Fármacos anticolinérgicos para la discinesia tardía inducida por antipsicóticos
Resumen
Antecedentes
La medicación antipsicótica (neuroléptica) se utiliza ampliamente para tratar a las personas con enfermedades mentales graves. Sin embargo, se asocia con una amplia gama de efectos adversos, incluidos los trastornos del movimiento. Debido a esto, muchas personas tratadas con fármacos antipsicóticos también reciben fármacos anticolinérgicos para reducir algunos de los efectos secundarios asociados con el movimiento. Sin embargo, también se ha propuesto a partir de experimentos con animales de que la administración crónica de anticolinérgicos podría causar discinesia tardía.
Objetivos
Determinar si el uso o la retirada de fármacos anticolinérgicos (benzhexol, benztropina, biperideno, orfenadrina, prociclidina, escopolamina o trihexilfenidilo) son clínicamente eficaces para el tratamiento de personas con discinesia tardía inducida por antipsicóticos y con esquizofrenia u otras enfermedades mentales crónicas.
Métodos de búsqueda
Se recuperaron 712 referencias a partir de las búsquedas en el Registro de Ensayos del Grupo Cochrane de Esquizofrenia basado en estudios, incluidos los registros de ensayos clínicos (16 de julio de 2015 y 26 de abril de 2017). Además, se examinaron las referencias de todos los estudios identificados para obtener más ensayos y se contactó con los autores de los ensayos para obtener información adicional.
Criterios de selección
Se incluyeron los informes identificados en la búsqueda si se trataba de ensayos controlados que trataban de personas con discinesia tardía inducida por antipsicóticos y esquizofrenia u otras enfermedades mentales crónicas que habían sido asignadas al azar a (a) medicación anticolinérgica versus placebo (o ninguna intervención), (b) medicación anticolinérgica versus cualquier otra intervención para el tratamiento de la discinesia tardía, o (c) retiro de la medicación anticolinérgica versus continuación de la medicación anticolinérgica.
Obtención y análisis de los datos
Se extrajeron de forma independiente los datos de los ensayos incluidos y se estimaron los cocientes de riesgo relativo (RR) con intervalos de confianza (IC) del 95%. Se asumió que los pacientes que abandonaron de manera temprana no presentaron mejoría. Se evaluó el riesgo de sesgo y se creó una tabla "Resumen de los hallazgos" con la metodología GRADE.
Resultados principales
La versión anterior de esta revisión no incluía ningún ensayo. A partir de las búsquedas de 2015 y 2017 se identificaron dos ensayos que podrían incluirse. Se asignaron al azar 30 pacientes ingresados y ambulatorios con esquizofrenia en los EE.UU. y en Alemania. En general, el riesgo de sesgo en los estudios incluidos fue incierto, principalmente debido a la deficiente información: no se describió la ocultación de la asignación; la generación de la secuencia no era explícita; los estudios no estaban claramente cegados; y los datos de los resultados no fueron informados en su totalidad.
Los hallazgos fueron escasos. Un estudio informó sobre las medidas de resultado principales y encontró que un número significativamente mayor de participantes asignados a la prociclidina (anticolinérgico) no había mejorado en una medida clínicamente importante en comparación con los asignados a la isocarboxazida (inhibidor de la MAO) después de 40 semanas de tratamiento (1 ECA, n = 20; RR 4,20; IC del 95%: 1,40 a 12.58; evidencia de muybaja calidad); que no hubo pruebas de una diferencia en la incidencia de cualquier efecto adverso (1 ECA, n = 20; RR 0,33; IC del 95%: 0,02 a 7,32; evidencia de muy baja calidad); o la aceptabilidad del tratamiento (medida por los participantes que abandonaron el estudio antes de tiempo) (1 ECA, n = 20; RR 0,33; IC del 95%: 0,02 a 7,32; evidencia de muy baja calidad). El otro ensayo comparó la retirada del anticolinérgico con la continuación del anticolinérgico y no encontró evidencia de una diferencia en la incidencia de la aceptabilidad del tratamiento (medida por los participantes que abandonaron el estudio antes de tiempo) (1 ECA, n = 10; RR 2,14; IC del 95%: 0,11 a 42,52; evidencia de muy baja calidad).
Ningún ensayo informó sobre la confianza social, la inclusión social, las redes sociales o la calidad de vida personalizada ‐ resultados designados como importantes para los pacientes. No se encontraron estudios que compararan i. los anticolinérgicos con el placebo o ningún tratamiento, o ii. estudios sobre la retirada de anticolinérgicos, que informaran sobre el resultado principal "ninguna mejoría clínicamente importante en los síntomas de la DT y de los eventos adversos".
Conclusiones de los autores
Sobre la base de la evidencia actualmente disponible, no se puede hacer ninguna declaración fiable acerca de la eficacia de los anticolinérgicos para tratar a las personas con discinesia tardía inducida por antipsicóticos. Lo mismo se aplica a la retirada de esos medicamentos. Si la retirada de los anticolinérgicos puede beneficiar a las personas con DT inducida por antipsicóticos debe evaluarse en un ensayo aleatorio controlado por placebo de grupos paralelos, con un tamaño de muestra adecuado y al menos 6 semanas de seguimiento.
PICOs
Resumen en términos sencillos
Fármacos anticolinérgicos para las personas que tienen discinesia tardía después de tomar fármacos antipsicóticos
Pregunta de la revisión.
¿Son los fármacos anticolinérgicos o la abstinencia de fármacos anticolinérgicos eficaces en el tratamiento de la discinesia tardía en personas con esquizofrenia u otros problemas similares de salud mental?
Antecedentes.
Las personas con esquizofrenia suelen oír voces y ver cosas (alucinaciones) y tienen creencias que no coinciden con las de las personas sin esquizofrenia (delirios). El tratamiento principal de la esquizofrenia son los fármacos antipsicóticos. Sin embargo, estos medicamentos pueden tener efectos secundarios debilitantes. La discinesia tardía es un movimiento involuntario que causa que la cara, la boca, la lengua y la mandíbula presenten convulsiones, espasmos y muecas. Es causada por el uso a largo plazo o las dosis altas de los fármacos antipsicóticos, es difícil de tratar y puede ser incurable. Muchas personas que están siendo tratadas con fármacos antipsicóticos también reciben medicamentos anticolinérgicos para tratar de reducir algunos de estos efectos secundarios del movimiento. Sin embargo, hay evidencia de experimentos en animales de que los fármacos anticolinérgicos podrían causar discinesia tardía.
Características de los estudios.
La revisión incluye dos estudios aleatorizados pequeños con un total de 30 personas con esquizofrenia que también habían desarrollado discinesia tardía inducida por antipsicóticos. Los participantes en un estudio recibieron el fármaco anticolinérgico prociclidina o el isocarboxácido, un fármaco antidepresivo. A un grupo de participantes del otro estudio se les retiró el fármaco anticolinérgico biperiden, mientras que el otro grupo de participantes siguió tomando biperiden.
Resultados clave.
Hubo escasos hallazgos provenientes de los dos ensayos pequeños y mal informados. No se sabe con certeza si la administración de fármacos anticolinérgicos es útil para el tratamiento de la discinesia tardía en las personas que toman fármacos antipsicóticos. Tampoco se sabe con certeza si la retirada de los fármacos anticolinérgicos mejora los síntomas de la discinesia tardía.
Calidad de la evidencia.
La calidad de la evidencia disponible es de muy baja o baja calidad, limitada y de pequeña escala. No es posible recomendar estos fármacos o su retirada como tratamiento para la discinesia tardía. Para investigar a fondo si la retirada de los fármacos anticolinérgicos tiene algún efecto positivo para las personas con discinesia tardía, se necesitan más datos de investigación de alta calidad.
Este resumen en lenguaje sencillo fue adaptado por los autores de la revisión a partir de un resumen originalmente escrito por Ben Gray, Investigador Principal de la Fundación McPin (mcpin.org).
Authors' conclusions
Summary of findings
| Anticholinergic medication compared with other treatments for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: patients with antipsychotic‐induced tardive dyskinesia Settings: anywhere. Intervention: any anticholinergic Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| risk with placebo | risk with anticholinergic drugs | |||||
| Tardive dyskinesia: not improved to a clinically important extent | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Tardive dyskinesia: deterioration of symptoms | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Mental state | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Adverse effect: any adverse effects | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Acceptability of the treatment: leaving the study early | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Social confidence, social inclusion, social networks, or personalised quality of life | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded one level for risk of bias: the included study did not adequately describe randomisation procedure or allocation concealment, and there was no mention of the study being blinded. 2 Downgraded two levels for imprecision: very small sample size (n = 20). 3 Downgraded two levels for imprecision: very wide CI that includes appreciable benefit for both groups; very small sample size (n = 20). 4 Downgraded one level for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability. | ||||||
| Anticholinergic medication compared with other treatments for antipsychotic‐induced tardive dyskiesia | ||||||
| Patient or population: chronic schizophrenia patients with antipsychotic‐induced tardive dyskinesia Settings: outpatients in the USA. Intervention: procyclidine (anticholinergic), 5 mg twice/day Comparison: isocarboxazid (MAO‐inhibitor), 10 mg twice/day | ||||||
| Outcomes | Illustrative comparative risks* (CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| risk with MAO‐inhibitor | risk with anticholinergic drugs | |||||
| Tardive dyskinesia: Not improved to a clinically important extent | 200 per 1000 | 840 per 1000 | RR 4.20 (1.40 to 12.58) | 20 | ⊕⊝⊝⊝ | |
| Tardive dyskinesia: deterioration of symptoms | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Mental state | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Adverse effect: any adverse effects | 100 per 1000 | 33 per 1000 | RR 0.33 (0.02 to 7.32) | 20 | ⊕⊝⊝⊝ | |
| Acceptability of the treatment: leaving the study early | 100 per 1000 | 33 per 1000 | RR 0.33 (0.02 to 7.32) | 20 | ⊕⊝⊝⊝ | |
| Social confidence, social inclusion, social networks, or personalised quality of life | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded one level for risk of bias: the included study did not adequately describe randomisation procedure or allocation concealment, and there was no mention of the study being blinded. 2 Downgraded two levels for imprecision: very small sample size (n = 20). 3 Downgraded two levels for imprecision: very wide CI that includes appreciable benefit for both groups; very small sample size (n = 20). 4 Downgraded one level for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability. | ||||||
| Withdrawal of anticholinergic medication compared to continuing anticholigergic medication for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: chronic schizophrenia patients with antipsychotic‐induced tardive dyskinesia | ||||||
| Outcomes | Anticipated absolute effects* (CI) | Relative effect | № of participants | Quality of the evidence | Comments | |
| Risk with continuation of anticholinergic drugs | Risk with withdrawal of anticholinergic drugs | |||||
| Tardive dyskinesia: not improved to a clinically important extent | see comment | see comment | not estimable | 0 (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Tardive dyskinesia: deterioration of symptoms | see comment | see comment | not estimable | 0 (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Mental state | see comment | see comment | not estimable | 0 (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Adverse effects | see comment | see comment | not estimable | 0 (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Acceptability of the treatment: leaving the study early | 0 per 1,000 | 0 per 1,000 | RR 2.14 | 10 | ⊕⊝⊝⊝ | |
| Social confidence, social inclusion, social networks, or personalised quality of life | see comment | see comment | not estimable | 0 (0 studies) | ‐ | None of the included studies reported on this outcome. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded one level for risk of bias: the included study did not adequately describe randomisation procedure or allocation concealment. 2 Downgraded one level for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability. In addition, the continuation of anticholinergic medication group stopped biperiden after 4 weeks but the results were measured after 7 weeks. 3 Downgraded two levels for imprecision: very wide CI that includes appreciable benefit for both groups; very small sample size (n = 10). | ||||||
Background
Description of the condition
Since the 1950s antipsychotic (neuroleptic) medication has been used extensively to treat people with chronic mental illnesses, such as schizophrenia. These drugs can effectively control symptoms such as abnormal perceptions (hallucinations), disordered thinking and fixed false beliefs (delusions). In addition, maintenance therapy with antipsychotics is associated with a reduced risk of relapses (Schooler 1993). However, antipsychotic medication has also been associated with a wide range of adverse effects, including movement disorders. The appearance of these disorders can be extremely disfiguring, compounds stigma, and is associated with poor compliance to antipsychotic treatment (Barnes 1993; Tarsy 2011).
Tardive dyskinesia (TD) is one such movement disorder and is characterised by abnormal, repetitive and involuntary movements. TD is a chronic condition of insidious onset, the severity of which spontaneously fluctuates (APA 1992). The clinical features include tongue protrusion, side‐to‐side or rotatory movement of the jaw, lip smacking, puckering and pursing, and rapid eye blinking (Casey 1994). In some people rapid movements of the arms, legs, and trunk may also occur. Studies on the natural history of TD have reported widely variable remission rates (1% to 62%) depending on patient age, psychiatric diagnosis, course of the psychiatric disorder, and duration of therapy (Bergen 1989; Fernandez 2001; Glazer 1990). It occurs in more than 20% of those using antipsychotic medication continually for longer than three months. Every year 4% to 5% of adults and 25% to 30% of elderly persons who continually use these drugs begin to show signs of TD (APA 1992; Correll 2004). This disorder can result in considerable social and physical disability (Barnes 1993).
The prevalence of TD is often thought to be decreasing based on the use of second generation antipsychotics (SGA) in place of first generation antipsychotics (FGA) (Cloud 2014). A systematic review found that the incidence of TD associated with SGAs (2% to 4%) was significantly lower than that for FGAs (5% to 8%) (Correll 2008). Despite this, widespread use of SGAs in clinical settings may still result in an overall increase in the number of cases of TD (Glazer 2000).
Although the most frequent cause of TD is the use of antipsychotic medication it is striking that dose reduction can lead to a temporary exacerbation in symptoms. Conversely, increasing the dose is often associated with a temporary remission (Cavallaro 1993; Smith 1980). Antipsychotic drugs block certain chemical receptor sites in the brain — one of these is specific for dopamine (Casey 1994). One hypothesis explaining the cause of antipsychotic‐induced TD is that chronic blockade of dopamine receptors in specific cells of the brain (neurones from the nigrostriatum) causes an overgrowth of these receptors (Casey 1994). Consequently, interactions between antipsychotic drugs and dopamine receptors in the brain have been proposed as both the mechanisms for their beneficial effects in psychoses as well as the cause of the movement disorder side effects, including TD (Jeste 1982). In addition, there is evidence to suggest that an imbalance between cells that use dopamine and cells that use acetylcholine may be a cause of TD (Alphs 1983, Casey 1994).
Description of the intervention
Drugs that reduce the activity of the cholinergic cells (anticholinergic drugs) are widely used to help treat other antipsychotic‐induced movement disorders such as parkinsonism and dystonia (APA 1992). Many acutely psychotic patients who receive antipsychotic medication also receive anticholinergic drugs in order to reduce some of the movement side effects associated with antipsychotic medication. However, anticholinergic drugs can cause many undesirable side effects, such as dryness of mouth, constipation, blurring of vision, and confusion (APA 1992).
How the intervention might work
The rationale for the use of anticholinergic drugs in TD is less clear, as there is a suggestion from animal experiments that the chronic administration of anticholinergics could increase the supersensitivity of dopamine receptors and consequently cause TD (Kane 1994). As a result these drugs have not been widely used for the treatment of antipsychotic‐induced TD.
Why it is important to do this review
Several SGAs have been produced in the last decades that are claimed to cause less or no TD (Lieberman 1996). These claims may or may not be true: certainly evidence does indicate that thoughtful use of older generation drugs is not associated with more TD than occurs with newer treatments (Chouinard 2008). Furthermore it is likely that the less expensive and more familiar drugs — such as chlorpromazine or haloperidol — will continue to be the mainstay of treatment of people with schizophrenia in a global context (WHO Essential List 2010). Use of drugs such as these is associated with emergence of TD and therefore this condition will remain a problem for years to come.
Given the high incidence and prevalence of TD among people taking antipsychotic medication, the need for prevention or treatment is clear. Unfortunately, there has been sparse evidence to guide clinicians (NICE 2014; Taylor 2009). Although many treatments have been tested, no one intervention has been shown clearly to be effective. Cessation or reduction of the dose of antipsychotic medication is the ideal management for TD. In clinical practice this is not always possible, not least because in many individuals such a reduction would lead to relapse. This review focuses on whether the addition or withdrawal of anticholinergic drugs to those already receiving antipsychotic medication is likely to help TD.
This review is one in a series of Cochrane Reviews (see Table 1) evaluating treatments for antipsychotic‐induced TD, and is an update of a Cochrane Review first published in 1997 (Soares‐Weiser 1997).
| Interventions | Reference |
| Anticholinergic medication | This review |
| Benzodiazepines | Bhoopathi 2006; update to be published |
| Calcium channel blockers | Essali 2011; update to be published |
| Cholinergic medication | Tammenmaa 2002; update to be published |
| Gamma‐aminobutyric acid agonists | Alabed 2011; update to be published |
| Miscellaneous treatments | Soares‐Weiser 2003; update to be published |
| Neuroleptic reduction and/or cessation and neuroleptics | Soares‐Weiser 2006; update to be published |
| Non‐neuroleptic catecholaminergic drugs | El‐Sayeh 2006; update to be published |
| Vitamin E | Soares‐Weiser 2011; update to be published |
Objectives
To determine whether the use or the withdrawal of anticholinergic drugs (benzhexol, benztropine, biperiden, orphenadrine, procyclidine, scopolamine, or trihexyphenidyl) are clinically effective for the treatment of people with both antipsychotic‐induced tardive dyskinesia and schizophrenia or other chronic mental illnesses.
Methods
Criteria for considering studies for this review
Types of studies
All relevant randomised controlled trials. Where a trial was described as 'double‐blind' but it implied that the study was randomised and the demographic details of each group were similar, we included it. We had planned to exclude quasi‐randomised studies, such as those allocated by using alternate days of the week (see Differences between protocol and review).
Types of participants
Adults, however defined, with schizophrenia or related disorders, including schizophreniform disorder, schizoaffective disorder and delusional disorder, by any means of diagnosis. We are interested in making sure that information is as relevant as possible to the current care of people with schizophrenia, so if information was available we highlighted the current clinical state of participants (acute, early post‐acute, partial remission, remission), the stage (prodromal, first episode, early illness, persistent) and whether the studies primarily focused on people with particular problems (for example negative symptoms, treatment‐resistant illnesses).
Types of interventions
i. Anticholinergic drugs (benzhexol, benztropine, biperiden, dexetimide, orphenadrine, procyclidine, scopolamine, trihexyphenidyl) compared to placebo, or no intervention;
ii. anticholinergic drugs (as above) compared to any other intervention to treat TD; or
iii. the withdrawal of the above anticholinergic drugs compared with the continuation of the treatment.
Types of outcome measures
We have defined clinical efficacy as an improvement in the symptoms of TD of more than 50%, on any scale. We grouped outcomes into short term (less than 6 weeks), medium term (between 6 weeks and six months) and long term (more than six months).
Primary outcomes
1. Tardive dyskinesia
No clinically important improvement in the symptoms of individuals, defined as more than 50% improvement on any TD scale ‒ any time period.
2. Adverse effects
No clinically significant extrapyramidal adverse effects ‒ any time period.
Secondary outcomes
1. Tardive dyskinesia (TD)
1.1 Any improvement in the symptoms of individuals on any TD scale, as opposed to no improvement.
1.2 Deterioration in the symptoms of individuals, defined as any deleterious change on any TD scale.
1.3 Average change in severity of TD during the trial period.
1.4 Average difference in severity of TD at the end of the trial.
2. General mental state changes
2.1 Deterioration in general psychiatric symptoms (such as delusions and hallucinations) defined as any deleterious change on any scale.
2.2 Average difference in severity of psychiatric symptoms at the end of the trial.
3. Acceptability of the treatment
3.1 Acceptability of the intervention to the participant group as measured by numbers of people dropping out during the trial.
4. Adverse effects
4.1 Use of any anti‐parkinsonism drugs.
4.2 Average score/change in extrapyramidal adverse effects.
4.3 Acute dystonia.
5. Other adverse effects, general and specific
6. Hospital and service utilisation outcomes
6.1 Hospital admission.
6.2 Average change in days in hospital.
6.3 Improvement in hospital status (for example: change from formal to informal admission status, use of seclusion, level of observation).
7. Economic outcomes
7.1 Average change in total cost of medical and mental health care.
7.2 Total indirect and direct costs.
8. Social confidence, social inclusion, social networks, or personalised quality of life measures
8.1. No significant change in social confidence, social inclusion, social networks, or personalised quality of life measures.
8.2 Average score/change in social confidence, social inclusion, social networks, or personalised quality of life measures.
9. Behaviour
9.1 Clinically significant agitation.
9.2 Use of adjunctive medication for sedation.
9.3 Aggression to self or others.
10. Cognitive state
10.1 No clinically important change.
10.2 No change, general and specific.
'Summary of findings' table
We used the GRADE approach to interpret findings (Schünemann 2008); and GRADEPRO to import data from Review Manager to create 'Summary of findings' tables. These tables provide outcome‐specific information concerning the overall quality of evidence from each included study in the comparison, the magnitude of effect of the interventions examined, and the sum of the available data on all outcomes we rated as important to patient care and decision making. This summary was used to guide our conclusions and recommendations. We selected the following main outcomes for inclusion in the 'Summary of findings' table.
1. Tardive dyskinesia
1.1 Improved to a clinically important extent.
1.2 Deteriorated.
2. Mental state
2.1 Deterioration.
3. Adverse effects
3.1 Any adverse event.
3.2 Adverse effects: no clinically significant extrapyramidal adverse effects.
4. Acceptability of treatment
4.1 Leaving the study early.
5. Social confidence, social inclusion, social networks, or personalised quality‐of‐life measures*
5.1 No significant change in social confidence, social inclusion, social networks, or personalised quality of life measures for either recipients of care or caregivers.
* Outcome designated important to patients. We wished to add perspectives from people’s personal experience with TD to the research agenda. A consultation with service users was planned where a previously published version of a review in the Cochrane TD series and a lay overview of that review gave the foundation for the discussions (Soares‐Weiser 2011; Table 1). The session was planned to provide time to reflect on current research on TD and consider gaps in knowledge. The report is not completed but we will add a link to it within this review. In the meantime we have added one figure showing a service user's feelings concerning this neglected area of research (Figure 1). Informed by the results of the consultation, for this review we included outcomes important to service users to the 'Summary of findings' table.
Message from one of the participants of the Public and patient involvement consultation of service user perspectives on tardive dyskinesia research.
Search methods for identification of studies
Electronic searches
The 2017 review update was carried out in parallel with updating eight other TD reviews: see Table 1 for details. The search covered all nine TD reviews.
Cochrane Schizophrenia Group's Study‐Based Register of Trials
On 16 July 2015 and 26 April 2017, the Information Specialist searched the register using the following search strategy:
*Tardive Dyskinesia* in Health Care Condition Field of STUDY
In such study‐based registers, searching the major concept retrieves all the synonyms and relevant studies because all the studies have already been organised based on their interventions and linked to the relevant topics (Shokraneh 2017).
This register is compiled by systematic searches of major resources (AMED, BIOSIS, CINAHL, ClinicalTrials.gov, Embase, MEDLINE, PsycINFO, PubMed, WHO ICTRP) and their monthly updates; ProQuest Dissertations and Theses A&I and its quarterly update; Chinese databases (CBM, CNKI, and Wanfang) and their annual updates; handsearches; grey literature; and conference proceedings (see Group's Module). There are no language, date, document type, or publication status limitations for inclusion of records into the register.
For previous searches, please see Appendix 1.
Searching other resources
1. Reference searching
We inspected references of all included studies for further relevant studies.
2. Personal contact
Where necessary, we contacted the first author of each included study for information regarding unpublished trials. We noted the outcome of this contact in the Included studies or Studies awaiting classification tables.
Data collection and analysis
Selection of studies
For the 2017 update, reviewers RA and AG (see Acknowledgements) inspected all abstracts of studies identified as above for potentially relevant reports. We resolved disagreement by discussion; or, where there was still doubt, we acquired the full article for further inspection. We acquired the full articles of relevant reports/abstracts meeting initial criteria for reassessment and carefully inspected for a final decision on inclusion (see Criteria for considering studies for this review). RA and AG were not blinded to the names of the authors, institutions or journal of publication. Where difficulties or disputes arose, we asked author HB for help; and where it was impossible to decide or if adequate information was not available to make a decision, we added these studies to Studies awaiting classification and contacted the authors of the papers for clarification.
Data extraction and management
1. Extraction
For the 2017 update, reviewers RA and HB independently extracted data from all included studies. Again, we discussed any disagreement and documented decisions. KSW helped clarify issues with any remaining problems and we documented these final decisions. We extracted data presented only in graphs and figures whenever possible, but included them only if two reviewers independently had the same result. We attempted to contact authors through an open‐ended request in order to obtain missing information or for clarification whenever necessary. If studies were multi‐centre, where possible we extracted data relevant to each component centre separately.
2. Management
2.1 Forms
For the 2017 update we extracted data to simple forms. Extracted data are available here with a link to the original source PDF for each item.
2.2 Scale‐derived data
We included continuous data from rating scales only if:
a) the psychometric properties of the measuring instrument have been described in a peer‐reviewed journal (Marshall 2000);
b) the measuring instrument has not been written or modified by one of the trialists for that particular trial; and
c) the instrument should be a global assessment of an area of functioning and not sub‐scores which are not, in themselves, validated or shown to be reliable. However there are exceptions, we included sub‐scores from mental state scales measuring positive and negative symptoms of schizophrenia.
Ideally the measuring instrument should either be i. a self‐report or ii. completed by an independent rater or relative (not the therapist). We realise that this is not often reported clearly; we noted in Description of studies if this was the case or not.
2.3 Endpoint versus change data
There are advantages of both endpoint and change data. Change data can remove a component of between‐person variability from the analysis. On the other hand calculation of change needs two assessments (baseline and endpoint) which can be difficult in unstable and difficult‐to‐measure conditions such as schizophrenia. We decided to primarily use endpoint data, and only use change data if the former were not available. We combined endpoint and change data in the analysis as we preferred to use mean differences (MD) rather than standardised mean differences throughout (Higgins 2011).
2.4 Skewed data
Continuous data on clinical and social outcomes are often not normally distributed. To avoid the pitfall of applying parametric tests to non‐parametric data, we applied the following standards to relevant data before inclusion; see (a) and (b) below.
Please note: we would have entered data from studies of at least 200 participants in the analysis, because skewed data pose less of a problem in large studies. We also would have entered all relevant change data as when continuous data are presented on a scale that includes a possibility of negative values (such as change data), it is difficult to tell whether data are skewed or not.
For endpoint data from studies of fewer than 200 participants:
(a) when a scale starts from the finite number zero, we planned to subtract the lowest possible value from the mean, and divide this by the standard deviation. If this value was lower than 1, it strongly suggests a skew and we would have excluded these data. If this ratio was higher than 1 but below 2, there is suggestion of skew. We would have entered these data and tested whether its inclusion or exclusion changed the results substantially. Finally, if the ratio was larger than 2 we would have included these data, because skew is less likely (Altman 1996; Higgins 2011).
(b) if a scale starts from a positive value (such as the Positive and Negative Syndrome Scale (PANSS), (Kay 1986)) which can have values from 30 to 210), we would have modified the calculation described above to take the scale starting point into account. In these cases skew is present if 2 SD > (S − S min), where S is the mean score and 'S min' is the minimum score.
2.5 Common measure
Where relevant, to facilitate comparison between trials we would have converted variables that can be reported in different metrics, such as days in hospital (mean days per year, per week or per month) to a common metric (e.g. mean days per month).
2.6 Conversion of continuous to binary
Where possible, we converted continuous outcome measures to dichotomous data. This can be done by identifying cut‐off points on rating scales and dividing participants accordingly into 'clinically improved' or 'not clinically improved'. It is generally assumed that if there is a 50% reduction in a scale‐derived score such as the Brief Psychiatric Rating Scale (BPRS, Overall 1962) or the Positive and Negative Syndrome Scale (PANSS, Kay 1986), this can be considered as a clinically significant response (Leucht 2005a, Leucht 2005b). If data based on these thresholds were not available, we used the primary cut‐off presented by the original authors.
2.7 Direction of graphs
Where possible, we entered data in such a way that the area to the left of the line of no effect indicated a favourable outcome for anticholinergic medication. Where keeping to this made it impossible to avoid outcome titles with clumsy double‐negatives (e.g. 'Not un‐improved') we presented data where the left of the line indicates an unfavourable outcome and noted this in the relevant graphs.
Assessment of risk of bias in included studies
Reviewers RA and HB independently assessed risk of bias within the included studies by using criteria described in the Cochrane Handbook for Systematic Reviews of Interventions to assess trial quality (Higgins 2011). This set of criteria is based on evidence of associations between overestimate of effect and high risk of bias of the article such as sequence generation, allocation concealment, blinding, incomplete outcome data and selective reporting.
If the raters disagreed, we made the final rating by consensus, with the involvement of another member of the review group. Where inadequate details of randomisation and other characteristics of trials were provided, we contacted authors of the studies in order to obtain further information. If non‐concurrence occurred, we reported this.
We noted the level of risk of bias in the text of the review and in Figure 2, Figure 3, summary of findings Table 3 and summary of findings Table 2.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Measures of treatment effect
1. Binary data
For binary outcomes we calculated a standard estimation of the risk ratio (RR) and its 95% confidence interval (CI). It has been shown that RR is more intuitive than odds ratios (Boissel 1999), as odds ratios tend to be interpreted as RR by clinicians (Deeks 2000).
2. Continuous data
For continuous outcomes we estimated mean difference (MD) between groups. We preferred not to calculate effect size measures (standardised mean difference (SMD)). However, if scales of very considerable similarity were used, we presumed there is a small difference in measurement, and calculated effect size and transformed the effect back to the units of one or more of the specific instruments.
Unit of analysis issues
1. Cluster trials
Studies increasingly employ 'cluster randomisation' (such as randomisation by clinician or practice) but analysis and pooling of clustered data can be a problem. Authors often fail to account for intra‐class correlation in clustered studies, leading to a 'unit of analysis' error (Divine 1992), whereby P values are spuriously low, confidence intervals unduly narrow and statistical significance overestimated. This causes type I errors (Bland 1997; Gulliford 1999).
If any of the included trials had randomised participants by clusters, and where clustering is not accounted for in primary studies, we would have presented such data in a table, with a (*) symbol to indicate the presence of a probable 'unit of analysis' error. In subsequent versions of this review we will seek to contact first authors of studies to obtain intra‐class correlation coefficients for their clustered data and to adjust for this by using accepted methods (Gulliford 1999). Where clustering has been incorporated into the analysis of primary studies, we will present these data as if from a non‐cluster randomised study, but adjust for the clustering effect.
We have sought statistical advice and have been advised that the binary data as presented in a report should be divided by a 'design effect'. This is calculated using the mean number of participants per cluster (m) and the intra‐class correlation coefficient (ICC) (Design effect = 1 + (m − 1) * ICC) (Donner 2002). If the ICC is not reported it will be assumed to be 0.1 (Ukoumunne 1999).
If cluster studies have been appropriately analysed taking into account intra‐class correlation coefficients and relevant data documented in the report, synthesis with other studies would be possible using the generic inverse variance technique.
2. Cross‐over trials
A major concern of cross‐over trials is the carry‐over effect. It occurs if an effect (pharmacological, physiological or psychological) of the treatment in the first phase is carried over to the second phase. As a consequence on entry to the second phase the participants can differ systemically from their initial state despite a wash‐out phase. For the same reason cross‐over trials are not appropriate if the condition of interest is unstable (Elbourne 2002). As both effects are very likely in severe mental illness, we only used data of the first phase of cross‐over studies.
3. Studies with multiple treatment groups
Where a study involves more than two treatment arms, if relevant we presented the additional treatment arms in comparisons. If data were binary we simply added and combined within the two‐by‐two table. If data were continuous we combined data following the formula in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We did not use data where the additional treatment arms were not relevant.
Dealing with missing data
1. Overall loss of credibility
At some degree of loss to follow‐up, data must lose credibility (Xia 2009). We chose that, for any particular outcome, should more than 50% of data be unaccounted for, we would not reproduce these data or use them within analyses. If, however, more than 50% of those in one arm of a study were lost, but the total loss was less than 50%, we addressed this within the 'Summary of findings' table/s by down‐rating quality. We also downgraded quality within the 'Summary of findings' table/s should loss be 25% to 50% in total.
2. Binary
In the case where attrition for a binary outcome is between 0% and 50% and where these data are not clearly described, we presented data on a 'once‐randomised‐always‐analyse' basis (an 'intention to treat' analysis). We assumed all those leaving the study early had no improvement. We undertook a sensitivity analysis testing how prone the primary outcomes were to change by comparing data only from people who completed the study to that point to the 'intention to treat' analysis using the above assumptions.
3. Continuous
3.1 Attrition
We reported and used data where attrition for a continuous outcome was between 0% and 50%, and data only from people who completed the study to that point were reported.
3.2 Standard deviations
If standard deviations were not reported, we first tried to obtain the missing values from the authors. If not available, where there were missing measures of variance for continuous data but an exact standard error and confidence intervals available for group means, and either P value or t value available for differences in mean, we calculated them according to the rules described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011): when only the standard error (SE) is reported, standard deviations (SDs) are calculated by the formula SD = SE * √(n). Chapters 7.7.3 and 16.1.3 of the Cochrane Handbook for Systematic Reviews of Interventions present detailed formulae for estimating SDs from P, t or F values, confidence intervals, ranges or other statistics (Higgins 2011). If these formulae did not apply, we calculated the SDs according to a validated imputation method which is based on the SDs of the other included studies (Furukawa 2006). Although some of these imputation strategies can introduce error, the alternative would be to exclude a given study’s outcome and thus to lose information. We nevertheless examined the validity of the imputations in a sensitivity analysis excluding imputed values.
3.3 Assumptions about participants who left the trials early or were lost to follow‐up
Various methods are available to account for participants who left the trials early or were lost to follow‐up. Some trials just present the results of study completers, others use the method of last observation carried forward (LOCF), while more recently methods such as multiple imputation or mixed‐effects models for repeated measurements (MMRM) have become more of a standard. While the last two methods seem to be somewhat better than LOCF (Leon 2006), we feel that the high percentage of participants leaving the studies early and differences in the reasons for leaving the studies early between groups is often the core problem in randomised schizophrenia trials. We therefore did not exclude studies based on which statistical approach had been used. However, we preferred to use the more sophisticated approaches (e.g. MMRM or 'multiple‐imputation') and only presented completer analyses if some kind of ITT data were not available at all. Moreover, we addressed this issue in the item 'Incomplete outcome data' of the 'Risk of bias' tool.
Assessment of heterogeneity
1. Clinical heterogeneity
We considered all included studies initially, without seeing comparison data, to judge clinical heterogeneity. We simply inspected all studies for clearly outlying people or situations which we had not predicted would arise and discussed in the text if they arose.
2. Methodological heterogeneity
We considered all included studies initially, without seeing comparison data, to judge methodological heterogeneity. We simply inspected all studies for clearly outlying methods which we had not predicted would arise and discussed in the text if they arose.
3. Statistical heterogeneity
3.1 Visual inspection
We visually inspected graphs to investigate the possibility of statistical heterogeneity.
3.2 Employing the I² statistic
We investigated heterogeneity between studies by considering the I² method alongside the Chi² P value. The I² provides an estimate of the percentage of inconsistency thought to be due to chance (Higgins 2003). The importance of the observed value of I² depends on i. magnitude and direction of effects and ii. strength of evidence for heterogeneity (e.g. P value from Chi² test, or a confidence interval for I²). An I² estimate equal to or greater than around 50% accompanied by a statistically significant Chi² statistic can be interpreted as evidence of substantial levels of heterogeneity (Section 9.5.2 Cochrane Handbook for Systematic Reviews of Interventions;Higgins 2011). We explored and discussed in the text potential reasons for substantial levels of heterogeneity (Subgroup analysis and investigation of heterogeneity).
Assessment of reporting biases
Reporting biases arise when the dissemination of research findings is influenced by the nature and direction of results (Egger 1997). These are described in Section 10 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We are aware that funnel plots may be useful in investigating reporting biases but are of limited power to detect small‐study effects. We would not have used funnel plots for outcomes where there were 10 or fewer studies, or where all studies were of similar sizes. In future versions of this review, if funnel plots are possible we will seek statistical advice in their interpretation.
Data synthesis
We understand that there is no closed argument for preference of fixed‐effect models over random‐effects models, or vice versa. The random‐effects method incorporates an assumption that the different studies are estimating different, yet related, intervention effects. This often seems to be true to us and the random‐effects model takes into account differences between studies even if there is no statistically significant heterogeneity. There is, however, a disadvantage to the random‐effects model: it puts added weight onto small studies which often are the most biased ones. Depending on the direction of effect, these studies can either inflate or deflate the effect size. We chose the fixed‐effect model for all analyses.
Subgroup analysis and investigation of heterogeneity
1. Subgroup analyses
1.1 Primary outcomes
We anticipated one sub‐group analysis to test the hypothesis that the modification of anticholinergic medication is most effective for those with early onset TD (less than five years). We had hoped to present data for this subgroup for the primary outcomes.
1.2 Clinical state, stage or problem
We proposed to undertake this review and provide an overview of the effects of anticholinergic medication for people with schizophrenia in general. In addition, however, we had wanted to report data on subgroups of people in the same clinical state, stage and with similar problems.
2. Investigation of heterogeneity
We would have reported when inconsistency was high. First we would have investigated whether data were entered correctly. Second, if data were correct, we would have visually inspected the graph and successively removed studies from the company of the rest to see if homogeneity was restored. For this review we decided that should this occur with data contributing to the summary finding of no more than around 10% of the total weighting, we would present data. If not, we would not pool such data but would discuss issues. We know of no supporting research for this 10% cut off but are investigating use of prediction intervals as an alternative to this unsatisfactory state.
When unanticipated clinical or methodological heterogeneity were obvious, we simply discussed. We did not undertake sensitivity analyses relating to these.
Sensitivity analysis
1. Implication of randomisation
If trials were described in some way as to imply randomisation we undertook a sensitivity analysis for the primary outcomes. We included these studies in the analyses and if there was no substantive difference when the implied randomised studies were added to those with better description of randomisation, then we used relevant data from these studies.
2. Assumptions for lost binary data
Where assumptions had to be made regarding people lost to follow‐up (see Dealing with missing data) we compared the findings of the primary outcomes when we used our assumption compared with 'completer' data only. If there was a substantial difference, we reported and discussed these results but continued to employ our assumption.
Where assumptions have to be made regarding missing SDs data (see Dealing with missing data), we compared the findings on primary outcomes when we used our assumption compared with 'completer' data only. We undertook a sensitivity analysis testing how prone results were to change when 'completer' data only were compared to the imputed data using the above assumption. If there was a substantial difference, we reported and discussed these results but continued to employ our assumption.
3. Risk of bias
We analysed the effects of excluding trials that we judged to be at high risk of bias across one or more of the domains of randomisation (implied as randomised with no further details available), allocation concealment, blinding and outcome reporting for the meta‐analysis of the primary outcome. If the exclusion of trials at high risk of bias did not substantially alter the direction of effect or the precision of the effect estimates, we included data from these trials in the analysis.
4. Imputed values
Had cluster trials been included, we would have undertaken a sensitivity analysis to assess the effects of including data from trials where we used imputed values for ICC in calculating the design effect.
If we found substantial differences in the direction or precision of effect estimates in any of the sensitivity analyses listed above, we did not pool data from the excluded trials with the other trials contributing to the outcome, but presented them separately.
5. Fixed and random effects
We synthesised data using a fixed‐effect model; however, we also synthesised data for the primary outcome using a random‐effects model to evaluate whether this altered the significance of the results.
Results
Description of studies
Please see Characteristics of included studies; Characteristics of excluded studies; Characteristics of studies awaiting classification.
Results of the search
The 2015 and 2017 update searches were part of an update search of nine Cochrane Reviews; see Table 1. The 2015 search retrieved 704 references for 344 studies; see Figure 4 for study flow diagram. After excluding irrelevant references at title and abstract screening, we screened full texts of 31 references (25 studies). As a result of updating the methods and outcomes considered in this review, we have now included two studies that we previously excluded because of a lack of placebo control (Bucci 1971), and uncertainty around the number of participants (Greil 1984); see Included studies. These two studies are the only studies included in this review. One study is awaiting classification (Zeng 1996).

Study flow diagram for 2015 and 2017 searches.
The 2017 search found eight records (five studies). Editorial base of Cochrane Schizophrenia screened these records and no new studies were relevant to this review. They could be relevant to the other reviews in this series of TD reviews (see Table 1), and have been put into 'Studies awaiting classification' of the Soares‐Weiser 2003 'miscellaneous treatments' review.
Included studies
The review now includes two studies with 30 participants, published in 1971 and 1984.
1. Methods
Both studies were stated to be randomised and Greil 1984 also reported being double blind. For further details, please see Risk of bias in included studies (below) on allocation and blinding.
2. Design
Both studies presented a parallel longitudinal design.
3. Duration
The study by Greil 1984 lasted for 7 weeks while Bucci 1971 lasted 40 weeks.
4. Participants
Participants, totalling 30 people, were mostly women in their 50s, with diagnoses of chronic schizophrenia. All were reported to have antipsychotic‐induced TD; however, no criteria for the diagnosis of TD were reported. The number of participants ranged from 10 (Greil 1984) to 20 (Bucci 1971).
5. Setting
One study was performed in hospital outpatients in the USA (Bucci 1971); the other was set in Germany but did not report whether participants were out‐ or inpatients (Greil 1984).
6. Interventions
6.1 Anticholinergic medications
6.1.1 Procyclidine
Procyclidine was used by Bucci 1971 in a 5 mg dose, twice daily.
6.1.2 Biperiden
Biperiden was used by Greil 1984 in the same dose that participants received before the trial. This trial compared the withdrawal of biperiden after 1 week and 4 weeks.
6.2 Comparison group
Greil 1984 compared the withdrawal of biperiden over two time periods. Bucci 1971 used isocarboxazid — a monoamine oxidase inhibitor — 10 mg twice per day as a control.
7. Outcomes
7.1 TD symptoms
Only one study provided useable data on TD symptoms (Bucci 1971). This appears to be a clinical assessment and not a validated scale.
7.2 Adverse events
Only one study provided useable data on adverse events as a result of medication (Bucci 1971). This was reported simply as the number of events in both groups.
Studies awaiting classification
We identified one study, published in Chinese (Zeng 1996). We have contacted the study authors to determine if participants were diagnosed with TD but at the time of preparing this review we had not had a response.
Ongoing studies
We have identified no ongoing studies.
Excluded studies
There are 22 excluded studies. Twelve studies were not randomised (Casey 1977; Gardos 1984; Gerlach 1976; Gerlach 1978; Jus 1974; Konig 1996; Lejoyeux 1993; Smith 1979; Tamminga 1977; Wirshing 1989a; Wirshing 1989b; Zwanikken 1976). Four studies were randomised but included participants with schizophrenia but not TD (DiMascio 1976; Double 1993; Elie 1972; Fann 1976). One study did not report data separately on the minority of participants with TD and the author confirmed that these data are unavailable (Klett 1972). Four studies were cross‐over trials that did not provide data before the first phase before crossing over to the next treatment. We contacted authors of three of these studies and received no data (Friis 1983; Lieberman 1988; NDSG 1986). For one of these studies we were not able to identify up‐to‐date contact details, and we consider it is very unlikely that we will receive a reply with data so many years later (Silver 1995). One study did not provide any usable data, despite our making contact with the authors (Ludatscher 1989).
Risk of bias in included studies
Please refer to Figure 2 and Figure 3 for graphical overviews of the risk of bias in the included studies.
Allocation
While both studies claimed to be randomised, neither described explicitly how the randomisation sequence was generated or how allocation concealment was ensured. As a result we have rated them as having unclear risk of bias.
Blinding
Although Greil 1984 was conducted on a double‐blind basis, only blinding of the treatment provider was explicitly described. Bucci 1971 did not mention blinding of providers, participants, or outcome assessors.
Incomplete outcome data
In each included study there was one person who did not complete the study. In all cases, however, we tried to ensure that every person randomised was analysed.
Selective reporting
All data in this review originates from published reports. The expected outcomes (impact on TD symptoms) were not reported sufficiently by Greil 1984. Both studies did not fully report outcomes that were measured during the study and were rated at high risk of reporting bias. Attempts to contact authors of trials for additional data were unsuccessful.
Other potential sources of bias
Both studies had very small sample sizes. There was very little information reported on which to base further concerns regarding risk of bias.
Effects of interventions
See: Summary of findings for the main comparison Anticholinergic medication compared with placebo for antipsychotic‐induced tardive dyskinesia; Summary of findings 2 Anticholinergic medication compared with other treatments for antipsychotic‐induced tardive dyskinesia; Summary of findings 3 Withdrawal of anticholinergic medication compared to continuing anticholinergic medication for antipsychotic‐induced tardive dyskinesia
1. Comparison 1: anticholinergic drugs versus placebo or no treatment
No studies were identified that assessed this comparison.
2. Comparison 2: anticholinergic drugs versus other compounds
2.1 TD symptoms
We had chosen 'any improvement in TD symptoms of more than 50% on any TD scale ‒ any time period' as a primary outcome. Although the data we found in trials did not fit this exactly we feel that the outcome 'not improved to a clinically important extent' fits best with what we had hoped to find.
2.1.1 Not improved to a clinically important extent
One study found a significant difference on 'no clinically important improvement in TD symptoms favouring isocarboxazid (MAO‐inhibitor) compared with procyclidine (anticholinergic) after 40 weeks' (low‐quality evidence, 1 trial, 20 people; RR 4.20, 95% CI 1.40 to 12.58; Analysis 1.1).
2.1.2 Not any improvement
For the outcome of 'not any improvement in TD symptoms', procyclidine resulted in a worse outcome than isocarboxazid after 40 weeks (low‐quality evidence, 1 trial, 20 people; RR 7.00, 95% CI 1.57 to 31.15; Analysis 1.2).
2.2 Adverse effects
2.2.1 Any adverse effects
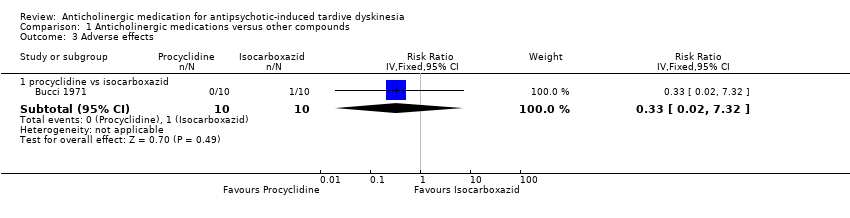
There was no significant difference in the incidence of any adverse effects between procyclidine and isocarboxazid after 40 weeks (very low quality evidence, 1 trial, 20 people; RR 0.33, 95% CI 0.02 to 7.32; Analysis 1.3).
2.3 Leaving the study early
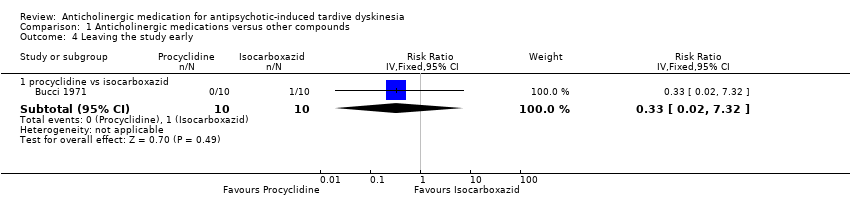
Using procyclidine did not significantly affect the chances of a person leaving the study early compared to isocarboxazid after 40 weeks (very low quality evidence, 1 trial, 20 people; RR 0.33, 95% CI 0.02 to 7.32; Analysis 1.4).
We did not identify any studies that reported on hospital and service utilisation outcomes, economic outcomes, social confidence, social inclusion, social networks, personalised quality of life, behaviour, or cognitive state.
3. Comparison 3: continuation versus withdrawal of anticholinergic drugs
3.1 Leaving the study early
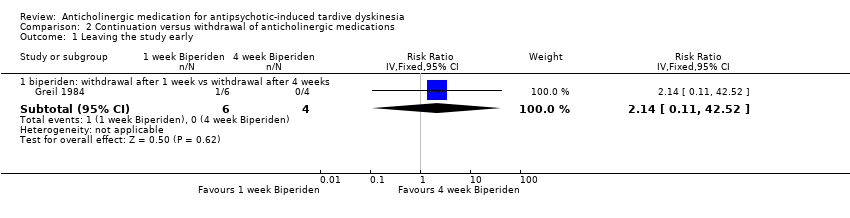
The only usable data showed no significant difference on leaving the study early between withdrawal of biperiden after 1 week compared with continuation of the drug for 4 weeks (very low quality evidence, 1 trial, 10 people; RR 2.14, 95% CI 0.11 to 42.52; Analysis 2.1).
We did not identify any studies that reported on TD symptoms, adverse events, hospital and service utilisation outcomes, economic outcomes, social confidence, social inclusion, social networks, personalised quality of life, behaviour, or cognitive state.
4. Subgroup analyses
4.1 Clinical stage: recent onset TD
It was not possible to evaluate whether those with recent onset TD responded differently to those with more established problems, since no trial reported data for groups with different durations of TD that could be extracted for separate analyses, and since only one study per comparison was included.
4.2 Duration of follow‐up
It was not possible to evaluate whether the effect of anticholinergic drugs changed in relation to duration of follow‐up; only one study per comparison was included.
5. Heterogeneity
Only one study per comparison was included. Therefore, investigation into heterogeneity was not relevant, and we could not detect clinical, methodological or statistical heterogeneity as described in Assessment of heterogeneity.
6. Sensitivity analyses
6.1 Implication of randomisation
We aimed to include trials in a sensitivity analysis if they were described in some way as to imply randomisation. We have not undertaken this sensitivity analysis as only one study was included per comparison, and both studies were stated to be randomised.
6.2 Assumptions for lost binary data
Where assumptions had to be made regarding people lost to follow‐up (see Dealing with missing data) we compared the findings when we used our assumption with 'completer' data only. Using 'completer' data only for anticholinergic drugs (procyclidine) versus isocarboxazid, we found that there was no substantial alteration to the direction of effect or the precision of the effect estimates for the primary outcome 'no clinically important improvement' (1 trial, 19 people; RR 3.82, 95% CI 1.30 to 11.26; analysis not shown).
6.3 Risk of bias
It was not possible to evaluate whether excluding trials that we judged to be at high risk of bias across one or more of the domains would alter the effect estimate; only one study was included per comparison.
6.4 Imputed values
We would have undertaken a sensitivity analysis to assess the effects of including data from cluster randomised trials where we used imputed values for ICC in calculating the design effect. However, no cluster randomised trials were included.
6.5 Fixed and random effects
We also synthesised data for the primary outcome using a random‐effects model. This did not alter the results.
Discussion
Summary of main results
1. The search
This area of research does not seem to be active. The 2017 update has identified additional data, but all trials predate 1990. This could be because of reasons such as less concern with TD, or less emergence of the problem in research‐active communities because of more thoughtful use of antipsychotic drugs.
2. Few data
Only 30 people were included in this review. For this reason it is very likely that real — and important — effects have not been highlighted because of the necessarily wide CIs of the findings. Many outcomes were not measured at all, including several of our pre‐stated outcome measures (see Overall completeness and applicability of evidence).
3. Comparison 1: anticholinergic drugs versus placebo or no treatment
We found no included study that compared the efficacy or safety of an anticholinergic drug compared with placebo or no treatment (summary of findings Table for the main comparison).
4. Comparison 2: anticholinergic drugs versus other compounds
We identified one very small trial reporting few outcomes (summary of findings Table 2). There were no data on mental state or social outcomes.
4.1 TD symptoms
One study found that more participants on isocarboxazid (MAO‐inhibitor) than on procyclidine (anticholinergic) improved to a clinically important level at long term (RR 4.20, 95% CI 1.40 to 12.58; N = 20). However, the quality of the evidence is very low and therefore we have very little confidence in the effect estimate and CIs — the true effect is likely to be substantially different.
4.2 Adverse effects
One study found no clear difference in adverse events between procyclidine (anticholinergic) (0/10) and isocarboxazid (MAO‐inhibitor) (1/10) (RR 0.33, 95% CI 0.02 to 7.32; N = 20). Evidence was of very low quality, therefore we are uncertain about the result.
4.3 Leaving the study early
One study found no clear difference in leaving the study early between procyclidine (anticholinergic) (0/10) and isocarboxazid (MAO‐inhibitor) (1/10) (RR 0.33, 95% CI 0.02 to 7.32; N = 20). Evidence was of very low quality, therefore we are uncertain about the result.
5. Comparison 3. continuation versus withdrawal of anticholinergic drugs
We identified one very small trial reporting few outcomes (summary of findings Table 3). There were no data on tardive dyskinesia, adverse effects, mental state or social outcomes.
5.1 Leaving the study early
One study found no significant difference in leaving the study early between anticholinergic withdrawal after 1 week (1/6) and anticholinergic continuation for 4 weeks (0/4) (RR 2.14, 95% CI 0.11 to 42.52; N = 10). Evidence was of very low quality, therefore we are uncertain about the result.
Overall completeness and applicability of evidence
1. Completeness
Only two small studies with few useable data were included, not sufficient to address whether the use or withdrawal of anticholinergic drugs was associated with an improvement in antipsychotic‐induced TD in people with schizophrenia or other chronic mental illness, let alone to examine whether there was a differential effect among the different anticholinergic drugs. We only identified usable data on TD symptoms from a study comparing anticholinergic medication with another compound, the antidepressant isocarboxazid, a drug which is experimental in the treatment of TD. We found few usable data on adverse events, and none on mental state, social confidence, social inclusion, social networks, or personalised quality of life. If reporting had been better we might have been able to include more data from these studies, and we might have had some data to present from the excluded studies (Friis 1983; Lieberman 1988; Ludatscher 1989; NDSG 1986; Silver 1995).
2. Applicability
Trials included both in‐ and outpatients who were mostly women in their 50s with schizophrenia. They were people who would be recognisable in everyday care. The interventions in question — anticholinergic drugs — are readily accessible and most outcomes are understandable in terms of clinical practice. Should anticholinergic drugs have had important effects the findings might well have been applicable.
Quality of the evidence
We cannot draw any robust conclusions regarding the effects of anticholinergic drugs on TD: only two studies with 30 participants could be included, which severely limited the quality of the evidence. The larger trial randomised only 20 people: a trial of this size is unable to detect subtle, yet important, differences due to an intervention with any confidence. In order to detect a 20% difference between groups, probably about 150 people are needed in each arm of the study (alpha 0.05, beta 0.8). Overall the quality of reporting of these trials was poor (see Figure 3). Allocation concealment was not described, generation of the sequence was not explicit, studies were not clearly blinded, and data were not fully reported. The small sample size and the poor reporting means that we have very little confidence in the effect estimates, and the true effects are likely to be substantially different from the estimates of the effects.
Potential biases in the review process
1. Missing studies
We made every effort to identify relevant trials. However, these studies are both small and it is likely that we have failed to identify other studies of limited power. It is likely that such studies would also not be in favour of the anticholinergics group: if they had been so, it is more likely that they would have been published in accessible literature. We do not, however, think it likely that we have failed to identify large relevant studies.
2. Introducing bias
We have tried to be balanced in our appraisal of the evidence but could have inadvertently introduced bias. We welcome comments or criticisms. New methods and innovations now make it possible to report data where, in the past, we could not report data at all or had to report data in a different way. We believe 'Summary of findings' table is a valuable innovation but problematic to those not ‘blind’ to the outcome data: it is possible to ‘cherry pick’ significant findings for presentation in this table. We have tried to decrease the chance of doing this by asking a new reviewer (HB) to select outcomes relevant for this table before becoming familiar with the data.
Agreements and disagreements with other studies or reviews
The only other relevant quantitative review we know of is the previous Cochrane Review (Soares‐Weiser 1997). This update identified two studies to include (as discussed in Results of the search and Potential biases in the review process), but the very sparse and low‐quality evidence lead to no substantial change in the conclusions.
Message from one of the participants of the Public and patient involvement consultation of service user perspectives on tardive dyskinesia research.
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Study flow diagram for 2015 and 2017 searches.

Comparison 1 Anticholinergic medications versus other compounds, Outcome 1 TD symptoms: no clinically significant improvement.

Comparison 1 Anticholinergic medications versus other compounds, Outcome 2 TD symptoms: not any improvement.
Comparison 1 Anticholinergic medications versus other compounds, Outcome 3 Adverse effects.
Comparison 1 Anticholinergic medications versus other compounds, Outcome 4 Leaving the study early.
Comparison 2 Continuation versus withdrawal of anticholinergic medications, Outcome 1 Leaving the study early.
| Methods | Allocation: randomised, with sequence generation and concealment of allocation clearly described. |
| Participants | People with antipsychotic‐induced tardive dyskinesia.* |
| Interventions | 1. Anticholinergic withdrawal (N = 150) versus anticholinergic continuation (N = 150). OR 2. Specific anticholinergic (N = 150) versus placebo (N = 150). |
| Outcomes | Tardive dyskinesia: any clinically important improvement in TD, any improvement, deterioration.*** |
| Notes | * This could be diagnosed by clinical decision. If funds were permitting, all participants could be screened using operational criteria; otherwise a random sample should suffice. ** Size of study with sufficient power to highlight about a 10% difference between groups for primary outcome. |
| Anticholinergic medication compared with other treatments for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: patients with antipsychotic‐induced tardive dyskinesia Settings: anywhere. Intervention: any anticholinergic Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| risk with placebo | risk with anticholinergic drugs | |||||
| Tardive dyskinesia: not improved to a clinically important extent | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Tardive dyskinesia: deterioration of symptoms | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Mental state | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Adverse effect: any adverse effects | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Acceptability of the treatment: leaving the study early | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Social confidence, social inclusion, social networks, or personalised quality of life | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded one level for risk of bias: the included study did not adequately describe randomisation procedure or allocation concealment, and there was no mention of the study being blinded. 2 Downgraded two levels for imprecision: very small sample size (n = 20). 3 Downgraded two levels for imprecision: very wide CI that includes appreciable benefit for both groups; very small sample size (n = 20). 4 Downgraded one level for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability. | ||||||
| Anticholinergic medication compared with other treatments for antipsychotic‐induced tardive dyskiesia | ||||||
| Patient or population: chronic schizophrenia patients with antipsychotic‐induced tardive dyskinesia Settings: outpatients in the USA. Intervention: procyclidine (anticholinergic), 5 mg twice/day Comparison: isocarboxazid (MAO‐inhibitor), 10 mg twice/day | ||||||
| Outcomes | Illustrative comparative risks* (CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| risk with MAO‐inhibitor | risk with anticholinergic drugs | |||||
| Tardive dyskinesia: Not improved to a clinically important extent | 200 per 1000 | 840 per 1000 | RR 4.20 (1.40 to 12.58) | 20 | ⊕⊝⊝⊝ | |
| Tardive dyskinesia: deterioration of symptoms | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Mental state | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Adverse effect: any adverse effects | 100 per 1000 | 33 per 1000 | RR 0.33 (0.02 to 7.32) | 20 | ⊕⊝⊝⊝ | |
| Acceptability of the treatment: leaving the study early | 100 per 1000 | 33 per 1000 | RR 0.33 (0.02 to 7.32) | 20 | ⊕⊝⊝⊝ | |
| Social confidence, social inclusion, social networks, or personalised quality of life | see comment | see comment | not estimable | (0 studies) | ‐ | None of the included studies reported on this outcome. |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded one level for risk of bias: the included study did not adequately describe randomisation procedure or allocation concealment, and there was no mention of the study being blinded. 2 Downgraded two levels for imprecision: very small sample size (n = 20). 3 Downgraded two levels for imprecision: very wide CI that includes appreciable benefit for both groups; very small sample size (n = 20). 4 Downgraded one level for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability. | ||||||
| Withdrawal of anticholinergic medication compared to continuing anticholigergic medication for antipsychotic‐induced tardive dyskinesia | ||||||
| Patient or population: chronic schizophrenia patients with antipsychotic‐induced tardive dyskinesia | ||||||
| Outcomes | Anticipated absolute effects* (CI) | Relative effect | № of participants | Quality of the evidence | Comments | |
| Risk with continuation of anticholinergic drugs | Risk with withdrawal of anticholinergic drugs | |||||
| Tardive dyskinesia: not improved to a clinically important extent | see comment | see comment | not estimable | 0 (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Tardive dyskinesia: deterioration of symptoms | see comment | see comment | not estimable | 0 (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Mental state | see comment | see comment | not estimable | 0 (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Adverse effects | see comment | see comment | not estimable | 0 (0 studies) | ‐ | None of the included studies reported on this outcome. |
| Acceptability of the treatment: leaving the study early | 0 per 1,000 | 0 per 1,000 | RR 2.14 | 10 | ⊕⊝⊝⊝ | |
| Social confidence, social inclusion, social networks, or personalised quality of life | see comment | see comment | not estimable | 0 (0 studies) | ‐ | None of the included studies reported on this outcome. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded one level for risk of bias: the included study did not adequately describe randomisation procedure or allocation concealment. 2 Downgraded one level for indirectness: leaving the study early can give an indication, but is not a direct measurement, of treatment acceptability. In addition, the continuation of anticholinergic medication group stopped biperiden after 4 weeks but the results were measured after 7 weeks. 3 Downgraded two levels for imprecision: very wide CI that includes appreciable benefit for both groups; very small sample size (n = 10). | ||||||
| Interventions | Reference |
| Anticholinergic medication | This review |
| Benzodiazepines | Bhoopathi 2006; update to be published |
| Calcium channel blockers | Essali 2011; update to be published |
| Cholinergic medication | Tammenmaa 2002; update to be published |
| Gamma‐aminobutyric acid agonists | Alabed 2011; update to be published |
| Miscellaneous treatments | Soares‐Weiser 2003; update to be published |
| Neuroleptic reduction and/or cessation and neuroleptics | Soares‐Weiser 2006; update to be published |
| Non‐neuroleptic catecholaminergic drugs | El‐Sayeh 2006; update to be published |
| Vitamin E | Soares‐Weiser 2011; update to be published |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 TD symptoms: no clinically significant improvement Show forest plot | 1 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1 procyclidine vs isocarboxazid | 1 | 20 | Risk Ratio (IV, Fixed, 95% CI) | 4.2 [1.40, 12.58] |
| 2 TD symptoms: not any improvement Show forest plot | 1 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 2.1 procyclidine vs isocarboxazid | 1 | 20 | Risk Ratio (IV, Fixed, 95% CI) | 7.0 [1.57, 31.15] |
| 3 Adverse effects Show forest plot | 1 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 3.1 procyclidine vs isocarboxazid | 1 | 20 | Risk Ratio (IV, Fixed, 95% CI) | 0.33 [0.02, 7.32] |
| 4 Leaving the study early Show forest plot | 1 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 4.1 procyclidine vs isocarboxazid | 1 | 20 | Risk Ratio (IV, Fixed, 95% CI) | 0.33 [0.02, 7.32] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Leaving the study early Show forest plot | 1 | Risk Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1 biperiden: withdrawal after 1 week vs withdrawal after 4 weeks | 1 | 10 | Risk Ratio (IV, Fixed, 95% CI) | 2.14 [0.11, 42.52] |