Schulische Kurzinterventionen und Verhaltens‐Endpunkte bei drogenkonsumierenden Jugendlichen
Abstract
Background
Adolescent substance use is a major problem in and of itself, and because it acts as a risk factor for other problem behaviours. As substance use during adolescence can lead to adverse and often long‐term health and social consequences, it is important to intervene early in order to prevent progression to more severe problems. Brief interventions have been shown to reduce problematic substance use among adolescents and are especially useful for individuals who have moderately risky patterns of substance use. Such interventions can be conducted in school settings. This review set out to evaluate the effectiveness of brief school‐based interventions for adolescent substance use.
Objectives
To evaluate the effectiveness of brief school‐based interventions in reducing substance use and other behavioural outcomes among adolescents compared to another intervention or assessment‐only conditions.
Search methods
We conducted the original literature search in March 2013 and performed the search update to February 2015. For both review stages (original and update), we searched 10 electronic databases and six websites on evidence‐based interventions, and the reference lists of included studies and reviews, from 1966 to February 2015. We also contacted authors and organisations to identify any additional studies.
Selection criteria
We included randomised controlled trials that evaluated the effects of brief school‐based interventions for substance‐using adolescents.
The primary outcomes were reduction or cessation of substance use. The secondary outcomes were engagement in criminal activity and engagement in delinquent or problem behaviours related to substance use.
Data collection and analysis
We used the standard methodological procedures outlined by The Cochrane Collaboration, including the GRADE approach for evaluating the quality of evidence.
Main results
We included six trials with 1176 adolescents that measured outcomes at different follow‐up periods in this review. Three studies with 732 adolescents compared brief interventions (Bls) with information provision only, and three studies with 444 adolescents compared Bls with assessment only. Reasons for downgrading the quality of evidence included risk of bias of the included studies, imprecision, and inconsistency. For outcomes that concern substance abuse, the retrieved studies only assessed alcohol and cannabis. We generally found moderate‐quality evidence that, compared to information provision only, BIs did not have a significant effect on any of the substance use outcomes at short‐, medium‐, or long‐term follow‐up. They also did not have a significant effect on delinquent‐type behaviour outcomes among adolescents. When compared to assessment‐only controls, we found low‐ or very low‐quality evidence that BIs reduced cannabis frequency at short‐term follow‐up in one study (standardised mean difference (SMD) ‐0.83; 95% confidence interval (CI) ‐1.14 to ‐0.53, n = 269). BIs also significantly reduced frequency of alcohol use (SMD ‐0.91; 95% CI ‐1.21 to ‐0.61, n = 242), alcohol abuse (SMD ‐0.38; 95% CI ‐0.7 to ‐0.07, n = 190) and dependence (SMD ‐0.58; 95% CI ‐0.9 to ‐0.26, n = 190), and cannabis abuse (SMD ‐0.34; 95% CI ‐0.65 to ‐0.02, n = 190) at medium‐term follow‐up in one study. At long‐term follow‐up, BIs also reduced alcohol abuse (SMD ‐0.72; 95% CI ‐1.05 to ‐0.40, n = 181), cannabis frequency (SMD ‐0.56; 95% CI ‐0.75 to ‐0.36, n = 181), abuse (SMD ‐0.62; 95% CI ‐0.95 to ‐0.29, n = 181), and dependence (SMD ‐0.96; 95% CI ‐1.30 to ‐0.63, n = 181) in one study. However, the evidence from studies that compared brief interventions to assessment‐only conditions was generally of low quality. Brief interventions also had mixed effects on adolescents' delinquent or problem behaviours, although the effect at long‐term follow‐up on these outcomes in the assessment‐only comparison was significant (SMD ‐0.78; 95% CI ‐1.11 to ‐0.45).
Authors' conclusions
We found low‐ or very low‐quality evidence that brief school‐based interventions may be more effective in reducing alcohol and cannabis use than the assessment‐only condition and that these reductions were sustained at long‐term follow‐up. We found moderate‐quality evidence that, when compared to information provision, brief interventions probably did not have a significant effect on substance use outcomes. It is premature to make definitive statements about the effectiveness of brief school‐based interventions for reducing adolescent substance use. Further high‐quality studies examining the relative effectiveness of BIs for substance use and other problem behaviours need to be conducted, particularly in low‐ and middle‐income countries.
PICOs
Laienverständliche Zusammenfassung
Können Kurzinterventionen, die in der Schule stattfinden, Drogenkonsum unter Jugendlichen reduzieren?
Fragestellung: Wir haben die Evidenz zur Wirkung von schulischen Kurzinterventionen auf Drogenkonsum und Problem‐Verhalten im Zusammenhang mit Drogen unter Jugendlichen erfasst. Wir fanden sechs Studien.
Hintergrund: Es ist bekannt, dass Jugendliche weltweit sowohl legale als auch illegale Drogen konsumieren, was zu weiteren Problemen führen kann. Die hohen Raten an Drogenkonsum sind beunruhigend, da ein früher Einstieg in den Drogenkonsum ein hoher Risikofaktor für konsumbedingte Störungen im späteren Leben ist, und Alkohol und illegale Drogen wurden bei jungen Menschen von 10 bis 24 Jahren mit verlorenen Lebensjahren aufgrund von Behinderungen assoziiert.
Wir wollten wissen ob schulische Kurzinterventionen eine Wirkung auf Drogenmissbrauch bei Jugendlichen haben. Kurzinterventionen sind kurze Gesprächsprogramme, die darauf abzielen den Drogenkonsum zu reduzieren oder zu beenden. Dieser Review ist die Aktualisierung eines Reviews, der 2014 veröffentlicht wurde.
Datum der Suche: Die Evidenz ist auf dem Stand von Februar 2015.
Studienmerkmale: Wir haben sechs Studien mit insgesamt 1176 Jugendlichen in diesen Review eingeschlossen. Das durchschnittliche Alter der Jugendlichen lag bei 16,9 Jahren. Wir waren interessiert an Studien mit kurzer, mittel‐ und langfristiger Nachbeobachtung, um zu ermitteln ob die Kurzintervention wirksam ist. Die Studien verglichen Kurzinterventionen hauptsächlich mit zwei Arten von Vergleichs‐ oder Kontrollgruppen: 1) eine Gruppe, die nur Informationsversorgung erhielt (allgemeine Materialien zur Gesundheitsförderung und Informationen zur Schadensminderung) und 2) eine Gruppe, die nur einer Begutachtung unterzogen wurde, bei der die Jugendlichen keine Maßnahmen erhielten, aber ihren Drogenkonsum und anderes Verhalten an Nachbeobachtungsterminen zu unterschiedlichen Zeitpunkten nach dem Vollzug der Maßnahme evaluiert wurde. Drei Studien mit insgesamt 732 Jugendlichen verglichen Kurzinterventionen mit reiner Informationsversorgung, während die drei anderen Studien mit insgesamt 444 Jugendlichen Kurzinterventionen mit reiner Begutachtung verglichen.
Die Studien waren entweder in den USA oder im Vereinigten Königreich durchgeführt worden.
Die Maßnahmen fanden vor Ort als persönliches Feedback mit einzelnen Personen oder Gruppen der Mittel‐ oder Oberstufe verschiedener Schulen statt. Alle Kurzinterventionen verliefen über bis zu vier Sitzungen.
Unser primärer Endpunkt war Abstinenz von oder Reduzierung des Drogenkonsums, und unsere sekundären Endpunkte waren das Betreiben krimineller Aktivitäten und straffälligen Verhaltens im Zusammenhang mit Drogenkonsum.
Hauptergebnisse: Für Endpunkte in Bezug auf Drogenkonsum bewerteten die Studien Alkohol‐ und Cannabiskonsum. Im Vergleich zur reinen Informationsversorgung sind Kurzinterventionen wahrscheinlich nicht wirksamer zur Reduzierung von Drogenkonsum oder straffälligem Verhalten. Im Vergleich zu den Begutachtungskontrollgruppen haben die Maßnahmen möglicherweise eine signifikante Wirkung auf Drogenkonsum und Verhalten. In einer Studie reduzierten Kurzinterventionen die Häufigkeit von Cannabiskonsum signifikant bei kurzer Nachbeobachtung. In einer Studie reduzierten Kurzinterventionen die Häufigkeit von Alkoholkonsum, Alkoholmissbrauch und ‐abhängigkeitssymptomen, sowie Cannabismissbrauchsymptome signifikant bei mittelfristiger Nachbeobachtung. In einer Studie reduzierten Kurzinterventionen Alkoholmissbrauch, die Häufigkeit von Cannabiskonsum, sowie Cannabismissbrauch und ‐abhängigkeitssymptome signifikant bei langfristiger Nachbeobachtung.
Das Muster der Ergebnisse deutet darauf hin, dass Jugendliche, die eine Kurzintervention erhielten, generell ihren Alkohol‐ und Cannabiskonsum eher reduzierten als Jugendliche, die gar keine Maßnahmen erhielten. Allerdings schienen Jugendliche, die eine Kurzintervention erhielten, generell ihren Alkohol‐ und Cannabiskonsum nicht wahrscheinlicher zu reduzieren als Jugendliche, die reine Informationsversorgung erhielten. Es ist daher verfrüht endgültige Aussagen über die Wirksamkeit von schulischen Kurzinterventionen zur Reduzierung von jugendlichem Drogenkonsum zu treffen.
Qualität der Evidenz: Insgesamt war die Evidenz von moderater oder niedriger Qualität, wobei für zwei Endpunkte eine sehr niedrige Qualität der Evidenz festgestellt wurde. Es gab drei große Probleme bei allen Studien: 1) die Jugendlichen wurden nicht verblindet, 2) es war nicht klar, ob die Zuteilung der Teilnehmer zu Studiengruppen verborgen war, und 3) eine kleine Gesamtzahl an Jugendlichen und Ereignissen. Keine der eingeschlossenen Studien berichtete Informationen zu Finanzierungsquellen oder Interessenkonflikten.
Authors' conclusions
Summary of findings
| Brief intervention compared to information provision for substance‐using adolescents | ||||||
| Patient or population: Substance‐using adolescents | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Estimate effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Information provision | Brief intervention | |||||
| Alcohol frequency | See comment | The standardised mean alcohol frequency in the intervention groups was 0.01 standard deviations lower | SMD ‐0.01 (‐0.20 to 0.18) | 434 | ⊕⊕⊕⊝ | Number of days of alcohol use |
| Alcohol quantity Medium‐term follow‐up: 4 to 6 months | See comment | The standardised mean alcohol quantity in the intervention groups was 0.14 standard deviations lower | SMD ‐0.14 (‐0.33 to 0.05) | 434 | ⊕⊕⊕⊝ | Number of standard alcohol units |
| Cannabis dependence | See comment | The standardised mean cannabis dependence score in the intervention groups was 0.09 standard deviations lower (0.27 lower to 0.09 higher) | SMD ‐0.09 (‐0.27 to 0.09) | 470 | ⊕⊕⊕⊝ | Mean dependence score |
| Cannabis frequency | See comment | The mean cannabis frequency in the intervention groups was | SMD ‐0.07 (‐0.25 to 0.11) | 470 | ⊕⊕⊕⊝ | Number of days cannabis use |
| Secondary outcomes related to substance use Short‐term follow‐up: 1 to 3 months | See comment | The mean behavioural outcomes related to substance use in the intervention groups was | SMD ‐0.01 (‐0.19 to 0.17) | 470 | ⊕⊕⊕⊝ | Interactional Problems Score |
| *The basis for the assumed risk (e.g. the mean control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the estimate effect of the intervention (and its 95% CI). The estimate effects for certain outcomes were not estimable due to only one study assessing the specific outcome, or extremely high levels of heterogeneity making effects across studies difficult to compare. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Risk of bias (‐1): It was not possible to blind the participants in all of the included studies. There was also uncertainty in two of the studies about allocation concealment and blinding of outcome assessor (Walker 2011; Werch 2005). | ||||||
| Brief intervention compared to assessment only for substance‐using adolescents | ||||||
| Patient or population: Substance‐using adolescents | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Estimate effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Assessment only | Brief intervention | |||||
| Alcohol frequency Self report questionnaires | See comment | The standardised mean alcohol frequency in the intervention groups was 0.91 standard deviations lower | SMD ‐0.91 (‐1.21 to ‐0.61) | 242 | ⊕⊕⊝⊝ | Number of days of alcohol use |
| Alcohol quantity Medium‐term follow‐up: 4 to 6 months | See comment | The standardised mean alcohol quantity in the intervention groups was 0.16 standard deviations lower | SMD ‐0.16 (‐0.45 to 0.14) | 179 (1 study) | ⊕⊕⊝⊝ | Number of standard alcohol units |
| Cannabis dependence | See comment | The mean cannabis dependence in the intervention groups was | SMD ‐0.26 (‐0.57 to 0.36) | 190 | ⊕⊕⊝⊝ | Mean dependence score |
| Cannabis frequency | See comment | The mean cannabis frequency in the intervention groups was | SMD ‐0.54 (‐0.77 to ‐0.31) | 338 | ⊕⊕⊝⊝ | Number of days of cannabis use |
| Secondary outcomes related to substance use Self report questionnaires Medium‐term follow‐up: 4 to 6 months | See comment | The mean mean behavioural outcomes related to substance use in the intervention groups was | SMD ‐0.65 (‐1.58 to 0.28) | 242 | ⊕⊕⊝⊝ | Interactional Problems Score |
| *The basis for the assumed risk (e.g. the mean control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the estimate effect of the intervention (and its 95% CI). The estimate effects for certain outcomes were not estimable due to only one study assessing the specific outcome, or extremely high levels of heterogeneity making effects across studies difficult to compare. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Risk of bias (‐1): It was not possible to blind the participants in all of the included studies. There was no allocation concealment in two of the included studies, and it was unclear whether the outcome assessor was blinded (Winters 2007b; Winters 2012). The other study was also not free of selective reporting bias (McCambridge 2004). | ||||||
Background
Description of the condition
Substance use among adolescents refers to the use of licit substances (including alcohol and prescription or over‐the‐counter medicines) and illicit drugs (cannabis, heroin, cocaine, amphetamines, methaqualone, hallucinogenic drugs). Globally, alcohol and cannabis (after tobacco) are the most commonly used substances among young people (Hingson 2006; UNODC 2012), and alcohol initiation is occurring at earlier ages, which is associated with substance dependence and other related problems later on in life (Hingson 2006). Middle and secondary or high school is an especially high‐risk period for the initiation of substance use as adolescents transition from one type of schooling to another and face numerous challenges (Jackson 2013). School surveys conducted in different regions of the world, such as Europe (Hibell 2012), Australia (White 2012), the United States (Johnston 2015), and South Africa (Reddy 2013), have reported a high prevalence of alcohol use among young people as well as high levels of other drug use. For example, a study of adolescent drug use across 35 European countries reported that 70% of students reported lifetime alcohol use (in some countries this was as high as 95%), while 18% had engaged in illicit drug use (Hibell 2012). An Australian school survey similarly indicated that 84% of students reported lifetime use of alcohol, 14.8% reported lifetime use of cannabis, and 17.3% reported lifetime inhalant use (White 2012). In the United States national Monitoring the Future survey, lifetime and past 30‐day use of alcohol was 46% and 23% respectively, while lifetime and past 30‐day use of cannabis was 31% and 14% respectively (Johnston 2015). In addition, the national Youth Risk Behavior Survey (YRBS) in the United States reported that the lifetime prevalences for alcohol, cannabis, prescription drugs, and inhalants were 66%, 41%, 28%, and 9% respectively (Kann 2013). The most recent South African national YRBS found lifetime prevalence rates of 49% for alcohol use, 13% for cannabis use, and 12% for inhalants or prescription drug use (Reddy 2013).
These high rates of substance use among adolescents are cause for concern, not only because the early initiation of substance use is a risk factor for substance use disorders in later life (Winters 2008), but also because of its association with increased morbidity and mortality among young people. For example, the most recent Global Burden of Disease study found that alcohol (7%) and illegal drugs (2%) were two of the main risk factors for incident disability‐adjusted life‐years for youth aged 10 to 24 years (Gore 2011).
It is important to intervene early with adolescents who use substances as substance use is often associated with a number of other problem behaviours including withdrawal from school involvement, drinking and driving, violent behaviour, and general delinquency. These kinds of behavioural outcomes have been consistently associated with adolescent substance use in studies throughout the world (Feldstein 2006; Hallfors 2006; Plüddemann 2010; Storr 2007). For example, the YRBS in the United States found that 10% of high school students had driven a car or vehicle after alcohol use in the past month (Kann 2013), while in South Africa, this was reported to be 13% (Reddy 2013). Studies also show that substance use can play a role in criminal behaviour. In a recent study, youth offenders reported that they committed crimes in order to finance their drug habit (Leoschut 2007). Some also reported that substance use gave them the courage to commit their crimes, or an excuse if they were apprehended. Ward 2007 also suggested that when young people are under the influence of substances they may not be able to monitor or self regulate their behaviour as well as when they are sober.
Adolescents who become involved with the legal system due to substance use are more likely to associate with deviant networks and be disadvantaged in terms of education and employment. They are also more likely to participate in criminal activity during adulthood (Mulvey 2010). Adolescents involved in the criminal justice system often have more psychiatric problems and are more in need of drug treatment in adulthood than their peers who are not involved in the criminal justice system (Kutcher 2009; Lanctôt 2007). For example, Corneau 2004 estimated that 12% of institutionalised adolescents need drug treatment as adults. Furthermore, substance‐using adolescents who are involved in the criminal justice system are more likely to have negative interpersonal relationships, including violent intimate partner relationships (Lanctôt 2007). If an intervention can take place early on with these adolescents, it may be able to prevent the development of some of these negative consequences.
Description of the intervention
Brief interventions (BIs)
Brief interventions (BIs) are targeted, time‐limited, low‐threshold services that aim to reduce substance use and its associated risks, as well as prevent progression to more severe levels of use and potential negative consequences (Babor 2007). In general, BIs are delivered in person and provide information or advice, increase motivation not to use substances, and teach behaviour change skills with the aim of reducing substance use. The way that BIs have been defined and delivered has varied in the literature in terms of number of sessions provided, length of the intervention sessions, and format of delivery (Young 2012). It is thus important to recognise common elements used to define BI. One such component is the screening of potential participants. Although screening has formed part of BIs in other settings, it often does not take place in schools, with a few exceptions (Hallfors 2006). A second common element of BIs is their short length, as they generally last between one and five intervention sessions (Moyer 2002; Tevyaw 2004).
In addition to advice‐giving, the common elements of successful BIs are referred to by the acronym FRAMES, and include provision of the following:
-
Feedback on behaviour and its consequences to the client;
-
Responsibility for change as the responsibility of the individual;
-
Advice for change;
-
Menu of options for change;
-
Empathy;
-
Self efficacy for change (Bien 1993).
These kinds of interventions were developed based upon the theoretical assumption that people are not always ready to change their patterns of substance use. In such cases, straightforward advice‐giving is of limited use, and the adolescents need to recognise for themselves that their behaviour is problematic and identify their own reasons for wanting to change their behaviour. The development of this brief method was guided by a number of principles: it should be useable in time‐limited consultations; the training of practitioners should take between 12 and 15 hours; interviewers should be able to raise the subject of behaviour change in a sensitive and respectful manner; and the method itself should be flexible, meaning that it can be used with individuals at various stages of readiness to change (Rollnick 1995). Most BIs rely on principles of motivational interviewing, in Winters 2007a, or brief motivational enhancement therapy, in Tevyaw 2004, which focus on building adolescents' readiness to change their behaviours. This technique provides personalised feedback on substance use together with a motivational‐interviewing counselling style (Miller 2002).
Relevance for adolescents
BIs have been identified as useful for individuals who have moderately risky patterns of substance use (Barry 1999). This makes this type of intervention relevant for use with adolescents, who for the most part have not yet developed substance dependence. BIs seem to be better suited for those adolescents who are less set in a delinquent lifestyle and who are not institutionalised (Brunelle 2000). Tevyaw 2004 characterises BI methods as accepting adolescents as individuals, instead of confronting them and their behaviour or lecturing them as their teachers, parents, and other authority figures may do. BIs could therefore be a more effective strategy for building rapport and a collaborative therapeutic relationship with adolescents than other confrontational forms of interacting with adolescents. Furthermore, the methods are seen as a cost‐effective alternative to traditional, lengthier treatments of adolescents who use substances (Tevyaw 2004).
Ideal conditions: what we do and do not know
BIs have traditionally been used in healthcare and substance abuse treatment settings (Bien 1993), but studies have suggested that their use could be expanded to other settings, such as schools (Winters 2007a). There are a number of advantages of school‐based BIs for substance‐using adolescents. Firstly, adolescents usually are not dependent on substances yet, although a number of them may exhibit mild or moderate use, which makes them good candidates for BI. Secondly, research has shown that BIs can be conducted during school or after‐school hours, making the intervention very accessible to students. Finally, the growing volume of BI material on how to conduct BI sessions means that they can often be run by staff available to schools, and not just health professionals (Winters 2007a). There is also some research suggesting that BIs may work in other settings as well, such as family interventions for school‐going adolescents in terms of alcohol and cannabis use (Spoth 2001). Recent research has also suggested that web‐based BI programmes may be useful in reducing substance use in young adults (Bingham 2010). Despite the promise of school‐based BI programmes, meta‐analyses of school‐based interventions have not yet been conducted.
How the intervention might work
The goals of BIs are to assess substance use in adolescents, provide advice on these behaviours, facilitate behaviour change with regards to substance use, and motivate the adolescents to receive further treatment if necessary (Bien 1993). The primary focus of these types of interventions is to systematically target problematic behaviours (Tevyaw 2004), using a motivational‐interviewing framework.
The theoretical basis for BIs is grounded in client‐centred therapy, behavioural therapy, and the transtheoretical model of behaviour change. The transtheoretical model of behaviour change argues that readiness for change develops along a series of stages rather than as a fixed event that either occurs or does not occur. These steps are pre‐contemplation, contemplation, preparation, action, and maintenance, and individuals usually move between these stages before reaching termination (Prochaska 1993). From this perspective, motivation is seen as a state that can be altered rather than a trait that is inherent and cannot be changed. Since BIs are typically organised around a developmental theory of normative and non‐normative patterns of substance use, this is an appropriate theoretical orientation for a behaviour change strategy aimed at adolescents (Winters 2007a).
Why it is important to do this review
Brief interventions are recognised as an appropriate treatment for adolescents who use substances, yet there have been only a few reviews of the effectiveness of BI for adolescent substance use. Tait 2003 conducted a systematic review of 11 studies of BIs for adolescent substance use and found that BI was effective in reducing alcohol use among adolescents, but not in reducing polysubstance use. Only two of these studies were conducted in schools (with one conducted by nurses over the telephone); these two studies showed moderate effect sizes of between 0.38 and 0.52. BIs also did not have a significant effect on drinking in the last seven days. In their review of brief motivational interventions among adolescents, Tevyaw 2004 reported significant reductions in alcohol‐related problems such as drinking and driving, traffic violations and, to a lesser extent, drinking rates. While the reviewed studies were conducted in a number of settings, including emergency rooms and colleges, not many of these settings were high schools. Furthermore, existing reviews were conducted a number of years ago and have not been updated. It is useful to re‐examine the evidence in an updated review.
No existing Cochrane reviews examine the effectiveness of BIs for reducing substance use among high school (or the equivalent of high school) students, while a recent systematic review that addressed alcohol use among adolescents only included two studies conducted in a high school setting. These results were inconclusive, as in one study the BI was effective, but in the other it was ineffective (Patton 2014). Furthermore, there are no reviews that address BIs for substance use as a primary outcome and related behavioural outcomes (for example problem behaviours) as secondary outcomes. The current review is the first to examine both outcomes.
Objectives
To evaluate the effectiveness of brief school‐based interventions in comparison to another intervention or assessment only on reducing substance use and related behavioural outcomes among adolescents.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials that evaluated the effects of BIs on substance use as well as on behavioural outcomes associated with adolescent substance use. We excluded studies that recruited adolescents from anywhere else other than an educational setting.
Types of participants
Participants were adolescents under the age of 19 who were attending high school, secondary school, or a further education training college that provided alternative schooling or vocational training for adolescents between 16 and 18 years of age, and who used alcohol or other drugs, or both, but did not meet the criteria for substance dependence. In addition, adolescents had faced negative behavioural consequences due to their substance use.
Types of interventions
Experimental intervention
The intervention should have been labelled as a BI, but could also have been defined as motivational interviewing, brief skills‐orientation, motivational enhancement, or other specific types of BIs that were up to four sessions long and used BI principles to facilitate change. The focus should have been on building the individual's motivation to change. The BIs could have been offered as a stand‐alone option, integrated with other intervention efforts, or as a precursor to other treatments. Only BIs that were offered to individuals in a face‐to‐face modality were included in this review.
Control intervention
The control could have been no intervention, placebo, assessment only, or other types of interventions or education.
Types of outcome measures
Primary outcomes
-
Abstinence or reduction of substance use behaviour.
The outcome measures could have been self reported measures, including dichotomous and continuous outcomes. In addition, substance use could have been measured with standardised measures of substance use that are appropriate for adolescents such as the Alcohol Diagostic Interview (ADI), Adolescent Drug Abuse Diagnosis (ADAD), Adolescent Drug Involvement Scale (ADIS), Adolescent Alcohol and Drug Involvement Scale (AADIS), and Personal Experience Inventory (PEI), which are all self report measures.
Any biological testing could also have been included, such as urinalysis for drug use and breathalyser tests for alcohol use.
Secondary outcomes
-
Engagement in criminal activity (such as theft, drug and alcohol crimes, property crimes) related to substance use.
-
Engagement in delinquent‐type behaviours (such as drinking and driving, aggression and fighting, bullying, carrying weapons to school, buying and selling drugs, gang involvement, truancy, suspension and expulsion, and disobeying rules in general) related to substance use.
It was not expected that the included BIs would have adverse effects on the primary or secondary outcomes.
Search methods for identification of studies
Included studies were published from 1966 onwards, the year that BIs were first introduced.
Electronic searches
We obtained relevant trials from searching the following sources:
-
CDAG Specialized Register (February 2015);
-
Cochrane Central Register of Controlled Trials (CENTRAL in the Cochrane Library, issue 2, 2015);
-
PubMed (January 1966 to February 2015);
-
EMBASE (1974 to March 2013);
-
PsycINFO (January 1966 to February 2015);
-
ERIC (Education Resources Information Center) (January 1966 to February 2015);
-
ISAP (Index to South African Periodicals), Social Science Index (January 1966 to February 2015);
-
Academic Search Premier (January 1966 to March 2013);
-
LILACS (2004 to March 2013);
-
Alcohol and Alcohol Problems Science Database (1972 to March 2013);
-
Web of Science Social Science Citation Index (January 1966 to March 2013).
We developed a detailed search strategy for each database. The search strategy combined the subject search with the Cochrane Highly Sensitive Search Strategy (CHSSS) for identifying randomised trials in PubMed, sensitivity maximising version (2008 revision), as referenced in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
The subject search utilised a combination of controlled vocabulary and free text terms based on the strategy for searching PubMed. We adapted this search strategy as appropriate for the other databases (see Appendix 1; Appendix 2; Appendix 3; Appendix 4; Appendix 5; Appendix 6; Appendix 7 for all searches). We applied no language restrictions.
Searching other resources
We contacted relevant authors and searched citations in all relevant papers to obtain information on potential additional randomised controlled trials. We also searched for other unpublished studies and assessed relevant conference proceedings for additional references. We searched the following websites:
-
http://nrepp.samhsa.gov/
-
http://sbirt.samhsa.gov/core_comp/brief_int.htm
-
http://motivationalinterview.org
-
Current Controlled Trials (http://www.controlled‐trials.com/)
-
ClinicalTrials.gov
-
Trialsjournal.com
Data collection and analysis
Selection of studies
Two review authors (TC and BM) assessed the title, abstract, and keywords of all the papers from the electronic searches against the eligibility criteria for this review, and retrieved the full texts of studies deemed potentially eligible. These included randomised controlled trial or clinical trials and substance use, alcohol use, drug use (and related terms), alcohol or drug use or substance use reduction strategies (and related terms), problem behaviours (including but not limited to aggression, fighting, suspension, expulsion, weapon‐carrying), interventions, school staff or settings or both (and related terms). If the title, abstract, and keywords did not provide enough information to make an informed decision with regards to inclusion of the paper, the full text of the paper was obtained.
Two review authors (TC and BM) assessed the full texts of potentially relevant studies for inclusion. A third review author (JL) was on hand to resolve any disagreements, however there were no disagreements about the inclusion of studies.
Data extraction and management
Two review authors (TC and BM) independently extracted data using a piloted data extraction form based on the Cochrane Collaborative Drugs and Alcohol Review Group's extraction form and subsequently entered the data into The Cochrane Collaboration software Review Manager 5.1 for analysis (the data extraction form is available on request from TC) (RevMan 2014). We extracted data from studies on the following information: study design and method, allocation process, participant data, intervention, and outcomes. When information was missing from the original studies on outcomes or other important information, we contacted the corresponding author via e‐mail in order to request additional data. Certain statistics were not readily available in the articles; if authors were not able to provide this information to us we calculated them from existing data, consulting the Cochrane Handbook for Systematic Reviews of Interventions for guidance (Higgins 2011).
Assessment of risk of bias in included studies
Two review authors independently assessed potential biases resulting from the trial design. Any discrepancies between the review authors were resolved by discussion.
We performed the 'Risk of bias' assessment for trials included in this review using the criteria recommended by the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). The recommended approach for assessing risk of bias in studies included in a Cochrane review is a two‐part tool addressing seven specific domains, namely sequence generation and allocation concealment (selection bias), blinding of participants and providers (performance bias), blinding of outcome assessor (detection bias), incomplete outcome data (attrition bias), selective outcome reporting (reporting bias), and other source of bias. The first part of the tool involves describing what was reported to have happened in the study. The second part of the tool involves assigning a judgement relating to the risk of bias for that entry, in terms of low, high, or unclear risk. To make these judgments we used the criteria indicated by the Cochrane Handbook for Systematic Reviews of Interventions adapted to the addiction field.
If the first two review authors struggled to make a judgement, we contacted the author of the article in an attempt to obtain more information about the particular bias domain, and only if it was still unclear did we assign it a judgement of 'unclear'.
For other domains, we examined the following:
-
appropriateness of the statistical tests used in data analysis;
-
compliance with the intervention(s);
-
validity and reliability of outcome measures.
For a detailed description of the criteria used to assess risk of bias, please see Appendix 8.
Grading of evidence
We assessed the overall quality of the evidence for the primary outcome using the Grading of Recommendation, Assessment, Development and Evaluation (GRADE) system. The Grading of Recommendation, Assessment, Development and Evaluation Working Group developed a system for grading the quality of evidence that takes into account issues not only related to internal validity but also to external validity, such as directness of results (GRADE 2004; Guyatt 2008; Guyatt 2011; Schünemann 2006). The 'Summary of findings' tables present the main findings of a review in a transparent and simple tabular format. In particular, they provide key information concerning the quality of evidence, the magnitude of effect of the interventions examined, and the sum of available data on the main outcomes.
The GRADE system uses the following criteria for assigning grades of evidence:
-
High: further research is very unlikely to change our confidence in the estimate of effect.
-
Moderate: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
-
Low: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
-
Very low: any estimate of effect is very uncertain.
Grading is decreased for the following reasons:
-
Serious (‐1) or very serious (‐2) limitation to study quality.
-
Important inconsistency (‐1).
-
Some (‐1) or major (‐2) uncertainty about directness.
-
Imprecise or sparse data (‐1).
-
High probability of reporting bias (‐1).
Grading is increased for the following reasons:
-
Strong evidence of association ‐ significant risk ratio of > 2 (0.5) based on consistent evidence from two or more observational studies, with no plausible confounders (+1).
-
Very strong evidence of association ‐ significant risk ratio of > 2 (< 0.5) based on direct evidence with no major threats to validity (+2).
-
Evidence of a dose response gradient (+1).
-
All plausible confounders would have reduced the effect (+1).
Measures of treatment effect
We compared the outcomes of the experimental and control groups at different follow‐up appointments. We categorised the findings into short‐term follow‐up appointments (one to three months), medium‐term follow‐up appointments (four to 11 months), and long‐term follow‐up appointments (12 months and longer). We assessed dichotomous outcome measures by calculating the risk ratio with the 95% confidence interval, while for continuous outcome measures the standardised mean difference with 95% confidence interval was the treatment measure used as the summary statistic. It is common in meta‐analysis for studies assess the same outcome but measure it in a variety of ways, so the same outcome may be measured with different scales (Higgins 2011). If standard deviations for the mean values were not provided, we used the standard errors that were provided and employed the calculation in the Cochrane Handbook for Systematic Reviews of Interventions to change them to standard deviations (Higgins 2011).
Unit of analysis issues
The analysis of clinical trials needs to take into account the level at which randomisation occurred. While this can be on an individual basis, cluster‐randomised trials have groups of individuals (for example schools, community) as opposed to individuals as the unit of analysis. The review authors originally planned to measure the intracluster correlation coefficient (ICC) in these studies and then use the ICC to measure the design effect, which is an inflation factor that is used to increase the statistical power of the study (Campbell 2000). However, as the authors of the cluster‐randomised trials used the Huber‐White estimator of variance to control for the effects of clustered recruitment, further calculations were not necessary. While the review authors had decided to use a conversion rate of 4.29 (30 days/7) where outcomes across studies used different measurement times other than monthly frequency, doing any additional conversions was unnecessary as the measures in the studies were of monthly use (for example frequency of use, quantity of use).
Dealing with missing data
We contacted the original investigators of the included studies up to three times to request any missing data (missing studies, outcomes, summary data, individuals, and study‐level characteristics). We needed to decide whether the data were missing at random (not related to the actual data) or not missing at random (related to the actual data). When study data were assumed to be missing at random, only the available data were analysed. For data that were not missing at random, this needed to be addressed by performing a sensitivity analysis or, if this was not possible, by replacing missing data with specified values (Higgins 2011). The imputation of missing data with specific replacement values was not needed for the studies included in this review.
Assessment of heterogeneity
We assessed the extent of heterogeneity across the studies using the Chi² test and I² statistic and looking at whether the P values were statistically significant (Higgins 2011), with a P value of 0.10 or less showing significant heterogeneity.
Assessment of reporting biases
We planned to use funnel plots (plots of the effect estimate from each study against the sample size or effect standard error) in an attempt to assess any publication bias. More specifically, we planned to examine the funnel plots for asymmetry as an indication of publication bias. However, asymmetrical funnel plots are not always caused by publication bias, and publication bias does not always cause asymmetrical funnel plots (Higgins 2011). This was not possible for the current review because fewer than 10 studies were included.
Data synthesis
We performed a meta‐analysis was performed, as there were more than two individual trials with comparable intervention methods and outcomes that could be analysed. We used random‐effects models based on the fact that we expected different types of interventions to be included in the review and combined in the meta‐analysis (such as interventions of different duration and using different follow‐up measures).
Subgroup analysis and investigation of heterogeneity
Although we originally had planned to conduct subgroup analyses for studies with low and unclear risk of bias and, if possible, for different ages, gender, and school grades for adolescent study participants, this was not possible. Only a small number of studies were included in the meta‐analysis, and the results were not reported by these variables of interest.
Sensitivity analysis
We decided that if there was significant unexplained heterogeneity and more than 10 studies were included in the analysis, we would perform a sensitivity analysis to consider if the following had an impact on effect size:
-
studies conducted in settings other than traditional high or secondary schools (e.g. alternative high schools, reform school);
-
studies that utilised quasi‐experimental designs (as long as an experimental and a control group were included);
-
studies that had attrition rates of more than 20%.
Since we included only six studies in the review, these sensitivity analyses were unnecessary.
Results
Description of studies
See Characteristics of included studies; Characteristics of excluded studies.
Results of the search
This is an update of a Cochrane review first published in February 2014. In the first edition of this review, we identified through bibliographic searches 1037 potentially relevant articles after removing duplicates. We excluded 1010 studies on the basis of title and abstract, and retrieved 27 articles in full text for more detailed evaluation. We excluded 21 of these; the remaining six trials (in eight articles) satisfied all the criteria for inclusion in the review (see Figure 1 for flowchart).
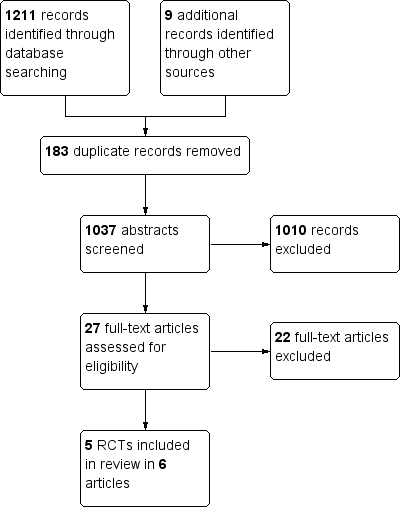
In the present update, we identified an additional 1264 records, giving us a total of 939 reports after removing 325 duplicates. We excluded 910 of these reports on the basis of title and abstract. We retrieved 29 articles in full text for more detailed evaluation, of which we excluded 28. We included no new trials in the review, although we included one additional article that reported on the long‐term follow‐up of one trial (See Figure 2). We have summarised the reasons for exclusion in the Characteristics of excluded studies table. The six randomised controlled trials (RCTs) from the original review (reported in eight separate articles) met our inclusion criteria and are described in detail in the Characteristics of included studies table.

Study flow diagram for updated review.
Included studies
We identified six studies (reported in eight articles) that were published between 2004 and February 2015 for inclusion in this review. These studies at their start included a total of 1176 adolescents. The total number of adolescents that were analysed at the follow‐up appointments varied according to the length of follow‐up period of the studies (short‐term follow‐up: n = 470; medium‐term follow‐up: n = 855; long‐term follow‐up: n = 529). All six studies were RCTs, of which two were cluster‐RCTs (McCambridge 2004; McCambridge 2008). All interventions were provided on a face‐to‐face individual basis.
Four out of the six studies included only adolescents engaging in cannabis or alcohol use or abuse, whereas the other two studies included adolescents engaging in any form of substance abuse.
Types of comparison
-
Brief intervention versus information provision, three studies, 732 adolescents at baseline (McCambridge 2008; Walker 2011; Werch 2005).
-
Brief intervention versus assessment only, three studies, 444 adolescents at baseline (McCambridge 2004; Winters 2007b; Winters 2012).
Location
All of the studies were based in educational settings. Four were based in public secondary schools (Walker 2011; Werch 2005; Winters 2007b; Winters 2012), while two were based in further education colleges, which provided alternative schooling and training for adolescents 16 to 18 years of age (McCambridge 2004; McCambridge 2008). The former four studies were conducted in the United States (Walker 2011; Werch 2005; Winters 2007b; Winters 2012), while the latter two studies were conducted in the United Kingdom (McCambridge 2004; McCambridge 2008).
Length and description of intervention
The six interventions met the criteria for brief interventions (BIs). Adolescents received some or all of the following: screening, motivational interviewing, information provision and discussion, brochures, and follow‐up appointments. Three of the studies provided adolescents with a single BI session (McCambridge 2004; McCambridge 2008; Werch 2005), while the other three studies held two intervention sessions with the adolescents (Walker 2011; Winters 2007b; Winters 2012).
Screening and outcomes measures
All six of the studies used self report measures. To measure substance abuse some studies used established screening and diagnostic tools such as the Global Appraisal of Individual Needs Interview (GAIN‐I) (Walker 2011), Alcohol Use Disorders Identification Test (AUDIT) (McCambridge 2004; McCambridge 2008), Timeline Followback (TLFB) interview (Winters 2007b; Winters 2012), Severity of Dependence Scale (SDS) (McCambridge 2008), and Substance Use Disorder Manual of the Adolescent Diagnostic Interview (ADI) (Winters 2007b; Winters 2012). Other studies used substance use questionnaires such as the Alcohol Beverage Youth Survey (Werch 2005). A combination of instruments was also used to measure alcohol behaviours. There was consistency regarding the measures of alcohol and cannabis frequency (number of days used) and quantity (number of units used). The Fagerström Test was also used in one study to measure nicotine dependence (McCambridge 2008).
Measures of behavioural outcomes were less clear and seemed to ask about the general consequences of the adolescents' drug use. McCambridge 2008 used a measure that assessed interactional problems, and was adapted from its original use for adolescents who had alcohol problems to include those who used drugs. Walker 2011 used the Marijuana Problem Inventory to measure problem behaviours associated with cannabis use. Two of the other studies used the Personal Consequences Scale, which measured legal, health, motor vehicle, social, and family problems experienced due to substance use (Winters 2007b; Winters 2012).
Length of follow‐up
The trials differed in terms of outcomes measured at follow‐up. While some of the trials conducted short‐term follow‐up appointments, such as McCambridge 2004, McCambridge 2008, and Walker 2011 at three months, they also conducted medium‐ and longer‐term follow‐ups. McCambridge 2008 also conducted six‐month follow‐up appointments, while Walker 2011 also conducted 12‐month follow‐ups. Two trials only reported one medium‐term follow‐up, at four months (Werch 2005), and six months (Winters 2007b), respectively. The remaining study reported outcomes at both six months and 12 months (Winters 2012).
Secondary population group
Two of the trials reported a secondary population group, namely the parents of the adolescents who used substances (Winters 2007b; Winters 2012). This made up a third experimental group, where both adolescents and parents received the intervention. While we considered these secondary population groups to be important, we did not compare them in the meta‐analysis, as the four other studies only had one experimental group with adolescents as the population, and no other interventions that worked with parents. However, we have written up these findings in the text of the review.
Excluded studies
We excluded 29 potentially eligible studies that were obtained and read in full. We excluded three of these studies because the length of the interventions did not fit the criteria for brief intervention, while another seven were prevention studies and not early‐intervention studies. Ten of the studies were not school based; they were either based at college level or in the community. Finally, we excluded some studies for methodological reasons, such as being pilot/feasibility studies and having no control group, not being RCTs, or not containing any information about interventions.
Risk of bias in included studies
Figure 3 provides a summary of the 'Risk of bias' assessments for all the studies. Figure 4 provides a summary of the risk of bias for each study and in each area.
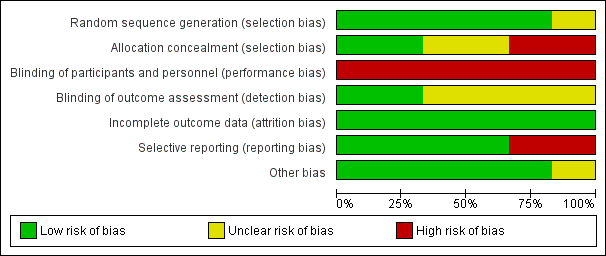
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Generation of randomisation sequence
We judged sequence generation as adequate in all but one of the studies (Werch 2005), which referred to random allocation, but this was not clarified and we were not able to contact the authors for further information. We therefore found the level of bias for this study to be unclear.
Concealment of allocation
Concealment of allocation was adequate in two of the studies (McCambridge 2004; McCambridge 2008). It was unclear in two of the studies (Walker 2011; Werch 2005), and once again contacting the authors proved unsuccessful. In the remaining two studies, allocation concealment did not take place (Winters 2007b; Winters 2012). Communication with the authors revealed that this was not done because it was believed that it would negatively affect study participation, so we judged these two studies to be at high risk of selection bias.
Blinding
Performance bias
This review reports on psychological interventions such as motivational interviewing, where it was not possible to blind the participants or staff who worked on the study to the intervention. The risk of performance bias can actually influence the outcomes if they are self reported and not objective. Because all the six included studies used self‐report measures, all the studies were judges at high risk of performance bias.
Detection bias
Outcome assessors were blinded to study condition in two of the studies (McCambridge 2004; McCambridge 2008). In four studies there was insufficient information to evaluate the risk of bias in terms of blinding (Walker 2011; Werch 2005; Winters 2007b; Winters 2012), and we could not contact the authors.
Incomplete outcome data
We reported all six of the studies to have low risk of bias because either the rates of attrition were low, or factors associated with attrition were identified and controlled for in both groups in the original analysis.
Selective reporting
Four of the studies were free of selective reporting, and reported on all prespecified outcomes (McCambridge 2008; Walker 2011; Winters 2007b; Winters 2012). One of the trials did not report on all longer‐term outcomes as the findings were no longer significant (McCambridge 2004), and the sixth study did not report all outcomes (Werch 2005), so we judged these two studies to be at high risk of selective reporting.
Other potential sources of bias
We identified no other sources of bias (appropriateness of statistical tests used in data analysis; compliance with the intervention(s); validity and reliability of outcome measures).
Effects of interventions
See: Summary of findings for the main comparison Brief intervention compared to information provision for substance‐using adolescents; Summary of findings 2 Brief intervention compared to assessment only for substance‐using adolescents
Due to high levels of heterogeneity, we could not combine the effects across studies for some of the outcomes. While a meta‐analysis of results across one study was not possible (see summary of findings Table for the main comparison; summary of findings Table 2), we have reported the effect of the intervention compared to the control group below.
1. Comparison of BI to information provision
Primary outcomes
See summary of findings Table for the main comparison
Alcohol frequency: Two studies measured alcohol frequency at different follow‐up periods. One study measured alcohol frequency at both short‐ and medium‐term follow‐ up (McCambridge 2008), while the other measured alcohol frequency only at medium‐term follow‐up (Werch 2005). There were a total of 269 adolescents at short‐term follow‐up and 434 adolescents at medium‐term follow‐up. We found no significant difference between BI and information provision for both of the follow‐up periods, with a standardised mean difference (SMD) of ‐0.05 (95% confidence interval (CI) ‐0.29 to 0.19) at short‐term follow‐up (one study) and SMD of ‐0.01 (95% CI ‐0.20 to 0.18) I² = 0%, Chi² = 0.34, P = 0.56, at medium‐term follow‐up (two studies). See Analysis 1.1.
Alcohol quantity: Two studies measured alcohol quantity at different follow‐up periods. McCambridge 2008 measured alcohol quantity at both short‐ and medium‐term follow‐up. Werch 2005 measured alcohol frequency only at medium‐term follow‐up. There were a total of 269 adolescents at short‐term follow‐up and 434 adolescents at medium‐term follow‐up. We found no significant difference in both of the follow‐up periods, with SMD of 0.02 (95% CI ‐0.22 to 0.26) at short‐term follow‐up (one study) and SMD of ‐0.14 (95% CI ‐0.33 to 0.05) Chi² = 0.62, P = 0.43, I² = 0%, at medium‐term follow‐up (two studies).
Cannabis quantity: One study with 269 adolescents at short‐term follow‐up and 264 adolescents at medium‐term follow‐up reported on quantity of cannabis use (McCambridge 2008). The SMD was ‐0.00 (95% CI ‐0.24 to 0.24) at short‐term follow‐up and ‐0.15 (95% CI ‐0.39 to 0.09) at medium‐term follow‐up. See Analysis 1.3.
Cannabis dependence: Two studies reported on cannabis dependence (McCambridge 2008; Walker 2011). Both studies reported on this outcome at short‐term follow‐up (n = 470). The SMD was ‐0.09, which was not significant (95% CI ‐0.27 to 0.09). There was no heterogeneity (Chi² = 0.45, P = 0.50, I² = 0%). Only one of the studies reported this outcome at medium‐term follow‐up (n = 264) (McCambridge 2008), and the SMD was 0.06 (95% CI ‐0.18 to 0.30). Walker 2011 also measured cannabis dependence at long‐term follow‐up appointments (n = 186). The SMD was ‐0.09 (95% CI ‐0.38 to 0.20). See Analysis 1.4.
Cannabis frequency: Two studies reported on cannabis frequency (McCambridge 2008; Walker 2011). Both reported on this outcome at short‐term follow‐up (n = 470). The SMD was ‐0.07, which was not significant (95% CI ‐0.25 to 0.11) Chi² = 0.43, P = 0.51, I² = 0%. McCambridge 2008 also reported cannabis frequency at medium‐term follow‐up (n = 264), and the SMD was ‐0.06 (95% CI ‐0.30 to 0.18). Walker 2011 also measured cannabis frequency at long‐term follow‐up appointments (n = 186). The SMD was ‐0.02 (95% CI ‐0.31 to 0.26). See Analysis 1.5.
Secondary outcomes
The information pooled in the meta‐analysis for the secondary outcomes included engagement in criminal activity and delinquent‐type behaviours associated with alcohol or cannabis use, or both, such as drug selling, drug‐related crime, and arrests for being intoxicated. Two studies reported on our secondary outcomes at different follow‐up periods (McCambridge 2008; Walker 2011). Both studies reported on our secondary outcomes at short‐term follow‐up (n = 470) (McCambridge 2008; Walker 2011). The SMD was ‐0.01 (95% CI ‐0.19 to 0.17) Chi² = 0.23, P = 0.63, I² = 0%. McCambridge 2008 reported on our secondary outcomes at medium‐term follow‐up (n = 264). The SMD was ‐0.13 (95% CI ‐0.37 to 0.11). Walker 2011 reported on our secondary outcomes at long‐term follow‐up (n = 186); the SMD was ‐0.10 (95% CI ‐0.39 to 0.19). See Analysis 1.6.
2. Comparison of BI to assessment only
Primary outcomes
See summary of findings Table 2
Alcohol frequency: Two studies measured alcohol frequency (Winters 2007b; Winters 2012). At medium‐term follow‐up for these studies with 242 adolescents in total, there was a significant difference in favour of BI: SMD ‐0.91 (95% CI ‐1.21 to ‐0.61), with very little heterogeneity (I² = 5%, Chi² = 1.06, P = 0.30). Only the Winters 2012 study measured alcohol frequency at long‐term follow‐up (n = 170), but the SMD was ‐0.20, which was not significant (95% CI ‐0.53 to 0.14). See Analysis 2.1.
Alcohol quantity: One study with 179 adolescents at medium‐term follow‐up and 162 adolescents at long‐term follow‐up measured alcohol quantity (McCambridge 2004). At medium‐term follow‐up, there was not a significant difference between the group that received the intervention and the group that received an assessment only (SMD ‐0.16; 95% CI ‐0.45 to 0.14). At long‐term follow‐up, this difference was also not significant (SMD ‐0.16; 95% CI ‐0.47 to 0.15). See Analysis 2.2.
Alcohol abuse:Winters 2012 reported the number of alcohol abuse symptoms among 190 adolescents at medium‐term follow‐up and 170 adolescents at long‐term follow‐up. There were significant differences in favour of BI at both medium‐term (SMD ‐0.38, 95% CI ‐0.70 to ‐0.07) and long‐term follow‐up (SMD ‐0.72, 95% CI ‐1.07 to ‐0.38). See Analysis 2.3.
Alcohol dependence: Only one study reported the number of alcohol dependence symptoms (Winters 2012), among 190 adolescents at medium‐term follow‐up and 170 adolescents at long‐term follow‐up. While the difference was significant at medium‐term follow‐up (SMD ‐0.58, 95% CI ‐0.90 to ‐0.26) in favour of BI, it was not significant at long‐term follow‐up (SMD ‐0.13, 95% CI ‐0.47 to ‐0.20). See Analysis 2.4.
Cannabis frequency: Three studies reported on cannabis frequency (McCambridge 2004; Winters 2007b; Winters 2012). Only McCambridge 2004 measured cannabis frequency at short‐term follow‐up (n = 179), and the SMD was ‐0.83, which was significant (95% CI ‐1.14 to ‐0.53) in favour of BI. Both Winters 2007b and Winters 2012 measured cannabis frequency at medium‐term follow‐up (n = 242), but the difference was not significant (SMD ‐0.23, 95% CI ‐0.50 to 0.05) Chi² = 0.56, P = 0.45, I² = 0%. McCambridge 2004 and Winters 2012 measured this outcome at long‐term follow‐up (n = 338), and the difference was significant in favour of BI (SMD ‐0.54, 95% CI ‐0.77 to ‐0.31) Chi² = 0.12, P = 0.73, I² = 0%. See Analysis 2.5.
Cannabis abuse:Winters 2012 reported the number of cannabis abuse symptoms among 190 adolescents at medium‐term follow‐up and 170 adolescents at long‐term follow‐up. The differences were significant at both medium‐term (SMD ‐0.34, 95% CI ‐0.65 to ‐0.02) and long‐term follow‐up (SMD ‐0.62, 95% CI ‐0.96 to ‐0.28) in favour of BI. See Analysis 2.6.
Cannabis dependence: Only one study reported the number of alcohol dependence symptoms (Winters 2012), among 190 adolescents at medium‐term follow‐up and 170 adolescents at long‐term follow‐up. While the difference was not significant at medium‐term follow‐up (SMD ‐0.26, 95% CI ‐0.57 to 0.06), it was significant at long‐term follow‐up (SMD ‐0.96, 95% CI ‐1.32 to ‐0.62) in favour of BI. See Analysis 2.7.
Secondary outcomes
Two studies with a total of 242 adolescents at medium‐term follow‐up and a total of 170 adolescents at long‐term follow‐up measured engagement in delinquent‐type behaviours or engagement in criminal activity, which were secondary outcomes for this review (Winters 2007b; Winters 2012). There were not significant differences at medium‐term follow‐up (SMD ‐0.65, 95% CI ‐1.58 to 0.28) Chi² = 7.75, P = 0.005, I² = 87%, but there was a significant difference at long‐term follow‐up in Winters 2012 (SMD ‐0.78, 95% CI ‐1.13 to ‐0.44) in favour of BI. See Analysis 2.8.
McCambridge 2004 reported on these behaviours using dichotomous outcomes. At medium‐term follow‐up, adolescents in the control group were found to be almost twice as likely to have sold drugs to friends (risk ratio 0.38, 95% CI 0.23 to 0.66). This outcome was not reported at long‐term follow‐up.
Discussion
Summary of main results
We were interested in assessing whether brief intervention (BI) is more effective than assessment only or information provision in reducing alcohol and other drug use. We found low‐ or very low‐quality evidence that, compared to an assessment‐only control, BI may have an effect on the following alcohol outcomes: reduction of alcohol frequency at medium‐term follow‐up, alcohol abuse at medium‐ and long‐term follow‐up, and alcohol dependence at medium‐term follow‐up. In terms of outcomes related to cannabis use, BI may reduce cannabis frequency of use and cannabis abuse at both short‐ and medium‐term follow‐up, and on cannabis dependence at long‐term follow‐up. When comparing BI to the information‐only control, we found moderate‐quality evidence that the effects were generally not significant.
BIs did not change engagement in delinquent‐type behaviours or criminal activity for the experimental groups in comparison to both control comparisons (namely information provision and assessment only), except in the Winters 2012 study, which indicated that the intervention had a significant effect on these behavioural outcomes at long‐term follow‐up. Other findings from the McCambridge 2004 study, although not included in the meta‐analysis, also indicated that BIs led to reductions in drug selling to friends (odds ratio = 0.42, P = 0.008).
Overall completeness and applicability of evidence
This review included a small number of studies (n = 6). These studies covered a narrow age range, with the mean age range being from 15.4 to 18 years old, and three of the six studies reported a mean age of 17 to 18 years old (McCambridge 2004; McCambridge 2008; Werch 2005). This makes it somewhat difficult to generalise the results to students who are in early adolescence, who are at a different phase of social and cognitive development. Also, in the United Kingdom, where some of the studies were conducted (McCambridge 2004; McCambridge 2008), the minimum legal drinking age is 18 years (International Center for Alcohol Policies 2010), in comparison to the United States, where the legal drinking age is 21 years. Alcohol use is more acceptable and therefore may be more common among this age group in this context. Adolescents may need interventions that are tailored specifically for their age group, which the National Institute for Health and Care Excellence (NICE) guidelines for school‐based interventions for alcohol advise (NICE 2007).
While our secondary outcomes were described as those that measured criminal or delinquent behaviours, it was difficult to disentangle these behaviours from other interactional and social behaviours in the results, as many studies used scales with specific psychometric properties that made looking at a single item difficult (McCambridge 2004; McCambridge 2008; Walker 2011; Winters 2007b; Winters 2012). Additional research using rigorous methods measuring an array of these outcomes is needed before generalisations and specific recommendations can be made about whether BIs for substance use can curb delinquent behaviours.
Only three published programmes (adapted motivational interviewing, 'Teen Intervene', brief experimental alcohol beverage‐tailored programme) were used or adapted for use in the six studies included in this review. This limited variability in the interventions that were delivered might limit the generalisability of the findings further. These interventions were developed either in the United States or the United Kingdom, which might limit the applicability of the evidence to students in schools within high‐income countries. We are uncertain how applicable these findings are to low‐ and middle‐income countries, and in particular countries with different cultural and social norms around alcohol use.
Quality of the evidence
We used the GRADE approach to assess the quality of evidence for the five key outcomes at the follow‐up periods. See summary of findings Table for the main comparison; summary of findings Table 2.
The quality of the evidence for the outcomes varied from very low to moderate. We downgraded the evidence on account of risk of bias including that it was not possible to blind adolescents and providers, blinding of the outcome assessor was often unclear, and all outcomes were self report data, unexplained significant heterogeneity, and imprecision. Overall, the quality of the evidence seemed to be higher for the comparison BI versus information provision and lower for the comparison BI versus assessment only. For the first set of comparisons, namely BI versus information provision, we had insufficient information in one of the two studies to be certain about the risk of bias in a number of areas; we therefore downgraded the quality of the evidence to moderate. The quality of the evidence was therefore further downgraded. For the comparison BI versus assessment only, there were issues with risk of bias across all of the outcomes. There was also imprecision in some of the outcomes, which led to further downgrading of the evidence quality. There was a large amount of unexplained heterogeneity in addition to the issues with risk of bias and imprecision for two of the outcomes, resulting in the quality of the evidence being downgraded to very low.
Potential biases in the review process
We believe that we have identified all of the studies that focused on the effect of BIs on general substance use as a primary outcome, and behavioural outcomes related to substance use as secondary outcomes, that met our study design and adolescent inclusion criteria up to February 2015. We used a comprehensive search strategy designed with assistance from the Cochrane Drugs and Alcohol Review Group, and ensured that there was independent assessment for inclusion eligibility, risk of bias, and data extraction. We also attempted to locate possible unpublished literature, but were not very successful. A small possibility does exist that unpublished RCTs were excluded from the review. We also took into account that journal articles have strict word or page limits, and contacted authors for additional information where necessary. With one exception, the authors we contacted were very responsive and were able to provide the requested information. Certain questions about risk of bias remain unanswered in the studies whose authors we could not contact. We applied strict criteria in the process of grading the evidence and were transparent about the judgements that led to the decisions on how the studies were rated for the various outcomes.
Agreements and disagreements with other studies or reviews
We found a significant effect size for most comparisons between BI and assessment‐only control conditions. Tait 2003's review reported similar effect sizes, although the studies included in their review were conducted in multiple settings, while the studies included in this review were conducted in educational settings only. Similarly, although the Jensen 2011 review looked at motivational interviewing only and included studies that were again conducted in a number of settings, our effect sizes were comparable with their range of results. The meta‐analysis on alcohol use among adolescents by Watchel 2010, while conducted in clinical settings (and not school settings), found that motivational interviewing (one form of BI) was partially successful, with the most encouraging results being those related to harm minimisation (looking at harms associated with drinking).
In addition, the BIs included in the Watchel 2010 review were not particularly effective in reducing secondary behavioural outcomes such as health, legal, and social harms. Unfortunately, our effect sizes were not directly comparable to these previous reviews, as ours included standardised mean differences, while the other studies included Cohen's d for their effect sizes.
Study flow diagram for updated review.
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
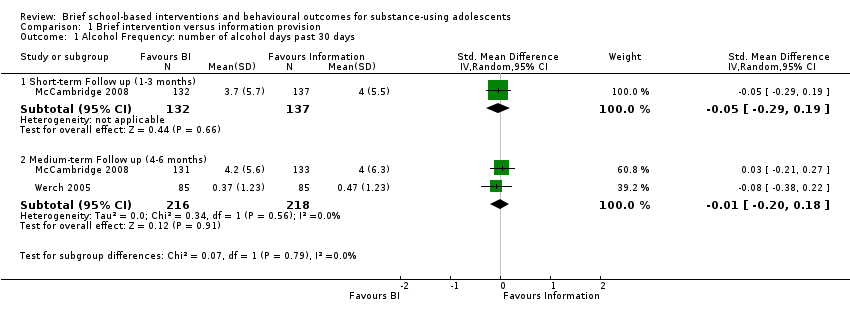
Comparison 1 Brief intervention versus information provision, Outcome 1 Alcohol Frequency: number of alcohol days past 30 days.
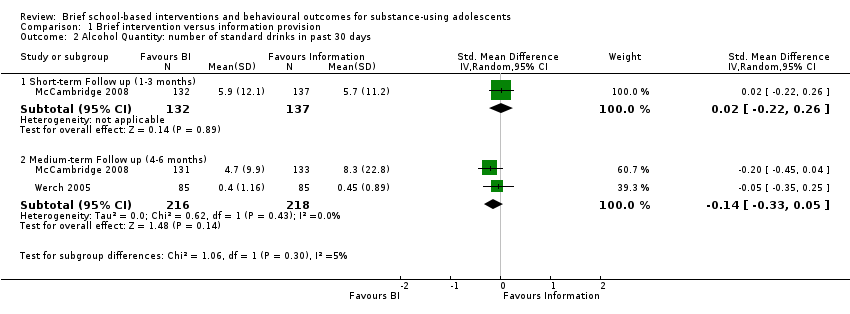
Comparison 1 Brief intervention versus information provision, Outcome 2 Alcohol Quantity: number of standard drinks in past 30 days.

Comparison 1 Brief intervention versus information provision, Outcome 3 Cannabis Quantity: number of joints smoked in past 30 days.

Comparison 1 Brief intervention versus information provision, Outcome 4 Cannabis Mean Dependence Score.

Comparison 1 Brief intervention versus information provision, Outcome 5 Cannabis frequency: number of days smoked cannabis in past 30 days.

Comparison 1 Brief intervention versus information provision, Outcome 6 Secondary outcomes related to substance use: Mean Problem Score.
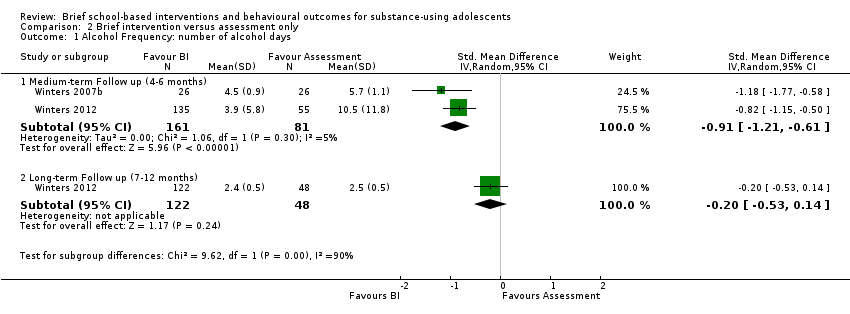
Comparison 2 Brief intervention versus assessment only, Outcome 1 Alcohol Frequency: number of alcohol days.
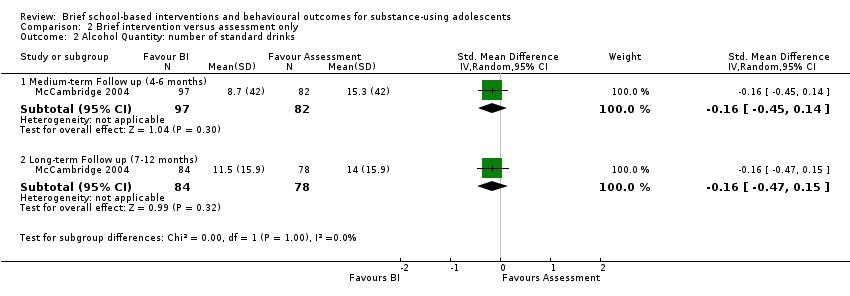
Comparison 2 Brief intervention versus assessment only, Outcome 2 Alcohol Quantity: number of standard drinks.

Comparison 2 Brief intervention versus assessment only, Outcome 3 Alcohol Abuse: number of symptoms.
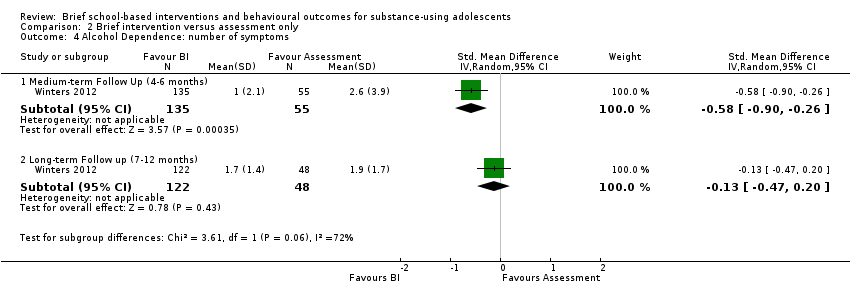
Comparison 2 Brief intervention versus assessment only, Outcome 4 Alcohol Dependence: number of symptoms.
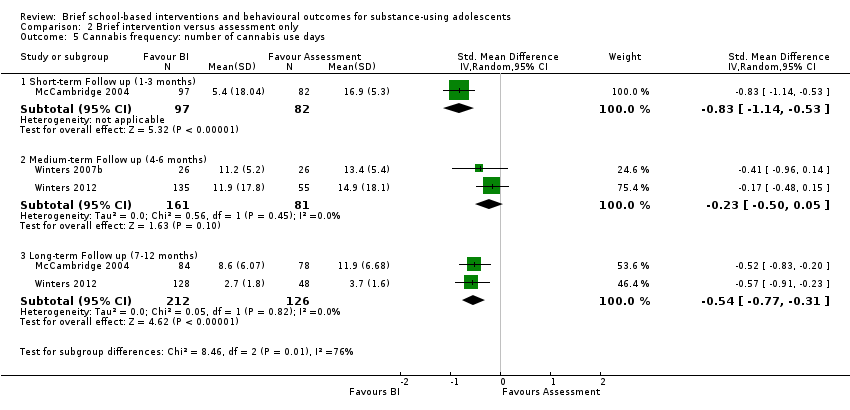
Comparison 2 Brief intervention versus assessment only, Outcome 5 Cannabis frequency: number of cannabis use days.
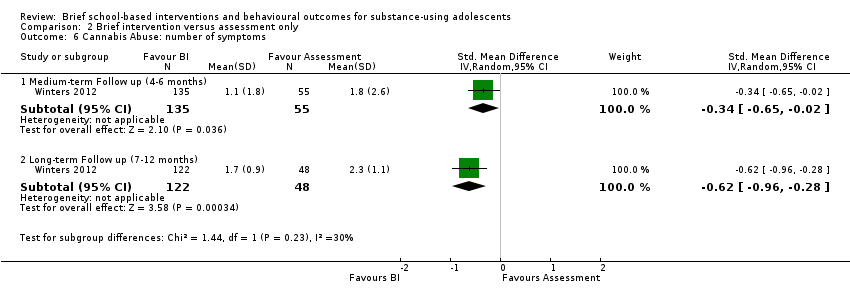
Comparison 2 Brief intervention versus assessment only, Outcome 6 Cannabis Abuse: number of symptoms.

Comparison 2 Brief intervention versus assessment only, Outcome 7 Cannabis Dependence: number of symptoms.

Comparison 2 Brief intervention versus assessment only, Outcome 8 Secondary outcomes related to substance use: Mean score on personal consequences scale.
| Brief intervention compared to information provision for substance‐using adolescents | ||||||
| Patient or population: Substance‐using adolescents | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Estimate effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Information provision | Brief intervention | |||||
| Alcohol frequency | See comment | The standardised mean alcohol frequency in the intervention groups was 0.01 standard deviations lower | SMD ‐0.01 (‐0.20 to 0.18) | 434 | ⊕⊕⊕⊝ | Number of days of alcohol use |
| Alcohol quantity Medium‐term follow‐up: 4 to 6 months | See comment | The standardised mean alcohol quantity in the intervention groups was 0.14 standard deviations lower | SMD ‐0.14 (‐0.33 to 0.05) | 434 | ⊕⊕⊕⊝ | Number of standard alcohol units |
| Cannabis dependence | See comment | The standardised mean cannabis dependence score in the intervention groups was 0.09 standard deviations lower (0.27 lower to 0.09 higher) | SMD ‐0.09 (‐0.27 to 0.09) | 470 | ⊕⊕⊕⊝ | Mean dependence score |
| Cannabis frequency | See comment | The mean cannabis frequency in the intervention groups was | SMD ‐0.07 (‐0.25 to 0.11) | 470 | ⊕⊕⊕⊝ | Number of days cannabis use |
| Secondary outcomes related to substance use Short‐term follow‐up: 1 to 3 months | See comment | The mean behavioural outcomes related to substance use in the intervention groups was | SMD ‐0.01 (‐0.19 to 0.17) | 470 | ⊕⊕⊕⊝ | Interactional Problems Score |
| *The basis for the assumed risk (e.g. the mean control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the estimate effect of the intervention (and its 95% CI). The estimate effects for certain outcomes were not estimable due to only one study assessing the specific outcome, or extremely high levels of heterogeneity making effects across studies difficult to compare. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Risk of bias (‐1): It was not possible to blind the participants in all of the included studies. There was also uncertainty in two of the studies about allocation concealment and blinding of outcome assessor (Walker 2011; Werch 2005). | ||||||
| Brief intervention compared to assessment only for substance‐using adolescents | ||||||
| Patient or population: Substance‐using adolescents | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Estimate effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Assessment only | Brief intervention | |||||
| Alcohol frequency Self report questionnaires | See comment | The standardised mean alcohol frequency in the intervention groups was 0.91 standard deviations lower | SMD ‐0.91 (‐1.21 to ‐0.61) | 242 | ⊕⊕⊝⊝ | Number of days of alcohol use |
| Alcohol quantity Medium‐term follow‐up: 4 to 6 months | See comment | The standardised mean alcohol quantity in the intervention groups was 0.16 standard deviations lower | SMD ‐0.16 (‐0.45 to 0.14) | 179 (1 study) | ⊕⊕⊝⊝ | Number of standard alcohol units |
| Cannabis dependence | See comment | The mean cannabis dependence in the intervention groups was | SMD ‐0.26 (‐0.57 to 0.36) | 190 | ⊕⊕⊝⊝ | Mean dependence score |
| Cannabis frequency | See comment | The mean cannabis frequency in the intervention groups was | SMD ‐0.54 (‐0.77 to ‐0.31) | 338 | ⊕⊕⊝⊝ | Number of days of cannabis use |
| Secondary outcomes related to substance use Self report questionnaires Medium‐term follow‐up: 4 to 6 months | See comment | The mean mean behavioural outcomes related to substance use in the intervention groups was | SMD ‐0.65 (‐1.58 to 0.28) | 242 | ⊕⊕⊝⊝ | Interactional Problems Score |
| *The basis for the assumed risk (e.g. the mean control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the estimate effect of the intervention (and its 95% CI). The estimate effects for certain outcomes were not estimable due to only one study assessing the specific outcome, or extremely high levels of heterogeneity making effects across studies difficult to compare. | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Risk of bias (‐1): It was not possible to blind the participants in all of the included studies. There was no allocation concealment in two of the included studies, and it was unclear whether the outcome assessor was blinded (Winters 2007b; Winters 2012). The other study was also not free of selective reporting bias (McCambridge 2004). | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Alcohol Frequency: number of alcohol days past 30 days Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 Short‐term Follow up (1‐3 months) | 1 | 269 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.05 [‐0.29, 0.19] |
| 1.2 Medium‐term Follow up (4‐6 months) | 2 | 434 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.01 [‐0.20, 0.18] |
| 2 Alcohol Quantity: number of standard drinks in past 30 days Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 Short‐term Follow up (1‐3 months) | 1 | 269 | Std. Mean Difference (IV, Random, 95% CI) | 0.02 [‐0.22, 0.26] |
| 2.2 Medium‐term Follow up (4‐6 months) | 2 | 434 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.14 [‐0.33, 0.05] |
| 3 Cannabis Quantity: number of joints smoked in past 30 days Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 Short‐term Follow up (1‐3 months) | 1 | 269 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [‐0.24, 0.24] |
| 3.2 Medium‐term Follow up (4‐6 months) | 1 | 264 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.15 [‐0.39, 0.09] |
| 4 Cannabis Mean Dependence Score Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 4.1 Short‐term Follow up (1‐3 months) | 2 | 470 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.27, 0.09] |
| 4.2 Medium‐term Follow up (4‐6 months) | 1 | 264 | Std. Mean Difference (IV, Random, 95% CI) | 0.06 [‐0.18, 0.30] |
| 4.3 Long‐term Follow up (7‐12 months) | 1 | 186 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.38, 0.20] |
| 5 Cannabis frequency: number of days smoked cannabis in past 30 days Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 5.1 Short‐term Follow up (1‐3 months) | 2 | 470 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.07 [‐0.25, 0.11] |
| 5.2 Medium‐term Follow up (4‐6 months) | 1 | 264 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.06 [‐0.30, 0.18] |
| 5.3 Long‐term Follow up (7‐12 months) | 1 | 186 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.02 [‐0.31, 0.26] |
| 6 Secondary outcomes related to substance use: Mean Problem Score Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 6.1 Short‐term Follow up (1‐3 months) | 2 | 470 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.01 [‐0.19, 0.17] |
| 6.2 Medium‐term Follow up (4‐6 months) | 1 | 264 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.37, 0.11] |
| 6.3 Long‐term Follow up (7‐12 months) | 1 | 186 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.10 [‐0.39, 0.19] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Alcohol Frequency: number of alcohol days Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 Medium‐term Follow up (4‐6 months) | 2 | 242 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.91 [‐1.21, ‐0.61] |
| 1.2 Long‐term Follow up (7‐12 months) | 1 | 170 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.20 [‐0.53, 0.14] |
| 2 Alcohol Quantity: number of standard drinks Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 Medium‐term Follow up (4‐6 months) | 1 | 179 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.16 [‐0.45, 0.14] |
| 2.2 Long‐term Follow up (7‐12 months) | 1 | 162 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.16 [‐0.47, 0.15] |
| 3 Alcohol Abuse: number of symptoms Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 Medium‐term Follow up (4‐6 months) | 1 | 190 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.38 [‐0.70, ‐0.07] |
| 3.2 Long‐term Follow up (7‐12 months) | 1 | 170 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.72 [‐1.07, ‐0.38] |
| 4 Alcohol Dependence: number of symptoms Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 4.1 Medium‐term Follow Up (4‐6 months) | 1 | 190 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.58 [‐0.90, ‐0.26] |
| 4.2 Long‐term Follow up (7‐12 months) | 1 | 170 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.47, 0.20] |
| 5 Cannabis frequency: number of cannabis use days Show forest plot | 3 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 5.1 Short‐term Follow up (1‐3 months) | 1 | 179 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.83 [‐1.14, ‐0.53] |
| 5.2 Medium‐term Follow up (4‐6 months) | 2 | 242 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.23 [‐0.50, 0.05] |
| 5.3 Long‐term Follow up (7‐12 months) | 2 | 338 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.54 [‐0.77, ‐0.31] |
| 6 Cannabis Abuse: number of symptoms Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 6.1 Medium‐term Follow up (4‐6 months) | 1 | 190 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.34 [‐0.65, ‐0.02] |
| 6.2 Long‐term Follow up (7‐12 months) | 1 | 170 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.62 [‐0.96, ‐0.28] |
| 7 Cannabis Dependence: number of symptoms Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 7.1 Medium‐term Follow up (4‐6 months) | 1 | 190 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.26 [‐0.57, 0.06] |
| 7.2 Long‐term Follow up (7‐12 months) | 1 | 170 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.97 [‐1.32, ‐0.62] |
| 8 Secondary outcomes related to substance use: Mean score on personal consequences scale Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 8.1 Medium‐term Follow up (4‐6 months) | 2 | 242 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.65 [‐1.58, 0.28] |
| 8.2 Long‐term Follow up (7‐12 months) | 1 | 170 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.78 [‐1.13, ‐0.44] |