Clinically‐indicated replacement versus routine replacement of peripheral venous catheters
References
References to studies included in this review
References to studies excluded from this review
Additional references
References to other published versions of this review
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Jump to:
| Methods | Study design: Single‐centre RCT. Method of randomisation: Computer generated. Concealment of allocation: Sealed envelopes. | |
| Participants | Country: England. Number: 47 patients in general medical or surgical wards. Clinically indicated: 43 catheters were inserted in 26 patients. Routine replacement: 41 catheters were inserted in 21 patients. Age: Clinically indicated 60.5 yrs (15.5); routine replacement 62.7 yrs (18.2). Sex (M/F): Clinically indicated 15/11; routine replacement 14/7. Inclusion criteria: Hospital inpatients receiving crystalloids and drugs. Exclusion criteria: Not stated. | |
| Interventions | Clinically indicated: Catheters were removed if the site became painful, the catheter dislodged or there were signs of PVT. Routine replacement: Catheters were replaced every 48 hours. | |
| Outcomes | Primary: Incidence of PVT defined as "the development of two or more of the following: pain, erythema, swelling, excessive warmth or a palpable venous cord". | |
| Notes | PVT was defined as "the development of two or more of the following: pain, erythema, swelling, excessive warmth or a palpable venous cord". However, in the discussion, the author stated that "even a small area of erythema was recorded as phlebitis" (i.e., only one sign). It is unclear what proportion of patients were on continuous infusion. Catheters were inserted "at the instruction of the principal investigator". "All patients were reviewed daily by the principal investigator, and examined for signs of PVT at the current and all previous infusion sites". | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: Computer generated (personal communication with author). |
| Allocation concealment (selection bias) | Low risk | Comment: Sealed envelopes (personal communication with author). |
| Blinding (performance bias and detection bias) | High risk | Comment: Neither study personnel nor participants were blinded. |
| Incomplete outcome data (attrition bias) | High risk | Comment: In this small sample, there were five fewer patients in the routine replacement group. No explanation was provided for the unequal sample size. No dropouts or loss to follow up were reported. |
| Selective reporting (reporting bias) | Low risk | Comment: Phlebitis was the only outcome planned. |
| Other bias | High risk | Comment: The chief investigator allocated patients and was responsible for outcome evaluation. No sample size calculation. |
| Methods | Study design: Single‐centre RCT. Method of randomisation: Not stated Concealment of allocation: Sequentially numbered sealed envelopes. | |
| Participants | Country: India. Number: 42 patients in surgical wards. Clinically indicated: 21. Routine replacement: 21. Age: Clinically indicated 40.2 yrs (15.0); routine replacement 42.9 yrs (15.0). Sex (M/F): Clinically indicated 17/4; routine replacement 16/5. Inclusion criteria: Hospital inpatients admitted for major abdominal surgery Exclusion criteria: Receiving total parenteral nutrition, duration of therapy expected to be < three days, if a cannula was already in situ, terminally ill patients. | |
| Interventions | Clinically indicated: Catheters were removed if the site became painful, the catheter dislodged or there were signs of PVT. Routine replacement: Catheters were replaced every 48 hours. | |
| Outcomes | Primary: Incidence of PVT defined as "the development of two or more of the following: pain, erythema, swelling, excessive warmth or a palpable venous cord". | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated. |
| Allocation concealment (selection bias) | Low risk | Quote "group name was placed (on) an opaque serially numbered sealed envelope (SNOSE)." Comment: Presumably the authors meant 'in' an opaque serially numbered sealed envelope ‐ based on subsequent information. |
| Blinding (performance bias and detection bias) | High risk | Evidence for participants: Quote "unblinded study".
Evidence for personnel: As above.
Evidence for outcomes: As above. |
| Incomplete outcome data (attrition bias) | Low risk | Comment: Data for all patients were available. |
| Selective reporting (reporting bias) | Low risk | Comment: Stated outcomes were reported but original protocol not sighted. |
| Other bias | Unclear risk | Extreme results: In this small trial, 100% of participants in the clinically indicated group developed phlebitis compared with 9% in the 2‐day change group, which suggests that chance or other unknown bias affected results. |
| Methods | Study design: Single‐centre RCT. Method of randomisation: Computer generated. Concealment of allocation: Telephone service. | |
| Participants | Country: Australia. Number: 362 patients requiring IV therapy in general medical or surgical wards. Clinically indicated: 280 catheters were inserted in 185 patients. Routine replacement: 323 catheters were inserted in 177 patients. Age: Clinically indicated 62.7 yrs (15.5); routine replacement 65.1 yrs (17.3). Sex (M/F): Clinically indicated 82/103; routine replacement 81/91. Inclusion criteria: Patients in over 18 years, expected to have a peripheral intravenous device (IVD), requiring IV therapy for at least 4 days. Exclusion criteria: Patients who were immunosuppressed, had an existing bloodstream infection or those in whom an IVD had been in place for > 48 hours. | |
| Interventions | Clinically indicated: Catheters were removed if there were signs of phlebitis, local infection, bacteraemia, infiltration or blockage. Routine replacement: Catheters were replaced every 72 ‐ 96 hours. | |
| Outcomes | Primary: Phlebitis per person and per 1000 IVD days (defined as two or more of the following: pain, erythema, purulence, infiltration, palpable venous cord). IVD‐related bacteraemia. Secondary: Hours of catheterisation; number of IV devices; device‐related bloodstream infection; infiltration; local infection. | |
| Notes | Approximately 75% of patients were receiving a continuous infusion. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: Computer generated. |
| Allocation concealment (selection bias) | Low risk | Quote "assignment was concealed until randomisation by use of a telephone service". |
| Blinding (performance bias and detection bias) | High risk | Comment: Neither study personnel nor participants were blinded. |
| Incomplete outcome data (attrition bias) | Low risk | Comment: Results from all enrolled patients were reported. |
| Selective reporting (reporting bias) | Low risk | Comment: The protocol was available. All nominated outcomes were reported. |
| Other bias | Unclear risk | Comment: Significantly more patients in the routine change group received IV antibiotics (73.1% versus 62.9%). |
| Methods | Study design: Multi‐centre RCT. Method of randomisation: Computer generated, stratified by site. Concealment of allocation: Allocation concealed until eligibility criteria was entered into a hand‐held computer. | |
| Participants | Country: Australia. Number: 3283 patients requiring IV therapy in general medical or surgical wards. Clinically indicated: 1593 patients. Routine replacement: 1690 patients. Age: Clinically indicated 55.1 yrs (18.6); routine replacement 55.0 yrs (18.4). Sex (M/F): Clinically indicated 1022/571; routine replacement 1034/656. Inclusion criteria: Patients, or their representative able to provide written consent; over 18 years, expected to have a peripheral intravenous device (IVD) in situ, requiring IV therapy for at least 4 days. Exclusion criteria: Patients who were immunosuppressed, had an existing blood stream infection or those in whom an IVD had been in place for > 48 hours or it was planned for the catheter to be removed < 24 hours. | |
| Interventions | Clinically indicated: Catheters were removed if there were signs of phlebitis, local infection, bacteraemia, infiltration or blockage. Routine replacement: Catheters were replaced every 72 ‐ 96 hours. | |
| Outcomes | Primary: Phlebitis during catheterisation or within 48 hrs of removal (defined as two or more of the following: pain, erythema, swelling, purulent discharge, palpable venous cord). Secondary: Catheter‐related bloodstream infection, all‐cause bloodstream infection, local venous infection, colonisation of the catheter tip, infusion failure, number of catheters per patient, overall duration of intravenous therapy, cost, mortality. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Random allocations were computer‐generated". |
| Allocation concealment (selection bias) | Low risk | Quote: "Random allocations were computer‐generated on a hand‐held device, at the point of each patient's entry, and thus were concealed to patients, clinical staff and research staff until this time". |
| Blinding (performance bias and detection bias) | High risk | Evidence for participants: Quote "Patients and clinical staff could not be blinded".
Evidence for personnel: Quote "Research nurses were similarly not masked".
Evidence for outcomes: Quote "... laboratory staff were masked for rating of all microbiological end‐points, and a masked, independent medical rater diagnosed catheter‐related infections and all bloodstream infections". |
| Incomplete outcome data (attrition bias) | Low risk | ITT analysis reported. |
| Selective reporting (reporting bias) | Low risk | The protocol was available and all pre‐defined outcomes were reported. |
| Other bias | Low risk | No other known risks of bias. |
| Methods | Study design: RCT. Method of randomisation: Computer generated. Concealment of allocation: Sealed envelopes. | |
| Participants | Country: Australia. Number: 200. Clinically indicated: 105 patients. Routine replacement: 95 patients. Age: Clinically indicated 62.8 yrs (18.2); routine replacement 54.5 yrs (19.0). Sex (M/F): Not stated. Inclusion criteria: Adult patients who could be treated at home for an acute illness and had a 20, 22, or 24 gauge catheter inserted in an upper extremity. Exclusion criteria: Not stated. | |
| Interventions | Clinically indicated: Catheters were removed if there were signs of phlebitis, local infection, bacteraemia, infiltration or blockage. Routine replacement: Catheters were replaced every 72 ‐ 96 hours. | |
| Outcomes | Primary: Phlebitis per patient and per 1000 device days (phlebitis was defined as a total score of 2 or more points from the following factors: pain (on a 10‐point scale, 1 = 1 point, and 2 or more = 2 points; redness (less than 1cm = 1 point, and 1 or more cm = 2 points); swelling (as for redness); and discharge (haemoserous ooze under dressing = 1 point, and haemoserous ooze requiring dressing change or purulence = 2 points). Also reported on: Suspected IVD‐related bacteraemia and occlusion/blockage. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: Computer generated allocation (personal communication with author). |
| Allocation concealment (selection bias) | Low risk | Quote: "Randomization was concealed until treatment via sealed envelopes". |
| Blinding (performance bias and detection bias) | High risk | Comment: Neither study personnel nor participants were blinded. |
| Incomplete outcome data (attrition bias) | Low risk | Comment: Participant flow chart provided. Results from all enrolled patients were reported. |
| Selective reporting (reporting bias) | Low risk | Comment: All planned outcomes were reported. |
| Other bias | Low risk | No other known risks of bias. |
| Methods | Study design: Single‐centre RCT. Method of randomisation: Computer generated. Concealment of allocation: Allocation concealed until telephone contact made with an independent person. | |
| Participants | Country: Australia. Number: 206. Clinically indicated: 103 patients. Routine replacement: 103 patients. Age: Clinically indicated 60.2 yrs (16.2); routine replacement 63.1 yrs (17.3). Sex (M/F): Clinically indicated 53/50; routine replacement 54/49. Inclusion criteria: At least 18 yrs of age, expected to have a peripheral intravenous device (IVD) in situ, requiring IV therapy for at least 4 days, catheter inserted by a member of the IV team. Exclusion criteria: Immunosuppressed patients and those with an existing bloodstream infection. | |
| Interventions | Clinically indicated: Catheters removed if there were signs of phlebitis, local infection, bacteraemia, infiltration or blockage. Routine replacement: Catheters replaced every 3 days. | |
| Outcomes | Primary: Composite measure of any reason for an unplanned catheter removal. Secondary: Cost (For intermittent infusion: 20 minutes nursing/medical time, a cannula, a 3 way tap, a basic dressing pack, gloves, a syringe, transparent adhesive dressing, skin disinfection and local anaesthetic per insertion. For patients receiving a continuous infusion: all the above costs plus the additional cost of replacing all associated lines, solutions and additives which are discarded when an IV catheter is changed (based on an intravenous administration set, 1 litre sodium chloride 0.09%). | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomization was by computer generated random number list, stratified by oncology status". |
| Allocation concealment (selection bias) | Low risk | Quote: "Allocation was made by phoning a person who was independent of the recruitment process". |
| Blinding (performance bias and detection bias) | High risk | Evidence for participants: Comment: Participants could not be blinded.
Evidence for personnel: Quote "clinical staff were subsequently aware of the treatment group".
Evidence for outcomes: Quote: "research staff had no involvement in nominating the reason for catheter removal or in diagnosing phlebitis". "Staff in the microbiological laboratory were blind to group assignment of catheters submitted for testing". |
| Incomplete outcome data (attrition bias) | Low risk | Comment: All recruited patients were accounted for in the results. |
| Selective reporting (reporting bias) | Low risk | Comment: Protocol was available. All planned outcomes were reported. |
| Other bias | Low risk | No other known risks of bias. |
| Methods | Study design: Single‐centre RCT. Method of randomisation: Computer generated. Concealment of allocation: Telephone randomisation. | |
| Participants | Country: Australia. Number: 755. Clinically indicated: 379 patients. Routine replacement: 376 patients. Age: Clinically indicated 60.1 yrs (17.1); routine replacement 58.8 yrs (18.8). Sex (M/F): Clinically indicated 248/131; routine replacement 233/143. Inclusion criteria: At least 18 yrs of age, expected to have a IVD in situ, requiring IV therapy for at least 4 days. Exclusion criteria: Immunosuppressed patients and those with an existing bloodstream infection. | |
| Interventions | Clinically indicated: Catheter removed if there were signs of phlebitis, local infection, bacteraemia, infiltration or blockage. Routine replacement: Catheter replaced every 3 days. | |
| Outcomes | Primary: A composite measure of phlebitis (defined as two or more of the following: pain, erythema, purulence, infiltration, palpable venous cord) and infiltration. Secondary: Infusion‐related costs. Cost (For intermittent infusion: 20‐minutes nursing/medical time, a cannula, a 3‐way tap, a basic dressing pack, gloves, a syringe, transparent adhesive dressing, skin disinfection and local anaesthetic per insertion. For patients receiving a continuous infusion: all the above costs plus the additional cost of replacing all associated lines, solutions and additives which are discarded when an IV catheter is changed (based on an intravenous administration set, 1 litre sodium chloride 0.09%). Individual reasons for catheter failure (occlusion/blockage, local infection). Also reported: Bacteraemia rate. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Block randomisation was by a computer generated random number list". |
| Allocation concealment (selection bias) | Low risk | Quote: ".... telephoned a contact who was independent of the recruitment process for allocation consignment". |
| Blinding (performance bias and detection bias) | High risk | Neither study personnel nor participants were blinded. |
| Incomplete outcome data (attrition bias) | Low risk | All recruited patients were accounted for in the results. |
| Selective reporting (reporting bias) | Low risk | Protocol was available. All planned outcomes were reported. |
| Other bias | Low risk | No other known risks of bias. |
IV: intravenous
IVD: peripheral intravenous device
PVT: peripheral vein infusion thrombophlebitis
RCT: randomised controlled trial
Characteristics of excluded studies [ordered by study ID]
Jump to:
| Study | Reason for exclusion |
| Not a randomised controlled trial | |
| Involved central, not peripheral lines | |
| Involved pulmonary artery or arterial catheters, not peripheral catheters | |
| End point was lymphangitis | |
| Patients were receiving parenteral nutrition | |
| Patients were receiving parenteral nutrition | |
| Involved central, not peripheral lines | |
| Compared the use of a single intraoperative and postoperative catheters with two catheters, one used intraoperatively and a separate catheter for postoperative use | |
| Involved central, not peripheral lines |
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Catheter‐related blood stream infection Show forest plot | 5 | 4806 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.08, 4.68] |
| Analysis 1.1  Comparison 1 Clinically‐indicated versus routine change, Outcome 1 Catheter‐related blood stream infection. | ||||
| 2 Phlebitis Show forest plot | 5 | 4806 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.93, 1.39] |
| Analysis 1.2  Comparison 1 Clinically‐indicated versus routine change, Outcome 2 Phlebitis. | ||||
| 2.1 Continuous infusion | 4 | 4606 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.11 [0.89, 1.39] |
| 2.2 Intermittent infusion | 1 | 200 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.29 [0.85, 1.96] |
| 3 Phlebitis per device days Show forest plot | 5 | 26191 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.84, 1.27] |
| Analysis 1.3 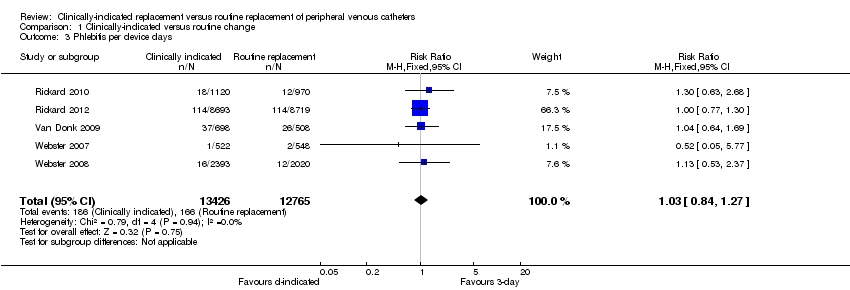 Comparison 1 Clinically‐indicated versus routine change, Outcome 3 Phlebitis per device days. | ||||
| 4 All‐cause blood stream infection Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| Analysis 1.4 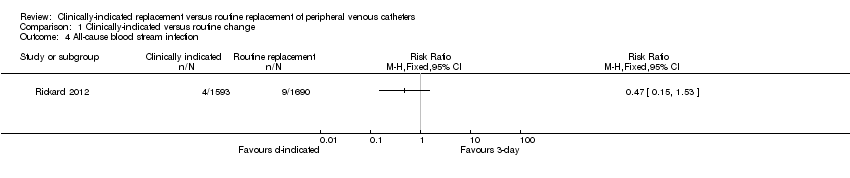 Comparison 1 Clinically‐indicated versus routine change, Outcome 4 All‐cause blood stream infection. | ||||
| 5 Cost Show forest plot | 3 | 4244 | Mean Difference (IV, Fixed, 95% CI) | ‐6.96 [‐9.05, ‐4.86] |
| Analysis 1.5 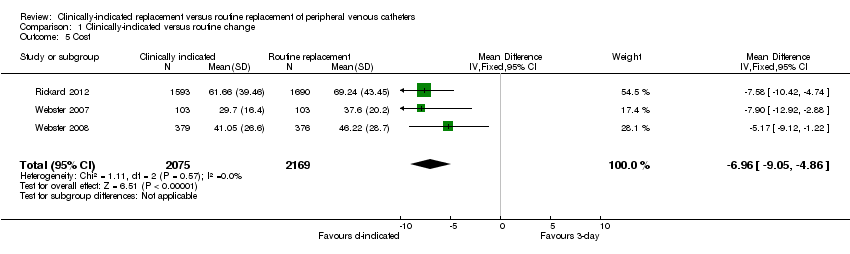 Comparison 1 Clinically‐indicated versus routine change, Outcome 5 Cost. | ||||
| 6 Infiltration Show forest plot | 4 | 4606 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.17 [1.05, 1.31] |
| Analysis 1.6 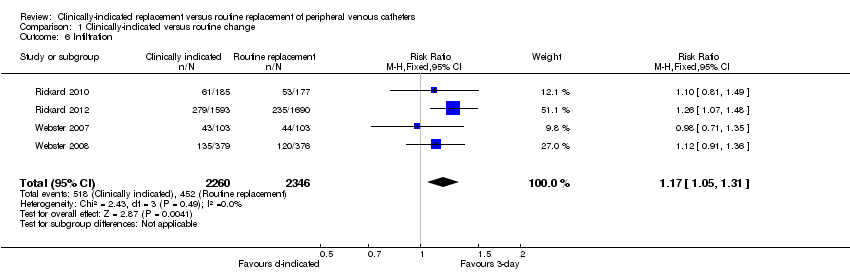 Comparison 1 Clinically‐indicated versus routine change, Outcome 6 Infiltration. | ||||
| 7 Catheter blockage Show forest plot | 5 | 4806 | Risk Ratio (M‐H, Random, 95% CI) | 1.25 [0.91, 1.71] |
| Analysis 1.7 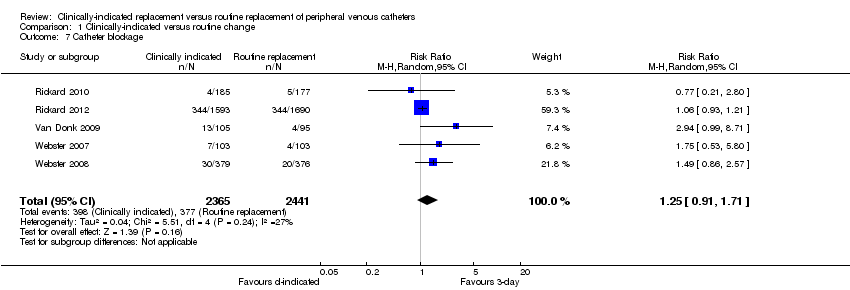 Comparison 1 Clinically‐indicated versus routine change, Outcome 7 Catheter blockage. | ||||
| 8 Local infection Show forest plot | 4 | 4606 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.96 [0.24, 102.98] |
| Analysis 1.8 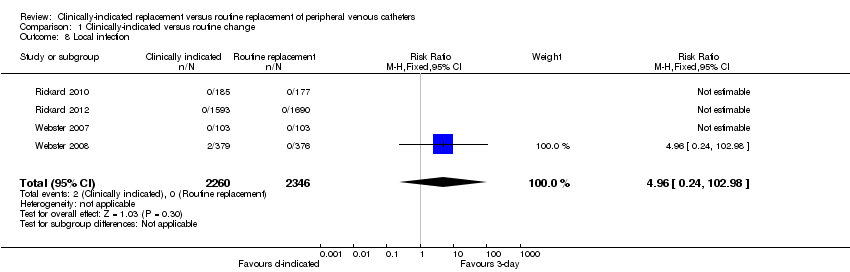 Comparison 1 Clinically‐indicated versus routine change, Outcome 8 Local infection. | ||||
| 9 Mortality Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| Analysis 1.9 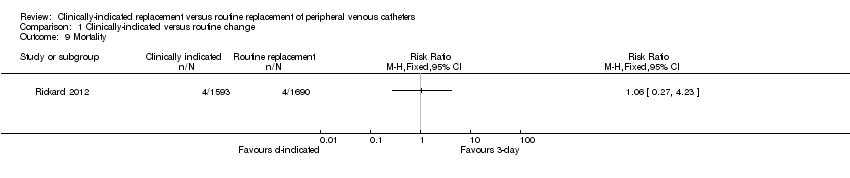 Comparison 1 Clinically‐indicated versus routine change, Outcome 9 Mortality. | ||||

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Forest plot of comparison: 1 Clinically‐indicated versus routine change, outcome: 1.1 Catheter‐related bloodstream infection.
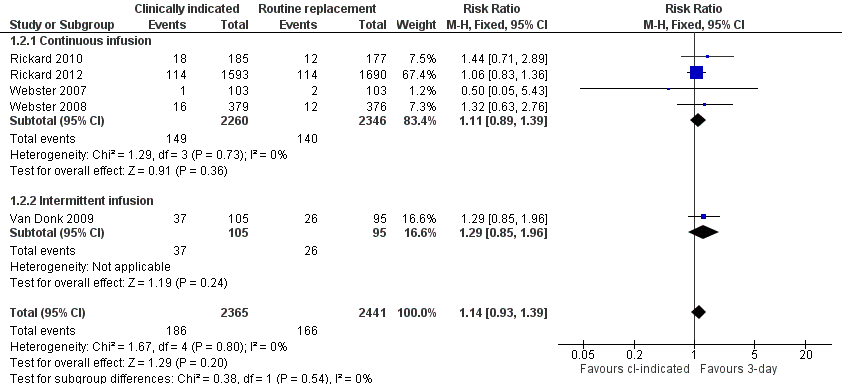
Forest plot of comparison: 1 Clinically‐indicated versus routine change, outcome: 1.2 Phlebitis.
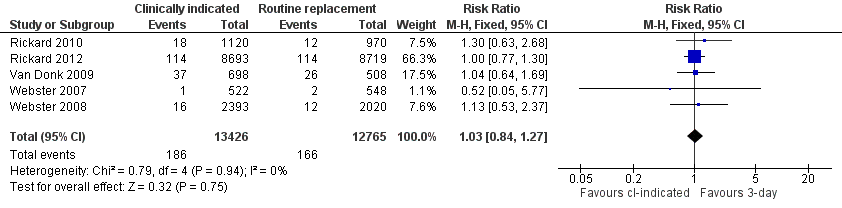
Forest plot of comparison: 1 Clinically‐indicated versus routine change, outcome: 1.3 Phlebitis per device days.

Forest plot of comparison: 1 Clinically‐indicated versus routine change, outcome: 1.4 All‐cause bloodstream infection.

Forest plot of comparison: 1 Clinically‐indicated versus routine change, outcome: 1.5 Cost.

Forest plot of comparison: 1 Clinically‐indicated versus routine change, outcome: 1.6 Infiltration.
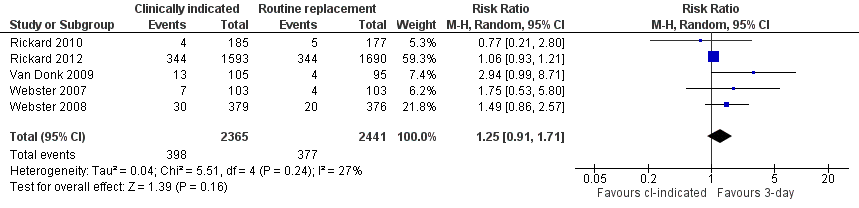
Forest plot of comparison: 1 Clinically‐indicated versus routine change, outcome: 1.7 Catheter blockage.
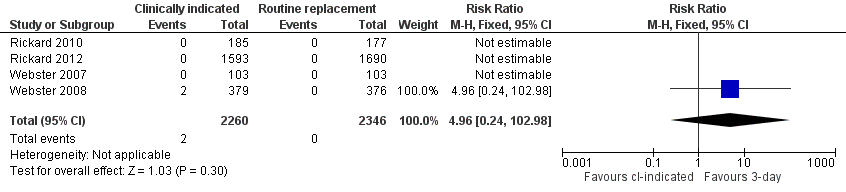
Forest plot of comparison: 1 Clinically‐indicated versus routine change, outcome: 1.8 Local infection.

Forest plot of comparison: 1 Clinically‐indicated versus routine change, outcome: 1.9 Mortality.
Comparison 1 Clinically‐indicated versus routine change, Outcome 1 Catheter‐related blood stream infection.
Comparison 1 Clinically‐indicated versus routine change, Outcome 2 Phlebitis.
Comparison 1 Clinically‐indicated versus routine change, Outcome 3 Phlebitis per device days.
Comparison 1 Clinically‐indicated versus routine change, Outcome 4 All‐cause blood stream infection.
Comparison 1 Clinically‐indicated versus routine change, Outcome 5 Cost.
Comparison 1 Clinically‐indicated versus routine change, Outcome 6 Infiltration.
Comparison 1 Clinically‐indicated versus routine change, Outcome 7 Catheter blockage.
Comparison 1 Clinically‐indicated versus routine change, Outcome 8 Local infection.
Comparison 1 Clinically‐indicated versus routine change, Outcome 9 Mortality.
| Clinically‐indicated versus routine changes for peripheral venous catheter‐related complications | ||||||
| Patient or population: patients with peripheral venous catheter‐related complications | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Clinically indicated versus routine changes | |||||
| Catheter‐related bloodstream infection | Study population | RR 0.61 | 4806 | ⊕⊕⊕⊖ | ||
| 1 per 1000 | 1 per 1000 | |||||
| Moderate | ||||||
| 0 per 1000 | 0 per 1000 | |||||
| Phlebitis | Study population | RR 1.14 | 4806 | ⊕⊕⊕⊕ | ||
| 68 per 1000 | 78 per 1000 | |||||
| Moderate | ||||||
| 68 per 1000 | 78 per 1000 | |||||
| All‐cause bloodstream infection | Study population | RR 0.47 | 3283 | ⊕⊕⊕⊕ | ||
| 5 per 1000 | 3 per 1000 | |||||
| Moderate | ||||||
| 5 per 1000 | 2 per 1000 | |||||
| Cost | The mean cost in the intervention groups was | 4244 | ⊕⊕⊕⊕ | |||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 Although patients and those recording outcomes were aware of group allocation, it seems unlikely that this knowledge would have affected results. None of those recording outcomes were investigators and the diagnosis was based on verifiable data in patients medical records. | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Catheter‐related blood stream infection Show forest plot | 5 | 4806 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.08, 4.68] |
| 2 Phlebitis Show forest plot | 5 | 4806 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.93, 1.39] |
| 2.1 Continuous infusion | 4 | 4606 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.11 [0.89, 1.39] |
| 2.2 Intermittent infusion | 1 | 200 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.29 [0.85, 1.96] |
| 3 Phlebitis per device days Show forest plot | 5 | 26191 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.84, 1.27] |
| 4 All‐cause blood stream infection Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 5 Cost Show forest plot | 3 | 4244 | Mean Difference (IV, Fixed, 95% CI) | ‐6.96 [‐9.05, ‐4.86] |
| 6 Infiltration Show forest plot | 4 | 4606 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.17 [1.05, 1.31] |
| 7 Catheter blockage Show forest plot | 5 | 4806 | Risk Ratio (M‐H, Random, 95% CI) | 1.25 [0.91, 1.71] |
| 8 Local infection Show forest plot | 4 | 4606 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.96 [0.24, 102.98] |
| 9 Mortality Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |