Intervenções para prevenir e tratar dor pélvica e lombar na gravidez
Resumo
Introdução
Mais de dois terços das grávidas apresentam lombalgia, e quase um quinto delas apresenta dor pélvica. A dor aumenta com o avançar da gravidez e interfere no trabalho, nas atividades diárias e na qualidade do sono.
Objetivos
Avaliar os efeitos das intervenções para prevenir e tratar a dor pélvica e lombar na gravidez.
Métodos de busca
Nós pesquisamos o Cochrane Pregnancy and Childbirth Group's Trials Register (18 de julho de 2012), identificamos estudos e revisões relacionados a partir da estratégia de busca do Cochrane Back Review Group até julho de 2012 e examinamos as referências dos estudos e revisões em busca de outros estudos de interesse.
Critério de seleção
Incluímos ensaios clínicos randomizados (ECR) que avaliaram qualquer tratamento para prevenção e redução da incidência ou da gravidade da dor pélvica ou lombar durante a gravidez.
Coleta dos dados e análises
Dois revisores independentes avaliaram o risco de viés e extraíram os dados dos estudos. A qualidade das evidências dos desfechos foi avaliada através dos cinco critérios definidos pelo GRADE Working Group.
Principais resultados
Nesta atualização, nós incluímos 26 estudos com 4.093 grávidas. Onze estudos avaliaram lombalgia (n = 1312), quatro eram sobre dor pélvica (n = 661) e onze avaliaram dor lombar e pélvica (n = 2120). O diagnóstico era feito de forma variável, desde queixas auto‐referidas até com testes específicos. Todas as intervenções eram feitas em combinação com os cuidados habituais de pré‐natal, a não ser quando especificado, e foram comparadas com os cuidados habituais do pré‐natal.
As evidências para dor lombar foram em geral de baixa qualidade. Os exercícios reduziram significativamente a dor (diferença média padrão, SMD, de ‐0,80; intervalo de confiança de 95%, 95% CI, de ‐1,07 a ‐0,53; 6 ECR; n = 543), e a incapacidade física (SMD ‐0,56; 95% CI ‐0,89 a ‐0,,23; dois ECR, n = 146). A hidroginástica reduziu significativamente as licenças relacionadas à dor lombar (risco relativo, RR, 0,40; 95% CI 0,17 a 0,92; um ECR, n = 241).Evidência de baixa qualidade, proveniente de ECR isolados, sugere não haver diferença significativa na dor ou na função física entre dois tipos de cinta de suporte, entre manipulação osteopática (OMT) e cuidados de rotina ou ultrassom simulado (sham US). Evidências de muito baixa qualidade sugerem que um tipo de travesseiro especialmente desenhado pode reduzir mais a dor noturna do que o travesseiro habitual.
Para dor pélvica, evidências de moderada qualidade sugerem que a acupuntura é melhor que o exercício na redução da dor noturna, e ambas as práticas foram melhores que o cuidado médico habitual. Evidência de baixa qualidade proveniente de ECR isolados sugere que a associação de cinta abdominal rígida ao exercício melhorou o nível médio de dor, mas não a função; que a acupuntura foi significativamente melhor que a simulação de acupuntura na melhora da dor noturna e na função física, mas não no nível médio de dor, e que o alívio da dor foi semelhante tanto com a acupuntura profunda quanto com a superficial.
Para dor lombopélvica, evidências de moderada qualidade indicam que um programa de exercícios de 8 a 20 semanas reduziu o risco de as mulheres reclamarem de dor lombopélvica (RR 0,85; 95% CI 0,73 a 1,00; quatro ECR, n = 1.344); mas que um programa de 16 a 20 semanas não foi melhor do que o cuidado médico habitual na prevenção da dor pélvica (um ECR, n = 257).Evidências de baixa qualidade sugeriram que os exercícios reduziram significativamente a licença relacionada à dor lombopélvica (RR 0,76; 95% CI 0,62 to 0,94, dois ECR, n = 1.062), e melhoraram a função física. Estudos de baixa qualidade sugeriram que a manipulação osteopática reduziu significativamente a dor e melhorou a função física; tanto a intervenção multimodal (MOM), que inclui massagem manual, exercício e educação, ou o cuidado médico habitual reduziram a disfunção, mas somente a manipulação multimodal melhorou a dor e função física; a acupuntura melhorou a dor e a função física mais que o cuidado habitual ou a fisioterapia; a melhora da dor e da função física foi maior quando se iniciou a acupuntura a partir da 26ª semana de gestação do que na 20ª semana; a acupuntura auricular melhorou significativamente os desfechos estudados em relação à simulação de acupuntura.
Os efeitos colaterais, quando relatados, foram mínimos e passageiros.
Conclusão dos autores
Evidências de moderada qualidade sugeriram que tanto acupuntura quanto o exercício físico, adaptado à fase da gravidez, reduziram significativamente a dor pélvica noturna e a dor lombopélvica em relação ao cuidado médico habitual isolado; a acupuntura foi significantemente mais efetiva do que exercícios físicos para a redução da dor pélvica noturna, e um programa de exercícios de 16 a 20 semanas não obteve mais sucesso do que os cuidados do pré‐natal habituais na prevenção da dor pélvica ou lombalgia.Evidências de baixa qualidade sugerem que o exercício físico reduziu significativamente a dor e a incapacidade física provocada pela lombalgia.
Para os outros desfechos, há evidências de baixa qualidade, devido ao alto risco de viés e à escassez de dados. Devido à heterogeneidade clínica, não foi possível combinar os dados. Não podemos descartar a possibilidade de vieses de publicação e de seleção.
A fisioterapia, a manipulação osteopática, a acupuntura, a intervenção multimodal ou o uso de cinta pélvica rígida pareceram aliviar a dor pélvica lombar mais do que somente o cuidado médico habitual. A acupuntura foi mais efetiva do que a fisioterapia no alívio da dor lombopélvica noturna e da incapacidade e melhorou a dor e função física quando iniciada na 26a semana de gestação, e não na 20a semana, embora os efeitos tenham sido pequenos.
Não houve diferença significativa na dor lombopélvica e função física com o uso de diferentes tipos de cinta, exercícios, técnicas neuroemocionais ou de manipulação espinhal (SMT), ou para dor noturna pélvica comparando acupuntura profunda ou superficial.
Evidência de muito baixa qualidade sugeriu que um travesseiro especialmente projetado pode reduzir a dor lombar noturna.
É provável que estudos adicionais tenham importante impacto em nossa confiança na avaliação dos efeitos, e é provável que as estimativas sejam alteradas. Pesquisas futuras se beneficiariam da introdução de um sistema de classificação consensual das mulheres de acordo com os sintomas apresentados.
PICO
Resumo para leigos
Intervenções para prevenir e tratar a dor pélvica ou lombar na gravidez
Muitas mulheres apresentam lombalgia ou dor pélvica durante a gravidez. A dor geralmente aumenta conforme a gravidez avança e pode atrapalhar o trabalho, as atividades diárias e afetar o sono.
Nós incluímos 26 estudos com 4.093 grávidas. Onze estudos avaliaram lombalgia (n = 1312), quatro examinaram dor pélvica (n = 661) e onze examinaram ambas as condições associadas (n = 2.120). A menos que anotado de forma diferente, as intervenções foram sempre adicionadas aos cuidados habituais de pré‐natal e comparadas aos cuidados habituais.
Evidências de moderada qualidade mostraram que a acupuntura ou o exercício físico, adaptado à fase da gravidez, reduziram significativamente a dor noturna pélvica ou a dor lombopélvica. A acupuntura foi significantemente mais efetiva do que o exercício para a redução da dor pélvica noturna. Um programa de exercícios de 16 a 20 semanas não foi mais efetivo do que os cuidados do pré‐natal habituais na prevenção da dor pélvica ou lombalgia. Evidências de baixa qualidade sugeriram que o exercício físico reduziu a dor e a incapacidade física provocada pela lombalgia. Os efeitos colaterais, quando relatados, foram mínimos e passageiros. É provável que estudos adicionais alterem a avaliação dos efeitos das intervenções. É tempo de se criar um sistema para categorizar os sintomas de dor das gestantes.
Evidências de baixa qualidadesugerem que o exercício reduz significativamente a dor lombar (seis estudos)e a incapacidade (dois estudos). Estudos isolados mostraram que a hidroginástica reduziu significativamente a licença médica devido à dor lombar; porém não houve diferença para a dor e a função física quando se usou cinta de suporte pélvico ou terapia com manipulação osteopática comparadas com cuidado habitual ou simulação de ultrassom. Evidências de muito baixa qualidade sugeriram que um travesseiro especialmente projetado pode melhorar a dor noturna mais do que o travesseiro comum.
Para dor pélvica, evidências de moderada qualidadesugerem que a acupuntura foi melhor que os exercícios na redução da dor noturnae ambas as práticas foram melhores que o cuidado médico habitual (um ensaio clínico randomizado, ECR). Estudos isolados sugeriram que: a associação de cinta abdominal rígida com exercício melhorou a dor média, mas não a função, a acupuntura foi melhor que simulação de acupuntura na melhora da dor noturna e na função física, mas não na média da dor. Não houve diferença na dor noturna após a acupuntura profunda ou superficial.
Para dor lombopélvica: Evidências de qualidade moderada mostraram que um programa de exercícios de 8 a 20 semanas reduziu o risco para a dor lombopélvica, mas que um programa de 16 a 20 semanas não foi melhor do que o cuidado médico habitual na prevenção da dor (quatro ECR). Com base em estudos isolados: o exercício reduziu significativamente a licença relacionada à dor lombopélvica e melhorou a função física; a manipulação osteopática melhorou significativamente a dor e a função física; a combinação de terapia manual, exercício e educação melhorou a dor e a função física; a acupuntura melhorou os desfechos mais que o cuidado habitual ou a fisioterapia; a acupuntura iniciada na 26a semana de gestação melhorou a dor e a função mais do que quando iniciada com 20 semanas. A acupuntura auricular melhorou significativamente os desfechos estudados em relação à acupuntura simulada.
Authors' conclusions
Summary of findings
| Low‐back pain: any exercises + usual prenatal care versus usual prenatal care for treating back pain in pregnancy | ||||||
| Patient or population: pregnant women with back pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Low‐back pain: any exercises + usual prenatal care versus usual prenatal care | |||||
| Pain intensity measured by a number of different measurements; lower score = better | The mean pain intensity in the control groups was18.75 | The mean pain intensity in the intervention groups was | SMD ‐0.80 (‐1.07, ‐0.53) | 543 | ⊕⊕⊝⊝ | |
| Disability measured by Roland Morris Disability Questionnaire and Oswestry Disability Index | The mean disability in the control groups was 26.6 | The mean disability in the intervention groups was | SMD ‐0.56 (‐0.89 to ‐0.23) | 146 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 poor or no description of randomisation process, allocation concealment, blinding of research personnel | ||||||
| Low‐back pain: water gymnastics + usual prenatal care versus usual prenatal care for treating back pain in pregnancy | ||||||
| Patient or population: pregnant women with back pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control (usual care) | water gymnastics | |||||
| Number of women taking sick leave because of back pain after 32 weeks' gestation | Study population | RR 0.4 | 241 | ⊕⊕⊝⊝ | ||
| 144 per 1000 | 58 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 unclear methods of randomisation; research personnel not blinded | ||||||
| Low‐back pain: support belts for preventing and treating pelvic and back pain in pregnancy | ||||||
| Patient or population: pregnant women with back pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Low‐back pain: support belts | |||||
| BellyBra versus Tubigrip ‐ Low‐back Pain | The mean Bellybra versus Tubigrip back pain in the control group was 4.7, measured on VAS 0 to 10 | The mean Bellybra versus Tubigrip ‐ back pain in the intervention group was 0.2 lower (1.19 lower to 0.79 higher) | MD ‐0.20 (95% CI ‐1.19 to 0.79) | 94 | ⊕⊕⊝⊝ | |
| BellyBra versus Tubigrip ‐ ADL | The mean Bellybra versus Tubigrip ability to perform activities of daily living in the control group was 5.6, measured as a total of several activities | The mean Bellybra versus Tubigrip ability to perform activities of daily living in the intervention group was 0.9 lower | MD ‐0.90 (95% CI ‐1.81 to 0.01) | 94 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 no blinding of research personnel described; no explanation provided for lost‐to‐follow‐up data; different co‐interventions and compliance between groups | ||||||
| Pelvic pain: deep versus superficial acupuncture for preventing and treating pelvic and back pain in pregnancy | ||||||
| Patient or population: pregnant women with pelvic pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control (superficial) | Intervention (deep) | |||||
| evening pain, reported as better, based on women's report on Visual Analogue Scale | Study population | RR 1.06 | 47 | ⊕⊕⊝⊝ | ||
| 682 per 1000 | 723 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 randomisation process and attrition rate/explanations not described | ||||||
| Pelvic + low‐back pain: any exercises + usual prenatal care versus usual prenatal care for preventing and treating pelvic and back pain in pregnancy | ||||||
| Patient or population: pregnant women with, or at risk of developing, pelvic and back pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control (usual prenatal care) | Any exercises + usual prenatal care | |||||
| Number of women who reported pain on Visual Analogue Scale | Study population | RR 0.85 | 1344 | ⊕⊕⊕⊝ | ||
| 747 per 1000 | 635 per 1000 | |||||
| Number of women who reported LBP/PGP‐related sick leave | Study population | RR 0.76 | 1062 (2 studies) | ⊕⊕⊕⊝ | ||
| 288 per 1000 | 219 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 there was a mix of potential biases among the four studies: no allocation concealment (1); no blinding of research personnel (all); poor/no description of drop‐outs, co‐interventions and baseline inequality (mixed) | ||||||
| Pelvic + low‐back pain: acupuncture + usual prenatal care versus usual prenatal care for preventing and treating pelvic and back pain in pregnancy | ||||||
| Patient or population: pregnant women with, or at risk of developing, pelvic and back pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Pelvic + low‐back pain: acupuncture + usual prenatal care versus usual prenatal care | |||||
| Number of women who reported decreased pain | Study population | RR 4.16 | 72 | ⊕⊕⊝⊝ | ||
| 143 per 1000 | 594 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 no blinding of research personnel, over 20% attrition, different co‐interventions | ||||||
| Pelvic + low‐back pain: acupuncture + usual prenatal care versus individualised physio + usual prenatal care for preventing and treating pelvic and back pain in pregnancy | ||||||
| Patient or population: pregnant women with, or at risk of developing, pelvic and back pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control (individualised physio + usual prenatal care) | acupuncture + usual prenatal care | |||||
| Numbers of women rating treatment as good or excellent | Study population | RR 1.24 | 46 | ⊕⊕⊝⊝ | ||
| 778 per 1000 | 964 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 no description of randomisation process, no blinding of research personnel described, uneven attrition (12 dropped out of physio group, while none dropped out of the acupuncture group) and co‐interventions between groups | ||||||
Background
Description of the condition
Back and pelvic pain are common in pregnancy and tend to increase as pregnancy advances; in some cases the pain radiates into the buttock and leg. However, much still remains unclear about these very distinct but related conditions (Vermani 2010; Vleeming 2008). For many women, pain can become so severe that it interferes with ordinary daily activities, disturbs sleep and contributes to high levels of sick leave (Kalus 2007; Mogren 2006; Skaggs 2007). Global prevalence is reported to range from 24% to 90%, in part, because there is currently no universally recognised classification system for the condition (Vermani 2010; Vleeming 2008). A recent prospective study of 325 pregnant women from the Middle East found that almost two‐thirds reported low‐back pain (LBP), pelvic pain or both, during their current pregnancy (Mousavi 2007), with similar proportions reported by a sample of pregnant women (N = 599) in the United States (Skaggs 2007). Relapse rates are high in subsequent pregnancies (Mogren 2005; Skaggs 2007), and a postpartum prevalence of 24.7% (range 0.6% to 67%) (Wu 2004) underlines the importance of developing effective treatment programmes for this condition. Despite these figures, it is estimated that over 50% of women receive little or no intervention from healthcare providers (Greenwood 2001; Skaggs 2007). These numbers suggest that more studies are needed to establish the underlying aetiology and pathogenesis of the conditions (Mørkved 2007). Current theories include: altered posture with the increased lumbar lordosis (exaggerated curvature of the lower spine) necessary to balance the increasing anterior weight of the womb, and inefficient neuromuscular control (Vleeming 2008). Several risk factors have also been identified including increased weight during pregnancy, previous history of LBP and low job satisfaction (Albert 2006; Vleeming 2008).
Whilst back and pelvic pain may occur together in pregnancy, pelvic pain (posterior pain arising from the region of the sacroiliac joints, anterior pain from the pubic symphysis, or both) can often occur on its own, along with residual symptoms postpartum. A follow‐up to a cohort study of 870 pregnant women with pelvic pain found that 10% still experienced moderate or severe pain 18 months after delivery, and were seriously hindered in more than one activity (Rost 2006). Estimates of the prevalence of pregnancy‐related pelvic pain vary (depending on the type of study, diagnostic criteria and precision of identifying the pain), however, the best evidence suggests a point prevalence of 20% (Vleeming 2008). Van de Pol 2007 also reported that, whilst prognosis was generally good, those women reporting pelvic pain were less mobile than those reporting back pain only, and experienced more co‐morbidity and depressive symptoms; these findings are supported by a recent review (Vermani 2010). The need for a uniform terminology in order to promote research and management of these conditions is widely recognised. There are a number of tests validated for distinguishing low‐back from pelvic pain; Vermani 2010 and Vleeming 2008 provide details of these tests.
Description of the intervention
European guidelines recommend that low‐back (Airaksinen 2006) and pelvic pain (Vleeming 2008), are managed by providing adequate information and reassurance to the patient, encouraging her to stay active, continue normal daily activities and work if possible, and by offering individualised exercises where appropriate. Similarly, pre‐natal practitioners in the United Kingdom and Nordic countries give women information on how to manage LBP, pelvic pain or both during their pregnancy and may refer them to physiotherapy for a more specific treatment programme. In the United States, women are taught that LBP is a normal part of pregnancy. Interventions that have been used to date to help manage the pain include exercises, frequent rest, hot and cold compresses, an abdominal support belt, massage, acupuncture, chiropractic, aromatherapy, relaxation, herbs, yoga, Reiki and acetaminophen (Vermani 2010).
For this review, we conducted a broad search for studies that assessed the effects of any intervention that prevented or treated back pain, pelvic pain, or a combination for women in any stage of their pregnancy. We identified studies investigating the effects of: exercise (land‐ or water‐based), pelvic belts, osteopathic manipulation (OMT), spinal manipulation (SMT) and neuro emotional techniques, a special pillow, acupuncture, acupuncture plus exercises, and a multi‐modal approach incorporating manual therapy, exercise and education.
How the intervention might work
Exercise (land‐ or water‐based)
Exercise therapy is a management strategy that is supervised or 'prescribed' and encompasses a group of interventions ranging from general physical fitness or aerobic exercise, to muscle strengthening, various types of flexibility and stretching exercises (Cochrane Back Review Group). Regular exercise can have both physical and psychological benefits, depending on the content of each programme, and the individual’s adherence (ACSM 2006). The exercises recommended for pregnancy‐related LBP are similar to those used for non‐specific LBP, with minor modifications, and are thought to have a similar mechanism of action (Vermani 2010).
Manual therapy (SMT and OMT)
Spinal manipulation (SMT) is defined as a high velocity thrust to a joint beyond its restricted range of movement. Spinal mobilisation involves low‐velocity, passive movements within or at the limit of joint range (Cochrane Back Review Group). Most studies do not make a clear distinction between these two, because in clinical practice, these two techniques are part of a 'manual therapy package', that may also include soft tissue/myofascial release. Manual therapy is thought to influence the spinal ‘gating’ mechanism and the descending pain suppression system at spinal and supraspinal levels to decrease pain. In addition, it is thought to return a vertebra to its normal position or restore lost mobility (Maigne 2003).
Osteopathic manipulation (OMT) is a hands‐on, whole body approach to diagnose, treat, and prevent illness or injury, during which the osteopathic physician moves muscles and joints using techniques including stretching, gentle pressure and resistance (American Osteopathic Association).
Acupuncture, alone or with exercises
Acupuncture is needle puncture at classical meridian points, aimed at promoting the flow of ‘Qi’ or energy. The acupuncturist must avoid certain acupuncture points in pregnancy that supply the cervix and uterus (which have been used to induce labour), but the technique in general is considered to be safe (Moffatt 2013; Vermani 2010). Needles may be stimulated manually or electrically. Acupuncture is thought to stimulate the body’s own pain relieving opioid mechanisms (Lin 2008). Placebo or sham acupuncture is needling of traditionally unimportant sites, superficial insertion or non‐stimulation of the needles once placed. There is some evidence that sham acupuncture may produce similar results to real acupuncture, raising the possibility that the effect of acupuncture may be a result of the stimulation of pressure receptors, regardless of their location (Field 2008).
Multi‐modal approach, including manual therapy, exercise and education
A combination of aspects of manual therapy and exercise, along with education that includes information about correct posture, relaxation techniques (Vermani 2010), instructions to keep the knees together and bent when turning in bed, and to avoid activities such as jarring, bouncing and stretching joints to their extreme (Lile 2003; Mens 2009).
Pelvic belts and pillows
Pelvic belts are a form of lumbar support that can help to: (1) correct deformity; (2) limit spinal motion; (3) stabilise the lumbar spine; (4) reduce mechanical loading; and (5) provide miscellaneous effects such as massage, heat or placebo. They may be made of flexible or rigid materials (Cochrane Back Review Group). Mens 2006 suggests that pelvic belts may stimulate the action of the corset muscle around the tummy and stabilising muscle of the spine along with the pelvic floor muscles.
Pillows are used to provide support and reduce mechanical loading of symptomatic joints in women with pregnancy‐related pelvic and/or back pain.
Why it is important to do this review
Given the number of new studies investigating the effectiveness of interventions for preventing and managing back and pelvic pain in pregnancy and the change in methodological standards for Cochrane reviews, it seemed prudent to update this review again.
Objectives
To assess the effects of interventions for preventing and treating pelvic and back pain in pregnancy.
Methods
Criteria for considering studies for this review
Types of studies
Any randomised controlled trials that evaluated any intervention for preventing or treating pelvic and back pain in pregnancy. We excluded quasi‐randomised trials (those which use techniques for allocating participants to groups that may be prone to bias).
Types of participants
Trials that included pregnant women at any point in their pregnancy who were at risk of developing, or suffering from pelvic or back pain, as reported symptomatically by the women or diagnosed by clinicians using specific diagnostic tests.
Types of interventions
Trials that examined any intervention intended to reduce the incidence or severity of pelvic and back pain in pregnancy. We did not put parameters on the types of interventions. We grouped the trials to allow us to examine interventions that specifically addressed back pain, pelvic pain or the two in combination. Under each population, we grouped the interventions under exercise, manual therapy, acupuncture, multi‐modal approach, pelvic belts and pillows, depending on the trials identified. Interventions were compared to usual prenatal care (in some trials referred to as 'no treatment'), or usual prenatal care plus another intervention.
Types of outcome measures
We excluded studies that diagnosed back or pelvic pain, identified back or pelvic pain as intermediate or proxy outcomes only, started interventions prior to pregnancy but measured the back or pelvic pain during pregnancy, or started the trial during pregnancy when their goal was to assess postpartum outcomes and therefore the only measurements conducted during pregnancy were baseline values.
Primary outcomes
Women’s own rating of usefulness of a treatment, reduction of symptoms, participation in usual activities and adverse effects (reported by women and assessors) measured at the end of treatment, during pregnancy.
-
Pain intensity (pain levels);
-
activities of daily living;
-
days off work; or
-
adverse effects for women and infants; as defined by trialist.
Search methods for identification of studies
Electronic searches
We searched the Cochrane Pregnancy and Childbirth Group’s Trials Register by contacting the Trials Search Co‐ordinator (18 July 2012).
The Cochrane Pregnancy and Childbirth Group’s Trials Register is maintained by the Trials Search Co‐ordinator and contains trials identified from:
-
monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL);
-
weekly searches of MEDLINE;
-
weekly searches of Embase;
-
handsearches of 30 journals and the proceedings of major conferences;
-
weekly current awareness alerts for a further 44 journals plus monthly BioMed Central email alerts.
Details of the search strategies for CENTRAL, MEDLINE and Embase, the list of handsearched journals and conference proceedings, and the list of journals reviewed via the current awareness service can be found in the ‘Specialized Register’ section within the editorial information about the Cochrane Pregnancy and Childbirth Group.
Trials identified through the searching activities described above are each assigned to a review topic (or topics). The Trials Search Co‐ordinator searches the register for each review using the topic list rather than keywords.
We also identified potential trials by searching the Trials Register of the Cochrane Back Review Group (CBRG) by contacting the Trials Search Co‐ordinator, most recently in July 2012 and by following up on trials that were listed as 'ongoing' in prior literature searches. The CBRG Trials Register is populated by the results of monthly electronic database searches (MEDLINE, Embase, CINAHL, PsycInfo, Index to Chiropractic Literature), by handsearching selected journals and conference proceedings, by quarterly searches of CENTRAL and international healthcare guideline sources and by the results of specific searches and reference checks of included studies for individual reviews (Cochrane Back Review Group). Regular searches for ongoing trials of back and neck pain treatments are conducted in the U.S National Institute of Health database of clinical trials, ClinicalTrials.gov, as well as via the World Health Organization’s International Clinical Trials Registry Platform Search Portal.
Searching other resources
We checked the reference lists of included studies and related systematic reviews (Airaksinen 2006; Anderson 2005; Ee 2008 ; Field 2008; Richards 2012; Vermani 2010).
We did not apply any language restrictions.
Data collection and analysis
For the methods used when assessing the studies identified in the previous version of this review (Pennick 2007),seeAppendix 1.
For this update, we used the following methods when assessing the 47 trial reports identified by the updated search to July 2012 (Abolhasani 2010; Bandpei 2010; Beyaz 2011; Chitryniewicz 2010; de Jonge‐Vors 2011; Depledge 2005; Eggen 2012; Ekdahl 2010; Elden 2008; Elden 2008b; Elden 2008c; Field 1999a; Field 2012; Foxcroft 2011; Gil 2011; Gross 2012; Granath 2006; Greene 2009; Hagberg 2007; Hagen 2010; Haugland 2006; Hensel 2008; Kalus 2006; Kalus 2007; Kashanian 2009; Kluge 2011; Kohama 2006; Ladefoged 2012; Lund 2006; Licciardone 2007; Licciardone 2010; Mens 2012; Moholdt 2011; Momoi 1999; Mørkved 2007; Peters 2007; Peterson 2012; Schoenfeld 2011; Singh 2008; Sedaghati 2007; Stafne 2012; Thorell 2012; Torstensson 2009; Wang 2007; Wang 2008; Wang 2009b; Zand 2011.
Selection of studies
The two review authors independently assessed all the potential studies we identified as a result of the search strategy. Based on information from the titles and abstracts, we obtained the full text of any articles that appeared to meet the inclusion criteria, or lacked sufficient information to make a decision. We made all final decisions for inclusion after reading the full‐text of the article, discussing our individual thoughts and reaching consensus when needed. A former review author (Gavin Young) was available if needed for further consultation. Reports that were not in English were assessed for inclusion by colleagues with the appropriate language skills, by using Google Translate (Google Translate) to translate the article into English, or both.
Data extraction and management
We used the data extraction form developed by the Cochrane Pregnancy and Childbirth Group to extract data. For eligible trials, two review authors independently extracted the data, resolving discrepancies through discussion, entered them into Review Manager software (RevMan 2012) and checked for accuracy.
When information regarding any of the above was unclear, we attempted (without success in all but three cases (Eggen 2012; Elden 2005; Stafne 2012) to contact authors of the original reports to provide further details. The trials to which this refers are identified in the notes section of the Characteristics of included studies table.
Assessment of risk of bias in included studies
The two review authors independently assessed the risk of bias for each study using the criteria outlined below and in The Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Again, we shared our findings and resolved disagreement through discussion. We entered our decisions and supporting documentation into the 'Risk of bias' tables.
(1) Random sequence generation (checking for possible selection bias)
For each included trial, we described the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups.
We assessed the method as:
-
low risk of bias (any truly random process, e.g. random number table; computer random number generator);
-
high risk of bias (any non‐random process, e.g. odd or even date of birth; hospital or clinic record number);
-
unclear risk of bias.
(2) Allocation concealment (checking for possible selection bias)
For each included trial, we described the method used to conceal the allocation sequence in sufficient detail to determine whether the intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment.
We assessed the methods as:
-
low risk of bias (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes);
-
high risk of bias (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth);
-
unclear risk of bias.
(3.1) Blinding of participants and personnel (checking for possible performance bias)
For each included trial, we described the methods used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. Trials were judged at low risk of bias if they were blinded, or if we judged that the lack of blinding could not have affected the results. Blinding was assessed separately for different outcomes or classes of outcomes.
We assessed the methods as:
-
low, high or unclear risk of bias for participants;
-
low, high or unclear risk of bias for personnel.
(3.2) Blinding of outcome assessment (checking for possible detection bias)
For each included trial, we described the methods used, if any, to blind outcome assessors from knowledge of which intervention a participant received. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed methods used to blind outcome assessment as:
-
low, high or unclear risk of bias.
(4) Incomplete outcome data (checking for possible attrition bias due to the amount, nature and handling of incomplete outcome data)
For each included trial, and for each outcome or class of outcomes, we described the completeness of data, including attrition and exclusions from the analysis. We stated whether attrition and exclusions were reported and the numbers included in the analysis at each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. Where sufficient information was reported, or supplied by the trial authors, we re‐included missing data in the analyses which we undertook.
We assessed methods as:
-
low risk of bias (e.g. no missing outcome data; missing outcome data balanced across groups and less than 20%);
-
high risk of bias (e.g. numbers or reasons for missing data imbalanced across groups; ‘as treated’ analysis done with substantial departure of intervention received from that assigned at randomisation);
-
unclear risk of bias.
(5) Selective reporting (checking for reporting bias)
For each included trial, we described how we investigated the possibility of selective outcome reporting bias and what we found.
We assessed the methods as:
-
low risk of bias (where it was clear that all of the trial's pre‐specified outcomes and all expected outcomes of interest to the review were reported);
-
high risk of bias (where not all the trial's pre‐specified outcomes were reported; one or more reported primary outcomes were not prespecified; outcomes of interest were reported incompletely and so could not be used; trial failed to include results of a key outcome that would have been expected to have been reported);
-
unclear risk of bias.
(6) Other bias (checking for bias due to problems not covered by (1) to (5) above)
For each included trial, we described any important concerns we had about other possible sources of bias: Were the groups similar at baseline regarding the most important prognostic indicators? Were co‐interventions avoided or similar? Was the compliance acceptable in all groups? Was the timing of the outcome assessment similar in all groups? Other?
We assessed whether each trial was free of other problems that could put it at risk of bias:
-
low risk of other bias;
-
high risk of other bias;
-
unclear whether there is risk of other bias.
(7) Overall risk of bias
We made explicit judgements about whether trials were at high risk of bias, according to the criteria given in the Cochrane Handbook (Higgins 2011). With sufficient data, we would have assessed the likely magnitude and direction of the bias and whether it was likely to have impacted the findings by undertaking sensitivity analyses.
Measures of treatment effect
Dichotomous data
For dichotomous data (e.g. absenteeism, presence of pain, satisfaction with treatment), we present results as summary risk ratios (RR) with 95% confidence intervals (95% CI).
Continuous data
For continuous data (e.g. intensity of pain, disability), we used the mean difference (MD) if outcomes were measured in the same way between trials. We used the standardised mean difference (SMD) to combine trials that measured the same outcome, but used different methods. We presented both summary results with 95% CI.
We used Cohen's three levels to guide our classification of the estimates of effect as small, medium or large (Cohen 1988).
-
Small (MD less than 10% of the scale (e.g. less than 10 mm on a 100 mm visual analogue scale (VAS)); SMD or “d” scores less than 0.5; RR, less than 1.25 or greater than 0.8 (depending on whether it reports risk of benefit or risk of harm)).
-
Medium (MD 10% to 20% of the scale; SMD or “d” scores from 0.5 to less than 0.8; RR between 1.25 to 2.0, or 0.5 to 0.8).
-
Large (MD greater than 20% of the scale; SMD or “d” scores equal to or greater than 0.8; RR greater than 2.0 or less than 0.5).
To determine if an estimate of effect was clinically significant, we were guided by work conducted in low‐back pain research; we considered 30% on VAS/numerical rating scale (NRS) for pain as clinically significant (Ostelo 2008), and two to three points on the Roland‐Morris Disability Questionnaire (RMDQ) or 8% to 12% for function (Bombardier 2001).
Unit of analysis issues
Cross‐over trials
One cross‐over trial met the inclusion criteria in an earlier version of this review. Should we identify further cross‐over trials, we will extract data from the phases of the trial, as parallel trials, and consider the impact of incorporating the data with those of parallel trials.
Dealing with missing data
For included studies, we noted levels of and reasons for attrition. With sufficient data, we would have explored the impact of including studies with high levels of missing data (more than 20%) in the overall assessment of treatment effect by using sensitivity analyses.
For all outcomes, we carried out analyses, as far as possible, on an intention‐to‐treat basis, i.e. we attempted to include all participants randomised to each group in the analyses, and all participants were analysed in the group to which they were allocated, regardless of whether or not they received the allocated intervention. The denominator for each outcome in each study was the number randomised minus any participants whose outcomes were known to be missing.
Assessment of heterogeneity
We only combined the results of studies that we determined were clinically homogeneous for population, intervention, comparison and outcome. We assessed statistical heterogeneity in each meta‐analysis using the Tau², I² and Chi² statistics. We regarded heterogeneity as substantial if the I² was greater than 30% and either the Tau² was greater than zero, or there was a low P value (less than 0.10) in the Chi² test for heterogeneity (Riley 2011).
Assessment of reporting biases
Had there been 10 or more trials in a meta‐analysis, we would have investigated reporting biases (such as publication bias) using funnel plots.
Data synthesis
For trials we considered to be clinically homogeneous, we combined the data using the Review Manager software (RevMan 2012) and a fixed‐effect method. If there was some clinical heterogeneity, but a summary effect was still considered to be clinically meaningful, or if there was substantial statistical heterogeneity, we used random‐effects meta‐analysis. For random‐effects analyses, we presented the results as the average treatment effect with 95% confidence intervals, and the estimates of Tau² and I² statistics.
For all outcomes, we assessed the quality of the body of evidence by using the five criteria outlined by the GRADE Working Group (Schünemann 2009; Appendix 3). When we used RevMan to calculate the estimate of effect, we also created a 'Summary of findings' table to illustrate the results and quality of the evidence. If we either extracted data directly from the papers or data were not provided, we assessed the quality of the evidence with the GRADE criteria and accompanied our results with a brief description of the criteria that contributed to the downgrade (i.e. study design, inconsistency, indirectness, sparse data, publication bias).
Subgroup analysis and investigation of heterogeneity
Had there been sufficient data, we had planned to conduct subgroup and sensitivity analyses to investigate heterogeneity for all primary outcomes.
With sufficient data, we had planned to carry out the following subgroup analyses.
-
Gestational age by trimester.
-
Different techniques and duration of interventions.
-
Number of previous pregnancies.
-
Number of fetuses.
In future updates, with sufficient data, we will carry out subgroup analyses and assess subgroup differences by interaction tests available within RevMan (RevMan 2012). We will report the results of subgroup analyses quoting the Chi² statistic and P value, and the interaction test I² value.
Sensitivity analysis
With sufficient data, we had planned to conduct sensitivity analyses to determine the effects of selection, performance and attrition bias on the estimates of effect, by excluding trials at high risk of bias due to these potential biases from the analyses, in order to assess whether this made any difference to the overall result. In future updates, with sufficient data, we plan to do so.
Results
Description of studies
Results of the search
The review completed in 2002 (Young 2002) contained three trials: two examined interventions for women with low‐back pain (Kihlstrand 1999; Thomas 1989), one examined an intervention for a mixed population with pelvic and low‐back pain (LBP) (Wedenberg 2000). One trial was excluded because it used a quasi‐randomised sequence generation.
The first update of the review (Pennick 2007) included eight trials (1305 women), described in nine publications. Seven were randomised controlled trials, and the eighth used a cross‐over design (Thomas 1989). The literature search, updated to February 6, 2006 had identified 11 potentially relevant reports: five trials, described in six reports, were included: two trials examined women with low‐back pain (Garshasbi 2005; Suputtitada 2002), one examined women with pelvic pain (Elden 2005), and two more examined a mixed population with pelvic and back pain (Kvorning 2004; Martins 2005); two trials were identified as ongoing, and three were excluded because they were quasi‐randomised trials (QRCTs).
The current update includes 26 trials, described in 30 reports. The literature search, updated to July 18, 2012, identified 47 potentially relevant reports from both the Cochrane Pregnancy and Childbirth and the Cochrane Back Review Groups' Trials Registers.
Included studies
We included 18 new randomised trials in this update, reported in 30 publications: five were reported in multiple publications: Eggen 2012; Elden 2008; Kalus 2007; Licciardone 2010; and Wang 2009a; 13 were published in single reports (Bandpei 2010; Depledge 2005; Ekdahl 2010; Gil 2011; Gross 2012; Kashanian 2009; Kluge 2011; Lund 2006; Mørkved 2007; Peters 2007; Peterson 2012; Sedaghati 2007; Stafne 2012); four were ongoing trials (Abolhasani 2010; Greene 2009; Hensel 2008; Moholdt 2011).
This review now includes 26 randomised trials examining 4093 pregnant women. Eleven trials examined LBP (N = 1312; Bandpei 2010; Garshasbi 2005; Gil 2011; Kalus 2007; Kashanian 2009; Kihlstrand 1999; Licciardone 2010; Peterson 2012; Sedaghati 2007; Suputtitada 2002; Thomas 1989); four looked at pelvic pain (N = 661; Depledge 2005; Elden 2005; Elden 2008; Lund 2006); and 11 trials examined women with both LBP and pelvic pain (N = 2120; Eggen 2012; Ekdahl 2010; Gross 2012; Kluge 2011; Kvorning 2004; Martins 2005; Mørkved 2007; Peters 2007; Stafne 2012; Wang 2009a; Wedenberg 2000).
The LBP trials looked at the effects of exercise, on land (Bandpei 2010; Garshasbi 2005; Gil 2011; Kashanian 2009; Sedaghati 2007; Suputtitada 2002), and in water (Kihlstrand 1999), use of pelvic belts (Kalus 2007), osteopathic manipulation (OMT) (Licciardone 2010), spinal manipulation (SMT) and neuro emotional technique Peterson 2012, and use of a special pillow (Thomas 1989). Trials investigating pelvic pain included pelvic belts (Depledge 2005), acupuncture (Elden 2008; Lund 2006), and acupuncture plus exercises (Elden 2005). Women with both LBP and pelvic pain were given exercises (Eggen 2012; Kluge 2011; Martins 2005; Mørkved 2007; Stafne 2012), OMT (Peters 2007), a multi‐modal approach of manual therapy, exercise and education (Gross 2012), and acupuncture (Ekdahl 2010; Kvorning 2004; Wang 2009a; Wedenberg 2000).
The controls used were generally described as 'no treatment', which was usual prenatal care. The more recent acupuncture trials used sham acupuncture as a control (Elden 2008; Wang 2009a), tested the optimal time to start treatment with acupuncture (Ekdahl 2010), examined different acupuncture stimulation modes (Lund 2006), or the relative effectiveness against physiotherapy (Wedenberg 2000). Relative effectiveness was examined between spinal manipulation and neuro emotional technique (Peterson 2012), two types of pelvic belts (Kalus 2007) and pillows (Thomas 1989); sham ultrasound was used as a control against OMT (Licciardone 2010).
All trials looked at treatment; two trials also looked at interventions that may prevent LBP (Sedaghati 2007; Thomas 1989) and two that may prevent lumbo‐pelvic pain (Eggen 2012; Mørkved 2007).
See tables of Characteristics of included studies; Characteristics of ongoing studies for further details.
Excluded studies
The review authors for the original review and the 2007 update excluded four trials after full‐text review because they were QRCTs. For this update, we excluded 17 trials after review of the full‐text: eight were QRCTs or CCTs, one measured postpartum outcomes only, five lacked a clear description of study design or were not parallel studies, two were investigating depression, not LBP, and one included women who were not pregnant at the time of the intervention, but were at the inception of the back pain. See table of Characteristics of excluded studies for further details.
Risk of bias in included studies
Overall, the risks of bias were high, raising concerns about the confidence we could put in the estimates of effect. See Figure 1 for a summary of these risks of bias in each trial; see the 'Risk of bias' tables in the Characteristics of included studies for details.

'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Of the 26 reports, only 13 of them adequately reported on the method of randomisation, although all but one were identified as 'randomised controlled trials'; 14 adequately reported on an appropriate method of allocation concealment.
Blinding
Blinding is very difficult to carry out in non‐pharmacological trials, especially when symptoms are the outcomes of interest; nonetheless, lack of blinding of research personnel and participants still has the potential to introduce bias. Four trials reported that the providers and the participants were blinded, while six reported that the outcome assessors were blinded. Of these, only one reduced the bias for blinding by asking all participants if they felt the treatment they had received was credible (Wang 2009a).
Incomplete outcome data
Eleven trials reported that the women were analysed in the groups to which they were randomised; most of the trials only analysed data from those who completed trials, although two (Licciardone 2010; Peterson 2012) imputed missing data in order to present a full data set. Attrition rates ranged from zero to more than 20%. In seven of the trial reports, it was difficult to determine the exact numbers randomised and withdrawn, reasons for the withdrawal and the group membership of those who withdrew. Eleven of the more recent publications included a CONSORT flow chart that traced the enrolment, randomisation, follow‐up and analysis of participants (Schulz 2010).
Selective reporting
We did not specifically search for protocols to determine what outcomes had been planned, however, five studies were identified from study registration databases during the most recent literature search update (Eggen 2012; Elden 2008; Kalus 2007; Licciardone 2010; Wang 2009a). Seventeen trials provided data on the outcomes they had identified in the description of the methods in either the publication or the study registration report, in a form that enabled us to include them in analyses; for one trial, we calculated the end of treatment score and standard deviation using the RevMan calculator to enable us to include the data (Bandpei 2010).
Other potential sources of bias
Six trials were either dissimilar at baseline in important prognostic characteristics (Gil 2011; Martins 2005; Peterson 2012; Wedenberg 2000), reported very different co‐interventions between the groups, or reported co‐interventions that would make it difficult to determine the real effect of the intervention (Gil 2011; Kalus 2007; Kvorning 2004; Martins 2005; Wedenberg 2000). Seven trials provided insufficient information on baseline equality between groups or similarity of co‐interventions to allow us to determine if they were at risk for these biases: three trials were either abstracts or short communications, for which we were unable to obtain the full reports (Gross 2012; Kashanian 2009; Peters 2007), while four more full reports failed to include sufficient details (Mørkved 2007; Sedaghati 2007; Suputtitada 2002; Thomas 1989).
One trial used a cross‐over design in which all participants were analysed at the end of each treatment, without allowing for either a wash‐out period, or at an advanced stage of pregnancy and increased risk of back pain. The data were presented as summaries for each treatment rather than comparing the groups at the end of each phase. We did not include these data in our analyses.
Effects of interventions
See: Summary of findings for the main comparison Low‐back pain: any exercises + usual prenatal care versus usual prenatal care for treating back pain in pregnancy; Summary of findings 2 Low‐back pain: water gymnastics + usual prenatal care versus usual prenatal care for treating back pain in pregnancy; Summary of findings 3 Low‐back pain: support belts for treating back pain in pregnancy; Summary of findings 4 Pelvic pain: deep versus superficial acupuncture for treating pelvic pain in pregnancy; Summary of findings 5 Pelvic + low‐back pain: any exercises + usual prenatal care versus usual prenatal care for preventing and treating pelvic and back pain in pregnancy; Summary of findings 6 Pelvic + low‐back pain: acupuncture + usual prenatal care versus usual prenatal care for preventing and treating pelvic and back pain in pregnancy; Summary of findings 7 Pelvic + low‐back pain: acupuncture + usual prenatal care versus individualised physio + usual prenatal care for preventing and treating pelvic and back pain in pregnancy
Low‐back pain (LBP)
This review now includes 11 trials that examined women with pregnancy‐related LBP (N = 1312 randomised). Seven trials investigated the effects of exercise, either on land (N = 627 randomised; Bandpei 2010; Garshasbi 2005; Gil 2011; Kashanian 2009; Sedaghati 2007; Suputtitada 2002), or in water (N = 258 randomised; Kihlstrand 1999), one trial studied the effects of spinal manipulation (SMT) and neuro emotional technique (N = 57 randomised; Peterson 2012), and one the use of a special pillow to relieve pregnancy‐related low‐back pain (N = 109 randomised; Thomas 1989). The land‐ and water‐based exercises were added to usual prenatal care and compared to prenatal care alone; Kalus 2007 (N = 115 randomised) compared the effects of the BellyBra against those of Tubigrip; Licciardone 2010 (N = 146 randomised) added osteopathic manipulation (OMT) to usual prenatal care and compared it with sham ultrasound (sham US) added to usual prenatal care and usual care by itself.
Exercise (land‐ or water‐based)
There was low‐quality evidence from six trials (543 women analysed; Bandpei 2010; Garshasbi 2005; Gil 2011; Kashanian 2009; Sedaghati 2007; Suputtitada 2002) that exercise ‐ in general ‐ added to usual prenatal care significantly reduced pain (standardised mean difference (SMD) ‐0.80; 95% confidence interval (CI) ‐1.07 to ‐0.53; Tau² = 0.05; I² = 50% Analysis 1.1) and disability (SMD ‐0.56; 95% CI ‐0.89 to ‐0.23;Tau² = 0.00; I² = 0%; Analysis 1.2; two trials,146 women analysed; Bandpei 2010; Gil 2011; summary of findings Table for the main comparison) more than usual prenatal care by itself. All of the trials reported effects in the same direction, so the intervention seemed to reduce pain and disability, but there is considerable uncertainty about the size of the effect, due to concern about the accuracy of reporting in Gil 2011 and Suputtitada 2002. See further details in the Discussion. None of the interventions, gestational ages or outcomes was sufficiently similar, nor were sufficient data provided to allow us to perform a meta‐analysis to determine the estimate of effect of any specific exercise for a specific group of pregnant women.
There was low‐quality evidence from one trial that water‐based exercises added to usual prenatal care reduced LBP‐related sick leave more than usual prenatal care by itself. In Kihlstrand 1999 (N = 241 analysed), women were 40% less likely to take sick leave due to their LBP at 32‐weeks' gestation (risk ratio (RR) 0.40; 95% CI 0.17 to 0.92; Analysis 2.1; summary of findings Table 2). Low‐back pain was not measured until one week postpartum, which is outside the timelines of this review.
Manual therapy
There was low‐quality evidence (study design limitations, sparse data) from one trial (Licciardone 2010, N = 144 analysed) that there was no significant difference in pain relief between usual prenatal care plus OMT and usual prenatal care alone (effect size 0.27; 95% CI ‐0.13 to 0.68), while back‐related function deteriorated significantly less in the usual care plus OMT group (effect size 0.72; 95% CI 0.13 to 1.14). There was also low‐quality evidence suggesting that usual care plus OMT did not significantly reduce pain (effect size 0.14. 95% CI ‐0.26 to 0.55) or improve back‐related function (effect size 0.35, 95% CI ‐0.06 to 0.76) any more than usual care plus sham US. All results were extracted directly from the paper.
There was low‐quality evidence (study design limitations, sparse data) from one trial (Peterson 2012, N = 50 analysed) that while the majority of women in each of the groups (exercise, neuro emotional technique and SMT) improved in function and pain, there was no statistically significant difference between the groups. All results were extracted directly from the paper.
Pelvic belts and pillows
There was low‐quality evidence from one trial (Kalus 2007; N = 94 analysed) that there was no significant difference between the BellyBra's and the Tubigrip's ability to relieve pain (mean difference (MD) ‐0.20; 95% CI ‐1.19 to 0.79) or to increase the women's ability to perform activities of daily living (MD ‐0.90; 95% CI ‐1.81 to 0.01; Analysis 3.1; summary of findings Table 3).
There was very low‐quality evidence from one trial (serious study design limitations, sparse data) that the Ozzlo pillow (a specially‐designed pillow) placed under the pregnant abdomen relieved night‐time pain better than a regular pillow in the same position. When using the Ozzlo pillow (Thomas 1989; N = 92 analysed), women reported significantly lower intensity of backache at night and during the day, but no significant difference in their ability to sleep through the night. The women's impressions were that the Ozzlo pillow was at least moderately more effective than a regular pillow for preventing or relieving their back pain and at least moderately more valuable for supporting them while sleeping.These results should be regarded with caution since the estimate of effect was measured for all women who used each pillow, rather than comparing each phase of this cross‐over trial independently.
Adverse effects
There were no serious adverse effects noted for either the mother or the neonate in any of the studies. Women who participated in water‐based exercise did not develop any more urinary tract or uterine infections than those who received usual prenatal care. There were no data reported on the (primary) preventative aspects of any of these interventions, although there was a sense that they may have prevented further development of pain and disability, therefore may have had some secondary preventative consequences.
Pelvic pain
This review now includes four trials (N = 661 randomised) investigating interventions for managing pelvic pain; (Depledge 2005; N = 90 randomised) compared the effects of two types of pelvic belts (rigid versus non‐rigid) added to exercise with exercise alone; different acupuncture techniques were compared in two trials (Elden 2008; Lund 2006; N = 185 randomised), and acupuncture or exercise was added to and compared to usual prenatal care in one trial (Elden 2005; N = 386 randomised).
Pelvic belts with exercise
There was low‐quality evidence (study design limitations, sparse data) from one trial (Depledge 2005; N = 87 analysed) that there was a significant reduction of average pain in the group that received exercise alone or exercise plus a rigid belt and no significant pain reduction in the group that had exercise plus a non‐rigid belt, but there were no data provided that compared results between groups. There was also low‐quality evidence that there was no significant difference between the three groups in pelvic girdle pain‐related function. Data were not presented in a fashion that allowed us to analyse them.
Acupuncture, alone or with exercise
Since the techniques studied were different in the two trials, we were unable to pool the data on the most effective method of providing acupuncture.
There was low‐quality evidence (study design limitations, sparse data) from one trial (Elden 2008; N = 108 analysed) that there was no significant difference in pain relief between usual care plus acupuncture and usual care plus non‐penetrating sham acupuncture (median evening pain on VAS 36 and 41 respectively, P = 0.483); usual care plus acupuncture showed significant improvement in activities of daily living over usual care plus non‐penetrating sham acupuncture (median disability rating index (DRI) 44 and 55 respectively, P = 0.001), which was further illustrated in the two groups by the number of women who worked regularly (28/57 (acupuncture) versus 16/57 (control group), P = 0.041). All results were extracted directly from the paper.
There was also low‐quality evidence from one trial (Lund 2006; N = 47 analysed) that there was no significant difference in evening pain between women who received deep acupuncture and those who received superficial acupuncture (RR 1.06; 95% CI 0.73 to 1.54; Analysis 4.1; summary of findings Table 4). Data for activities of daily living were provided for the participants as one group, therefore we cannot provide results for individual techniques.
One trial examined the effects on pelvic pain of adding acupuncture or stabilising exercises to usual prenatal care versus usual prenatal care alone (Elden 2005; N = 330 analysed). There was moderate quality evidence (sparse data) that after one week of treatment, those who received usual care reported significantly more intense evening pain than those who had received either acupuncture (difference of medians: 27; 25th to 75th percentiles 13.3 to 29.5; P < 0.001) or stabilising exercises (difference of medians:13; 25th to 75% percentiles 2.7 to 17.5; P = 0.0245). Those who received acupuncture reported significantly less intense evening pain than those who received stabilising exercises (difference of medians: ‐14; 25th to 75th percentiles ‐18 to ‐3.3; P = 0.0130). These data were taken directly from the published report.
There were no lasting adverse effects noted; complaints of needle pain, slight bleeding, fainting, and sleepiness were noted for both acupuncture and sham acupuncture.
Mixed population with pelvic and low‐back pain
This review now includes 11 trials (N = 2120 randomised) that examined women who had both LBP and pelvic pain; they were given exercises (Eggen 2012; Kluge 2011; Martins 2005; Mørkved 2007; Stafne 2012; N = 1532 randomised), osteopathic manipulation (Peters 2007; N = 60 randomised), a multi‐modal intervention that included manual therapy, exercise and education (Gross 2012; N = 169 randomised); or acupuncture alone (Ekdahl 2010; Kvorning 2004; Wang 2009a; Wedenberg 2000; N = 359 randomised).
Exercise
There was moderate quality evidence from four trials (Eggen 2012; Martins 2005; Mørkved 2007; Stafne 2012; N = 1344 analysed) that an eight‐ to 20‐week exercise training program reduced the risk of women reporting lumbo‐pelvic pain by 15% (RR 0.85; 95% CI 0.73 to 1.00; Tau² = 0.02; I² = 82%; Analysis 5.1; summary of findings Table 5); however, heterogeneity was high. This suggests that the average reduction amongst trials ranged from 0% to 27%, while the distribution of effects in individual trials were wider than this, possibly explaining, in part, some of the heterogeneity. There was moderate quality evidence from two trials (Mørkved 2007; Stafne 2012; N = 1062 analysed) that a 12‐week training program reduced the risk of women reporting lumbo‐pelvic‐related sick leave by 24% (RR 0.76; 95% CI 0.62 to 0.94; Tau² = 0.00; I² = 0%; Analysis 5.2), and improved functional status (results could not be pooled). As with the LBP trials, there was insufficient clinical homogeneity amongst exercise trials to be able to analyse or support a specific set of exercises for a specific group of women.
Manual therapy
There was low‐quality evidence (study design limitations, sparse data) from one trial (Peters 2007; N = 57 analysed) that OMT significantly reduced pain (68% improvement versus 0%; P < 0.0005) and improved disability (28% improvement versus 20% deterioration); data were extracted directly from the paper.
Multi‐modal
There was low‐quality evidence (study design limitations, sparse data) from one trial (Gross 2012; N = 169 analysed) that women who received either a multi‐modal intervention that included manual therapy, exercise and education (MOM) or usual care reported significantly improved disability, but only those in the MOM group reported improved pain and physical function (P < 0.05; further data not provided).
Acupuncture
Four trials measured the effects of adding acupuncture to usual prenatal care. However, because of differences in interventions, comparisons, techniques and outcome measures, we were unable to pool any of the results. Therefore, there is only low‐quality evidence for any of the outcomes, although each trial reported positive results in favour of acupuncture in pain reduction and improved function (summary of findings Table 6).
Ekdahl 2010 (N = 32 analysed) examined the difference between acupuncture started at 20 weeks' and 26 weeks' gestation. They found that both regimens relieved pain, but significantly more in the group that started later. The later group also reported improvement in function despite increased physical restrictions, but data were not provided for between‐group comparisons.
In Kvorning 2004 (N = 72 analysed), 60% of the women who completed the acupuncture treatment reported their pain intensity had decreased, compared to only 14% of the control group, who received usual prenatal care, suggesting a four‐fold benefit from acupuncture (RR 4.16; 95% CI 1.77 to 9.78; Analysis 6.1). The women who received usual prenatal care also used analgesics (5/35), TENS (6/35), physiotherapy (6/35) and a sacroiliac belt (15/35) to help them relieve the pain. Four out of the 37 women in the acupuncture group also used a sacroiliac belt for support.
Wang 2009a (N = 152 analysed) compared the effects of auricular (ear) acupuncture, sham auricular acupuncture and a waiting list control. All women reported pain relief and improved functional status, but those in the acupuncture group reported significantly more pain relief and functional improvement than those in either the sham acupuncture or control group; data were not provided for between‐group comparisons. Sixty‐eight per cent of those in the acupuncture group reported a clinically significant improvement in pain after two weeks of treatment (paper states 30% reduction is clinically significant), as compared to 32% in the sham acupuncture group (P = 0.02) and 18% in the control group (P < 0.001). These data were extracted directly from the paper.
Women who received either acupuncture or physiotherapy (Wedenberg 2000; N = 46 analysed) all reported a reduction in evening pain intensity and disability after completing their program, with the acupuncture group reporting significantly less intense pain (P < 0.01) and lower disability scores than the physiotherapy group. Neither summary data nor analyses were provided for pain. Of note: none of the 30 participants were lost to follow‐up in the acupuncture group (two were not analysed because they received both treatments), while 12/30 were lost to follow‐up in the physiotherapy group; for those who completed the study, there was no significant difference between groups for satisfaction with treatment, with a RR of 1.24 (95% CI 0.96 to 1.60; Analysis 7.1; summary of findings Table 7).
Prevention
There was low‐quality evidence (study design limitations, sparse data) from one trial (Mørkved 2007; N = 301 analysed) that suggested a 12‐week training program prevented lumbo‐pelvic pain in every one in 8.1 women treated (NNT analysis), and moderate quality evidence (sparse data) from one trial (Eggen 2012; N = 213 analysed) that a 16‐ to 20‐week training program was no more successful than usual prenatal care at preventing pelvic pain (odds ratio (OR) 1.03 (95% CI 0.66 to 1.59)) or LBP (OR 0.77 (95% CI 0.50 to 1.19)); data extracted directly from papers. In Mørkved 2007, 95% CI for number NNTB (number needed to benefit) was not provided.
Adverse effects
There were only minor, transient adverse effects reported by those who received acupuncture (small subcutaneous haematomas at insertion site) in Wedenberg 2000 and Wang 2009a. Although the adverse effects reported by those women who received physiotherapy (preterm uterine contractions, pre‐eclampsia) were unlikely to have been caused by the physiotherapy, they withdrew from the study (Wedenberg 2000). Thirty‐eight per cent of the women who received acupuncture in Kvorning 2004 also reported some minor, transient adverse effects (local pain, heat or sweating, local haematoma, tiredness, nausea, weakness). There were no reported problems with any of the deliveries or neonates.
Discussion
Summary of main results
We included 26 randomised trials examining 4093 pregnant women in this updated review, a substantial increase over Pennick 2007 (eight RCTs; 1305 participants). Eleven trials examined LBP (N = 1312 randomised/1164 analysed); four looked at pelvic pain (N = 661 randomised/572 analysed); and 11 examined women with both LBP and pelvic pain (N = 2120 randomised/1918 analysed). Overall, 89% of the women were included in the analyses; the number of women lost to follow‐up ranged from none reported to over 20%.
In summary, for LBP , low‐quality evidence suggested that exercise (land‐ or water‐based) significantly reduced pain, disability and LBP‐related absenteeism more than usual prenatal care by itself. Very low‐quality evidence suggested that a specially‐designed pillow that supports the pregnant abdomen in bed reduced the intensity of backache at night better than a regular pillow.
Low‐quality evidence from single trials suggested there was no significant difference in pain or women's ability to perform activities of daily living when comparing two types of pelvic support belt; in pain relief between osteopathic manipulation (OMT) and usual care; or in pain relief and back‐related function when OMT was compared with sham US.
In summary, for pelvic pain , moderate quality evidence suggested that acupuncture was better than stabilising exercises at reducing evening pain and both of them were better than usual prenatal care.
Low‐quality evidence from single trials suggested that acupuncture improved activities of daily living, including work, better than sham acupuncture; exercise alone or with the use of a rigid belt significantly reduced average pain, but not functional status. There was no statistical difference in functional status or average pain between groups who exercised with a non‐rigid belt; in pain between acupuncture and sham acupuncture or in evening pain between women who received deep or superficial acupuncture.
In summary, for lumbo‐pelvic pain , moderate quality evidence suggested that an eight‐ to 20‐week exercise training program significantly reduced the risk of women reporting lumbo‐pelvic pain, and a 12‐week training program reduced the risk of women reporting lumbo‐pelvic‐related sick leave and improved functional status.
Low‐quality evidence from single trials suggested that OMT significantly reduced pain and improved disability; women who received a multi‐modal intervention that included manual therapy, exercise and education (MOM) reported improved pain and physical function; and acupuncture reduced pain better than usual prenatal care. Acupuncture started at 26 weeks' gestation reduced pain and disability better than acupuncture started at 20 weeks'; and acupuncture significantly reduced pain and improved functional status better than either physiotherapy, sham acupuncture or usual care.
Prevention: four trials also sought an effective intervention to prevent back or pelvic pain. One provided the results of a numbers needed to treat analysis for improvement in pain and disability following participation in an exercise training program for pelvic and LBP, but no measures of variability (Mørkved 2007); another suggested that a 16‐ to 20‐week training program was no more successful than usual prenatal care at preventing pelvic pain or LBP (Eggen 2012); Thomas 1989 measured women's overall impressions of a special pillow for preventing backache, but there were no data to support this impression; and finally Sedaghati 2007 only provided data on treatment effects, not primary prevention.
Overall completeness and applicability of evidence
The studies included in this updated review were conducted in Iran, Brazil, USA, Sweden, Thailand, Australia, New Zealand, Norway, South Africa and Germany, which would suggest that the women who participated broadly represented pregnant women in general. However, women entered the studies at various times in their pregnancies and were diagnosed with pelvic, back pain or both using a variety of methods ranging from self‐reported symptoms to different diagnostic tests (depending on the study), making the internal validity and reliability of the classification of each condition questionable.
Primary outcomes of interest for this review were pain, disability, absenteeism from work and adverse events. While pain was measured in all the studies, disability and functional status were not, nor was absenteeism from work or adverse events. Only four studies (Elden 2008; Kihlstrand 1999; Mørkved 2007; Stafne 2012) reported on the positive impact of the interventions on the women's absenteeism from work due to their back or pelvic pain. Considering the number of women who now participate in the paid workforce, this is a limitation that should be addressed in future studies.
Women who participated in additional exercise programs, received acupuncture or OMT, or used a pillow or abdominal support generally expressed satisfaction with the interventions and felt they would consider them in subsequent pregnancies. In general, women in the studies who received more than usual prenatal care appeared to experience some pain relief, although the results varied. Three pooled estimates of effect were moderate (SMD 0.5 to < 0.8, Analysis 1.2; or large in size (SMD ≥ 0.8; Analysis 1.1; Analysis 3.1; Cohen 1988) and would likely be considered clinically significant. On the other hand, had the potential for risks of bias been lower, the estimates of effect may also have been lower, since it has been shown that trials with lower risks of bias have lower effect sizes (Van Tulder 2009). This was bourne out by the sensitivity analyses and re‐analyses of Analysis 1.1 and Analysis 1.2. Data from Gil 2011 and Suputtitada 2002 were clear outliers in the meta‐analyses, which raised the concern that standard errors had been inadvertently reported instead of standard deviations. With the original data, the results were SMD ‐2.04 (95% CI ‐3.03 to ‐1.04) for pain and SMD ‐1.86 (95% CI ‐4.63 to 0.91) for disability. Removing them from the analyses resulted in smaller estimates of effect: SMD ‐0.75 (95% CI ‐1.10 to ‐0.40) for pain and SMD ‐0.49 (95% CI ‐0.87 to ‐0.12) for disability; re‐calculating the standard deviation and using the new values in the meta‐analyses resulted in less heterogeneity and more modest estimates of effect that were closer to the sensitivity analyses (SMD ‐0.80; 95% CI ‐1.07 to ‐0.53 for pain and SMD ‐0.56; 95% CI ‐0.89 to ‐0.23 for disability).
Considering the quality of the evidence in this review, these results must be considered with caution and generalising the results to all pregnant women is likely premature.
Incorporating the evidence into clinical practice may be challenging since 'usual prenatal care' and 'standard physiotherapy' are not described in sufficient detail in the trials and are likely to vary across jurisdictions. Similarly, there were insufficient details provided about other interventions that would make it difficult to replicate in another clinical setting.
Quality of the evidence
No outcomes were supported by high‐quality evidence and only three by moderate‐quality evidence (acupuncture for pelvic pain, exercise for lumbo‐pelvic pain and lumbo‐pelvic work absenteeism). Overall, there was low‐quality evidence for outcomes because of high risks of bias and sparse data. Trials were generally small (range 30 to 855 women; with only three trials including over 300 women, the GRADE rule of thumb for imprecision/sparse data; Schünemann 2009). Clinically heterogeneous populations, interventions, comparisons and outcome measures precluded pooling the results to arrive at overall estimates of effect in all but the exercise interventions for LBP and combined pelvic and back pain. Inclusion criteria were quite different across studies; women were admitted at different points in their pregnancy, 'diagnoses' of LBP and pelvic pain ranged from self‐report of symptoms to clinical interpretation of the results of special tests, such as the posterior pelvic pain provocation test, resulting in a heterogenous population. Pain and disability were measured in a variety of ways; pain was measured as intensity, presence, change in pain within groups, numbers or percentage who reported improvement, and disability was measured as back‐specific function, general function, ability to perform activities of daily living, change in abilities within groups, numbers or percentage who reported improved function, time off work and sleep disturbance. Outcomes were measured daily, weekly, in the morning, in the evening, over the course of the pregnancy and during the postpartum period; the latter outcomes were outside the scope of this review.
Besides the paucity of usable data, the risks of bias contribute to the lack of confidence we have in the results. Overall, the trial reports were poorly written and it was difficult to follow some of the analyses, although more recent trials tended to be more complete. We only included RCTs (one of which used a cross‐over design) in this review, but in 13 of the trials, the methods of randomisation were unclear and in 14, the methods of allocation concealment were unclear. On the other hand, we excluded eight trials because the techniques they described for randomisation were at high risk for bias, or allocation procedures were simply unclear. Current wisdom suggests that randomisation and concealment of allocation are key study characteristics that reduce the potential for bias. Blinding of personnel remains difficult in non‐pharmaceutical trials, a reality that increases the risk of bias, especially in self‐reported measures of symptoms. Some of the more recent trials did attempt to minimise bias by recruiting, for example, only participants who were naive to acupuncture (Elden 2005; Elden 2008) or by conducting credibility checks (Wang 2009a) to determine the participants' expectations of the study interventions they were offered. In Gil 2011, Martins 2005 and Ekdahl 2010, baseline pain was different in the two groups. In Wedenberg 2000, 12 of 30 women dropped out of the physiotherapy group, while none withdrew from the acupuncture group (although two were excluded from analysis due to receiving both treatments), leading to potential attrition bias. Based on baseline data, there were no obvious reasons for the difference in withdrawals between the two groups.
For this update, we decided not to use the data from Thomas 1989, the cross‐over study looking at the effects of different pillows. Rather than comparing the results from each phase separately, they had calculated the outcomes from all of the women when they were using the Ozzlo pillow against their outcomes when they were using the standard pillow, making it look as if there were 184 women analysed in the study instead of just 92. In addition, the study design did not allow the effects of one pillow to subside before starting to use the second, and women in group two were one week further into their pregnancy. While this is not a long time, many women report that back pain increases as pregnancy progresses making this a notable study design flaw which puts the two groups at a different risk for back pain. The authors did report that there were no differences in the main outcomes between the two weeks, however if future cross‐over studies are included, it would be important to divide the results from the two phases.
There were only minor, transient adverse effects reported in this review by those who received acupuncture (small subcutaneous hematomas at insertion site) in Wedenberg 2000 and Wang 2009a. A systematic review on the safety profile of acupuncture for back pain concluded, from reports on over 100,000 patients from the US, UK, and Sweden, that reported incidents from acupuncture were, on the whole, minor and transient. They listed fainting (10 patients), unexpected exacerbation of symptoms (12 patients), pain at site of needle (six patients), needle left in place (five patients), seizure after needle insertion (one patient with known epilepsy), slurred speech (one patient), pneumothorax (two patients), broken needle (two patients) and minor bleeding at site (15% of treatments) as the most notable problems (Cherkin 2003). More recently Moffatt 2013 has concluded that there is no firm evidence to suggest that acupuncture treatment can cause detrimental effects for the fetus or the maintenance of pregnancy. Therefore, provided that certain points that supply the cervix and uterus are avoided Vermani 2010, the current evidence would suggest that acupuncture is relatively safe for pregnant women with no other complications.
Potential biases in the review process
This review was updated using the updated Cochrane methodology for assessing risk of bias and quality of the evidence. The international literature was searched and trials in languages other than English were retrieved. However, while the English articles were identified and assessed by two review authors independently, the four non‐English reports were only reviewed by one person (Bandpei 2010; Gil 2011; Martins 2005; Peters 2007); Gil 2011 was also translated using Google Translate (Google Translate). Three non‐English reports were also excluded by one person only (Chitryniewicz 2010; Momoi 1999; Zand 2011). This has the potential to lead to some errors, but considering the lack of overall data in the English reports, this is not likely to make a substantial change in the results or quality of the evidence.
Agreements and disagreements with other studies or reviews
Pennick 2007 included eight RCTs (1305 women with pelvic, back pain or both) and found that adding pregnancy‐specific exercises, physiotherapy, acupuncture and pillows to usual prenatal care reduced pain intensity, disability, and absenteeism. However, seven of the eight trials had moderate to high risks of bias and readers were advised to view the results with caution.
A number of non‐Cochrane systematic reviews have been published since Pennick 2007. While they do have different foci and different search dates, Ee 2008; Kanakaris 2011; Richards 2012; Vermani 2010 and this current review are essentially in agreement for the aspects of overlap. Field 2008 reviewed research on the effectiveness of complementary and alternative medicine for pregnancy and labour and concluded that the evidence suggests they are effective for reducing pregnancy‐related back and leg pain, amongst other symptoms and bio‐markers outside the scope of this review, but 'the research has several methodological limitations'. Anderson 2005 investigated the effectiveness of complementary and alternative medicine in obstetrics and included two of the trials included in this review that examined the effects of acupuncture on pregnancy‐related LBP (Kvorning 2004; Wedenberg 2000). They came to the same conclusions as we did.

'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
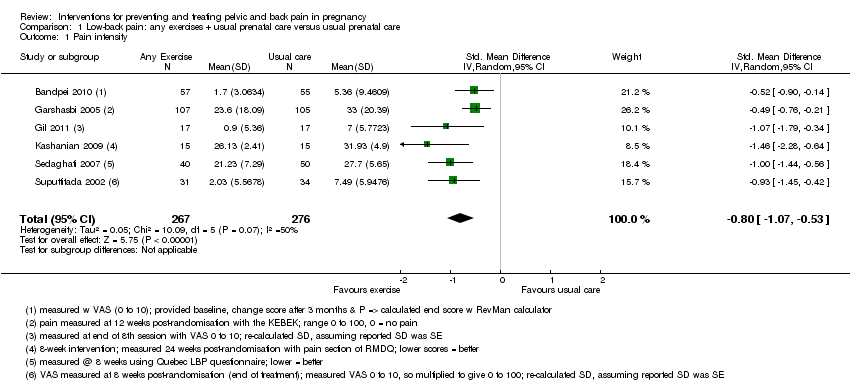
Comparison 1 Low‐back pain: any exercises + usual prenatal care versus usual prenatal care, Outcome 1 Pain intensity.

Comparison 1 Low‐back pain: any exercises + usual prenatal care versus usual prenatal care, Outcome 2 Disability.

Comparison 2 Low‐back pain: water gymnastics + usual prenatal care versus usual prenatal care, Outcome 1 Number of women taking sick leave because of back pain after 32 weeks' gestation.

Comparison 3 Low‐back pain: support belts, Outcome 1 Low‐back pain, measured with VAS; 0 to 10; 0 = no pain.
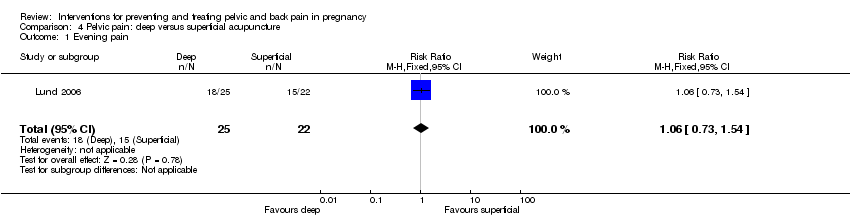
Comparison 4 Pelvic pain: deep versus superficial acupuncture, Outcome 1 Evening pain.

Comparison 5 Pelvic + low‐back pain: any exercises + usual prenatal care versus usual prenatal care, Outcome 1 Women who reported pain on Visual Analogue Scale.
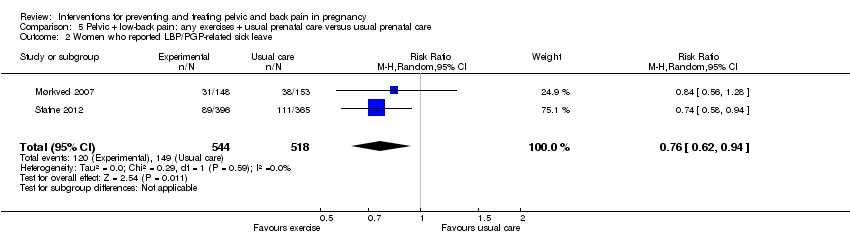
Comparison 5 Pelvic + low‐back pain: any exercises + usual prenatal care versus usual prenatal care, Outcome 2 Women who reported LBP/PGP‐related sick leave.

Comparison 6 Pelvic + low‐back pain: acupuncture + usual prenatal care versus usual prenatal care, Outcome 1 Number of women who reported decreased pain.
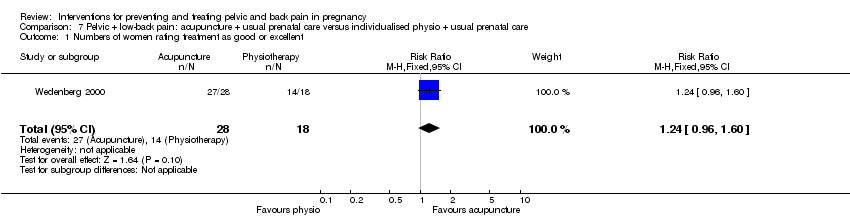
Comparison 7 Pelvic + low‐back pain: acupuncture + usual prenatal care versus individualised physio + usual prenatal care, Outcome 1 Numbers of women rating treatment as good or excellent.
| Low‐back pain: any exercises + usual prenatal care versus usual prenatal care for treating back pain in pregnancy | ||||||
| Patient or population: pregnant women with back pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Low‐back pain: any exercises + usual prenatal care versus usual prenatal care | |||||
| Pain intensity measured by a number of different measurements; lower score = better | The mean pain intensity in the control groups was18.75 | The mean pain intensity in the intervention groups was | SMD ‐0.80 (‐1.07, ‐0.53) | 543 | ⊕⊕⊝⊝ | |
| Disability measured by Roland Morris Disability Questionnaire and Oswestry Disability Index | The mean disability in the control groups was 26.6 | The mean disability in the intervention groups was | SMD ‐0.56 (‐0.89 to ‐0.23) | 146 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 poor or no description of randomisation process, allocation concealment, blinding of research personnel | ||||||
| Low‐back pain: water gymnastics + usual prenatal care versus usual prenatal care for treating back pain in pregnancy | ||||||
| Patient or population: pregnant women with back pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control (usual care) | water gymnastics | |||||
| Number of women taking sick leave because of back pain after 32 weeks' gestation | Study population | RR 0.4 | 241 | ⊕⊕⊝⊝ | ||
| 144 per 1000 | 58 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 unclear methods of randomisation; research personnel not blinded | ||||||
| Low‐back pain: support belts for preventing and treating pelvic and back pain in pregnancy | ||||||
| Patient or population: pregnant women with back pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Low‐back pain: support belts | |||||
| BellyBra versus Tubigrip ‐ Low‐back Pain | The mean Bellybra versus Tubigrip back pain in the control group was 4.7, measured on VAS 0 to 10 | The mean Bellybra versus Tubigrip ‐ back pain in the intervention group was 0.2 lower (1.19 lower to 0.79 higher) | MD ‐0.20 (95% CI ‐1.19 to 0.79) | 94 | ⊕⊕⊝⊝ | |
| BellyBra versus Tubigrip ‐ ADL | The mean Bellybra versus Tubigrip ability to perform activities of daily living in the control group was 5.6, measured as a total of several activities | The mean Bellybra versus Tubigrip ability to perform activities of daily living in the intervention group was 0.9 lower | MD ‐0.90 (95% CI ‐1.81 to 0.01) | 94 | ⊕⊕⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 no blinding of research personnel described; no explanation provided for lost‐to‐follow‐up data; different co‐interventions and compliance between groups | ||||||
| Pelvic pain: deep versus superficial acupuncture for preventing and treating pelvic and back pain in pregnancy | ||||||
| Patient or population: pregnant women with pelvic pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control (superficial) | Intervention (deep) | |||||
| evening pain, reported as better, based on women's report on Visual Analogue Scale | Study population | RR 1.06 | 47 | ⊕⊕⊝⊝ | ||
| 682 per 1000 | 723 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 randomisation process and attrition rate/explanations not described | ||||||
| Pelvic + low‐back pain: any exercises + usual prenatal care versus usual prenatal care for preventing and treating pelvic and back pain in pregnancy | ||||||
| Patient or population: pregnant women with, or at risk of developing, pelvic and back pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control (usual prenatal care) | Any exercises + usual prenatal care | |||||
| Number of women who reported pain on Visual Analogue Scale | Study population | RR 0.85 | 1344 | ⊕⊕⊕⊝ | ||
| 747 per 1000 | 635 per 1000 | |||||
| Number of women who reported LBP/PGP‐related sick leave | Study population | RR 0.76 | 1062 (2 studies) | ⊕⊕⊕⊝ | ||
| 288 per 1000 | 219 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 there was a mix of potential biases among the four studies: no allocation concealment (1); no blinding of research personnel (all); poor/no description of drop‐outs, co‐interventions and baseline inequality (mixed) | ||||||
| Pelvic + low‐back pain: acupuncture + usual prenatal care versus usual prenatal care for preventing and treating pelvic and back pain in pregnancy | ||||||
| Patient or population: pregnant women with, or at risk of developing, pelvic and back pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Pelvic + low‐back pain: acupuncture + usual prenatal care versus usual prenatal care | |||||
| Number of women who reported decreased pain | Study population | RR 4.16 | 72 | ⊕⊕⊝⊝ | ||
| 143 per 1000 | 594 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 no blinding of research personnel, over 20% attrition, different co‐interventions | ||||||
| Pelvic + low‐back pain: acupuncture + usual prenatal care versus individualised physio + usual prenatal care for preventing and treating pelvic and back pain in pregnancy | ||||||
| Patient or population: pregnant women with, or at risk of developing, pelvic and back pain | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control (individualised physio + usual prenatal care) | acupuncture + usual prenatal care | |||||
| Numbers of women rating treatment as good or excellent | Study population | RR 1.24 | 46 | ⊕⊕⊝⊝ | ||
| 778 per 1000 | 964 per 1000 | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 no description of randomisation process, no blinding of research personnel described, uneven attrition (12 dropped out of physio group, while none dropped out of the acupuncture group) and co‐interventions between groups | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pain intensity Show forest plot | 6 | 543 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.80 [‐1.07, ‐0.53] |
| 2 Disability Show forest plot | 2 | 146 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.56 [‐0.89, ‐0.23] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Number of women taking sick leave because of back pain after 32 weeks' gestation Show forest plot | 1 | 241 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.40 [0.17, 0.92] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Low‐back pain, measured with VAS; 0 to 10; 0 = no pain Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1 Low‐back Pain | 1 | 94 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐1.19, 0.79] |
| 1.2 ADL | 1 | 94 | Mean Difference (IV, Fixed, 95% CI) | ‐0.90 [‐1.81, 0.01] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Evening pain Show forest plot | 1 | 47 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.06 [0.73, 1.54] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Women who reported pain on Visual Analogue Scale Show forest plot | 4 | 1344 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.73, 1.00] |
| 2 Women who reported LBP/PGP‐related sick leave Show forest plot | 2 | 1062 | Risk Ratio (M‐H, Random, 95% CI) | 0.76 [0.62, 0.94] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Number of women who reported decreased pain Show forest plot | 1 | 72 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.16 [1.77, 9.78] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Numbers of women rating treatment as good or excellent Show forest plot | 1 | 46 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.24 [0.96, 1.60] |