Whole body vibration exercise training for fibromyalgia
Information
- DOI:
- https://doi.org/10.1002/14651858.CD011755.pub2Copy DOI

- Database:
-
- Cochrane Database of Systematic Reviews
- Version published:
-
- 26 September 2017see what's new
- Type:
-
- Intervention
- Stage:
-
- Review
- Cochrane Editorial Group:
-
Cochrane Musculoskeletal Group
- Copyright:
-
- Copyright © 2017 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Article metrics
Altmetric:
Cited by:
Authors
Contributions of authors
Initials correspond to authors as they are listed under the review title.
JB: leading WBV exercise training review team, designing and reviewing review protocol, assessing eligibility of studies, participating in discussion regarding review design and methods, screening studies for eligibility for inclusion in the review, conducting data extraction, conducting methodological and statistical analyses, drafting and reviewing the manuscript, collaborating with consumers throughout creation of the plain language summary, and reading and approving the final manuscript.
AJB: responsible for leading and coordinating Fibromyalgia and Exercise Team, designing and reviewing review protocol, assessing eligibility of studies, supporting and managing data extraction, supervising methodological and statistical analyses, and collaborating in meetings regarding plain language summary, discussion, and conclusions. Read and approved the final manuscript.
IVDS: designing and reviewing review protocol, extracting data, assessing risk of bias, contributing to creation of tables, and participating in discussion and conclusions. Reading and approving the final manuscript.
ST: designing and reviewing review protocol, collaborating on data extraction, providing content expertise on pain, supporting interpretation of findings and contributing to creation of tables, and writing and reviewing discussion and conclusions. Reading and approving the final manuscript.
SYK: designing and reviewing review protocol, collaborating on data extraction, providing content expertise on musculoskeletal matters, writing and reviewing drafts, and approving the final manuscript.
CB: performing literature searches, participating in discussion regarding methods, working on plain language summary with consumers, working on tables and figures, conducting searches to support background and discussion sections of the manuscript, and writing and reviewing the manuscript. Reading and approving the final manuscript.
Sources of support
Internal sources
-
No funding support has been received, Canada.
External sources
-
No funding support has been received, Canada.
Declarations of interest
We confirm that we have listed below any present or past affiliations or other involvement in any organization or entity with an interest in the review that might lead me/us to have a real or perceived conflict of interest.
Initials correspond to authors as they are listed under the review title.
JB: none known; AJB: none known; IVDS: none known; ST: none known; SYK: none known; CB: none known.
Acknowledgements
We would like to acknowledge the following.
-
Exercise for Fibromyalgia Cochrane Review Team.
-
The review team contributed to various tasks related to reviews of exercise and fibromyalgia (screening of citations, abstracts, and full‐text articles for inclusion/exclusion and related consensus activities; data extraction and related consensus activities; regular attendance at monthly meetings; contributing to discussion regarding relevant concepts; interpretation and discussion of results; translation of knowledge gained; presentation of workshops or seminars when possible).
-
Currently, the review team is led by Dr. Angela Busch, and is made up of 14 members, including two consumers (Janet Gunderson and Anne Lyddiatt), one librarian/information specialist (Catherine Boden), and 11 reviewers (kinesiologists ‐ Julia Bidonde, Suelen Goés, Heather Foulds; physical therapists ‐ Tom Overend, Candice Schachter, Sandra Webber, Kristen Musselman, Susan Tupper, Soo Kim, Ina van der Spuy, and Vanina Dal Bello Haas). Former members of the team include Mary Brachaniec, Tamara Rader, Rachel Richards, Laurel Schafer, Adrienne Danyliw, Mary Brachaniec, Joelle Harris, and Christopher Ross.
-
-
The following individuals voluntarily helped in translating publications and communicating with study authors in their original languages: Julia Bidonde, Nora Chavarria, Beliz Arcan, Patricia Mancini, and Suelen Gomez, translating from Spanish, German, Turkish, and Portuguese (not all articles were used in this review).
-
Renea Johnston and Rachelle Buchbinder, members of the editorial team of the Cochrane Musculoskeletal Group (Monash, Australia).
-
The team gratefully acknowledges the assistance of JoAnn Nilson, PT (Saskatoon Health Region), for her thoughtful comments and insight into important clinical aspects of this review.
Version history
| Published | Title | Stage | Authors | Version |
| 2017 Sep 26 | Whole body vibration exercise training for fibromyalgia | Review | Julia Bidonde, Angela J Busch, Ina van der Spuy, Susan Tupper, Soo Y Kim, Catherine Boden | |
| 2015 Jun 17 | Whole body vibration exercise for fibromyalgia | Protocol | Angela J Busch, Ina van der Spuy, Susan Tupper, Soo Y Kim, Julia Bidonde, Tom J Overend | |
Differences between protocol and review
This review is one of a series of reviews undertaken to update previous reviews completed in 2002 and 2007 on exercise for fibromyalgia. Given the growth in literature, this review has been split into several reviews (ie, resistance, aquatic, mixed, aerobic, flexibility, and vibration).
Differences between the protocol (Busch 2015) and this review included the following.
-
Revisions to search terms and databases: three HTA‐specific databases added.
-
Changes in membership of the review team (change in the lead author (AJB/JB), dropout of one review author (TO), addition of a new review author (CB) and two consumers (AL and JG).
-
Addition of the word "training" to the title of the review.
-
Use of new software in addition to electronic forms for selection of studies; this software, which is called Covidence, was recently developed to conduct screening for creating and maintaining systematic reviews (https://www.covidence.org/).
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
- Combined Modality Therapy [methods];
- Exercise Therapy [*methods];
- Fatigue [diagnosis];
- Fibromyalgia [*therapy];
- Muscle Rigidity;
- Pain Measurement;
- Patient Dropouts [statistics & numerical data];
- Quality of Life;
- Relaxation Therapy [*methods];
- Treatment Outcome;
- Vibration [adverse effects, *therapeutic use];
Medical Subject Headings Check Words
Adult; Female; Humans;
PICOs

Study flow diagram for vibration training interventions.

Galileo Fitness Platform (Copyright © 2008‐2015 Novotec Medical GmbH; reproduced with permission)

Copyright © 2012 Wellsports GmbH Krefeld ‐ PowerPlate International B.V., The Netherlands ‐ awaiting response.Sept15
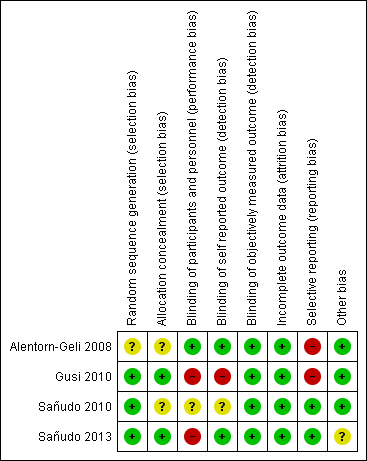
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Comparison 1 WBV vs C, Outcome 1 HRQL, 1‐100 scale, lower means better HRQL.
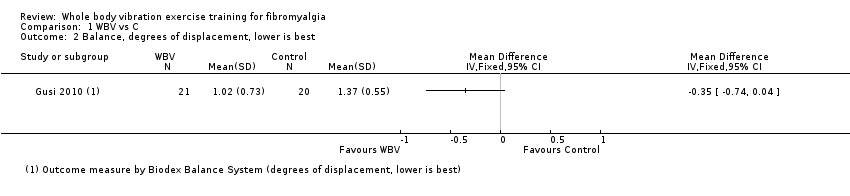
Comparison 1 WBV vs C, Outcome 2 Balance, degrees of displacement, lower is best.

Comparison 1 WBV vs C, Outcome 3 Withdrawal.

Comparison 2 WBV + MX vs C, Outcome 1 WBV + MX vs C: HRQL, 0‐100 scale, lower is best.
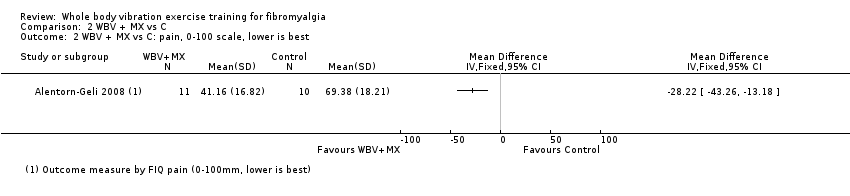
Comparison 2 WBV + MX vs C, Outcome 2 WBV + MX vs C: pain, 0‐100 scale, lower is best.

Comparison 2 WBV + MX vs C, Outcome 3 WBV + MX vs C: fatigue, 0‐100 scale, lower is best.
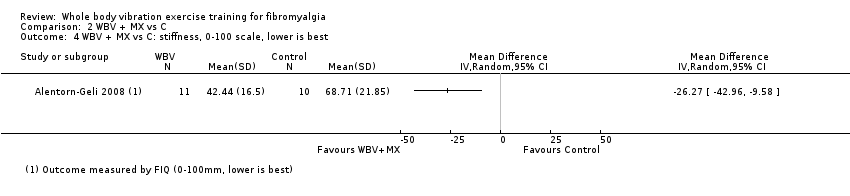
Comparison 2 WBV + MX vs C, Outcome 4 WBV + MX vs C: stiffness, 0‐100 scale, lower is best.

Comparison 2 WBV + MX vs C, Outcome 5 WBV + MX vs C: balance, overall stability index ‐ eyes closed (degrees of displacement 0 to 20 scale, lower is best).

Comparison 2 WBV + MX vs C, Outcome 6 Withdrawal.

Comparison 3 WBV + MX vs Other, Outcome 1 WBV + MX vs Other: HRQL, 0‐100 scale, lower is best.
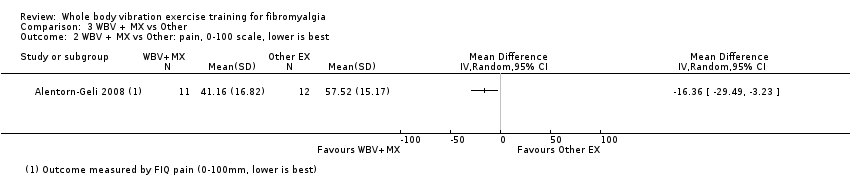
Comparison 3 WBV + MX vs Other, Outcome 2 WBV + MX vs Other: pain, 0‐100 scale, lower is best.

Comparison 3 WBV + MX vs Other, Outcome 3 WBV + MX vs Other: fatigue, 0‐100 scale, lower is best.

Comparison 3 WBV + MX vs Other, Outcome 4 WBV + MX vs Other: stiffness, 0‐100 scale, lower is best.

Comparison 3 WBV + MX vs Other, Outcome 5 WBV + MX vs Other: strength, measured in newtons and number of reps, higher values are best.
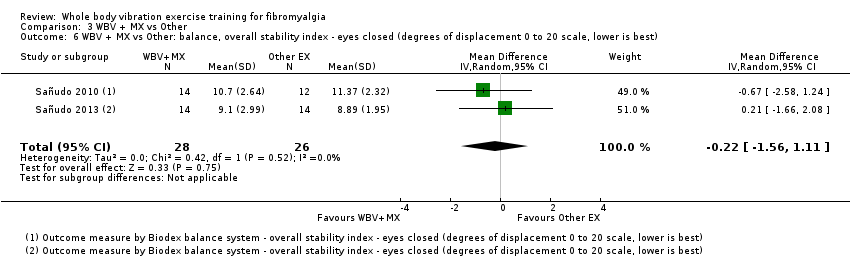
Comparison 3 WBV + MX vs Other, Outcome 6 WBV + MX vs Other: balance, overall stability index ‐ eyes closed (degrees of displacement 0 to 20 scale, lower is best).
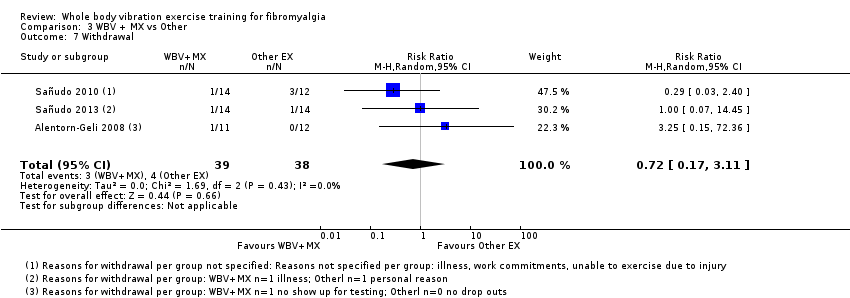
Comparison 3 WBV + MX vs Other, Outcome 7 Withdrawal.
| Whole body vibration versus control | ||||||
| Patient or population: individuals with fibromyalgia | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No. of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with WBV | |||||
| Health‐related quality of life Follow‐up: 12 weeks | Mean health‐related quality of life was 59 points | Mean health‐related quality of life in intervention group was 3.73 points lower (10.81 lower to 3.35 higher) at post‐test than in control group | ‐ | 41 | ♁◯◯◯ | Absolute improvement: 4% (95% CI 11% better to 3% worse) Relative change: 6.7% improvement (95% CI 19.6% improvement to 6.1% worse) NNTB: n/ac |
| Pain intensity | Not measured | Not measured | ‐ | Not measured | Not measured | Not measured |
| Fatigue | Not measured | Not measured | ‐ | Not measured | Not measured | Not measured |
| Stiffness | Not measured | Not measured | ‐ | Not measured | Not measured | Not measured |
| Physical function | Not measured | Not measured | ‐ | Not measured | Not measured | Not measured |
| Adverse events | Gusi 2010: "The program was reasonably safe: only 5% of the participants (n = 1) dropped out of the program because of acute pain in the legs. The program was completed by 85% of the participants, without secondary adverse effects" (page 1076; 1 study) | |||||
| All‐cause withdrawal | Study population | RR 1.43 (0.27 to 7.67) | 41 | ♁◯◯◯ | Absolute risk difference: 4% more events (95% CI 16% fewer to 24% more) Relative change: 43% more (73% fewer to 667% more) NNTH: n/ac | |
| 10 per 100 (2 of 20) | 14 per 100 (3 of 21) | |||||
| *Risk in the intervention group (and its 95% confidence interval) is based on assumed risk in the comparison group and relative effect of the intervention (and its 95% CI) | ||||||
| GRADE Working Group grades of evidence | ||||||
| aImpresicion: number of participants lower than 400 rule of thumb; wide confidence interval (downgraded twice) bHigh risk of biases including detection, performance, and reporting biases cNumber needed to treat for an additional beneficial outcome (NNTB) or number needed to treat for an additional harmful outcome (NNTH) not applicable (n/a) when result is not statistically significant. NNT for dichotomous outcomes calculated with Cates NNT calculator (http://www.nntonline.net/visualrx/). NNT for continuous outcomes calculated with Wells calculator (CMSG Editorial Office) | ||||||
| Whole body vibration plus mixed exercise versus control | ||||||
| Patient or population: individuals with fibromyalgia | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | No. of participants | Quality of the evidence | Comments | |
| Risk with control | Risk with WBV + MX | |||||
| Health‐related quality of life | Mean health‐related quality of life was 59.64 points at the end of the study | Mean health‐related quality of life in the intervention group was 16.02 points lower (31.57 lower to 0.47 lower) at post‐test than in the control group | ‐ | 21 | ♁◯◯◯ | Absolute difference: 16% improvement (95% CI 32% to 0.5% improvement). Relative change: 24% (47% to 0.7%)c NNTBd: 3 (2 to 237) |
| Pain Intensity | Mean pain intensity was 69.38 mm in the control group at the end of the study | Mean pain Intensity in the intervention group was 28.22 mm lower (43.26 lower to 13.18 lower) at post‐test than in the control group | ‐ | 21 | ♁◯◯◯ | Absolute difference: 28% (95% CI 43% to 13%). Relative difference: 39% (95% CI 18% to 60%) NNTBd: 2 (1 to 4) |
| Fatigue | Mean fatigue was 75.17 mm at the end of the study | Mean fatigue in the intervention group was 32.84 mm lower (49.2 lower to 16.48 lower) at post‐test than in the control group | ‐ | 21 | ♁◯◯◯ | Absolute difference: 33% (95% CI 49% to 16%). Relative difference: 47% (95% CI 23% to 70%) NNTBd: 2 (1 to 4) |
| Stiffness | Mean stiffness was 68.71 mm at the end of the study | Mean stiffness in the intervention group was 26.27 mm lower (42.96 lower to 9.58 lower) at post‐test than in the control group | ‐ | 21 | ♁◯◯◯ | Absolute difference 26% (95% CI 43% to 10%). Relative difference: 36.5% (95% CI 60% to 23%) NNTBd: 2 (1 to 6) |
| Physical function | Not measured | Not measured | ‐ | Not measured | Not measured | Not measured |
| Adverse events (narrative) | Alentorn‐Geli 2008: "This program neither exacerbated FM‐related symptoms nor resulted in musculoskeletal injuries; however, 1 patient exhibited a mild anxiety attack on the first session of WBV" (page 978) Sañudo 2013: "This study, however, demonstrated that WBV training is safe (no adverse events)..." (page 683) | |||||
| All‐cause withdrawal | 33 per 100 (7 of 21) | 8 per 100 | RR 0.25, 95% CI 0.06 to 1.12 | 46 | ♁◯◯◯ | Absolute risk difference: 24% (95% CI 3 to 51) NNTHd: n/a |
| *Risk in the intervention group (and its 95% confidence interval) is based on assumed risk in the comparison group and relative effect of the intervention (and its 95% CI) | ||||||
| GRADE Working Group grades of evidence | ||||||
| aImprecision: Number of participants lower than 400 rule of thumb; wide confidence interval. Need for more studies with more participants to reach optimal information size (downgraded twice) bHigh risk of biases including reporting and selection biases. Need for methodologically better designed and executed studies cBaseline control group mean (SD) = 67 (15.81), n = 10 dNumber needed to treat for an additional beneficial outcome (NNTB) or number needed to treat for an additional harmful outcome (NNTH) not applicable (n/a) when result is not statistically significant. NNT for dichotomous outcomes calculated with Cates NNT calculator (http://www.nntonline.net/visualrx/). NNT for continuous outcomes calculated with Wells calculator (CMSG Editorial Office) | ||||||
| Term | Definition |
| Allodynia | Pain resulting from a stimulus that would not normally provoke pain |
| Amplitude | Absolute value of maximum displacement from a zero value during 1 period of an oscillation |
| Damping | Energy dissipation properties of a material or system under cyclic stress |
| Endurance | Two forms of endurance that refer to health‐related physical fitness include cardiorespiratory endurance (also known as cardiovascular endurance, aerobic fitness, aerobic endurance, exercise tolerance), which "relates to the ability of the circulatory and respiratory systems to supply fuel during sustained physical activity and to eliminate waste products after supplying fuel," and muscle endurance, which "relates to the ability of muscle groups to exert external force for many repetitions" (Caspersen 1985) |
| Frequency | Number of cycles or completed alternations per unit time of a wave or oscillation |
| Hertz | One hertz is 1 cycle per second; therefore, when an individual is exposed to a vibration of 30 Hz, targeted muscles receive 30 cycles of vibration per second, which makes muscles contract and relax 30 times in the same period |
| Hyperalgesia | Increased pain from a stimulus that normally provokes pain |
| Natural frequency | Frequency at which a system oscillates when not subjected to continuous or repeated external forces |
| Paresthesia | Abnormal sensation that is spontaneous or is evoked by a stimulus (eg, numbness) |
| Phase angle | Particular stage or point of advancement in a cycle; fractional part of the period through which time has advanced, measured from some arbitrary origin often expressed as an angle (phase angle); the entire period being taken is 360° |
| Abbreviation | Description |
| A | amplitude |
| ACR | American College of Rheumatology |
| ACSM | American College of Sports Medicine |
| AE | aerobic exercise |
| EMG | electromyography |
| f | frequency |
| FIQ | Fibromyalgia Impact Questionnaire |
| FX | flexibility |
| g | gravitational load (G‐force) = 1 cm/s2 |
| HR | heart rate |
| HRQL | health‐related quality of life |
| hz | Hertz |
| ITT | intention‐to‐treat |
| kg | kilogram |
| m/s2 | unit of acceleration: 1 Gal = 0.01 m/s2 |
| MCID | minimal clinically important difference |
| MD | mean difference |
| MX | mixed intervention (includes more than 1 mode of physical activity) |
| n | number of studies |
| N | number of individuals |
| RD | risk difference |
| Relax | relaxation |
| RT | resistance training |
| s | seconds |
| SD | standard deviation |
| SE | standard error |
| SMD | standardized mean difference |
| sTNFR1 and sTNFR2 | soluble tumor necrosis factor receptor 1 and 2 |
| VAS | visual analogue scale |
| WBV | whole body vibration |
| wk | week(s) |
| WU | warm‐up |
| Vibration + Mixed vs Mixed + Placebo vs Control | |||||||||
| Author, year | Intervention | Frequency (times per week | length in weeks) | Total duration | Supervised or home program | Aerobic component | Resistance component | Flexibility Component | Other | |
| I (intensity): ACSM classification and physiological measure; M (mode): mode of exercise; T (time): duration of aerobic component in minutes | M (muscle groups, joints or areas of body); I (intensity resistance, repetitions, sets); T (type), T (time) | M (muscle groups, joints or areas of body); T (type of stretch, repetition, set), T (time) | |||||||
| AE + FX + Relax | 2 times/wk | 6 weeks | 90’ | Not specified | I: moderate to vigorous (65%‐85% HR max), T: primarily level ground walking with games and dance, T: 30' | Not applicable | M: 5 whole body stretches involving lower and upper limbs, neck, back; T: dynamic, 5 reps held for 30 s with 30 s rests, T: 25' | Relaxation | |
| Vibration + Mixed vs Mixed | |||||||||
| AE + RT + FX | 2 times/wk | 6 weeks | 60’ | Supervised | I: light to moderate (50%‐69% HR max), M: not specified, T: 4‐6 intervals of 2‐3’, 1‐2’ rest between intervals | M: major muscle groups, I: 8 exercises, 1 × 8‐10 reps with 1‐3 kg, T: not specified | M: not specified, I: 1x 3 reps holding for 30s, T: not specified | ||
| AE + RT + FX | 2 times/wk | 8 weeks | 45‐60’ | Supervised | I: moderate (65%‐70% HR max), M: not specified, T: 10‐15’ | M: deltoids, biceps, neck, hips, back, and chest, I: 1 set of 8‐10 reps for 8 different muscle groups against 1‐3 kg, T: 15‐20’ | M: deltoids, biceps, neck, hips, back, and chest I: 1 set of 3 reps for 8‐9 different ex, maintained for 30 s, T: 10’ | ||
| Study name/year | Name of device | Vibration frequency and amplitude | Position of participant | Stabilizing support | Footwear | Static/Dynamic; unilateral/bilateral |
| PowerPlate (PowerPlate International B.V., Badhoevendorp, The Netherlands) | 30 Hz; 2 mm vertical amplitude | The following 6 exercises were performed for 30 s each during whole body vibration (WBV) and were repeated 6 times with recovery of 3 minutes between repetitions (a) static squat at 100° of knee flexion (b) dynamic squat between 90° and 130° of knee flexion (c) maintained ankle plantar‐flexion with legs in extension (d) flexion‐extension of right leg between 100° and 130° of knee flexion (e) flexion‐extension of left leg between 100° and 130° of knee flexion (f) squat at 100° of knee flexion shifting body weight from 1 leg to the other For adaptation purposes, only tasks (a), (b), and (c) (repeated 3 times) were performed during first 2 sessions | Yes ‐ for all tasks, individuals held onto the supporting bar | Does not state | Static bilateral | |
| Galileo Fitness Platform (Novotec Medical, Pforzheim, Germany) | 12.5 Hz; 3 mm vertical amplitude | Participants alternated between 2 stances for each repetition Stance A: feet perpendicular to midline axis of the platform with right foot placed slightly ahead of left foot. Toes of right foot and heel of left foot lifted 4 mm above surface of the platform. Knees bent to 45° angle. Back and head kept straight Stance B: as per Stance A, except with left foot placed slightly ahead of right foot | Not reported and not pictured in Figure 2 | Balance testing was performed barefoot. Does not specify that exercise was done barefoot, but Figure 2 indicates this | Static and dynamic both unilateral and bilateral | |
| Galileo Fitness Platform (Novotec Medical, Pforzheim, Germany) | 20 Hz; variable amplitude of 2‐3 mm | Three sets of 45 s of bilateral static squat with 120 s recovery between sets (amplitude = 3 mm) followed by 4 sets of 15 s of unilateral static squat on each leg (amplitude = 2 mm). During WBV, participants stood with both knees in 120° isometric knee flexion (half‐squatting position) as measured by a goniometer | Does not state | Does not state | Static unilateral and bilateral | |
| PowerPlate, North America Inc., Northbrook, IL, United States | 30 Hz; vertical displacement of 4 mm (71.1 m/s‐2 ≈ 7.2 g) | Standing on the platform, with knees in 120º isometric knee flexion (measured by a goniometer) and trunk upright Bilateral static squat: 6 sets of 30 s, with 45‐s recovery between sets Unilateral static squat: 4 sets of 30 s each leg | Does not state | All participants wore sport shoes for vibration exercises | Static unilateral and bilateral |
| Quality assessment | No. of participants | Quality | Importance | |||||||
| No. of studies | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | Aerobic exercise (AE) intervention | AE control | ||
| Health‐related quality of life (HRQL), 0‐100, lower is best | ||||||||||
| 2 | Randomized trial | Very serious1 | Not serious | Not serious | Serious2 | 23 | 26 | ⊕⊝⊝⊝ | CRITICAL | |
| Pain intensity, 0‐100, lower is best | ||||||||||
| 1 | Randomized trial | Serious3 | Not serious | Not serious | Serious2 | One very small study | 11 | 12 | ⊕⊝⊝⊝ | CRITICAL |
| Fatigue, 0‐100, lower is best | ||||||||||
| 1 | Randomized trial | Serious1 | Not serious | Not serious | Serious2 | One very small study | 11 | 12 | ⊕⊝⊝⊝ | IMPORTANT |
| Stiffness, 0‐100, lower is best | ||||||||||
| 1 | Randomized trial | Serious1 | Not serious | Not serious | Serious2 | One very small study | 11 | 12 | ⊕⊝⊝⊝ | IMPORTANT |
| Physical function, not reported | ||||||||||
| Withdrawals | ||||||||||
| 3 | Randomized trial | Very serious4 | Not serious | Not serious | Serious2 | 3/39 (7.69%) | 4/38 (10.52%) | ⊕⊝⊝⊝ | IMPORTANT | |
| Adverse events:Alentorn‐Geli 2008: "This program neither exacerbated FM‐related symptoms nor resulted in musculoskeletal injuries; however, one patient exhibited a mild anxiety attack on the first session of WBV" (page 978); Sañudo 2010: Trial authors clarified that one person in the comparison group ("other exercise group") dropped out owing to an injury that was not an injury related to the program (participant fell down on the street); Sañudo 2013: "This study, however, demonstrated that WBV training is a safe (no adverse effects), suitable (no dropouts due to the intervention), and effective (increased lower limb muscle strength) way to exercise the musculoskeletal system, and potentially a feasible intervention for those patients who cannot participate in conventional strength training" (page 683) | ||||||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 HRQL, 1‐100 scale, lower means better HRQL Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Balance, degrees of displacement, lower is best Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3 Withdrawal Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 WBV + MX vs C: HRQL, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2 WBV + MX vs C: pain, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3 WBV + MX vs C: fatigue, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4 WBV + MX vs C: stiffness, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5 WBV + MX vs C: balance, overall stability index ‐ eyes closed (degrees of displacement 0 to 20 scale, lower is best) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6 Withdrawal Show forest plot | 2 | 46 | Risk Ratio (M‐H, Random, 95% CI) | 0.25 [0.06, 1.12] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 WBV + MX vs Other: HRQL, 0‐100 scale, lower is best Show forest plot | 2 | 49 | Mean Difference (IV, Random, 95% CI) | ‐6.67 [‐14.65, 1.31] |
| 2 WBV + MX vs Other: pain, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3 WBV + MX vs Other: fatigue, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4 WBV + MX vs Other: stiffness, 0‐100 scale, lower is best Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5 WBV + MX vs Other: strength, measured in newtons and number of reps, higher values are best Show forest plot | 2 | 54 | Std. Mean Difference (IV, Random, 95% CI) | 0.77 [0.20, 1.35] |
| 6 WBV + MX vs Other: balance, overall stability index ‐ eyes closed (degrees of displacement 0 to 20 scale, lower is best) Show forest plot | 2 | 54 | Mean Difference (IV, Random, 95% CI) | ‐0.22 [‐1.56, 1.11] |
| 7 Withdrawal Show forest plot | 3 | 77 | Risk Ratio (M‐H, Random, 95% CI) | 0.72 [0.17, 3.11] |