Cirugía de fundoplicatura laparoscópica versus tratamiento médico para la enfermedad por reflujo gastroesofágico (ERGE) en adultos
Resumen
Antecedentes
La enfermedad por reflujo gastroesofágico (ERGE) es un trastorno frecuente que se observa en el 3% al 33% de las personas de diferentes partes del mundo. Existen dudas considerables acerca de si los pacientes con ERGE deben ser sometidos a cirugía o recibir tratamiento médico para controlar el trastorno.
Objetivos
Evaluar los efectos beneficiosos y perjudiciales de la fundoplicatura laparoscópica versus tratamiento médico para los pacientes con enfermedad por reflujo gastroesofágico.
Métodos de búsqueda
Se realizaron búsquedas en el Registro de Ensayos del Grupo Cochrane de Enfermedades Esofago‐gástricas, del Intestino Delgado y Pancreáticas (Cochrane Upper Gastrointestinal and Pancreatic Diseases Group, UGPD) (junio de 2015), Registro Cochrane Central de Ensayos Controlados (Cochrane Central Register of Controlled Trial, CENTRAL) (Cochrane Library número 6, 2015), Ovid MEDLINE (de 1966 a junio de 2015) y EMBASE (de 1980 a junio de 2015) para identificar ensayos controlados. También se revisaron las referencias de los ensayos incluidos para identificar ensayos adicionales.
Criterios de selección
Para su inclusión en la revisión se consideraron solamente los ensayos controlados aleatorios (ECA) que compararon la fundoplicatura laparoscópica con el tratamiento médico en pacientes con ERGE independientemente del idioma, el cegamiento o el estado de publicación.
Obtención y análisis de los datos
Dos autores de la revisión de forma independiente identificaron los ensayos y extrajeron los datos. Se calculó el cociente de riesgos (CR) o diferencia de medias estandarizada (DME) con los intervalos de confianza (IC) del 95%, y se utilizaron los modelos de efectos fijos y efectos aleatorios en RevMan 5, según el análisis de casos disponibles.
Resultados principales
Cuatro estudios cumplieron los criterios de inclusión para la revisión y proporcionaron información sobre uno o más resultados de la revisión. En los cuatro ECA se asignaron al azar 1160 participantes a fundoplicatura laparoscópica (589 participantes) o a tratamiento médico con inhibidores de la bomba de protones (571 participantes). Todos los ensayos incluyeron participantes que habían presentado síntomas de reflujo durante al menos seis meses y habían recibido tratamiento supresor de ácidos a largo plazo. Todos los ensayos incluyeron solamente participantes que podían ser sometidos a cirugía si eran asignados al azar al brazo de cirugía. Todos los ensayos presentaron un alto riesgo de sesgo. La calidad general de las pruebas fue baja o muy baja. Ninguno de los ensayos informó la calidad de vida relacionada con la salud (CdVRS) a largo plazo ni la calidad de vida (CdV) específica de la ERGE.
La diferencia entre la fundoplicatura laparoscópica y el tratamiento médico fue imprecisa para la CdVRS general a corto plazo (DME 0,14; IC del 95%: ‐0,02 a 0,30; participantes = 605; estudios = 3), la CdVRS a plazo medio (DME 0,03; IC del 95%: ‐0,19 a 0,24; participantes = 323; estudios = 2), la CdV específica de la ERGE a plazo medio (DME 0,28; IC del 95%: ‐0,27 a 0,84; participantes = 994; estudios = 3), la proporción de pacientes con eventos adversos (cirugía: 7/43 [porcentaje ajustado = 14,0%]; médico: 0/40 [0,0%]; CR 13,98; IC del 95%: 0,82 a 237,07; participantes = 83; estudios = 1), la disfagia a largo plazo (cirugía: 27/118 [porcentaje ajustado = 22,9%]; médico: 28/110 [25,5%]; CR 0,90; IC del 95%: 0,57 a 1,42; participantes = 228; estudios = 1) y los síntomas de reflujo a largo plazo (cirugía: 29/118 [porcentaje ajustado = 24,6%]; médico: 41/115 [35,7%]; CR 0,69; IC del 95%: 0,46 a 1,03; participantes = 233; estudios = 1).
La CdV específica de la ERGE a corto plazo fue mejor en el grupo de fundoplicatura laparoscópica que en el grupo de tratamiento médico (DME 0,58; IC del 95%: 0,46 a 0,70; participantes = 1160; estudios = 4).
La proporción de pacientes con eventos adversos graves (cirugía: 60/331 [porcentaje ajustado = 18,1%]; médico: 38/306 [12,4%]; CR 1,46; IC del 95%: 1,01 a 2,11; participantes = 637; estudios = 2), disfagia a corto plazo (cirugía: 44/331 [porcentaje ajustado = 12,9%]; médico: 11/306 [3,6%]; CR 3,58; IC del 95%: 1,91 a 6,71; participantes = 637; estudios = 2) y disfagia a plazo medio (cirugía: 29/288 [porcentaje ajustado = 10,2%]; médico: 5/266 (1,9%); CR 5,36; IC del 95%: 2,1 a 13,64; participantes = 554; estudios = 1) fue mayor en el grupo de fundoplicatura laparoscópica que en el grupo de tratamiento médico.
La proporción de pacientes con pirosis a corto plazo (cirugía: 29/288 [porcentaje ajustado = 10,0%]; médico: 59/266 [22,2%]; CR 0,45, IC del 95%: 0,30 a 0,69; participantes = 554; estudios = 1), a plazo medio (cirugía: 12/288 [porcentaje ajustado = 4,2%]; médico: 59/266 [22,2%]; CR 0,19; IC del 95%: 0,10 a 0,34; participantes = 554; estudios = 1), a largo plazo (cirugía: 46/111 [porcentaje ajustado = 41,2%]; médico: 78/106 [73,6%]; CR 0,56; IC del 95%: 0,44 a 0,72); participantes = 217; estudios = 1) y de pacientes con síntomas de reflujo a corto plazo (cirugía: 6/288 [porcentaje ajustado = 2,0%]; médico: 53/266 [19,9%]; CR 0,10; IC del 95%: 0,05 a 0,24; participantes = 554; estudios = 1) y a plazo medio (cirugía: 6/288 [porcentaje ajustado = 2,1%]; médico: 37/266 [13,9%]; CR 0,15; IC del 95%: 0,06 a 0,35; participantes = 554; estudios = 1) fue menor en el grupo de fundoplicatura laparoscópica que en el grupo de tratamiento médico.
Conclusiones de los autores
Existen dudas considerables en cuanto al equilibrio entre los efectos beneficiosos versus perjudiciales de la fundoplicatura laparoscópica en comparación con el tratamiento médico a largo plazo con inhibidores de la bomba de protones. Se deben realizar ECA adicionales de fundoplicatura laparoscópica versus tratamiento médico en pacientes con ERGE en los que se realice el cegamiento del evaluador de resultados y que incluyan a todos los participantes en el análisis. Dichos ensayos deben incluir resultados a largo plazo orientados a los pacientes como los eventos adversos relacionados con el tratamiento (incluida la gravedad) y la calidad de vida, así como informar sobre el impacto social y económico de los eventos adversos y los síntomas.
PICOs
Resumen en términos sencillos
Cirugía mínimamente invasiva versus tratamiento médico para adultos con pirosis o regurgitación ácida
Pregunta de la revisión
¿La fundoplicatura laparoscópica (cirugía mínimamente invasiva en la que se envuelve la parte superior del estómago alrededor de la parte inferior del esófago para formar una válvula nueva) es beneficiosa o perjudicial en comparación con el tratamiento médico en adultos con pirosis o regurgitación ácida (enfermedad por reflujo gastroesofágico [ERGE])?
Antecedentes
Las enfermedad por reflujo gastroesofágico o ERGE es un trastorno que se presenta cuando los contenidos del estómago regurgitan hacia el esófago, lo que causa síntomas molestos como pirosis (sensación de ardor en la parte inferior del esternón) o regurgitación (percepción de flujo del contenido del estómago en la garganta o la boca). Las complicaciones a largo plazo de la ERGE incluyen esofagitis por reflujo (lesión en el recubrimiento del esófago), hemorragia del esófago, estrechamiento del esófago y cambio en la naturaleza del recubrimiento del esófago que a veces puede dar lugar a cáncer de esófago. Aproximadamente del 3% al 33% de las personas en todo el mundo presentan ERGE. Los factores de riesgo de ERGE incluyen antecedentes familiares de enfermedad de reflujo en los familiares inmediatos, el embarazo, la edad avanzada, la obesidad, el hábito de fumar y el consumo excesivo de alcohol. Además de los cambios en el estilo de vida (como el abandono del hábito de fumar) y los cambios en la dieta (evitar alimentos que causan pirosis), las formas principales de tratamiento para la ERGE son médicas y quirúrgicas. El tratamiento médico generalmente tiene como finalidad la reducción de la acidez en el estómago. Actualmente un grupo de fármacos que suprimen la secreción de ácidos, denominados inhibidores de la bomba de protones, se consideran lo mejor para disminuir la secreción de ácidos. El principal tratamiento quirúrgico es la fundoplicatura, que incluye la envoltura de la parte inferior del esófago con el estómago. Este procedimiento puede ser realizado con cirugía tradicional abierta, cirugía mínimamente invasiva o cirugía realizada sin hacer ningún corte desde el interior del estómago con la ayuda de un endoscopio (en este contexto, se introduce un tubo flexible a través de la boca para obtener una visión del esófago y el estómago). No se conocen los efectos beneficiosos y perjudiciales de la fundoplicatura laparoscópica en comparación con el tratamiento médico en los pacientes con ERGE. Se intentó resolver este problema mediante la búsqueda de los estudios existentes sobre el tema. Se incluyeron todos los estudios cuyos resultados se presentaron hasta el 1 de octubre de 2014.
Características de los estudios
Cuatro estudios cumplieron los criterios de inclusión para la revisión y proporcionaron información. Un total de 1160 participantes fueron sometidos a fundoplicatura laparoscópica (589 participantes) o recibieron tratamiento médico (571 participantes). La decisión sobre si un participante recibía cirugía o tratamiento médico se realizó mediante el uso de métodos similares a lanzar una moneda, lo que aseguró que los participantes de los dos grupos fueran similares. Todos los ensayos incluyeron a pacientes que habían presentado síntomas de reflujo durante al menos seis meses, habían recibido tratamiento supresor de ácidos a largo plazo y podían ser sometidos a la fundoplicatura laparoscópica si fuera necesario.
Resultados clave
Ninguno de los ensayos informó la calidad de vida relacionada con la salud (CdVRS) a largo plazo ni la calidad de vida (CdV) específica de la ERGE. La diferencia entre la fundoplicatura laparoscópica y el tratamiento médico fue imprecisa para la CdVRS general a corto plazo, la CdVRS a plazo medio, la CdV específica de la ERGE a plazo medio, el porcentaje de pacientes con eventos adversos, la disfagia a largo plazo (dificultad para tragar) y la regurgitación ácida a largo plazo. La calidad de vida específica de la ERGE a corto plazo fue mejor en el grupo de fundoplicatura laparoscópica que en el grupo de tratamiento médico. Sin embargo, no estuvo claro en qué medida esta mejoría benefició al paciente. La proporción de pacientes con eventos adversos graves, disfagia a corto plazo y disfagia a plazo medio fue mayor en el grupo de fundoplicatura laparoscópica que en el grupo de tratamiento médico. La proporción de pacientes con pirosis a corto plazo, a plazo medio y a largo plazo y de pacientes que presentaron regurgitación ácida a corto plazo y a plazo medio fue menor en el grupo de fundoplicatura laparoscópica que en el grupo de tratamiento médico. No se informó la gravedad de la dificultad para tragar, la pirosis, ni la regurgitación ácida. Existen dudas considerables en cuanto al equilibrio entre los efectos beneficiosos versus perjudiciales de la fundoplicatura laparoscópica en comparación con el tratamiento médico a largo plazo con inhibidores de la bomba de protones. Debido a la calidad deficiente de los ensayos, se necesitan estudios futuros de alta calidad en esta área.
Calidad de la evidencia
La calidad de las pruebas fue baja o muy baja. Como resultado, hay mucha incertidumbre con respecto a los resultados.
Authors' conclusions
Summary of findings
| Laparoscopic fundoplication versus medical management for gastro‐oesophageal reflux disease (GORD) in adults | ||||||
| Patient or population: Patients with gastro‐oesophageal reflux disease (GORD) in adults Control: Medical management | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Medical management | Laparoscopic fundoplication | |||||
| Health‐related quality of life | ||||||
| (< 1 year) | The mean health‐related quality of life (< 1 year) in the intervention groups was | 605 | ⊕⊝⊝⊝ | SMD 0.14 (‐0.02 to 0.3) | ||
| (1 to 5 years) | The mean health‐related quality of life (1 to 5 years) in the intervention groups was | 323 | ⊕⊝⊝⊝ | SMD 0.03 (‐0.19 to 0.24) | ||
| GORD‐specific quality of life | ||||||
| (< 1 year) | The mean GORD‐specific quality of life (< 1 year) in the intervention groups was | 1160 | ⊕⊕⊝⊝ | SMD 0.58 (0.46 to 0.7) | ||
| (1 to 5 years) | The mean GORD‐specific quality of life (1 to 5 years) in the intervention groups was | 994 | ⊕⊝⊝⊝ | SMD 0.28 (‐0.27 to 0.84) | ||
| Adverse events | ||||||
| Serious adverse events | 124 per 1000 | 181 per 1000 | RR 1.46 | 637 | ⊕⊝⊝⊝ | |
| Adverse events | 10 per 1000 | 140 per 1000 | RR 13.98 | 83 | ⊕⊝⊝⊝ | |
| Dysphagia | ||||||
| (< 1 year) | 36 per 1000 | 129 per 1000 | RR 3.58 | 637 | ⊕⊝⊝⊝ | |
| (1 to 5 years) | 19 per 1000 | 101 per 1000 | RR 5.36 | 554 | ⊕⊝⊝⊝ | |
| (5 years or more) | 255 per 1000 | 229 per 1000 | RR 0.9 | 228 | ⊕⊝⊝⊝ | |
| Heartburn | ||||||
| (< 1 year) | 222 per 1000 | 100 per 1000 | RR 0.45 | 554 | ⊕⊝⊝⊝ | |
| (1 to 5 years) | 222 per 1000 | 42 per 1000 | RR 0.19 | 554 | ⊕⊝⊝⊝ | |
| (5 years or more) | 736 per 1000 | 412 per 1000 | RR 0.56 | 217 | ⊕⊝⊝⊝ | |
| Reflux | ||||||
| (< 1 year) | 199 per 1000 | 20 per 1000 | RR 0.1 | 554 | ⊕⊝⊝⊝ | |
| (1 to 5 years) | 139 per 1000 | 21 per 1000 | RR 0.15 | 554 | ⊕⊝⊝⊝ | |
| (5 years or more) | 357 per 1000 | 246 per 1000 | RR 0.69 | 233 | ⊕⊝⊝⊝ | |
| Long‐term overall health‐related quality of life and long‐term GORD‐specific quality of life were not reported in any of the trials. | ||||||
| *The basis for the assumed risk was the mean control group risk across studies for all outcomes other than adverse events. For control group risk, 1% was used as the control group risk since there were no adverse events in the control group in the only trial that reported this outcome (Anvari 2011). The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 The trial(s) was/were at high risk of bias. | ||||||
Background
Description of the condition
Gastro‐oesophageal reflux disease or GORD (GERD in North America, as oesophagus is spelt 'esophagus') is a condition which develops when the reflux of stomach contents causes troublesome symptoms or complications or both (Vakil 2006). The symptoms related to GORD are retrosternal burning sensation (heartburn) and regurgitation (perception of flow of refluxed gastric content into the mouth or laryngopharynx) (Vakil 2006). Patients have to determine whether the symptoms are troublesome (Vakil 2006). In general, mild symptoms occurring on two or more days in a week and moderate or severe symptoms occurring on one or more days in a week are considered troublesome by patients (Vakil 2006). The complications include reflux oesophagitis (oesophageal mucosal injury), upper gastrointestinal bleeding, reflux stricture (persistent narrowing of the oesophagus), and Barrett's oesophagus (replacement of the normal stratified squamous epithelium lining of the lower end of oesophagus with simple columnar epithelial lining which is similar to the lining of the stomach) (Vakil 2006), which in turn is a risk factor for oesophageal cancer (Solaymani‐Dodaran 2004). Other researchers have hypothesised that there is a direct link between symptomatic GORD and oesophageal cancer based on their observation of increased oesophageal cancer irrespective of the presence of Barrett's oesophagus (Cook 2014; Lagergren 1999). While there has been significant controversy over the definition of GORD, the international consensus definition of GORD includes asymptomatic patients with complications, does not stipulate the method of diagnosis, and includes reflux which may be weakly acidic or gaseous (Vakil 2006).
There is global variation in the prevalence of GORD. The prevalence is higher in Europe, North and South America, and the Middle East, with a prevalence ranging between 9% and 33% of adults compared to a prevalence ranging between 3% and 8% in East Asia (Dent 2005; El‐Serag 2014). The incidence of GORD is available from the UK and the USA and is about five cases of GORD per 1000 person‐years (Dent 2005; El‐Serag 2014). The risk factors for GORD include genetic factors such as a family history of reflux disease in immediate relatives; demographic factors such as pregnancy, older age and obesity; behavioural factors such as cigarette smoking, excessive alcohol consumption, drug treatments such as non‐steroidal anti‐inflammatory drugs (NSAIDs), oral steroids; and co‐morbidities such as abdominal pain, irritable bowel syndrome, gallstone disease, asthma, chronic obstructive pulmonary disease, chest pain, and angina. Coffee consumption, oral contraceptive consumption, and hormonal replacement therapy are associated with lower prevalence of GORD (Dent 2005). It should be noted that these are associations and no causal association can be shown for many of these factors.
Gastric contents are prevented from entering into the oesophagus by the lower oesophageal sphincter (LOS). However, LOS relaxes transiently resulting in the reflux of gastric contents into the oesophagus, even in normal individuals (Boeckxstaens 2014b). However, increased reflux of gastric contents into the oesophagus and prolonged exposure of the lower oesophagus to gastric contents are believed to contribute to the symptoms and complications of GORD (Boeckxstaens 2014b). Hiatus hernia lowers the competence and pressure of the LOS, reduces the length of the gastro‐oesophageal junction, and alters the opening characteristics of the gastro‐oesophageal junction. This results in an increase in the exposure of the oesophagus to acid (Boeckxstaens 2014b; Gordon 2004). Hiatus hernia is associated with severe GORD symptoms and complications (Boeckxstaens 2014b; Gordon 2004; Vakil 2006).
Based on the international consensus conference definition, GORD may be diagnosed based on typical symptoms alone (heartburn and regurgitation) without any additional diagnostic tests (Vakil 2006). Diagnostic tests that may be performed to confirm the diagnosis include pH testing, impedence monitoring, upper gastrointestinal endoscopy with or without histological examination, or electron microscopy to confirm the presence of one or more of the complications such as reflux oesophagitis, Barrett's oesophagus, and oesophageal cancer (Vakil 2006). Although a number of classification systems based on endoscopic findings are still commonly used (Dent 2008), the international consensus conference classifies GORD into oesophageal syndrome (presence of heartburn, regurgitation, upper abdominal pain, chest pain, which may be sometimes be similar to that of anginal chest pain, reflux oesophagitis, upper gastrointestinal bleeding, stricture, Barrett’s oesophagus, and oesophageal cancer) and extraoesophageal syndromes (chronic cough, chronic laryngitis, asthma, and dental erosions).
Description of the intervention
Apart from lifestyle and diet modifications, the major forms of treatment for GORD are surgical and medical treatments (Boeckxstaens 2014a).
Surgical treatment for GORD is in the form of fundoplication. There are various modifications to original complete fundoplication suggested by Nissen, mainly with regards to the amount and area of the gastric fundus which is plicated and where the wrap is fixed (Watson 1998). Fundoplication can be performed by open or laparoscopic surgery (Watson 1998). Recently endoscopic endoluminal fundoplication, which involves fundoplication without any incision, has been proposed (Zacherl 2014). The complications related to fundoplication include injury to nearby structures such as the liver, spleen, or oesophagus; dysphagia (troublesome difficulty in swallowing) (5%); wrap migration (1%); recurrent regurgitation (1%); recurrent heartburn (1% to 10%); and chest complications (3%) (Singhal 2009; Wileman 2010). Overall, 1% to 14% of patients undergoing fundoplication develop complications (Wileman 2010).
The medical treatment is usually aimed at decreasing acidity in the stomach (which may be in the form of proton pump inhibitors, H2 (histamine H2 receptor) blockers or H2 receptor antagonists, antacids, prokinetic drugs) and surgical treatment (usually in the form of fundoplication, which can be performed by open surgery, laparoscopic surgery, or by endoscopic endoluminal fundoplication) (Boeckxstaens 2014a; Lundell 2001; Moayyedi 2008; Van Meer 2013; Wileman 2010; Zacherl 2014).
For GORD, the medical treatment is usually given orally. Proton pump inhibitors are currently considered the main treatment of GORD (Katz 2010a). Various proton pump inhibitors include omeprazole, lansoprazole, pantoprazole, rabeprazole, and esomeprazole (Katz 2010a). Proton pump inhibitors are generally well tolerated, and adverse effects are relatively infrequent. The adverse effects reported most often with proton pump inhibitors are headache, gastrointestinal disturbances, and rash. Occasionally severe allergic reactions, anaphylactic reactions, muscle weakness, reversible confusional states, mental disturbances, liver failure, kidney damage, and angina have been reported (Martindale 2011).
The proton pump inhibitors may be supplemented with H2 blockers such as ranitidine, antacids such as magnesium hydroxide, and prokinetic agents such as metoclopramide or domperidone (Achem 1998; Boeckxstaens 2014a). Adverse reactions to H2 blockers are generally infrequent. The most common adverse effects reported are diarrhoea and other gastrointestinal disturbances, dizziness, tiredness, headache, muscle and joint pain, and rash (Martindale 2011). The antacids are generally safe. Adverse effects depend upon the antacid taken and the additional ingredients that the antacid preparation contains. The reported adverse effects include constipation, diarrhoea, and flatulence (Martindale 2011). Adverse effects related to prokinetic agents include extrapyramidal symptoms (usually acute dystonic reactions). Parkinsonism and tardive dyskinesia have occasionally been reported, usually during prolonged treatment in elderly patients. Metoclopramide may also cause galactorrhoea or related disorders (Martindale 2011).
How the intervention might work
Fundoplication compresses the lower oesophagus, increasing the LOS pressure and decreasing the intermittent relaxations of the LOS (Watson 1998). This decreases the amount of gastric acid which reaches the oesophagus. Medical treatments such as proton pump inhibitors and H2 (histamine H2 receptor) blockers work by decreasing the acid secretion (Achem 1998; Katz 2010a). Antacids neutralise the gastric acid (Achem 1998). Prokinetics improve the gastric motility and hence acid clearance by the oesophagus (Achem 1998).
Why it is important to do this review
GORD is the most common gastrointestinal diagnosis in outpatient clinical visits in the USA resulting in more than nine million outpatient visits annually (Peery 2012). The estimated direct and indirect costs of treatment and lost productivity due to GORD is USD 10 billion annually in US, EUR 9.3 billion annually in Germany, EUR 2.9 billion annually in Italy, and EUR 1.9 billion annually in Spain (Darba 2011; Sandler 2002). There is currently no consensus in the treatment of GORD. The previous Cochrane Review on Medical versus surgical management for gastro‐oesophageal reflux disease (GORD) in adults included medical management versus laparoscopic fundoplication surgery and concluded that laparoscopic fundoplication surgery is more effective than medical management for the treatment of GORD in the short term to medium term (Wileman 2010). This review is an update of the above review with revised methodology that reflects the current Cochrane methodology (Higgins 2011a). This review will provide the best level of evidence on the comparative benefits and harms of laparoscopic versus medical management for GORD, and so allow patients and the healthcare providers involved in their care to make informed decisions.
Objectives
To assess the benefits and harms of laparoscopic fundoplication versus medical treatment for people with gastro‐oesophageal reflux disease.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs). We included studies reported as full text, those published as abstract only, and unpublished data. We excluded quasi‐randomised studies and observational studies because of the high risk of bias in such study designs.
Types of participants
We included adults (> 16 years of age) with GORD irrespective of the presence of symptoms, complications, or hiatus hernia and judged to be suitable for either surgical or medical management. We excluded patients who have symptomatic oesophageal stricture due to GORD or those who have oesophageal dysplasia or cancer.
Types of interventions
We included trials comparing laparoscopic fundoplication versus medical treatment for gastro‐oesophageal disease irrespective of the nature of the laparoscopic fundoplication or medical treatment. We excluded trials in which the comparisons solely involve comparison of different forms of medical treatment or different forms of laparoscopic fundoplications. We accepted co‐interventions, for example, the use of lifestyle modification advice, provided that they were used equally in both the groups.
Types of outcome measures
Primary outcomes
-
Health‐related quality of life (HRQoL) (using any validated scale).
-
Short‐term (four weeks to 12 months).
-
Medium‐term (one year to five years).
-
Long‐term (five years or more).
-
-
GORD‐specific quality of life (QoL)
-
Short‐term (four weeks to 12 months).
-
Medium‐term (one year to five years).
-
Long‐term (five years or more).
-
-
Serious adverse events (within three months of cessation of treatment ‐ for surgery this period refers to three months after index surgery). We will accept the following definitions of serious adverse events.
-
ICH‐GCP International Conference on Harmonisation ‐ Good Clinical Practice guideline (ICH‐GCP 1996): serious adverse events defined as any untoward medical occurrence that results in death, is life‐threatening, requires inpatient hospitalisation or prolongation of existing hospitalisation, results in persistent or significant disability/incapacity.
-
Other variations of ICH‐GCP classifications such as Food and Drug Administration (FDA) classification (FDA 2006), Medicines and Healthcare products Regulatory Agency (MHRA) classification (MHRA 2013).
-
Secondary outcomes
-
Adverse events (within three months of cessation of treatment ‐ for surgery this period refers to three months after index surgery). We will accept all adverse events reported by the study author irrespective of the severity of the adverse event.
-
Dysphagia.
-
Short‐term (four weeks to 12 months).
-
Medium‐term (one year to five years).
-
Long‐term (five years or more).
-
-
Heartburn.
-
Short‐term (four weeks to 12 months).
-
Medium‐term (one year to five years).
-
Long‐term (five years or more).
-
-
Reflux.
-
Short‐term (four weeks to 12 months).
-
Medium‐term (one year to five years).
-
Long‐term (five years or more).
-
The choice of the above clinical outcomes was to assess the comparative safety and clinical improvement, in terms of reduced symptoms and complications, resulting in an improvement in the health‐related quality of life between surgical and medical treatment in patients with GORD.
Reporting of the outcomes listed here were not an inclusion criteria for the review.
Search methods for identification of studies
Electronic searches
We conducted a literature search to identify all published and unpublished randomised controlled trials (RCTs). The literature search identified potential studies in all languages. We planned to translate the non‐English language papers and fully assess them for potential inclusion in the review as necessary.
We searched the following electronic databases (via the OVID platform) to identify potential studies:
-
Cochrane Central Register of Controlled Trials (CENTRAL), (The Cochrane Library Issue 6, 2015 (Appendix 1);
-
Cochrane Upper Gastrointestinal and Pancreatic Diseases Group (UGPD) Trials Register (June 2015);
-
Ovid MEDLINE (1966 to June 2015) (Appendix 2); and
-
EMBASE (1980 to June 2015) (Appendix 3).
Details of the previous search strategies are provided in Appendix 4
Searching other resources
We checked reference lists of all primary studies and review articles for additional references. We contacted authors of identified trials and asked them to identify other published and unpublished studies.
We searched for errata or retractions from eligible trials on http://www.ncbi.nlm.nih.gov/pubmed and report the date this was done within the review.
Data collection and analysis
Selection of studies
Two review authors (SG and KG) independently screened titles and abstracts of all the potential studies we identified as a result of the search and coded them as 'retrieve' (eligible or potentially eligible/unclear) or 'do not retrieve'. We retrieved the full‐text study reports and two review authors (SG and KG) independently screened the full text and identified studies for inclusion. We identified and recorded reasons for exclusion of the ineligible studies. We resolved any disagreement through discussion. We identified and excluded duplicates and collated multiple reports of the same study so that each study rather than each report was the unit of interest in the review. We recorded the selection process in sufficient detail to complete a PRISMA flow diagram and characteristics of excluded studies table.
Data extraction and management
We used a standard data collection form for study characteristics and outcome data which has been piloted on at least one study in the review. Two review authors (SG and KG) extracted the following study characteristics from the included studies.
-
Methods: study design, total duration of the study and run in, number of study centres and location, study setting, withdrawals, date of study.
-
Participants: number (n), mean age, age range, gender, hiatal hernia status, Barrett's oesophagus status, body mass index, inclusion criteria, exclusion criteria.
-
Interventions: intervention, comparison, concomitant interventions.
-
Outcomes: primary and secondary outcomes specified and collected, time points reported.
-
Notes: funding for trial, notable conflicts of interest of trial authors.
Two review authors (SG and KG) independently extracted outcome data from the included studies. If outcomes were reported multiple times for the same time point, for example, short‐term health‐related quality of life was reported at three months and 12 months, the later time point (i.e. 12 months) was chosen for data extraction. For time‐to‐event outcomes, we planned to extract data to calculate the natural logarithm of the hazard ratio and its standard error using the methods suggested by Parmar et al (Parmar 1998).
We included all randomised participants for medium outcomes (for example, dysphagia) and this was not conditional upon the short‐term outcomes (for example, having or not having a dysphagia at 12 months).
We planned to note in the characteristics of included studies table if outcome data were reported in an unusable way. We resolved disagreements by consensus. One review author (KG) copied across the data from the data collection form into the Review Manager file (Review Manager 2014). We double checked that the data were entered correctly by comparing the study reports with how the data are presented in the systematic review.
Assessment of risk of bias in included studies
Two review authors (SG and KG) independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011b). Any disagreement was resolved by discussion. We assessed the risk of bias according to the following domains;
-
random sequence generation;
-
allocation concealment;
-
blinding of participants and personnel;
-
blinding of outcome assessment;
-
incomplete outcome data;
-
selective outcome reporting;
-
other bias.
We graded each potential source of bias as high, low or unclear and provide a quote from the study report together with a justification for our judgment in the risk of bias table. We have summarised the risk of bias judgements across different studies for each of the domains listed. Where information on risk of bias relates to unpublished data or correspondence with a trialist, we have noted this in the risk of bias table.
When considering treatment effects, we have taken into account the risk of bias for the studies that contributed to that outcome.
Assesment of bias in conducting the systematic review
We have conducted the review according to the current guidelines of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011a). We have reported any deviations from the previous review in the 'Differences between current review and previous review' section of the systematic review.
Measures of treatment effect
We have analysed dichotomous data as risk ratio (RR) and continuous data as standardised mean difference (SMD) since different scales were used for measuring the quality of life. We have ensured that higher scores for continuous outcomes have the same meaning for the particular outcome, explained the direction to the reader and reported where the directions were reversed if this was necessary. We have calculated the rate ratio for outcomes such as adverse events and serious adverse events, where it is possible for the same person to develop more than one adverse event (or serious adverse event). If the authors had calculated the rate ratio of adverse events (or serious adverse events) in the intervention versus control based on Poisson regression, we planned to obtain the rate ratio by the Poisson regression method in preference to rate ratio calculated based on the number of adverse events (or serious adverse events) during a certain period. We planned to calculate the hazard ratio (HR) for time‐to‐event outcomes such as time‐to‐first adverse event (or serious adverse event).
We have undertaken meta‐analyses if this was meaningful, that is if the treatments, participants and the underlying clinical question were similar enough for pooling to make sense.
A common way that trialists indicate when they have skewed data is by reporting medians and interquartile ranges. When we encountered this we planned to note that the data is skewed and consider the implication of this.
Where multiple trial arms are reported in a single trial, we planned to include only the relevant arms. If two comparisons (e.g. omeprazole versus laparoscopic fundoplication and lansoprazole versus laparoscopic fundoplication) must be entered into the same meta‐analysis, we planned to halve the control group to avoid double counting. The alternative way of including such trials with multiple arms is to pool the results of the omeprazole and lansoprazole and compare it with laparoscopic fundoplication. We planned to perform a sensitivity analysis to determine if the results of the two methods of dealing with multi‐arm trials lead to different conclusions.
Unit of analysis issues
The units of analyses were individual patients with GORD. If cluster‐randomised trials were identified, we planned to obtain the effect estimate adjusted for the clustering effect. If this was not available, we planned to perform a sensitivity analysis excluding the trial from the meta‐analysis as the variance of the effect estimate unadjusted for cluster effect is less than the actual variance which is adjusted for cluster‐effect, giving inappropriately more weight to the cluster RCT in the meta‐analysis.
Dealing with missing data
We attempted to contact investigators or study sponsors in order to verify key study characteristics and obtain missing numerical outcome data where possible (e.g. when a study is identified as abstract only). If we were unable to obtain the information from the investigators or study sponsors, we planned to impute mean from median (i.e. consider median as the mean) and standard deviation from standard error, inter‐quartile range, or P values according to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011c) but planned to assess the impact of including such studies as indicated in a sensitivity analysis. If we were unable to calculate the standard deviation from standard error, inter‐quartile range, or P values, we planned to impute standard deviation as the highest standard deviation in the remaining trials included in the outcome, fully aware that this method of imputation would decrease the weight of the studies in the meta‐analysis of mean difference and shift the effect towards no effect for standardised mean difference.
Assessment of heterogeneity
We used the I² statistic to measure heterogeneity among the trials in each analysis (Higgins 2003). If we identified substantial heterogeneity as per the Cochrane Handbook for Systematic Reviews of Interventions (> 50% to 60%), we planned to explore it by pre‐specified subgroup analysis.
Assessment of reporting biases
We attempted to contact study authors to ask them to provide missing outcome data. When this was not possible, and the missing data were thought to introduce serious bias, we planned to assess the impact of including such studies in the overall assessment of results by a sensitivity analysis.
Since there were fewer than 10 trials for all the outcomes, we did not create and examine a funnel plot to explore possible publication biases. We planned to use Egger's test to determine the statistical significance of the reporting bias (Egger 1997). We planned to use a P value less than 0.05 to show statistically significant reporting bias.
Data synthesis
We performed analyses using RevMan 5.3 (Review Manager 2014). We used the Mantel Haenszel method for dichotomous data, inverse variance method for continuous data, and generic inverse variance for count data. We planned to use generic inverse variance for time‐to‐event data. We used both the fixed‐effect model and random‐effects model for the analysis. We have used a random‐effects model (DerSimonian 1986) and a fixed‐effect model (Demets 1987). In case of discrepancy between the two models, we have reported both results; otherwise we have reported only the results from the fixed‐effect model.
'Summary of findings' table
We created a 'Summary of findings' table using all outcomes. We used the five GRADE (Grades of Recommendation, Assessment, Development and Evaluation) considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the quality of a body of evidence as it related to the studies that contributed data to the meta‐analyses for prespecified outcomes.
We used methods and recommendations as described in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviews of Interventions (Schünemann 2011) and used GRADEpro software (GRADEpro GDT). We justified all decisions to downgrade or upgrade the quality of studies by using footnotes and making comments to aid the reader's understanding of the review whenever necessary. We planned to consider whether any additional outcome information could not be incorporated into the meta‐analyses and noted this in the comments, stating whether it supported or contradicted the information derived from the meta‐analyses.
Subgroup analysis and investigation of heterogeneity
We planned to carry out the following subgroup analyses.
-
Presence versus absence of hiatus hernia.
-
Includes proton pump inhibitor as part of treatment versus those that do not include proton pump inhibitors as part of treatment.
-
Standard recommended dose versus high dose medical treatment.
-
Different methods of fundoplication.
We planned to use all the primary outcomes in subgroup analysis. We planned to use the formal chi2 test for subgroup differences to test for subgroup interactions.
Sensitivity analysis
We planned to perform sensitivity analysis to assess the robustness of our conclusions. This would have involved:
-
Excluding trials at unclear or high risk of bias (one of more of the risk of bias domains (other than blinding of surgeon) classified as unclear or high).
-
Excluding trials in which either mean or standard deviation or both were imputed.
-
Excluding cluster RCTs in which the adjusted effect estimates were not reported.
-
Different methods of dealing with multi‐arm trials (please see Measures of treatment effect).
Reaching conclusions
We have based our conclusions only on findings from the quantitative or narrative synthesis of included studies for this review. We have avoided making recommendations for practice and our implications for research explain any remaining uncertainties to the reader, giving a clear sense of what the focus of any future research in the area should be.
Results
Description of studies
Results of the search
We identified 222 references through electronic searches of the different databases. After removing duplicate references there were 173 references. We excluded 147 clearly irrelevant references through reading abstracts. A total of 26 references were retrieved for further assessment in detail, from the full publication. We excluded nine references for the reasons listed in the 'Characteristics of excluded studies'. Seventeen references of four randomised controlled trials (RCTs) fulfilled the inclusion criteria (Characteristics of included studies). The reference flow is shown in Figure 1.
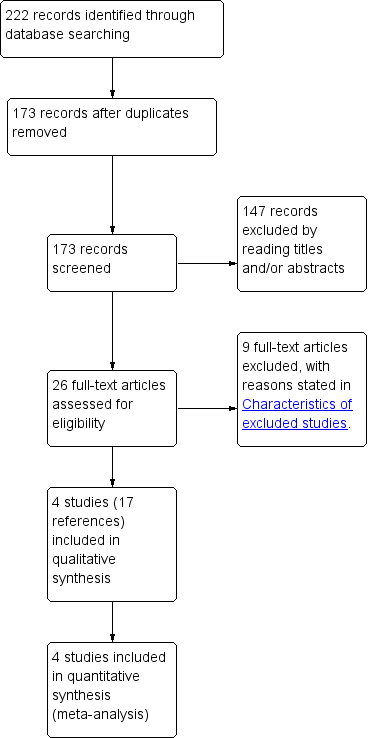
Study flow diagram.
Included studies
The four studies were published between 2005 and 2011. Two were performed in multiple centres in the UK (Grant 2008; Mahon 2005), one was conducted in 11 European countries (Lundell 2008) and the remaining study was conducted at a single centre in Canada (Anvari 2011). The characteristics of the included studies are described in the 'Characteristics of included studies' table. Sample sizes in the trials ranged from 104 to 554 participants, with a total of 1232 randomised participants. Seventy two of these participants were excluded in two trials (Anvari 2011; Mahon 2005). Outcomes were reported on the remaining 1160 participants in the four trials.
Participants
The mean age of participants in the included trials ranged from 43 to 48 years (Anvari 2011; Grant 2008; Lundell 2008; Mahon 2005). The proportion of women in the trials ranged from 28% to 59% in the three trials that provided this information (Anvari 2011; Grant 2008; Lundell 2008). In two trials, the participants had had reflux symptoms for at least 12 months (Anvari 2011; Grant 2008). In the remaining two trials, the participants had had reflux symptoms for at least six months (Lundell 2008; Mahon 2005). In two trials, the participants had received acid suppressive therapy for at least 12 months (Anvari 2011; Grant 2008). In one trial, the participants had received acid suppressive therapy for at least three months (Mahon 2005). In the remaining trial, the participants had received long‐term acid suppressive therapy but the minimum duration of this treatment was not reported (Lundell 2008). None of the trials reported the proportion of participants who had hiatus hernia or Barrett's oesophagus. All the trials included participants who could undergo surgery if randomised to the surgery arm.
Intervention and control
Surgery was by laparoscopic Nissen fundoplication in three trials (Anvari 2011; Lundell 2008; Mahon 2005). In the remaining trial, laparoscopic fundoplication was performed according to the surgeon's preference (Grant 2008). In all the four trials, laparoscopic fundoplications were performed by experienced surgeons (Anvari 2011; Grant 2008; Lundell 2008; Mahon 2005). In all four trials, the medical treatment was proton pump inhibitor. In one trial, the proton pump inhibitor used was esomeprazole 20 mg daily that could be increased step‐wise up to 40 mg daily and could be adjusted to 20 mg twice daily (Lundell 2008). In the remaining trials, proton pump inhibitors were administered according to local protocol (Anvari 2011; Grant 2008; Mahon 2005).
Excluded studies
Two references were non‐randomised studies (Gutschow 2009; Rantanen 2013). Four references included open anti‐reflux surgery (Lundell 2000; Lundell 2007; Lundell 2009; Spechler 2001) and three references included endoscopic anti‐reflux surgery (Trad 2013; Trad 2014; Witteman 2013) as the method of anti‐reflux surgery.
Risk of bias in included studies
The risk of bias is summarised in Figure 2 and Figure 3.

Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.

Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
Allocation
Two trials described the method of random sequence generation and allocation concealment and can be considered to be at low risk of selection bias (Anvari 2011; Grant 2008). The random sequence generation and allocation concealment were not reported in the remaining two trials (Lundell 2008; Mahon 2005).
Blinding
It is impossible to blind participants and the healthcare providers who perform the intervention in trials comparing medical and surgical treatments. So, all the trials were at high risk of performance bias. It is possible to blind the outcome assessors. However, none of the trials reported blinding of outcome assessors. So, all the trials were at unclear or high risk of detection bias.
Incomplete outcome data
In two trials, 20% and 24% of participants were excluded from analysis (Anvari 2011; Mahon 2005). These trials were at high risk of attrition bias. In the remaining two trials, an intention‐to‐treat analysis was performed and so these two trials were at low risk of attrition bias (Grant 2008; Lundell 2008).
Selective reporting
We were unable to identify a published protocol of any of the trials. Two trials reported the important clinical outcomes adequately and are considered to be at low risk of selective reporting bias (Anvari 2011; Lundell 2008). The remaining two trials did not report the treatment‐related complications adequately and are at high risk of selective reporting bias (Grant 2008; Mahon 2005).
Other potential sources of bias
Two trials were funded by organisations with vested interests in the results and are subject to bias due to their source of funding (Lundell 2008; Mahon 2005). The remaining two trials were funded by organisations without vested interests in the results and were at low risk of source‐of‐funding bias. The surgeons in all the trials were experienced in laparoscopic fundoplication and are free from differential expertise bias.
Effects of interventions
The effect of intervention on various outcomes is summarised in the 'Summary of findings' Table. Long‐term overall health‐related quality of life and long‐term GORD‐specific quality of life were not reported in any of the trials.
Health related quality of life (HRQoL)
Short‐term (four weeks to 12 months)
Three trials reported short‐term HRQoL (Anvari 2011; Grant 2008; Mahon 2005). One trial used SF‐36 to measure HRQoL (Anvari 2011). One trial used EQ‐5D to measure HRQoL (Grant 2008). The last trial used a general well‐being score to measure HRQoL (Mahon 2005). There was no statistically significant difference in HRQoL between the two groups (SMD 0.14, 95% CI ‐0.02 to 0.30; participants = 605; studies = 3; I2 = 64%). There was substantial heterogeneity in the results. Using the random‐effects model did not alter the conclusions.
Medium‐term (one year to five years)
Two trials reported medium‐term HRQoL (Anvari 2011; Grant 2008). One trial used SF‐36 to measure HRQoL (Anvari 2011). The other trial used EQ‐5D to measure HRQoL (Grant 2008). There was no statistically significant difference in HRQoL between the two groups (SMD 0.03, 95% CI ‐0.19 to 0.24; participants = 323; studies = 2; I2 = 65%). There was substantial heterogeneity in the results. Using the random‐effects model did not alter the conclusions.
GORD‐specific quality of life (QoL)
Short‐term (four weeks to 12 months)
All four trials reported short‐term GORD‐specific QoL (Anvari 2011; Grant 2008; Lundell 2008; Mahon 2005). One trial used the Gastroesophageal Reflux Symptom Score (GERSS) to measure GORD‐specific QoL (Anvari 2011). One trial used REFLUX QoL to measure GORD‐specific QoL (Grant 2008). One trial used the Gastrointestinal Symptom Rating Scale (GSRS) to measure GORD‐specific QoL (Lundell 2008). The last trial used a gastrointestinal well‐being score to measure GORD‐specific QoL (Mahon 2005). The GORD‐specific QoL was significantly better with laparoscopic fundoplication than medical treatment (SMD 0.58, 95% CI 0.46 to 0.70; participants = 1160; studies = 4; I2 = 40%). The heterogeneity was not considered important since all the studies were suggesting better GORD‐specific QoL in the surgical groups than in the medical treatment groups. Using the random‐effects model did not alter the conclusions.
Medium‐term (one year to five years)
Three trials reported medium‐term GORD‐specific QoL (Anvari 2011; Grant 2008; Lundell 2008). One trial used the Gastroesophageal Reflux Symptom Score (GERSS) to measure GORD‐specific QoL (Anvari 2011). One trial used REFLUX QoL to measure GORD‐specific QoL (Grant 2008). The last trial used Gastrointestinal Symptom Rating Scale (GSRS) to measure GORD‐specific QoL (Lundell 2008). The GORD‐specific QoL was significantly better with laparoscopic fundoplication than medical treatment (SMD 0.34, 95% CI 0.22 to 0.47; participants = 994; studies = 3; I2 = 94%) when the fixed‐effect model was used, but on using the random‐effects model, there was no statistically significant difference in GORD‐specific QoL between the two groups (SMD 0.28, 95% CI ‐0.27 to 0.84; participants = 994; studies = 3; I2 = 94%). There was considerable heterogeneity in the results between the studies.
Serious adverse events
Two trials reported the severity of complications (Anvari 2011; Lundell 2008). There were no serious adverse events in either group in one trial (Anvari 2011). In the other trial, the proportion of people with serious adverse events was statistically significantly higher in the laparoscopic fundoplication group than in the medical treatment group (RR 1.46, 95% CI 1.01 to 2.11; participants = 637; studies = 2). Since only one trial contributed to the meta‐analysis (the other trial being a zero‐event trial), we did not assess heterogeneity and the issue of fixed‐effect model versus random‐effects model does not arise.
Adverse events
One trial reported all adverse events (Anvari 2011). There was no statistically significant difference in the proportion of people with adverse events between the groups (RR 13.98, 95% CI 0.82 to 237.07; participants = 83; studies = 1). Since only one trial was included in this outcome, we did not assess heterogeneity and the issue of fixed‐effect model versus random‐effects model does not arise.
Dysphagia
Short‐term (four weeks to 12 months)
Two trials reported short‐term dysphagia (Anvari 2011; Lundell 2008). The proportion of people with dysphagia was statistically significantly higher after laparoscopic fundoplication than medical treatment (RR 3.58, 95% CI 1.91 to 6.71; participants = 637; studies = 2; I2 = 0%). There was no heterogeneity in the results between the studies. Using the random‐effects model did not alter the conclusions.
Medium‐term (one year to five years)
One trial reported medium‐term dysphagia (Lundell 2008). The proportion of people with dysphagia was statistically significantly higher after laparoscopic fundoplication than medical treatment (RR 5.36, 95% CI 2.10 to 13.64; participants = 554; studies = 1). Since only one trial was included in this outcome, we did not assess heterogeneity and the issue of fixed‐effect model versus random‐effects model does not arise.
Long‐term (five years or more)
One trial reported long‐term dysphagia (Grant 2008). There was no statistically significant difference in the proportion of people with dysphagia between the two groups (RR 0.90, 95% CI 0.57 to 1.42; participants = 228; studies = 1). Since only one trial was included in this outcome, we did not assess heterogeneity and the issue of fixed‐effect model versus random‐effects model does not arise.
Heartburn
Short‐term (four weeks to 12 months)
One trial reported short‐term heartburn (Lundell 2008). The proportion of people with heartburn was statistically significantly less after laparoscopic fundoplication than medical treatment (RR 0.45, 95% CI 0.30 to 0.69; participants = 554; studies = 1). Since only one trial was included in this outcome, we did not assess heterogeneity and the issue of fixed‐effect model versus random‐effects model does not arise.
Medium‐term (one year to five years)
One trial reported medium‐term heartburn (Lundell 2008). The proportion of people with heartburn was statistically significantly less after laparoscopic fundoplication than medical treatment (RR 0.19, 95% CI 0.10 to 0.34; participants = 554; studies = 1). Since only one trial was included in this outcome, we did not assess heterogeneity and the issue of fixed‐effect model versus random‐effects model does not arise.
Long‐term (five years or more)
One trial reported long‐term heartburn (Grant 2008). The proportion of people with heartburn was statistically significantly less after laparoscopic fundoplication than medical treatment (RR 0.56, 95% CI 0.44 to 0.72; participants = 217; studies = 1). Since only one trial was included in this outcome, we did not assess heterogeneity and the issue of fixed‐effect model versus random‐effects model does not arise.
Reflux
Short‐term (four weeks to 12 months)
One trial reported short‐term reflux (Lundell 2008). The proportion of people with reflux was statistically significantly less after laparoscopic fundoplication than medical treatment (RR 0.10, 95% CI 0.05 to 0.24; participants = 554; studies = 1). Since only one trial was included in this outcome, we did not assess heterogeneity and the issue of fixed‐effect model versus random‐effects model does not arise.
Medium‐term (one year to five years)
One trial reported medium‐term reflux (Lundell 2008). The proportion of people with reflux was statistically significantly less after laparoscopic fundoplication than medical treatment (RR 0.15, 95% CI 0.06 to 0.35; participants = 554; studies = 1). Since only one trial was included in this outcome, we did not assess heterogeneity and the issue of fixed‐effect model versus random‐effects model does not arise.
Long‐term (five years or more)
One trial reported long‐term reflux (Grant 2008). There was no statistically significant difference in the proportion of people with reflux between the two groups (RR 0.69, 95% CI 0.46 to 1.03; participants = 233; studies = 1). Since only one trial was included in this outcome, we did not assess heterogeneity and the issue of fixed‐effect model versus random‐effects model does not arise.
Subgroup analysis
We did not perform any subgroup analysis. None of the trials reported the results separately for participants with hiatus hernia, so a subgroup analysis of participants with hiatus hernia could not be performed. All the trials included proton pump inhibitors as part of the medical treatment, so a subgroup analysis of trials that included proton pump inhibitors as part of treatment versus those that did not include proton pump inhibitors as part of treatment could not be performed. Only one of the trials specified the dose of proton pump inhibitor, so a subgroup analysis of standard recommended dose versus high dose medical treatment could not be performed. Three trials used laparoscopic Nissen fundoplication and one trial used laparoscopic fundoplication according to the surgeon's preference, so a subgroup analysis of different methods of fundoplication could not be performed.
Sensitivity analysis
We did not perform any sensitivity analysis. All the trials were at high risk of bias, so a sensitivity analysis excluding trials at unclear or high risk of bias could not be performed. We did not impute the mean or standard deviation for any of the comparisons, so a sensitivity analysis excluding trials in which either mean or standard deviation or both were imputed could not be performed. There were no cluster RCTs, so a sensitivity analysis excluding cluster RCTs in which the adjusted effect estimates were not reported could not be performed. All the trials were two‐armed trials, so a sensitivity analysis excluding different methods of dealing with multi‐arm trials could not be performed.
Reporting bias
Two trials did not report the treatment‐related complications adequately. Hence the outcomes 'serious adverse events' and 'adverse events' are subject to reporting bias. Since there were fewer than 10 trials for all the outcomes, we did not create and examine a funnel plot to explore possible publication biases.
Discussion
Summary of main results
In this systematic review of laparoscopic fundoplication versus medical treatment, we identified four RCTs. There was no evidence of any difference in the overall short‐term or medium‐term health‐related quality of life between the groups. The short‐term GORD‐specific quality of life was better in the laparoscopic fundoplication group than in the medical treatment group. However, there was no evidence of any difference in the medium‐term GORD‐specific quality of life. None of the trials reported long‐term overall or GORD‐specific quality of life. The proportion of people with serious adverse events was higher in the laparoscopic fundoplication group than in the medical treatment group. There was no evidence of any difference in the proportion of people with overall adverse events between the groups. The proportion of people with dysphagia was greater in the laparoscopic fundoplication group than in the medical treatment group in the short and medium terms. There was no evidence of any difference in the proportion of people with long‐term dysphagia between the groups. The proportion of people with heartburn was less in the laparoscopic fundoplication group than in the medical treatment group at short term, medium term and long term, and the proportion of people with reflux symptoms was also less in the laparoscopic fundoplication group than in the medical treatment group at short term and medium term. There was no evidence of any difference in the proportion of people with long‐term reflux symptoms between the groups.
All the studies indicated better GORD‐specific quality of life in the short term in the laparoscopic fundoplication group compared to the medical treatment group. Despite using valid scales to measure the GORD‐specific quality of life, it is not clear how the difference translates into clinical importance to the patient, such as fewer work days lost or improved social activity. There was no evidence of a difference in the GORD‐specific quality of life beyond the short term. There was no evidence of a difference in the health‐related quality of life between the groups at any time‐point. It is not reasonable to prefer one treatment over another because of the short‐lived benefits of laparoscopic fundoplication over medical treatment.
Dysphagia was higher in the laparoscopic fundoplication group than in the medical treatment group in the short and medium terms. Heartburn and reflux symptoms were less in the laparoscopic fundoplication group than in the medical treatment group in the short and medium terms. Long‐term heartburn symptoms were less in the laparoscopic fundoplication group than in the medical treatment group but there was no evidence of a difference in the long‐term dysphagia or reflux symptoms. Severity and impact (social and economic) were not reported, so it is difficult to recommend treatments based on these outcomes.
Adverse events and their severity were not reported adequately in two trials (Grant 2008; Mahon 2005). It is important to know the complications related to the two treatment groups and the severity of these complications before the treatment can be recommended. It was not possible to assess this from this systematic review. A review of a US database including 13,050 patients who had undergone laparoscopic fundoplication reported a reoperation rate of approximately 5% at 5 years and 7% at 10 years (Zhou 2015). The majority of these reoperations were 'redo' fundoplications (87% of reoperations) while the remaining 13% of reoperations were reversal of fundoplication (Zhou 2015). Redo fundoplications are generally carried out for failure of improvement of existing symptoms or new symptoms of GORD (Smith 2005). Reversal of fundoplication is usually performed because of symptoms such as bloating and dysphagia. A review of a Danish database including 2465 patients who had undergone an open or laparoscopic fundoplication reported a 30‐day mortality of 0.46% and a reoperation rate of 5% (Funch‐Jensen 2008). Thus, the complications of laparoscopic fundoplication cannot be taken lightly. The major adverse events associated with long‐term proton pump inhibitor treatment are a modest increase in the risk of osteoporosis‐related fractures; an increase in the risk of Clostridium difficile infections in people who are admitted to hospital, from 0.3% to 0.9%; an increase in community‐acquired pneumonias; and an increase of approximately 30% in hospital‐acquired pneumonias from the baseline rate of 2% (Gray 2010; Herzig 2009; Howell 2010; Katz 2010b; Lambert 2015).
The choice between surgical and medical treatment is therefore likely to be based on whether people prefer to undergo a procedure that has a risk of mortality of around 0.5% and a reoperation rate of around 5%, or take long‐term medical treatment which carries a modest increased risk of fractures, Clostridium difficile infections if admitted to hospital, and pneumonia.
Overall completeness and applicability of evidence
All four studies included in this review compared laparoscopic fundoplication with proton pump inhibitor treatment. The results of this systematic review are therefore only applicable when the choice has to be made between laparoscopic fundoplication and proton pump inhibitor treatment in people for whom laparoscopic fundoplication or long‐term proton pump inhibitor treatment is a viable option.
Quality of the evidence
All the trials were considered to be at high risk of bias. While it is impossible to blind participants and healthcare providers who perform the treatment, it is possible to blind outcome assessors. Given that most of the outcomes are subjective outcomes, lack of outcome assessor blinding introduces bias to the effect estimates. Another major source of bias is the post‐randomisation drop‐out of 20% and 24% in two trials (Anvari 2011; Mahon 2005). In another trial, only 60% to 65% of participants were included in the long‐term outcomes (Grant 2008) reflecting the difficulty in long‐term follow‐up of trial participants. Exclusion of the participants is likely to overestimate the treatment benefits. The proportion of people who underwent surgery and who started taking medical treatment (hence exposing the patients to the risk of long‐term medical treatment) was not clear from the trials. There was substantial heterogeneity in some of the outcomes (short‐term and medium‐term overall health‐related quality of life and medium‐term GORD‐specific quality of life). In the absence of significant heterogeneity in participants and treatment (three trials used laparoscopic Nissen fundoplication and one trial used laparoscopic fundoplication according to the surgeon's preference; three trials used a pragmatic approach of medical treatment according to local protocol), the heterogeneity could be because of the instruments used to measure the quality of life. This also introduces additional uncertainty since different validated instruments result in different results. Many of the outcomes had only been reported by one of the included trials. This introduces uncertainty since we can consider that these results were never reproduced. Overall, the quality of evidence was low or very low for all the outcomes.
Potential biases in the review process
We took a systematic approach to each stage in the review process, including the search for literature, selection of titles and abstracts for full critical appraisal and data extraction. Two authors independently assessed all studies and disagreements were resolved by discussion.
Agreements and disagreements with other studies or reviews
The previous version of this review suggested that laparoscopic fundoplication surgery was more effective than medical management for the treatment of GORD at least in the short to medium term, that surgery carries some risk, and whether the benefits of surgery are sustained in the long term remains uncertain (Wileman 2010). Our conclusions have changed with use of current Cochrane Handbook guidelines to interpret the evidence.
Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.
Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
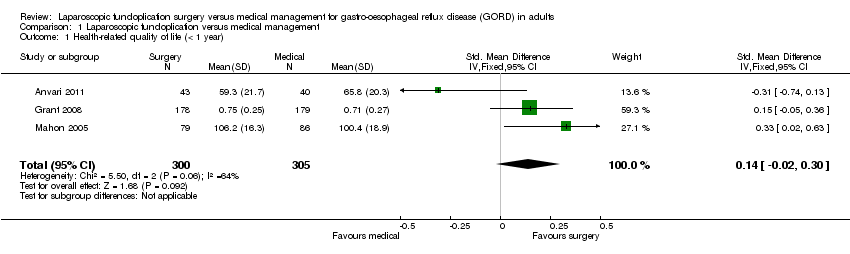
Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 1 Health‐related quality of life (< 1 year).
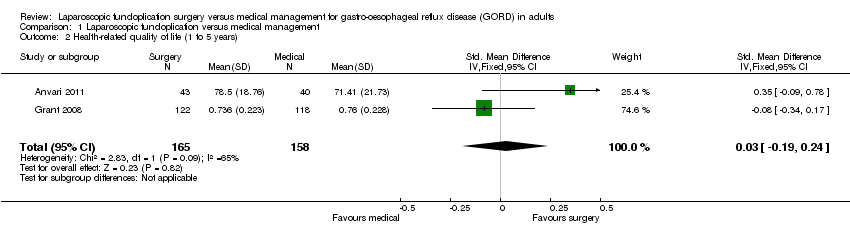
Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 2 Health‐related quality of life (1 to 5 years).

Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 3 GORD‐specific quality of life (< 1 year).
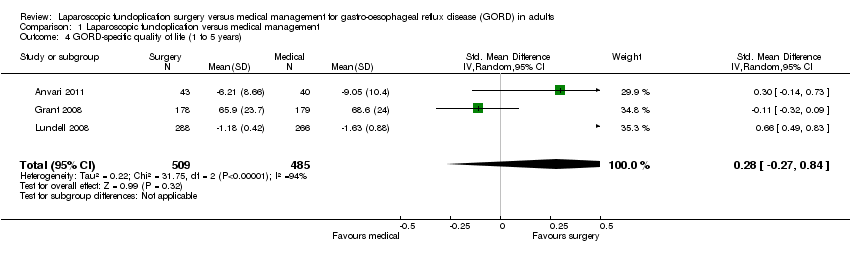
Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 4 GORD‐specific quality of life (1 to 5 years).

Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 5 Serious adverse events.

Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 6 Adverse events.

Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 7 Dysphagia (< 1 year).
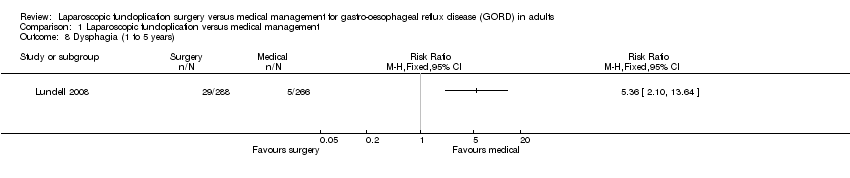
Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 8 Dysphagia (1 to 5 years).

Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 9 Dysphagia (5 years or more).
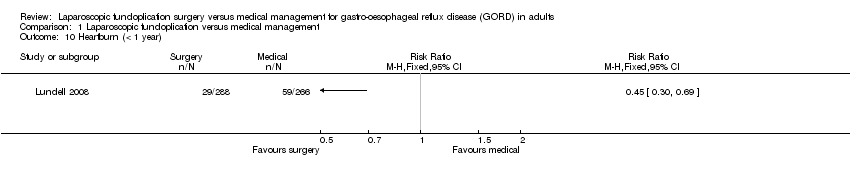
Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 10 Heartburn (< 1 year).
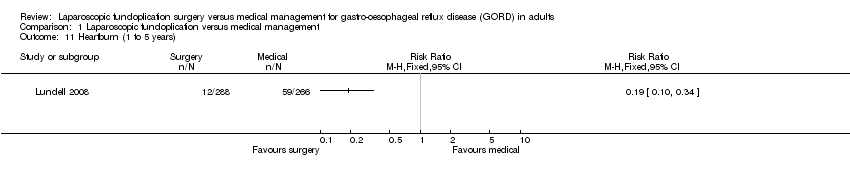
Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 11 Heartburn (1 to 5 years).

Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 12 Heartburn (5 years or more).

Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 13 Reflux (< 1 year).

Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 14 Reflux (1 to 5 years).
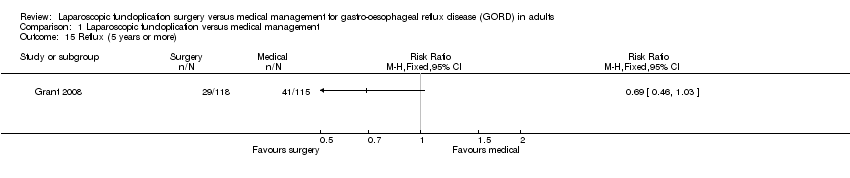
Comparison 1 Laparoscopic fundoplication versus medical management, Outcome 15 Reflux (5 years or more).
| Laparoscopic fundoplication versus medical management for gastro‐oesophageal reflux disease (GORD) in adults | ||||||
| Patient or population: Patients with gastro‐oesophageal reflux disease (GORD) in adults Control: Medical management | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Medical management | Laparoscopic fundoplication | |||||
| Health‐related quality of life | ||||||
| (< 1 year) | The mean health‐related quality of life (< 1 year) in the intervention groups was | 605 | ⊕⊝⊝⊝ | SMD 0.14 (‐0.02 to 0.3) | ||
| (1 to 5 years) | The mean health‐related quality of life (1 to 5 years) in the intervention groups was | 323 | ⊕⊝⊝⊝ | SMD 0.03 (‐0.19 to 0.24) | ||
| GORD‐specific quality of life | ||||||
| (< 1 year) | The mean GORD‐specific quality of life (< 1 year) in the intervention groups was | 1160 | ⊕⊕⊝⊝ | SMD 0.58 (0.46 to 0.7) | ||
| (1 to 5 years) | The mean GORD‐specific quality of life (1 to 5 years) in the intervention groups was | 994 | ⊕⊝⊝⊝ | SMD 0.28 (‐0.27 to 0.84) | ||
| Adverse events | ||||||
| Serious adverse events | 124 per 1000 | 181 per 1000 | RR 1.46 | 637 | ⊕⊝⊝⊝ | |
| Adverse events | 10 per 1000 | 140 per 1000 | RR 13.98 | 83 | ⊕⊝⊝⊝ | |
| Dysphagia | ||||||
| (< 1 year) | 36 per 1000 | 129 per 1000 | RR 3.58 | 637 | ⊕⊝⊝⊝ | |
| (1 to 5 years) | 19 per 1000 | 101 per 1000 | RR 5.36 | 554 | ⊕⊝⊝⊝ | |
| (5 years or more) | 255 per 1000 | 229 per 1000 | RR 0.9 | 228 | ⊕⊝⊝⊝ | |
| Heartburn | ||||||
| (< 1 year) | 222 per 1000 | 100 per 1000 | RR 0.45 | 554 | ⊕⊝⊝⊝ | |
| (1 to 5 years) | 222 per 1000 | 42 per 1000 | RR 0.19 | 554 | ⊕⊝⊝⊝ | |
| (5 years or more) | 736 per 1000 | 412 per 1000 | RR 0.56 | 217 | ⊕⊝⊝⊝ | |
| Reflux | ||||||
| (< 1 year) | 199 per 1000 | 20 per 1000 | RR 0.1 | 554 | ⊕⊝⊝⊝ | |
| (1 to 5 years) | 139 per 1000 | 21 per 1000 | RR 0.15 | 554 | ⊕⊝⊝⊝ | |
| (5 years or more) | 357 per 1000 | 246 per 1000 | RR 0.69 | 233 | ⊕⊝⊝⊝ | |
| Long‐term overall health‐related quality of life and long‐term GORD‐specific quality of life were not reported in any of the trials. | ||||||
| *The basis for the assumed risk was the mean control group risk across studies for all outcomes other than adverse events. For control group risk, 1% was used as the control group risk since there were no adverse events in the control group in the only trial that reported this outcome (Anvari 2011). The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1 The trial(s) was/were at high risk of bias. | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Health‐related quality of life (< 1 year) Show forest plot | 3 | 605 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.14 [‐0.02, 0.30] |
| 2 Health‐related quality of life (1 to 5 years) Show forest plot | 2 | 323 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.03 [‐0.19, 0.24] |
| 3 GORD‐specific quality of life (< 1 year) Show forest plot | 4 | 1160 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.58 [0.46, 0.70] |
| 4 GORD‐specific quality of life (1 to 5 years) Show forest plot | 3 | 994 | Std. Mean Difference (IV, Random, 95% CI) | 0.28 [‐0.27, 0.84] |
| 5 Serious adverse events Show forest plot | 2 | 637 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.46 [1.01, 2.11] |
| 6 Adverse events Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7 Dysphagia (< 1 year) Show forest plot | 2 | 637 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.58 [1.91, 6.71] |
| 8 Dysphagia (1 to 5 years) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 9 Dysphagia (5 years or more) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 10 Heartburn (< 1 year) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 11 Heartburn (1 to 5 years) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 12 Heartburn (5 years or more) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 13 Reflux (< 1 year) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 14 Reflux (1 to 5 years) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 15 Reflux (5 years or more) Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |