使用封闭剂预防恒牙龋
摘要
研究背景
上世纪60年代牙齿密封剂被引入,用于预防牙齿咬合表面出现的窝沟和裂隙。封闭剂可以抑制引发龋齿的细菌滋生。有证据表明,窝沟封闭剂可以预防儿童和青少年龋齿,其效果可能与人群患龋率有关。
研究目的
比较不同种类窝沟封闭剂预防儿童和青少年恒牙龋的效果.
检索策略
我们检索了Cochrane口腔卫生注册试验组(至2012年11月);Cochrane对照试验注册库(CENTRAL)(Cochrane图书馆,第7期);MEDLINE(通过OVID检索界面,自1946年至2012年11月1日);EMBASE(通过OVID界面,1980年至2012年11月1日);SCISEARCH, CAplus, INSPEC, NTIS,PASCAL(通过STN Easy界面,至2012年9月1日);以及DARE,NHS EEDH和HTA(通过CAIRS界面检索至2012年3月29日,后通过Metaxis界面检索至2012年9月)。检索不受语言或出版日期限制。另外,我们也检索了ClinicalTrials.gov中正在进行的试验(至2012年7月23日)。
标准/纳入排除标准
使用封闭剂预防20岁以下儿童或青少年前臼齿或臼齿咬合面或邻近面龋齿并至少持续12个月,与不使用封闭剂或其他封闭剂比较的随机或准随机对照试验。
数据收集与分析
两名研究者独立地进行文献筛选,数据提取及方法学质量评估。我们使用比值比(Odds ratio, OR)对恒臼齿咬合面有无龋齿进行统计。采用自身口腔左右对照的试验则使用Becker‐Balagtas比值比的方法。我们使用平均差来统计龋齿均增长数。所有测量值取95%置信区间(confidence intervals , CI)。
证据质量通过GRADE方法来评估。
在进行meta分析时,若同一比较类型中含3个以上试验,使用随机效应模型,否则使用固定效应模型。
主要结果
此篇综述共纳入34项试验。12项试验评价了与不使用封闭剂相比,使用封闭剂的效果(涉及2575人)(12个试验中只一个说明了齿对数);21个试验评估了两种不同封闭剂比较的效果(涉及3202人);1个试验评估了两种不同封闭剂与不使用封闭剂比较的效果(涉及751人)。儿童的年龄范围在5到16岁。所有试验几乎都没有报告受试者的氟化物暴露史的或基线龋齿患病率。
树脂密封胶与不使用密封胶比较:与不使用密封胶相比,第二,第三或第四代树脂密封胶预防5‐10岁儿童第一批恒臼牙出现龋齿的情况(2年随访结果,OR值0.12,95%CI 0.07‐0.19,6个试验(其中5个发表于20世纪70年代,另一个发表于2012年),低偏移风险,1259名儿童随机入组,分析了1066名儿童的数据,等级中等)。假设对照组2年随访期牙齿表面出现龋齿的概率为40%(即每1000出现400个龋齿),那么使用树脂密封胶后牙齿表面龋齿发生率降至6.25%(95%CI 3.84%‐9.63%);同理假设牙齿表面龋齿率为70% (每1000出现700龋齿),那么使用树脂密封胶后龋齿发生率降至18.92%(95% CI 12.28%‐27.18%)。这种龋齿预防效果可在长时间随访中维持但是证据的质量和数量都会下降(例如在48至54个月的随访,OR值0.21,95%CI 0.16‐0.28,4个试验(两个为低偏倚风险,两个为高偏倚风险),对482位儿童进行评价;相对危险值(RR值)0.24,95%CI 0.12‐0.45,一个试验偏倚风险不清楚,对203位儿童进行评价)。
玻璃电密封剂与不使用密封剂相比:无充足证据说明在24个月的随访期中,与不使用密封剂相比,玻璃电密封剂预防龋齿的效果(DFS平均差为‐0.18,95%CI为‐0.39至0,03,一个试验偏倚风险不清楚,452名儿童随机入组,404名儿童数据纳入分析,证据质量较差)。
一种密封剂与另一种密封剂比较:本篇综述并没有对不同类型密封剂的相对效应给出确定的结论。
21项试验直接比较了两种不同密封剂的疗效。根据密封胶类型,结局指标和随访时间的不同分为几种不同的对照类型。对照类型,结局指标,结局测量时点和氟化物暴露史,在21项试验中有很大不同。
在玻璃离子与树脂密封剂对比的15项试验中,没有足够证据能对这两种材料的优效性做出任何结论。 尽管有15个试验,但各试验事件率很低,而限制了对结果的贡献。
3项研究比较了树脂玻璃离子和树脂密封剂,但报告的结果不一致。
2项低质量试验比较了多酸复合树脂与树脂密封剂的疗效,发现2年后龋齿的发生率不存在差异。
不良反应:仅2个试验报告了不良反应,均表示研究中无不良事件发生。
作者结论
推荐应用密封剂以预防或控制龋齿。与不使用密封剂相比,儿童和青少年恒磨牙咬合面使用密封剂能减少48个月内龋齿发生率,而较长期的随访证据数量和质量降低。本文表明密封剂对高危儿童有效,而有关其他人群效能大小的证据则很少。不同类型密封剂的相对效应仍待研究。
PICO
概要
使用封闭剂预防恒牙龋
现今儿童和青少年牙齿与过去相比更健康,但蛀牙(龋齿)问题仍然困扰着某些个体和人群,实际上影响了全世界大量的人们。 儿童和青少年龋齿多集中在后臼齿咬合面。 预防蛀牙的方法包括刷牙、补充氟化物(例如嚼口香糖)和局部应用氟化物和应用牙科诊所的密封剂。
预防蛀牙是一个亟待解决的公共卫生问题,因而Cochrane口腔健康小组对现有证据进行综述以探究使用牙科密封剂能否用来防止蛀牙。 本篇综述纳入了34项试验, 涉及5到16岁的儿童和青少年,且均为普通人群。
文献更新检索至2012年11月1日。
使用牙齿密封剂的目的是防止细菌生长,而这种细菌会促进后牙槽发生龋齿。 牙医或牙齿护理其他相关人员建议在后牙凹槽使用密封剂。 目前存在多种密封胶材料,其中使用最为广泛的是树脂密封胶和玻璃离子粘固剂。
本综述纳入了34个独立研究,共6529名年轻人,涉及多种用于预防龋齿的牙齿密封剂,结果表明使用密封剂与不使用相比,能减少后牙咬合面龋齿的发生。
34篇文献中的12篇,比较了使用树脂密封剂和不使用密封剂,发现后牙使用了牙齿密封剂的儿童与不使用密封剂的儿童相比,更不易患龋齿。例如,如果后牙两年龋齿发生率为40%,那么使用密封胶后降低到6%。而如果另一儿童群体两年龋齿发生率为70%,使用密封剂则可降低到19%。这些结果基于6项研究(5篇发表在20世纪70年代),使用牙齿密封剂的儿童为5到10岁。树脂密封剂的类似益处最长能延至9年。但并未确证哪种密封剂更优。
Authors' conclusions
Summary of findings
| Resin‐based sealant compared to control without sealant for preventing dental caries | ||||||
| Patient or population: Children and adolescents | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | Number of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control teeth | Sealed teeth | |||||
| Dentine caries in permanent molars Follow‐up: 2 years | Incidence of carious first molars (40%) 400 per 10001 | Incidence of carious first molars (6.3%) 63 per 1000 (38 to 96) | OR 0.12 (0.07 to 0.19) 2 | 1259 children randomised & 1066 evaluated after 2 years | ⊕⊕⊕⊝ |
Benefits of resin‐sealant maintained up to at least 48 months of follow‐up6 |
| Incidence of carious first molars (70%) 700 per 10001 | Incidence of carious first molars (19%) 190 per 1000 (122 to 272) | OR 0.12 (0.07 to 0.19) 2 | 1259 children randomised & 1066 evaluated after 2 years | ⊕⊕⊕⊝ |
Benefits of resin‐based sealant maintained up to at least 48 months of follow‐up6 | |
| CI: confidence interval; OR: odds ratio | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 The incidence of carious control teeth in the five split‐mouth trials included in this comparison ranged from 37% to 69% (studies published between 1976 and 1979). We have shown the effect of sealants at each end of this range. These studies did not give information on the baseline caries prevalence of the children. 2 There was considerable heterogeneity in this estimate (I2 = 77% P = 0.0007) but all of the trials showed a statistically significant effect favouring sealants. 3 Six studies at low risk of bias for the four key domains of allocation concealment, incomplete outcome data, selective reporting and baseline comparability of the groups. 4All studies recruited children aged 5‐10 years. Three studies conducted in areas with fluoridated water, two studies stated water was not fluoridated and the remaining one study did not report whether water supplies were fluoridated. 5 Five trials were published between 1976 and 1979 and one in 2012. One further parallel group trial from Thailand at unclear risk of bias reporting DFS increment published in 1995 also found a benefit in favour of resin‐based sealant (mean difference in DFS increment ‐0.65, 95% CI ‐0.83 to ‐0.47, 276 children evaluated). 6 The benefit associated with sealant use is maintained at all of the follow‐up estimates (up to 9 years) though the number of studies and the number of children available for evaluation reduced markedly over this period (e.g. at 48 to 54 months of follow‐up odds ratio 0.21, 95% CI 0.16 to 0.28, two studies at low risk of bias and two studies at high risk of bias, 482 children evaluated; risk ratio 0.24, 95% CI 0.12 to 0.45, one study at unclear risk of bias, 203 children evaluated). | ||||||
| Glass ionomer sealant compared to control without sealant for preventing dental caries | ||||||
| Patient or population: Children and adolescents | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | Number of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control teeth | Sealed teeth | |||||
| Caries as DFS increment in permanent molars Follow‐up: 2 years | The mean DFS increment of control tooth surfaces 0.701 | The mean DFS increment of sealed tooth surfaces 0.52 | The mean DFS difference ‐0.18 | 452 children randomised and 404 evaluated after 2 years follow‐up | ⊕⊝⊝⊝ |
Extended follow‐up4 |
| CI: confidence interval; OR: odds ratio; RR: risk ratio; DFS: decayed and filled occlusal tooth surfaces of molars | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 This is a low caries prevalence population from Thailand according to WHO figures (WHO 2003) (mean baseline DMFT of 1.81). 2 A single study at unclear risk of bias (no information on sequence generation or allocation concealment). 3 Children aged 12‐13 years at baseline. Study conducted in an area with naturally fluoridated water. 4 Study published in 1995. 5 Follow‐up only reported for 2 years in this study. | ||||||
| Glass ionomer sealants compared to resin sealants for preventing caries | ||||
| Patient or population: Children and adolescents Settings: RCTs conducted in the UK, Scandinavia, Asia, Australia, Brazil and the Arab world Intervention: Glass ionomer sealant (including Fuji III, VII, IX, Ketac Silver, Ketac‐fil, Ketac Molar Easymix or Baseline) Comparison: Resin sealant | ||||
| Outcomes | Impact Inconsistent effect | Number of participants | Quality of the evidence | Comments |
| Dentine caries in permanent molars Follow‐up: 1, 2, 3, 4, 5 and 7 years | Inconsistent effect. There were differences in: comparisons, outcomes, outcome reporting times and background fluoride exposure including water fluoridation | 15 trials1,2 (2939 participants randomised) | ⊕⊝⊝⊝ | |
| RCT: randomised controlled trial | ||||
| GRADE Working Group grades of evidence | ||||
| 1 Five trials at high risk of bias, four at unclear risk of bias, and six at low risk of bias (for the four key domains of allocation concealment, incomplete outcome data, selective reporting and baseline comparability of the groups). 2 Trials published between 1993 and 2012. | ||||
| Resin‐modified glass ionomer sealants compared to resin sealants for preventing caries | ||||
| Patient or population: Children and adolescents Settings: RCTs conducted in Norway, Egypt & Brazil Intervention: Resin‐modified glass ionomer sealant (Fuji II LC, Vitrebond or Vitremer) Comparison: Resin sealant (Helioseal, Tetric Flow, Fluoroshield or Concise White) | ||||
| Outcomes | Impact Inconsistent effect | Number of participants | Quality of the evidence | Comments |
| Dentine caries in permanent molars Follow‐up: 1, 2 and 3 years | Inconsistent effect. Different products, outcomes, outcome reporting times and age groups | 3 trials1,2,3 (418 participants randomised) | ⊕⊝⊝⊝ | |
| RCT: randomised controlled trial | ||||
| GRADE Working Group grades of evidence | ||||
| 1Two trials at unclear risk of bias and one at low risk of bias (for the four key domains of allocation concealment, incomplete outcome data, selective reporting and baseline comparability of the groups). 2 No information on background fluoride exposure or baseline caries prevalence. 3 Trials published between 1996 and 2010. | ||||
| Polyacid‐modified resin sealants compared to resin sealants for preventing caries | ||||
| Patient or population: Children and adolescents Settings: RCTs conducted in Sweden and Turkey Intervention: Polyacid‐modified resin composite (Dyract Seal) Comparison: Resin sealant (3rd or 4th generation Delton) | ||||
| Outcomes | Impact No difference | Number of participants | Quality of the evidence | Comments |
| Dentine caries in permanent molars Follow‐up: 2 years | No difference in caries after 2 years | 2 trials1,2,3 (84 participants randomised and 68 evaluated after 2 years) | ⊕⊝⊝⊝ | |
| RCT: randomised controlled trial | ||||
| GRADE Working Group grades of evidence | ||||
| 1Two trials, different products compared. 2One trial at high risk of bias and one at unclear risk of bias. 3 Water not fluoridated in one study and no information on background fluoride in the other, age at baseline 6‐13 years, no information on baseline caries prevalence. | ||||
Background
Dental sealants were introduced in the 1960s as part of the preventive programmes to protect pits and fissures on the occlusal tooth surfaces from dental caries. They prevent the growth of bacteria that promote dental decay. In the 1970s and 1980s, the prevalence of dental caries among children and adolescents declined in industrialized countries (Marthaler 1996; Marthaler 2004; Petersson 1996). The reasons for this decline are not fully understood, but increased access to fluoride may have played the main role (Bratthall 1996). Part of the caries decline has been attributed to the use of dental sealants (Brown 1995). Children and adolescents of today have healthier teeth than children some decades ago, and the use of dental sealants in low caries prevalence populations has been questioned. However, dental caries is still a problem in some individuals even in low caries prevalence populations. Occlusal surfaces of posterior teeth are the most vulnerable sites of teeth due to their anatomy favouring plaque retention and the rate of occlusal caries has not fallen to the same extent as caries on smooth surfaces (Brown 1995). Among school‐aged children the majority of the increment in dental caries has been detected on pit and fissure surfaces of first and second molars (Batchelor 2004; Brown 1995;McDonald 1992). In addition, recent data show that the caries decline has stabilized in many areas and even increases in prevalence have been reported (Dye 2007; Haugejorden 2006). Also, there are areas, for example, in many Eastern Europe and South America countries, where the prevalence of caries at 12‐year olds has been reported to be moderate or high (WHO 2003). On the other hand, it has been stated that the caries progression rate in permanent teeth has changed and has become slower during recent decades (Whelton 2004).
In addition to preventing caries on teeth surfaces, sealants are increasingly considered as an active agent in controlling and managing caries on the occlusal and approximal surfaces (Splieth 2010). The first material used for pit and fissure sealing was methyl cyanoacrylate (Cueto 1967). Later, a viscous resin (BIS‐GMA) was developed by Buonocore (1970) and this material formed a basis for the development of numerous resin‐based sealants/composites available today. The other main type of pit and fissure sealant materials presently used is glass ionomer cement, used either as the original chemically curable type or as light curable type which is modified with resin for rapid initiation of the curing process. Later, in the 1990s, novel materials called compomers (polyacid‐modified composite resins) were introduced (Nicholson 2007; Ruse 1999).
The resin‐based sealants are divided into generations according to their mechanism for polymerisation or their content. The development of sealants has progressed from first generation sealants, which were activated with ultraviolet light, through to second and third generation sealants, which are autopolymerised and visible‐light activated, and finally to fourth generation sealants containing fluoride. First generation sealants are no longer marketed. The effectiveness of resin‐based sealants has been demonstrated in many studies (Llodra 1993; Mejàre 2003) and the effectiveness depends on the longevity of sealant coverage (i.e. clinical retention) (Ripa 1993). Whether the fluoride release from sealants has any additional beneficial effects in caries prevention is questionable (Carlsson 1997).
The second main type of sealant material is glass ionomer cements, which were introduced in 1974 by McLean and Wilson (McLean 1974). Since then, studies on these sealants have been conducted by several researchers (Boksman 1987; Forss 1998; Mejàre 1990; Shimokobe 1986). However, the results of glass ionomer sealant studies have so far been contradictory. Glass ionomer cements contain fluoride and they are thought to prevent caries through their fluoride release. The main disadvantage of glass ionomer sealants has been inadequate retention. Nevertheless, it has been suggested that glass ionomer sealants, through their fluoride release, can prevent the development of caries even after the visible loss of sealant material (Seppä 1991).
Some reports have been published concerning adverse effects of dental sealants such as allergic reactions and oestrogen‐like effects. Chemically curable glass ionomer cements are considered safe but a few allergic reactions have been reported with resin‐based materials (ADA 2003). Some resin‐based sealant materials have recently been incorporated into discussion of possible oestrogen‐like effects of resin Bisphenol A (BPA). This chemical substance is widely used in manufacturing of plastics, which are commonly used in ordinary consumer products. Pure BPA is rarely used as an ingredient in dental materials (ADA 2010). However, some resin‐based sealants can include its derivatives. A transient amount of Bisphenol A (BPA) has been detected in the saliva of some patients directly after sealant application (Arenholt 1999; Schmalz 1999; Zimmerman‐Downs 2010). Of the potential oestrogenicity of BPA derivatives there is very little research (Fleisch 2010).
The current evidence suggests that patients are not at risk for oestrogen‐like effects when sealants are used (ADA 2010; Azarpazhooh 2008; Fleisch 2010).
Why it is important to do this review
Although sealants are effective in preventing caries, their efficacy may be related to the caries risk levels and to the caries progression rate in the population.
Objectives
Primary objectives
-
To evaluate the caries prevention of pit and fissure sealants versus no treatment in children and adolescents. This was carried out for different background levels of caries in the population.
-
To compare the effect of different sealant materials for preventing dental caries in children and adolescents.
Secondary objectives
-
To document and report on data concerning the retention of sealants.
-
To document and report on any data concerning the safety of sealants and possible harmful effects.
The secondary objectives simply entail reporting. Retention of sealants is not studied here as a main outcome.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised or quasi‐randomised controlled trials of at least 12 months in duration in which sealants were used for preventing caries in children and adolescents. Both parallel group and split‐mouth study designs were included. The unit of randomisation could be individual, group (school, school class etc.), tooth or tooth pair.
We decided to consider only studies with a full‐text report in this review. Studies reported only as abstracts were excluded. This is because there is evidence that there are discrepancies between data reported in the abstract and the final published full report and that information on trial quality indicators is often lacking (Chokkalingam 1998; Hopewell 2006). Thus we saw that the full‐text report is required to ensure reliable data extraction and assessment of the risk of bias. To diminish the risk of publication bias we contacted authors of potential abstracts to obtain information whether a full‐text report of the study (unpublished or published) was available.
Types of participants
Children and adolescents from the general population, under 20 years of age at the start of the study.
Types of interventions
The review was concerned with:
(A) comparing sealant material with a control without sealant (all sealant materials accepted except the first generation resin‐based sealants) and
(B) comparing one type of fissure sealant with another sealant.
The control teeth or control groups in this review were those that did not have a sealant placed (A). When comparing the effectiveness of resin sealants with the effectiveness of other sealant materials, the resin sealant group was used as a control group (B).
We included studies where sealants were placed on the occlusal or approximal surfaces of permanent premolar or molar teeth for the purpose of preventing caries, regardless of who did the application. Applications of sealants could be either on sound surfaces or on enamel lesions not previously sealed.
The sealant application method used in the study could be either that of (a) direct application on the tooth surface or (b) application after mechanically preparing the tooth surface.
We excluded studies where fissure sealants were used concurrently with fillings.
Studies that tested any other caries preventive treatments (such as fluoride varnishes) concurrently with the sealants were not included in this review. Studies where fissure sealants were used concurrently both in test and control groups with fluoride toothpaste or with fluoridated water were included.
Types of outcome measures
Incidence of caries expressed in terms of caries or no caries on occlusal surfaces of permanent molar teeth.
Caries was defined as caries in the dentine. Enamel lesions were regarded as sound surfaces.
Search methods for identification of studies
Electronic searches
For the identification of studies included or considered for this review, we developed detailed search strategies for each database searched. These were based on the search strategy developed for MEDLINE (OVID) but revised appropriately for each database. The search strategy used a combination of controlled vocabulary and free text terms and was linked with the Cochrane Highly Sensitive Search Strategy (CHSSS) for identifying randomised trials (RCTs) in MEDLINE: sensitivity maximising version (2008 revision) as referenced in Chapter 6.4.11.1 and detailed in box 6.4.c of the Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). Details of the MEDLINE search are provided in Appendix 3. The search of EMBASE was linked to the Cochrane Oral Health Group filter for identifying RCTs.
Detailed search strategies are described in the appendices.
The following electronic databases were searched.
-
The Cochrane Oral Health Group's Trials Register (to 1 November 2012) (Appendix 1).
-
The Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2012, Issue 7) (Appendix 2).
-
MEDLINE via OVID (1946 to 1 November 2012) (Appendix 3).
-
EMBASE via OVID (1980 to 1 November 2012) (Appendix 4).
-
SCISEARCH, CAplus, INSPEC, NTIS, and PASCAL via STN Easy (to 1 September 2012) (Appendix 5).
-
Centre for Reviews and Dissemination databases (CRD): DARE (Database of Abstracts of Reviews of Effectiveness), NHS EED (NHS Economic Evaluation Database), HTA (Health Technology Assessment) via the CAIRS web interface to 29 March 2012 and thereafter via Metaxis interface to September 2012) (Appendix 6).
-
The System for Information on Grey Literature in Europe (SIGLE) via STN Easy (1976 to December 2004) (Appendix 7). SIGLE is currently known as OpenGrey. The search strategy was adapted to the new system's search language. The search was run on the Exalead search engine at http://www.opengrey.eu/ (from 9 October 2010 to 1 September 2012).
-
JICST‐EPLUS via STN Easy (to February 2002) (Appendix 8). An updated search of this database was planned in the 2008 review update but the database was no longer available via STN Easy (closed in 2007).
-
ClinicalTrials.gov (to 23 July 2012) (Appendix 9).
In this update, search strategies were amended for the following databases: MEDLINE, the Cochrane Oral Health Group's Trials Register, CENTRAL, SCISEARCH, CAplus, INSPEC, NTIS, PASCAL, and CRD, DARE, NHS EED. Amendments to the search strategies for each of these databases are described in Appendix 1; Appendix 2; Appendix 3; Appendix 5; and Appendix 6.
There were no language or publication restrictions.
Searching other resources
We analysed the reference lists from already identified trials and review articles for additional, appropriate studies.
For the 2008 review version, seven companies known to manufacture sealant materials were contacted and data and references from all published and unpublished trials on sealants were requested.
Data collection and analysis
Selection of studies
Two review authors (Anneli Ahovuo‐Saloranta (AAS) and Helena Forss (HF)) independently carried out the selection of papers on the basis of the title, keywords and abstract, and the decisions about eligibility. The full‐text of every study considered for inclusion was obtained. If the information relevant to the inclusion criteria was not available in the abstract or if the title was relevant but the abstract was not available, the full‐text of the report was obtained.
Data extraction and management
Data were extracted independently and in duplicate by two review authors (AAS, HF) using a previously prepared data extraction form. The extraction form was pilot‐tested independently by two review authors in the previous review version (AAS, Anne Hiiri (AH)) with a sample of studies to be included. Data were to be excluded if agreement could not be reached, though this was not the case in this review.
We contacted the authors of the included studies to obtain additional information on the data if needed.
We extracted the following data.
(1) Study characteristics: study design, the year the study began, location where the study was conducted (country and setting where participants were recruited), length of follow‐up/s, and funding.
(2) Participant characteristics: number of children and number of their teeth in treatment and control groups at start and after follow‐up; age (range) and mean age at start; caries severity at start (average number of decayed, missing and filled deciduous teeth (dmft); decayed, missing and filled deciduous surfaces (dmfs); decayed, missing and filled permanent surfaces (DMFS); decayed, filled permanent surfaces (DFS); or other measure); background exposure to fluoride sources (toothpaste, water etc.); criteria for accepting subjects into the study (intact surfaces or incipient caries lesions allowed).
(3) Intervention characteristics: different intervention comparisons (sealant versus control without sealant or sealant versus sealant), materials used in the study, reapplication of sealants, isolation method, who applied the sealants.
(4) Outcome characteristics: incidence of caries, as measured by caries in dentine involved per occlusal surface.
If during the study a filling had been put on the occlusal surface or the tooth had been extracted because of caries, it was coded as caries. Data presented only in graphs and figures were extracted whenever possible. The data of the included studies are collected in the Additional Table 1 and Table 2.
Also the following secondary outcomes were recorded when reported: retention of sealants (data collected in Additional Table 3) and safety of sealants.
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 12 MONTHS | ||||||||
| Split‐mouth studies | Study | Both sound | FS sound / | FS carious / | Both carious | Proportion of the decayed control tooth surfaces to total control surfaces | RR (95% CI) based on paired data | Becker‐Balagtas marginal |
| Bojanini 1976 | 188 | 79 | 6 | 2 | 0.29 | RR = 0.099 (0.049, 0.201) | OR = 0.07 (0.03, 0.15) ICC 0.02 | |
| Charbeneau 1979 | 104 | 82 | 5 | 11 | 0.46 | RR = 0.172 (0.107, 0.276) | OR = 0.10 (0.06, 0.17) ICC 0.13 | |
| Sheykholeslam 1978 | 132 | 49 | 2 | 3 | 0.28 | RR = 0.096 (0.040, 0.229) | OR = 0.07 (0.03, 0.18) ICC 0.12 | |
| Split‐mouth studies | Study | FS sound | FS carious | Control sound | Control carious | Proportion of the decayed control tooth surfaces to total control surfaces | Becker‐Balagtas marginal | |
| Erdoğan 1987 | 103 | 15 | 96 | 22 | 0.19 | OR = 0.64 ICC 0.05 | ||
| Richardson 1978 | 375 | 18 | 300 | 93 | 0.24 | OR = 0.15 ICC 0.05 | ||
| Rock 1978 | 347 | 15 | 316 | 46 | 0.13 | OR = 0.30 ICC 0.05 | ||
| POOLED | OR = 0.16 | |||||||
| Split‐mouth studies without summary data of tooth pairs | Study | Description of the data | ||||||
| Reisbick 1982 | Paired summary data reported only by tooth sites (3 sites per occlusal surface) but not by tooth surfaces which were the analysis units in this review. However, effectiveness based on paired tooth surfaces was reported to be 90% at 14 months. | |||||||
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 24 MONTHS | ||||||||
| Split‐mouth studies | Study | Both sound | FS sound / | FS carious / | Both carious | Proportion of the decayed control tooth surfaces to total control surfaces | RR (95% CI) based on paired data | Becker‐Balagtas marginal |
| Brooks 1979 | 144 | 64 | 3 | 22 | 0.37 | RR = 0.29 | OR = 0.21 (0.14, 0.31) ICC 0.37 | |
| Charbeneau 1979 | 53 | 100 | 4 | 29 | 0.69 | RR = 0.256 | OR = 0.10 (0.06, 0.15) ICC 0.19 | |
| Sheykholeslam 1978 | 85 | 79 | 1 | 10 | 0.51 | RR = 0.124 | OR = 0.06 (0.03, 0.12) ICC 0.21 | |
| Split‐mouth studies | Study | FS sound | FS carious | Control sound | Control carious | Proportion of the decayed control tooth surfaces to total control surfaces | Becker‐Balagtas marginal | |
| Bojanini 1976 | 245 | 7 | 159 | 93 | 0.37 | OR = 0.05 ICC 0.05 | ||
| Richardson 1978 | 326 | 26 | 222 | 130 | 0.37 | OR = 0.14 ICC 0.05 | ||
| Parallel group studies | Study | Description of the data | OR (95% CI) | |||||
| Liu 2012 | OR based on the model of the multilevel GEE logistic regression. | OR = 0.32 | ||||||
| POOLED | OR = 0.12 | |||||||
| Split‐mouth studies without summary data of tooth pairs | Study | Description of the data | ||||||
| Reisbick 1982 | Paired summary data reported only by tooth sites (3 sites per occlusal surface) but not by tooth surfaces which were the analysis units in this review. However, effectiveness based on paired tooth surfaces was reported to be 80% at 20 months. | |||||||
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 32‐36 MONTHS | ||||||||
| Split‐mouth studies | Study | Both sound | FS sound / | FS carious / | Both carious | Proportion of the decayed control tooth surfaces to total control surfaces | RR (95% CI) based on paired data | Becker‐Balagtas marginal |
| Brooks 1979 | 111 | 63 | 4 | 23 | 0.43 | RR = 0.314 | OR = 0.21 (0.14, 0.31) ICC 0.34 | |
| Charbeneau 1979 | 45 | 96 | 5 | 47 | 0.74 | RR = 0.364 | OR = 0.13 (0.09, 0.19) ICC 0.23 | |
| Hunter 1988 | 302 | 163 | 9 | 35 | 0.39 | RR = 0.222 | OR = 0.15 (0.11, 0.20) ICC 0.26 | |
| Split‐mouth studies | Study | FS sound | FS carious | Control sound | Control carious | Proportion of the decayed control tooth surfaces to total control surfaces | Becker‐Balagtas marginal | |
| Bojanini 1976 | 250 | 22 | 128 | 144 | 0.53 | OR = 0.08 | ||
| Sheykholeslam 1978 | 142 | 22 | 63 | 101 | 0.62 | OR = 0.10 | ||
| Richardson 1978 | 279 | 58 | 176 | 161 | 0.48 | OR = 0.23 | ||
| Rock 1978 | 253 | 55 | 222 | 86 | 0.28 | OR = 0.56 ICC 0.05 | ||
| POOLED | OR = 0.17 | |||||||
| Split‐mouth studies without summary data of tooth pairs | Study | Description of the data | ||||||
| Reisbick 1982 | Paired summary data reported only by tooth sites (3 sites per occlusal surface) but not by tooth surfaces which were the analysis units in this review. However, effectiveness based on paired tooth surfaces was reported to be 70% at 32 months. | |||||||
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 48‐54 MONTHS | ||||||||
| Split‐mouth studies | Study | Both sound | FS sound / | FS carious / | Both carious | Proportion of the decayed control tooth surfaces to total control surfaces | RR (95% CI) based on paired data | Becker‐Balagtas marginal |
| Brooks 1979 | 61 | 67 | 3 | 37 | 0.62 | RR = 0.385 | OR = 0.19 (0.13, 0.28) ICC 0.35 | |
| Charbeneau 1979 | 37 | 81 | 3 | 64 | 0.78 | RR = 0.462 | OR = 0.16 (0.11, 0.23) ICC 0.31 | |
| Split‐mouth studies | Study | FS sound | FS carious | Control sound | Control carious | Proportion of the decayed control tooth surfaces to total control surfaces | Becker‐Balagtas marginal | |
| Erdoğan 1987 (54 months) | 82 | 14 | 67 | 29 | 0.30 | OR = 0.39 | ||
| Richardson 1978 (48 months) | 262 | 68 | 151 | 179 | 0.54 | OR = 0.22 | ||
| POOLED | OR = 0.21 | |||||||
| Parallel group studies | Study | Description of the data | RR (95% CI) | |||||
| Bravo 2005 | Data are based on requested risk ratio (RR) value with cluster corrected standard error (SE). | RR = 0.24 | ||||||
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 5 YEARS | ||||||||
| Split‐mouth studies | Study | FS sound | FS carious | Control sound | Control carious | Proportion of the decayed control tooth surfaces to total control surfaces | Becker‐Balagtas marginal | |
| Richardson 1978 | 246 | 85 | 157 | 174 | 0.53 | OR = 0.31 | ||
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 6 YEARS | ||||||||
| Split‐mouth studies | Study | Both sound | FS sound / | FS carious / | Both carious | Proportion of the decayed control tooth surfaces to total control surfaces | RR (95% CI) based on paired data | Becker‐Balagtas marginal |
| Brooks 1979 | 50 | 57 | 5 | 38 | 0.63 | RR = 0.45 | OR = 0.23 (0.16, 0.35) ICC 0.329 | |
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 7 YEARS | ||||||||
| Split‐mouth studies | Study | Both sound | FS sound / | FS carious / | Both carious | Proportion of the decayed control tooth surfaces to total control surfaces | RR (95% CI) based on paired data | Becker‐Balagtas marginal |
| Brooks 1979 | 29 | 41 | 2 | 30 | 0.70 | RR = 0.45 | OR = 0.20 (0.12, 0.32) ICC 0.355 | |
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 9 YEARS | ||||||||
| Parallel group studies | Study | Description of the data | RR (95% CI) | |||||
| Bravo 2005 | Data are based on requested risk ratio (RR) value with cluster corrected standard error (SE). | RR = 0.35 | ||||||
| GLASS IONOMER (GI) SEALANT VERSUS RESIN SEALANT: 12 MONTHS | ||||||||
| Split‐mouth studies | Study | GI sound | GI carious | Resin sound | Resin carious | Becker‐Balagtas marginal | ||
| Dhar 2012 | 23 | 2 | 24 | 1 | OR = 2.09 P = 0.76 | |||
| Dhar 2012 | 25 | 0 | 25 | 0 | Not estimable | |||
| Karlzen‐Reuterving 1995 (no difference) | 72 | 0 | 70 | 2 | OR = 0.19 P = 0.25 | |||
| Rock 1996 (no difference) | 151 | 7 | 157 | 1 | OR = 7.28 (0.91, 58.12) P = 0.07 | |||
| Sipahier 1995 (no difference) | 80 | 6 | 81 | 5 | OR = 1.22 P = 0.75 | |||
| RESIN‐MODIFIED GLASS IONOMER (GI) VERSUS RESIN SEALANT: 12 MONTHS | ||||||||
| Split‐mouth studies | Study | GI sound | GI carious | Resin sound | Resin carious | Becker‐Balagtas marginal | ||
| Baseggio 2010 (no difference) | 640 | 0 | 640 | 0 | Not estimable | |||
| Parallel group studies | Study | Description of the data | OR (95% Cl) | |||||
| Amin 2008 (no difference) | Clustered data (2 teeth per child). | OR = 1.08 | ||||||
| GLASS IONOMER (GI) SEALANT VERSUS RESIN SEALANT: 24 MONTHS | ||||||||
| Split‐mouth studies | Study | Both sound | GI sound / | GI carious / | Both carious | RR (95% CI) based on paired data | Becker‐Balagtas marginal | |
| Poulsen 2001 (resin slightly better) | 191 | 2 | 9 | 1 | RR = 3.33 | OR = 3.46 (1.03, 11.63) | ||
| Ganesh 2006 (no difference) | 100 | 0 | 0 | 0 | Not estimable | Not estimable | ||
| Mills 1993 (no difference) | 59 | 0 | 0 | 0 | Not estimable | Not estimable | ||
| Split‐mouth studies | Study | GI sound | GI carious | Resin sound | Resin carious | Becker‐Balagtas marginal | ||
| Dhar 2012 | 23 | 2 | 22 | 3 | OR = 0.64 P = 0.81 | |||
| Dhar 2012 | 24 | 1 | 21 | 4 | OR = 0.22 P = 0.38 | |||
| Forss 1998 (no difference) | 144 | 7 | 144 | 7 | OR = 1 (0.35, 2.85) | |||
| Karlzen‐Reuterving 1995 (no difference) | 71 | 1 | 70 | 2 | OR = 0.49 (0.05, 5.25) P = 0.77 | |||
| Rock 1996 (resin better) | 116 | 16 | 130 | 2 | OR = 8.96 (2.07, 38.82) | |||
| Williams 1996 (resin better) | 274 | 21 | 289 | 6 | OR = 3.69 (1.50, 9.09) P = 0.004 | |||
| Parallel group studies | Study | Description of the data | OR (95% Cl) | |||||
| Chen 2012 | Data of glass ionomer sealant groups were combined (Ketac Molar Easymix with or without LED high energy curing light). | OR = 1.67 | ||||||
| RESIN‐MODIFIED GLASS IONOMER (GI) VERSUS RESIN SEALANT: 24 MONTHS | ||||||||
| Split‐mouth studies | Study | GI sound | GI carious | Resin sound | Resin carious | Becker‐Balagtas marginal | ||
| Baseggio 2010 | 583 | 57 | 620 | 20 | OR = 3.03 (1.82, 5.05) P < 0.0001 | |||
| Parallel group studies | Study | Description of the data | OR (95% Cl) | |||||
| Amin 2008 (no difference) | Clustered data (2 teeth per child). | OR = 1.14 | ||||||
| GLASS IONOMER (GI) SEALANT VERSUS RESIN SEALANT: 36‐48 MONTHS | ||||||||
| Split‐mouth studies | Study | Both sound | GI sound / | GI carious / | Both carious | RR (95% CI) based on paired data | Becker‐Balagtas marginal | |
| Poulsen 2001 | 156 | 6 | 37 | 7 | RR = 3.385 | OR = 4.03 (2.23, 7.29) | ||
| Arrow 1995 | 378 | 28 | 3 | 3 | RR = 0.194 | OR = 0.18 (0.08, 0.41) P < 0.001 | ||
| Kervanto‐Seppälä 2008 | 625 | 5 | 25 | 2 | RR = 3.857 | OR = 3.98 (1.80, 8.80) P < 0.001 | ||
| Split‐mouth studies | Study | GI sound | GI carious | Resin sound | Resin carious | Becker‐Balagtas marginal | ||
| Karlzen‐Reuterving 1995 (no difference) | 71 | 1 | 69 | 3 | OR = 0.32 (0.03, 3.03) P = 0.63 | |||
| Rock 1996 (resin better) | 106 | 24 | 126 | 4 | OR = 7.13 (2.45, 20.76) P < 0.001 | |||
| Williams 1996 (no difference) | 200 | 22 | 206 | 16 | OR = 1.42 (0.73, 2.73) P = 0.34 | |||
| Study | Description of the data | RR (95% CI) | ||||||
| Parallel group studies | Beiruti 2006 (ionomer better) | Data are based on reported risk ratio (RR) value with cluster corrected standard error (SE). | After 3 years: After 4 years: | |||||
| RESIN‐MODIFIED GLASS IONOMER (GI) VERSUS RESIN SEALANT: 36 MONTHS | ||||||||
| Study | GI sound | GI carious | Resin sound | Resin carious | Becker‐Balagtas marginal | |||
| Split‐mouth studies | Baseggio 2010 (resin better) | 502 | 126 | 572 | 56 | OR = 2.56 (1.84, 3.56) P < 0.001 | ||
| Raadal 1996 (resin better) | 64 | 9 | 73 | 0 | OR = 11.38 (1.47, 88.42) P = 0.012 | |||
| POOLED | OR = 2.66 P < 0.00001 Het. Chi2 | |||||||
| GLASS IONOMER (GI) SEALANT VERSUS RESIN SEALANT: 5 YEARS | ||||||||
| Study | Description of the data | RR (95% CI) | ||||||
| Parallel group studies | Beiruti 2006 (ionomer better) | Data are based on reported risk ratio (RR) value with cluster corrected standard error (SE). | RR = 0.28 | |||||
| Barja‐Fidalgo 2009 | Raw data were obtained from the authors because several of a child's teeth had been sealed (a child is a cluster). Raw data were used in calculations. | RR = 0.38 | ||||||
| POOLED | RR = 0.30 P = 0.0005 Het. Chi2 | |||||||
| GLASS IONOMER (GI) SEALANT VERSUS RESIN SEALANT: 7 YEARS | ||||||||
| Study | Both sound | GI sound / | GI carious / | Both carious | RR (95% CI) based on paired data | Becker‐Balagtas marginal | ||
| Split‐mouth studies | Forss 1998 | 66 | 8 | 15 | 8 | RR = 1.44 (0.88, 2.35) | OR = 1.57 (0.86, 2.89) P = 0.21 | |
| POLYACID‐MODIFIED RESIN COMPOSITE VERSUS RESIN SEALANT: 24 MONTHS | ||||||||
| Study | Both sound | Composite sound / | Composite carious / | Both carious | Becker‐Balagtas marginal | |||
| Split‐mouth studies | Lampa 2004 | 41 | 3 | 0 | 0 | OR = 0.23 (0.03, 1.76) | ||
| Güngör 2004 | 50 | 10 | 8 | 2 | OR = 0.80 (0.33, 1.97) | |||
| POOLED | OR = 0.65 (0.29, 1.48) P = 0.31 Het. Chi2 | |||||||
CI = confidence interval; df = degrees of freedom; ICC = intra‐cluster correlation coefficient; OR = odds ratio; RR = risk ratio.
| Comparison | Control number | Control mean | Control SD | Test number | Test mean | Test SD | Mean DFS diff. | 95% CI | P value |
| Control versus resin | 143 | 0.70 | 0.96 | 133 | 0.05 | 0.57 | 0.65 | 0.47 to 0.83 | < 0.00001 |
| Control versus GI | 143 | 0.70 | 0.96 | 261 | 0.52 | 1.09 | 0.18 | ‐0.03 to 0.39 | 0.09 |
| Resin versus GI | 133 | 0.05 | 0.57 | 261 | 0.52 | 1.09 | ‐0.47 | ‐0.63 to ‐0.31 | < 0.00001 |
CI = confidence interval; DFS = decayed and filled occlusal surfaces; GI = glass ionomer; SD = standard deviation.
| Time | Study | Sealant | Complete (%) | Partial (%) | Lost (%) | Decayed or filled (%) | Total (%) |
| Sealant retention: | Amin 2008 | FUJI II LC (resin‐modified glass ionomer) | 46 | 27 | 27 | = 100 | |
| Amin 2008 | Tetric Flow, Helioseal F (resins, data combined) | 82 | 12.5 | 5.5 | = 100 | ||
| Baseggio 2010 | Vitremer (resin‐modified glass ionomer) | 14 | 33 | 54 | = 101 | ||
| Baseggio 2010 | Fluoroshield (resin) | 94 | 6 | 0 | = 100 | ||
| Bojanini 1976 | Delton (resin) | 91 | 6 | 3 | = 100 | ||
| Charbeneau 1979 | Kerr (resin) | 79 | 17 | 4 | = 100 | ||
| de Luca‐Fraga 2001 | Vitremer (resin‐modified glass ionomer) | 86 | 14 | 0 | = 100 | ||
| de Luca‐Fraga 2001 | Dyract (polyacid‐modified composite resin) | 96 | 2 | 2 | = 100 | ||
| Dhar 2012 | GC Fuji Ionomer VII light pink (glass ionomer‐based sealant), without preparation | 0 | 16 | 84 | = 100 | ||
| Dhar 2012 | Clinpro pink (fluoride releasing resin‐based sealant), without preparation | 24 | 28 | 48 | = 100 | ||
| Erdoğan 1987 | Delton (resin) | 77 | 19 | 4 | = 100 | ||
| Karlzen‐Reuterving 1995 | FUJI III (ionomer) | 72 | 17 | 11 | = 100 | ||
| Karlzen‐Reuterving 1995 | Delton (resin) | 97 | 3 | 0 | = 100 | ||
| Pardi 2005 | Vitremer (resin‐modified glass ionomer) | 77 | 17 | 6 | = 100 | ||
| Pardi 2005 | Revolution (flowable resin composite) | 84 | 14 | 2 | = 100 | ||
| Pardi 2005 | Dyract Flow (compomer) | 76 | 22 | 2 | = 100 | ||
| Reisbick 1982 (14 months) | Oralin (chemically polymerized resin) | 89 | |||||
| Richardson 1978 | resin (the name of the material not stated) | 90 | 6 | 4 | = 100 | ||
| Rock 1978 | Delton (resin) | 53 | 22 | 25 | = 100 | ||
| Rock 1996 | Baseline (ionomer) | 0 | 0 | 96 | 4 | = 100 | |
| Rock 1996 | Fluoroshield (resin) | 76.6 | 9.5 | 13.3 | 1.3 | = 101 | |
| Sheykholeslam 1978 | Delton (resin) | 92 | 5 | 0 | 3 | = 100 | |
| Sipahier 1995 | Ketac‐Silver (glass ionomer‐silver‐cermet cement) | 23 | 34 | 43 | = 100 | ||
| Sipahier 1995 | Delton (resin) | 41 | 48 | 11 | = 100 | ||
| Sealant retention: 24 months | Amin 2008 | FUJI II LC (resin‐modified glass ionomer) | 25 | 21 | 54 | = 100 | |
| Amin 2008 | Tetric Flow, Helioseal F (resins, data combined) | 83 | 9 | 8 | = 100 | ||
| Baseggio 2010 | Vitremer (resin‐modified glass ionomer) | 9 | 12 | 80 | = 101 | ||
| Baseggio 2010 | Fluoroshield (resin) | 94 | 6 | 0 | = 100 | ||
| Bojanini 1976 | Delton (resin) | 89 | 7 | 4 | = 100 | ||
| Brooks 1979 | Delton (resin) | 84 | 10 | 6 | = 100 | ||
| Charbeneau 1979 | Kerr (resin) | 71 | 18 | 11 | = 100 | ||
| Chen 2012 | Ketac Molar Easymix (glass ionomer) | 22 | |||||
| Chen 2012 | Ketac Molar Easymix plus LED high energy curing light (glass ionomer) | 20 | |||||
| Chen 2012 | Clinpro Sealant (fluoride releasing resin‐based sealant) | 14 | |||||
| Dhar 2012 | GC Fuji Ionomer VII light pink (glass ionomer‐based sealant), without preparation | 0 | 0 | 100 | = 100 | ||
| Dhar 2012 | Clinpro pink (fluoride releasing resin‐based sealant), without preparation | 0 | 20 | 80 | = 100 | ||
| Forss 1998 | Fuji III (ionomer) | 26 | 26 | 48 | = 100 | ||
| Forss 1998 | Light‐cured Delton (resin) | 82 | 9 | 9 | = 100 | ||
| Ganesh 2006 | Fuji VII (ionomer) | 2 | 68 | 30 | = 100 | ||
| Ganesh 2006 | Concise (resin) | 4 | 66 | 30 | = 100 | ||
| Güngör 2004 | Dyract Seal (PMRC) | 80 | 16 | 4 | = 100 | ||
| Güngör 2004 | Delton FS+ (resin) | 71 | 16 | 13 | = 100 | ||
| Karlzen‐Reuterving 1995 | FUJI III (ionomer) | 43 | |||||
| Karlzen‐Reuterving 1995 | Delton (resin) | 90 | 10 | 0 | = 100 | ||
| Lampa 2004 | Dyract Seal (PMRC) | 16 | 44 | 40 | = 100 | ||
| Lampa 2004 | Delton DDS (resin) | 66 | 23 | 11 | = 100 | ||
| Liu 2012 | Clinpro Sealant (fluoride releasing resin‐based sealant) | 54 | |||||
| Mills 1993 | Ketac‐Silver (ionomer) | 83 | 12 | 6 | = 101 | ||
| Mills 1993 | Delton (resin) | 58 | 17 | 25 | = 100 | ||
| Pardi 2005 | Vitremer (resin‐modified glass ionomer) | 47 | 37 | 16 | = 100 | ||
| Pardi 2005 | Revolution (flowable resin composite) | 76 | 17 | 7 | = 100 | ||
| Pardi 2005 | Dyract Flow (compomer) | 58 | 28 | 14 | = 100 | ||
| Poulsen 2001 | Fuji III (ionomer) | 9 | 9 | 82 | = 100 | ||
| Poulsen 2001 | Delton (resin) | 80 | 7 | 13 | = 100 | ||
| Reisbick 1982 | Oralin (chemically polymerized resin) | 82 | |||||
| Richardson 1978 | resin (the name of the material not stated) | 86 | 9 | 5 | = 100 | ||
| Rock 1996 | Baseline (ionomer) | 0 | 0 | 88 | 12 | = 100 | |
| Rock 1996 | Fluoroshield (resin) | 70 | 10 | 19 | 1 | = 100 | |
| Sheykholeslam 1978 | Delton (resin) | 85 | 7 | 2 | 6 | = 100 | |
| Songpaisan 1995 | Fuji III (ionomer) | < 1 | |||||
| Songpaisan 1995 | Delton (resin) | 85 | |||||
| Tagliaferro 2011 | (resin‐modified glass ionomer) | 16 | |||||
| Williams 1996 | Fuji III (ionomer) | 4 | 3 | 93 | = 100 | ||
| Williams 1996 | Delton (resin) | 80 | 2 | 18 | = 100 | ||
| Sealant retention: | Baseggio 2010 | Vitremer (resin‐modified glass ionomer) | 5 | 6 | 89 | = 100 | |
| Baseggio 2010 | Fluoroshield (resin) | 91 | 8 | 1 | = 100 | ||
| Beiruti 2006 | Fuji IX (ionomer) | 60 | |||||
| Beiruti 2006 | Visio‐Seal (composite resin) | 60 | |||||
| Bojanini 1976 | Delton (resin) | 87 | 9 | 4 | = 100 | ||
| Brooks 1979 | Delton (resin) | 80 | 10 | 10 | = 100 | ||
| Charbeneau 1979 | Kerr (resin) | 61 | 23 | 16 | = 100 | ||
| Hunter 1988 | Delton (resin) | 64 | 19 | 8 | 9 | = 100 | |
| Karlzen‐Reuterving 1995 | FUJI III (ionomer) | 28 | 35 | 37 | = 100 | ||
| Karlzen‐Reuterving 1995 | Delton (resin) | 79 | 21 | 0 | = 100 | ||
| Poulsen 2001 | Fuji III (ionomer) | 3 | 7 | 89 | = 100 | ||
| Poulsen 2001 | Delton (resin) | 74 | 16 | 10 | = 100 | ||
| Raadal 1996 | Vitrebond (resin‐reinforced glass ionomer) | 5 | 4 | 91 | = 100 | ||
| Raadal 1996 | Concise White Sealant (resin) | 97 | 1.5 | 1.5 | = 100 | ||
| Reisbick 1982 (32 months) | Oralin (chemically polymerized resin) | 78 | |||||
| Richardson 1978 | resin (the name of the material not stated) | 75 | 14 | 11 | = 100 | ||
| Rock 1978 | Delton (resin) | 41 | 16 | 43 | = 100 | ||
| Rock 1996 | Baseline (ionomer) | 0 | 0 | 81.5 | 18.4 | = 100 | |
| Rock 1996 | Fluoroshield (resin) | 70 | 9.2 | 17.7 | 3.2 | = 100 | |
| Sheykholeslam 1978 | Delton (resin) | 77 | 9 | 4 | ? | ||
| Kervanto‐Seppälä 2008 | In total 559 tooth pairs: in 1% ionomer retained, resin lost; in 89% ionomer lost, resin retained; in 6% ionomer retained, resin retained; in 4% ionomer lost, resin lost = 100% | ||||||
| Sealant retention: | Arrow 1995 | In total 465 tooth pairs: in 10% ionomer retained, resin lost; in 18% ionomer lost, resin retained; in 10% ionomer retained, resin retained; in 62% ionomer lost, resin lost = 100% | |||||
| Sealant retention: | Charbeneau 1979 | Kerr (resin) | 52 | 26 | 22 | = 100 | |
| Richardson 1978 | resin (the name of the material not stated) | 69 | 10 | 21 | = 100 | ||
| Williams 1996 | Fuji III (ionomer) | 4 | 2 | 94 | = 100 | ||
| Williams 1996 | Delton (resin) | 61 | 11 | 28 | = 100 | ||
| Sealant retention: | Brooks 1979 | Delton (resin) | 72 | 14 | 14 | = 100 | |
| Erdoğan 1987 | Delton (resin) | 74 | 22 | 4 | = 100 | ||
| Sealant retention: | Barja‐Fidalgo 2009 | Fuji IX (ionomer) | 29 | 29 | 42 | = 100 | |
| Barja‐Fidalgo 2009 | Delton (resin) | 21 | 21 | 58 | = 100 | ||
| Beiruti 2006 | Fuji IX (ionomer) | 88 | |||||
| Beiruti 2006 | Visio‐Seal (composite resin) | 86 | |||||
| Richardson 1978 | resin (the name of the material not stated) | 67 | 10 | 23 | = 100 | ||
| Sealant retention: | Brooks 1979 | Delton (resin) | 68 | 16 | 16 | = 100 | |
| Sealant retention: | Brooks 1979 | Delton (resin) | 66 | 14 | 20 | = 100 | |
| Forss 1998 | In total 97 tooth pairs: in 6% ionomer retained, resin lost; in 41% ionomer lost, resin retained; in 4% ionomer retained, resin retained; in 49% ionomer lost, resin lost = 100% | ||||||
| Sealant retention: | Bravo 2005 | Delton (resin) | 39 |
In some studies the results were stated at more than one period of follow‐up. All data were extracted of pre‐selected times, which were 1, 2, 3, 4, 5 years etc. (annually). Meta‐analyses were carried out at these pre‐selected times based on the available data.
(5) Information relating to calibration of examiners and Kappa statistics were also extracted.
Assessment of risk of bias in included studies
Two review authors (AAS, HF) assessed independently the risk of bias in the included studies. Any disagreements between them were resolved by consensus. Attempts were made to contact authors of studies for clarification. As recommended by the Cochrane Handbook for Systematic Reviews of Interventions 5.1.0 (Higgins 2011a) the following six domains were assessed. Within each domain, a description of what happened, as reported in the study, was recorded along with a judgement of either 'Low', 'High' or 'Unclear' risk of bias.
Random sequence generation (selection bias)
Was the method used to generate the allocation sequence appropriate to produce comparable groups? This domain was graded 'Low risk' of bias if the authors described a random component in the sequence generation process (e.g. random number table, coin tossing, drawing of lots). In split‐mouth study designs, we, however, saw that the study could also be graded 'Low risk' of bias in case the method of allocating a tooth to an intervention was not random but quasi‐random (systematic methods that were intended to produce similar groups; e.g. sequence generated by odd or even date of birth or by some rule based on date of admission). Although quasi‐random sequence generation methods include some systematic, non‐random component, we saw that in preventive split‐mouth studies (with mainly sound tooth surfaces) the risk of selection bias is insignificant. Our justification is based on the assumption that there is no right‐left asymmetry between contralateral teeth regarding caries risk, as shown by Larmas 1995 when they evaluated timing of the change from a sound erupting tooth to a filled tooth.
Studies without random or quasi‐random sequence generation were excluded in this review for eliminating selection bias.
Allocation concealment (selection bias)
Was the method used to conceal the allocation sequence appropriate to prevent the allocation being known in advance of, or during, enrolment? This domain was graded 'Low risk' of bias if the authors described adequate concealment (for example, by means of central randomisation, or sequentially numbered, opaque and sealed envelopes), and graded 'High risk' of bias if inadequate concealment was documented (for example, alternation, use of case record numbers, dates of birth or day of the week) or allocation concealment was not used. If there was insufficient or no information on allocation concealment, the judgement was 'Unclear risk'. In split‐mouth study designs, we, however, saw that the study could be graded 'Low risk' of bias in case the information of allocation concealment was incomplete or the sequence generation method was quasi‐random.This is because we saw that in preventive split‐mouth designs the risk of selection bias is insignificant.
Blinding of outcome assessment (detection bias)
Were outcome assessors blinded about the intervention a participant had received? Neither blinding of study personnel nor mostly of participants (performance bias) is possible in sealant studies, since the sealant may be visible. Blinding of the outcome assessor may be possible, and therefore it was the only criterion for judgement of blinding. However, blinding of the outcome assessor is possible only when the sealant is lost or the used sealant materials look similar to each other.
We decided to grade this domain 'Low risk' of bias if the study stated blinded outcome assessment or blinding was indicated (for example, examinations performed independently of previous records), and 'High risk' of bias if the outcome assessor was not blinded. However, we saw that this domain is not a fundamental domain when classifying the overall risk of bias for the main outcomes within a study. This is because in practice the outcome assessor cannot always be truly blinded, even though blinding was intended.
Incomplete outcome data (attrition bias)
How complete were the outcome data for the primary caries outcomes? Were drop‐out rates and reasons for withdrawals reported? Were missing data imputed appropriately? In caries prevention studies follow‐up times can be several years. Studies with a long follow‐up have, however, the problem of high drop‐out rates causing uncertainty in data. We decided to base the judgement of this domain on caries efficacy outcomes at 24 or 36 months (commonly used follow‐up times in sealant studies). In case both follow‐up times were reported, the judgement was based on 24 months. If either of these two follow‐up times was not reported, the judgement was based on the first caries efficacy outcome reported in the study (which in this review should be at least 1 year). However, the risk of bias was separately assessed and reported in the 'Risk of bias' table for caries outcomes despite the follow‐up time, and the assessments were taken into account in the overall risk of bias assessment for caries outcomes within a study.
We decided to grade this domain 'Low risk' of bias if the total proportion of missing outcome data was marginal (less than 5%); or the proportion of the missing outcome data was less than 25% regardless of the follow‐up time and the groups (in parallel group studies) were balanced in numbers for missing data; or missing data have been imputed using appropriate methods. If the proportion of missing data was documented as total proportion (5% to 25%), not by group in parallel group studies, the judgement was 'Unclear risk'. Classifying the missing data over 25% as 'High risk' of bias in all study designs was a pragmatic approach to this domain to make the judgement uniform and transparent. If there were several teeth sealed in a child's mouth (a child is a cluster) the missing outcome data had to be stated (or to be counted) at child level (not at tooth level).
Selective reporting (reporting bias)
Were appropriate outcomes reported and were key outcomes missing? To be included in this review, caries outcomes had to be reported. Studies could, however, report the outcome in different ways, for example incidence of dentinal carious lesion on treated occlusal or approximal surfaces of molars or premolars (yes or no); changes in mean figures of decayed, missing and filled surfaces (DMFS); or progression of caries lesion into enamel or dentine. In this review, free of selective outcome reporting was graded 'Low risk' of bias if the study's pre‐specified caries outcomes had been reported in the pre‐specified way.
Other sources of bias
This domain included information on the comparability of the intervention and control groups, and on possible use of the co‐interventions by group. Both of these features were assessed in their own entries.
(1) We decided to base the judgement of the entry 'Comparability of the groups' on the baseline information given to the groups evaluable at follow‐ups. This is because if only information at the start of the study is available, it is impossible to assess whether the groups are balanced with each other also after the follow‐up time. The comparability of the groups after follow‐up is especially a problem when small studies include children with several teeth under observation and the drop‐out rate is high, even when the drop‐outs of children were balanced in numbers and reasons between groups. If there was no information for the groups evaluable at the follow‐up time, we decided that if the drop‐out rate (regardless of the follow‐up time) was under 25% and the drop‐outs were balanced in numbers and reasons by group, the judgement could be based on the information given for groups at the start of the study.
This entry was graded 'Low risk' of bias if the groups were balanced in demographic characteristics (such as sex, age, and social class), in baseline caries risk level, and in the baseline condition of the tooth surfaces to be treated. The characteristic of baseline condition of the tooth surfaces was considered only in case the study included also teeth with small dentine lesions (but the majority of tooth surfaces was sound or with enamel lesions). This entry was also graded 'Low risk' of bias if there was imbalance of the groups at baseline or after follow‐up or both but that was taken adequately into account in the analyses.
If the baseline characteristics in parallel group studies were not given to the groups available at follow‐up and the drop‐out rate was over 25%, this entry was graded 'Unclear risk'.
(2) To be included in this review, only fluoride toothpaste and fluoridated water were accepted as co‐interventions. The co‐intervention entry was graded 'Low risk' of bias if the groups were balanced in amount and quality of co‐interventions or no co‐interventions were included in the protocol, and graded 'High risk' of bias if the groups received different amount or quality of co‐interventions during the trial. If no information was provided on co‐interventions this entry was graded 'Unclear risk'.
A 'Risk of bias' table was completed for each included study (Risk of bias in included studies in Characteristics of included studies). Results are presented graphically by domain over all studies (Figure 1) and by study (Figure 2).

Risk of bias graph: review authors' judgements about each risk of bias domain presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias domain for each included study.
Summary assessments of risk of bias
To draw conclusions about the overall risk of bias for the caries outcomes within a study, we decided to classify the studies into three categories: studies with low, unclear or high risk of bias. The caries outcomes were determined by data of the included studies (all caries data were extracted of pre‐selected times, which were 1, 2, 3, 4, 5 years etc. (annually)).
Our classification was based on four domains which were seen most fundamental in assessing the risk of bias of studies: allocation concealment, incomplete outcome data, selective outcome reporting, and other bias (baseline comparability of the groups).
The risk of bias categories were defined as follows.
(A) Low risk of bias (plausible bias unlikely to seriously alter the results) if all four fundamental domains defined above were graded as low risk of bias.
(B) Unclear risk of bias (plausible bias that raises some doubt about results) if one or more of the domains were graded as unclear.
(C) High risk of bias (plausible bias that seriously weakens confidence in the results) if one or more domains were graded as high risk of bias.
GRADEprofiler software version 3.2 (GRADEpro 2008) was used to provide the overall grading of the quality of evidence for the caries outcomes for the following comparisons: resin‐based sealants compared to no treatment (summary of findings Table for the main comparison); glass ionomer sealants compared to no treatment (summary of findings Table 2); glass ionomer sealants versus resin sealants (summary of findings Table 3); resin‐modified glass ionomer sealants versus resin sealants (summary of findings Table 4); and polyacid‐modified resin composite versus resin sealants (summary of findings Table 5).
Measures of treatment effect
In all studies except two (Songpaisan 1995; Tagliaferro 2011), the outcome results were presented in dichotomous form.
For the split‐mouth studies, odds ratios were calculated for differences of paired tooth surfaces being carious or not, along with the appropriate standard errors and 95% confidence intervals. The odds ratios were calculated by using the Becker‐Balagtas method outlined in Curtin 2002 by R software version 2.13.1. We chose the Becker‐Balagtas method because we included in this update also studies which reported data only in marginals (as parallel group studies not as 2x2 cross‐classification for paired data) and this method facilitated data synthesis. The intra‐cluster correlation coefficient (ICC) in the studies with data only as marginals was chosen to be the conservative 0.05. In the studies with data presented as tooth pairs, the ICC was calculated from the data.
In the previous version, only those split‐mouth studies, which stated data as tooth pairs, were included. In that review version, risk ratios were calculated for the paired differences for whether surfaces were carious or not, along with the appropriate standard errors and 95% confidence intervals by using Stata software version 9.1.The results of those studies are presented both as risk ratios and Becker‐Balagtas odds ratios in Additional Table 1. This is because risk ratio's interpretation is more understandable for clinicians than odds ratio's. The ease with interpretation of the results and the comparability between studies in some comparisons are the reasons why results are presented as risk ratios in this review, if seen to be sensible.
The minority of the 32 studies with dichotomous data were parallel group studies (Amin 2008; Barja‐Fidalgo 2009; Beiruti 2006; Bravo 2005; Chen 2012; Liu 2012) and all of those studies had clustered data (clustering of the children in a school class or several teeth in a child's mouth). Two of those six studies had analysed their effect estimates as risk ratios (Beiruti 2006; Bravo 2005), and one study as odds ratios (Liu 2012), with cluster corrected standard errors. The results of those studies could be used as such in further analysis in this review. For the other three studies, risk ratios or odds ratios were calculated for differences for whether surfaces were carious or not, along with the appropriate standard errors and 95% confidence intervals. The selection of the measure depended on the measure used in the other studies at each follow‐up (to allow comparability between studies). In the study of Barja‐Fidalgo 2009 with raw data available, the risk ratio was calculated by Stata software using glm command, with robust standard errors and correcting for clustering. In the studies of Amin 2008 and Chen 2012 without raw data available, the data could be dichotomised (whether a child had caries or not) because the numbers of decayed occlusal surfaces were small. The original results of Chen 2012 (although considering for clustering of teeth per child) were not reported in useable form for this review when the study calculated cumulative survival percentages of dentine carious lesion free pits and fissures of first permanent molars combined.
It was intended to analyse the mean DFS (the number of decayed and filled tooth surfaces) data as continuous data, the effect estimate being the difference in mean DFS. The mean DFS was calculated for the occlusal surfaces of teeth included in the test and control groups. It was intended to use the standardized mean difference, and 95% confidence intervals to pool the effect estimates from each study, however only one study had data presented in this way.
Unit of analysis issues
In parallel group studies the unit of analysis was an individual. Where more than one measurement was made (i.e. more than one tooth/surface), then the standard errors of the estimates were adjusted to take the multiplicity or clustering into account.
In cluster randomised trials, the unit of analysis was also chosen to be an individual. The standard errors of the effect estimates were corrected taking the clustering into account (for example, clustering of children at school class level).
In split‐mouth studies the unit of analysis was a tooth pair. We anticipated that the majority of studies would be split‐mouth studies, which included one or more pairs of tooth surfaces per child, the interventions being randomly allocated to tooth surfaces within each pair (usually the pairs being surfaces in upper and lower teeth). Strictly these pairs are not independent and should be analysed as 'paired data' on a child basis. However, we decided to analyse the pairs independently as otherwise we would be excluding most of the trials and losing useful information from these studies (we are unaware of any widely used methods to correct and account for dependence of the tooth pairs when e.g. only marginals are reported). This meant that the confidence intervals would be slightly narrower than they should be, and this was taken into consideration when we interpreted the results.
Dealing with missing data
The analyses were performed by using an available case data analysis as represented in the Cochrane Handbook for Systematic Reviews of Interventions 5.1.0 (Higgins 2011b).
In caries prevention studies, follow‐up times can be several years. Studies with a long follow‐up have, however, the problem of high drop‐out rates causing uncertainty in data. The usual drop‐out reason is children moving from the study area. In this update, we decided to include the data of all studies in the analyses (regardless of the drop‐out rate). The studies with a high drop‐out rate (drop‐out rate over 25% regardless of the follow‐up time) were assessed to be at high risk of bias. The effect of the risk of bias grading on the results was evaluated in the sensitivity analyses.
Assessment of heterogeneity
The significance of any discrepancies in the estimates of the treatment effects from the different studies was assessed by means of Cochran's test for heterogeneity and by a measure of I2. The measure I2 describes the percentage of the variability in effect estimates that is due to heterogeneity rather than sampling error. A value greater than 50% may be considered to represent substantial heterogeneity (Higgins 2003).
We planned to investigate clinical heterogeneity between the studies by examining different baseline caries prevalence levels of the populations. However, there was insufficient information from the studies to do this.
Assessment of reporting biases
If there had been sufficient numbers of trials (more than 10) in any meta‐analysis, publication bias would have been assessed according to the recommendations on testing for funnel plot asymmetry as described in the Cochrane Handbook for Systematic Reviews of Interventions 5.1.0 (Sterne 2011). If asymmetry was identified we would have examined possible causes.
Data synthesis
The data consisted of comparisons for sealant versus control without sealant, and sealant material versus sealant material.
The meta‐analyses were conducted in Review Manager (RevMan) 5, using the generic inverse variance method with either the fixed‐effect or the random‐effects model. In meta‐analyses including two or three studies, we used the fixed‐effect model, and in meta‐analyses including four or more studies we used the random‐effects model. We decided to pool the data of the studies in each comparison regardless of the risk of bias classification of the studies. The effect of the risk of bias grading on the results were evaluated in the sensitivity analyses.
When feasible, odds ratios from parallel group studies and split‐mouth studies were pooled in the same meta‐analysis, by using Becker‐Balagtas odds ratios in split‐mouth studies, as outlined in the article by Stedman 2011.
Subgroup analysis and investigation of heterogeneity
It was planned to examine the effectiveness of sealants at different caries prevalence levels. Due to insufficient information from the studies, it was not possible to create subgroups for further analyses.
Sensitivity analysis
To test the robustness of results, sensitivity analyses were undertaken to explore the effect of risk of bias grading of the studies for the caries outcomes.
Results
Description of studies
Results of the search
In this 2013 update, a total of 475 new records were retrieved (when duplicates were removed from searches of the Cochrane Oral Health Group's Trials Register (147), CENTRAL (145), MEDLINE (290), EMBASE (197), via STN Easy searched databases (80), and CRD databases (17)). Three of the 475 records were identified by checking reference lists from already identified trials and review articles.
The total number of records considered from all updates was 3982 including 3507 records from the earlier searches and 475 new records from the latest search. Of the 3982 records, 3599 records were rejected as definitely not meeting the inclusion criteria simply on the basis of title or abstract or because they were duplicates. Altogether 383 full‐text reports were obtained. All non‐English language reports were translated to assess the studies. The review authors could read reports in English, German and in the Scandinavian languages. Outside translators were consulted to identify and assess the reports in Italian, Portuguese, Spanish, French, Hungarian, Russian, Polish, Romanian, Chinese, Japanese and Thai. From these 383 full‐text reports, 259 were clearly irrelevant for this review leaving 124 full‐text reports for final assessment. The main reasons for ineligibility were: trials without control, studies with only retention results, studies with first generation sealant material or unclear materials, studies comparing sealant materials of the same type, the study clearly included other preventive treatments, preventive programmes or patients were older than 20 years.
In total there were 124 full‐text reports and 10 conference abstracts to be considered in detail. Although only studies with a full‐text report were included in this review, the conference abstracts were reviewed to determine the need to establish if a full‐text report was available. Finally 55 reports representing 34 individual studies were considered eligible for inclusion in the review. Compared to the previous version of this review, 18 new studies were included (eight recently published studies (Amin 2008; Barja‐Fidalgo 2009; Baseggio 2010; Chen 2012; Dhar 2012; Liu 2012; Pardi 2005; Tagliaferro 2011), and 10 studies excluded in the previous version of this review (mainly because data were stated only as marginals) (de Luca‐Fraga 2001; Erdoğan 1987; Karlzén‐Reuterving 1995; Raadal 1996; Reisbick 1982; Richardson 1978; Rock 1978; Rock 1996; Sipahier 1995; Williams 1996)). The reasons for exclusion of the 63 studies (including 53 studies with full‐text reports and 10 conference abstracts) with in total 76 reports are explained in the Characteristics of excluded studies table.
Three studies are awaiting assessment (Antonson 2012; Madléna 1993; Markovic 2012).
The electronic search identified one ongoing trial of sealants: NCT00674869.
Included studies
Thirty‐four studies were included in the review; 13 studies provided data for comparison of sealant versus control without sealant (Bojanini 1976; Bravo 2005; Brooks 1979; Charbeneau 1979; Erdoğan 1987; Hunter 1988; Liu 2012; Reisbick 1982; Richardson 1978; Rock 1978; Sheykholeslam 1978; Songpaisan 1995; Tagliaferro 2011) and 22 studies for comparison of sealant material versus sealant material (Amin 2008; Arrow 1995; Barja‐Fidalgo 2009; Baseggio 2010; Beiruti 2006; Chen 2012; de Luca‐Fraga 2001; Dhar 2012; Forss 1998; Ganesh 2006; Güngör 2004; Karlzén‐Reuterving 1995; Kervanto‐Seppälä 2008; Lampa 2004; Mills 1993; Pardi 2005; Poulsen 2001; Raadal 1996; Rock 1996; Sipahier 1995; Songpaisan 1995; Williams 1996). The study of Songpaisan 1995 was included in three comparisons (resin‐based sealant versus control without sealant, glass ionomer sealant versus control without sealant, and glass ionomer sealant versus resin‐based sealant).
One of the 13 studies comparing sealant to control without sealant evaluated actually whether there is additional benefit by using sealants among children receiving regular oral health education (Tagliaferro 2011). This evaluation was carried out separately in populations with high and low risk of caries.
The sealant comparisons were: glass ionomer sealant versus resin‐based sealant (n = 15) (Arrow 1995; Barja‐Fidalgo 2009; Beiruti 2006; Chen 2012; Dhar 2012; Forss 1998; Ganesh 2006; Karlzén‐Reuterving 1995; Kervanto‐Seppälä 2008; Mills 1993; Poulsen 2001; Rock 1996; Sipahier 1995; Songpaisan 1995; Williams 1996); resin‐modified glass ionomer sealant versus resin sealant (n = 3) (Amin 2008; Baseggio 2010; Raadal 1996); polyacid‐modified composite versus resin‐based sealant (n = 2) (Güngör 2004; Lampa 2004); and resin‐modified glass ionomer sealant versus polyacid‐modified composite (1) (de Luca‐Fraga 2001). The study of Pardi 2005 had three sealant arms (resin‐modified glass ionomer, resin sealant, and compomer). The data in the study of Pardi 2005 were, however, not reported in suitable form for this review (there was no clear description how many teeth there were with dentine caries or with filling in each group), and the data were not included in the comparisons of this review. The results as stated in the original article are, however, reported in this review.
Nine out of all 34 included studies were designed as a parallel group design (Amin 2008; Barja‐Fidalgo 2009; Beiruti 2006; Bravo 2005; Chen 2012; Liu 2012; Pardi 2005; Songpaisan 1995; Tagliaferro 2011) and the 25 other studies were designed as split‐mouth studies, where the two interventions (fissure sealant versus control/no treatment or sealant material versus sealant material) were randomly or quasi‐randomly allocated to teeth within a tooth pair.
To clarify the description of studies, the study of Songpaisan 1995 with three comparisons (resin‐based sealant versus control without sealant, glass ionomer sealant versus control without sealant, and glass ionomer sealant versus resin‐based sealant) was included in the comparison of sealant versus no treatment. Thus the total number of studies comparing sealant to no treatment is 13 and the total number of the studies comparing sealant to sealant is 21.
In the description of the risk of bias assessment of 'Incomplete outcome data', the study of Songpaisan 1995 was, however, considered in all the following comparisons: resin‐based sealant versus control without sealant, glass ionomer sealant versus control without sealant, and glass ionomer sealant versus resin‐based sealant.
Description of the studies comparing sealant versus no treatment
Of the 13 studies providing data for comparison of sealant versus control without sealant, four studies were conducted in the USA (Brooks 1979; Charbeneau 1979; Reisbick 1982; Sheykholeslam 1978), one in Brazil (Tagliaferro 2011), one in Canada (Richardson 1978), one in China (Liu 2012), one in Colombia (Bojanini 1976), one in New Zealand (Hunter 1988), one in Spain (Bravo 2005), one in Thailand (Songpaisan 1995), one in Turkey (Erdoğan 1987), and one in UK (Rock 1978). In most studies the children were recruited from selected schools or dental clinics.
In the studies comparing sealant with no treatment, sealants were mainly applied on sound occlusal surfaces of permanent first molars in children aged 5 to 10 years. The resin‐based sealant material was autopolymerised resin sealant (bis‐GMA) in 10 studies, visible‐light‐polymerised resin sealant in one study (Bravo 2005), and light‐polymerised resin sealant with fluoride in one study (Liu 2012). The study of Songpaisan 1995 used autopolymerised glass ionomer sealants, and the study of Tagliaferro 2011 resin‐modified glass ionomer cement. None of the studies reported sealant application on approximal surfaces of permanent premolar or molar teeth.
Reapplication of sealants was reported in two studies (Bravo 2005; Songpaisan 1995). In the study of Songpaisan 1995 reapplication was done for those children whose sealants were partially or all missing at the 6‐month examination. In the study of Bravo 2005 sealants were reapplied if there had been partial or total loss since the previous examination after 6, 12, 18, 24 and 36 months.
The baseline caries prevalence of the study population was stated in two studies from the 1990s (Bravo 2005; Songpaisan 1995) and in one study from the 2000s (Liu 2012). In the study of Songpaisan 1995 the mean baseline DMFT of age group 12 to 13 was reported to be 1.81 ± 1.84; in the study of Bravo 2005 the mean dft was 2.98 in the control group and 2.24 in the sealant group in the 6 to 8 years age group; and in the study of Liu 2012 the mean baseline dmft level of children aged 8 to 10 was 3.4. A further three studies comparing sealant with no treatment from the 1970s documented that caries‐free children were not included in the studies (Bojanini 1976; Brooks 1979; Sheykholeslam 1978).
Tap water was fluoridated in the areas in which three of the studies took place (Bojanini 1976; Brooks 1979; Sheykholeslam 1978). In one study (Hunter 1988) half the children used fluoridated water and half did not.
Three studies were at least partly supported by a sealant manufacturer (Brooks 1979; Rock 1978; Sheykholeslam 1978), and in the study of Bojanini 1976 two of the authors had affiliation to a sealant manufacturer. The studies of Bravo 2005; Liu 2012; Songpaisan 1995 and Tagliaferro 2011 were supported by governmental or academic sources or independent research foundations (in the study of Songpaisan 1995 one sealant material was donated by a sealant manufacturer). The other five studies did not report information on funding.
Description of the studies comparing sealant versus sealant
Of the 21 studies comparing sealant to sealant, four studies were conducted in Brazil (Barja‐Fidalgo 2009; Baseggio 2010; de Luca‐Fraga 2001; Pardi 2005), three in UK (Mills 1993; Rock 1996; Williams 1996), two in Finland (Forss 1998; Kervanto‐Seppälä 2008), two in India (Dhar 2012; Ganesh 2006), two in Sweden (Karlzén‐Reuterving 1995; Lampa 2004), two in the Syrian Arab Republic (Beiruti 2006; Poulsen 2001), two in Turkey (Güngör 2004; Sipahier 1995), one in Australia (Arrow 1995), one in China (Chen 2012), one in Egypt (Amin 2008), and one in Norway (Raadal 1996). Children were mainly recruited from selected schools or dental clinics.
In the studies comparing sealant material to another sealant material, the sealants were applied on sound occlusal surfaces of permanent first or second molars in children aged 5 to 16 years. The sealant materials were mainly autopolymerised or visible‐light‐polymerised resin‐based sealants and autopolymerised glass ionomers. In addition to sound surfaces, five studies comparing different sealant materials included occlusal surfaces with enamel or dentine lesions (Barja‐Fidalgo 2009; Beiruti 2006; Chen 2012; Güngör 2004; Poulsen 2001). In the study of Beiruti 2006 less than 10% of surfaces had a small dentine lesion, in the study of Güngör 2004 all surfaces had enamel lesions, and in the other three studies some surfaces had enamel lesions and the other surfaces were sound (Barja‐Fidalgo 2009; Chen 2012; Poulsen 2001). Further, two studies documented that sealants were applied on tooth surfaces at caries risk (Kervanto‐Seppälä 2008; Lampa 2004), and two studies required deep fissures of the surfaces (Amin 2008; Baseggio 2010).
Reapplication of sealants was reported in four studies (Arrow 1995; Forss 1998; Kervanto‐Seppälä 2008; Williams 1996). In the study of Arrow 1995, three out of 465 teeth (0.6%) were resealed once with glass ionomer and four out of 465 teeth (0.9%) with Delton during the trial. In the study of Forss 1998, 22% of glass ionomer sealants were reapplied during the first 2 years. In the study of Kervanto‐Seppälä 2008, a total of 15% of the initially resin sealed teeth were resealed after the sealant was found to be defective. In the study of Williams 1996, 7% of sealants were reapplied at 4 years of follow‐up (27 teeth with glass ionomer and six teeth with resin).
Of the 21 studies comparing sealant to sealant, five studies reported the baseline caries prevalence of the study population (Arrow 1995; Chen 2012; Dhar 2012; Kervanto‐Seppälä 2008; Poulsen 2001). In the study of Arrow 1995 the initial dmf (± standard deviation (SD)) of children (mean age 7 years) was reported as 1.64 ± 2.45, and in the study of Chen 2012 with children aged 7 to 9 the initial dmft with SD was 5.0 (2.5). In the study of Dhar 2012 with children aged 6 to10, the caries prevalence was reported to be 63% and DMFT of 2.60. In the study of Kervanto‐Seppälä 2008 the baseline DMFT was 0.57 in the age group of 13 years. The study of Poulsen 2001 did not give baseline caries information for the children included in the study but the article referred to general information of caries levels in Syria. The average DMFT value was stated as 0.6 to 0.7 in 6 to 7 year old children in Damascus based on data collected by the WHO Regional Demonstration, Training and Research Center for Oral Health. Further, two studies documented that caries‐free children were not included in the studies (Barja‐Fidalgo 2009; Rock 1996). Three studies assumed the caries risk of the study populations: in one study the caries risk of the children was assumed to be low (Forss 1998), in one study low or moderate (Beiruti 2006) and in one study from low to high (Ganesh 2006).
Three studies were conducted among children resident in a fluoridated area (Arrow 1995; Barja‐Fidalgo 2009; Rock 1996).
Excluded studies
The Characteristics of excluded studies table presents the reasons for exclusion of controlled clinical studies. Only those controlled clinical studies which compared sealant with a control without sealant or sealant versus sealant for prevention of caries were included in the table. Studies without control were excluded.
The reasons for exclusion were varied and in many studies there were several reasons for exclusion. In 21 out of the 63 excluded studies the only reason for exclusion was no mention of random or quasi‐random allocation; a further 15 studies were clearly not randomised or quasi‐randomised. Other reasons for exclusion were mainly that the study design was not eligible for this review or the study included other preventive treatments.
Risk of bias in included studies
We contacted the authors of the included studies to obtain additional information to assess the methodological quality issues if the information in the report was insufficient to make final decisions. We requested additional information from 20 studies (Amin 2008; Barja‐Fidalgo 2009; Beiruti 2006; Bravo 2005; Chen 2012; de Luca‐Fraga 2001; Dhar 2012; Forss 1998; Ganesh 2006; Güngör 2004; Karlzén‐Reuterving 1995; Kervanto‐Seppälä 2008; Lampa 2004; Liu 2012; Pardi 2005; Poulsen 2001; Raadal 1996; Sipahier 1995; Songpaisan 1995; Tagliaferro 2011). Additional information for six of those studies was not available for this update (Amin 2008; de Luca‐Fraga 2001; Karlzén‐Reuterving 1995; Lampa 2004; Raadal 1996; Songpaisan 1995).
Allocation
Studies comparing sealant versus no treatment
Random sequence generation was adequate indicating low risk of bias in 11 out of 13 (85%) studies providing data at this comparison (Bojanini 1976; Bravo 2005; Brooks 1979; Charbeneau 1979; Hunter 1988; Liu 2012; Reisbick 1982; Richardson 1978; Rock 1978; Sheykholeslam 1978; Tagliaferro 2011).The random sequence generation was mainly made by using a previously established randomisation table or list of random numbers, or by a dice or tossing coin. In one split‐mouth study, the allocating of a tooth to an intervention was not random but quasi‐random (Hunter 1988).
Allocation concealment was graded 'Low risk' of bias in the same 11 studies as those assessed to have adequate random sequence generation. Eight of those 11 studies were split‐mouth studies. None of these split‐mouth studies reported typical random allocation methods (e.g. central allocation). However, the description of the whole randomisation procedure in five split‐mouth studies gave an impression that realisation of the random sequence generation was real. For example, the study of Brooks 1979 reported that each child received the record form, and had a piece of tape placed on his/her cheek to indicate the previously assigned treatment side (random sequence generation made by a randomised assignment sheet). Two split‐mouth studies reported the information of allocation concealment incompletely and one split‐mouth study was quasi‐randomised but these studies were graded as having low risk of bias in this domain. This is because we saw that in split‐mouth studies the risk of selection bias is in any case insignificant (because we assumed that there were no right‐left asymmetry between contralateral teeth regarding caries risk, as shown by Larmas 1995 when they evaluated timing of the change from a sound erupting tooth to a filled tooth).
Two studies did not give any information on random sequence generation or allocation concealment methods (Erdoğan 1987; Songpaisan 1995) and the judgement was 'Unclear'.
Studies comparing sealant versus sealant
Random sequence generation was assessed to be adequate indicating low risk of bias in 13 out of 21 (62%) studies comparing different sealant materials (Arrow 1995; Barja‐Fidalgo 2009; Baseggio 2010; Chen 2012; Dhar 2012; Forss 1998; Ganesh 2006; Güngör 2004; Mills 1993; Pardi 2005; Poulsen 2001; Rock 1996; Williams 1996). In two of the split‐mouth studies, allocation of a tooth to an intervention was not random but quasi‐random (Arrow 1995; Baseggio 2010). The other eight of the 21 studies did not give any information on sequence generation and the judgement was 'Unclear'.
Allocation concealment was graded 'Low risk' of bias in 12 out of 21 (57%) studies (Arrow 1995; Barja‐Fidalgo 2009; Baseggio 2010; Chen 2012; Dhar 2012; Forss 1998; Ganesh 2006; Güngör 2004; Mills 1993; Poulsen 2001; Rock 1996; Williams 1996). Ten of those 12 studies were split‐mouth studies.
Nine of the 21 studies did not give any information on random allocation concealment methods and the judgement was 'Unclear'.
Blinding
Studies comparing sealant versus no treatment
Blinding of outcome assessors was documented and assessed as adequate in nine out of the 13 (69%) studies comparing sealant to control without sealant (Bravo 2005; Brooks 1979; Hunter 1988; Liu 2012; Reisbick 1982; Richardson 1978; Rock 1978; Sheykholeslam 1978; Tagliaferro 2011). In most of those studies, new evaluation forms were used for recording the presence or absence of the sealant and any caries, or the records were not checked prior to examination. The other four studies did not report about the blinding and the judgement was 'Unclear'.
Studies comparing sealant versus sealant
Blinding of outcome assessors was documented and assessed as adequate in seven out of the 21 studies (33%) comparing different sealant materials (Barja‐Fidalgo 2009; Chen 2012; Dhar 2012; Ganesh 2006; Güngör 2004; Raadal 1996; Sipahier 1995). The other 14 studies did not report about the blinding and the judgement was 'Unclear'.
Incomplete outcome data
Studies comparing resin sealant versus no treatment
At 12 months of follow‐up, five out of six studies comparing resin sealant to control without sealant were assessed to have low risk of bias at this domain (Bojanini 1976; Charbeneau 1979; Richardson 1978; Rock 1978; Sheykholeslam 1978), and one study to have high risk of bias (Erdoğan 1987).
At 24 months of follow‐up, all seven studies were assessed to have low risk of bias in this domain (Bojanini 1976; Brooks 1979; Charbeneau 1979; Liu 2012; Richardson 1978; Sheykholeslam 1978; Songpaisan 1995).
At 36 months of follow‐up, five out of seven studies were assessed to have low risk of bias (Bojanini 1976; Charbeneau 1979; Hunter 1988; Richardson 1978; Sheykholeslam 1978), and two studies high risk of bias (Brooks 1979; Rock 1978).
At 48‐54 months of follow‐up, two out of five studies were assessed to have low risk of bias (Charbeneau 1979; Richardson 1978), and two studies high risk of bias (Brooks 1979; Erdoğan 1987). In one study there was no information on drop‐outs by group (Bravo 2005) and the judgement was 'Unclear'.
At 5 years, the only study was assessed to be at low risk of bias (Richardson 1978).
The only studies at 6 and 7 years (Brooks 1979) and at 9 years (Bravo 2005) were assessed to be at high risk of bias in this domain.
The study of Reisbick 1982 was assessed to be at high risk of bias in this domain at all the reported follow‐ups (14, 20 and 32 months).
Studies comparing glass ionomer or resin‐modified glass ionomer sealant versus no treatment
At 24 months of follow‐up, the studies of Songpaisan 1995 and Tagliaferro 2011 were assessed to have low risk of bias in this domain.
Studies comparing sealant versus sealant
Glass ionomer versus resin sealant
At 12 months of follow‐up, all four studies were assessed to have low risk of bias in this domain (Dhar 2012; Karlzén‐Reuterving 1995; Rock 1996; Sipahier 1995).
At 24 months of follow‐up, seven out of 10 studies were assessed to have low risk of bias (Chen 2012; Dhar 2012; Forss 1998; Ganesh 2006; Karlzén‐Reuterving 1995; Rock 1996; Songpaisan 1995), and three studies to have high risk of bias (Mills 1993; Poulsen 2001; Williams 1996).
At 36‐48 months of follow‐up, four out of seven studies were assessed to be at low risk of bias in this domain (Arrow 1995; Beiruti 2006; Karlzén‐Reuterving 1995; Rock 1996); and three studies at high risk of bias (Kervanto‐Seppälä 2008; Poulsen 2001; Williams 1996).
At 5 years, both of the two studies at this comparison were assessed to have high risk of bias (Barja‐Fidalgo 2009; Beiruti 2006). At 7 years, the only study at this comparison was also assessed to have high risk of bias (Forss 1998).
Resin‐modified glass ionomer versus resin
All three studies at this comparison were assessed to have low risk of bias in this domain at all follow‐ups (Amin 2008 at 12 and 24 months; Baseggio 2010 at 12, 24, and 36 months; and Raadal 1996 at 36 months).
Polyacid‐modified resin composite versus resin sealant
One of the two studies at this comparison was assessed to have low risk of bias (Lampa 2004), and the other study to have high risk of bias (Güngör 2004) in this domain.
Other comparisons
The studies of de Luca‐Fraga 2001 and Pardi 2005 were assessed to have low risk of bias in this domain.
Selective reporting
Studies comparing sealant versus no treatment
All 13 studies at this comparison reported all pre‐specified outcomes adequately.
Studies comparing sealant versus sealant
All 21 studies at this comparison reported all pre‐specified outcomes adequately.
Other potential sources of bias
Studies comparing sealant versus no treatment
Comparability of the groups
Demographic characteristics (such as sex, age, and social class), baseline caries risk level, and baseline condition of the tooth surfaces to be treated were described and assessed to be balanced across the groups in all 13 studies.
Co‐interventions
In 10 out of the 13 studies (77%) this domain was graded as having low risk of bias. If co‐interventions were used, they were fluoridated tap water or toothpaste which were allowed in the protocol of this review. In three studies the judgement was 'Unclear' because no information was provided.
Studies comparing sealant versus sealant
Comparability of the groups
Demographic characteristics, baseline caries risk level, and baseline condition of the sealed tooth surfaces were described and assessed to be balanced across the groups in 19 out of 21 (90%) studies comparing different sealant materials. In the study of Barja‐Fidalgo 2009 the groups at the analysis point (5 years) were assessed to be imbalanced. In the study of Kervanto‐Seppälä 2008 the information was insufficient to assess this domain and the judgement was 'Unclear'.
Co‐interventions
In 11 out of the 21 studies (52%) this domain was graded as having low risk of bias. In 10 studies the judgement was 'Unclear' because no information was provided.
Effects of interventions
See: Summary of findings for the main comparison Resin‐based sealants compared to no treatment for preventing dental caries; Summary of findings 2 Glass ionomer sealants compared to no treatment for preventing dental caries; Summary of findings 3 Glass ionomer sealants versus resin sealants; Summary of findings 4 Resin‐modified glass ionomer sealants versus resin sealants; Summary of findings 5 Polyacid‐modified resin composite versus resin sealants
All studies reported data and results on sealant application on occlusal surfaces of permanent molars only, and none on approximal surfaces.
Sealant material versus control without sealant
Resin fissure sealant versus no treatment (Comparison 1)
Resin fissure sealant versus no treatment at 12, 24, 36, and 48‐54 months
Twelve (12) studies provided data for comparison of resin sealants to control without a sealant (nine split‐mouth studies and three parallel group studies). Nine of the 12 studies could be pooled in the meta‐analyses (one parallel group study and eight of the nine split‐mouth studies reporting summary data as paired form or as marginals). The number of studies in each meta‐analysis was: six studies at 12 months, six studies at 24 months, seven studies at 36 months, and four studies at 48‐54 months.
The results of these nine studies comparing resin sealant with a control were all highly significant (P < 0.00001), with pooled odds ratio (OR) values of 0.16 (95% confidence interval (CI) 0.08 to 0.30), 0.12 (95% CI 0.07 to 0.19), 0.17 (95% CI 0.11 to 0.27), and 0.21 (95% CI 0.16 to 0.28) at 12, 24, 36 and 48‐54 months follow‐up, respectively (Additional Table 1; Analysis 1.1; Analysis 1.2; Analysis 1.3; Analysis 1.4). In all analyses, the odds ratios of the split‐mouth studies were the Becker‐Balagtas odds ratios.
There was significant heterogeneity for these comparisons (Comparison 1, Outcomes 1.1 to 1.4). However, as all the results from each individual trial showed significant benefit for the sealant we felt it was appropriate to pool the results in a meta‐analysis and decided to use random‐effects models to do this.
The main finding at each of these follow‐ups (12, 24, 36, and 48‐54 months) is the result based on all studies which provided data at follow‐up (and these are the results presented also in summary of findings Table for the main comparison). This is because in the sensitivity analyses, the interpretation of the results did not alter.
In all comparisons, the results of the studies with data reported in paired form were slightly more favouring sealants than the studies with data presented only as marginals, with pooled OR values of 0.09 (95% CI 0.06 to 0.13), 0.11 (95% CI 0.06 to 0.22), 0.16 (95% CI 0.12 to 0.20), and 0.17 (95% CI 0.13 to 0.23) at 12, 24, 36 and 48‐54 months follow‐up, respectively (P < 0.0001). This is because the conservative intra‐cluster correlation coefficient (ICC) 0.05 was used in the calculations of studies with data presented only as marginals.
The effect of the risk of bias grading on the results was evaluated in the sensitivity analyses. When excluding studies with high risk of bias from each analysis, the results did not alter significantly and they highly favoured sealants with pooled OR values of 0.12 (95% CI 0.07 to 0.21), 0.12 (95% CI 0.07 to 0.19), 0.13 (95% CI 0.09 to 0.19), and 0.19 (95% CI 0.13 to 0.26) at 12, 24, 36 and 48‐54 months follow‐up, respectively (data not shown). The number of studies remaining for analyses (when high risk of bias studies were excluded) was: five out of six studies at 12 months; six out of six at 24 months; five out of seven at 36 months; and two out of four at 48‐54 months.
Two parallel group studies confirmed the results of the meta‐analyses, at 24 and 48 months. The 24‐month study by Songpaisan 1995 at unclear risk of bias supplied data comparing second generation resin sealant with a control in children aged 12 to 13 and found significantly (P < 0.00001) more caries in the control group children, with a difference of mean number of decayed, filled permanent surfaces (DFS) = ‐0.65 (95% CI ‐0.83 to ‐0.47) (Additional Table 2; Analysis 1.6). The other study by Bravo 2005 at unclear risk of bias found significantly (P < 0.0001) more caries in the control group children, with a risk ratio value (RR) of 0.24 (cluster corrected 95% CI 0.12 to 0.45) at 4 years of follow‐up (Additional Table 1; Analysis 1.5).
The ninth split‐mouth study by Reisbick 1982 at high risk of bias stated also benefit of sealants compared to control without sealants. The study reported effectiveness to be 90%, 80%, and 70%, at 14 months, 20 months, and 32 months of follow‐up, respectively.
Resin fissure sealant versus no treatment at 5 years
The only study at 5 years of follow‐up by Richardson 1978 at low risk of bias found significantly more caries in the control teeth with a Becker‐Balagtas odds ratio (BB OR) value of 0.31 (95% CI 0.23 to 0.43; P < 0.00001) (Analysis 1.7).
Resin fissure sealant versus no treatment at 6 and 7 years
One split‐mouth study at high risk of bias (because of high drop‐out rate at 6 and 7 years of follow‐up) provided data for these comparisons (Brooks 1979). The study found significantly more caries in the control teeth, with a RR value of 0.45 (95% CI 0.36 to 0.58) and 0.45 (95% CI 0.34 to 0.59) at 6 and 7 years of follow‐up, respectively (Analysis 1.8; Analysis 1.9). The reductions in caries therefore were 55% at 6 and 7 years.
Resin fissure sealant versus no treatment at 9 years
One cluster randomised study with high risk of bias (because of high drop‐out rate at this follow‐up) provided data for this comparison (Bravo 2005). The study found significantly more caries in the control group children, with a RR value of 0.35 (cluster corrected 95% CI 0.22 to 0.55; P < 0.0001) (Analysis 1.10). After 9 years 27% of sealed surfaces were decayed compared to 77% of surfaces without sealant.
Glass ionomer sealant versus no treatment (Comparison 2)
Glass ionomer sealant versus no treatment at 24 months
One study with unclear risk of bias provided data for this comparison (Songpaisan 1995). This parallel group study compared the 24‐month DFS increments for two glass ionomer sealant groups with one control group receiving no treatment for age group 12 to 13 years. We have combined the data from the two glass ionomer groups. The difference failed to reach significance with mean difference in DFS ‐0.18 (95% CI ‐0.39 to 0.03; P = 0.09) (Additional Table 2; Analysis 2.1).
Resin‐modified glass ionomer cement plus oral health education versus oral health education alone at 24 months
One study at low risk of bias (Tagliaferro 2011) provided results for comparison resin‐modified glass ionomer cement plus oral health education every 3 months versus oral health education every 3 months alone. The comparison was performed separately for high risk children and for low risk children. The groups to be compared were: HRS (high risk children with sealant application plus oral health education) versus HRC (high risk children with oral health education alone); and LRS (low risk children with sealant application plus oral health education) versus LRC (low risk children with oral health education alone).
The study reported their results to be: after 24 months, only the HRS group showed statistically lower DMF (decayed, missed and filled) increments on occlusal surfaces of first permanent molars compared with the HRC group. For low risk groups, no statistical difference was observed among the treatments. The study authors concluded "that in a 2‐year period, oral health education was sufficient to control occlusal caries in low risk children while for high risk children, sealant application in addition to oral health education was considered the best strategy". The retention rate was reported to be 84% after 24 months (16% of sealed teeth showed total sealant loss).
Sealant material versus sealant material
Glass ionomer versus resin sealant (Comparison 3)
Fifteen studies provided data for comparison of chemically cured glass ionomer sealant to resin‐based sealant at 24, 36‐48, 60 and 84 months of follow‐ups. Four of those 15 studies found better caries reductions for resin‐based sealants than for glass ionomers (Kervanto‐Seppälä 2008; Poulsen 2001; Rock 1996; Songpaisan 1995), two studies for glass ionomers (Arrow 1995; Beiruti 2006) than for resin‐based sealants, and nine studies (Barja‐Fidalgo 2009; Chen 2012; Dhar 2012; Forss 1998; Ganesh 2006; Karlzén‐Reuterving 1995; Mills 1993; Sipahier 1995; Williams 1996) did not find a difference between these materials. The study of Williams 1996 found resin‐based sealants better than glass ionomers at 24 months but not at 48 months.
As the results of these studies with different follow‐up times were divergent, no meta‐analyses were attempted with one exception. At 5 years of follow‐up, the data of the two studies included in this comparison were seen sensible to be pooled.
Glass ionomer versus resin sealant at 12 months
Four split‐mouth studies with data stated only as marginals did not find a difference between the resin‐based and glass ionomer sealants at this follow‐up (Dhar 2012; Karlzén‐Reuterving 1995; Rock 1996; Sipahier 1995) (Additional Table 1; Analysis 3.1). Two of the studies were graded as low risk of bias (Dhar 2012; Rock 1996), and the other two studies as unclear risk of bias.
The study by Dhar 2012 reported results also for teeth where occlusal surfaces were prepared before sealant application. No teeth developed caries during 12 months of follow‐up.
Glass ionomer versus resin sealant at 24 months
There were eight split‐mouth studies at this comparison (Dhar 2012; Forss 1998; Ganesh 2006; Karlzén‐Reuterving 1995; Mills 1993; Poulsen 2001; Rock 1996; Williams 1996), and two parallel group studies (Chen 2012; Songpaisan 1995).
Two of the eight split‐mouth studies found resin‐based sealants superior compared to glass ionomers: Rock 1996 with a BB OR of 8.96 (95% CI 2.07 to 38.82), and Williams 1996 with a BB OR of 3.69 (95% CI 1.50 to 9.09). One study found resin sealants slightly better than glass ionomer (Poulsen 2001 with a BB OR of 3.46 (95% CI 1.03 to 11.63)).
Three split‐mouth studies did not find a difference between the materials (Dhar 2012; Forss 1998; Karlzén‐Reuterving 1995); and in further two studies (Ganesh 2006; Mills 1993) no teeth developed caries during 24 months of follow‐up (Analysis 3.2).
One of the two parallel group studies found a significant benefit in favour of second generation resin sealant at 24‐month follow‐up, with DFS mean difference 0.47 (95% CI 0.31 to 0.63; P < 0.00001) compared to glass ionomer cement (Songpaisan 1995) (Analysis 3.3). The other parallel group study by Chen 2012 did not find difference between the materials with an OR value of 1.67 (95% CI 0.44 to 6.30) (Analysis 3.2).
Five studies at this comparison were assessed to be at low risk of bias (Chen 2012; Dhar 2012; Forss 1998; Ganesh 2006; Rock 1996); two studies at unclear risk of bias (Karlzén‐Reuterving 1995; Songpaisan 1995); and three studies at high risk of bias (Mills 1993; Poulsen 2001; Williams 1996).
The study by Dhar 2012 did not find a significant difference between the materials in teeth with preparation of occlusal surface before sealant application with a BB OR of 0.22 (95% CI 0.02 to 2.02) (Additional Table 1).
Glass ionomer versus resin sealant at 36‐48 months
There were six split‐mouth studies at this comparison (Arrow 1995; Karlzén‐Reuterving 1995; Kervanto‐Seppälä 2008; Poulsen 2001; Rock 1996; Williams 1996), and one parallel group study (Beiruti 2006).
In all, the number of decayed sealed teeth in these studies was rather small. The proportion of sound surfaces ranged from 86% to 97%.
Three studies found resin‐based sealants superior compared to glass ionomers (Kervanto‐Seppälä 2008; Poulsen 2001; Rock 1996), and two studies found glass ionomers better than resin‐based sealants (Arrow 1995; Beiruti 2006) at 36‐48 months of follow‐up (Additional Table 1).
At 36 months of follow‐up, the study of Poulsen 2001 found a benefit for second generation resin sealant with a BB OR of 4.03 (95% CI 2.23 to 7.29), the study of Kervanto‐Seppälä 2008 for third generation sealant with a BB OR of 3.98 (95% CI 1.80 to 8.80), and the study of Rock 1996 for fourth generation sealant with a BB OR of 7.13 (95% CI 2.45 to 20.76) compared to chemical cured glass ionomers (Analysis 3.4).
The split‐mouth study of Arrow 1995 found a difference in favour of the glass ionomer sealant compared to second generation resin sealant at 44 months (BB OR 0.18 (95% CI 0.08 to 0.41)) (Analysis 3.4).The parallel group study of Beiruti 2006 reported significantly more caries on resin sealed teeth (light‐polymerised) than on high‐viscosity glass ionomer sealed teeth with a RR of 0.22 (cluster corrected 95% CI 0.06 to 0.82) and 0.32 (cluster corrected 95% CI 0.14 to 0.73) over 36 and 48 months, respectively (Additional Table 1).
Two studies did not find a difference between the materials at 36‐48 months (Karlzén‐Reuterving 1995; Williams 1996) (Analysis 3.4).
Two studies at this comparison were assessed to be at low risk of bias (Arrow 1995; Rock 1996); two studies at unclear risk of bias (Beiruti 2006; Karlzén‐Reuterving 1995); and three studies at high risk of bias (Kervanto‐Seppälä 2008; Poulsen 2001; Williams 1996).
Glass ionomer versus resin sealant over 5 years
Two parallel group studies provided data for this comparison over 5 years (Barja‐Fidalgo 2009; Beiruti 2006). The study of Beiruti 2006 found a significant difference for glass ionomers compared to resins with a RR of 0.28 (cluster corrected 95% CI 0.13 to 0.61). The small study of Barja‐Fidalgo 2009 did not find a difference between the materials with a RR value of 0.38 (cluster corrected 95% CI 0.09 to 1.60). The fixed‐effect meta‐analysis RR is 0.30 (95% CI 0.15 to 0.59; P = 0.0005) favouring glass ionomers, which was significant (Analysis 3.5). In the study of Beiruti 2006, sealant retention was reported to be poor for both materials (sealants were lost almost in 90% of cases at 5 years (Additional Table 3).
Both of these studies were assessed to be at high risk of bias (the study of Beiruti 2006 because of high drop‐out rates after this long follow‐up time; and the study of Barja‐Fidalgo 2009 because of high drop‐out rates and of imbalance between the intervention groups).
Glass ionomer versus resin sealant at 7 years
One split‐mouth study compared glass ionomers with resins at 7 years of follow‐up (Forss 1998). The study of Forss 1998 did not find statistically significant difference between the materials with a RR of 1.44 (95% CI 0.88 to 2.35) (Analysis 3.6; Additional Table 1). At the 7‐year follow‐up, 23.5% of the occlusal surfaces sealed with glass ionomer and 16.5% of those sealed with resins were carious or filled. The study was assessed to be at high risk of bias because of the high drop‐out rate.
Resin‐modified glass ionomer versus resin sealant (Comparison 4)
Resin‐modified glass ionomer versus resin sealant at 12 months
Two studies provided data for this comparison at 12 months of follow‐up (Amin 2008; Baseggio 2010). Neither of these studies found any difference between resin‐modified glass ionomer sealants and resin sealants (the study by Baseggio 2010 with a BB OR value of 1 (95% CI 0.02 to 47.8; P = 1.00) (Analysis 4.1); and the parallel group study of Amin 2008 with OR 1.08 (95% CI 0.09 to 13.15; P = 0.95) (Analysis 4.2). The study of Baseggio 2010 was assessed to be at low risk of bias, and the study of Amin 2008 at unclear risk of bias.
Resin‐modified glass ionomer versus resin sealant at 24 months
Two studies provided data for this comparison at 24 months of follow‐up (Amin 2008; Baseggio 2010). The study by Baseggio 2010 at low risk of bias found benefit for resins compared to resin‐modified glass ionomers with a BB OR of 3.03 (95% CI 1.82 to 5.05; P < 0.0001) (Analysis 4.3). The study of Amin 2008 at unclear risk of bias did not find any difference with OR 1.14 (95% CI 0.09 to 13.89; P = 0.92) (Analysis 4.4).
Resin‐modified glass ionomer versus resin sealant at 36 months
Two studies compared resin‐modified glass ionomer to resin sealant at 36 months (Baseggio 2010; Raadal 1996).The study of Baseggio 2010 found a significant benefit in favour of fluoride‐releasing resin‐based sealant with a BB OR of 2.56 (95% CI 1.84 to 3.56), and the study of Raadal 1996 in favour of second generation resin sealant with a BB OR of 11.38 (95% CI 1.47 to 88.42) compared to resin‐modified glass ionomer. The fixed‐effect meta‐analysis OR is 2.66 (95% CI 1.92 to 3.68; P < 0.00001) which was significant (Analysis 4.5).
In all, in these two studies the number of sound sealed teeth was rather large; 86% of the teeth were sound after 36 months.
The study of Baseggio 2010 was assessed to be at low risk of bias, and the study of Raadal 1996 at unclear risk of bias.
Polyacid‐modified resin composite versus resin sealant (Comparison 5)
Polyacid‐modified resin composite versus resin sealant at 24 months
Two studies compared polyacid‐modified resin composite to resin sealant at 24 months (Güngör 2004; Lampa 2004). These studies did not find a difference between the materials; the study of Güngör 2004 at high risk of bias with a BB OR of 0.80 (95% CI 0.33 to 1.97) and the study of Lampa 2004 at unclear risk of bias with a BB OR of 0.23 (95% CI 0.03 to 1.76). The fixed‐effect meta‐analysis OR is 0.65 (95% CI 0.29 to 1.48; P = 0.31) which was not significant (Analysis 5.1).
In all, in these two studies the number of sound sealed tooth pairs was rather large; 80% of the tooth pairs were sound after 24 months.
Other comparisons
The results of the study of de Luca‐Fraga 2001
The study by de Luca‐Fraga 2001 at unclear risk of bias compared resin‐modified glass ionomer (Vitremer) with polyacid‐modified composite resin sealant (Dyract) on the occlusal surfaces of caries‐free mandibular first permanent molars (split‐mouth design).
Because the chemical compounds of these two materials are close to each other and the materials are not compared to resin, the results given in the article are as such reported: two amalgam restorations were observed in the Dyract sealed teeth at 1 year follow‐up. Sealants were totally retained on 86% of the tooth surfaces sealed with Vitremer, and on 96% of teeth sealed with Dyract.
The results of the study of Pardi 2005
The study of Pardi 2005 at unclear risk of bias compared the following sealant materials: resin‐modified glass ionomer (Vitremer), flowable resin composite (Revolution), and compomer (Dyract Flow). Each child received only one of those three materials (a child had on average 3.2 sealed teeth). All tooth surfaces were conditioned with 37% phosphoric acid regardless of the sealant material used.
Data of this study were not used in the analyses in this review because the data reported were not in suitable form for this review (there was no clear description how many teeth there were with dentine caries or with filling in each group). The results as reported in the original article were: after 2 years, 3.1% of the teeth sealed with Vitremer, 4.3% of the teeth sealed with Revolution, and 6.7% of the teeth sealed with Dyract Flow, were carious or filled. Caries was defined as active white spot lesion (translucent enamel alteration) or presence of a microcavity (diameter under 1.5 mm across fissure) or large cavity or filling. After 2 years, sealants were totally retained on 47% of the tooth surfaces sealed with Vitremer, on 76% of the teeth sealed with Revolution, and on 58% of teeth sealed with Dyract Flow.
Baseline caries prevalence in the population related to the effectiveness of pit and fissure sealants
One primary objective of this review was to evaluate the effectiveness of pit and fissure sealants in children and adolescents related to different background levels of caries in the population. Caries prevalence information was given only in eight of the 34 studies: in three studies comparing sealant to a control group without sealant (Bravo 2005; Liu 2012; Songpaisan 1995) and in five studies comparing sealant material to another sealant material (Arrow 1995; Chen 2012; Dhar 2012; Kervanto‐Seppälä 2008; Poulsen 2001). Because of the small number of studies with information on baseline caries prevalence and with different follow‐ups, this primary objective could not be addressed in this review.
Retention of sealants
All 34 studies documented data for retention of sealants (Additional Table 3).
Studies comparing sealant with no sealant
At 12 months of follow‐up, four of the seven studies reported the complete retention of resin sealants to be about 90% (Bojanini 1976; Reisbick 1982; Richardson 1978; Sheykholeslam 1978). The study of Rock 1978 reported the smallest retention figures (complete retention 53% at 12 months). At 24 months of follow‐up, six of the eight studies reported over 80% of complete retention for resin sealants (Bojanini 1976; Brooks 1979; Reisbick 1982; Richardson 1978; Sheykholeslam 1978; Songpaisan 1995). At the 36‐month follow‐up, the complete retention varied from 41% (Rock 1978) to 87% (Bojanini 1976). Even after 48‐54 months, the complete retention of resin‐based sealants was 70% in three of the five studies (Brooks 1979; Erdoğan 1987; Richardson 1978).
In the study of Bravo 2005 the complete retention was reported to be 39% at the 9‐year follow‐up.
In the study of Songpaisan 1995 the complete retention for resin‐based sealants was 85% and for glass ionomer sealants under 1% at 2 years.
Studies comparing different sealant materials
Glass ionomer versus resin sealant
Eight of the 15 studies comparing resin‐based sealant with glass ionomer reported clearly better retention for resin‐based sealants than for glass ionomers (Forss 1998; Karlzén‐Reuterving 1995; Kervanto‐Seppälä 2008; Poulsen 2001; Rock 1996; Sipahier 1995; Songpaisan 1995; Williams 1996). For example, at 36‐48 months of follow‐up, the mean complete retention rate for resin‐based sealants was 76%, and for glass ionomers 8% (based on five studies available at these follow‐ups). The study of Forss 1998 reported a significantly higher retention rate for the resin‐based sealants than for glass ionomers at 7 years of follow‐up (10.3% of glass ionomers and 45.4% of resin sealants were completely present).
In four studies the retention of both sealant materials were reported to be low (Arrow 1995; Beiruti 2006; Dhar 2012; Ganesh 2006). In the study of Ganesh 2006 the complete retention at the 24‐month follow‐up was less than 5% for both materials. In the study of Beiruti 2006, 60% of both sealant materials were lost after 36 months. In the study of Dhar 2012, 80% of resin sealants (without preparation of the surface before sealant application) and 100% of glass ionomer sealants (without preparation of the surface before sealant application) were lost after 2 years. In the study of Arrow 1995 nearly two‐thirds of the participants were judged to have lost both sealant materials by the 44‐month follow‐up.
In the study of Mills 1993, the complete retention of both materials at the 24‐month follow‐up was reported to be high (83% for glass ionomer and 58% for resin‐based sealant). In the study of Chen 2012, only 20% of both sealant materials were lost after 24 months.
The study of Barja‐Fidalgo 2009 reported a complete retention rate for resins of 29% and for glass ionomers of 21% at 5 years.
Resin‐modified glass ionomer versus resin sealant
Both studies comparing resin‐modified glass ionomers to resins at 36 months, reported clearly better complete retention rates for resins (mean 94% for resins and 5% for resin‐modified glass ionomers) (Baseggio 2010; Raadal 1996).
Polyacid‐modified resin composite versus resin sealant
In one of the two studies comparing polyacid‐modified resin composite with resin sealant, the complete retention at the 24‐month follow‐up for both materials was reported to be over 70% (Güngör 2004). In the other study, the complete retention at the 24‐month follow‐up was 16% for polyacid‐modified composites and 66% for resin sealants (Lampa 2004).
Safety of sealants
Only two studies (Bravo 2005; Liu 2012) assessed side effects of the sealants. No adverse effects were detected or reported by patients included in the studies.
Discussion
Summary of main results
Effectiveness of pit and fissure sealants
The resin‐based sealants applied on sound occlusal surfaces were found to be effective for the 9 years of follow‐up studied. Nine split‐mouth studies and three parallel group studies with 5 to 10 year old children found a significant difference in favour of second or third or fourth generation resin‐based sealants on first permanent molars, compared to a control without sealant. The confidence intervals of odds ratios and risk ratios used in the split‐mouth studies are now slightly narrower than they should be because of the dependence of tooth pairs in a child. This is because only one study included only one pair of tooth surfaces per child. In the other studies the average number of tooth pairs per child was 1.6 (children had either one or two tooth pairs under observation). Strictly the pairs are not independent and should be analysed as 'paired data' on a child basis. However, we decided to analyse the pairs independently as otherwise we would be excluding the trials (to our knowledge there are no methods to correct and account for dependence of the tooth pairs when e.g. only marginals are reported). Due to the substantive evidence for benefit of resin‐based sealants, the interpretation of the results would have been the same. The sensitivity analyses, for exploring the effect of risk of bias grading of the studies to outcomes, did not change the interpretation of the results.
The study of Bravo 2005 with 9 years of follow‐up reported 27% of sealed surfaces to be decayed compared to 77% of surfaces without sealant.
The study of Songpaisan 1995 with children aged 12 to 13 years, supported the effectiveness of resin‐based sealants and found significantly more caries in the control group children than in the treatment group children at the 24‐month follow‐up.
The effectiveness of resin‐based sealants is related to the retention of sealants. The retention of resin sealants was good in studies comparing sealant with a control without sealant. At the 12 and 24 months of follow‐up, resin sealants were retained completely on average in 80% of cases. Even after 48‐54 months, the complete retention of resin‐based sealants was 70% in most studies. In the study of Bravo 2005, the sealants were reapplied up to 36 months, and the study reported the complete retention to be 39% at the 9‐year follow‐up.
Only one study with an unclear risk of bias provided data for the comparison of glass ionomer sealant with no treatment (Songpaisan 1995). In this parallel group study, results were not significant. The retention of glass ionomers was poor.
None of the studies reported sealant application on approximal surfaces of permanent premolar or molar teeth.
Sealant versus sealant comparisons
The relative effectiveness of different types of sealants remained inconclusive in this review. Further, no conclusion on the relative effectiveness of the materials at different caries risk levels can be drawn.
Glass ionomer versus resin sealant
When interpreting the results of the studies comparing glass ionomers to resin‐based sealants, it should be noted that the settings of the included studies remained somewhat unclear and that the proportion of sealed decayed surfaces in these studies was, in total, rather small regardless of the material used. For example, in seven studies providing data at 36‐48 months, the proportion of the decayed sealed surfaces ranged from 3% to 14% at 36‐48 months. Only four out of these seven studies gave information on the baseline caries risk level of the children included in the studies. These four studies reported or were assessed to be conducted at low or moderate caries risk populations. In all seven studies, control teeth or control groups without sealants were lacking for further estimating caries risk levels (six of the seven studies were split‐mouth designs, and the only parallel group study at this comparison did not report either the caries prevalence of the population).
In the three studies which found statistically significantly more caries in glass ionomer sealed teeth at 36‐48 months than in resin‐sealed teeth, the complete retention for resin sealants was documented to be good (mean 80%), and for glass ionomers low (mean 3%) (Kervanto‐Seppälä 2008; Poulsen 2001; Rock 1996). Two other studies with similar retention figures (favouring resins) did not find a difference between the materials in caries figures (Karlzén‐Reuterving 1995; Williams 1996). In those two studies, in which glass ionomers were found to be better regarding caries figures, the retention of both sealant materials was reported as low (resin‐based sealants were lost in 60% to 72% of cases and glass ionomers in 60% to 79% of cases after 36 months) (Arrow 1995; Beiruti 2006). There might be many reasons behind the divergent results (in caries figures) between the studies comparing glass ionomers to resin‐based sealants, and a straightforward conclusion can, however, not be drawn based only on retention.
Other sealant material comparisons
Although two of the three studies comparing resin‐modified glass ionomers with resin‐based sealants favoured resins (regarding caries figures) (Baseggio 2010; Raadal 1996), straightforward conclusions on the relative effectiveness of these two materials cannot be drawn based only on so few data. In both studies, the complete retention was stated to be over 90% for resins but only 5% for resin‐modified glass ionomer sealants. The studies did not report information on the caries prevalence of the population.
The two studies comparing polyacid‐modified composite resins to resin‐based sealants did not give any more information about the superiority of the sealant materials (Güngör 2004; Lampa 2004).
Safety of sealants
Only two studies in this review assessed or considered adverse effects of sealants (Bravo 2005; Liu 2012). In these studies no adverse events (such as allergic reactions) were detected. This is understandable because rare adverse events or long‐term adverse effects are unlikely to be observed in clinical trials.
However, some systematic reports have recently considered the possible oestrogen‐like effects of resin‐based materials including Bisphenol A (BPA) (Azarpazhooh 2008; Fleisch 2010). This synthetic chemical resin is widely used in the production of plastic products intended for common life but rarely used as such in dental materials (ADA 2010). Dental resins include primarily BPA derivatives (like bis‐GMA, and bis‐DMA) rather than pure BPA. The derivatives can hydrolyze to BPA and be detected transiently in saliva (Arenholt 1999; Schmalz 1999). BPA has been detected in saliva for up to 3 hours after application of resin sealants (Fleisch 2010).
The systematic review by Fleisch 2010 found two studies which measured systemic absorption of BPA after application of resin sealants with hydrolysis to BPA. The review concluded that the quantity and duration of systemic BPA absorption after resin placement is not clear from the available data. Further, the total BPA intake (like contaminated food) can confound the data.
The current evidence suggests that patients are not at risk for oestrogen‐like effects when sealants are used (ADA 2010; Azarpazhooh 2008; Fleisch 2010).The American Dental Association concluded that the estimated BPA exposure from dental materials is very low level compared to the total estimated daily BPA exposure from food and environmental sources (ADA 2010).
Overall completeness and applicability of evidence
Sealant materials and settings
Nine of the 12 studies comparing resin‐based sealant with a control without sealant were conducted in industrialised countries in the 1970s or 1980s. Two studies were from the 1990s (the study of Bravo 2005 conducted in Spain, and the study of Songpaisan 1995 conducted in Thailand), and one study was from the 2000s (the study of Liu 2012 conducted in China).
All studies except two (Bravo 2005; Liu 2012) comparing resin‐based sealant with a control without sealant used second generation resin‐based sealants.
The studies comparing different sealant materials were published between 1993 and 2012.
In most of all 34 included studies the children were recruited from schools or community‐oriented dental clinics. In general, these studies were conducted in well‐equipped dental settings.
Variation in baseline caries level
One primary objective of this review was to evaluate the effectiveness of pit and fissure sealants in children and adolescents related to different background levels of caries in the population. When interpreting the results one essential question is: does the treatment benefit vary according to the baseline risk of the children and how effective are the sealants in children at high caries risk and how effective in children at low or moderate caries risk.
The three studies with parallel group design comparing resin‐based sealant to control without sealant reported information on the baseline caries prevalence of the children (Bravo 2005; Liu 2012; Songpaisan 1995). However, different outcome measures and follow‐up times between these studies made it difficult to compare the results. Further, it has been stated that the caries progression rate has changed and has become slower during recent decades (Whelton 2004), which still complicates making conclusions on results when considering baseline caries prevalence.
All the three studies giving information on the baseline caries prevalence of the children, found statistically significantly more caries in control group children compared to resin‐sealant group children. The study by Liu 2012 with children aged 8 to 10 years, conducted at mean baseline dmft level of 3.4, detected in total small number of carious occlusal surfaces of first molars after 2 years (3% in resin sealant group and 7.4% in placebo group). The study by Bravo 2005 with children aged 6 to 8 years (study started 1990), with mean baseline dft level in sealant group 2.24 and in control group 2.98, found resin‐based sealants to be effective even after 9 years of follow‐up (27% of sealed surfaces were decayed compared to 77% of surfaces without sealant). The study of Songpaisan 1995 with a mean baseline DMFT of 1.81 among children aged 12 to 13 found also resin‐based sealants to be effective after 2 years, with a difference of mean number of decayed and filled occlusal surfaces of permanent molars between groups (DFS) = 0.65 (95% CI 0.47 to 0.83). According to the World Health Organization (WHO), the study by Songpaisan 1995 represented low caries prevalence population (WHO 2003).
None of the nine split‐mouth studies comparing resin‐based sealant to control without sealant gave information on the baseline caries risk. Three of those nine studies (with fluoridated tap water) stated that the children included in the studies had to have caries at baseline and the children had to have at least one sound tooth pair. It is obvious, however, that on average, the children in these studies had risk of caries. At the 1‐year follow‐up, five of the available six studies stated 19% to 46% of the control tooth surfaces to be decayed. At the 2‐year follow‐up, the five available studies stated 37% to 69% of the control tooth surfaces to be decayed. (Two of the nine split‐mouth studies were not considered in these calculations: Hunter 1988 with only 3‐year results, and Reisbick 1982 where the figure was not possible to calculate because of the way data were reported in the study).
On the whole, there was not sufficient information to conclude how effective sealants are at different caries prevalence levels. The data of studies comparing resin sealants to control without sealants reveal that resin‐based sealants are effective in children at high caries risk but the information for the other caries prevalence levels is very scarce. To be able to evaluate the benefit of sealants at different conditions, long‐term follow‐up studies are needed, especially because caries progression rates in permanent teeth in future are difficult to predict.
Diagnosis
This review was focused on the effect of sealants in preventing or controlling caries, and sealant trials that were mainly intended to manage dental caries were excluded from the review. Studies with sound occlusal surfaces of molars and premolars or with enamel lesions were accepted. However, we included the study by Beiruti 2006 comparing glass ionomers to resin sealants, where less than 10% of tooth surfaces had a small dentine caries lesion and most tooth surfaces were reported to be sound.
Caries diagnosis of occlusal surfaces can be challenging. In general, using conventional visual, tactile and radiographic methods in occlusal caries lesion diagnosis, it is not accurate enough to identify whether a lesion extends into the dentine or not (McComb 2001). New technologies such as DIAGNOdent laser fluorescence devices may be more sensitive in detecting occlusal dentinal caries (Bader 2004; Lussi 2004). However, the likelihood of false‐positive diagnoses may increase when using laser‐fluorescence compared with visual methods (Bader 2004). Regardless of the caries diagnostic method used, the condition of an occlusal surface to be sealed remains, however, in any case somewhat unclear.
In the resin‐based sealant versus no treatment comparisons, 10 out of the 12 studies reported sealants to be applied on sound occlusal surfaces. Two studies included also occlusal surfaces with enamel lesion (Liu 2012; Richardson 1978). The study of Richardson 1978 accepted sticky surfaces (surfaces which offered resistance to explorer removal after moderate pressure, without any visual signs of caries were deemed sticky), and the study of Liu 2012 included surfaces with signs of enamel caries viewed as wet, with opacities and discolouration. The diagnosis of the surface to be sealed was based on clinical examination in nine studies, one further study used also a DIAGNOdent device (Liu 2012). In two studies, diagnosis was based on visual and roentgenographic examinations (Erdoğan 1987; Reisbick 1982).
Quality of the evidence
The body of evidence comparing resin‐based sealants with a no‐sealant control group comprised 12 randomised trials and was assessed as being of moderate quality according to the GRADE assessment criteria. This grade of 'moderate' implies that further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. After 2 years of follow‐up in six studies, the odds ratio for caries was 0.12 (95% confidence interval 0.07 to 0.19). As five of these six trials were published as early as between 1976 and 1979, it is not unreasonable to anticipate that a new study could change this estimate, even if it found the sealants effective.
The quality of the body of evidence for glass ionomer sealants compared to a no‐sealant control (based on one study) is very low, as is the evidence for comparing one type of sealant against another. This was due to inconsistent effects on caries outcomes, due to the diversity in the interventions, comparisons and time of outcomes reported in the trials, the age groups of children included and variation in reporting of background exposure to fluoride.
Potential biases in the review process
Study design
The efficacy of sealants in preventing caries has been commonly connected with the retention of resin‐based sealants. However, the aim of this review was to examine the effectiveness of sealants in caries prevention by caries and not by retention. Furthermore the effectiveness of sealants was evaluated without other preventive treatments.
Studies with first generation sealants were excluded from this review because retention and caries protection have been shown to be superior for later sealant materials; further, first generation sealants are no longer marketed (Ripa 1993). One reason for the rather small number of included studies with a control group without sealant was that from the 1980s most of the clinical sealant studies were retention studies. Overall, many of the sealant studies did not fulfil the quality criteria and for that reason were not included. Further, where it was impossible to assess the pure effectiveness of sealants (i.e. where studies included other preventive treatments or caries prevention programmes) the studies were not included.
In this review only randomised or quasi‐randomised controlled trials were included. The unit of randomisation could be individual, group (school, school class etc.), tooth or tooth pair. Studies without random or quasi‐random sequence generation were excluded in this review so as to eliminate the possibilities that the person applying sealants chose intentionally teeth or children for sealing, or that certain teeth or children were systematically sealed leaving systematically some teeth or children without sealant.
We decided to consider only studies with a full‐text report in this review. Studies reported only as abstracts were excluded. This is because there is evidence that discrepancies exist between data reported in the abstract and the final published full report and that information on trial quality indicators is often lacking (Chokkalingam 1998; Hopewell 2006). Thus we saw that the full‐text report is required to ensure reliable data extraction and assessment of the risk of bias. To diminish the risk of publication bias we contacted authors of potential abstracts to obtain information whether a full‐text report of the study (unpublished or published) was available.
Analysis issues
In the previous version of this review, it was required that clustered data should have been taken into account in the study analysis. Studies with inadequate analyses were excluded. This was because in the context of a meta‐analysis, studies in which clustering (e.g. clustering of children in schools, teeth within a child, tooth within a tooth pair) has been ignored in the analyses will have too narrow confidence intervals and will receive a wrong weighting in a meta‐analysis (Deeks 2008). In particular, when only a few studies are included in a specific meta‐analysis, the role of the weights is important.
In this 2013 review update, all studies which fulfilled the inclusion criteria were, however, included despite whether the data were adequately analysed or not. In split‐mouth studies which ignored the paired data in their analysis, the marginal Becker‐Balagtas method was used for calculating odds ratios with appropriate standard errors taking the clustering of the teeth within a tooth pair into account. The Becker‐Balagtas method as proposed in the articles by Curtin 2002 and later by Elbourne 2002 was used because The Cochrane Collaboration recommends it in their handbook for systematic reviews of interventions (Higgins 2011b). (The Becker‐Balagtas method described in the article by Elbourne 2002 has been corrected in the article by Stedman 2011.) The alternative method introduced by Barker 2011 (which is based on a hierarchical Bayes structure) is still quite novel but it will be considered in future updates.
Heterogeneity
There was significant heterogeneity for comparisons between the resin sealant versus no treatment at several of the time points. There were, however, insufficient studies to investigate reasons for this.
Confounding factors
Most of the studies did not report on other factors that might be related to caries incidence. Such factors are individual behavioural factors such as the frequency of eating sugary snacks, the use of fluoridated toothpaste, and other caries preventive procedures during the trial (e.g. topical fluoride applications).
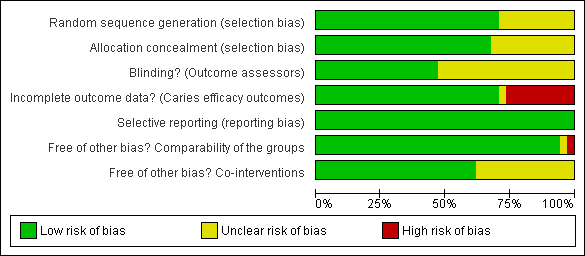
Risk of bias graph: review authors' judgements about each risk of bias domain presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias domain for each included study.

Comparison 1 Resin sealant versus no treatment, Outcome 1 Caries yes/no at 12 months.

Comparison 1 Resin sealant versus no treatment, Outcome 2 Caries yes/no at 24 months.

Comparison 1 Resin sealant versus no treatment, Outcome 3 Caries yes/no at 36 months.

Comparison 1 Resin sealant versus no treatment, Outcome 4 Caries yes/no at 48‐54 months.
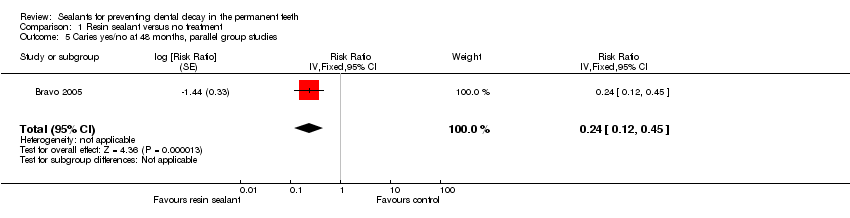
Comparison 1 Resin sealant versus no treatment, Outcome 5 Caries yes/no at 48 months, parallel group studies.

Comparison 1 Resin sealant versus no treatment, Outcome 6 12‐13 years ‐ 2‐year DFS increment.

Comparison 1 Resin sealant versus no treatment, Outcome 7 Caries yes/no at 5 years.

Comparison 1 Resin sealant versus no treatment, Outcome 8 Caries yes/no at 6 years.

Comparison 1 Resin sealant versus no treatment, Outcome 9 Caries yes/no at 7 years.

Comparison 1 Resin sealant versus no treatment, Outcome 10 Caries yes/no at 9 years, parallel group studies.

Comparison 2 Glass ionomer sealant versus no treatment, Outcome 1 12‐13 years ‐ 2‐year DFS increment.

Comparison 3 Glass ionomer versus resin sealant, Outcome 1 Caries yes/no at 12 months.

Comparison 3 Glass ionomer versus resin sealant, Outcome 2 Caries yes/no at 24 months.

Comparison 3 Glass ionomer versus resin sealant, Outcome 3 12‐13 years ‐ 2‐year DFS increment.

Comparison 3 Glass ionomer versus resin sealant, Outcome 4 Caries yes/no at 36‐48 months.

Comparison 3 Glass ionomer versus resin sealant, Outcome 5 Caries yes/no at 5 years, parallel group studies.

Comparison 3 Glass ionomer versus resin sealant, Outcome 6 Caries yes/no at 7 years.

Comparison 4 Resin‐modified glass ionomer versus resin sealant, Outcome 1 Caries yes/no at 12 months.

Comparison 4 Resin‐modified glass ionomer versus resin sealant, Outcome 2 Caries yes/no at 12 months, parallel group studies.

Comparison 4 Resin‐modified glass ionomer versus resin sealant, Outcome 3 Caries yes/no at 24 months.

Comparison 4 Resin‐modified glass ionomer versus resin sealant, Outcome 4 Caries yes/no at 24 months, parallel group studies.

Comparison 4 Resin‐modified glass ionomer versus resin sealant, Outcome 5 Caries yes/no at 36 months.

Comparison 5 Polyacid‐modified resin composite versus resin sealant, Outcome 1 Caries yes/no at 24 months.
| Resin‐based sealant compared to control without sealant for preventing dental caries | ||||||
| Patient or population: Children and adolescents | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | Number of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control teeth | Sealed teeth | |||||
| Dentine caries in permanent molars Follow‐up: 2 years | Incidence of carious first molars (40%) 400 per 10001 | Incidence of carious first molars (6.3%) 63 per 1000 (38 to 96) | OR 0.12 (0.07 to 0.19) 2 | 1259 children randomised & 1066 evaluated after 2 years | ⊕⊕⊕⊝ |
Benefits of resin‐sealant maintained up to at least 48 months of follow‐up6 |
| Incidence of carious first molars (70%) 700 per 10001 | Incidence of carious first molars (19%) 190 per 1000 (122 to 272) | OR 0.12 (0.07 to 0.19) 2 | 1259 children randomised & 1066 evaluated after 2 years | ⊕⊕⊕⊝ |
Benefits of resin‐based sealant maintained up to at least 48 months of follow‐up6 | |
| CI: confidence interval; OR: odds ratio | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 The incidence of carious control teeth in the five split‐mouth trials included in this comparison ranged from 37% to 69% (studies published between 1976 and 1979). We have shown the effect of sealants at each end of this range. These studies did not give information on the baseline caries prevalence of the children. 2 There was considerable heterogeneity in this estimate (I2 = 77% P = 0.0007) but all of the trials showed a statistically significant effect favouring sealants. 3 Six studies at low risk of bias for the four key domains of allocation concealment, incomplete outcome data, selective reporting and baseline comparability of the groups. 4All studies recruited children aged 5‐10 years. Three studies conducted in areas with fluoridated water, two studies stated water was not fluoridated and the remaining one study did not report whether water supplies were fluoridated. 5 Five trials were published between 1976 and 1979 and one in 2012. One further parallel group trial from Thailand at unclear risk of bias reporting DFS increment published in 1995 also found a benefit in favour of resin‐based sealant (mean difference in DFS increment ‐0.65, 95% CI ‐0.83 to ‐0.47, 276 children evaluated). 6 The benefit associated with sealant use is maintained at all of the follow‐up estimates (up to 9 years) though the number of studies and the number of children available for evaluation reduced markedly over this period (e.g. at 48 to 54 months of follow‐up odds ratio 0.21, 95% CI 0.16 to 0.28, two studies at low risk of bias and two studies at high risk of bias, 482 children evaluated; risk ratio 0.24, 95% CI 0.12 to 0.45, one study at unclear risk of bias, 203 children evaluated). | ||||||
| Glass ionomer sealant compared to control without sealant for preventing dental caries | ||||||
| Patient or population: Children and adolescents | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | Number of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control teeth | Sealed teeth | |||||
| Caries as DFS increment in permanent molars Follow‐up: 2 years | The mean DFS increment of control tooth surfaces 0.701 | The mean DFS increment of sealed tooth surfaces 0.52 | The mean DFS difference ‐0.18 | 452 children randomised and 404 evaluated after 2 years follow‐up | ⊕⊝⊝⊝ |
Extended follow‐up4 |
| CI: confidence interval; OR: odds ratio; RR: risk ratio; DFS: decayed and filled occlusal tooth surfaces of molars | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 This is a low caries prevalence population from Thailand according to WHO figures (WHO 2003) (mean baseline DMFT of 1.81). 2 A single study at unclear risk of bias (no information on sequence generation or allocation concealment). 3 Children aged 12‐13 years at baseline. Study conducted in an area with naturally fluoridated water. 4 Study published in 1995. 5 Follow‐up only reported for 2 years in this study. | ||||||
| Glass ionomer sealants compared to resin sealants for preventing caries | ||||
| Patient or population: Children and adolescents Settings: RCTs conducted in the UK, Scandinavia, Asia, Australia, Brazil and the Arab world Intervention: Glass ionomer sealant (including Fuji III, VII, IX, Ketac Silver, Ketac‐fil, Ketac Molar Easymix or Baseline) Comparison: Resin sealant | ||||
| Outcomes | Impact Inconsistent effect | Number of participants | Quality of the evidence | Comments |
| Dentine caries in permanent molars Follow‐up: 1, 2, 3, 4, 5 and 7 years | Inconsistent effect. There were differences in: comparisons, outcomes, outcome reporting times and background fluoride exposure including water fluoridation | 15 trials1,2 (2939 participants randomised) | ⊕⊝⊝⊝ | |
| RCT: randomised controlled trial | ||||
| GRADE Working Group grades of evidence | ||||
| 1 Five trials at high risk of bias, four at unclear risk of bias, and six at low risk of bias (for the four key domains of allocation concealment, incomplete outcome data, selective reporting and baseline comparability of the groups). 2 Trials published between 1993 and 2012. | ||||
| Resin‐modified glass ionomer sealants compared to resin sealants for preventing caries | ||||
| Patient or population: Children and adolescents Settings: RCTs conducted in Norway, Egypt & Brazil Intervention: Resin‐modified glass ionomer sealant (Fuji II LC, Vitrebond or Vitremer) Comparison: Resin sealant (Helioseal, Tetric Flow, Fluoroshield or Concise White) | ||||
| Outcomes | Impact Inconsistent effect | Number of participants | Quality of the evidence | Comments |
| Dentine caries in permanent molars Follow‐up: 1, 2 and 3 years | Inconsistent effect. Different products, outcomes, outcome reporting times and age groups | 3 trials1,2,3 (418 participants randomised) | ⊕⊝⊝⊝ | |
| RCT: randomised controlled trial | ||||
| GRADE Working Group grades of evidence | ||||
| 1Two trials at unclear risk of bias and one at low risk of bias (for the four key domains of allocation concealment, incomplete outcome data, selective reporting and baseline comparability of the groups). 2 No information on background fluoride exposure or baseline caries prevalence. 3 Trials published between 1996 and 2010. | ||||
| Polyacid‐modified resin sealants compared to resin sealants for preventing caries | ||||
| Patient or population: Children and adolescents Settings: RCTs conducted in Sweden and Turkey Intervention: Polyacid‐modified resin composite (Dyract Seal) Comparison: Resin sealant (3rd or 4th generation Delton) | ||||
| Outcomes | Impact No difference | Number of participants | Quality of the evidence | Comments |
| Dentine caries in permanent molars Follow‐up: 2 years | No difference in caries after 2 years | 2 trials1,2,3 (84 participants randomised and 68 evaluated after 2 years) | ⊕⊝⊝⊝ | |
| RCT: randomised controlled trial | ||||
| GRADE Working Group grades of evidence | ||||
| 1Two trials, different products compared. 2One trial at high risk of bias and one at unclear risk of bias. 3 Water not fluoridated in one study and no information on background fluoride in the other, age at baseline 6‐13 years, no information on baseline caries prevalence. | ||||
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 12 MONTHS | ||||||||
| Split‐mouth studies | Study | Both sound | FS sound / | FS carious / | Both carious | Proportion of the decayed control tooth surfaces to total control surfaces | RR (95% CI) based on paired data | Becker‐Balagtas marginal |
| Bojanini 1976 | 188 | 79 | 6 | 2 | 0.29 | RR = 0.099 (0.049, 0.201) | OR = 0.07 (0.03, 0.15) ICC 0.02 | |
| Charbeneau 1979 | 104 | 82 | 5 | 11 | 0.46 | RR = 0.172 (0.107, 0.276) | OR = 0.10 (0.06, 0.17) ICC 0.13 | |
| Sheykholeslam 1978 | 132 | 49 | 2 | 3 | 0.28 | RR = 0.096 (0.040, 0.229) | OR = 0.07 (0.03, 0.18) ICC 0.12 | |
| Split‐mouth studies | Study | FS sound | FS carious | Control sound | Control carious | Proportion of the decayed control tooth surfaces to total control surfaces | Becker‐Balagtas marginal | |
| Erdoğan 1987 | 103 | 15 | 96 | 22 | 0.19 | OR = 0.64 ICC 0.05 | ||
| Richardson 1978 | 375 | 18 | 300 | 93 | 0.24 | OR = 0.15 ICC 0.05 | ||
| Rock 1978 | 347 | 15 | 316 | 46 | 0.13 | OR = 0.30 ICC 0.05 | ||
| POOLED | OR = 0.16 | |||||||
| Split‐mouth studies without summary data of tooth pairs | Study | Description of the data | ||||||
| Reisbick 1982 | Paired summary data reported only by tooth sites (3 sites per occlusal surface) but not by tooth surfaces which were the analysis units in this review. However, effectiveness based on paired tooth surfaces was reported to be 90% at 14 months. | |||||||
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 24 MONTHS | ||||||||
| Split‐mouth studies | Study | Both sound | FS sound / | FS carious / | Both carious | Proportion of the decayed control tooth surfaces to total control surfaces | RR (95% CI) based on paired data | Becker‐Balagtas marginal |
| Brooks 1979 | 144 | 64 | 3 | 22 | 0.37 | RR = 0.29 | OR = 0.21 (0.14, 0.31) ICC 0.37 | |
| Charbeneau 1979 | 53 | 100 | 4 | 29 | 0.69 | RR = 0.256 | OR = 0.10 (0.06, 0.15) ICC 0.19 | |
| Sheykholeslam 1978 | 85 | 79 | 1 | 10 | 0.51 | RR = 0.124 | OR = 0.06 (0.03, 0.12) ICC 0.21 | |
| Split‐mouth studies | Study | FS sound | FS carious | Control sound | Control carious | Proportion of the decayed control tooth surfaces to total control surfaces | Becker‐Balagtas marginal | |
| Bojanini 1976 | 245 | 7 | 159 | 93 | 0.37 | OR = 0.05 ICC 0.05 | ||
| Richardson 1978 | 326 | 26 | 222 | 130 | 0.37 | OR = 0.14 ICC 0.05 | ||
| Parallel group studies | Study | Description of the data | OR (95% CI) | |||||
| Liu 2012 | OR based on the model of the multilevel GEE logistic regression. | OR = 0.32 | ||||||
| POOLED | OR = 0.12 | |||||||
| Split‐mouth studies without summary data of tooth pairs | Study | Description of the data | ||||||
| Reisbick 1982 | Paired summary data reported only by tooth sites (3 sites per occlusal surface) but not by tooth surfaces which were the analysis units in this review. However, effectiveness based on paired tooth surfaces was reported to be 80% at 20 months. | |||||||
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 32‐36 MONTHS | ||||||||
| Split‐mouth studies | Study | Both sound | FS sound / | FS carious / | Both carious | Proportion of the decayed control tooth surfaces to total control surfaces | RR (95% CI) based on paired data | Becker‐Balagtas marginal |
| Brooks 1979 | 111 | 63 | 4 | 23 | 0.43 | RR = 0.314 | OR = 0.21 (0.14, 0.31) ICC 0.34 | |
| Charbeneau 1979 | 45 | 96 | 5 | 47 | 0.74 | RR = 0.364 | OR = 0.13 (0.09, 0.19) ICC 0.23 | |
| Hunter 1988 | 302 | 163 | 9 | 35 | 0.39 | RR = 0.222 | OR = 0.15 (0.11, 0.20) ICC 0.26 | |
| Split‐mouth studies | Study | FS sound | FS carious | Control sound | Control carious | Proportion of the decayed control tooth surfaces to total control surfaces | Becker‐Balagtas marginal | |
| Bojanini 1976 | 250 | 22 | 128 | 144 | 0.53 | OR = 0.08 | ||
| Sheykholeslam 1978 | 142 | 22 | 63 | 101 | 0.62 | OR = 0.10 | ||
| Richardson 1978 | 279 | 58 | 176 | 161 | 0.48 | OR = 0.23 | ||
| Rock 1978 | 253 | 55 | 222 | 86 | 0.28 | OR = 0.56 ICC 0.05 | ||
| POOLED | OR = 0.17 | |||||||
| Split‐mouth studies without summary data of tooth pairs | Study | Description of the data | ||||||
| Reisbick 1982 | Paired summary data reported only by tooth sites (3 sites per occlusal surface) but not by tooth surfaces which were the analysis units in this review. However, effectiveness based on paired tooth surfaces was reported to be 70% at 32 months. | |||||||
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 48‐54 MONTHS | ||||||||
| Split‐mouth studies | Study | Both sound | FS sound / | FS carious / | Both carious | Proportion of the decayed control tooth surfaces to total control surfaces | RR (95% CI) based on paired data | Becker‐Balagtas marginal |
| Brooks 1979 | 61 | 67 | 3 | 37 | 0.62 | RR = 0.385 | OR = 0.19 (0.13, 0.28) ICC 0.35 | |
| Charbeneau 1979 | 37 | 81 | 3 | 64 | 0.78 | RR = 0.462 | OR = 0.16 (0.11, 0.23) ICC 0.31 | |
| Split‐mouth studies | Study | FS sound | FS carious | Control sound | Control carious | Proportion of the decayed control tooth surfaces to total control surfaces | Becker‐Balagtas marginal | |
| Erdoğan 1987 (54 months) | 82 | 14 | 67 | 29 | 0.30 | OR = 0.39 | ||
| Richardson 1978 (48 months) | 262 | 68 | 151 | 179 | 0.54 | OR = 0.22 | ||
| POOLED | OR = 0.21 | |||||||
| Parallel group studies | Study | Description of the data | RR (95% CI) | |||||
| Bravo 2005 | Data are based on requested risk ratio (RR) value with cluster corrected standard error (SE). | RR = 0.24 | ||||||
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 5 YEARS | ||||||||
| Split‐mouth studies | Study | FS sound | FS carious | Control sound | Control carious | Proportion of the decayed control tooth surfaces to total control surfaces | Becker‐Balagtas marginal | |
| Richardson 1978 | 246 | 85 | 157 | 174 | 0.53 | OR = 0.31 | ||
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 6 YEARS | ||||||||
| Split‐mouth studies | Study | Both sound | FS sound / | FS carious / | Both carious | Proportion of the decayed control tooth surfaces to total control surfaces | RR (95% CI) based on paired data | Becker‐Balagtas marginal |
| Brooks 1979 | 50 | 57 | 5 | 38 | 0.63 | RR = 0.45 | OR = 0.23 (0.16, 0.35) ICC 0.329 | |
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 7 YEARS | ||||||||
| Split‐mouth studies | Study | Both sound | FS sound / | FS carious / | Both carious | Proportion of the decayed control tooth surfaces to total control surfaces | RR (95% CI) based on paired data | Becker‐Balagtas marginal |
| Brooks 1979 | 29 | 41 | 2 | 30 | 0.70 | RR = 0.45 | OR = 0.20 (0.12, 0.32) ICC 0.355 | |
| RESIN FISSURE SEALANT (FS) VERSUS NO TREATMENT: 9 YEARS | ||||||||
| Parallel group studies | Study | Description of the data | RR (95% CI) | |||||
| Bravo 2005 | Data are based on requested risk ratio (RR) value with cluster corrected standard error (SE). | RR = 0.35 | ||||||
| GLASS IONOMER (GI) SEALANT VERSUS RESIN SEALANT: 12 MONTHS | ||||||||
| Split‐mouth studies | Study | GI sound | GI carious | Resin sound | Resin carious | Becker‐Balagtas marginal | ||
| Dhar 2012 | 23 | 2 | 24 | 1 | OR = 2.09 P = 0.76 | |||
| Dhar 2012 | 25 | 0 | 25 | 0 | Not estimable | |||
| Karlzen‐Reuterving 1995 (no difference) | 72 | 0 | 70 | 2 | OR = 0.19 P = 0.25 | |||
| Rock 1996 (no difference) | 151 | 7 | 157 | 1 | OR = 7.28 (0.91, 58.12) P = 0.07 | |||
| Sipahier 1995 (no difference) | 80 | 6 | 81 | 5 | OR = 1.22 P = 0.75 | |||
| RESIN‐MODIFIED GLASS IONOMER (GI) VERSUS RESIN SEALANT: 12 MONTHS | ||||||||
| Split‐mouth studies | Study | GI sound | GI carious | Resin sound | Resin carious | Becker‐Balagtas marginal | ||
| Baseggio 2010 (no difference) | 640 | 0 | 640 | 0 | Not estimable | |||
| Parallel group studies | Study | Description of the data | OR (95% Cl) | |||||
| Amin 2008 (no difference) | Clustered data (2 teeth per child). | OR = 1.08 | ||||||
| GLASS IONOMER (GI) SEALANT VERSUS RESIN SEALANT: 24 MONTHS | ||||||||
| Split‐mouth studies | Study | Both sound | GI sound / | GI carious / | Both carious | RR (95% CI) based on paired data | Becker‐Balagtas marginal | |
| Poulsen 2001 (resin slightly better) | 191 | 2 | 9 | 1 | RR = 3.33 | OR = 3.46 (1.03, 11.63) | ||
| Ganesh 2006 (no difference) | 100 | 0 | 0 | 0 | Not estimable | Not estimable | ||
| Mills 1993 (no difference) | 59 | 0 | 0 | 0 | Not estimable | Not estimable | ||
| Split‐mouth studies | Study | GI sound | GI carious | Resin sound | Resin carious | Becker‐Balagtas marginal | ||
| Dhar 2012 | 23 | 2 | 22 | 3 | OR = 0.64 P = 0.81 | |||
| Dhar 2012 | 24 | 1 | 21 | 4 | OR = 0.22 P = 0.38 | |||
| Forss 1998 (no difference) | 144 | 7 | 144 | 7 | OR = 1 (0.35, 2.85) | |||
| Karlzen‐Reuterving 1995 (no difference) | 71 | 1 | 70 | 2 | OR = 0.49 (0.05, 5.25) P = 0.77 | |||
| Rock 1996 (resin better) | 116 | 16 | 130 | 2 | OR = 8.96 (2.07, 38.82) | |||
| Williams 1996 (resin better) | 274 | 21 | 289 | 6 | OR = 3.69 (1.50, 9.09) P = 0.004 | |||
| Parallel group studies | Study | Description of the data | OR (95% Cl) | |||||
| Chen 2012 | Data of glass ionomer sealant groups were combined (Ketac Molar Easymix with or without LED high energy curing light). | OR = 1.67 | ||||||
| RESIN‐MODIFIED GLASS IONOMER (GI) VERSUS RESIN SEALANT: 24 MONTHS | ||||||||
| Split‐mouth studies | Study | GI sound | GI carious | Resin sound | Resin carious | Becker‐Balagtas marginal | ||
| Baseggio 2010 | 583 | 57 | 620 | 20 | OR = 3.03 (1.82, 5.05) P < 0.0001 | |||
| Parallel group studies | Study | Description of the data | OR (95% Cl) | |||||
| Amin 2008 (no difference) | Clustered data (2 teeth per child). | OR = 1.14 | ||||||
| GLASS IONOMER (GI) SEALANT VERSUS RESIN SEALANT: 36‐48 MONTHS | ||||||||
| Split‐mouth studies | Study | Both sound | GI sound / | GI carious / | Both carious | RR (95% CI) based on paired data | Becker‐Balagtas marginal | |
| Poulsen 2001 | 156 | 6 | 37 | 7 | RR = 3.385 | OR = 4.03 (2.23, 7.29) | ||
| Arrow 1995 | 378 | 28 | 3 | 3 | RR = 0.194 | OR = 0.18 (0.08, 0.41) P < 0.001 | ||
| Kervanto‐Seppälä 2008 | 625 | 5 | 25 | 2 | RR = 3.857 | OR = 3.98 (1.80, 8.80) P < 0.001 | ||
| Split‐mouth studies | Study | GI sound | GI carious | Resin sound | Resin carious | Becker‐Balagtas marginal | ||
| Karlzen‐Reuterving 1995 (no difference) | 71 | 1 | 69 | 3 | OR = 0.32 (0.03, 3.03) P = 0.63 | |||
| Rock 1996 (resin better) | 106 | 24 | 126 | 4 | OR = 7.13 (2.45, 20.76) P < 0.001 | |||
| Williams 1996 (no difference) | 200 | 22 | 206 | 16 | OR = 1.42 (0.73, 2.73) P = 0.34 | |||
| Study | Description of the data | RR (95% CI) | ||||||
| Parallel group studies | Beiruti 2006 (ionomer better) | Data are based on reported risk ratio (RR) value with cluster corrected standard error (SE). | After 3 years: After 4 years: | |||||
| RESIN‐MODIFIED GLASS IONOMER (GI) VERSUS RESIN SEALANT: 36 MONTHS | ||||||||
| Study | GI sound | GI carious | Resin sound | Resin carious | Becker‐Balagtas marginal | |||
| Split‐mouth studies | Baseggio 2010 (resin better) | 502 | 126 | 572 | 56 | OR = 2.56 (1.84, 3.56) P < 0.001 | ||
| Raadal 1996 (resin better) | 64 | 9 | 73 | 0 | OR = 11.38 (1.47, 88.42) P = 0.012 | |||
| POOLED | OR = 2.66 P < 0.00001 Het. Chi2 | |||||||
| GLASS IONOMER (GI) SEALANT VERSUS RESIN SEALANT: 5 YEARS | ||||||||
| Study | Description of the data | RR (95% CI) | ||||||
| Parallel group studies | Beiruti 2006 (ionomer better) | Data are based on reported risk ratio (RR) value with cluster corrected standard error (SE). | RR = 0.28 | |||||
| Barja‐Fidalgo 2009 | Raw data were obtained from the authors because several of a child's teeth had been sealed (a child is a cluster). Raw data were used in calculations. | RR = 0.38 | ||||||
| POOLED | RR = 0.30 P = 0.0005 Het. Chi2 | |||||||
| GLASS IONOMER (GI) SEALANT VERSUS RESIN SEALANT: 7 YEARS | ||||||||
| Study | Both sound | GI sound / | GI carious / | Both carious | RR (95% CI) based on paired data | Becker‐Balagtas marginal | ||
| Split‐mouth studies | Forss 1998 | 66 | 8 | 15 | 8 | RR = 1.44 (0.88, 2.35) | OR = 1.57 (0.86, 2.89) P = 0.21 | |
| POLYACID‐MODIFIED RESIN COMPOSITE VERSUS RESIN SEALANT: 24 MONTHS | ||||||||
| Study | Both sound | Composite sound / | Composite carious / | Both carious | Becker‐Balagtas marginal | |||
| Split‐mouth studies | Lampa 2004 | 41 | 3 | 0 | 0 | OR = 0.23 (0.03, 1.76) | ||
| Güngör 2004 | 50 | 10 | 8 | 2 | OR = 0.80 (0.33, 1.97) | |||
| POOLED | OR = 0.65 (0.29, 1.48) P = 0.31 Het. Chi2 | |||||||
| CI = confidence interval; df = degrees of freedom; ICC = intra‐cluster correlation coefficient; OR = odds ratio; RR = risk ratio. | ||||||||
| Comparison | Control number | Control mean | Control SD | Test number | Test mean | Test SD | Mean DFS diff. | 95% CI | P value |
| Control versus resin | 143 | 0.70 | 0.96 | 133 | 0.05 | 0.57 | 0.65 | 0.47 to 0.83 | < 0.00001 |
| Control versus GI | 143 | 0.70 | 0.96 | 261 | 0.52 | 1.09 | 0.18 | ‐0.03 to 0.39 | 0.09 |
| Resin versus GI | 133 | 0.05 | 0.57 | 261 | 0.52 | 1.09 | ‐0.47 | ‐0.63 to ‐0.31 | < 0.00001 |
| CI = confidence interval; DFS = decayed and filled occlusal surfaces; GI = glass ionomer; SD = standard deviation. | |||||||||
| Time | Study | Sealant | Complete (%) | Partial (%) | Lost (%) | Decayed or filled (%) | Total (%) |
| Sealant retention: | Amin 2008 | FUJI II LC (resin‐modified glass ionomer) | 46 | 27 | 27 | = 100 | |
| Amin 2008 | Tetric Flow, Helioseal F (resins, data combined) | 82 | 12.5 | 5.5 | = 100 | ||
| Baseggio 2010 | Vitremer (resin‐modified glass ionomer) | 14 | 33 | 54 | = 101 | ||
| Baseggio 2010 | Fluoroshield (resin) | 94 | 6 | 0 | = 100 | ||
| Bojanini 1976 | Delton (resin) | 91 | 6 | 3 | = 100 | ||
| Charbeneau 1979 | Kerr (resin) | 79 | 17 | 4 | = 100 | ||
| de Luca‐Fraga 2001 | Vitremer (resin‐modified glass ionomer) | 86 | 14 | 0 | = 100 | ||
| de Luca‐Fraga 2001 | Dyract (polyacid‐modified composite resin) | 96 | 2 | 2 | = 100 | ||
| Dhar 2012 | GC Fuji Ionomer VII light pink (glass ionomer‐based sealant), without preparation | 0 | 16 | 84 | = 100 | ||
| Dhar 2012 | Clinpro pink (fluoride releasing resin‐based sealant), without preparation | 24 | 28 | 48 | = 100 | ||
| Erdoğan 1987 | Delton (resin) | 77 | 19 | 4 | = 100 | ||
| Karlzen‐Reuterving 1995 | FUJI III (ionomer) | 72 | 17 | 11 | = 100 | ||
| Karlzen‐Reuterving 1995 | Delton (resin) | 97 | 3 | 0 | = 100 | ||
| Pardi 2005 | Vitremer (resin‐modified glass ionomer) | 77 | 17 | 6 | = 100 | ||
| Pardi 2005 | Revolution (flowable resin composite) | 84 | 14 | 2 | = 100 | ||
| Pardi 2005 | Dyract Flow (compomer) | 76 | 22 | 2 | = 100 | ||
| Reisbick 1982 (14 months) | Oralin (chemically polymerized resin) | 89 | |||||
| Richardson 1978 | resin (the name of the material not stated) | 90 | 6 | 4 | = 100 | ||
| Rock 1978 | Delton (resin) | 53 | 22 | 25 | = 100 | ||
| Rock 1996 | Baseline (ionomer) | 0 | 0 | 96 | 4 | = 100 | |
| Rock 1996 | Fluoroshield (resin) | 76.6 | 9.5 | 13.3 | 1.3 | = 101 | |
| Sheykholeslam 1978 | Delton (resin) | 92 | 5 | 0 | 3 | = 100 | |
| Sipahier 1995 | Ketac‐Silver (glass ionomer‐silver‐cermet cement) | 23 | 34 | 43 | = 100 | ||
| Sipahier 1995 | Delton (resin) | 41 | 48 | 11 | = 100 | ||
| Sealant retention: 24 months | Amin 2008 | FUJI II LC (resin‐modified glass ionomer) | 25 | 21 | 54 | = 100 | |
| Amin 2008 | Tetric Flow, Helioseal F (resins, data combined) | 83 | 9 | 8 | = 100 | ||
| Baseggio 2010 | Vitremer (resin‐modified glass ionomer) | 9 | 12 | 80 | = 101 | ||
| Baseggio 2010 | Fluoroshield (resin) | 94 | 6 | 0 | = 100 | ||
| Bojanini 1976 | Delton (resin) | 89 | 7 | 4 | = 100 | ||
| Brooks 1979 | Delton (resin) | 84 | 10 | 6 | = 100 | ||
| Charbeneau 1979 | Kerr (resin) | 71 | 18 | 11 | = 100 | ||
| Chen 2012 | Ketac Molar Easymix (glass ionomer) | 22 | |||||
| Chen 2012 | Ketac Molar Easymix plus LED high energy curing light (glass ionomer) | 20 | |||||
| Chen 2012 | Clinpro Sealant (fluoride releasing resin‐based sealant) | 14 | |||||
| Dhar 2012 | GC Fuji Ionomer VII light pink (glass ionomer‐based sealant), without preparation | 0 | 0 | 100 | = 100 | ||
| Dhar 2012 | Clinpro pink (fluoride releasing resin‐based sealant), without preparation | 0 | 20 | 80 | = 100 | ||
| Forss 1998 | Fuji III (ionomer) | 26 | 26 | 48 | = 100 | ||
| Forss 1998 | Light‐cured Delton (resin) | 82 | 9 | 9 | = 100 | ||
| Ganesh 2006 | Fuji VII (ionomer) | 2 | 68 | 30 | = 100 | ||
| Ganesh 2006 | Concise (resin) | 4 | 66 | 30 | = 100 | ||
| Güngör 2004 | Dyract Seal (PMRC) | 80 | 16 | 4 | = 100 | ||
| Güngör 2004 | Delton FS+ (resin) | 71 | 16 | 13 | = 100 | ||
| Karlzen‐Reuterving 1995 | FUJI III (ionomer) | 43 | |||||
| Karlzen‐Reuterving 1995 | Delton (resin) | 90 | 10 | 0 | = 100 | ||
| Lampa 2004 | Dyract Seal (PMRC) | 16 | 44 | 40 | = 100 | ||
| Lampa 2004 | Delton DDS (resin) | 66 | 23 | 11 | = 100 | ||
| Liu 2012 | Clinpro Sealant (fluoride releasing resin‐based sealant) | 54 | |||||
| Mills 1993 | Ketac‐Silver (ionomer) | 83 | 12 | 6 | = 101 | ||
| Mills 1993 | Delton (resin) | 58 | 17 | 25 | = 100 | ||
| Pardi 2005 | Vitremer (resin‐modified glass ionomer) | 47 | 37 | 16 | = 100 | ||
| Pardi 2005 | Revolution (flowable resin composite) | 76 | 17 | 7 | = 100 | ||
| Pardi 2005 | Dyract Flow (compomer) | 58 | 28 | 14 | = 100 | ||
| Poulsen 2001 | Fuji III (ionomer) | 9 | 9 | 82 | = 100 | ||
| Poulsen 2001 | Delton (resin) | 80 | 7 | 13 | = 100 | ||
| Reisbick 1982 | Oralin (chemically polymerized resin) | 82 | |||||
| Richardson 1978 | resin (the name of the material not stated) | 86 | 9 | 5 | = 100 | ||
| Rock 1996 | Baseline (ionomer) | 0 | 0 | 88 | 12 | = 100 | |
| Rock 1996 | Fluoroshield (resin) | 70 | 10 | 19 | 1 | = 100 | |
| Sheykholeslam 1978 | Delton (resin) | 85 | 7 | 2 | 6 | = 100 | |
| Songpaisan 1995 | Fuji III (ionomer) | < 1 | |||||
| Songpaisan 1995 | Delton (resin) | 85 | |||||
| Tagliaferro 2011 | (resin‐modified glass ionomer) | 16 | |||||
| Williams 1996 | Fuji III (ionomer) | 4 | 3 | 93 | = 100 | ||
| Williams 1996 | Delton (resin) | 80 | 2 | 18 | = 100 | ||
| Sealant retention: | Baseggio 2010 | Vitremer (resin‐modified glass ionomer) | 5 | 6 | 89 | = 100 | |
| Baseggio 2010 | Fluoroshield (resin) | 91 | 8 | 1 | = 100 | ||
| Beiruti 2006 | Fuji IX (ionomer) | 60 | |||||
| Beiruti 2006 | Visio‐Seal (composite resin) | 60 | |||||
| Bojanini 1976 | Delton (resin) | 87 | 9 | 4 | = 100 | ||
| Brooks 1979 | Delton (resin) | 80 | 10 | 10 | = 100 | ||
| Charbeneau 1979 | Kerr (resin) | 61 | 23 | 16 | = 100 | ||
| Hunter 1988 | Delton (resin) | 64 | 19 | 8 | 9 | = 100 | |
| Karlzen‐Reuterving 1995 | FUJI III (ionomer) | 28 | 35 | 37 | = 100 | ||
| Karlzen‐Reuterving 1995 | Delton (resin) | 79 | 21 | 0 | = 100 | ||
| Poulsen 2001 | Fuji III (ionomer) | 3 | 7 | 89 | = 100 | ||
| Poulsen 2001 | Delton (resin) | 74 | 16 | 10 | = 100 | ||
| Raadal 1996 | Vitrebond (resin‐reinforced glass ionomer) | 5 | 4 | 91 | = 100 | ||
| Raadal 1996 | Concise White Sealant (resin) | 97 | 1.5 | 1.5 | = 100 | ||
| Reisbick 1982 (32 months) | Oralin (chemically polymerized resin) | 78 | |||||
| Richardson 1978 | resin (the name of the material not stated) | 75 | 14 | 11 | = 100 | ||
| Rock 1978 | Delton (resin) | 41 | 16 | 43 | = 100 | ||
| Rock 1996 | Baseline (ionomer) | 0 | 0 | 81.5 | 18.4 | = 100 | |
| Rock 1996 | Fluoroshield (resin) | 70 | 9.2 | 17.7 | 3.2 | = 100 | |
| Sheykholeslam 1978 | Delton (resin) | 77 | 9 | 4 | ? | ||
| Kervanto‐Seppälä 2008 | In total 559 tooth pairs: in 1% ionomer retained, resin lost; in 89% ionomer lost, resin retained; in 6% ionomer retained, resin retained; in 4% ionomer lost, resin lost = 100% | ||||||
| Sealant retention: | Arrow 1995 | In total 465 tooth pairs: in 10% ionomer retained, resin lost; in 18% ionomer lost, resin retained; in 10% ionomer retained, resin retained; in 62% ionomer lost, resin lost = 100% | |||||
| Sealant retention: | Charbeneau 1979 | Kerr (resin) | 52 | 26 | 22 | = 100 | |
| Richardson 1978 | resin (the name of the material not stated) | 69 | 10 | 21 | = 100 | ||
| Williams 1996 | Fuji III (ionomer) | 4 | 2 | 94 | = 100 | ||
| Williams 1996 | Delton (resin) | 61 | 11 | 28 | = 100 | ||
| Sealant retention: | Brooks 1979 | Delton (resin) | 72 | 14 | 14 | = 100 | |
| Erdoğan 1987 | Delton (resin) | 74 | 22 | 4 | = 100 | ||
| Sealant retention: | Barja‐Fidalgo 2009 | Fuji IX (ionomer) | 29 | 29 | 42 | = 100 | |
| Barja‐Fidalgo 2009 | Delton (resin) | 21 | 21 | 58 | = 100 | ||
| Beiruti 2006 | Fuji IX (ionomer) | 88 | |||||
| Beiruti 2006 | Visio‐Seal (composite resin) | 86 | |||||
| Richardson 1978 | resin (the name of the material not stated) | 67 | 10 | 23 | = 100 | ||
| Sealant retention: | Brooks 1979 | Delton (resin) | 68 | 16 | 16 | = 100 | |
| Sealant retention: | Brooks 1979 | Delton (resin) | 66 | 14 | 20 | = 100 | |
| Forss 1998 | In total 97 tooth pairs: in 6% ionomer retained, resin lost; in 41% ionomer lost, resin retained; in 4% ionomer retained, resin retained; in 49% ionomer lost, resin lost = 100% | ||||||
| Sealant retention: | Bravo 2005 | Delton (resin) | 39 |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Caries yes/no at 12 months Show forest plot | 6 | Odds Ratio (Random, 95% CI) | 0.16 [0.08, 0.30] | |
| 1.1 Split‐mouth studies with paired data | 3 | Odds Ratio (Random, 95% CI) | 0.09 [0.06, 0.13] | |
| 1.2 Split‐mouth studies with data stated as marginals | 3 | Odds Ratio (Random, 95% CI) | 0.30 [0.14, 0.66] | |
| 2 Caries yes/no at 24 months Show forest plot | 6 | Odds Ratio (Random, 95% CI) | 0.12 [0.07, 0.19] | |
| 2.1 Split‐mouth studies with paired data | 3 | Odds Ratio (Random, 95% CI) | 0.11 [0.06, 0.22] | |
| 2.2 Split‐mouth studies with data stated as marginals | 2 | Odds Ratio (Random, 95% CI) | 0.09 [0.03, 0.23] | |
| 2.3 Parallel group studies | 1 | Odds Ratio (Random, 95% CI) | 0.32 [0.13, 0.80] | |
| 3 Caries yes/no at 36 months Show forest plot | 7 | Odds Ratio (Random, 95% CI) | 0.17 [0.11, 0.27] | |
| 3.1 Split‐mouth studies with paired data | 3 | Odds Ratio (Random, 95% CI) | 0.16 [0.12, 0.20] | |
| 3.2 Split‐mouth studies with data stated as marginals | 4 | Odds Ratio (Random, 95% CI) | 0.18 [0.07, 0.43] | |
| 4 Caries yes/no at 48‐54 months Show forest plot | 4 | Odds Ratio (Random, 95% CI) | 0.21 [0.16, 0.28] | |
| 4.1 Split‐mouth studies with paired data | 2 | Odds Ratio (Random, 95% CI) | 0.17 [0.13, 0.23] | |
| 4.2 Split‐mouth studies with data stated as marginals | 2 | Odds Ratio (Random, 95% CI) | 0.27 [0.16, 0.47] | |
| 5 Caries yes/no at 48 months, parallel group studies Show forest plot | 1 | Risk Ratio (Fixed, 95% CI) | 0.24 [0.12, 0.45] | |
| 6 12‐13 years ‐ 2‐year DFS increment Show forest plot | 1 | 276 | Mean Difference (IV, Fixed, 95% CI) | ‐0.65 [‐0.83, ‐0.47] |
| 7 Caries yes/no at 5 years Show forest plot | 1 | Odds Ratio (Fixed, 95% CI) | 0.31 [0.23, 0.43] | |
| 8 Caries yes/no at 6 years Show forest plot | 1 | Risk Ratio (Fixed, 95% CI) | 0.45 [0.36, 0.58] | |
| 9 Caries yes/no at 7 years Show forest plot | 1 | Risk Ratio (Fixed, 95% CI) | 0.45 [0.34, 0.59] | |
| 10 Caries yes/no at 9 years, parallel group studies Show forest plot | 1 | Risk Ratio (Fixed, 95% CI) | 0.35 [0.22, 0.55] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 12‐13 years ‐ 2‐year DFS increment Show forest plot | 1 | 404 | Mean Difference (IV, Fixed, 95% CI) | ‐0.18 [‐0.39, 0.03] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Caries yes/no at 12 months Show forest plot | 4 | Odds Ratio (Fixed, 95% CI) | Totals not selected | |
| 1.1 Split‐mouth studies with data stated as marginals | 4 | Odds Ratio (Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Caries yes/no at 24 months Show forest plot | 7 | Odds Ratio (Random, 95% CI) | Totals not selected | |
| 2.1 Split‐mouth studies with paired data | 1 | Odds Ratio (Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Split‐mouth studies with data stated as marginals | 5 | Odds Ratio (Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 Parallel group studies | 1 | Odds Ratio (Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 12‐13 years ‐ 2‐year DFS increment Show forest plot | 1 | 394 | Mean Difference (IV, Fixed, 95% CI) | 0.47 [0.31, 0.63] |
| 4 Caries yes/no at 36‐48 months Show forest plot | 6 | Odds Ratio (Random, 95% CI) | Totals not selected | |
| 4.1 Split‐mouth studies with paired data | 3 | Odds Ratio (Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Split‐mouth studies with data stated as marginals | 3 | Odds Ratio (Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Caries yes/no at 5 years, parallel group studies Show forest plot | 2 | Risk Ratio (Fixed, 95% CI) | 0.30 [0.15, 0.59] | |
| 6 Caries yes/no at 7 years Show forest plot | 1 | Risk Ratio (Fixed, 95% CI) | 1.44 [0.88, 2.35] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Caries yes/no at 12 months Show forest plot | 1 | Odds Ratio (Fixed, 95% CI) | 1.0 [0.02, 47.80] | |
| 2 Caries yes/no at 12 months, parallel group studies Show forest plot | 1 | 41 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.09, 13.15] |
| 3 Caries yes/no at 24 months Show forest plot | 1 | Odds Ratio (Fixed, 95% CI) | 3.03 [1.82, 5.05] | |
| 4 Caries yes/no at 24 months, parallel group studies Show forest plot | 1 | 39 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.09, 13.89] |
| 5 Caries yes/no at 36 months Show forest plot | 2 | Odds Ratio (Fixed, 95% CI) | 2.66 [1.92, 3.68] | |
| 5.1 Split‐mouth studies with data stated as marginals | 2 | Odds Ratio (Fixed, 95% CI) | 2.66 [1.92, 3.68] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Caries yes/no at 24 months Show forest plot | 2 | Odds ratio (Fixed, 95% CI) | 0.65 [0.29, 1.48] | |