Универсальная (на базе школ) профилактика незаконного употребления наркотиков
Referencias
References to studies included in this review
References to studies excluded from this review
References to studies awaiting assessment
References to ongoing studies
Additional references
References to other published versions of this review
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods | RCT | |
| Participants | 1360 6th‐grade students enrolled from 2 southern New England towns, USA. Academic years 1980 to 1981, 1981 to 1982 | |
| Interventions | Experimental: ADM (Adolescent Decision‐Making) is a cognitive‐behavioural skills intervention to familiarise students with the basic concepts of effective decision‐making, to promote role flexibility, to increase students' abilities to recognise and manage peer pressure, and to enhance students' ability to turn to others for information and support when faced with decisions Social competence approach Deliverer: not reported n = 680 Modality: not reported N of sessions: 12 sessions during 6th grade Booster: no Duration of the intervention: 3 months Control: type of intervention not reported, n = 680 | |
| Outcomes | Improvement of decision‐making processes Tobacco, alcohol, marijuana, hard drugs use | |
| Notes | Outcome assessed at post‐test (at the end of the intervention) and at 24 months (at 8th grade) after the end of the intervention. Analysis sample at 24 months follow‐up = 1075 (79% of the original sample), intervention group n = 545, control group n = 530 Attrition: 8.9% at post‐test Data suitable for inclusion in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "at a first step in randomisation, schools were grouped into homogeneous clusters based on socioeconomic status and ethnic composition; classrooms were then randomly divided into Program and Control group" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | There were no significant differences in attrition rate between groups; logistic regression revealed an interaction for alcohol at baseline (control drop‐outs were more likely to use alcohol at baseline than control 'stayers'); no interaction was found for tobacco, marijuana or hard drugs |
| Similarity of groups at baseline | Unclear risk | Information not reported |
| Blinding of outcome assessment (detection bias) | Low risk | Questionnaires had code number but no name of the students. Trained raters scored coded questionnaires without knowledge of group assignment |
| Methods | Cluster‐RCT | |
| Participants | 6527 7th to 8th grade students enrolled from 30 junior high schools in California and Oregon (USA), 1984 to 1990 school years. 3912 students completed baseline survey | |
| Interventions | Experimental: project ALERT, targeting alcohol, cigarettes and marijuana use, seeking to motivate the students to resist pro‐drug influences and to give them the skills to do so Social influence approach. n = not reported (20 schools): Group 1: adult health educator alone led n = not reported Group 2: adult health educator led, teen assisted n = not reported Deliverer: Group 1 taught by an adult health educator alone Interactive modality N of sessions: 8 lessons in 7th grade and 3 in the booster session the following year Booster: yes Duration of the intervention: overall over 2 school years, n of months not reported Control: usual curricula, n: not reported | |
| Outcomes | Use of alcohol, cigarettes and marijuana, measured by a questionnaire administered before and after delivery of 7th grade curriculum (baseline and 3 months later), before and after 8th grade booster lessons (12 and 15 months after baseline). Beliefs about consequences of using substances, perceptions about use in peers, resistance self efficacy, expectations of use in next 6 months | |
| Notes | Outcome assessed at post‐test and at 3 months follow‐up after the end of the intervention Analysis sample n = 3916, n intervention group not reported, n control group not reported No data suitable for inclusion in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "blocked randomisation by district, assignment restriction to a subset that produced little unbalance among experimental conditions in school test score, language spoken at home and drug use"; unit of randomisation: schools |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | Quote: "we found no evidence that either attrition rates or which students were lost from the analysis varied across experimental conditions" |
| Similarity of groups at baseline | Low risk | Regression methods were used at the analysis stage to adjust for chance differences among the groups |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | Cluster‐RCT | |
| Participants | 5412 7th grade students enrolled from 55 middle schools in South Dakota (USA), 1997 to 1999 school years | |
| Interventions | Experimental: project ALERT (revised), targeting alcohol, cigarettes and marijuana use, seeking to change student's beliefs about drug norms and consequences, and to help them to identify and resist pro‐drug pressures Social influence approach n = 2810 Deliverer: teacher Interactive modality N of sessions: 11 lessons in 7th grade and 3 in 8th grade Booster: no Duration of the intervention: 18 months | |
| Outcomes | Use of marijuana, measured by a questionnaire administered before the delivery of 7th grade curriculum and after the administration of 8th grade lessons (approximately 18 months later). Drug use was assessed for lifetime use, past month and weekly use | |
| Notes | Outcome assessed: at post‐test Attrition at post‐test (18th month): 8.8% | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Stratified randomisation by geographic area and community size and type (city, town and rural area). Within each strata blocked randomisation with blocks of 3 was used. Unit of allocation: school. A restricted assignment was used to reduce imbalance among groups using an index of school academic performance and socioeconomic status and the existence of a drug prevention programme in the district |
| Allocation concealment (selection bias) | Unclear risk | A restricted assignment was used to reduce imbalance among groups using an index of school academic performance and socioeconomic status and the existence of a drug prevention programme in the district |
| Incomplete outcome data (attrition bias) | Low risk | Students who dropped out were more likely to be non‐white, of lower socioeconomic class and to have tried alcohol, cigarettes and marijuana. However, the attrition rate and characteristic of students dropped out were similar across groups |
| Similarity of groups at baseline | Low risk | Students in the control group were less likely to be white and more likely to use marijuana. To reduce the effects of these differences there was adjustment for baseline covariates (use of drug, demographic characteristics, intentions and belief about drug use, perceived norms, pressure and social approval) |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | Cluster‐RCT | |
| Participants | 1649 7th grade students from 8 Pennsylvania middle schools (USA) | |
| Interventions | Experimental: project ALERT (revised), targeting alcohol, cigarettes and marijuana use, seeking to change student's beliefs about drug norms and consequences, and to help them to identify and resist pro‐drug pressures Social influence approach Group 1: adult led, n = not reported Group 2: adult led, teen assisted, n = not reported Deliverer: project staff Interactive modality N of sessions: 11 lessons in 7th grade and 3 in 8th grade Booster: no Duration of the intervention: overall over 2 school years, n of months not reported Control group: types of intervention: not reported, n: not reported | |
| Outcomes | Marijuana use (last month, last year, lifetime) on a 5‐point scale | |
| Notes | Attrition (overall): 27.5% Outcome assessed at post‐test and 12 months after the end of the intervention No data suitable for inclusion in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "each of the eight schools randomly assigned two 7th grade classrooms to each of three conditions: adult led project ALERT, teen assisted Project ALERT, control" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | Quote: "attrition was comparable across the three conditions" |
| Similarity of groups at baseline | Low risk | Quote: "no consistent pattern of differences emerged from the cohort, there was satisfactory evidence od equivalence among the treatment and control condition" |
| Blinding of outcome assessment (detection bias) | Low risk | Quote: "self report questionnaire was administered by school personnel to treatment and control classrooms" |
| Methods | Cluster‐RCT | |
| Participants | 5883 6th grade students from 34 schools in the USA 2004 to 2005 and 2005 to 2006 school years | |
| Interventions | Experimental: ALERT programme. Manualised classroom‐based substance use prevention curriculum which targets cigarette, alcohol, marijuana and inhalant use, motivates students not to use substances, provides skills to resist pressure from peers, supports attitudes and beliefs that mitigate substance use, addresses normative perceptions about peer use and acceptance Social influence approach N = 2817 Deliverer: teacher Interactive modality N of sessions: 11 lessons in 6th grade and 3 in the booster session the following year Booster: yes Duration of the intervention: overall over 2 school years, n of months not reported Control: usual curricula, n: 3045 | |
| Outcomes | Marijuana use, inhalants use. Drug use was assessed for lifetime use; last 30 days | |
| Notes | Outcome assessed: at post‐test and 1 year after the end of the intervention Attrition (overall): 21% | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "assignment was implemented through the use of computer generated random numbers" |
| Allocation concealment (selection bias) | High risk | Quote: "one of us randomly assigned schools to the experimental condition, blocked by school district. Assignments were made on a flow basis as soon as a district were paired and randomly assigned to a condition" |
| Incomplete outcome data (attrition bias) | Low risk | Quote: "differential attrition was not a problem because attrition was near 21% in both groups" |
| Similarity of groups at baseline | High risk | Schools in the control groups were more likely to offer prevention programmes not related to Project ALERT |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | RCT | |
| Participants | 33 7th grade students from a mid‐school in Albuquerque, New Mexico (USA). January 1985 to September 1985 | |
| Interventions | Experimental: ASAP (Alcohol and Substance Abuse Prevention Program) Knowledge‐focused approach Control group: Berkeley Health Education Curriculum: the curriculum presented short‐term and long‐term consequences of alcohol and drug abuse in a traditional work‐book and didactic format, as well as role‐play exercises, small group exercises and out of class assignments; discussing peer pressure and strategies to resist peer pressure. (n = 16) Knowledge‐focused approach Deliverer: project staff Interactive modality N of sessions: not reported Booster: no Duration of the intervention: 6 months | |
| Outcomes | Knowledge: consequences of use | |
| Notes | Outcome assessed at post‐test and at 8 months follow‐up after the end of the intervention No data suitable for inclusion in the meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "subjects were randomly assigned to either an experimental or control group |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Unclear risk | Information not reported |
| Similarity of groups at baseline | Unclear risk | Information not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | Cluster‐RCT | |
| Participants | 1416 2nd to 6th grade students enrolled across 4 Catholic schools in Louisiana (USA): 670 participants initially | |
| Interventions | Experimental: ATD programme (Alcohol/Tobacco/Drug use/abuse), targeting alcohol, cigarettes and marijuana use Social influence approach n = 348 Deliverer: teacher Modality not reported N of sessions: not reported Booster: no Duration of the intervention: overall over 2 school years, n of months = 18 Control: HEE programme; active control condition focused on obesity prevention (the Healthy Eating and Exercise), n: 313 | |
| Outcomes | Tobacco and alcohol expectancy Tobacco, alcohol and drug use | |
| Notes | Outcome assessed at 6, 12 and 18 months after the initiation of the intervention Attrition not reported Data on substance expectancies for meta‐analysis are partially reported in text and needed recalculation, while data on substance use are presented as beta and only in the footnotes of table 5; absolute numbers are reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Low risk | Quote: "The randomization was conducted by biostatisticians at Pennington Biomedical Research Center after the baseline data collection was completed. Therefore, treatment condition assignment was unknown to all parties prior to that point" |
| Incomplete outcome data (attrition bias) | Unclear risk | Seems to be a per protocol analysis |
| Similarity of groups at baseline | High risk | Statistically significant differences in: % with family member(s) who smoke |
| Blinding of outcome assessment (detection bias) | High risk | Quote: "Participants and research team members interfacing with the schools could not remain blind to |
| Methods | Cluster‐RCT | |
| Participants | 764 students; mean age 13 years form 10 high school cross Sidney metropolitan area (Australia) | |
| Interventions | Experimental: Climate Schools Alcohol and Cannabis course: each lesson included 15 to 20 minutes of Internet‐based lesson completed individually where students followed a cartoon storyline of teenagers experiencing real‐life situations and problems with alcohol and cannabis. The second part of each lesson was a predetermined activity delivered by the teacher to reinforce the information taught by the cartoon Social influence approach n = 397 Deliverer: teacher Interactive modality N of sessions: 12 Booster: no Duration of the intervention: 6 months Control group: usual health classes: n = 367 participants | |
| Outcomes | Cannabis knowledge questionnaire adapted form the Cannabis Quiz Cannabis use: assessed from a questionnaire in the 2007 National Drug Strategy Household Survey (NDSHS); assessed the frequency of use | |
| Notes | Attrition (overall): 20% Outcome assessed at post‐test, 6 and 12 months after the end of the intervention No data suitable for meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "the 10 participating schools were assigned randomly using an online randomisation system (www.randomized.org) to either a control condition or the intervention condition" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | 48% of the students completed the post‐test survey in the experimental group and 69% in the control group. (3% completed the 18 months follow‐up survey in the experimental group and 75% in the control group. There was no evidence of differential attrition |
| Similarity of groups at baseline | Unclear risk | The intervention group had higher alcohol and cannabis‐related knowledge and higher alcohol consumption |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | Cluster‐RCT | |
| Participants | 798 students from 3 senior high schools in Wuhan, a city in central China, participated in the study at baseline; school years not reported | |
| Interventions | Experimental: project CMER was designed to address the major cognitive, attitude, motivation and coping skills as the keys to prevent illicit drug use, such as general drug information, the negative impact of drug use, the relationship between the behaviour of drug use and AIDS, peer resistance skills, emotion adjusting skills Social competence approach n = 798 Deliverer: teacher Interactive modality N of sessions: 6 lessons Booster: no Duration of the intervention: 3 months Control: not reported | |
| Outcomes | Attitude to drug use, knowledge of drugs, type of drug, social impact of drug use, drug use consequences for health Addiction, motivation to use drug, peer resistance skills Illegal substance use at least once, drug use in the previous 30 days, drug use more times | |
| Notes | No attrition Outcome assessed at 3 months after the intervention Data are suitable for meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not specified |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Incomplete outcome data (attrition bias) | Low risk | Quote: "A missing data analysis was performed to ensure completeness of the questionnaires. Incomplete cases were excluded and descriptive analyses were performed." |
| Similarity of groups at baseline | Low risk | Quote: "A series of t‐tests examined whether the 2 groups differed in any of the variables, and the results showed that there were no significant differences (all P>0.05) in any of the substance use variables except for the mean scores of drug use consequences to health. This indicated a high degree of comparability between groups prior to the intervention." |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | RCT | |
| Participants | 114 8th and 9th grade students volunteering for 2 service opportunity courses (Cross‐Age‐Tutoring and School Store). Initial sample included 58 students in Cross‐Age‐Tutoring and 56 students in School Store. Spring 1979 to Spring 1980. California, USA | |
| Interventions | Experimental 1. Cross‐Age‐Tutoring: students were taught tutoring and communication skills and spent 4 days a week tutoring elementary students (n = 29) 2. School Store: students were taught business and interpersonal skills and operated an on‐campus store (N = 28 experimental) Deliverer: project staff Interactive modality N of sessions: not reported Booster: no Duration of the intervention: 6 months Control: no intervention (n = 29 in Cross‐Age study; n = 28 in School Store study | |
| Outcomes | Any drug current use, drug knowledge | |
| Notes | Outcome assessed at post‐test and at 1 year after the end of the intervention No data suitable for inclusion in the meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "voluntary students were randomly assigned to experimental or control condition" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | Attrition similar in all conditions |
| Similarity of groups at baseline | Unclear risk | Information not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | Cluster‐RCT | |
| Participants | 2071 6th grade students in the Lexington‐Fayette County public schools, Kentucky (USA), 1987 to 1988 school year | |
| Interventions | Experimental: DARE programme. Cognitive, affective and social skills strategies, aimed to increase students' awareness of adverse consequences of drug use, build self esteem, improve decision‐making and assertiveness in social settings (n = 1550) Deliverer: police officers Interactive modality N of sessions: not reported in 6th grade Booster: no Duration of the intervention: 4 months | |
| Outcomes | Frequency of past year use of marijuana. | |
| Notes | Outcome assessed at post‐test, 1, 2 , 5 and 10 years after the end of the intervention No data suitable for inclusion in the meta‐analysis. Authors contacted without reply | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Information not reported |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | 22.1% for the experimental group and 20.7% for the control group at 2 years follow‐up (8th grade) |
| Similarity of groups at baseline | Low risk | Chi² analysis revealed that there were no significant differences in attrition by condition at any follow‐up period |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not provided |
| Methods | Cluster‐RCT | |
| Participants | 1402 5th and 6th grade students from 20 North Carolina elementary schools (USA) | |
| Interventions | Experimental: DARE programme was a cognitive, affective and social skills strategies, aimed to increase students' awareness of adverse consequences of drug use, build self esteem, improve decision‐making and assertiveness in social settings Social competence approach n = 685: Deliverer: law officer Modality not reported N of sessions: 17 weekly lessons Booster: no Duration of the intervention: 4 months (August 1988 to December 1988) Control: usual curricula, n= 585 | |
| Outcomes | Self reported use of alcohol, tobacco, marijuana and inhalants, intentions use of these substances, several selected attitudinal variables Lifetime use, current use | |
| Notes | Outcome assessed at post‐test (not reported) Analysis sample n = 1270, n intervention group not reported, n control group not reported Data suitable for inclusion in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "schools were randomly assigned to receive DARE project or to be placed in the control condition" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | Quote: "students were equally likely not be present in the DARE and control schools. There were no consistent patterns indicating that students who did not completed the study were at greater risk for drug abuse" |
| Similarity of groups at baseline | Low risk | Groups not similar at baseline for some characteristics but adjustment for imbalance was done during the analysis using appropriate methods |
| Blinding of outcome assessment (detection bias) | Low risk | Questionnaires were compiled by participants using an anonym code and in a manner that ensured privacy without access by teachers, parents or project staff |
| Methods | Cluster‐RCT | |
| Participants | 6728 7th and 8th grade students from 24 middle and junior schools in Minnesota (USA), 1999 to 2001 school years. 6237 students completed baseline survey | |
| Interventions | Experimental: 2 conditions: 1. DARE only: provided skills in resisting influences to use drugs and in handling violent situations. Its also focused on character building and citizenship skills Social competence approach n = 2226 Deliverer: law officer + teachers Modality not reported N of sessions: 10 Booster: no Duration of the intervention: 2 school years 2. DARE + DARE Plus: DARE Plus had 2 components: the first was a classroom‐based, peer‐led, parental involvement programme focused on influences and skills related to peers, social groups, media and role models. The second component involved extra school activities Social competence approach n = 2221: Deliverer: law officer + teachers Modality not reported N of sessions: 10 sessions implemented by law officer + 4 sessions implemented by teachers Booster: no Duration of the intervention: 4 weeks Control: "delayed program", n = 1790 (had the opportunity to receive the DARE Plus programmes in 2001 to 2002, after the final follow‐up) | |
| Outcomes | Self reported tobacco, alcohol and marijuana use; multidrug use; violent behaviours among the students, physical victimisation Past use of alcohol, current use of tobacco | |
| Notes | Outcome assessed at post‐test (not reported) Analysis sample n = 5239, n intervention group not reported, n control group not reported No data suitable for inclusion in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The study design involved 24 middle and junior high schools in Minnesota that were matched on socioeconomic measures, drug use and size, and randomly assigned to 1 of 3 conditions |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Incomplete outcome data (attrition bias) | Unclear risk | 84.0% retention at final follow‐up. Reasons for loss to follow‐up included students relocating (10.8%), absenteeism (1.4%), parental refusal or non‐deliverable consent form (2.3%), student refusal (1.0%), and home schooling, limited English or special education (0.5%). Loss to follow‐up rates did not differ by study condition. The main outcomes of the study were analysed using growth curve analyses. This analytic method permits retention of participants who do not have complete data |
| Similarity of groups at baseline | Low risk | Quote: ''At baseline, there were no significant differences between the 3 conditions." |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | Cluster‐RCT | |
| Participants | 465 students from a high school in southwestern USA | |
| Interventions | Experimental: Drug Resistance Strategies project was a communicative resistance skills training through film and live performance. The curriculum utilised actual narrative accounts that were performed by actors and couched in a musical drama format. The film curriculum was produced on film and transferred to videotape; the screenplay was then adapted into a live performance format 4 experimental conditions: Social competence approach n = not reported Deliverer: project staff Modality not reported Booster: no Duration of the intervention: 1 month Control: programme not reported, n = 89 | |
| Outcomes | Students were pre‐tested with a questionnaire containing demographic information, current usage and amount, use of resistance skills, confidence and difficulty of resistance, attitudes, perceived normative support for use of drugs and alcohol, and use of planning to avoid drugs | |
| Notes | Outcome assessed at post‐test 1 day after; assessed at follow‐up after 1 month Analysis sample n = 5239, n intervention group not reported, n control group not reported No data suitable for inclusion in the meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: " 21 classes were randomly assigned to one of four intervention conditions and one control condition" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Unclear risk | Unclear attrition rate |
| Similarity of groups at baseline | Unclear risk | Information not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | Cluster‐RCT | |
| Participants | 2678 students aged 13 to 14 years from 12 metropolitan and 4 country district in Australia, 1997 to 1999 school years. 2678 students completed baseline survey | |
| Interventions | Experimental: Gatehouse Project aimed at increase the level of emotional well being and reduce the substance use through: building a sense of security and trust, increasing skills and opportunities for good communication and building a sense of positive regard through valued participation in aspects of school life Social competence approach n = 1335 Deliverer: project staff Modality not reported N of sessions: 20 Booster: yes Duration of the intervention: 3 months Control: n = 1343 | |
| Outcomes | Mental health status: reported anxiety/depressive symptoms Social relation: availability of attachment and conflictual relationship Victimisation School engagement Tobacco, alcohol and cannabis use: current use of tobacco and alcohol, past month use of tobacco and past 2 weeks use of alcohol; regular use of tobacco and alcohol; use of cannabis in the previous 6 months | |
| Notes | Outcome assessed at the end of year 8, 9, 10 (12, 24, 36 months after the initiation of the intervention, first surveys at 5 months after the end of intervention) Analysis sample not reported, n intervention group not reported, n control group not reported Data suitable for inclusion in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "district were randomly allocated to experimental or control condition. Using simple random sampling 12 school in the metropolitan area and 4 in the country region were selected from the intervention district and 12 and 4 from the control district" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | Analysis done with the intention‐to‐treat principle |
| Similarity of groups at baseline | Low risk | The intervention group reported only slightly lower levels of risk factors such as parental separation and parental smoking |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | RCT | |
| Participants | 678 1st grade students from 9 primary schools in the USA, 1993 school year | |
| Interventions | Experimental: 2 experimental conditions: GBG programme involves a whole class strategy to decrease disruptive behaviour and reduce early‐onset tobacco smoking n = 192 Booster: no ‐ Family‐school partnership intervention improves achievement and reduces early aggression and shy behaviour by enhancing parent‐school communication and providing parents with effective teaching and child behaviour management strategies n = 178 Booster: yes Other approach Deliverer: teacher Interactive modality N of sessions: not reported Duration of the intervention: 1 school year Control: standard educational setting, n = 196 | |
| Outcomes | Tobacco, alcohol, marijuana, inhalants and other illegal drug use | |
| Notes | Outcome assessed at 5, 6 and 7 years (6th through 8th grades) Analysis sample n = 566, 192 intervention group, 178 control group Data suitable for inclusion in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "students were assigned at random to the three designated classrooms with balancing for male‐female ratio" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | Quote: "attrition across follow up period was unrelated to intervention status and participants lost at follow up did not differ from participants with complete data with respect to baseline teacher rating, academic achievement and demographic characteristics." |
| Similarity of groups at baseline | Low risk | Quote: "we found no statistically significant differences in terms of sociodemographic characteristics across groups" |
| Blinding of outcome assessment (detection bias) | Low risk | Quote: "audio computer assisted self interview (ACASI) methods were used to administer standardized items; the student marked their responses under private conditions that were maintained by a member of the assessment staff, who took care not observe the responding and to prevent observations by the vicinity" |
| Methods | Cluster‐RCT | |
| Participants | 19 schools, 41 classrooms, 407 first grade children within 5 urban areas in Baltimore during 1985 to 1986 | |
| Interventions | Experimental group: 8 GBG classrooms (n = 238) Based on life course/social field theory "The teacher posted basic classroom rules of student behavior, and during a particular game period all teams received a reward if they accumulated four or fewer infractions of acceptable student behavior. The GBG was played during periods of the day when the classroom environment was less structured, such as when the teacher was working with one student or a small group while the rest of the class was instructed to work on assigned tasks independently. Over time, the game was played at different times of the day and during different activities. In this manner, the GBG evolved from a precise procedure that was highly predictable and visible, with a number of immediate rewards, to a procedure with an unpredictable occurrence and location, with deferred rewards." Other approach Deliverer: trained teacher Modality: interactive Duration: 2 years Sessions: 3 per week lasting 10 minutes, increasing to 40 minutes Booster: no Control group: no intervention : 6 classrooms (n = 169) | |
| Outcomes | CIDI‐UM modified (Composite International Diagnostic Interview ‐ University of Michigan: a scale for occurrence of drug abuse and dependece disordes), to reflect the Diagnostic and Statistical Manual of Mental Disorders‐IV (DSM‐IV) diagnostic criteria, was used to determine the lifetime, past year and past month occurrence of drug abuse and dependence disorders. Diagnoses were derived in accordance with the DSM‐IV criteria, using a computerised scoring algorithm | |
| Notes | Outcome assessed at age 19 to 21 by blinded interviewers Attrition 24.1% | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Multilevel randomised design; no further description of sequence generation Quote: "The first stage of the design involved selecting five distinctly different socio‐demographic urban areas in Baltimore. The second stage of the design involved assigning individual children to first grade classrooms within each school so that classrooms were nearly identical before they were assigned to the intervention condition. The third stage of this design was random assignment of classrooms and teachers to intervention condition within each intervention school" |
| Allocation concealment (selection bias) | Unclear risk | No description of method of allocation concealment |
| Incomplete outcome data (attrition bias) | High risk | 24.1% attrition |
| Similarity of groups at baseline | Low risk | No differences between the GBG and control sample were found |
| Blinding of outcome assessment (detection bias) | Low risk | The interviewers were masked to the first grade intervention condition |
| Methods | RCT | |
| Participants | 511 students from 4th, 5th and 6th grade from 23 classes of 6 elementary schools in northwest Arkansas (USA), during spring 1989. 501 students completed baseline survey | |
| Interventions | Experimental: Keep A Clear Mind Program (KACM) was based on a social skills training model, aimed to help children to develop specific skills to refuse and avoid "gateway" drug use Social competence approach n = not reported Deliverer: project staff + teacher Modality not reported N of sessions: 4 Booster: no Duration of the intervention: 1 month Control: not reported, n= not reported | |
| Outcomes | Alcohol, tobacco and marijuana use; intentions, beliefs and knowledge | |
| Notes | Outcome assessed at post‐test: 2 weeks after the implementation of the programme Attrition at post‐test: 11% No data suitable for inclusion in the meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "students were blocked on school and grade level then randomly assigned by class to either an intervention or control group" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | Quote: "similar proportions of students completed the post test questionnaire in both groups" |
| Similarity of groups at baseline | Low risk | Quote: "no significant differences were found between intervention and control group at pretest on the primary variables with one exception: the control group included a great number of black students" |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | Cluster‐RCT | |
| Participants | 6035 7th grade students from 35 middle schools in Arizona, USA. During 1997 to 1998. 4234 students completed baseline survey | |
| Interventions | Experimental: Drug Resistance Strategies Project (DRS) implemented and evaluated in the "Keepin' it REAL curriculum". The curriculum is aimed to develop drug resistance strategies, life skills and decision‐making, communication competences, knowledge. 3 parallel versions: a Mexican American centred version (oriented toward Mexican American culture), a Black and White centred version (oriented toward European American and African American culture) and a multicultural version Social competence approach n = 25 schools Deliverer: teacher Interactive modality N of sessions: 10 sessions in 7th grade Booster: yes Duration of the intervention: 18 months Control: already existing substance use prevention programmes, n = 10 schools | |
| Outcomes | Recent substance use (alcohol, tobacco, marijuana). Resistance strategies (alcohol, tobacco, marijuana). Self efficacy. Intent to accept. Positive expectancies. Norms | |
| Notes | Outcome assessed at: post‐test after the implementation of the booster (6 months after the initiation of the intervention), 8 months after curriculum implementation and 14 months after curriculum completion Analysis sample n = 4234, n intervention group not reported, n control group not reported No data suitable for inclusion in the meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The research team stratified the 35 participating public schools according to enrollment and ethnicity (% Hispanic) and then used block randomisation to assign each school to one of 4 conditions (Mexican American, Black/White, multicultural and control; 8, 9, 8 and 10 schools |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Incomplete outcome data (attrition bias) | Unclear risk | The anonymisation process linked 24% of the students over all 4 waves, an additional 22% over 3 waves, and another 19% between only 2 of the waves. Altogether, 55% of the respondents had a pretest questionnaire linked to at least 1 of the post‐tests |
| Similarity of groups at baseline | Low risk | Statistically significant differences in racial and socioeconomic conditions, but data adjusted for baseline characteristics |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | Cluster‐RCT | |
| Participants | At baseline, 1566 5th grade students from 23 public middle schools (81 homerooms) in Phoenix, Arizona (USA). School year 2004 to 2006 | |
| Interventions | Experimental: keepin 'it REAL (kiR) adapted multicultural curriculum for the 5th grade. The 5th grade version uses the same basic curriculum content as the standard 7th grade multicultural version, differing primarily in communication level/format, the concreteness of the presentation of concepts, and the age‐based relevance of the examples. Although the core content of the standard curriculum uses several strategies deemed successful with preadolescent children (narrative, participatory modelling, Social competence approach n = 10 schools Deliverer: teacher Interactive modality N of sessions: 12 sessions in 5th grade, 3 to 6 boosters Booster: yes Duration of the intervention: 18 months Control: standard intervention, n = 13 schools | |
| Outcomes | Socio‐demographic characteristics Hypothetical alcohol resistance Students' active decision‐making style Intentions to use substances Parents' anti‐drug injunctive norms Friends' anti‐drug injunctive norms Personal anti‐drug norms Descriptive norms Substance use expectancies Lifetime prevalence of alcohol, tobacco, marijuana, inhalants Past month's prevalence of alcohol, tobacco, marijuana | |
| Notes | Outcome assessed at the end of the intervention (12 months follow‐up) and at the end of the booster session (18 months) Analysis sample n = 1566, n intervention group not reported, n control group not reported Data suitable for inclusion in the meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not specified |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Incomplete outcome data (attrition bias) | High risk | 91% of the students who participated in the baseline assessment also participated at wave 2; and 72% of the students who participated in the baseline assessment also participated at wave 3. Schools reported students transferring out at rates of between 10% and 25% (average transfer out rate of 16%), which accounts for much of the attrition between baseline and wave 3 |
| Similarity of groups at baseline | Low risk | A test of homogeneity of proportions indicated that the 7 student participation patterns did not vary between the 2 study conditions (F(3.58, 78.82) = 0.545, P value = 0.684). Thus, there does not appear to be evidence of differential participation. Although it is possible that the students in the 2 conditions differed with respect to unobserved characteristics, the data presented in Table 1 suggest that they did not differ with respect to some observed characteristics that have been shown to be correlated with substance use among adolescents |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | Cluster‐RCT | |
| Participants | At baseline 1984 students from 5th grade from 29 public elementary schools in Phoenix, Arizona, 2004 school year | |
| Interventions | Experimental: participants were assigned to 6 conditions: The 5th grade versions use the same basic curriculum content as the 7th grade versions, differing primarily in Social competence approach n = not reported Deliverer: not reported Modality not reported Booster: yes Duration of the intervention: 18 months Control: school's regularly scheduled, substance use prevention programme, n = not reported | |
| Outcomes | Lifetime substance use prevalence (alcohol, tobacco, marijuana, inhalants); past month prevalence; intention to use substances; refusal efficacy; hypothetical alcohol resistance; number of substance use resistance strategies; descriptive substance use norms (scales); personal anti‐drug norms; positive substance use expectancies (scales) | |
| Notes | Outcome assessed at 8th grade ‐ wave 6, 48 months after (baseline ‐ W1 at the beginning of the 5th grade = fall 2004; 5th follow‐up ‐ W6 during 8th grade = winter 2007 to 2008) Analysis sample n = 1984, n intervention group not reported, n control group not reported No data suitable for inclusion in the meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Stratified randomisation |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Incomplete outcome data (attrition bias) | High risk | Student participation fell to 45% of the original sample by the final assessment, with losses concentrated in 3 of the original 29 schools |
| Similarity of groups at baseline | Unclear risk | Not specified |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | Cluster‐RCT | |
| Participants | 1311 7th grade students from 10 suburban New York junior high schools, USA. 1185 students completed baseline survey | |
| Interventions | Experimental: Life Skills Training Program (LST) is a multicomponent substance abuse prevention programme consisting of 5 major components: cognitive, decision‐making, anxiety, managing, social skills training, self improvement, with the following experimental conditions (factorial design): Social competence approach n = 8 schools Deliverer: teacher, peer (older students) Modality: not reported N of sessions: 20 sessions in 7th grade, 10 sessions for booster Booster: yes Duration of the intervention: 2 school years Control: not reported, n = 2 schools | |
| Outcomes | Smoking status, problem drinking, marijuana use (ever tried, monthly, weekly, daily), cognitive measures, attitudinal measures, personality measures | |
| Notes | Outcome assessed at: post‐test (4 months after the pre‐test),12 months after the implementation of the intervention No data suitable for inclusion in the meta‐analysis: the absolute numbers of participants in the groups are not given. Authors contacted without reply | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "the 10 schools had been randomly assigned to the five conditions. Two schools were assigned to each experimental condition and two schools were assigned to the control condition" |
| Allocation concealment (selection bias) | Unclear risk | Information not provided |
| Incomplete outcome data (attrition bias) | Low risk | Attrition at post‐test: 9.6% |
| Similarity of groups at baseline | Unclear risk | Information not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | Cluster‐RCT | |
| Participants | 5954 7th grade students from 56 schools in the New York State (USA), fall of 1985 to 1986 school year 4466 students completed baseline survey | |
| Interventions | Experimental: Life Skills Training Program: a cognitive‐behavioural resistance skills prevention programme, with 3 experimental conditions: Social competence approach Deliverer: teacher, project staff Modality: not reported N of sessions: 15 sessions in 7th grade, 10 sessions for booster in 8th grade and 5 in 9th grade Booster: yes Duration of the intervention: 3 school years Control: as usual, n = 1142 | |
| Outcomes | Monthly and weekly prevalence of cigarette smoking, alcohol, marijuana and other drugs consumption; knowledge attitude; normative beliefs; skills; psychologic characteristics | |
| Notes | Outcome assessed at: post‐test (at the end of the intervention), and at 6 years follow‐up (3 years after the end of the intervention) Attrition at post‐test: 25% 782 students were excluded from the analysis sample because of failure to meet the inclusion criteria Attrition after 6 years: 39.6%. Analysis sample: n = 3597 Data suitable for inclusion in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "In a randomized block design, schools were assigned to receive one of the three interventions". School were divided in 3 groups on the basis of the geographic area of New York city. Within each area schools were also divided into 3 groups on the basis of cigarette smoking prevalence rates (high, medium or low) and assigned to the experimental conditions within each group and geographic area |
| Allocation concealment (selection bias) | Unclear risk | Information not provided |
| Incomplete outcome data (attrition bias) | Low risk | 25% of the original sample unavailable at 6 years follow‐up. Attrition analysis examining the effect of baseline drug use and condition revealed higher attrition among marijuana users at baseline, among students in control condition and among marijuana users in control condition 40% of the original sample unavailable at 6 years follow‐up. Attrition analysis examining the effect of baseline drug use and condition revealed no differential attrition effect |
| Similarity of groups at baseline | Low risk | No significant differences for behavioural outcome measures |
| Blinding of outcome assessment (detection bias) | High risk | Quote: "students were assessed by questionnaires administered by project staff" |
| Methods | Cluster‐RCT 6 schools were matched according to demographics and randomly assigned to receive one of 3 interventions | |
| Participants | 757 7th grade students from 6 junior high schools in New York (USA), school year not specified | |
| Interventions | Experimental: 2 experimental conditions: Social competence approach Deliverer: project staff + peer Interactive modality N of sessions: 15 at an average rate of 2 sessions per week in the 7th grade Booster: yes in the 8th grade Duration of the intervention: 18 months Control group: information only, n = 124 | |
| Outcomes | Marijuana use (assessed on a 9‐point scale: never tried, tried but don't use now, less than once a month, about once a month, about 2 or 3 times a month, about once a week, a few times a week, about once a day, more than once a day) Knowledge Intention to use | |
| Notes | Outcome assessed at post‐test and at 18 months after the end of the intervention Attrition at post‐test: 16%. Analysis sample: n = 639 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Schools were randomly assigned to receive one of the three interventions" |
| Allocation concealment (selection bias) | Unclear risk | Information not provided |
| Incomplete outcome data (attrition bias) | Low risk | Attrition analysis revealed no significant attrition effect on pretest drinking status; there were slightly more attrition among marijuana users in the control intervention |
| Similarity of groups at baseline | High risk | Culturally focused intervention is targeted only at high‐risk individuals, but it is not reported how high‐risk was defined; moreover in this case only some of the students in the schools randomised to this intervention should have received the intervention (i.e. the high‐risk students) but this information is not provided |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not provided |
| Methods | Cluster‐RCT | |
| Participants | 5222 7th grade students from 29 New York City public schools (USA), school year not specified. 3621 (69%) students completed baseline survey | |
| Interventions | Experimental: Drug Abuse Prevention Program, teaching drug resistance skills, anti‐drug norms, and facilitating the development of personal and social skills. These skills were taught using a combination of teaching techniques including group discussion, demonstration, modelling, behavioural rehearsal, feedback and reinforcing, and behavioural homework assignments Social competence approach n = 2144 Deliverer: teacher Modality: not reported N of sessions: 15 sessions in 7th grade, 10 sessions for booster in the 8th grade Booster: yes Duration of the intervention: 2 school years Control: programme that was normally in place at New York City schools, n = 1477 | |
| Outcomes | Tobacco, alcohol, marijuana, inhalants use; behavioural intentions; normative expectations; drug attitudes and knowledge; social and personal competence Students provided data at the pre‐test and post‐test (grade 7), as well as at the 1‐year follow‐up (grade 8) | |
| Notes | Outcome assessed at: post‐test (3 months after the end of the intervention) and 1 year after the end of the intervention Analysis sample n = 3621, n intervention group not reported, n control group not reported Data for inclusion in the tables were obtained from authors | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Blocked randomised design. Prior to randomisation, schools were surveyed and divided into high, medium, or low smoking prevalence. From within these groups, each of the 29 participating schools were randomised to either receive the intervention (16 schools) or be in the control group (13 schools)" |
| Allocation concealment (selection bias) | Unclear risk | Information not provided |
| Incomplete outcome data (attrition bias) | Low risk | Attrition analysis examining the effect of baseline drug use and condition revealed higher attrition among marijuana users at baseline, and among marijuana users in control condition |
| Similarity of groups at baseline | Low risk | No significant difference in any substance use variables or gender: there were more black students in the experimental condition and more Hispanic students in the control conditions |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not provided |
| Methods | Randomised pretest and post‐test comparative design (it seems that individuals are sample unit) | |
| Participants | 170 Thai high school students from grades 7 to 12, years not specified | |
| Interventions | Experimental: LST programme provided students with information and skills specifically related to drug and tobacco use, such as the effects of drugs, self awareness skills, decision‐making and problem‐solving skills, stress and coping skills, and refusal skills Social competence approach n = 85 Deliverer: not reported Interactive modality N of sessions: 10 Booster: no Duration of the intervention: not reported Control: tobacco and drug education curriculum normally provided, n = 85 | |
| Outcomes | Knowledge about the health consequences of tobacco and drug use Attitudes toward tobacco and drug use Life skills, refusal, decision‐making and problem‐solving skills Tobacco and drug use frequency in the past 2 months | |
| Notes | Outcome assessed at: post‐test (6 months after the end of the intervention) Analysis sample n = 170, n intervention group not reported, n control group not reported Attrition at post‐test not reported No data suitable for inclusion in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not specified |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Incomplete outcome data (attrition bias) | Unclear risk | Not specified |
| Similarity of groups at baseline | Low risk | The results revealed no significant differences between the control and the intervention groups at pretest |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | Cluster‐RCT | |
| Participants | 36 public schools from 2 South African provinces, KwaZulu‐Natal and the Western Cape, school year not specified. 5266 students completed baseline survey. | |
| Interventions | Experimental : Keep Left South African version and Life Skill Training South African version: decision‐making framework, stress management, resisting peer pressure Social competence approach Group 1: Keep Left South African version; n = 12 schools, 1978 students ‐Group 2: LST South African version; n = 12 schools, 1717 students Deliverer: teacher Interactive modality N of sessions: 16 sessions for Keep Left and 16 sessions for LST Booster: no Duration of the intervention: 2 school years (8th grade and 9th grade) Control: usual tobacco and substance use education, n = 12 schools, 1571 students | |
| Outcomes | The primary outcome was past month use of cigarettes; secondary outcomes were: daily marijuana and hard drug use, daily binge drinking | |
| Notes | Outcome assessed at: post‐test 1 (after 1 year, at the end of the 8th grade) and at post‐test 2 (after 2 years, at the end of the 9th grade) Analysis sample at post‐test 2 n = 3267, n intervention group at post‐test 2 = 2256, n control group at post‐test 2 = 1011 Data suitable for inclusion in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Schools were then randomly selected within each ethnicity, size and SES strata. The target sample was 36 or 12 per experimental group |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Incomplete outcome data (attrition bias) | High risk | Students completed questionnaires on 3 occasions: (1) baseline at the beginning of 8th grade, (2) post‐test 1 at the end of 8th grade, and (3) post‐test 2 at the end of9th grade. For the 2 post‐test assessments, only individuals who were in the school at the beginning of grade 8 and who completed the baseline evaluation were asked to complete questionnaires. Thus, there was selective attrition in the study |
| Similarity of groups at baseline | Low risk | At baseline, the 3 intervention groups did not differ on any of the socio‐demographic or substance |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | Cluster‐RCT | |
| Participants | 416 students aged 16 to 19 years old recruited in 12 London Further Education colleges without regard to substance use status. The response was encouraging with 12 out of 21 colleges approached agreeing to participate. Age 16 to 19 years was adopted as the sole inclusion criterion, and there were no formal exclusion criteria | |
| Interventions | Experimental: motivational Interview: highly individualised intervention. Its aim is to help the participant explore their own behaviour. Particular emphasis is given to perceptions of risk and problem recognition, concerns and consideration of change, and also to the activity of the practitioner in directing attention towards the resolution of ambivalence Deliverer: not reported Interactive modality N of sessions: 1 Booster: no Duration of the intervention: 1 hour Control group: "Drug Awareness" (DA): 16‐question quiz on the effects of cigarette smoking, alcohol consumption and cannabis use, followed by further discussion components and the provision of leaflets giving accurate information on the effects of target drugs | |
| Outcomes | Prevalence, initiation and cessation rates for cannabis use | |
| Notes | Outcome assessed at 3 and 12 months follow‐up Attrition: 3 months: 11%, 12 months: 16.5% | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Computerised randomisation was undertaken by the local Clinical Trials Unit and decisions were communicated by telephone to researchers after recruitment and baseline data collection on an individual college basis to preserve allocation concealment. We stratified allocation by college, so that equivalent numbers of groups recruited from any one college would be allocated to each study condition." |
| Allocation concealment (selection bias) | Low risk | Quote: "Computerised randomisation was undertaken by the local Clinical Trials Unit and decisions were communicated by telephone to researchers after recruitment and baseline data collection on an individual college basis to preserve allocation concealment. We stratified allocation by college, so that equivalent numbers of groups recruited from any one college would be allocated to each study condition." |
| Incomplete outcome data (attrition bias) | Low risk | Attrition was not differential between the study groups |
| Similarity of groups at baseline | Low risk | Randomisation successfully created baseline equivalence between groups |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | RCT | |
| Participants | 473 students from 7th and 9th grade attending 2 junior high schools in a suburban community in Northern California (USA), during second semester of the academic year 1980 to 1981. 399 students completed baseline survey | |
| Interventions | Experimental: Napa Project focus on motivation and decision‐making skills, personal goals, assertiveness, knowledge Social competence approach n = 237 Deliverer: project staff Interactive modality N of sessions: 12 sessions from February through May 1981 Booster: no Duration of the intervention: 4 months Control: programme that was normally in place at New York City schools, n = 236 | |
| Outcomes | Any drug Drug knowledge, general drug attitude, alcohol benefits, pot benefits, alcohol costs, pot costs, soft attitudes, soft peer attitudes, soft peer use, alcohol involvement, cigarette involvement, pot involvement, pill benefits, pill cost, hard peer attitude, hard peer use, hard attitude | |
| Notes | Outcome assessed at: post‐test (May 1981, at the end of the intervention) and at 5 months (October 1981) Analysis sample n = 352, n intervention group not reported, n control group not reported No data suitable for inclusion in the meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "classes were paired on pretest attitudes and involvement in alcohol, cigarette and marijuana use. One class in each pair was then randomly assigned to receive the experimental intervention and the other to the control group" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Unclear risk | Information not reported |
| Similarity of groups at baseline | Unclear risk | Information not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | Cluster‐RCT | |
| Participants | 7846 participants, first 3 years of 48 schools (24 experimental and 24 control), Hong Kong | |
| Interventions | Experimental intervention: Positive Adolescent Training through Holistic Social Programmes. There are 2 tiers of programmes in the Project PATHS. Both tiers are developed with reference to 15 positive youth development constructs, including bonding, resilience, social competence, recognition of positive behaviour, emotional competence, cognitive competence, behavioural competence, moral competence, self determination, self efficacy, clear and positive identity, beliefs in the future, prosocial involvement, prosocial norms and thriving. An important feature of the Project PATHS is its systematic evaluation approaches (e.g. interim evaluation, focus group interview, survey on subjective and objective outcomes, programme implementers' evaluation, student weekly diary, etc.), which enable researchers to examine the effectiveness of the programme thoroughly= (n = 4049) Other approach Deliverer: teacher and social worker Interactive Number of sessions: 120 (40 every school year) Booster: only a parallel tier 2 programme for students with special needs Duration of intervention: 36 months | |
| Outcomes | Use of drugs: composite score of illegal drug use (ketamine, cannabis, ecstasy, heroine) Likert scale (0 to 7) | |
| Notes | Process evaluation year 1 to 3 (wave 1 to 6). 3 and 12 months after the end (wave 7, 8) Attrition Wave (W) 1, W2, W3, W4, W5, W6, W7, W8 Experimental: 4049, 3734, 3174, 2999, 3119, 3006, 2879 (71%), 2852 (70%) Control: 3797, 3654, 3765, 3698, 3757, 3727, 3669 (96%), 3640 (96%) No data suitable for meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Eighty schools, representative of schools in the three region areas, were randomized to either control or intervention arm. Five schools (6.3%) from the control arm withdrew before the baseline survey and were not replaced. There were no differences found between the schools that withdrew and participating schools." |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Eighty schools, representative of schools in the three region areas, were randomized to either control or intervention arm. Five schools (6.3%) from the control arm withdrew before the baseline survey and were not replaced. There were no differences found between the schools that withdrew and participating schools." |
| Incomplete outcome data (attrition bias) | High risk | High attrition in the experimental group (30%) and unbalanced (only 4% in the control group) |
| Similarity of groups at baseline | Unclear risk | Quote: "With schools being the units of analysis, results indicated that the 19 experimental schools and 24 control schools did not differ in school characteristics in terms of banding (i.e., categorizing based on students academic competence), geographic district, religious affiliation, sex ratio of the students, Data not reported for substance use at baseline |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | RCT | |
| Participants | 283 junior and senior high school students (volunteers) from the public schools of Milwaukee, Wisconsin (USA). 1979 to 1980 and 1980 to 1981 school years | |
| Interventions | Experimental: PAY programme (Positive Alternatives for Youth), aimed to increase alternatives to drug abuse, such as personal awareness, interpersonal relations, self reliance development, vocational skills, aesthetic and intellectual experiences, social‐political involvement, sexual expression, meditation, spiritual‐mystical experiences and creative experiences Social competence approach n = 160 Deliverer: project staff and teacher Interactive modality. N of sessions: 48 sessions during 2 school years (1979 to 1980 and 1980 to 1981) Booster: no Duration of the intervention: 6 months Control: no treatment, n = 123 | |
| Outcomes | Drug and alcohol use, activities participation, feelings and remedies, marijuana and alcohol involvement, attitudes and perceptions of one's social skills, peer pressure resistance, self esteem, future orientation, stress management, attitudes towards drugs and alcohol, responsible use, activity attitudes | |
| Notes | Outcome assessed at: post‐test 1 (during the spring semester of 1980) and at post‐test 2 (at the end of the programme, during the spring semester of 1980) Analysis sample at post‐test 2 n = 105, n intervention group 58, n control group 50 Attrition at post‐test (first year): 14.4% for the experimental group, 10.9% for the control group No data suitable for inclusion in the meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "students were randomly assigned to either the PAY alternative classes or to a no treatment control group" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Unclear risk | Drop‐out balanced in numbers across intervention groups but reasons for dropping out and characteristics of students who dropped out compared with characteristics of students who remained are not reported |
| Similarity of groups at baseline | Unclear risk | Information not reported, apart from sex and ethnicity |
| Blinding of outcome assessment (detection bias) | Low risk | Questionnaires were compiled by participants using an anonym code and in a manner that ensured privacy without access by teachers, parents or project staff |
| Methods | Matched‐pair, cluster‐randomised, controlled design, | |
| Participants | 1714 first or second grade children at baseline from 20 public elementary (kindergarten to 5th or 6th grade) schools on 3 Hawaiian islands. Our study followed students who were in 1st or 2nd grade at baseline (the 2001 to 2002 academic year) and who stayed in the study schools through 5th grade (the 2005 to –2006 academic year for the first grade cohort, and the 2004 to 2005 academic year for the second grade cohort) | |
| Interventions | Experimental: the Positive Action programme is a multicomponent school‐based social and character development programme designed to improve academics, student behaviours and character. Lessons are grouped into 6 major units: self concept, mind and body positive actions (e.g. nutrition, physical activity, decision‐making skills, motivation to learn), social and emotional actions for managing oneself responsibly (e.g. emotion regulation, time management), getting along with others (e.g. empathy, respect, treating others as one would like to be treated), being honest with yourself and others, and self improvement (e.g. goal‐setting, courage to try new things, persistence) Social competence approach 10 schools, N = 976 Deliverer: teacher Interactive modality N. of session: 140 per year over 5 years (total 700) Booster: yes Control: business as usual 10 schools , N = 738 | |
| Outcomes | Lifetime prevalence of substance use, self reported (N = 1714) and observed by teacher (N = 1225) (yes/no and scale) | |
| Notes | Outcome assessed at post‐test Attrition: not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Stratified randomisation |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Incomplete outcome data (attrition bias) | High risk | Students who left study schools during the study period were dropped from the study, and students who joined study schools during the study period were added to the study (without collecting baseline data). Thus, our study also included students who entered the schools at any year during the course of the study and who were in 5th grade at the end of the study |
| Similarity of groups at baseline | Low risk | No significant differences (P value ≥ 0.05) were observed between reports from control and intervention schools, |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | RCT | |
| Participants | Of the 512 adolescents recruited into the study (students attending 2 public high schools in northeast Florida during fall 2008), 93.6% (n = 479) participated in the baseline data collection, with 19 students grade‐ineligible and 14 students absent from school | |
| Interventions | Experimental: Project Active 9‐item life skills screen assessing target health behaviours, a one‐on‐one consultation with slides presenting positive image feedback tailored to screen results, a set of concrete behavioural recommendations for enhancing future fitness, and a personal fitness goal‐setting and commitment strategy linking positive image attainment with specific health behaviour change. Intervention content and strategies were based on the Behaviour‐Image Model (n = 237) Deliverer: not reported Passive modality N of sessions: 1 Booster: no Duration of the intervention: 1 hour Control group: 15‐page booklet titled: "What Everyone Should Know ABOUT WELLNESS",which included information and illustrations about smoking, alcohol and drug use avoidance, exercise types and benefits, eating nutritious foods, managing stress, getting adequate sleep and maintaining a positive attitude (n = 242) | |
| Outcomes | Frequency and quantity of marijuana use, scored as 30‐day frequency (ranging from 1 = 0 days through 11 = 28 to 30 days) and 30‐day quantity (ranging from 1 = 0 marijuana times used per day through 12 = 31 or more times using marijuana) | |
| Notes | Outcome assessed at 3 months follow‐up Attrition: 6% | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A randomised controlled trial was conducted using a within‐school design at 2 schools. Participants were |
| Allocation concealment (selection bias) | Low risk | Computer‐generated random numbers |
| Incomplete outcome data (attrition bias) | Low risk | Most participants (94.1%) successfully completed the post‐intervention data collection. Of those lost to follow‐up, 24 participants (85.7%) moved away from school and 4 (14.3%) were lost due to repeated absence from school, resulting in a total of 451 participants. No differences were found in the proportion of those who dropped out between treatment groups or participating schools |
| Similarity of groups at baseline | Low risk | No differences were found for any of the socio‐demographic or target health behaviour measures between treatment groups at baseline |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | RCT | |
| Participants | 140 students attending a school in Hackney (London), aged 7 to 10 years, school year not specified. 120 students completed baseline survey | |
| Interventions | Experimental: Project CHARLIE (Chemical Abuse Resolution Lies in Education) is based on lessons focused on increase of self esteem, decision‐making power, resistance skills and knowledge, Social competence approach n = 65 students Deliverer: teacher Modality. not reported N of sessions: 40 sessions during 2 school years (1979 to 1980 and 1980 to 1981) Booster: no Duration of the intervention: 12 months Control: no intervention, n = 55 students | |
| Outcomes | Resistance and decision‐making skills | |
| Notes | Outcome assessed at post‐test (at the end of the intervention) Analysis sample at post‐test 2 n = not reported, n intervention group not reported, n control group not reported. Attrition: 10.9% in the intervention group Data suitable for inclusion in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "all the children attending the selected two forms entry junior school were randomly selected to receive the Project Charlie" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Unclear risk | Reasons for drop‐out not reported |
| Similarity of groups at baseline | Low risk | No significant differences in socio‐demographic characteristics between groups |
| Blinding of outcome assessment (detection bias) | Low risk | Quote: "pre and post‐testing was carried out by one of the authors with no involvement in the teaching of Project Charlie and commissioned to carry out the independent evaluation" |
| Methods | RCT | |
| Participants | A total of 604 participants, 335 9th grade and 269 11th grade students from a suburban high school in northeast Florida, participated in this study | |
| Interventions | Experimental: Project Sport The project consisted of a brief consultation and in‐person health behaviour screen, a one‐on‐one consultation, a take‐home fitness prescription targeting adolescent health promoting behaviours and alcohol use risk and protective factors, and a flyer reinforcing key content provided during the consultation mailed to the home. These brief prevention technologies Deliverer: project staff Passive modality N of sessions: 1 Booster: no Duration of the intervention: 1 day Control group: minimal intervention consisting of a wellness brochure provided in school and a pamphlet about teen health and fitness mailed to the home (n = 302) | |
| Outcomes | Drug use behaviours measured included 30‐day frequency of cigarette smoking and marijuana use, paralleling the alcohol frequency measure. Similarly, measures of cigarette and marijuana stage of initiation were taken, which also corresponded to the measure of alcohol use initiation. Mediators evaluated only for alcohol | |
| Notes | Outcome assessed at 3 and 12 months after the end of the intervention Attrition: 15% at 12 months | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A randomised controlled trial was conducted, with participating students randomly assigned within grade levels (9th and 11th grades) by computer to either the intervention or control group |
| Allocation concealment (selection bias) | Low risk | A randomised controlled trial was conducted, with participating students randomly assigned within grade levels (9th and 11th grades) by computer to either the intervention or control group |
| Incomplete outcome data (attrition bias) | Unclear risk | Attrition analyses showed that at 12‐month follow‐up, 85% of the sample was successfully maintained (n = 514), with comparable numbers of missing adolescents equally distributed across the intervention (n = 42) and control (n = 48) groups. A comparison of participants who dropped from the study in each group at 12‐months was conducted using baseline data. No differences were found between drop‐outs in the 2 groups on any of the alcohol and drug consumption measures, or exercise behaviour measures. Also, no differences were found between drop‐outs by group on any of the socio‐demographic measures with one exception regarding parental alcohol use |
| Similarity of groups at baseline | Low risk | No differences were found on any of the socio‐demographic measures between groups with one exception. A greater proportion of control adolescents (42.7%) reported a family alcohol or drug problem, than intervention adolescents (34.9%), Chi² = 3.89, 1 df, P value = 0.05 |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | RCT | |
| Participants | 42 3rd grade children in a public school in a rural community of southwestern Virginia (USA) | |
| Interventions | Experimental: 1. Rehearsal‐plus. Children were taught specific drug refusal techniques and appropriate social skills, and were provided a rationale for each response (n = 15) Social influence approach 2. Children in the traditional condition received instruction derived from a "Just to say no" drug programme, based on discussions about peer pressure situations, different ways of saying no and informal practice (n = 15) Social influence approach Deliverer: project staff Interactive modality N of sessions: 2 Booster: no Duration of the intervention: 2 days Control group: members received more formalised lecture and discussion‐based instruction on drug abuse, without discussing the subject of peer pressure (n = 12) Knowledge‐based approach | |
| Outcomes | Knowledge | |
| Notes | Outcome assessed at post‐test Short‐term evaluation | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "children were randomly assigned to one of three experimental conditions" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | No loss to follow‐up |
| Similarity of groups at baseline | Unclear risk | Information not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | RCT | |
| Participants | 74 3rd grade children from a primarily lower middle‐class neighbourhood attending an elementary school in southwestern Virginia (USA), school year not specified | |
| Interventions | Experimental: Students were randomly assigned to 1 of 3 conditions Deliverer: psychology majors Interactive modality N of sessions: 3 Booster: no Duration of the intervention: 3 days Control: children received drug education only after they received post assessment, n = 26 students | |
| Outcomes | Decision making, rationale, drug knowledge, assertiveness, general knowledge and behavioural skills | |
| Notes | Outcome assessed at post‐test (at the end of the intervention) and at follow‐up (4 weeks after the intervention, only participants in experimental conditions) Analysis sample at post‐test n = 57, n intervention group = R+ 22, GI 16, n control group = 19 Attrition: 23%: 8.3% in group A, 30% in group B, 27% in group C Data suitable for inclusion in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "subjects were randomly assigned to one of three groups" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | High risk | Significant differences in drop‐out across groups |
| Similarity of groups at baseline | Low risk | Multivariate analysis of pretest variables revealed no significant differences between groups |
| Blinding of outcome assessment (detection bias) | High risk | Quote: "ten psychology majors who served as trainers and 11 others who served as assessors were responsible for teaching drug education in the experimental condition" |
| Methods | RCT | |
| Participants | 34 3rd grade children from a primarily lower middle‐class neighbourhood attending an elementary school in a rural community of southwestern Virginia (USA), school year not specified | |
| Interventions | Experimental: Students were randomly assigned to 1 of 3 conditions: Social competence approach Deliverer: psychology majors Interactive modality N of sessions: 3 Booster: no Duration of the intervention: 3 days Control: no training, n = 8 students | |
| Outcomes | Decision making, rationale, drug knowledge, assertiveness, general knowledge and behavioural skills | |
| Notes | Outcome assessed at post‐test (at the end of the intervention) Analysis sample at post‐test not reported, n intervention group not reported, n control group not reported Attrition: 0% Data suitable for inclusion in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "children were randomly assigned to one of three experimental condition" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | No loss to follow‐up |
| Similarity of groups at baseline | Unclear risk | Information not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | RCT | |
| Participants | 1575 students, 5th grade through 9th grade; New York, USA. September 1980 to June 1981 | |
| Interventions | Experimental: 5 broad categories of prevention programmes were analysed Social competence focused, n = 260 Social competence focused, n = 377 Other type of intervention, n = 433 Deliverer: not reported Modality: passive for the knowledge‐focused, not reported for the other types of interventions N of sessions: not reported Booster: no Duration of the intervention: 6 months Control group: n = 299 | |
| Outcomes | Alcohol, marijuana, psychedelics, CNS stimulants, CNS depressants, glue, solvents and spray abuse were assessed using a modified version of the New York State survey of substance abuse, the Periodic Assessment of Drug Abuse among Youth | |
| Notes | Outcome assessed at post‐test Attrition: not reported No data suitable for inclusion in the meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Quote: "One‐sixth of students were then assigned at random to the control group in each program. Control students from all programs were combined in analysis, to form one cross‐model control group. This procedure resulted in random assignment to prevention and control condition within each model but not across model. Random assignment to program was not an option open to researchers " |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Unclear risk | Information not reported |
| Similarity of groups at baseline | Unclear risk | Information not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | RCT | |
| Participants | 363 students, 3rd grade through 6th grade, from 24 classrooms in 4 metropolitan Catholic schools, USA. School year not specified | |
| Interventions | Experimental: 4 knowledge‐focused curricula were implemented Each child listened to the assigned curriculum on a personal tape recorder, using headphones, while following along in a workbook. One researcher was randomly assigned to oversee each group Knowledge‐based approach n = not reported Deliverer: project staff Passive modality N of sessions: 3 Booster: no Duration of the intervention: 3 days | |
| Outcomes | Knowledge about dangerous effect of cocaine; intention to use cocaine | |
| Notes | Outcome assessed 10 days after the intervention Attrition at post‐test: 7.2%. Analysis sample n = 337 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Children were randomly assigned to four intervention groups, within each of the 19 same grade groupings." |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | Information not reported but attrition rate is low |
| Similarity of groups at baseline | Low risk | Quote: "chi square analysis indicated no association between curriculum group and sex, grade or ethnicity. One way ANOVAs indicated no significant differences among the four curriculum groups in family socioeconomic index and mother's education" |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | Cluster‐RCT: schools are the unit of assignment | |
| Participants | 34 middle schools (n = 7426 consented 6th graders, 71% of the eligible population) were recruited from 4 school districts in 3 major metropolitan areas of the USA during the fall and winter of 1997 to 1998 | |
| Interventions | Experimental: Lions–Quest 'Skills for Adolescence' (SFA) utilises a comprehensive array of strategies to teach social competency and refusal skills Social competence approach Deliverer: teacher n = not reported Modality: not reported N of sessions: 40 sessions during 7th grade Booster: no Duration of the intervention: 12 months Control: standard interventions, n = not reported | |
| Outcomes | Tobacco, alcohol and illegal drug use prevalence rates Behavioural intentions, social influences, interpersonal perceptions, perception of harmful effects of drugs, and communication skills and self efficacy around drug use refusal The main focus of this report is the change in prevalence of substances used over the 1‐year study interval from baseline through the end of the intervention year | |
| Notes | Outcome assessed at post‐test (at the end of the intervention) and at 12 months after the end of the intervention Analysis sample at post‐test = 6239, n intervention group not reported, n control group not reported No data suitable for meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | School districts and middle schools were recruited via a 2‐stage cluster sampling plan |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Incomplete outcome data (attrition bias) | Low risk | Outcome analyses were conducted using a conservative 'intent to treat' approach, i.e. students in each condition were retained in the analyses based on their 7th grade school assignment and without regard to amount of programme exposure |
| Similarity of groups at baseline | Low risk | The baseline analysis indicated an overall 30‐day prevalence rate of 14% for a composite measure of 'any drug use' (no/yes) and that the 17 SFA and the 17 control schools were equivalent with respect to self reported drug use prior to the 7th grade SFA intervention programme (14% versus 14%) |
| Blinding of outcome assessment (detection bias) | Low risk | With few exceptions, the data collectors were blind to each school's treatment condition |
| Methods | Cluster‐RCT | |
| Participants | 2863 7th grade students from 44 junior high school complexes in the Los Angeles Unified School District (USA) | |
| Interventions | Experimental 1: Project SMART (Self Management and Resistance Training). Affective curriculum. The affective programme focused on personal decision‐making, values clarification and stress management techniques (n = not reported) Social competence approach Social influence approach Deliverer: teacher and project staff + peer leader assistant Interactive modality N of sessions: 12 Booster: no Duration of the intervention: not reported Control condition: no intervention (n = not reported) | |
| Outcomes | Pre‐ and post‐test data were collected using specific questionnaires and by the collection of saliva specimens Marijuana use: lifetime use, 30 days use, 7 days use, customary use | |
| Notes | Outcome assessed at 12 and 24 months after the initiation of the intervention No data suitable for inclusion in the meta‐analysis: the absolute numbers of participants in the groups are not given Authors contacted: data no longer available | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "schools were randomly assigned to experimental or control conditions using a multi attribute approach to enhance comparability" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | Quote: "there was differential attrition by condition at first follow‐up assessment (p: 0,008) and at the final follow‐up (p< 0.0001). However the differential attrition among conditions appears to be mitigated by the fact that this attrition was not related to substance use" |
| Similarity of groups at baseline | High risk | Quote: "there were significant differences between social curriculum and control subjects in alcohol use and tobacco use but not for marijuana" |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | Cluster‐RCT | |
| Participants | 3027 7th grade students from 12 junior high school in Los Angeles and Orange Counties, California (USA). School year 1987 to 1988 | |
| Interventions | Experimental: Social competence approach Social influence approach Deliverer: project staff Interactive modality N of sessions: 9 Booster: no Duration of the intervention: not reported Control group: information (ICU) on social and health consequences of using alcohol and other drugs: knowledge‐focused, n = 32 classrooms Number of sessions: 4 | |
| Outcomes | Marijuana (lifetime use; past 30 days use) | |
| Notes | Outcome assessed at 1 and 2 years after initiation of the intervention Attrition: 22% at 1‐year follow‐up | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "schools were stratified by size, tests scores and ethnic compositions and then randomly assigned to receive one of the four interventions" |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | High risk | Information about distribution of drop‐out from the study across groups not reported |
| Similarity of groups at baseline | Unclear risk | Information not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | Cluster‐RCT A multilevel or hierarchical logistic model was used to adjust for the intra‐cluster correlation and to describe attrition | |
| Participants | 19,220 7th grade students from 83 schools from 6 metropolitan areas in the USA. Academic year not specified. Included in the study only the 17,300 students for which baseline data were available | |
| Interventions | Experimental: Take Charge of Your Life Program (TCYL): focused on demonstrating to students that there are personal, social and legal risks and consequences of alcohol, tobacco and marijuana use, that the belief that "everybody does it" are not congruent with reported usage data from national studies. The programme also provided students with life skills such communication, decision‐making, assertiveness and refusal skills Combined (social influence + social competence) approach n = 10,028 Deliverer: project staff Interactive modality N of sessions: 10 lessons in 7th grade and 7 in 9th grade Booster: yes Duration of the intervention: overall over 2 school years, n of months not reported Control group: no intervention, n = 7302 | |
| Outcomes | Substance use: marijuana use for the 30 days and 12 months prior to survey | |
| Notes | Outcome assessed at post‐test, 12 and 24 months after the end of the intervention Attrition at post‐test: 1%, at 9th grade post‐test: 35%, at 2 years follow‐up: 47% | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Cluster‐randomisation. Schools were the unit of randomisation |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Low risk | Attrition analysis by adjusted logistic regression. Drop‐outs were more likely to be older, non‐white, users of alcohol, marijuana and tobacco. Differential attrition across condition was noted for race/ethnicity with those coded as "other" race being more likely to be in the control condition |
| Similarity of groups at baseline | Low risk | Quote: "at baseline demographic characteristics and substance use of treatment and control groups were comparable" |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
| Methods | Cluster (community) randomised | |
| Participants | 1216 students from 5th to 6th grade enrolled from the school systems of 14 frontier, isolated, rural communities in Alaska, during the 2006 to 2007 school years. 658 were eligible for the survey | |
| Interventions | Experimental: the Think Smart curriculum is a modified form of the Personal Intervention Curriculum, which is based on an abstinence‐based prevention model developed by Stephen Schinke for a Pacific Northwest American Indian population, that include sessions on stereotypes and drug facts and an introduction of a problem‐solving model known as SODAS (Stop, Options, Decide, Act, Self‐Talk), which emphasises refusal and self assertiveness skills. The stereotypes session addresses the concept of peer norms and cultural identify Social competence approach Deliverer: teacher n = not reported Interactive modality N of sessions: 12 sessions + 3 booster sessions during 5th to 6th grades Booster: yes, 3 sessions 2 to 3 months after the intervention Duration of the intervention: 6 months Control: not reported, n = not reported | |
| Outcomes | 30‐day use of tobacco, alcohol, marijuana, hashish and various legal substances Knowledge of drug and consequences, assertiveness skills, cultural identity, peer use of harmful legal products, peer normative beliefs about HLPs | |
| Notes | Outcome assessed at post‐test (at the end of the intervention, in May 2007) and at 6 months after the end of the intervention (in 6th to 7th grades, in fall 2007) Analysis sample not reported, n intervention group not reported, n control group not reported Attrition: not reported Data presented with beta and SE No data suitable for inclusion in the meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Following the matching, a Microsoft Excel spreadsheet was generated using its automatic function “RAND” to finalize the assignment of the communities in the experimental and control conditions. One control group community dropped out of the study; therefore, we also dropped the matched intervention community, reducing the number of communities available for the outcome assessment to 14 communities." "These analyses explore the possibility that the a priori pairwise random assignment of communities to intervention and comparison group may be systematically different on a larger set of community |
| Allocation concealment (selection bias) | Low risk | Quote: "Following the matching, a Microsoft Excel spreadsheet was generated using its automatic function “RAND” to finalize the assignment of the communities in the experimental and control conditions. One control group community dropped out of the study; therefore, we also dropped the matched intervention community, reducing the number of communities available for the outcome assessment to 14 communities." |
| Incomplete outcome data (attrition bias) | Low risk | Quote: "The one characteristic on which droppers and stayers differed is that Caucasians were more likely to leave the study at both post‐test and follow‐up. However, the magnitude of this difference was not impressive at post‐test (d = 0.32) or follow‐up (d = 0.24). As a result of these analyses, no further treatment is given to attrition. Missing covariate and mediator of substance‐use data were imputed using the Expectation Maximization (EM) algorithm" |
| Similarity of groups at baseline | Unclear risk | Quote: "Although, in aggregate, the two groups are similar... there is considerable community diversity within each group (e.g., variation in community size, proportion of Alaska Natives, proximity to the larger |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | Cluster‐RCT | |
| Participants | 1587 students from 21 continuation high schools (students who are unable to remain in the regular school system for functional reasons, including substance abuse when reaching high school age), California (USA). October 1994 through May 1995. Age 14 to 19 years | |
| Interventions | Experimental: Project Towards No Drug abuse (TND) Deliverer: health educator Interactive modality N of sessions: 9 lessons in high schools Booster: no Duration of the intervention: 1 month Control group: standard care: n = 7 schools; n = not reported | |
| Outcomes | Marijuana use assessed by a questionnaire (past 30 days use) Hard drug use (past 30 days use) | |
| Notes | Outcome assessed at post‐test, 12 and 48 months follow‐up after the end of programme Attrition at 1 year: 23%. Analysis sample n = 1074 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "schools were blocked by estimates of drug use prevalence, ethnic composition of the school and the community, student enrolment and standardized achievement test scores, and were randomly assigned by block to one of the three experimental conditions." |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Unclear risk | Quote: "there were no statistically significant differences od any assessed variables between subjects assessed only at pretest and those assessed at pretest and at post test"; not reported if % of attrition significantly differed between groups randomised to different interventions |
| Similarity of groups at baseline | Low risk | Quote: "no statistical evidence that would indicate that the condition systematically varies n any of the pretest measures beyond random error was found, indicating successful randomisation" |
| Blinding of outcome assessment (detection bias) | Unclear risk | Quote: "data collection was conducted by project staff who were not responsible for instruction of that particular set of students" |
| Methods | Cluster‐RCT | |
| Participants | 1208 9th, 10th and 11th grade students in general high schools in Los Angeles (USA) | |
| Interventions | Experimental: Project Towards No Drug abuse (TND) Combined approach Deliverer: health educator Interactive modality N of sessions: 9 lessons in high schools Booster: no Duration of the intervention: 3 weeks Control group: standard care condition, n = not reported | |
| Outcomes | A school‐wide pretest survey was conducted at each of the 26 classrooms immediately before the programme implementation and 1 year later Marijuana use assessed by a questionnaire (past 30 days use) | |
| Notes | Outcome assessed at 12 months follow‐up (after the end of the intervention) Attrition at 1 year: 37.1%. Analysis sample n = 679 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Information not provided. Classrooms were the unit of allocation and analysis |
| Allocation concealment (selection bias) | Unclear risk | Information not provided |
| Incomplete outcome data (attrition bias) | Low risk | Attrition analysis revealed no statistically significant difference for drug use at baseline and demographic characteristics between pretest sample and sample not lost at follow‐up |
| Similarity of groups at baseline | Low risk | Quote: "no statistical evidence was found that would indicate that the condition groups systematically varied on any of the pretest measures indicating successful randomisation" |
| Blinding of outcome assessment (detection bias) | Unclear risk | Quote: "project staff previously unknown to the student assessed outcomes"; not clear if the project staff knew to which group the participant has been allocated |
| Methods | Cluster‐RCT | |
| Participants | 1037 students from 18 continuation high school (students who are unable to remain in the regular school system for functional reasons, including substance abuse when reaching high school age), South California (USA). October 1997 through May 2000 | |
| Interventions | Experimental: Project Towards No Drug abuse (TND) Deliverer: health educator Interactive modality N of sessions: 12 lessons in high schools Booster: no Duration of the intervention: 1 month Control group: standard care, n = not reported | |
| Outcomes | Marijuana use (past 30 days use); hard drug use (past 30 days use) A school‐wide pretest survey was conducted at each of the 18 schools immediately before the programme implementation and 1 year later | |
| Notes | Outcome assessed at 12 and 24 months follow‐up Attrition at 2 years: 44.6%. Analysis sample n = 575 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Selected schools were blocked by estimates of drug use prevalence, ethnic composition of the school and the community, student enrolment and standardized achievement test scores, and were randomly assigned by block to one of the three experimental conditions. Linear composite scores composed of these variables were created for each school; adjacent scores were used to form six triplets that then were randomly assigned to condition." |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | Unclear risk | Quote: "there were no statistically significant differences od any assessed variables between subjects assessed only at pretest and those assessed at pretest and at post test"; not reported if % of attrition significantly differed between groups randomised to different intervention |
| Similarity of groups at baseline | Unclear risk | Information not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Quote: "data collection was conducted by project staff who were not responsible for instruction of that particular set of students" |
| Methods | Cluster‐RCT High schools in Southern California (n = 18) were randomly assigned to 1 of 3 conditions: cognitive perception information curriculum, cognitive perception information + behavioural skills curriculum or standard care (control) | |
| Participants | A total of 3908 high school students were enrolled in the classrooms selected for participation in the study. Access was | |
| Interventions | Experimental: Project Towards No Drug abuse (TND) Deliverer: health educator + teacher Interactive modality N of sessions: 12 lessons in high schools Booster: no Duration of the intervention: 1 month Control group: standard care: n = not reported | |
| Outcomes | Marijuana use (past 30 days use); hard drug use (past 30 days use) | |
| Notes | Duration of the intervention: Outcome assessed at 12 months follow‐up, end of the intervention Attrition: 32.5% at 12 months Data reported as OR. No data suitable for meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Blocked randomisation |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Incomplete outcome data (attrition bias) | Unclear risk | Quote: "Among the twelve comparisons, five statistically significant differences were detected. Compared to the lost‐to‐followup sample, the retained sample was slightly younger (15.7 versus 15.9 years of age), less likely to smoke cigarettes (21.9% versus 26.4%), less likely to be male (52.9% vs. 61.0%), less likely to be African American (7.2% vs. 10.4%) and more likely to be Latino (65.7% vs. 61.9%), and more likely to live with both parents (59.4% versus 49.3%). Although the retention rate was found to be significantly lower among CHS (64.6%) vs. RHS (80.4%) students, it did not differ across programme conditions (73.0% in Control, 73.5% in Cognitive Only, and 71.1% in Combined)." |
| Similarity of groups at baseline | Low risk | The data show that cross‐condition comparability was achieved for age, gender, programme provider, attrition rate and the 4 drug use outcomes |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Methods | Cluster‐RCT At the analysis stage a multilevel modelling approach was used in order to take into account the hierarchical structure of the data and the cluster effect | |
| Participants | 7079 junior high school students from 170 schools (12 to 14 years old) in Austria, Belgium, Germany, Greece, Italy, Spain and Sweden. Pretest data collected during September to October 2004. 2 schools dropped out after baseline survey, 1 from the control arm and 1 from the intervention arm. Post‐test survey completed with 6604 students | |
| Interventions | Experimental: Project UNPLUGGED. Comprehensive social influence approach incorporating components of critical thinking, decision‐making, problem‐solving, creative thinking, effective communication, interpersonal relationship skills, self awareness, empathy, coping with emotions and stress, normative belief, knowledge about the harmful effect of drugs Group 1. Basic arm, n = 1190 Group 2. Parent arm: parents invited to participate in 3 workshops, n = 1164 Group 3. Peer arm: 2 students per class had the task to conduct short meetings with their classmates, n = 1193 Combined (social influence + social competence) approach Deliverer: teacher + peer Interactive modality N of sessions: 12 Booster: no Duration of the intervention: 3 months Control group: no intervention, n = 3532 | |
| Outcomes | Use of any drugs and cannabis measured as any use in the past 30 days. Changes in knowledge, intention to use | |
| Notes | Outcome assessed at 3 months and 12 months after the end of the intervention Attrition at post‐test: 3.5%; at 12 months follow‐up: 28.2% | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Cluster‐randomised trial. The randomisation was stratified by socio‐economic level |
| Allocation concealment (selection bias) | Low risk | Central randomisation |
| Incomplete outcome data (attrition bias) | Low risk | Quote: "to assess the possible attrition bias we analysed the program effect after carrying forward the outcome status last assessed. Also, we repeated the analysis according to the best case‐worst case scenario. In the first case all non participating were considered non users, in the second case they were considered users" |
| Similarity of groups at baseline | Low risk | Quote: "significant differences in the prevalence of some substance use between intervention and control group were detected. It appeared to be due to the inclusion among control schools to one school with an unusually high prevalence of substance use. After excluding this school the baseline prevalence was very similar across groups" |
| Blinding of outcome assessment (detection bias) | Low risk | Self completed anonymous questionnaire |
| Methods | Cluster‐RCT | |
| Participants | 1874 participants 6th grade, 74 schools Czech Republic | |
| Interventions | Experimental intervention: Unplugged focuses on knowledge and attitudes (4 units), interpersonal skills (4 units) and intrapersonal skills (4 units), n = 1022 Combined (competence + influence) approach Deliverer: teacher Interactive Number of sessions: 12 Booster: no Duration of intervention: 1 school year (10 months) | |
| Outcomes | Self reported use of legal substances and cannabis in the past 30 days, self reported lifetime illegal drug use (ever used any of marijuana, heroin, amphetamine, ecstasy, LSD or hallucinogens, GHB or tranquillisers without a medical prescription) | |
| Notes | Outcome assessed at post‐test, 3, 12, 15, 24 months Attrition at: Post‐test: experimental 12%, control 9.27% 3 months: experimental 6.46%, control 0% 12 months: experimental 5.77%, control 0% 15 months: experimental 7.2%, control 0.7% Final wave (24 months): experimental: 10.57%, control: 1.5% Data for inclusion in meta‐analysis provided by authors | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Information not reported |
| Allocation concealment (selection bias) | Unclear risk | Information not reported |
| Incomplete outcome data (attrition bias) | High risk | Higher attrition in the experimental group and unbalanced |
| Similarity of groups at baseline | Low risk | No statistically significant differences in demographic characteristics (sex, age, family income level) between the experimental and the control groups at baseline period. At baseline, the experimental group showed no statistically significant differences in substance use as compared to the control group, after the correction for number of tests |
| Blinding of outcome assessment (detection bias) | Unclear risk | Information not reported |
ADM: Adolescent Decision‐Making programme
ASAP: Alcohol and Substance Abuse Prevention programme
ATD: Alcohol/Tobacco/Drug use/abuse programme
CHARLIE: Chemical Abuse Resolution Lies in Education project
CNS: central nervous system
DARE: Drug Abuse Resistance Education project
GBG: Good Behavior Game project
GHB: gamma‐hydroxybutyric acid
KACM: Keep A Clear Mind project
kiR: 'keepin' it REAL' project
LST: Life Skills Training
OR: odds ratio
RCT: randomised controlled trial
SE: standard error
SES: socioeconomic status
SMART: Self Management and Resistance Training project
TCYL: Take Charge of Your Life project
TND: Towards No Drug (abuse) project
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
| RCT. Randomisation failed: selection of schools to be enrolled occurred after the assignment of the intervention. No attempt to control for confounding variables at the analysis stage | |
| No random allocation | |
| Controlled, non‐randomised, prospective study | |
| Not exclusively school‐based | |
| DARE project | |
| Schools selected on the basis of drug use risk | |
| Excluded because primary outcome is transition from pattern drug use to another, and not incidence of use. Moreover, it seems that randomisation is subject and not class‐based, with a high suspicion of contamination. Finally, high attrition (25%) suggests a high risk of bias | |
| Controlled, non‐randomised, prospective study | |
| Controlled, non‐randomised, prospective study | |
| RCT. Follow‐up analysis of a sub‐sample of the original study ( LST 1990, Botvin 1995, included): only 447 students out of 3597 participating in the original study completed the drug use questionnaire | |
| RCT. Unclear attrition rate. No useful measures investigating drug use. Some evidence of failure of the randomisation procedure | |
| RCT | |
| Effects of illegal drugs not measured because of the low percentage of users at this age | |
| Effects of illegal drugs not measured because of the low percentage of users at this age | |
| Selective prevention programme | |
| Longitudinal follow‐up of a RCT population | |
| Outcome not assessed in the target population | |
| Substance use not assessed | |
| Selective programme | |
| Controlled, non‐randomised, prospective study | |
| Participants are already users | |
| Controlled, non‐randomised, prospective study | |
| RCT. The units of randomisation were too limited to assure the validity of the method. No confounding adjustment at the analysis stage. No data are presented for drug use or mediating variables | |
| Controlled, non‐randomised, prospective study | |
| Unclear randomisation procedure. Process evaluation; high attrition rates (54%). No measure useful for the review | |
| Controlled, non‐randomised, prospective study | |
| RCT. Unclear methods of analysis; initial random assignment to the groups was not taken into account at the analysis stage | |
| Controlled, non‐randomised, prospective study | |
| RCT. No criteria for selecting students were presented. Intervention consisted of the broadcast of an interactive CD during a morning session. Post‐test was carried out the day after the intervention | |
| Substance use not assessed | |
| Controlled, non‐randomised, prospective study | |
| RCT. Analysis of 3 cohorts (1989, 1990, 1991 school years); the programme offered was different for the third cohort. The experimental conditions were merged at the analysis stage. Some evidence of failed randomisation. The second paper (Thompson 1997) compared late versus early cohort effects | |
| No behavioural outcomes | |
| Controlled, non‐randomised, prospective study | |
| Life Skills Training programme modified | |
| SMART Project | |
| Substance use not assessed | |
| The programme targeted a particular population | |
| Focused on coaching as a means to improve the quality with which teachers implemented All Star curriculum | |
| Substance use not assessed | |
| SMART 1990 Project | |
| Controlled, non‐randomised, prospective study | |
| RCT. Secondary analysis of a sub‐sample of the original study (LST 001, Botvin 2001, included), based on risk level | |
| Indicated prevention programme | |
| Controlled, non‐randomised, prospective study | |
| Pilot study for the All Stars Plus programme. Controlled, non‐randomised, prospective study | |
| No focused on drug use | |
| Controlled, non‐randomised, prospective study | |
| Observational study | |
| No behavioural outcomes | |
| Controlled, non‐randomised, prospective study | |
| Controlled, non‐randomised, prospective study | |
| Outcome measures did not meet the inclusion criteria | |
| RCT. Unclear methods; some evidence of randomisation failure. High attrition rates (51%) | |
| Selected population | |
| Not substance use assessed | |
| Controlled, non‐randomised, prospective study | |
| Controlled, non‐randomised, prospective study | |
| Schools selected on the basis of drug use risk | |
| Participants did not meet the inclusion criteria: high‐risk population | |
| PRIDE Project | |
| Controlled, non‐randomised, prospective study | |
| No focused on drug use | |
| Controlled, non‐randomised, prospective study | |
| Controlled, non‐randomised, prospective study | |
| Controlled, non‐randomised, prospective study | |
| No behavioural outcomes | |
| Controlled, non‐randomised, prospective study | |
| Quasi‐experimental study. The randomisation procedure was applied only to a sub‐sample of the study population. Inadequate control for confounding variables at the analysis stage | |
| Not focused on substance use | |
| Selective prevention programme | |
| Longitudinal follow‐up of a RCT population | |
| RCT. No results were presented for control group | |
| Midwestern Prevention Project | |
| Controlled, non‐randomised, prospective study | |
| EARLY ALLIANCE Prevention Trial | |
| Selected population | |
| Controlled, non‐randomised, prospective study | |
| Selective prevention programme | |
| Focused on coaching as a means to improve the quality with which teachers implemented All Star curriculum | |
| Not focused on substance use | |
| KICK Project | |
| Controlled, non‐randomised, prospective study | |
| Controlled, non‐randomised, prospective study | |
| Controlled, non‐randomised, prospective study | |
| Type of outcomes assessed | |
| The programme targeted a particular population | |
| RCT. Students enrolled in the study were Native Americans from reservations in USA; the programme was focused on Native American culture, values and traditions | |
| Selective prevention programme | |
| RCT. Randomisation failed. No control for confounding variables at the analysis stage. Unclear attrition rates | |
| Participants assigned to intervention and control group are subsamples of different population groups | |
| Controlled, non‐randomised, prospective study | |
| RCT. Secondary analysis of a sub‐sample of the original study (ADM 1992, Gersick 1988, included), based on students' family household status | |
| Prescription drugs | |
| Controlled, non‐randomised, prospective study | |
| Family intervention carried out in the school | |
| Schools selected on the basis of high drug use risk of students | |
| Substance use not assessed | |
| Selective prevention programme | |
| Controlled, non‐randomised, prospective study. No random allocation | |
| Controlled, non‐randomised, prospective study | |
| Urban Youth Connection | |
| RCT. Randomisation failed. No control for confounding variables at the analysis stage | |
| Selective prevention programme | |
| Intervention focused only on prevention of alcohol abuse | |
| Intervention not realised in a school setting | |
| Controlled, non‐randomised, prospective study |
DARE: Drug Abuse Resistance Education project
RCT: randomised controlled trial
Characteristics of studies awaiting assessment [ordered by study ID]
| Methods | Prospective RCT |
| Participants | Approximately 500 4th to 5th grade students (5 schools, 27 classrooms) from inner city Cleveland |
| Interventions | Healthy Futures Initiative: 10‐week curriculum |
| Outcomes | Knowledge, behaviour, minutes of physical activity, BMI measurement, substance use |
| Notes | — |
| Methods | RCT |
| Participants | 1st to 3rd grade students from 12 schools |
| Interventions | Whole Day First Grade Program (WD) had a multilevel structure and aimed at 2 early antecedents drug abuse and other problem behaviours (aggressive, disruptive behaviour and poor academic achievement) |
| Outcomes | Skills and aggressive behaviour, children’s learning |
| Notes | — |
| Methods | Randomised pretest and post‐test comparative design |
| Participants | 107 Thai high school students from 7th to 12th grade |
| Interventions | Life skills training programme (LST) provided information and skills specifically related to drug and tobacco use. 10 class periods |
| Outcomes | Knowledge level; attitude toward tobacco and drug use prevention; refusal, decision‐making and problem‐solving skills; frequency |
| Notes | — |
BMI: body mass index
RCT: randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
| Trial name or title | E‐health4Uth |
| Methods | E‐health4Uth and E‐health4Uth combined with personal counselling (E‐health4Uth+counselling). 3‐armed cluster‐RCT |
| Participants | 4th grade students from the Netherlands |
| Interventions | E‐health4Uth involves internet‐based, tailored health messages focused on 9 topics related to heath behaviour and well‐being. Students in the E‐health4Uth + counselling group are also invited for an appointment to see the nurse when they are at risk of mental health problems |
| Outcomes | Primary: health behaviour (alcohol, drugs, smoking, safe sex) and mental status Secondary: health‐related quality of life |
| Starting date | Not reported |
| Contact information | — |
| Notes | — |
| Trial name or title | Not reported |
| Methods | Cluster‐RCT |
| Participants | 7th to 10th grade students from 32 schools in disadvantaged areas |
| Interventions | Comprehensive resilience intervention |
| Outcomes | Primary: tobacco, alcohol, marijuana and other illicit drug use |
| Starting date | Not reported |
| Contact information | — |
| Notes | — |
| Trial name or title | Drug education in Victorian schools (DEVS) |
| Methods | Cluster‐RCT |
| Participants | 1746 junior high school students (aged 13 to 15 years) in 21 Victorian secondary schools over a period of 3 years |
| Interventions | Comprehensive, evidence‐based, harm reduction‐focused school drug education programme. Comprises 10 lessons in year 8 (13 to 14‐year olds) and 8 in year 9 (14 to 15‐year olds) that address issues around the use of alcohol, tobacco, cannabis and other illicit drugs |
| Outcomes | Knowledge, patterns and context of use, attitudes and harms experienced in relation to alcohol, tobacco, cannabis and other illicit drug use |
| Starting date | Not reported |
| Contact information | — |
| Notes | — |
| Trial name or title | CAP (Climate and Preventure) intervention |
| Methods | Cluster‐RCT |
| Participants | 24 Australian schools |
| Interventions | CAP (Climate and Preventure) intervention combines the 'universal' Climate and 'indicated' Preventure programmes. A comprehensive approach to substance use |
| Outcomes | Drug knowledge, drug use, related harms and mental health symptoms |
| Starting date | Not reported |
| Contact information | — |
| Notes | — |
| Trial name or title | CAP (Climate and Preventure) intervention |
| Methods | Cluster‐RCT |
| Participants | Students aged 13 to 14 years old from 27 secondary schools in New South Wales and Victoria, Australia |
| Interventions | The CAP study is an integrated approach to alcohol misuse prevention, which combines the effective universal internet‐based Climate Schools programme with the effective selective personality‐targeted Preventure programme |
| Outcomes | Primary: the uptake and harmful use of alcohol and alcohol‐related harms. Secondary: alcohol and cannabis‐related knowledge, cannabis‐related harms, intentions to use and symptoms of mental health |
| Starting date | Not reported |
| Contact information | — |
| Notes | — |
RCT: randomised controlled trial
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Marijuana use < 12 months Show forest plot | 4 | 9456 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.81, 1.01] |
| Analysis 1.1  Comparison 1 Social competence versus usual curricula, Outcome 1 Marijuana use < 12 months. | ||||
| 2 Marijuana use < 12 months Show forest plot | 1 | 3417 | Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐0.20, ‐0.00] |
| Analysis 1.2  Comparison 1 Social competence versus usual curricula, Outcome 2 Marijuana use < 12 months. | ||||
| 3 Marijuana use ≥ 12 months Show forest plot | 1 | 2678 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.74, 1.00] |
| Analysis 1.3  Comparison 1 Social competence versus usual curricula, Outcome 3 Marijuana use ≥ 12 months. | ||||
| 4 Marijuana use ≥ 12 months Show forest plot | 1 | 1075 | Mean Difference (IV, Fixed, 95% CI) | ‐0.02 [‐0.10, 0.06] |
| Analysis 1.4  Comparison 1 Social competence versus usual curricula, Outcome 4 Marijuana use ≥ 12 months. | ||||
| 5 Hard drug use < 12 months Show forest plot | 1 | 2090 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.69 [0.40, 1.18] |
| Analysis 1.5  Comparison 1 Social competence versus usual curricula, Outcome 5 Hard drug use < 12 months. | ||||
| 6 Hard drugs use ≥ 12 months Show forest plot | 1 | 1075 | Mean Difference (IV, Fixed, 95% CI) | ‐0.01 [‐0.06, 0.04] |
| Analysis 1.6  Comparison 1 Social competence versus usual curricula, Outcome 6 Hard drugs use ≥ 12 months. | ||||
| 7 Other drug use < 12 months Show forest plot | 1 | 1270 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.53, 0.98] |
| Analysis 1.7  Comparison 1 Social competence versus usual curricula, Outcome 7 Other drug use < 12 months. | ||||
| 8 Other drugs use < 12 months Show forest plot | 1 | 3434 | Mean Difference (IV, Fixed, 95% CI) | ‐0.05 [‐0.11, 0.01] |
| Analysis 1.8  Comparison 1 Social competence versus usual curricula, Outcome 8 Other drugs use < 12 months. | ||||
| 9 Any drug use < 12 months Show forest plot | 2 | 2512 | Risk Ratio (M‐H, Random, 95% CI) | 0.27 [0.14, 0.51] |
| Analysis 1.9  Comparison 1 Social competence versus usual curricula, Outcome 9 Any drug use < 12 months. | ||||
| 10 Any drug use < 12 months Show forest plot | 1 | 1566 | Mean Difference (IV, Fixed, 95% CI) | 0.02 [‐0.05, 0.09] |
| Analysis 1.10  Comparison 1 Social competence versus usual curricula, Outcome 10 Any drug use < 12 months. | ||||
| 11 Drug knowledge < 12 months Show forest plot | 4 | 3593 | Std. Mean Difference (IV, Random, 95% CI) | 1.02 [0.11, 1.93] |
| Analysis 1.11  Comparison 1 Social competence versus usual curricula, Outcome 11 Drug knowledge < 12 months. | ||||
| 11.1 Rehearsal plus | 2 | 91 | Std. Mean Difference (IV, Random, 95% CI) | 1.72 [1.19, 2.24] |
| 11.2 Other programs | 2 | 3502 | Std. Mean Difference (IV, Random, 95% CI) | 0.34 [‐0.43, 1.11] |
| 12 Intention to use marijuana < 12 months Show forest plot | 1 | 3417 | Mean Difference (IV, Fixed, 95% CI) | ‐0.12 [‐0.19, ‐0.05] |
| Analysis 1.12  Comparison 1 Social competence versus usual curricula, Outcome 12 Intention to use marijuana < 12 months. | ||||
| 13 Intention to use hard drugs < 12 months Show forest plot | 1 | 3417 | Mean Difference (IV, Fixed, 95% CI) | ‐0.01 [‐0.04, 0.02] |
| Analysis 1.13  Comparison 1 Social competence versus usual curricula, Outcome 13 Intention to use hard drugs < 12 months. | ||||
| 14 Intention to use other drugs < 12 months Show forest plot | 1 | 3417 | Mean Difference (IV, Fixed, 95% CI) | ‐0.04 [‐0.07, ‐0.01] |
| Analysis 1.14  Comparison 1 Social competence versus usual curricula, Outcome 14 Intention to use other drugs < 12 months. | ||||
| 15 Intention to use any drug < 12 months Show forest plot | 1 | 120 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.21 [0.02, 1.84] |
| Analysis 1.15  Comparison 1 Social competence versus usual curricula, Outcome 15 Intention to use any drug < 12 months. | ||||
| 16 Intention to use any drug < 12 months Show forest plot | 1 | 1566 | Mean Difference (IV, Fixed, 95% CI) | 0.04 [‐0.07, 0.15] |
| Analysis 1.16  Comparison 1 Social competence versus usual curricula, Outcome 16 Intention to use any drug < 12 months. | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Marijuana use < 12 months Show forest plot | 3 | 10716 | Risk Ratio (M‐H, Random, 95% CI) | 0.88 [0.72, 1.07] |
| Analysis 2.1  Comparison 2 Social influence versus usual curricula, Outcome 1 Marijuana use < 12 months. | ||||
| 1.1 Alert | 2 | 10138 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.69, 0.97] |
| 1.2 Other programs | 1 | 578 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [0.79, 1.58] |
| 2 Marijuana use < 12 months Show forest plot | 1 | 764 | Mean Difference (IV, Fixed, 95% CI) | ‐0.26 [‐0.48, ‐0.04] |
| Analysis 2.2  Comparison 2 Social influence versus usual curricula, Outcome 2 Marijuana use < 12 months. | ||||
| 3 Marijuana use ≥ 12 months Show forest plot | 1 | 5862 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.81, 1.13] |
| Analysis 2.3  Comparison 2 Social influence versus usual curricula, Outcome 3 Marijuana use ≥ 12 months. | ||||
| 4 Marijuana use ≥12 months Show forest plot | 1 | 764 | Mean Difference (IV, Fixed, 95% CI) | ‐0.22 [‐0.46, 0.02] |
| Analysis 2.4  Comparison 2 Social influence versus usual curricula, Outcome 4 Marijuana use ≥12 months. | ||||
| 5 Other drug use < 12 months Show forest plot | 1 | 5862 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.93, 1.27] |
| Analysis 2.5  Comparison 2 Social influence versus usual curricula, Outcome 5 Other drug use < 12 months. | ||||
| 6 Other drugs use ≥ 12 months Show forest plot | 1 | 5862 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.33 [1.13, 1.57] |
| Analysis 2.6  Comparison 2 Social influence versus usual curricula, Outcome 6 Other drugs use ≥ 12 months. | ||||
| 7 Drug knowledge < 12 months Show forest plot | 1 | 764 | Mean Difference (IV, Fixed, 95% CI) | 1.5 [0.58, 2.42] |
| Analysis 2.7  Comparison 2 Social influence versus usual curricula, Outcome 7 Drug knowledge < 12 months. | ||||
| 8 Drug knowledge ≥ 12 months Show forest plot | 1 | 764 | Mean Difference (IV, Fixed, 95% CI) | 1.65 [0.69, 2.61] |
| Analysis 2.8  Comparison 2 Social influence versus usual curricula, Outcome 8 Drug knowledge ≥ 12 months. | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Marijuana use < 12 months Show forest plot | 3 | 8701 | Risk Ratio (M‐H, Random, 95% CI) | 0.79 [0.59, 1.05] |
| Analysis 3.1  Comparison 3 Combined versus usual curricula, Outcome 1 Marijuana use < 12 months. | ||||
| 1.1 Unplugged | 2 | 8008 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.56, 0.82] |
| 1.2 Other programs | 1 | 693 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.79, 1.14] |
| 2 Marijuana use < 12 months Show forest plot | 1 | 693 | Mean Difference (IV, Fixed, 95% CI) | ‐1.90 [‐5.83, 2.03] |
| Analysis 3.2  Comparison 3 Combined versus usual curricula, Outcome 2 Marijuana use < 12 months. | ||||
| 3 Marijuana use ≥ 12 months Show forest plot | 6 | 26910 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.69, 0.99] |
| Analysis 3.3  Comparison 3 Combined versus usual curricula, Outcome 3 Marijuana use ≥ 12 months. | ||||
| 3.1 Unplugged | 2 | 7321 | Risk Ratio (M‐H, Random, 95% CI) | 0.47 [0.20, 1.11] |
| 3.2 TND | 3 | 2269 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.83, 1.09] |
| 3.3 Other programmes | 1 | 17320 | Risk Ratio (M‐H, Random, 95% CI) | 0.94 [0.89, 1.00] |
| 4 Marijuana use ≥12 months Show forest plot | 1 | 690 | Mean Difference (IV, Fixed, 95% CI) | ‐0.80 [‐4.39, 2.79] |
| Analysis 3.4  Comparison 3 Combined versus usual curricula, Outcome 4 Marijuana use ≥12 months. | ||||
| 5 Hard drug use < 12 months Show forest plot | 1 | 693 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.85 [0.63, 1.14] |
| Analysis 3.5  Comparison 3 Combined versus usual curricula, Outcome 5 Hard drug use < 12 months. | ||||
| 6 Hard drug use < 12 months Show forest plot | 1 | 693 | Mean Difference (IV, Fixed, 95% CI) | ‐3.1 [‐5.90, ‐0.30] |
| Analysis 3.6  Comparison 3 Combined versus usual curricula, Outcome 6 Hard drug use < 12 months. | ||||
| 7 Hard drug use ≥ 12 months Show forest plot | 2 | 1066 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.39, 1.90] |
| Analysis 3.7  Comparison 3 Combined versus usual curricula, Outcome 7 Hard drug use ≥ 12 months. | ||||
| 8 Hard drug use ≥ 12 months Show forest plot | 1 | 690 | Mean Difference (IV, Fixed, 95% CI) | 0.30 [‐1.36, 1.96] |
| Analysis 3.8  Comparison 3 Combined versus usual curricula, Outcome 8 Hard drug use ≥ 12 months. | ||||
| 9 Any drugs use < 12 months Show forest plot | 1 | 6362 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.64, 0.89] |
| Analysis 3.9  Comparison 3 Combined versus usual curricula, Outcome 9 Any drugs use < 12 months. | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Drug knowledge < 12 months Show forest plot | 1 | 165 | Mean Difference (IV, Random, 95% CI) | 0.10 [0.05, 0.15] |
| Analysis 4.1  Comparison 4 Knowledge versus usual curricula, Outcome 1 Drug knowledge < 12 months. | ||||
| 2 Intention to use hard drugs < 12 months Show forest plot | 1 | 165 | Mean Difference (IV, Fixed, 95% CI) | ‐0.05 [‐0.24, 0.14] |
| Analysis 4.2  Comparison 4 Knowledge versus usual curricula, Outcome 2 Intention to use hard drugs < 12 months. | ||||
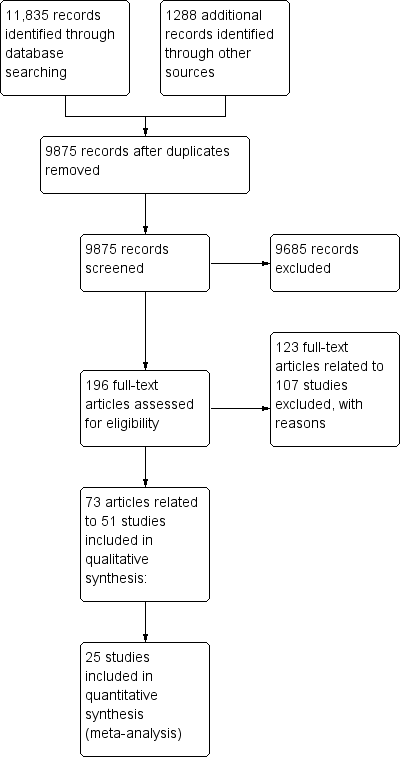
Study flow diagram.

'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.

Comparison 1 Social competence versus usual curricula, Outcome 1 Marijuana use < 12 months.

Comparison 1 Social competence versus usual curricula, Outcome 2 Marijuana use < 12 months.

Comparison 1 Social competence versus usual curricula, Outcome 3 Marijuana use ≥ 12 months.
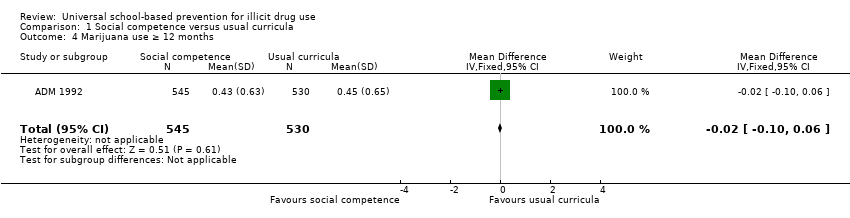
Comparison 1 Social competence versus usual curricula, Outcome 4 Marijuana use ≥ 12 months.

Comparison 1 Social competence versus usual curricula, Outcome 5 Hard drug use < 12 months.
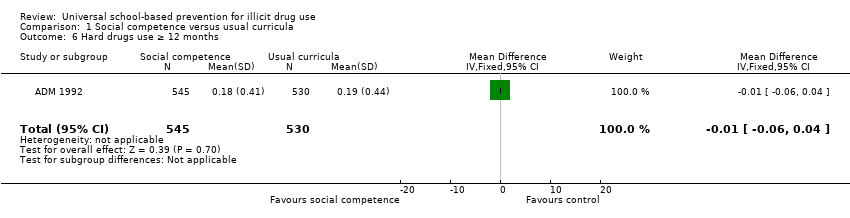
Comparison 1 Social competence versus usual curricula, Outcome 6 Hard drugs use ≥ 12 months.

Comparison 1 Social competence versus usual curricula, Outcome 7 Other drug use < 12 months.

Comparison 1 Social competence versus usual curricula, Outcome 8 Other drugs use < 12 months.
Comparison 1 Social competence versus usual curricula, Outcome 9 Any drug use < 12 months.
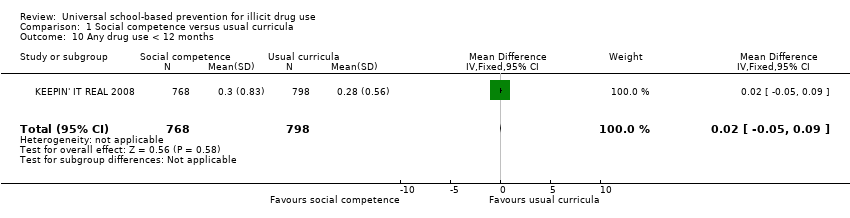
Comparison 1 Social competence versus usual curricula, Outcome 10 Any drug use < 12 months.
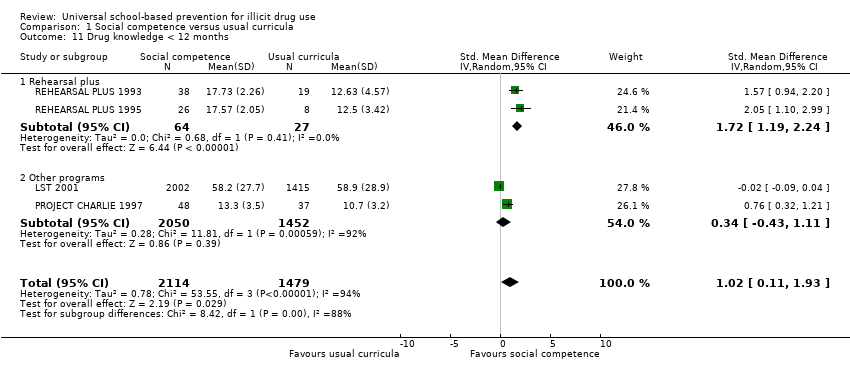
Comparison 1 Social competence versus usual curricula, Outcome 11 Drug knowledge < 12 months.

Comparison 1 Social competence versus usual curricula, Outcome 12 Intention to use marijuana < 12 months.

Comparison 1 Social competence versus usual curricula, Outcome 13 Intention to use hard drugs < 12 months.

Comparison 1 Social competence versus usual curricula, Outcome 14 Intention to use other drugs < 12 months.
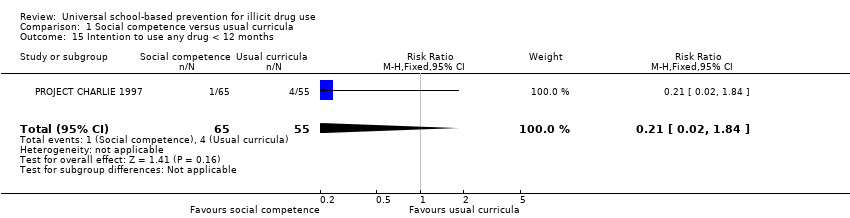
Comparison 1 Social competence versus usual curricula, Outcome 15 Intention to use any drug < 12 months.
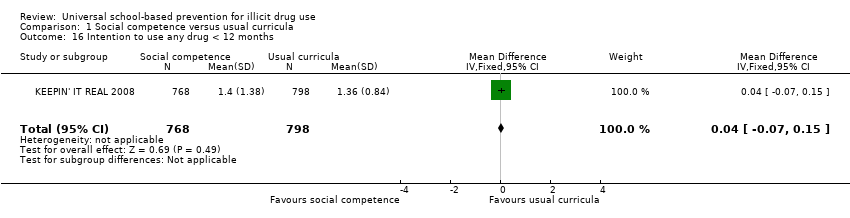
Comparison 1 Social competence versus usual curricula, Outcome 16 Intention to use any drug < 12 months.

Comparison 2 Social influence versus usual curricula, Outcome 1 Marijuana use < 12 months.
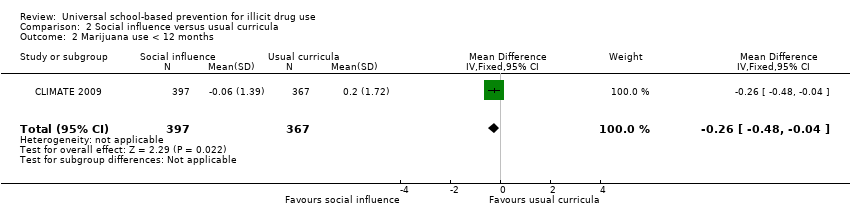
Comparison 2 Social influence versus usual curricula, Outcome 2 Marijuana use < 12 months.
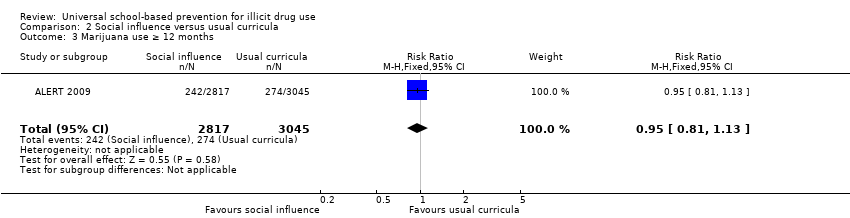
Comparison 2 Social influence versus usual curricula, Outcome 3 Marijuana use ≥ 12 months.
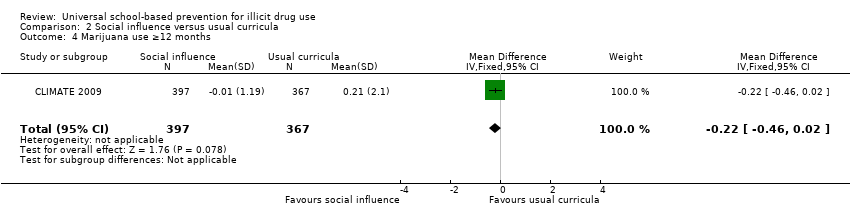
Comparison 2 Social influence versus usual curricula, Outcome 4 Marijuana use ≥12 months.

Comparison 2 Social influence versus usual curricula, Outcome 5 Other drug use < 12 months.
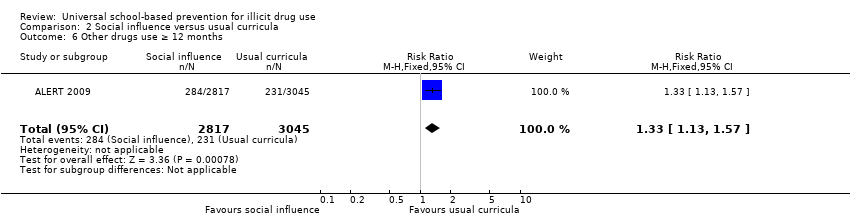
Comparison 2 Social influence versus usual curricula, Outcome 6 Other drugs use ≥ 12 months.
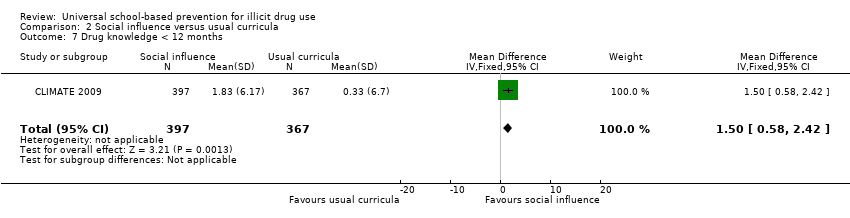
Comparison 2 Social influence versus usual curricula, Outcome 7 Drug knowledge < 12 months.

Comparison 2 Social influence versus usual curricula, Outcome 8 Drug knowledge ≥ 12 months.

Comparison 3 Combined versus usual curricula, Outcome 1 Marijuana use < 12 months.

Comparison 3 Combined versus usual curricula, Outcome 2 Marijuana use < 12 months.

Comparison 3 Combined versus usual curricula, Outcome 3 Marijuana use ≥ 12 months.

Comparison 3 Combined versus usual curricula, Outcome 4 Marijuana use ≥12 months.

Comparison 3 Combined versus usual curricula, Outcome 5 Hard drug use < 12 months.
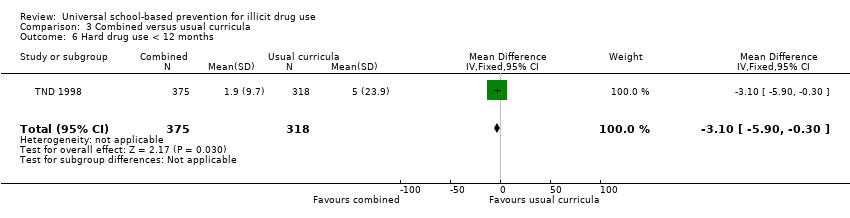
Comparison 3 Combined versus usual curricula, Outcome 6 Hard drug use < 12 months.
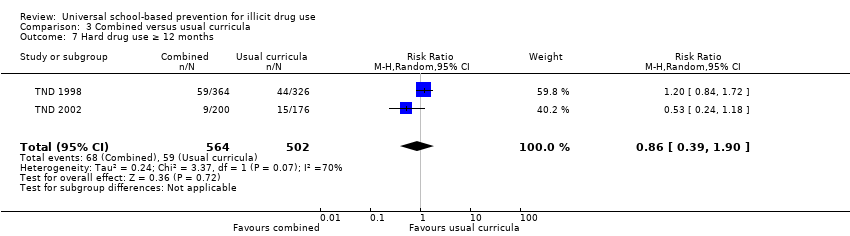
Comparison 3 Combined versus usual curricula, Outcome 7 Hard drug use ≥ 12 months.

Comparison 3 Combined versus usual curricula, Outcome 8 Hard drug use ≥ 12 months.
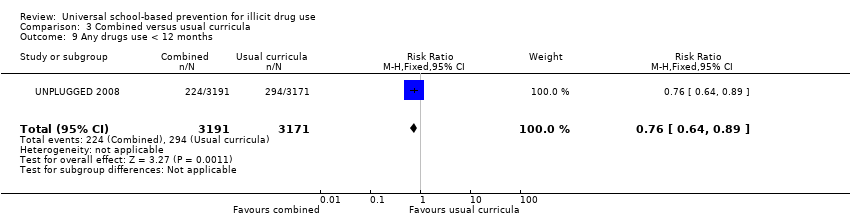
Comparison 3 Combined versus usual curricula, Outcome 9 Any drugs use < 12 months.
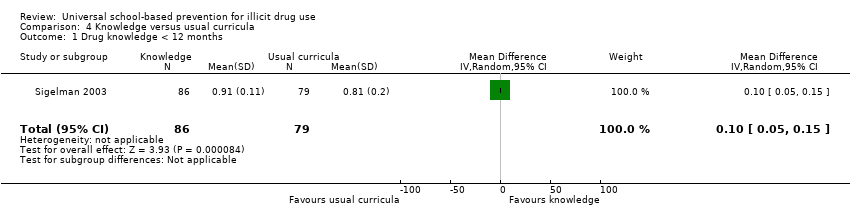
Comparison 4 Knowledge versus usual curricula, Outcome 1 Drug knowledge < 12 months.

Comparison 4 Knowledge versus usual curricula, Outcome 2 Intention to use hard drugs < 12 months.
| Social competence versus usual curricula for illicit drug use | ||||||
| Patients or population: primary or secondary school pupils | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Usual curricula | Social competence | |||||
| Marijuana use < 12 months | Study population | RR 0.9 | 9456 | ⊕⊕⊕⊝ | ||
| 119 per 1000 | 107 per 1000 | |||||
| Moderate | ||||||
| 121 per 1000 | 109 per 1000 | |||||
| Marijuana use ≥ 12 months | Study population | RR 0.86 | 2678 | ⊕⊕⊕⊕ | ||
| 217 per 1000 | 186 per 1000 | |||||
| Moderate | ||||||
| 217 per 1000 | 187 per 1000 | |||||
| Hard drug use < 12 months | Study population | RR 0.69 | 2090 | ⊕⊕⊕⊝ | ||
| 30 per 1000 | 20 per 1000 | |||||
| Moderate | ||||||
| 30 per 1000 | 21 per 1000 | |||||
| Hard drugs use ≥ 12 months | mean drug use 019 (SD 044) | The mean hard drug use at ≥ 12 months in the intervention groups was | 1075 | ⊕⊕⊕⊕ | ||
| Any drug use < 12 months | Study population | RR 0.27 | 2512 | ⊕⊕⊕⊝ | ||
| 31 per 1000 | 8 per 1000 | |||||
| Moderate | ||||||
| 27 per 1000 | 7 per 1000 | |||||
| Any drug use < 12 months | mean drug use 0.28 (SD 0.56) | The mean any drug use < 12 months in the intervention groups was | 1566 | ⊕⊕⊕⊝ | ||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1One study at high risk of detection bias, one study at high risk of attrition bias. | ||||||
| Social influence versus usual curricula for illicit drug use | ||||||
| Patients or population: primary or secondary school pupils | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Usual curricula | Social influence | |||||
| Marijuana use < 12 months | Study population | RR 0.88 | 10716 | ⊕⊕⊕⊝ | ||
| 100 per 1000 | 88 per 1000 | |||||
| Moderate | ||||||
| 170 per 1000 | 150 per 1000 | |||||
| Marijuana use ≥ 12 months | Study population | RR 0.95 | 5862 | ⊕⊕⊕⊝ | ||
| 90 per 1000 | 85 per 1000 | |||||
| Moderate | ||||||
| 90 per 1000 | 86 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1One study at high risk of selection bias, one at high risk of detection bias. | ||||||
| Combined programmes versus usual curricula for illicit drug use | ||||||
| Patients or population: primary or secondary school pupils | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Combined versus usual curricula | |||||
| Marijuana use < 12 months | Study population | RR 0.79 | 8701 | ⊕⊕⊕⊝ | ||
| 90 per 1000 | 71 per 1000 | |||||
| Moderate | ||||||
| 73 per 1000 | 58 per 1000 | |||||
| Marijuana use ≥12 months | Study population | RR 0.83 | 26910 | ⊕⊕⊕⊝ | ||
| 168 per 1000 | 139 per 1000 | |||||
| Moderate | ||||||
| 210 per 1000 | 174 per 1000 | |||||
| Hard drug use < 12 months | Study population | RR 0.85 | 693 | ⊕⊕⊕⊕ | ||
| 217 per 1000 | 184 per 1000 | |||||
| Moderate | ||||||
| 217 per 1000 | 184 per 1000 | |||||
| Hard drugs use ≥12 months | Study population | RR 0.86 | 1066 | ⊕⊕⊕⊕ | ||
| 118 per 1000 | 101 per 1000 | |||||
| Moderate | ||||||
| 110 per 1000 | 95 per 1000 | |||||
| Any drugs use < 12 months | Study population | RR 0.76 | 6362 | ⊕⊕⊕⊕ | ||
| 93 per 1000 | 70 per 1000 | |||||
| Moderate | ||||||
| 93 per 1000 | 71 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1One study at high risk of attrition bias. | ||||||
| Study reference | Programme name Study ID | Outcomes | ||
| Drug use | Intention to use | Knowledge | ||
| Clayton 1991‐1996; Lynam 1999 | DARE 1999 | Marijuana: | NA | NA |
| Perry 2003 | DARE+ DARE PLUS 2003 | NA | Marijuana: Other drugs: | NA |
| DARE 2003 | NA | Marijuana: Other drug: | NA | |
| Hecht 1993 | DRS 1993 | Marijuana: Hard drugs: | NA | NA |
| Werch 1991 | KACM 1991 | NA | NA | LFU mean difference score = 0, NS. |
| Hecht 2003 | KEEPIN' IT REAL 2003 | Marijuana: | NA | NA |
| Elek 2010 | KEEPIN' IT REAL 2010 | Any drug: | Any drug: | NA |
| KEEPIN' IT REAL PLUS | Any drug: | Any drug: | NA | |
| Botvin 1984 | LST 1984 | Marijuana: | NA | Marijuana: |
| Seal 2006 | LST 2006 | NA | NA | Favours treatment: mean knowledge score (SD); control = 10.4 (1.6), intervention = 16.5 (1.9), P value < 0.05 |
| Moskovitz 1984 | NAPA 1984 | NA | NA | SFU no significant differences LFU favours intervention (males); P value <= 0.05 |
| Shek 2012 | PATHS 2012 | Any drug: | Any drug: | NA |
| Cook 1984 | PAY 1984 | Any drug: Marijuana: Hard drugs: | NA | NA |
| Eisen 2002, Eisen 2003 | SKILLS FOR ADOL 2002 | Marijuana: Other illicit substances: | NA | NA |
| Marijuana: | Marijuana: Crack cocaine: favours intervention, NS | NA | ||
| Hansen 1988 | SMART 1988 | Marijuana: LFU favours controls; P value <= 0.05 | NA | NA |
| Sexter 1984 | Sexter 1984 | Marijuana: Other drugs: Hard drugs: | NA | NA |
| Johnson 2009 | THINK SMART 2009 | Marijuana: Other drugs: | NA | NA |
| P value <= 0.05: statistically significant | ||||
| Study reference | Programme name Study ID | Outcomes | ||
| Drug use | Intention to use | Knowledge | ||
| Ellickson 1990 | ALERT 2005 (Same intervention led either by adult educators only or adult assisted by teen leaders ‐ versus control) | Marijuana: | NA | NA |
| St Pierre 2005 | ALERT 2005 (Intervention – adult led or adult led and teen assisted ‐ versus control) | Marijuana: | Marijuana: | NA |
| Hansen 1988 | SMART 1988 | Marijuana: | NA | NA |
| Sun 2008 | TND arm A 2008 | Marijuana: Hard drugs: | NA | NA |
| P value <= 0.05: statistically significant | ||||
| Study reference | Programme name Study ID | Outcomes | ||
| Drug use | Intention to use | Knowledge | ||
| Dent 2001 | TND 2001 | Hard drugs: | NA | NA |
| Sun 2008 | TND arm b 2008 | Marijuana: Hard drugs: | NA | NA |
| P value <= 0.05: statistically significant | ||||
| Study reference | Programme name Study ID | Outcomes | ||
| Drug use | Intention to use | Knowledge | ||
| Sexter 1984 | Sexter 1984 | Marijuana: Other drugs: Hard drugs: | NA | NA |
| LFU: long‐term follow‐up (12+ months) | ||||
| Study reference | Programme name Study ID | Comparison | Outcomes | ||
| Drug use | Intention to use | Knowledge | |||
| Berstein 1987 | ASAP 1987 | Trigger‐based programme (visit to emergency department and detention centre) versus usual curricula | NA | NA | Consequences of drug use, NS |
| Furr Holden 2004 | GOOD BEHAVIOR GAME (GBG) 2004 | GBG (Classroom‐centred intervention (CC) and Family‐school partnership intervention) versus curricular intervention | Marijuana: Hard drugs: | NA | NA |
| Kellam 2012 | GOOD BEHAVIOR GAME (GBG) 2012 | GBG versus no intervention | Drug abuse and dependence: (19% GBG versus 38% controls, P value = 0.01) | NA | NA |
| Sexter 1984 | Sexter 1984 | Parent effectiveness model, network model versus no intervention | Marijuana: Other drugs: Hard drugs: | NA | NA |
| P value <= 0.05: statistically significant | |||||
| Study reference | Programme name Study ID | Comparison | Outcomes | ||
| Drug use | Intention to use | Knowledge | |||
| Malvin 1985 | CROSS AGE TUTORING 1985 | Other (students were taught tutoring and communication skills and tutored elementary students) versus other (same graders were taught business and interpersonal skills and operated an on‐campus store) | NA | NA | SFU: NS LFU: NS |
| Botvin 1994 | LST 1994 | LST versus a culturally focused programme | NA | Marijuana: Other drugs:SFU in favour of programme, P value <= 0.05 | Marijuana: |
| McCambridge 2011 | MOTIVATIONAL INTERVIEW (MI) 2011 | Motivational interview versus knowledge | Marijuana: | NA | NA |
| Werch 2011 | PROJECT ACTIVE 2011 | One‐to‐one consultation about physical activity versus a booklet | Marijuana: | NA | NA |
| Werch 2005 | PROJECT SPORT 2005 | Brief consultation and in‐person health behaviour screen versus wellness brochure | Marijuana: | NA | NA |
| Jones 1995 | REHEARSAL PLUS 1995 | Skills‐based programme versus general information | NA | NA | SFU in favour of treatment, P value <= 0.05 |
| Hansen 1991 | SMART 1991 | Social competence versus social influence programmes | Marijuana: | NA | NA |
| Hansen 1991 | SMART 1991 | Social competence versus combined (social competence + social influence) | Marijuana: | NA | NA |
| Hansen 1991 | SMART 1991 | Social influence versus combined (social competence + social influence) | Marijuana: LFU in favour of combined; P value <= 0.05 | NA | NA |
| Hansen 1991 | SMART 1991 | Social competence and social influence versus knowledge | Marijuana: | NA | NA |
| P value <= 0.05: statistically significant | |||||
| Study reference | Name of the programme Study ID | Duration (months) | N. of sessions | Deliverer | Time of outcome assessment (from programme end) | Drug use | Intention to use | Knowledge | Data for meta‐analysis |
| Snow 1992 | Adolescent Decision‐Making (ADM 1992) | 3 | 12 | Not Reported | 24 months | Marijuana, hard drugs | no | no | yes |
| Guo 2010 | CMER 2010 | 3 | 6 | Teacher | 3 months | Any drug | no | yes | yes |
| Perry 2003 | DARE 2003 | 10 | 10 | Police officer | Post‐test | Marijuana, any drug | no | no | no |
| Perry 2003 | DARE + DARE plus 2003 | 4 + extra school activities | 1 | Police officer, teacher | Post‐test | Marijuana, any drug | no | no | no |
| Ringwalt 1991 | DARE 1991 b | 4 | 17 | Law officer | Post‐test | Other drugs | no | no | yes |
| Clayton 1991 | DARE 1991 | 4 | Not Reported | Project staff | Post‐test, 1 months, 2 months, 5 monhts and 10 years | Marijuana 30 days, past year | no | no | no |
| Hecht 1993 | Drug Resistance Strategies (DRS 1993) | < 1 | 2 | Project staff | Post‐test (1 day) | Marijuana, other drugs | yes | no | no |
| Bond 2004 | GATEHOUSE 2004 | 3 | 20 | Project staff | Post‐test, 12, 24 | Marijuana in the past 6 months | no | no | yes |
| Werch 1991 | KACM 1991 | 1 | 4 | Project staff, teacher | Post‐test | Marijuana | yes | yes | no |
| Hecht 2003 | KEEPIN’IT REAL 2003 | 18 | 10 | Teacher | Post‐test , 8 months, 14 months | Marijuana | no | no | no |
| Hecht 2008 | KEEPIN’IT REAL 2008 | 18 | 12 + 3 ‐ 6 boosters | Teacher | Post‐test | Any drug | yes | no | yes |
| Elek 2010 | KEEPIN’IT REAL 2010 | 18 | 15 | Not Reported | 12 months | Any drug | yes | no | no |
| Botvin 1984 | LST 1984 | 24 | 20 (+ 10 boosters) | Teacher/peer | Post‐test, 12 months | Marijuana 30 days | no | yes | no |
| Botvin 1990 | LST 1990 | 36 | 15 (+ 15 boosters) | Teacher/project staff | Post‐test, 36 months | Marijuana 30 days | no | no | yes |
| Botvin 2001 | LST 2001 | 2 school years | 15 + 10 boosters | Teacher | Post‐test | Marijuana frequency, not clear in which period; other drugs, same as above | yes | yes | yes |
| Seal 2006 | LST 2006 | Not Reported | 10 | Not Reported | 6 months | NR | no | yes | no |
| Resnicow 2008 | LST and KEPT LEFT 2008 | 24 | 16 LST and 16 KEPT LEFT | Teacher | Post‐test | Marijuana, hard drugs | no | no | yes |
| Moskovitz 1984 | NAPA 1984 | 4 | 12 | Project staff | Post‐test, follow‐up (5 months) | no | no | yes | no |
| Shek 2012 | PATHS 2012 | 36 | 120 (40 every school year) | Teacher and social worker | Process evaluation year 1 to 3 (wave 1 to 6). 3 and 12 months after the end (wave 7, 8) | Legal and illegal (ketamine, cannabis, ecstasy, heroine) | yes | no | no |
| Cook 1984 | PAY 1984 | 6 | 48 | Project staff/teacher | Post‐test | Marijuana, hard drugs, other drugs | no | no | no |
| Beets 2009 | POSITIVE ACTION 2009 | 60 | 700 | Teacher | Post‐test | Any drug lifetime use | no | no | yes |
| Hurry 1997 | PROJECT CHARLIE 1997 | 12 | 40 | Teacher | Post‐test | no | yes | yes | yes |
| Corbin 1993 | REHEARSAL PLUS | < 1 | 3 | Psychology majors | Post‐test, 3 | no | no | yes | yes |
| Jones 1995 | REHEARSAL PLUS | < 1 | 3 | Undergraduate psychology majors | Post‐test | no | no | yes | yes |
| Sexter 1984 | Sexter 1984 | 6 | Not Rerported | Not Reported | 6 months | Marijuana, other drugs | no | no | no |
| Eisen 2002 | SKILLS FOR ADOL 2002 | 12 | 40 | Teacher | 12,months 24 months | Marijuana, other drugs | no | no | no |
| Hansen 1988 | SMART 1988 | Not Reported | 12 | Project staff, teacher + peer | 12 months, 24 months since programme beginning | Marijuana | no | no | no |
| Johnson 2009 | THINK SMART 2009 | 6 | 15 (12 + 3 boosters) | Teacher | Post‐test (wave 2), 6 m (wave 3) | Marijuana, other drugs | no | yes | no |
| m: months | |||||||||
| Study reference | Name of the program Study ID | Duration (months) | N. of sessions | Deliverer | Time of outcome assessment (from programme end) | Drug use | Intention to use | Knowledge | Data for meta‐analysis |
| Ellickson 1990 | ALERT 1990 | 2 school years | 8 + 3 (boosters) | 1. Educator + peer 2. Educator alone | Post‐test, 3 months | Marijuana | yes | yes | no |
| Ellickson 2003 | ALERT 2003 | 18 | 14 | Teacher | Post‐test | Marijuana | no | no | yes |
| St Pierre 2005 | ALERT 2005 | 2 school years | 14 | Project staff + peer | Post‐test, 12 monhts | Marijuana, 30 days use | no | no | no |
| Ringwalt 2009 | ALERT 2009 | 2 school years | 14 | Teacher | Post‐test, 12 months | Marijuana, 30 days use, Other drugs, 30 days use | no | no | yes |
| Copeland 2010 | ATD 2010 | 18 | Not Reported | Teacher | Post‐test | Marijuana | no | no | yes |
| Newton 2009 | CLIMATE 2009 | 6 | 12 | Teacher | Post‐test, 6 months, 12 months | Marijuana, 30 days use | no | yes | yes |
| Hansen 1988 | SMART 1998 | NR | 12 | Project staff, teacher + peer | 12 months, 24 months from programme beginning | Marijuana | no | no | no |
| Sun 2008 | TND 2008 Arm A | 1 | 12 | Project staff and teacher | 12 moths | Marijuana, 30 days use | no | no | no |
| m: months | |||||||||
| Study reference | Name of the programme Study ID | Duration (months) | N. of sessions | Deliverer | Time of outcome assessment (from programme end) | Drug use | Intention to use | Knowledge | Data for meta‐analysis |
| Sloboda 2009 | TCYL 2009 | 2 school years | 10 + 7 (booster) | Project staff | 24 months | Marijuana, 30 days | no | no | yes |
| Sussman 1998 and Sun 2006 | TND 1998 | 1 | 9 | Project staff | Post‐test, 12, 48 months | Marijuana, 30 days | no | no | yes |
| Dent 2001 | TND 2001 | 1 | 9 | Project staff | 12 months | Marijuana, 30 days | no | no | yes |
| Sussman 2002 | TND 2002 | 1 | 12 | Project staff | 24 months | Marijuana, 30 days | no | no | yes |
| Sun 2008 | TND 2008 Arm B | 1 | 12 | Project staff and teacher | 12 months | Marijuana, 30 days | no | no | no |
| Faggiano 2010 | UNPLUGGED 2008 | 3 | 12 | Teacher + peer | 3 months, 12 months | Marijuana, 30 days | no | no | yes |
| Gabrhelik 2012 | UNPLUGGED 2012 | 1 school year | 12 | Teacher | Post‐test, 3moths, 12 months, 15 mnths, 24 months | Marijuana, 30 days Lifetime any drugs use including marijuana | no | no | yes |
| Study reference | Name of the programme Study ID | Duration (months) | N. of sessions | Deliverer | Time of outcome assessment (from programme end) | Drug use | Intention to use | Knowledge | Data for meta‐analysis |
| Sexter 1984 | Sexter 1984 | 6 | Not Reported | Not Reported | Post‐test | Marijuana, other drugs | no | no | no |
| Sigelman 2003 | Sigelman 2003 | < 1 | 3 | Project staff | Post‐test | no | yes | yes | yes |
| Study reference | Name of the programme Study ID | Comparison | Duration (months): D N. of sessions: N | Deliverer | Time of outcome assessment (from programme end) | Drug use | Intention to use | Knowledge | Data for meta‐analysis |
| Berstein 1987 | ASAP 1987 | Trigger‐based programme (visit to emergency department and detention centre) versus usual curricula | D: 6 N: Not Reported | Project staff | Post‐test, 8 months | Any drugs | no | yes | Meta‐analysis not performed due to high heterogeneity |
| Furr Holden 2004 | GOOD BEHAVIOR GAME (GBG) 2004 | GBG versus curricular intervention | D: 12 N: Not Reported | Teacher | 5 years, 6 years, 7 years | Marijuana, other drugs, hard drugs | no | no | Meta‐analysis not performed due to high heterogeneity |
| Kellam 2012 | GOOD BEHAVIOR GAME (GBG) 2012 | GBG versus no intervention | D: 24 N: 3 times/week for 10 minutes, increasing in duration to 40 minutes | Trained teacher | 15 years | CIDI‐UM modified to reflect DSM‐IV diagnostic criteria was used to determine the lifetime, past year and past month occurrence of drug abuse and dependence disorders | no | no | Meta‐analysis not performed due to high heterogeneity |
| Sexter 1984 | Sexter 1984 | Parent effectiveness model, network model versus no intervention | D: 6 N: Not Reported | Not Reported | Post‐test | Marijuana, other drugs | no | no | Meta‐analysis not performed due to high heterogeneity |
| CIDI‐UM: Composite International Diagnostic Interview ‐ University of Michigan (scale for occurrence of drug abuse and dependece disordes) DSM‐IV: Diagnostic and Statistical Manual of Mental Disorders, 4th Edition | |||||||||
| Study reference | Name of the programme Study ID | Comparison | Duration (months): D Number of sessions: N | Deliverer | Time of outcome assessment (from programme end) | Drug use | Intention to use | Knowledge | Data for meta‐analysis | |
| Malvin 1985 | CROSS AGE TUTORING/SCHOOL STORE | Other (students were taught tutoring and communication skills and tutored elementary students) versus other (same graders were taught business and interpersonal skills and operated an on‐campus store) | D: 6 N: Not Reported | Project staff | Post‐test, 12 months | Any drug | no | yes | Meta‐analysis not performed due to high heterogeneity | |
| Botvin 1994 | LST 1994 | LST versus a culturally focused programme | D: 7 N: 15 | Project staff + peer | Post‐test, 18 months | no | yes | yes | Meta‐analysis not performed due to high heterogeneity | |
| McCambridge 2011 | MOTIVATIONAL INTERVIEW | Motivational interview versus knowledge | D: 1 hour N: 1 | Not reported | 3 months ,12 months | Marijuana | no | no | Meta‐analysis not performed due to high heterogeneity | |
| Hansen 1991 | SMART 1991 | Social competence versus social influence programmes | D: Not Reported N: 9 | Project staff | 12 months, 24 months | Marijuana | no | no | Meta‐analysis not performed due to high heterogeneity | |
| Hansen 1991 | SMART 1991 | Social competence versus combined (social competence + social influence) | D: Not Reported N: 9 | Project staff | 12 months, 24 months | Marijuana | no | no | Meta‐analysis not performed due to high heterogeneity | |
| Hansen 1991 | SMART 1991 | Social influence versus combined (social competence + social influence) | D: Not Reported N: 9 | Project staff | 12 months, 24 months | Marijuana | no | no | Meta‐analysis not performed due to high heterogeneity | |
| Hansen 1991 | SMART 1991 | Social competence and social influence versus knowledge | D:Not Reported N: Not Reported | Project staff | 12 months, 24 months | Marijuana | no | no | Meta‐analysis not performed due to high heterogeneity | |
| Werch 2011 | PROJECT ACTIVE 2011 | One‐to‐one consultation about physical activity versus a booklet | D: 1 day N: 1 | Not reported | 3 months | Marijuana | no | no | Meta‐analysis not performed due to high heterogeneity | |
| Werch 2005 | PROJECT SPORT 2005 | Brief consultation and in‐person health behaviour screen versus wellness brochure | D: 1 day N: 1 | Project staff | 3 months, 12 months | Marijuana | no | no | Meta‐analysis not performed due to high heterogeneity | |
| Jones 1990 | REHEARSAL PLUS 1990 | Skills‐based programme versus general information | D: 2 days N: 2 | Project staff | Post‐test | no | no | yes | Meta‐analysis not performed due to high heterogeneity | |
| LST: Life Skill Training | ||||||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Marijuana use < 12 months Show forest plot | 4 | 9456 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.81, 1.01] |
| 2 Marijuana use < 12 months Show forest plot | 1 | 3417 | Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐0.20, ‐0.00] |
| 3 Marijuana use ≥ 12 months Show forest plot | 1 | 2678 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.74, 1.00] |
| 4 Marijuana use ≥ 12 months Show forest plot | 1 | 1075 | Mean Difference (IV, Fixed, 95% CI) | ‐0.02 [‐0.10, 0.06] |
| 5 Hard drug use < 12 months Show forest plot | 1 | 2090 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.69 [0.40, 1.18] |
| 6 Hard drugs use ≥ 12 months Show forest plot | 1 | 1075 | Mean Difference (IV, Fixed, 95% CI) | ‐0.01 [‐0.06, 0.04] |
| 7 Other drug use < 12 months Show forest plot | 1 | 1270 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.53, 0.98] |
| 8 Other drugs use < 12 months Show forest plot | 1 | 3434 | Mean Difference (IV, Fixed, 95% CI) | ‐0.05 [‐0.11, 0.01] |
| 9 Any drug use < 12 months Show forest plot | 2 | 2512 | Risk Ratio (M‐H, Random, 95% CI) | 0.27 [0.14, 0.51] |
| 10 Any drug use < 12 months Show forest plot | 1 | 1566 | Mean Difference (IV, Fixed, 95% CI) | 0.02 [‐0.05, 0.09] |
| 11 Drug knowledge < 12 months Show forest plot | 4 | 3593 | Std. Mean Difference (IV, Random, 95% CI) | 1.02 [0.11, 1.93] |
| 11.1 Rehearsal plus | 2 | 91 | Std. Mean Difference (IV, Random, 95% CI) | 1.72 [1.19, 2.24] |
| 11.2 Other programs | 2 | 3502 | Std. Mean Difference (IV, Random, 95% CI) | 0.34 [‐0.43, 1.11] |
| 12 Intention to use marijuana < 12 months Show forest plot | 1 | 3417 | Mean Difference (IV, Fixed, 95% CI) | ‐0.12 [‐0.19, ‐0.05] |
| 13 Intention to use hard drugs < 12 months Show forest plot | 1 | 3417 | Mean Difference (IV, Fixed, 95% CI) | ‐0.01 [‐0.04, 0.02] |
| 14 Intention to use other drugs < 12 months Show forest plot | 1 | 3417 | Mean Difference (IV, Fixed, 95% CI) | ‐0.04 [‐0.07, ‐0.01] |
| 15 Intention to use any drug < 12 months Show forest plot | 1 | 120 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.21 [0.02, 1.84] |
| 16 Intention to use any drug < 12 months Show forest plot | 1 | 1566 | Mean Difference (IV, Fixed, 95% CI) | 0.04 [‐0.07, 0.15] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Marijuana use < 12 months Show forest plot | 3 | 10716 | Risk Ratio (M‐H, Random, 95% CI) | 0.88 [0.72, 1.07] |
| 1.1 Alert | 2 | 10138 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.69, 0.97] |
| 1.2 Other programs | 1 | 578 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [0.79, 1.58] |
| 2 Marijuana use < 12 months Show forest plot | 1 | 764 | Mean Difference (IV, Fixed, 95% CI) | ‐0.26 [‐0.48, ‐0.04] |
| 3 Marijuana use ≥ 12 months Show forest plot | 1 | 5862 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.81, 1.13] |
| 4 Marijuana use ≥12 months Show forest plot | 1 | 764 | Mean Difference (IV, Fixed, 95% CI) | ‐0.22 [‐0.46, 0.02] |
| 5 Other drug use < 12 months Show forest plot | 1 | 5862 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.93, 1.27] |
| 6 Other drugs use ≥ 12 months Show forest plot | 1 | 5862 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.33 [1.13, 1.57] |
| 7 Drug knowledge < 12 months Show forest plot | 1 | 764 | Mean Difference (IV, Fixed, 95% CI) | 1.5 [0.58, 2.42] |
| 8 Drug knowledge ≥ 12 months Show forest plot | 1 | 764 | Mean Difference (IV, Fixed, 95% CI) | 1.65 [0.69, 2.61] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Marijuana use < 12 months Show forest plot | 3 | 8701 | Risk Ratio (M‐H, Random, 95% CI) | 0.79 [0.59, 1.05] |
| 1.1 Unplugged | 2 | 8008 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.56, 0.82] |
| 1.2 Other programs | 1 | 693 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.79, 1.14] |
| 2 Marijuana use < 12 months Show forest plot | 1 | 693 | Mean Difference (IV, Fixed, 95% CI) | ‐1.90 [‐5.83, 2.03] |
| 3 Marijuana use ≥ 12 months Show forest plot | 6 | 26910 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.69, 0.99] |
| 3.1 Unplugged | 2 | 7321 | Risk Ratio (M‐H, Random, 95% CI) | 0.47 [0.20, 1.11] |
| 3.2 TND | 3 | 2269 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.83, 1.09] |
| 3.3 Other programmes | 1 | 17320 | Risk Ratio (M‐H, Random, 95% CI) | 0.94 [0.89, 1.00] |
| 4 Marijuana use ≥12 months Show forest plot | 1 | 690 | Mean Difference (IV, Fixed, 95% CI) | ‐0.80 [‐4.39, 2.79] |
| 5 Hard drug use < 12 months Show forest plot | 1 | 693 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.85 [0.63, 1.14] |
| 6 Hard drug use < 12 months Show forest plot | 1 | 693 | Mean Difference (IV, Fixed, 95% CI) | ‐3.1 [‐5.90, ‐0.30] |
| 7 Hard drug use ≥ 12 months Show forest plot | 2 | 1066 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.39, 1.90] |
| 8 Hard drug use ≥ 12 months Show forest plot | 1 | 690 | Mean Difference (IV, Fixed, 95% CI) | 0.30 [‐1.36, 1.96] |
| 9 Any drugs use < 12 months Show forest plot | 1 | 6362 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.64, 0.89] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Drug knowledge < 12 months Show forest plot | 1 | 165 | Mean Difference (IV, Random, 95% CI) | 0.10 [0.05, 0.15] |
| 2 Intention to use hard drugs < 12 months Show forest plot | 1 | 165 | Mean Difference (IV, Fixed, 95% CI) | ‐0.05 [‐0.24, 0.14] |