Interwencje w środkach masowego przekazu stosowane w celu profilaktyki palenia tytoniu wśród młodych ludzi
Abstract
Background
Mass media interventions can be used as a way of delivering preventive health messages. They have the potential to reach and modify the knowledge, attitudes and behaviour of a large proportion of the community.
Objectives
To assess the effects of mass media interventions on preventing smoking in young people, and whether it can reduce smoking uptake among youth (under 25 years), improve smoking attitudes, intentions and knowledge, improve self‐efficacy/self‐esteem, and improve perceptions about smoking, including the choice to follow positive role models.
Search methods
We searched the Cochrane Tobacco Addiction Group Specialized Register, with additional searches of MEDLINE and Embase in June 2016. This is an update of a review first published in 1998.
Selection criteria
Randomized trials, controlled trials without randomization and interrupted time‐series studies that assessed the effect of mass media campaigns (defined as channels of communication such as television, radio, newspapers, social media, billboards, posters, leaflets or booklets intended to reach large numbers of people and which are not dependent on person‐to‐person contact) in influencing the smoking behaviour (either objective or self‐reported) of young people under the age of 25 years. We define smoking behaviour as the presence or absence of tobacco smoking or other tobacco use, or both, and the frequency of tobacco use. Eligible comparators included education or no intervention.
Data collection and analysis
Two review authors independently extracted information relating to the characteristics and the content of media interventions, participants, outcomes, methods of the study and risks of bias. We combined studies using qualitative narrative synthesis. We assessed the risks of bias for each study using the Cochrane 'Risk of bias' tool, alongside additional domains to account for the nature of the intervention. We assessed the quality of evidence contributing to outcomes using GRADE.
Main results
We identified eight eligible studies reporting information about mass media smoking campaigns, one of which is new for this update. Seven of the studies used a controlled trial design and one an interrupted time‐series analysis. Risks of bias were high across all included studies and there was considerable heterogeneity in study design, intervention and population being assessed.Three studies (n = 17,385), one of which compared a mass media intervention to no intervention and two of which evaluated mass media interventions as adjuncts to school‐based interventions, found that the mass media interventions reduced the smoking behaviour of young people. The remaining five studies (n = 72,740) did not detect a significant effect on smoking behaviour. These included three studies comparing a mass media intervention to no intervention, one study evaluating a mass media intervention as an adjunct to a school‐based intervention, and one interrupted time‐series study of a social media intervention. The three campaigns which found a significant effect described their theoretical basis, used formative research in designing the campaign messages, and used message broadcast of reasonable intensity over extensive periods of time. However, some of the campaigns which did not detect an effect also exhibited these characteristics. Effective campaigns tended to last longer (minimum 3 years) and were more intense (more contact time) for both school‐based lessons (minimum eight lessons per grade) and media spots (minimum four weeks' duration across multiple media channels with between 167 and 350 TV and radio spots). Implementation of combined school‐based components (e.g. school posters) and the use of repetitive media messages delivered by multiple channels (e.g. newspapers, radio, television) appeared to contribute to successful campaigns.
Authors' conclusions
Certainty about the effects of mass media campaigns on smoking behaviour in youth is very low, due to inconsistency between studies in both design and results, and due to methodological issues amongst the included studies. It would therefore be unwise to offer firm conclusions based on the evidence in this review. Methodologically rigorous studies investigating the effect of social media and novel forms of technology as part of tobacco prevention campaigns for youth are needed.
PICO
Streszczenie prostym językiem
Czy kampanie medialne (telewizyjne, w radiu, prasie, na bilbordach oraz broszurach) mogą powstrzymać młode osoby od rozpoczęcia palenia tytoniu?
Wprowadzenie
Palenie tytoniu jest epidemią współczesnych czasów, a zapobieganie paleniu wśród młodzieży pozostaje głównym priorytetem działań prozdrowotnych, gdyż eksperymentowanie z papierosami rozpoczyna się w młodym wieku. Jedną z metod osiągnięcia tego celu jest dotarcie do młodzieży za pośrednictwem środków masowego przekazu, co może wpłynąć na zmianę postawy, stan wiedzy i zachowania dużej części populacji.
Pytanie badawcze
Czy prowadzenie kampanii w środkach masowego przekazu może zniechęcić młode osoby do palenia tytoniu?
Charakterystyka badań
Spośród 1326 publikacji wybraliśmy 8 badań, w których wzięło udział łącznie 52 746 uczestników. W niniejszej aktualizacji przeglądu uwzględniono jedno nowe badanie. Ostatnie wyszukiwanie przeprowadzono w czerwcu 2016 roku. Wszystkie badania dotyczyły młodych osób w wieku poniżej 25 lat. Siedem badań przeprowadzono w Stanach Zjednoczonych, a jedno badanie w Norwegii. Rodzaj środka masowego przekazu (np. telewizja) oraz niektóre cechy uczestników badań (np. wiek), jak również długość okresu obserwacji różniły się w poszczególnych badaniach.
Główne wyniki
W trzech spośród ośmiu badań stwierdzono, że stosowanie różnych interwencji skutecznie zapobiegało paleniu tytoniu wśród młodzieży. W pozostałych pięciu badaniach nie odnotowano żadnego efektu. Pomimo tego, że pewne cechy zarówno skutecznych jak i nieskutecznych działań były podobne, to kampanie efektywne trwały dłużej (co najmniej 3 lata) i były bardziej intensywne (dłuższy czas kontaktu młodzieży z interwencją), co obejmowało zarówno zajęcia lekcyjne (co najmniej 8 godzin lekcyjnych na jedną klasę) jak i spoty medialne (obejmujące od 167 do 350 spotów telewizyjnych i radiowych emitowanych w wielu kanałach przez co najmniej 4 tygodnie). Wdrożenie łączonych programów szkolnych (np. plakatów) i wykorzystanie powtarzających się przekazów medialnych za pośrednictwem wielu kanałów (prasa, radio, telewizja) przyczyniły się do sukcesu kampanii.
Jakość danych naukowych
Jakość danych naukowych przedstawionych w tym przeglądzie jest ograniczona ze względu na problemy z raportowaniem wyników oraz zaplanowaniem samego badania. Badania różniły się pod względem metodyki, badanej interwencji oraz grupy badanej. Wyniki w badaniach były zróżnicowane. W szczególności, w żadnym z badań nie zaślepiono uczestników (nie są informowani jakiej interwencji lub leczeniu są poddani; przyp. tłum.), jednocześnie powstają wątpliwości co do sposobu przydzielenia osób do grupy badanej i kontrolnej. Nierozsądne byłoby zatem przedstawienie jednoznacznych wniosków na podstawie dostępnych danych. Wykazane i włączenie do przeglądu jedynie dwóch badań przeprowadzonych w ciągu ostatnich 10 lat jest niepokojące, biorąc pod uwagę rosnącą popularność mediów społecznościowych wśród młodzieży. Konieczne jest zatem przeprowadzenie dalszych wysokiej jakości badań.
Authors' conclusions
Summary of findings
| Mass media interventions for preventing smoking in young people | ||||
| Patient or population: Young people aged less than 25 years Settings: Schools, community groups, television, radio, newspapers, billboards, posters, leaflets or booklets Intervention: Mass media channels of communication intended to reach large numbers of people and which are not dependent on person‐to‐person contact Comparison: Usual care, minimal education, no intervention or co‐interventions | ||||
| Outcomes | Impact | No of Participants | Quality of the evidence | Comments |
| Smoking rates (follow‐up 18 months to 6 years) | 3 (n = 17,385), 1 which compared a mass media intervention to no intervention and 2 which evaluated mass media interventions as adjuncts to school‐based interventions, found that the mass media interventions reduced the smoking behaviour of young people. The remaining 5 studies (n = 72,740) did not detect a significant effect on smoking behaviour. These included 3 studies comparing a mass media intervention with no intervention, 1 study evaluating a mass media intervention as an adjunct to a school‐based intervention, and 1 interrupted time‐series study of a social media intervention. | 90,125 (8 studies) | ⊕⊝⊝⊝ | The 3 campaigns for which a significant effect was detected described a theoretical basis, used formative research in designing the campaign messages, and used message broadcast of reasonable intensity over extensive periods of time. However, some of the campaigns which did not detect an effect also exhibited these characteristics. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||
| GRADE Working Group grades of evidence | ||||
| 1Downgraded two levels due to serious risk of bias: all included studies were rated high risk of bias in at least four domains. | ||||
Background
Description of the condition
Smoking is a modern‐day epidemic (Mead 2014) and a major cause of premature death worldwide (Jha 2013; Shiels 2017). Smoking tobacco is a risk factor for six of the eight leading causes of death in the world; namely, chronic obstructive pulmonary disease (COPD), ischaemic heart disease, trachea, bronchus and lung cancers, cerebrovascular disease, lower respiratory tract infection and tuberculosis (World Health Organization 2009). As such, it remains one of the most important public health hazards (Jha 2013; Lortet‐Tieulent 2016; Schroeder 2013; Thun 2013).
Exposure to smoke, whether through active or passive smoking, is especially concerning for children, and leads to both short‐term and long‐term health effects. Exposure to second‐ or third‐hand smoke can lead to increased respiratory symptoms, diminished lung function and respiratory tract infections (Henderson 2008; Kum‐Nji 2006; Pattenden 2006), as well as declines in cognitive function (Chen 2013). For instance, youth who are exposed to smoke have an increased risk of developing asthma (Gilliland 2006) and have a decline in cardiopulmonary function and exercise tolerance, with as little as one month's worth of exposure to passive smoking (Das 2003). When young people take up active smoking, typically during adolescence, the health effects on the respiratory system are thought to immediately worsen (Henderson 2008) and adversely affect their health. For example, immediate neurological changes can be witnessed (Abreu‐Villaca 2003; Jacobsen 2007).
Description of the intervention
Mass media consist of any channel of communication that has the capacity to reach large numbers of people and therefore have the ability to achieve population‐level change (Wakefield 2010). This type of media does not rely on person‐to‐person contact to achieve the intended goal. It covers a wide variety of channels and vehicles, including but not limited to television, radio, newspapers, flyers, pamphlets and even social media. An attractive aspect of mass media as an avenue for message delivery is that it has the potential to reach a large proportion of the population whilst being relatively low cost.
Mass media have been widely used to achieve population‐wide developmental goals and affect particular outcomes such as education, migration and social capital (Ferrara 2015). Examples of health‐improvement campaigns disseminated at a population level can be found from as early as the 1700s (Noar 2006; Wakefield 2010). The purpose of mass media health campaigns is to increase the prominence of particular health issues and to increase awareness of the potential problems resulting in favourable behavioural change (Randolph 2004). This helps to keep the health topic on the social and political agenda, whilst being a trigger for other interventions/initiatives and giving legitimacy to community programmes (Wellings 2000).
How the intervention might work
Using mass media for health promotion relies on the ability of the platform to reach a large audience (Randolph 2004). The bigger the exposure, the more chance that its content is perceived and the desired effect reached. While this may sound relatively simple, the efficacy of mass media campaigns also relies on many other factors, including message type, specifics of exposure, the target group at hand, execution of the messages, as well as the specific theoretical foundation on which it is (ideally) built (Flay 1987c; Noar 2006; Wakefield 2003). Failure to take these criteria sufficiently into account can lead to lower or even no effects, regardless of the exposure rate. The specific theoretical foundation (if any is used) can determine or guide the content of the above‐mentioned criteria.
Mass media campaigns can either be directed at the individual level or can be focused on changing social norms in a greater proportion of society (Wellings 2000). Many mass media campaigns have some sort of basis in social learning theory (Bandura 1977; Bandura 2001), regardless of whether they intend to do so or not, with a main focus on the use of role models to shape the behaviours of individuals. The aim of these campaigns is to let youth identify with the models and learn from them by replicating their attitudes or behaviours (positive model), or rejecting the behaviour (negative model). Other campaigns place more focus on risk perception and fear appeal in the construction of their campaign (Pechmann 2003; Witte 2000). The rationale in these interventions is that an individual first needs to recognize a risk or threat before one can take the preventive measures associated with health improvement. More recently, mass media campaigns have been based on social marketing (Fallin 2015), which uses commercial marketing techniques to create health behavioural change (Grier 2005). The focus of social marketing messages is on incentives for voluntary change, making sure that the perceived benefits of the health behaviour outweigh the perceived costs, thereby encouraging behaviour change.
Mass media campaigns can also stimulate interpersonal communication on important health topics, thereby indirectly influencing health behaviour rather than directly targeting it (Southwell 2007). By creating interpersonal communication, the intervention can lead to changing social norms, which is dubbed 'the social diffusion model' (Wellings 2000). Campaigns that centre on social diffusion aim to create a catalytic health promotion effect in society rather than specific behavioural changes in one individual.
Why it is important to do this review
The benefits of tobacco prevention on the health of the individual are well known (US DHHS 2012). One Australian study found that a hypothetical 1% reduction in absolute smoking over 12 months (between 2001 and 2002) would have resulted in 1000 fewer hospitalizations for acute myocardial infarction and 350 fewer hospitalizations for stroke, producing a cost saving of over AUD 20.4 million in direct healthcare costs (Hurley 2005). Addiction to nicotine usually begins during adolescence, and young people who start to smoke at an early age have more difficulty quitting in later years (Reed 1993; Giovino 1994). Therefore, reducing the prevalence of tobacco use amongst adolescents remains a key public health priority (BMA 2008). Evidence from Australia demonstrates the extent of the problem; each year approximately 15,000 Australians die from a lifetime of tobacco use (Scollo 2015). Despite the well‐known morbidity and mortality consequences (Warren 2006), these smokers are being replaced by 70,000 young Australians every year who are taking up the habit (Scollo 2015). Experimentation with cigarettes has been reported to start early, with 19.1% of school students who had never smoked cigarettes indicating they were susceptible to starting to smoke during the next year (MMWR 2008). The New Jersey Youth Tobacco Survey estimated that 90 million cigarettes, or 4.2 million packs of cigarettes were consumed by high‐school students annually in 2006 (UMDNJ 2007). Smoking behaviour among adolescent girls is increasing over that of boys (Warren 2009; Mahalik 2013). Smoking prevalence in 1994 was 10% for boys and 13% for girls aged between 11 and 15 years (Walters 1996). However a 2006 survey in Scotland demonstrated that smoking prevalence amongst boys decreased from 29% to 12%, but the rate of decline for girls was significantly less, from 26% to 18% (BMA 2008). This all points to the importance of targeting youth to limit the uptake of smoking.
At the end of the last century it was suggested that mass media were particularly appropriate for delivering anti‐smoking messages to young people because of their engagement and interest in the media (US DHHS 1994). On average, American children between the ages of eight and 18 are reported to spend seven‐and‐a‐ half hours a day using and interacting with media (Common Sense Media 2012). The mass media, particularly television, can influence a young person's perception of what constitutes the real world and acceptable social behaviour, and help to mould cultural norms and convey important and believable messages about the behaviours it depicts (Strasburger 1995). While the media landscape has changed with the rise of the internet and new technologies over the past decade (e.g. smartphones and tablet devices), television remains the predominant form of media used by children and adolescents (Strasburger 2013), either watched by itself or playing in the background when performing other activities (Brasel 2011). From this we can see that youth engagement with mass media has not diminished and indeed has increased over time.
A review by Kremers 2004 argued that smoking prevention should aim at influencing the image of non‐smoking (i.e. positively influencing the identity of non‐smokers) by using mass media interventions and restrictive policies. Evidence is accruing that media campaigns designed around persuasive health messages to change social norms may be effective tools to obtain behaviour change (Brown 1990; Lawrence 2010; Pechman 2000; Zucker 2000). This has been described and supported further among adolescents and young people (Callery 2011; Kupersmidt 2012; Macy 2012).
This review is limited to people younger than 25 years of age. Please see Bala 2013 for a review on the effects of mass media interventions for smoking cessation in adults.
Objectives
To assess the effects of mass media interventions on preventing smoking in young people, and whether it can:
-
Reduce smoking uptake among youth (< 25 years)
-
Improve smoking attitudes, intentions and knowledge
-
Improve self‐efficacy/self‐esteem
-
Improve perceptions about smoking, including the choice to follow positive role models.
Methods
Criteria for considering studies for this review
Types of studies
Any study that evaluated the effect of any kind of mass media campaign in influencing smoking behaviour in young people, using one of the following designs:
-
Cluster‐randomized controlled trial (cRCT) in which the unit of randomization was the school, community or geographical region. Randomized controlled trials not randomized by cluster were not available due to the nature of the intervention
-
Controlled trial without randomization allocating schools, communities or geographical regions
-
Interrupted time series (i.e. data collection for one individual at regular intervals over a period of time)
We excluded uncontrolled before‐and‐after studies and uncontrolled studies with post‐intervention measurements only (no baseline measurement).
Types of participants
Young people aged less than 25 years.
Types of interventions
Mass media are defined here as channels of communication such as television, radio, newspapers, billboards, posters, leaflets or booklets intended to reach large numbers of people and which are not dependent on person‐to‐person contact. The purpose of the mass media campaign must be primarily to prevent the uptake of smoking in young people. We also included studies of mass media campaigns combined with school‐based programmes designed to influence smoking behaviour in young people, as well as studies considering social media (e.g. Facebook, Twitter, MySpace, Instagram, YouTube and Snapchat).
Comparators included usual care, minimal education (e.g. pamphlet resource) or no intervention. We also considered co‐interventions (where both the intervention and control populations received the same intervention other than that of the mass media intervention) for inclusion.
Types of outcome measures
Primary outcome:
Smoking/tobacco use status: daily, weekly, monthly, ever, non‐smoker, smokeless tobacco user, smoker (frequency/quantity unspecified). We excluded studies which did not report smoking behaviour.
Young people may be classified as smokers or non‐smokers in different ways; where possible we preferred the strictest definition, in which young people with any history of cigarette use were defined as smokers.
Secondary outcome (for studies reporting a smoking outcome):
-
Smoking attitudes: attitude toward smoking (total), advantages/positives, disadvantages/negatives, perceived peer attitudes, 'smokers look better', 'smokers more popular', 'non‐smokers aren't affected', 'smokers are thinner', 'okay for young people to smoke'
-
Intentions to smoke
-
Smoking knowledge: addictive properties of smokeless tobacco, harmfulness of first use, effects of mild cigarettes, ease of quitting, tobacco companies' ability to target children
-
Self‐esteem/self‐efficacy
-
Smoking perception: perceived norms, perceived adult smoking, perceived peer smoking, perceived sibling smoking
-
Process measures: media reach
-
Cost effectiveness
We excluded mass media campaigns which have been assessed only in terms of intermediate outcomes or process measures.
Search methods for identification of studies
We searched the Cochrane Tobacco Addiction Group Specialized Register of trials. This is derived from regular systematic searches of bibliographic databases including the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase, PsycINFO and Science Citation Index (see Tobacco Addiction Group Module for search strategies and dates). Reports of trials of mass media interventions to prevent smoking uptake are identified as potentially relevant when new reports are added to the Register. As a check that all reports of mass media prevention studies had been identified, we searched MEDLINE and Embase using a combination of topic‐related terms, age‐limiting terms, and the tobacco and study design terms used for the main searches. Topic‐related terms included the following; mass media, videotape recording, telecommunications, radio motion pictures, audiovisual aids, radio, television, television (TV), campaign, advertising. Full search strategies are given in Appendix 1. The most recent search was conducted on the 2nd of June 2016.
Searches for the first version of this review covered a larger range of databases; we did not find that the scope of the other databases or their indexing terms helped to retrieve additional study reports. Databases and strategies for the original version of this review are listed in Appendix 2. We also searched some communication journals individually through the Social Science Citation Index, but have not repeated this for the current update, as it did not yield additional studies in previous versions of the review.
The Register contains a variety of studies published in foreign languages. We did not exclude trials on the basis of language or publication date.
Data collection and analysis
For this update, from the title, abstract, or descriptors, a combination of two review authors (from KC, FS, KS) reviewed all literature searches. We excluded all studies that were clearly not RCTs, controlled clinical trials (CCTs) or interrupted time‐series or that clearly did not fit the inclusion criteria. We then independently reviewed all other citations in full text, assessing for inclusion based on study design, population, intervention and outcome.
We reached the decision not to attempt a quantitative synthesis of the study results by an a priori assessment of the large number of sources of possible heterogeneity amongst studies likely to be eligible. These include features of the programme under evaluation, such as type of media used, target audience, and duration and intensity of the intervention. Study variables including design, measures of smoking behaviour reported and length of follow‐up would also contribute to potential variation in outcome.
Where necessary, we have contacted authors for clarification on individual studies. We present information on each study in the 'Characteristics of included studies' tables. We report individual results for all studies with statistically significant differences in outcomes between intervention and control groups in the 'Data and analyses' tables.
Data extraction and management
For this update, two review authors (from KC, FS and KS) independently extracted data for the trials using a standardized data extraction form before data were entered into the Cochrane software programme Review Manager 5. KC and the previous review authors corresponded with authors of the included studies to obtain missing and raw data. We also obtained data from the authors of Flynn 1995, Hafstad 1997 and Worden 1983.
Assessment of risk of bias in included studies
We assessed the risks of bias using the Cochrane 'Risk of bias' assessment tool, in line with the recommendations made in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), which includes allocation sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other potential threats to validity in the studies. We also include four supplementary categories as recommended by the Effective Practice and Organisation of Care (EPOC) guidelines, due to the nature of the intervention, and the potential increase in risk of bias in these sorts of studies (EPOC 2009). These include imbalance of outcome measures at baseline, comparability of intervention and control group characteristics at baseline, protection against contamination, and selective recruitment of participants.
Data synthesis
We entered data into Review Manager 5 software. We analyzed the studies using narrative synthesis.
'Summary of findings' table
Following standard Cochrane methodology, we created a 'Summary of findings' table for all of the review outcomes, and used the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the quality of the body of evidence for each outcome, and to draw conclusions about the quality of evidence within the text of the review.
Results
Description of studies
A detailed description of each included study is available in Characteristics of included studies. Details about the excluded but possibly relevant studies are also available, with reasons for exclusion: see Characteristics of excluded studies.
Results of the search
Eight studies met all of the inclusion criteria, from 1326 records (after duplicates were removed; see Figure 1). Seven of the included studies used a controlled trial design, whilst one 2015 study, identified from the most recent update of the literature search, conducted an interrupted time‐series evaluation. We also found two new excluded but relevant studies in this search, bringing the total up to 80.

Study flow diagram.
Included studies
All studies investigated the effect of a mass media prevention effort directed at young people (under 25 years of age). The eight studies were published between 1983 and 2015. Seven studies originated from the USA (Bauman 1991; Fallin 2015; Flay 1995; Flynn 1995; Flynn 2010; Longshore 2006; Worden 1983), and one from Norway (Hafstad 1997).
Participants
Approximately 52,746 participants were included in these eight studies. Clusters were reported in two different ways: one was at the level of community (n = 6), which included standard metropolitan statistical areas (SMSAs), nightclubs and counties (studies in this classification included Bauman 1991, Flynn 1995, Fallin 2015 and Hafstad 1997). The other method of clustering was at the school level (n = 338), ranging from middle‐ to high‐school students (used by Flay 1995, Flynn 2010, Longshore 2006 and Worden 1983).
Participants varied across studies; some studies targeted specific high‐risk groups such as girls (Hafstad 1997) or young people at higher risk of becoming smokers, as defined by parental education and income level (Flynn 1995). The age of the targeted participants also varied, ranging from nine to 26 years across the different studies.
Follow‐up
Overall follow‐up time periods ranged from 18 months (Worden 1983) to six years (Flynn 1995) post‐baseline. However, in some cases the time line was not clear.
-
In Bauman 1991 the follow‐up was two years after baseline, 11 to 17 months after the broadcast and two to eight months after the mailed intervention.
-
The Fallin 2015 study, which used an interrupted time‐series model, followed cohorts in the study in three consecutive years (2010 to 2012).
-
Measurement of smoking behaviour in Flay 1995 was immediately after the six‐week intervention period, plus one‐ and two‐year follow‐ups (approximately 28 months after the baseline survey).
-
Flynn 1995 measured smoking behaviour at five points in time after the first baseline survey. The first three measurements took place during the intervention, one immediately post‐intervention and the final measurement two years after the four‐year intervention had been completed.
-
The later Flynn 2010 study measured the population at baseline and then four years later. The intervention continued for the duration of the study period.
-
Hafstad 1997 measured smoking behaviour four years after the baseline survey, one year after the third and final campaign.
-
Longshore 2006 followed up participants for two years, although the media intervention ran intermittently for the entire duration of the study period.
-
Worden 1983 had follow‐up at 12 months from baseline (after two of the three campaigns) and at 18 months from baseline (immediately after completion of all three campaigns).
Characteristics of interventions
Four studies used mass media interventions alone (Bauman 1991; Flynn 2010; Hafstad 1997; Worden 1983), three studies used mass media together with a schools‐based educational component (Flay 1995; Flynn 1995; Longshore 2006), and one combined social media peer‐led anti‐tobacco messaging in nightclubs (Fallin 2015). The theories on which the campaigns were based differed between studies, although most used aspects of the social influences or Social Learning Theory approach. The intensity and duration of the individual media campaigns varied greatly between studies.
Bauman 1991 evaluated the effect of radio messages about the expected consequences of smoking, together with a TV, radio and mailed brochures component to stimulate personal encouragement not to smoke, over a 15‐month period. The most recent Flynn 2010 study used Social Cognitive Theory. Hafstad 1997 evaluated the effect of a three‐week prevention media campaign shown annually for three years, based on provocative emotional appeals (where emotional reactions are thought to influence behaviour), which mainly targeted girls. Worden 1983 evaluated smoking prevention messages broadcast on TV, which were based on the social influences approach, for three 13‐week periods over an 18‐month period overall.
In Flay 1995 schools‐based programmes that emphasized skills to resist social influences to smoke were combined with TV segments, which were broadcast over a period of six weeks. Flynn 1995 tested the effect of adding TV and radio spots to schools‐based smoking prevention programmes based on the Social Learning Theory approach, at regular intervals over a four‐year period. Longshore 2006 used a combination of the social influences theory, combined with the health belief model (HBM) and self‐efficacy theory of behaviour change, using six months of in‐school curriculum plus a campaign which ran intermittently throughout the follow‐up period; the campaign went 'national' for one year between July 1998 and July 1999, and during a third phase which ran from September 1999 to Spring 2004.
Finally, Fallin 2015 conducted a social media campaign (YouTube, Twitter and Facebook) underpinned by a social branding intervention model conducted over three years.
Five of the studies purchased broadcasting time (Bauman 1991; Flynn 1995; Flynn 2010; Hafstad 1997; Worden 1983). Purchased broadcasting time allows more control over when messages are aired and therefore offers more scope for achieving optimal exposure of the message to the target audience.
Outcomes measured
All studies assessed smoking behaviour by self‐report, with one study (Bauman 1991) validating its findings biochemically, using alveolar carbon monoxide (CO) and saliva thiocyanate levels. Two studies used 'bogus pipeline' measures (where participants are told that samples of their saliva will be analyzed for thiocyanate levels and may be used to verify self‐reports of smoking status), in addition to self‐reported data (Flay 1995; Flynn 1995).
A number of different intermediate outcomes, such as knowledge about the effects of smoking, attitudes towards smoking, and intentions to smoke in the future, were assessed in seven of the eight studies (the exception being Fallin 2015). Process measures such as programme reach were recorded in six of the studies (Bauman 1991; Fallin 2015; Flynn 1995; Flynn 2010; Longshore 2006; Worden 1983).
Excluded studies
We considered 80 studies published between 1963 and 2014 to be relevant, but they did not meet all of the inclusion criteria for this review. We give the reasons for exclusion in the Characteristics of excluded studies tables.
Risk of bias in included studies
We summarize the key features for risks of bias in the eight included studies in Figure 2, as well as in the 'Risk of bias' tables in the Characteristics of included studies sections. Although we assessed the eight studies as meeting the criteria for inclusion in this review, there were important methodological limitations in all studies, discussed below. The review authors (a combination of KC, KS and FS) reached agreement on the assessment of risks of bias in accordance with Cochrane standard practice, as given the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
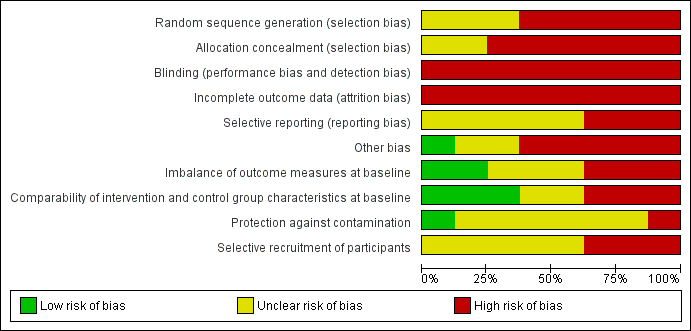
Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.
Sequence generation
Sequence generation was unclear in three studies (Flay 1995; Flynn 2010; Longshore 2006), and at high risk in the remaining five (Bauman 1991; Fallin 2015; Flynn 1995; Hafstad 1997; Worden 1983).
Methods for choosing intervention and control areas varied across studies and were influenced by the availability of non‐overlapping broadcast regions and by the prohibitive cost of advertising in some areas. Methods for selecting respondents varied between studies, and were largely dependent upon whether a schools‐based component was included in the intervention. When interventions were a combination of mass media and schools‐based programmes respondents were students within the intervention and control schools (Flay 1995; Flynn 1995; Longshore 2006).
In those studies where the mass media campaign was the only intervention, methods of selecting respondents differed. In Bauman 1991, a cluster sampling procedure was used to identify a probability sample of households within each SMSA. Households were then screened for young people aged 12 to 14 years. This resulted in a sample of 2534 eligible respondents, of whom 83% participated in baseline measurement. Hafstad 1997 included all young people aged 14 to 15 years from the two communities allocated to intervention and control groups. Worden 1983 selected respondents from 93 schools, although no information is given as to how the schools were selected and no intervention was carried out within the schools. Flynn 2010 used designated market areas (DMAs) to match four pairs of metropolitan areas across four states, with a total of 98 middle‐ and high‐school clusters available for evaluation at four‐year follow‐up. These selections were focused on districts serving lower‐income and lower‐education populations. Fallin 2015 recruited youth at social events/locations (10 HAVOC events occurred each year over three years).
Allocation concealment
Allocation concealment was unclear in two studies (Flay 1995; Flynn 2010) and at high risk in the remaining six (Bauman 1991; Fallin 2015; Flynn 1995; Hafstad 1997; Longshore 2006; Worden 1983).
Blinding for participants and outcome assessors
All studies were at high risk for blinding of participants due to the nature of the intervention. No authors mentioned an attempt to conceal allocation from outcome assessors.
Incomplete outcome data
Incomplete outcome reporting of data could not be excluded in any of the seven controlled trials and we rated all of them at high risk of bias due to a lack of information from individual study authors. Rates of attrition varied between the seven controlled studies, which could in part be due to differences in the length of follow‐up. The study with the longest duration and follow‐up also had a high rate of attrition (62% at six‐year follow‐up) (Flynn 1995). Attrition rates were also higher in those studies that only included participants in the analysis if they had been present for all of the measurement sessions.
Some studies gave percentages of dropouts according to the reason for non‐response; for example, in Flynn 1995 82% of dropouts left the community or transferred to private schools and three per cent were refusals to participate in further assessments. Some studies reported differences between those lost to follow‐up and those who were available throughout the intervention period. For example, significantly less baseline smoking was reported in those available at follow‐up compared with those lost to follow‐up (1.3% versus 5.1%, P < 0.01) (Flynn 1995).
Selective outcome reporting
Selective reporting was unclear in five studies, due to a lack of information reported in the publications (Fallin 2015; Flay 1995; Hafstad 1997; Longshore 2006; Worden 1983), and at high risk in the remaining three studies (Bauman 1991; Flynn 1995; Flynn 2010). For example, in Bauman 1991 additional data collected were not presented in any of the publications and data from 1000 adolescents were excluded from the analysis.
Imbalance of outcome measures at baseline
Three studies (Bauman 1991; Flay 1995; Hafstad 1997) failed to address an imbalance in outcome measures at baseline, three studies (Fallin 2015; Flynn 1995; Worden 1983) were unclear, leaving two studies (Longshore 2006; Flynn 2010) which adequately addressed this outcome. For example, in Bauman 1991 significant differences in smoking rates were observed, which were at higher significance levels following adjustments to the data. In Flay 1995 the control group were reported to be more likely not to start smoking at baseline, while Hafstad 1997 reported more male daily smokers in the intervention county at baseline than in the control area.
Comparability of intervention and control group characteristics at baseline (i.e. similar characteristics of participants in each study arm)
Comparability of interventions at baseline for participant characteristics was unclear in two studies (Fallin 2015; Hafstad 1997), at high risk in three (Bauman 1991; Flynn 1995; Worden 1983) and addressed in three (Flay 1995; Longshore 2006; Flynn 2010).
In Bauman 1991 there was substantial variation in baseline smoking rates between SMSAs, with smoking levels ranging from 0.6% to 5.2%. This occurred despite selecting regionally‐matched communities and adjusting statistically for 10 sociodemographic and personality correlates of adolescent cigarette smoking. However, in some of the included studies minimal or no differences were reported between groups at baseline. For example, Flynn 1995 found differences between groups in the percentage of female participants (52% versus 47%, P = 0.02) and in the ages of participants (10.7 versus 10.8 years, P = 0.002), but no differences in a number of other variables measured at baseline in the same study. The reason for these statistically significant differences is probably to do with the statistical power of the large sample size, rather than differences of clinical significance. In addition, differences found were adjusted for in subsequent analyses.
Protection against contamination
Protection against contamination was unclear in six studies (Bauman 1991; Fallin 2015; Flynn 1995; Hafstad 1997; Longshore 2006; Worden 1983); one was adequately addressed (i.e. no contamination) (Flay 1995), and one study reported significant contamination within the control populations (Flynn 2010). However, due to the nature of mass media interventions, it is very difficult to find a comparable control group that is not exposed to the intervention media.
In Flynn 2010, authors report significant contamination through state‐funded tobacco control programmes via the Master Settlement Agreement (MSA) running for the duration of the study period (2000 to 2005). During 2002, the first campaign year for this research project, these states spent an average of 26% of the Centers for Disease Control and Prevention (CDC) recommended minimum expenditure on tobacco control programming. The CDC estimated that the median number of state‐funded anti‐tobacco advertising exposures among youth increased from 0.04 a month in 1999 to 0.80 in 2002. Furthermore, a large national youth‐focused anti‐tobacco media campaign, also funded by the MSA, began in 2000. Authors report that this campaign was active in all of the intervention and comparison DMAs at a high level of intensity throughout the intervention campaigns.
Selective recruitment of participants (i.e. selection bias or representation of community, or both)
Selective recruitment of participants could not be excluded in three studies (Bauman 1991; Flay 1995; Hafstad 1997), and was unclear in five (Fallin 2015; Flynn 1995; Flynn 2010; Longshore 2006; Worden 1983). Among those with a high risk of bias for selective recruitment, the Bauman 1991 study populations were selected based on location and community traits to reduce overlap/contamination. Students were recruited by phone at random, but the selection methods were not described. Personal contacts were made for one intervention group (RPEER) more than any other. In Flay 1995 n‐values varied depending on the number of participants available for each outcome, i.e. those with data in one outcome but not in another were still included in that one outcome. Finally in Hafstad 1997 the participant cluster site was selected by study staff.
Other potential threats to validity
Five studies had other potential threats to validity (Bauman 1991; Flay 1995; Flynn 1995; Hafstad 1997; Longshore 2006), as described below under 'statistical analysis', two (Worden 1983; Fallin 2015) were at unclear risk due to insufficient reporting of information in the publications, and one was free of other potential threats to validity as it had a published prespecified protocol (Flynn 2010).
Statistical Analysis
Seven of the eight studies allocated either communities, areas or schools to intervention or control groups, while Fallin 2015, which used an interrupted time‐series design, recruited from across several nightclubs and bars. In five studies the main analysis was then presented with the individual as the unit of analysis. All these five studies took account of the unit‐of‐allocation issue in their analyses (Bauman 1991; Flay 1995; Flynn 1995; Flynn 2010; Longshore 2006), but given that randomization occurred at the community/school level with data reported for individuals, the increase in sample size to adjust for clustering effects was not sufficient. For example, one study (Flynn 1995) included the community as a random factor nested within treatment, the school a random factor nested within community and the individual a random factor nested within school. Statistical significance associated with the intervention was determined by using community within treatment as the error term. Similarly, another study (Flay 1995) modelled individual outcomes as three‐level data (students within classrooms within schools), with differences between schools and differences between classrooms treated as random effects and differences between treatments as fixed effects. In Bauman 1991 data were analyzed by area and by individual; the latter examined treatment effects with the area nested within treatment.
Effects of interventions
See: Summary of findings for the main comparison
The summary of findings Table for the main comparison provides an overview of the primary outcome.
Primary outcome
We have evaluated eight different mass media programmes as a method of preventing the uptake of smoking in young people. We found three of the eight interventions (n = 17,385) to be associated with reductions in smoking behaviour (Flynn 1995; Hafstad 1997; Longshore 2006), whilst the remaining five (n = 72,740) showed no evidence of an effect (Bauman 1991; Fallin 2015; Flay 1995; Flynn 2010; Worden 1983) (see Analysis 1.1). Campaign components are summarized in Appendix 3 and findings are summarized by comparison below.
Mass media campaigns versus no intervention
The first comparison concerned the effect of mass media campaigns, compared with no intervention in influencing the smoking behaviour of young people. Four of the eight studies made this direct comparison (Bauman 1991; Flynn 2010; Hafstad 1997; Worden 1983) and one study used a factorial design (i.e. a design consisting of two or more factors, in which the experimental units take on all possible combinations of these levels across all such factors) in which this comparison was made (Flay 1995).
A provocative media campaign, aimed primarily at girls, designed to create negative affective reactions was carried out in one county in Norway (Hafstad 1997; n = 6234). The effects of newspaper advertisements, posters, TV and cinema spots of three weeks' duration over three consecutive years were compared to a control county receiving no intervention. Comparison areas were matched on variables such as county size, education level, parental income and smoking prevalence. The overall increase in the proportion of female daily smokers at one‐year follow‐up was four per cent lower in the media county than in the control county (8.6% compared with 12.4% respectively, P < 0.01). Although not statistically significant, the same trend was apparent for boys; 6.8% in the intervention county compared with 10.5% in the control county. The odds ratio (OR) for being a smoker in the intervention county compared with being a smoker in the control county was 0.74 (95% confidence interval (CI) 0.64 to 0.86), after adjustment for smoking at baseline and gender.
A difficulty with the interpretation of the findings in this study was the difference in survey response rates between the intervention and the control counties (65% versus 70% respectively). In addition, more of the participants lost to follow‐up in the intervention county were smokers at baseline than in the control county (18% versus 13%). We recalculated the odds of being a smoker, controlling for smoking habits at baseline and taking into account the differences in response rates between the two counties (OR 0.84, 95% CI 0.76 to 0.95). Also, no adjustment was made in the analyses for the community being the unit of allocation and the individual the unit of analysis.
In a second study (Worden 1983; n = 4005), TV messages designed to prevent the uptake of smoking were targeted at 10‐ to 12‐year‐olds within the range of a rural network‐affiliate TV station in the USA, over an 18‐month period. School districts in adjacent counties, which were out of range of the signal, were matched using census data, and formed the control group. At 18‐month follow‐up no statistically significant differences were found in smoking behaviour between the intervention and control counties (numerical data not available).
One study (Bauman 1991, n = 1637) compared three different forms of mass media with a control which did not receive any intervention. Radio messages were used to broadcast the negative consequences of smoking; added to this was the promotion of a sweepstake offer, first using the radio and secondly the television. The sweepstake offer encouraged young people to recruit friends into the contest in the hope that discussion about not smoking would take place. Cluster sampling procedures were used to identify probability samples of households within each area, from whom data were collected. Smoking prevalence increased from baseline to follow‐up (ranging from two to eight months post‐intervention) in all groups, but no significant differences between groups were detected (authors state that F < 1.00 for all groups). There was however substantial variation in baseline smoking between the SMSAs from which the groups were selected (range from 0.6% to 5.2%). This occurred despite selecting regionally‐matched communities and adjusting statistically for 10 sociodemographic and personality correlates of adolescent cigarette smoking. The observed rates of adolescent smoking made detection of effects attributable to the campaigns impossible (Bauman 1991; La Prelle 1992).
Flynn 2010 (n = 23,246) compared four simultaneous campaigns consisting of specially‐developed messages based on behavioural theory (social cognitive theory) and targeting different age groups of racially and ethnically diverse youth. Thirty‐ and 60‐second TV and radio messages were broadcast using purchased time with approximately three to four exposures a week. Approximately 10 messages were chosen for each campaign in 2002. Five additional messages were developed annually for each campaign in 2003 to 2005 (60 in total). Intervention impact on cigarette use in the past 30 days did not show an effect. The 30‐day smoking rates appeared to decline in both groups over the four‐year interval between baseline and follow‐up surveys for participants in both conditions, but this trend was not significant (18.9% to 16.9% for intervention; 17.8% to 15.5% for comparison). Similar results were obtained for seven‐day prevalence (weekly smoking) (15.0% to 13.1% for intervention; 13.6% to 11.6% for comparison).
Mass media campaigns combined with schools‐based programmes versus no intervention
The second comparison concerned the effect of mass media campaigns combined with schools‐based programmes compared with no intervention in influencing the smoking behaviour of young people. No study tested this comparison directly, although one study used a factorial design in which this single comparison was made (Flay 1995) (discussed separately).
Mass media campaigns combined with schools‐based programmes versus mass media campaigns alone
The third comparison concerned the effect of mass media campaigns combined with schools‐based programmes compared with media campaigns alone in influencing the smoking behaviour of young people. Only one study addressed this comparison in a factorial design expressing combinations of TV only, TV plus classroom curriculum (CR), CR only, and two control groups: treatment as usual and attention control (Flay 1995) (discussed in detail later).
Mass media campaigns combined with schools‐based programmes versus schools‐based programmes
The fourth comparison concerned the effect of mass media campaigns combined with schools‐based programmes compared with schools‐based programmes alone in influencing the smoking behaviour of young people. Two studies made this direct comparison (Flynn 1995; Longshore 2006) and one study addressed it in a factorial design (Flay 1995).
In Flynn 1995 (n = 2860), students in communities where TV and radio messages were broadcast over a four‐year period combined with a schools‐based programme teaching refusal skills and skills to resist advertising pressure, were found at two‐year follow‐up to be at lower risk for weekly smoking than those in communities receiving only the schools‐based component (OR 0.62, 95% CI 0.49 to 0.78). Communities were matched on variables such as size, education level, income and smoking prevalence. There were, however, a few significant differences at baseline between the groups, with the media plus schools‐based group having more girls (52% versus 47%, P = 0.02), younger participants (mean 10.7 years versus 10.8 years, P < 0.01) and more participants with an older sibling that smoked (15.8% versus 11.3%, P = 0.06). These differences were, however, adjusted for in subsequent analyses.
The findings of preliminary research conducted with high‐risk youth were used to develop the TV and radio spots in this study. When smoking behaviour was examined separately for high‐ and low‐risk youth at two‐year follow‐up, a 7.3% difference in weekly smoking prevalence favouring the media‐school group was found in the high‐risk group (28.6% for the media‐school group and 35.9% in the school‐only group) compared with a 4.3% difference favouring the media‐school group in lower‐risk students (15.9% in the media‐school group and 20.2% in the school‐only group). Higher‐risk youths were found to report more frequent use of both radio and TV (Flynn 1995). The success of this programme may have been partly due to the experience gained from an earlier study evaluating the effect of a mass media campaign aimed at preventing the onset of smoking in young people (Worden 1983; n = 4005).
Longshore 2006 (n = 8291) used a combination of school‐based curricula, ALERT (middle‐schools) and ALERT Plus (high‐schools) in addition to an established media intervention, the National Youth Anti‐Drug Media Campaign. This was part of an effort by the Office of National Drug Control Policy to combat illegal drug use among America’s youth by means of an advertising and social marketing programme focusing on the dangers of drug use. This campaign targeted a combination of marijuana, alcohol and tobacco prevention for youth. The ALERT condition was a basic prevention curriculum delivered in seventh and eighth grades, whilst ALERT Plus consisted of the same curriculum with the addition of booster lessons added for ninth and tenth grades (i.e. extra annual lessons), compared to a control condition of no intervention. Overall smoking behaviour favoured both ALERT and ALERT Plus, producing a 19% and 23% reduction respectively in weekly and monthly smokers (P < 0.01) by 18‐month post‐baseline surveys for both groups combined (ALERT and ALERT Plus together). During the same time, cigarette initiation rates in the control schools climbed to 31.6% by the end of eighth grade. However, initiation rates were significantly lower (25.5%) in the ALERT schools by the same time. Notably, any effect of the mass media intervention is confounded by the other ALERT programme components and it is therefore impossible to discern if the observed differences are due to the mass media campaign or to other elements of the ALERT programme.
Another study (Flay 1995; n = 4134) compared five different programmes; TV only, TV plus classroom programme, classroom only, and two control groups ('attention control' and a 'no intervention control') to influence the smoking behaviour of young people. All programmes were based on the social influences approach for prevention and cessation. A blocked randomized design was used to allocate schools within two counties in the USA to either intervention or control conditions. At two‐year follow‐up there were no significant programme effects on smoking behaviour or smoking intentions in any of the intervention groups (Control pretest mean = 2.09 versus two‐year follow‐up = 2.76; TV intervention group pretest mean = 2.06 versus two‐year follow‐up = 2.91). However, it should be noted that the TV component of the programme did not meet the original objectives, in that social resistance skills were not demonstrated in the way that is necessary for adequate learning to take place. Scripted demonstrations of prevention skills were not allowed to be shown due to commercial news organization (Flay 1995).
Time series studies
One study used time series to evaluate the efficacy of a social media campaign (Fallin 2015; n = 3348). Smoking rates did not change in the total sample (44.1% at Time 1, 45.0% at Time 2 and 47.4% at Time 3, P = 0.17); Participants unable to recall HAVOC messages were significantly more likely (P = 0.003) to be daily (OR 1.58, 95% CI 1.16 to 2.17) and non‐daily (OR 1.81, 95% CI 1.43 to 2.30) smokers compared to participants who could recall HAVOC messages. Similarly, 'Partiers' (described as participants who frequently attended nightclubs, desired to engage in ‘exclusive’ experiences such as VIP lounges, were fashion‐conscious, and were concerned with physical attractiveness and achieving social status by exuding an image of confidence and financial success) who recalled HAVOC messaging were significantly less likely to smoke daily than those who could not recall HAVOC messaging (OR 0.30, 95% CI 0.10 to 0.95; P < 0.05).
Secondary outcomes
Overall, the findings relating to intermediate variables including attitudes (Analysis 2.1), intentions to smoke (Analysis 2.2), knowledge (Analysis 2.3), self‐efficacy (Analysis 2.4) and smoking perceptions (Analysis 2.5) were inconsistent across studies. In a few cases they improved relative to control conditions, in some studies they did not differ and in others improvement was found in the control groups. This inconsistency was apparent both between and within studies, depending upon the variable that was measured.
Smoking attitudes
Five studies reported on smoking attitudes (Analysis 2.1), with two favouring the intervention, two showing no evidence of any effect and Flynn 2010 favouring the control.
In Flay 1995 (n = 4134) a marginally significant overall effect (P < 0.06) was observed. However there was a significant interaction between television and social resistance conditions at immediate post‐test, (P < 0.03). In San Diego there was more positive change in the social resistance condition, (P < 0.003) toward disapproval of parental smoking (Intervention description 4 in Characteristics of included studies table). In Flynn 1995 (n = 2860), attitudes towards smoking (change score of 0.37 versus 0.25 on a multiple‐item Likert scale, P < 0.05) changed in a positive direction in the media‐schools group compared with the schools‐only group. When analyzing attitudes in Flynn 2010 (n = 23,246), positive outcome expectation scores increased significantly over time in both study groups, an unfavourable change, whilst negative outcome expectation scores decreased in the comparison but not in the intervention group, although this was not statistically significant.
Smoking intentions
Four studies assessed intentions (Analysis 2.2), with two studies favouring the intervention and two showing no evidence of any effect. In Hafstad 1997 (n = 6234) statistically significant differences were found between the intervention and control groups in intentions to smoke in the future. Nine per cent of the intervention group compared with 13% of the control group reported that they expected to be a smoker within three years (P < 0.01). In Flynn 1995 (n = 2860) a significant difference in change over time was found between girls in the two treatment groups, with a lower increase among girls in the media‐school communities in intentions to smoke cigarettes (P < 0.01). In the more recent Flynn 2010 (n = 23,246), however, intentions to smoke declined in both intervention and control groups, but this was not statistically significant.
Smoking knowledge
Only one study (Flay 1995) reported on knowledge, producing a negative finding. By two‐year follow‐up, greater knowledge was found in the health information‐based control group compared to the three intervention groups.
Self‐esteem/self‐efficacy
Two studies reported on self‐esteem/self‐efficacy, producing no evidence of any effect (Flay 1995; n = 4134; Longshore 2006; n = 8291). In Flay 1995 the intervention group that received social‐resistance training significantly increased their social‐resistance skills knowledge relative to other groups (P < 0.01), but actual refusal self‐efficacy did not differ significantly between groups.
Smoking perception
Four studies reported on smoking perceptions, two of which found no evidence of any effect (Longshore 2006; n = 8291; Flynn 2010; n = 23,246), whilst the other two favoured the intervention (Flay 1995; n = 4134; Flynn 1995; n = 2860). In Flynn 2010 significant favourable changes were identified in both study groups for perceived peer prevalence and peer norms, whilst in Longshore 2006 neither group changed significantly. Smoking norms in Flynn 1995 (4.94 versus 5.56, P < 0.05) changed in a positive direction in the media‐schools group compared with the schools‐only group. For Flay 1995 there were significantly lower prevalence estimates for social peer resistance (P < 0.001) and television (P < 0.006) conditions. At two years the main effect of the social resistance conditions remained. However, the presence of a significant interaction between the television and social resistance conditions (P < 0.05) indicated that the lower prevalence estimates of the social resistance condition was increased in the television plus social resistance condition.
Process measures
Programme reach varied in the five studies where it was recorded. In one study 81% of those in the intervention group reported hearing or seeing at least one of the TV or radio messages (Brown 1990; Bauman 1991; n = 1637). In another study (Worden 1983; n = 4005), recall was presented according to whether participants were light or heavy TV viewers. In those who were light viewers recall of messages was 32% compared with 57% in heavy users. Longshore 2006 (n = 8291) reported 77% viewing by young people of at least one anti‐drug advertisement a week. More specifically, recall of television advertisements aired by the campaign had increased over time from 37% in 2000 to 76% in 2003. In Flynn 2010 (n = 23,246), grades seven and eight intervention youth recorded a 41% recall for TV messages and 32% for radio, whilst grades nine to 12 youth recorded 32% recall for TV messages and 37% for radio.
Cost effectiveness
Only one of the included studies reported any information about the costs involved in broadcasting a media campaign (Flynn 1995; n = 2860; Secker‐Walker 1997). The cost of developing and broadcasting the campaign was USD 759,436 and the cost per student potentially exposed was USD 41. The cost per student averted was USD 754 (95% CI USD 531 to USD 1296) and the cost per life‐year gained discounted at 3% was USD 696 (95% CI USD 445 to USD 1296). This cost per life‐year gained was reported to compare favourably with other preventive and therapeutic strategies.
Discussion
Summary of main results
To summarize, three out of eight studies demonstrated statistically and clinically significant reductions for smoking uptake in young people. The remaining five studies did not detect a statistically significant effect. Common features in these successful campaigns included multiple channels for media delivery (e.g. newspapers, television, radio, posters, etc.), combined school and media components (through school posters or school‐based curricula, or both), and repeated exposure to campaign messages consecutively delivered for the same cohort of students over a minimum period of three years. Two of the three successful campaigns were based on the 'social influences' or 'social learning theory' approach, one of which also incorporated the HBM. The other successful campaign used provocative messages to cause effective personal reactions. However two of the remaining five studies, which did not produce any statistical benefit, also used the social influences approach. Two of the five unsuccessful studies had short campaign durations (two weeks for one study, and four weeks for another), and were less intense than the successful campaigns. The remaining three studies demonstrating no benefit had longer durations (three periods of 13‐week television smoking prevention messages ‐ 39 weeks in total; Flynn 2010 ran for the full four‐year study period, whilst the more recent Fallin 2015 included multiple events over three years). However, the lack of a structured curriculum component to support these messages, such as those in the combined school‐based studies, is one possible explanation for the eventual failure in preventing the uptake of smoking in young people.
It has been suggested that a number of mass media campaigns have failed to achieve their objectives as they were not adequately piloted prior to implementation (Chollat‐Traquet 1996). However, most of the studies included in this review devoted considerable time and resources to the development and refinement of intervention components (formative research). In most studies data were collected from groups of people who represented the potential target audience, for example in both the Flynn studies the messages were developed from intensive diagnostic surveys and focus groups with the target population. Depending upon the response from group participants, modifications were made to specific components of the campaign. New sets of spots were created on an annual basis to keep pace with the changing interests of the target audience (Flynn 1995; Flynn 2010). Similarly, one study found that the preferences differed for either radio or TV, depending upon the age of the participants, with older youths preferring the radio (Worden 1983). Worden 1983 tested the appropriateness of the time of broadcast in reaching the target audience during the developmental stage of the programme. Qualitative formative research was also conducted in Fallin 2015, through six two‐hour focus groups among 43 participants. From this research, six different peer crowds were identified (i.e. country, hipster, lesbian, gay, bisexual and transgender (LGBT), partier, mainstream and urban), which then directed the focus of the intervention.
The importance of adequate design and development prior to the launch of any media campaign is emphasized in the Social Marketing Approach. This approach attempts to apply the principles of advertising and marketing to the 'selling' of positive health behaviours (Wallack 1990). Emphasis is placed on the involvement of small groups of representative samples of those at whom the campaign is directed. Such groups might, for example, be involved in message development. This approach gives a strong focus to consumer needs and differs from other approaches where message development was carried out with little input from the intended audience.
The three successful campaigns were similar in intensity and duration, which was more varied across the studies which did not report positive findings. In Flynn 1995 there were averages of 190 TV, 350 cable TV and 350 radio spots purchased in each of the four years during which the campaign was running. Similarly, 167 TV and cinema spots were shown in each of the three annual campaigns described by Hafstad 1997. Longshore 2006 used the National Youth Anti‐Drug Media Campaign, which ran for six‐and‐a‐half years and used television (local, cable, and network), radio, websites, magazines, movie theatres and several other media. In comparison, both the intensity and duration of the campaigns in the other studies were much reduced. Both the intensity and duration of any campaign are likely to be important factors in influencing health‐related behaviour. A review assessing the effect of the mass media as a smoking cessation intervention with adults also found that campaigns that were more intense in reach, frequency and duration were the most effective in reducing smoking rates (Flay 1987b).
Two of the three studies reducing smoking behaviour targeted specific populations; Hafstad 1997 targeted girls, while Flynn 1995 targeted higher‐risk groups, defined by parental education attainment and income levels. Longshore 2006 also presented data in subanalysis based around high‐risk populations. Worden 1983 also targeted girls, who had higher baseline smoking rates than boys. There are large and persistent racial, gender and class differences in smoking rates (Cleary 1988). Rates of smoking have been reported to vary among subgroups within the teenage population (Babar 2010; Badovinac 1995). In the UK, socio‐economic differences in smoking rates have been reported in the 16‐ to 24‐year‐old age group. For example, smoking rates among non‐manual groups is 25%, compared with 35% for manual groups (HEA 1997). Most media campaigns to date have not specifically targeted high‐risk groups.
Overall completeness and applicability of evidence
Based on an assessment of the most methodologically rigorous set of studies evaluating the effect of mass media campaigns directed at youth, there is some evidence that some media campaigns can be effective in preventing the uptake of smoking in young people; however the evidence is not strong and contains a number of methodological flaws, and most of the studies did not detect an effect. Moreover, inclusion of only eight studies presented in such a way as not to facilitate presentation as a meta‐analysis further reduces our ability to draw reliable conclusions based on the available evidence. Findings from this review should therefor be interpreted with caution, and the questions posed by this review remains unanswered.
In addition, most of the media programmes described in the included studies were made up of several different components, including the use of different media channels such as television, radio, newspapers, etc. However, most programmes did not assess the independent effect of the separate components. There is therefore little information about which aspect of the campaign had the most impact with which group(s). It is also important to note that any influence mass media may have on the prevention of adolescent smoking may be negated by social, family and peer pressures in each individual's environment, as noted by Wakefield 2003. This study also concluded that anti‐smoking advertising appeared to have more reliable positive effects on those in pre‐adolescence or early adolescence by preventing smoking uptake. Furthermore, reaching youth through the tried and tested mass media outlets as outlined in this review is becoming more difficult, with rapid advances in communications and technologies such as TIVO, which allows viewers to skip over advertisements. Other media outlets popular with youth need to be targeted for future campaigns, such as social media, including Facebook, Instagram, Snapchat and Twitter. For example, a study in Greece piloted a Facebook‐integrated educational intervention in a single high school among 225 students aged 15 to 18 years. The lecture was designed to stimulate social mobilization in online networks. Three days after the lecture, 15.9% of students had posted a smoking‐related sentence in their Facebook account which was spread as a note on their wall through news feeds, reaching a cumulative total of 20,095 Facebook friends (Kousoulis 2016).
Quality of the evidence
As shown in summary of findings Table for the main comparison, we rated the overall quality of the evidence in this review as very low according to GRADE standards. This is due to inconsistency in study characteristics and findings, and to serious issues with risks of bias. All the included studies in this review had at least four significant methodological limitations based on the 'Risk of bias' assessments (see Figure 2 and Risk of bias in included studies). Findings from these studies should therefore be interpreted with caution, given the general limitations of primary research in this area. A problem common to several of the studies is the allocation of communities, areas or schools to intervention or control, followed by analysis at the level of the individual. Individuals are often used as the unit of analysis because this increases the power of the study, which in turn gives a greater chance of finding positive programme effects. Ignoring the correct unit of analysis may lead to spurious positive findings (Altman 1997). Study participants should not be treated as independent individuals, as it is likely that participants within a community will be more alike than a random sample of participants from several communities. Two sources of variation exist: that between individuals in a community and that between communities. The variability between communities must be taken into account in the analysis (Bland 1997). One way of overcoming this problem is to correct at the individual‐level analysis for community‐ or school‐level variation using multilevel data. Five of the included studies accounted for the unit of allocation in their analyses (Bauman 1991; Flay 1995; Flynn 1995; Flynn 2010; Longshore 2006).
Due to the nature of the intervention it is not possible to blind participants to the intervention they receive. Although the individual student's awareness may not have a direct effect on the outcome, the staff and teachers at schools may introduce a bias into this population, as evidenced in Bauman 1991, where 85% of the population in one school enrolled after a teacher had been assigned by the principal to serve as school co‐ordinator for the local 'Great American Smokeout', sponsored by the American Cancer Society. She heard the sweepstakes offer on the radio, obtained a copy of the broadcast tape from a local radio station, played the tape over the school's electronic announcement system, and then organized the mail‐in campaign. Control group participants may therefore have been exposed to the radio segments.
Differences at baseline between control and intervention communities was a problem common to many of the studies, making it difficult to attribute any differences at follow‐up to the intervention alone. Differences at baseline between the groups may cause different rates of change in the outcome of interest. Attrition was also a problem common to most studies in this review, and ranged from 22% to 62%. When the effect of an intervention is expected to be small or the incidence of a behaviour is low, or both conditions apply, as with adolescent tobacco use, collecting follow‐up data from as many participants as possible is vital for achieving adequate statistical power to be able to determine the effect of the intervention (Morrison 1997). The results reported in the eight studies tended to be based on outcome data relating to a subsample of participants rather than on the basis of allocation to groups. Evaluation of effect on the basis of data provided by those participants available at follow‐up is likely to be biased. For example, in three studies dropouts were reported as more likely to be smokers or at risk of becoming a smoker, than those respondents available at follow‐up (Bauman 1991; Flynn 1995; Hafstad 1997). In addition, in one study (Flynn 1995) significantly less baseline smoking was reported in those available at follow‐up compared with those lost to follow‐up (1.3% versus 5.1%, P < 0.01). This is particularly problematic when there are more dropouts who are at risk in the intervention group than in the control group. This was the case in Hafstad 1997, where 18% of those lost to follow‐up were smokers in the intervention group, compared with 13% in the control group. We recalculated the odds of becoming a smoker, controlling for smoking habits at baseline and assuming that the proportion of smokers who dropped out in the intervention group was three times higher than among the respondents. We assumed that the proportion of smokers who dropped out from the control group was twice as high as among respondents. The OR for being a smoker in the intervention group compared with the control group was then 0.84 (95% CI 0.8 to 0.9).
Potential biases in the review process
Despite the problems common to most of the studies which met the inclusion criteria for this review, they represent the most methodologically rigorous set of studies evaluating the effect of the mass media in influencing the smoking behaviour of young people. We had to exclude many studies relating to smoking prevention campaigns, due to design issues or simply that no smoking‐related outcomes were reported (See Characteristics of excluded studies table). In particular, we excluded one previously included study due to an inadequate comparison between groups. The intervention population was made up of self‐selected schools and the control group contained schools which did not respond to the invitation to participate (Flay 1987a), thus affecting the validity of comparing groups. Another study (Sly 2001), which examined the Florida "truth" campaign met all the inclusion criteria, but we excluded it just before completion of this review as no information was presented or available for the control population at follow‐up. Other evaluations of this campaign could also not be included for the same reasons. Campaigns have frequently either not been evaluated, i.e. they are merely described, or evaluation has been by a survey of the number of people who report awareness of the campaign. We had to exclude one of the most expensive media campaigns in the smoking field, due to a lack of proper evaluation. The California Tobacco Education Media Campaign cost USD 28.6 million, funded out of a state‐mandated charge on cigarettes. Evaluation consisted of comparing smoking behaviour pre‐ and post‐intervention in different samples, including school‐age youths, plus comparisons between students who reported being unexposed and exposed to the campaign (Popham 1994).
As we found only eight studies for inclusion within the review it is difficult to determine the extent to which the results can be generalized. It is also possible that we may have missed unpublished programme evaluations which may have met our inclusion criteria; given the absence of study registers for these sorts of assessments, we were unable to systematically search the 'grey' literature for unpublished studies.
Agreements and disagreements with other studies or reviews
A Cochrane Review of mass media interventions for smoking cessation in adults included 11 studies, with evidence of benefit for the mass media campaigns (Bala 2013). Of these studies, only three did not show significant decreases in smoking. The authors report that the intensity and duration of mass media campaigns are likely to influence efficacy. However, they found no consistent relationship between campaign effect, age, education, ethnicity or gender. Another Cochrane Review evaluating mass media campaigns for preventing illicit drug use amongst youth included 23 studies, but because of varying scales used to assess outcomes could not formulate a reliable conclusion (Ferri 2013; Allara 2015). Pooled results from five randomized controlled trials did not identify any effect for the mass media intervention. A third Cochrane Review (Thomas 2013), focusing specifically on school‐based programmes for preventing smoking in youth, included 134 studies, with tobacco prevention cohorts producing a significant effect at longest follow‐up for the school‐based programmes (average 12% reduction in starting smoking compared to the control group). However, at one year or less no overall effect was detected. Studies that combined social competence with social influence interventions were the most effective, while the least effective were those using only social influences, multimodal interventions and information‐only interventions. Another study focusing specifically on adolescents from a tribal area in India found that school programmes may have some limitations due to high‐school dropout and low enrolment (Zahiruddin 2011). This highlights the need for a broader message delivery system such as mass media that does not rely solely on the school system.
A review examining the equity impact of interventions and policies for reducing smoking in youth (Brown 2014) identified 38 studies involving various interventions, including smoke‐free policies, taxation, mass media campaigns, advertising controls, access restrictions, etc. Very few of these studies assessed the equity impact (consideration of populations with lower socioeconomic status and minority groups), highlighting a gap in the current literature. Another review of 34 studies (Allen 2015) evaluating the potential effect of anti‐tobacco media campaigns across racial/ethnic populations with consideration of the socio‐economic status of participants confirms these findings. Despite the large number of included studies, the authors concluded that there was insufficient evidence to determine whether campaign outcomes differ by socio‐economic status and population density. One Cochrane Review of three studies focusing specifically on tobacco prevention for Indigenous youth found some potentially problematic results, with more participants in the control population of one included trial reporting less smoking at final follow‐up compared to those in the intervention group (Carson 2012). Authors of that trial confirm that the results were not adjusted for ethnicity, as there were more Indigenous youth in the intervention arm and Indigenous youth were more likely to take up smoking, which would subsequently influence the results (Glover 2009). However, this outcome highlights that tobacco prevention interventions need to be effectively evaluated, as there is potential for harm. This is of particular relevance for large‐scale government‐funded campaigns such as 'The Real Cost', which is an anti‐tobacco media campaign funded by the USA Food and Drug Administration (FDA 2014). To enhance the efficacy and cost effectiveness of these programmes scientific evaluations must be conducted throughout the entire campaign.
In the Allen 2015 review reported above, it is also worth noting that campaigns that were more likely to have messages retained, included those with personal testimonials, a surprising narrative, intense images, sound and editing. Importantly, evidence supporting messages about health consequences were mixed. In the past anti‐tobacco messages using scare tactics have not been successful in deterring initiation of tobacco use or reducing the number of cigarettes smoked by youth (Lantz 2000). It is not a coincidence that tobacco company‐funded anti‐smoking campaigns, such as the Philip Morris ‘Think. Don’t smoke’ campaign, use these scare tactics and have subsequently been associated with poor tobacco prevention outcomes, in some cases leaving youth open to the idea of smoking (Farrelly 2002). These campaigns have a focus on the negative side of tobacco and use standard print brochures, rather than empowerment and new forms of technology. Technology‐based message delivery has the potential to be an effective vehicle for youth health interventions, as there is an opportunity to tailor and individualize, focusing on particular characteristics of the user (e.g. gender, age and heritage), thereby increasing the relevance of the health message and lowering the risk of attrition (Bennett 2009). A 2010 study identified that the average time spent with screen media among eight‐ to 18‐year‐olds is more than twice the average amount of time spent in school each year (Kaiser Family Foundation 2010). Health interventions using (social) media, games and the internet have been found to be effective, specifically when offering more than merely an educational non‐interactive experience (Hieftje 2013).
Previous reviews of the literature have assessed the effect of mass media campaigns in influencing smoking behaviour in young people. They have, however, included other types of intervention such as schools‐based programmes or community initiatives, and have not included all relevant studies in any one area (Farrelly 2003; Friend 2002; Michell 1994; Reid 1995; Reid 1996; Silver 2001; Stead 1996; US DHHS 1994). Overall, these reviews have reported mixed results for the effect of the mass media, particularly for smaller community‐level campaigns. Regardless of this, the potential to influence youth smoking rates has still been demonstrated. There have been other reviews of the literature which have concentrated exclusively on the mass media, but smoking cessation with adult smokers has been the focus (Flay 1987b). These reviews of smoking cessation have concluded that mass media campaigns can reduce smoking rates, particularly campaigns that are more intense in terms of reach, frequency and duration (Flay 1987b; Flay 1987c).
A systematic review of the literature has identified a number of different environmental, sociodemographic, behavioural and personal factors associated with the onset of smoking (Tyas 1997). The peer group, in particular, has been thought to play an important role in influencing smoking behaviour. A key theoretical perspective used to explain the association between peer smoking and adolescents' smoking is the 'social influences' or Social Learning Theory approach, which predicts that young people will anticipate, initiate and adopt smoking as part of the socialization process (Cleary 1988). Social Learning Theory not only explains how people acquire and maintain behaviours but also provides the basis for intervention and behaviour change.
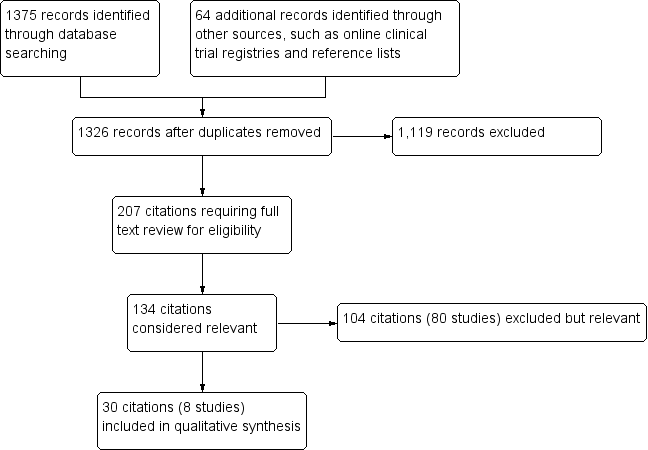
Study flow diagram.

Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.
| Study | Sample size at follow‐up | Outcomes analyzed | Results |
| Bauman 1991 | Clusters n = 2 (SMSAs) Individuals n = 1637 | Weekly and ever‐smoking | Overall outcome ‐ No evidence of an effect Means of all smoking variables changed significantly in the direction of more smoking. No P values are significant (authors state that F > 1.00 in all instances). Data consistent with the conclusion that the campaign did not influence smoking. |
| Fallin 2015 | Clusters n = 33 (nightclubs/bars) Individuals n = 3348 | Daily and non‐daily smoking | Overall outcome ‐ No evidence of an effect Smoking rates did not change across the 3 time periods (P = 0.17), but partiers who recalled the HAVOC intervention had lower daily smoking (OR 0.30, 95% CI 0.10 to 0.95; P < 0.05), compared to those who did not recall the intervention |
| Flay 1995 | Clusters n = 47 (schools) Individuals n = 4134 | Smoker (No quantity) | Overall outcome ‐ No evidence of an effect There were no consistent programme effects on smoking outcomes, suggesting that the treatment was no more or less effective for different groups |
| Flynn 1995 | Clusters n = 2 (communities) Individuals n = 2860 | Daily, weekly and smokeless tobacco | Overall outcome ‐ Favours intervention Significant difference in the school‐and‐media group only within the final 2 years, a consistent trend toward less smoking was noted prior to this. In the 5th year the relative differences for daily smoking was 34% and for weekly smoking 35% between school‐and‐media and school‐only groups. For smokeless tobacco behaviour the 2 groups did not differ significantly, except in the 4th year when the school‐only group was more likely to report use. |
| Flynn 2010 | Clusters n = 98 (schools) Individuals n = 23,246 | Weekly and monthly | Overall outcome ‐ No evidence of an effect The 30‐day smoking rates appeared to decline over the 4‐year interval between baseline and follow‐up surveys for participants in both conditions, but this trend was not significant. Similar results were obtained for 7‐day prevalence. |
| Hafstad 1997 | Clusters n = 2 (counties) Individuals n = 6234 | Daily, weekly, monthly, non‐smoker and smoker (No quantity) | Overall outcome ‐ Favours intervention Among non‐smokers, a significantly lower proportion of adolescents of both genders had started to smoke in the intervention county compared to the proportion in the control county. Among those who were smokers at baseline, significantly more girls in the intervention county had stopped than in the control county, while no significant differences were detected among boys. |
| Longshore 2006 | Clusters n = 100 (schools) Individuals: ALERT n = 4276 ALERT Plus n = 4015 | Weekly and monthly | Overall outcome ‐ Favours intervention ALERT Plus held down current (past month) and regular (weekly) smoking producing a 23% reduction in both measures of use, P < 0.01. Project ALERT curbed current use among the high‐risk experimenters and the even higher‐risk baseline smokers (users) by approximately 20% (P < 0.03), and cut regular (weekly) cigarette use across all 3 groups by anywhere from 19% (P < 0.06) to 39% (P < 0.02). |
| Worden 1983 | Clusters n = 93 (schools) Individuals n = 4005 | Weekly | Overall outcome ‐ No evidence of an effect There were no significant differences in smoking between intervention and control groups. A trend (non‐significant) favouring the intervention group toward a lower level of smoking was noted. P values were not provided. |
Comparison 1 Primary outcomes for Mass media smoking prevention programmes, Outcome 1 Smoking outcomes.
| Study | Sample size at follow‐up | Outcomes analyzed | Results |
| Bauman 1991 | Clusters n = 2 (SMSAs) Individuals n = 1637 | Attitudes toward smoking (total), perceived peer attitudes | Overall outcome ‐ No evidence of an effect No statistically significant post‐campaign differences in attitudes, suggesting that the peer‐involvement component did not impact on those characteristics. |
| Flay 1995 | Clusters n = 47 (schools) Individuals n = 4134 | Disadvantages/negatives (toward parental smoking) | Overall outcome ‐ Favours intervention Marginally significant overall effect (P < 0.06), but there was a significant interaction between television and social resistance conditions at immediate post‐test, (P < 0.03). In San Diego there was more positive change in the social resistance condition, (P < 0.003) toward disapproval of parental smoking (Intervention description 4 in Characteristics of included studies table). |
| Flynn 1995 | Clusters n = 2 (communities) Individuals n = 2860 | Attitude toward smoking (total), advantages/positives, disadvantages/negatives | Overall outcome ‐ Favours intervention A significant difference in change over time was found between girls in the 2 treatment groups with scores increasing less among girls in the media‐school communities, for positive attitudes toward smoking (P < 0.02). |
| Flynn 2010 | Clusters n = 98 (schools) Individuals n = 23,246 | Advantages/positives, disadvantages/negatives | Overall outcome ‐ Favours control Positive outcome expectation scores increased significantly over time in both study groups, an unfavourable change. Negative outcome expectation scores may have decreased in the comparison but not in the intervention group, although this difference was not significant. |
| Longshore 2006 | Clusters n = 100 (schools) Individuals ALERT n = 4276 ALERT Plus n = 4015 | Advantages/positives, disadvantages/negatives, perceived peer attitudes | Overall outcome ‐ No evidence of an effect Neither boys nor girls exhibited significant differences for tobacco cognitions. |
Comparison 2 Intermediate outcomes for Mass media smoking prevention programmes, Outcome 1 Smoking attitudes.
| Study | Sample size at follow‐up | Outcomes analyzed | Results |
| Flay 1995 | Clusters n = 47 (schools) Individuals n = 4134 | Intentions to smoke | Overall outcome ‐ No evidence of an effect There were no significant condition‐related differences at any wave in Los Angeles or San Diego. No consistent programme effects on behaviours |
| Flynn 1995 | Clusters n = 2 (communities) Individuals n = 2860 | Intentions to smoke | Overall outcomes ‐ Favours intervention A significant difference in change over time was found between girls in the 2 treatment groups, with a lower increase among girls in the media‐school communities in intentions to smoke cigarettes (P < 0.01). |
| Flynn 2010 | Clusters n = 98 (schools) Individuals n = 23,246 | Intentions to smoke | Overall outcome ‐ No evidence of an effect Intentions to smoke appeared to decline over the 4‐year interval between baseline and follow‐up surveys for participants in both conditions, but this trend was not significant. |
| Hafstad 1997 | Clusters n = 2 (counties) Individuals n = 6234 | Intentions to smoke | Overall outcomes ‐ Favours intervention A significant difference between the intervention and the control counties was detected regarding expectation of future smoking habits measured in 1995. In the intervention county, 9% expected to be smokers in 3 years, with 13% in the control county (P < 0.01). No significant gender difference was revealed. |
Comparison 2 Intermediate outcomes for Mass media smoking prevention programmes, Outcome 2 Smoking intentions.
| Study | Sample size at follow‐up | Outcomes analyzed | Results |
| Flay 1995 | Clusters n = 47 (schools) Individuals n = 4134 | Tobacco and health knowledge (overall) | Overall outcome ‐ Favours control Tobacco and health knowledge was significantly higher in the attention control group than in any of the other conditions in Los Angeles at the immediate post‐test (P < 0.001), 1‐year follow‐up (P < 0.001) and 2‐year follow‐up (P < 0.001). However, both smokers and non‐smokers in the attention control condition learned more than students in any of the other conditions. Unexpectedly, tobacco and health knowledge also increased in the social resistances programme in San Diego at the immediate post‐test (P < 0.001). However, this effect was not statistically significant at the 1‐ and 2‐year follow‐ups. There were significant differences in the social influences and resistance skills knowledge scale between conditions in Los Angeles at the immediate post‐test (P < 0.001), 1‐year follow‐up (P < 0.001) and 2‐year follow‐up (P < 0.001). The combined television and social resistance condition did not improve as much, relative to the control conditions, as the social resistance condition. |
Comparison 2 Intermediate outcomes for Mass media smoking prevention programmes, Outcome 3 Smoking knowledge.
| Study | Sample size at follow‐up | Outcomes analyzed | Results |
| Flay 1995 | Clusters n = 47 (schools) Individuals n = 4134 (whole sample) n = 2245 for control sample only | Self‐efficacy | Overall outcome ‐ No evidence of an effect Refusal self‐efficacy did not differ significantly between groups for the primary population comparison. In Los Angeles, there were no significant condition‐related effects at any of the waves. In San Diego, refusal/self‐efficacy was unexpectedly improved in the control condition, relative to the social resistance condition, at the immediate post‐test, (P < 0.004). |
| Longshore 2006 | Clusters n=100 (schools) Individuals ALERT n=4276 ALERT Plus n=4015 | Self‐efficacy | Overall outcome ‐ No evidence of an effect Neither group exhibited significant differences for tobacco cognitions. |
Comparison 2 Intermediate outcomes for Mass media smoking prevention programmes, Outcome 4 Self‐esteem/self‐efficacy.
| Study | Sample size at follow‐up | Outcomes analyzed | Results |
| Flay 1995 | Clusters n = 47 (schools) Individuals n = 4134 | Perceived adult smoking, perceived peer smoking | Overall outcome ‐ Favours intervention There were significantly lower prevalence estimates, (peer) for the social resistance, (P < 0.001) and television (P < 0.006) conditions, and at 2 years the main effect of the social resistance conditions remained. However, the presence of a significant interaction between the television and social resistance conditions (P < 0.05) indicated that the lower prevalence estimates of the social resistance condition was increased in the television plus social resistance condition. |
| Flynn 1995 | Clusters n = 2 (communities) Individuals n = 2860 | Perceived norms, perceived adult smoking, perceived peer smoking, perceived sibling smoking. | Overall outcome ‐ Favours intervention A significant difference in change over time was found between girls in the 2 treatment groups with scores increasing less among girls in the media‐school communities, for perceived peer smoking (P < 0.01). This difference was likely due to the slightly older age and greater representation of boys in the school‐only group. A significant difference was evident at grades 5 to 7, that persisted at grades 8 to 10, for perceived norms (P < 0.01). |
| Flynn 2010 | Clusters n = 98 (schools) Individuals n = 23,246 | Perceived norms, perceived peer smoking | Overall outcome ‐ No evidence of an effect Significant favourable changes in both study groups for perceived prevalence and peer norms, but there were no between‐group differences |
| Longshore 2006 | Clusters n = 100 (schools) Individuals ALERT n = 4276 ALERT Plus n = 4015 | Perceived norms | Overall outcome ‐ No evidence of an effect Neither group exhibited significant differences for tobacco cognitions. |
Comparison 2 Intermediate outcomes for Mass media smoking prevention programmes, Outcome 5 Smoking perceptions.
| Mass media interventions for preventing smoking in young people | ||||
| Patient or population: Young people aged less than 25 years Settings: Schools, community groups, television, radio, newspapers, billboards, posters, leaflets or booklets Intervention: Mass media channels of communication intended to reach large numbers of people and which are not dependent on person‐to‐person contact Comparison: Usual care, minimal education, no intervention or co‐interventions | ||||
| Outcomes | Impact | No of Participants | Quality of the evidence | Comments |
| Smoking rates (follow‐up 18 months to 6 years) | 3 (n = 17,385), 1 which compared a mass media intervention to no intervention and 2 which evaluated mass media interventions as adjuncts to school‐based interventions, found that the mass media interventions reduced the smoking behaviour of young people. The remaining 5 studies (n = 72,740) did not detect a significant effect on smoking behaviour. These included 3 studies comparing a mass media intervention with no intervention, 1 study evaluating a mass media intervention as an adjunct to a school‐based intervention, and 1 interrupted time‐series study of a social media intervention. | 90,125 (8 studies) | ⊕⊝⊝⊝ | The 3 campaigns for which a significant effect was detected described a theoretical basis, used formative research in designing the campaign messages, and used message broadcast of reasonable intensity over extensive periods of time. However, some of the campaigns which did not detect an effect also exhibited these characteristics. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||
| GRADE Working Group grades of evidence | ||||
| 1Downgraded two levels due to serious risk of bias: all included studies were rated high risk of bias in at least four domains. | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Smoking outcomes Show forest plot | Other data | No numeric data | ||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Smoking attitudes Show forest plot | Other data | No numeric data | ||
| 2 Smoking intentions Show forest plot | Other data | No numeric data | ||
| 3 Smoking knowledge Show forest plot | Other data | No numeric data | ||
| 4 Self‐esteem/self‐efficacy Show forest plot | Other data | No numeric data | ||
| 5 Smoking perceptions Show forest plot | Other data | No numeric data | ||