Percussion, diuresis, and inversion therapy for the passage of lower pole kidney stones following shock wave lithotripsy
References
References to studies included in this review
References to studies excluded from this review
Additional references
References to other published versions of this review
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Jump to:
| Methods |
| |
| Participants |
| |
| Interventions | Treatment group
Control group
| |
| Outcomes |
| |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Using simple randomization by computer" |
| Allocation concealment (selection bias) | Unclear risk | "Patients were randomized to a control group or SWL plus percussion, diuresis, inversion therapy group using simple randomization by computer" |
| Blinding of participants and personnel (performance bias) | High risk | Blinded to the radiologist only |
| Blinding of outcome assessment (detection bias) | Low risk | Blinded to the radiologist only |
| Incomplete outcome data (attrition bias) | Low risk | ITT analysis reported. 2.7% of randomised patients were lost to follow‐up, however data for all patients were reported |
| Selective reporting (reporting bias) | Low risk | Stone‐free rate and the overall reduction in stone size had been reported. Study protocol was not available |
| Other bias | Low risk | Supported by a National Healthcare Group research grant (Singapore) |
| Methods |
| |
| Participants |
| |
| Interventions | Treatment group
Control group
| |
| Outcomes |
| |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Patients were randomised with simple block randomisation |
| Allocation concealment (selection bias) | Unclear risk | Patients were randomised with simple block randomisation to treatment group or observation group. |
| Blinding of participants and personnel (performance bias) | High risk | Blinded to the radiologist only |
| Blinding of outcome assessment (detection bias) | Low risk | "A blinded radiologist adjudicated all films to determine final stone free state" |
| Incomplete outcome data (attrition bias) | Low risk | ITT analysis reported, 11.5% of randomised patients were lost to follow‐up, however data for all patients has been reported |
| Selective reporting (reporting bias) | Low risk | Primary outcomes (stone free rate and stone burden reduction rate) were reported. Study protocol was available |
| Other bias | Unclear risk | Source of funding not stated |
ITT, intention‐to‐treat; IVP, intravenous pyelogram; RCT, randomised controlled trial; SWL, shock wave lithotripsy
Characteristics of excluded studies [ordered by study ID]
Jump to:
| Study | Reason for exclusion |
| Not RCT | |
| Did not assess percussion, diuresis, and inversion therapy for passage of lower pole kidney stones | |
| Did not assess percussion, diuresis, and inversion therapy for passage of lower pole kidney stones | |
| Did not assess percussion, diuresis, and inversion therapy for passage of lower pole kidney stones | |
| Did not assess percussion, diuresis, and inversion therapy for passage of lower pole kidney stones | |
| Did not assess percussion, diuresis, and inversion therapy for passage of lower pole kidney stones | |
| Did not assess percussion, diuresis, and inversion therapy for passage of lower pole kidney stones | |
| Did not assess percussion, diuresis and inversion therapy for passage of lower pole kidney stones |
RCT, randomised controlled trial
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Stone‐free rate Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Analysis 1.1 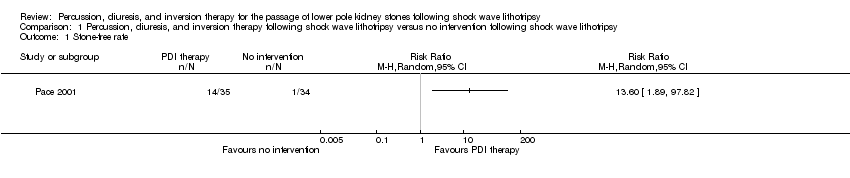 Comparison 1 Percussion, diuresis, and inversion therapy following shock wave lithotripsy versus no intervention following shock wave lithotripsy, Outcome 1 Stone‐free rate. | ||||
| 2 Stone burden reduction Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| Analysis 1.2 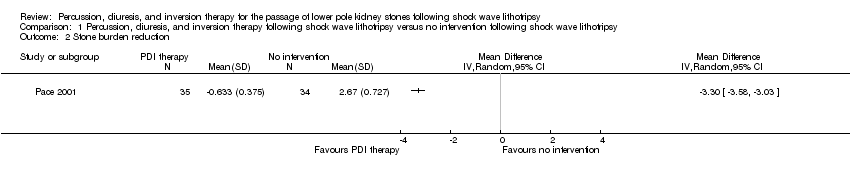 Comparison 1 Percussion, diuresis, and inversion therapy following shock wave lithotripsy versus no intervention following shock wave lithotripsy, Outcome 2 Stone burden reduction. | ||||
| 3 Complications Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Analysis 1.3  Comparison 1 Percussion, diuresis, and inversion therapy following shock wave lithotripsy versus no intervention following shock wave lithotripsy, Outcome 3 Complications. | ||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Stone‐free rate Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Analysis 2.1  Comparison 2 Percussion, diuresis, and inversion plus shock wave lithotripsy therapy versus shock wave lithotripsy alone, Outcome 1 Stone‐free rate. | ||||
| 2 Stone burden reduction Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| Analysis 2.2 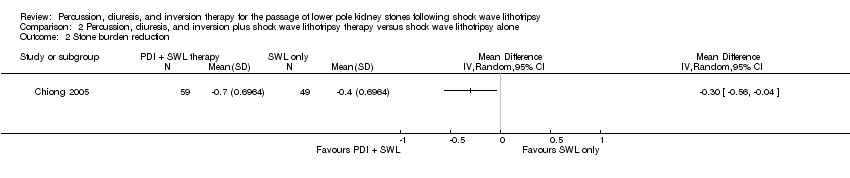 Comparison 2 Percussion, diuresis, and inversion plus shock wave lithotripsy therapy versus shock wave lithotripsy alone, Outcome 2 Stone burden reduction. | ||||
| 3 Complications Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Analysis 2.3  Comparison 2 Percussion, diuresis, and inversion plus shock wave lithotripsy therapy versus shock wave lithotripsy alone, Outcome 3 Complications. | ||||


Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Comparison 1 Percussion, diuresis, and inversion therapy following shock wave lithotripsy versus no intervention following shock wave lithotripsy, Outcome 1 Stone‐free rate.
Comparison 1 Percussion, diuresis, and inversion therapy following shock wave lithotripsy versus no intervention following shock wave lithotripsy, Outcome 2 Stone burden reduction.
Comparison 1 Percussion, diuresis, and inversion therapy following shock wave lithotripsy versus no intervention following shock wave lithotripsy, Outcome 3 Complications.
Comparison 2 Percussion, diuresis, and inversion plus shock wave lithotripsy therapy versus shock wave lithotripsy alone, Outcome 1 Stone‐free rate.
Comparison 2 Percussion, diuresis, and inversion plus shock wave lithotripsy therapy versus shock wave lithotripsy alone, Outcome 2 Stone burden reduction.
Comparison 2 Percussion, diuresis, and inversion plus shock wave lithotripsy therapy versus shock wave lithotripsy alone, Outcome 3 Complications.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Stone‐free rate Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Stone burden reduction Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3 Complications Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Stone‐free rate Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 2 Stone burden reduction Show forest plot | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3 Complications Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |