Preparación vaginal con solución antiséptica antes de la cesárea para la prevención de las infecciones posoperatorias
Información
- DOI:
- https://doi.org/10.1002/14651858.CD007892.pub7Copiar DOI

- Base de datos:
-
- Cochrane Database of Systematic Reviews
- Versión publicada:
-
- 26 abril 2020see what's new
- Tipo:
-
- Intervention
- Etapa:
-
- Review
- Grupo Editorial Cochrane:
-
Grupo Cochrane de Embarazo y parto
- Copyright:
-
- Copyright © 2020 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Cifras del artículo
Altmetric:
Citado por:
Autores
Contributions of authors
David Haas is the guarantor for the review. Drs. Haas, Morgan, and Contreras developed the original protocol, data extraction sheet, and preparation of results and final original report and previous updates. Dr Kimball (nee Enders) was added for the 2018 update and all four authors contributed to study selection, data extraction, and preparation of results and final report for this update.
Sources of support
Internal sources
-
Indiana University School of Medicine, Indianapolis, USA
External sources
-
No sources of support supplied
Declarations of interest
David Haas is the Principal Investigator for a randomized trial included in this review (Haas 2010). He holds grants from the US National Insitute of Health for work unrelated to this review. He has no financial conflicts of interest to disclose.
Sarah Morgan is also an investigator in the Haas 2010 trial. She has no financial conflicts of interest to disclose.
Trial authors for Haas 2010 were not involved in assessing trial quality or extracting data from the Haas 2010 study. This task was carried out by Karenrose Contreras and a third party (Dr Jon Hathaway, MD, PhD).
Karenrose Contreras has no financial conflicts of interest to disclose.
Savannah Enders Kimball has no financial conflicts of interest to disclose.
Acknowledgements
The authors thank Dr Jon Hathaway for his independent assessment of trial quality and data extraction for the Haas 2010 study (original version of the review) and Erika Ota for preparing the 'Summary of findings' table for the previous version of this review (Haas 2014b). At that time, Erika Ota's work was financially supported by the UNDP/UNFPA/UNICEF/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP), Department of Reproductive Health and Research (RHR), World Health Organization.
The 'Summary of findings' table in this update was prepared by Myfanwy Williams, PhD using GradePro software (GRADEpro GDT 2015).
As part of the prepublication editorial process, this review has been commented on by four peers (an editor and three referees who are external to the editorial team) and the Group's Statistical Adviser. The authors are grateful to the following peer reviewers for their time and comments: Dr Charles Anawo Ameh, Centre for Maternal and Newborn Health, International Public Health, Liverpool School of Tropical Medicine, UK; Robert S Kerr, Department of Obstetrics and Gynaecology, St Michael’s Hospital, Bristol, UK; Carolina C Ribeiro‐do‐Valle, MD, MSc, Department of Obstetrics and Gynecology, School of Medical Sciences, University of Campinas, Campinas, Brazil.
This project was supported by the National Institute for Health Research (NIHR), via Cochrane Infrastructure funding to Cochrane Pregnancy and Childbirth. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Evidence Synthesis Programme, the NIHR, National Health Service (NHS) or the Department of Health and Social Care.
This review is supported by funding from the World Health Organization (WHO) and the UNDP‐UNFPA‐UNICEF‐WHO‐World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP) awarded to Cochrane Pregnancy and Childbirth. HRP supports and coordinates research on a global scale, synthesizes research through systematic reviews of literature, builds research capacity in low‐income countries and develops dissemination tools to make efficient use of ever‐increasing research information. In addition to its cosponsors, the International Planned Parenthood Federation (IPPF) and UNAIDS are both members of HRP’s governing body.
We wish to thank Dr Ida Envall of Stockholm, who brought a trial to our attention that had been missed in our search methodology after the 2014 update (Haas 2014b).
We thank Pisake Lumbiganon for help with translation of the methods section of Charoenviboonphan 2011.
Version history
| Published | Title | Stage | Authors | Version |
| 2020 Apr 26 | Vaginal preparation with antiseptic solution before cesarean section for preventing postoperative infections | Review | David M Haas, Sarah Morgan, Karenrose Contreras, Savannah Kimball | |
| 2018 Jul 17 | Vaginal preparation with antiseptic solution before cesarean section for preventing postoperative infections | Review | David M Haas, Sarah Morgan, Karenrose Contreras, Savannah Enders | |
| 2014 Dec 21 | Vaginal preparation with antiseptic solution before cesarean section for preventing postoperative infections | Review | David M Haas, Sarah Morgan, Karenrose Contreras | |
| 2014 Sep 09 | Vaginal preparation with antiseptic solution before cesarean section for preventing postoperative infections | Review | David M Haas, Sarah Morgan, Karenrose Contreras | |
| 2013 Jan 31 | Vaginal preparation with antiseptic solution before cesarean section for preventing postoperative infections | Review | David M Haas, Sarah Morgan, Karenrose Contreras | |
| 2010 Mar 17 | Vaginal preparation with antiseptic solution before cesarean section for preventing postoperative infections | Review | David M Haas, Sarah Morgan Al Darei, Karenrose Contreras | |
| 2009 Jul 08 | Vaginal preparation with antiseptic solution before cesarean section for preventing postoperative infections | Protocol | David M Haas, Sarah Al Darei, Karenrose Contreras | |
Differences between protocol and review
We were unable to perform three of the planned subgroup analyses as they were not reported in the trials.
In the 2018 update, we added an additional search of ClinicalTrials.gov and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) for unpublished, planned and ongoing trial reports.
In the 2018 update, we edited the list of outcomes for use in GRADE. We edited, postpartum endometritis, postoperative wound infection and postoperative fever to include definitions as per the list of outcomes in the main methods/types of outcomes. We also added 'Composite wound complications or endometritis' to our list of outcomes for use in GRADE.
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
- Administration, Intravaginal;
- Anti-Infective Agents, Local [*administration & dosage];
- Benzalkonium Compounds [administration & dosage];
- Cesarean Section [*adverse effects];
- Chlorhexidine [administration & dosage];
- Disinfection [*methods];
- Endometritis [*prevention & control];
- Fever [prevention & control];
- Povidone-Iodine [administration & dosage];
- Preoperative Care [*methods];
- Randomized Controlled Trials as Topic;
- Surgical Wound Infection [*prevention & control];
Medical Subject Headings Check Words
Female; Humans; Pregnancy;
PICO
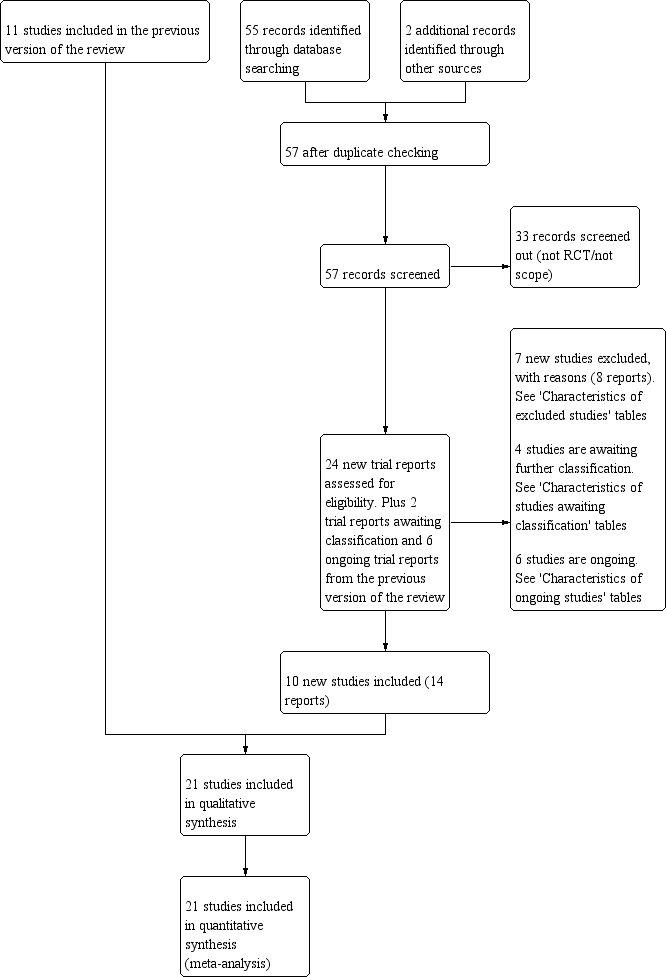
Study flow diagram.

Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.

Methodological quality summary: review authors' judgements about each methodological quality item for each included study.

Funnel plot of comparison: 1 Vaginal preparation with antiseptic solution versus control (no preparation or saline preparation), outcome: 1.1 Post‐cesarean endometritis.

Comparison 1: Vaginal preparation with antiseptic solution before cesarean section versus control (no preparation or saline preparation), Outcome 1: Post‐cesarean endometritis

Comparison 1: Vaginal preparation with antiseptic solution before cesarean section versus control (no preparation or saline preparation), Outcome 2: Postoperative fever

Comparison 1: Vaginal preparation with antiseptic solution before cesarean section versus control (no preparation or saline preparation), Outcome 3: Postoperative wound infection

Comparison 1: Vaginal preparation with antiseptic solution before cesarean section versus control (no preparation or saline preparation), Outcome 4: Composite wound complication

Comparison 1: Vaginal preparation with antiseptic solution before cesarean section versus control (no preparation or saline preparation), Outcome 5: Composite wound complication or endometritis

Comparison 2: Vaginal preparation with antiseptic solution versus control (no preparation or saline preparation) ‐ stratified by presence of labor, Outcome 1: Post‐cesarean endometritis

Comparison 2: Vaginal preparation with antiseptic solution versus control (no preparation or saline preparation) ‐ stratified by presence of labor, Outcome 2: Postoperative fever

Comparison 2: Vaginal preparation with antiseptic solution versus control (no preparation or saline preparation) ‐ stratified by presence of labor, Outcome 3: Postoperative wound infection

Comparison 2: Vaginal preparation with antiseptic solution versus control (no preparation or saline preparation) ‐ stratified by presence of labor, Outcome 4: Composite wound complication

Comparison 2: Vaginal preparation with antiseptic solution versus control (no preparation or saline preparation) ‐ stratified by presence of labor, Outcome 5: Composite wound complication or endometritis

Comparison 3: Vaginal preparation with antiseptic solution versus control (no preparation or saline preparation) ‐ stratified by presence of ruptured membranes, Outcome 1: Post‐cesarean endometritis

Comparison 3: Vaginal preparation with antiseptic solution versus control (no preparation or saline preparation) ‐ stratified by presence of ruptured membranes, Outcome 2: Postoperative fever

Comparison 3: Vaginal preparation with antiseptic solution versus control (no preparation or saline preparation) ‐ stratified by presence of ruptured membranes, Outcome 3: Postoperative wound infection

Comparison 3: Vaginal preparation with antiseptic solution versus control (no preparation or saline preparation) ‐ stratified by presence of ruptured membranes, Outcome 4: Composite wound complication

Comparison 3: Vaginal preparation with antiseptic solution versus control (no preparation or saline preparation) ‐ stratified by presence of ruptured membranes, Outcome 5: Composite wound complication or endometritis
| Vaginal preparation with antiseptic solution compared to control (no preparation or saline preparation) for preventing postoperative infections | ||||||
| Patient or population: pregnant women undergoing cesarean section | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Risk with control (no preparation or saline preparation) | Risk with vaginal preparation with antiseptic solution | |||||
| Post‐cesarean endometritis | Study population | RR 0.41 | 6918 | ⊕⊕⊕⊝ | ||
| 72 per 1000 | 30 per 1000 | |||||
| Postoperative fever | Study population | RR 0.64 | 6163 | ⊕⊕⊕⊝ | ||
| 120 per 1000 | 77 per 1000 | |||||
| Postoperative wound infection | Study population | RR 0.62 | 6385 | ⊕⊕⊕⊝ | ||
| 61 per 1000 | 38 per 1000 | |||||
| Composite wound complication or endometritis | Study population | RR 0.46 | 499 | ⊕⊕⊕⊝ | ||
| 135 per 1000 | 62 per 1000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| aThere is some funnel plot asymmetry. Having conducted sensitivity analyses to investigate the contribution of small studies and studies at high risk of bias, we do not believe that the effect estimate has been biased by possible missing results due to non‐publication. We did not downgrade. | ||||||
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1.1 Post‐cesarean endometritis Show forest plot | 20 | 6918 | Risk Ratio (M‐H, Random, 95% CI) | 0.41 [0.29, 0.58] |
| 1.1.1 Iodine‐based solution | 16 | 6197 | Risk Ratio (M‐H, Random, 95% CI) | 0.41 [0.28, 0.60] |
| 1.1.2 Chlorhexidine‐based solution | 4 | 721 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.16, 0.89] |
| 1.2 Postoperative fever Show forest plot | 16 | 6163 | Risk Ratio (M‐H, Random, 95% CI) | 0.64 [0.50, 0.82] |
| 1.2.1 Iodine‐based solution | 14 | 5763 | Risk Ratio (M‐H, Random, 95% CI) | 0.66 [0.50, 0.87] |
| 1.2.2 Chlorhexidine‐based solution | 2 | 400 | Risk Ratio (M‐H, Random, 95% CI) | 0.44 [0.23, 0.83] |
| 1.3 Postoperative wound infection Show forest plot | 18 | 6385 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.62 [0.50, 0.77] |
| 1.3.1 Iodine‐based solution | 15 | 5767 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.64 [0.50, 0.81] |
| 1.3.2 Chlorhexidine‐based solution | 3 | 618 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.53 [0.31, 0.90] |
| 1.4 Composite wound complication Show forest plot | 2 | 729 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.63 [0.37, 1.07] |
| 1.5 Composite wound complication or endometritis Show forest plot | 2 | 499 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.46 [0.26, 0.82] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 2.1 Post‐cesarean endometritis Show forest plot | 7 | 2677 | Risk Ratio (M‐H, Random, 95% CI) | 0.47 [0.27, 0.81] |
| 2.1.1 Women in labor | 6 | 1634 | Risk Ratio (M‐H, Random, 95% CI) | 0.35 [0.19, 0.67] |
| 2.1.2 Women not in labor | 5 | 1043 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.33, 2.21] |
| 2.2 Postoperative fever Show forest plot | 5 | 2233 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.55, 0.95] |
| 2.2.1 Women in labor | 5 | 1415 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.42, 0.87] |
| 2.2.2 Women not in labor | 3 | 818 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.60, 1.43] |
| 2.3 Postoperative wound infection Show forest plot | 5 | 2233 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.57 [0.37, 0.88] |
| 2.3.1 Women in labor | 5 | 1415 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.52 [0.30, 0.90] |
| 2.3.2 Women not in labor | 3 | 818 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.35, 1.31] |
| 2.4 Composite wound complication Show forest plot | 2 | 729 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.64 [0.38, 1.09] |
| 2.4.1 Women in labor | 2 | 314 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.77 [0.36, 1.61] |
| 2.4.2 Women not in labor | 2 | 415 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.54 [0.25, 1.16] |
| 2.5 Composite wound complication or endometritis Show forest plot | 2 | 499 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.47 [0.27, 0.85] |
| 2.5.1 Women in labor | 2 | 164 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.34 [0.13, 0.87] |
| 2.5.2 Women not in labor | 2 | 335 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.60 [0.29, 1.26] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 3.1 Post‐cesarean endometritis Show forest plot | 9 | 2634 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.41 [0.30, 0.55] |
| 3.1.1 Women with ruptured membranes | 5 | 552 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.23 [0.12, 0.45] |
| 3.1.2 Women with intact membranes | 8 | 2082 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.48 [0.34, 0.68] |
| 3.2 Postoperative fever Show forest plot | 8 | 2474 | Risk Ratio (M‐H, Random, 95% CI) | 0.54 [0.38, 0.78] |
| 3.2.1 Women with ruptured membranes | 4 | 480 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.22, 0.80] |
| 3.2.2 Women with intact membranes | 7 | 1994 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.49, 0.99] |
| 3.3 Postoperative wound infection Show forest plot | 9 | 2634 | Risk Ratio (M‐H, Random, 95% CI) | 0.66 [0.47, 0.91] |
| 3.3.1 Women with ruptured membranes | 5 | 552 | Risk Ratio (M‐H, Random, 95% CI) | 0.54 [0.19, 1.50] |
| 3.3.2 Women with intact membranes | 8 | 2082 | Risk Ratio (M‐H, Random, 95% CI) | 0.73 [0.50, 1.07] |
| 3.4 Composite wound complication Show forest plot | 1 | 300 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.64 [0.28, 1.44] |
| 3.4.1 Women with ruptured membranes | 1 | 76 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.53 [0.15, 1.89] |
| 3.4.2 Women with intact membranes | 1 | 224 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.73 [0.25, 2.10] |
| 3.5 Composite wound complication or endometritis Show forest plot | 2 | 500 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.48 [0.27, 0.85] |
| 3.5.1 Women with ruptured membranes | 2 | 134 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.39 [0.13, 1.13] |
| 3.5.2 Women with intact membranes | 2 | 366 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.52 [0.26, 1.04] |