Tonsillectomy for periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis syndrome (PFAPA)
Information
- DOI:
- https://doi.org/10.1002/14651858.CD008669.pub2Copy DOI

- Database:
-
- Cochrane Database of Systematic Reviews
- Version published:
-
- 11 September 2014see what's new
- Type:
-
- Intervention
- Stage:
-
- Review
- Cochrane Editorial Group:
-
Cochrane ENT Group
- Copyright:
-
- Copyright © 2014 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Article metrics
Altmetric:
Cited by:
Authors
Contributions of authors
Martin Burton: conceived protocol, extracted data, conducted analysis, reported results, contributed to final paper.
Andrew Pollard: conceived protocol, contributed to final paper.
James Ramsden: conceived protocol, extracted data, conducted analysis, reported results, contributed to final paper.
Roderick Venekamp: conducted searches, identified studies, extracted data, conducted analysis and prepared manuscript for the updated review in 2014.
Lee Yee Chong: identified studies, contacted authors, extracted data, conducted analysis and prepared manuscript for the update review in 2014.
All authors have reviewed and provided comment on the updated version of the review.
Sources of support
Internal sources
-
None, Other.
External sources
-
None, Other.
Declarations of interest
None known.
Acknowledgements
We gratefully acknowledge the assistance received from the staff at the Cochrane ENT Disorders Group editorial base in Oxford and gratefully thank Samantha Faulkner and Gemma Sandberg for their support with the search strategy and searches. We would also like to thank the peer reviewers, Mr William McKerrow and Dr Andrew Riordan, and editors for their valuable feedback, and the study authors (Marjo Renko) for responding to our queries.
Version history
| Published | Title | Stage | Authors | Version |
| 2019 Dec 30 | Tonsillectomy for periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis syndrome (PFAPA) | Review | Martin J Burton, Andrew J Pollard, James D Ramsden, Lee‐Yee Chong, Roderick P Venekamp | |
| 2014 Sep 11 | Tonsillectomy for periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis syndrome (PFAPA) | Review | Martin J Burton, Andrew J Pollard, James D Ramsden, Lee Yee Chong, Roderick P Venekamp | |
| 2010 Sep 08 | Tonsillectomy for periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis syndrome (PFAPA) | Review | Martin J Burton, Andrew J Pollard, James D Ramsden | |
Differences between protocol and review
In the 2014 update, we expanded the objective of the review to include evaluation of both clinical effectiveness and safety. We added additional outcomes to the review protocol, to ensure that both potential harms and benefits that are important to patients were captured in the review. These were complications of surgery (haemorrhage and number of days with postoperative pain), number of courses of corticosteroids, absence or time off school and quality of life.
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
Medical Subject Headings Check Words
Adolescent; Child; Child, Preschool; Humans; Infant;
PICOs

Process for sifting search results and selecting studies for inclusion

'Risk of bias' graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.

'Risk of bias' summary: review authors' judgements about each methodological quality item for each included study.
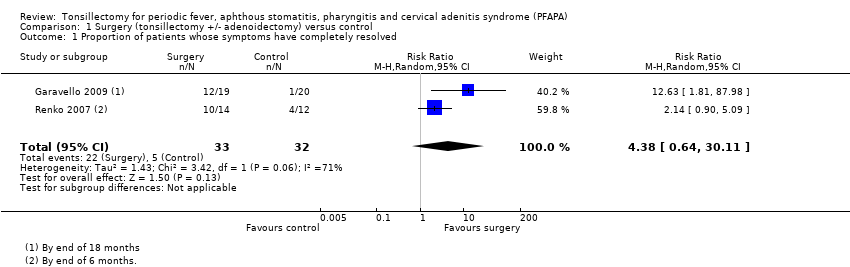
Comparison 1 Surgery (tonsillectomy +/‐ adenoidectomy) versus control, Outcome 1 Proportion of patients whose symptoms have completely resolved.
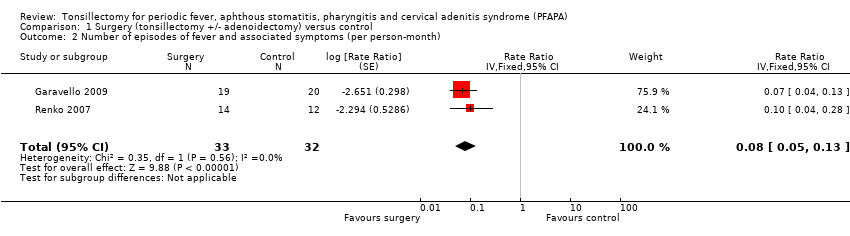
Comparison 1 Surgery (tonsillectomy +/‐ adenoidectomy) versus control, Outcome 2 Number of episodes of fever and associated symptoms (per person‐month).

Comparison 1 Surgery (tonsillectomy +/‐ adenoidectomy) versus control, Outcome 3 Use of corticosteroids.
| Surgery (tonsillectomy +/‐ adenoidectomy) for children with periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis syndrome (PFAPA) | ||||||
| Patient or population: children with PFAPA | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Surgery (tonsillectomy +/‐ adenoidectomy) | |||||
| Complete resolution of symptoms (proportion of patients with 'immediate and persistent resolution of symptoms' from the point of surgery/randomisation up to end of study follow‐up) | Study population (average) | RR 4.38 | 65 | ⊕⊕⊕⊝ | The NNTB based on the study population risk was 1/(684‐156)*1000 = 1.89 1 study followed up patients up to 6 months; another up to 18 months | |
| 156 per 1000 | 684 per 1000 | |||||
| Medium risk population | ||||||
| 192 per 1000 | 841 per 1000 | |||||
| Complications of surgery (haemorrhage and days with pain) | Both studies reported no complications from surgery Days of pain not reported as an outcome | |||||
| Number of episodes of fever and associated symptoms (episodes per person per month) | Mean 0.5 episode per person per month (1 episode every 2 months) | Mean 0.04 episode per person per month (1 episode every 25 months) | Rate ratio: 0.08 (0.05 to 0.13) | 65 | ⊕⊕⊕⊝ | |
| Severity of episodes (number of days with fever and the associated symptoms (per episode)) | Mean 3.5 (range of 2 to 6) days per episode | Mean 1.7 (range of 2 to 4) days per episode | Mean difference: 1.8 days per episode | 39 (1 study) | ⊕⊕⊕⊝ | Study reported statistical significance. Standard deviations were not reported in the study for average number of days per episode |
| Use of corticosteroids (proportion of patients using corticosteroids) | Study population (average) | RR 0.58 (0.37 to 0.92) | 39 (1 study) | ⊕⊕⊝⊝ | Review intended to report number of courses/patient, but these data were not available in the studies | |
| 900 per 1000 | 522 per 1000 | |||||
| Absence or time off school | None of the studies reported this | |||||
| Quality of life | None of the studies reported this | |||||
| *The basis for the assumed risk was the median risk in the control groups for "medium risk population" and for "study population", this was the average (i.e. total number of participants with events divided by total number of participants included in the meta‐analysis). The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Quality (confidence in the evidence) was reduced because of the small size of the studies and broad confidence intervals. There was also concern as to whether the treatment received by the control group reflects current practice. The criteria for recruitment of patients into one of the studies was not stringent and could have included patients who did not have PFAPA (Renko 2007). | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Proportion of patients whose symptoms have completely resolved Show forest plot | 2 | 65 | Risk Ratio (M‐H, Random, 95% CI) | 4.38 [0.64, 30.11] |
| 2 Number of episodes of fever and associated symptoms (per person‐month) Show forest plot | 2 | 65 | Rate Ratio (Fixed, 95% CI) | 0.08 [0.05, 0.13] |
| 3 Use of corticosteroids Show forest plot | 1 | 39 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.58 [0.37, 0.92] |