Water, sanitation and hygiene (WASH) interventions: effects on child development in low‐ and middle‐income countries
Abstract
This is a protocol for a Cochrane Review (Intervention). The objectives are as follows:
Main objective
The main objective is to assess the effect of interventions to improve sanitation, hygiene, water quality and supply within low‐ and middle‐income countries on child development.
Secondary objectives
The secondary objectives are to:
-
analyse any measured effect of water, sanitation and hygiene (WASH) interventions on school or preschool enrolment and attendance;
-
examine the feasibility of WASH interventions with regard to their implementation fidelity and participant compliance;
-
evaluate the effect of WASH interventions on intermediary outcomes of environmental contamination, gastrointestinal diseases and reduction in the burden of water collection and water costs; and
-
identify any adverse impact that WASH interventions may have for participants.
Background
Introduction
Poor water, sanitation and hygiene (WASH) and suboptimal nutrition are important risk factors for morbidity and mortality in children less than 5 years of age (Walker 2007; Arnold 2013). The synergistic effects of infection and under‐nutrition during the first thousand days of life (www.thousanddays.org) have been shown in several studies to have long‐term effects on health, growth and cognitive development (Guerrant 2008; Victora 2008; Engle 2010; Walker 2011a).
A recent Cochrane systematic review (Dangour 2013) examined the available evidence regarding the impact of WASH interventions on child growth. Although no trials of sanitation interventions were found, the effect of solar disinfection of water, provision of soap and improvement in water quality on linear and ponderal growth in children under five years of age was assessed. A meta‐analysis of data from the five available cluster‐randomised controlled trials showed no significant effect on weight‐for‐age, but a borderline statistically significant effect on height‐for‐age. However, the duration of the studies was relatively short (between 9 and 12 months); also, adherence was only measured in two of the five studies, and was found to vary considerably. None of the trials masked the nature of the intervention so that none were judged to be of high methodological quality (Dangour 2013). Although the quality of evidence was poor, the overall conclusion was that WASH interventions confer a small growth benefit, but that additional information from current ongoing studies should provide further evidence.
Although there is now, therefore, evidence for the impact of WASH interventions on child growth, there has been no systematic review of the available evidence for the effect of WASH interventions on child development. Child growth is typically defined by anthropometric measurement (predominantly weight and height). By contrast, child development is a measure of brain function, traditionally assessed through tests of gross and fine motor coordination, language and socio‐emotional skills, with more academic (cognitive) measures such as literacy and numeracy for older children. It would make sense that many of the factors that promote early‐life physical development also impact child development outcomes in children. Synthesis of the evidence combined with available implementation data on the included studies will help to interpret existing research findings, inform future studies, and guide policy in the health, education and WASH sectors (Britto 2016).
With this in mind, interventions targeted at improving WASH have recently been found to be strongly associated with both improved growth and cognitive outcomes, after adjusting for various potential confounders, in several observational studies and clinical trials (Spears 2011). For example, the installation of pit latrines during the first year of Indian children's life, as part of the Total Sanitation Campaign, was associated with an improvement in their literacy (Spears 2013). Five‐year follow‐up of children in a handwashing trial in Karachi (Luby 2006) showed significant benefits of handwashing on motor and cognitive development at 30 months of age (Bowen 2012). Longitudinal evidence is also emerging: the Institute of Nutrition of Central America and Panama (INCAP) studies, which have monitored growth and development over 50 years, have shown that environmental factors relating to poverty have more impact on growth and functional development than do genetic factors (Martorell 2010a). Although observational studies are susceptible to confounding, there is increasing evidence that low socioeconomic status and malnutrition negatively impact child development in multiple ways, beyond solely an increased risk of illness (Brown 1996). These other factors include lethargy and reduced exploration in the child and the lack of stimulation, education and expectations from carers and the community (Brown 1996). The recent emerging evidence for WASH interventions on child development therefore highlights the importance of conducting a systematic review in this area.
Description of the condition
Malnutrition, infection and enteropathy: effects on child development
The potential impact of WASH on neurocognitive development may operate through multiple pathways, including effects on malnutrition, enteropathy and infection. Malnutrition can be divided into two predominant types: wasting (low weight‐for‐height) and stunting (low height‐for‐age). Stunting (defined as a height‐for‐age greater than 2 standard deviations below the population median) affects 26% of children under the age of 5 years globally. Poor growth and stunting has been shown to be a major risk factor for delayed child development (Walker 2011a) and subsequent reduced human capital (Grantham‐McGregor 2007; Walker 2007; Victora 2008). Similarly, interventions on early child development have been shown to give benefits across the life course (Black 2016; Britto 2016). Among children exposed to poverty, follow‐up studies show long‐term beneficial effects of interventions that provided early‐life stimulation (Walker 2011b; Gertler 2014) or nutrition (Hoddinott 2008). Positive effects were noted on educational attainment and intelligence quotient (Stein 2008; Maluccio 2009; Walker 2011b; Gertler 2014) as well as adult wage earning (Martorell 2010b; Gertler 2014). Early child stimulation was also associated with adult health improvements in lowered blood pressure and signs of metabolic syndrome (Campbell 2014), as well as reductions in violence and depressive symptoms (Walker 2011b). The intergenerational risk of stunting (Walker 2015) can also be significantly improved with early intervention (Behrman 2009). These findings provide strong economic justification for investment in early childhood growth and development, particularly within the first 1000 days (Doyle 2009; Hoddinott 2013; Black 2016).
Studies have shown that dietary interventions alone do not normalise linear growth in the first two years of life among children in developing countries (Dewey 2008; Lassi 2013). Growth faltering therefore remains a challenge despite extensive research (Nabwera 2017). This may be partly due to recurrent symptomatic infections (e.g. diarrhoea, pneumonia) (Guerrant 2008). Individual episodes of diarrhoea have not generally been strongly implicated in stunting (Briend 1990), due to catch‐up growth between episodes (Briend 1989; Poskitt 1999). However, a higher cumulative burden of diarrhoea prior to 24 months has been shown to increase the risk of stunting at 24 months (Checkley 2008) and in one study to act as an independent risk factor for impaired neurodevelopment (Pinkerton 2016). A recent analysis of data from 137 developing countries identified diarrhoea and lack of improved sanitation as two of the leading risk factors for stunting (Danaei 2016).
It is becoming apparent that subclinical infections and chronic inflammation, particularly arising from the intestinal tract, may be an important cause of growth failure (Humphrey 2009). Environmental enteric dysfunction (EED) is a complex inflammatory small intestinal disorder, likely arising from recurrent exposure to pathogenic bacteria, leading to a shift in microbiota assembly, and chronic gut inflammation (Prendergast 2012). This causes intestinal damage, characterised by flattened villi (Kelly 2004) and an inflammatory cell infiltrate, leading to modest malabsorption of nutrients and increased intestinal permeability (Kelly 2016). Loss of intestinal barrier function enables microbial translocation across a damaged gut mucosa, which is thought to drive a chronic state of systemic immune activation. Overall, this chronic, low‐grade inflammation may lead to poor linear growth, anaemia of inflammation and impaired neurodevelopment in children (Humphrey 2009; Arnold 2013; Ngure 2013; Ngure 2014). A recent observational study of rural Zimbabwean infants showed that many have high exposure to Escherichia coli, due to active ingestion of soil and chicken faeces together with feco‐oral transmission through contaminated fingers and drinking water (Ngure 2013). Widespread environmental contamination with E. coli has similarly been demonstrated in other countries such as Peru (Gil 2014), indicating that exposure to pathogenic microbes is common among children living in impoverished conditions.
There is now increasing evidence that children living in unsanitary conditions have raised inflammatory biomarkers indicative of EED, which are associated with stunting (Kosek 2013; Lin 2013). For example, studies from the Gambia showed that infants had elevated levels of antibodies against bacterial endotoxin (lipopolysaccharide, LPS), which correlated with intestinal permeability (Campbell 2003), and raised inflammatory markers, which correlated inversely with growth (Campbell 2003). More recent studies have shown that markers of intestinal inflammation (Kosek 2013), intestinal repair (Peterson 2013) and systemic inflammation (Lin 2013; Prendergast 2014) are inversely associated with linear growth in several developing country populations. As well as diverting energy and resources away from growth and towards chronic inflammation, low‐grade inflammation may also mediate stunting through suppression of the growth hormone‐IGF‐1 axis (Prendergast 2014), in a similar way to children with Crohn’s disease (Walters 2009).
Chronic inflammation and insulin‐like growth factor (IGF‐1) levels may also be important determinants of early‐life neurodevelopment. There is increasing evidence that the nutrient priority for brain development is mediated particularly through IGF‐1 (Lee 1999), which has been linked with improved neurodevelopment in children (Gunnell 2005). Isolated human genetic cases of IGF‐1 deficiency have significantly impaired growth and development (Netchine 2009) and, in murine models, show poor brain development (Ni 1997). A recent study has also shown improvement of head circumference (a reliable measure of brain volume) (Cheong 2008) in 11 out of 13 children with Laron syndrome, a rare syndrome due to lack of IGF‐1, who were treated with IGF‐1 (Laron 2012). IGF‐1 has also been shown to be significantly higher among babies with intra‐uterine growth restriction (IUGR) exhibiting catch‐up linear growth, compared to those who do not (Ozkan 1999). Linear growth reflects protein intake and is closely related to the development of organs, including the brain (Cusick 2012). Given the impact of chronic inflammation, arising predominantly from EED and recurrent infections, on stunting and similarly reduced IGF‐1 levels (Prendergast 2014), this suggests a plausible physiological mechanism through which chronic inflammation may influence brain development in early life.
Taken together, there is emerging evidence that subclinical infections, inflammation and EED may underlie growth failure and impaired neurodevelopment in early life. It is therefore plausible that WASH interventions, which may reduce diarrhoea and other infections, pathogen exposure and EED, may be important in promoting optimal child development in developing countries.
Description of the intervention
The provision of safe water, sanitary disposal of human waste, and personal hygiene have long been known to have profound effects on human health (Bartram 2010). Despite progress in extending access to water and sanitation through the Millennium Development Goals (MDGs), over one third of the global population live in households without these basic services (Cumming 2014). The prevalence of safe hygiene practices is difficult to estimate but is likely to be even lower than for water and sanitation (Freeman 2014). The absence of safe water, sanitation and hygiene (WASH) results in a large disease burden with approximately one million preventable diarrhoeal deaths each year (Pruss‐Ustun 2014) as well as a range of other infectious diseases (Bartram 2010).
WASH interventions are defined in line with previous Cochrane reviews (Clasen 2006; Clasen 2010; Dangour 2013; Clasen 2015) according to the following four categories:
-
Water quantity or supply improvement is any intervention to provide any new or improved water supply or distribution system. This includes the installation of a new hand pump, a household connection to a piped water supply, or a rainwater harvesting technology.
-
Water quality is any intervention to prevent, remove or inactivate microbiological pathogens, both at ‘source’ and at ‘point of use’. This includes household, or water source‐level treatment systems involving filtration, sedimentation, chemical treatment, heat treatment, ultraviolet (UV) radiation or education on improving water quality. Additionally, this includes protection of water before consumption (protected distribution, residual disinfection or improved storage facilities).
-
Sanitation is any intervention to provide or promote new or improved sanitation, or expand and improve excreta disposal. This includes flush/pour flush toilets, pit latrines, composting toilets, or connections to onsite (e.g. septic tanks) or off‐site systems (e.g. sewerage).
-
Hygiene is any intervention to initiate or promote further practice of handwashing with soap or other agents after defecation, after disposal of child faeces, and prior to preparing, eating and handling food. This includes interventions to promote changes in hygiene (group discussions, media campaigns, leaflets, songs, dramas, school initiatives), and interventions providing soap or other agents to improve hygiene and/or equipment to facilitate handwashing (e.g. handwashing stations, ‘Tippy Taps’).
How the intervention might work
A role for WASH in neurodevelopment?
There is increasing interest in the hypothesis that WASH interventions could reduce microbial exposure and prevent or ameliorate EED and symptomatic diarrhoea, thereby improving not only growth and anaemia but also neurodevelopmental outcomes (Ngure 2014). Strategies to date for improving child development have centred mainly on parenting education and preschool support to provide stimulation (Engle 2011). However, it is plausible that WASH interventions could impact early child development in multiple ways.
We have developed a conceptual framework to illustrate how poor WASH may affect child development (Figure 1). We propose four key domains through which WASH may operate: 1) gut pathology, 2) inflammation and infection, 3) socioeconomic status and maternal health, and 4) behavioural and home factors. Interactions between microbial exposure and enteropathy lead to malnutrition and chronic inflammation, with resultant anaemia and stunting, which impair brain development. Poor WASH also exerts a burden of water collection and cost, which has effects on socioeconomic and maternal domains. Food insecurity contributes to malnutrition and maternal stress, which also reduces maternal‐child interaction. This itself impacts stunting and a cyclical interaction of home, school and behavioural development factors. Anaemia, stunting and societal factors cause impaired brain development and resultant delayed early child development. Whilst the conceptual framework simplifies the complex interactions between these individual factors and the four domains, it demonstrates the plausibility of the effect of exposure/outcome relationship that is the subject of this review, and provides a foundation for the search strategy described below.
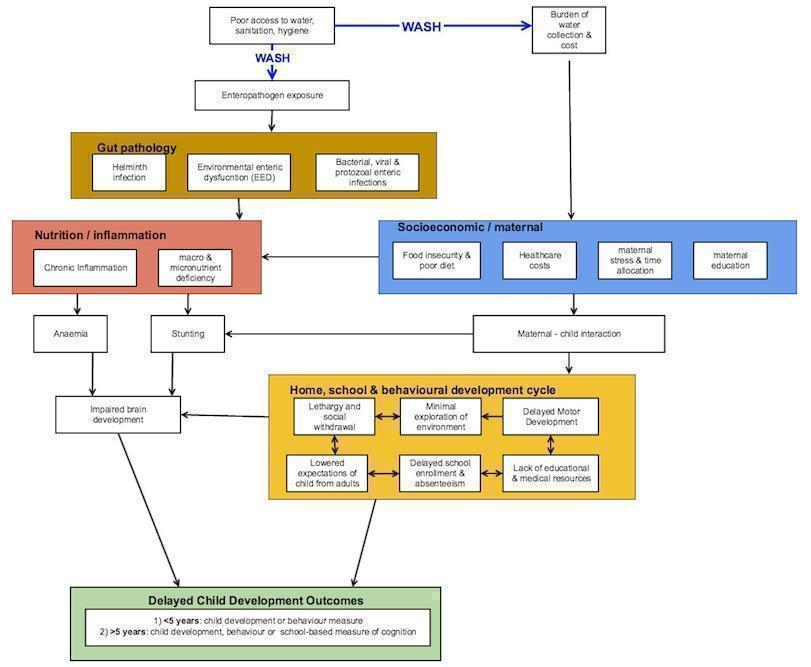
Conceptual framework showing plausible associations between water, sanitation and hygiene (WASH) interventions and gut pathology, nutrition/inflammation, socioeconomic/maternal, home/school environment domains and delayed child development.
The proposed impact of WASH interventions is to reduce both enteropathogen exposure and the socioeconomic burden of water collection. Considering each WASH intervention in turn: improvements in sanitation are likely to reduce environmental enteric dysfunction and helminth reinfection (Strunz 2014). There is less direct evidence for sanitation reducing symptomatic episodes of diarrhoea (Cairncross 2010). However, there remains good evidence that hygiene and handwashing decrease diarrhoeal (Cairncross 2010) and other illnesses (Aiello 2008), as well as helminth infections (Mascarini‐Serra 2011) and are likely to reduce environmental enteric dysfunction (Ngure 2013). Water quality alone has an inconsistent effect on reported diarrhoea (Fewtrell 2005; Cairncross 2010), suggesting the importance of other infective routes (Kirchhoff 1985). However, improving water quality is likely to have some effect in reducing the helminth burden through improved personal hygiene (Fewtrell 2005; Strunz 2014) and also reducing environmental enteric dysfunction (Ngure 2014). Increased water quantity has been shown to have some effect on reducing illness burden (Esrey 1992) and is likely to have an impact on the social determinants of health.
Reductions in the burden and cost of water collection likely improve family food security and well‐being (UNICEF 2011; Campbell 2015), with potential improvements in child macro‐ and micronutrient status. Reduced maternal stress may increase maternal‐child interaction (Harnish 1995), leading to improved motor development, exploration and expectations of achievement from adults (Brown 1996). Finally, there is some evidence that improvements in water and sanitation facilities can improve staffing in both educational (Adugna 2001) and health (Henderson 2008) facilities, and reduce absenteeism in schools (Jasper 2012).
WASH, growth and neurodevelopment
An association has been shown between improved water and sanitation and better growth outcomes in children across multiple countries (Esrey 1996; Merchant 2003; Fenn 2012; Lin 2013). A recent Cochrane review of randomised trials demonstrated a small but significant impact of handwashing and water treatment interventions on height (Dangour 2013). Although no sanitation studies were included, a number of ongoing trials were identified (Clasen 2012; Arnold 2013; Dangour 2013; SHINE 2015). A recent cluster‐randomised trial on community‐led total sanitation has also showed a benefit to child growth in Mali (Pickering 2015). A recent systematic review showed that antibiotics have beneficial effects on weight and length growth of children in low‐ and middle‐income countries (Gough 2014), possibly by reducing subclinical infections and modulating the gut microbiota. There is, therefore, emerging evidence of a role for interventions that may operate through reducing infections and preventing EED, on stunting. We will confine our search to low‐ and middle‐income countries (LMICs) as poor water, sanitation and hygiene conditions are highly concentrated in these regions whilst access to improved water, sanitation and hygiene infrastructure is near universal in most high‐income countries (HICs) (UNICEF 2015) and has been since at least the baseline of the MDGs in 1990. We will use a historical inclusion criterion, so that studies conducted in ‘transitioned’ countries (i.e. those that are currently classified as HIC but were previously classified as LMIC when the study was conducted) will be included.
Stunting has been shown to be strongly associated with reduced measures of early child development (ECD) (Berkman 2002; Grantham‐McGregor 2007; Spears 2011; Walker 2011a), as well as with later school outcomes (Grantham‐McGregor 2007). Outcomes in these studies vary, as multiple scales of cognitive development have been used, with few of these validated in LMICs (Fernald 2009; Frongillo 2014). However, local adaptations of these scales are possible and have been applied, for example, in Uganda (Nampijja 2010) and Kenya (Abubakar 2008). Long‐term studies have demonstrated how early child nutrition and height, educational attainment and subsequent employment may be linked (Pollitt 1993; Maluccio 2009; Vogl 2014; Richter 2016).
WASH effects on anaemia
Iron is essential for brain development through its roles in myelination, neurotransmission and protein expression (Lozoff 2007). Some studies focusing on children from preschool age to adolescence, report poorer cognitive, motor and social development and persisting neurophysiological differences due to iron deficiency anaemia (Lozoff 2006). For example, anaemic infants without iron supplementation crawled later, had reduced social interaction and were generally more passive to stimulation compared to non‐anaemic infants (Lozoff 2003). Children with iron deficiency have reduced auditory brain responses and visual evoked potentials, corroborating the role of iron in myelination (Algarin 2003). There is also longitudinal evidence that infants aged 6 to 24 months with iron deficiency anaemia are at risk of deficits in cognition and school achievement up to 10 years later (Lozoff 2000). However, a recent study in Nepal showed no benefit for iron‐folate or zinc supplementation on motor or language milestones (Surkan 2013) and supplementations findings in general have been inconsistent (Siegel 2011).
Anaemia due to chronic inflammation is the second most prevalent form of anaemia after iron deficiency (Weiss 2005). Chronic inflammation may itself drive iron deficiency through hepatic production of the hormone hepcidin (Drakesmith 2012), which reduces iron absorption and diverts iron from the circulation into macrophages. Chronic inflammation may also affect iron utilisation by other target tissues critical for child development. Lack of adequate toilet facilities has been shown in one study to be a risk factor for anaemia in women of reproductive age in Tanzania (Wilunda 2013). Given that EED, stunting and anaemia appear to be linked through the process of chronic inflammation, it is therefore plausible that interventions to ameliorate these coexisting pathologies may improve early child development.
Helminths and early child development
Soil‐transmitted helminth and schistosome infections often occur in the same geographical areas as malnutrition and poor WASH facilities, causing worsening of malnutrition, anaemia, and other nutrient deficiencies (Stephenson 1994). For example, hookworm infection reduces the work capacity and productivity of children and adults and increases maternal and fetal morbidity, as well as susceptibility to other infections (Stephenson 1994). The eradication of hookworm in the American South has been linked to improved school attendance and literacy (Bleakley 2007). Although the treatment was in mothers, a recent randomised controlled trial of anti‐helminthic treatment in pregnant women showed a small but significant effect of 2 worm species on children’s cognitive development at 15 months in Uganda (Nampijja 2012).
A recent systematic review of randomised controlled trials of helminth eradication showed slight benefits for weight, but was inconclusive for cognitive development (Taylor‐Robinson 2012). Subsequent to this, the DEVTA trial showed no benefit of widespread helminth eradication on child mortality (Awasthi 2013). Measurement of cognitive development is complex and often difficult to compare across studies using different assessment tools. Sanitation interventions have been shown to decrease soil‐transmitted helminth infection in a meta‐analysis (Ziegelbauer 2012), whilst water treatment and hygiene interventions also have some effect (Strunz 2014). Therefore this is another potential mechanism for improving child cognitive development (Ezeamama 2005).
WASH interventions in schools
Some studies have demonstrated that malnutrition affects school enrolment (Glewwe 1995), whilst school‐based WASH interventions improve attendance (Master 1997), particularly among girls in developing countries (Freeman 2012). A school‐based handwashing program has been shown to decrease both absenteeism and length of absence (Bowen 2007). Preschool handwashing education programs have also demonstrated improved handwashing practice although not a reduction in preschool absenteeism (Rosen 2006). Improvement and maintenance of facilities is also key to reducing episodes of illness (Koopman 1978). The school remains an important source for behaviour change and knowledge on WASH interventions in older children (Blanton 2007; Jasper 2012; Joshi 2013). However, the predominant impact on early child nutrition and development is likely to be prior to school age.
Why it is important to do this review
There has been no systematic review to date of the available evidence for WASH interventions on child development (Spears 2013). Synthesis of the evidence will help to interpret existing research findings and underpin future studies, and will inform policy in the health, education and WASH sectors (Britto 2016). The aim of this review is to examine the best available evidence linking specific WASH interventions to child development by undertaking a systematic review of both published and unpublished evidence from low‐ and middle‐income countries.
Objectives
Main objective
The main objective is to assess the effect of interventions to improve sanitation, hygiene, water quality and supply within low‐ and middle‐income countries on child development.
Secondary objectives
The secondary objectives are to:
-
analyse any measured effect of water, sanitation and hygiene (WASH) interventions on school or preschool enrolment and attendance;
-
examine the feasibility of WASH interventions with regard to their implementation fidelity and participant compliance;
-
evaluate the effect of WASH interventions on intermediary outcomes of environmental contamination, gastrointestinal diseases and reduction in the burden of water collection and water costs; and
-
identify any adverse impact that WASH interventions may have for participants.
Methods
Criteria for considering studies for this review
Types of studies
Studies will be included according to the Effective Practice and Organisation of Care (EPOC) study design criteria (EPOC 2015). Both published studies and protocols of planned/ongoing studies will be considered.
Inclusion criteria
Only studies with a clearly described intervention and concurrently enrolled control group will be eligible for inclusion in the review. Eligible study designs include: randomised trial, cluster‐randomised and quasi‐randomised controlled trials. Also included will be controlled before‐after (CBA) studies, where observations are made before and after the implementation of an intervention, where there is a control group that does not receive it. Interrupted time series (ITS) studies, which use observations at multiple points before and after an intervention, will be included (providing at least three measurement points before and after an intervention are measured). ITS are designed to detect whether the intervention has had an effect significantly different from the general trend. Finally, repeated measures studies (RMS) will be included; these are similar to ITS but the measurements are made in the same individuals at each time point.
Exclusion criteria
We will exclude: case series, case reports, case‐control studies, cross‐sectional studies, simulation studies and outbreak investigations. Studies that do not have both a WASH intervention and a measure of child development or cognitive development or school attainment will be excluded.
Types of participants
Inclusion criteria
Children younger than 18 years of age in low‐ and middle‐income countries (including those countries that made the transition to high‐income country status after the study was conducted). The inclusion criteria includes children up to 18 years of age because of the potential impact of WASH interventions on important educational outcomes (e.g. literacy and numeracy) that would not be detected below 5 years of age. Countries will be defined according to World Bank statistics of gross national income (GNI) per capita, and will also include previous names of countries such as Zaire, USSR, etc.
Exclusion criteria
Studies that include participants older than 18 years or exclusively from high‐income countries. Studies that only report on a child subgroup will also be excluded.
Types of interventions
Inclusion criteria
Interventions will be defined as those that improve water quality and quantity, as well as sanitation and hygiene interventions. This will be defined as previously reported (Dangour 2013) to include any combination of the household, institutional (e.g. schools) and community‐level interventions listed below.
-
Any intervention aimed at improving water quality, including:
-
preventing, removing or inactivating microbiological pathogens, both at ‘source’ and at ‘point of use’, through treatment (e.g. filtration, sedimentation, chemical treatment, heat treatment, UV radiation); and
-
protecting the microbiological quality of water prior to consumption (e.g. residual disinfection, protected distribution, improved storage).
-
-
Water quantity or supply improvements: interventions to provide any new or improved water supply or distribution system, for example installation of a hand pump, household or local connection or rainwater collection.
-
Sanitation: interventions to provide or promote new or improved sanitation or expand and improve excreta disposal; any intervention that reduces direct and indirect contact with human faeces (e.g. through pour‐flush, composting or water‐sealed flush toilets, piped sewer systems, septic tanks or pit latrines). This also includes improvement to existing facilities such as ventilated improved pit (VIP) latrines or reduction in open defecation such as use of a potty or scoop for disposal of child faeces.
-
Hygiene: interventions to promote handwashing with soap or other agents after defecation, after disposal of child faeces, and prior to preparing and handling food; and/or interventions providing soap or other agents and/or equipment to facilitate handwashing (e.g. handwashing stations, tippy taps). This also includes any educational method (e.g. media campaigns, leaflets, dramas, group discussions).
No minimum duration of intervention will be defined.
Controls
-
Water quality: study participants who continue their usual practice or a reduced version of the intervention (e.g. a new borehole but no household disinfection).
-
Water supply: study participants who have not benefited from additional water and continue with usual practice.
-
Sanitation: study participants who receive a reduced version of a sanitation intervention or who continue to practice open defecation or usual practice of excreta disposal.
-
Hygiene: no hand‐washing or disinfection promotion, with participants who continue with usual practice.
Types of outcome measures
Primary outcomes
The primary outcome for children under five years of age includes any standardised and validated observed, or caregiver‐reported, measure of child development. This includes the measurement of child development in four areas (domains):
a) gross motor: for example how the child walks, crawls, runs, etc;
b) fine motor: for example how the child has fine control of coordination;
c) language and communication: for example how the child talks and responds to language; and
d) social‐emotional components and cognitive outcomes: for example how the child feeds, clothes, engages in play and chores, etc.
It also includes any behavioural outcomes that have standardised and validated tools of measurement, as well as any overall measure of child development.
Only standardised tools that have a total and domain‐specific score as a measure of development will be used in this review. These include validated measures of child development such as Batelle Development inventory, Griffiths, Ages and Stages questionnaire, Bayley III and Malawi Development Assesssment Tool. This should also detect any evidence of developmental delay.
For children over five years, any school‐age measure of cognition, such as validated assessments of literacy, numeracy, school achievement and behavioural outcomes, which provide a standard deviation and effect size, will also be included.
Secondary outcomes
Preschool and school enrolment and attendance will be included as a secondary outcome.
Other secondary outcomes for WASH interventions include:
a) any outcome measure for reduced environmental contamination, decreased enteropathogen exposure or reduced burden of water collection and costs associated with the WASH intervention;
b) any measures of intervention fidelity and participant compliance; and
c) any reported adverse outcomes on participants caused by the WASH intervention.
Ongoing trials will also be described. The review will be undertaken and reported in accordance with the PRISMA statement (Liberati 2009). Where possible, intermediary outcome data will be included which may be used for possible meta‐analysis. From the included studies, any further publications that may have additional implementation information will also be sought.
Exclusion criteria
-
Studies that include a WASH intervention but no measure of child development, cognitive function, school performance, enrolment or attendance.
Search methods for identification of studies
Electronic searches
We will search:
-
Cochrane Central Register of Controlled Trials (CENTRAL);
-
MEDLINE (including In‐Process and Other Non‐Indexed Citations);
-
Web of Science (including Science Citation Index Expanded (SCI‐EXPANDED) 1970 to present; Social Science Citation Index (SSCI) 1970 to present; Conference Proceedings Citation Index‐Science (CPCI‐S) and Social Science & Humanities (CPCI‐SSH) 1990 to present;
-
Embase;
-
Econlit (economics) via EBSCO;
-
Global Health (public health) via EBSCO; and
-
PsycINFO.
MeSH headings will be used in addition to keywords in MEDLINE and EMTREE terms in Embase. We will not restrict the initial search based on language, but any non‐English literature that is found will be analysed on a case‐by‐case basis. To find protocols for planned trials/trials in progress we will search the World Health Organization International Clinical Trials Registry Platform (WHO ICTRP) which is a central database for a number of trials registries including Clinical Trials.gov, controlledtrials.gov, the EU Clinical Trials Register and Pan African Clinical Trials Registry. Databases will all be searched from their start date to the present.
Reference lists and citations of identified studies and review articles will also be scrutinised to find additional relevant studies. Known search strategies for identifying trials will be combined with the keywords as listed in Appendix 1 (Dangour 2013).
Searching other resources
A predefined list of experts in the field will be consulted to identify any potentially‐relevant studies missed by the above search strategy. We will also examine the Community Management of Acute Malnutrition (CMAM) forum, the Food and Nutrition Technical Assistance Project (FANTA) and food and nutrition library. Other grey literature databases such as European Association for Grey Literature via OpenSIGLE for Europe, the Healthcare Management Information Consortium (HMIC) for the UK and the National Technical Information Service (NTIS) (Cochrane 2011) will also be searched.
We will also search the Grey Literature report in public health www.greylit.org, African index Medicus (www.indexmedicus.afro.int) and resources specific to south east Asia (www.imsear.hellis.org) and the western Pacific (www.wprim.org), plus the WHO Virtual Health Sciences Library (www.emro.who.int/information‐resources/vhsl/) and 3ie impact.
Additional data: where possible, we will contact study authors to retrieve original data and any further unpublished results which are relevant.
Also the following (Dangour 2013) will be contacted for appropriate grey literature.
-
Public‐Private Partnership for Handwashing with Soap (www.globalhandwashing.org/)
-
IRC International Water and Sanitation Centre (www.ircwash.org/)
-
World Health Organization (www.who.int/en/)
-
United Nations Children’s Fund (UNICEF) (www.unicef.org.uk/)
-
Department of Maternal, Newborn, Child and Adolescent Health (WHO) (www.who.int/maternal_child_adolescent/en/)
-
Water, Sanitation and Health Programme (WHO) (www.who.int/water_sanitation_health/en/)
-
World Bank (www.worldbank.org/); World Bank Water and Sanitation Programme (water.worldbank.org/related‐topics/water‐and‐sanitation‐program)
-
International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B) (www.icddrb.org/)
-
Environmental Health Project (USAID) (www.ehproject.org/) and USAID (http://www.usaid.gov/)
-
Foodborne and Diarrheal Diseases Branch, Centers for Disease Control and Prevention (CDC) (www.cdc.gov/ncezid/dfwed/)
-
UK Department for International Development (DFID) (www.dfid.gov.uk/)
-
Action Contre la Faim (www.actioncontrelafaim.org/en/)
-
Water and Sanitation Program (www.wsp.org/)
-
Wateraid (www.wateraid.org/uk/)
Data collection and analysis
Selection of studies
Two authors (JP and JC) will review the titles and abstracts retrieved through the search strategy independently to identify and select potentially‐relevant studies using the predefined inclusion criteria, and the full text of all articles will then be retrieved for a full text review. References will be extracted independently by JP and JC for each included study and will be exported to EndNote X7, with duplicates identified and removed. Two authors (JP and JC) will make an initial assessment of suitability from the article title, then two authors (JP and JC) will review the summaries independently to determine study eligibility. If there is a difference of opinion, disagreement will be resolved through discussion with a third review author (OC). We will use a PRISMA flow chart to describe the results found.
All studies that initially appear to meet the inclusion criteria but upon reading the full text do not will be detailed in the 'Characteristics of excluded studies' table with reasons for exclusion. Where possible, authors will be contacted to see if there are additional data relating to child development outcomes from these studies.
Data extraction and management
Two authors (JP and JC) will independently extract data from all relevant articles, and will then contact authors to supply missing data where possible. Data extraction forms will be based on the Cochrane Public Health Group and EPOC Group 'Good practice data extraction form', modified for this study. The data extraction form will be piloted by all authors to ensure comparable results are retrieved. Any discrepancies will be resolved by a third author (OC). Data will be entered into Review Manager 5.3.5. Below is a brief description of the categories of data that will be collected.
-
Publication details: First author, title, publication date, journal, volume, issue, page numbers
-
Population characteristics: country, setting, number, gender percentage, other relevant sociodemographic variables, ages of recruitment, intervention and measurement, length of follow up, measure of socioeconomic status (if available), parental education and employment (if available)
-
Intervention characteristics: WASH intervention, type of randomisation, control group details
-
Outcome: measure of child development/school attainment, (P values, confidence intervals and standard errors of effect if available), additional results on nutritional outcomes if available: weight, height, growth velocity and head circumference
-
Assessment of methodological quality: study type and size, confounding variables and attempts to correct for them, blinding and allocation concealment
-
Implementation factors: quantitative fidelity to measure the degree to which any intervention is delivered as intended, participant compliance to assess the extent any behaviour change occurred, intervention and monitoring, costs and sustainability data, if available
-
Source of funding of study
All potential confounders of study outcomes will be included in the data extraction form. Where a single study of effectiveness provides data at multiple points in time or on multiple similar outcomes, this will be analysed within the same study and related outcome. A standard approach will be used where comparisons of multiple reports and publications of the same study will be checked to ensure data are only used once. Authors of primary studies will be contacted where information is needed. RevMan 5.3.5 will be used to manage data storage and analysis.
Assessment of risk of bias in included studies
Two authors (JP and JC) will independently assess the risk of bias of included studies. This will be using the EPOC 'Risk of bias' tool for studies with a separate control group (EPOC 2015). This tool includes assessment of allocation, baseline characteristics, baseline outcome, incomplete outcome data, blinding, selective outcome reporting and contamination of the treatment groups. It also contains additional items to assess the risk of incomplete data, selection bias, attrition bias and subsequent confounding. For non‐randomised studies, there are also items that assess the risk of selection bias and subsequent confounding. For interrupted time series (ITS) studies, the EPOC 'Risk of bias' tool for ITS study designs will be used. This assesses performance, attrition, detection and reporting bias as well as the ITS‐specific items:
-
was the intervention independent of other changes?
-
was the shape of the intervention effect prespecified? and
-
was the intervention likely to affect data collection?
Studies will be assessed for bias with an answer of 'low', 'unclear' or 'high' risk of bias, and supporting information will be included in the 'Risk of bias' tables. Where possible, study authors will be contacted for additional information. Any discrepancies will be resolved by a third author (OC).
Risk of bias will also be summarised at the outcome level with an overall risk of bias level of ‘low’, ‘medium’ or ‘high’ from the risks noted in the table for each study.
Measures of treatment effect
Measures of difference in treatment effect (i.e. between the post‐intervention values of both the intervention and control groups) will be presented as a mean difference for continuous outcomes and recorded using their original scale. Means or changes in mean scores of development studies or school assessments will be recorded. It is likely that studies will use different scales, so standardised mean differences will be reported. All measures of effect will be presented with 95% confidence intervals (CI).
Measures of difference in treatment effect (i.e. between the post‐intervention values of both the intervention and control groups) will be presented as a risk ratio for binary outcomes.
Unit of analysis issues
If studies with multiple intervention groups are encountered, the overall effects of the intervention versus the control (means and SDs) will be examined by pooling the effects of the intervention versus control and weighting the overall values for the numbers in each arm. Care will be taken not to include the same participants twice in the same meta‐analysis; if necessary, the control group participants will be divided. Data from non‐randomised trials will not be pooled with those from randomised controlled trials.
Cluster randomised trials will be identified in the review and when necessary and possible they will be re‐analysed to take into account the clustered nature of the design. Where appropriate, cluster randomised trials will be combined with individually randomised trials in the same meta‐analysis (Cochrane 2011).
Dealing with missing data
Authors of included studies will be contacted to request any missing information if data are unclear or not fully reported and to obtain unpublished trial protocols where available; if the information cannot be obtained this will be reflected in the 'Risk of bias' table. We will record all completion rates of both the intervention and outcomes and classify them according to completion. Missing data will not be imputed.
Assessment of heterogeneity
Heterogeneity will be assessed by exploration of the forest plots and estimated using the I2 statistic according to the Cochrane Handbook (Cochrane 2011). We are planning a random‐effects meta‐analysis, where we plan to generate and report the I2 value as a measure of the heterogeneity. Clinical heterogeneity will be explored by examination of the baseline characteristics, such as socioeconomic status, age, gender, comorbidities, household size and initial WASH facilities. As we are planning a random‐effects meta‐analysis, any heterogeneity will be further explored in the individual patient data analysis that would allow for adjustment in the analysis.
Assessment of reporting biases
Where possible, we will attempt to find any WASH studies that collected but did not report developmental measures. Assessment of reporting bias will also be attempted by using funnel plots if a reasonable number of studies is found. If there are more than 10 studies, statistical tests of reporting bias will be attempted (Cochrane 2011).
Data synthesis
The available evidence will be synthesised narratively and where possible, statistically. We will report all statistically significant and non‐significant outcomes according to type of study design. If meta‐analysis is possible, data synthesis of study outcomes by group (WASH intervention and control) will be performed using RevMan 5.3.5. A random‐effects model meta‐analysis will be carried out. A forest plot with appropriate effect sizes and 95% confidence intervals will be provided for each analysis along with a measure of heterogeneity (I2). A pooled analysis of all WASH interventions will be performed.
If a narrative synthesis is performed due to lack of appropriate data, then studies will be compared that have similar subgroups of age and low‐ or middle‐income country as discussed later. If there are sufficient studies, they will also be grouped by the type of WASH intervention.
For either narrative or quantitative analysis, the review findings will be summarised by the GRADE considerations (see 'Certainty of the evidence' below) to assess the quality of the evidence for each outcome. This will be combined with the magnitude of the effect found to inform the strength of any policy recommendations. All assessments will be documented, together with a ‘Summary of findings’ table, which will include the evidence for each type of WASH intervention, the effect on different measures of child development, and any other effect on school achievement.
The child development outcomes of most importance, which will be presented in a 'Summary of findings' table, are as follows.
-
Overall child development (summative score)
-
Language and communication
-
Social‐emotional components and cognitive outcomes
-
Fine motor
-
Gross motor
-
School literacy and numeracy
-
School enrolment/attendance
Within these, it is difficult to categorise importance because developmental domains do not function as discrete entities but influence each other (Sabanathan 2015). However, whilst correlations between motor tests and later child achievement are variable (Roze 2010), language development has been shown as more closely linked to school achievement (Roze 2010). Oral language may serve as a foundation for later literacy (Network 2005).
Any child development assessment generally gives only a snapshot of the child at that time point and the age of the child development assessment may also affect the strength of the findings (Sabanathan 2015). In low‐income countries, it has been shown that stability and predictive validity are poor below 24 months, but improve after 24 months of age (Pollitt 1999). For younger children, any developmental delay found may also be less reliable than at a later age: for example, preterm children with developmental delay at age 2 years have been shown to have a variety of developmental trajectories (with some catching up and others developing further difficulties). Therefore assessment of outcomes at a later age (over 5 years) may be more reliable (Roberts 2010). Hence for primary outcomes, language outcomes are more predictive, as are outcomes measured at a later age.
School literacy and numeracy may be more linked with longer‐term outcomes than earlier developmental outcomes (Currie 1999; Victora 2008; Martorell 2010b). They may also include the beneficial effects of catch‐up growth and development (Crookston 2013).
To assess the strength of the findings, it will be important to assess the quality of the child development tools used, by noting how they were developed, validated and maintained with any quality control (Fernald 2009). For a new test, it is important that its psychometric properties were analysed in detail by an interdisciplinary team, which included local expertise and bilingual psychologists. The new instrument should have shown a broad psychometric domain and applicability to the group being measured, including sufficient piloting with a representative sample, which would also develop norms and standards (Fernald 2009). For a local adaption of existing tests, it is important that sufficient translation and back‐translation and checking of cultural and functional equivalence was performed, again using similar input from local psychologists and the community. Adaption of tests also requires sufficient piloting and further modifications to establish local norms and standards for validity (Fernald 2009). For all tests, the assessors need to be adequately trained and monitored with interrater reliability and accuracy testing performed.
Where available, the typical burden of each outcome in the control population will be stated. When appropriate, both the absolute and relative magnitude of effect on each outcome will be included. The number of participants and number of studies addressing these outcomes will be included. A grade for the overall quality of the body of evidence for each outcome will be provided and any other relevant comments will be noted.
Certainty of the evidence
We will assess evidence for each outcome (primary and secondary outcomes reported) as very low, low, moderate or high quality by considering the GRADE domains and these assessments will be reported alongside the outcomes findings, where appropriate in the 'Summary of findings' table (for primary outcomes) abstract, plain language and main text of the review. Table 1 presents definitions for these ratings (Balshem 2011). The GRADE approach to rating the quality, or certainty, of evidence begins with the study design (randomised trials start as high quality, observational studies generally start as low) and then addresses five reasons to possibly downgrade the quality of evidence (Balshem 2011). GRADE criteria for downgrading certainty of evidence encompass study limitations, inconsistency, imprecision, indirectness, publication bias, and other considerations (Balshem 2011). If a criterion exists, it is classified either as serious (leading to downgrading by one level) or very serious (downgrading by two levels).
| Quality level | Definition |
| High ++++ | We are very confident that the true effect lies close to that of the estimate of the effect. |
| Moderate +++ | We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. |
| Low ++ | Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. |
| Very low + | We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. |
Subgroup analysis and investigation of heterogeneity
A subgroup analysis by age group will be performed, with subgroups of less than 5years and 5 to 18 years. This is to separate earlier child development from later measures of child development, including school attendance, literacy and numeracy. School‐age neurodevelopment may also be more predictive than preschool development, on longer‐term outcomes. Subgroup analysis by gender will be performed to capture the potential differential effects of WASH interventions on developmental and school outcomes between boys and girls.
A subgroup analysis by country type will be performed, with subgroups of low‐income and middle‐income countries. Low‐income countries may have a stronger direct association between poor WASH infrastructure and child development compared to middle‐income countries (Bowen 2012; McCoy 2016), which may have relatively better WASH facilities and access to health care, with less exposure to gut pathology and burden of water collection (see Figure 1 conceptual framework). Hence there may be a greater effect of other factors such as educational facilities, maternal education and socioeconomic inequality (Walker 2011a; Rubio‐Codina 2015; Black 2016). Therefore countries will be separated between low‐ and middle‐income based on their World Bank definition (Nielsen 2011; World Bank 2016).
Data for this are clearly available from 1987. Before this, the classification is less clearly defined although the original low‐income country GNI of 250 dollars in 1976 is a useful benchmark (Nielsen 2011). For any historical studies found prior to World Bank classification, a judgement will be based on the location and the country’s economic status at that time and recorded in the analysis.
If sufficient data are available, further subgroup analyses will also be performed for the individual WASH interventions of water quality, water quantity, sanitation and hygiene measures. If possible, we will stratify by subintervention to explore any variation in effects. For example, this could be examining the difference between onsite and offsite sanitation intervention. If there are enough data, then the duration of follow‐up and context of urban/rural location or by continent can be explored.
Sensitivity analysis
We plan to conduct a sensitivity analysis by restricting the analysis to trials classified as having low risk of bias overall.
Interrupted time series (ITS) data analysis
If available, then ITS data on child development that are collected at multiple time points (at least three measurements before and after the WASH intervention, as recommended in the EPOC guide) would be included, as stated previously (Dangour 2013; Wolf 2014). ITS may be useful for large‐scale interventions when it is difficult to identify a control group, however they remain sensitive to confounding effects that occur at the same time, and are not randomised (Eccles 2003). If available, a statistical analysis of time trends before and after the WASH intervention will be performed. If there are enough observations, adjustment for autocorrelation and seasonality will also be undertaken.
Controlled before‐after (CBA) studies
If available, data from CBA studies of WASH effects on child development will be included, although this type of study also remains vulnerable to confounding.
Outcomes included will be those that measure child development. We are uncertain at present whether the results can be combined into a meta‐analysis. Any discrepancies regarding study inclusion or data handling will be discussed between JP and JC and referred to OC if no consensus is reached.
Individual patient data (IPD) analysis
We plan to carry out an IPD analysis of all randomised controlled trials included in the aggregate data meta‐analysis. The main author of the trials will be contacted and asked to provide IPD, which will be collated into a database. Authors will be provided with a list of required data elements. We will carry out checks on the data and clarify any discrepancies with the authors. These will include range checks and checking that tabulations correspond to values in original publication.
The outcomes will be the same as for the aggregated meta‐analysis and we will estimate the effects of the interventions on outcomes using appropriate regression models adjusting for baseline measures of the continuous outcomes and other covariates where possible. The analysis will use random‐effects models to allow for both within‐study and within‐cluster variability, where cluster is the unit of randomisation in each study. Heterogeneity of treatment effects across trials will be tested by including a random slope for the intervention. Children with missing data will be removed from the analysis. We will pool the data from studies with more than one intervention arm to allow comparison of outcome of children in intervention and control arms. The IPD analysis will be conducted on an intention‐to‐treat basis.
Subgroup effects will be estimated by estimating treatment multiplied by covariate interaction terms in the models.
Conceptual framework showing plausible associations between water, sanitation and hygiene (WASH) interventions and gut pathology, nutrition/inflammation, socioeconomic/maternal, home/school environment domains and delayed child development.
| Quality level | Definition |
| High ++++ | We are very confident that the true effect lies close to that of the estimate of the effect. |
| Moderate +++ | We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. |
| Low ++ | Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. |
| Very low + | We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. |