Hysteroscopy for treating subfertility associated with suspected major uterine cavity abnormalities
Information
- DOI:
- https://doi.org/10.1002/14651858.CD009461.pub4Copy DOI

- Database:
-
- Cochrane Database of Systematic Reviews
- Version published:
-
- 05 December 2018see what's new
- Type:
-
- Intervention
- Stage:
-
- Review
- Cochrane Editorial Group:
-
Cochrane Gynaecology and Fertility Group
- Copyright:
-
- Copyright © 2018 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Article metrics
Altmetric:
Cited by:
Authors
Contributions of authors
JB: co‐ordinated the writing of the protocol and review and its update.
SVW and MB: assisted in the literature search and study selection.
FB and TD: independently assessed the retrieved published reports for inclusion of potentially eligible studies.
JB and SW: independently extracted study data.
FB and BWM: gave advice on review methodology and content and critically appraised the Cochrane Review.
Sources of support
Internal sources
-
CEBAM, Belgium.
Research grant was obtained through CEBAM, the Centre for Evidence‐based Medicine, Belgian Branch of Cochrane
External sources
-
No sources of support supplied
Declarations of interest
FB (principal investigator) and BWM (co‐investigator) were involved in the design and conduct of the 'inSIGHT trial' (SIGnificance of Routine Hysteroscopy Prior to a First 'in Vitro Fertilization' Treatment Cycle: NCT 01242852), which was financially supported by ZonMw, a Dutch government operated consortium responsible for granting funds in the field of clinical practice research.
Thomas D'Hooghe is paid full time by Merck KGaA, Darmstadt, Germany as Vice‐President and Head of Global Medical Affairs Fertility since October 1st 2015. He is also part time employed by KU Leuven (University of Leuven, Belgium) as Professor in Reproductive Medicine and by Yale University as Adjunct Professor Obstetrics and Gynecology. His co‐authorship on the current paper is part of his academic activity, and Merck KGaA does not have marketed products related to hysteroscopy. Professor D'Hooghe's employment by Merck is not in breach of Cochrane's Commercial Sponsorship Policy (clause 2) as he does not have a real or potential financial interest in the outcome of this review. This matter was referred to Cochrane's Funding Arbiter for advice.
FB has received monetary compensation for the following: member of the external advisory board for Merck Serono and Ferring, the Netherlands; educational activities for Ferring BV, the Netherlands; consultancy work for Gedeon Richter, Belgium; strategic co‐operation with Roche on automated anti‐Müllerian hormone (AMH) assay development; and research co‐operation with Ansh Labs.
BWM has received consultancy from ObsEva Geneva, Guerbet, and Merck; payment for review preparation from European Journal of Obstetrics and Gynecology and Reproductive Biology; and travel/accommodation/meeting expenses for various non‐commercial scientific meetings.
JB, SW, SVW and MB do not have conflicts of interest for the research presented in this updated Cochrane Review.
The first published version of the present Cochrane Review has been part of a PhD thesis entitled "Studies on the effectiveness of endoscopic surgery in reproductive medicine" (dare.uva.nl/record/497164), which has been successfully defended at the faculty of Medicine of the University of Amsterdam, the Netherlands on 2 September 2014 by the first author (JB).
Acknowledgements
Cochrane Gynaecology and Fertility (CGF) Group: we wish to thank Prof Cindy Farquhar, CGF Co‐ordinating Editor; Ms Jane Clarke, former CGF Managing Editor; Ms Helen Nagels, CGF Managing Editor and Ms Jane Marjoribanks, CGF Assistant Managing Editor for their advice and support. We have used the Cochrane Consumers and Communication Group (CCCG) supplementary author advice for describing the results of the present updated Cochrane Review (Ryan 2016). We thank Ms Marian Showell, CGF Information Specialist for assistance in searching the CGF Specialised Register and the handsearch.
Biomedical Library Gasthuisberg, Catholic University, Leuven, Belgium. Many thanks to Mr Jens De Groot for skilful assistance in developing the literature search strategy.
Prof Tirso Pérez‐Medina, head of the department of Gynaecology at the University Hospital Puerta de Hierro, Madrid, Spain, has answered all the queries concerning the randomised controlled trial on the effectiveness of hysteroscopic polypectomy prior to IUI.
The Board of the European Society of Gynaecological Endoscopy (ESGE). Prof Hans Brolmann (Past ESGE President) and Dr Rudi Campo (Former ESGE Secretary) have been very helpful in contacting a group of experts in hysteroscopy in the field of Reproductive Medicine. Dr Rudi Campo (ZOL Genk, Belgium), Dr Dick Schoot (Catharina Hospital, Eindhoven, the Netherlands), Prof Attilio Di Spiezio Sardo (University of Naples 'Frederico II', Naples, Italy), Prof Hervé Fernandez (Hôpital Bicêtre, Le Kremin‐Bicêtre, France), Prof Kristine Juul Hare ( Gynækologisk‐Obstetrisk afdeling, Hvidovre Hospital, Hvidovre, Denmark) and Dr Matthew Prior (Newcastle Fertility Centre, Newcastle, UK) have provided data on published or ongoing randomised trials relevant to the research questions.
Dr Ben Cohlen (Fertility Centre Isala, Zwolle, the Netherlands), Prof Willem Ombelet (ZOL, Genk, Belgium) and Prof Carl Spiessens (Leuven University Fertility Centre, Leuven, Belgium) have provided useful data on the clinical pregnancy rates after gonadotropin stimulation and IUI. Dr Mariette Goddijn (AMC Amsterdam, the Netherlands) has given valuable feedback on the risk of bias assessment for one of the included trials at the occasion of the oral opposition and defence of the PhD thesis of the first author.
Ms Elizabeth Bosselaers (Managing Secretary CEBAM, Cochrane Belgium) has assisted in improving the plain language summary.
We acknowledge comments sent by Prof Hossam Eldin Shawki Abdalla MD of the Obstetrics & Gynecology Department, Faculty of Medicine, El‐Minia University, Egypt. Our formal response was published in October 2014 and the points made were taken into account in this update.
The authors of the 2018 update thank Dr Jenneke Kasius for her contributions to previous versions of this review.
Version history
| Published | Title | Stage | Authors | Version |
| 2018 Dec 05 | Hysteroscopy for treating subfertility associated with suspected major uterine cavity abnormalities | Review | Jan Bosteels, Steffi van Wessel, Steven Weyers, Frank J Broekmans, Thomas M D'Hooghe, M Y Bongers, Ben Willem J Mol | |
| 2015 Feb 21 | Hysteroscopy for treating subfertility associated with suspected major uterine cavity abnormalities | Review | Jan Bosteels, Jenneke Kasius, Steven Weyers, Frank J Broekmans, Ben Willem J Mol, Thomas M D'Hooghe | |
| 2013 Jan 31 | Hysteroscopy for treating subfertility associated with suspected major uterine cavity abnormalities | Review | Jan Bosteels, Jenneke Kasius, Steven Weyers, Frank J Broekmans, Ben Willem J Mol, Thomas M D'Hooghe | |
| 2011 Nov 09 | Hysteroscopy for treating subfertility associated with suspected major uterine cavity abnormalities. | Protocol | Jan Bosteels, Jenneke Kasius, Steven Weyers, Frank J Broekmans, Ben Willem J Mol, Thomas M D'Hooghe | |
Differences between protocol and review
At the 2014 update:
-
As a result of further peer review, the objectives of the review have been rephrased. The descriptions in the Types of interventions and Data synthesis sections were modified accordingly. For both comparisons, we made a stratification according to the types of uterine pathology; for the second comparison, we made a clear distinction between IUI, IVF or ICSI.
-
'Summary of findings' tables using the GRADE approach were added.
-
In the Assessment of risk of bias in included studies section of the review, the items 'blinding of participants and personnel' and 'blinding of outcome assessors' were reinserted as requested by the editorial reviewers. We assessed all six items including blinding of participants, personnel and outcome assessors in the final review as opposed to the protocol.
-
In the Assessment of heterogeneity section of the review, we added the Q‐statistic.
-
In the Subgroup analysis and investigation of heterogeneity section of the review, we planned to conduct a further subgroup analysis based on the women's age.
At the 2018 update:
-
We added a fourth exclusion criterion in the section Types of participants: women of reproductive age with no major uterine cavity abnormalities detected by US, SIS, GIS, HSG, diagnostic hysteroscopy or any combination of these methods. The objective of this review was to assess the effectiveness of operative hysteroscopy in women with suspected uterine cavity abnormalities. The effectiveness of hysteroscopy in women without suspected uterine cavity abnormalities is the objective of a second Cochrane review. The addition of this fourth exclusion criterion is to emphasise the difference between the reviews since they include different study populations.
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
- Coitus;
- Endometrium;
- Fertilization in Vitro;
- *Hysteroscopy [adverse effects];
- Infertility [etiology, *surgery];
- Insemination, Artificial [methods];
- Leiomyoma [*surgery];
- Live Birth;
- Polyps [*surgery];
- Randomized Controlled Trials as Topic;
- Tissue Adhesions [surgery];
- Uterine Diseases [*surgery];
- Uterus [abnormalities];
Medical Subject Headings Check Words
Female; Humans; Pregnancy;
PICOs
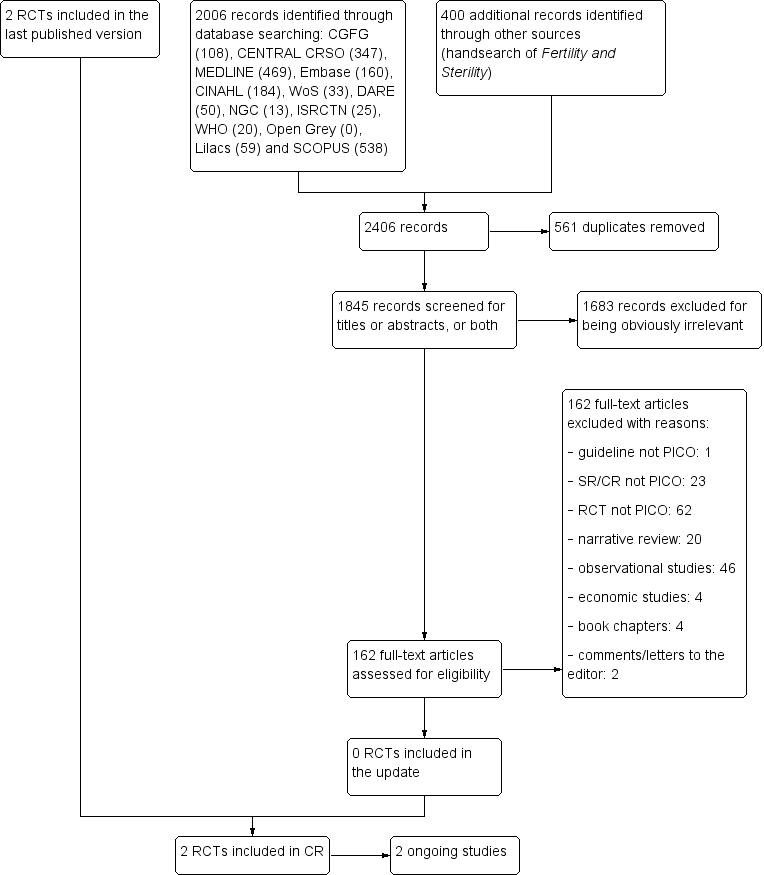
Study flow diagram: summary of searches since 2014. CR: Cochrane Review; PICO: Population, Intervention, Comparator, Outcome; RCT: randomised controlled trial; SR: systematic review.

'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
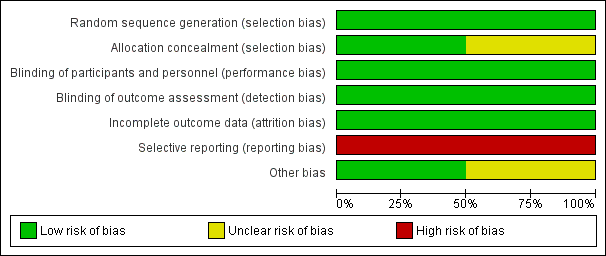
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Forest plot of comparison: 1 Hysteroscopic myomectomy vs no surgery in women with unexplained subfertility and submucous fibroids. Outcome: 1.1 Clinical pregnancy per woman randomised.
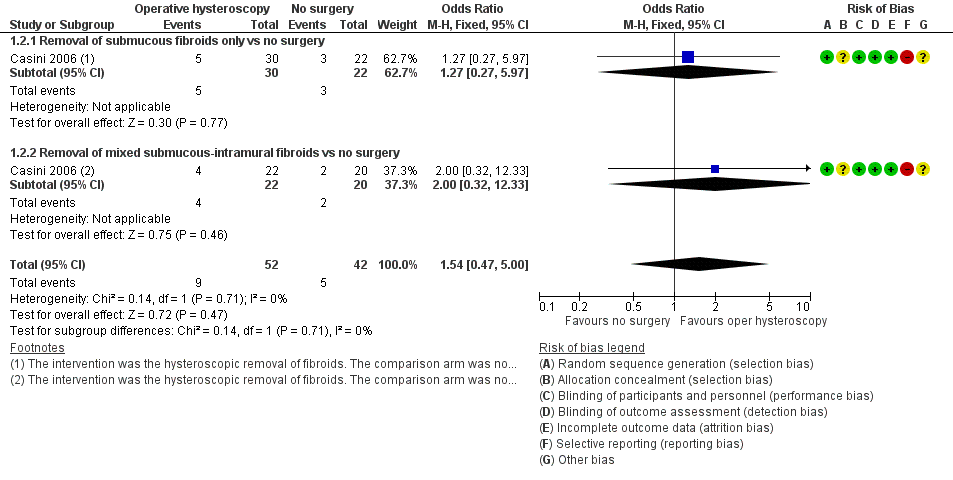
Forest plot of comparison: 1 Hysteroscopic myomectomy vs no surgery in women with unexplained subfertility and submucous fibroids. Outcome: 1.2 Miscarriage per clinical pregnancy.
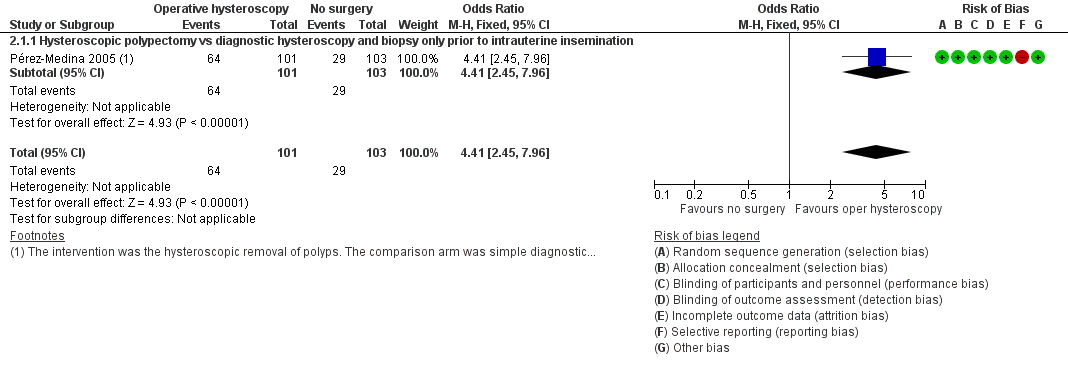
Forest plot of comparison: 2 Hysteroscopic removal of polyps vs diagnostic hysteroscopy and biopsy only prior to intrauterine insemination. Outcome: 2.1 Clinical pregnancy per woman randomised.

Comparison 1 Operative hysteroscopy versus control in women with otherwise unexplained subfertility and suspected major uterine cavity abnormalities, Outcome 1 Clinical pregnancy.

Comparison 1 Operative hysteroscopy versus control in women with otherwise unexplained subfertility and suspected major uterine cavity abnormalities, Outcome 2 Adverse events: miscarriage.

Comparison 2 Operative hysteroscopy versus control in women undergoing medically assisted reproduction with suspected major uterine cavity abnormalities, Outcome 1 Clinical pregnancy.
| Operative hysteroscopy versus control in women with otherwise unexplained subfertility and suspected major uterine cavity abnormalities | ||||||
| Patient or population: women with submucous fibroids and otherwise unexplained subfertility Settings: infertility centre in Rome, Italy Intervention: hysteroscopic removal of 1 submucous fibroid ≤ 40 mm Comparison: no surgery | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| No surgery | Myomectomy | |||||
| Live birth | No data reported. | |||||
| Adverse events: hysteroscopy complications | No data reported. | |||||
| Clinical pregnancya Ultrasound 12 months | 214 per 1000 | 400 per 1000 | OR 2.44 (0.97 to 6.17) | 94 | ⊕⊝⊝⊝ | — |
| Adverse events: miscarriaged Ultrasound 12 months | 119 per 1000 | 172 per 1000 | OR 1.54 (0.47 to 5.00) | 94 women | ⊕⊝⊝⊝ | — |
| *The basis for the assumed risk is the control group risk of the single included study (Casini 2006). The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aClinical pregnancy defined by the visualisation of an embryo with cardiac activity at six to seven weeks' gestational age. bDowngraded by two levels for very serious risk of bias (unclear allocation concealment, high risk of selective outcome reporting and unclear whether there is other bias caused by imbalance in the baseline characteristics). cDowngraded by one level for serious imprecision (wide confidence interval of the effect size estimate). dMiscarriage was defined by the clinical loss of an intrauterine pregnancy between the 7th and 12th weeks of gestation. | ||||||
| Operative hysteroscopy versus control in women undergoing medically assisted reproduction with suspected major uterine cavity abnormalities | ||||||
| Patient or population: subfertile women with endometrial polyps diagnosed by ultrasonography prior to treatment with gonadotropin and intrauterine insemination Settings: infertility unit of a university tertiary hospital in Madrid, Spain Intervention: hysteroscopic polypectomy using a 5.5 mm continuous flow office hysteroscope with a 1.5 mm scissors and forceps Comparison: diagnostic hysteroscopy using a 5.5 mm continuous flow office hysteroscope and polyp biopsy | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Polypectomy | |||||
| Live birth | No data reported. | |||||
| Adverse events: hysteroscopy complications | No data reported. | |||||
| Clinical pregnancya Ultrasound 4 intrauterine insemination cycles | 282 per 1000 | 634 per 1000 | OR 4.41 (2.45 to 7.96) | 204 | ⊕⊕⊝⊝ | — |
| Adverse events: miscarriage | No data were reported for this secondary outcome. | |||||
| *The basis for the assumed risk is the control group risk of the single included study (Pérez‐Medina 2005). The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aClinical pregnancy was defined by the presence of at least one gestational sac on ultrasound. bDowngraded by one level for serious risk of bias (high risk for selective outcome reporting). cDowngraded by one level for serious imprecision (wide confidence interval of the effect size estimate). | ||||||
| Polyp size | Clinical pregnancya | Clinical pregnancy rate (95% CI)b |
| < 5 mm | 19/25 | 76% (72% to 80%) |
| 5–10 mm | 18/32 | 56% (53% to 59%) |
| 11–20 mm | 16/26 | 61% (58% to 65%) |
| > 20 mm | 11/18 | 61% (58% to 64%) |
| CI: confidence interval. aClinical pregnancy is defined by a pregnancy diagnosed by ultrasound visualisation of at least one gestational sac per woman randomised. bNo significant difference was found for the clinical pregnancy rates between the 4 subgroups (P = 0.32). | ||
| Quality assessment Submucous fibroids and unexplained subfertility | ||||||
| No of studies | Design | Limitations | Inconsistency | Indirectness | Imprecision | Other considerations |
| Clinical pregnancy (follow‐up 1 year; ultrasounda) | ||||||
| 1 | RCT | Very seriousb | Not serious | Not indirectness | Seriousc | None |
| Miscarriage (follow‐up 1 year; ultrasoundd) | ||||||
| 1 | RCT | Very seriousb | Not serious | Not serious | Seriousc | None |
| aA clinical pregnancy was defined by the visualisation of an embryo with cardiac activity at six to seven weeks' gestational age. bUnclear allocation concealment and high risk of selective outcome reporting. cWide confidence intervals. dMiscarriage was defined by the clinical loss of an intrauterine pregnancy between the 7th and 12th weeks of gestation. | ||||||
| Quality assessment Endometrial polyps prior to gonadotropin and IUI treatment | ||||||
| No of studies | Design | Limitations | Inconsistency | Indirectness | Imprecision | Other considerations |
| Clinical pregnancy (follow‐up 4 IUI cycles; ultrasounda) | ||||||
| 1 | RCT | Seriousb | Not serious | Not serious | Not serious | None |
| IUI: intrauterine insemination; RCT: randomised controlled trial. aClinical pregnancy was defined by the presence of at least one gestational sac on ultrasound. bThere was high risk for selective outcome reporting bias. | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Clinical pregnancy Show forest plot | 1 | 94 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.44 [0.97, 6.17] |
| 1.1 Removal of submucous fibroids only vs no surgery | 1 | 52 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.04 [0.62, 6.66] |
| 1.2 Removal of mixed submucous‐intramural fibroids vs no surgery | 1 | 42 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.24 [0.72, 14.57] |
| 2 Adverse events: miscarriage Show forest plot | 1 | 94 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.54 [0.47, 5.00] |
| 2.1 Removal of submucous fibroids only vs no surgery | 1 | 52 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.27 [0.27, 5.97] |
| 2.2 Removal of mixed submucous‐intramural fibroids vs no surgery | 1 | 42 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.0 [0.32, 12.33] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Clinical pregnancy Show forest plot | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.41 [2.45, 7.96] |
| 1.1 Hysteroscopic polypectomy vs diagnostic hysteroscopy and biopsy only prior to intrauterine insemination | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.41 [2.45, 7.96] |