Metadona para el dolor por cáncer
References
References to studies included in this review
References to studies excluded from this review
Additional references
References to other published versions of this review
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Jump to:
| Methods | Randomised, double‐blind (double dummy), cross‐over study Single doses with assessment at 6 h | |
| Participants | Chronic pain due to cancer N = 43 started, 37 completed at least 1 series (M: 11, F: 26) Mean age 48 years (range 34‐59 years) | |
| Interventions | Morphine (IM or oral) or methadone (IM or oral) in a range of doses from 8 mg to 48 mg 4 doses for each series and 4 different series | |
| Outcomes | PI: categorical scale (5 points), measured over 6 h 50% pain relief Adverse events | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Stated to be randomised |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding of participants and personnel (performance bias) | Low risk | "in the oral‐parenteral study both capsules and an injection, one of which was a dummy, were administered" |
| Blinding of outcome assessment (detection bias) | Low risk | "in the oral‐parenteral study both capsules and an injection, one of which was a dummy, were administered" |
| Incomplete outcome data (attrition bias) | High risk | Only completed cross‐overs were analysed for efficacy |
| Selective reporting (reporting bias) | Unclear risk | Some participants contributed more than one set of data |
| Size | High risk | < 50 participants per treatment arm |
| Methods | Randomised, double‐blind, parallel‐group; duration 28 days | |
| Participants | Outpatients with cancer pain determined by a validated clinical assessment. Differentiated between neuropathic and non‐neuropathic pain N = 103 patients randomised (methadone 49, morphine 54), 66 completed (methadone 29, morphine 37) M: 37, F: 66 Age: methadone median age 59 years (range 26‐84 years); morphine median age 60 years (range 31‐87 years) | |
| Interventions | Oral methadone 7.5 mg twice daily with 5 mg 4‐hourly as needed. Oral morphine 15 mg twice daily with 5 mg 4‐hourly as needed | |
| Outcomes | Participant‐reported data, daily on days 1 to 8, then weekly thereafter: pain, sedation, confusion, nausea, constipation, recorded on 0‐10 NRS Adverse events | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "generated centrally by computer generated numbers stratified by center" |
| Allocation concealment (selection bias) | Low risk | Pharmacy at each centre advised of treatment assigned but the code was kept in a sealed envelope and not released to clinicians unless clinical emergency |
| Blinding of participants and personnel (performance bias) | Low risk | Stated to be double blind, "in identical capsules" |
| Blinding of outcome assessment (detection bias) | Low risk | Stated to be double blind, "in identical capsules" |
| Incomplete outcome data (attrition bias) | Low risk | Similar rates of withdrawals in both groups and for similar reasons. BOCF for dichotomised end points |
| Selective reporting (reporting bias) | Low risk | All intended outcomes reported upon |
| Size | High risk | 49 participants in one arm and 54 in the other |
| Methods | Prospective randomised parallel‐group study Participants treated until death | |
| Participants | Advanced cancer requiring strong opioids for pain management N = 40 M: 19, F: 21 Age: morphine mean age 65 years ± 2.7; methadone mean age 61 years ± 2.9 | |
| Interventions | Oral morphine modified‐release, titrated to need Oral methadone solution, titrated to need Other palliative care drugs allowed including non‐opioid analgesics. No anticancer therapy | |
| Outcomes | Pain intensity self report (when possible, otherwise doctor‐rated) Symptoms related to cancer or adverse events | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Stated to be 'randomised' |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding of participants and personnel (performance bias) | High risk | Commercially available products used |
| Blinding of outcome assessment (detection bias) | High risk | Commercially available products used |
| Incomplete outcome data (attrition bias) | Low risk | No problems identified |
| Selective reporting (reporting bias) | Unclear risk | Some pain measurements may have been physician‐ or carer‐assessed but not clearly specified |
| Size | High risk | 20 participants per treatment arm |
| Methods | Multicentre, randomised, open, parallel‐group study: duration 4 weeks Fixed starting dose of study medication, adjusted to balance analgesia and adverse effects Assessment at baseline and weekly intervals | |
| Participants | Adults with advanced cancer requiring strong opioids who had received opioids for mild to moderate pain, including tramadol and codeine at doses of at least 300 mg and 180 mg respectively, without adequate analgesia. Expected survival > 3 months Breast cancer was the most frequent diagnosis (16 participants), and mixed nociceptive‐neuropathic syndromes (18 participants) the most dominant pain type N = 108 (70 completed) M: 36, F: 34 (completers) Mean age 59 years (range 18‐78) (completers) | |
| Interventions | Oral methadone, 15 mg/d in 3 divided doses, n = 36 Modified‐release oral morphine, initially 60 mg/d, n = 36 Transdermal fentanyl patch, initially 0.6 mg/d (25 μg/h), n = 36 Rescue medication: oral morphine at 1/6 24‐h oral equivalent requirement | |
| Outcomes | Symptoms associated with opioid therapy (e.g. nausea, drowsiness, confusion): 4‐point scale (not at all, slight, a lot, severe) Constipation: 4‐point scale (0 = 1 passage every 1‐2 days, 1 = one passage every 3‐4 days, 2 = one passage > 4 days, 3 = rectal measures) Distress score calculated from sum of symptom intensities PI: NRS (0‐10) Time to achieve dose stabilisation Number of daily dose changes Opioid escalation index QoL using Spitzer QoL index (activity, daily life, health perceptions, social support, Behaviour rated on Likert 3‐point scale (0‐2) Cost | |
| Notes | Other medication for 'symptoms' were allowed during the study, which included anti‐inflammatories, antidepressants and anticonvulsants, which may have an impact on pain; these were either continued or introduced as needed during the study | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "computer‐generated" |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) | High risk | Not blinded; used "commercially available" products |
| Blinding of outcome assessment (detection bias) | High risk | Not blinded; used "commercially available" products |
| Incomplete outcome data (attrition bias) | High risk | Efficacy data (group means) for participants remaining in study (completers). States numbers of dropouts equally distributed between groups |
| Selective reporting (reporting bias) | Low risk | No problems identified |
| Size | High risk | 36 per treatment arm |
| Methods | Randomised, double‐blind, parallel‐group: duration 4 weeks approximately | |
| Participants | Cancer pain; participants with terminal cancer with severe pain Median age 63 years | |
| Interventions | Diamorphine elixir with cocaine 10 mg, n = 26 Oral methadone, n = 20 Dose titrated to pain relief | |
| Outcomes | VAS for pain, nausea and mood, assessed twice daily | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly allocated"; method not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) | Low risk | "drugs were dispensed in undistinguishable solutions" |
| Blinding of outcome assessment (detection bias) | Low risk | "drugs were dispensed in undistinguishable solutions" |
| Incomplete outcome data (attrition bias) | Low risk | All participants accounted for |
| Selective reporting (reporting bias) | Low risk | No problems identified |
| Size | High risk | < 50 participants per treatment arm (20 and 26) |
| Methods | Randomised, parallel‐group: duration 14 days | |
| Participants | Advanced cancer requiring strong opioids for "excruciating pain" N = 66 (randomised), 54 (completed) M: 31, F: 23 | |
| Interventions | Oral methadone 1 mg/ml, dose 8‐28 mg daily, given as divided dose every 6 h for 3 d, then every 8 h, n = 27 Oral morphine 4 mg/ml dose 4‐24 mg every 4 h, n = 27 All participants received diclofenac 150 mg daily and haloperidol 20 mg daily by injection | |
| Outcomes | PI: 5‐point categorical scale (converted to integrated pain score, which took into account duration) Achieved no worse than mild pain (VAS ≤ 30/100) Adverse events Withdrawals | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Stated to be "randomised", method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) | High risk | Not described. Presumed open‐label, since different dosing regimens |
| Blinding of outcome assessment (detection bias) | High risk | Not described. Presumed open‐label, since different dosing regimens |
| Incomplete outcome data (attrition bias) | High risk | Completer analysis |
| Selective reporting (reporting bias) | Low risk | No problems identified |
| Size | High risk | < 50 participants per treatment arm |
BOCF: baseline observation carried forward; F: female; h: hours; IM: intramuscular; M: male; mg: milligrams; N: number of participants in study; n: number of participants in treatment arm; NRS: Numerical Rating Scale; PI: pain intensity; QoL: quality of life; VAS: Visual Analogue Scale; VRS: Verbal Rating Scale
Characteristics of excluded studies [ordered by study ID]
Jump to:
| Study | Reason for exclusion |
| Study of methadone in combination with acetaminophen (paracetamol) | |
| 28 participants across 4 groups. Likely to be fewer than 10 participants per treatment group | |
| Fewer than 10 participants per treatment group | |
| Fewer than 10 participants per treatment group | |
| Study of methadone in combination with other agents | |
| Not specifically cancer pain ‐ only 15 out of 90 participants reported cancer‐related pain | |
| Study of switching methods using methadone | |
| Double‐blind randomised controlled cross‐over trial of methadone for neuropathic pain. Excluded cancer pain | |
| Only 1 participant recruited | |
| Only 1 participant recruited | |
| Not a study of methadone |
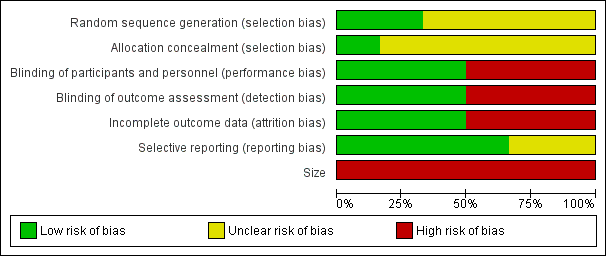
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
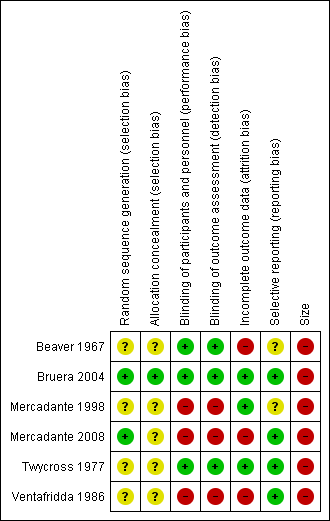
Risk of bias summary: review authors' judgements about each risk of bias item for each included study
| Methadone compared to morphine for cancer pain | ||||||
| Patient or population: people with cancer pain | ||||||
| Outcomes | Assumed risk | Corresponding risk | Relative effect | No of participants | Quality of the evidence | Comments |
| Morphine | Methadone | |||||
| Participant‐reported pain intensity | Pain intensity scores: One study (103 participants) reported > 20% improvement in pain scores for 76% of morphine and 75% methadone participants in those that completed No worse than mild pain (pain score of 3/10 or less after treatment): One study (54 participants) reported all achieved no worse than mild pain based on mean pain scores. Two studies (148 participants) reported mean pain scores very close to a score of 3 | ⊕⊕⊝⊝ | Downgraded two points for reasons stated | |||
| Adverse events: appetite, thirst, somnolence | Not estimable | Not estimable | Not estimable | 342 | ⊕⊝⊝⊝ | Downgraded three points for reasons stated |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of effect, but there is a possibility that it is substantially different Low quality: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect Very low quality: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect | ||||||
| 1 Risk of bias: random allocation and allocation concealment unclear, all had sample size of less than 200 per treatment arm. | ||||||