Administración prenatal de progestágenos para la prevención del parto prematuro espontáneo en pacientes con un embarazo múltiple
References
References to studies included in this review
References to studies excluded from this review
References to studies awaiting assessment
References to ongoing studies
Additional references
References to other published versions of this review
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods | Single‐centre, prospective, placebo‐controlled randomised clinical trial. | |
| Participants | 313 women at high risk of preterm birth, including 91 with twin pregnancy, with pregnancies conceived by IVF or ICSI Inclusion criteria: healthy pregnant women who conceived after IVF/ICSI between 18 to 24 weeks of gestation, with a first pregnancy, singleton or dichorionic twins, normal uterine and cervical anatomy, and normal fetal anatomy Exclusion criteria: previous pregnancy, serious fetal anomalies for which termination may be considered such as major heart anomaly or major CNS anomaly All women received progesterone injections as luteal phase support which they continued if pregnant until the day of the first ultrasound | |
| Interventions | Intervention group: vaginal progesterone 200 mg twice daily from randomisation until delivery or 37 weeks’ gestation. Total number randomised: n = 161 women (161 analysed, 210 babies) Control group: placebo vaginal suppositories from randomisation until 37 weeks’ gestation. Total number randomised: n = 152 women (145 women analysed, 187 babies) | |
| Outcomes | Primary outcomes: preterm birth of singleton and twin pregnancies before 37 completed weeks and before 34 completed weeks | |
| Notes | Funding sources: none reported. Declarations of interest: the authors report no financial or commercial conflicts of interest | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | States “Dark, sealed envelopes containing the intervention taken from a table of numbers” ‐ assume random as randomised study |
| Allocation concealment (selection bias) | Low risk | Refers to “dark, sealed, sequentially numbered envelopes” and the envelopes were picked by a nurse not involved in the study. The envelopes had been created by a third party not involved in the allocation process |
| Blinding of participants and personnel (performance bias) | Low risk | States “single blinding” and that “the patient was informed about the allocated arm” so presumably the clinician/personnel were blinded |
| Blinding of outcome assessment (detection bias) | Low risk | Not clear, but probably low risk. Placebo‐controlled trial |
| Incomplete outcome data (attrition bias) | Low risk | Study flow diagram clearly displays participant flow in the study 410 women recruited, 313 randomised; none lost to follow‐up in progesterone group and 6 lost to follow‐up in placebo group, and 1 excluded because of termination of pregnancy after diagnosis of trisomy 21. States “Intention‐to‐treat principle was followed during data analysis” |
| Selective reporting (reporting bias) | High risk | Trial registered after recruitment had started |
| Other bias | Low risk | Sample size calculation met. ITT analysis undertaken |
| Methods | Single‐centred, controlled, double‐blind trial with randomisation into 1 of 2 parallel groups, with a treatment‐to‐placebo ratio of 2:1. | |
| Participants | 293 women aged 18 years or more, with an ultrasound‐diagnosed twin pregnancy Exclusion criteria: ultrasonographically‐diagnosed fetal anomalies; elective cervical cerclage before 14 weeks' gestation; hypertension; diabetes; mellitus; asthma; history of deep vein thrombosis; history of hepatic disease or abnormal liver enzymes; pre‐existing renal disease or abnormal kidney function; and seizure disorders | |
| Interventions | Intervention group: participants received weekly injections of 250 mg 17‐hydroxyprogesterone caproate from 16 ‐ 20 weeks to 36 weeks of gestation Control group: participants received weekly placebo from 16 ‐ 20 weeks to 36 weeks of gestation | |
| Outcomes | Primary outcome: preterm birth prior to 37 weeks of gestation Secondary clinical outcomes measures included: early preterm birth (prior to 32 and 28 weeks of gestation); low birthweight < 2500 g or very low birthweight < 1500 g or extremely low birthweight < 1000 g; neonatal morbidity; perinatal mortality; and maternal morbidity. Neonatal morbidity defined as any of the following: respiratory distress syndrome; pneumonia; culture‐confirmed sepsis; intraventricular haemorrhage grade III or IV; necrotising enterocolitis; periventricular leukomalacia; retinopathy of prematurity; patent ductus arteriosus; seizures; and/or bronchopulmonary dysplasia. Maternal morbidity included any of the following maternal complications occurring during the course of pregnancy: gestational diabetes mellitus; hypertensive disorders; and preterm premature rupture of the membranes Safety outcome measures: local side effects and systemic adverse events | |
| Notes | Funding sources: This study was funded by a grant from the Medical Practice Plan at the American University of Beirut, Beirut, Lebanon (principal investigator: Anwar H. Nassar, MD). Declarations of interest: none of the authors of this article had any conflicts of interest to report | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Permutated block randomisation method. Random sequence generation used random‐number tables |
| Allocation concealment (selection bias) | Low risk | Randomisation envelopes prepared in pharmacy department. Research assistants opened the next opaque envelope following recruitment |
| Blinding of participants and personnel (performance bias) | Low risk | Treating doctors, investigators, ancillary personnel, and participants were all blinded to treatment assignment for the duration of the trial |
| Blinding of outcome assessment (detection bias) | Low risk | Investigators and ancillary personnel blinded for the duration of the trial |
| Incomplete outcome data (attrition bias) | Low risk | Outcome data reported for all randomised participants |
| Selective reporting (reporting bias) | Low risk | Stated outcomes reported |
| Other bias | Low risk | Sample size calculation met. ITT analysis undertaken. Ethics approval obtained |
| Methods | Placebo‐controlled, double‐blind randomised controlled trial. Participants were recruited from University of Mississippi Obstetric Clinics or Antenatal Diagnostic Unit, Mississippi. | |
| Participants | 30 women with twin gestations were randomised Inclusion criteria: between 20 – 30 weeks’ gestation, intact membranes, ability to understand and sign the consent form Exclusion criteria: severe medical disorders such as sickle cell disease, insulin‐dependent diabetes mellitus, chronic hypertension, cervical dilatation 1 cm, intrauterine growth restriction (10th percentile), growth discordancy between twins (20%), cerclage, uterine abnormalities or unwillingness to participate in the study protocol | |
| Interventions | Intervention group: participants received weekly injections of 250 mg 17‐alphahydroxyprogesterone from the time of randomisation until 34 weeks' gestation or delivery (whichever came first) Control group: participants received weekly injections of placebo (castor oil) from the time of randomisation until 34 weeks' gestation or delivery (whichever came first) | |
| Outcomes | Primary outcome: delivery before 35 completed weeks’ of gestation Preselected secondary outcomes: development of preterm labour, preterm rupture of the membranes and gestational age at delivery Selected infant data, including birthweight, Apgar score, total days in the NICU and occurrence of neonatal morbidity such as RDS, PDA, IVH, or NEC were also recorded. Those infants who died or were discharged with a neurologic handicap were also noted | |
| Notes | PharmaAmerica donated the 17‐hp Funding sources: not reported Declarations of interest: not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Women who met the above criteria were randomised when they presented to our outpatient facility by the selection of sequentially numbered, sealed, opaque envelopes generated and opened by a disinterested third party (UMC Pharmacy)" Assume random sequence generation. |
| Allocation concealment (selection bias) | Low risk | "Sequentially numbered, sealed, opaque envelopes." |
| Blinding of participants and personnel (performance bias) | Low risk | "An order was written by the treating physician that the patient was participating in the Twins‐progesterone trial. This order was submitted to pharmacy and an opaque, number‐coded syringe was returned to the treatment area." ...."The participating women, as well as research personnel and physicians/nurses, were unaware of the study group assessment." |
| Blinding of outcome assessment (detection bias) | Low risk | "research personnel and physicians/nurses, were unaware of the study group assessment." |
| Incomplete outcome data (attrition bias) | Low risk | Data available for all women who were randomised |
| Selective reporting (reporting bias) | High risk | Trial was not registered and no published protocol |
| Other bias | Low risk | Sample size calculation met. ITT not stated. |
| Methods | Double‐blind, placebo‐controlled randomised trial conducted at the Multiple Pregnancy Unit of the Obstetrics Department at Sao Paulo University of Medicine, Brazil | |
| Participants | 390 women with naturally‐conceived diamniotic twin pregnancies. Inclusion criteria: no history of preterm delivery (< 37 weeks’ gestation), gestational age of 18 to 21 weeks and 6 days at random assignment, absence of major fetal abnormalities (such as neural tube defects, abdominal wall defects, cardiac defects, hydrocephalus, and malformations that are associated with polyhydramnios) at the anomaly scan, no allergies to progesterone or peanuts (peanut oil is an excipient that is used in vaginal ovules), absence of hepatic dysfunction, porphyria, otosclerosis, malignant disease, severe depressive state, current or previous thromboembolic disease, uterine malformation, and prophylactic cerclage Exclusion criteria: subsequent diagnosis of major fetal abnormalities, the presence of ovular infection, or being lost to follow‐up | |
| Interventions | Intervention group: vaginal progesterone ovules (200 mg of natural micronised progesterone that also contained excipients such as peanut oil, soybean lecithin, glycerol, and titanium dioxide). Control group: placebo ovules | |
| Outcomes | Primary outcome: difference in mean gestational age at delivery Secondary outcomes included: spontaneous delivery at < 34 weeks’ gestation and the postnatal data until hospital discharge: birthweight, Apgar score < 7 at 5 minutes, hypoglycaemia, IVH grade 3, jaundice, NEC, PDA, retinopathy, septicaemia, admission to the NICU, RDS, the need for mechanical ventilation, death before hospital discharge, and composite neonatal outcome (defined as the occurrence of any of the following events: IVH, NEC, RDS, sepsis, and death before hospital discharge). | |
| Notes | Agra 2016 reports secondary analysis Funding sources: none reported. Declarations of interest: the authors report no conflict of interest | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random assignment was performed with a computer‐generated system with balanced blocks of 20 patients in each block |
| Allocation concealment (selection bias) | Low risk | The hospital's pharmacy department was responsible for packing and labelling the ovules (A and B); random assignment code was kept secret until data analysis |
| Blinding of participants and personnel (performance bias) | Low risk | Patients, researchers, and clinicians who were involved in clinical and ultrasonographic evaluations were blinded to the treatment assignment for the duration of the study |
| Blinding of outcome assessment (detection bias) | Low risk | Researchers blinded for duration of study. Code was kept secret until data analysis |
| Incomplete outcome data (attrition bias) | High risk | Outcome data missing for > 20% of neonates as they were born at other hospitals |
| Selective reporting (reporting bias) | Low risk | The trial was registered prospectively and expected outcomes were reported. (ClinicalTrials.gov Identifier: NCT01031017) |
| Other bias | Low risk | Sample size calculation met. No baseline differences in characteristics |
| Methods | Randomised, double‐blinded, placebo‐controlled trial | |
| Participants | 134 women with multiple pregnancies Inclusion criteria: < 21 weeks of gestation when randomised, pregnant women with triplets were eligible if their gestational age was at least 16 weeks and no more than 20 weeks | |
| Interventions | Intervention group: weekly injections of 17‐OHPC (250 mg in 1 mL castor oil) starting at 16 ‐ 20 + 6 weeks and ending at delivery or 35 weeks’ gestation | |
| Outcomes | Primary outcomes: composite of delivery or fetal loss before 35 completed weeks of gestation (245 days) ‐ fetal loss included:miscarriage, termination, or stillbirth occurring any time after randomisation. Secondary outcomes: selected individual maternal and neonatal outcomes and a composite of serious adverse neonatal outcomes, including: neonatal death, RDS, culture‐proven sepsis, NEC stage II or III, bronchopulmonary dysplasia, IVH grade III or IV, or periventricular leucomalacia or severe retinopathy of prematurity stage III or higher | |
| Notes | ClincialTrials.gov: NCT00099164 Funding sources: supported by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, (HD21410; HD27869; HD40512; HD27915; HD40485; HD34208; HD40500; HD34116; HD40560; HD40544; HD27917; HD27860; HD40545; HD53097; HD36801; HD34136) Declarations of interest: the authors disclosed no potential conflicts of interest | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “The simple urn‐method of randomization with stratification according to clinical center, was used to create a randomization sequence for each center.” |
| Allocation concealment (selection bias) | Low risk | The injections were prepared by a research pharmacy and boxes of 17‐OHPC and placebo were packaged for each centre according to randomisation sequences ‐ so appears to be central allocation ‐ pharmacy controlled |
| Blinding of participants and personnel (performance bias) | Low risk | “The participating women, their caregivers, and the research personnel were not aware of the study group assignment”. Also described as “double‐blinded” |
| Blinding of outcome assessment (detection bias) | Low risk | Not reported |
| Incomplete outcome data (attrition bias) | Low risk | “Outcome data were available for 100% of the assigned women, and for all of the 402 fetuses.” No exclusions apparent |
| Selective reporting (reporting bias) | Low risk | All expected outcomes appear to have been reported |
| Other bias | Low risk | No group differences in baseline characteristics. Sample size calculation met. ITT analysis undertaken |
| Methods | Randomised placebo‐controlled double‐blind study Department of Obstetrics and Gynecology, Istanbul, Turkey | |
| Participants | 170 women recruited (n = 160 randomised): 84 allocated to intervention and 76 allocated to placebo. Inclusion criteria: high‐risk pregnant women: twin pregnancies; pregnancies with at least 1 spontaneous preterm birth; uterine malformation; randomisation at 24 weeks' gestation Exclusion criteria: not stated. 2 abortions, 7 deliveries between 20 ‐ 24 weeks and 1 woman with prophylactic cerclage were excluded | |
| Interventions | Intervention group: micronised progesterone (100 mg) administered daily by vaginal suppository between 24 and 34 weeks of gestation | |
| Outcomes | Delivery < 37 weeks | |
| Notes | Funding sources: not reported Declarations of interest: not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random‐number list ‐ “Patients were allocated according to randomised number table”. |
| Allocation concealment (selection bias) | Low risk | Random‐number list generated centrally by research hospital pharmacy |
| Blinding of participants and personnel (performance bias) | Low risk | “The participating women, their caregivers, and the research personnel were unaware of the woman’s study‐group assignments.” |
| Blinding of outcome assessment (detection bias) | Low risk | Treatment assignment blinded until delivery of last pregnant woman |
| Incomplete outcome data (attrition bias) | Low risk | 160 women were randomised ‐ 10 lost during follow‐up, 6 from the placebo group and 4 from intervention group |
| Selective reporting (reporting bias) | High risk | Trial was not registered and no published protocol |
| Other bias | Low risk | Sample size calculation met. No baseline group differences. ITT analysis undertaken Ethics approval obtained |
| Methods | Double‐blind, randomised clinical trial | |
| Participants | 81 women randomised: 56 allocated to 17‐hp and 25 to placebo. Exclusion criteria: women with symptomatic uterine contractions, rupture of fetal membranes, any contraindication to interventions intended to prolong the pregnancy, a pre‐existing medical condition that might be worsened by progesterone, or a pre‐existing medical condition carrying a high risk of preterm delivery. Women less than 18 years of age, had an allergy to 17‐hp or the oil vehicle, had taken any progesterone‐derivative medication after 15 weeks of gestation, or had undergone placement of cervical cerclage for treatment of cervical change in the current pregnancy | |
| Interventions | Intervention group: 17‐alpha‐hydroxyprogesterone caproate (250 mg in 1 mL castor oil) ‐ weekly injections starting at 16 ‐ 22 weeks and continued until 34 weeks or delivery. Weekly repeat injections were carried out at the site or at home with partner administering after training. Injection diary for partner injections and measurement of unused medication returned by participant used to assess compliance with home administration | |
| Outcomes | Primary outcomes: composite neonatal morbidity defined as 1 or more of: perinatal death (stillbirth, neonatal death, miscarriage); RDS; use of oxygen therapy at 28 days of life; neonatal sepsis proven by blood culture; pneumonia; IVH (grade III or IV); periventricular leucomalacia; NEC requiring surgery; retinopathy of prematurity; newborn asphyxia Secondary outcomes: individual neonatal morbidities listed above; gestational age at delivery; birthweight; maternal side effects | |
| Notes | The trial was conducted under Investigational New Drug (IND) approval Number 69‐536, assigned by the United States Food and Drug Administration (FDA). Clinicaltrials.gov: NCT00163020 An independent Data and Safety Monitoring Board (DSMB) supervised the trial, reviewed adverse event reports, and conducted an interim analysis of efficacy Funding sources: supported by a grant from the Center for Research and Education, Pediatrix Medical Group, Sunrise, FL Declarations of interest: not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated scheme. Random‐number generated centrally by pharmacy |
| Allocation concealment (selection bias) | Low risk | Random‐number generated centrally by pharmacy. “Progesterone or identical‐appearing placebo was compounded by pharmacy and shipped in advance to each study site in coded pre‐numbered kits. To randomise the research nurse contacted the central pharmacy by telephone or fax to obtain the code number for the kit assigned to that patient.” |
| Blinding of participants and personnel (performance bias) | Low risk | “Subjects, physicians, and study personnel remained blinded as to group assignment until after completion of the trial.” |
| Blinding of outcome assessment (detection bias) | Low risk | “Data were abstracted by study personnel who remained blinded to each subject’s group assignment.” |
| Incomplete outcome data (attrition bias) | Low risk | 248 women identified with triplets, 147 eligible for trial inclusion. Of these 89 gave consent (61%) and were given trial injection. 81 (91%) returned for randomisation |
| Selective reporting (reporting bias) | Low risk | Yes ‐ all expected outcomes reported |
| Other bias | Low risk | Sample size calculation undertaken, but power based on number of neonates and so underpowered to detect differences in maternal outcomes. No baseline group differences. ITT analysis undertaken |
| Methods | Double‐blind, randomised clinical trial | |
| Participants | 240 women randomised: 160 allocated to 17‐hp and 80 to placebo. Inclusion criteria: women were eligible if they had a dichorionic‐diamniotic twin pregnancy at 15 ‐ 23 weeks’ gestation and if they had completed a detailed ultrasound examination, showing no major fetal anomalies Exclusion criteria: women < 18 years old, taken any progestins > 15 weeks of gestation, had symptomatic uterine contractions, rupture of the fetal membranes, any contraindication to prolonging the pregnancy, any pre‐existing condition that might be worsened by progesterone, or a pre‐existing medical condition carrying a high risk of preterm delivery | |
| Interventions | Intervention group: 17 alpha‐hydroxyprogesterone caproate (250 mg in 1 mL castor oil) ‐ weekly injections starting at 16 ‐ 24 weeks and continued until 34 weeks or delivery. Weekly repeat injections were carried out at the site or at home with partner administering after training. Injection diary for partner injections and measurement of unused medication returned by participant used to assess compliance with home administration Control/Comparison group: identical‐appearing placebo (in 1 mL castor oil) | |
| Outcomes | Primary outcomes: composite neonatal morbidity defined as 1 or more of: perinatal death (stillbirth, neonatal death, miscarriage); RDS; use of oxygen therapy at 28 days of life; neonatal sepsis proven by blood culture; pneumonia; IVH (grade III or IV); periventricular leucomalacia; NEC requiring surgery; retinopathy of prematurity; newborn asphyxia | |
| Notes | Funding sources: supported by a grant from the Center for Research, Education, and Quality, Pediatrix Medical Group, Mednax Inc, Sunrise, FL (groups of clinicians) Declarations of interest: not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated scheme. Random‐number generated centrally by pharmacy |
| Allocation concealment (selection bias) | Low risk | Random‐number generated centrally by pharmacy. “Progesterone or identical‐appearing placebo was compounded by pharmacy and shipped in advance to each study site in coded pre‐numbered kits. To randomise the research nurse contacted the central pharmacy by telephone or fax to obtain the code number for the kit assigned to that patient.” |
| Blinding of participants and personnel (performance bias) | Low risk | “Subjects, physicians, and study personnel remained blinded as to group assignment until after completion of the trial.” |
| Blinding of outcome assessment (detection bias) | Low risk | Study personnel remained blinded until after completion of the trial |
| Incomplete outcome data (attrition bias) | Low risk | No loss in progesterone group ‐ 160 women allocated, 160 mothers delivered and 320 perinates with known outcome. 80 women allocated to placebo ‐ 2 lost to follow‐up |
| Selective reporting (reporting bias) | High risk | Trial was not registered and no published protocol |
| Other bias | Low risk | Sample size calculation met. Interim analysis undertaken when 50% of data collected; primary outcome adjusted for this. No baseline group differences. Compliance 96.4% in the 17‐ph group and 98.7% in the placebo group (P .07) |
| Methods | Randomised controlled study. Mansoura University Hospital and private practice settings in Mansoura, Egypt Participants were recruited from June 2012 until November 2014 | |
| Participants | 225 women were recruited. Data for 116 intervention group and 108 controls Women with previous preterm birth were included (approximately 25% of each arm) Inclusion criteria: women aged 20 – 35 years old with dichorionic twin pregnancy were selected for measurement of cervical length by transvaginal sonography (TVS) at 20 – 24 weeks of gestation; cervical length of 20 – 25 mm with no symptoms or signs of impending preterm labour Exclusion criteria: known allergy or contraindication (relative or absolute) to progesterone therapy, monochorionic twins, known major fetal structural or chromosomal abnormality, single fetal demise, fetal reduction in current pregnancy, cervical cerclage in current pregnancy, medical conditions that may lead to preterm labour, rupture of membranes, vaginal bleeding | |
| Interventions | Intervention group: received vaginal progesterone suppositories (Cyclogest®, Actavis, Barnstaple, EX32 8NS, United Kingdom) in a dose of 400 mg daily, beginning 20 ‐ 24 weeks of gestation until 37 weeks of gestation Contol/comparison group: women received standard antenatal care | |
| Outcomes | Primary outcome: preterm labour before 34 weeks of gestation Secondary outcomes: neonatal RDS, early neonatal death (END) (not defined). | |
| Notes | Funding sources: not reported Declarations of interest: no conflicts of interests | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers |
| Allocation concealment (selection bias) | Low risk | Sealed unlabeled, opaque envelopes |
| Blinding of participants and personnel (performance bias) | High risk | The participants, caregivers and investigators were not blinded to group assignment |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not stated |
| Incomplete outcome data (attrition bias) | High risk | 9 of 125 (7%) women were lost to follow‐up in the intervention group and 17 of 125 (14%) in the control group. In addition to these 26, 42 women discontinued treatment due to noncompliance or perinatal complications. 182 women received the full course of treatment. Data for 224 |
| Selective reporting (reporting bias) | High risk | Trial was not registered and no published protocol |
| Other bias | Low risk | Sample size calculation met. No baseline group differences. ITT not stated |
| Methods | Setting: Finland, dates unclear Method of randomisation: stated to be “placebo controlled and double blind”. Data available for 77 women | |
| Participants | 77 women randomised; 39 women received 17‐hp and 38 received placebo Inclusion criteria: women with a twin pregnancy, between 28 and 33 weeks of gestation, no signs of preterm labour. | |
| Interventions | Intervention group: weekly intramuscular injections of 250 mg 17‐alpha hydroxyprogesterone caproate from 28 weeks until 37 weeks of gestation or birth, whichever came first. Comparison/control group: placebo in an equivalent volume from 28 weeks until 37 weeks of gestation or birth, whichever came first. 71 of 77 women had prophylactic bed rest from the 32nd week to the 36th gestational week | |
| Outcomes | Clinical outcomes included preterm birth before 37 weeks of gestation and perinatal mortality | |
| Notes | Funding sources: not reported Declarations of interest: not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not specified |
| Allocation concealment (selection bias) | Low risk | 'Medication code' specified |
| Blinding of participants and personnel (performance bias) | Unclear risk | Not specified |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not specified |
| Incomplete outcome data (attrition bias) | Low risk | Data available on all women randomised |
| Selective reporting (reporting bias) | High risk | Trial was not registered and no published protocol |
| Other bias | Unclear risk | No baseline group differences. Sample size calculation not described. ITT not stated |
| Methods | Multicentre, double‐bind, placebo‐controlled randomised trial Between July 2006 and August 2009 | |
| Participants | 671 women randomised: 336 allocated to progesterone and 335 allocated to placebo. Inclusion criteria: women with a multiple pregnancy and gestational age between 15 and 19 weeks Exclusion criteria: women with a previous spontaneous preterm birth before 34 weeks, serious congenital defects or death of 1 or more fetuses, early signs of twin‐to‐twin transfusion syndrome, or primary cerclage were excluded from participation | |
| Interventions | Intervention group: 1 mL 17‐hydoxyprogesterone caproate (250 mg/mL in castor oil) ‐ starting between 16 and 20 weeks and continuing to 36 weeks. Injections were administered at the clinic, by a general practitioner or, if the participant or a family member had a background in medical practice, at the participant’s home Control/Comparison group: 1 mL placebo (castor oil) ‐ study medication and placebo were identical in packaging, colour and consistency | |
| Outcomes | Primary outcomes: composite adverse neonatal outcome ‐ severe RDS; bronchopulmonary dysplasia; IVH grade II B or worse; NEC; proven sepsis; death before discharge Secondary outcomes: side effects (soreness, itching, and swelling; gestational age at delivery; preterm birth before 28, 32 and 37 weeks; length of admission to the NICU; maternal morbidity; hospitalisation of the mother due to (threatened) preterm labour; costs | |
| Notes | Funding sources: Funded by ZonMw, the Netherlands organization for health research and development (grant number 62200019) Declarations of interest: The authors did not report any potential conflicts of interest | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “An independent data manager rendered a computer‐generated list that was stratified by chorionicity, parity, and number of multiples, using random blocks of maximum block size.” |
| Allocation concealment (selection bias) | Low risk | Web‐based randomisation ‐ “Randomization was accessible through a website” and “Allocation code was known only to ACE Pharmaceuticals" |
| Blinding of participants and personnel (performance bias) | Low risk | “The participants, caregivers, and data collectors were all blinded to allocation." |
| Blinding of outcome assessment (detection bias) | Low risk | Data collectors were blinded. |
| Incomplete outcome data (attrition bias) | Low risk | Only 4 infants lost to follow‐up |
| Selective reporting (reporting bias) | Low risk | All expected outcomes reported |
| Other bias | Unclear risk | Other bias not apparent |
| Methods | Double‐blind randomised placebo‐controlled trial | |
| Participants | 500 women randomised: 250 allocated to progesterone and 250 allocated to placebo Inclusion criteria: women with twin pregnancy, with gestation and chorionicity established by scan before 20 weeks’ gestation and attending the antenatal clinic during the recruitment period Exclusion criteria: pregnancy complicated by a recognised structural or chromosomal fetal abnormality at the time of recruitment, or if they had contraindications to progesterone, planned cervical suture, planned elective delivery before 34 weeks’ gestation, or planned intervention for twin‐to‐twin transfusion before 22 weeks’ gestation. Women with higher multiple pregnancy were also excluded | |
| Interventions | Intervention group: daily vaginal progesterone gel 90 mg starting at 24 weeks and 0 days of gestation. Each applicator of intervention contained 1.45 g of gel and delivered 1.125 g of gel containing 8% progesterone Control/Comparison group: placebo gel ‐ administered in the same way as active treatment, daily from 24 weeks’ gestation. Each applicator of intervention contained 1.45 g of gel and delivered 1.125g of gel containing 8% excipients | |
| Outcomes | Primary outcome: delivery or intrauterine death before 34 weeks and 0 days of gestation. Delivery of the first twin was used to define the time of delivery. If 1 twin died in utero before 34 weeks and the other was born alive after 34 weeks, intrauterine fetal death was defined as occurring before 34 weeks. The gestational age was calculated from ultrasound scan done before 20 weeks Maternal secondary outcomes: gestation at delivery, method of delivery (spontaneous vaginal delivery, vaginal breech, forceps or ventouse, or caesarean section), duration of each stage of labour, and safety outcomes such as duration of stay in hospital. Neonatal secondary outcomes were neonatal unit admission and duration of neonatal unit care. Maternal satisfaction by questionnaire | |
| Notes | Funding sources: the authors disclosed receipt of the following financial support for the research and/or authorship of this article: grants CZB/4/408 from Chief Scientist Office (www.cso.scot.nhs.uk), Scottish Government; grant SP4068 from Action Medical Research (www.action.org.uk) and grants from Wellcome ‘‘Value in People’’ (www.wellcome.ac.uk) and the Jennifer Brown Research Laboratory (www.piggybankkids. org). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article Declarations of interest: the authors do not declare any conflicts of interest | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “We used a randomisation schedule with permuted blocks of randomly mixed sizes to make up treatment packs (either active or placebo) for every patient, which were held in individual hospital pharmacies until use.” |
| Allocation concealment (selection bias) | Low risk | Central allocation from research network ‐ local researcher telephoned the interactive voice response randomisation application at the UK Clinical Research Network registered trials unit to be given a participant number that corresponded to a specific treatment pack |
| Blinding of participants and personnel (performance bias) | Low risk | “All study personnel and participants were masked to treatment assignment for the duration of the study.” |
| Blinding of outcome assessment (detection bias) | Low risk | Study personnel masked to treatment |
| Incomplete outcome data (attrition bias) | Low risk | Only 6 women of 500 (3 from each treatment group) lost to follow‐up from 500 randomised participants. Analysis was ITT |
| Selective reporting (reporting bias) | Low risk | Expected outcomes reported |
| Other bias | Unclear risk | Other bias not apparent |
| Methods | Randomised, double‐blind, placebo‐controlled trial Between 1 June 2006 and 31 October 2008 | |
| Participants | 677 women were randomised: 334 allocated to progesterone and 343 allocated to placebo Inclusion criteria: women with a live, diamniotic twin pregnancy and chorionicity assessed by ultrasound before 16 weeks’ gestation were eligible for recruitment Exclusion criteria: age < 18 years; known allergy to progesterone or peanuts (active treatment contained peanuts); history of hormone‐associated thromboembolic disorders; rupture of membranes; treatment for or signs of twin‐to‐twin transfusion syndrome; intentional fetal reduction; known major structural or chromosomal fetal abnormality; known or suspected malignancy in genitals or breasts; known liver disease; women with higher‐order multiple pregnancies; women who did not speak and understand Danish or German | |
| Interventions | Intervention group: vaginal micronised progesterone pessaries (200 mg) ‐ self‐administered daily by participants ‐ starting from 20 ‐ 24 weeks until 34 weeks’ gestation | |
| Outcomes | Primary outcome: incidence of delivery before 34 + 0 weeks' gestation Prespecified secondary outcomes: delivery before 22, 28 and 32 weeks' gestation, number of liveborn infants, treatment with tocolytics and corticosteroids, birthweight, selected neonatal complications, neurophysiological development 6 and 18 months after the estimated date of delivery | |
| Notes | Funding sources: funding was provided by The Danish Medical Research Council, The Fetal Medicine Foundation, The Copenhagen University Hospital’s Research Fund, The Aase and Ejnar Danielsens Fund, The Augustinus Fund, The Ivan Nielsen Fund, The Doctor Sofus Carl Emil Friis and wife Olga Doris Friis’ Fund, The Simon Fougner Hartmanns Family Fund, The Danish Medical Society in Copenhagen and The A.P. Moeller Foundation Declarations of interest: the authors declare no conflict of interest | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random‐number sequence was used by the trial statistician to generate a randomisation code |
| Allocation concealment (selection bias) | Low risk | The boxes of progesterone and placebo were packed and labelled by Bilcare (Waller House, Wales, UK) according to this randomisation sequence and shipped to Copenhagen University Hospital, from where the study medication was distributed to the participating departments. Each local researcher telephoned the randomisation system, entered the participant's social security number and chorionicity, and was given a randomisation number that corresponded to a specific treatment box from a given batch |
| Blinding of participants and personnel (performance bias) | Low risk | All participants and study personnel were blinded to treatment assignment for the duration of the trial |
| Blinding of outcome assessment (detection bias) | Low risk | The randomisation code was not broken before all data had been collected |
| Incomplete outcome data (attrition bias) | Low risk | 2 women of 675 lost to follow‐up |
| Selective reporting (reporting bias) | Low risk | Stated outcomes reported |
| Other bias | Unclear risk | Other bias not apparent |
| Methods | Placebo‐controlled double‐blind randomised trial Trial conducted in 14 centres by the Maternal‐Fetal Medicine Network, USA From April 2004 until February 2006 | |
| Participants | 661 women with a twin pregnancy were randomised. Inclusion criteria: women carrying twins with a gestational age of at least 16 weeks and no more than 20 weeks and 3 days Exclusion criteria: known fetal anomaly, spontaneous fetal death of a fetus after 12 weeks, presumed mono‐amniotic placenta, suspected twin‐twin transfusion syndrome, marked ultrasonographic growth discordance, progesterone or heparin treatment during pregnancy, current or planned cervical cerclage, hypertension, insulin‐dependent diabetes, and twin pregnancies that were the result of intentional fetal reduction | |
| Interventions | Intervention group: weekly intramuscular injection of 250 mg 17‐hydroxyprogesterone caproate from 16 ‐ 20 + 3 weeks until 34 completed weeks’ gestation, or birth if earlier Control group: weekly intramuscular injection of placebo (castor oil) from 16 ‐ 20 + 3 weeks until 34 completed weeks’ gestation, or birth if earlier | |
| Outcomes | Primary outcome: composite of delivery or death prior to 35 weeks’ gestation Secondary outcomes: randomisation to delivery interval; composite adverse outcomes (retinopathy of prematurity, RDS, sepsis, NEC, bronchopulmonary dysplasia, grade III or IV IVH, periventricular leucomalacia), birthweight (less than 2500 g and less than 1500 g), 5‐minute Apgar score < 7, PDA, pneumonia, mechanical ventilation, seizures. Pretermbirth before 37 weeks’ gestation; birthweight less than 2.5 kg; stillbirth; neonatal death; IVH; RDS; bronchopulmonary dysplasia; sepsis; NEC; retinopathy of prematurity | |
| Notes | Funding sources: supported by grants (HD27869, HD21410, HD40512, HD34136, HD34208, HD40485, HD27915, HD40544, HD40560, HD27917, HD40500, HD34116, HD40545, HD27860, and HD36801) from the National Institute of Child Health and Human Development Declarations of interest: no potential sources of interest declared | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “The simple urn method of randomisation with stratification according to clinical center was used by the George Washington University Biostatistical Co‐ordinating Center to create a randomization sequence for each center...” |
| Allocation concealment (selection bias) | Low risk | Identical‐appearing treatment packs |
| Blinding of participants and personnel (performance bias) | Low risk | Women, caregivers and outcome assessors blinded |
| Blinding of outcome assessment (detection bias) | Low risk | Women, caregivers and outcome assessors blinded |
| Incomplete outcome data (attrition bias) | Low risk | Outcome data available for 655 of 661 women (less than 1% loss to follow‐up) |
| Selective reporting (reporting bias) | Low risk | All expected outcomes reported (delivery or fetal death before 35 weeks’ gestation; other obstetric and neonatal outcomes) |
| Other bias | Unclear risk | Other bias not apparent |
| Methods | Open‐label multicentre, randomised controlled trial France ‐ 13 French University Hospitals Between June 2006 and January 2010 | |
| Participants | 165 women randomised, 82 women randomised to the treatment group and 83 women randomised to the no‐treatment group Inclusion criteria: women older than 18 years, carrying twins, asymptomatic, and with a cervical length of 25 mm or less measured in the sagittal plane by routine transvaginal ultrasound according to the standard technique were eligible for inclusion. Women were 24+0 to 31+6 weeks' gestation Exclusion: cervical dilatation greater than 3 cm, premature rupture of the membranes, placenta previa, monochorial mono‐amniotic pregnancy, signs of twin‐to‐twin transfusion syndrome, severe intrauterine growth restriction of at least 1 fetus, known major structural or chromosomal fetal abnormality, death of 1 fetus, any maternal or fetal disease requiring preterm birth, progesterone therapy before inclusion, ongoing anticonvulsant treatment, or participation in any other treatment trial. Twin gestations resulting from intentional fetal reduction were also excluded | |
| Interventions | Intervention group: 500 mg of intramuscular 17‐alpha‐hydroxyprogesterone caproate, to be repeated twice weekly until 36 weeks or preterm delivery, whichever occurred first Control group: no treatment | |
| Outcomes | Primary outcome: time from randomisation to delivery Prespecified secondary outcomes: (1) obstetric criteria: rates of preterm birth before 37, 34, and 32 weeks and number of readmissions for preterm labour; (2) neonatal criteria: birthweight, transfer to the NICU, RDS, bronchopulmonary dysplasia, NEC, periventricular leukomalacia, and death; and (3) safety criteria: any severe maternal or neonatal adverse effects (congenital anomalies or other ill effects) | |
| Notes | Funding sources: this study was supported by a research grant from the Département à la Recherche Clinique Ile‐de‐France, Assistance Publique–Hôpitaux de Paris, which also sponsored the study (PHRC AOM 04038) Declarations of interest: the authors declare no conflicts of interest | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | An independent computer‐generated randomisation sequence was used for this allocation, based on a randomisation list established by the study statistician, according to a permutated block method |
| Allocation concealment (selection bias) | Low risk | States ‐ central randomisation. “A centralised, computer generated randomised process in a 1:1 ratio.” |
| Blinding of participants and personnel (performance bias) | High risk | Open‐label study |
| Blinding of outcome assessment (detection bias) | Unclear risk | Not stated |
| Incomplete outcome data (attrition bias) | Low risk | Data available on all participants |
| Selective reporting (reporting bias) | Low risk | Stated outcomes reported |
| Other bias | Unclear risk | Other bias not apparent |
| Methods | 3‐arm randomised controlled trial 5 University hospital centres in Spain Between December 2005 and January 2008. | |
| Participants | 294 women Inclusion criteria: women were recruited at 11 ‐ 13 weeks’ gestation. If they had previously been treated with vaginal progesterone it was stopped. Women were 18 years or more, dichorionic, diamniotic twin pregnancy Exclusion criteria: singleton pregnancy; monochorionic twin pregnancies; triplets or higher multiple pregnancies; elective cervical cerclage before 14 weeks’ gestation; history of hepatic problems; pregnancy cholestasis; abnormal liver or kidney function; allergy to peanuts or study medication; recurrent vaginal bleeding or infection; fetal anomalies; alcohol or illicit drug use and smoking more than 10 cigarettes per day | |
| Interventions | Intervention: | |
| Outcomes | Preterm birth rate < 37 weeks of gestation; early preterm birth rate < 34, 32, 28 weeks of gestation; need for tocolytic treatment; steroid treatment; rate of preterm premature rupture of membranes < 37 weeks of gestation; cervical length measurements at 20, 24, 28 weeks of gestation; perinatal mortality and morbidity; caesarean section. Local tolerance to the treatment; number of serious systemic adverse effects Perinatal outcomes: short‐term neonatal morbidity (RDS; pneumonia; early onset sepsis; seizures; graded III ‐ IV IVH; stage IIII NEC; and/or PDA). Long‐term neonatal morbidity included: broncho‐pulmonary dysplasia; periventricular leucomalacia; and/or severe retinopathy of prematurity, birthweight < 2500 g; 5 minute Apgar score; major congenital malformation; admission to NICU; mechanical ventilation; neonatal death | |
| Notes | Funding sources: the trial was funded by grant EF489‐2004/1 from Laboratorios Effik S.A. (Madrid, Spain) Declarations of interest: the authors declare no conflict of interest | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Randomisation was performed by computer (SPSS Random Number Generator, using a randomisation sequence 1:1:1 ratio (blocks of nine, with no stratification).” |
| Allocation concealment (selection bias) | Low risk | Central allocation “An external monitoring centre provided a randomisation code number for each pregnant woman” “The medication was given at each visit by the hospital pharmacy department”. |
| Blinding of participants and personnel (performance bias) | Low risk | Women and staff were blinded. Medication packs were coded and contained identical‐appearing pessaries |
| Blinding of outcome assessment (detection bias) | Low risk | It was reported that all study personnel were blind to treatment allocation for the duration of the project |
| Incomplete outcome data (attrition bias) | Low risk | There was very little loss to follow‐up It was stated that an ITT analysis was carried out |
| Selective reporting (reporting bias) | Unclear risk | Most expected outcomes reported upon. However ‐ individual outcome results for short‐term and long‐term neonatal morbidity were not reported, e.g. RDS, periventricular leucomalacia. |
| Other bias | Unclear risk | Other bias not apparent. |
| Methods | Double‐blinded, placebo‐controlled randomised trial Antenatal clinics at a tertiary care centre and an academic community hospital in Calgary, AB, Canada June 2006 and October 2010. | |
| Participants | 84 women were randomised Inclusion criteria: 2 or more live fetuses confirmed at their 16‐ to 18‐week ultrasound and were between 16 + 0 and 20 + 6 weeks gestation at the time of randomisation. Pregnancies reduced from higher‐order multiples to twins were also included if the reduction was carried out before 13 weeks gestation Exclusion: placenta previa, pre‐existing hypertension, known major fetal anomaly detected on ultrasound, monoamniotic monozygotic multiple pregnancies, maternal seizure disorder, active or history of thromboembolic disease, maternal liver disease, known or suspected breast malignancy or pathology, known or suspected progesterone‐dependent neoplasia, plans to move to another city during pregnancy, previous participation in this trial or other perinatal clinical trials during this pregnancy, or known sensitivity to progesterone | |
| Interventions | Intervention group: received daily doses of 90 mg progesterone 8% vaginal gel Control/Comparison group: daily doses of identical applicators containing gel without progesterone | |
| Outcomes | Primary outcome: gestational age at delivery Maternal secondary outcomes: preterm birth before 35 weeks ’ gestation; preterm birth before 37 weeks ’ gestation; the proportion of women who had a spontaneous delivery; length of hospital stay; the proportion of women who received tocolytic therapy; and compliance with treatment as measured by diary self‐report and return of unused applicators Infant secondary outcomes were length of hospital stay; RDS, defined as requiring assisted ventilation via endotracheal tube and supplemental oxygen both within the first 24 hours of life and for duration of ≥ 24 hours and either an X‐ray compatible with RDS or surfactant given between the first 2 and 24th hour of life; BPD, defined as requiring oxygen at postnatal GA of 36 completed weeks and X‐ray compatible with BPD; IVH grade III or IV diagnosed by cranial ultrasound or at autopsy; NEC, defined as perforation of the intestine, pneumatosis intestinalis, or air in the portal vein, diagnosed by X‐ray, surgery, or at autopsy; number of days of ventilator therapy; birthweight; stillbirth; and neonatal death. Any possible maternal or infant serious adverse events up to 28 days after delivery. | |
| Notes | Funding sources: This study was funded by the Calgary Health Region Perinatal Funding Competition (peer reviewed funding). We are grateful to Columbia Laboratories (Livingston, NJ, USA) who donated blinded active treatment and placebo gels Declarations of interest: the authors declared no conflicts of interest | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Used a random‐number generator with random block sizes of 2 or 4 |
| Allocation concealment (selection bias) | Low risk | The allocation sequence generated by the trial statistician was provided to the dispensing pharmacy. Once a woman consented, the pharmacy dispensed treatment according to the next randomisation allocation from the stratum to which the woman belonged |
| Blinding of participants and personnel (performance bias) | Low risk | Double‐blinded study |
| Blinding of outcome assessment (detection bias) | Low risk | Research nurse assessing dates was blinded to allocation. Assume true for outcome assessment |
| Incomplete outcome data (attrition bias) | Low risk | Outcomes reported for all randomised women and their infants |
| Selective reporting (reporting bias) | Low risk | Stated outcomes are reported |
| Other bias | Unclear risk | Other bias not apparent |
17‐hp: 17‐alphahydroxyprogesterone
17‐OHPC: 17 alpha‐hydroxyprogesterone caproate
BPD: bronchopulmonary dysplasia
ITT: intention to treat
IVH: intraventricular haemorrhage
NEC: necrotising enterocolitis
NICU: neonatal intensive care unit
PDA: patent ductus arteriosus
RDS: respiratory distress syndrome
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
| The comparison was not relevant (progesterone vs cerclage) | |
| Appears to be trial registration for a study examining effect of cervical pessary on preterm birth in twins, so not looking at progesterone | |
| No multiple pregnancies included | |
| 2 different types of progesterone compared | |
| Women in this study were already at term (36 ‐ 38 weeks) and no separate data for multiples | |
| Brief abstract ‐ comparison of progesterone with cerclage | |
| Women included in this study were at risk of preterm birth because of recurrent miscarriage and not because of multiple pregnancy | |
| This study included singletons only | |
| This study included singletons only | |
| It was not clear that this was a randomised trial | |
| This study included singletons only | |
| It was not clear that this was a randomised trial | |
| Comparison of progesterone versus cerclage ‐ not a relevant comparison for this review | |
| The criteria for high risk of preterm birth in this study did not include multiple pregnancy in current pregnancy | |
| This was not a randomised controlled trial. Alternate allocation | |
| Secondary analysis | |
| Abstract only, secondary analysis | |
| This study included singletons only | |
| This is secondary analysis for a trial that excluded multiple pregnancies | |
| This study examines the effects of type of conception on outcomes in twins | |
| This study included singletons only | |
| This is a study focusing on women at risk of preterm birth because of age | |
| Insufficient information to assess eligibility for inclusion | |
| This is a trial registration for a trial that has now been completed. The study examined relevant progesterone versus tocolytics and was aimed at delaying birth in preterm labour | |
| Trial registration for a study comparing progesterone with pessary device (not relevant comparison) | |
| This study included singletons only | |
| This study included singletons only | |
| This was a study of women in labour (or with symptoms of preterm labour) | |
| This study included singletons only | |
| Trial of progesterone versus cerclage which is not a relevant comparison for this review | |
| It was not clear that this was a randomised controlled trial | |
| This was not a randomised controlled trial (alternate allocation) | |
| This study examines the use of progesterone to prevent miscarriage |
Characteristics of studies awaiting assessment [ordered by study ID]
| Methods | RCT |
| Participants | Women with twin pregnancies |
| Interventions | 17OHP |
| Outcomes | Specifically looking at effectiveness in overweight and obese women |
| Notes | This may be secondary analysis of Meis 2003b but uncertain, and published only as an abstract. Awaiting assessment pending publication of fuller report. |
| Methods | Probably RCT ‐ women were "divided into 2 groups" |
| Participants | 100 women with twins |
| Interventions | Vaginal progesterone 200 mg daily from 24 ‐ 34 weeks versus placebo |
| Outcomes | Spontaneous preterm labour |
| Notes | Methods and outcomes unclear. We have been unable to find an email address for the trial authors. Awaiting assessment pending further information becoming available |
| Methods | RCT |
| Participants | Women with a short cervix as assessed by TV ultrasound at 22 weeks |
| Interventions | Vaginal progesterone |
| Outcomes | Spontaneous preterm birth less than 34 weeks, plus neonatal morbidity and adverse effects |
| Notes | Potentially eligible but twin outcomes not reported separately. Insufficient information to include |
| Methods | RCT |
| Participants | Twin pregnancies |
| Interventions | Progesterone vaginal gel |
| Outcomes | Preterm birth |
| Notes | Awaiting assessment pending further publications; no results are available yet |
| Methods | RCT |
| Participants | Women with DCDA twin pregnancies and short cervix |
| Interventions | Vaginal progesterone |
| Outcomes | Primary outcome = delivery before 37 weeks |
| Notes | Only trial registration available. Awaiting assessment pending further publications |
| Methods | RCT |
| Participants | 121 pregnant women at high risk for preterm delivery, inpatient? |
| Interventions | IM progesterone, oral progesterone versus oral (3 groups) |
| Outcomes | Abstract is not reported in a way to ascertain what outcomes were collected |
| Notes | Insufficient information to include/exclude as yet |
| Methods | Interventional study |
| Participants | 100 pregnant women |
| Interventions | IM 17OHP versus placebo |
| Outcomes | Gestational age, birthweight |
| Notes | This is potentially relevant and multiples are not explicitly excluded, there are no data for multiples; insufficient information to include |
17OHP: 17 alpha‐hydroxyprogesterone
DCDA: dichorionic diamniotic
IM: intramuscular
RCT: randomised controlled trial
TV: transvaginal
Characteristics of ongoing studies [ordered by study ID]
| Trial name or title | Progesterone after previous preterm birth for prevention of neonatal respiratory distress syndrome: the PROGRESS trial |
| Methods | Randomised, double‐blind, placebo‐controlled trial |
| Participants | 787 women recruited Women were eligible if they had a live fetus (singleton or twins), between 18 and 23 + 6 weeks' gestation and a history of prior preterm birth at < 37 weeks' gestation in the immediately preceding pregnancy (where the onset of labour occurred spontaneously, or in association with cervical incompetence, or following preterm prelabour ruptured membranes) |
| Interventions | Intervention: nightly vaginal pessaries of 100 mg progesterone from 20 weeks' gestation until birth or 34 weeks' gestation Control: nightly vaginal pessaries of similar‐appearing placebo, from 20 weeks' gestation until birth or 34 weeks' gestation |
| Outcomes | Preterm birth Infant respiratory distress syndrome |
| Starting date | Not clear |
| Contact information | Caroline Crowther |
| Notes | Waiting for trial to be published. Will be included when results are available |
| Trial name or title | Prevention of preterm birth in twin pregnancies ‐ “Randomised trial of progesterone versus placebo” |
| Methods | Multicentre, double‐blind, placebo‐controlled, randomised trial |
| Participants | Target number of women: 1180 Inclusion criteria: women with a twin pregnancy attending for their routine first trimester scan, 18 or over, DCDA or MCDA twin pregnancies, live fetuses at 11 ‐ 13 weeks of gestation, English‐ or Spanish‐speaking (otherwise interpreters will be used) Exclusion criteria: pregnancies complicated by major fetal abnormality identified at the 11‐13 weeks assessment, including nuchal translucency thickness > 3.5 mm, in MCDA twin pregnancies there are early signs of twin‐to‐twin transfusion syndrome (TTTS) (20% discordance in CRL and/or nuchal translucency), women who are unconscious or severely ill, those with learning difficulties, or serious mental illness, hypersensitivity to progesterone, concurrent participation in another drug trial or at any time within the previous 28 days, any other reason the clinical investigators think will prevent the potential participant from complying with the trial protocol |
| Interventions | Intervention: participants are required to insert a 300 mg progesterone suppository twice daily until 34 weeks’ gestation, or earlier in the event of preterm delivery |
| Outcomes | Primary outcome: Incidence of spontaneous delivery before 34 weeks (238 days) of gestation Secondary outcomes: 1. The incidence of spontaneous preterm birth < 37 weeks (259 days) of gestation |
| Starting date | April 2016 |
| Contact information | Dr Catalina De Paco Fetal Medicine Unit |
| Notes |
| Trial name or title | Comparing double dose of vaginal progesterone to no treatment for prevention of preterm birth in twins and short cervix |
| Methods | Open‐label, parallel, randomised trial |
| Participants | Estimated enrolment: 214 Inclusion criteria: twin gestation, certain dating (documented first trimester ultrasound, or a reliable menstrual date confirmed by an ultrasound performed before 20 weeks of gestation), age > 18 years, gestational age 16 ‐ 26, cervical length < 25 mm, intact membranes, informed consent Exclusion criteria: major malformation or chromosomal abnormality to at least 1 fetus, higher order pregnancy, mocochorional‐monoamniotic twin, death of 1 fetus, cervical dilatation > 3 cm, chronic medical conditions that would interfere with study participation or evaluation of the treatment (e.g. seizures, psychiatric disorders, uncontrolled chronic hypertension, congestive heart failure, chronic renal failure, uncontrolled diabetes mellitus with end‐organ dysfunction, active thrombophlebitis or a thromboembolic disorder, history of hormone‐associated thrombophlebitis or thromboembolic disorders, active liver dysfunction or disease, known or suspected malignancy of the breast or genital organs) |
| Interventions | Intervention: treatment with 400 mg micronised progesterone (Utrogestan) daily up to 36 weeks of gestation |
| Outcomes | Preterm delivery (time frame: up to 25 weeks from randomisation) |
| Starting date | January 2015 |
| Contact information | Noah Zafran |
| Notes |
| Trial name or title | A randomised trial of Pessary and Progesterone for Preterm Prevention in Twin Gestation With a Short Cervix (PROSPECT) |
| Methods | 3‐armed, double‐blind, parallel, randomised trial |
| Participants | 600 women randomised Inclusion criteria: women with twin pregnancy, cervical length of < 30 millimetres, gestation 16 ‐ 24 weeks Exclusion criteria: cervical dilation (internal os) 2 cm or greater on digital examination or evidence of prolapsed membranes beyond the external cervical os, monoamniotic gestation, twin‐twin transfusion syndrome, evidence of severe IUGR, fetal anomaly in either twin or imminent fetal demise, placenta previa, active vaginal bleeding greater than spotting at the time of randomisation, symptomatic, untreated vaginal or cervical infection, rupture of membranes, more than 6 contractions per hour, known major Mullerian anomaly of the uterus, any fetal/maternal condition which would require invasive in‐utero assessment or treatment, major maternal medical illness associated with increased risk for adverse pregnancy outcome or indicated preterm birth, planned cerclage or cerclage already in place, planned indicated delivery prior to 35 weeks, planned or actual progesterone treatment of any type or form after 14 weeks 6 days during the current pregnancy, allergy to progesterone or excipients in the study drug or placebo, participation in another interventional study that influences gestational age at delivery or neonatal morbidity or mortality, participation in this trial in a previous pregnancy, prenatal care or delivery planned elsewhere |
| Interventions | Intervention 1: progesterone‐ 200 mg micronised vaginal progesterone soft gel capsule, daily from randomisation to < 35 weeks Intervention 2: Arabin pessary placement management from randomisation to < 35 weeks |
| Outcomes | Primary outcome: Delivery prior to 35 weeks or fetal loss Secondary outcomes: 1. Randomisation to delivery interval 2. Gestational age at delivery 3. Neonatal morbidity and mortality 4. Lower genital tract or urinary tract infection 5. Physician interventions |
| Starting date | October 2015 |
| Contact information | Uma Reddy |
| Notes |
CRL: crown‐rump length
DCDA: dichorionic diamniotic
IUGR: intra‐uterine growth retardation
NICU: neonatal intensive care unit
OVH: intraventricular haemorrhage
MCDA: monochorionic diamniotic
NEC: necrotising enterocolitis
RDS: respiratory distress syndrome
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Preterm birth less than 34 weeks Show forest plot | 2 | 399 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.54 [1.06, 2.26] |
| Analysis 1.1 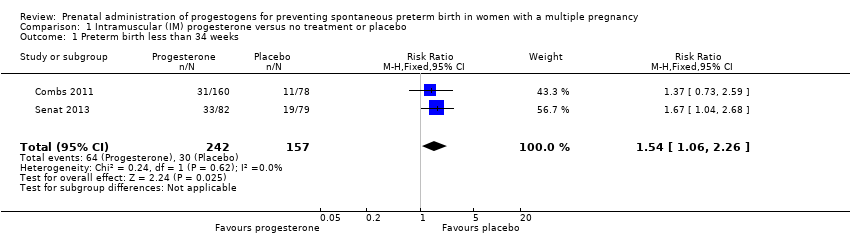 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 1 Preterm birth less than 34 weeks. | ||||
| 2 Preterm birth less than 34 weeks subgroup by dose Show forest plot | 2 | 399 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.54 [1.06, 2.26] |
| Analysis 1.2 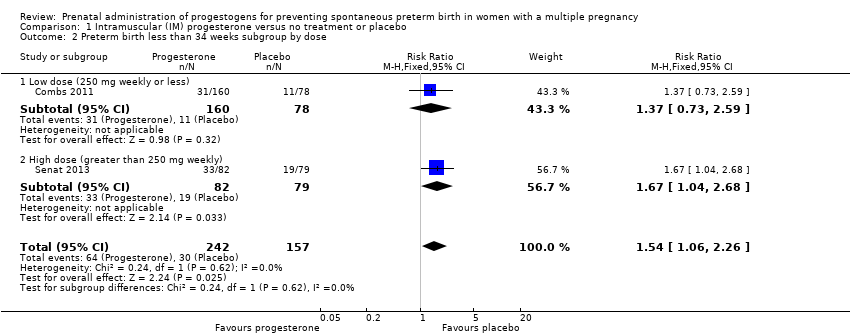 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 2 Preterm birth less than 34 weeks subgroup by dose. | ||||
| 2.1 Low dose (250 mg weekly or less) | 1 | 238 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.37 [0.73, 2.59] |
| 2.2 High dose (greater than 250 mg weekly) | 1 | 161 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.67 [1.04, 2.68] |
| 3 Preterm birth less than 34 week subgroup by timing Show forest plot | 2 | 399 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.54 [1.06, 2.26] |
| Analysis 1.3 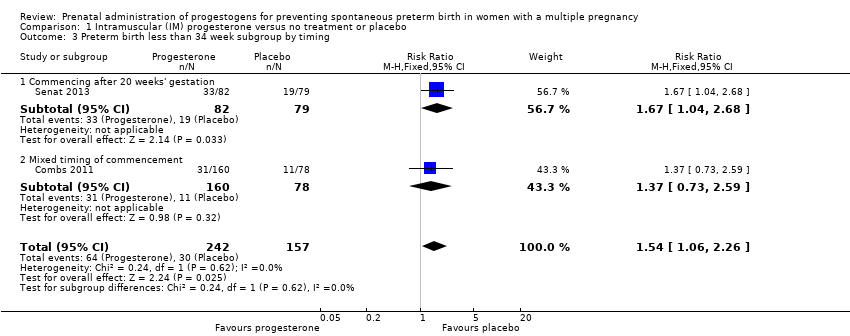 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 3 Preterm birth less than 34 week subgroup by timing. | ||||
| 3.1 Commencing after 20 weeks' gestation | 1 | 161 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.67 [1.04, 2.68] |
| 3.2 Mixed timing of commencement | 1 | 238 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.37 [0.73, 2.59] |
| 4 Perinatal death Show forest plot | 6 | 3089 | Risk Ratio (M‐H, Random, 95% CI) | 1.45 [0.60, 3.51] |
| Analysis 1.4 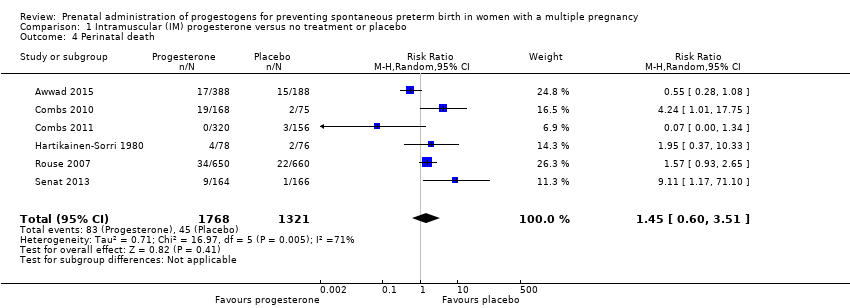 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 4 Perinatal death. | ||||
| 5 Perinatal death subgroup by dose Show forest plot | 6 | 3089 | Risk Ratio (M‐H, Random, 95% CI) | 1.45 [0.60, 3.51] |
| Analysis 1.5 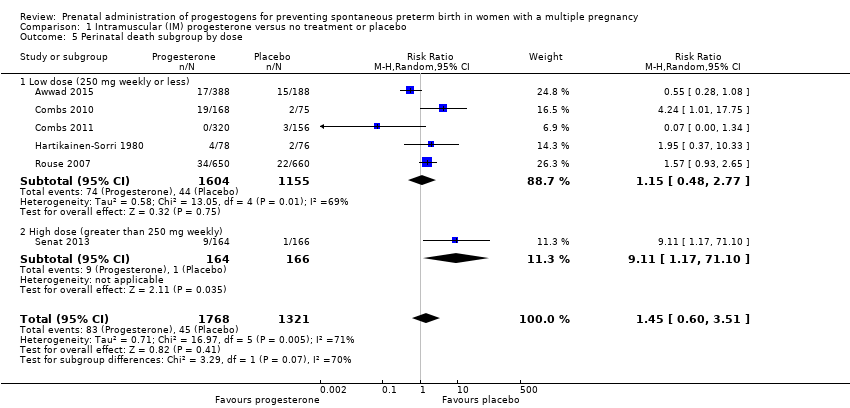 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 5 Perinatal death subgroup by dose. | ||||
| 5.1 Low dose (250 mg weekly or less) | 5 | 2759 | Risk Ratio (M‐H, Random, 95% CI) | 1.15 [0.48, 2.77] |
| 5.2 High dose (greater than 250 mg weekly) | 1 | 330 | Risk Ratio (M‐H, Random, 95% CI) | 9.11 [1.17, 71.10] |
| 6 Perinatal death subgroup by timing Show forest plot | 6 | 3089 | Risk Ratio (M‐H, Random, 95% CI) | 1.45 [0.60, 3.51] |
| Analysis 1.6 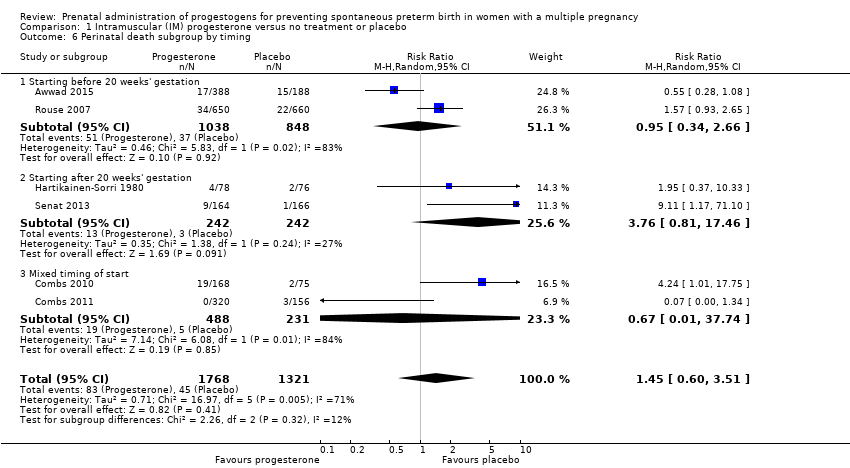 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 6 Perinatal death subgroup by timing. | ||||
| 6.1 Starting before 20 weeks' gestation | 2 | 1886 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.34, 2.66] |
| 6.2 Starting after 20 weeks' gestation | 2 | 484 | Risk Ratio (M‐H, Random, 95% CI) | 3.76 [0.81, 17.46] |
| 6.3 Mixed timing of start | 2 | 719 | Risk Ratio (M‐H, Random, 95% CI) | 0.67 [0.01, 37.74] |
| 7 Prelabour rupture of the membranes Show forest plot | 6 | 1257 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.17 [0.84, 1.63] |
| Analysis 1.7 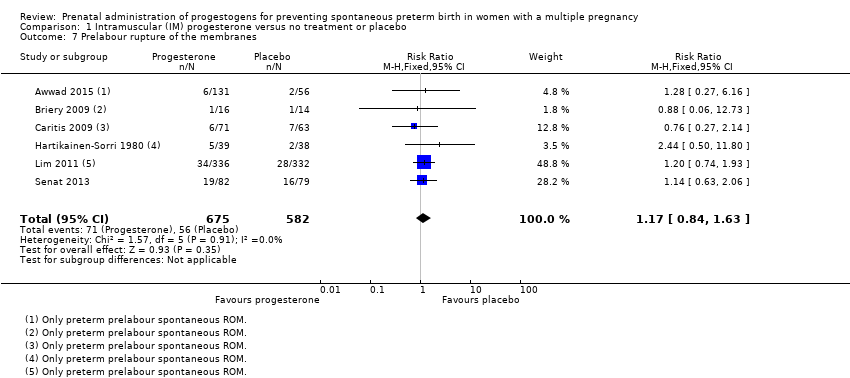 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 7 Prelabour rupture of the membranes. | ||||
| 8 Preterm birth less than 37 weeks Show forest plot | 5 | 2010 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.98, 1.13] |
| Analysis 1.8 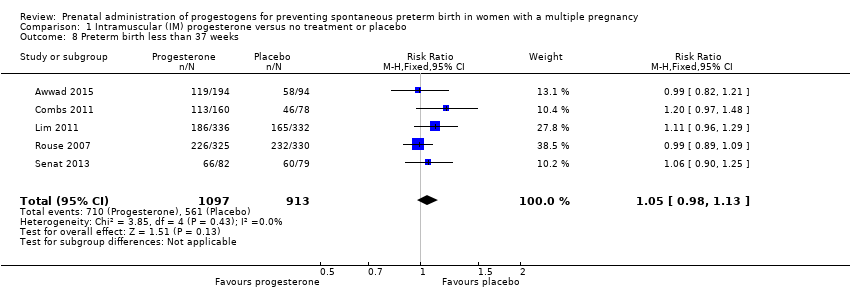 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 8 Preterm birth less than 37 weeks. | ||||
| 9 Preterm birth less than 28 weeks Show forest plot | 5 | 1920 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.75, 1.55] |
| Analysis 1.9 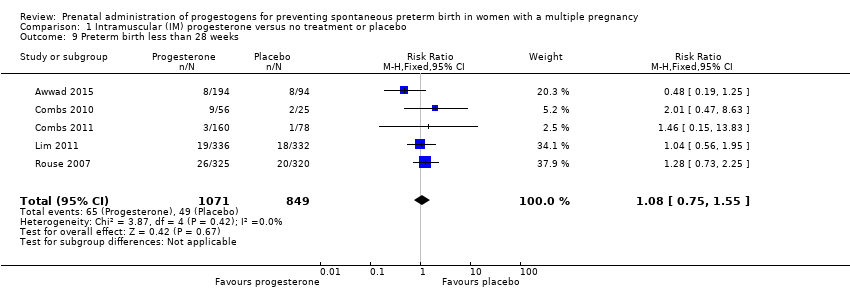 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 9 Preterm birth less than 28 weeks. | ||||
| 10 Adverse drug reaction Show forest plot | 2 | 1316 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.63, 1.32] |
| Analysis 1.10 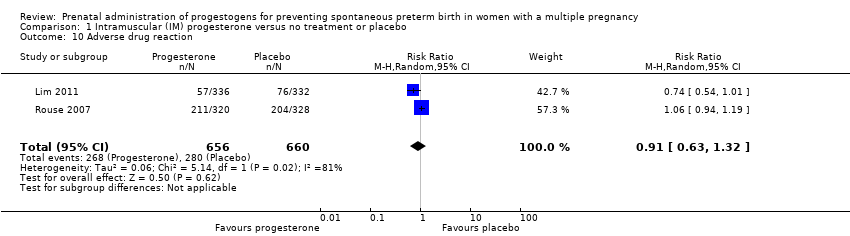 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 10 Adverse drug reaction. | ||||
| 11 Caesarean section Show forest plot | 7 | 2222 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.95, 1.08] |
| Analysis 1.11 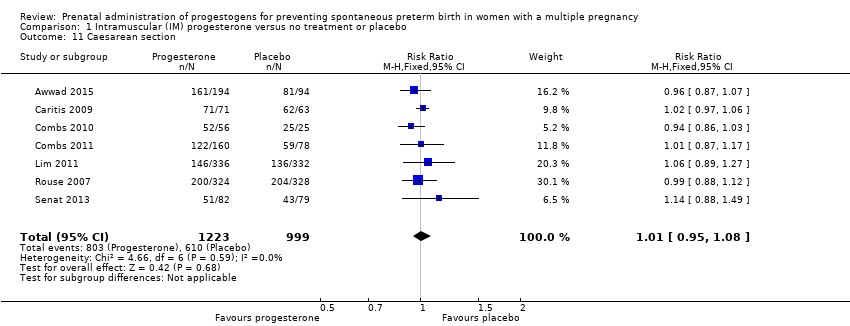 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 11 Caesarean section. | ||||
| 12 Antenatal tocolysis Show forest plot | 7 | 2218 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.85, 1.10] |
| Analysis 1.12 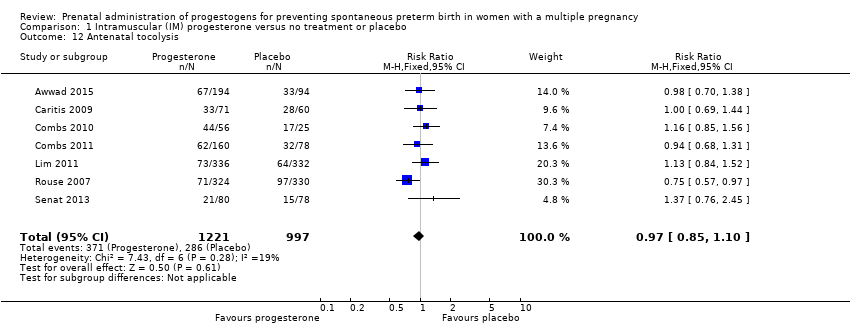 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 12 Antenatal tocolysis. | ||||
| 13 Antenatal corticosteroids Show forest plot | 7 | 2221 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.88, 1.11] |
| Analysis 1.13 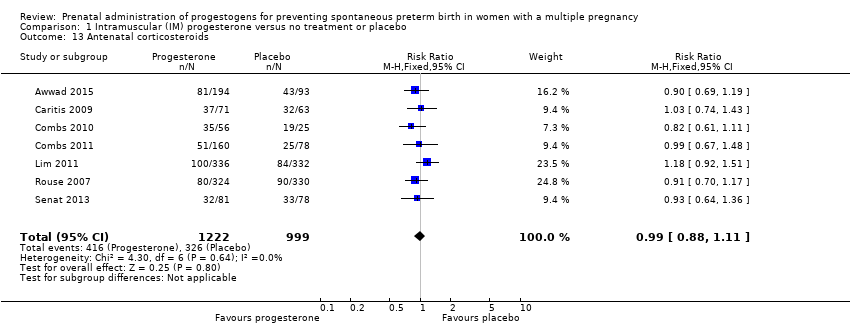 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 13 Antenatal corticosteroids. | ||||
| 14 Infant birthweight less than 2500 g Show forest plot | 5 | 4071 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.90, 1.08] |
| Analysis 1.14 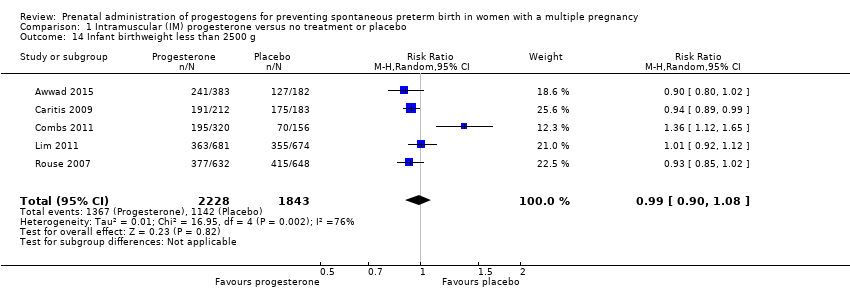 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 14 Infant birthweight less than 2500 g. | ||||
| 15 Apgar score < 7 at 5 minutes Show forest plot | 4 | 3606 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.89 [0.68, 1.15] |
| Analysis 1.15 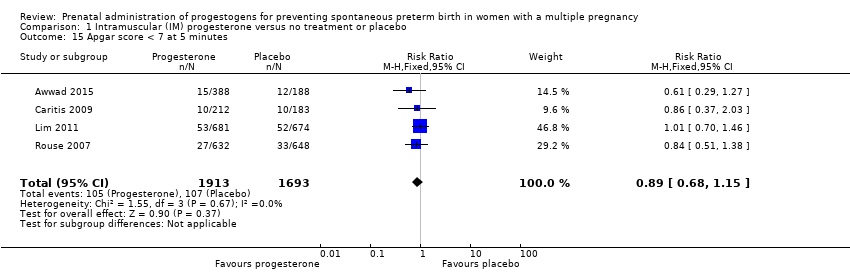 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 15 Apgar score < 7 at 5 minutes. | ||||
| 16 Neonatal sepsis Show forest plot | 6 | 3327 | Risk Ratio (M‐H, Random, 95% CI) | 1.02 [0.41, 2.51] |
| Analysis 1.16 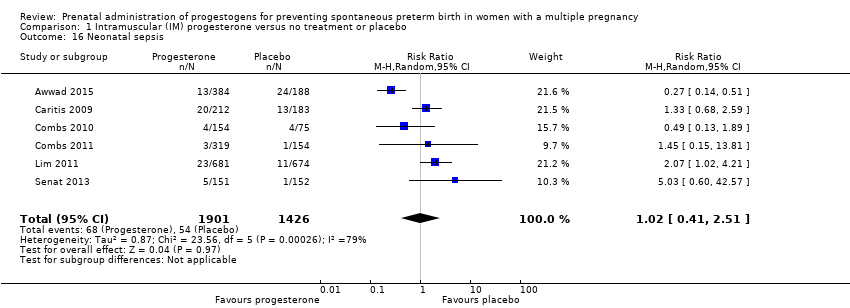 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 16 Neonatal sepsis. | ||||
| 17 Respiratory distress syndrome Show forest plot | 8 | 4670 | Risk Ratio (M‐H, Random, 95% CI) | 1.07 [0.85, 1.34] |
| Analysis 1.17 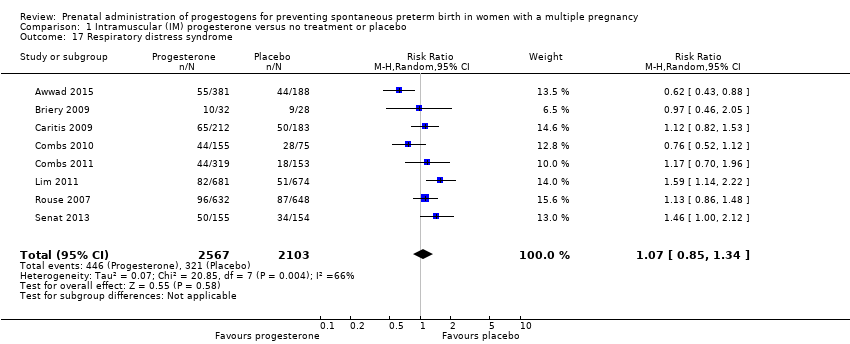 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 17 Respiratory distress syndrome. | ||||
| 18 Use of mechanical ventilation Show forest plot | 3 | 2233 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.69, 1.17] |
| Analysis 1.18 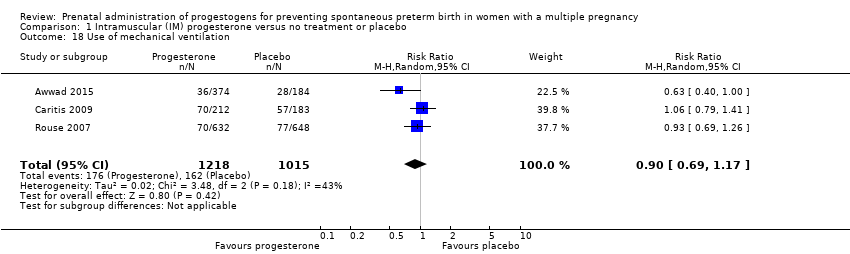 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 18 Use of mechanical ventilation. | ||||
| 19 Intraventricular haemorrhage ‐ all grades Show forest plot | 1 | 1355 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.98 [0.36, 10.77] |
| Analysis 1.19 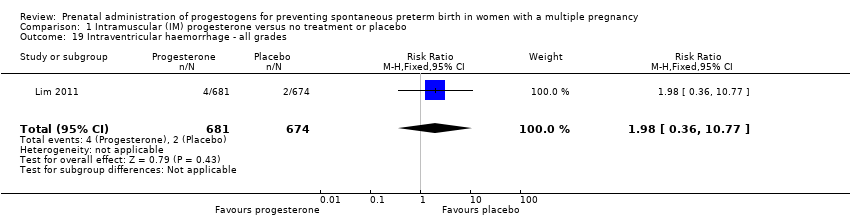 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 19 Intraventricular haemorrhage ‐ all grades. | ||||
| 20 Retinopathy of prematurity Show forest plot | 5 | 2807 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.34 [0.16, 0.74] |
| Analysis 1.20 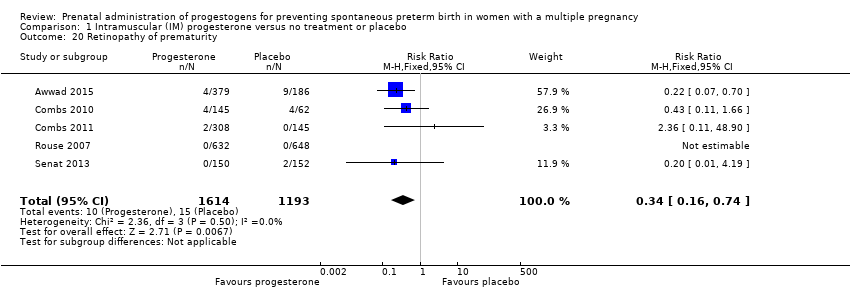 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 20 Retinopathy of prematurity. | ||||
| 21 Chronic lung disease Show forest plot | 2 | 681 | Risk Ratio (M‐H, Random, 95% CI) | 1.91 [0.13, 27.80] |
| Analysis 1.21 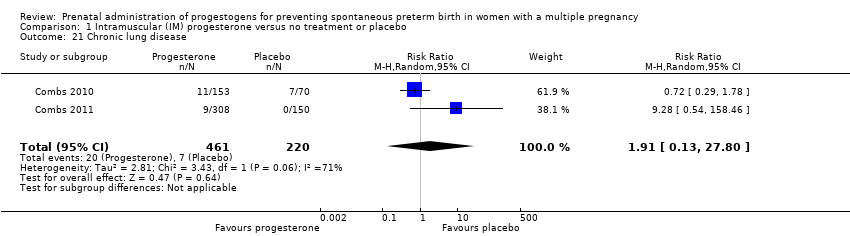 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 21 Chronic lung disease. | ||||
| 22 Necrotising enterocolitis Show forest plot | 5 | 2610 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.74 [0.36, 1.51] |
| Analysis 1.22 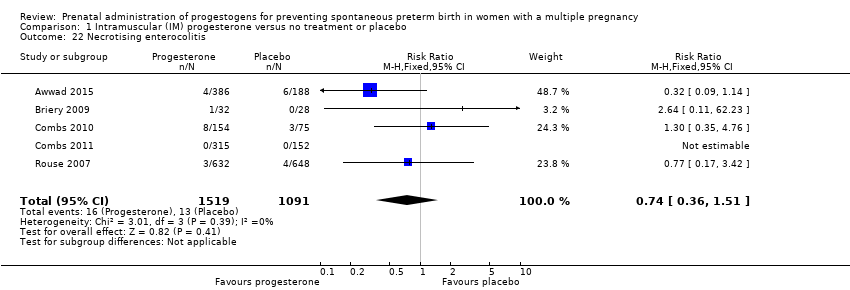 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 22 Necrotising enterocolitis. | ||||
| 23 Fetal death Show forest plot | 4 | 3536 | Risk Ratio (M‐H, Random, 95% CI) | 0.93 [0.39, 2.20] |
| Analysis 1.23 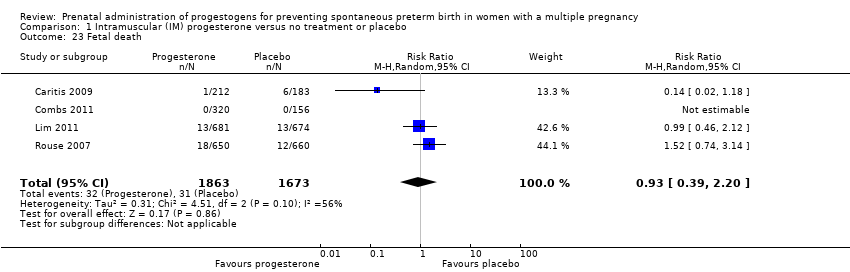 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 23 Fetal death. | ||||
| 24 Neonatal death Show forest plot | 7 | 3399 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.44, 1.91] |
| Analysis 1.24 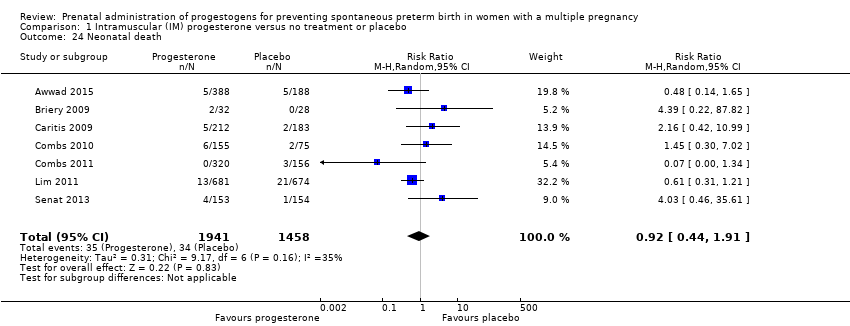 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 24 Neonatal death. | ||||
| 25 Admission to NICU Show forest plot | 2 | 1668 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.33 [1.13, 1.58] |
| Analysis 1.25 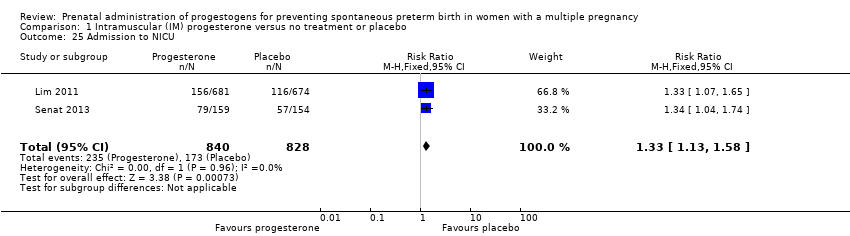 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 25 Admission to NICU. | ||||
| 26 Patent ductus arteriosus Show forest plot | 4 | 2290 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.37, 2.21] |
| Analysis 1.26 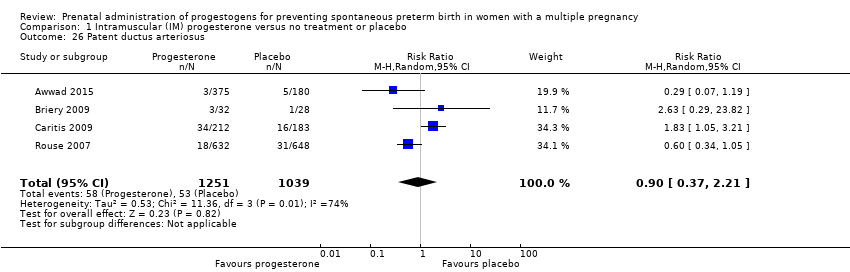 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 26 Patent ductus arteriosus. | ||||
| 27 Sensitivity analysis for perinatal death (assuming total dependence) Show forest plot | 6 | 1517 | Risk Ratio (M‐H, Random, 95% CI) | 1.35 [0.57, 3.20] |
| Analysis 1.27 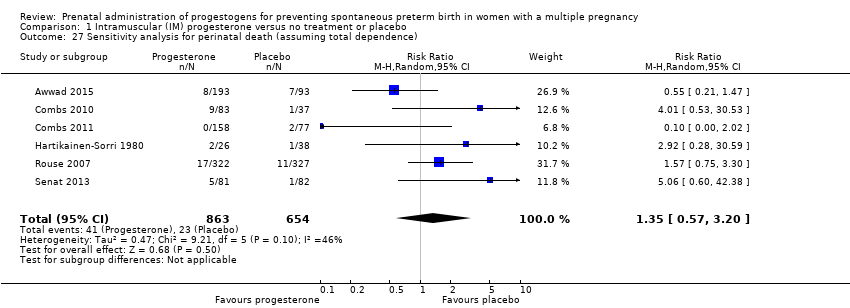 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 27 Sensitivity analysis for perinatal death (assuming total dependence). | ||||
| 28 Sensitivity analysis for perinatal death (assuming 1% dependence) Show forest plot | 6 | 3021 | Risk Ratio (M‐H, Random, 95% CI) | 1.45 [0.60, 3.49] |
| Analysis 1.28 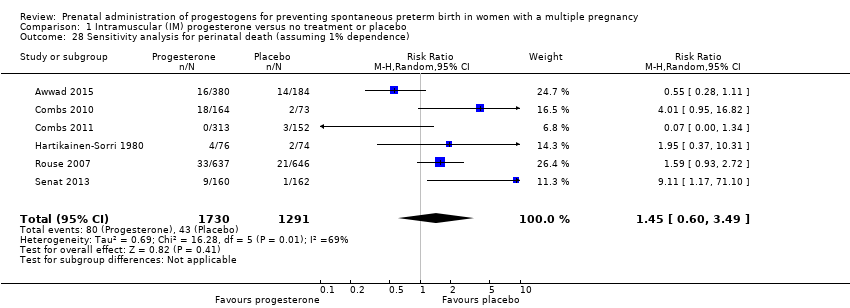 Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 28 Sensitivity analysis for perinatal death (assuming 1% dependence). | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Preterm birth less than 34 weeks Show forest plot | 6 | 1727 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.63, 1.09] |
| Analysis 2.1 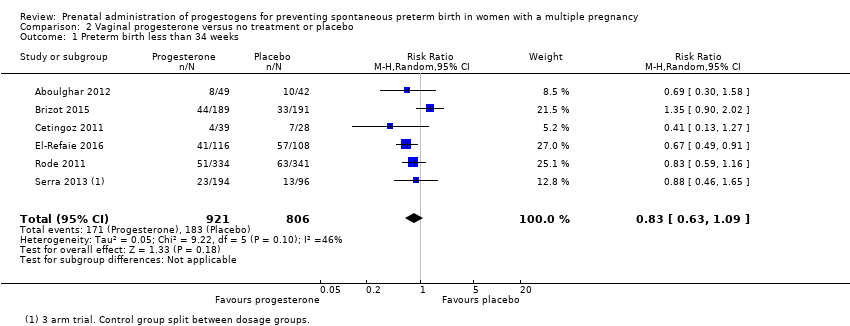 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 1 Preterm birth less than 34 weeks. | ||||
| 2 Preterm birth less than 34 weeks subgroup by dose Show forest plot | 6 | 1727 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.64, 1.07] |
| Analysis 2.2 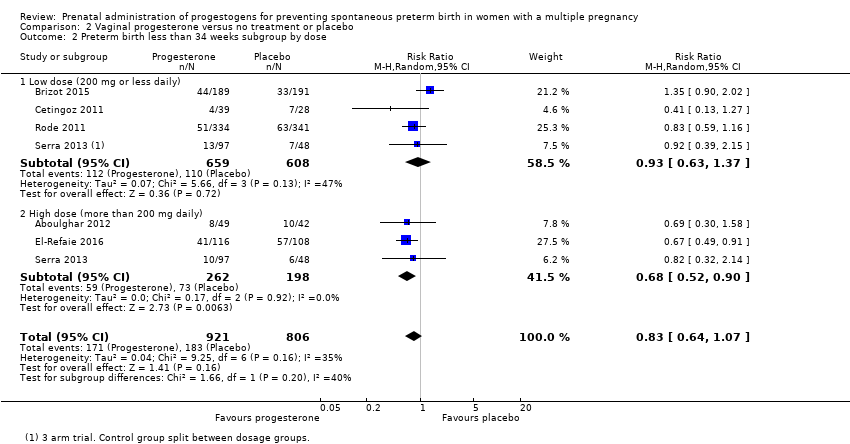 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 2 Preterm birth less than 34 weeks subgroup by dose. | ||||
| 2.1 Low dose (200 mg or less daily) | 4 | 1267 | Risk Ratio (M‐H, Random, 95% CI) | 0.93 [0.63, 1.37] |
| 2.2 High dose (more than 200 mg daily) | 3 | 460 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.52, 0.90] |
| 3 Preterm birth less than 34 weeks subgroup by timing Show forest plot | 6 | 1727 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.63, 1.09] |
| Analysis 2.3 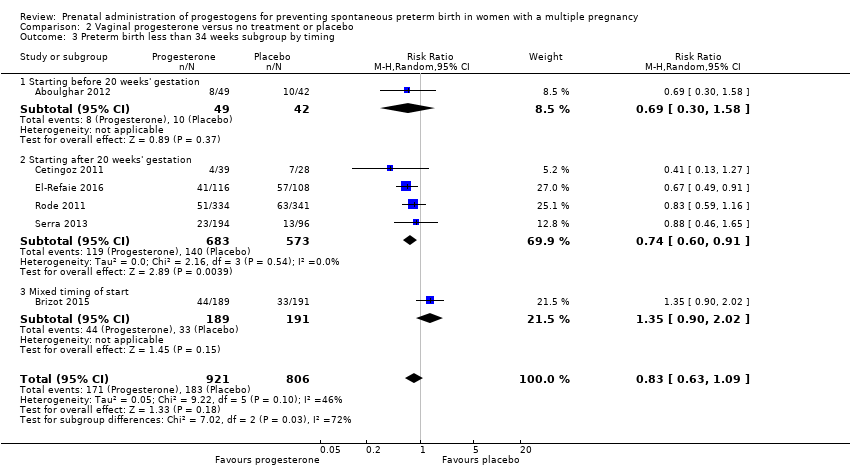 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 3 Preterm birth less than 34 weeks subgroup by timing. | ||||
| 3.1 Starting before 20 weeks' gestation | 1 | 91 | Risk Ratio (M‐H, Random, 95% CI) | 0.69 [0.30, 1.58] |
| 3.2 Starting after 20 weeks' gestation | 4 | 1256 | Risk Ratio (M‐H, Random, 95% CI) | 0.74 [0.60, 0.91] |
| 3.3 Mixed timing of start | 1 | 380 | Risk Ratio (M‐H, Random, 95% CI) | 1.35 [0.90, 2.02] |
| 4 Perinatal death Show forest plot | 3 | 2287 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.74, 2.06] |
| Analysis 2.4 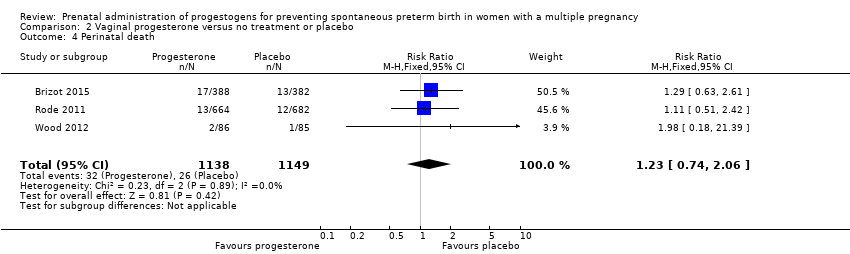 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 4 Perinatal death. | ||||
| 5 Perinatal death subgroup by dose Show forest plot | 3 | 2287 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.74, 2.06] |
| Analysis 2.5 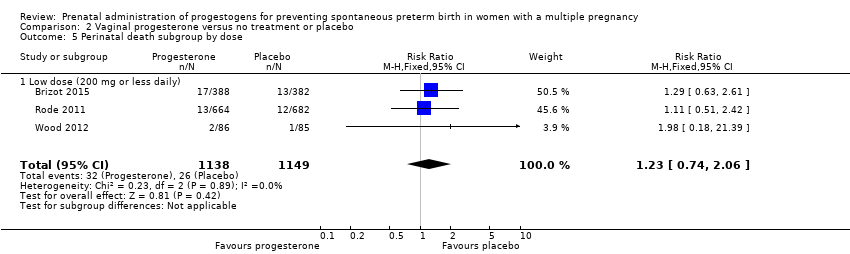 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 5 Perinatal death subgroup by dose. | ||||
| 5.1 Low dose (200 mg or less daily) | 3 | 2287 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.74, 2.06] |
| 6 Perinatal death subgroup by timing Show forest plot | 3 | 2287 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.74, 2.06] |
| Analysis 2.6 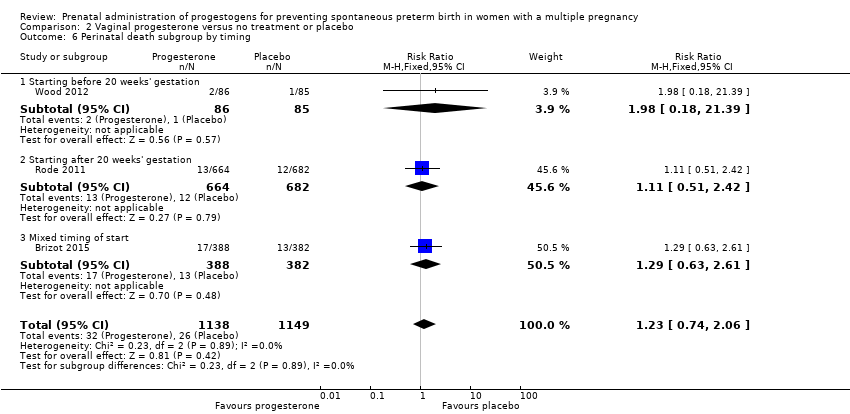 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 6 Perinatal death subgroup by timing. | ||||
| 6.1 Starting before 20 weeks' gestation | 1 | 171 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.98 [0.18, 21.39] |
| 6.2 Starting after 20 weeks' gestation | 1 | 1346 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.11 [0.51, 2.42] |
| 6.3 Mixed timing of start | 1 | 770 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.29 [0.63, 2.61] |
| 7 Prelabour rupture of the membranes Show forest plot | 2 | 514 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.23, 1.60] |
| Analysis 2.7 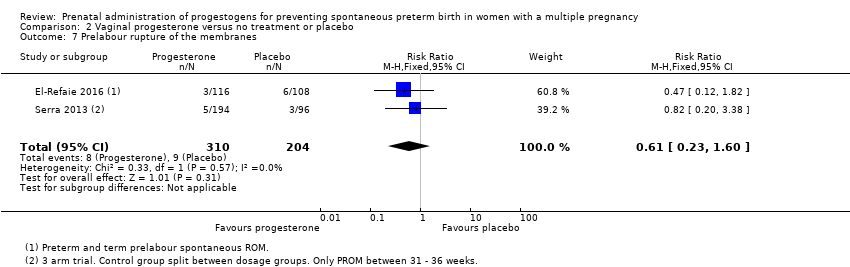 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 7 Prelabour rupture of the membranes. | ||||
| 8 Preterm birth less than 37 weeks Show forest plot | 6 | 1597 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.89, 1.06] |
| Analysis 2.8 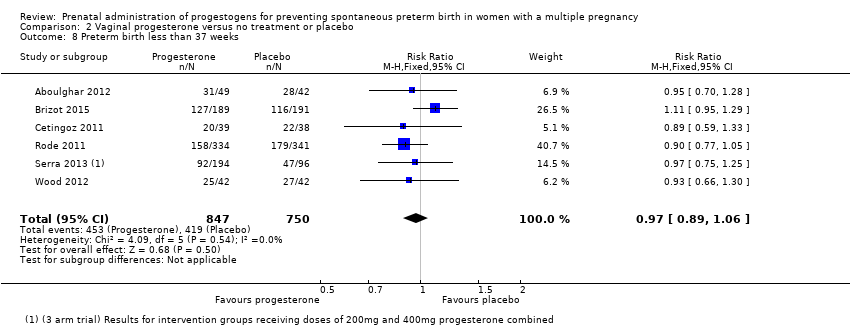 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 8 Preterm birth less than 37 weeks. | ||||
| 9 Preterm birth less than 28 weeks Show forest plot | 4 | 1569 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.22 [0.68, 2.21] |
| Analysis 2.9 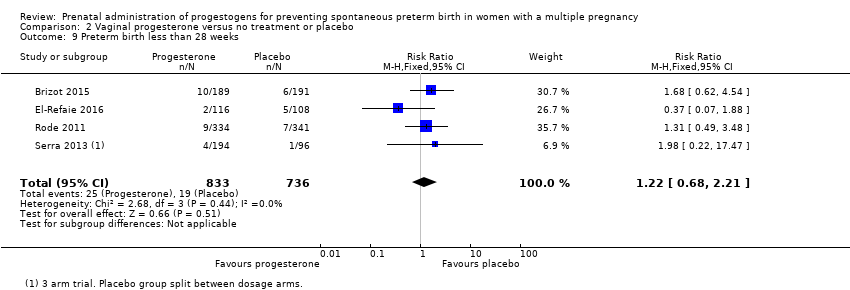 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 9 Preterm birth less than 28 weeks. | ||||
| 10 Adverse drug reaction Show forest plot | 2 | 562 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.90, 1.09] |
| Analysis 2.10 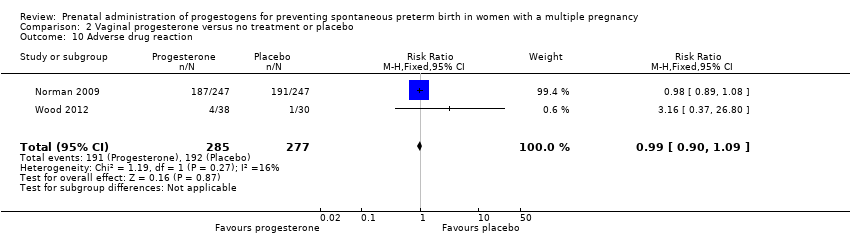 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 10 Adverse drug reaction. | ||||
| 11 Caesarean section Show forest plot | 6 | 2143 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.88, 0.98] |
| Analysis 2.11 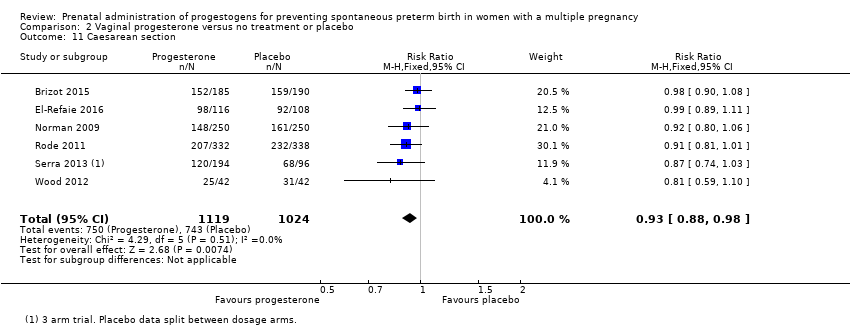 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 11 Caesarean section. | ||||
| 12 Satisfaction with therapy Show forest plot | 1 | 494 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [‐0.35, 0.35] |
| Analysis 2.12 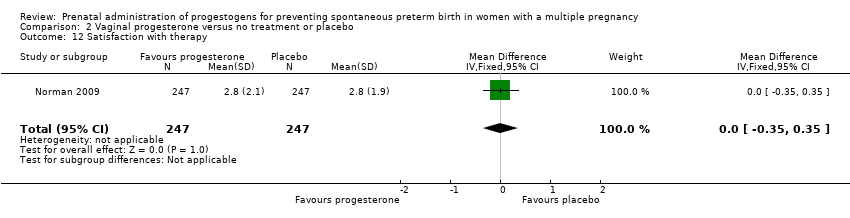 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 12 Satisfaction with therapy. | ||||
| 13 Antenatal tocolysis Show forest plot | 4 | 1420 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.62, 1.02] |
| Analysis 2.13 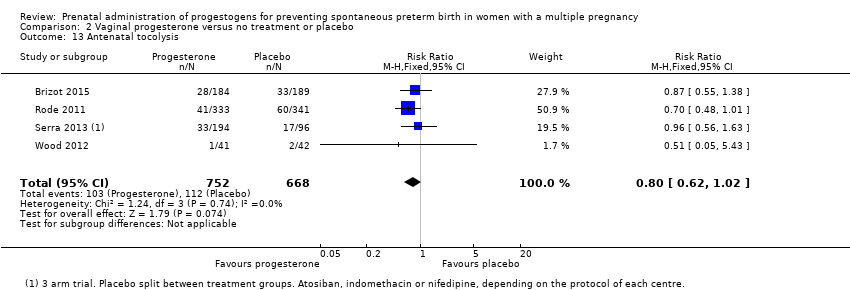 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 13 Antenatal tocolysis. | ||||
| 14 Antenatal corticosteroids Show forest plot | 4 | 1422 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.71, 1.06] |
| Analysis 2.14 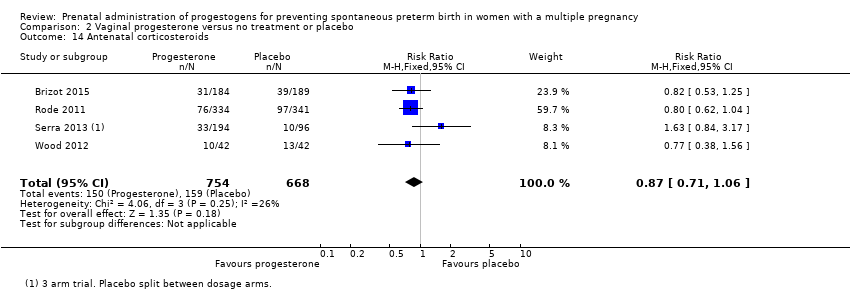 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 14 Antenatal corticosteroids. | ||||
| 15 Infant birthweight less than 2500 g Show forest plot | 4 | 3079 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.88, 1.03] |
| Analysis 2.15 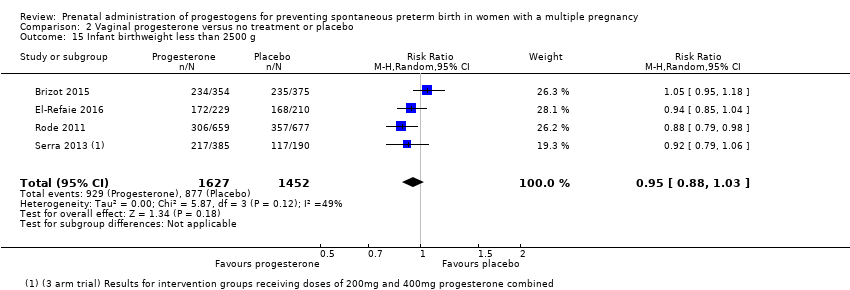 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 15 Infant birthweight less than 2500 g. | ||||
| 16 Apgar score < 7 at 5 minutes Show forest plot | 3 | 2410 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.65 [0.35, 1.19] |
| Analysis 2.16 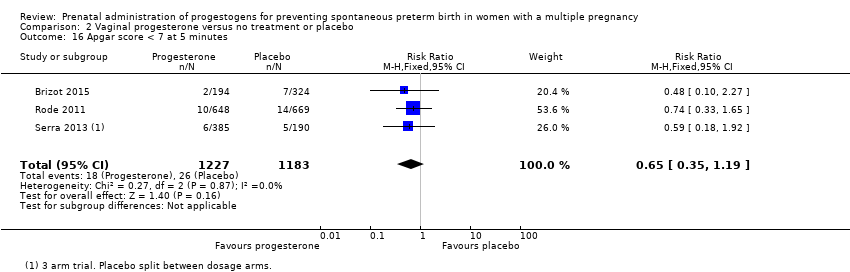 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 16 Apgar score < 7 at 5 minutes. | ||||
| 17 Respiratory distress syndrome Show forest plot | 4 | 2560 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.64, 1.10] |
| Analysis 2.17 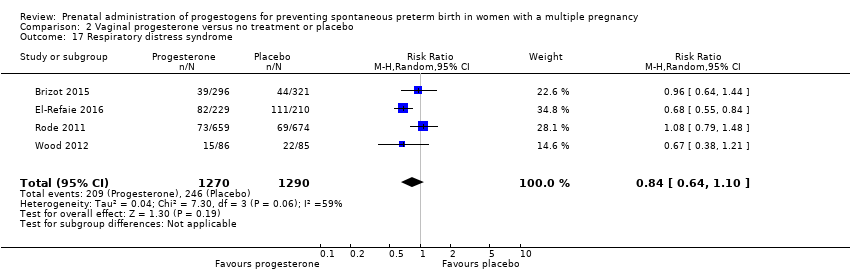 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 17 Respiratory distress syndrome. | ||||
| 18 Use of mechanical ventilation Show forest plot | 5 | 3134 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.48, 0.77] |
| Analysis 2.18 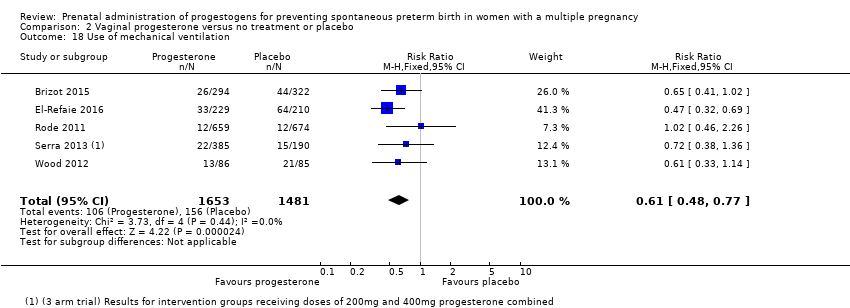 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 18 Use of mechanical ventilation. | ||||
| 19 Intraventricular haemorrhage ‐ all grades Show forest plot | 1 | 1333 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.70 [0.62, 4.66] |
| Analysis 2.19 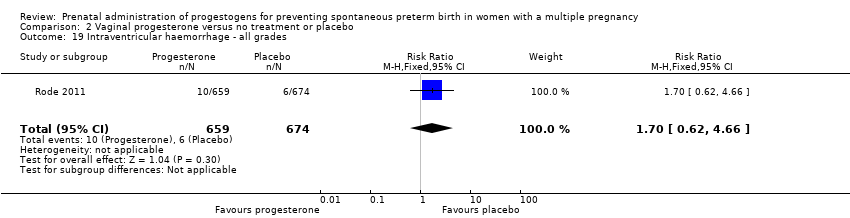 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 19 Intraventricular haemorrhage ‐ all grades. | ||||
| 20 Retinopathy of prematurity Show forest plot | 2 | 1945 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [0.45, 2.54] |
| Analysis 2.20 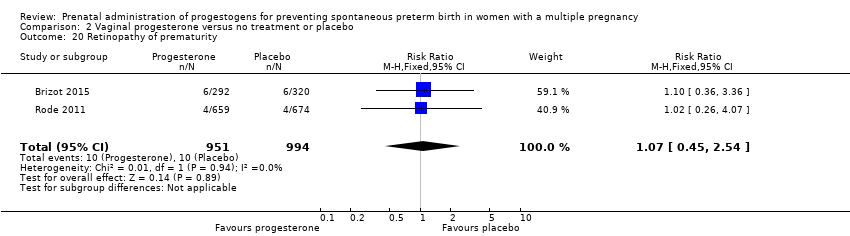 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 20 Retinopathy of prematurity. | ||||
| 21 Necrotising enterocolitis Show forest plot | 3 | 2117 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.52 [0.13, 2.06] |
| Analysis 2.21 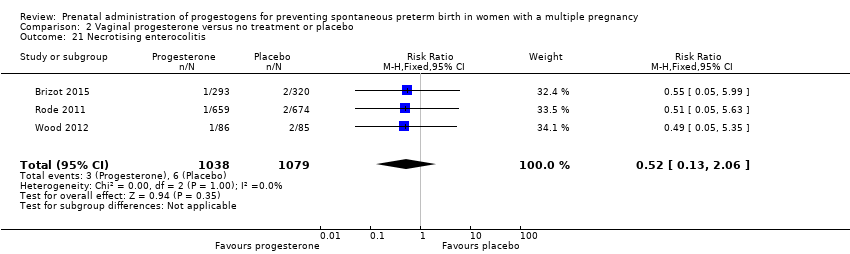 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 21 Necrotising enterocolitis. | ||||
| 22 Neonatal sepsis Show forest plot | 2 | 1944 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.41 [0.86, 2.33] |
| Analysis 2.22 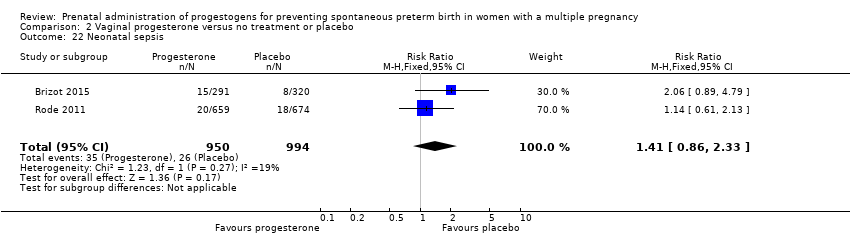 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 22 Neonatal sepsis. | ||||
| 23 Fetal death Show forest plot | 3 | 2328 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.38 [0.65, 2.90] |
| Analysis 2.23 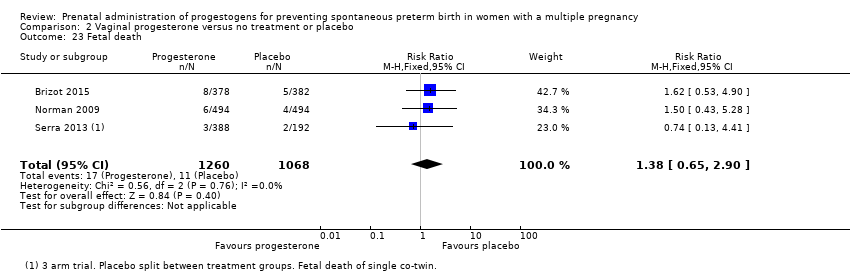 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 23 Fetal death. | ||||
| 24 Neonatal death Show forest plot | 3 | 2905 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.53 [0.75, 3.15] |
| Analysis 2.24 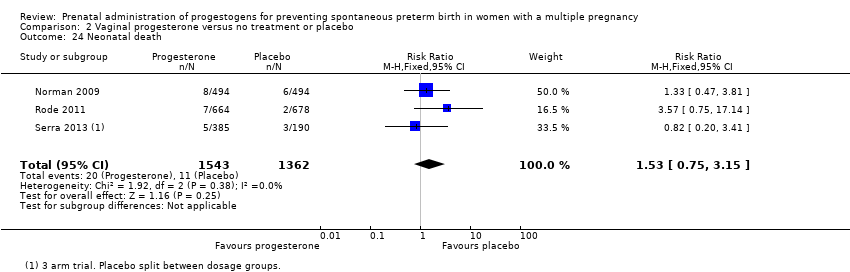 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 24 Neonatal death. | ||||
| 25 Admission to NICU Show forest plot | 5 | 4052 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.87, 1.00] |
| Analysis 2.25 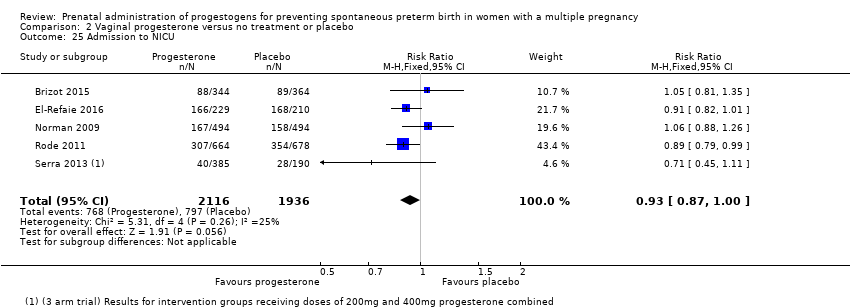 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 25 Admission to NICU. | ||||
| 26 Patent ductus arteriosus Show forest plot | 2 | 1946 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.47, 1.22] |
| Analysis 2.26 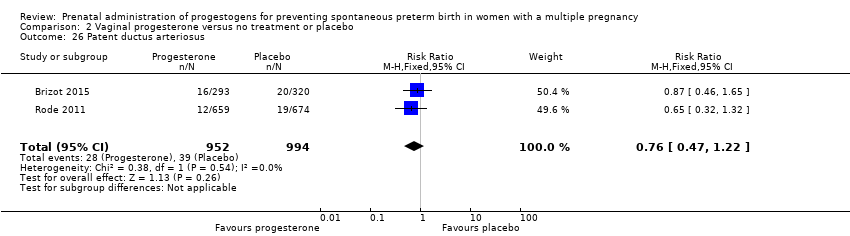 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 26 Patent ductus arteriosus. | ||||
| 27 Sensitivity analysis for perinatal death (assuming total non‐independence) Show forest plot | 3 | 1144 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.22 [0.61, 2.44] |
| Analysis 2.27 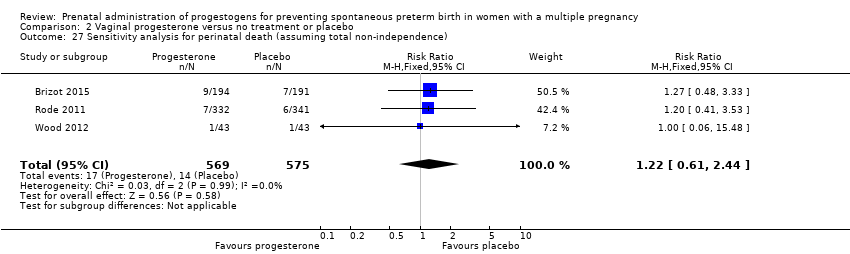 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 27 Sensitivity analysis for perinatal death (assuming total non‐independence). | ||||
| 28 Sensitivity analysis for perinatal death (assuming 1% non‐independence) Show forest plot | 3 | 2263 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.74, 2.06] |
| Analysis 2.28 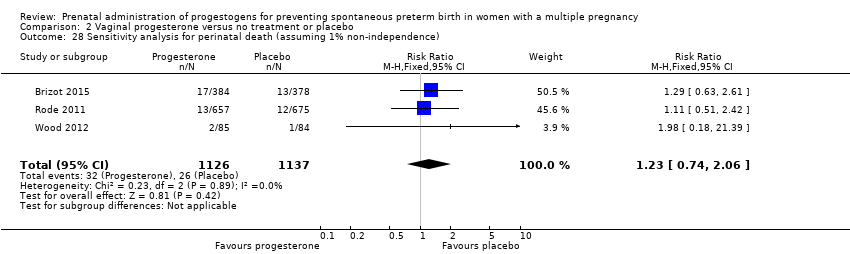 Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 28 Sensitivity analysis for perinatal death (assuming 1% non‐independence). | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Preterm birth less than 34 weeks Show forest plot | 1 | 161 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.67 [1.04, 2.68] |
| Analysis 3.1 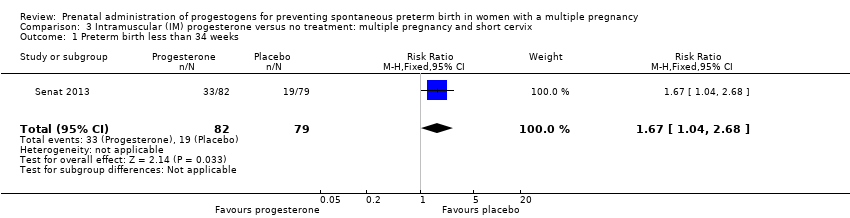 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 1 Preterm birth less than 34 weeks. | ||||
| 2 Perinatal death Show forest plot | 1 | 330 | Risk Ratio (M‐H, Fixed, 95% CI) | 9.11 [1.17, 71.10] |
| Analysis 3.2 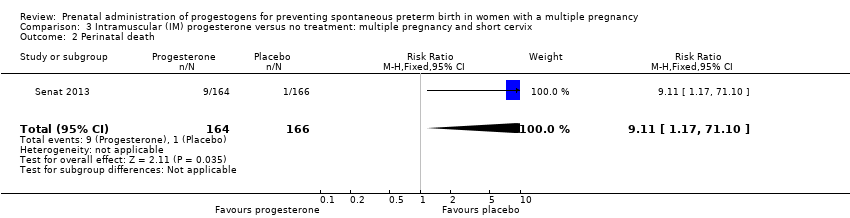 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 2 Perinatal death. | ||||
| 3 Prelabour rupture of the membranes Show forest plot | 1 | 161 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.63, 2.06] |
| Analysis 3.3 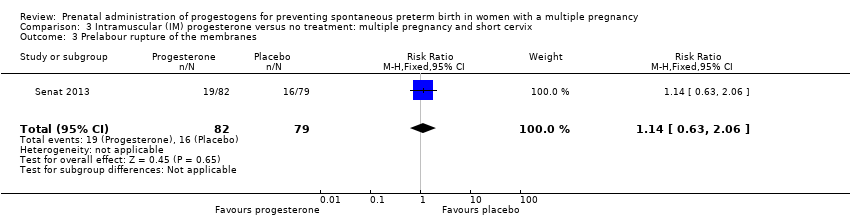 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 3 Prelabour rupture of the membranes. | ||||
| 4 Preterm birth less than 37 weeks Show forest plot | 1 | 161 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.06 [0.90, 1.25] |
| Analysis 3.4 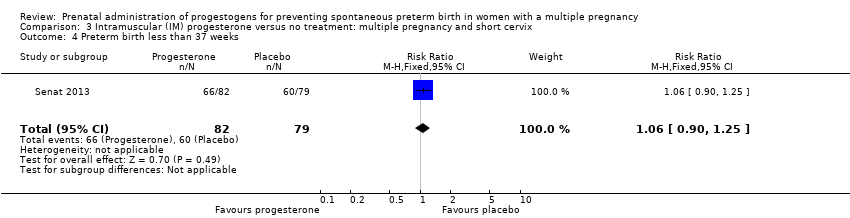 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 4 Preterm birth less than 37 weeks. | ||||
| 5 Caesarean section Show forest plot | 1 | 161 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.88, 1.49] |
| Analysis 3.5 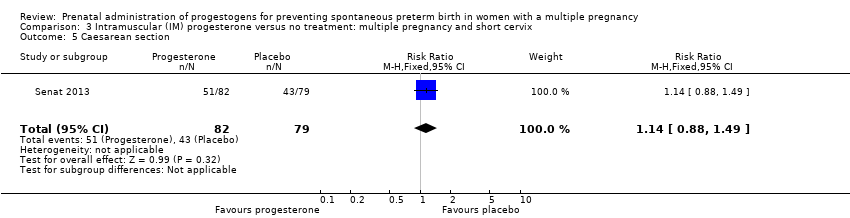 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 5 Caesarean section. | ||||
| 6 Antenatal tocolysis Show forest plot | 1 | 158 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.37 [0.76, 2.45] |
| Analysis 3.6 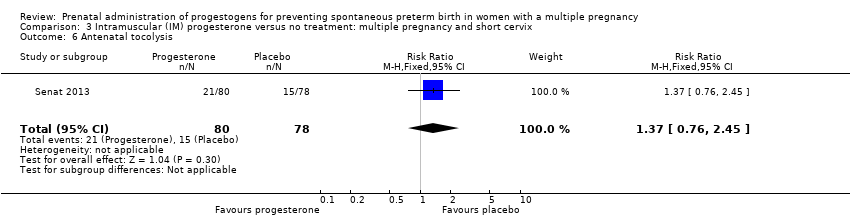 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 6 Antenatal tocolysis. | ||||
| 7 Antenatal corticosteroids Show forest plot | 1 | 159 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.64, 1.36] |
| Analysis 3.7 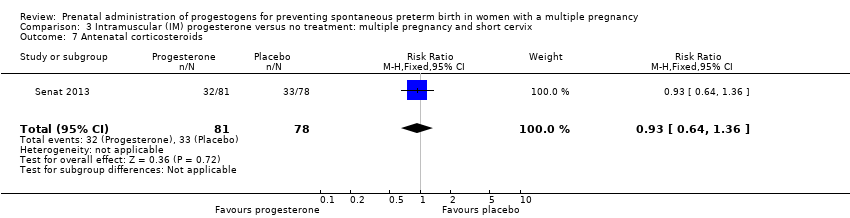 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 7 Antenatal corticosteroids. | ||||
| 8 Neonatal sepsis Show forest plot | 1 | 303 | Risk Ratio (M‐H, Fixed, 95% CI) | 5.03 [0.60, 42.57] |
| Analysis 3.8 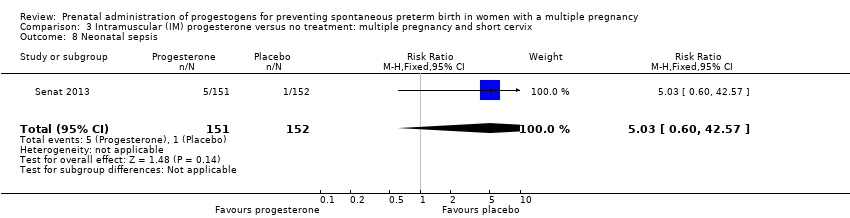 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 8 Neonatal sepsis. | ||||
| 9 Respiratory distress syndrome Show forest plot | 1 | 309 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.46 [1.00, 2.12] |
| Analysis 3.9 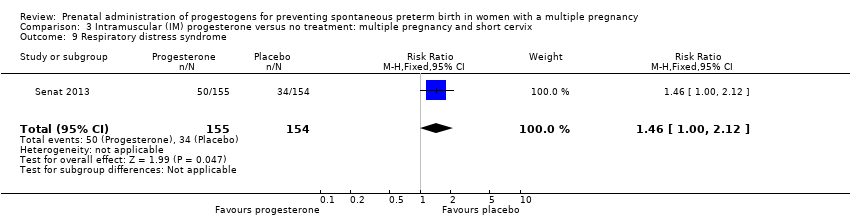 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 9 Respiratory distress syndrome. | ||||
| 10 Retinopathy of prematurity Show forest plot | 1 | 302 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.20 [0.01, 4.19] |
| Analysis 3.10 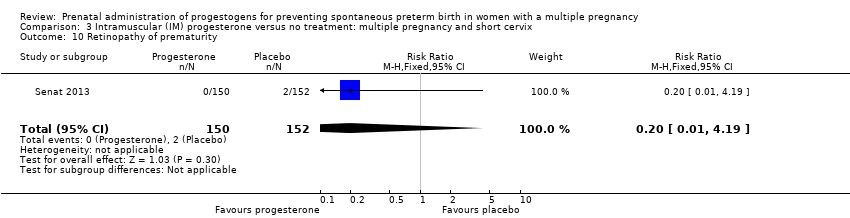 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 10 Retinopathy of prematurity. | ||||
| 11 Neonatal death Show forest plot | 1 | 307 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.03 [0.46, 35.61] |
| Analysis 3.11 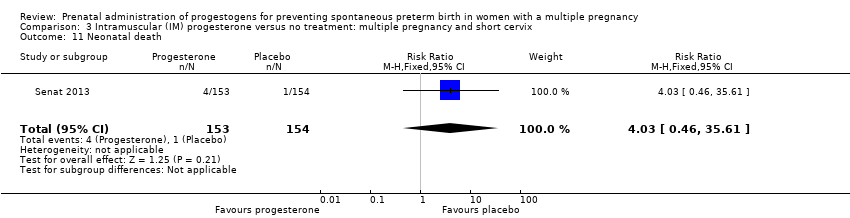 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 11 Neonatal death. | ||||
| 12 Admission to NICU Show forest plot | 1 | 313 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.34 [1.04, 1.74] |
| Analysis 3.12 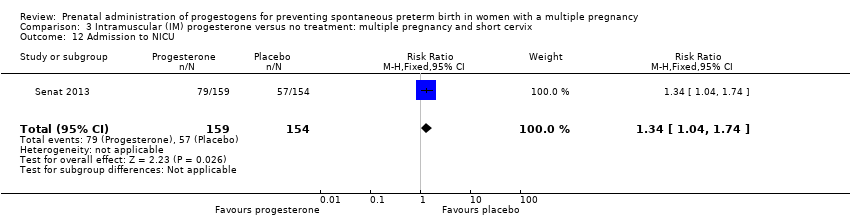 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 12 Admission to NICU. | ||||
| 13 Sensitivity analysis for perinatal death (assuming total dependence) Show forest plot | 1 | 163 | Risk Ratio (M‐H, Fixed, 95% CI) | 5.06 [0.60, 42.38] |
| Analysis 3.13 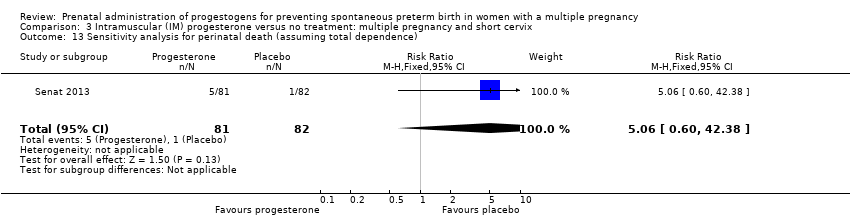 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 13 Sensitivity analysis for perinatal death (assuming total dependence). | ||||
| 14 Sensitivity analysis for perinatal death (assuming 1% dependence) Show forest plot | 1 | 322 | Risk Ratio (M‐H, Fixed, 95% CI) | 9.11 [1.17, 71.10] |
| Analysis 3.14 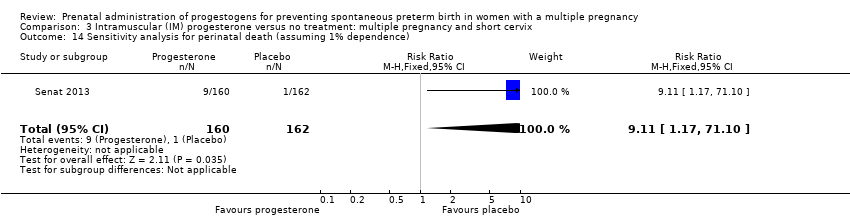 Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 14 Sensitivity analysis for perinatal death (assuming 1% dependence). | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Preterm birth less than 34 weeks Show forest plot | 1 | 224 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.49, 0.91] |
| Analysis 4.1 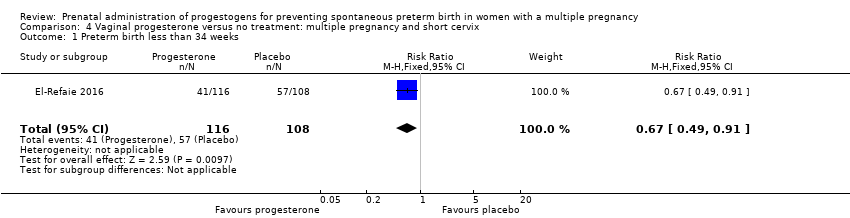 Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 1 Preterm birth less than 34 weeks. | ||||
| 2 Prelabour rupture of the membranes Show forest plot | 1 | 224 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.47 [0.12, 1.82] |
| Analysis 4.2 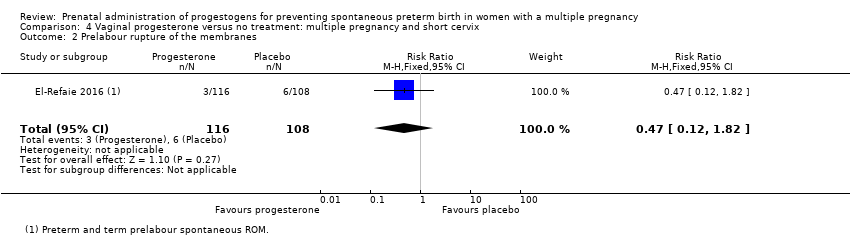 Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 2 Prelabour rupture of the membranes. | ||||
| 3 Preterm birth less than 28 weeks Show forest plot | 1 | 224 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.37 [0.07, 1.88] |
| Analysis 4.3 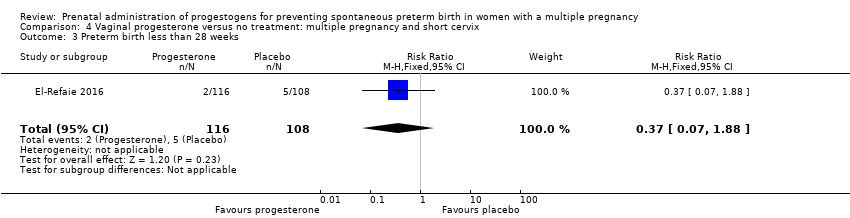 Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 3 Preterm birth less than 28 weeks. | ||||
| 4 Caesarean section Show forest plot | 1 | 224 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.89, 1.11] |
| Analysis 4.4 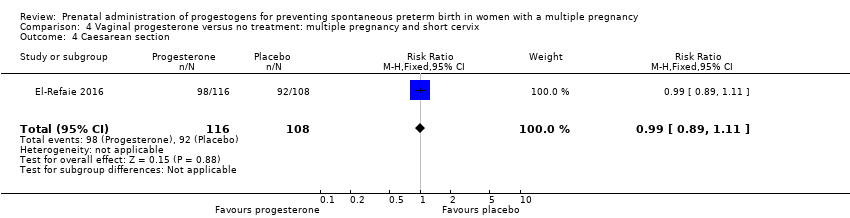 Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 4 Caesarean section. | ||||
| 5 Infant birthweight less than 2500 g Show forest plot | 1 | 439 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.85, 1.04] |
| Analysis 4.5 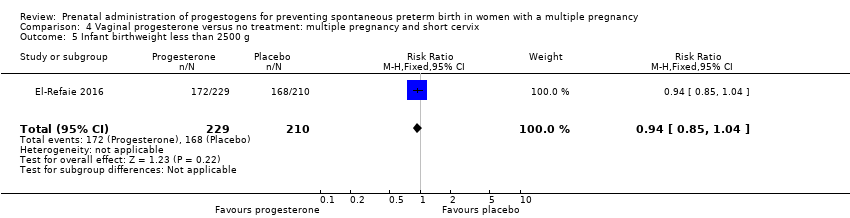 Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 5 Infant birthweight less than 2500 g. | ||||
| 6 Respiratory distress syndrome Show forest plot | 1 | 439 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.68 [0.55, 0.84] |
| Analysis 4.6 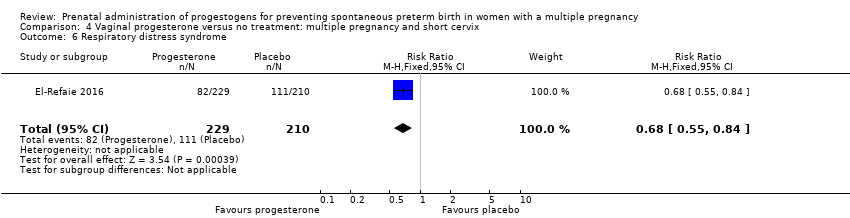 Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 6 Respiratory distress syndrome. | ||||
| 7 Use of mechanical ventilation Show forest plot | 1 | 439 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.47 [0.32, 0.69] |
| Analysis 4.7 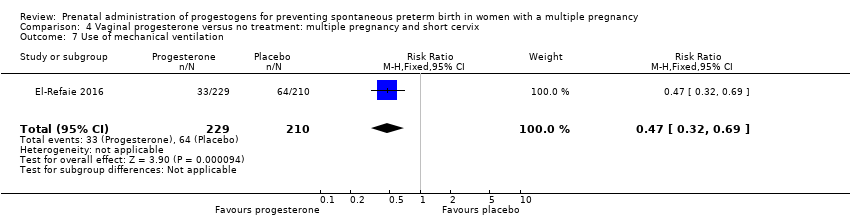 Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 7 Use of mechanical ventilation. | ||||
| 8 Admission to NICU Show forest plot | 1 | 439 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.91 [0.82, 1.01] |
| Analysis 4.8 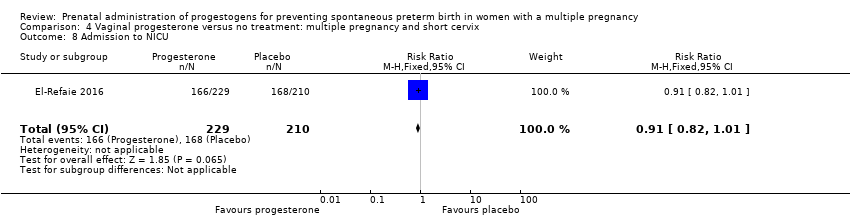 Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 8 Admission to NICU. | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Preterm birth less than 34 weeks Show forest plot | 2 | 158 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.57 [0.29, 1.10] |
| Analysis 5.1 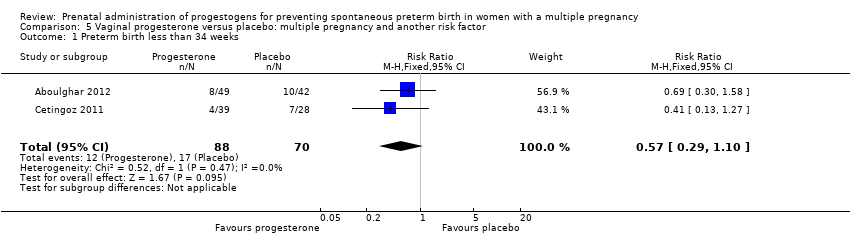 Comparison 5 Vaginal progesterone versus placebo: multiple pregnancy and another risk factor, Outcome 1 Preterm birth less than 34 weeks. | ||||
| 2 Preterm birth less than 37 weeks Show forest plot | 2 | 168 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.72, 1.18] |
| Analysis 5.2 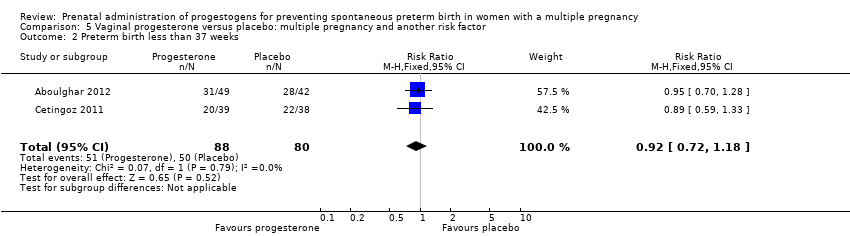 Comparison 5 Vaginal progesterone versus placebo: multiple pregnancy and another risk factor, Outcome 2 Preterm birth less than 37 weeks. | ||||
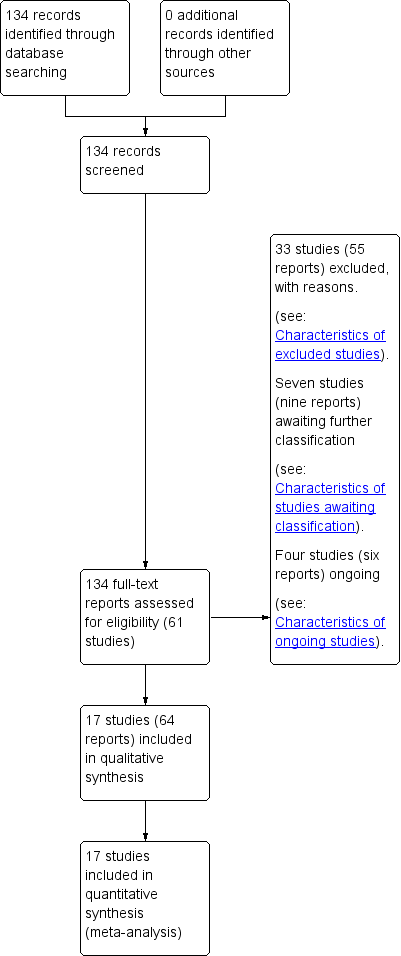
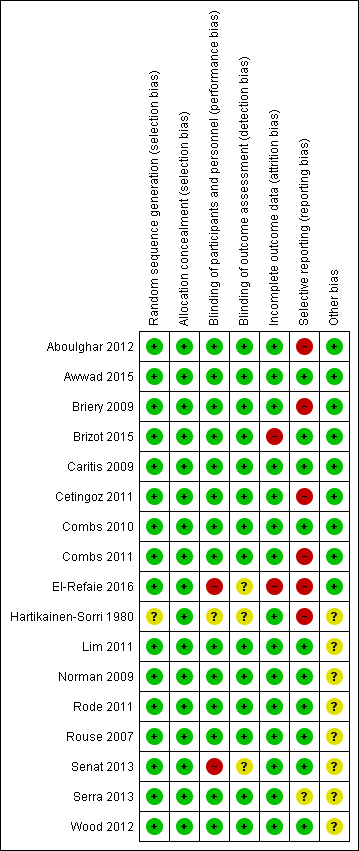
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 1 Preterm birth less than 34 weeks.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 2 Preterm birth less than 34 weeks subgroup by dose.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 3 Preterm birth less than 34 week subgroup by timing.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 4 Perinatal death.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 5 Perinatal death subgroup by dose.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 6 Perinatal death subgroup by timing.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 7 Prelabour rupture of the membranes.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 8 Preterm birth less than 37 weeks.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 9 Preterm birth less than 28 weeks.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 10 Adverse drug reaction.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 11 Caesarean section.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 12 Antenatal tocolysis.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 13 Antenatal corticosteroids.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 14 Infant birthweight less than 2500 g.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 15 Apgar score < 7 at 5 minutes.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 16 Neonatal sepsis.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 17 Respiratory distress syndrome.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 18 Use of mechanical ventilation.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 19 Intraventricular haemorrhage ‐ all grades.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 20 Retinopathy of prematurity.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 21 Chronic lung disease.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 22 Necrotising enterocolitis.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 23 Fetal death.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 24 Neonatal death.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 25 Admission to NICU.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 26 Patent ductus arteriosus.
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 27 Sensitivity analysis for perinatal death (assuming total dependence).
Comparison 1 Intramuscular (IM) progesterone versus no treatment or placebo, Outcome 28 Sensitivity analysis for perinatal death (assuming 1% dependence).
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 1 Preterm birth less than 34 weeks.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 2 Preterm birth less than 34 weeks subgroup by dose.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 3 Preterm birth less than 34 weeks subgroup by timing.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 4 Perinatal death.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 5 Perinatal death subgroup by dose.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 6 Perinatal death subgroup by timing.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 7 Prelabour rupture of the membranes.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 8 Preterm birth less than 37 weeks.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 9 Preterm birth less than 28 weeks.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 10 Adverse drug reaction.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 11 Caesarean section.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 12 Satisfaction with therapy.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 13 Antenatal tocolysis.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 14 Antenatal corticosteroids.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 15 Infant birthweight less than 2500 g.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 16 Apgar score < 7 at 5 minutes.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 17 Respiratory distress syndrome.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 18 Use of mechanical ventilation.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 19 Intraventricular haemorrhage ‐ all grades.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 20 Retinopathy of prematurity.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 21 Necrotising enterocolitis.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 22 Neonatal sepsis.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 23 Fetal death.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 24 Neonatal death.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 25 Admission to NICU.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 26 Patent ductus arteriosus.
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 27 Sensitivity analysis for perinatal death (assuming total non‐independence).
Comparison 2 Vaginal progesterone versus no treatment or placebo, Outcome 28 Sensitivity analysis for perinatal death (assuming 1% non‐independence).
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 1 Preterm birth less than 34 weeks.
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 2 Perinatal death.
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 3 Prelabour rupture of the membranes.
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 4 Preterm birth less than 37 weeks.
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 5 Caesarean section.
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 6 Antenatal tocolysis.
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 7 Antenatal corticosteroids.
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 8 Neonatal sepsis.
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 9 Respiratory distress syndrome.
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 10 Retinopathy of prematurity.
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 11 Neonatal death.
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 12 Admission to NICU.
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 13 Sensitivity analysis for perinatal death (assuming total dependence).
Comparison 3 Intramuscular (IM) progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 14 Sensitivity analysis for perinatal death (assuming 1% dependence).
Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 1 Preterm birth less than 34 weeks.
Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 2 Prelabour rupture of the membranes.
Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 3 Preterm birth less than 28 weeks.
Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 4 Caesarean section.
Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 5 Infant birthweight less than 2500 g.
Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 6 Respiratory distress syndrome.
Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 7 Use of mechanical ventilation.
Comparison 4 Vaginal progesterone versus no treatment: multiple pregnancy and short cervix, Outcome 8 Admission to NICU.
Comparison 5 Vaginal progesterone versus placebo: multiple pregnancy and another risk factor, Outcome 1 Preterm birth less than 34 weeks.
Comparison 5 Vaginal progesterone versus placebo: multiple pregnancy and another risk factor, Outcome 2 Preterm birth less than 37 weeks.
| Intramuscular (IM) progesterone compared to no treatment or placebo for preventing spontaneous preterm birth in women with a multiple pregnancy | ||||||
| Patient or population: Women with a multiple pregnancy | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | Comments | |
| Risk with no treatment or placebo | Risk with intramuscular (IM) progesterone | |||||
| Perinatal death | Study population | RR 1.45 | 3089 | ⊕⊕⊝⊝ LOW 1, 2 | ‐ | |
| 34 per 1000 | 49 per 1000 | |||||
| Preterm birth less than 34 weeks | Study population | RR 1.54 | 399 | ⊕⊕⊝⊝ | ‐ | |
| 191 per 1000 | 298 per 1000 | |||||
| Major neurodevelopmental disability at childhood follow‐up | Study population | ‐ | (0 studies) | ‐ | None of the included trial reported this outcome | |
| see comment | see comment | |||||
| Infant birthweight less than 2500 g | Study population | RR 0.99 | 4071 | ⊕⊕⊕⊝ | ‐ | |
| 620 per 1000 | 613 per 1000 | |||||
| Preterm birth less than 28 weeks | Study population | RR 1.08 | 1920 | ⊕⊕⊕⊝ | ‐ | |
| ‐58 per 1000 | 62 per 1000 | |||||
| Preterm birth less than 37 weeks | Study population | RR 1.05 | 2010 | ⊕⊕⊕⊕ | ‐ | |
| 614 per 1000 | 639 per 1000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Statistical heterogeneity (I2 > 60%). Variation in size and direction of effect (‐1). | ||||||
| Vaginal progesterone compared to no treatment or placebo for preventing spontaneous preterm birth in women with a multiple pregnancy | ||||||
| Patient or population: Women with a multiple pregnancy | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Quality of the evidence | Comments | |
| Risk with no treatment or placebo | Risk with vaginal progesterone | |||||
| Perinatal death | Study population | RR 1.23 | 2287 | ⊕⊕⊝⊝ | ‐ | |
| 23 per 1000 | 28 per 1000 | |||||
| Preterm birth less than 34 weeks | Study population | RR 0.83 | 1727 | ⊕⊕⊝⊝ | ‐ | |
| 227 per 1000 | 188 per 1000 | |||||
| Major neurodevelopmental disability at childhood follow‐up | Study population | ‐ | (0 study) | ‐ | None of the included trial reported this outcome. | |
| see comment | see comment | |||||
| Infant birthweight less than 2500 g | Study population | RR 0.95 | 3079 | ⊕⊕⊕⊝ | ‐ | |
| 604 per 1000 | 574 per 1000 | |||||
| Preterm birth less than 37 weeks | Study population | RR 0.97 | 1597 | ⊕⊕⊕⊝ | ‐ | |
| 559 per 1000 | 547 per 1000 | |||||
| Preterm birth less than 28 weeks | Study population | RR 1.22 | 1569 | ⊕⊕⊝⊝ | ‐ | |
| 26 per 1000 | 31 per 1000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1One study contributing data with design limitations (weight of 52.1%) (‐1). | ||||||
| Trial | Fetal death (FD) | Intrapartum death | Stillbirth | Neonatal death (NND) | Perinatal death (PND) | Included in Dodd 2013? | Decision for PND for multiples review? |
| ‐ | ‐ | ‐ | Reported as maternal outcome. From text appears as if at least one pregnancy affected by demise of both twins | ‐ | Yes | Cannot reliably convert maternal denominator for neonatal outcome. Data not included | |
| Yes | ‐ | ‐ | ‐ | Yes, as a baby outcome. | N/A | Include | |
| No death data | ‐ | ‐ | ‐ | ‐ | No PND reported | N/A | |
| No death data | ‐ | ‐ | ‐ | ‐ | No PND reported | N/A | |
| Fetal death reported as maternal outcome and only as a single co‐twin demise outcome. Unsure if any pregnancies where both twins died | ‐ | ‐ | Yes, as a baby outcome | Not reported. Cannot convert fetal death into a baby outcome because only reported if single twin demise likely to underestimate | Yes | Data not included. | |
| Reported as a maternal outcome and denominator not clear | ‐ | ‐ | Yes | No | No | No | |
| Yes. as maternal outcome but specifies only 1 twin affected in each of those pregnancies | ‐ | ‐ | Yes | In text | Yes | Yes | |
| ‐ | ‐ | ‐ | ‐ | Yes, as infant outcome | N/A | Yes | |
| ‐ | ‐ | Yes | Yes | Yes, as infant outcome | N/A | Yes | |
| ‐ | ‐ | ‐ | Yes | ‐ | No PND reported | N/A | |
| Combs 2010 triplets | ‐ | ‐ | ‐ | Yes | Yes | Yes | Yes |
| Combs 2011 twins | ‐ | ‐ | ‐ | Yes | Yes | Yes | Yes |
| ‐ | ‐ | ‐ | ‐ | Yes in text | Yes | Yes | |
| ‐ | 1 or more died during delivery after 24 wks and also any IUD before onset labour or onset delivery | Reported “all live births” | ‐ | No, and cannot be reliably added up from data presented | Yes | Data not included | |
| Yes | ‐ | ‐ | Yes | Yes, from text (not in table) | No ‐ not sure why data not included | Yes | |
| Yes | Yes | ‐ | Yes | Can add NND and FD (IP and IU); all Ns clear | No ‐ not sure why data not included | Yes. Extrapolated from text and checked | |
| Yes, as a maternal outcome | ‐ | ‐ | Yes | Cannot add FD and NND because FD reported as a maternal outcome | No | Data not included | |
| IP: intrapartum | |||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Preterm birth less than 34 weeks Show forest plot | 2 | 399 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.54 [1.06, 2.26] |
| 2 Preterm birth less than 34 weeks subgroup by dose Show forest plot | 2 | 399 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.54 [1.06, 2.26] |
| 2.1 Low dose (250 mg weekly or less) | 1 | 238 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.37 [0.73, 2.59] |
| 2.2 High dose (greater than 250 mg weekly) | 1 | 161 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.67 [1.04, 2.68] |
| 3 Preterm birth less than 34 week subgroup by timing Show forest plot | 2 | 399 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.54 [1.06, 2.26] |
| 3.1 Commencing after 20 weeks' gestation | 1 | 161 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.67 [1.04, 2.68] |
| 3.2 Mixed timing of commencement | 1 | 238 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.37 [0.73, 2.59] |
| 4 Perinatal death Show forest plot | 6 | 3089 | Risk Ratio (M‐H, Random, 95% CI) | 1.45 [0.60, 3.51] |
| 5 Perinatal death subgroup by dose Show forest plot | 6 | 3089 | Risk Ratio (M‐H, Random, 95% CI) | 1.45 [0.60, 3.51] |
| 5.1 Low dose (250 mg weekly or less) | 5 | 2759 | Risk Ratio (M‐H, Random, 95% CI) | 1.15 [0.48, 2.77] |
| 5.2 High dose (greater than 250 mg weekly) | 1 | 330 | Risk Ratio (M‐H, Random, 95% CI) | 9.11 [1.17, 71.10] |
| 6 Perinatal death subgroup by timing Show forest plot | 6 | 3089 | Risk Ratio (M‐H, Random, 95% CI) | 1.45 [0.60, 3.51] |
| 6.1 Starting before 20 weeks' gestation | 2 | 1886 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.34, 2.66] |
| 6.2 Starting after 20 weeks' gestation | 2 | 484 | Risk Ratio (M‐H, Random, 95% CI) | 3.76 [0.81, 17.46] |
| 6.3 Mixed timing of start | 2 | 719 | Risk Ratio (M‐H, Random, 95% CI) | 0.67 [0.01, 37.74] |
| 7 Prelabour rupture of the membranes Show forest plot | 6 | 1257 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.17 [0.84, 1.63] |
| 8 Preterm birth less than 37 weeks Show forest plot | 5 | 2010 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.98, 1.13] |
| 9 Preterm birth less than 28 weeks Show forest plot | 5 | 1920 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.75, 1.55] |
| 10 Adverse drug reaction Show forest plot | 2 | 1316 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.63, 1.32] |
| 11 Caesarean section Show forest plot | 7 | 2222 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.95, 1.08] |
| 12 Antenatal tocolysis Show forest plot | 7 | 2218 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.85, 1.10] |
| 13 Antenatal corticosteroids Show forest plot | 7 | 2221 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.88, 1.11] |
| 14 Infant birthweight less than 2500 g Show forest plot | 5 | 4071 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.90, 1.08] |
| 15 Apgar score < 7 at 5 minutes Show forest plot | 4 | 3606 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.89 [0.68, 1.15] |
| 16 Neonatal sepsis Show forest plot | 6 | 3327 | Risk Ratio (M‐H, Random, 95% CI) | 1.02 [0.41, 2.51] |
| 17 Respiratory distress syndrome Show forest plot | 8 | 4670 | Risk Ratio (M‐H, Random, 95% CI) | 1.07 [0.85, 1.34] |
| 18 Use of mechanical ventilation Show forest plot | 3 | 2233 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.69, 1.17] |
| 19 Intraventricular haemorrhage ‐ all grades Show forest plot | 1 | 1355 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.98 [0.36, 10.77] |
| 20 Retinopathy of prematurity Show forest plot | 5 | 2807 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.34 [0.16, 0.74] |
| 21 Chronic lung disease Show forest plot | 2 | 681 | Risk Ratio (M‐H, Random, 95% CI) | 1.91 [0.13, 27.80] |
| 22 Necrotising enterocolitis Show forest plot | 5 | 2610 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.74 [0.36, 1.51] |
| 23 Fetal death Show forest plot | 4 | 3536 | Risk Ratio (M‐H, Random, 95% CI) | 0.93 [0.39, 2.20] |
| 24 Neonatal death Show forest plot | 7 | 3399 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.44, 1.91] |
| 25 Admission to NICU Show forest plot | 2 | 1668 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.33 [1.13, 1.58] |
| 26 Patent ductus arteriosus Show forest plot | 4 | 2290 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.37, 2.21] |
| 27 Sensitivity analysis for perinatal death (assuming total dependence) Show forest plot | 6 | 1517 | Risk Ratio (M‐H, Random, 95% CI) | 1.35 [0.57, 3.20] |
| 28 Sensitivity analysis for perinatal death (assuming 1% dependence) Show forest plot | 6 | 3021 | Risk Ratio (M‐H, Random, 95% CI) | 1.45 [0.60, 3.49] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Preterm birth less than 34 weeks Show forest plot | 6 | 1727 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.63, 1.09] |
| 2 Preterm birth less than 34 weeks subgroup by dose Show forest plot | 6 | 1727 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.64, 1.07] |
| 2.1 Low dose (200 mg or less daily) | 4 | 1267 | Risk Ratio (M‐H, Random, 95% CI) | 0.93 [0.63, 1.37] |
| 2.2 High dose (more than 200 mg daily) | 3 | 460 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.52, 0.90] |
| 3 Preterm birth less than 34 weeks subgroup by timing Show forest plot | 6 | 1727 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.63, 1.09] |
| 3.1 Starting before 20 weeks' gestation | 1 | 91 | Risk Ratio (M‐H, Random, 95% CI) | 0.69 [0.30, 1.58] |
| 3.2 Starting after 20 weeks' gestation | 4 | 1256 | Risk Ratio (M‐H, Random, 95% CI) | 0.74 [0.60, 0.91] |
| 3.3 Mixed timing of start | 1 | 380 | Risk Ratio (M‐H, Random, 95% CI) | 1.35 [0.90, 2.02] |
| 4 Perinatal death Show forest plot | 3 | 2287 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.74, 2.06] |
| 5 Perinatal death subgroup by dose Show forest plot | 3 | 2287 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.74, 2.06] |
| 5.1 Low dose (200 mg or less daily) | 3 | 2287 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.74, 2.06] |
| 6 Perinatal death subgroup by timing Show forest plot | 3 | 2287 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.74, 2.06] |
| 6.1 Starting before 20 weeks' gestation | 1 | 171 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.98 [0.18, 21.39] |
| 6.2 Starting after 20 weeks' gestation | 1 | 1346 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.11 [0.51, 2.42] |
| 6.3 Mixed timing of start | 1 | 770 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.29 [0.63, 2.61] |
| 7 Prelabour rupture of the membranes Show forest plot | 2 | 514 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.23, 1.60] |
| 8 Preterm birth less than 37 weeks Show forest plot | 6 | 1597 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.89, 1.06] |
| 9 Preterm birth less than 28 weeks Show forest plot | 4 | 1569 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.22 [0.68, 2.21] |
| 10 Adverse drug reaction Show forest plot | 2 | 562 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.90, 1.09] |
| 11 Caesarean section Show forest plot | 6 | 2143 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.88, 0.98] |
| 12 Satisfaction with therapy Show forest plot | 1 | 494 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [‐0.35, 0.35] |
| 13 Antenatal tocolysis Show forest plot | 4 | 1420 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.62, 1.02] |
| 14 Antenatal corticosteroids Show forest plot | 4 | 1422 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.71, 1.06] |
| 15 Infant birthweight less than 2500 g Show forest plot | 4 | 3079 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.88, 1.03] |
| 16 Apgar score < 7 at 5 minutes Show forest plot | 3 | 2410 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.65 [0.35, 1.19] |
| 17 Respiratory distress syndrome Show forest plot | 4 | 2560 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.64, 1.10] |
| 18 Use of mechanical ventilation Show forest plot | 5 | 3134 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.48, 0.77] |
| 19 Intraventricular haemorrhage ‐ all grades Show forest plot | 1 | 1333 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.70 [0.62, 4.66] |
| 20 Retinopathy of prematurity Show forest plot | 2 | 1945 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [0.45, 2.54] |
| 21 Necrotising enterocolitis Show forest plot | 3 | 2117 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.52 [0.13, 2.06] |
| 22 Neonatal sepsis Show forest plot | 2 | 1944 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.41 [0.86, 2.33] |
| 23 Fetal death Show forest plot | 3 | 2328 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.38 [0.65, 2.90] |
| 24 Neonatal death Show forest plot | 3 | 2905 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.53 [0.75, 3.15] |
| 25 Admission to NICU Show forest plot | 5 | 4052 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.87, 1.00] |
| 26 Patent ductus arteriosus Show forest plot | 2 | 1946 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.47, 1.22] |
| 27 Sensitivity analysis for perinatal death (assuming total non‐independence) Show forest plot | 3 | 1144 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.22 [0.61, 2.44] |
| 28 Sensitivity analysis for perinatal death (assuming 1% non‐independence) Show forest plot | 3 | 2263 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.23 [0.74, 2.06] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Preterm birth less than 34 weeks Show forest plot | 1 | 161 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.67 [1.04, 2.68] |
| 2 Perinatal death Show forest plot | 1 | 330 | Risk Ratio (M‐H, Fixed, 95% CI) | 9.11 [1.17, 71.10] |
| 3 Prelabour rupture of the membranes Show forest plot | 1 | 161 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.63, 2.06] |
| 4 Preterm birth less than 37 weeks Show forest plot | 1 | 161 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.06 [0.90, 1.25] |
| 5 Caesarean section Show forest plot | 1 | 161 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.88, 1.49] |
| 6 Antenatal tocolysis Show forest plot | 1 | 158 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.37 [0.76, 2.45] |
| 7 Antenatal corticosteroids Show forest plot | 1 | 159 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.64, 1.36] |
| 8 Neonatal sepsis Show forest plot | 1 | 303 | Risk Ratio (M‐H, Fixed, 95% CI) | 5.03 [0.60, 42.57] |
| 9 Respiratory distress syndrome Show forest plot | 1 | 309 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.46 [1.00, 2.12] |
| 10 Retinopathy of prematurity Show forest plot | 1 | 302 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.20 [0.01, 4.19] |
| 11 Neonatal death Show forest plot | 1 | 307 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.03 [0.46, 35.61] |
| 12 Admission to NICU Show forest plot | 1 | 313 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.34 [1.04, 1.74] |
| 13 Sensitivity analysis for perinatal death (assuming total dependence) Show forest plot | 1 | 163 | Risk Ratio (M‐H, Fixed, 95% CI) | 5.06 [0.60, 42.38] |
| 14 Sensitivity analysis for perinatal death (assuming 1% dependence) Show forest plot | 1 | 322 | Risk Ratio (M‐H, Fixed, 95% CI) | 9.11 [1.17, 71.10] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Preterm birth less than 34 weeks Show forest plot | 1 | 224 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.49, 0.91] |
| 2 Prelabour rupture of the membranes Show forest plot | 1 | 224 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.47 [0.12, 1.82] |
| 3 Preterm birth less than 28 weeks Show forest plot | 1 | 224 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.37 [0.07, 1.88] |
| 4 Caesarean section Show forest plot | 1 | 224 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.89, 1.11] |
| 5 Infant birthweight less than 2500 g Show forest plot | 1 | 439 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.85, 1.04] |
| 6 Respiratory distress syndrome Show forest plot | 1 | 439 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.68 [0.55, 0.84] |
| 7 Use of mechanical ventilation Show forest plot | 1 | 439 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.47 [0.32, 0.69] |
| 8 Admission to NICU Show forest plot | 1 | 439 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.91 [0.82, 1.01] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Preterm birth less than 34 weeks Show forest plot | 2 | 158 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.57 [0.29, 1.10] |
| 2 Preterm birth less than 37 weeks Show forest plot | 2 | 168 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.72, 1.18] |