Factors that influence the provision of intrapartum and postnatal care by skilled birth attendants in low‐ and middle‐income countries: a qualitative evidence synthesis
Abstract
Background
In many low‐ and middle‐income countries women are encouraged to give birth in clinics and hospitals so that they can receive care from skilled birth attendants. A skilled birth attendant (SBA) is a health worker such as a midwife, doctor, or nurse who is trained to manage normal pregnancy and childbirth. (S)he is also trained to identify, manage, and refer any health problems that arise for mother and baby. The skills, attitudes and behaviour of SBAs, and the extent to which they work in an enabling working environment, impact on the quality of care provided. If any of these factors are missing, mothers and babies are likely to receive suboptimal care.
Objectives
To explore the views, experiences, and behaviours of skilled birth attendants and those who support them; to identify factors that influence the delivery of intrapartum and postnatal care in low‐ and middle‐income countries; and to explore the extent to which these factors were reflected in intervention studies.
Search methods
Our search strategies specified key and free text terms related to the perinatal period, and the health provider, and included methodological filters for qualitative evidence syntheses and for low‐ and middle‐income countries. We searched MEDLINE, OvidSP (searched 21 November 2016), Embase, OvidSP (searched 28 November 2016), PsycINFO, OvidSP (searched 30 November 2016), POPLINE, K4Health (searched 30 November 2016), CINAHL, EBSCOhost (searched 30 November 2016), ProQuest Dissertations and Theses (searched 15 August 2013), Web of Science (searched 1 December 2016), World Health Organization Reproductive Health Library (searched 16 August 2013), and World Health Organization Global Health Library for WHO databases (searched 1 December 2016).
Selection criteria
We included qualitative studies that focused on the views, experiences, and behaviours of SBAs and those who work with them as part of the team. We included studies from all levels of health care in low‐ and middle‐income countries.
Data collection and analysis
One review author extracted data and assessed study quality, and another review author checked the data. We synthesised data using the best fit framework synthesis approach and assessed confidence in the evidence using the GRADE‐CERQual (Confidence in the Evidence from Reviews of Qualitative research) approach. We used a matrix approach to explore whether the factors identified by health workers in our synthesis as important for providing maternity care were reflected in the interventions evaluated in the studies in a related intervention review.
Main results
We included 31 studies that explored the views and experiences of different types of SBAs, including doctors, midwives, nurses, auxiliary nurses and their managers. The included studies took place in Africa, Asia, and Latin America.
Our synthesis pointed to a number of factors affecting SBAs’ provision of quality care. The following factors were based on evidence assessed as of moderate to high confidence. Skilled birth attendants reported that they were not always given sufficient training during their education or after they had begun clinical work. Also, inadequate staffing of facilities could increase the workloads of skilled birth attendants, make it difficult to provide supervision and result in mothers being offered poorer care. In addition, SBAs did not always believe that their salaries and benefits reflected their tasks and responsibilities and the personal risks they undertook. Together with poor living and working conditions, these issues were seen to increase stress and to negatively affect family life. Some SBAs also felt that managers lacked capacity and skills, and felt unsupported when their workplace concerns were not addressed.
Possible causes of staff shortages in facilities included problems with hiring and assigning health workers to facilities where they were needed; lack of funding; poor management and bureaucratic systems; and low salaries. Skilled birth attendants and their managers suggested factors that could help recruit, keep, and motivate health workers, and improve the quality of care; these included good‐quality housing, allowances for extra work, paid vacations, continuing education, appropriate assessments of their work, and rewards.
Skilled birth attendants’ ability to provide quality care was also limited by a lack of equipment, supplies, and drugs; blood and the infrastructure to manage blood transfusions; electricity and water supplies; and adequate space and amenities on maternity wards. These factors were seen to reduce SBAs’ morale, increase their workload and infection risk, and make them less efficient in their work. A lack of transport sometimes made it difficult for SBAs to refer women on to higher levels of care. In addition, women’s negative perceptions of the health system could make them reluctant to accept referral.
We identified some other factors that also may have affected the quality of care, which were based on findings assessed as of low or very low confidence. Poor teamwork and lack of trust and collaboration between health workers appeared to negatively influence care. In contrast, good collaboration and teamwork appeared to increase skilled birth attendants’ motivation, their decision‐making abilities, and the quality of care. Skilled birth attendants’ workloads and staff shortages influenced their interactions with mothers. In addition, poor communication undermined trust between skilled birth attendants and mothers.
Authors' conclusions
Many factors influence the care that SBAs are able to provide to mothers during childbirth. These include access to training and supervision; staff numbers and workloads; salaries and living conditions; and access to well‐equipped, well‐organised healthcare facilities with water, electricity, and transport. Other factors that may play a role include the existence of teamwork and of trust, collaboration, and communication between health workers and with mothers. Skilled birth attendants reported many problems tied to all of these factors.
Plain language summary
What factors influence the delivery of care by skilled birth attendants in low‐ and middle‐income countries?
Review aim
The aim of this Cochrane synthesis of qualitative evidence was to identify factors that influence the provision of care by skilled birth attendants. To answer this question, we searched for and analysed qualitative studies of skilled birth attendants’ views, experiences, and behaviour.
This synthesis complements another Cochrane Review assessing the effect of strategies to promote women’s use of healthcare facilities when giving birth.
Key messages
Many factors influence the care that skilled birth attendants provide to mothers during childbirth. These include access to training and supervision; staff numbers and workloads; salaries and living conditions; and access to well‐equipped, well‐organised healthcare facilities with water, electricity, and transport. Other factors that may play a role include the existence of teamwork, trust, collaboration, and communication between health workers and with mothers. Skilled birth attendants reported many problems tied to these factors.
What did we study in the synthesis?
In low‐ and middle‐income countries, many mothers still die during childbirth. Women are encouraged to give birth in health facilities rather than at home so they can receive care from skilled birth attendants. A skilled birth attendant is a health worker such as a midwife, doctor, or nurse who is trained to manage a normal pregnancy and childbirth, and refer the mother and newborn when complications arise.
By exploring skilled birth attendants’ views, experiences, and behaviour, this synthesis aimed to identify factors that can influence their ability to provide quality care.
Main findings
We included 31 studies conducted in Africa, Asia, and Latin America. Participants were skilled birth attendants including doctors, midwives, nurses, auxiliary nurses and their managers.
Our synthesis pointed to several factors that affected skilled birth attendants’ provision of quality care. The following factors are based on evidence assessed as of moderate to high confidence. Skilled birth attendants reported that they sometimes had insufficient training during their education or after they had begun work. Where facilities lacked staff, skilled birth attendants’ workloads could increase, it could become difficult to provide supervision, and mothers could receive poorer care. In addition, skilled birth attendants did not always believe that their salaries and benefits reflected their tasks and responsibilities and the personal risks they undertook. Together with poor living and working conditions, these issues could lead to stress and affect skilled birth attendants' family life. Some skilled birth attendants felt that managers lacked capacity and skills, and they felt unsupported when their workplace concerns were not addressed.
Possible causes of staff shortages included problems with hiring and assigning health workers to health facilities; lack of funding; poor management and bureaucratic systems; and low salaries. Skilled birth attendants and their managers suggested factors that could help recruit, keep, and motivate health workers, and improve the quality of their work; these included good‐quality housing, allowances for extra work, paid vacations, continued education, proper assessments of their work, and rewards.
Skilled birth attendants’ ability to provide quality care was also limited by a lack of equipment, drugs, and supplies; blood and the infrastructure to manage blood transfusions; electricity and water supplies; and adequate space and amenities on maternity wards. These factors were seen to reduce skilled birth attendants’ morale, increase their workload and infection risk, and make them less efficient in their work. A lack of transport sometimes made it difficult for skilled birth attendants to refer women to higher levels of care. In addition, women’s negative perceptions of the health system could make them reluctant to accept referral.
We identified some other factors that also may have affected the quality of care, which were based on findings assessed as of low or very low confidence. Poor teamwork and lack of trust and collaboration between health workers appeared to negatively influence care. In contrast, good collaboration and teamwork appeared to increase skilled birth attendants’ motivation, their decision‐making abilities, and the quality of care. Skilled birth attendants’ workloads and staff shortages influenced their interactions with mothers. In addition, poor communication undermined trust between skilled birth attendants and mothers.
How up‐to‐date is this review?
We searched for studies published before November 2016.
Authors' conclusions
Summary of findings
| Summary of review finding | Studies contributing to the review finding | CERQual assessment of confidence in the evidence | Explanation of CERQual assessment |
| SOCIOCULTURAL | |||
| Sociocultural barriers sometimes hindered mothers from receiving care in hospitals. For instance, women preferred not to be examined by male health providers, or for cultural reasons preferred a particular position in which to deliver, or for religious reasons did not divulge information that was needed for their care. | Low confidence | Due to moderate concerns about adequacy; and moderate concerns about relevance | |
| PROFESSIONAL ASSOCIATIONS | |||
| Health workers had conflicting views on the role of professional councils. For instance, some viewed professional councils as advocates for their members, while others viewed them as a regulatory body with punitive functions. | Very low confidence | Due to moderate concerns about methodological quality; and moderate concerns about relevance; and severe concerns about adequacy | |
| HUMAN RESOURCES | |||
| Staff shortage was a widely reported problem and led to increased workloads, which in turn compromised quality of care. For instance, heavy workload limited health worker time for history taking and thorough assessment of women, and hand hygiene was sometimes compromised. Staff shortages and work overload jeopardised health workers’ ability to provide timely care, and manage routine care as well as emergency cases. In addition, shortage of staff sometimes led health workers to exceed their scope of practice, and influenced a health facility's ability to provide 24‐hour care. | Afsana 2001; Anwar 2009; Barua 2011; Bradley 2009; Conde‐Agudelo 2008; Fränngård 2006; Fujita 2012; Graner 2010; Hassan‐Bitar 2011; Ith 2012; Khalaf 2009; Lugina 2001; Maputle 2010; Mathole 2006; Mondiwa 2007; Spangler 2012; Thorsen 2012; VSO 2012 | Moderate confidence | Due to minor concerns about coherence; and minor concerns about methodological limitations |
| A lack of specialists or experienced staff, including absence of health workers with key skills such as anaesthetists, influenced the provision of care and supervision of junior staff. When no specialists were available, some tasks such as emergency obstetric care were not delivered at all, or tasks were transferred to health workers who were not properly qualified or trained to deliver them. When senior experienced health workers were not available, junior health workers lacked supervision. | Afsana 2001; Anwar 2009; Blum 2006; Bradley 2009; De Brouwere 2009; Fränngård 2006; Hassan‐Bitar 2011; Khalaf 2009; Penfold 2013; Pitchforth 2010; Spangler 2012; VSO 2012 | Moderate confidence | Due to moderate concerns about methodological limitations |
| Health workers had vague job descriptions that sometimes led them to perform tasks that were beyond their expertise or scope of practice. | Very low confidence | Due to minor concerns about methodological limitations; and serious concerns about relevance and adequacy | |
| Staff shortages and work overload could jeopardise health workers’ ability to display support, empathy, and friendliness to women in labour. | Very low confidence | Due to minor concerns about methodological limitations; and moderate concerns about relevance and adequacy | |
| Staff shortages and increased workload, as well as living and work conditions, sometimes caused stress and frustration, affected health workers' family life, and led to concerns about personal safety. | Anwar 2009; Blum 2006; Fränngård 2006; Graner 2010; Lester 2003; VSO 2012 | Moderate confidence | Due to moderate concerns about methodological limitations; and minor concerns about relevance and adequacy |
| A wide range of interlinked reasons for staff shortages were suggested. These included limited funds to recruit health workers; bureaucratic processes of the recruitment process, e.g. absence of committees responsible for recruitment at the district level; scarcity of health workers especially in rural areas; and other factors that deterred retention of health workers (see finding on factors affecting recruitment, Table 1). In addition, institutional arrangements, e.g. when health facilities hired contract staff in order to reduce labour costs, and inefficient deployment of available staff sometimes created staff shortages. Facilities with staff shortages and work overload were viewed as unattractive places to work, and made it difficult for managers to transfer staff from well‐served to underserved areas, thus compounding/increasing the problem. | Anwar 2009; Graner 2010; Molina 2011; Pitchforth 2010; VSO 2012 | Moderate confidence | Due to moderate concerns about adequacy; and minor concerns about relevance and methodological limitations |
| Health workers' salaries and benefits were considered insufficient for the work done, the responsibility and personal risk, and the additional responsibilities assigned, e.g. through informal task‐shifting. In addition, salaries were insufficient for their personal needs, e.g. to send their children to school and for transport costs to visit their husbands. | Anwar 2009; Belizan 2007; De Brouwere 2009; Fränngård 2006; Graner 2010; Hassan‐Bitar 2011; Ith 2012; Molina 2011 | Moderate confidence | Due to moderate concerns about methodological limitations; and minor concerns about relevance and adequacy |
| Factors reported by health workers or their managers to influence recruitment, retention, motivation, or performance of health workers were: good‐quality accommodation for health workers provided by government, allowances for extra project‐related work, paid vacations for 1 month of the year, improved access to and funding for continued education/in‐service training, career progression, non‐biased evaluations or performance‐related rewards or promotions, e.g. for those doing better, working longer, or taking on added responsibilities, and verbal recognition by supervisors and management. The following factors were reported as discouraging health workers from working in rural or remote health facilities: facilities that lacked good equipment and did not provide sufficient work needed to maintain clinical skills, lack of family amenities, limited opportunities for private practice, lack of electricity, TV, or internet, coupled with poor roads and lack of transport deterred health workers from undertaking rural employment. In addition, interference in treatment decisions by local politicians and mismanagement of posting and transfer from the national level were demotivating to health workers working in rural facilities. | Anwar 2009; Bradley 2009; De Brouwere 2009; Fränngård 2006; Hassan‐Bitar 2011; Ith 2012; VSO 2012 | Moderate confidence | Due to minor concerns for methodological limitations and relevance |
| Health workers perceived managers as lacking in management capacity and skills and sometimes felt unsupported. Health workers also complained that concerns about the workplace were sometimes left unheard, and no solutions or feedback given. | Anwar 2009; Bradley 2009; Ith 2012; Lester 2003; Mondiwa 2007; VSO 2012 | Moderate confidence | Due to moderate concerns about relevance; and minor concerns about methodological limitations and adequacy |
| Helping women access financial assistance for out‐of‐pocket payments was sometimes time‐consuming for health workers. | Very low confidence | Due to serious concerns about relevance and adequacy | |
| HEALTH WORKER EDUCATION AND TRAINING | |||
| Inadequate pre‐service and in‐service training sometimes limited health workers' skills and ability to provide care. For instance, some health workers lacked training to attend home births or manage complicated pregnancies or deliveries, e.g. eclampsia or HIV in pregnancy. In contrast, training allowed midwives to practice assisting women to deliver in non‐supine positions and enabled them to get accustomed to this practice. | Afsana 2001; Barua 2011; Blum 2006; DeMaria 2012; Fujita 2012; Graner 2010; Lester 2003; Mathole 2006 | High confidence | ‐ |
| Health worker competencies and opportunities for on‐the job training were sometimes limited by poor scheduling of in‐service education sessions, high cost of continuing education for health workers, inequitable selection for professional development opportunities, lack of ongoing training and follow‐up, and shortage of instructors for upgrading courses. In addition, the variation in quality of pre‐service training resulted in varying levels of need for in‐service training, and these needs were not always met, resulting in wide variation in proficiency among health workers. | Moderate confidence | Due to minor concerns about methodological limitations and relevance; and moderate concerns about adequacy | |
| Learning through practical application facilitated acquisition of skills and confidence. The experience gained through, for example, internship, social service year, and working in the community, was identified as important for building doctors' and midwives' practical experience and confidence in providing care. | Very low confidence | Due to moderate concerns about methodological limitations and relevance; and severe concerns about adequacy | |
| Health workers reported several barriers to implementing recommended practice. Firstly, health workers were sometimes unaware of current recommended effective practices. Secondly, health workers' flexibility, attitudes, and beliefs about medical knowledge and skills sometimes influenced their receptivity to new practice knowledge. For example, health worker attitudes did not view medical education as dynamic; held beliefs that no significant progress had been made and clinical practice was similar to techniques learnt many years ago; or were not flexible or willing to implement alternative positions of delivery, even though these were preferred by women. | Low confidence | Due to moderate concerns about relevance and adequacy | |
| Lack of time, infrastructure, and skills limited health workers' ability to seek knowledge and practice new clinical skills. For instance, chronic staff shortages meant less time available for health workers to seek information. This was sometimes further compounded by lack of information sources such as internet access, and poorly resourced hospital libraries. In addition, lack of training and skills in networking, epidemiology, research appraisal, or critical thinking about clinical practice limited health workers' awareness and receptivity to clinical practice changes, and this lack of skills led some professionals to prefer old, familiar procedures. | Low confidence | Due to moderate concerns about relevance and adequacy; and minor concerns about methodological limitations | |
| STANDARDS AND PROTOCOLS | |||
| Lack of guidelines/protocols, or where they were inconsistent or health workers were not aware or were uncertain of them, could impact patient care and outcomes and cause harm. | Barua 2011; de Carvalho 2012; Khalaf 2009; Lugina 2001; Mathole 2006 | Low confidence | Due to moderate concerns about adequacy; and minor concerns about methodological limitations |
| Health workers did not always adhere to protocols/guidelines, even when they were aware of them. Guidelines/protocols were not followed for a number of reasons. Some health workers felt that guidelines were insufficient without consensus from staff. Some studies described how health workers continued to practice ineffective procedures because they were considered routine; due to lack of time; because they lacked the autonomy to avoid using what they knew to be inappropriate care; because the resources at the institution were not aligned with the protocols for postpartum care; or when it was unclear who was professionally responsible, e.g. in using the partograph. | Belizan 2007; de Carvalho 2012; Conde‐Agudelo 2008; Molina 2011; Pettersson 2006 | Low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy |
| Health workers sometimes used unnecessary diagnostic tests and did not follow recommended practice when they feared malpractice suits. This fear could lead to practitioners retaining practices they believed were ‘safer’. | Very low confidence | Due to moderate concerns about relevance; serious concerns about adequacy; and minor concerns about methodological limitations | |
| Some health workers did not use recommended interventions when delivering care because of concerns about negative outcomes for the baby or the mother. Examples included the use of magnesium sulphate administered with anaesthesia during Caesarean sections or when monitoring of serum magnesium sulphate levels was not possible. | Very low confidence | Due to moderate concerns about relevance; serious concerns about adequacy; and minor concerns about methodological limitations | |
| Health workers were sometimes reluctant to admit their lack of skills in delivering care for fear of blame and criticisms from managers. This fear of criticism could undermine health worker confidence and performance. | Low confidence | Due to minor concerns about relevance; and moderate concerns about adequacy | |
| COMMODITIES AND HEALTH SERVICES INFRASTRUCTURE | |||
| Insufficient stock and/or lack of drugs such as hydralazine, magnesium sulphate, oxytocin, misoprostol, antiretrovirals, and supplies such as gloves, sometimes influenced the quality of care provided to mothers and their babies. For instance, health workers had to use less effective alternative drugs, e.g. diazepam instead of magnesium sulphate. Lack of supplies sometimes limited good hygiene and practice of aseptic techniques, resulting in unsafe practices, e.g. reuse of disposable gloves could increase the risk of HIV infection. Lack of supplies sometimes led to poor outcomes and increased the length of stay in health facilities. Lack of supplies could determine if a new clinical practice was implemented and maintained over time. | Anwar 2009; Belizan 2007; Bradley 2009; de Carvalho 2012; Foster 2006; Fränngård 2006; Graner 2010; Ith 2012; Lester 2003; Mathole 2006; Penfold 2013; Pitchforth 2010; Spangler 2012; VSO 2012 | Moderate confidence | Due to moderate concerns about methodological limitations |
| Lack of drugs or supplies meant mothers or their carers had to purchase their own. This sometimes led to wasted time in procuring the drugs and supplies and the creation of informal markets and corruption at health facilities. | Barua 2011; Foster 2006; Fränngård 2006; Lester 2003; Pitchforth 2010; Spangler 2012; VSO 2012 | Low confidence | Due to moderate concerns about methodological limitations and adequacy; and minor concerns about coherence |
| Lack of equipment limits health workers' ability to deliver quality care to mothers and their babies. As a result of this lack of equipment, mothers and their babies sometimes received poor quality care. | Barua 2011; Fränngård 2006; Graner 2010; Lester 2003; Molina 2011; Penfold 2013; Pettersson 2006; Pitchforth 2010 | High confidence | ‐ |
| Lack of blood or limited infrastructure to manage blood transfusion limited health workers from delivering appropriate care. | Moderate confidence | Due to moderate concerns about adequacy; and minor concerns about relevance | |
| Lack of equipment, supplies, or drugs sometimes wasted health workers' time, increased their workload and risk of infection, and led to low morale. | Belizan 2007; Bradley 2009; Foster 2006; Graner 2010; Lester 2003; Mathole 2006; Penfold 2013; Pitchforth 2010; VSO 2012 | Moderate confidence | Due to moderate concerns about methodological limitations; and minor concerns about coherence |
| Poor, incomplete, and non‐systematised patient information could lead to delayed or incorrect management of high‐risk mothers, or interfered with continuity of care. | Low confidence | Due to serious concerns about adequacy | |
| Lack of or unreliable supply of electricity, including a lack of fuel to run generators, and lack of water influenced health providers' ability to deliver quality care. | Moderate confidence | Due to moderate concerns about methodological limitations | |
| The lack of space and amenities as well as poor physical layout and organisation of wards limited the delivery of quality care. | Belizan 2007; Conde‐Agudelo 2008; DeMaria 2012; Fränngård 2006; Khalaf 2009; Lester 2003; Molina 2011; Pettersson 2006; Pitchforth 2010 | Moderate confidence | Due to minor concerns about adequacy, relevance, and methodological limitations |
| The lack of funds and material resources sometimes prevented health facility managers from adequately maintaining equipment and physical infrastructure. | Low confidence | Due to minor concerns about coherence; and moderate concerns about methodological limitations and adequacy | |
| Health facilities varied in the availability, functionality, and quality of interventions assigned as signal functions for obstetric care. At the lower‐level facilities, most of these functions were not available, e.g. parenteral antibiotics or anticonvulsants or neonatal resuscitation. At the higher levels, some of these functions appeared to be available, but functionality varied, for instance when there were drug stock‐outs or unqualified providers of care. | Very low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy | |
| Health workers felt it was easier to deliver care in facilities than at home. Some of the positive aspects about delivering care at the health facility were that they were able to do other work while monitoring labour; provide care for several mothers; work schedules were more regular; and care was available 24 hours a day. Furthermore, at facilities other skilled providers were available to assist when needed, and some procedures (e.g. episiotomies) were easier to perform. In addition, health facilities provided a secure, controlled, hygienic work environment, where electricity, equipment, and medications were always available. | Very low confidence | Due to moderate concerns about relevance; and serious concerns about adequacy | |
| REFERRAL MECHANISMS | |||
| Where primary care workers in lower‐level facilities lacked the knowledge and the skills to determine the need for referral, or were unable to provide emergency care, mothers could receive inadequate care. This lack of skills could also result in unnecessary referrals to other health facilities. | Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about relevance; and serious concerns about adequacy | |
| Lack of trust and professional rivalries between midwives, doctors, and obstetrician gynaecologists may delay referral of mothers and their babies. Midwives sometimes felt blamed by physicians when complications arose and hesitated to seek support from the medical teams at the receiving facilities. Some midwives did not travel with the mothers to the referring facility for fear of blame for any negative occurrence during the referral process. | Low confidence | Due to moderate concerns about adequacy and relevance | |
| Respondents felt that maternal perceptions of the health system could make mothers reluctant to accept referral. For instance, mothers were sceptical about the cost of care, poor management and care at the next‐level facility, the procedures used, the high levels of Caesarean sections, and fear of complications. Also mothers may have already travelled far to reach the facility they perceive as a good one, or feared unfamiliar, urbanised settings. As a result of mothers' reluctance to accept referral, midwives may feel pressured to conduct high‐risk deliveries or spend a lot of time convincing reluctant mothers or their families. | Barua 2011; Blum 2006; Graner 2010; Lester 2003; Tabatabaie 2012 | Moderate confidence | Due to minor concerns about methodological limitations, coherence, relevance, and adequacy |
| The presence of trust between mothers and midwives may influence a mother's willingness to be referred. Referral may be delayed when facilities lack midwives or other primary care workers whom the mothers trust and who can convince mothers of the need for referral. | Very low confidence | Due to minor concerns about coherence and methodological limitations; moderate concerns about relevance; and serious concerns about adequacy | |
| Lack of transport hinders referral of women and their babies to higher levels of care. For instance, this occurred when health facilities lacked ambulances, or when facility budgets were insufficient to purchase fuel for vehicles. | Moderate confidence | Due to minor concerns about relevance and adequacy | |
| Lack of fuel for vehicles when the need for referral arises is frustrating to nurses and midwives and leaves them feeling helpless when mothers' and babies' lives are at risk. | Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about relevance; and serious concerns about adequacy | |
| When health facilities lack fuel for vehicles, mothers and their families are sometimes asked to pay their own transport costs. Many families could not afford this. | Low confidence | Due to moderate concerns about relevance and adequacy | |
| Several situations could lead health workers to refer mothers and shift responsibility to higher levels of care, including when they lacked the skills or confidence to provide care, or were working in isolation; when they were concerned about the facility's reputation when poor patient outcomes arose; or when they lacked supplies, drugs, or equipment to provide care. Some of these referrals were unnecessary and resulted in increased workloads at higher levels of care. | Low confidence | Due to moderate concerns about adequacy and relevance | |
| When secondary‐level care was non‐existent, mothers were sometimes referred to tertiary‐level care, which resulted in congestion at the tertiary level. | Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about relevance; and serious concerns about adequacy | |
| Administrative processes and paperwork and poor communication between referring and receiving levels of care could influence the efficient transfer of mothers and their babies to receiving units. | Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about coherence and relevance; and serious concerns about adequacy | |
| Lack of feedback between the referring and receiving facilities could influence midwives' practice and patient outcomes. Midwives perceived this feedback as useful for improving their practice and patient outcomes. | Very low confidence | Due to moderate concerns about relevance; and serious concerns about adequacy | |
| INTERPERSONAL RELATIONS | |||
| Poor attitude and unethical behaviour among health workers could influence the quality of care. For instance, when health workers are harsh, rude, or impatient with mothers; or display poor cultural sensitivity, e.g. by not maintaining women's privacy; or when health workers are absent from their duty stations or involved in the illegal sale of drugs and supplies or expect 'back door' payments for services. Some of the suggested underlying reasons for these attitudes and behaviours were wrong intrinsic reasons for joining the profession and physical exhaustion from long, solitary hours of work. | Low confidence | Due to moderate concerns about methodological limitations and adequacy; and minor concerns about relevance | |
| Mothers' participation in decision‐making during labour could be limited by health worker attitudes and authoritarian behaviour, for instance when health workers conducted procedures without asking mothers for their opinion, or when physicians did not seek feedback from mothers about practices or outcomes and expected women to co‐operate. Lack of patient participation in decision‐making can threaten quality of care. Some of the reasons for this behaviour were related to health workers’ attitudes about the woman’s preferences and role during delivery of her baby. | Belizan 2007; de Carvalho 2012; Conde‐Agudelo 2008; DeMaria 2012; Maputle 2010 | Low confidence | Due to minor concerns about coherence and adequacy; and moderate concerns about methodological limitations and relevance |
| Some health workers did not value communication, communicated poorly, or said they had problems with communication. Poor communication and interaction could threaten the trust between health workers and mothers, for instance when health workers considered communication with mothers as a waste of time, and there was insufficient communication between staff and families, or when skilled birth attendants were abrasive and demeaning in their interactions with women and showed no concern for women's families. Language barriers could interfere with effective communication between mothers and health workers. As a result, mothers sometimes appeared not to listen to health workers while health workers mechanically worked through the process of providing care. Health workers acknowledged the need to respect and involve men, women's families, and the community in maternal health, e.g. in understanding cultural beliefs related to postpartum care. | Blum 2006; de Carvalho 2012; Hassan‐Bitar 2011; Lugina 2001; Maputle 2010 | Very low confidence | Due to moderate concerns about relevance and adequacy; and serious concerns about methodological limitations |
| Mismatch between people's expectations of health workers and what health workers were actually able to deliver or thought was appropriate could lead to antagonism. For instance, health workers that delivered home‐based care could experience social pressure from families and communities, e.g. to give injections to speed up delivery as opposed to waiting for labour to progress normally. Health workers providing maternity care at health facilities were sometimes treated harshly by people from the community when there was a lack of supplies and materials. In addition, misconceptions that midwives were not working when they took a break from their work, or that health workers sold drugs, threatened the trust between health workers and the community. | Low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy | |
| Health workers valued the appreciation, respect, trust, and praise from mothers, or when they made friends among mothers or worked with the community. Midwives in particular were delighted when a baby was given their name and seeing the baby grow. | Low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy | |
| Midwife‐led shared care was perceived to improve the interaction between mothers, families, and health workers, and could improve health workers' self esteem and lead to a change in hospital culture with respect to service provision. For instance, midwife‐led shared care increased communication between midwives, women, and their families; enabled the presence and participation of family members; and together increased satisfaction in the care provided. As a result, the need for medication during delivery was minimised, which reduced the financial burden experienced by families. The supportive environment for mothers, the good interaction between mothers and health workers, as well as recognition of professional expertise among midwives increased self esteem. Midwife‐led shared care enabled other hospital staff to reflect on their own routine activities and manner of communication with families and clients, leading to a change in hospital culture with respect to service provision. | Very low confidence | Due to moderate concerns about relevance; and severe concerns about adequacy | |
| Disrespectful communication, lack of trust, inadequate opportunities to review clinical practice, and poor teamwork and co‐ordination sometimes led to poor interprofessional relations. Also, tensions arose when health providers did not recognise each others' capabilities, and when they acted in a way that reinforced clinical hierarchy, e.g. disrespectful interprofessional communication between physicians and midwives. Midwives with lower‐level training could manage normal birth, but they felt marginalised and less motivated to provide care because midwives with higher levels of training and doctors used qualification, status, and their roles to dominate clinical practice. Tensions were reported between doctors and clinical officers due to salary differentials, benefits, workload, and status. There was sometimes a lack of understanding of competencies and alternative models of care. | Belizan 2007; Bradley 2009; DeMaria 2012; Hassan‐Bitar 2011; Ith 2012; Pettersson 2006 | Low confidence | Due to moderate concerns about relevance and adequacy |
| Nurses and midwives valued and were motivated by a good team dynamic where health workers provided feedback, supported, and co‐operated to ensure all shifts were covered. For instance, midwives valued good interprofessional collaboration that made them feel accepted as part of the professional team and provided an opportunity to improve their competence through on‐spot education provided by obstetricians. When midwives worked together in a team led by midwives, this increased their ability to share experiences and new practices and their decision‐making responsibility; improved their self esteem; and provided quality assurance and improved the quality of care provided. This teamwork was especially useful when emergencies arose. In another study, researchers observed that nurses had a strong teamwork ethic and functioned well together to complete work. | Bradley 2009; Foster 2006; Fränngård 2006; Lester 2003; Pettersson 2006 | Low confidence | Due to moderate concerns about relevance and adequacy |
| Factors reported by health workers or their managers as influencing recruitment, retention, motivation, or performance of health workers were: good‐quality accommodation for health workers provided by government, allowances for extra project‐related work, paid vacations for one month of the year, improved access to and funding for continued education/in‐service training, career progression, non‐biased evaluations or performance‐related rewards or promotions, e.g. for those doing better, working longer, or taking on added responsibilities, and verbal recognition by supervisors and management. The following factors were reported as discouraging health workers from working in rural or remote health facilities: facilities that lack good equipment and do not provide sufficient work needed to maintain clinical skills, lack of family amenities, limited opportunities for private practice, lack of electricity, TV, or internet, coupled with poor roads and lack of transport. In addition, interference in treatment decisions by local politicians, and mismanagement of posting and transfer from the national level, were demotivating to health workers working in rural facilities. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 6 studies; ethical considerations were not reported in 4 studies; and sampling methods were not reported in 3 studies. However, these may not have influenced the finding. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns, as 1 study reports managers’ perceptions of factors health workers describe as influencing recruitment and retention. |
| Adequacy | No to very minor concerns, though some studies reported thin data for specific parts of the finding. |
| Overall CERQual assessment | |
| Moderate confidence | Due to minor concerns for methodological limitations and relevance |
| Contributing studies/setting | |
| Africa (4), E. Asia (1), Middle East &N Africa (1), S. Asia (1) Bradley 2009: Malawi, rural mission hospitals Anwar 2009: Bangladesh, basic and comprehensive emergency obsteric care facilities, public VSO 2012: Uganda, hospitals and health centres Fränngård 2006: Uganda, district hospital and health centre IVs Ith 2012: Cambodia, provincial and regional hospitals, health centres De Brouwere 2009: Senegal, district hospitals | |
Background
The United Nations' fifth Millennium Development Goal (MDG) aimed to reduce maternal death rates by increasing the proportion of births conducted by skilled birth attendants. Low‐ and middle‐income countries promoted the skilled attendance at birth strategy in order to reduce high maternal mortality rates. Globally, from 1990 to 2014, a 12% increase in the proportion of births attended by skilled birth attendants was achieved (UN 2015). But while several low‐ and middle‐income countries managed to improve access to skilled care at birth, several did not manage to reduce their high maternal mortality rates. The sub‐Saharan Africa region was reported to have the highest number of maternal deaths (510 deaths per 100,000 live births), while South Asia, Oceania, and the Caribbean each had 190 deaths per 100,000 live births. Whereas attention at the policy level was given to increasing access to skilled care at birth, this was not matched with improvements in the quality of care available at health facilities, and this may have contributed to the slow decline in maternal mortality (Campbell 2016, Koblinsky 2016; Graham 2012).
The United Nations' Sustainable Development Goals represent a renewed call to action to sustain the gains achieved in the MDG era and to further improve priority areas such as maternal health (UN 2015b). Their third goal aims to reduce global maternal mortality ratio to fewer than 70 maternal deaths per 100,000 live births by 2030. The provision of quality maternal care, delivered through a resilient health system with well‐staffed health facilities that are capable of managing routine and emergency maternity care, has been identified among the priorities for action over the next five years (Koblinsky 2016).
Description of the condition
In order to provide good‐quality care to mothers and their babies, healthcare workers need to possess appropriate skills, attitudes, and behaviours, and also need access to drugs, supplies, and equipment, as well as tools for communication and referral when complications arise. Such components have been referred to as supply‐side factors (Gabrysch 2009; Say 2007). When these components are not available at health facilities for mothers in active labour, they contribute to one source of delay in accessing care (Thaddeus 1994). The absence of these components can influence the technical quality of care provided at health facilities and lead to poor maternal and child outcomes. The absence of these components can also influence how care is perceived by mothers and mothers' choice in place of delivery, and can contribute to delays in providing adequate care for mothers in labour.
Description of the intervention
Skilled birth attendance refers to "the process by which a woman is provided with adequate care during labour, delivery and the postpartum period" (SMIAG 2000). This process requires both a skilled attendant and an enabling environment. An enabling environment has been described as one that provides supportive regulation, policies and infrastructure, communication, referral, logistics, and supplies, inputs that are necessary for a skilled attendant to provide care (Maclean 2003). A joint statement from the World Health Organization, the International Confederation of Midwives, and the International Federation of Gynecology and Obstetrics defines a skilled birth attendant as an "accredited health professional such as a midwife, doctor or nurse that is trained to proficiency and has the necessary skills to manage a normal pregnancy, childbirth and provide postnatal care as well as the skills to detect, manage and refer any complications in the mother and neonate" (WHO 2004). Possessing a core set of skills would imply that the health professional is able to manage a normal, uncomplicated vaginal delivery. However, studies have demonstrated great variation between countries in the cadre, as well as the level of skills and competence, possessed by skilled birth attendants (Harvey 2007; Adegoke 2012; Utz 2013). In addition, the scope of practice of the skilled birth attendant varies widely to include a few or all components of basic and comprehensive emergency obstetric care. Basic emergency obstetric care is a package of care that provides the seven signal functions needed to provide lifesaving interventions to women with obstetric complications and their babies (WHO 2008). The seven signal functions are: administration of parental antibiotics; administration of oxytocic drugs; administration of anticonvulsants; manual removal of the placenta; removal of retained products of conception; conducting assisted vaginal deliveries; and performing neonatal resuscitation. In addition to the seven signal functions defined as basic care, comprehensive emergency obstetric care provides blood transfusion and surgery. Skilled birth attendants need to possess advanced skills in order to provide comprehensive emergency obstetric care.
In this synthesis, we have focused on care provided during the intrapartum and postpartum period. This includes normal, uncomplicated maternity care, basic and comprehensive emergency obstetric care, as well as postpartum care. By postpartum care we refer to the period immediately after birth and up to six weeks.
How the intervention might work
The rationale for promoting skilled birth attendance at delivery is based on evidence that at least 75% of maternal deaths occur from late pregnancy to 48 hours following delivery (Abou‐Zahr 1998). The scientific evidence of the impact of skilled birth attendance on maternal mortality is weak due to the ethical issues around randomising mothers to non‐skilled attendants. The available evidence is obtained from quasi‐experimental studies that show a link between reduced maternal mortality rates and skilled attendance at birth (Maine 1996), and challenges related to confounding mean the causal link between maternal mortality and access to skilled birth attendance is not firmly established. Additional evidence from statistical modelling suggests that 16% to 33% of all maternal deaths could be prevented by skilled birth attendance (Graham 2001). Historical data from Sweden, the United States of America, Malaysia, and China also suggest a correlation between the decline in maternal mortality rates and the increase in skilled attendance at birth (De Brouwere 1998; Koblinsky 1999; Loudon 1992). However, the contribution of factors such as the environment under which these births were conducted and other ongoing social and economic changes is difficult to estimate.
The conceptual framework for skilled birth attendance at delivery guided the development of this synthesis (Graham 2001). In this framework, Graham and colleagues suggest key elements that can influence the provision of skilled attendance at birth and thereby maternal, neonatal, and provider outcomes and cost‐effectiveness. These elements are organised into structure, inputs, outputs, and outcomes. First, the framework highlights elements in the structure or environment where care is provided, including the political or policy environment and the social/cultural environment. According to the framework, this environment influences the inputs available, such as human resources, education, technical quality of care, financing, and supplies. These inputs in turn influence the process of care such as health facility access or availability; the mix or ratio of providers; interactions, such as between health workers and clients; and referral processes. Finally, these outputs influence the health outcomes (maternal and baby and provider outcomes and cost‐effectiveness). See Figure 1 for the Graham 2001 framework.

Why it is important to do this synthesis
By synthesising existing qualitative evidence, we aimed to identify the range of factors, including barriers and facilitators, in low‐ and middle‐income settings that influence the provision of intrapartum and postnatal care by skilled attendants. Evidence on barriers and facilitators is useful for policymakers and managers seeking to develop implementation strategies to improve the quality of maternity care. The evidence generated in this synthesis provides information for understanding the basic needs and experiences of health personnel when providing maternity care. Health workers' experiences may, in turn, influence the quality of maternal health services provided, as well as the success or failure of strategies to promote facility‐based deliveries and recruit and retain skilled birth attendants. Information about the experiences of skilled birth attendants, the ways in which they deliver care, as well as other factors influencing the process of care may not be reported in effectiveness studies. While Cochrane intervention reviews are not designed to answer these types of questions, there is growing acknowledgement that syntheses of qualitative research can make important contributions in this area (Glenton 2013). Our synthesis complements the evidence generated by a Cochrane intervention review entitled 'The effectiveness of policies promoting facility‐based deliveries in reducing maternal and infant morbidity and mortality in low and middle‐income countries' (Dudley 2009).
Objectives
To explore the views, experiences, and behaviours of skilled birth attendants and those who support them; to identify factors that influence the delivery of intrapartum and postnatal care in low‐ and middle‐income countries; and to explore the extent to which these factors were reflected in intervention studies.
Methods
Criteria for considering studies for this synthesis
Types of studies
We included all studies that utilised qualitative methods for data collection (e.g. focus group interviews, individual interviews, observation, document analysis) and that utilised qualitative methods for data analysis (e.g. thematic analysis, framework analysis, grounded theory). We excluded studies that collected data using qualitative methods but did not perform a qualitative analysis (e.g. open‐ended survey questions where the responses are analysed using descriptive statistics). We included mixed‐methods studies where it was possible to extract findings derived from qualitative research.
Types of participants
Setting
We included studies based in primary, secondary, and tertiary levels of health care in low‐ and middle‐income countries. We utilised the World Bank 2013 definition of low‐ and middle‐income countries. We chose to focus only on low‐ and middle‐income countries because these are the regions where skilled birth attendance was actively promoted by the global health community in response to high maternal mortality rates (UN 2015).
Participants
We included studies of skilled birth attendants providing intrapartum and postnatal care. We defined a skilled birth attendant as an "accredited health professional such as a midwife, doctor or nurse that is trained to proficiency and has the necessary skills to manage a normal pregnancy, childbirth and provide postnatal care as well as the skills to detect, manage and refer any complications in the mother and neonate" (WHO 2004). We also included studies of auxiliary cadres such as auxiliary nurse midwives and associate clinicians (non‐physician clinicians) where these staff were employed at the health facility, worked independently or as part of a team, and were recognised within that setting as skilled birth attendants. In some instances, we were not able to tell if health workers fit our definition of skilled birth attendants, in which case we contacted the authors of the study for more information and included these studies as long as the health workers were recognised as skilled birth attendants in that particular setting.
We also included studies that collected data from managers of health units and other providers who support skilled birth attendants as part of the team at a facility. We considered that these providers work closely with skilled birth attendants and have views and experiences of factors that influence the provision of care.
We excluded studies of student nurses' or midwives' attitudes and experiences, as we were concerned with factors affecting the delivery of care in routine settings rather than in teaching settings.
We also excluded studies that focused exclusively on traditional birth attendants, as these are outside the definition of skilled birth attendants (WHO 2008). In addition, we excluded studies that documented women's views and experiences of care, as this topic is covered in another qualitative evidence synthesis (Bohren 2014). Where eligible studies included both women's and health workers' views of care, we included these but only extracted data on health worker views.
Phenomenon of interest
We focused on the views, experiences, and behaviours of skilled birth attendants when providing intrapartum and postnatal care. Of particular interest were their views and experiences of factors that facilitate (or hinder) the provision of high‐quality care. We use the term 'quality of care' to imply care that meets technical standards of care, is timely, evidence based, effective, safe, equitable, and provides a good experience of care (Dickson 2014; Donabedian 1978; Hulton 2000; Tunçalp 2015).
Although skilled birth attendants have an important role to play along the continuum of care for reproductive, maternal, and newborn health, in this synthesis we have focused on the intrapartum and postpartum period. Studies on antenatal care are part of a separate, complementary Cochrane qualitative evidence synthesis (Downe 2016). Maternity care may have been provided during a normal vaginal delivery or through basic or comprehensive emergency obstetric care when complications arose. As described above, basic emergency obstetric care is a package of care that provides the seven signal functions needed to provide lifesaving interventions to women and their newborn babies if complications arise. In addition to the seven signal functions, comprehensive emergency obstetric care includes surgery and blood transfusion. By 'postpartum care', we refer to the period immediately after birth and up to six weeks.
We did not include studies on abortion and postabortion care and antenatal care. These studies are likely to focus on factors that differ from those identified in studies that focus on intrapartum and postnatal care.
Search methods for identification of studies
Electronic searches
Our search strategies were based on a search strategy developed for two reviews: the Cochrane Review ‘Effectiveness of policies promoting facility‐based deliveries in reducing maternal and infant morbidity and mortality in low and middle‐income countries' (Dudley 2009), and a qualitative evidence synthesis by authors at the World Health Organization: ‘Facilitators and barriers to facility‐based delivery in low‐ and middle‐income countries: a qualitative evidence synthesis’ (Bohren 2014). The search strategy specified key and free text terms related to the perinatal period such as ‘maternal health’, ‘delivery’, ‘obstetric care’ and terms related to ‘doctor’, ‘midwife’, ‘nurse’, or ‘physician’. We included a methodological filter for qualitative evidence syntheses and for low‐ and middle‐income countries (EPOC 2017). See Appendix 1 for all strategies used.
We searched the following databases for eligible studies.
-
MEDLINE In‐Process & Other Non‐Indexed Citations, MEDLINE Daily, and MEDLINE (1946 to 21 November 2016), OvidSP
-
Embase Classic + Embase (1947 to 2016 week 47), OvidSP (searched up to 28 November 2016)
-
PsycINFO (1806 to November week 3 2016), OvidSP (searched up to 30 November 2016)
-
POPLINE, K4Health (1827 to 30 November 2016)
-
CINAHL (Cumulative Index to Nursing and Allied Health Literature) (1980 to 30 November 2016), EBSCOhost
-
ProQuest Dissertations and Theses (1861 to 15 August 2013)
-
Web of Science Conference Proceedings Citation index, ISI Web of Knowledge (1990 to 1 December 2016)
-
World Health Organization Reproductive Health Library (searched up to 16 August 2013)
-
World Health Organization Global Health Library for WHO databases (Regional Indexes) (searched up to 1 December 2016)
Searching other resources
At the time of developing this synthesis, a related Cochrane intervention review was under development (Dudley 2009). We checked the bibliography of effectiveness studies that were included in this review in order to identify any qualitative studies that were linked to these studies. We only searched bibliographies of effectiveness studies published in the last five years (2008 to 2013). Checking recent studies as opposed to older studies was more likely to lead to identification of eligible studies, given the increase in the number of effectiveness studies that also include qualitative research in recent years (O'Cathain 2013).
Data collection and analysis
Selection of studies
We collated records obtained from the searches and removed duplicates. Two review authors then independently assessed titles and abstracts to identify potentially eligible studies. We retrieved the full‐text articles of potentially eligible references, and two review authors independently assessed these to determine their eligibility. Any disagreements between review authors were resolved by discussion or by seeking the opinion of a third review author.
Data extraction and management
We developed a data extraction form to guide the collection of data. We extracted data on the following.
-
First author of the study, year of publication, country of study, study setting (urban/rural, level of care).
-
Cadre of skilled birth attendant (e.g. nurse, doctor, midwife, or other cadre identified as a skilled birth attendant)
-
Data describing the views, experiences, and behaviour of skilled birth attendants when providing intrapartum and postnatal care. In this qualitative evidence synthesis, we regarded the authors of the individual studies to be our 'informants' rather than the participants in these studies. The authors’ interpretations, presented for instance through themes and categories, therefore represent our data. While the authors’ interpretations were primarily collected from the results sections of each paper, author interpretations were sometimes also found in the discussion sections, and these were also extracted when relevant and when well‐supported by data. We used the Graham 2001 framework on factors that influence skilled birth attendance (Figure 1) to organise these data.
One review author extracted the data and another checked the data for any discrepancies. Disagreements were resolved by discussion or in consultation with a third review author.
Appraisal of the methodological limitations of included studies
Our inclusion criteria specified that to be included a study must have used qualitative methods for both data collection and data analysis. This criterion constitutes a basic quality threshold. We discarded studies that did not meet this standard. We used a modified version of the Critical Appraisal Skills Programme qualitative appraisal checklist to assess methodological limitations of each included study (Appendix 2) (Atkins 2008). One review author applied the criteria to each included study, and another review author checked the data for any errors or missing data. Any discrepancies were discussed and agreed upon by the two review authors. We did not exclude any studies on the basis of our assessment of methodological limitations but utilised this information to assess our confidence in the review findings. We were likely to have higher confidence in findings that are drawn from well‐conducted studies, as these findings are more trustworthy.
Table 2 includes a summary of the assessment of methodological limitations of included studies.
| Author year | Is study qualitative research? | Research questions clear? | Ethical issues? | Is qualitative approach justified? | Is approach appropriate for research question? | Is study context clearly described? | Role of researcher described? | Sampling method clearly described? | Sampling strategy appropriate? | Method of data collection clear? | Method of data collection appropriate to question? | Method of data analysis clear? | Method of data analysis suitable? | Are claims supported by evidence? | Overall assessment |
| Yes | Yes | Yes | No | Yes | Yes | No | No | Not clear | Yes | Yes | Yes | Yes | Yes | Medium | |
| Yes | Yes | No | Yes | Yes | Yes | No | Yes | Yes | Yes | Not clear | Yes | Yes | Yes | Good | |
| Yes | Yes | Yes | Yes | Yes | Yes | Not clear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Not clear | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Yes | Yes | Yes | Yes | Yes | Yes | Not clear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Yes | Yes | Yes | Yes | Yes | Yes | Not clear | Not clear | Not sure | Yes | Yes | Yes | Yes | Yes | Good | |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Mixed methods | Yes | No | Yes | Yes | Yes | No | No | No | Yes | Yes | No | Not clear | Yes | Low | |
| Yes | Yes | Yes | No | Not clear | Not clear | No | No | No | Yes | Yes | Not clear | Not clear | Yes | Low | |
| Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Medium | |
| Yes | No | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | Low | |
| Yes | Yes | Yes | Yes | Yes | Yes | No | No | Not clear | Yes | Yes | Yes | Yes | Yes | Medium | |
| Yes | Not clear | No | No | Not clear | Yes | Not clear | Yes | Yes | Yes | Not sure | Yes | Yes | Yes | Low | |
| Mixed methods | Yes | No | No | Not clear | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Medium | |
| Mixed methods | Yes | Yes | Yes | Yes | Yes | No | Not clear | Not clear | Yes | Yes | Yes | Yes | Yes | Medium | |
| Mixed methods | Clear objectives | Yes | Yes | Yes | Yes | Not clear | No | Not clear | Yes | Yes | Yes | Yes | Yes | Medium | |
| Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Yes | No | No | No | Not clear | Not sufficient | Not clear | No | Not clear | Yes | Unclear | No | Not clear | Yes | Low | |
| Yes | Objectives clear | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Medium | |
| Mixed methods | Objectives clear | Yes | Yes | Yes | Yes | Not clear | Not clear | Not clear | Yes | Yes | Yes | Yes | Yes | Medium | |
| Mixed methods | Objectives clear | Yes | No | Yes | Yes | No | Not clear | Not clear | Yes | Yes | Yes | Yes | Yes | Medium | |
| Yes | Yes | Yes | No | Not clear | Not sufficient | Not clear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | medium | |
| Yes | Objective is clear but questions are not stated. | No | No | Not clear | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low | |
| Mixed methods | Aim is clear. | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Yes | Clear objectives | Yes | No | Not clear | Yes | Not clear | Unclear | Not clear | Yes | Yes | Yes | Yes | No | Low | |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Good | |
| Yes | Yes | Yes | Yes | Yes | Not sufficient | No | Yes | Yes | Yes | Yes | Yes | Not clear | Yes | Low | |
| Yes | Objective clear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Mixed methods | Objective clear | No | No | Not clear | Yes | No | Unclear | Not clear | Yes | Yes | Yes | Yes | No | Low | |
| Yes | Objective clear | No | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Medium | |
| Yes | objective clear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good |
Assessment of confidence in the review findings
We used the GRADE‐CERQual (Confidence in the Evidence from Reviews of Qualitative research) approach to summarise our confidence in the evidence(Lewin 2016). CERQual assesses confidence in the evidence, based on the following four key components.
-
Methodological limitations of included studies: the extent to which there are concerns about the design or conduct of the primary studies that contributed evidence to an individual review finding.
-
Coherence of the review finding: an assessment of how clear and cogent the fit is between the data from the primary studies and a review finding that synthesises those data. By cogent, we mean well supported or compelling.
-
Adequacy of the data contributing to a review finding: an overall determination of the degree of richness and quantity of data supporting a review finding.
-
Relevance of the included studies to the review question: the extent to which the body of evidence from the primary studies supporting a review finding is applicable to the context (perspective or population, phenomenon of interest, setting) specified in the review question.
After assessing each of the four components, we made a judgement about the overall confidence in the evidence supporting the review finding. We judged confidence as high, moderate, low, or very low. All findings started as high confidence and were then graded down if there were important concerns regarding any of the CERQual components. The starting point of high confidence reflects a view that each review finding should be seen as a reasonable representation of the phenomenon of interest unless there are factors that would weaken this assumption.
Data synthesis
Given that relevant data were likely to be thin and descriptive and not theorised or conceptual (Noyes 2011), we based our data synthesis on a best fit framework approach (Carroll 2011; Carroll 2013), using a 'theory' on how skilled birth attendance influences health outcomes as our framework (see Appendix 3) (Noyes 2016)
'Summary of qualitative findings' table
Our key findings are presented in the summary of findings Table for the main comparison. The table also provides our assessment of confidence in the evidence as well as an explanation of this assessment, based on the GRADE‐CERQual approach (Lewin 2016).
Supplementing the Cochrane intervention review with synthesised qualitative findings
We explored how the findings from our synthesis related to, and helped to explain, the findings of the related Cochrane intervention review (Dudley 2009). To do this we utilised a matrix model similar to one used previously by Candy 2011 and Ames 2017. Our matrix explored whether the factors that were identified by health workers in our synthesis as important for providing maternity care were reflected in the interventions evaluated in the studies in the related intervention review. This review is in progress, and the data we used in this synthesis were obtained from the review authors.
To create the matrix we undertook the following steps: first, we went through each of the synthesis findings and identified factors identified by health workers as important for providing maternity care. Where we had presented factors as barriers or facilitators, we rephrased these as neutral descriptions of health services inputs.
Secondly, we created a table listing these factors. We then assessed whether these factors were addressed in the interventions evaluated in the studies included in Dudley 2009. As the Dudley review also included interventions targeting mothers and communities, we screened the included studies to identify those where the intervention targeted health workers and health systems. Out of 30 included studies in the Dudley review, 11 targeted health workers or health system issues and were therefore relevant for this synthesis.
Results
Results of the search
We retrieved and screened 17,594 unique titles and abstracts. We assessed 166 full‐text articles for inclusion. Thirty‐one of these studies fulfilled the inclusion criteria and were included in this synthesis (Figure 2).
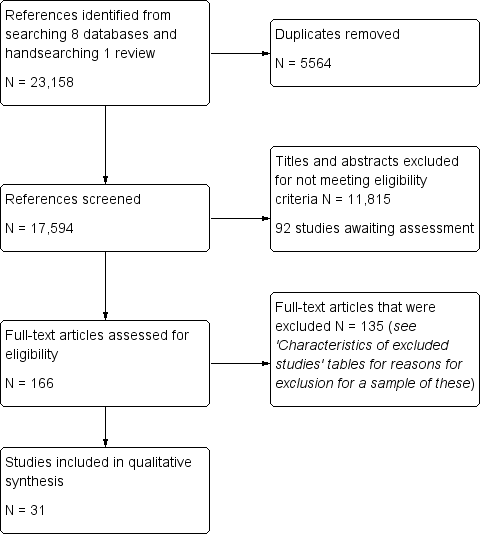
Study flow diagram.
Description of studies
Study respondents
Participants in the included studies were from a broad range of health worker cadre, including obstetricians, intern doctors, general practitioners, and various nurse midwife cadre (see Characteristics of included studies tables). Three studies only included midwives, and three included only nurse midwife (dual‐trained) cadre. Other participants were clinical officers and medical assistants, paramedics or lady visitors with six months training in midwifery, nursing assistants or auxiliary nurses, physiotherapist, pharmacist, social welfare staff, surgical assistants, and anaesthetists. A few studies included heads of departments, health facility or program managers among participants.
Skilled birth attendant characteristics
Few studies described the core education of participants or if participants had received any additional training. Two studies indicated that the general practitioners had received additional training, that is eight months training in De Brouwere 2009 and one year of specialised training in maternity care in Molina 2011.
Of the four studies that included clinical officers and medical assistants (Bradley 2009; Graner 2010; Spangler 2012; VSO 2012), only Bradley 2009 reported that clinical officers and medical assistants had shorter pre‐service training and lower qualifications compared to doctors, although they conducted most of the major emergency obstetric operations in the hospitals.
A few studies reported varying levels of information regarding the core/additional training of midwives. In Hassan‐Bitar 2011, midwives had university degrees, while midwives in Fränngård 2006 had two to three years' midwifery training after secondary school. Other studies indicated that midwives had two to three years of nurse training and one year of midwifery following primary or secondary school education (Blum 2006; Ith 2012; Lugina 2001; Mathole 2006).
Two studies reported that nurses held university‐level degrees (DeMaria 2012; Khalaf 2009). In DeMaria 2012, nurses had a four‐year university‐level training that included one year of midwifery training. In other studies, nurses had two to three years of nursing training, while a few had diploma‐level or certificate‐level training in midwifery (Mathole 2006; Mondiwa 2007).
Other studies that mentioned core/additional training of participants indicated that auxiliary nurse midwives had one‐year training in nursing after high school (Foster 2006; Pettersson 2006); surgical assistants were auxiliary nurses trained in surgical assistance for three months (De Brouwere 2009); and lady visitors were paramedics with at least six months' midwifery training (Blum 2006).
Few studies provided information on the years of experience of the participants, which ranged from a few months to 33 years (see Characteristics of included studies tables).
Very few studies reported any information on participants' remuneration or salaries. For the few studies where this information was available, monthly salaries ranged from USD 170 to USD 700.
Setting
Sixteen of the studies were conducted in low‐income countries: Bangladesh (Afsana 2001; Anwar 2009; Blum 2006; Pitchforth 2006), Benin (Fujita 2012), Ethiopia (Pitchforth 2010), Malawi (Bradley 2009; Mondiwa 2007; Thorsen 2012), Mozambique (Pettersson 2006), Tanzania (Lugina 2001; Penfold 2013; Spangler 2012), Uganda (Fränngård 2006; VSO 2012), and Zimbabwe (Mathole 2006).
Fifteen of the studies were conducted in middle‐income countries: Brazil (de Carvalho 2012), Cambodia (Ith 2012), Colombia (Conde‐Agudelo 2008; Molina 2011), Dominican Republic (Foster 2006), India (Barua 2011), Iran (Tabatabaie 2012), Jordan (Khalaf 2009), Mexico (DeMaria 2012), Palestine (Hassan‐Bitar 2011), Senegal (De Brouwere 2009), South Africa (Lester 2003; Maputle 2010), and Vietnam (Graner 2010). One study was conducted in Argentina and Uruguay (Belizan 2007). Argentina is a middle‐income country. Uruguay is now categorised as a high‐income country, but was categorised as middle‐income country at the time of the study.
Most studies did not indicate whether the studies were based in urban or rural settings. Eight studies indicated that participants were based in urban areas, seven studies indicated rural areas, while four studies indicated both urban and rural areas.
Level of care
Most of the studies were conducted among participants who worked at tertiary, secondary, or both levels of care, for example national referral hospitals or district hospitals (Anwar 2009; Barua 2011; Belizan 2007; Bradley 2009; Conde‐Agudelo 2008; de Carvalho 2012; De Brouwere 2009; DeMaria 2012; Foster 2006; Fujita 2012; Hassan‐Bitar 2011; Lugina 2001; Maputle 2010; Mondiwa 2007; Pettersson 2006; Pitchforth 2006; Pitchforth 2010; Thorsen 2012). A few studies included participants from primary levels of care, including health centres or dispensaries (Afsana 2001; Fränngård 2006; Graner 2010; Khalaf 2009; Mathole 2006; Molina 2011; Penfold 2013; Spangler 2012; VSO 2012). Participants in two studies provided care at home, but health providers were based at primary care units or private clinics (Blum 2006; Tabatabaie 2012). In one study, participants worked at a primary care unit located in a hospital (Lester 2003).
Focus of the included studies
The studies described health workers’ views and experiences of a wide range of issues when providing maternity care. These included the delivery of obstetric or perinatal care and/or priorities for improving maternity care (Afsana 2001; Anwar 2009; Graner 2010; Hassan‐Bitar 2011; Maputle 2010; Molina 2011; Pettersson 2006; Pitchforth 2010; Spangler 2012); the provision of postpartum care (Khalaf 2009; Lugina 2001); the management of postpartum haemorrhage, (Foster 2006), or eclampsia (Barua 2011); and the provision of care to HIV‐infected mothers (Mathole 2006; Mondiwa 2007).
Participants in some studies described their perceptions of human resource issues, including factors affecting retention, motivation, and performance (Bradley 2009; Ith 2012), professional life (Fränngård 2006), and training/scope of practice (DeMaria 2012); and conditions underlying unethical behaviour and service inadequacies (VSO 2012). One study described health workers' experiences of task shifting of emergency obstetric services (De Brouwere 2009).
Participants in some studies described their experiences of different models of care, including humanised care (Fujita 2012), home–based versus facility‐based care (Blum 2006), and midwife‐led obstetric unit in a hospital setting (Lester 2003). Some studies described health workers' perceptions of evidence‐based care. In one study this was explored as part of the development of guidelines (Belizan 2007), while another study described the state of practice in relation to evidence‐based guidelines (Conde‐Agudelo 2008). Participants in one study described reasons for the continued use of harmful birth practices (de Carvalho 2012).
Other studies described health workers' perceptions of the functionality and availability of equipment, drugs, and supplies (Penfold 2013); barriers to facility births among private providers (Tabatabaie 2012); health workers' decision‐making processes to enable women access to financial assistance (Pitchforth 2006); and facility‐based factors that contribute to maternal deaths (Thorsen 2012).
Few studies provided any information on the range of specific tasks delivered by health workers. Where these were reported, the tasks varied widely by cadre and are reported in the Characteristics of included studies tables.
Methodological limitations of the included studies
Most of the included studies did not report in detail the sampling or data analysis methods used, or researcher reflexivity (see Table 2). In addition, some studies did not report ethical considerations.
Confidence in the review findings
Out of 51 findings, we graded two as high confidence, 16 as moderate confidence, and the remaining findings as low or very low confidence using the CERQual approach. (See summary of findings Table for the main comparison). Our explanation for each CERQual assessment is shown in the Evidence Profiles (See Table 3 to Table 53).
| Staff shortage was a widely reported problem, and led to increased workloads, which in turn sometimes compromised quality of care. For instance, heavy workload limited health worker time for history taking and thorough assessment of women, and hand hygiene was sometimes compromised. Staff shortages and work overload jeopardised health workers’ ability to provide timely care and manage routine care as well as emergency cases. In addition, shortage of staff sometimes led health workers to exceed their scope of practice and influenced a health facility's ability to provide 24‐hour care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 13 studies; ethical consideration was not reported in 6 studies; and a small number of studies did not report sampling strategy or data analysis methods. However, these may not influence the finding. |
| Coherence | Minor concerns because 1 study reported that doctors were able to rest despite the workload, another study indicated nurses did not exceed scope of practice. These data imply that the finding may relate only to a few cadre. |
| Relevance | No to very minor concerns, as data were drawn from a wide range of settings and covered different levels of care. |
| Adequacy | No to very minor concerns because many studies reported data on this finding, though some studies provided thin data. |
| Overall CERQual assessment | |
| Moderate confidence | Due to minor concerns about coherence; and minor concerns about methodological limitations |
| Contributing studies/setting | |
| Middle E&N Africa (2), Africa (9), E. Asia (2), S. Asia (3), Latin America & Caribbean (1) Hassan‐Bitar 2011: Palestine, public referral hospital Bradley 2009 Malawi, rural mission hospitals Khalaf 2009: Jordan, maternal and child health centres Graner 2010: Vietnam, primary health care Lugina 2001: Tanzania, municipal hospitals Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries Fränngård 2006: Uganda, district hospital and health centre IVs Fujita 2012: Benin, tertiary hospital Anwar 2009: Bangladesh, basic and comprehensive emergency obsteric care facilities, public Maputle 2010: South Africa, tertiary care hospital VSO 2012: Uganda, hospitals and health centres Conde‐Agudelo 2008: Colombia, public and private hospitals Thorsen 2012: Malawi, a secondary and tertiary hospital Mathole 2006: Zimbabwe, health centres in the district Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals Afsana 2001: Bangladesh, health centre Ith 2012: Cambodia, public maternity settings in provincial hospital, two regional hospitals and two health centres | |
Synthesis findings
In this section we have reported the categories identified in the synthesis and the findings from the synthesis that belong in each category.
As described above, our analysis was guided by Graham's conceptual framework for skilled birth attendance at delivery (Graham 2001). We did not make major changes to the categories in Graham’s framework. However, while Graham grouped these categories as either "structure", "inputs", "outputs", or "outcomes", we chose not to group the categories in this way. This was because we experienced overlap of some categories (e.g. referral processes and mechanisms could be categorised as inputs or outputs), and because grouping the categories in this way downplayed the interrelationships between the categories. We instead chose to group the categories according to the level at which they operate; namely, the macro‐environment or the meso‐ or microenvironment. We did not use two of Graham’s categories. We did not find any studies that reported data on the “financing” category. We did not consider the second category, “technical quality of care”, to be a separate category, as it is relevant to all other categories as an immediate outcome of the process of providing care. Figure 3 represents our adaptation of Graham's conceptual framework for skilled birth attendance at delivery (Graham 2001), and reflects the findings from this synthesis as well as the categories for which we had no data. Factors tied to the macro‐, meso‐, and microenvironment may influence available quality of care and health worker performance and motivation; maternal experiences of care; as well as health facility functionality or capability. Some of the maternal experiences of care included satisfaction and participation in decision‐making. These factors are discussed further in the section below.
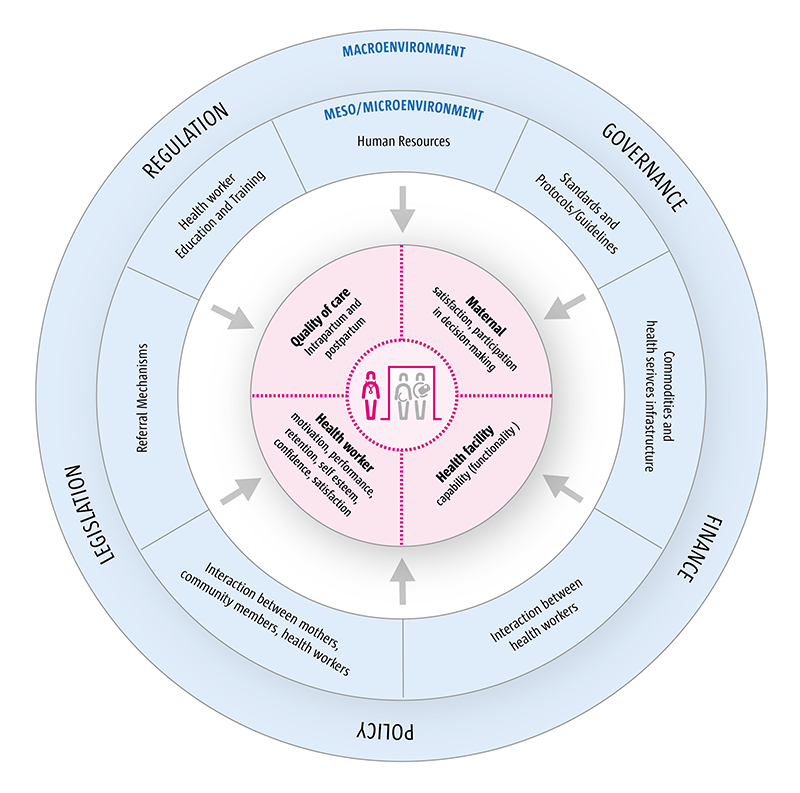
Factors that influence the delivery of intrapartum and postpartum care by skilled birth attendants.
Factors tied to the meso‐ and microenvironment
We have used the terms 'meso‐' and 'microenvironment' to refer to elements within the intermediate and immediate work environment that influenced the delivery of care by health workers. These elements are often interrelated, and separating them would be artificial.
Human resources
Staff shortages were widely reported as a problem (Anwar 2009; Barua 2011; Conde‐Agudelo 2008; Fränngård 2006; Graner 2010; Maputle 2010; Spangler 2012), and led to increased workloads (Barua 2011; Hassan‐Bitar 2011; Khalaf 2009; VSO 2012), which in turn sometimes compromised quality of care (moderate confidence; Table 3) (Barua 2011,De Brouwere 2009, Khalaf 2009,Maputle 2010,Mathole 2006). For instance, one study reported that heavy workloads limited the time that health workers had for conducting thorough assessments of women, and only women suspected to have complications were examined (Khalaf 2009). Heavy workloads could also lead midwives to omit some aspects of care, such as changing gloves or hand hygiene (Hassan‐Bitar 2011,Ith 2012, Mathole 2006), potentially increasing the risk of cross‐transmission of infection (Mondiwa 2007). Doctors in one study reported incomplete history‐taking and examination of women as a result of heavy workloads (Hassan‐Bitar 2011). Health workers’ ability to provide timely care (Thorsen 2012), and to manage routine care as well as emergency cases could also be jeopardised (Barua 2011, VSO 2012). When faced with heavy workloads, health workers were sometimes not able to provide privacy to all mothers but only to those who requested it (Khalaf 2009), or felt unable to provide personalised care (Fujita 2012). In addition, shortage of staff could lead health workers to exceed their scope of practice (Bradley 2009), and could influence a facility's ability to provide 24‐hour care (Anwar 2009, Fränngård 2006). Women’s motivation to attend clinics could also be influenced by heavy workloads and busy clinics (Lugina 2001).
A lack of specialists or experienced staff or teams trained in obstetrics surgery and anaesthesia presented a particular challenge for the delivery of maternity care and supervision of junior staff (moderate confidence; Table 4). For instance, certain tasks, such as emergency obstetric care (Afsana 2001, Anwar 2009, De Brouwere 2009), were not delivered at all in some cases, or were transferred to health workers who were not properly qualified or trained to deliver them (Pitchforth 2010, VSO 2012). When health workers exceeded their scope of practice (informal task‐shifting), this could again lead to increased workloads, fear of blame from their managers, as well as poor community relations whenever poor outcomes occurred (VSO 2012). In a number of studies, where experienced health workers were not available, health workers lacked supervision (Blum 2006, Bradley 2009,Fränngård 2006, Hassan‐Bitar 2011,Ith 2012, Pitchforth 2010, Spangler 2012), and staff appraisal was not done (Bradley 2009). Where senior staff were available, supervision was reported as being inadequate, largely negative, and corrective in nature, focusing on mistakes and gaps in work rather than quality of work (Blum 2006, Bradley 2009,Fränngård 2006, Hassan‐Bitar 2011, Penfold 2013,Spangler 2012). Reasons that were given for poor or lack of supervision included lack of staff and lack of time (Bradley 2009, Fränngård 2006, Hassan‐Bitar 2011). Health workers who sometimes attended home deliveries reported that verbal reporting or indirect supervision after conducting home delivery was inadequate, and expressed a need for supervision while in the field so as to enhance their competence, foster confidence in working in difficult conditions, and remove potential blame from the risk during home deliveries (Blum 2006). In another study, a lack of supervision was believed to lead to a climate that fostered inappropriate behaviour (Spangler 2012).
| A lack of specialists or experienced staff, including absence of health workers with key skills such as anaesthetics, could influence the provision of care and supervision of junior staff. When no specialists were available, some tasks for instance emergency obstetric care were not delivered at all, or tasks were transferred to health workers who were not properly qualified or trained to deliver them. When senior experienced health workers were not available, junior health workers sometimes lacked supervision. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 9 studies; ethical considerations were not reported in 5 studies; and several studies did not report sampling strategy or data analysis methods. |
| Coherence | No to very minor concerns |
| Relevance | No to very minor concerns |
| Adequacy | No to very minor concerns |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about methodological limitations |
| Contributing studies/setting | |
| Africa (7), Middle E&N Africa (2), S. Asia (3) Hassan‐Bitar 2011: Palestine, public referral hospital Bradley 2009: Malawi, rural mission hospitals Khalaf 2009: Jordan, maternal and child health centres Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries Fränngård 2006: Uganda, district hospital and health centre IVs Anwar 2009: Bangladesh, basic and comprehensive emergency obsteric care facilities, public VSO 2012: Uganda, hospitals and health centres Afsana 2001: Bangladesh, health centre Blum 2006: Bangladesh, home‐based maternity care Penfold 2013: Tanzania, hospitals, health centres, dispensaries De Brouwere 2009: Senegal, district hospitals Pitchforth 2010: Ethiopia, teaching hospital | |
In settings where staff shortages were a major problem, informal task‐shifting was possible because health workers had vague job descriptions that led them to perform tasks that were beyond their expertise or scope of practice (very low confidence; Table 5) (Bradley 2009). In one study, health workers were given jobs where the contract included a clause that allowed a manager to assign any job to an employee. As a result, some health workers exceeded their scope of practice (Bradley 2009).
| Health workers had vague job descriptions that sometimes led them to perform tasks that were beyond their expertise or scope of practice. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns. Although reflexivity and ethical considerations were not reported, these may not have influenced the finding. |
| Coherence | No to very minor concerns |
| Relevance | Serious concerns. Data were from only 1 region. |
| Adequacy | Serious concerns. Data were from 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about methodological limitations; and serious concerns about relevance and adequacy |
| Contributing studies/setting | |
| (Africa 1) | |
Staff shortages and work overload could jeopardise health workers’ ability to display support, empathy, and friendliness to women in labour (very low confidence; Table 6) (Conde‐Agudelo 2008, Maputle 2010). For instance, some midwives had limited time to verify women's preferences when providing care to more than two women at the same time (Maputle 2010). Studies described midwives and nurses as feeling stretched to the limit (VSO 2012), resulting in burnout, reducing staff motivation, and leaving them feeling unable to meet the demands of work (Lugina 2001). Other studies described midwives that felt overwhelmed by expectations to provide postpartum care as well (Khalaf 2009); nurses referring to themselves as machines and describing their work as insane and a cause of stress (Hassan‐Bitar 2011); and paramedics describing their work as hectic with long hours and constant responsibility (Afsana 2001).
| Staff shortages and work overload could jeopardise health workers’ ability to display support, empathy, and friendliness to women in labour. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 2 studies; ethical considerations were not reported in 1 study; and sampling strategy was not clear in 2 studies. However these may not influence the finding. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because data were from a limited number of regions and level‐of‐care settings. |
| Adequacy | Moderate concerns because data were from 3 studies with very thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about methodological limitations; and moderate concerns about relevance and adequacy |
| Contributing studies/setting | |
| Africa (2), Latin America & Caribbean (1) Maputle 2010: South Africa, tertiary care hospital Conde‐Agudelo 2008: Colombia, public and private hospitals, 44% were university teaching hospitals VSO 2012: Uganda, hospitals and health centres | |
Staff shortages and increased workloads, combined with difficult living and work conditions, sometimes caused stress and frustration, affected health workers' family life, and led to concerns about personal safety (moderate confidence; Table 7). Staff shortages and increased workloads meant that health workers often worked alone and for long hours (Anwar 2009, Fränngård 2006, VSO 2012), with limited collegial support when emergencies arose, and health workers reported feeling frustrated and stressed (Graner 2010, VSO 2012). A manager in one study described how one midwife had worked alone for five months (VSO 2012). Heavy workloads also had implications for health workers' family life, as they sometimes had to stay at health centres away from husbands and family members (Fränngård 2006), or slept with their children in disused wards to allow them to attend to mothers late into the night (VSO 2012). Limited space and privacy for midwives' accommodation as well as long distances to husbands' work stations could result in relationship problems between spouses (Fränngård 2006). Family relations were further constrained by long work hours and busy schedules (Fränngård 2006, Graner 2010), lack of money for transport to meet partners, and poor communication between villages (Fränngård 2006). Some health workers reported fearing for their personal safety, for instance when working alone in the community (Blum 2006), and felt that they might be at increased risk of HIV transmission due to the pressure of work (Lester 2003).
| Staff shortages and increased workload as well as living and work conditions sometimes caused stress and frustration, affected family life, and led to concerns about personal safety among health workers. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 4 studies; ethical considerations were not reported in 3 studies; and some studies did not report sampling or data analysis methods. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns because data referred mainly to midlevel providers of care. |
| Adequacy | Minor concerns because data were from several studies, though some studies had thin data. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about methodological limitations; and minor concerns about relevance and adequacy |
| Contributing studies/setting | |
| Africa (3), S. Asia (2), E. Asia & Pacific (1) Fränngård 2006: Uganda, district hospital and health centre IVs Blum 2006: Bangladesh, home‐based maternity care Lester 2003: South Africa, maternity obstetric unit located in large academic hospital Anwar 2009: Bangladesh, basic and comprehensive emergency obsteric care facilities, public VSO 2012: Uganda, hospitals and health centres | |
A wide range of interlinked reasons for staff shortages were suggested. These included limited funds to recruit health workers (Graner 2010,VSO 2012); bureaucracy in the recruitment process (e.g. absence of committees responsible for recruitment at the district level) (VSO 2012); scarcity of health workers, especially in rural areas (VSO 2012); and other factors that deterred the retention of health workers once recruited (moderate confidence; Table 8) (see also section below on factors that influence recruitment, retention, motivation, or performance of health workers) (Anwar 2009). Other reasons for staff shortages were institutional arrangements, for instance when health facilities hired contract staff in order to reduce labour costs (Molina 2011), and inefficient deployment of available staff that created a perception of staff shortages (Pitchforth 2010). Facilities with staff shortages and high workloads were also seen as unattractive places to work, making it difficult for managers to transfer staff from well‐served to underserved areas (VSO 2012), thus compounding the problem.
| A wide range of interlinked reasons for staff shortages were suggested. These included limited funds to recruit health workers, bureaucratic processes of the recruitment process (e.g. absence of committees responsible for recruitment at the district level), scarcity of health workers especially in rural areas, and other factors that deter retention of health workers once recruited (see Table 1). In addition, institutional arrangements (e.g. when health facilities hire contract staff in order to reduce labour costs) and inefficient deployment of available staff may create staff shortages. Facilities with staff shortages and work overload were also seen as unattractive places to work, making it difficult for managers to transfer staff from well‐served to underserved areas, thus compounding/increasing the problem. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 4 studies, and ethical considerations were not reported in 3 studies. However, these may not influence the finding. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns because some studies refer to institutional‐level factors, while others refer to district‐level factors. |
| Adequacy | Moderate concerns because data were from few studies with thin data. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about adequacy; and minor concerns about relevance and methodological limitations |
| Contributing studies/setting | |
| Africa (2), Latin America and Caribbean (1), E. Asia (1), S. Asia (1) Graner 2010: Vietnam, primary health care Anwar 2009: Bangladesh, basic and comprehensive emergency obsteric care facilities, public VSO 2012: Uganda, hospitals and health centres Pitchforth 2010: Ethiopia, teaching hospital Molina 2011: Colombia, primary, secondary, and tertiary care facilities | |
Health workers considered their salaries and benefits to be insufficient for the work done (Fränngård 2006, Hassan‐Bitar 2011), for the responsibility and personal risk (Graner 2010), and for the additional responsibilities assigned to them, for instance through informal task‐shifting (De Brouwere 2009). In addition, salaries were regarded as insufficient for their personal needs, such as sending their children to school and paying for transport costs to visit their husbands (Fränngård 2006). Low salaries and incentives sometimes led to a lack of motivation and poor performance, absenteeism, and increased rates of dual practice (moderate confidence; Table 9) (Ith 2012, Molina 2011). To supplement their income, health workers sometimes took on other jobs apart from their job at the health facility (i.e. 'dual practice') (Belizan 2007, Ith 2012,Molina 2011), which could also lead to long working hours and fatigue (Molina 2011). Some health workers demanded informal payments for certain procedures, referred mothers on to their own private practice, or provided unnecessary services for a fee (Ith 2012). Dual practice also led to absenteeism (Anwar 2009, Ith 2012), which increased the staffing problem at the health facility, and because doctors spent little time in public hospitals, sometimes led to lack of agreement on clinical practice (Belizan 2007).
| Health workers' salaries and benefits were considered insufficient for the work done, the responsibility and personal risk, and the additional responsibilities assigned, e.g. through informal task‐shifting. In addition, salaries were insufficient for health workers' personal needs, e.g. to send their children to school and for transport costs to visit their husbands. Low salaries and incentives sometimes led to a lack of motivation and poor performance, absenteeism, and increased rates of dual practice. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns, as reflexivity was not reported in 7 studies; ethics consideration was not reported in 3 studies; and sampling or data analysis methods were not reported in 4 studies. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns because 1 study included health workers on contract, which may be a different arrangement from other studies. |
| Adequacy | Minor concerns because several studies had thin data. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about methodological limitations; and minor concerns about relevance and adequacy |
| Contributing studies/setting | |
| Middle E&N Africa (1), E. Asia (2), Latin America & Caribbean (2), Africa (2), S. Asia (1) Hassan‐Bitar 2011: Palestine, public referral hospital Belizan 2007: Argentina/Uruguay, public hospitals Anwar 2009: Bangladesh, basic and comprehensive emergency obsteric care facilities, public Fränngård 2006: Uganda, district hospital and health centre IVs Ith 2012: Cambodia, provincial and regional hospitals, health centres De Brouwere 2009: Senegal, district hospitals Graner 2010: Vietnam, primary health care Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obsteric services | |
Apart from salaries, the following factors were considered by health workers or their managers to facilitate recruitment, retention, motivation, or performance of health workers: good‐quality accommodation for health workers (Fränngård 2006, VSO 2012); allowances for extra project‐related work (Fränngård 2006); paid vacations for one month of the year (Fränngård 2006); improved access to and funding for continued education/in‐service training (Bradley 2009,De Brouwere 2009, Fränngård 2006,VSO 2012); career progression (Bradley 2009,De Brouwere 2009); non‐biased evaluations(Hassan‐Bitar 2011); performance‐related rewards or promotions for those doing better, working longer, or taking on added responsibilities (Anwar 2009,Bradley 2009,De Brouwere 2009, VSO 2012); and verbal recognition by supervisors and management (Ith 2012). Conversely, the following factors were reported as discouraging health workers from working in rural or remote health facilities: facilities that lacked good equipment and did not provide sufficient work experience needed to maintain clinical skills (De Brouwere 2009); poor staff accommodation (VSO 2012); lack of family amenities (Anwar 2009); limited opportunities for private practice (Anwar 2009); and lack of electricity, TV, or internet, coupled with poor roads and lack of transport (VSO 2012). In addition, interference in treatment decisions by local politicians, VSO 2012, and mismanagement by national level officers of posting and transfer to new workstations, were demotivating to health workers working in rural facilities (moderate confidence; Table 1) (Anwar 2009). Health workers therefore preferred to work in urban areas to provide their children access to better schools, and for better amenities such as communication, water, and electricity. An exception was reported in one study, where a midwife preferred to work in a rural area where her family lived (Fränngård 2006).
Heath workers' working environments were sometimes worsened by poor management. For instance, health workers perceived managers as lacking in management capacity and skills, felt unsupported in their work (Bradley 2009,Lester 2003), and complained that concerns about the workplace were sometimes left unheard and no solutions or feedback were given (moderate confidence; Table 10) ( Ith 2012, Lester 2003). Health workers complained about unfair duty rosters that led to heavy workloads (VSO 2012), and were also concerned about management bias when staff were selected for promotion (Bradley 2009). Some studies reported that supervisors and management rarely conducted recognition and positive performance appraisal (Ith 2012), leaving health workers with low motivation and low career advancement opportunities (Ith 2012).
| Health workers perceived managers as lacking in management capacity and skills and sometimes felt unsupported. Health workers also complained that concerns about the workplace were sometimes left unheard, and no solutions or feedback given. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, as reflexivity was not reported in 4 studies, and ethical considerations were not reported in 3 studies. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as only 3 regions were represented; data were from health workers’ views of management; and 1 study referred to lack of management support at a midwife‐led unit in a hospital setting. |
| Adequacy | Minor concerns because some studies had thin data. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about relevance; and minor concerns about methodological limitations and adequacy |
| Contributing studies/setting | |
| Africa (4), S. Asia (1), E. Asia (1) Bradley 2009: Malawi, rural mission hospitals VSO 2012: Uganda, hospitals and health centres Ith 2012: Cambodia, provincial and regional hospitals, health centres Anwar 2009: Bangladesh, basic and comprehensive emergency obstetric care facilities, public Lester 2003: South Africa, maternity obstetric unit located in large academic hospital Mondiwa 2007: Malawi, large government hospital | |
Funding mechanisms to provide financial assistance to mothers for out‐of‐pocket payments were sometimes in place, for instance through government social welfare funds or informal systems established by doctors in obstetric wards. However, bureaucratic processes sometimes denied mothers, especially those facing emergencies, access to the funds they needed to obtain care, and health workers' time was sometimes wasted as they helped mothers to access these funds (very low confidence, Table 11) (Pitchforth 2010).
| Helping women access financial assistance for out‐of‐pocket payments was sometimes time‐consuming for health workers. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, though reflexivity was not reported. |
| Coherence | No to very minor concerns |
| Relevance | Serious concerns because only 1 region and teaching hospital population were represented. |
| Adequacy | Serious concerns because data are from 1 study with very thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to serious concerns about relevance and adequacy |
| Contributing studies/setting | |
| S. Asia (1) Pitchforth 2006: Bangladesh, teaching hospital | |
Health worker education and training
Inadequate pre‐service and in‐service training sometimes limited health workers' skills and their ability to provide care (high confidence; Table 12). Some studies described how health workers sometimes lacked training in communication and were thus limited in their ability to share information with mothers (Afsana 2001); and sometimes also lacked sufficient training to attend home births (Blum 2006), to manage complicated pregnancies or deliveries, such as HIV in pregnancy (Afsana 2001, Barua 2011, Mathole 2006), and to provide loading doses of magnesium sulphate when managing pre‐eclampsia and eclampsia (Barua 2011). Some doctors lacked training in non‐pharmacological pain management (Graner 2010), and were thus limited in their ability to manage pain, while others lacked the training to conduct Caesarean sections or repair extensive lacerations (DeMaria 2012). Specialist doctors were therefore necessary to manage complicated cases. Midwives' basic education did not always provide them with the practical skills to work independently in midwife‐led obstetric units (Lester 2003), or to manage labour in positions other than the supine position (Afsana 2001). In contrast, one study showed how training and allowing midwives to practice assisting women in delivering in non‐supine positions enabled them to get accustomed to this practice (Fujita 2012).
| Inadequate pre‐service and in‐service training sometimes limited health workers’ skills and ability to provide care. For instance, some health workers lacked training to attend home births or manage complicated pregnancies or deliveries, e.g. HIV in pregnancy or eclampsia. In contrast, training allowed midwives to practice assisting women to deliver in non‐supine positions and enabled them to get accustomed to this practice. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because ethical considerations were not reported in 3 studies; reflexivity was not reported in 5 studies; and sampling strategy was not clear in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | No to very minor concerns |
| Adequacy | No to very minor concerns |
| Overall CERQual assessment | |
| High confidence | ‐ |
| Contributing studies/setting | |
| Latin America & Caribbean (1), Africa (3), S. Asia (3), E. Asia & Pacific (1) Fujita 2012: Benin, tertiary hospital Blum 2006: Bangladesh, home‐based maternity care DeMaria 2012. Mexico, public and non‐governmental hospitals Lester 2003: South Africa, maternity obstetric unit located in large academic hospital Mathole 2006: Zimbabwe, health centres in the district Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals Afsana 2001: Bangladesh, health centre Graner 2010: Vietnam, primary health care | |
Health worker competencies and opportunities for on‐the‐job training were sometimes limited by poor scheduling of education sessions, high cost, inequitable selection of participants, lack of ongoing training and follow‐up, and shortage of instructors (moderate confidence; Table 13). For instance, midwives did not benefit from classes that were inappropriately scheduled, such as after working a night shift (Pettersson 2006), or when the content did not apply to midwives' daily reality. Midwives sometimes missed opportunities to upgrade from enrolled to registered midwifery when they lacked adequate funds (Fränngård 2006). Professional status and hierarchy sometimes also meant that the selection of candidates for training was not fair; junior midwives in one study often missed opportunities to upgrade their skills for this reason (Ith 2012). In the same study, training programs were often not combined with support supervision and feedback for improving performance among health workers (Ith 2012), and in another study had a shortage of instructors for upgrading courses in midwifery (Spangler 2012). In addition, the variation in quality of pre‐service training resulted in varying levels of need for in‐service training, and these needs were not always met, resulting in wide variation in proficiency among health workers (Pettersson 2006, Spangler 2012). In contrast, learning through practical application was reported as facilitating the acquisition of skills and confidence. The experience gained through, for example, internship, social service year, and working in the community was identified as important for building doctors' and midwives' practical experience and confidence in providing care (very low confidence; Table 14) (DeMaria 2012).
| Health worker competencies and opportunities for on‐the‐job training were sometimes limited by poor scheduling of in‐service education sessions, the high cost of continuing education for health workers, inequitable selection for professional development opportunities, lack of ongoing training and follow‐up, and shortage of instructors for upgrading courses. In addition, variation in the quality of pre‐service training resulted in varying levels of need for in‐service training, and these needs were not always met, resulting in wide variation in proficiency among health workers. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 2 studies; ethics considerations were not reported in 1 study; and sampling strategy or data analysis methods were not reported in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns, as only 2 regions were represented. |
| Adequacy | Moderate concerns, as data were from only 4 studies with thin data. |
| Overall CERQual assessment | |
| Moderate confidence | Due to minor concerns about methodological limitations and relevance; and moderate concerns about adequacy |
| Contributing studies/setting | |
| Africa (3), East Asia (1) Pettersson 2006: Mozambique, tertiary hospital Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries Ith 2012: Cambodia, provincial and regional hospitals, health centres Fränngård 2006: Uganda, district hospital and health centre IVs | |
| Learning through practical application facilitated acquisition of skills and confidence. The experience gained through, for example, internship, social service year, and working in the community were identified as important for building doctors' and midwives' practical experience and confidence in providing care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns, as reflexivity and sampling strategy were not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as data refer to hospitals that had different models of care (3 with pure models of care, i.e. allopathic medical model, midwifery, obstetric nurse; 2 with mixed models, i.e. medical/midwifery and medical/obstetric nurses). Only 1 region was represented. |
| Adequacy | Severe concerns, as data were from only 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about methodological limitations and relevance; and severe concerns about adequacy |
| Contributing studies/setting | |
| Latin America & Caribbean (1) DeMaria 2012: Mexico, public and non‐governmental hospitals | |
Health workers reported several barriers to implementing recommended practice. Firstly, health workers were sometimes unaware of current recommended effective practices (Conde‐Agudelo 2008). Secondly, health workers' flexibility, attitudes, and beliefs about medical knowledge and skills sometimes influenced their receptivity to new practice knowledge (Belizan 2007). For example, some health workers were reported as being inflexible or unwilling to implement alternative positions of delivery even though these were preferred by women (Afsana 2001, Pettersson 2006); having attitudes that did not view medical knowledge as dynamic; or holding beliefs that no significant progress had been made and that clinical practice was similar to techniques learnt many years ago (low confidence; Table 15) (Belizan 2007). The lack of knowledge of current recommended practice was not always viewed as problematic by health workers since they had textbook knowledge on case management (Pitchforth 2010). In some cases, health workers were reported as being ignorant of the effectiveness of certain practices or sceptical about the use of evidence‐based medicine in obstetrics (Conde‐Agudelo 2008). Although conferences provided an opportunity for learning, these were considered by some health workers as repetitive, offering basic information, and leaving them unmotivated to seek new practice knowledge (Belizan 2007). In situations where health workers were unaware of recommended effective practice, the culture of practice was sometimes based on "norms and routines dictated by opinion leaders" (Conde‐Agudelo 2008).
| Health workers reported several barriers to implementing recommended practice. Firstly, health workers were sometimes unaware of current recommended effective practices. Secondly, health workers flexibility, attitudes, and beliefs about medical knowledge and skills sometimes influenced their receptivity to new practice knowledge. For example, health worker attitudes did not view medical education as dynamic; held beliefs that no significant progress had been made and that clinical practice was similar to techniques learnt many years ago; or were not flexible or willing to implement alternative positions of delivery even though these were preferred by women. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, as reflexivity was not reported in 3 studies, and sampling strategy was not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as only hospital populations from 2 regions were represented. |
| Adequacy | Moderate concerns, as only 3 studies with thin data reported this finding. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about relevance and adequacy |
| Contributing studies/setting | |
| Africa (1), Latin Am & Caribbean (2) Belizan 2007: Argentina/Uruguay, public hospitals Pitchforth 2010: Ethiopia, teaching hospital Conde‐Agudelo 2008: Colombia, public and private hospitals, 44% were university teaching hospitals | |
Lack of time, skills, and infrastructure limited health workers' ability to seek knowledge and practice new clinical skills (low confidence; Table 16). For instance, chronic staff shortages meant less time available for health workers to seek information (Belizan 2007,Conde‐Agudelo 2008). This was sometimes further compounded by a lack of information sources such as internet access, and poorly facilitated hospital libraries (Belizan 2007). In addition, lack of training and skills in networking, epidemiology, research appraisal, or critical thinking about clinical practice could limit health workers' awareness and receptivity to clinical practice changes (Belizan 2007, Conde‐Agudelo 2008, Lugina 2001). In addition, professionals sometimes preferred old, familiar procedures when they lacked the skills to adopt new practices (Afsana 2001, Belizan 2007). In contrast, some doctors, such as those in university residence programmes, hesitated to use methods that did not require interventions, and preferred new technologies and skills and wanted to implement them. University residency programmes were therefore viewed as an opportunity for residents to practice new procedures, but were also a disadvantage when motivated residents did not follow recommendations about when these interventions, such as selective episiotomies, should be used (Belizan 2007). Other factors that health workers considered important for introducing and maintaining new clinical practices were management support, training in implementation of clinical guidelines, the extent to which the changes were promoted by doctors who were considered well informed by their peers, and how those changes were perceived by their peers (Belizan 2007).
| Lack of time, infrastructure, and skills limited health workers' ability to seek knowledge and practice new clinical skills. For instance, chronic staff shortages meant less time available for health workers to seek information. This was sometimes further compounded by lack of information sources such as internet access and poorly resourced hospital libraries. In addition, lack of training and skills in networking, epidemiology, research appraisal, or critical thinking about clinical practice limited health workers' awareness and receptivity to clinical practice changes, and this lack of skills led some professionals to prefer old, familiar procedures. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 2 studies, and sampling strategy was not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as only 2 regions were represented, and data were from hospital populations. |
| Adequacy | Moderate concerns, as had only 3 studies with thin data. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about relevance and adequacy; and minor concerns about methodological limitations |
| Contributing studies/setting | |
| Africa (1), Latin Am & Caribbean (2) Belizan 2007: Argentina/Uruguay, public hospitals Conde‐Agudelo 2008: Colombia, public and private hospitals, 44% were university teaching hospitals Lugina 2001: Tanzania, municipal hospitals | |
Standards and protocols
Where guidelines and protocols were lacking or were inconsistent, or where health workers were not aware or were uncertain of them, patient care and outcomes could be impacted and harm caused (low confidence; Table 17). The included studies showed examples of health workers lacking guidelines and protocols (de Carvalho 2012), for instance for the management of complications in pregnancy such as pre‐ and posteclampsia (Barua 2011, Mathole 2006); for uncommon diseases in pregnancy and childbirth (Mathole 2006); and for postpartum care (Lugina 2001). This could lead to a lack of direction (Lugina 2001), and inconsistent and harmful care (de Carvalho 2012). Different hospital units sometimes followed different guidelines/protocols for the same procedures (Barua 2011). Occasionally, guidelines were contradicted in the media (Mathole 2006), for instance health workers who were implementing World Health Organization (WHO) guidelines on breastfeeding for the prevention of mother‐to‐child HIV transmission were confused when the media gave contradictory messages. In another study, health workers were unaware of health standards of care for reproductive care (Khalaf 2009).
Health workers did not always comply with protocols and guidelines, even when aware of them. For example, when providing postpartum care, health workers did not always monitor bleeding and uterine involution, or check vital signs every 15 minutes (low confidence; Table 18) (Molina 2011). Guidelines and protocols were not followed for a number of reasons. Some health workers felt that guidelines were insufficient without consensus from staff (Belizan 2007). Some studies described how health workers continued to practice ineffective procedures because they were considered routine (Conde‐Agudelo 2008); due to lack of time (Lester 2003); because health workers lacked the autonomy not to follow what they knew to be inappropriate care (de Carvalho 2012); because the resources at the institution were not aligned with the protocols for postpartum care (Mathole 2006); or when it was unclear who was responsible for carrying out specific tasks, such as using a partograph (Pettersson 2006).
| Lack of guidelines/protocols, or where they were inconsistent or health workers were not aware or were uncertain of them, could impact patient care and outcomes and cause harm. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, as reflexivity was not reported in 3 studies; ethical considerations were not reported in 1 study; and sampling strategy and data analysis were not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | No to very minor concerns |
| Adequacy | Moderate concerns, as data were from only 5 studies, several with thin data. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about adequacy; and minor concerns about methodological limitations |
| Contributing studies/setting | |
| Africa (2), Latin American & Caribbean (1), S. Asia (1), Middle East & North Africa (1) Lugina 2001: Tanzania, municipal hospitals Khalaf 2009: Jordan, maternal and child health centres Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals Mathole 2006: Zimbabwe, health centres in the district de Carvalho 2012: Brazil, university teaching hospital | |
| Health workers did not always adhere to protocols/guidelines, even when aware of them. Guidelines/protocols were not followed for a number of reasons. Some health workers felt that guidelines were insufficient without consensus from staff. Some studies described how health workers continued to practice ineffective procedures because they were considered routine; due to lack of time; because health workers lacked the autonomy to avoid using what they knew to be inappropriate care; or because the resources at the institution were not aligned with the protocols for postpartum care, or when it was unclear who was professionally responsible, for example in using the partograph. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns, as reflexivity was not reported in 5 studies; ethics considerations were not reported in 2 studies; and sampling strategy was not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns due to partial data from each of the studies; studies were mainly from 1 region and primarily hospitals. |
| Adequacy | Moderate concerns due to thin data in several studies. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy |
| Contributing studies/setting | |
| Latin America and Caribbean (4), Africa (1) Pettersson 2006: Mozambique, tertiary hospital Belizan 2007: Argentina/Uruguay, public hospitals de Carvalho 2012: Brazil, university teaching hospital Conde‐Agudelo 2008: Colombia, public and private hospitals, 44% were university teaching hospitals Molina 2011: Colombia, primary, secondary, and tertiary hospitals | |
Health worker compliance with protocols and guidelines was also guided by health workers' perceptions of the consequences of their practice. For example, health workers sometimes used unnecessary diagnostic tests and did not follow recommended practice when they feared malpractice suits. This fear could lead to practitioners retaining practices they believed were ‘safer’ (very low confidence; Table 19) (Belizan 2007). Some health workers did not use recommended interventions when delivering care due to concerns about negative outcomes for the baby or the mother. Examples included the use of magnesium sulphate administered with anaesthesia during Caesarean sections or when monitoring of serum magnesium sulphate levels was not possible (very low confidence; Table 20) (Barua 2011). Health workers were sometimes reluctant to admit their lack of skills in delivering care for fear of blame and criticism from managers (Barua 2011, Lugina 2001,Pettersson 2006,Thorsen 2012), and were fearful of admitting ignorance about childbearing when they were expected to be knowledgeable (Lugina 2001). This fear of criticism could undermine health worker confidence and performance (low confidence; Table 21) (Pettersson 2006).
| Health workers sometimes used unnecessary diagnostic tests and did not follow recommended practice when they feared malpractice suits. This fear could lead to practitioners retaining practices they believed were ‘safer’. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, as no reflexivity was reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as only 1 region was represented. |
| Adequacy | Serious concerns, as data were from 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about relevance; serious concerns about adequacy; and minor concerns about methodological limitations |
| Contributing studies/setting | |
| Latin America & Caribbean (1) Belizan 2007: Argentina/Uruguay, public hospitals | |
| Some health workers did not use recommended interventions when delivering care because of concerns about negative outcomes for the baby or the mother. Examples included the use of magnesium sulphate administered with anaesthesia during Caesarean sections or when monitoring of serum magnesium sulphate levels was not possible. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, as reflexivity was not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as data are from only 1 region. |
| Adequacy | Serious concerns, as included only 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about relevance; serious concerns about adequacy; and minor concerns about methodological limitations |
| Contributing studies/setting | |
| S. Asia (1) Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals | |
| Health workers were sometimes reluctant to admit their lack of skills in delivering care for fear of blame and criticism from managers. This fear of criticism could undermine health worker confidence and performance. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, though reflexivity was not reported in 1 study, and sampling was not clear in another. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns, as data were from only 1 region and hospital populations. |
| Adequacy | Moderate concerns, as had few studies with thin data. |
| Overall CERQual assessment | |
| Low confidence | Due to minor concerns about relevance; and moderate concerns about adequacy |
| Contributing studies/setting | |
| Africa (3) Pettersson 2006: Mozambique, tertiary hospital Lugina 2001: Tanzania, municipal hospitals Thorsen 2012: Malawi, a secondary and tertiary hospital | |
Commodities and health services infrastructure
Insufficient stock or lack of drugs and supplies, or both, sometimes influenced the quality of care provided to mothers and their babies (moderate confidence; Table 22). For instance, studies reported insufficient stock and/or lack of drugs such as hydralazine, magnesium sulphate, oxytocin, misoprostol, or antiretrovirals (Anwar 2009,de Carvalho 2012, Fränngård 2006,Ith 2012, Penfold 2013,Pitchforth 2006,Pitchforth 2010). Supplies such as gloves were likewise reported to be insufficient or out of stock in several studies (Fränngård 2006,Graner 2010,Lester 2003, Mathole 2006,Pitchforth 2006,Pitchforth 2010,Spangler 2012,VSO 2012). Health workers in one study had to use less effective alternative drugs such as diazepam instead of magnesium sulphate when managing eclampsia (Pitchforth 2010). In other studies, a lack of supplies limited good hygiene practices and practice of aseptic techniques (Graner 2010, Mathole 2006), resulting in unsafe practices such as the reuse of disposable gloves, potentially increasing the risk of HIV infection (Graner 2010, Lester 2003), leading to poor outcomes and increasing the length of stay in health facilities (Bradley 2009). The lack of supplies and drugs was attributed in part to the long time it took to replenish these and the wastage that occurred when health facilities received supplies that they had not requested (Penfold 2013). As a result of this lack of drugs or supplies, mothers or their carers had to purchase their own (Foster 2006, Fränngård 2006, VSO 2012), which sometimes led to wasted time in procuring the drug and the creation of informal markets and corruption at health facilities (low confidence; Table 23) (Barua 2011; Spangler 2012).
| Insufficient stock and/or lack of drugs such as hydralazine, magnesium sulphate, oxytocin, misoprostol, and antiretrovirals, and supplies such as gloves, sometimes influenced the quality of care provided to mothers and their babies. For instance, health workers had to use less effective alternative drugs (e.g. diazepam) instead of magnesium sulphate. Lack of supplies sometimes limited good hygiene and practice of aseptic techniques, resulting in unsafe practices (e.g. reuse of disposable gloves), which could increase the risk of HIV infection. The lack of supplies sometimes led to poor outcomes and increased the length of stay in health facilities. Lack of supplies could determine if a new clinical practice was implemented and maintained over time. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 8 studies; ethics considerations were not reported in 4 studies; sampling methods were unclear in 3 studies; and data analysis methods were unclear in 3 studies. |
| Coherence | No or very minor concerns |
| Relevance | No or very minor concerns |
| Adequacy | No or very minor concerns, although data were thin, many studies from several regions reported this finding. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about methodological limitations |
| Contributing studies/setting | |
| Africa (8), E. Asia (2), Latin America and Caribbean (3), S. Asia (2) Bradley 2009: Malawi, rural mission hospitals Pitchforth 2010: Ethiopia, teaching hospital Graner 2010: Vietnam, primary health care Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries de Carvalho 2012: Brazil, university teaching hospital Belizan 2007: Argentina/Uruguay, public hospitals Fränngård 2006: Uganda, district hospital and health centres Anwar 2009: Bangladesh, basic and comprehensive emergency obstetric care facilities, public VSO 2012: Uganda, hospitals and health centres Mathole 2006: Zimbabwe, health centres in the district Penfold 2013: Tanzania, hospitals, health centres, dispensaries Foster 2006: Dominican Republic, hospital Lester 2003: South Africa, maternity obstetric unit located in large academic hospital Ith 2012: Cambodia, provincial and regional hospitals, health centres Pitchforth 2006: Bangladesh, teaching hospital | |
| As a result of this lack of drugs or supplies, mothers or their carers had to purchase their own. This sometimes led to wasted time in procuring the drugs and supplies and the creation of informal markets and corruption at health facilities. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 5 studies; ethics considerations were not reported in 2 studies; sampling methods were not clear in 4 studies; and data analysis methods were not reported in 2 studies. Lack of reflexivity can influence findings, as health workers may not report corruption. |
| Coherence | Minor concerns because all studies refer to women or their carers purchasing their own supplies, but only 1 study refers to informal markets and corruption. |
| Relevance | No to very minor concerns |
| Adequacy | Moderate concerns due to thin data |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about methodological limitations and adequacy; and minor concerns about coherence |
| Contributing studies/setting | |
| Africa (5), S. Asia (1), Latin America and Caribbean (1) Pitchforth 2010: Ethiopia, teaching hospital VSO 2012: Uganda, hospitals and health centres Foster 2006: Dominican Republic, hospital Lester 2003: South Africa, maternity obstetric unit located in large academic hospital Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries Fränngård 2006: Uganda, district hospital and health centres Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals | |
Lack of equipment also limited health workers' ability to provide quality care to mothers and their babies (high confidence; Table 24). For instance, studies reported a lack of stethoscopes and blood pressure machines (Pettersson 2006), cord clamps and delivery kits (Fränngård 2006, VSO 2012), complete vacuum evacuation sets (Pitchforth 2010), instruments to repair lacerations (Graner 2010), Ambu bags (and oxygen) for neonatal resuscitation (Pettersson 2006), sterilising equipment such as autoclaves (Anwar 2009, Graner 2010), and laboratory and diagnostic tools (Barua 2011). Some mothers and their babies received poor quality care as a result of this lack of equipment. In some studies, obstetricians managed eclamptic mothers without adequate investigative support (Barua 2011); neonates were not resuscitated due to lack of Ambu bags or oxygen (Pettersson 2006); monitoring of mothers and their babies was insufficient due to lack of equipment (Pettersson 2006); and lacerations were left unrepaired due to lack of instruments (Graner 2010).
| Lack of equipment limited health workers' ability to deliver quality care to mothers and their babies. As a result of this lack of equipment, mothers and their babies sometimes received poor quality care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity was not reported in 8 studies; ethical considerations were not reported in 3 studies; sampling was not reported in 4 studies; and data analysis was not reported in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | No to very minor concerns |
| Adequacy | No to very minor concerns |
| Overall CERQual assessment | |
| High confidence | ‐ |
| Contributing studies/setting | |
| Africa (6), S. Asia (2), East Asia & Pacific (1), Latin America & Caribbean (1) Pitchforth 2010: Ethiopia, teaching hospital Pettersson 2006: Mozambique, tertiary hospital Graner 2010: Vietnam, primary health care Fränngård 2006: Uganda, district hospital and health centres Anwar 2009: Bangladesh, basic and comprehensive emergency obstetric care facilities, public VSO 2012: Uganda, hospitals and health centres Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services Penfold 2013: Tanzania, hospitals, health centres, dispensaries Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals Lester 2003: South Africa, maternity obstetric unit located in large academic hospital | |
Lack of blood or poor infrastructure to manage blood transfusion limited health workers' ability to provide appropriate care (moderate confidence; Table 25) (Afsana 2001,Anwar 2009,Ith 2012). Lack of blood sometimes led to unnecessary referral (Afsana 2001), and in one study, resulted in death (Ith 2012). Where blood was available, some rural health facilities lacked the laboratory personnel or facilities for grouping and cross‐matching that are necessary for blood transfusion (Anwar 2009). In that study, blood was managed at the district‐level health facilities, and mothers needed to attend private diagnostic centers for grouping and cross‐matching.
| Lack of blood or limited infrastructure to manage blood transfusion prevented health workers from delivering appropriate care. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns; though ethical considerations were not reported in 2 studies and reflexivity was not reported in 2 studies, these may not influence the finding. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns because have 3 studies from 2 regions |
| Adequacy | Moderate concerns due to few studies with thin data |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about adequacy; and minor concerns about relevance |
| Contributing studies/setting | |
| S. Asia (2), E. Asia (1) Anwar 2009: Bangladesh, basic and comprehensive emergency obstetric care facilities, public Afsana 2001: Bangladesh, health centre Ith 2012: Cambodia, public maternity settings in provincial hospital, 2 regional hospitals, and 2 health centres | |
Lack of equipment, supplies, or drugs sometimes wasted health workers' time, increased their workloads and risk of infection, and led to low morale (moderate confidence; Table 26). For instance, a lack of supplies could increase workloads when health workers had to source items from other facilities (Penfold 2013), or could increase the workloads of health workers at receiving facilities whenever unnecessary referrals occurred. Health workers also wasted time trying to improvise in order to provide care (Bradley 2009, Lester 2003,VSO 2012), in the process sometimes using unrecommended practices that increased their fear as well as the risk of cross‐transmission of infection (Bradley 2009, Graner 2010, Lester 2003, Penfold 2013). The lack of supplies could lead to feelings of frustration and hopelessness among health workers and could wear them out (Belizan 2007; Foster 2006). In one study, the lack of antiretroviral therapy in particular left health workers feeling helpless when they watched mothers and their infants die (Mathole 2006).
| Lack of equipment, supplies, or drugs sometimes wasted health workers' time, increased their workload and risk of infection, and led to low morale. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 6 studies; ethics considerations were not reported in 3 studies; and sampling and data analysis methods were not clear in 2 studies. |
| Coherence | Minor concerns because some of the studies only reflect a portion of the findings. |
| Relevance | No to very minor concerns |
| Adequacy | No to very minor concerns; although the data are thin, many studies reported this finding. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about methodological limitations; and minor concerns about coherence |
| Contributing studies/setting | |
| Africa (6), E. Asia (1), Latin America and Caribbean (2) Bradley 2009: Malawi, rural mission hospitals Pitchforth 2010: Ethiopia, teaching hospital Graner 2010: Vietnam, primary health care Belizan 2007: Argentina/Uruguay, public hospitals VSO 2012: Uganda, hospitals and health centres Mathole 2006: Zimbabwe, health centres in the district Penfold 2013: Tanzania, hospitals, health centres, dispensaries Foster 2006: Dominican Republic, hospital Lester 2003: South Africa, maternity obstetric unit located in large academic hospital | |
Poor, incomplete, and non‐systematised patient information could lead to delayed or incorrect management of high‐risk mothers (Pettersson 2006), or interfere with continuity of care (low confidence; Table 27) (Molina 2011). For instance, when maternity records were missing, incomplete, or non‐systematised, high‐risk mothers did not always receive timely treatment (Pettersson 2006), or mothers might not be followed as they move from one facility to another (Molina 2011).
| Poor, incomplete, and non‐systematised patient information could lead to delayed or incorrect management of high‐risk patients, or interfere with continuity of care. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns; though reflexivity and ethical considerations were not reported in 1 study, and sampling methods not reported in 2 studies, these may not have influenced findings. |
| Coherence | No to very minor concerns |
| Relevance | No to very minor concerns |
| Adequacy | Serious concerns because few studies with very thin data reported this finding. |
| Overall CERQual assessment | |
| Low confidence | Due to serious concerns about adequacy |
| Contributing studies/setting | |
| Africa (1), Latin America & Caribbean (1) Pettersson 2006: Mozambique, tertiary hospital Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services | |
Apart from essential equipment, drugs, and supplies, a lack of or unreliable supply of electricity (Anwar 2009,Pitchforth 2010,Spangler 2012,VSO 2012), including a lack of fuel to run generators, and lack of water (Spangler 2012), influenced health workers' ability to provide quality care (moderate confidence; Table 28). In some studies, electricity was described as non‐existent, unreliable, or irregular (Anwar 2009, Spangler 2012, VSO 2012), and this interrupted the use of equipment such as ultrasound scans or hospital communication systems, interfered with the warming of babies, and placed health workers at increased risk of infection while working in the dark. In one study, health workers reported delaying repairs of episiotomies to daytime. One study reported that lower‐level health centres had no indoor running water and used water from outdoor wells (Spangler 2012).
| Lack of or unreliable supply of electricity, including a lack of fuel to run generators, and lack of water influenced health providers' ability to deliver quality care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 4 studies; ethics considerations were not reported in 3 studies; and sampling or data analysis methods were not reported in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | No to minor concerns, although data mainly represent Africa (3 studies), and electricity and water are vital for delivering quality care. |
| Adequacy | No to minor concerns; although description of the link between electricity/water and quality of care is thin, we consider this to be sufficient. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about methodological limitations |
| Contributing studies/setting | |
| Africa (3), S. Asia (1) Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries Anwar 2009: Bangladesh, basic and comprehensive emergency obstetric care facilities, public VSO 2012: Uganda, hospitals and health centres Pitchforth 2010: Ethiopia, teaching hospital | |
Lack of space and amenities as well as poor physical layout and organisation of wards also limited the provision of quality care (moderate confidence; Table 29) (Fränngård 2006,Khalaf 2009,Lester 2003,Molina 2011,Pettersson 2006,Pitchforth 2010). For instance, lack of space meant that some women had to deliver on the floor in corridors, and it was not possible to have companions in labour wards (Belizan 2007, Pitchforth 2010). Lack of space could also compromise women's privacy and dignity during labour (Khalaf 2009, Pitchforth 2010). The physical layout and separation of wards was sometimes counteractive to teamwork among health workers and interfered with the observation of mothers and their babies (Pettersson 2006). The lack of space and poor layout of wards could be further worsened by the large demand for delivery care (Molina 2011), in part due to unnecessary referrals from lower‐level facilities (Pettersson 2006), or policy changes that did not consider staffing and resources (Lester 2003). The large demand for delivery care could lead to overcrowding in health facilities. Together, overcrowding and limited physical infrastructure sometimes led to poor hand hygiene Ith 2012), a poor, stressful working environment for health workers (Fränngård 2006, Lester 2003), and incorrect diagnoses and medical errors (Khalaf 2009). A shortage of beds and overcrowding sometimes resulted in an increased risk of cross‐infection (Pettersson 2006), for instance when mothers and their babies had to share beds or use the floor. Overcrowding and limited infrastructure could also interfere with personalised care (Khalaf 2009), and limit the mobility of women in labour (Conde‐Agudelo 2008, DeMaria 2012). Health workers perceived hierarchical management between local health facility management teams and the national Ministry of Health; poor communication between these levels; and a lack of funds as barriers to the reorganisation of maternal wards (Pettersson 2006). Lack of funds and material resources sometimes prevented health facility managers from regularly maintaining physical infrastructure (low confidence; Table 30) (Ith 2012, Pitchforth 2010). Managers in one study queried the continued expansion of infrastructure when existing health facilities were not fully functional to provide good‐quality care (VSO 2012).
| The lack of space and amenities as well as poor physical layout and organisation of wards limited the delivery of quality care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 7 studies; ethics considerations were not reported in 1 study; sampling methods were not reported in 5 studies; and data analysis methods were not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns because data were from only 2 regions. |
| Adequacy | Minor concerns because data for some of the studies were thin. |
| Overall CERQual assessment | |
| Moderate confidence | Due to minor concerns about adequacy, relevance, and methodological limitations |
| Contributing studies/setting | |
| Africa (4), Latin America and Caribbean (4), Middle East & North Africa (1) Khalaf 2009: Jordan, maternal and child health centres Pitchforth 2010: Ethiopia, teaching hospital Pettersson 2006: Mozambique, tertiary hospital Belizan 2007: Argentina/Uruguay, public hospitals Fränngård 2006: Uganda, district hospital and health centres Conde‐Agudelo 2008: Colombia, public and private hospitals DeMaria 2012. Mexico, public and non‐governmental hospitals Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services Lester 2003: South Africa, maternity obstetric unit located in large academic hospital | |
| The lack of funds and material resources sometimes prevented health facility managers from regularly maintaining equipment and physical infrastructure. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 2 studies, and sampling strategy, ethical considerations, and methods of data analysis were not reported in 1 study. |
| Coherence | Minor concerns because we do not know why there was no maintenance in 1 study. |
| Relevance | No to very minor concerns |
| Adequacy | Moderate concerns because few studies with thin data reported this finding. |
| Overall CERQual assessment | |
| Low confidence | Due to minor concerns about coherence; and moderate concerns about methodological limitations and adequacy |
| Contributing studies/setting | |
| Africa (2), E. Asia (1) Pettersson 2006: Mozambique, tertiary hospital VSO 2012: Uganda, hospitals and health centres Ith 2012: Cambodia, provincial, regional hospitals and health centres | |
Health facilities varied in the availability, functionality, and quality of interventions assigned as signal functions for obstetric care (very low confidence; Table 31) (Afsana 2001, Spangler 2012). In one study, most of these functions, including provision of parenteral antibiotics, anticonvulsants, or neonatal resuscitation, were not available at lower‐level facilities (Spangler 2012). In the same study, some of these functions appeared to be available at higher‐level facilities, but functionality varied, for instance due to drug stock‐outs or unqualified providers of care.
| Health facilities varied in the availability, functionality, and quality of interventions assigned as signal functions for obstetric care. At the lower‐level facilities, most of these functions were not available, for instance parenteral antibiotics or anticonvulsants or neonatal resuscitation. At the higher levels, some of these functions appeared to be available, but functionality was variable, for instance when they had drug stock‐outs or unqualified providers of care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity and ethical considerations were not reported in 2 studies, 1 study was an observational study, no interviews with health providers. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because data were drawn from only 2 regions. |
| Adequacy | Moderate concerns because few studies with thin data reported this finding. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy |
| Contributing studies/setting | |
| Africa (1), S. Asia (1) Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries Afsana 2001: Bangladesh, health centre | |
One included study reported health worker perceptions on providing maternity care in health facilities compared to home (Blum 2006). These health workers felt it was easier to deliver care in facilities than at home (very low confidence; Table 32). Some of the positive aspects about delivering care at the health facility were that they were able to do other work while monitoring labour and provide care for several mothers, and that work schedules were more regular and care was available 24 hours a day. Furthermore, at facilities other skilled providers were available to assist when needed and some procedures, such as episiotomies, were easier to perform. In addition, health facilities could provide a secure, controlled, hygienic work environment, where electricity, equipment, and medications were always available.
| Health workers felt it was easier to deliver care in facilities than at home. Some of the positive aspects of delivering care at the health facility were that health workers were able to do other work while monitoring labour; provide care for several mothers; work schedules were more regular and care was available 24 hours a day. Furthermore, at facilities, other skilled providers were available to assist when needed, and some procedures (e.g. episiotomies) were easier to perform. In addition, health facilities provided a secure, controlled, hygienic work environment, where electricity, equipment, and medications were always available. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, though ethical considerations and reflexivity were not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because data are from only 1 study where a policy change allowed health workers to compare home‐based maternity care to facility‐based model of care. |
| Adequacy | Serious concerns because data are from only 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| S. Asia (1) Blum 2006: Bangladesh, home‐based maternity care | |
Referral mechanisms
When primary healthcare workers lacked the knowledge and skills to determine the need for referral or were unable to provide emergency care, poor‐quality care could result, such as mothers not being referred or inadequate care being offered at lower‐level facilities (very low confidence; Table 33) (Molina 2011).
| Where primary care workers in lower‐level facilities lacked the knowledge and skills to determine the need for referral, or were unable to provide emergency care, mothers could receive inadequate care. This lack of skills could also result in unnecessary referrals to other health facilities. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity, ethical considerations, and sampling methods were not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as only 1 region is represented. |
| Adequacy | Serious concerns, as included only 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| Latin America & Caribbean (1) Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services | |
When health workers referred mothers and their babies to higher levels of care, several factors were reported by health workers to interfere with the referral process. For instance, lack of trust and professional rivalries between midwives, doctors, and obstetrician gynaecologists could delay referral of mothers and their babies (Tabatabaie 2012). Midwives sometimes felt blamed by doctors when complications arose and hesitated to seek support from the medical teams at the receiving facilities (Tabatabaie 2012). Some midwives did not travel with mothers to the referring facility for fear of blame for any negative occurrences during the referral process (although this was also attributed to the scarcity of other health workers at the lower level) (low confidence; Table 34) (Ith 2012).
| Lack of trust and professional rivalries between midwives, doctors, and obstetrician gynaecologists could delay referral of mothers and their babies. Midwives sometimes felt blamed by physicians when complications arose and hesitated to seek support from the medical teams at the receiving facilities. Some midwives did not travel with the mothers to the referring facility for fear of blame for any negative occurrence during the referral process. | |
| Assessment for each CERQual component | |
| Methodological limitations | No or very minor concerns, though 1 study did not report reflexivity. |
| Coherence | No or very minor concerns |
| Relevance | Moderate concerns because in 1 study some midwives worked in private facilities but were referring mothers to public facilities, and only 2 regions represented. |
| Adequacy | Moderate concerns, as data are from few studies. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about adequacy and relevance |
| Contributing studies/setting | |
| E. Asia (1), Middle East & N Africa (1) Tabatabaie 2012: Iran, home births by midwives from hospitals and private clinics Ith 2012: Cambodia, provincial and regional hospitals, health centres | |
Respondents also felt that mothers' perceptions of the health system could also make them reluctant to accept referral (moderate confidence; Table 35). For instance, mothers were reported as being sceptical about the cost of care (Blum 2006, Graner 2010, Tabatabaie 2012); concerned about poor management and care at the next‐level facility, the procedures used, and the high levels of Caesarean sections; and fearful of complications (Barua 2011, Blum 2006, Graner 2010, Tabatabaie 2012). Mothers may also have already travelled far to reach the facility they perceived as a good one (Lester 2003), or feared unfamiliar urbanised settings (Blum 2006). As a result of mothers' reluctance to accept referral, health workers could spend a lot of time convincing reluctant mothers or their families (Blum 2006), or could feel pressured to conduct high‐risk deliveries or unnecessary procedures such as ultrasound scans to assess foetal condition (Graner 2010). In one study, health workers did ultrasound scans at seven to nine months to rule out deformity of the foetus and avoid blame by the mother and her family.
| Maternal perceptions of the health system could make mothers reluctant to accept referral. For instance, mothers were sceptical about the cost of care, poor management and care at the next‐level facility, the procedures used, the high levels of Caesarean sections, and fear of complications. Also, mothers may have already travelled far to reach the facility they perceived as a good one, or fear unfamiliar urbanised settings. As a result of mothers' reluctance to accept referral, midwives may feel pressured to conduct high‐risk deliveries or spend a lot of time convincing reluctant mothers or their families. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity was not reported in 4 studies, and ethical issues were not reported in 1 study. |
| Coherence | Minor concerns because while all of the studies support how women are reluctant to be referred, not all studies illustrate how this reluctance pressures health workers to conduct risky delivery. |
| Relevance | Minor concerns, as data are taken from health worker perceptions about mothers (indirect), and 1 study from Africa was conducted at a primary care unit in a tertiary centre. |
| Adequacy | Minor concerns due to thin data |
| Overall CERQual assessment | |
| Moderate confidence | Due to minor concerns about methodological limitations, coherence, relevance, and adequacy |
| Contributing studies/setting | |
| E. Asia & Pacific (1), S. Asia (2), Middle East & N Africa (1), Africa (1) Graner 2010: Vietnam, primary health care Blum 2006: Bangladesh, home‐based maternity care Tabatabaie 2012: Iran, home births by midwives from hospitals and private clinics Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals Lester 2003: South Africa, maternity obstetric unit located in large academic hospital | |
The presence of trust between mothers and midwives could influence mothers' willingness to be referred. Referral could be delayed when facilities lacked trusted midwives or other primary care workers to convince mothers of the need for referral ( very low confidence; Table 36) (Tabatabaie 2012). Where midwives or other primary care workers were available, they sometimes lacked the knowledge and communication skills to manage women's reluctance (Tabatabaie 2012).
| The presence of trust between mothers and midwives may influence a mother's willingness to be referred. Referral may be delayed when facilities lack midwives or other primary care workers whom the mothers trust that can convince mothers of the need for referral. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity unclear, and no ethical considerations reported. |
| Coherence | Minor concerns, as it was not clear if the data were related to the finding. |
| Relevance | Moderate concerns, as data refer to private providers referring mothers to public facilities. |
| Adequacy | Severe concerns, as only 1 study with thin data was included. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about coherence and methodological limitations; moderate concerns about relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| Middle East & N Africa (1) Tabatabaie 2012: Iran, home births by midwives from hospitals and private clinics | |
Lack of transport was reported to hinder referral of women and their babies to higher levels of care (Graner 2010), for instance when health facilities lacked ambulances (Molina 2011), or health facility budgets were insufficient to purchase fuel for vehicles (moderate confidence; Table 37) (Fränngård 2006,VSO 2012). Lack of fuel for vehicles when the need for referral arose was frustrating to nurses and midwives and left them feeling helpless when mothers' and babies' lives were at risk (very low confidence; Table 38) (VSO 2012). When health facilities lacked fuel for vehicles, mothers and their families were sometimes asked to pay their own transport costs, which many families could not afford (low confidence; Table 39) (Fränngård 2006,VSO 2012).
| Lack of transport hinders referral of women and their babies to higher levels of care. This happened for instance when health facilities lacked ambulances, or facility budgets were insufficient to purchase fuel for vehicles. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, though reflexivity was not reported in 3 studies, and ethics considerations were not reported in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns, as only 3 regions are represented, and in 1 region data are from 1 country. |
| Adequacy | Minor concerns due to very thin data |
| Overall CERQual assessment | |
| Moderate confidence | Due to minor concerns about relevance and adequacy |
| Contributing studies/setting | |
| E. Asia & Pacific (1), Africa (2), Latin America & Caribbean (1) Graner 2010: Vietnam, primary health care Fränngård 2006: Uganda, district hospital and health centres VSO 2012: Uganda, hospitals and health centres Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services | |
| Lack of fuel for vehicles when the need for referral arises is frustrating to nurses and midwives and leaves them feeling helpless when mothers' and babies' lives are at risk. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity, ethics considerations, sampling and data analysis methods were not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as only 1 region is represented. |
| Adequacy | Severe concerns because data are from only 1 study. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| Africa (1) VSO 2012: Uganda, hospitals and health centres | |
| When health facilities lacked fuel for vehicles, mothers and their families were sometimes asked to pay their own transport costs. Many families could not afford this. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, although reflexivity was not reported in 2 studies, and ethics considerations were not reported in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because data are from only 1 country representing 1 region. |
| Adequacy | Moderate concerns due to very thin data from 2 studies |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about relevance and adequacy |
| Contributing studies/setting | |
| Africa (2) Fränngård 2006: Uganda, district hospital and health centres VSO 2012: Uganda, hospitals and health centres | |
Several situations could lead health workers to refer mothers and shift responsibility to higher levels of care, including when they lacked the skills or confidence to provide care or when they worked in isolation (Blum 2006); when they were concerned about the facility's reputation when poor patient outcomes arose (Barua 2011); or when they lacked supplies, drugs, or equipment to provide care (low confidence; Table 40) (Ith 2012, Penfold 2013). When secondary‐level care was not available, mothers were sometimes referred to tertiary levels of care, which could result in congestion at the receiving facilities (very low confidence; Table 41) (Molina 2011). Unnecessary referrals resulted in increased workloads at higher levels of care (Penfold 2013).
| Several situations could lead health workers to refer mothers and shift responsibility to higher levels of care, including when health workers lacked the skills or confidence to provide care or when they worked in isolation; when they were concerned about the facility's reputation when poor patient outcomes arose; or when they lacked supplies, drugs, or equipment to provide care. Some of these referrals were unnecessary and resulted in increased workloads at higher levels of care. | |
| Assessment for each CERQual component | |
| Methodological limitations | No or very minor concerns, though ethical considerations were reported in 2 studies, and reflexivity was not reported in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as 1 study refers to health worker conducting home‐based deliveries without team support. |
| Adequacy | Moderate concerns due to few studies with thin data |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about adequacy and relevance |
| Contributing studies/setting | |
| S. Asia (3), E. Asia (1) Blum 2006: Bangladesh, home‐based maternity care Anwar 2009: Bangladesh, basic and comprehensive emergency obstetric facilities, public Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals Ith 2012: Cambodia, public maternity settings in provincial hospital, 2 regional hospitals, and 2 health centres | |
| When secondary‐level care was non‐existent, mothers were sometimes referred to tertiary‐level care, which resulted in congestion at the tertiary level. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity, ethics consideration, sampling methods were not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because only 1 region is represented. |
| Adequacy | Serious concerns because data are from only 1 study with very thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| Latin America and Carribbean (1) Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services | |
Administrative processes, including approval of mothers' insurance coverage, and poor communication, could influence the efficient referral of mothers and their babies to receiving units (very low confidence; Table 42) (Molina 2011). Lack of feedback from receiving to referring health facilities could influence midwives' practice and patient outcomes. Midwives perceived this information as useful for their practice and patient outcomes (very low confidence; Table 43) (Fränngård 2006).
| Administrative processes and paperwork and poor communication between referring and receiving levels of care could influence the efficient transfer of mothers and their babies to receiving units. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity, ethics consideration, sampling methods were not reported. |
| Coherence | Moderate concerns because it was unclear whether the data match our finding. |
| Relevance | Moderate concerns because only 1 region is represented. |
| Adequacy | Serious concerns because data are from only 1 study with very thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about coherence and relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| Latin America and Carribbean (1) Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services | |
| Lack of feedback between referring and receiving facilities could influence midwives' practice and patient outcomes. Midwives perceived this feedback as useful for improving their practice and patient outcomes. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, though reflexivity and sampling methods were not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because only 1 region is represented. |
| Adequacy | Severe concerns because data are from only 1 study. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| Africa (1) Fränngård 2006: Uganda, district hospital and health centres | |
Interaction between mothers, community members, and health workers
Poor attitudes and unethical behaviour among health workers could influence the quality of care. Examples of this included when health workers were harsh, rude, or impatient with mothers (Afsana 2001, Hassan‐Bitar 2011,VSO 2012); when they displayed poor cultural sensitivity, for instance by not maintaining women's privacy (Afsana 2001,Spangler 2012); or when they were absent from their duty stations or involved in the illegal sale of drugs and supplies or expected "back door" payments for services (low confidence; Table 44) (Spangler 2012). Study participants suggested several reasons for these behaviours, including wrong intrinsic reasons for joining the nursing profession (VSO 2012), long, solitary working hours, physical exhaustion, and the perpetual responsibility of looking after mothers (Hassan‐Bitar 2011, VSO 2012). These could lead midwives to show tough/harsh behaviour and lack of patience with mothers (Hassan‐Bitar 2011, VSO 2012), or could lead them to be absent when expected to provide 24‐hour care in health centres (Spangler 2012, VSO 2012). System‐wide behavioural and attitudinal problems were thought to explain why health workers displayed underdeveloped cultural sensitivity and weak interpersonal communication (Spangler 2012).
| Poor attitude and unethical behaviour among health workers could influence the quality of care, such as when health workers are harsh, rude, or impatient with mothers; display poor cultural sensitivity, e.g. by not maintaining women's privacy; or when health workers are absent from their duty stations or involved in the illegal sale of drugs and supplies or expect 'back door' payments for services. Some of the suggested underlying reasons for these attitudes and behaviours were wrong intrinsic reasons for joining the profession and physical exhaustion from the long, solitary hours of work. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 3 studies; ethical considerations were not reported in 2 studies; and sampling methods were not clear in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns because few regions represented. |
| Adequacy | Moderate concerns because data are from few studies, some with thin data. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about methodological limitations and adequacy; and minor concerns about relevance |
| Contributing studies/setting | |
| Africa (2), Middle East & N. Africa (1), S. Asia (1) Hassan‐Bitar 2011: Palestine, public referral hospital Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries VSO 2012: Uganda, hospitals and health centres Afsana 2001: Bangladesh, health centre | |
Mothers' participation in decision‐making during labour could be limited by health worker attitudes and authoritarian behaviour. Health workers sometimes conducted procedures without asking mothers for their opinion (de Carvalho 2012), or did not seek feedback from mothers about practices or outcomes (Belizan 2007), but expected mothers to co‐operate (DeMaria 2012). One reason for this lack of participation appeared to be health workers’ attitudes and assumptions about the mother's capabilities, preferences, and role during delivery of her baby (low confidence; Table 45). Health workers in some studies believed that certain decisions about care did not concern the mother (de Carvalho 2012), and did not want to be restrained by the mother's or her companion's preferences (Belizan 2007, Conde‐Agudelo 2008). These health workers believed that the woman in labour was in no condition to give her opinion about what was best for her and the baby (de Carvalho 2012), or that her low socioeconomic status, lack of information, or family problems made her unwilling or unable to provide input (Belizan 2007, Maputle 2010), and that women were comfortable leaving decision‐making to health workers (Maputle 2010). Some midwives found this lack of participation stressful, for example when mothers did not voice their opinions about their care (Maputle 2010). Some midwives indicated that they promoted, supported, and respected mothers' preferences as long as they were not harmful to mother and baby (Maputle 2010).
| Mothers' participation in decision‐making during labour could be limited by health worker attitudes and authoritarian behaviour, for instance when health workers conducted procedures without asking mothers for their opinion, or physicians did not seek feedback from patients about practices or outcomes and expected women to co‐operate. Lack of patient participation in decision‐making can threaten quality of care. Some of the reasons for this behaviour were related to health workers’ attitudes about the woman's preferences and role during delivery of her baby. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 4 studies; ethics considerations were not reported in 1 study; and sampling methods were not clear in 3 studies. |
| Coherence | Minor concerns because there were several reasons authoritarian behaviour and poor attitudes of health workers could explain mothers' non‐participation in decision‐making. Other explanations could be women’s lack of empowerment and cultural reasons on how to behave. |
| Relevance | Moderate concerns because only 2 regions were represented. |
| Adequacy | Minor concerns because data are from few studies. |
| Overall CERQual assessment | |
| Low confidence | Due to minor concerns about coherence and adequacy; and moderate concerns about methodological limitations and relevance |
| Contributing studies/setting | |
| Africa (1), Latin America & Caribbean (4) de Carvalho 2012: Brazil, university teaching hospital Belizan 2007: Argentina/Uruguay, public hospitals Maputle 2010: South Africa, tertiary care hospital Conde‐Agudelo 2008: Colombia, public and private hospitals DeMaria 2012: Mexico, public and non‐governmental hospitals | |
Some health workers did not value communication with mothers, communicated poorly, or said they had problems with communication. Poor communication and interaction could threaten the trust between health workers and mothers (very low confidence; Table 46). Some studies reported that health workers considered communication with mothers as a waste of time (Hassan‐Bitar 2011), and described situations where there was insufficient communication between staff and families (de Carvalho 2012,Hassan‐Bitar 2011), or where skilled birth attendants were abrasive and demeaning in their interaction with women and showed no concern for women's families, for instance women were reprimanded when they arrived late in labour, refused to expose their genitalia, or had too many children (Blum 2006). Language barriers could interfere with effective communication between mothers and health workers (Maputle 2010, DeMaria 2012). As a result, mothers sometimes appeared not to listen to health workers while health workers mechanically worked through the process of providing care (Maputle 2010) . Some health workers acknowledged the need to respect and involve men, women's families, and the community in maternal health, for example in understanding cultural beliefs related to postpartum care (Lugina 2001).
| Some health workers did not value communication, communicated poorly, or said they had problems with communication. Poor communication and interaction could threaten the trust between health workers and mothers, for instance when health workers considered communication with mothers a waste of time and there was insufficient communication between staff and families, or when skilled birth attendants were abrasive and demeaning in their interactions with women and showed no concern for women's families. Language barriers could interfere with effective communication between mothers and health workers. As a result, mothers sometimes appeared not to listen to health workers while health workers mechanically worked through the process of providing care. Health workers acknowledged the need to respect and involve men, women's families, and the community in maternal health, for example in understanding cultural beliefs related to postpartum care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Serious concerns because reflexivity was not reported in 3 studies; sampling methods were not clear in 2 studies; ethical considerations were not reported in 1 study; and data analysis methods were not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because only 4 regions were represented. |
| Adequacy | Moderate concerns because data are from few studies with thin data, and in 2 studies it is unclear if data support finding. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about relevance and adequacy; and serious concerns about methodological limitations |
| Contributing studies/setting | |
| Africa (2), Latin America & Caribbean (1), Middle East & N. Africa (1) Hassan‐Bitar 2011: Palestine, public referral hospital de Carvalho 2012: Brazil, university teaching hospital Blum 2006: Bangladesh, home‐based maternity care Maputle 2010: South Africa, tertiary care hospital Lugina 2001: Tanzania, municipal hospitals | |
In contrast, other health workers described how they valued the appreciation, respect, trust, and praise they received from mothers (Bradley 2009,VSO 2012), making friends among mothers, or working with the community (Bradley 2009,Fränngård 2006). Midwives in particular were delighted when a baby was given their name and to see the baby grow (low confidence; Table 47) (VSO 2012).
| Health workers valued the appreciation, respect, trust, and praise from patients, or when they made friends among mothers or worked with the community. Midwives in particular were delighted when a baby was given their name and seeing the baby grow. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because ethical considerations were not reported in 2 studies; reflexivity was not reported in 3 studies; sampling strategy was not clear in 2 studies; and data analysis methods were not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because only 1 region is represented. |
| Adequacy | Moderate concerns because data are from few studies with very thin data. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy |
| Contributing studies/setting | |
| Africa (3) VSO 2012: Uganda, hospitals and health centres Bradley 2009: Malawi, rural mission hospitals Fränngård 2006: Uganda, district hospital and health centre level IV | |
Some studies reported how a mismatch between peoples' expectations of health workers and what health workers were actually able to deliver or thought was appropriate could lead to antagonism. For instance, health workers that delivered home‐based care could experience social pressure from families and communities, such as to give injections to speed up delivery as opposed to waiting for labour to progress normally (Blum 2006). Families might not understand why a health worker had to refer the mother to hospital, or the community might prefer a different delivery practice from what the health worker could provide (Blum 2006). Health workers providing maternity care at health facilities were sometimes treated harshly by people from the community when there was a lack of supplies and materials (Hassan‐Bitar 2011). In addition, misconceptions that midwives were not working when they took a break from their work (VSO 2012), or that health workers sold drugs threatened the trust between health workers and the community (low confidence; Table 48) (Blum 2006).
| Mismatch between people's expectations of health workers and what health workers were actually able to deliver or thought was appropriate could lead to antagonism. For instance, health workers who delivered home‐based care could experience social pressure from families and communities, e.g. to give injections to speed up delivery as opposed to waiting for labour to progress normally. Health workers providing obstetric care at health facilities were sometimes treated harshly by people from the community when there was a lack of supplies and materials. In addition, misconceptions that midwives were not working when they took a break from their work or that health workers sold drugs threatened the trust between health workers and the community. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 3 studies; sampling was not reported in 2 studies; ethical considerations were not reported in 2 studies; and data analysis methods were not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because data are from only 3 regions, and data seem to relate more to midwives and nurses than to doctors. |
| Adequacy | Moderate concerns due to thin data |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy |
| Contributing studies/setting | |
| Middle East & N Africa (1), S. Asia (2), Africa (1) Hassan‐Bitar 2011: Palestine, public referral hospital Blum 2006: Bangladesh, home‐based maternity care VSO 2012: Uganda, hospitals and health centres Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals | |
In one study, midwife‐led shared care was perceived to improve the interaction between mothers, families, and health workers, and could improve health workers' self esteem and lead to a change in hospital culture with respect to service provision (very low confidence; Table 49) (Fujita 2012). In this study, midwife‐led shared care increased communication between midwives, women, and their families; enabled the presence and participation of family members; and increased satisfaction in the care provided. As a result, the need for medication during delivery was minimised, which in turn reduced the financial burden experienced by families. The supportive environment for mothers, the good interaction between mothers and health workers, as well as recognition of professional expertise among midwives increased self esteem. Midwife‐led shared care enabled other hospital staff to reflect on their own routine activities and manner of communication with families and clients, leading to a change in hospital culture with respect to service provision (Fujita 2012).
| Midwife‐led shared care was perceived as improving the interaction between mothers, families, and health workers, and could improve health workers' self esteem and lead to a change in hospital culture with respect to service provision. For instance, midwife‐led shared care increased communication between midwives, women and their families; enabled the presence and participation of family members; and together increased satisfaction in the care provided. As a result, the need for medication during delivery was minimised, which reduced the financial burden experienced by families. The supportive environment for mothers, the good interaction between mothers and health workers, as well as recognition of professional expertise among midwives increased self esteem. Midwife‐led shared care enabled other hospital staff to reflect on their own routine activities and manner of communication with families and clients, leading to a change in hospital culture with respect to service provision. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported, and sampling strategy was not clear. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because only 1 region was represented. |
| Adequacy | Serious concerns because data are from only 1 study. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about relevance; and severe concerns about adequacy |
| Contributing studies/setting | |
| Africa (1) Fujita 2012: Benin, tertiary hospital | |
Interaction between health workers
Disrespectful communication, lack of trust, poor teamwork and co‐ordination, and inadequate opportunities to discuss clinical practice could lead to poor interprofessional relations. Tensions could also arise when health workers did not recognise each others' capabilities or when they acted in a way that reinforced clinical hierarchies (low confidence; Table 50). Some studies reported instances of disrespectful interprofessional communication (Hassan‐Bitar 2011, Pettersson 2006). For instance, when doctors shouted at midwives, midwives could feel humiliated and lack confidence, and lead them to believe that they were not trusted, or that their opinions were not welcomed and could delay the delivery of care (Pettersson 2006). Midwives with lower levels of training reported feeling marginalised and less motivated to provide care because midwives with higher levels of training and doctors used their qualifications, status, and roles to dominate clinical practice (Ith 2012). Tensions were also reported between doctors and clinical officers due to differences in salary, benefits, workload, and status (Bradley 2009). Some studies reported a lack of understanding of competencies and alternative models of care. For instance, doctors did not always have a clear understanding of the midwifery profession, which could result in conflict or professional jealousy (DeMaria 2012). Teamwork could also be threatened when doctors worked in a small number of shifts, and had minimal contact with other professionals (Belizan 2007), or when staff meetings were infrequent (Hassan‐Bitar 2011). This sometimes resulted in lack of co‐ordination and varying decision‐making procedures and standards of care (Belizan 2007, Hassan‐Bitar 2011).
| Disrespectful communication, lack of trust, inadequate opportunities to review clinical practice, and poor teamwork and co‐ordination could lead to poor interprofessional relations. Also, tensions could arise when health providers did not recognise each others' capabilities and when acting in a way that reinforces clinical hierarchy, for instance disrespectful interprofessional communication between physicians and midwives. Midwives with lower‐level training could manage normal birth, but they sometimes felt marginalised and less motivated to provide care because midwives with higher levels of training and doctors used qualification, status, and their roles to dominate clinical practice. Tensions were sometimes reported between doctors and clinical officers due to salary differentials, benefits, workload, and status. There was sometimes a lack of understanding of competencies and alternative models of care. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns though reflexivity was not reported in 4 studies; ethical considerations were not reported in 1 study; and sampling methods were not clear in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because models of care, scope of practice, and cadre differed in various settings and may not apply in different context; only 3 regions represented. |
| Adequacy | Moderate concerns because data are from few studies. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about relevance and adequacy |
| Contributing studies/setting | |
| Africa (1), Latin Am & Caribbean (1), E. Asia (1) Bradley 2009: Malawi, rural mission hospitals DeMaria 2012: Mexico, public and non‐governmental hospitals Ith 2012: Cambodia, provincial, regional hospitals and health centres | |
Nurses and midwives valued and were motivated by a good team dynamic where health workers provided feedback, supported, and co‐operated to ensure all shifts were covered (low confidence; Table 51) (Bradley 2009,Fränngård 2006). For instance, midwives in one study valued good interprofessional collaboration, which made them feel accepted as part of the professional team and provided an opportunity to improve their competence through on‐the‐spot education provided by obstetricians (Pettersson 2006). In another study, midwives worked together in a team led by midwives, which increased their ability to share experiences and new practices and their decision‐making responsibility, improved their self esteem, provided quality assurance, and improved the quality of care provided (Lester 2003). In one study, researchers observed that nurses had a strong teamwork ethic and functioned well together to complete work (Foster 2006).
| Nurses and midwives valued and were motivated by a good team dynamic where health workers provided feedback, supported and co‐operated to ensure all shifts were covered. For instance, midwives valued good interprofessional collaboration, which made them feel accepted as part of the professional team and provided them an opportunity to improve their competence through on‐spot education provided by obstetricians. When midwives worked together in a team led by midwives, this increased their ability to share experiences and new practices and their decision‐making responsibility; improved their self esteem; and provided quality assurance and improved the quality of care provided. This teamwork was especially useful when emergencies arose. In another study, researchers observed that nurses had a strong teamwork ethic and functioned well together to complete work. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, though reflexivity was not reported in 4 studies; ethics considerations were not reported in 2 studies; data analysis methods were not clear in 2 studies; and sampling was not clear in 3 studies. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because only 2 regions are represented. |
| Adequacy | Moderate concerns due to thin data |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about relevance and adequacy |
| Contributing studies/setting | |
| Africa (3), Latin Am & Caribbean (1) Pettersson 2006: Mozambique, tertiary hospital Bradley 2009: Malawi, rural mission hospitals Fränngård 2006: Uganda, district hospital and health centre IVs Foster 2006: Dominican Republic, hospital | |
Factors tied to the microenvironment
We have used the term 'microenvironment' to describe the broad structural context within which health workers and those who support them deliver maternity care. Some of the included studies reported data on health workers' views and perceptions of professional associations and sociocultural factors. None of the studies reported data on health worker views and perceptions of legislation, regulation, financing, or broader governance or policy issues.
Professional associations
Health workers had conflicting views on the role of professional councils (very low confidence; Table 52). For instance, some perceived professional councils as advocates for their members, while others perceived them as a regulatory bodies with punitive functions (VSO 2012).
| Health workers had conflicting views on the role of professional councils. For instance, some viewed professional councils as advocates for their members, while others considered them to be a regulatory body with punitive functions. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because ethical considerations, reflexivity, sampling and data analysis methods were not reported. |
| Coherence | No or very minor concerns |
| Relevance | Moderate concerns because data were from only 1 study and represented only 1 region. |
| Adequacy | Serious concerns because data were from only 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about methodological quality and relevance; and severe concerns about adequacy |
| Contributing studies/setting | |
| Africa (1) | |
Social/cultural environment
Sociocultural barriers sometimes hindered mothers from receiving care in hospitals (low confidence; Table 53). For instance, some women preferred not to be examined by male health providers (Khalaf 2009), or preferred a particular position in which to deliver for cultural reasons, but preference for that birthing position may not have been accepted by the health worker (Blum 2006). In other instances, mothers did not divulge information that was needed for their care for religious reasons (Thorsen 2012).
| Sociocultural barriers sometimes hindered mothers from receiving care in hospitals. For instance, women preferred not to be examined by male health providers for cultural reasons, preferred a particular position in which to deliver, or for religious reasons did not divulge information that was needed for their care. | |
| Assessment for each CERQual component | |
| Methodological limitations | No or very minor concerns, though reflexivity was not reported in 4 studies, and ethical considerations were not reported in 2 studies. |
| Coherence | No or very minor concerns |
| Relevance | Moderate concerns because data were from health worker perceptions about mothers and represented only 3 regions. |
| Adequacy | Moderate concerns because data were from only 3 studies, 2 of which had thin data. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about adequacy and relevance |
| Contributing studies/setting | |
| Africa (1), Middle East & N Africa (1), S. Asia (1) Khalaf 2009: Jordan, maternal and child health centres Thorsen 2012: Malawi, a secondary and tertiary hospital Blum 2006: Bangladesh, home‐based maternity care | |
On the other hand, professional midwives and obstetric nurses perceived themselves as empathetic and having a gender advantage for delivering maternity care. They therefore considered themselves better placed than male providers to attend low‐risk births (DeMaria 2012).
Integrating the findings from this synthesis with the findings of relevant Cochrane intervention reviews
Our synthesis identified a number of factors that were considered important by health workers for the delivery of intrapartum and postpartum care. We classified several of these factors as health service inputs, including health worker training; available human resources; access to equipment, drugs, supplies, blood, electricity, water, and transport for referral; physical infrastructure, in particular available space and layout of wards; and interprofessional communication and teamwork. In Table 54 we have presented our matrix model mapping these factors against the interventions in studies included in Dudley 2009. At the time of publication of this synthesis, the Dudley review was not yet completed, so this synthesis includes a matrix table based on the studies that have been included to date. The findings in the matrix may change when the full effectiveness review findings are available. We will consider the data on effects of the intervention when the related review is completed.
| Health services inputs identified as important in this synthesis | |||||||||||
| Intervention studies selected from Dudley 2009 review | Number of health workers to manage workload | Other human resource strategies | Training of health workers | Communication strategies | Access to available and functional equipment | Sufficient drugs and supplies | Regular reliable electricity or alternative source of power | Blood supply and infrastructure | Transport for referral or alternative mechanism for transport | General infrastructural inputs, e.g. renovating, reorganisation of wards | Other health services input |
| Manandhar 2004 | No information | No information | Training in essential newborn care of government health staff, CHW, and TBA | No information | Equipped primary care centres with Resuscitaires, phototherapy | Essential neonatal drugs/discussions on resupply with managers | No information | No information | No information | No information | No information |
| Lui 2003 | No information | Task‐shifting ‐ village doctors (assume these are CHW take on health education tasks of midwives) | Training in project management (heads of counties and health teams) | No information | No information | No information | No information | No information | No information | Established EMOC centres for training of BEMOC staff, technical assistance, referral | Quality improvement of hospital (not clear what this entailed) |
| Pardeshi 2011 | Employed staff to fill vacant positions. New cadre, general nurse‐midwife appointed at PHC level | No information | MOs trained in lifesaving anaesthesia skills, MOs and paramedics trained in essential obstetric care | No information | Provided oxygen cylinders, baby warmers | No information | Inverters and solar heaters (electricity backup) at PHC level | Blood storage facility at first‐referral levels | Provided funds for transport during emergencies | Infrastructural improvements, e.g. delivery rooms constructed, repairs and renovations at PHC level | Food and escorts (peer supporters?) during inpatient stay, gave clothes and coconut to mother at discharge |
| Powell‐Jackson 2009 | No information | Pay‐for‐performance of health worker, e.g. attend home birth, conduct facility delivery | No information | No information | No information | No information | No information | No information | No information | No information | No information |
| Wu 2011 | No information | No information | Training of midwives on prenatal care of rural women | No information | No information | No information | No information | No information | No information | No information | No information |
| Tripathy 2010 | No information | No information | Training of front‐line health staff in appreciative inquiry | No information | No information | No information | No information | No information | No information | No information | Health committees for community input into health services design and management |
| Colbourn 2013 | No information | No information | Training health staff in QI methodology (used Plan‐Do‐Study‐Act cycles) | No information | No information | No information | No information | No information | No information | No information | No information |
| Kirkwood 2013 | No information | No information | Training in essential newborn care | No information | No information | No information | No information | No information | No information | No information | Discussions about newborn care practice between district, subdistrict management teams, and health workers at facilities to harmonise practice |
| Amudhan 2013 | Recruited additional auxiliary nurse midwife to PHC level | No information | No information | No information | No information | No information | No information | No information | No information | Upgraded PHC to provide 24‐hour service (not clear what this entailed) | No information |
| Ensar 2014 | No information | No information | No information | No information | Equipped health facilities | Provided supplies for health facilities | No information | No information | Motorcycle ambulances at health centres. Maintenance by the community | No information | No information |
| Pasha 2013 | No information | No information | Training of providers in EMONC | No information | No information | No information | No information | No information | No information | No information | Quality improvement activities (maternal and perinatal audits, facility reviews) |
Manandhar 2004: Setting: Nepal, community. Participants: women in reproductive age group.
Lui 2003: Setting: China, community. Participants: poor pregnant women, managers of target county and health bureaus, obstetric medical staff of township hospitals.
Pardeshi 2011: Setting: India, community. Participants: women who had delivered in the five months prior to the survey.
Powell‐Jackson 2009: Setting: Nepal. Participants: women with fewer than two children, delivering at a health facility. Doctors, nurses, midwife, health assistant, auxiliary health worker, or maternal child health worker attending a delivery at home or in a public health facility.
Wu 2011: Setting: China, community. Participants: midwives based at township hospitals, pregnant mothers.
Tripathy 2010: Setting: India, community. Participants: women in reproductive age group who had recently given birth; cluster‐level village health committees, front‐line government health staff.
Colbourn 2013: Setting: Malawi, community. Participants: pregnant women, health workers at dispensaries and health centres.
Kirkwood 2013: Setting: Ghana, community. Participants: pregnant women and their newborn babies; community‐based surveillance volunteers.
Amudhan 2013: Setting: India, community. Participants: pregnant women of low socioeconomic status.
Ensar 2014: Setting: Zambia, community. Participants: pregnant women, the community including men, women (including older women), and community leaders.
Pasha 2013: Setting: multicentre trial in India, Pakistan, Kenya, Zambia, Argentina, and Guatemala. Participants: pregnant women and their newborn babies, families at community level, community birth attendants, facility‐based healthcare providers.
Abbreviations: BEMOC(basic emergency obstetric care), CHW(community health worker), EMOC(emergency obstetric care),EMONC(emergency obstetric and neonatal care),MO(medical officers), PHC(primary health care), QI(quality improvement), TBA (traditional birth attendant).
Whereas the studies included in this synthesis were conducted among health workers based at health facilities, studies in the Dudley review were largely community‐based studies that targeted pregnant women and their families. The studies in the intervention review focused on a different phase of skilled birth attendance, that is demand generation, whereas studies in our synthesis focused on the supply side. Therefore, when linking the findings from this synthesis to the Dudley review, we considered only 11 intervention studies that included health system strengthening components as part of the intervention. We considered these 11 studies comparable to the studies included in this synthesis given the focus on supply‐side factors for providing maternity care.
Overall, very few of the factors identified as important in our synthesis appear to have been specifically addressed in the 11 studies in the Dudley review. Most of the studies addressed between one and four of these factors. Eight of these studies included health worker training as part of the intervention. This training was focused largely on the technical skills of the health workers, apart from one study that provided training in project management and another on appreciative inquiry. None of the studies included training on communication for health workers. Additional factors that were included by at least one intervention study were the recruitment of additional health workers, the use of task‐shifting or pay for performance approaches, improvement in supplies and provision of equipment, improvements in physical infrastructure such as renovation, and the establishment of emergency obstetric care (EmOC) centres and the upgrading of units to provide 24‐hour care.
Only one of the intervention studies included a broad range of health system changes (Pardeshi 2011). This study assessed the trend in facility deliveries following a seven‐year programme to improve access and strengthen health services in rural India. In this study, delivery rooms were constructed, repairs and renovations at the primary healthcare level were done, a blood storage facility was provided at first referral levels, inverters and solar heaters (electricity backup) were made available at the primary care level, vacant positions were filled, funds were provided for referral transport, and equipment, including oxygen cylinders and baby warmers, was provided.
It is perhaps unsurprising that most interventions included training, given that training courses may be easier to organise and demand less time and resources than other inputs such as infrastructural changes. However, we suggest that future intervention studies also take into account other factors identified by our synthesis. The presence or absence of these factors could also serve as the basis for subgroup analyses in systematic reviews of the effectiveness of these types of interventions.
Discussion
Summary of main results
This synthesis included evidence from 31 studies from low‐ and middle‐income countries on factors that influence the provision of intrapartum and postnatal care among skilled birth attendants and those who support them. Key findings for which we had high or moderate confidence focused on education, human resources, health services infrastructure, referral mechanisms, and interaction between health workers.
The synthesis shows that inadequate pre‐service and in‐service training limited health workers' skills and their ability to provide quality care (high confidence). While on‐the‐job training provided opportunities for improving these skills, opportunities were limited by the cost, availability, and varying quality of training (moderate confidence).
The problem of staff shortages was widely reported and could increase health workers' workloads and compromise their ability to provide care. A lack of specialists or experienced staff could lead to problems with supervision and situations where emergency obstetric care was not provided or was provided by less qualified staff. These issues, coupled with poor living and working conditions, caused health workers stress and frustration, and affected their family life. The synthesis highlights a number of possible causes for staff shortages, including inadequate hiring and deployment of staff, limited funding, poor management and bureaucracy, poor salaries, and other factors that influence retention of health workers. In addition, health workers perceived managers as lacking in management capacity and skills and sometimes felt unsupported when concerns about the workplace were left unheard. We had moderate confidence in these findings.
Lack of equipment, insufficient supply, and/or lack of drugs; lack of blood or the limited infrastructure to manage blood transfusion; lack of or unreliable supply of electricity, including a lack of fuel to run generators; and lack of water limited health workers' ability to provide quality care to mothers and their babies. Lack of equipment, supplies, or drugs resulted in low morale among health workers, wasted health workers' time, and increased their workload and risk of infection. The lack of space and amenities as well as poor physical layout and organisation of maternity wards also limited the provision of quality care. We had high confidence in the finding that lack of equipment limits health workers ability to deliver care, and moderate confidence in all other findings.
Respondents felt that maternal perceptions of the health system sometimes made them reluctant to accept referral. Lack of transport including lack of ambulances or funds to fuel vehicles for transport to higher levels of care hindered referral. We had moderate confidence in these findings.
Health worker interprofessional relations were sometimes limited by disrespectful communication, lack of trust, poor teamwork and co‐ordination, and inadequate opportunities to discuss clinical practice. Tensions arose when health providers did not recognise each others' capabilities, and when they acted in ways that reinforced clinical hierarchy. We had moderate confidence in these findings.
Other factors that we considered to be important, but for which we had low or very low confidence in the findings, are as follows:
-
how staff shortages and heavy workload interfered with health workers' interaction with mothers;
-
lack of protocols/standards of practice or guidelines, or where they were inconsistent or health workers were unaware of them could influence patient care and cause harm;
-
lack of time, limited infrastructure and skills in research appraisal influenced health workers' ability to seek knowledge on current recommended practice;
-
lack of health worker knowledge and skills to determine the need for referral;
-
lack of trust between health workers and mothers and lack of interprofessional trust between health workers at referring and receiving health facilities may delay referral of mothers to higher levels of care. Good interprofessional collaboration and teamwork, e.g. through midwife‐led shared care, influenced health worker motivation, decision‐making ability, quality of care, and hospital culture with respect to service provision.
Overall completeness and applicability of evidence
This synthesis found that poor quality of pre‐service training and other barriers to on‐the‐job training were among the reasons for variations in health workers' competence and skills. This finding implies that health workers who have had poor‐quality pre‐service training may not improve their skills during in‐service training. Furthermore, a lack of supervision and follow‐up of trainees means that the benefits of training may not be fully obtained. Although on‐the‐job training courses are often available in many settings, managers need to consider how to fully maximise benefits from this training, for instance by ensuring that it reflects the needs of health workers and by developing a coherent strategy to support and follow up trainees. Some of the training needs identified from this synthesis included: management of complicated pregnancies or deliveries, management of home births, alternative delivery positions, epidemiology, research appraisal, or critical thinking about clinical practice.
This synthesis also illustrates how health workers' abilities to provide care to mothers and their babies were limited by the poor equipment, drugs, supplies, and physical infrastructure available at the health facilities. Our findings reflect system‐wide challenges, and how these deficiencies influence the technical quality of care provided by health workers; health worker morale and their sense of personal safety; and show the extra financial costs to mothers and their families. In addition, our synthesis reflects how these systemic challenges influence the implementation of patient‐centred, dignified, 24‐hour care, and how they can lead to the creation of informal markets at health facilities and other health system challenges such as corruption, absenteeism, and dual practice. The importance of an enabling environment in order for health workers to deliver good‐quality care has been emphasised previously (Maclean 2003). Although the United Nations' fifth Millennium Development Goal (MDG) era promoted access to health facilities and skilled birth attendance, basic infrastructure and logistics management at health facilities remain a challenge in several settings (Adair‐Rohani 2013).
Our findings suggest that the shortage of personnel and resulting workload led health workers to increase their scope of practice or task‐shifting to another cadre. This may have been made possible in part through vague job descriptions that allowed managers to assign any job to a health worker. Whereas formal task‐shifting is seen as a remedy for human resource shortages, our findings suggest that informal task‐shifting may have implications for quality of care, for example when specialists are lacking and emergency maternity care is provided by poorly trained or unqualified health workers. In addition, our findings indicate that task‐shifting may further increase workload for a workforce that already feels underpaid for work done. The review by Colvin 2013 similarly identified inadequate training, unclear job descriptions, and health worker concerns about increased workload as among the challenges to implementing task‐shifting. These factors are important for managers to consider when implementing task‐shifting.
Several of our findings suggested the importance of building trust between health workers, mothers, and communities, as well as between health worker teams. In a study by Sheppard 2004, health worker communication skills and women’s perceptions of institutional barriers are identified as factors that may influence the building of trust between patients and health workers. With regard to trust between health workers, a review by Zwarenstein 2009 suggests that incorporating routines such as interprofessional meetings and ward rounds into clinical practice supports health worker interaction and can improve healthcare processes and outcomes.
At the start of this synthesis process, we did not intend to document health worker perceptions regarding respectful care of women during childbirth. However, there was increasing interest in this topic among the global health community during the development of this synthesis (Bohren 2015). While it is neither ethical nor acceptable for health workers to disrespect women, our findings may at least partly explain why this phenomenon occurs. Our findings indicate that poor training and harsh working conditions, a lack of supplies, long, solitary hours of work, and disrespect from colleagues may jeopardise health workers’ abilities to display support, empathy, and friendliness to women in labour.
Stress, physical exhaustion, and the emotional demands of the job may leave health workers emotionally worn out, and therefore incapable of providing social support to mothers under their care. Other studies have described a similar phenomenon, where health workers distance themselves from their patients, for example by not emotionally connecting with patients under their care as a coping strategy for stressful work conditions (Van Der Walt 1999), or where the health system does not provide health workers with support for such emotional care (Petersen 2002). We also hypothesise that when working under difficult conditions, health workers may place good social interaction and care lower in the hierarchy of quality of care than other medical interventions. In addition, most health workers that provide maternity care are female and may have experienced several forms of disempowerment in the workplace, and are therefore not able to advocate within the health system for better treatment of the women they care for. As a result, poor health worker‐mother interaction may be normalised as part of the 'culture' of the health system in some settings, and both health workers and mothers may come to accept this as the norm (Bohren 2017, Rominski 2017, Sadler 2016). The perspective of Leape and colleagues on the nature and causes of disrespectful behaviour by physicians supports this hypothesis (Leape 2012). Here, the authors argue that when some practices become ingrained in the health system, they may not be recognised as wrong and may become routine. Our finding that health workers themselves experienced disrespectful interprofessional communication at the health facility supports this hypothesis.
This synthesis included studies that represented a broad range of cadre and settings in low‐ and middle‐income countries. Participants were drawn from a broad range of cadre from tertiary, secondary, and primary settings, and included managers and others who support health workers to deliver maternity care. Two studies were conducted among facility‐based health workers that delivered care in the community or at private clinics. Most studies were conducted in settings that used mixed models of maternity care; two studies were conducted in midwifery‐led units. However, several of the findings were only drawn from a narrow range of cadre and settings, which may have influenced our confidence in these findings.
Our synthesis included few studies that addressed health worker perceptions of sociocultural barriers and professional associations, factors in the broad macroenvironment that influence health workers' delivery of care. This synthesis was based on a broad search, but did not retrieve or include studies that addressed health worker perceptions of upstream system‐level factors on governance, policy, financing, logistics, or legislation. Some of these studies may be published in grey literature, which we did not search. These data are important since the broader issues influence the work and life of a health worker at the front‐line of the health service, for example how policies or policy changes, or different financing models affect health workers' ability to provide maternity care.
Our synthesis focused on intrapartum and postnatal care. However, most of the included studies focused on intrapartum care, with only two focusing on postpartum care. This may reflect the body of literature and attention given to intrapartum care. We did not intend to include qualitative studies that focused on antenatal care, as this topic is covered in a separate review (Downe 2016). In addition, we sought to extract data on both barriers as well as facilitators reported by health workers. However, the included studies largely reported data on barriers, and we identified minimal data on facilitators. Whereas it has been suggested that facilitators are the opposite of barriers, this may not always be the case. However, we did not find sufficient data to support or refute this argument.
We used the CERQual approach to assess relevance and adequacy of data from the included studies that contributed to individual findings (see Methods section). These assessments reflect the applicability and completeness of data contributing to a finding. See additional information in the section below.
Confidence in the findings
Based on our CERQual assessments, we had high confidence in two findings and moderate confidence in 16 findings that the studies were a good representation of the phenomenon of interest. We had several findings where we had low or very low confidence that the studies were a good representation of the phenomenon of interest, and it was therefore difficult to draw conclusions from these findings. Our main concerns were connected to the methodological limitations of the studies, and the relevance and adequacy of the data. Common methodological limitations included a lack of researcher reflexivity as well as poor reporting of ethical considerations, sampling, and data analysis methods. We often assessed the data as being only partially relevant, mainly because the included studies represented few regions, with a focus on hospital settings, and few populations, with a focus on midlevel health workers. Finally, our concerns about adequacy were mainly tied to the limited number of studies and the thinness of the data contributing to many of the findings.
Agreements and disagreements with other studies or reviews
Table 55 summarises the scope of other related reviews when compared to this synthesis. Our findings are complementary to the findings in the Filby 2016 review. We agree that barriers to providing good quality midwifery care arise from the quality of education of health providers, for example in the regulation of pre‐service education, and that this limits professional development. However, our synthesis considers health services infrastructural barriers (e.g. limited staff numbers, lack of transport, weak facility management, and poor working conditions) separately from education or training (all categorised professional barriers in Filby 2016). We likewise found that salaries were low or insufficient for skilled birth attendants' personal needs, work done, and personal risk. Our finding for instance that health workers fear for their personal safety when they work alone, and that long, lonely hours of work affect their spousal relations, provide additional evidence of social barriers reported in the Filby review 2016.
| Author | Title of review | Comparison of the scope of the review and this synthesis |
| What prevents quality midwifery care? A systematic mapping of barriers in low and middle income countries from the provider perspective | Review searched a wide range of literature mainly from grey literature, and only included studies where skilled birth attendants had midwifery skills. In contrast, our synthesis searched web‐based databases and was not limited to providers with midwifery skills, but included a broad range of health providers that delivered obstetric care. | |
| Factors that influence the uptake of routine antenatal care services by pregnant women: a qualitative evidence synthesis | Review covers women’s views and experiences, and factors that influence uptake of antenatal care. Includes global literature. Our synthesis focuses on health workers' views, behaviours, and experiences when delivering intrapartum and postnatal care, and includes only studies conducted in low‐ and middle‐income countries. | |
| Disrespectful intrapartum care during facility‐based delivery in sub‐Saharan Africa: a qualitative systematic review and thematic synthesis of women's perceptions and experiences | Review focused on facility‐based deliveries in sub‐Saharan Africa and documented women's perceptions and experiences of intrapartum care. Our synthesis focuses on health workers' views, behaviours, and experiences when delivering intrapartum and postnatal care, in low‐ and middle‐income country settings. | |
| Bohren 2016 | The mistreatment of women during childbirth in health facilities globally: a mixed‐methods systematic review | Global review that focused on mistreatment of women during childbirth and included the perceptions and experiences of women during childbirth as well as health workers. Our synthesis focuses on health workers' views, behaviours, and experiences when delivering intrapartum and postnatal care, in low‐ and middle‐income country settings. |
While our synthesis focused on intrapartum and postnatal care, Downe 2016 covered antenatal care and is therefore complementary to our synthesis. The Downe 2016 review indicated that positive interpersonal behaviour of health providers as well as their clinical, cultural, and social skills and competence are important for pregnant women. Pregnant women also required private spaces that facilitated their interaction with health providers. Our synthesis identifies some of the factors that may undermine health providers ability to provide this care, such as lack of skills in communication, heavy workload, and limited and poorly organised space. In addition, Downe 2016 found that shortage of staff, low salaries and heavy workload, lack of medicines and equipment, and poor conditions in clinics including lack of water and electricity prevented providers from providing good‐quality antenatal care.
The Bradley 2016 review suggests that midwives attempted to assert power and control over women in their care, for example when they controlled how women behaved during labour, and that midwives' behaviour was part of a strategy to maintain their professional, technical, and social status. Our finding that health workers did not let mothers participate in decision‐making because of health worker attitudes about women's preferences and role during delivery of her baby, and health workers' authoritarian behaviour, supports this hypothesis. However, Bradley 2016 briefly identifies work environments and resources as part of the health system structural drivers underpinning disrespect of mothers. Our synthesis provides additional evidence that points to structural challenges health workers experience when providing care. We hypothesise that these structural challenges in part influence health worker behaviour.
The typology in Bohren 2015 identified health systems conditions and constraints such as physical condition of facilities, shortage of staff and supplies, and lack of privacy as a form of mistreatment of women. Our synthesis supports the Bohren 2015 finding on health systems constraints and likewise identified several barriers in health services infrastructure and human resources that interfered with health workers ability to provide good‐quality maternity care.
In addition, Bohren 2015 identified poor rapport between women and providers as another form of mistreatment of women. Included in this category was ineffective communication such as poor communication, dismissal of women's concerns, poor staff attitudes, and language barriers. Our finding that health workers did not value communication, or communicated poorly or had problems with communication (Table 50), supports this finding.
Also included in the poor rapport between women and providers category of the Bohren 2015 review were lack of supportive care, for instance denial of birth companions, and lack of autonomy when women preferred an alternative birth position. Our synthesis provided some explanations for these findings. For instance, health workers may not allow companions in delivery rooms when physical space is limited, and in order to provide privacy to other mothers in labour (see Results section on health services and infrastructure). In addition, lack of training in alternative positions of delivery may limit health workers' ability to provide care in positions other than the supine delivery position. However, we also found that health workers had poor attitudes about the labouring mother's role in her care and did not empower mothers to be active participants in their care. Such negative attitudes may interact with structural problems and further limit women‐centred care in these settings.
Reflexivity
As recommended as part of primary qualitative research, we reflected on how our backgrounds and positions might have influenced our choice of review topic, study selection, data extraction, analysis, and interpretation of data. SMB, CG, SL, and AF are employed by the Norwegian Public Health Institute, and HN is employed by Uganda National Health Research Organisation. SMB, SL, AF, and HN are trained physicians, while CG is a social scientist. SMB, SL, AF, and HN have all previously worked as clinicians in low‐ and middle‐income settings. In these roles, we have to varying degrees experienced working conditions characterised by poor resources and have seen how this influenced our own motivation and our ability to provide patient‐centred care. We are therefore sympathetic to the challenges experienced by health workers in these kinds of settings. We are also of the opinion that discussions about the quality of intrapartum and postnatal care are sometimes characterised by strong criticisms of the behaviour of health workers and of the care they provide, and a failure to adequately reflect on and consider the conditions under which these health workers provide care and the system‐level reasons for these conditions.


Study flow diagram.
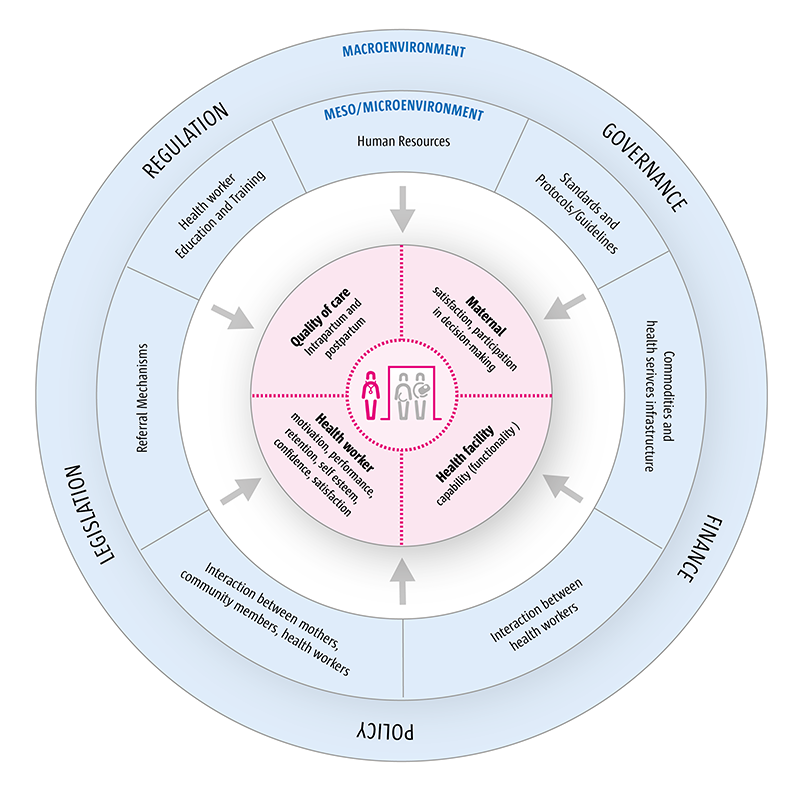
Factors that influence the delivery of intrapartum and postpartum care by skilled birth attendants.
| Summary of review finding | Studies contributing to the review finding | CERQual assessment of confidence in the evidence | Explanation of CERQual assessment |
| SOCIOCULTURAL | |||
| Sociocultural barriers sometimes hindered mothers from receiving care in hospitals. For instance, women preferred not to be examined by male health providers, or for cultural reasons preferred a particular position in which to deliver, or for religious reasons did not divulge information that was needed for their care. | Low confidence | Due to moderate concerns about adequacy; and moderate concerns about relevance | |
| PROFESSIONAL ASSOCIATIONS | |||
| Health workers had conflicting views on the role of professional councils. For instance, some viewed professional councils as advocates for their members, while others viewed them as a regulatory body with punitive functions. | Very low confidence | Due to moderate concerns about methodological quality; and moderate concerns about relevance; and severe concerns about adequacy | |
| HUMAN RESOURCES | |||
| Staff shortage was a widely reported problem and led to increased workloads, which in turn compromised quality of care. For instance, heavy workload limited health worker time for history taking and thorough assessment of women, and hand hygiene was sometimes compromised. Staff shortages and work overload jeopardised health workers’ ability to provide timely care, and manage routine care as well as emergency cases. In addition, shortage of staff sometimes led health workers to exceed their scope of practice, and influenced a health facility's ability to provide 24‐hour care. | Afsana 2001; Anwar 2009; Barua 2011; Bradley 2009; Conde‐Agudelo 2008; Fränngård 2006; Fujita 2012; Graner 2010; Hassan‐Bitar 2011; Ith 2012; Khalaf 2009; Lugina 2001; Maputle 2010; Mathole 2006; Mondiwa 2007; Spangler 2012; Thorsen 2012; VSO 2012 | Moderate confidence | Due to minor concerns about coherence; and minor concerns about methodological limitations |
| A lack of specialists or experienced staff, including absence of health workers with key skills such as anaesthetists, influenced the provision of care and supervision of junior staff. When no specialists were available, some tasks such as emergency obstetric care were not delivered at all, or tasks were transferred to health workers who were not properly qualified or trained to deliver them. When senior experienced health workers were not available, junior health workers lacked supervision. | Afsana 2001; Anwar 2009; Blum 2006; Bradley 2009; De Brouwere 2009; Fränngård 2006; Hassan‐Bitar 2011; Khalaf 2009; Penfold 2013; Pitchforth 2010; Spangler 2012; VSO 2012 | Moderate confidence | Due to moderate concerns about methodological limitations |
| Health workers had vague job descriptions that sometimes led them to perform tasks that were beyond their expertise or scope of practice. | Very low confidence | Due to minor concerns about methodological limitations; and serious concerns about relevance and adequacy | |
| Staff shortages and work overload could jeopardise health workers’ ability to display support, empathy, and friendliness to women in labour. | Very low confidence | Due to minor concerns about methodological limitations; and moderate concerns about relevance and adequacy | |
| Staff shortages and increased workload, as well as living and work conditions, sometimes caused stress and frustration, affected health workers' family life, and led to concerns about personal safety. | Anwar 2009; Blum 2006; Fränngård 2006; Graner 2010; Lester 2003; VSO 2012 | Moderate confidence | Due to moderate concerns about methodological limitations; and minor concerns about relevance and adequacy |
| A wide range of interlinked reasons for staff shortages were suggested. These included limited funds to recruit health workers; bureaucratic processes of the recruitment process, e.g. absence of committees responsible for recruitment at the district level; scarcity of health workers especially in rural areas; and other factors that deterred retention of health workers (see finding on factors affecting recruitment, Table 1). In addition, institutional arrangements, e.g. when health facilities hired contract staff in order to reduce labour costs, and inefficient deployment of available staff sometimes created staff shortages. Facilities with staff shortages and work overload were viewed as unattractive places to work, and made it difficult for managers to transfer staff from well‐served to underserved areas, thus compounding/increasing the problem. | Anwar 2009; Graner 2010; Molina 2011; Pitchforth 2010; VSO 2012 | Moderate confidence | Due to moderate concerns about adequacy; and minor concerns about relevance and methodological limitations |
| Health workers' salaries and benefits were considered insufficient for the work done, the responsibility and personal risk, and the additional responsibilities assigned, e.g. through informal task‐shifting. In addition, salaries were insufficient for their personal needs, e.g. to send their children to school and for transport costs to visit their husbands. | Anwar 2009; Belizan 2007; De Brouwere 2009; Fränngård 2006; Graner 2010; Hassan‐Bitar 2011; Ith 2012; Molina 2011 | Moderate confidence | Due to moderate concerns about methodological limitations; and minor concerns about relevance and adequacy |
| Factors reported by health workers or their managers to influence recruitment, retention, motivation, or performance of health workers were: good‐quality accommodation for health workers provided by government, allowances for extra project‐related work, paid vacations for 1 month of the year, improved access to and funding for continued education/in‐service training, career progression, non‐biased evaluations or performance‐related rewards or promotions, e.g. for those doing better, working longer, or taking on added responsibilities, and verbal recognition by supervisors and management. The following factors were reported as discouraging health workers from working in rural or remote health facilities: facilities that lacked good equipment and did not provide sufficient work needed to maintain clinical skills, lack of family amenities, limited opportunities for private practice, lack of electricity, TV, or internet, coupled with poor roads and lack of transport deterred health workers from undertaking rural employment. In addition, interference in treatment decisions by local politicians and mismanagement of posting and transfer from the national level were demotivating to health workers working in rural facilities. | Anwar 2009; Bradley 2009; De Brouwere 2009; Fränngård 2006; Hassan‐Bitar 2011; Ith 2012; VSO 2012 | Moderate confidence | Due to minor concerns for methodological limitations and relevance |
| Health workers perceived managers as lacking in management capacity and skills and sometimes felt unsupported. Health workers also complained that concerns about the workplace were sometimes left unheard, and no solutions or feedback given. | Anwar 2009; Bradley 2009; Ith 2012; Lester 2003; Mondiwa 2007; VSO 2012 | Moderate confidence | Due to moderate concerns about relevance; and minor concerns about methodological limitations and adequacy |
| Helping women access financial assistance for out‐of‐pocket payments was sometimes time‐consuming for health workers. | Very low confidence | Due to serious concerns about relevance and adequacy | |
| HEALTH WORKER EDUCATION AND TRAINING | |||
| Inadequate pre‐service and in‐service training sometimes limited health workers' skills and ability to provide care. For instance, some health workers lacked training to attend home births or manage complicated pregnancies or deliveries, e.g. eclampsia or HIV in pregnancy. In contrast, training allowed midwives to practice assisting women to deliver in non‐supine positions and enabled them to get accustomed to this practice. | Afsana 2001; Barua 2011; Blum 2006; DeMaria 2012; Fujita 2012; Graner 2010; Lester 2003; Mathole 2006 | High confidence | ‐ |
| Health worker competencies and opportunities for on‐the job training were sometimes limited by poor scheduling of in‐service education sessions, high cost of continuing education for health workers, inequitable selection for professional development opportunities, lack of ongoing training and follow‐up, and shortage of instructors for upgrading courses. In addition, the variation in quality of pre‐service training resulted in varying levels of need for in‐service training, and these needs were not always met, resulting in wide variation in proficiency among health workers. | Moderate confidence | Due to minor concerns about methodological limitations and relevance; and moderate concerns about adequacy | |
| Learning through practical application facilitated acquisition of skills and confidence. The experience gained through, for example, internship, social service year, and working in the community, was identified as important for building doctors' and midwives' practical experience and confidence in providing care. | Very low confidence | Due to moderate concerns about methodological limitations and relevance; and severe concerns about adequacy | |
| Health workers reported several barriers to implementing recommended practice. Firstly, health workers were sometimes unaware of current recommended effective practices. Secondly, health workers' flexibility, attitudes, and beliefs about medical knowledge and skills sometimes influenced their receptivity to new practice knowledge. For example, health worker attitudes did not view medical education as dynamic; held beliefs that no significant progress had been made and clinical practice was similar to techniques learnt many years ago; or were not flexible or willing to implement alternative positions of delivery, even though these were preferred by women. | Low confidence | Due to moderate concerns about relevance and adequacy | |
| Lack of time, infrastructure, and skills limited health workers' ability to seek knowledge and practice new clinical skills. For instance, chronic staff shortages meant less time available for health workers to seek information. This was sometimes further compounded by lack of information sources such as internet access, and poorly resourced hospital libraries. In addition, lack of training and skills in networking, epidemiology, research appraisal, or critical thinking about clinical practice limited health workers' awareness and receptivity to clinical practice changes, and this lack of skills led some professionals to prefer old, familiar procedures. | Low confidence | Due to moderate concerns about relevance and adequacy; and minor concerns about methodological limitations | |
| STANDARDS AND PROTOCOLS | |||
| Lack of guidelines/protocols, or where they were inconsistent or health workers were not aware or were uncertain of them, could impact patient care and outcomes and cause harm. | Barua 2011; de Carvalho 2012; Khalaf 2009; Lugina 2001; Mathole 2006 | Low confidence | Due to moderate concerns about adequacy; and minor concerns about methodological limitations |
| Health workers did not always adhere to protocols/guidelines, even when they were aware of them. Guidelines/protocols were not followed for a number of reasons. Some health workers felt that guidelines were insufficient without consensus from staff. Some studies described how health workers continued to practice ineffective procedures because they were considered routine; due to lack of time; because they lacked the autonomy to avoid using what they knew to be inappropriate care; because the resources at the institution were not aligned with the protocols for postpartum care; or when it was unclear who was professionally responsible, e.g. in using the partograph. | Belizan 2007; de Carvalho 2012; Conde‐Agudelo 2008; Molina 2011; Pettersson 2006 | Low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy |
| Health workers sometimes used unnecessary diagnostic tests and did not follow recommended practice when they feared malpractice suits. This fear could lead to practitioners retaining practices they believed were ‘safer’. | Very low confidence | Due to moderate concerns about relevance; serious concerns about adequacy; and minor concerns about methodological limitations | |
| Some health workers did not use recommended interventions when delivering care because of concerns about negative outcomes for the baby or the mother. Examples included the use of magnesium sulphate administered with anaesthesia during Caesarean sections or when monitoring of serum magnesium sulphate levels was not possible. | Very low confidence | Due to moderate concerns about relevance; serious concerns about adequacy; and minor concerns about methodological limitations | |
| Health workers were sometimes reluctant to admit their lack of skills in delivering care for fear of blame and criticisms from managers. This fear of criticism could undermine health worker confidence and performance. | Low confidence | Due to minor concerns about relevance; and moderate concerns about adequacy | |
| COMMODITIES AND HEALTH SERVICES INFRASTRUCTURE | |||
| Insufficient stock and/or lack of drugs such as hydralazine, magnesium sulphate, oxytocin, misoprostol, antiretrovirals, and supplies such as gloves, sometimes influenced the quality of care provided to mothers and their babies. For instance, health workers had to use less effective alternative drugs, e.g. diazepam instead of magnesium sulphate. Lack of supplies sometimes limited good hygiene and practice of aseptic techniques, resulting in unsafe practices, e.g. reuse of disposable gloves could increase the risk of HIV infection. Lack of supplies sometimes led to poor outcomes and increased the length of stay in health facilities. Lack of supplies could determine if a new clinical practice was implemented and maintained over time. | Anwar 2009; Belizan 2007; Bradley 2009; de Carvalho 2012; Foster 2006; Fränngård 2006; Graner 2010; Ith 2012; Lester 2003; Mathole 2006; Penfold 2013; Pitchforth 2010; Spangler 2012; VSO 2012 | Moderate confidence | Due to moderate concerns about methodological limitations |
| Lack of drugs or supplies meant mothers or their carers had to purchase their own. This sometimes led to wasted time in procuring the drugs and supplies and the creation of informal markets and corruption at health facilities. | Barua 2011; Foster 2006; Fränngård 2006; Lester 2003; Pitchforth 2010; Spangler 2012; VSO 2012 | Low confidence | Due to moderate concerns about methodological limitations and adequacy; and minor concerns about coherence |
| Lack of equipment limits health workers' ability to deliver quality care to mothers and their babies. As a result of this lack of equipment, mothers and their babies sometimes received poor quality care. | Barua 2011; Fränngård 2006; Graner 2010; Lester 2003; Molina 2011; Penfold 2013; Pettersson 2006; Pitchforth 2010 | High confidence | ‐ |
| Lack of blood or limited infrastructure to manage blood transfusion limited health workers from delivering appropriate care. | Moderate confidence | Due to moderate concerns about adequacy; and minor concerns about relevance | |
| Lack of equipment, supplies, or drugs sometimes wasted health workers' time, increased their workload and risk of infection, and led to low morale. | Belizan 2007; Bradley 2009; Foster 2006; Graner 2010; Lester 2003; Mathole 2006; Penfold 2013; Pitchforth 2010; VSO 2012 | Moderate confidence | Due to moderate concerns about methodological limitations; and minor concerns about coherence |
| Poor, incomplete, and non‐systematised patient information could lead to delayed or incorrect management of high‐risk mothers, or interfered with continuity of care. | Low confidence | Due to serious concerns about adequacy | |
| Lack of or unreliable supply of electricity, including a lack of fuel to run generators, and lack of water influenced health providers' ability to deliver quality care. | Moderate confidence | Due to moderate concerns about methodological limitations | |
| The lack of space and amenities as well as poor physical layout and organisation of wards limited the delivery of quality care. | Belizan 2007; Conde‐Agudelo 2008; DeMaria 2012; Fränngård 2006; Khalaf 2009; Lester 2003; Molina 2011; Pettersson 2006; Pitchforth 2010 | Moderate confidence | Due to minor concerns about adequacy, relevance, and methodological limitations |
| The lack of funds and material resources sometimes prevented health facility managers from adequately maintaining equipment and physical infrastructure. | Low confidence | Due to minor concerns about coherence; and moderate concerns about methodological limitations and adequacy | |
| Health facilities varied in the availability, functionality, and quality of interventions assigned as signal functions for obstetric care. At the lower‐level facilities, most of these functions were not available, e.g. parenteral antibiotics or anticonvulsants or neonatal resuscitation. At the higher levels, some of these functions appeared to be available, but functionality varied, for instance when there were drug stock‐outs or unqualified providers of care. | Very low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy | |
| Health workers felt it was easier to deliver care in facilities than at home. Some of the positive aspects about delivering care at the health facility were that they were able to do other work while monitoring labour; provide care for several mothers; work schedules were more regular; and care was available 24 hours a day. Furthermore, at facilities other skilled providers were available to assist when needed, and some procedures (e.g. episiotomies) were easier to perform. In addition, health facilities provided a secure, controlled, hygienic work environment, where electricity, equipment, and medications were always available. | Very low confidence | Due to moderate concerns about relevance; and serious concerns about adequacy | |
| REFERRAL MECHANISMS | |||
| Where primary care workers in lower‐level facilities lacked the knowledge and the skills to determine the need for referral, or were unable to provide emergency care, mothers could receive inadequate care. This lack of skills could also result in unnecessary referrals to other health facilities. | Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about relevance; and serious concerns about adequacy | |
| Lack of trust and professional rivalries between midwives, doctors, and obstetrician gynaecologists may delay referral of mothers and their babies. Midwives sometimes felt blamed by physicians when complications arose and hesitated to seek support from the medical teams at the receiving facilities. Some midwives did not travel with the mothers to the referring facility for fear of blame for any negative occurrence during the referral process. | Low confidence | Due to moderate concerns about adequacy and relevance | |
| Respondents felt that maternal perceptions of the health system could make mothers reluctant to accept referral. For instance, mothers were sceptical about the cost of care, poor management and care at the next‐level facility, the procedures used, the high levels of Caesarean sections, and fear of complications. Also mothers may have already travelled far to reach the facility they perceive as a good one, or feared unfamiliar, urbanised settings. As a result of mothers' reluctance to accept referral, midwives may feel pressured to conduct high‐risk deliveries or spend a lot of time convincing reluctant mothers or their families. | Barua 2011; Blum 2006; Graner 2010; Lester 2003; Tabatabaie 2012 | Moderate confidence | Due to minor concerns about methodological limitations, coherence, relevance, and adequacy |
| The presence of trust between mothers and midwives may influence a mother's willingness to be referred. Referral may be delayed when facilities lack midwives or other primary care workers whom the mothers trust and who can convince mothers of the need for referral. | Very low confidence | Due to minor concerns about coherence and methodological limitations; moderate concerns about relevance; and serious concerns about adequacy | |
| Lack of transport hinders referral of women and their babies to higher levels of care. For instance, this occurred when health facilities lacked ambulances, or when facility budgets were insufficient to purchase fuel for vehicles. | Moderate confidence | Due to minor concerns about relevance and adequacy | |
| Lack of fuel for vehicles when the need for referral arises is frustrating to nurses and midwives and leaves them feeling helpless when mothers' and babies' lives are at risk. | Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about relevance; and serious concerns about adequacy | |
| When health facilities lack fuel for vehicles, mothers and their families are sometimes asked to pay their own transport costs. Many families could not afford this. | Low confidence | Due to moderate concerns about relevance and adequacy | |
| Several situations could lead health workers to refer mothers and shift responsibility to higher levels of care, including when they lacked the skills or confidence to provide care, or were working in isolation; when they were concerned about the facility's reputation when poor patient outcomes arose; or when they lacked supplies, drugs, or equipment to provide care. Some of these referrals were unnecessary and resulted in increased workloads at higher levels of care. | Low confidence | Due to moderate concerns about adequacy and relevance | |
| When secondary‐level care was non‐existent, mothers were sometimes referred to tertiary‐level care, which resulted in congestion at the tertiary level. | Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about relevance; and serious concerns about adequacy | |
| Administrative processes and paperwork and poor communication between referring and receiving levels of care could influence the efficient transfer of mothers and their babies to receiving units. | Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about coherence and relevance; and serious concerns about adequacy | |
| Lack of feedback between the referring and receiving facilities could influence midwives' practice and patient outcomes. Midwives perceived this feedback as useful for improving their practice and patient outcomes. | Very low confidence | Due to moderate concerns about relevance; and serious concerns about adequacy | |
| INTERPERSONAL RELATIONS | |||
| Poor attitude and unethical behaviour among health workers could influence the quality of care. For instance, when health workers are harsh, rude, or impatient with mothers; or display poor cultural sensitivity, e.g. by not maintaining women's privacy; or when health workers are absent from their duty stations or involved in the illegal sale of drugs and supplies or expect 'back door' payments for services. Some of the suggested underlying reasons for these attitudes and behaviours were wrong intrinsic reasons for joining the profession and physical exhaustion from long, solitary hours of work. | Low confidence | Due to moderate concerns about methodological limitations and adequacy; and minor concerns about relevance | |
| Mothers' participation in decision‐making during labour could be limited by health worker attitudes and authoritarian behaviour, for instance when health workers conducted procedures without asking mothers for their opinion, or when physicians did not seek feedback from mothers about practices or outcomes and expected women to co‐operate. Lack of patient participation in decision‐making can threaten quality of care. Some of the reasons for this behaviour were related to health workers’ attitudes about the woman’s preferences and role during delivery of her baby. | Belizan 2007; de Carvalho 2012; Conde‐Agudelo 2008; DeMaria 2012; Maputle 2010 | Low confidence | Due to minor concerns about coherence and adequacy; and moderate concerns about methodological limitations and relevance |
| Some health workers did not value communication, communicated poorly, or said they had problems with communication. Poor communication and interaction could threaten the trust between health workers and mothers, for instance when health workers considered communication with mothers as a waste of time, and there was insufficient communication between staff and families, or when skilled birth attendants were abrasive and demeaning in their interactions with women and showed no concern for women's families. Language barriers could interfere with effective communication between mothers and health workers. As a result, mothers sometimes appeared not to listen to health workers while health workers mechanically worked through the process of providing care. Health workers acknowledged the need to respect and involve men, women's families, and the community in maternal health, e.g. in understanding cultural beliefs related to postpartum care. | Blum 2006; de Carvalho 2012; Hassan‐Bitar 2011; Lugina 2001; Maputle 2010 | Very low confidence | Due to moderate concerns about relevance and adequacy; and serious concerns about methodological limitations |
| Mismatch between people's expectations of health workers and what health workers were actually able to deliver or thought was appropriate could lead to antagonism. For instance, health workers that delivered home‐based care could experience social pressure from families and communities, e.g. to give injections to speed up delivery as opposed to waiting for labour to progress normally. Health workers providing maternity care at health facilities were sometimes treated harshly by people from the community when there was a lack of supplies and materials. In addition, misconceptions that midwives were not working when they took a break from their work, or that health workers sold drugs, threatened the trust between health workers and the community. | Low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy | |
| Health workers valued the appreciation, respect, trust, and praise from mothers, or when they made friends among mothers or worked with the community. Midwives in particular were delighted when a baby was given their name and seeing the baby grow. | Low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy | |
| Midwife‐led shared care was perceived to improve the interaction between mothers, families, and health workers, and could improve health workers' self esteem and lead to a change in hospital culture with respect to service provision. For instance, midwife‐led shared care increased communication between midwives, women, and their families; enabled the presence and participation of family members; and together increased satisfaction in the care provided. As a result, the need for medication during delivery was minimised, which reduced the financial burden experienced by families. The supportive environment for mothers, the good interaction between mothers and health workers, as well as recognition of professional expertise among midwives increased self esteem. Midwife‐led shared care enabled other hospital staff to reflect on their own routine activities and manner of communication with families and clients, leading to a change in hospital culture with respect to service provision. | Very low confidence | Due to moderate concerns about relevance; and severe concerns about adequacy | |
| Disrespectful communication, lack of trust, inadequate opportunities to review clinical practice, and poor teamwork and co‐ordination sometimes led to poor interprofessional relations. Also, tensions arose when health providers did not recognise each others' capabilities, and when they acted in a way that reinforced clinical hierarchy, e.g. disrespectful interprofessional communication between physicians and midwives. Midwives with lower‐level training could manage normal birth, but they felt marginalised and less motivated to provide care because midwives with higher levels of training and doctors used qualification, status, and their roles to dominate clinical practice. Tensions were reported between doctors and clinical officers due to salary differentials, benefits, workload, and status. There was sometimes a lack of understanding of competencies and alternative models of care. | Belizan 2007; Bradley 2009; DeMaria 2012; Hassan‐Bitar 2011; Ith 2012; Pettersson 2006 | Low confidence | Due to moderate concerns about relevance and adequacy |
| Nurses and midwives valued and were motivated by a good team dynamic where health workers provided feedback, supported, and co‐operated to ensure all shifts were covered. For instance, midwives valued good interprofessional collaboration that made them feel accepted as part of the professional team and provided an opportunity to improve their competence through on‐spot education provided by obstetricians. When midwives worked together in a team led by midwives, this increased their ability to share experiences and new practices and their decision‐making responsibility; improved their self esteem; and provided quality assurance and improved the quality of care provided. This teamwork was especially useful when emergencies arose. In another study, researchers observed that nurses had a strong teamwork ethic and functioned well together to complete work. | Bradley 2009; Foster 2006; Fränngård 2006; Lester 2003; Pettersson 2006 | Low confidence | Due to moderate concerns about relevance and adequacy |
| Factors reported by health workers or their managers as influencing recruitment, retention, motivation, or performance of health workers were: good‐quality accommodation for health workers provided by government, allowances for extra project‐related work, paid vacations for one month of the year, improved access to and funding for continued education/in‐service training, career progression, non‐biased evaluations or performance‐related rewards or promotions, e.g. for those doing better, working longer, or taking on added responsibilities, and verbal recognition by supervisors and management. The following factors were reported as discouraging health workers from working in rural or remote health facilities: facilities that lack good equipment and do not provide sufficient work needed to maintain clinical skills, lack of family amenities, limited opportunities for private practice, lack of electricity, TV, or internet, coupled with poor roads and lack of transport. In addition, interference in treatment decisions by local politicians, and mismanagement of posting and transfer from the national level, were demotivating to health workers working in rural facilities. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 6 studies; ethical considerations were not reported in 4 studies; and sampling methods were not reported in 3 studies. However, these may not have influenced the finding. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns, as 1 study reports managers’ perceptions of factors health workers describe as influencing recruitment and retention. |
| Adequacy | No to very minor concerns, though some studies reported thin data for specific parts of the finding. |
| Overall CERQual assessment | |
| Moderate confidence | Due to minor concerns for methodological limitations and relevance |
| Contributing studies/setting | |
| Africa (4), E. Asia (1), Middle East &N Africa (1), S. Asia (1) Bradley 2009: Malawi, rural mission hospitals Anwar 2009: Bangladesh, basic and comprehensive emergency obsteric care facilities, public VSO 2012: Uganda, hospitals and health centres Fränngård 2006: Uganda, district hospital and health centre IVs Ith 2012: Cambodia, provincial and regional hospitals, health centres De Brouwere 2009: Senegal, district hospitals | |
| Author year | Is study qualitative research? | Research questions clear? | Ethical issues? | Is qualitative approach justified? | Is approach appropriate for research question? | Is study context clearly described? | Role of researcher described? | Sampling method clearly described? | Sampling strategy appropriate? | Method of data collection clear? | Method of data collection appropriate to question? | Method of data analysis clear? | Method of data analysis suitable? | Are claims supported by evidence? | Overall assessment |
| Yes | Yes | Yes | No | Yes | Yes | No | No | Not clear | Yes | Yes | Yes | Yes | Yes | Medium | |
| Yes | Yes | No | Yes | Yes | Yes | No | Yes | Yes | Yes | Not clear | Yes | Yes | Yes | Good | |
| Yes | Yes | Yes | Yes | Yes | Yes | Not clear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Not clear | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Yes | Yes | Yes | Yes | Yes | Yes | Not clear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Yes | Yes | Yes | Yes | Yes | Yes | Not clear | Not clear | Not sure | Yes | Yes | Yes | Yes | Yes | Good | |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Mixed methods | Yes | No | Yes | Yes | Yes | No | No | No | Yes | Yes | No | Not clear | Yes | Low | |
| Yes | Yes | Yes | No | Not clear | Not clear | No | No | No | Yes | Yes | Not clear | Not clear | Yes | Low | |
| Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Medium | |
| Yes | No | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | Low | |
| Yes | Yes | Yes | Yes | Yes | Yes | No | No | Not clear | Yes | Yes | Yes | Yes | Yes | Medium | |
| Yes | Not clear | No | No | Not clear | Yes | Not clear | Yes | Yes | Yes | Not sure | Yes | Yes | Yes | Low | |
| Mixed methods | Yes | No | No | Not clear | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Medium | |
| Mixed methods | Yes | Yes | Yes | Yes | Yes | No | Not clear | Not clear | Yes | Yes | Yes | Yes | Yes | Medium | |
| Mixed methods | Clear objectives | Yes | Yes | Yes | Yes | Not clear | No | Not clear | Yes | Yes | Yes | Yes | Yes | Medium | |
| Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Yes | No | No | No | Not clear | Not sufficient | Not clear | No | Not clear | Yes | Unclear | No | Not clear | Yes | Low | |
| Yes | Objectives clear | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Medium | |
| Mixed methods | Objectives clear | Yes | Yes | Yes | Yes | Not clear | Not clear | Not clear | Yes | Yes | Yes | Yes | Yes | Medium | |
| Mixed methods | Objectives clear | Yes | No | Yes | Yes | No | Not clear | Not clear | Yes | Yes | Yes | Yes | Yes | Medium | |
| Yes | Yes | Yes | No | Not clear | Not sufficient | Not clear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | medium | |
| Yes | Objective is clear but questions are not stated. | No | No | Not clear | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low | |
| Mixed methods | Aim is clear. | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Yes | Clear objectives | Yes | No | Not clear | Yes | Not clear | Unclear | Not clear | Yes | Yes | Yes | Yes | No | Low | |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Good | |
| Yes | Yes | Yes | Yes | Yes | Not sufficient | No | Yes | Yes | Yes | Yes | Yes | Not clear | Yes | Low | |
| Yes | Objective clear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good | |
| Mixed methods | Objective clear | No | No | Not clear | Yes | No | Unclear | Not clear | Yes | Yes | Yes | Yes | No | Low | |
| Yes | Objective clear | No | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Medium | |
| Yes | objective clear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Good |
| Staff shortage was a widely reported problem, and led to increased workloads, which in turn sometimes compromised quality of care. For instance, heavy workload limited health worker time for history taking and thorough assessment of women, and hand hygiene was sometimes compromised. Staff shortages and work overload jeopardised health workers’ ability to provide timely care and manage routine care as well as emergency cases. In addition, shortage of staff sometimes led health workers to exceed their scope of practice and influenced a health facility's ability to provide 24‐hour care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 13 studies; ethical consideration was not reported in 6 studies; and a small number of studies did not report sampling strategy or data analysis methods. However, these may not influence the finding. |
| Coherence | Minor concerns because 1 study reported that doctors were able to rest despite the workload, another study indicated nurses did not exceed scope of practice. These data imply that the finding may relate only to a few cadre. |
| Relevance | No to very minor concerns, as data were drawn from a wide range of settings and covered different levels of care. |
| Adequacy | No to very minor concerns because many studies reported data on this finding, though some studies provided thin data. |
| Overall CERQual assessment | |
| Moderate confidence | Due to minor concerns about coherence; and minor concerns about methodological limitations |
| Contributing studies/setting | |
| Middle E&N Africa (2), Africa (9), E. Asia (2), S. Asia (3), Latin America & Caribbean (1) Hassan‐Bitar 2011: Palestine, public referral hospital Bradley 2009 Malawi, rural mission hospitals Khalaf 2009: Jordan, maternal and child health centres Graner 2010: Vietnam, primary health care Lugina 2001: Tanzania, municipal hospitals Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries Fränngård 2006: Uganda, district hospital and health centre IVs Fujita 2012: Benin, tertiary hospital Anwar 2009: Bangladesh, basic and comprehensive emergency obsteric care facilities, public Maputle 2010: South Africa, tertiary care hospital VSO 2012: Uganda, hospitals and health centres Conde‐Agudelo 2008: Colombia, public and private hospitals Thorsen 2012: Malawi, a secondary and tertiary hospital Mathole 2006: Zimbabwe, health centres in the district Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals Afsana 2001: Bangladesh, health centre Ith 2012: Cambodia, public maternity settings in provincial hospital, two regional hospitals and two health centres | |
| A lack of specialists or experienced staff, including absence of health workers with key skills such as anaesthetics, could influence the provision of care and supervision of junior staff. When no specialists were available, some tasks for instance emergency obstetric care were not delivered at all, or tasks were transferred to health workers who were not properly qualified or trained to deliver them. When senior experienced health workers were not available, junior health workers sometimes lacked supervision. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 9 studies; ethical considerations were not reported in 5 studies; and several studies did not report sampling strategy or data analysis methods. |
| Coherence | No to very minor concerns |
| Relevance | No to very minor concerns |
| Adequacy | No to very minor concerns |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about methodological limitations |
| Contributing studies/setting | |
| Africa (7), Middle E&N Africa (2), S. Asia (3) Hassan‐Bitar 2011: Palestine, public referral hospital Bradley 2009: Malawi, rural mission hospitals Khalaf 2009: Jordan, maternal and child health centres Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries Fränngård 2006: Uganda, district hospital and health centre IVs Anwar 2009: Bangladesh, basic and comprehensive emergency obsteric care facilities, public VSO 2012: Uganda, hospitals and health centres Afsana 2001: Bangladesh, health centre Blum 2006: Bangladesh, home‐based maternity care Penfold 2013: Tanzania, hospitals, health centres, dispensaries De Brouwere 2009: Senegal, district hospitals Pitchforth 2010: Ethiopia, teaching hospital | |
| Health workers had vague job descriptions that sometimes led them to perform tasks that were beyond their expertise or scope of practice. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns. Although reflexivity and ethical considerations were not reported, these may not have influenced the finding. |
| Coherence | No to very minor concerns |
| Relevance | Serious concerns. Data were from only 1 region. |
| Adequacy | Serious concerns. Data were from 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about methodological limitations; and serious concerns about relevance and adequacy |
| Contributing studies/setting | |
| (Africa 1) | |
| Staff shortages and work overload could jeopardise health workers’ ability to display support, empathy, and friendliness to women in labour. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 2 studies; ethical considerations were not reported in 1 study; and sampling strategy was not clear in 2 studies. However these may not influence the finding. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because data were from a limited number of regions and level‐of‐care settings. |
| Adequacy | Moderate concerns because data were from 3 studies with very thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about methodological limitations; and moderate concerns about relevance and adequacy |
| Contributing studies/setting | |
| Africa (2), Latin America & Caribbean (1) Maputle 2010: South Africa, tertiary care hospital Conde‐Agudelo 2008: Colombia, public and private hospitals, 44% were university teaching hospitals VSO 2012: Uganda, hospitals and health centres | |
| Staff shortages and increased workload as well as living and work conditions sometimes caused stress and frustration, affected family life, and led to concerns about personal safety among health workers. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 4 studies; ethical considerations were not reported in 3 studies; and some studies did not report sampling or data analysis methods. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns because data referred mainly to midlevel providers of care. |
| Adequacy | Minor concerns because data were from several studies, though some studies had thin data. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about methodological limitations; and minor concerns about relevance and adequacy |
| Contributing studies/setting | |
| Africa (3), S. Asia (2), E. Asia & Pacific (1) Fränngård 2006: Uganda, district hospital and health centre IVs Blum 2006: Bangladesh, home‐based maternity care Lester 2003: South Africa, maternity obstetric unit located in large academic hospital Anwar 2009: Bangladesh, basic and comprehensive emergency obsteric care facilities, public VSO 2012: Uganda, hospitals and health centres | |
| A wide range of interlinked reasons for staff shortages were suggested. These included limited funds to recruit health workers, bureaucratic processes of the recruitment process (e.g. absence of committees responsible for recruitment at the district level), scarcity of health workers especially in rural areas, and other factors that deter retention of health workers once recruited (see Table 1). In addition, institutional arrangements (e.g. when health facilities hire contract staff in order to reduce labour costs) and inefficient deployment of available staff may create staff shortages. Facilities with staff shortages and work overload were also seen as unattractive places to work, making it difficult for managers to transfer staff from well‐served to underserved areas, thus compounding/increasing the problem. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 4 studies, and ethical considerations were not reported in 3 studies. However, these may not influence the finding. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns because some studies refer to institutional‐level factors, while others refer to district‐level factors. |
| Adequacy | Moderate concerns because data were from few studies with thin data. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about adequacy; and minor concerns about relevance and methodological limitations |
| Contributing studies/setting | |
| Africa (2), Latin America and Caribbean (1), E. Asia (1), S. Asia (1) Graner 2010: Vietnam, primary health care Anwar 2009: Bangladesh, basic and comprehensive emergency obsteric care facilities, public VSO 2012: Uganda, hospitals and health centres Pitchforth 2010: Ethiopia, teaching hospital Molina 2011: Colombia, primary, secondary, and tertiary care facilities | |
| Health workers' salaries and benefits were considered insufficient for the work done, the responsibility and personal risk, and the additional responsibilities assigned, e.g. through informal task‐shifting. In addition, salaries were insufficient for health workers' personal needs, e.g. to send their children to school and for transport costs to visit their husbands. Low salaries and incentives sometimes led to a lack of motivation and poor performance, absenteeism, and increased rates of dual practice. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns, as reflexivity was not reported in 7 studies; ethics consideration was not reported in 3 studies; and sampling or data analysis methods were not reported in 4 studies. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns because 1 study included health workers on contract, which may be a different arrangement from other studies. |
| Adequacy | Minor concerns because several studies had thin data. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about methodological limitations; and minor concerns about relevance and adequacy |
| Contributing studies/setting | |
| Middle E&N Africa (1), E. Asia (2), Latin America & Caribbean (2), Africa (2), S. Asia (1) Hassan‐Bitar 2011: Palestine, public referral hospital Belizan 2007: Argentina/Uruguay, public hospitals Anwar 2009: Bangladesh, basic and comprehensive emergency obsteric care facilities, public Fränngård 2006: Uganda, district hospital and health centre IVs Ith 2012: Cambodia, provincial and regional hospitals, health centres De Brouwere 2009: Senegal, district hospitals Graner 2010: Vietnam, primary health care Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obsteric services | |
| Health workers perceived managers as lacking in management capacity and skills and sometimes felt unsupported. Health workers also complained that concerns about the workplace were sometimes left unheard, and no solutions or feedback given. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, as reflexivity was not reported in 4 studies, and ethical considerations were not reported in 3 studies. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as only 3 regions were represented; data were from health workers’ views of management; and 1 study referred to lack of management support at a midwife‐led unit in a hospital setting. |
| Adequacy | Minor concerns because some studies had thin data. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about relevance; and minor concerns about methodological limitations and adequacy |
| Contributing studies/setting | |
| Africa (4), S. Asia (1), E. Asia (1) Bradley 2009: Malawi, rural mission hospitals VSO 2012: Uganda, hospitals and health centres Ith 2012: Cambodia, provincial and regional hospitals, health centres Anwar 2009: Bangladesh, basic and comprehensive emergency obstetric care facilities, public Lester 2003: South Africa, maternity obstetric unit located in large academic hospital Mondiwa 2007: Malawi, large government hospital | |
| Helping women access financial assistance for out‐of‐pocket payments was sometimes time‐consuming for health workers. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, though reflexivity was not reported. |
| Coherence | No to very minor concerns |
| Relevance | Serious concerns because only 1 region and teaching hospital population were represented. |
| Adequacy | Serious concerns because data are from 1 study with very thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to serious concerns about relevance and adequacy |
| Contributing studies/setting | |
| S. Asia (1) Pitchforth 2006: Bangladesh, teaching hospital | |
| Inadequate pre‐service and in‐service training sometimes limited health workers’ skills and ability to provide care. For instance, some health workers lacked training to attend home births or manage complicated pregnancies or deliveries, e.g. HIV in pregnancy or eclampsia. In contrast, training allowed midwives to practice assisting women to deliver in non‐supine positions and enabled them to get accustomed to this practice. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because ethical considerations were not reported in 3 studies; reflexivity was not reported in 5 studies; and sampling strategy was not clear in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | No to very minor concerns |
| Adequacy | No to very minor concerns |
| Overall CERQual assessment | |
| High confidence | ‐ |
| Contributing studies/setting | |
| Latin America & Caribbean (1), Africa (3), S. Asia (3), E. Asia & Pacific (1) Fujita 2012: Benin, tertiary hospital Blum 2006: Bangladesh, home‐based maternity care DeMaria 2012. Mexico, public and non‐governmental hospitals Lester 2003: South Africa, maternity obstetric unit located in large academic hospital Mathole 2006: Zimbabwe, health centres in the district Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals Afsana 2001: Bangladesh, health centre Graner 2010: Vietnam, primary health care | |
| Health worker competencies and opportunities for on‐the‐job training were sometimes limited by poor scheduling of in‐service education sessions, the high cost of continuing education for health workers, inequitable selection for professional development opportunities, lack of ongoing training and follow‐up, and shortage of instructors for upgrading courses. In addition, variation in the quality of pre‐service training resulted in varying levels of need for in‐service training, and these needs were not always met, resulting in wide variation in proficiency among health workers. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 2 studies; ethics considerations were not reported in 1 study; and sampling strategy or data analysis methods were not reported in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns, as only 2 regions were represented. |
| Adequacy | Moderate concerns, as data were from only 4 studies with thin data. |
| Overall CERQual assessment | |
| Moderate confidence | Due to minor concerns about methodological limitations and relevance; and moderate concerns about adequacy |
| Contributing studies/setting | |
| Africa (3), East Asia (1) Pettersson 2006: Mozambique, tertiary hospital Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries Ith 2012: Cambodia, provincial and regional hospitals, health centres Fränngård 2006: Uganda, district hospital and health centre IVs | |
| Learning through practical application facilitated acquisition of skills and confidence. The experience gained through, for example, internship, social service year, and working in the community were identified as important for building doctors' and midwives' practical experience and confidence in providing care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns, as reflexivity and sampling strategy were not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as data refer to hospitals that had different models of care (3 with pure models of care, i.e. allopathic medical model, midwifery, obstetric nurse; 2 with mixed models, i.e. medical/midwifery and medical/obstetric nurses). Only 1 region was represented. |
| Adequacy | Severe concerns, as data were from only 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about methodological limitations and relevance; and severe concerns about adequacy |
| Contributing studies/setting | |
| Latin America & Caribbean (1) DeMaria 2012: Mexico, public and non‐governmental hospitals | |
| Health workers reported several barriers to implementing recommended practice. Firstly, health workers were sometimes unaware of current recommended effective practices. Secondly, health workers flexibility, attitudes, and beliefs about medical knowledge and skills sometimes influenced their receptivity to new practice knowledge. For example, health worker attitudes did not view medical education as dynamic; held beliefs that no significant progress had been made and that clinical practice was similar to techniques learnt many years ago; or were not flexible or willing to implement alternative positions of delivery even though these were preferred by women. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, as reflexivity was not reported in 3 studies, and sampling strategy was not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as only hospital populations from 2 regions were represented. |
| Adequacy | Moderate concerns, as only 3 studies with thin data reported this finding. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about relevance and adequacy |
| Contributing studies/setting | |
| Africa (1), Latin Am & Caribbean (2) Belizan 2007: Argentina/Uruguay, public hospitals Pitchforth 2010: Ethiopia, teaching hospital Conde‐Agudelo 2008: Colombia, public and private hospitals, 44% were university teaching hospitals | |
| Lack of time, infrastructure, and skills limited health workers' ability to seek knowledge and practice new clinical skills. For instance, chronic staff shortages meant less time available for health workers to seek information. This was sometimes further compounded by lack of information sources such as internet access and poorly resourced hospital libraries. In addition, lack of training and skills in networking, epidemiology, research appraisal, or critical thinking about clinical practice limited health workers' awareness and receptivity to clinical practice changes, and this lack of skills led some professionals to prefer old, familiar procedures. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 2 studies, and sampling strategy was not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as only 2 regions were represented, and data were from hospital populations. |
| Adequacy | Moderate concerns, as had only 3 studies with thin data. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about relevance and adequacy; and minor concerns about methodological limitations |
| Contributing studies/setting | |
| Africa (1), Latin Am & Caribbean (2) Belizan 2007: Argentina/Uruguay, public hospitals Conde‐Agudelo 2008: Colombia, public and private hospitals, 44% were university teaching hospitals Lugina 2001: Tanzania, municipal hospitals | |
| Lack of guidelines/protocols, or where they were inconsistent or health workers were not aware or were uncertain of them, could impact patient care and outcomes and cause harm. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, as reflexivity was not reported in 3 studies; ethical considerations were not reported in 1 study; and sampling strategy and data analysis were not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | No to very minor concerns |
| Adequacy | Moderate concerns, as data were from only 5 studies, several with thin data. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about adequacy; and minor concerns about methodological limitations |
| Contributing studies/setting | |
| Africa (2), Latin American & Caribbean (1), S. Asia (1), Middle East & North Africa (1) Lugina 2001: Tanzania, municipal hospitals Khalaf 2009: Jordan, maternal and child health centres Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals Mathole 2006: Zimbabwe, health centres in the district de Carvalho 2012: Brazil, university teaching hospital | |
| Health workers did not always adhere to protocols/guidelines, even when aware of them. Guidelines/protocols were not followed for a number of reasons. Some health workers felt that guidelines were insufficient without consensus from staff. Some studies described how health workers continued to practice ineffective procedures because they were considered routine; due to lack of time; because health workers lacked the autonomy to avoid using what they knew to be inappropriate care; or because the resources at the institution were not aligned with the protocols for postpartum care, or when it was unclear who was professionally responsible, for example in using the partograph. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns, as reflexivity was not reported in 5 studies; ethics considerations were not reported in 2 studies; and sampling strategy was not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns due to partial data from each of the studies; studies were mainly from 1 region and primarily hospitals. |
| Adequacy | Moderate concerns due to thin data in several studies. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy |
| Contributing studies/setting | |
| Latin America and Caribbean (4), Africa (1) Pettersson 2006: Mozambique, tertiary hospital Belizan 2007: Argentina/Uruguay, public hospitals de Carvalho 2012: Brazil, university teaching hospital Conde‐Agudelo 2008: Colombia, public and private hospitals, 44% were university teaching hospitals Molina 2011: Colombia, primary, secondary, and tertiary hospitals | |
| Health workers sometimes used unnecessary diagnostic tests and did not follow recommended practice when they feared malpractice suits. This fear could lead to practitioners retaining practices they believed were ‘safer’. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, as no reflexivity was reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as only 1 region was represented. |
| Adequacy | Serious concerns, as data were from 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about relevance; serious concerns about adequacy; and minor concerns about methodological limitations |
| Contributing studies/setting | |
| Latin America & Caribbean (1) Belizan 2007: Argentina/Uruguay, public hospitals | |
| Some health workers did not use recommended interventions when delivering care because of concerns about negative outcomes for the baby or the mother. Examples included the use of magnesium sulphate administered with anaesthesia during Caesarean sections or when monitoring of serum magnesium sulphate levels was not possible. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, as reflexivity was not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as data are from only 1 region. |
| Adequacy | Serious concerns, as included only 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about relevance; serious concerns about adequacy; and minor concerns about methodological limitations |
| Contributing studies/setting | |
| S. Asia (1) Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals | |
| Health workers were sometimes reluctant to admit their lack of skills in delivering care for fear of blame and criticism from managers. This fear of criticism could undermine health worker confidence and performance. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, though reflexivity was not reported in 1 study, and sampling was not clear in another. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns, as data were from only 1 region and hospital populations. |
| Adequacy | Moderate concerns, as had few studies with thin data. |
| Overall CERQual assessment | |
| Low confidence | Due to minor concerns about relevance; and moderate concerns about adequacy |
| Contributing studies/setting | |
| Africa (3) Pettersson 2006: Mozambique, tertiary hospital Lugina 2001: Tanzania, municipal hospitals Thorsen 2012: Malawi, a secondary and tertiary hospital | |
| Insufficient stock and/or lack of drugs such as hydralazine, magnesium sulphate, oxytocin, misoprostol, and antiretrovirals, and supplies such as gloves, sometimes influenced the quality of care provided to mothers and their babies. For instance, health workers had to use less effective alternative drugs (e.g. diazepam) instead of magnesium sulphate. Lack of supplies sometimes limited good hygiene and practice of aseptic techniques, resulting in unsafe practices (e.g. reuse of disposable gloves), which could increase the risk of HIV infection. The lack of supplies sometimes led to poor outcomes and increased the length of stay in health facilities. Lack of supplies could determine if a new clinical practice was implemented and maintained over time. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 8 studies; ethics considerations were not reported in 4 studies; sampling methods were unclear in 3 studies; and data analysis methods were unclear in 3 studies. |
| Coherence | No or very minor concerns |
| Relevance | No or very minor concerns |
| Adequacy | No or very minor concerns, although data were thin, many studies from several regions reported this finding. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about methodological limitations |
| Contributing studies/setting | |
| Africa (8), E. Asia (2), Latin America and Caribbean (3), S. Asia (2) Bradley 2009: Malawi, rural mission hospitals Pitchforth 2010: Ethiopia, teaching hospital Graner 2010: Vietnam, primary health care Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries de Carvalho 2012: Brazil, university teaching hospital Belizan 2007: Argentina/Uruguay, public hospitals Fränngård 2006: Uganda, district hospital and health centres Anwar 2009: Bangladesh, basic and comprehensive emergency obstetric care facilities, public VSO 2012: Uganda, hospitals and health centres Mathole 2006: Zimbabwe, health centres in the district Penfold 2013: Tanzania, hospitals, health centres, dispensaries Foster 2006: Dominican Republic, hospital Lester 2003: South Africa, maternity obstetric unit located in large academic hospital Ith 2012: Cambodia, provincial and regional hospitals, health centres Pitchforth 2006: Bangladesh, teaching hospital | |
| As a result of this lack of drugs or supplies, mothers or their carers had to purchase their own. This sometimes led to wasted time in procuring the drugs and supplies and the creation of informal markets and corruption at health facilities. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 5 studies; ethics considerations were not reported in 2 studies; sampling methods were not clear in 4 studies; and data analysis methods were not reported in 2 studies. Lack of reflexivity can influence findings, as health workers may not report corruption. |
| Coherence | Minor concerns because all studies refer to women or their carers purchasing their own supplies, but only 1 study refers to informal markets and corruption. |
| Relevance | No to very minor concerns |
| Adequacy | Moderate concerns due to thin data |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about methodological limitations and adequacy; and minor concerns about coherence |
| Contributing studies/setting | |
| Africa (5), S. Asia (1), Latin America and Caribbean (1) Pitchforth 2010: Ethiopia, teaching hospital VSO 2012: Uganda, hospitals and health centres Foster 2006: Dominican Republic, hospital Lester 2003: South Africa, maternity obstetric unit located in large academic hospital Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries Fränngård 2006: Uganda, district hospital and health centres Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals | |
| Lack of equipment limited health workers' ability to deliver quality care to mothers and their babies. As a result of this lack of equipment, mothers and their babies sometimes received poor quality care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity was not reported in 8 studies; ethical considerations were not reported in 3 studies; sampling was not reported in 4 studies; and data analysis was not reported in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | No to very minor concerns |
| Adequacy | No to very minor concerns |
| Overall CERQual assessment | |
| High confidence | ‐ |
| Contributing studies/setting | |
| Africa (6), S. Asia (2), East Asia & Pacific (1), Latin America & Caribbean (1) Pitchforth 2010: Ethiopia, teaching hospital Pettersson 2006: Mozambique, tertiary hospital Graner 2010: Vietnam, primary health care Fränngård 2006: Uganda, district hospital and health centres Anwar 2009: Bangladesh, basic and comprehensive emergency obstetric care facilities, public VSO 2012: Uganda, hospitals and health centres Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services Penfold 2013: Tanzania, hospitals, health centres, dispensaries Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals Lester 2003: South Africa, maternity obstetric unit located in large academic hospital | |
| Lack of blood or limited infrastructure to manage blood transfusion prevented health workers from delivering appropriate care. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns; though ethical considerations were not reported in 2 studies and reflexivity was not reported in 2 studies, these may not influence the finding. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns because have 3 studies from 2 regions |
| Adequacy | Moderate concerns due to few studies with thin data |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about adequacy; and minor concerns about relevance |
| Contributing studies/setting | |
| S. Asia (2), E. Asia (1) Anwar 2009: Bangladesh, basic and comprehensive emergency obstetric care facilities, public Afsana 2001: Bangladesh, health centre Ith 2012: Cambodia, public maternity settings in provincial hospital, 2 regional hospitals, and 2 health centres | |
| Lack of equipment, supplies, or drugs sometimes wasted health workers' time, increased their workload and risk of infection, and led to low morale. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 6 studies; ethics considerations were not reported in 3 studies; and sampling and data analysis methods were not clear in 2 studies. |
| Coherence | Minor concerns because some of the studies only reflect a portion of the findings. |
| Relevance | No to very minor concerns |
| Adequacy | No to very minor concerns; although the data are thin, many studies reported this finding. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about methodological limitations; and minor concerns about coherence |
| Contributing studies/setting | |
| Africa (6), E. Asia (1), Latin America and Caribbean (2) Bradley 2009: Malawi, rural mission hospitals Pitchforth 2010: Ethiopia, teaching hospital Graner 2010: Vietnam, primary health care Belizan 2007: Argentina/Uruguay, public hospitals VSO 2012: Uganda, hospitals and health centres Mathole 2006: Zimbabwe, health centres in the district Penfold 2013: Tanzania, hospitals, health centres, dispensaries Foster 2006: Dominican Republic, hospital Lester 2003: South Africa, maternity obstetric unit located in large academic hospital | |
| Poor, incomplete, and non‐systematised patient information could lead to delayed or incorrect management of high‐risk patients, or interfere with continuity of care. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns; though reflexivity and ethical considerations were not reported in 1 study, and sampling methods not reported in 2 studies, these may not have influenced findings. |
| Coherence | No to very minor concerns |
| Relevance | No to very minor concerns |
| Adequacy | Serious concerns because few studies with very thin data reported this finding. |
| Overall CERQual assessment | |
| Low confidence | Due to serious concerns about adequacy |
| Contributing studies/setting | |
| Africa (1), Latin America & Caribbean (1) Pettersson 2006: Mozambique, tertiary hospital Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services | |
| Lack of or unreliable supply of electricity, including a lack of fuel to run generators, and lack of water influenced health providers' ability to deliver quality care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 4 studies; ethics considerations were not reported in 3 studies; and sampling or data analysis methods were not reported in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | No to minor concerns, although data mainly represent Africa (3 studies), and electricity and water are vital for delivering quality care. |
| Adequacy | No to minor concerns; although description of the link between electricity/water and quality of care is thin, we consider this to be sufficient. |
| Overall CERQual assessment | |
| Moderate confidence | Due to moderate concerns about methodological limitations |
| Contributing studies/setting | |
| Africa (3), S. Asia (1) Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries Anwar 2009: Bangladesh, basic and comprehensive emergency obstetric care facilities, public VSO 2012: Uganda, hospitals and health centres Pitchforth 2010: Ethiopia, teaching hospital | |
| The lack of space and amenities as well as poor physical layout and organisation of wards limited the delivery of quality care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported in 7 studies; ethics considerations were not reported in 1 study; sampling methods were not reported in 5 studies; and data analysis methods were not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns because data were from only 2 regions. |
| Adequacy | Minor concerns because data for some of the studies were thin. |
| Overall CERQual assessment | |
| Moderate confidence | Due to minor concerns about adequacy, relevance, and methodological limitations |
| Contributing studies/setting | |
| Africa (4), Latin America and Caribbean (4), Middle East & North Africa (1) Khalaf 2009: Jordan, maternal and child health centres Pitchforth 2010: Ethiopia, teaching hospital Pettersson 2006: Mozambique, tertiary hospital Belizan 2007: Argentina/Uruguay, public hospitals Fränngård 2006: Uganda, district hospital and health centres Conde‐Agudelo 2008: Colombia, public and private hospitals DeMaria 2012. Mexico, public and non‐governmental hospitals Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services Lester 2003: South Africa, maternity obstetric unit located in large academic hospital | |
| The lack of funds and material resources sometimes prevented health facility managers from regularly maintaining equipment and physical infrastructure. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 2 studies, and sampling strategy, ethical considerations, and methods of data analysis were not reported in 1 study. |
| Coherence | Minor concerns because we do not know why there was no maintenance in 1 study. |
| Relevance | No to very minor concerns |
| Adequacy | Moderate concerns because few studies with thin data reported this finding. |
| Overall CERQual assessment | |
| Low confidence | Due to minor concerns about coherence; and moderate concerns about methodological limitations and adequacy |
| Contributing studies/setting | |
| Africa (2), E. Asia (1) Pettersson 2006: Mozambique, tertiary hospital VSO 2012: Uganda, hospitals and health centres Ith 2012: Cambodia, provincial, regional hospitals and health centres | |
| Health facilities varied in the availability, functionality, and quality of interventions assigned as signal functions for obstetric care. At the lower‐level facilities, most of these functions were not available, for instance parenteral antibiotics or anticonvulsants or neonatal resuscitation. At the higher levels, some of these functions appeared to be available, but functionality was variable, for instance when they had drug stock‐outs or unqualified providers of care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity and ethical considerations were not reported in 2 studies, 1 study was an observational study, no interviews with health providers. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because data were drawn from only 2 regions. |
| Adequacy | Moderate concerns because few studies with thin data reported this finding. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy |
| Contributing studies/setting | |
| Africa (1), S. Asia (1) Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries Afsana 2001: Bangladesh, health centre | |
| Health workers felt it was easier to deliver care in facilities than at home. Some of the positive aspects of delivering care at the health facility were that health workers were able to do other work while monitoring labour; provide care for several mothers; work schedules were more regular and care was available 24 hours a day. Furthermore, at facilities, other skilled providers were available to assist when needed, and some procedures (e.g. episiotomies) were easier to perform. In addition, health facilities provided a secure, controlled, hygienic work environment, where electricity, equipment, and medications were always available. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, though ethical considerations and reflexivity were not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because data are from only 1 study where a policy change allowed health workers to compare home‐based maternity care to facility‐based model of care. |
| Adequacy | Serious concerns because data are from only 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| S. Asia (1) Blum 2006: Bangladesh, home‐based maternity care | |
| Where primary care workers in lower‐level facilities lacked the knowledge and skills to determine the need for referral, or were unable to provide emergency care, mothers could receive inadequate care. This lack of skills could also result in unnecessary referrals to other health facilities. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity, ethical considerations, and sampling methods were not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as only 1 region is represented. |
| Adequacy | Serious concerns, as included only 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| Latin America & Caribbean (1) Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services | |
| Lack of trust and professional rivalries between midwives, doctors, and obstetrician gynaecologists could delay referral of mothers and their babies. Midwives sometimes felt blamed by physicians when complications arose and hesitated to seek support from the medical teams at the receiving facilities. Some midwives did not travel with the mothers to the referring facility for fear of blame for any negative occurrence during the referral process. | |
| Assessment for each CERQual component | |
| Methodological limitations | No or very minor concerns, though 1 study did not report reflexivity. |
| Coherence | No or very minor concerns |
| Relevance | Moderate concerns because in 1 study some midwives worked in private facilities but were referring mothers to public facilities, and only 2 regions represented. |
| Adequacy | Moderate concerns, as data are from few studies. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about adequacy and relevance |
| Contributing studies/setting | |
| E. Asia (1), Middle East & N Africa (1) Tabatabaie 2012: Iran, home births by midwives from hospitals and private clinics Ith 2012: Cambodia, provincial and regional hospitals, health centres | |
| Maternal perceptions of the health system could make mothers reluctant to accept referral. For instance, mothers were sceptical about the cost of care, poor management and care at the next‐level facility, the procedures used, the high levels of Caesarean sections, and fear of complications. Also, mothers may have already travelled far to reach the facility they perceived as a good one, or fear unfamiliar urbanised settings. As a result of mothers' reluctance to accept referral, midwives may feel pressured to conduct high‐risk deliveries or spend a lot of time convincing reluctant mothers or their families. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity was not reported in 4 studies, and ethical issues were not reported in 1 study. |
| Coherence | Minor concerns because while all of the studies support how women are reluctant to be referred, not all studies illustrate how this reluctance pressures health workers to conduct risky delivery. |
| Relevance | Minor concerns, as data are taken from health worker perceptions about mothers (indirect), and 1 study from Africa was conducted at a primary care unit in a tertiary centre. |
| Adequacy | Minor concerns due to thin data |
| Overall CERQual assessment | |
| Moderate confidence | Due to minor concerns about methodological limitations, coherence, relevance, and adequacy |
| Contributing studies/setting | |
| E. Asia & Pacific (1), S. Asia (2), Middle East & N Africa (1), Africa (1) Graner 2010: Vietnam, primary health care Blum 2006: Bangladesh, home‐based maternity care Tabatabaie 2012: Iran, home births by midwives from hospitals and private clinics Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals Lester 2003: South Africa, maternity obstetric unit located in large academic hospital | |
| The presence of trust between mothers and midwives may influence a mother's willingness to be referred. Referral may be delayed when facilities lack midwives or other primary care workers whom the mothers trust that can convince mothers of the need for referral. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity unclear, and no ethical considerations reported. |
| Coherence | Minor concerns, as it was not clear if the data were related to the finding. |
| Relevance | Moderate concerns, as data refer to private providers referring mothers to public facilities. |
| Adequacy | Severe concerns, as only 1 study with thin data was included. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about coherence and methodological limitations; moderate concerns about relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| Middle East & N Africa (1) Tabatabaie 2012: Iran, home births by midwives from hospitals and private clinics | |
| Lack of transport hinders referral of women and their babies to higher levels of care. This happened for instance when health facilities lacked ambulances, or facility budgets were insufficient to purchase fuel for vehicles. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, though reflexivity was not reported in 3 studies, and ethics considerations were not reported in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns, as only 3 regions are represented, and in 1 region data are from 1 country. |
| Adequacy | Minor concerns due to very thin data |
| Overall CERQual assessment | |
| Moderate confidence | Due to minor concerns about relevance and adequacy |
| Contributing studies/setting | |
| E. Asia & Pacific (1), Africa (2), Latin America & Caribbean (1) Graner 2010: Vietnam, primary health care Fränngård 2006: Uganda, district hospital and health centres VSO 2012: Uganda, hospitals and health centres Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services | |
| Lack of fuel for vehicles when the need for referral arises is frustrating to nurses and midwives and leaves them feeling helpless when mothers' and babies' lives are at risk. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity, ethics considerations, sampling and data analysis methods were not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as only 1 region is represented. |
| Adequacy | Severe concerns because data are from only 1 study. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| Africa (1) VSO 2012: Uganda, hospitals and health centres | |
| When health facilities lacked fuel for vehicles, mothers and their families were sometimes asked to pay their own transport costs. Many families could not afford this. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, although reflexivity was not reported in 2 studies, and ethics considerations were not reported in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because data are from only 1 country representing 1 region. |
| Adequacy | Moderate concerns due to very thin data from 2 studies |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about relevance and adequacy |
| Contributing studies/setting | |
| Africa (2) Fränngård 2006: Uganda, district hospital and health centres VSO 2012: Uganda, hospitals and health centres | |
| Several situations could lead health workers to refer mothers and shift responsibility to higher levels of care, including when health workers lacked the skills or confidence to provide care or when they worked in isolation; when they were concerned about the facility's reputation when poor patient outcomes arose; or when they lacked supplies, drugs, or equipment to provide care. Some of these referrals were unnecessary and resulted in increased workloads at higher levels of care. | |
| Assessment for each CERQual component | |
| Methodological limitations | No or very minor concerns, though ethical considerations were reported in 2 studies, and reflexivity was not reported in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns, as 1 study refers to health worker conducting home‐based deliveries without team support. |
| Adequacy | Moderate concerns due to few studies with thin data |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about adequacy and relevance |
| Contributing studies/setting | |
| S. Asia (3), E. Asia (1) Blum 2006: Bangladesh, home‐based maternity care Anwar 2009: Bangladesh, basic and comprehensive emergency obstetric facilities, public Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals Ith 2012: Cambodia, public maternity settings in provincial hospital, 2 regional hospitals, and 2 health centres | |
| When secondary‐level care was non‐existent, mothers were sometimes referred to tertiary‐level care, which resulted in congestion at the tertiary level. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity, ethics consideration, sampling methods were not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because only 1 region is represented. |
| Adequacy | Serious concerns because data are from only 1 study with very thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| Latin America and Carribbean (1) Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services | |
| Administrative processes and paperwork and poor communication between referring and receiving levels of care could influence the efficient transfer of mothers and their babies to receiving units. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns, though reflexivity, ethics consideration, sampling methods were not reported. |
| Coherence | Moderate concerns because it was unclear whether the data match our finding. |
| Relevance | Moderate concerns because only 1 region is represented. |
| Adequacy | Serious concerns because data are from only 1 study with very thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to minor concerns about methodological limitations; moderate concerns about coherence and relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| Latin America and Carribbean (1) Molina 2011: Colombia, primary, secondary, and tertiary care providers offering obstetric services | |
| Lack of feedback between referring and receiving facilities could influence midwives' practice and patient outcomes. Midwives perceived this feedback as useful for improving their practice and patient outcomes. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, though reflexivity and sampling methods were not reported. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because only 1 region is represented. |
| Adequacy | Severe concerns because data are from only 1 study. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about relevance; and serious concerns about adequacy |
| Contributing studies/setting | |
| Africa (1) Fränngård 2006: Uganda, district hospital and health centres | |
| Poor attitude and unethical behaviour among health workers could influence the quality of care, such as when health workers are harsh, rude, or impatient with mothers; display poor cultural sensitivity, e.g. by not maintaining women's privacy; or when health workers are absent from their duty stations or involved in the illegal sale of drugs and supplies or expect 'back door' payments for services. Some of the suggested underlying reasons for these attitudes and behaviours were wrong intrinsic reasons for joining the profession and physical exhaustion from the long, solitary hours of work. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 3 studies; ethical considerations were not reported in 2 studies; and sampling methods were not clear in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | Minor concerns because few regions represented. |
| Adequacy | Moderate concerns because data are from few studies, some with thin data. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about methodological limitations and adequacy; and minor concerns about relevance |
| Contributing studies/setting | |
| Africa (2), Middle East & N. Africa (1), S. Asia (1) Hassan‐Bitar 2011: Palestine, public referral hospital Spangler 2012: Tanzania, district hospitals, health centres, and dispensaries VSO 2012: Uganda, hospitals and health centres Afsana 2001: Bangladesh, health centre | |
| Mothers' participation in decision‐making during labour could be limited by health worker attitudes and authoritarian behaviour, for instance when health workers conducted procedures without asking mothers for their opinion, or physicians did not seek feedback from patients about practices or outcomes and expected women to co‐operate. Lack of patient participation in decision‐making can threaten quality of care. Some of the reasons for this behaviour were related to health workers’ attitudes about the woman's preferences and role during delivery of her baby. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 4 studies; ethics considerations were not reported in 1 study; and sampling methods were not clear in 3 studies. |
| Coherence | Minor concerns because there were several reasons authoritarian behaviour and poor attitudes of health workers could explain mothers' non‐participation in decision‐making. Other explanations could be women’s lack of empowerment and cultural reasons on how to behave. |
| Relevance | Moderate concerns because only 2 regions were represented. |
| Adequacy | Minor concerns because data are from few studies. |
| Overall CERQual assessment | |
| Low confidence | Due to minor concerns about coherence and adequacy; and moderate concerns about methodological limitations and relevance |
| Contributing studies/setting | |
| Africa (1), Latin America & Caribbean (4) de Carvalho 2012: Brazil, university teaching hospital Belizan 2007: Argentina/Uruguay, public hospitals Maputle 2010: South Africa, tertiary care hospital Conde‐Agudelo 2008: Colombia, public and private hospitals DeMaria 2012: Mexico, public and non‐governmental hospitals | |
| Some health workers did not value communication, communicated poorly, or said they had problems with communication. Poor communication and interaction could threaten the trust between health workers and mothers, for instance when health workers considered communication with mothers a waste of time and there was insufficient communication between staff and families, or when skilled birth attendants were abrasive and demeaning in their interactions with women and showed no concern for women's families. Language barriers could interfere with effective communication between mothers and health workers. As a result, mothers sometimes appeared not to listen to health workers while health workers mechanically worked through the process of providing care. Health workers acknowledged the need to respect and involve men, women's families, and the community in maternal health, for example in understanding cultural beliefs related to postpartum care. | |
| Assessment for each CERQual component | |
| Methodological limitations | Serious concerns because reflexivity was not reported in 3 studies; sampling methods were not clear in 2 studies; ethical considerations were not reported in 1 study; and data analysis methods were not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because only 4 regions were represented. |
| Adequacy | Moderate concerns because data are from few studies with thin data, and in 2 studies it is unclear if data support finding. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about relevance and adequacy; and serious concerns about methodological limitations |
| Contributing studies/setting | |
| Africa (2), Latin America & Caribbean (1), Middle East & N. Africa (1) Hassan‐Bitar 2011: Palestine, public referral hospital de Carvalho 2012: Brazil, university teaching hospital Blum 2006: Bangladesh, home‐based maternity care Maputle 2010: South Africa, tertiary care hospital Lugina 2001: Tanzania, municipal hospitals | |
| Health workers valued the appreciation, respect, trust, and praise from patients, or when they made friends among mothers or worked with the community. Midwives in particular were delighted when a baby was given their name and seeing the baby grow. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because ethical considerations were not reported in 2 studies; reflexivity was not reported in 3 studies; sampling strategy was not clear in 2 studies; and data analysis methods were not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because only 1 region is represented. |
| Adequacy | Moderate concerns because data are from few studies with very thin data. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy |
| Contributing studies/setting | |
| Africa (3) VSO 2012: Uganda, hospitals and health centres Bradley 2009: Malawi, rural mission hospitals Fränngård 2006: Uganda, district hospital and health centre level IV | |
| Mismatch between people's expectations of health workers and what health workers were actually able to deliver or thought was appropriate could lead to antagonism. For instance, health workers who delivered home‐based care could experience social pressure from families and communities, e.g. to give injections to speed up delivery as opposed to waiting for labour to progress normally. Health workers providing obstetric care at health facilities were sometimes treated harshly by people from the community when there was a lack of supplies and materials. In addition, misconceptions that midwives were not working when they took a break from their work or that health workers sold drugs threatened the trust between health workers and the community. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because reflexivity was not reported in 3 studies; sampling was not reported in 2 studies; ethical considerations were not reported in 2 studies; and data analysis methods were not clear in 1 study. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because data are from only 3 regions, and data seem to relate more to midwives and nurses than to doctors. |
| Adequacy | Moderate concerns due to thin data |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about methodological limitations, relevance, and adequacy |
| Contributing studies/setting | |
| Middle East & N Africa (1), S. Asia (2), Africa (1) Hassan‐Bitar 2011: Palestine, public referral hospital Blum 2006: Bangladesh, home‐based maternity care VSO 2012: Uganda, hospitals and health centres Barua 2011: India, university teaching hospital (tertiary, referral level), 2 secondary‐level hospitals | |
| Midwife‐led shared care was perceived as improving the interaction between mothers, families, and health workers, and could improve health workers' self esteem and lead to a change in hospital culture with respect to service provision. For instance, midwife‐led shared care increased communication between midwives, women and their families; enabled the presence and participation of family members; and together increased satisfaction in the care provided. As a result, the need for medication during delivery was minimised, which reduced the financial burden experienced by families. The supportive environment for mothers, the good interaction between mothers and health workers, as well as recognition of professional expertise among midwives increased self esteem. Midwife‐led shared care enabled other hospital staff to reflect on their own routine activities and manner of communication with families and clients, leading to a change in hospital culture with respect to service provision. | |
| Assessment for each CERQual component | |
| Methodological limitations | Minor concerns because reflexivity was not reported, and sampling strategy was not clear. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because only 1 region was represented. |
| Adequacy | Serious concerns because data are from only 1 study. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about relevance; and severe concerns about adequacy |
| Contributing studies/setting | |
| Africa (1) Fujita 2012: Benin, tertiary hospital | |
| Disrespectful communication, lack of trust, inadequate opportunities to review clinical practice, and poor teamwork and co‐ordination could lead to poor interprofessional relations. Also, tensions could arise when health providers did not recognise each others' capabilities and when acting in a way that reinforces clinical hierarchy, for instance disrespectful interprofessional communication between physicians and midwives. Midwives with lower‐level training could manage normal birth, but they sometimes felt marginalised and less motivated to provide care because midwives with higher levels of training and doctors used qualification, status, and their roles to dominate clinical practice. Tensions were sometimes reported between doctors and clinical officers due to salary differentials, benefits, workload, and status. There was sometimes a lack of understanding of competencies and alternative models of care. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns though reflexivity was not reported in 4 studies; ethical considerations were not reported in 1 study; and sampling methods were not clear in 2 studies. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because models of care, scope of practice, and cadre differed in various settings and may not apply in different context; only 3 regions represented. |
| Adequacy | Moderate concerns because data are from few studies. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about relevance and adequacy |
| Contributing studies/setting | |
| Africa (1), Latin Am & Caribbean (1), E. Asia (1) Bradley 2009: Malawi, rural mission hospitals DeMaria 2012: Mexico, public and non‐governmental hospitals Ith 2012: Cambodia, provincial, regional hospitals and health centres | |
| Nurses and midwives valued and were motivated by a good team dynamic where health workers provided feedback, supported and co‐operated to ensure all shifts were covered. For instance, midwives valued good interprofessional collaboration, which made them feel accepted as part of the professional team and provided them an opportunity to improve their competence through on‐spot education provided by obstetricians. When midwives worked together in a team led by midwives, this increased their ability to share experiences and new practices and their decision‐making responsibility; improved their self esteem; and provided quality assurance and improved the quality of care provided. This teamwork was especially useful when emergencies arose. In another study, researchers observed that nurses had a strong teamwork ethic and functioned well together to complete work. | |
| Assessment for each CERQual component | |
| Methodological limitations | No to very minor concerns, though reflexivity was not reported in 4 studies; ethics considerations were not reported in 2 studies; data analysis methods were not clear in 2 studies; and sampling was not clear in 3 studies. |
| Coherence | No to very minor concerns |
| Relevance | Moderate concerns because only 2 regions are represented. |
| Adequacy | Moderate concerns due to thin data |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about relevance and adequacy |
| Contributing studies/setting | |
| Africa (3), Latin Am & Caribbean (1) Pettersson 2006: Mozambique, tertiary hospital Bradley 2009: Malawi, rural mission hospitals Fränngård 2006: Uganda, district hospital and health centre IVs Foster 2006: Dominican Republic, hospital | |
| Health workers had conflicting views on the role of professional councils. For instance, some viewed professional councils as advocates for their members, while others considered them to be a regulatory body with punitive functions. | |
| Assessment for each CERQual component | |
| Methodological limitations | Moderate concerns because ethical considerations, reflexivity, sampling and data analysis methods were not reported. |
| Coherence | No or very minor concerns |
| Relevance | Moderate concerns because data were from only 1 study and represented only 1 region. |
| Adequacy | Serious concerns because data were from only 1 study with thin data. |
| Overall CERQual assessment | |
| Very low confidence | Due to moderate concerns about methodological quality and relevance; and severe concerns about adequacy |
| Contributing studies/setting | |
| Africa (1) | |
| Sociocultural barriers sometimes hindered mothers from receiving care in hospitals. For instance, women preferred not to be examined by male health providers for cultural reasons, preferred a particular position in which to deliver, or for religious reasons did not divulge information that was needed for their care. | |
| Assessment for each CERQual component | |
| Methodological limitations | No or very minor concerns, though reflexivity was not reported in 4 studies, and ethical considerations were not reported in 2 studies. |
| Coherence | No or very minor concerns |
| Relevance | Moderate concerns because data were from health worker perceptions about mothers and represented only 3 regions. |
| Adequacy | Moderate concerns because data were from only 3 studies, 2 of which had thin data. |
| Overall CERQual assessment | |
| Low confidence | Due to moderate concerns about adequacy and relevance |
| Contributing studies/setting | |
| Africa (1), Middle East & N Africa (1), S. Asia (1) Khalaf 2009: Jordan, maternal and child health centres Thorsen 2012: Malawi, a secondary and tertiary hospital Blum 2006: Bangladesh, home‐based maternity care | |
| Health services inputs identified as important in this synthesis | |||||||||||
| Intervention studies selected from Dudley 2009 review | Number of health workers to manage workload | Other human resource strategies | Training of health workers | Communication strategies | Access to available and functional equipment | Sufficient drugs and supplies | Regular reliable electricity or alternative source of power | Blood supply and infrastructure | Transport for referral or alternative mechanism for transport | General infrastructural inputs, e.g. renovating, reorganisation of wards | Other health services input |
| Manandhar 2004 | No information | No information | Training in essential newborn care of government health staff, CHW, and TBA | No information | Equipped primary care centres with Resuscitaires, phototherapy | Essential neonatal drugs/discussions on resupply with managers | No information | No information | No information | No information | No information |
| Lui 2003 | No information | Task‐shifting ‐ village doctors (assume these are CHW take on health education tasks of midwives) | Training in project management (heads of counties and health teams) | No information | No information | No information | No information | No information | No information | Established EMOC centres for training of BEMOC staff, technical assistance, referral | Quality improvement of hospital (not clear what this entailed) |
| Pardeshi 2011 | Employed staff to fill vacant positions. New cadre, general nurse‐midwife appointed at PHC level | No information | MOs trained in lifesaving anaesthesia skills, MOs and paramedics trained in essential obstetric care | No information | Provided oxygen cylinders, baby warmers | No information | Inverters and solar heaters (electricity backup) at PHC level | Blood storage facility at first‐referral levels | Provided funds for transport during emergencies | Infrastructural improvements, e.g. delivery rooms constructed, repairs and renovations at PHC level | Food and escorts (peer supporters?) during inpatient stay, gave clothes and coconut to mother at discharge |
| Powell‐Jackson 2009 | No information | Pay‐for‐performance of health worker, e.g. attend home birth, conduct facility delivery | No information | No information | No information | No information | No information | No information | No information | No information | No information |
| Wu 2011 | No information | No information | Training of midwives on prenatal care of rural women | No information | No information | No information | No information | No information | No information | No information | No information |
| Tripathy 2010 | No information | No information | Training of front‐line health staff in appreciative inquiry | No information | No information | No information | No information | No information | No information | No information | Health committees for community input into health services design and management |
| Colbourn 2013 | No information | No information | Training health staff in QI methodology (used Plan‐Do‐Study‐Act cycles) | No information | No information | No information | No information | No information | No information | No information | No information |
| Kirkwood 2013 | No information | No information | Training in essential newborn care | No information | No information | No information | No information | No information | No information | No information | Discussions about newborn care practice between district, subdistrict management teams, and health workers at facilities to harmonise practice |
| Amudhan 2013 | Recruited additional auxiliary nurse midwife to PHC level | No information | No information | No information | No information | No information | No information | No information | No information | Upgraded PHC to provide 24‐hour service (not clear what this entailed) | No information |
| Ensar 2014 | No information | No information | No information | No information | Equipped health facilities | Provided supplies for health facilities | No information | No information | Motorcycle ambulances at health centres. Maintenance by the community | No information | No information |
| Pasha 2013 | No information | No information | Training of providers in EMONC | No information | No information | No information | No information | No information | No information | No information | Quality improvement activities (maternal and perinatal audits, facility reviews) |
| Manandhar 2004: Setting: Nepal, community. Participants: women in reproductive age group. Lui 2003: Setting: China, community. Participants: poor pregnant women, managers of target county and health bureaus, obstetric medical staff of township hospitals. Pardeshi 2011: Setting: India, community. Participants: women who had delivered in the five months prior to the survey. Powell‐Jackson 2009: Setting: Nepal. Participants: women with fewer than two children, delivering at a health facility. Doctors, nurses, midwife, health assistant, auxiliary health worker, or maternal child health worker attending a delivery at home or in a public health facility. Wu 2011: Setting: China, community. Participants: midwives based at township hospitals, pregnant mothers. Tripathy 2010: Setting: India, community. Participants: women in reproductive age group who had recently given birth; cluster‐level village health committees, front‐line government health staff. Colbourn 2013: Setting: Malawi, community. Participants: pregnant women, health workers at dispensaries and health centres. Kirkwood 2013: Setting: Ghana, community. Participants: pregnant women and their newborn babies; community‐based surveillance volunteers. Amudhan 2013: Setting: India, community. Participants: pregnant women of low socioeconomic status. Ensar 2014: Setting: Zambia, community. Participants: pregnant women, the community including men, women (including older women), and community leaders. Pasha 2013: Setting: multicentre trial in India, Pakistan, Kenya, Zambia, Argentina, and Guatemala. Participants: pregnant women and their newborn babies, families at community level, community birth attendants, facility‐based healthcare providers. Abbreviations: BEMOC(basic emergency obstetric care), CHW(community health worker), EMOC(emergency obstetric care),EMONC(emergency obstetric and neonatal care),MO(medical officers), PHC(primary health care), QI(quality improvement), TBA (traditional birth attendant). | |||||||||||
| Author | Title of review | Comparison of the scope of the review and this synthesis |
| What prevents quality midwifery care? A systematic mapping of barriers in low and middle income countries from the provider perspective | Review searched a wide range of literature mainly from grey literature, and only included studies where skilled birth attendants had midwifery skills. In contrast, our synthesis searched web‐based databases and was not limited to providers with midwifery skills, but included a broad range of health providers that delivered obstetric care. | |
| Factors that influence the uptake of routine antenatal care services by pregnant women: a qualitative evidence synthesis | Review covers women’s views and experiences, and factors that influence uptake of antenatal care. Includes global literature. Our synthesis focuses on health workers' views, behaviours, and experiences when delivering intrapartum and postnatal care, and includes only studies conducted in low‐ and middle‐income countries. | |
| Disrespectful intrapartum care during facility‐based delivery in sub‐Saharan Africa: a qualitative systematic review and thematic synthesis of women's perceptions and experiences | Review focused on facility‐based deliveries in sub‐Saharan Africa and documented women's perceptions and experiences of intrapartum care. Our synthesis focuses on health workers' views, behaviours, and experiences when delivering intrapartum and postnatal care, in low‐ and middle‐income country settings. | |
| Bohren 2016 | The mistreatment of women during childbirth in health facilities globally: a mixed‐methods systematic review | Global review that focused on mistreatment of women during childbirth and included the perceptions and experiences of women during childbirth as well as health workers. Our synthesis focuses on health workers' views, behaviours, and experiences when delivering intrapartum and postnatal care, in low‐ and middle‐income country settings. |