Tonsillectomy for periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis syndrome (PFAPA)
Abstract
Background
Periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis (PFAPA) syndrome is a rare clinical syndrome of unknown cause usually identified in children. Tonsillectomy is considered a potential treatment option for this syndrome. This is an update of a Cochrane review first published in 2010.
Objectives
To assess the effectiveness and safety of tonsillectomy (with or without adenoidectomy) in children with PFAPA.
Search methods
We searched the Cochrane Ear, Nose and Throat Disorders Group Trials Register; the Cochrane Central Register of Controlled Trials (CENTRAL); PubMed; EMBASE; CINAHL; Web of Science; Cambridge Scientific Abstracts; ICTRP and additional sources for published and unpublished trials. The date of the search was 30 October 2013.
Selection criteria
Randomised controlled trials comparing tonsillectomy (with or without adenoidectomy) with non‐surgical treatment in children with PFAPA.
Data collection and analysis
Two authors independently assessed trial quality and extracted data. We used the standard methodological procedures expected by The Cochrane Collaboration.
Main results
Two trials were included with a total of 67 children randomised (65 analysed); we judged both to be at low risk of bias.
One trial of 39 participants recruited children with PFAPA syndrome diagnosed according to rigid, standard criteria. The trial compared adenotonsillectomy to watchful waiting and followed up patients for 18 months. A smaller trial of 28 children applied less stringent criteria for diagnosing PFAPA and probably also included participants with alternative types of recurrent pharyngitis. This trial compared tonsillectomy alone to no treatment and followed up patients for six months.
Combining the trial results suggests that patients with PFAPA experience less fever and less severe episodes after surgery compared to those receiving no surgery. The risk ratio (RR) for immediate resolution of symptoms after surgery that persisted until the end of follow‐up was 4.38 (95% confidence interval (CI) 0.64 to 30.11); number needed to treat to benefit (NNTB) = 2, calculated based on an estimate that 156 in 1000 untreated children have a resolution).
There was a large overall reduction in the average number of episodes over the total length of follow‐up in these studies (rate ratio 0.08, 95% CI 0.05 to 0.13), reducing the average frequency of PFAPA episodes from one every two months to slightly less than one every two years. The severity, as indicated by the length of PFAPA symptoms during these episodes, was also reduced. One study reported that the average number of days per PFAPA episode was 1.7 days after receiving surgery, compared to 3.5 days in the control group. The proportion of patients requiring corticosteroids was also lower in the surgery group compared to those receiving no surgery (RR 0.58, 95% CI 0.37 to 0.92).
Both trials reported that there were no complications of surgery. However, the numbers of patients randomly allocated to surgery (19 and 14 patients respectively) were too small to detect potentially important complications such as haemorrhage. Other outcomes such as quality of life, number of days with pain after surgery and absence from school were not measured or reported.
Authors' conclusions
The evidence for the effectiveness of tonsillectomy in children with PFAPA syndrome is derived from two small randomised controlled trials. These trials reported significant beneficial effects of surgery compared to no surgery on immediate and complete symptom resolution (NNTB = 2) and a substantial reduction in the frequency and severity (length of episode) of any further symptoms experienced. However, the evidence is of moderate quality (further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate) due to the relatively small sample sizes of the studies and some concerns about the applicability of the results. Therefore, the parents and carers of children with PFAPA syndrome must weigh the risks and consequences of surgery against the alternative of using medications. It is well established that children with PFAPA syndrome recover spontaneously and medication can be administered to try and reduce the severity of individual episodes. It is uncertain whether adenoidectomy combined with tonsillectomy adds any additional benefit to tonsillectomy alone.
PICOs
Plain language summary
Tonsillectomy for PFAPA syndrome (a rare cause of recurrent fever, mouth ulcers, sore throat and swollen neck glands)
Review question
This review compared the clinical effectiveness and safety of removing the palatine tonsils (tonsillectomy), with and without removal of the adenoids, against non‐surgical management of children with periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis (PFAPA) syndrome. We searched for and included any randomised controlled trials published up to October 2013.
Background
PFAPA syndrome is a rare cause of regular, repeated episodes of fever, sore throat and swollen neck glands in children. It is a diagnosis that needs confirmation by paediatricians working in centres with expertise in this condition and most children who suffer from repeated sore throats and tonsillitis will not have it.
Study characteristics
We found two small randomised controlled trials, with a low risk of bias, comparing tonsillectomy or adenotonsillectomy against non‐surgical interventions (total of 67 participants, with data from 65 analysed). One study (39 participants) used the adenotonsillectomy procedure in the intervention group and followed up patients for 18 months. This study applied stringent criteria for diagnosing PFAPA when recruiting patients. The other trial (28 participants) only removed the tonsils and followed up patients for up to six months. Less stringent recruitment criteria were applied and it was possible that patients with other types of recurrent sore throats might have been recruited and included in the trial. Neither study masked participants and investigators to the type of treatment received. Participants in the control groups of both studies received standard medical treatment.
Key results
The two trials showed that children with PFAPA are likely to benefit from tonsillectomy. The results showed that children who had surgery were about four times more likely to be free of PFAPA symptoms from the point of surgery until the end of the follow‐up periods for these studies. There was an overall decrease in the number or frequency of PFAPA episodes experienced by the children in the surgery group. While the average child in the control arm had an average of one episode every two months, this was reduced to less than one‐tenth of that; i.e. about one episode every two years among children who had surgery. In addition, the length of each episode was also shortened by an average of 1.8 days (reduced from an average of 3.5 days to 1.7 days per episode) for children who had surgery.
Courses of corticosteroids can be used to treat episodes of symptoms in children with PFAPA. One trial reported that the proportion of children given a course of corticosteroids was lower in children who received surgery.
The trials reported no complications of surgery. However, these studies might be too small to detect important but rarer types of complications such as bleeding from the surgery. Other outcomes such as quality of life, absence from school or quality of life were not reported.
Quality of evidence
The quality of the evidence is moderate (that is, further research is likely to have an important impact on our confidence in the estimates of effects and may change these estimates). The studies are very small. Studies with larger numbers of patients are required to estimate the effects more precisely. There is also some uncertainly about whether the effects observed in these studies can be replicated in most children with PFAPA for two reasons. It is unclear whether some children who did not have PFAPA had been included in the study that applied less stringent inclusion criteria for PFAPA diagnosis. Secondly, it is uncertain whether the treatment received in the control arms of the studies was adequate and represented current practice.
Authors' conclusions
Summary of findings
| Surgery (tonsillectomy +/‐ adenoidectomy) for children with periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis syndrome (PFAPA) | ||||||
| Patient or population: children with PFAPA | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Surgery (tonsillectomy +/‐ adenoidectomy) | |||||
| Complete resolution of symptoms (proportion of patients with 'immediate and persistent resolution of symptoms' from the point of surgery/randomisation up to end of study follow‐up) | Study population (average) | RR 4.38 | 65 | ⊕⊕⊕⊝ | The NNTB based on the study population risk was 1/(684‐156)*1000 = 1.89 1 study followed up patients up to 6 months; another up to 18 months | |
| 156 per 1000 | 684 per 1000 | |||||
| Medium risk population | ||||||
| 192 per 1000 | 841 per 1000 | |||||
| Complications of surgery (haemorrhage and days with pain) | Both studies reported no complications from surgery Days of pain not reported as an outcome | |||||
| Number of episodes of fever and associated symptoms (episodes per person per month) | Mean 0.5 episode per person per month (1 episode every 2 months) | Mean 0.04 episode per person per month (1 episode every 25 months) | Rate ratio: 0.08 (0.05 to 0.13) | 65 | ⊕⊕⊕⊝ | |
| Severity of episodes (number of days with fever and the associated symptoms (per episode)) | Mean 3.5 (range of 2 to 6) days per episode | Mean 1.7 (range of 2 to 4) days per episode | Mean difference: 1.8 days per episode | 39 (1 study) | ⊕⊕⊕⊝ | Study reported statistical significance. Standard deviations were not reported in the study for average number of days per episode |
| Use of corticosteroids (proportion of patients using corticosteroids) | Study population (average) | RR 0.58 (0.37 to 0.92) | 39 (1 study) | ⊕⊕⊝⊝ | Review intended to report number of courses/patient, but these data were not available in the studies | |
| 900 per 1000 | 522 per 1000 | |||||
| Absence or time off school | None of the studies reported this | |||||
| Quality of life | None of the studies reported this | |||||
| *The basis for the assumed risk was the median risk in the control groups for "medium risk population" and for "study population", this was the average (i.e. total number of participants with events divided by total number of participants included in the meta‐analysis). The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Quality (confidence in the evidence) was reduced because of the small size of the studies and broad confidence intervals. There was also concern as to whether the treatment received by the control group reflects current practice. The criteria for recruitment of patients into one of the studies was not stringent and could have included patients who did not have PFAPA (Renko 2007). | ||||||
Background
Tonsillectomy is often performed for chronic or recurrent acute tonsillitis or sore throat. These are relatively common clinical conditions and important reasons for seeking medical attention and advice. Periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis (PFAPA) syndrome is a much rarer and more unusual condition but one for which tonsillectomy is thought to be beneficial. This is an update of a Cochrane review first published in 2010 (Burton 2010).
Description of the condition
PFAPA syndrome is a rare clinical syndrome, usually identified in children, and comprising those features described in its title. The original description is attributed to Marshall, Edwards, Butler and Lawton in 1987 (Marshall 1987). The same authors first used the acronym PFAPA, proposed a set of diagnostic criteria in 1989 (Marshall 1989), and re‐iterated these criteria in an often cited publication of 1999 (Thomas 1999). Case definition continues, however, to be an issue in this field. A more recently published large series of 105 patients, co‐authored by a physician involved in some of the earliest studies of the condition, identified PFAPA patients using criteria which differed somewhat from the standard (Feder 2010).
The cause of PFAPA syndrome is unknown and it occurs sporadically. There are a number of related, but distinct, periodic fever syndromes in which underlying genetic abnormalities have been characterised. The periodicity has been described as 'clockwork' (Long 2007) (and episodes are therefore 'predictable' by the parents and carers of affected children), with episodes occurring every 30 days (range 14 to 50) and lasting four days (range two to seven) (Feder 2010).
In children whose condition resolves spontaneously, Feder 2010 reported the mean and median duration of symptoms as 33 and 24 months respectively (range 8 to 92 months).
Description of the intervention
Tonsillectomy is one of the most common surgical procedures performed in children. The procedure has been a controversial one historically and it remains so. Opinions vary greatly as to the relative risks and benefits of the surgery and the indications are equally controversial. It is generally accepted that tonsillectomy (with adenoidectomy, if necessary) is indicated in children with obstructive sleep apnoea. In many countries large numbers of patients who have recurrent acute tonsillitis, chronic tonsillitis or recurrent 'sore throats' also have their tonsils removed. The frequency and severity of 'infections' required to justify surgery vary considerably. The effectiveness of tonsillectomy for chronic/recurrent acute tonsillitis and sore throat is the subject of another Cochrane review by some of us (Burton 2009).
Any benefit of tonsillectomy must offset the risks of surgery. These include those of the associated general anaesthesia and those specific to the procedure, for example bleeding immediately after surgery or in the 10‐ to 14‐day period after surgery. Equally relevant are the natural history of the untreated disease (many children with PFAPA syndrome will 'grow out' of the condition as they get older) and the availability and effectiveness of non‐surgical treatment to prevent or ameliorate symptomatic episodes. Medical treatment of PFAPA includes the use of corticosteroids for individual episodes or cimetidine for prophylaxis (Feder 2010). However, these treatments are not used in all countries (Renko 2008), and have not to our knowledge been evaluated in randomised controlled trials.
How the intervention might work
The cause of PFAPA is not known. The clinical features of periodicity and inflammation suggest that it may be a genetically regulated periodic fever, like other defined periodic fever syndromes. However, since tonsillectomy aborts the symptoms of PFAPA in many patients the inflammation is presumably driven from these lymphoid tissues. The inflammation might originate from dysregulated tonsillar cells directly or be initiated locally by a mediator from another tissue or a microbial stimulus. In either case removal of the tissues interrupts the inflammation.
Why it is important to do this review
Several non‐randomised studies have suggested that tonsillectomy has a dramatic effect in children with PFAPA. Abramson reported the unexpected complete resolution of symptoms in four children after tonsillectomy in 1989 (Abramson 1989). Long has described two 'major stumbling blocks' in testing treatments for PFAPA: the small number of patients with the condition and the difficulties confirming the diagnosis (Long 2009). This last observation underlines the importance of examining the participants in any study and asking the question: do all these children really have PFAPA syndrome? Or does the study population comprise a more heterogeneous group including some with other types of pharyngitis or tonsillitis? Answers to these questions will have a critical impact on the applicability of the results. The small number of patients means that individual studies are likely to be small. Yet, if the treatment effect size is large, a clinically and statistically significant difference between treatment and control groups may be identifiable. Combining the results of more than one study in a meta‐analysis may allow a smaller positive effect size to be demonstrated or increase the precision of the estimate of that effect size. This systematic review therefore examines the clinical effectiveness and safety of tonsillectomy (with or without adenoidectomy) for children with PFAPA syndrome.
Objectives
To determine the clinical effectiveness and safety of tonsillectomy (with or without adenoidectomy) compared with non‐surgical treatment in the management of children with PFAPA syndrome.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) of tonsillectomy (with or without adenoidectomy) versus non‐surgical treatment.
Types of participants
Children with a diagnosis of periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis (PFAPA) syndrome made by specialists (paediatricians) based on standard diagnostic criteria.
Types of interventions
Tonsillectomy (with or without adenoidectomy) versus non‐surgical treatment.
We included all different surgical methods of tonsillectomy (such as blunt dissection, bipolar electrocautery and coblation) in this review.
Non‐surgical treatment was defined as all forms of non‐surgical treatment, such as no treatment (including active monitoring/watchful waiting), analgesics and antipyretics, corticosteroids and cimetidine therapy. We intended to consider the different non‐surgical treatments as separate subgroups.
Types of outcome measures
We focused our data extraction on important patient‐relevant outcomes. Outcomes would ideally be assessed over a minimum period of 12 months, and preferably in the second and subsequent years after randomisation. In the first version of this review (Burton 2010), we had two primary outcomes. These were: (1) proportion of children whose symptoms have completely resolved, and (2) reduction in number and severity of episodes of fever and the associated symptoms. In this 2014 update, we retained the first primary outcome and the second outcome became two distinct secondary outcomes (number of episodes and severity of episodes). Furthermore, we added complications of surgery (haemorrhage and number of days of postoperative pain) as a primary outcome and use of corticosteroids, absence or time off school and quality of life as secondary outcomes.
Primary outcomes
-
Proportion of children whose symptoms have completely resolved
-
Complications of surgery (haemorrhage and number of days of postoperative pain)
Secondary outcomes
-
Number of episodes of fever and the associated symptoms
-
Severity of episodes
-
Use of corticosteroids
-
Absence or time off school
-
Quality of life
We defined severity of episodes as the number of days with fever and the associated symptoms per episode, while the use of corticosteroids is measured as number of courses per patient.
Search methods for identification of studies
We conducted systematic searches for RCTs. There were no language, publication year or publication status restrictions. We planned to contact original authors for clarification and further data if trial reports were unclear and to arrange translations of papers where necessary. The date of the latest search was 30 October 2013, following the original searches for the review in 2010.
Electronic searches
We identified published, unpublished and ongoing studies by searching the following databases from their inception: the Cochrane Central Register of Controlled Trials (CENTRAL) (2013, Issue 9); PubMed; EMBASE; CINAHL; ISRCTN; LILACS; KoreaMed; IndMed; PakMediNet; CAB Abstracts; Web of Science; ICTRP; Clinicaltrials.gov; Google Scholar and Google. In searches prior to 2013, we also searched BIOSIS Previews 1926 to 2012. For the original search in 2010, we searched NRR Archive 2000 to 2007.
We modelled subject strategies for databases on the search strategy designed for CENTRAL. Where appropriate, we combined subject strategies with adaptations of the highly sensitive search strategy designed by The Cochrane Collaboration for identifying randomised controlled trials and controlled clinical trials (as described in the Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0, Box 6.4.b. (Handbook 2011). Search strategies for major databases including CENTRAL are provided in Appendix 1.
Searching other resources
We scanned the reference lists of identified publications for additional trials and contacted trial authors if necessary. We searched PubMed, TRIPdatabase, The Cochrane Library and Google to retrieve existing systematic reviews relevant to this systematic review, so that we could scan their reference lists for additional trials.
Data collection and analysis
Selection of studies
Two review authors independently screened titles and abstracts of the studies obtained from the database searches and reviewed the full text of the potentially relevant titles and abstracts against the inclusion and exclusion criteria. We documented the exclusion of any studies from the review and described the reasons for exclusion in the Characteristics of excluded studies table. We resolved any differences over which studies to include or exclude by discussion and consensus.
Data extraction and management
In the first publication of this Cochrane review (Burton 2010), two authors (MJB and JR) independently extracted data from the studies using standardised, pre‐piloted forms. For this 2014 update, two new authors rechecked the data and, had additional studies been identified, we would have used the same methods to extract the data. We extracted data so as to allow an intention‐to‐treat analysis. Where data were missing, we contacted the trial authors to request further information or conducted an available case analysis if necessary.
Assessment of risk of bias in included studies
In the first publication of this Cochrane review (Burton 2010), two review authors (MJB and JR) undertook assessment of the risk of bias of the included trials independently, with the following taken into consideration, as guided by theCochrane Handbook for Systematic Reviews of Interventions (Handbook 2011):
-
sequence generation;
-
allocation concealment;
-
blinding;
-
incomplete outcome data; and
-
reporting bias
-
other sources of bias.
We used the Cochrane 'Risk of bias' tool, which involves describing each of these domains as reported in the trial and then assigning a judgement about the risk of bias of each domain: 'low', 'high' or 'unclear' risk of bias.
Measures of treatment effect
We proposed analysing the data according to the intention‐to‐treat principle, whereby all participants are analysed in the groups to which they were randomised.
We expressed dichotomous outcomes (e.g. proportion of patients with symptom resolution) as risk ratios (RR) and risk difference (RD) with 95% confidence intervals (CIs). Additionally, we calculated the number needed to treat to benefit (NNTB) from the pooled measure of treatment effect.
Due to the nature of the condition (episodic), the intervention being evaluated may reduce the frequency of the episodes or resolve the episodes completely. Therefore, most of the outcomes are count data and we analysed these as rate data whenever possible (whenever time of follow‐up was available). We proposed calculating the rate ratio of number of outcomes per person‐month for count data whenever possible.
Where there were missing data or there was loss to follow‐up, we planned an available case analysis.
Unit of analysis issues
We identified no studies with non‐standard designs, such as cross‐over or cluster‐randomised trials.
Dealing with missing data
In the case of missing data, we contacted the corresponding trial authors to obtain additional information. No imputations for missing data were pre‐planned, apart from standard calculations to obtain SD values for continuous data as detailed in the Cochrane Handbook for Systematic Reviews of Interventions (Handbook 2011).
Assessment of heterogeneity
We assessed clinical heterogeneity (which may be present even in the absence of statistical heterogeneity) by examining the included trials for potential differences between studies in the types of participants recruited, interventions or control used and outcomes measured. We did not identify any specific subgroups for subgroup analysis a priori.
We also assessed statistical heterogeneity using the Chi2 test (with a significance level set at P < 0.10) and the I2 statistic, which calculates the percentage of variability that is due to heterogeneity rather than chance, with I2 values over 50% suggesting substantial heterogeneity (Handbook 2011).
Assessment of reporting biases
We planned to compare the outcomes reported in the trial against the protocols for the studies, whenever possible, to assess for reporting bias. If a sufficient number of studies had been available, we would have conducted more formal assessments using funnel plots.
Data synthesis
For dichotomous data, we analysed treatment differences as risk ratio (RR) with 95% confidence interval (CI) calculated using the Mantel‐Haenszel method with a fixed‐effect model and the generic inverse‐variance method for the rate ratios. For dichotomous data, we calculated the number needed to treat to benefit (NNTB) using the results of the meta‐analysis (which itself used risk ratio) based on an assumed baseline risk. This assumed baseline risk is typically either (a) the median of the risks of the control groups in the included studies, this being used to represent a 'medium risk population' or, alternatively, (b) the average risk of the control groups in the included studies is used as the 'study population' (Handbook 2011). Should further studies be added in future updates it may also be appropriate to consider assumed baseline risk in (c) a low‐risk population and (d) a high‐risk population.
Subgroup analysis and investigation of heterogeneity
We did not plan or perform any subgroup analyses.
We assessed heterogeneity by visual inspection of the forest plots and consideration of the statistical tests for heterogeneity. We assessed statistical heterogeneity by considering the Chi2 test for significance at P < 0.1 or an I2 inconsistency statistic of more than 50% indicating significant heterogeneity.
We also planned to use a 'test of subgroup differences' to assess potential differences in effects between subgroups.
We used a fixed‐effect meta‐analysis where no heterogeneity was present. If statistical heterogeneity was detected but unresolved by subgroup or sensitivity analysis, then we employed a random‐effects (DerSimonian and Laird) model to provide a more conservative estimate of the effect.
Sensitivity analysis
We did not plan or perform any sensitivity analysis.
Results
Description of studies
See: Characteristics of included studies; Characteristics of excluded studies; Characteristics of ongoing studies.
Results of the search
This is an update of a Cochrane review first published in 2010 (Burton 2010). The original searches in January 2010 retrieved 110 results. After removal of duplicates and an initial sift for relevance, we were left with three potentially relevant references (Garavello 2009; Pignataro 2009; Renko 2007). We excluded one as a non‐randomised prospective study (Pignataro 2009), leaving two studies that could be included in the review (Garavello 2009; Renko 2007).
From the updated searches (January 2010 to 30 October 2013) we retrieved a total of 82 additional records. Removing duplicates left 36. After screening titles and abstracts, we identified two additional potentially relevant studies (Peridis 2010a; Ridder 2011). These two studies were, however, excluded as non‐randomised cohort studies. As a consequence, no additional trials were identified for the update of this review (Figure 1). We did not identify any ongoing trials.

Process for sifting search results and selecting studies for inclusion
Included studies
Two unblinded, randomised controlled trials are included in this review (Garavello 2009; Renko 2007). Full details on methods, participants, interventions and outcomes are provided in the Characteristics of included studies table. We contacted the authors of both studies for further information about the methods and results of studies in October 2013, but we only obtained additional information from the authors of Renko 2007.
Design
Both studies were unblinded randomised controlled trials (RCTs).
Setting
Both studies were undertaken in European tertiary/university hospitals. Participants were recruited from three tertiary hospital in Oulu Finland between 1999 and 2003 (Renko 2007), and the ENT department of the University Hospital of Milano‐Bicocca from 2003 to 2006 (Garavello 2009)
Participants
The studies included children aged between 1.5 and 14 years. The mean ages of the children were 4.1 (Renko 2007) and 5.1 (Garavello 2009) years. The studies differed in the diagnostic criteria used to define the participants as suffering from PFAPA syndrome.
The children included in Renko 2007 were characterised by a specific number of "PFAPA attacks" (at least five) and each attack needed to have been itself characterised by high fever (≥ 38.5 °C) of unknown origin. The attacks had to recur with "a typical, regular pattern" with "asymptomatic intervals of 2 to 5 weeks". Although any accompanying signs of aphthous stomatitis, pharyngitis and adenitis were "recorded", these features were not essential requirements of the diagnosis. In a subsequent letter the senior author clarified that "pharyngitis or tonsillitis caused by group A streptococcus was excluded on clinical grounds" and that "The diagnostic criteria presented by Thomas 1999 et al were not fulfilled in all our patients" (Renko 2008).
Garavello 2009 included children who had a diagnosis of PFAPA syndrome based on four criteria:
-
Onset of disease in early childhood (before five years of age).
-
Regular, recurring, abrupt episodes of fever lasting approximately five days, associated with constitutional symptoms and at least one of: aphthous stomatitis, pharyngitis or cervical adenitis in the absence of other signs of respiratory tract infection. These latter signs were present in the following proportions of participants: aphthous stomatitis ‐ 61% of surgery group, 58% of controls; pharyngitis ‐ 98% surgery, 97% controls; cervical adenitis ‐ 89% surgery, 82% controls.
-
Prompt remission of symptoms after corticosteroid administration and completely asymptomatic interval.
-
Normal growth and development.
Children with cyclic neutropenia, other auto‐inflammatory diseases and clinical and laboratory evidence of immunodeficiency, autoimmune disease or chronic infection were excluded.
Participants in Renko 2007 had on average 9.3 (range 4 to 20) episodes per year, while participants in Garavello 2009 had an average of 8.7 (range 4 to 12) episodes per year at baseline.
Interventions
The children in Renko 2007 received tonsillectomy (method unclear) within one month and in Garavello 2009 adenotonsillectomy (method unclear).
No details are given about the management of children in the control group of Renko 2007, but the author subsequently clarified that in Finland, where the study was performed, "cimetidine and prednisolone are not used for PFAPA ... and were not used in any of the patients in this series" (Renko 2008). Children in the control group were allowed tonsillectomy after six months if the symptoms persisted.
Garavello 2009 allowed children in both the control group and the surgical group to "use corticosteroids" and refers to this group receiving "expectant management". There is no indication of whether or not the control groups received prophylactic cimetidine.
Outcomes
Although symptom diaries were completed over a 12‐month period in Renko 2007, results are presented at six months. The study period in Garavello 2009 was 18 months.
Proportion of children whose symptoms have completely resolved
Both studies reported (as a primary outcome measure) the proportion of patients experiencing resolution of their PFAPA symptoms, but different definitions were used:
-
Renko 2007 defined it as "disappearance of fever episodes" six months after randomisation (counting the number of children without symptoms at the six‐month follow‐up).
-
Garavello 2009 used the definition of "immediate and persistent resolution of symptoms" (counting only children whose symptoms resolved from the point of surgery/randomisation and had no recurrence within the 18‐month follow‐up).
Due to the differences in definitions used for symptom resolution outcomes, we contacted the authors to obtain more information for the 2014 update. We obtained more information from the authors of Renko 2007, but not from Garavello 2009.
Number of episodes of fever and the associated symptoms
Data are presented for both treatment and control groups on the number of "fever episodes compatible with periodic fever" per person‐month at risk over the six‐month follow‐up period in Renko 2007. The absolute number of "PFAPA episodes" in both groups over 18 months is provided by Garavello 2009.
Complications of surgery (haemorrhage and number of days of postoperative pain)
Both studies reported that no complications were experienced by patients receiving surgery.
Other outcomes (severity of episodes, use of corticosteroids absence of time off school, quality of life)
Garavello 2009 reported on the proportion of patients who had received corticosteroids for each group, but not the number of courses required.
Other outcomes, such as number of days with pain, absence from school after surgery or quality of life, were not reported.
Excluded studies
Three studies were found to be non‐randomised cohort studies and we therefore excluded them from the review (Pignataro 2009; Peridis 2010a; Ridder 2011). See the Characteristics of excluded studies table.
Risk of bias in included studies
We judged both trials as at low risk of bias (Garavello 2009; Renko 2007). Details of the 'Risk of bias' assessment of the included trials are summarised in a 'Risk of bias' graph (Figure 2) and summary (Figure 3).

'Risk of bias' graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.

'Risk of bias' summary: review authors' judgements about each methodological quality item for each included study.
Allocation
One trial adequately described the method of random sequence generation and concealment of allocation (Garavello 2009). While this was unclear in the other trial, as no information was provided in the publication, we requested additional information on the method of random sequence generation and concealment of allocation and this was provided by the author of the trial; we subsequently judged the risk of selection bias to be low (Renko 2007).
Blinding
Neither of the trials used blinding. In this type of trial it is impossible for the surgeon, parent or child to be blind to the fact that the child has or has not had surgery. Using an episode of fever as an outcome measure is sensible and will tend to minimise bias, although a parent or carer may be biased in their decision as to whether or not to check the child's temperature. Therefore the risk of bias for blinding was unclear for both studies.
Incomplete outcome data
We judged the risk of attrition bias to be low. In one trial no children were lost to follow‐up (Garavello 2009), while missing data were limited in the other trial (Renko 2007): 2/28 children (7%) were not included in analyses at six months. These two children were equally distributed over the groups.
Selective reporting
We did not have access to study protocols and we did not have enough information to assess the risk of selective reporting bias. We noted that although Renko 2007 stated in the methods section that participants would be followed up for 12 months using patient diaries, only the six‐month results were reported. We therefore judged the risk of bias from selective reporting to be unclear.
As there were only two studies, we could not conduct formal assessment using funnel plots.
Other potential sources of bias
In one trial there appeared to be a small imbalance in the number of children without any symptoms other than fever between the tonsillectomy group and the control group: seven (50%) versus four (33%), respectively (Renko 2007). This might have some influence on the results.
Effects of interventions
The main findings are reported in summary of findings Table for the main comparison.
Primary outcomes
1. Proportion of children whose symptoms have completely resolved
As described in the Included studies section, Garavello 2009 reported the number of patients who had "immediate and persistent resolution of PFAPA syndrome" after the surgery/randomisation, which was sustained until the end of follow‐up (at 18 months): 12/19 in the surgery group and 1/20 in the control group.
For the 2014 update, we could obtain data with the same definition from the authors of Renko 2007 for the six‐month follow‐up period (their longest available follow‐up): 10/14 in the surgery group and 4/12 in the control group. Despite the difference in the length of follow‐up, we decided to pool these data in Analysis 1.1, since this measures the number of patients whose symptoms stopped immediately after surgery/randomisation.
However, it should be noted that the proportions of children who had "immediate and persistent symptom resolution" at six months follow‐up in Garavello 2009 would probably be higher than (or equal to) the numbers used in Analysis 1.1 (which used the 18‐month follow‐up data from Garavello 2009). It is possible that some children (from both arms) had symptom recurrence between six and 18 months.
The pooled risk ratio (RR) is 4.38 (95% confidence interval (CI) 0.64 to 30.11), which corresponds to a number needed to treat to benefit (NNTB) of two, if the average risks in the control groups of both studies (156 per 1000) are used as a baseline risk (Analysis 1.1). We observed substantial heterogeneity in this pooled risk ratio (I2 = 71%, P value = 0.06). Heterogeneity as measured by the I2 statistic appears to depend on the type of measure used. If the meta‐analysis is undertaken using an odds ratio (OR 11.04, 95% CI 1.77 to 69.08), the I2 value reduces to 44%; if a risk difference is used, the I2 is 0% (RD 0.52, 95% CI 0.32 to 0.72).
Apart from the length of follow‐up, the difference in recruitment criteria used could also have contributed to the heterogeneity. The risk in the control group was 5% in Garavello 2009 and 33% in Renko 2007.
The alternative way of defining and measuring resolution of symptoms was to look at number of patients who became 'symptom‐free' at a certain time point.
-
In Renko 2007, the number of patients who were symptom‐free at six months was 14/14 in the surgery group and 6/12 in the control group.
-
Garavello 2009 reported that all patients who received surgery were symptom‐free at the end of the follow‐up (18 months), but did not provide the numbers in the control group. No further information could be obtained from the authors.
Therefore, although we knew that all patients who received surgery in both studies were 'symptom‐free' at the end of their respective follow‐up periods, data for this outcome could not be analysed due to the lack of numbers provided for the control group in Garavello 2009.
2. Complications of surgery (haemorrhage and number of days of postoperative pain)
In both trials it was reported that there were "no complications" of tonsillectomy (Garavello 2009; Renko 2007). The number of days with postoperative pain was not reported in the studies.
Secondary outcomes
1. Number of episodes of fever and associated symptoms
Whilst neither study specifically reported on the severity of disease episodes, Renko 2007 reported the number of episodes of fever per person‐month and we were able to calculate the equivalent data from Garavello 2009. The results from Renko 2007 were 0.05 episodes per person‐month in the surgical group and 0.47 episodes per person‐month in the control group, based on the six‐month follow‐up period (34 events in 12 children over six months = 34/72 = 0.472, not 0.44 as reported in paper), with a corresponding rate ratio of 0.10 (95% CI 0.04 to 0.28).
Garavello 2009 reported the mean number of episodes of PFAPA during the 18‐month study period. The mean (± standard deviation) number of episodes was 0.7 ± 1.2 in the surgery group and 8.1 ± 3.9 in the control group. This was a statistically significant difference of 7.4 episodes (95% CI ‐9.19 to ‐5.61). However, these numbers are slightly different from the numbers Garavello 2009 provided in Table II of their publication, which reported a total of 12 episodes in the intervention group versus 179 episodes in the control group during the 18 months of follow‐up. We used the data provided in Table II of the paper and calculated rate data as follows: 0.04 episodes per person‐month in the surgical group and 0.50 episodes per person‐month in the control group, based on the 18‐month follow‐up period (rate ratio 0.07, 95% CI 0.04 to 0.13). When the results from the two studies are combined (Analysis 1.2), the summary rate ratio is 0.08 (95% CI 0.05 to 0.13) (I2 = 0%). This represents a 92% reduction in the number of episodes per patient per month in the intervention group, from an average of about one episode every two months to slightly less than one episode every two years.
This decrease in frequency and 'severity' (see below) means that over 18 months the average number of days a child in the study would experience fever and associated symptoms was 1.1 days in the surgery group and 31.3 in the control group, i.e. 0.06 days per month in the surgery group versus 1.7 days per month in the control group.
2. Severity of episodes
Garavello 2009 reported the mean number of days per episode among patients who still had symptoms after surgery (or randomisation, in the case of control group patients) until the end of follow‐up. This was 1.7 days (range 2 to 4) in the surgery group versus 3.5 days (range 2 to 5) in the control group.
3. Use of corticosteroids
Neither of the studies reported the number of courses of corticosteroids used.
Garavello 2009 reported that 50% of patients in the tonsillectomy group and 88% in the control group received corticosteroids, but it was unclear how many patients were included in the analysis out of the 19 recruited into the surgery arm and the 20 in the control arm. Under the assumption that all patients had been included in the analysis, this would work out as about 10/19 (53%) in the tonsillectomy group and 18/20 (90%) in the control group (RR 0.58, 95% CI 0.37 to 0.92). However, it is likely that not all patients were included in the study authors' reporting of percentages. We therefore also tested whether other possible values, such as '8/16 (50%) versus 13/15 (88%)', could be derived from these percentages. We found that these did not affect the RR and only widened the confidence intervals slightly (± 0.06).
4. Absence or time off school
Neither of the studies reported this outcome (Garavello 2009; Renko 2007).
5. Quality of life
Neither of the studies reported this outcome (Garavello 2009; Renko 2007).
Discussion
Summary of main results
Current evidence, which is derived from two small, non‐blinded randomised controlled trials (RCTs), suggests that tonsillectomy (with or without adenoidectomy) is highly effective in the management of children with periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis (PFAPA) syndrome. The risk ratio (RR) for immediate and persistent resolution of symptoms up to the end of study follow‐up periods was more than four times higher in the group receiving surgery (RR 4.38, 95% confidence interval (CI) 0.64 to 30.11). This corresponds to an absolute reduction in risk of about 50% and number needed to treat to benefit (NNTB) of two. By the end of follow‐up, both studies reported that all patients had complete resolution in the surgery group.
The effectiveness is also seen in the significant decrease in the rate of PFAPA episodes (rate ratio 0.08, 95% CI 0.05 to 0.13). In addition, surgery also seemed to improve the severity of PFAPA episodes; the average number of days per episode decreased from 3.5 days to 1.7 days in one of the studies (Garavello 2009). The same study also reported a decrease in the proportion of patients requiring corticosteroid treatment, but did not document the number of courses required by these patients.
Both studies reported that there were no complications of surgery, but these studies might be too small to detect rarer, but important, complications such as haemorrhage. The studies also did not report other important outcomes, such as number of days with postoperative pain, absence from school or quality of life.
Overall completeness and applicability of evidence
PFAPA syndrome is a rare condition so perhaps it is not surprising that only two small randomised controlled trials have evaluated the effectiveness of tonsillectomy (with or without adenoidectomy) in this condition. There were a total of 67 participants randomised in these studies and data from 65 participants were available for analysis.
These studies reported results for six months (Renko 2007) and up to 18 months (Garavello 2009), respectively. We could only obtain and analyse the number of patients who no longer had symptoms from the point of surgery up to the end of follow‐up (immediate and persistent resolution of symptoms), and we could not analyse the number of patients who were no longer symptomatic at the end of follow‐up. Garavello 2009 reported "immediate and complete resolution of PFAPA syndrome" after surgery and reported that all 19 participants in the surgery group had complete resolution of symptoms by the end of follow‐up (18 months). However, this study did not report how many participants in the control group also had complete resolution.
Although the data suggested that children who underwent surgery were more likely to be completely free of symptoms and those who still had symptoms had less prolonged episodes, it is unclear whether these advantages still persisted after 18 months. It is recognised that there is a spontaneous recovery rate and Feder 2010 reports a 20% rate, with a mean time to resolution of 33.2 months (range 8 to 92 months). The survey by Thomas 1999 followed up 83 patients of whom 34 (41%) had stopped having episodes after a mean of 4.5 years of illness.
Was the treatment provided to the control groups of these studies adequate? In the Garavello 2009 study, it has been suggested that the 'expectant treatment' with oral corticosteroids given to the control group was not adequate (Bharti 2010) and that these control patients should have been treated more 'actively'. The adequacy of the treatment provided to those in the control group in the Renko 2007 study has also been criticised (Spalding 2008). However, the greatest criticism has been levelled at the diagnostic inclusion criteria with Hofer 2008, Pignataro 2009 and Spalding 2008 suggesting that not all the children in the Renko 2007 study had classical PFAPA.
It is also uncertain whether adenoidectomy combined with tonsillectomy adds any additional benefit to tonsillectomy alone. Garavello 2009 performed adenotonsillectomy while Renko 2007 only removed the tonsils. The currently available data are insufficient to undertake a meaningful sensitivity analysis to compare the results of these two types of surgery.
Quality of the evidence
We considered the quality of the evidence (our confidence in the estimate of effects) for the key domains using the GRADE criteria: we assessed study limitations, indirectness, inconsistency, imprecision and other issues such as outcome reporting bias for each outcome (Balshem 2011).
Both studies were small and we judged the risk of bias to be low.
For the outcome of complete resolution of symptoms after surgery, the quality of evidence was moderate (further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate). A few factors contributed to this uncertainty: the sample sizes of the studies were small and there were some concerns about the applicability of the results to daily practice. One trial may have included children that did not have classical PFAPA (due to lack of stringent diagnostic inclusion criteria) and the treatment received in both control groups does not reflect current practice, which may have resulted in an overestimation of the relative efficacy of surgery.
Potential biases in the review process
Apart from the differences in patient recruitment criteria and risks of biases from study methodologies, the two studies also differed in the nature of the surgical intervention: tonsillectomy (Renko 2007) versus adenotonsillectomy (Garavello 2009). It is not possible to draw conclusions safely about the relative merits of one versus the other from the data provided (although some have tried to do so ‐ Bharti 2010). The combined procedure potentially removes a larger proportion of the tissue comprising Waldeyer's ring of lymphoid tissue. If the presence or severity of PFAPA syndrome is in some way proportional to the volume of pharyngeal lymphoid tissue, it might be expected that adenotonsillectomy would be better than tonsillectomy alone. From the practical surgical point of view there is a difference in 'risk' between the procedures in terms of operative time and postoperative morbidity, but this risk is very modest and most ENT surgeons consider it to be negligible.
Given the differences between the two study populations and the intervention, should the results be combined? Overall, the studies agree in their direction of effect for the outcomes reported and our a priori plan was to combine them, and investigate any heterogeneity should that be demonstrated.
For the primary outcome 'proportion of children whose symptoms have completely resolved' (based on 'immediate and complete resolution of symptoms' after surgery/randomisation), we observed that the degree of heterogeneity as measured by the I2 statistic depended on the choice of summary statistic used. There was large variation in the baseline risk of the control groups (5% risk in Garavello 2009 versus 50% in Renko 2007).
Agreements and disagreements with other studies or reviews
A systematic review conducted before the publication of the RCTs we have included in this review argued that tonsillectomy should not be used for patients with PFAPA (Leong 2006). The best evidence they found at the time of their review came from six retrospective reviews of case notes. The resolution rate for patients who had tonsillectomy ranged from 0% to 100%. Despite an overall success rate of more than 70% across the studies, it was felt that the evidence was too poor to justify the risk for a condition which could be treated medically or would resolve spontaneously. The RCTs included in this review provide further evidence that surgery is associated with a high rate of resolution, and provide better quality evidence to justify the procedure.
We identified another review which included a variety of study types (Peridis 2010b). However, we found a number methodological problems with the review and judged its overall quality to be low.
Although both studies in this review reported no complications observed for patients undergoing surgery, this may be because the studies were too small to capture these less common events. There are risks of primary and secondary haemorrhage, best estimated (from the UK National Tonsillectomy Audit) at 0.6% and 3% respectively (BAO‐HNS/RCSENG 2005). In addition, surgery involves the risks associated with any procedure conducted under general anaesthesia, a period in hospital (usually a day or one day and one night) and a postoperative recovery period characterised by sore throat requiring oral analgesics and lasting, in children, for several days. The child must be away from school or nursery during this period.
Process for sifting search results and selecting studies for inclusion
'Risk of bias' graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.
'Risk of bias' summary: review authors' judgements about each methodological quality item for each included study.
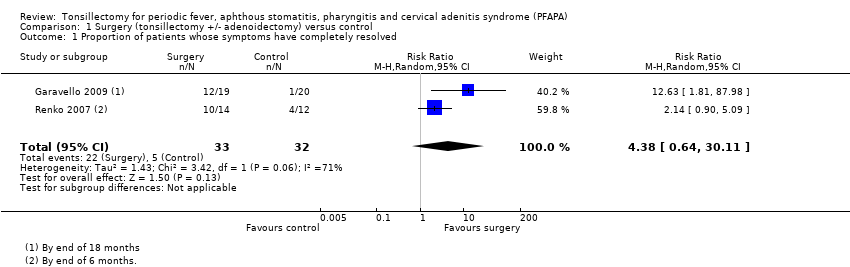
Comparison 1 Surgery (tonsillectomy +/‐ adenoidectomy) versus control, Outcome 1 Proportion of patients whose symptoms have completely resolved.
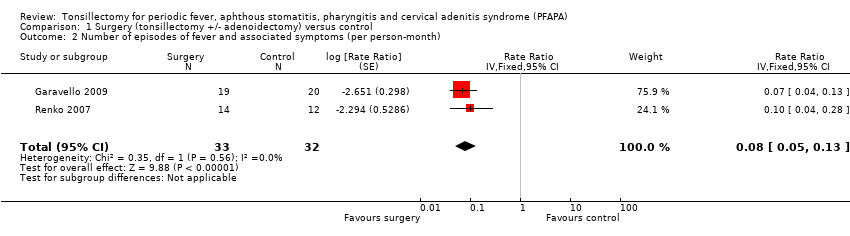
Comparison 1 Surgery (tonsillectomy +/‐ adenoidectomy) versus control, Outcome 2 Number of episodes of fever and associated symptoms (per person‐month).

Comparison 1 Surgery (tonsillectomy +/‐ adenoidectomy) versus control, Outcome 3 Use of corticosteroids.
| Surgery (tonsillectomy +/‐ adenoidectomy) for children with periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis syndrome (PFAPA) | ||||||
| Patient or population: children with PFAPA | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Surgery (tonsillectomy +/‐ adenoidectomy) | |||||
| Complete resolution of symptoms (proportion of patients with 'immediate and persistent resolution of symptoms' from the point of surgery/randomisation up to end of study follow‐up) | Study population (average) | RR 4.38 | 65 | ⊕⊕⊕⊝ | The NNTB based on the study population risk was 1/(684‐156)*1000 = 1.89 1 study followed up patients up to 6 months; another up to 18 months | |
| 156 per 1000 | 684 per 1000 | |||||
| Medium risk population | ||||||
| 192 per 1000 | 841 per 1000 | |||||
| Complications of surgery (haemorrhage and days with pain) | Both studies reported no complications from surgery Days of pain not reported as an outcome | |||||
| Number of episodes of fever and associated symptoms (episodes per person per month) | Mean 0.5 episode per person per month (1 episode every 2 months) | Mean 0.04 episode per person per month (1 episode every 25 months) | Rate ratio: 0.08 (0.05 to 0.13) | 65 | ⊕⊕⊕⊝ | |
| Severity of episodes (number of days with fever and the associated symptoms (per episode)) | Mean 3.5 (range of 2 to 6) days per episode | Mean 1.7 (range of 2 to 4) days per episode | Mean difference: 1.8 days per episode | 39 (1 study) | ⊕⊕⊕⊝ | Study reported statistical significance. Standard deviations were not reported in the study for average number of days per episode |
| Use of corticosteroids (proportion of patients using corticosteroids) | Study population (average) | RR 0.58 (0.37 to 0.92) | 39 (1 study) | ⊕⊕⊝⊝ | Review intended to report number of courses/patient, but these data were not available in the studies | |
| 900 per 1000 | 522 per 1000 | |||||
| Absence or time off school | None of the studies reported this | |||||
| Quality of life | None of the studies reported this | |||||
| *The basis for the assumed risk was the median risk in the control groups for "medium risk population" and for "study population", this was the average (i.e. total number of participants with events divided by total number of participants included in the meta‐analysis). The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1Quality (confidence in the evidence) was reduced because of the small size of the studies and broad confidence intervals. There was also concern as to whether the treatment received by the control group reflects current practice. The criteria for recruitment of patients into one of the studies was not stringent and could have included patients who did not have PFAPA (Renko 2007). | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Proportion of patients whose symptoms have completely resolved Show forest plot | 2 | 65 | Risk Ratio (M‐H, Random, 95% CI) | 4.38 [0.64, 30.11] |
| 2 Number of episodes of fever and associated symptoms (per person‐month) Show forest plot | 2 | 65 | Rate Ratio (Fixed, 95% CI) | 0.08 [0.05, 0.13] |
| 3 Use of corticosteroids Show forest plot | 1 | 39 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.58 [0.37, 0.92] |