Intermittent self‐dilatation for urethral stricture disease in males
Information
- DOI:
- https://doi.org/10.1002/14651858.CD010258.pub2Copy DOI

- Database:
-
- Cochrane Database of Systematic Reviews
- Version published:
-
- 19 December 2014see what's new
- Type:
-
- Intervention
- Stage:
-
- Review
- Cochrane Editorial Group:
-
Cochrane Incontinence Group
- Copyright:
-
- Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Article metrics
Altmetric:
Cited by:
Authors
Contributions of authors
Matthew Jackson (MJ), Rajan Veeratterapillay (RV), Chris Harding (CH) and Trevor Dorkin (TD) were responsible for the conception of the protocol. MJ and CH were responsible for screening search results, screening retrieved papers against the inclusion criteria and appraising the quality of papers. MJ, RV and TD were responsible for extracting data. MJ and TD were responsible for checking the data for inter‐observer agreement. MJ was responsible for entering data into Review Manager. MJ and RV were responsible for assessing risk of bias. MJ was responsible for carrying out the analysis. MJ and RV were responsible for interpreting the analysis. MJ, RV and CH were responsible for drafting the review. MJ, RV, CH and TD were responsible for reviewing the final manuscript.
Sources of support
Internal sources
-
No sources of support supplied
External sources
-
NIHR, UK.
The Cochrane Incontinence Group is supported by NIHR funding
Declarations of interest
Matthew J Jackson: nil
Rajan Veeraterapillay: nil
Christopher K Harding: speaker at meetings for Astellas, GSK, Lilly, Allergan and B Braun
Advisory Board for AMS
Trevor J Dorkin: speaker at meetings for Lilly, Pfizer and Astellas
Acknowledgements
We thank Sheila Wallace for undertaking the systematic literature search.
Version history
| Published | Title | Stage | Authors | Version |
| 2014 Dec 19 | Intermittent self‐dilatation for urethral stricture disease in males | Review | Matthew J Jackson, Rajan Veeratterapillay, Chris K Harding, Trevor J Dorkin | |
| 2012 Dec 12 | Intermittent self‐dilatation for urethral stricture disease in men | Protocol | Matthew J Jackson, Rajan Veeratterapillay, Chris Harding, Trevor Dorkin | |
Differences between protocol and review
Use of the GRADE methodology was not specified in the protocol but was adopted for the review to assess the quality of the evidence pertaining to the effect of intermittent self‐dilatation on risk of recurrent urethral stricture.
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
Medical Subject Headings Check Words
Humans; Male;
PICOs

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Comparison 1 ISD versus no treatment, Outcome 1 Recurrent urethral stricture.

Comparison 1 ISD versus no treatment, Outcome 2 Adverse events.

Comparison 2 One programme of ISD versus another, Outcome 1 Recurrent urethral stricture.

Comparison 3 One device for ISD versus another, Outcome 1 Recurrent urethral stricture (type of catheter).

Comparison 3 One device for ISD versus another, Outcome 2 Recurrent urethral stricture (catheter lubrication).
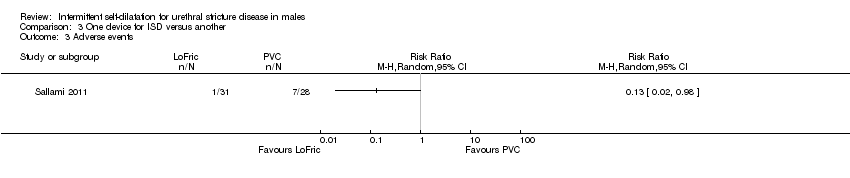
Comparison 3 One device for ISD versus another, Outcome 3 Adverse events.
| Intermittent self‐dilatation compared to no treatment for males after urethral stricture surgery | ||||||
| Population: males after urethral stricture surgery | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| No treatment | Intermittent self‐dilatation | |||||
| Recurrent urethral stricture | 618 per 1000 | 433 per 1000 | RR 0.7 | 404 | ⊕⊝⊝⊝ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Downgraded by two for risk of bias: all six trials comprising the quantitative synthesis were judged high risk of bias in two or more domains. | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Recurrent urethral stricture Show forest plot | 6 | 404 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.48, 1.00] |
| 2 Adverse events Show forest plot | 2 | 91 | Risk Ratio (M‐H, Random, 95% CI) | 0.60 [0.11, 3.26] |
| 2.1 Urinary tract infection/bacteriuria | 2 | 91 | Risk Ratio (M‐H, Random, 95% CI) | 0.60 [0.11, 3.26] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Recurrent urethral stricture Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.1 Short duration versus long duration of treatment | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Recurrent urethral stricture (type of catheter) Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 1.1 LoFric vs PVC | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Recurrent urethral stricture (catheter lubrication) Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2.1 Triamcinolone gel versus water‐based lubricant | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Adverse events Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |