35 | OR 0.67; 95% CI 0.10 to 4.58** |
| Participant assessment of normality of bowel function | 35 | OR 1.11; 95% CI 0.29 to 4.21** |
| Participant preference | 32 | 8/32 (magnesium hydroxide plus liquid paraffin) versus 19/32 (senna and lactulose group) |
| Adverse events | Unclear | In both groups, 1 participant found the treatment intolerably nauseating. 1 participant had gripping abdominal pain with lactulose and senna |
| Overall finding | ‐ | No difference in laxation response |
* If data available and appropriate effect estimate was presented as an odds ratio (OR) or a mean difference (MD) with 95% confidence interval (CI). If not available or appropriate then effect was reported as stated in the trial. **Effect outcome used data prior to cross‐over.
Laxation response
No difference was reported in laxation response between the cross‐over groups. The findings did not change by dose of opioid or by the order given in the cross‐over of senna plus lactulose with magnesium hydroxide plus liquid paraffin. They reported that the dosage of magnesium hydroxide plus liquid paraffin required to achieve the same frequency of bowel movements was significantly higher than the dosage required with senna plus lactulose. Using data from the pre‐cross‐over week, there was no significant difference in participants' perception of being constipated, or normality of bowel function. At the end of the trial, 54% of participants considered their bowel movements were normal.
Need for additional laxatives
Participants in both groups required rescue laxatives. They reported that a significantly greater proportion of participants needed rescue laxatives while taking senna plus lactulose compared with magnesium hydroxide plus liquid paraffin.
Constipation‐associated symptoms
The study did not evaluate constipation‐associated symptoms.
Acceptability and tolerability
There was no significant difference between treatments in participants reporting diarrhoea. In both groups, one participant found the treatment intolerably nauseating. One participant, while taking senna plus lactulose, experienced gripping abdominal pain. More participants preferred senna plus lactulose rather than magnesium hydroxide plus liquid paraffin.
Misrakasneham versus senna
One small study of 36 participants evaluated the effectiveness of up to 10 mL of misrakasneham versus senna 24 to 72 mg (both in liquid format) over two weeks (Ramesh 1998). Participants in the trial were taking various doses of morphine but results were not analysed in terms of whether different opioid dose influenced laxative results. Table 3 details the findings.
| Outcome or subgroup | Participants | Effect estimate* |
| Satisfactory bowel movements with no adverse effects | 28 | OR 7.67; 95% CI 0.37 to 158.01 |
| Overall finding | ‐ | No difference in laxation response |
* If data available and appropriate effect estimate was presented as an odds ratio (OR) or a mean difference (MD) with 95% confidence interval (CI). If not available or appropriate then effect was reported as stated in the trial.
Laxation response
There was no statistical difference between the misrakasneham and the senna groups in satisfactory bowel movements (defined as the comfortable feeling that a person experienced after having a free, effortless bowel movement at a frequency acceptable to him or her).
Need for additional laxatives
Six participants required rescue laxatives, five of whom were in the senna group.
Constipation‐associated symptoms
The study did not evaluate constipation‐associated symptoms.
Acceptability and tolerability
Nausea, vomiting and colicky pain were reported by two participants taking misrakasneham. None of the participants withdrew because of inefficiency. Participant preference was split between the groups.
Senna versus lactulose
One study of 75 participants evaluated the effectiveness of lactulose 10 mg to 40 mg versus senna 12 mg to 48 mg (both laxatives were in liquid format) over four weeks (Agra 1998). Doses of the laxatives were increased according to clinical response; the study authors do not provide details on mean doses. Results were not analysed in terms of whether different opioid doses influenced laxative results. Table 4 details the findings.
| Outcome or subgroup | Participants | Effect estimate* |
| Mean number of defecation days | 75 | MD ‐0.10; 95% CI ‐0.60 to 0.40 |
| Defecation‐free days | 75 | MD 0.00; 95% CI ‐0.48 to 0.48 |
| General state of health | 75 | MD ‐0.10; 95% CI ‐0.31 to 0.11 |
| Overall finding | ‐ | No difference in laxation response |
* If data available and appropriate effect estimate was presented as an odds ratio (OR) or a mean difference (MD) with 95% confidence interval (CI). If not available or appropriate then effect was reported as stated in the trial.
Laxation response
There was no statistical difference between the senna and the lactulose groups in laxation response, in defecation‐free periods and in the mean number of defecation days (senna: mean 8.9 days, SD 6.6; lactulose: mean 10.6 days, SD 7.3).
Need for additional laxatives
Thirty‐seven per cent of participants completing the study required combined lactulose and senna to relieve constipation.
Constipation‐associated symptoms
There was no statistical difference in the general state of health of the participants between the trial arms.
Acceptability and tolerability
An equal number of participants, three per trial group, reported diarrhoea, vomiting and cramps. There was no significant difference in the number of participants who dropped out between the trial arms. Participant preference was not evaluated.
Docusate plus senna versus placebo plus senna
One study of 74 participants evaluated docusate plus senna (sennosides) versus an active control of placebo plus senna over 10 days (Tarumi 2013). Details of the data analyses were not reported in full. Results were not analysed in terms of whether different opioid doses influenced laxative results. Table 5 details the findings.
| Outcome or subgroup | Participants | Effect estimate* |
| Stool frequency | 56 | No statistically significant difference in the overall mean number of bowel movements per day between the docusate plus senna (x statistic = 0.74 (SD 0.47) and placebo plus senna groups (x statistic = 0.69, SD 0.37) (P value = 0.58) |
| Bowel movement on ≥ 50% of days | 56 | OR 0.52; 95% CI 0.17 to 1.57 |
| Stool volume | 56 | Trialists reported no significant difference between trial arms in stool volume (P value = 0.06) |
| Stool consistency | 56 | Using the Bristol Stool Form Scale, more participants in the placebo plus senna group had Type 4 (smooth and soft) and Type 5 (soft blobs). In the docusate plus senna group, more participants had Type 3 (sausage, cracks in surface) and Type 6 (mushy stool) (P value = 0.01) |
| Participants' perceptions of the difficulty and completeness of defecation | 56 | No differences in reported difficulty in evacuation (13/40 in the docusate group versus 14/56 in the placebo group; OR 1.44; 95% CI 0.59 to 3.54). No difference in sense of completeness of evacuation (25/34 in the docustate plus senna group versus 44/56 in the placebo plus senna group ; OR 0.76; 95% CI 0.28 to 2.05) |
| Overall finding | ‐ | No difference in laxation response |
* If data available and appropriate effect estimate is presented as an odds ratio (OR) or a mean difference (MD). If not available or appropriate then effect is reported as stated in the trial. SD: standard deviation.
Laxation response
The study reported no statistical difference in laxation between docusate plus senna and placebo plus senna. This was in volume, difficulty and completeness of defecation, and having a bowel movement on 50% of the study days (where for instance the OR was 0.52 (95% CI 0.17 to 1.57)). Using the Bristol Stool chart, there was a significant difference (P value = 0.001) in stool consistency between the trial arms; with more participants in the placebo plus senna group having Type 4 (smooth and soft) or Type 5 (soft blobs) stools, and more participants in the docusate plus senna group having Type 3 (sausage like) or Type 6 (mushy) stools.
Need for additional laxatives
At least one type of additional laxative was given to 74% of participants in the placebo plus senna group and 68.6% of participants in the docusate plus senna group. The difference was not significant (P value = 0.77).
Constipation‐associated symptoms
The study measured symptoms, such as shortness of breath and drowsiness, using the Edmonton Symptom Assessment System. They report no significant difference between the trial arms.
Acceptability and tolerability
Twenty‐five participants in the docusate plus senna group and eight in the placebo plus senna group dropped out; reasons for attrition were not related to the treatments. Adverse effects were not reported. Preference was not measured.
Discusión
Resumen de los resultados principales
Esta revisión es la segunda actualización de una revisión Cochrane sobre la efectividad de los laxantes para el tratamiento del estreñimiento en pacientes que reciben cuidados paliativos. Las versiones anteriores se publicaron en 2006 y 2010, donde también se evaluaron los ensayos de metilnaltrexona. Estos ensayos se han eliminado ya que se incluyen en otra revisión en prensa. La revisión actual intentó determinar la efectividad de la administración de los laxantes para el tratamiento del estreñimiento en pacientes que reciben cuidados paliativos. Se incluyeron cinco estudios, cuatro de los cuales fueron identificados en la revisión anterior. Los estudios compararon la efectividad de dos laxantes diferentes o compararon el laxante con un control activo.
No se demostraron diferencias en la efectividad en:
-
lactulosa comparada con sen;
-
sen más lactulosa comparados con hidróxido de magnesio más parafina líquida;
-
misrakasneham comparado con sen;
-
docusato más sen comparados con placebo más sen.
En un estudio hubo resultados mixtos sobre sen más lactulosa comparados con codantrámero más poloxámero (Sykes 1991a). Hubo una diferencia significativa (valor de p < 0,01) en el subgrupo de 17 participantes que recibieron analgesia con opiáceos fuertes que favoreció al sen más lactulosa en comparación con codantrámero más poloxámero en la frecuencia de las deposiciones, y en general los participantes tomaron menos fármacos de rescate (9/51 en el grupo de sen más lactulosa en comparación con 19/51 en el grupo de codantrámero más poloxámero). Sin embargo, no hubo diferencias entre los laxantes en la evaluación general de los participantes sobre la función intestinal.
Cuatro estudios informaron que algunos participantes (uno a tres) experimentaron efectos adversos. Los efectos adversos más comunes fueron náuseas, vómitos, diarrea y dolor abdominal. En el estudio que comparó lactulosa más sen con hidróxido de magnesio más parafina líquida, un participante de cada grupo abandonó el estudio debido a náuseas intolerables y dolor abdominal punzante.
Las preferencias de los participantes se informaron en dos estudios. Un estudio mostró una preferencia por el sen más lactulosa sobre el hidróxido de magnesio más parafina líquida (Sykes 1991b). El otro estudio no encontró diferencias en la preferencia entre misrakasneham y sen (Ramesh 1998).
En todos los estudios incluidos, varios participantes continuaron con estreñimiento y se les administraron laxantes de rescate. Ninguno de los estudios exploró las diferencias entre los pacientes que respondieron al tratamiento y los que no respondieron en cuanto a las características al seguimiento, como la evolución de la enfermedad o la administración de fármacos (en particular los opiáceos).
Compleción y aplicabilidad general de las pruebas
Los hallazgos de nuestra revisión son limitados. Los estudios fueron pocos y en general tuvieron riesgo incierto de resultados sesgados. Los estudios incluyeron tamaños de la muestra pequeños y los dos ensayos cruzados (crossover) no incluyeron un período de lavado entre la prueba del efecto de los diferentes tratamientos. Hubo una superposición limitada con respecto a qué lactante se evaluó, lo que impidió que los resultados se combinaran en un análisis. La preferencia de los participantes se exploró de forma inadecuada. Sólo se ha completado un nuevo ensayo desde la última búsqueda en 2010. Sin embargo, quizás haya poco incentivo para las compañías farmacéuticas para patrocinar evaluaciones en los tratamientos establecidos como los laxantes y en el grupo relativamente pequeño de pacientes con cuidados paliativos (Bader 2012). Los laxantes se utilizan ampliamente en este grupo de pacientes, pero todavía se conoce poco acerca de las diferencias en el efecto y los eventos adversos entre los laxantes disponibles. No se sabe si algunos laxantes pueden ser más apropiados en ciertos pacientes que reciben cuidados paliativos que en otros pacientes.
Calidad de la evidencia
Hubo problemas en la calidad de las pruebas. Los tamaños de la muestra de la mayoría de los estudios (cuatro de cinco) probablemente tuvieron poco poder estadístico para encontrar un efecto cierto, ya que incluyeron menos de 100 participantes. Los estudios también tuvieron algunas limitaciones metodológicas; en tres estudios, el doble ciego no fue posible debido a que los medicamentos difirieron en su presentación (Ramesh 1998; Sykes 1991a; Sykes 1991b); en dos estudios, hubo una alta tasa de desgaste de más del 50% (Sykes 1991a; Sykes 1991b). Sin embargo, debido a que era una población de cuidados paliativos, una deserción de esta magnitud no es extraña.
Sesgos potenciales en el proceso de revisión
La inclusión se limitó a los estudios que especificaron que los participantes recibían cuidados paliativos o presentaban un estadio avanzado de la enfermedad. Es probable que lo anterior haya dado lugar a la pérdida de datos, ya que algunos estudios excluidos podrían haber incluido pacientes con enfermedad avanzada pero los autores no aportaron detalles sobre el estadio de la enfermedad.
Acuerdos y desacuerdos con otros estudios o revisiones
Hay una revisión Cochrane más grande sobre laxantes que está relacionada con la población adulta en general Dicha revisión tuvo como objetivo determinar cuál, si la lactulosa o el polietilenglicol, es más eficaz para tratar el estreñimiento crónico y la impactación fecal. Los autores pudieron combinar los resultados de algunos de los diez ensayos elegibles en diversos metanálisis. Encontraron que el polietilenglicol fue mejor que la lactulosa en los resultados de la frecuencia y la forma de las deposiciones, así como en la necesidad de laxantes de rescate.
No se identificaron ensayos de polietilenglicol en pacientes que reciben cuidados paliativos. Los resultados de las revisiones en poblaciones de atención no paliativa son informativos. Sin embargo, es importante evaluar los laxantes en las poblaciones de cuidados paliativos debido a las diferencias inherentes en este grupo que repercutirán, probablemente de forma negativa, sobre el efecto del laxante. En particular, los pacientes que reciben cuidados paliativos pueden diferir de otras poblaciones en cuanto a la fisiopatología multifactorial del estreñimiento, el curso rápido de la enfermedad, la presencia de insuficiencia orgánica múltiple, mayor debilidad, reducción en la ingesta de alimentos y tasas mayores de polimedicación. Los pacientes que reciben cuidados paliativos también pueden tener un mayor riesgo de efectos adversos (Bader 2012).
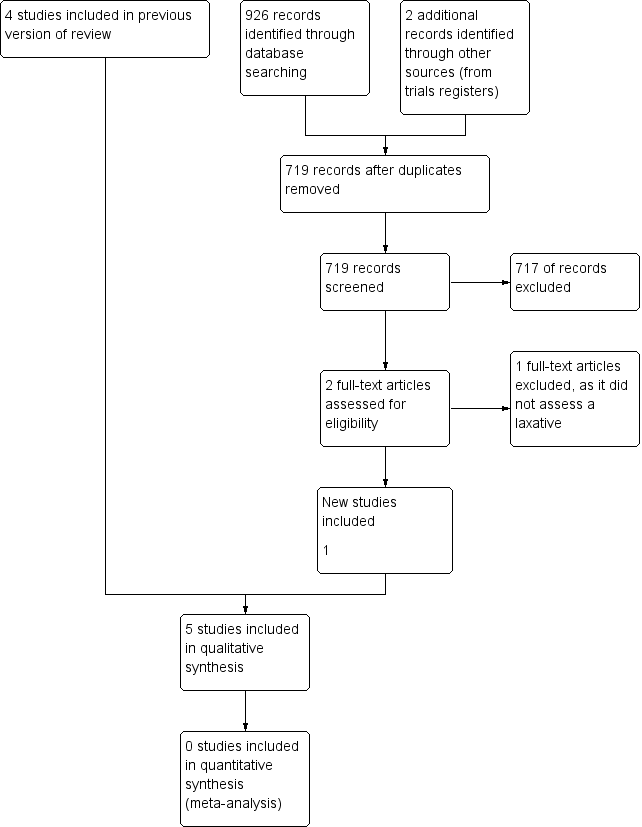
Study flow diagram for update search in 2014.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
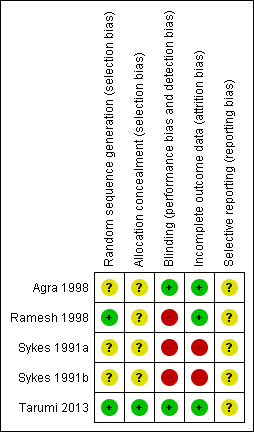
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
| Outcome or subgroup | Participants | Effect estimate* |
| Bowel movements in participants receiving strong opioid analgesia (taking ≥ 80 mg) | 17 | "Lactulose plus senna was associated with significantly higher frequency (regardless of which laxative taken first) (P value = < 0.01)" |
| Bowel movements in participants receiving opioid analgesia (< 80 mg) or no opioid analgesia | 21 | "No statistical difference between the trial arms" |
| No bowel movement in treatment week | Unclear | While participants were receiving co‐danthramer plus poloxamer, this occurred 11 times versus once in senna plus lactulose group (P value = 0.01) |
| Suspension of laxative therapy for 24 hours | Unclear | Occurred more frequently with lactulose plus senna (15 cases) than co‐danthramer plus poloxamer (5 cases) (P value = 0.05) |
| Rescue laxatives | Unclear | 14 participants received a rescue laxative only while taking co‐danthramer plus poloxamer but not with senna plus lactulose. 4 participants received rescue laxatives while taking senna plus lactulose but not with co‐danthramer plus poloxamer. 5 participants received rescue laxatives both while taking both trial treatments |
| Participant assessment of bowel function | Unclear | The reported mean change in participant assessment of their bowel function was not significant between drugs at the first week prior to cross‐over or in the week following cross‐over |
| Participant preference | 58 | "While favourable comments about agents effectiveness and flavour were evenly shared, twice as many patients disliked the flavour of co‐danthramer as that of lactulose with senna" |
| Diarrhoea | Unclear | "...diarrhoea resulted in the suspension of laxative therapy occurred more frequently with lactulose and senna compared to co‐danthramer (15 versus 5)" |
| Adverse effects | Unclear | 2 participants reported per‐anal soreness and burning on co‐danthramer plus poloxamer |
| Overall finding | ‐ | Outcomes were mixed on laxation response |
| * If data available and appropriate effect estimate was presented as an odds ratio (OR) or a mean difference (MD) with 95% confidence interval (CI). If not available or appropriate then effect was reported as stated in the trial. | ||
| Magnesium hydroxide plus liquid | Participants | Effect outcome* |
| Laxation response | 35 | "For all patients and for the subgroups who either were or were not receiving strong opioids there was no statistical difference in stool frequency between the two trial treatment groups". At the end of the trial, 19/35 (54%) participants had bowel function they accepted as normal |
| Treatment failure | 29 | 2 participants passed no spontaneous stool with either treatment |
| Loose stools | unclear | There was no significant difference between treatments in the proportion of participants reporting loose stools |
| Rescue laxatives | unclear | "...rectal measures were used on ten occasions during treatment with senna plus lactulose and 23 occasions while magnesium hydroxide plus liquid paraffin was being used" |
| Participant assessment of constipation | 35 | OR 1.10; 95% CI 0.28 to 4.26** |
| Participant assessment of diarrhoea | 35 | OR 0.67; 95% CI 0.10 to 4.58** |
| Participant assessment of normality of bowel function | 35 | OR 1.11; 95% CI 0.29 to 4.21** |
| Participant preference | 32 | 8/32 (magnesium hydroxide plus liquid paraffin) versus 19/32 (senna and lactulose group) |
| Adverse events | Unclear | In both groups, 1 participant found the treatment intolerably nauseating. 1 participant had gripping abdominal pain with lactulose and senna |
| Overall finding | ‐ | No difference in laxation response |
| * If data available and appropriate effect estimate was presented as an odds ratio (OR) or a mean difference (MD) with 95% confidence interval (CI). If not available or appropriate then effect was reported as stated in the trial. **Effect outcome used data prior to cross‐over. | ||
| Outcome or subgroup | Participants | Effect estimate* |
| Satisfactory bowel movements with no adverse effects | 28 | OR 7.67; 95% CI 0.37 to 158.01 |
| Overall finding | ‐ | No difference in laxation response |
| * If data available and appropriate effect estimate was presented as an odds ratio (OR) or a mean difference (MD) with 95% confidence interval (CI). If not available or appropriate then effect was reported as stated in the trial. | ||
| Outcome or subgroup | Participants | Effect estimate* |
| Mean number of defecation days | 75 | MD ‐0.10; 95% CI ‐0.60 to 0.40 |
| Defecation‐free days | 75 | MD 0.00; 95% CI ‐0.48 to 0.48 |
| General state of health | 75 | MD ‐0.10; 95% CI ‐0.31 to 0.11 |
| Overall finding | ‐ | No difference in laxation response |
| * If data available and appropriate effect estimate was presented as an odds ratio (OR) or a mean difference (MD) with 95% confidence interval (CI). If not available or appropriate then effect was reported as stated in the trial. | ||
| Outcome or subgroup | Participants | Effect estimate* |
| Stool frequency | 56 | No statistically significant difference in the overall mean number of bowel movements per day between the docusate plus senna (x statistic = 0.74 (SD 0.47) and placebo plus senna groups (x statistic = 0.69, SD 0.37) (P value = 0.58) |
| Bowel movement on ≥ 50% of days | 56 | OR 0.52; 95% CI 0.17 to 1.57 |
| Stool volume | 56 | Trialists reported no significant difference between trial arms in stool volume (P value = 0.06) |
| Stool consistency | 56 | Using the Bristol Stool Form Scale, more participants in the placebo plus senna group had Type 4 (smooth and soft) and Type 5 (soft blobs). In the docusate plus senna group, more participants had Type 3 (sausage, cracks in surface) and Type 6 (mushy stool) (P value = 0.01) |
| Participants' perceptions of the difficulty and completeness of defecation | 56 | No differences in reported difficulty in evacuation (13/40 in the docusate group versus 14/56 in the placebo group; OR 1.44; 95% CI 0.59 to 3.54). No difference in sense of completeness of evacuation (25/34 in the docustate plus senna group versus 44/56 in the placebo plus senna group ; OR 0.76; 95% CI 0.28 to 2.05) |
| Overall finding | ‐ | No difference in laxation response |
| * If data available and appropriate effect estimate is presented as an odds ratio (OR) or a mean difference (MD). If not available or appropriate then effect is reported as stated in the trial. SD: standard deviation. | ||