Profilaxis primaria para la tromboembolia venosa en pacientes sometidos a amputación mayor del miembro inferior
Resumen
Antecedentes
Los pacientes a los que se les realiza la amputación principal de un miembro inferior tienen un mayor riesgo de tromboembolia venosa (TEV). Los factores de riesgo de la TEV en los pacientes con una amputación incluyen edad avanzada, estilo de vida sedentario, enfermedades arteriales de larga duración y una afección con hipercoagulación identificable. La evidencia indica que la profilaxis farmacológica (por ejemplo, heparina, inhibidores del factor Xa, antagonistas de la vitamina K, inhibidores directos de la trombina, antiplaquetarios) es efectiva para prevenir la trombosis venosa profunda (TVP), pero se asocia con un mayor riesgo de hemorragia. Por otro lado, la profilaxis mecánica (por ejemplo, medias antiembolia, compresión neumática intermitente y dispositivos de impulso del pie) no es invasiva y tiene efectos secundarios mínimos. Sin embargo, la profilaxis mecánica no siempre es apropiada en personas con contraindicaciones como enfermedad arterial periférica (EAP), arteriosclerosis o amputaciones bilaterales de los miembros inferiores. Es importante determinar la tromboprofilaxis más efectiva para pacientes sometidos a una amputación mayor, ya sea como tratamiento solo o en combinación con otro. Ésta es una actualización de la revisión publicada por primera vez en 2013.
Objetivos
Determinar la efectividad de la tromboprofilaxis para prevenir la TEV en pacientes sometidos a amputación mayor de la extremidad inferior.
Métodos de búsqueda
El especialista en información del Grupo Cochrane Vascular (Cochrane Vascular Information Specialist) realizó búsquedas en el registro especializado del Grupo Cochrane Vascular (Cochrane Vascular Specialised Register), el Registro Cochrane Central de Ensayos Controlados (Cochrane Central Register of Controlled Trials), las bases de datos MEDLINE, Embase y Cumulative Index to Nursing and Allied Health Literature, y en los registros de ensayos de la Plataforma de registros internacionales de ensayos clínicos de la Organización Mundial de la Salud y ClinicalTrials.gov, hasta el 5 de noviembre de 2019. Se ha previsto realizar una verificación de las referencias de los ensayos identificados para identificar estudios adicionales. No se aplicaron restricciones de idioma.
Criterios de selección
Se incluyeron ensayos controlados aleatorizados y ensayos controlados cuasialeatorizados que asignaron a los pacientes a los que se les realizó una amputación mayor unilateral o bilateral (por ejemplo, desarticulación de la cadera, transfemoral, desarticulación de la rodilla y transtibial) de una extremidad inferior a diferentes tipos o regímenes de tromboprofilaxis (que incluyen profilaxis farmacológica o mecánica) o placebo.
Obtención y análisis de los datos
Dos autores de la revisión seleccionaron los estudios, extrajeron los datos y evaluaron el riesgo de sesgo de forma independiente. Los desacuerdos se resolvieron mediante discusión. Los desenlaces de interés fueron TEV (TVP y embolia pulmonar (EP)), mortalidad, eventos adversos y hemorragia. Se utilizaron los criterios GRADE para evaluar la certeza de la evidencia. Los dos estudios incluidos compararon tratamientos diferentes, por lo que no fue posible agrupar los datos en un metanálisis.
Resultados principales
No se identificaron estudios nuevos aptos para esta actualización. Dos estudios con 288 participantes cumplieron los criterios de inclusión para esta revisión.
Heparina de bajo peso molecular comparada con heparina no fraccionada
Un estudio comparó heparina no fraccionada con la heparina de bajo peso molecular y no encontró evidencia de una diferencia entre los tratamientos en la prevención de la TVP (odds ratio [OR] 1,23; intervalo de confianza [IC] del 95%: 0,28 a 5,35; 75 participantes; evidencia de certeza muy baja). No se produjeron eventos de hemorragia en ninguno de los dos grupos. Las muertes y los eventos adversos no se informaron. Este estudio fue abierto, por lo que tuvo alto riesgo de sesgo de realización. Además, el estudio no informó el método de asignación al azar, por lo que el riesgo de sesgo de selección no estaba claro.
Heparina comparada con placebo
En el segundo estudio, no hubo evidencia de beneficio del uso de heparina para prevenir la EP al compararla con (OR 0,84, IC del 95%: 0,35 a 2,01; 134 participantes; evidencia de certeza baja). Del mismo modo, no se detectó evidencia de mejoría cuando se consideró el nivel de amputación, con una incidencia similar de EP entre los dos grupos de tratamiento: amputación por encima de la rodilla (OR 0,79; IC del 95%: 0,31 a 1,97; 94 participantes; evidencia de baja certeza); y amputación por debajo de la rodilla (OR 1,53; IC del 95%: 0,09 a 26,43; 40 participantes; evidencia de baja certeza). Diez participantes murieron durante el estudio: a cinco se les realizaron autopsias y en tres, se encontró que habían tenido una EP reciente; todos habían pertenecido al grupo placebo (evidencia de certeza baja). Los eventos de hemorragia se informaron en menos del 10% de los participantes en ambos grupos de tratamiento, pero el estudio no presentó datos específicos (evidencia de certeza baja). No se informaron otros eventos adversos. Este estudio no informó los métodos utilizados para ocultar la asignación al tratamiento, por lo que no está claro si ocurrió sesgo de selección. Sin embargo, este estudio pareció estar libre de todas las otras fuentes de sesgo.
Ningún estudio analizó la profilaxis mecánica.
Conclusiones de los autores
No se identificaron estudios nuevos aptos para esta actualización. Como en esta revisión solamente se incluyeron dos estudios y cada uno comparó intervenciones diferentes, no hay evidencia suficiente para establecer alguna conclusión con respecto al régimen de tromboprofilaxis más efectivo en personas a las que se les realiza la amputación de un miembro inferior. Se requieren más estudios de buena calidad a gran escala.
PICO
Resumen en términos sencillos
Prevención de coágulos de sangre venosos en pacientes sometidos a la amputación de un miembro inferior
Antecedentes
La amputación de la pierna se realiza con mayor frecuencia para eliminar tejido muerto (gangrena), úlceras dolorosas, tumores o tejido con una irrigación sanguínea inadecuada. Una de las causas más frecuentes de irrigación sanguínea inadecuada es el estrechamiento de las arterias de las piernas, que representa aproximadamente el 70% de las amputaciones. En los pacientes con esta afección, los coágulos sanguíneos tienen mayores probabilidades de causar problemas como la tromboembolia venosa (TEV). La tromboembolia venosa comprende dos afecciones: un coágulo sanguíneo en las piernas (trombosis venosa profunda [TVP]) o un coágulo sanguíneo en las arterias pulmonares (embolia pulmonar [EP]). El riesgo de que estos eventos ocurran es mayor en los pacientes sometidos a amputaciones. Hay dos formas de medidas preventivas para la TEV: los fármacos y los dispositivos de compresión. Los fármacos resultan efectivos para prevenir la TEV, pero también tienen efectos secundarios adversos. Las medias o los dispositivos de compresión no causan efectos secundarios, pero no son apropiadas para todos. Las guías actuales recomiendan que a cualquier paciente al que se le realice una amputación de un miembro inferior, se le deben ofrecer fármacos para prevenir un coágulo sanguíneo. Sin embargo, en los pacientes con amputación de un miembro inferior, no está claro qué método es mejor. Esta revisión intentó establecer el mejor método.
Características del estudio y principales resultados
Esta revisión se publicó por primera vez en 2013, y se buscaron los estudios que se han realizado desde entonces (hasta el 5 de noviembre de 2019). No se encontraron estudios nuevos aptos para esta actualización. En esta revisión, se incluyen los dos estudios originales con un total combinado de 288 participantes.
Un estudio comparó dos formas del anticoagulante heparina. No se halló evidencia de una diferencia entre la heparina no fraccionada y la heparina de bajo peso molecular para la prevención de la TVP. Ninguno de los participantes informó sangrado. Sin embargo, en este estudio, los participantes y el personal del estudio estaban al tanto del tratamiento que se administraba. Lo anterior puede haber sesgado los resultados. No está claro si se introdujo otro sesgo porque el estudio no describió adecuadamente el proceso de asignación al azar al tratamiento.
El segundo estudio no halló evidencia de beneficio de la heparina comparada con placebo para prevenir una EP si la amputación fue por encima o por debajo de la rodilla. Se produjo hemorragia en menos del 10% de cada grupo de tratamiento, pero los autores del estudio no informaron números específicos y no fue posible analizar este desenlace. Este estudio no informó los métodos utilizados para ocultar la asignación al tratamiento, pero se consideró libre de otras fuentes de sesgo.
Esta revisión encontró que hay muy pocos ensayos para determinar la estrategia más efectiva para prevenir la TEV en pacientes sometidos a la amputación de un miembro inferior. Ningún estudio analizó las formas mecánicas de prevención de la TEV como los dispositivos de compresión, por lo que no es posible establecer alguna conclusión acerca de éstos. Se requieren más estudios de buena calidad y a gran escala.
Certeza de la evidencia
La certeza de la evidencia aportada por estos estudios es muy baja para la comparación de la heparina no fraccionada con la heparina de bajo peso molecular, y baja para la comparación de la heparina con el placebo. Se redujo la certeza de la evidencia debido al pequeño tamaño y al bajo número de estudios y a las preocupaciones sobre los métodos utilizados (riesgo de sesgo). Se necesitan estudios más grandes para determinar la mejor profilaxis de la tromboembolia venosa en pacientes sometidos a amputación importante del miembro inferior.
Authors' conclusions
Summary of findings
| UFH compared to LMWH for VTE prophylaxis in people undergoing major amputation of the lower extremity | ||||||
| Patient or population: people undergoing major amputation of the lower extremity | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Risk with LMWH | Risk with UFH | |||||
| Total VTE (fatal and non‐fatal) | — | — | — | — | — | Only DVT reported |
| DVT (symptomatic, asymptomatic, non‐fatal) (5 to 8 days after surgery) | Study population | OR 1.23 | 75 | ⊕⊝⊝⊝ | — | |
| 98 per 1000 | 117 per 1000 | |||||
| PE (symptomatic, asymptomatic, non‐fatal) | — | — | — | — | — | Not reported |
| All cause mortality | — | — | — | — | — | Not reported |
| Adverse events | — | — | — | — | — | Not reported |
| Bleeding (timing not specified) | — | — | — | — | — | No events occurred in either treatment group |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Low certainty: our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. | ||||||
| aWe downgraded by three steps due to serious concerns in risk of bias (performance bias related to open‐label design), imprecision (due to small sample and event sizes) and confidence intervals that included both benefit and harm. | ||||||
| Heparin compared to placebo for VTE prophylaxis in people undergoing major amputation of the lower extremity | ||||||
| Patient or population: people undergoing major amputation of the lower extremity | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Risk with placebo | Risk with heparin | |||||
| Total VTE (fatal and non‐fatal) | — | — | — | — | — | Only PE reported |
| DVT (symptomatic, asymptomatic, non‐fatal) | — | — | — | — | — | Not reported |
| PE (symptomatic, asymptomatic, non‐fatal) (timing not specified) | Study population | OR 0.84 | 134 | ⊕⊕⊝⊝ | — | |
| 200 per 1000 | 174 per 1000 | |||||
| Above knee amputation | OR 0.79 | 94 | ⊕⊕⊝⊝ | — | ||
| 293 per 1000 | 246 per 1000 | |||||
| Below knee amputation | OR 1.53 | 40 | ⊕⊕⊝⊝ | — | ||
| 42 per 1000 | 62 per 1000 | |||||
| All cause mortality (timing not specified) | 10 participants died during the study. Of these, 3/5 were reported to have had a recent PE following postmortem, all in the placebo group | — | 40 | ⊕⊕⊝⊝ | — | |
| Adverse events (timing not specified) | — | — | — | — | — | No adverse events reported apart from above PE |
| Bleeding (timing not specified) | The incidence of postoperative bleeding was less than 10% in both treatment groups (exact figures were not reported) | — | 40 | ⊕⊕⊝⊝ | — | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence Low certainty: our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. | ||||||
| aWe downgraded by two steps due to serious imprecision (due to small sample and event sizes) and confidence intervals that included both benefit and harm. bWe downgraded by two steps due to serious imprecision (due to small sample and event sizes) and study limitations (data not reported separately by treatment arm). | ||||||
Background
Description of the condition
Lower extremity amputation is performed to remove ischaemic (tissue with a restricted blood supply), infected or necrotic tissue, or in tumour involvement of the surrounding bone or tissue. Dysvascularities (loss of or defective blood supply in a limb), including those related to peripheral vascular disease (PVD) and diabetes mellitus, account for 72% of lower limb amputations in the UK and 75 to 78% in Germany (NASDAB 2009; Spoden 2019). Trauma, infection, malignancy and neurological disorders account for the remainder of cases (Dillingham 2002; Heikkinen 2007; Ziegler‐Graham 2008). PVD includes arterial, venous and lymphatic disease. The prevalence of PVD in the general population is 12% to 14%, and increases to 20% in those aged over 70 years (Shammas 2007). Furthermore, the prevalence is higher still in people with diabetes, an estimated 29% (American Diabetes Association 2003). The observed increase in life expectancy in the UK (Office for National Statistics 2011), coupled with the 50% increase in the incidence of diabetes since 1997 (Kanavos 2012), means that the prevalence of PVD is likely to rise. Despite this, the prevalence of major lower limb amputation in England fell by 17% over the 10 year period from 2003 to 2013 (Ahmad 2016).
People undergoing major lower extremity amputation are at high risk of venous thromboembolism (VTE) (Burke 2000; Harper 1973; Huang 2005; Libertiny 1999; Yeager 1995). Major lower limb amputations are classed as hip disarticulation, transfemoral (above knee), knee disarticulation and transtibial (below knee). Studies have shown the incidence of VTE in people undergoing major lower limb amputation to be between 9.4% (Bandeira 2008) and 13.2% (Struijk‐Mulder 2010a). Risk factors for VTE that are common to people undergoing amputations are advanced age, sedentary lifestyle, longstanding arterial disease and an identifiable hypercoagulable condition (Yeager 1995). While surgery itself is an important and established risk for VTE, it is thought that the slower blood flow proximal to the ligated veins, combined with the endothelial trauma to the veins during amputation, predisposes amputees to a higher risk of deep vein thrombosis (DVT) than other people having surgery (Lastória 2006).
Description of the intervention
There are two types of thromboprophylaxis: pharmacological and mechanical. The type of prophylaxis administered depends upon individual patient risk, amputation level and expected level of activity following amputation. Both pharmacological and mechanical prophylaxis have been shown to reduce the incidence of VTE in people after surgery (Keieme 2011). However, pharmacological prophylaxis is associated with adverse events, such as heparin‐induced thrombocytopenia (HIT) (a relative decrease of platelets in the blood) and bleeding. Clinicians have to consider the risk of VTE against the risk of adverse events. Unlike pharmacological prophylaxis, methods of mechanical prophylaxis are not associated with increased risk of bleeding. However, mechanical prophylaxis is not appropriate for people with peripheral arterial disease, arteriosclerosis, gangrene or double lower limb amputation. Furthermore, applying mechanical prophylaxis to just one leg may not prevent DVT in the proximal veins on the side undergoing amputation.
How the intervention might work
Pharmacological prophylaxis
There are several pharmacological agents for the prevention of VTE.
Heparins
Unfractionated heparin (UFH) acts as an anticoagulant, thus preventing the formation of clots or extensions of existing clots within the blood. It binds to the enzyme inhibitor antithrombin, which inactivates the effect of thrombin and other coagulation enzymes involved in blood clotting (X, IX, XI and XII) (Chuang 2001). UFH can be administered intravenously or by subcutaneous injection (UK National Clinical Guidelines 2010). UFH has a short half‐life of approximately one hour, so requires frequent or continuous infusions (Eikelboom 2002). However, its lower weight derivative (low molecular weight heparin (LMWH)) has a half‐life of four to five hours, allowing once‐daily dosing (Weitz 2004). National Institute for Health and Care Excellence (NICE) guidelines recommend LMWH as first‐line pharmacological VTE prophylaxis unless contraindicated (NICE 2018). Heparin can be used as a prophylactic measure or to treat VTE. Heparin can cause serious side effects, including HIT, defined as a decrease in platelet count during or following exposure to heparin (Warkentin 2004). Evidence has shown that approximately 0.1% to 5% of people on heparin will develop HIT (Baglin 1997; Kelton 2002; Salter 2016). HIT is a serious and potentially life‐threatening condition (Franchini 2005).
Factor Xa inhibitor
Fondaparinux also binds to antithrombin but, unlike heparin, it does not inhibit thrombin. Instead, the binding of fondaparinux to antithrombin selectively inactivates factor Xa, thus inhibiting coagulation (Bauer 2002). It has a longer half‐life than heparin, allowing it to be administered once daily as a subcutaneous injection (UK National Clinical Guidelines 2010). Fondaparinux has been shown to be as effective and as safe as adjusted dose, intravenous administration of UFH in the initial treatment of pulmonary embolism (PE) (Matisse 2003). Furthermore, as fondaparinux does not interact with platelets, there is no risk of HIT (Bauer 2001). Fondaparinux is more expensive than heparin, which may limit its use. Other factor Xa inhibitors, rivaroxaban and apixaban, are recommended as options for the prevention of VTE in people undergoing elective total hip or knee replacement (NICE 2018). A recent systematic review and network meta‐analysis showed that rivaroxaban and apixaban were the top two most effective strategies, respectively, for preventing DVT in people undergoing elective total knee replacement. (Lewis 2019). NICE published guidelines based on a review of evidence from four randomised controlled trials, that involved over 12,000 people undergoing total hip or knee replacement (NICE 2009). Results showed that, although rivaroxaban is at least as effective as LMWH in the prevention of VTE, it is associated with a higher rate of major bleeding. This was supported by a recent meta‐analysis, where rivaroxaban had the second highest odds ratio for major bleeding, after fondaparinux (Lewis 2019).
Vitamin K antagonists
Warfarin is a synthetic derivative of coumarin, a chemical found naturally in many plants. It acts as a vitamin K antagonist, which in turn reduces the amount of active clotting factors, thereby producing a state of anticoagulation (Holford 1986). The effect of warfarin is not immediate. It is administered at a variable dose that is adjusted until it reaches a therapeutic level, defined by an international normalised ratio (INR) of 2.5 (Ansell 2008). The response to warfarin varies according to several factors, including: age, genetic status, medications, diet, underlying medical conditions and smoking status (UK National Clinical Guidelines 2010). Due to the time taken to achieve a therapeutic level sufficient to protect against thromboembolic events, people undergoing surgery stop warfarin upon admission to hospital and receive heparin, which provides immediate anticoagulation (UK National Clinical Guidelines 2010). Bleeding is the primary adverse event associated with warfarin. Although the effects of warfarin can be reversed through discontinuation of the drug or administration of vitamin K or prothrombin concentrate, the reversal is permanent and often difficult to achieve (UK National Clinical Guidelines 2010).
Direct thrombin inhibitors
Direct thrombin inhibitors (DTIs) act as anticoagulants by directly inhibiting the enzyme thrombin and thus delaying blood clotting. The DTI dabigatran is recommended as an option for the prevention of VTE in people undergoing elective total hip or knee replacement (NICE 2018). Unlike warfarin, DTIs are immediately effective and do not require dose adjustment and close monitoring (UK National Clinical Guidelines 2010). However, the anticoagulation effect of DTIs is non‐reversible.
Antiplatelets
Aspirin has an antiplatelet effect by inhibiting the production of thromboxane. Guidelines have recommended aspirin as primary prophylaxis for the prevention of VTE following orthopaedic surgery (Falck‐Ytter 2012). Two recent meta‐analyses have shown that aspirin has similar efficacy and safety outcomes in people undergoing total hip and total knee replacements (Haykal 2019; Matharu 2020). Prolonged use of aspirin has been shown to increase the risk of gastrointestinal bleeding and stomach ulcers, particularly when taken with warfarin (Sørensen 2000).
Mechanical prophylaxis
Mechanical devices work to reduce venous stasis in the leg, a known risk factor for VTE (Morris 2004). They are non‐invasive and, unlike pharmacological prophylaxis, there is no risk of bleeding. Depending on the estimated risk of VTE, mechanical devices can be used alone or in combination with pharmacological prophylaxis (UK National Clinical Guidelines 2010). Methods include antiembolism stockings (AES), intermittent pneumatic compression devices (IPCD) and foot impulse devices (FID), also known as foot pumps.
Antiembolism stockings
AESs exert graded circumferential pressure from the distal to the proximal regions of the leg. They have two potential actions in preventing DVT in immobile people. First, exerting graduated compression increases blood flow velocity, which promotes venous return; and second, preventing passive venous distension is thought to prevent subendothelial tears and the activation of clotting factors (UK National Clinical Guidelines 2010). AESs are contraindicated in people with peripheral arterial disease and arteriosclerosis.
Intermittent pneumatic compression devices
IPCDs comprise inflatable cuffs placed around the foot, calf or thigh. The cuffs are intermittently inflated, powered by a pneumatic pump. The inflation and deflation process stimulates the calf muscle pump, thus forcing blood in the deep veins up towards the heart. This increases the velocity of blood flow in the deep veins of the leg, thereby reducing venous stasis and hypertension (Goucke 1989). Calf compression with an IPCD has also been shown to enhance fibrinolysis, a process that augments thrombus breakdown and prevents clot formation (Storti 1996).
Foot impulse devices
FIDs (or foot pumps) act by creating the effect of walking in immobilised people. During ambulation, the muscle pump in the foot forces blood in the deep veins upwards towards the heart. This action increases venous outflow in the deep veins, thereby reducing stasis and venous hypertension and preventing the formation of blood clots in the legs (Gardner 1983). FIDs recreate this physiological process through artificially stimulating the foot pump, thereby mimicking the effect of walking (UK National Clinical Guidelines 2010).
Why it is important to do this review
Evidence from observational studies in people undergoing major lower extremity amputation supports the use of pharmacological thromboprophylaxis (Burke 2000; Harper 1973; Hill 2010; Huang 2005; Lastória 2006; Yeager 1995). Indeed, one study reported that DVT occurred in 50% of people following major lower extremity amputation without prophylaxis (Harper 1973). In one randomised trial comparing LMWH and UFH for amputations, the incidence of DVT was similar in each group at about 10% (Lastória 2006). Nevertheless, some evidence suggests that, despite the use of pharmacological thromboprophylaxis (with LMWH), the rate of VTE in people undergoing amputation remains high (Struijk‐Mulder 2010a). Mechanical prophylaxis, including IPCDs and AESs, has been proposed as a useful addition to pharmacological prophylaxis (Struijk‐Mulder 2010b), but this is not always appropriate in amputees with contraindications.
The Scottish Intercollegiate Guidelines Network (SIGN) recommends thromboprophylaxis in all people undergoing all major lower extremity amputations (SIGN 2010). With conflicting reports regarding the efficacy of thromboprophylaxis, it is imperative to determine the most effective. This is an update of the review first published in 2013 (Robertson 2013a).
Objectives
To determine the effectiveness of thromboprophylaxis in preventing VTE in people undergoing major amputation of the lower extremity.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs) and quasi‐randomised controlled trials in which people undergoing an amputation of the lower extremity were allocated to receive different types of thromboprophylaxis. We included published studies and studies in progress if preliminary results were available. Non‐English studies were also eligible for inclusion in the review.
Types of participants
We included people undergoing major unilateral or bilateral amputation (hip disarticulation, transfemoral (above knee), knee disarticulation, ankle disarticulation and transtibial (below knee) of the lower extremity). We excluded people undergoing minor amputations of the toes or a portion of the foot.
Types of interventions
-
Pharmacological prophylaxis (LMWH, UFH, factor Xa inhibitors, vitamin K antagonists, DTIs, antiplatelets)
-
Mechanical prophylaxis (AES, IPCD, FID) (for unilateral amputees only)
Comparisons included:
-
One pharmacological prophylaxis versus another (e.g. LMWH versus UFH)
-
One mechanical prophylaxis versus another (e.g. AES versus FID)
-
Pharmacological prophylaxis versus mechanical prophylaxis
-
Pharmacological plus mechanical prophylaxis versus mechanical prophylaxis alone
-
Prophylaxis (pharmacological or mechanical, or both) versus placebo
Types of outcome measures
Primary outcomes
-
Total VTE (non‐fatal and fatal)
-
Symptomatic or asymptomatic non‐fatal VTE (DVT or PE) confirmed by diagnostics tests, including helical computed tomography (CT), CT angiography and ventilation‐perfusion lung scintigraphy for diagnosis of PE; and complete compression ultrasonography and impedance plethysmography (test in which air is used to determine circulatory capacity) for diagnosis of DVT
Secondary outcomes
-
All‐cause mortality
-
Adverse events (HIT)
-
Bleeding, as defined by the Bleeding Academic Research Consortium Definition for Bleeding (Mehran 2011):
-
type 0 ‐ no bleeding;
-
type 1 ‐ no actionable bleeding;
-
type 2 ‐ overt bleeding requiring either non‐surgical intervention or hospitalisation, or prompting evaluation;
-
type 3 ‐ overt bleeding with a drop in haemoglobin (Hb). Subdivided into 3a (Hb drop 3 to 5 g/dL, 3b (Hb drop > 5 g/dL or 3c (intracranial haemorrhage);
-
type 5 ‐ fatal bleeding.
-
Search methods for identification of studies
Electronic searches
For this update, the Cochrane Vascular Information Specialist conducted systematic searches of the following databases for RCTs and controlled clinical trials without language, publication year or publication status restrictions:
-
the Cochrane Vascular Specialised Register via the Cochrane Register of Studies (CRS‐Web searched 5 November 2019);
-
the Cochrane Central Register of Controlled Trials (CENTRAL) Cochrane Register of Studies Online (CRSO 2019, Issue 10);
-
MEDLINE (Ovid MEDLINE® Epub Ahead of Print, In‐Process & Other Non‐Indexed Citations, Ovid MEDLINE® Daily and Ovid MEDLINE®) (1 January 2017 to 5 November 2019);
-
Embase Ovid (1 January 2017 to 5 November 2019);
-
CINAHL EBSCO (Cumulative Index to Nursing and Allied Health Literature; 1 January 2017 to 5 November 2019);
-
AMED Ovid (Allied and Complementary Medicine; 1 January 2017 to 5 November 2019).
The Information Specialist modelled search strategies for other databases on the search strategy designed for CENTRAL. Where appropriate, they were combined with adaptations of the highly sensitive search strategy designed by Cochrane for identifying RCTs and controlled clinical trials (as described in the Cochrane Handbook for Systematic Reviews of Interventions Chapter 6, Lefebvre 2011). Search strategies for major databases are provided in Appendix 1.
The Information Specialist searched the following trials registries on 5 November 2019:
-
the World Health Organization International Clinical Trials Registry Platform (who.int/trialsearch);
-
ClinicalTrials.gov (clinicaltrials.gov).
Searching other resources
We translated non‐English language trials where required, and searched reference lists of identified studies.
Data collection and analysis
Selection of studies
Two review authors (DH, MT) screened the results of the 2019 search. These authors also independently assessed full‐text articles of potentially relevant studies. They resolved any disagreements by discussion or referred them to a third author for decision making (VP). For the previous version, one review author (LR) used the selection criteria to identify trials for inclusion and the second review author (AR) independently confirmed this selection (Robertson 2013a). We excluded studies which did not meet the inclusion criteria, and noted the reasons.
Data extraction and management
We did not identify any new eligible studies for this update. For the previous version of the review, two review authors (LR, AR) independently extracted the data. They recorded information about the trial design, type of amputation, baseline characteristics of participants and type of prophylaxis. They recorded non‐fatal and fatal VTE data as the primary outcome measures, and collected information on bleeding and deaths in accordance with the secondary outcome measures. They contacted the authors of included studies if they required further information or clarification. They resolved any disagreements about data extraction and management by discussion.
Assessment of risk of bias in included studies
We did not include any new studies in this update. For the previous version of the review, two review authors (LR, AR) independently used the Cochrane 'Risk of bias' tool to assess risk of bias for each of the included studies (Higgins 2011). The tool provides a protocol for judgements on sequence generation, allocation methods, blinding, incomplete outcome data, selective outcome reporting and any other relevant biases. They resolved any disagreements by discussion.
Measures of treatment effect
The analysis used intention‐to‐treat data from the individual clinical trials. As the primary and secondary outcomes were all binary measures, the effect measures were odds ratios (ORs) with 95% confidence intervals (CI).
Unit of analysis issues
The unit of analysis within each trial was the individual participant.
Dealing with missing data
The authors of the previous version of this review sought information about dropouts, withdrawals and other missing data and, if not reported, contacted study authors for this information.
Assessment of heterogeneity
The inclusion of studies on a wide range of medical treatments is likely to result in a high degree of heterogeneity. We planned to assess the heterogeneity between pooled studies by using the Chi2 test regarding the characteristics and quality of the included studies. We planned to use the I2 statistic to measure the degree of inconsistency between studies, with results of 50% representing moderate to substantial heterogeneity (Deeks 2011). However, we only included two studies in this review. The studies tested different drugs and it was not possible to pool the data. Therefore, we could not assess heterogeneity between studies.
Assessment of reporting biases
We planned to assess reporting biases such as publication bias by funnel plots. There are many reasons for funnel plot asymmetry and we consulted the Cochrane Handbook for Systematic Reviews of Interventions to aid the interpretation of the results (Sterne 2011). However, as we only included two studies in the review, it was not possible to test for funnel plot asymmetry.
Data synthesis
We did not identify any new eligible studies for this update. One of the previous review authors (LR) inputted the data into Review Manager (Review Manager 2014), and the second review author (AR) cross‐checked the data entry. They resolved any discrepancies by consulting the source publication. The previous authors planned to use a random‐effects model to analyse the data.
Subgroup analysis and investigation of heterogeneity
Where possible, we attempted to analyse clinically relevant subgroups based on type of prophylaxis and participant groupings. Subgroupings we intended to investigate if data were available included:
-
DVT or PE;
-
indication for amputation;
-
level of amputation (transfemoral, transtibial, exarticulation knee);
-
history of VTE;
-
diabetes;
-
PVD (arterial, venous and lymphatic disease);
-
smoking;
-
body mass index (BMI);
-
duration of prophylaxis.
Sensitivity analysis
We planned to conduct sensitivity analysis to examine the stability of the results in relation to the quality of the included studies. However, as we only included two studies in the review, it was not feasible to perform a sensitivity analysis.
Summary of findings and assessment of the certainty of the evidence
We prepared a 'Summary of findings' table to present the findings from our review for each comparison: 'Unfractionated heparin compared to low molecular weight heparin for venous thromboembolism prophylaxis in people undergoing major amputation of the lower extremity' (summary of findings Table 1), and 'Heparin compared to placebo for venous thromboembolism prophylaxis in people undergoing major amputation of the lower extremity' (summary of findings Table 2). We included the outcomes total VTE, DVT and PE, all cause mortality, adverse events and bleeding.
We used GRADEprofiler software to create the table (GRADEpro GDT). We used the GRADE criteria to rank the certainty of the evidence for each outcome based on risk of bias, inconsistency, indirectness, imprecision and publication bias (Guyatt 2008). We have provided a description for each step to downgrade the certainty of the evidence.
Results
Description of studies
Results of the search
Figure 1 shows the results of the search. For this update, we did not identify any new eligible studies and we excluded one new study (Casella 2015). We did not identify any ongoing studies or studies awaiting classification.
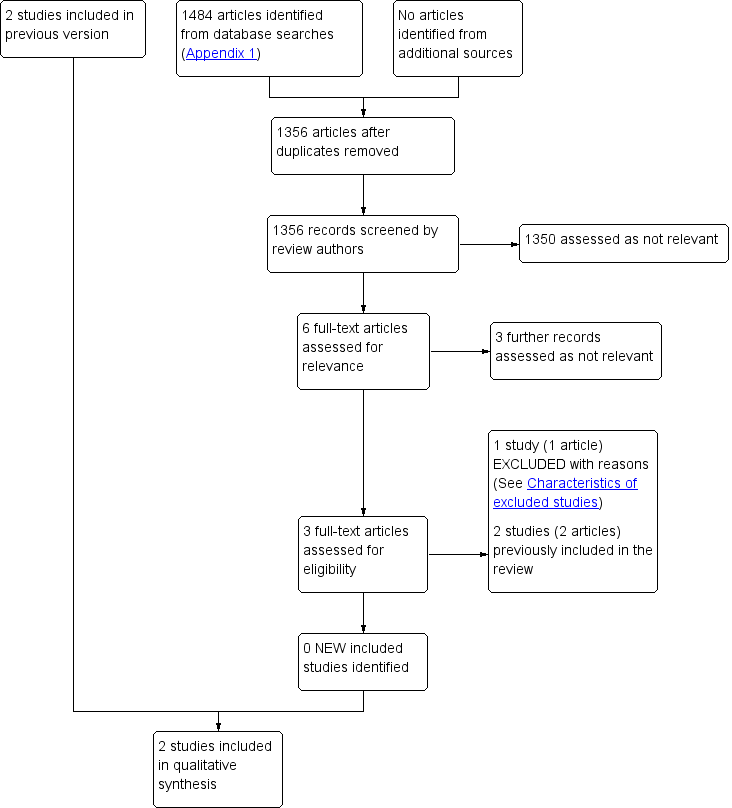
Study flow diagram.
Included studies
We did not identify any new eligible studies for this update. The previous version included two studies (Lastória 2006; Williams 1978). The 'Characteristics of included studies' table describes the included studies.
One study was an open‐label RCT, which randomised 75 participants undergoing elective or emergency lower limb amputation for critical limb ischaemia (CLI) to receive subcutaneous UFH (5000 IU twice daily) or 40 mg enoxaparin daily (Lastória 2006). The study excluded people with a previous VTE or a contraindication to anticoagulant prophylaxis. Prophylaxis began 12 hours before elective surgery or, in emergency cases, on the first day postoperatively. The trialists assessed DVT by daily clinical examination and duplex ultrasound before surgery, and again between five and eight days after surgery. The study diagnosed DVT as an 'abnormal venous flow and evidence of intraluminal thrombi confirmed with compressive ultrasonography'. Of the 75 participants, 30 underwent an above‐knee amputation while the remaining 45 had a below‐knee amputation. The study randomised 34 participants to UFH and 41 to LMWH.
The second study was a randomised, double‐blind trial (Williams 1978). This randomised 134 participants undergoing lower extremity amputation for the complications of ischaemic vascular disease to receive low dose heparin or placebo. Sixty‐nine participants with an amputation (53 above knee and 16 below knee) received 10,000 USP units/ml of sodium heparin subcutaneously, at a rate of 0.5 ml every 12 hours for two weeks or until discharge. Sixty‐five participants (41 above knee and 24 below knee) received saline. Treatment started approximately two hours before surgery. Participants had lung perfusion scans before surgery and then at weekly intervals for the duration of treatment. Participants with a new pulmonary perfusion defect underwent pulmonary arteriography and, if that was unclear,
selective pulmonary angiography. PE was diagnosed if a new lobar, segmental or subsegmental perfusion defect appeared that was not attributable to an infiltrate, pleural effusion, vascular congestion or atelectasis appearing on the chest roentgenogram.
Excluded studies
Details of excluded studies are listed in the 'Characteristics of excluded studies' Table.
We identified one new excluded study (Casella 2015), bringing the total number of excluded studies to 13 (Atkins 1978; Casella 2015; Covey 1975; Di Serio 1985; Haas 2005; Huttenen 1977; Kakkar 1978; Kakkar 2005; Kill 1979; Mantz 2011; Nicolaides 1972; Pachter 1977; Strand 1975). We excluded 11 studies as they did not include participants undergoing amputations (Atkins 1978; Covey 1975; Di Serio 1985; Haas 2005; Huttenen 1977; Kakkar 1978; Kakkar 2005; Kill 1979; Mantz 2011; Nicolaides 1972; Strand 1975). We excluded one study as the authors did not state what the control treatment was, and did not report the methods of diagnosing DVT and PE (Pachter 1977). We excluded the new study by Casella 2015 as it randomised a heterogenous cohort of participants that included people undergoing amputations, but did not provide results specific to these participants. We contacted the authors to obtain participant level data, but did not receive any response.
Risk of bias in included studies
Figure 2 shows our judgements about each bias domain, presented as percentages across both of the included studies. Figure 3 depicts our assessments of each study's risk of bias in each domain.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Although both studies were randomised, the study by Lastória 2006 did not provide any information on the method of randomisation used, so we could not assess the risk of selection bias. The study by Williams 1978 used a random number table, so was at low risk of selection bias. In terms of concealing the allocation of treatment, the study by Lastória 2006 used serial number envelopes while the study by Williams 1978 did not report the methods used.
Blinding
Of the two studies, one was open‐label and therefore at a high risk of performance bias (Lastória 2006). The remaining study blinded both study participants and personnel, so was at low risk of performance bias (Williams 1978). Both studies blinded outcome assessors to the treatment, and we deemed these to be at low risk of detection bias.
Incomplete outcome data
Both studies accounted for all incomplete outcome data, so we judged them to be at low risk of attrition bias.
Selective reporting
Both studies reported data on all prespecified primary and secondary outcomes. We therefore considered them to have a low risk of reporting bias.
Other potential sources of bias
The two studies appeared to be free from other sources of bias.
Effects of interventions
See: Summary of findings 1 Unfractionated heparin compared to low molecular weight heparin for venous thromboembolism prophylaxis in people undergoing major amputation of the lower extremity; Summary of findings 2 Heparin compared to placebo for venous thromboembolism prophylaxis in people undergoing major amputation of the lower extremity
We included two studies in this review (Lastória 2006; Williams 1978). Lastória 2006 compared UFH against LMWH, and Williams 1978 compared UFH with a placebo. We did not include any studies on mechanical prophylaxis, such as compression devices.
Unfractionated heparin (UFH) versus low molecular weight heparin (LMWH)
The study by Lastória 2006 reported this comparison. summary of findings Table 1 describes the outcomes.
Primary outcomes
Lastória 2006 did not report total VTE as an outcome.
Four of the 34 participants randomised to UFH had a DVT, compared to four of the 41 randomised to LMWH, showing no evidence of a difference between treatments (OR 1.23, 95% CI 0.28 to 5.35; 75 participants; very low‐certainty evidence; Analysis 1.1). The study authors reported the number of participants with above and below knee amputations, but did not present the results according to amputation type. We contacted the authors for this data, but they did not respond to our communication.
The study did not formally report PE events.
Secondary outcomes
No bleeding events occurred in either treatment group. The study did not formally report deaths or adverse events.
Heparin versus placebo
The study by Williams 1978 compared heparin with placebo. summary of findings Table 2 describes the outcomes for this comparison.
Primary outcomes
Williams 1978 did not report total VTE or DVT as outcomes.
The incidence of PE was similar in the heparin (14/69) and placebo (13/65) groups showing no evidence of a difference between the groups (OR 0.84, 95% CI 0.35 to 2.01; 134 participants; low‐certainty evidence; Analysis 2.1). When analysed by type of amputation, heparin offered no improvement over placebo: above knee amputation OR of 0.79 (95% CI 0.31 to 1.97; 94 participants; low‐certainty evidence), below knee amputation OR of 1.53 (95% CI 0.09 to 26.43; 40 participants; low‐certainty evidence). No differences were detected between the subgroups (P = 0.66).
Secondary outcomes
Williams 1978 reported that 10 participants died during the study. Of those 10 people, five underwent a postmortem and three were found to have had a recent PE, all of whom were on placebo (low‐certainty evidence).
The incidence of postoperative bleeding was less than 10% in both treatment groups, although the paper did not report the exact figures and the study authors did not respond to requests for these data (low‐certainty evidence). The trialists removed one participant (randomised to placebo) prematurely from the study, due to excessive bleeding.
There were no reports of other adverse events.
Discussion
Summary of main results
We did not identify any eligible new studies for this update. Only two studies fulfilled the eligibility criteria for inclusion in this review. The study by Lastória 2006 compared the effectiveness of UFH with LMWH in the prevention of DVT up to eight days postamputation. There was no evidence of a difference between the two interventions in terms of DVT risk, and no bleeding occurred in the study population. The study by Williams 1978 was concerned with pulmonary embolism. There was no evidence of a benefit of heparin compared with placebo for this outcome, regardless of the level of amputation. Neither study used mechanical prophylaxis in addition to pharmacological prophylaxis.
Overall completeness and applicability of evidence
At present, there is a severe lack of evidence concerning the effectiveness of pharmacological and mechanical prophylaxis in the prevention of VTE in people with lower limb amputation. The two studies tested different drugs and outcomes, so we could not pool their results in a meta‐analysis. Only one study presented data according to the level of amputation. Neither study used mechanical prophylaxis in addition to the drugs administered. Furthermore, we did not include any study on mechanical prophylaxis in the review.
Quality of the evidence
The methodological quality of reporting in the studies was generally good. The risk of selection bias was unclear as one study failed to report the process of randomisation (Lastória 2006), while the second study did not state the methods used to conceal allocation of treatment (Williams 1978). The study by Lastória 2006 was open‐label, and therefore at high risk of performance bias. Both study authors accounted for all missing data and reported data on all their primary and secondary outcomes, so minimised the chances of attrition and performance bias. The two studies included in this review were based on relatively small sample sizes. The effect estimates from our results were imprecise and the confidence intervals were compatible with both benefit and harm. Therefore, using the GRADE criteria, we downgraded the certainty of the evidence from high to very low for the comparison of UFH versus LWMH, and from high to low for the comparison of heparin versus placebo (see summary of findings Table 1; summary of findings Table 2).
Potential biases in the review process
None of the authors of this review were involved in any of the included or excluded studies. Furthermore, none have any commercial or other conflict of interest. The search was as comprehensive as possible, and two reviewers independently assessed all studies for inclusion. We are confident that we have included all relevant studies and we have attempted to reduce bias in the review process. However, the possibility remains that we may have missed studies which have not been published.
Agreements and disagreements with other studies or reviews
Many studies have measured the effectiveness of drug prophylaxis on the prevention of VTE after surgery, including a recent Cochrane Review on prolonged LMWH VTE prophylaxis after abdomino‐pelvic surgery (Felder 2019). A significant portion of studies have been conducted in people undergoing hip or knee replacement, including a Cochrane Review which found that extended‐duration direct oral anticoagulants showed reduced symptomatic VTE and DVT (Forster 2016). A recent network meta‐analysis showed that rivaroxaban was the most effective strategy in preventing DVT in the total knee replacement population (Lewis 2019). Despite this evidence, specific data for people undergoing amputation are rarely presented. Research on mechanical forms of prophylaxis in people with amputation is scarce. To date, no other systematic review has attempted to assess the effectiveness of prophylaxis in the prevention of VTE specifically in people undergoing amputation. This is an update of the review first published in 2013.

Study flow diagram.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Comparison 1: Unfractionated heparin versus low molecular weight heparin, Outcome 1: Deep vein thrombosis (DVT)

Comparison 2: Heparin versus placebo, Outcome 1: Pulmonary embolism
| UFH compared to LMWH for VTE prophylaxis in people undergoing major amputation of the lower extremity | ||||||
| Patient or population: people undergoing major amputation of the lower extremity | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Risk with LMWH | Risk with UFH | |||||
| Total VTE (fatal and non‐fatal) | — | — | — | — | — | Only DVT reported |
| DVT (symptomatic, asymptomatic, non‐fatal) (5 to 8 days after surgery) | Study population | OR 1.23 | 75 | ⊕⊝⊝⊝ | — | |
| 98 per 1000 | 117 per 1000 | |||||
| PE (symptomatic, asymptomatic, non‐fatal) | — | — | — | — | — | Not reported |
| All cause mortality | — | — | — | — | — | Not reported |
| Adverse events | — | — | — | — | — | Not reported |
| Bleeding (timing not specified) | — | — | — | — | — | No events occurred in either treatment group |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Low certainty: our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. | ||||||
| aWe downgraded by three steps due to serious concerns in risk of bias (performance bias related to open‐label design), imprecision (due to small sample and event sizes) and confidence intervals that included both benefit and harm. | ||||||
| Heparin compared to placebo for VTE prophylaxis in people undergoing major amputation of the lower extremity | ||||||
| Patient or population: people undergoing major amputation of the lower extremity | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Risk with placebo | Risk with heparin | |||||
| Total VTE (fatal and non‐fatal) | — | — | — | — | — | Only PE reported |
| DVT (symptomatic, asymptomatic, non‐fatal) | — | — | — | — | — | Not reported |
| PE (symptomatic, asymptomatic, non‐fatal) (timing not specified) | Study population | OR 0.84 | 134 | ⊕⊕⊝⊝ | — | |
| 200 per 1000 | 174 per 1000 | |||||
| Above knee amputation | OR 0.79 | 94 | ⊕⊕⊝⊝ | — | ||
| 293 per 1000 | 246 per 1000 | |||||
| Below knee amputation | OR 1.53 | 40 | ⊕⊕⊝⊝ | — | ||
| 42 per 1000 | 62 per 1000 | |||||
| All cause mortality (timing not specified) | 10 participants died during the study. Of these, 3/5 were reported to have had a recent PE following postmortem, all in the placebo group | — | 40 | ⊕⊕⊝⊝ | — | |
| Adverse events (timing not specified) | — | — | — | — | — | No adverse events reported apart from above PE |
| Bleeding (timing not specified) | The incidence of postoperative bleeding was less than 10% in both treatment groups (exact figures were not reported) | — | 40 | ⊕⊕⊝⊝ | — | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence Low certainty: our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. | ||||||
| aWe downgraded by two steps due to serious imprecision (due to small sample and event sizes) and confidence intervals that included both benefit and harm. bWe downgraded by two steps due to serious imprecision (due to small sample and event sizes) and study limitations (data not reported separately by treatment arm). | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1.1 Deep vein thrombosis (DVT) Show forest plot | 1 | Odds Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 2.1 Pulmonary embolism Show forest plot | 1 | 134 | Odds Ratio (M‐H, Random, 95% CI) | 0.84 [0.35, 2.01] |
| 2.1.1 Above knee amputation | 1 | 94 | Odds Ratio (M‐H, Random, 95% CI) | 0.79 [0.31, 1.97] |
| 2.1.2 Below knee amputation | 1 | 40 | Odds Ratio (M‐H, Random, 95% CI) | 1.53 [0.09, 26.43] |