Hydroxyurea (hydroxycarbamide) for sickle cell disease
Abstract
Background
Sickle cell disease (SCD) is one of the most common inherited diseases worldwide. It is associated with lifelong morbidity and a reduced life expectancy. Hydroxyurea (hydroxycarbamide), an oral chemotherapeutic drug, ameliorates some of the clinical problems of SCD, in particular that of pain, by raising fetal haemoglobin. This is an update of a previously published Cochrane Review.
Objectives
To assess the effects of hydroxyurea therapy in people with SCD (all genotypes), of any age, regardless of setting.
Search methods
We searched the Cochrane Cystic Fibrosis and Genetic Disorders Group Haemoglobinopathies Register, comprising of references identified from comprehensive electronic database searches and handsearches of relevant journals and abstract books of conference proceedings. We also searched online trial registries.
Date of the most recent search: 16 January 2017.
Selection criteria
Randomised and quasi‐randomised controlled trials, of one month or longer, comparing hydroxyurea with placebo, standard therapy or other interventions for people with SCD.
Data collection and analysis
Authors independently assessed studies for inclusion, carried out data extraction and assessed the risk of bias.
Main results
Seventeen studies were identified in the searches; eight randomised controlled trials were included, recruiting 899 adults and children with SCD (haemoglobin SS (HbSS), haemoglobin SC (HbSC) or haemoglobin Sβºthalassaemia (HbSβºthal) genotypes). Studies lasted from six to 30 months.
Four studies (577 adults and children with HbSS or HbSβºthal) compared hydroxyurea to placebo; three recruited individuals with only severe disease and one recruited individuals with all disease severities. There were statistically significant improvements in terms of pain alteration (using measures such as pain crisis frequency, duration, intensity, hospital admissions and opoid use), measures of fetal haemoglobin and neutrophil counts and fewer occurrences of acute chest syndrome and blood transfusions in the hydroxyurea groups. There were no consistent statistically significant differences in terms of quality of life and adverse events (including serious or life‐threatening events). Seven deaths occurred during the studies, but the rates by treatment group were not statistically significantly different.
Two studies (254 children with HbSS or HbSβºthal also with risk of primary or secondary stroke) compared hydroxyurea and phlebotomy to transfusion and chelation; there were statistically significant improvements in terms of measures of fetal haemoglobin and neutrophil counts, but more occurrences of acute chest syndrome and infections in the hydroxyurea and phlebotomy group. There were no consistent statistically significant differences in terms of pain alteration and adverse events (including serious or life‐threatening events). Two deaths occurred during the studies (one in a the hydroxyurea treatment arm and one in the control arm), but the rates by treatment group were not statistically significantly different. In the primary prevention study, no strokes occurred in either treatment group but in the secondary prevention study, seven strokes occurred in the hydroxyurea and phlebotomy group (none in the transfusion and chelation group) and the study was terminated early.
The quality of the evidence for the above two comparisons was judged as moderate to low as the studies contributing to these comparisons were mostly large and well designed (and at low risk of bias); however evidence was limited and imprecise for some outcomes such as quality of life, deaths during the studies and adverse events and results are applicable only to individuals with HbSS and HbSβºthal genotypes.
Of the remaining two studies, one (22 children with HbSS or HbSβºthal also at risk of stoke) compared hydroxyurea to observation; there were statistically significant improvements in terms of measures of fetal haemoglobin and neutrophil counts but no statistically significant differences in terms of adverse events (including serious or life‐threatening events).
The final study (44 adults and children with HbSC) compared treatment regimens with and without hydroxyurea – there was statistically significant improvement in terms of measures of fetal haemoglobin, but no statistically significant differences in terms of adverse events (including serious or life‐threatening events). No participants died in either of these studies and other outcomes relevant to the review were not reported.
The quality of the evidence for the above two comparisons was judged to be very low due to the limited number of participants, the lack of statistical power (as both studies were terminated early with approximately only 20% of their target sample size recruited) and the lack of applicability to all age groups and genotypes.
Authors' conclusions
There is evidence to suggest that hydroxyurea is effective in decreasing the frequency of pain episodes and other acute complications in adults and children with sickle cell anaemia of HbSS or HbSβºthal genotypes and in preventing life‐threatening neurological events in those with sickle cell anaemia at risk of primary stroke by maintaining transcranial doppler velocities. However, there is still insufficient evidence on the long‐term benefits of hydroxyurea, particularly in preventing chronic complications of SCD, recommending a standard dose or dose escalation to maximum tolerated dose. There is also insufficient evidence about the long‐term risks of hydroxyurea, including its effects on fertility and reproduction. Evidence is also limited on the effects of hydroxyurea on individuals with HbSC genotype. Future studies should be designed to address such uncertainties.
PICO
Plain language summary
Hydroxyurea (also known as hydroxycarbamide) for people with sickle cell disease
Review question
What is the effect of hydroxyurea on clinical outcomes (changes in pain crises, life‐threatening illnesses, survival, haemoglobin levels, quality of life and side effects) in people with sickle cell disease (SCD) of any genotype?
Background
SCD is an inherited genetic disorder that creates problems with haemoglobin (the substance in red blood cells that carries oxygen around the body). The disease can be inherited in different ways; people can inherit two sickle genes (HbSS genotype) or they can inherit the sickle gene from one parent and a different haemoglobin gene (such as haemoglobin C (HbSC genotype) or a beta thalassaemia gene (HbSβ+ or HbSβºthal genotype)) from the second parent.
In people with SCD the abnormal sickle haemoglobin forms long polymers (chains) within the red blood cells when they become de‐oxygenated. This damages the red blood cells and makes them stickier, leading to blockages and reduced blood flow, causing pain and organ damage. Fetal haemoglobin stops these polymers forming in the sickle haemoglobin within the red blood cell. The drug hydroxyurea is used to raise fetal haemoglobin and can reduce the effects of the disease. This is an update of a previously published Cochrane Review.
Search date
The evidence is current to 16 January 2017.
Study characteristics
We included eight studies (899 adults and children with SCD (HbSS, HbSC or HbSβºthal genotypes)). Studies lasted from six to 30 months.
Key results and quality of the evidence
In four studies, 577 adults and children with SCD were randomly selected to receive hydroxyurea or placebo. In two studies, 254 children with SCD, who were also at an increased risk of having a first or second stroke, were randomly selected to receive hydroxyurea and phlebotomy (collection of blood) or blood transfusion and chelation (administration of agents to remove excess iron from the body). These six studies only recruited people with HbSS or HbSβºthal genotypes so results do not apply to people with the HbSC genotype.
There was moderate quality evidence from these six studies that those receiving hydroxyurea experienced significant reductions in the frequency of pain crises, increases in fetal haemoglobin and decreases in neutrophil (white blood cell) counts compared to the comparator treatment. There was no difference between people receiving hydroxyurea or other treatments in terms of quality of life, deaths during the studies and side effects (including serious and life‐threatening side effects); however, there is less information about these outcomes in the studies, so the quality of this evidence is low.
Two further studies were included in the review. In one study, 22 children with SCD, who were also at an increased risk of having a stroke, were randomly selected to receive hydroxyurea or no treatment (observation only) and in one study 44 adults and children were randomly selected to receive treatments with or without adding hydroxyurea. Both studies showed an increase in fetal haemoglobin for people receiving hydroxyurea compared to the comparator treatment and there were no deaths during the studies. There was no difference between people receiving hydroxyurea or other treatments in terms of pain crises and side effects (including serious or life‐threatening side effects) and these studies did not measure quality of life. The quality of the evidence from these studies is very low, given the studies were very small and only recruited around 20% of the intended number of people and results do not apply to all people with SCD (different genotypes).
Conclusions
The evidence shows that hydroxyurea is likely to be effective in the short term at decreasing the frequency of painful episodes and raising fetal haemoglobin levels in the blood in people with SCD. Hydroxyurea is also likely to be effective in preventing first strokes for those at an increased risk of stroke and does not seem to be associated with an increase in any side effects (including serious and life‐threatening side effects).
There is currently not much evidence on whether hydroxyurea is beneficial over a long period of time, what the best dose to take is, or whether treatment causes any long‐term or serious side effects. More studies are needed to answer these questions.
Authors' conclusions
Summary of findings
| Hydroxyurea compared with placebo for sickle cell disease | ||||||
| Patient or population: adults and children with sickle cell disease Settings: outpatients Intervention: hydroxyurea Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Hydroxyurea | |||||
| Pain alteration1 Follow‐up: 6 ‐ 24 months | See comment | See comment | NA | 577 (4 studies)2 | ⊕⊕⊕⊝ | All studies showed a significant advantage to hydroxyurea compared to placebo (different measures of pain alteration presented)1. |
| Life‐threatening illness Follow‐up: 6 ‐ 24 months | See comment | See comment | NA | 552 (3 studies) | ⊕⊕⊕⊝ | Significantly fewer occurrences of ACS (2 studies) and transfusions (3 studies) on hydroxyurea compared to placebo. No significant differences in terms of stroke, hepatic or splenic sequestration (two studies). |
| Death during the study (all deaths) Follow‐up: 6 ‐ 24 months | 26 per 1000 | 10 per 1000 (0 to 51 per 1000) | RR 0.39 (0.08 to 1.96) | 577 (4 studies)2 | ⊕⊕⊕⊝ | There was also no significant difference between groups in terms of deaths related to SCD. |
| Measures of HbF (%) Follow‐up: 6 ‐ 24 months | See comment | See comment | NA | 577 (4 studies)2 | ⊕⊕⊕⊝ | There was a significant increase in HbF(%) in the hydroxyurea group compared to the placebo group in all studies (different measures presented)3. |
| Measures of ANC Follow‐up: 6 ‐ 24 months | See comment | See comment | NA | 517 (3 studies)2 | ⊕⊕⊕⊝ | There was a significant decrease in ANC in the hydroxyurea group compared to the placebo group in all studies (different measures presented)3. |
| Quality of life: 'Health Status Survey' the 'Profile of Mood States' and the 'Ladder of Life' Follow‐up: 24 months | See comment | See comment | NA | up to 277 (1 study) | ⊕⊕⊝⊝ low5,6 | No significant difference in terms of any domain of any scale except for pain recall at 18 months (MD 0.70, 95% CI 0.11 to 1.29, P = 0.02)4. |
| Adverse events or toxicity: differences in rates of specific adverse events Follow‐up: 6 ‐ 24 months | See comment | See comment | NA | 577 (4 studies)2 | ⊕⊕⊝⊝ low5,7 | Significantly fewer events of dactylitis and gastroenteritis on hydroxyurea compared to placebo. No significant differences between groups in terms of all other events. |
| The basis for the assumed risk is the event rate in the control group unless otherwise stated in the comments and footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
|
| ||||||
| Hydroxyurea and phlebotomy compared to transfusion and chelation for people with sickle cell disease and an increased risk of stroke | ||||||
| Patient or population: adults and children with sickle cell disease and an increased risk of stroke Settings: outpatients Intervention: hydroxyurea and phlebotomy Comparison: transfusion and chelation | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Transfusion and chelation | Hydroxyurea and phlebotomy | |||||
| Pain alteration: proportion experiencing serious VOC or sickle‐related pain events Follow‐up: 24 to 30 months | 213 per 1000 | 718 per 1000 (339 to 1000 per 1000) | RR 3.37 (95% CI 1.59 to 7.11) | 254 (2 studies) | ⊕⊕⊝⊝ low4,5 | No significant difference between treatment groups in terms of all pain events (serious and non‐serious) in 1 study (RR 1.03, 95% CI 0.81 to 1.30). |
| Life‐threatening illness Follow‐up: 24 ‐ 30 months | See comment | See comment | NA | 254 (2 studies) | ⊕⊕⊕⊝ | No significant difference between groups in life‐threatening neurological events, hepatobiliary disease and splenic sequestration; significantly more ACS and infections and infestations in the hydroxyurea and phlebotomy compared to the transfusion and chelation group. |
| Death during the study (all deaths) Follow‐up: 24 ‐ 30 months | 1 death occurred in the transfusion and chelation group of 1 study1. | 1 death occurred in the hydroxyurea and phlebotomy group of 1 study1. | RR 0.99 (95% CI 0.06 to 15.42) | 254 (2 studies) | ⊕⊕⊝⊝ low4,5 | |
| Measures of HbF (%) Follow‐up: 24 to 30 months | See comment | See comment | NA | 254 (2 studies) | ⊕⊕⊕⊝ | There was a significant increase in HbF(%) in the hydroxyurea and phlebotomy group compared to the transfusion and chelation group for both studies (different measures presented)2. |
| Measures of ANC Follow‐up: 24 to 30 months | See comment | See comment | NA | 254 (2 studies) | ⊕⊕⊕⊝ | There was a significant decrease in ANC in the hydroxyurea and phlebotomy group compared to the transfusion and chelation group for both studies (different measures presented)2. |
| Quality of life | Outcome not reported3 | NA | ||||
| Adverse events or toxicity: differences in rates of specific adverse events | See comment | See comment | NA | 254 (2 studies) | ⊕⊕⊝⊝ low4,6 | There was a statistically significant difference in terms of immune disorders (more in transfusion and chelation group), reticulocytopenia, neutropenia and anaemia (more in hydroxyurea and phlebotomy group) in 1 study and the rate of adverse events was balanced across groups in the other study. |
| The basis for the assumed risk is the event rate in the control group unless otherwise stated in the comments and footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1. Absolute data presented for number of deaths as the confidence interval of the relative effect very large due to the small number of events. | ||||||
| Hydroxyurea compared with observation for people with sickle cell disease and an increased risk of stroke | ||||||
| Patient or population: adults and children with sickle cell disease and an increased risk of stroke Settings: outpatients Intervention: hydroxyurea Comparison: observation | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Observation | Hydroxyurea | |||||
| Pain alteration Follow‐up: NA | Outcome not reported | NA | ||||
| Life‐threatening illness Follow‐up: 15 months | See comment | See comment | NA | 22 (1 study) | ⊕⊝⊝⊝ | No significant differences between groups in terms of ACS, blood transfusions required or acute splenic sequestration. |
| Death during the study Follow‐up: 15 months | No deaths occurred | No deaths occurred | NA | 22 (1 study) | ⊕⊝⊝⊝ | |
| Measures of HbF Follow‐up: 15 months | See comment | See comment | NA | 22 (1 study) | ⊕⊝⊝⊝ | There was a significant increase in HbF in the hydroxyurea group compared to the observation group1. |
| Measures of ANC Follow‐up: 15 months | See comment | See comment | NA | 22 (1 study) | ⊕⊝⊝⊝ | There was a significant decrease in ANC in the hydroxyurea group compared to the observation group1. |
| Quality of Life Follow‐up: NA | Outcome not reported2 | NA | ||||
| Adverse events or toxicity: differences in rates of specific adverse events Follow‐up: 15 months | See comment | See comment | NA | 22 (1 study) | ⊕⊝⊝⊝ | No significant differences between groups in terms of transient neutropenia, reticulocytopenia, parasite infestation, headache and dizziness. |
| The basis for the assumed risk is the event rate in the control group unless otherwise stated in the comments and footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1. Median values reported so data cannot be entered into analysis. | ||||||
| Hydroxyurea compared with no hydroxyurea for sickle cell disease | ||||||
| Patient or population: adults and children with sickle cell disease Settings: outpatients Intervention: hydroxyurea Comparison: no hydroxyurea | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| No hydroxyurea | Hydroxyurea | |||||
| Pain alteration Follow‐up: NA | Outcome not reported | NA | ||||
| Life‐threatening illness Follow‐up: NA | Outcome not reported | NA | ||||
| Death during the study Follow‐up: 11 months | No deaths occurred | No deaths occurred | NA | up to 44 (1 study)1 | ⊕⊝⊝⊝ | |
| Measures of HbF Follow‐up: 24 weeks | See comment | See comment | NA | up to 44 (1 study)1 | ⊕⊝⊝⊝ | There was a significant increase in HbF in the hydroxyurea group compared to the no hydroxyurea group1. |
| Measures of ANC Follow‐up: 24 weeks | See comment | See comment | NA | up to 44 (1 study)1 | ⊕⊝⊝⊝ | There was no significant difference in ANC between treatment groups1. |
| Quality of life Follow‐up: NA | Outcome not reported | NA | ||||
| Adverse events or toxicity Follow‐up: 11 months | See comment | See comment | NA | up to 44 (1 study)1 | ⊕⊝⊝⊝ | Vaso‐occlusive pain crises, headache / migraine, upper respiratory infection, skin rash diarrhoea and abdominal pain were the most common adverse events during the trial and these events were evenly distributed across treatment groups (not separated by group). |
| The basis for the assumed risk is the event rate in the control group unless otherwise stated in the comments and footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| 1. Due to the factorial design of the study (22 participants randomised to a treatment arm including hydroxyurea and 22 randomised to a treatment arm without hydroxyurea), results are not entered into analysis. All results of this trial are considered exploratory (CHAMPS 2011). | ||||||
Background
Description of the condition
Haemoglobinopathies, including sickle cell disease (SCD), are among the most common inherited disorders in the world. SCD affects people originating from sub‐Saharan Africa, Arab countries, the Mediterranean, the Indian subcontinent, the Caribbean and South America, as well as African‐Americans and descendants from immigrants from the above countries in other parts of the world. The genetic mutation gives carriers some advantage against malaria and for this reason has persisted. There is an estimated global birth rate of around 300,000 affected individuals per year, the majority of which are in Africa (Piel 2013). There are an estimated 90,000 to 100,000 individuals with SCD in the USA and approximately 12,000 to 15,000 in the UK (Brousseau 2010; Hassell 2010; NICE 2012).
Haemoglobin is responsible for transporting oxygen around the body packaged in red blood cells. SCD is caused by the recessive inheritance of abnormal haemoglobins. People who inherit only one sickle gene and the normal gene for adult haemoglobin (HbA) are sickle cell carriers (sickle cell trait or AS) and are healthy. When people are homozygous, because they have inherited two sickle genes (SS), they have sickle cell anaemia, which is a variable clinical condition, with the vast majority of individuals suffering some pain attacks and a reduced life expectancy. Clinically significant SCD also arises when people inherit the sickle gene from one parent and another variant haemoglobin gene from the second parent such as haemoglobin C (SC) or a beta thalassaemia gene (Sβ+ or Sβ0). Sickle haemoglobin, when not carrying oxygen, polymerises distorting the red blood cell into the classic 'sickle' shape. The clinical problems arise predominantly as a result of chronic anaemia and the blockage of small blood vessels, which stops oxygen delivery to the tissues causing pain or organ damage or both.
The most frequent clinical problem is pain which causes over 90% of acute hospital admissions (Brozovic 1987) and significant morbidity in the community (Fuggle 1996). Other acute complications include acute chest syndrome, stroke, splenic sequestration, priapism and an increased risk of infection. SCD is a multi‐organ disease with a high chronic disease burden which increases with increasing age. The majority of individuals are anaemic with haemoglobin levels of 60 to 90g/L in HbSS. Common chronic complications include chronic sickle lung damage, pulmonary hypertension, renal dysfunction, chronic bony damage (avascular necrosis), retinopathy and leg ulceration (Howard 2015).
Whilst the majority of those affected used to die in childhood, and still do within parts of the developing world (Chakravorty 2015; Grosse 2011), death rates in children in higher‐income countries have fallen over the past decades and the majority of children (over 95%) now survive to adulthood (Quinn 2010; Telfer 2007; van der Plas 2011). Data from the USA reviewing national mortality data from 1979 to 2005 has confirmed this decrease in mortality in children, but showed an increased mortality rate in adults with a median age of death of 42 years for women and 38 years for men (Lanzkron 2013). Earlier data from the USA showed a median survival for adults with HbSS in the USA of 42 years in men and 46 years in women and in HbSC of 60 years and 68 years, respectively (Platt 1994). This contrasts with Jamaican figures which show median survival for HbSS of 53 years for men and 58.5 years for women (Wierenga 2001) and recent single‐centre data from the UK has shown median survival of 67 years in people with HbSS and higher in those with HbSC (Gardner 2016). Data from the USA has also shown an increase in deaths following transition from paediatric to adult services (Quinn 2010). Death is generally SCD‐related and is caused either by chronic organ failure consequent to the sickling process (e.g. renal failure, pulmonary hypertension, hepatic failure) (Manci 2003) or as a result of an acute catastrophic event, such as stroke (Powars 1983), acute sickle chest syndrome, splenic sequestration (Rogers 1978), sepsis (Manci 2003; van der Plas 2011) or other complications (Gray 1991; Lanzkron 2013; Perronne 2002). The UK National Confidential Enquiry into Patient Outcome and Death (NCEPOD) report reviewed UK mortality data over 48 months and found six paediatric and 40 adult deaths. One paediatric death was due to pneumococcal sepsis and two were due to sub‐arachnoid haemorrhage. In adults the main causes of death were stroke, multi‐organ failure, acute chest syndrome, renal failure and non‐sickle causes (NCEPOD 2008).
Improvements in paediatric outcomes are related to the introduction of neonatal screening, early enrolment in comprehensive paediatric care, penicillin prophylaxis, vaccination to decrease life‐threatening infection and primary stroke prevention with transcranial Doppler screening. In adults, treatment has relied on the avoidance of factors that precipitate crisis (including dehydration, infection and cold), and symptomatic treatment of the acute painful episodes (Davies 1997a; Davies 1997b; Steinberg 1999; STOP 2006). Hydroxyurea is currently the only licensed treatment for SCD. Blood transfusion is often required and may be used to treat acute complications or in the long term to treat or prevent disease complications. Haemopoeitic stem cell transplantation is the only currently available curative treatment option and is offered to children with severe disease phenotype and an human leukocyte antigen (HLA)‐matched sibling donor. Other donor transplant options and adult transplant are currently only available in the context of clinical trials. Gene therapy offers another potential curative treatment and is currently being investigated in clinical trials.
Description of the intervention
Hydroxyurea (also known as hydroxycarbamide) is an anti‐neoplastic oral drug and an inhibitor of ribonucleotide reductase (BABY HUG 2011). The drug has been shown to have many beneficial effects for treating SCD; including increasing fetal haemoglobin (HbF) concentration in red blood cells, improving nitric oxide metabolism, reducing red cell‐endothelial interaction and erythrocyte density (Ware 2010). Such disease‐modifying effects have been shown to decrease episodes of pain, acute chest syndrome, hospital admissions and the need for transfusions among people with SCD (MSH 1995; Strouse 2008); however, frequent monitoring of the person's blood count is required, in addition to monitoring of toxicity. There are recognised, but mostly reversible, side effects of hydroxyurea, such as low neutrophil count, low platelet count, anaemia, rash, headache and occasionally nausea. Furthermore, it may have teratogenic effects and may have an effect on male fertility (Strouse 2008;Zimmerman 2004). Long‐term or serious adverse effects (or both) of hydroxyurea are rare (Steinberg 2010; Strouse 2008) and observational data suggest a survival advantage for those treated with hydroxyurea (Steinberg 2010; Voskaridou 2010).
How the intervention might work
It has long been recognised that raised HbF levels can ameliorate the clinical effects of SCD (Perrine 1978; Platt 1994). HbF levels are high at birth and decrease over the first year of life and and hence clinical manifestations are often delayed until the HbF levels decrease. In addition, individuals who inherit high levels of HbF display a milder disease phenotype. This is because the HbF interferes with the polymer formation of the sickle haemoglobin within the red blood cell. This polymerisation is the underlying pathology in SCD. The more HbF there is, the greater the inhibition. Hydroxyurea was first shown to raise HbF levels in SCD in the 1980s (Platt 1984; Veith 1985). Its intermittent toxicity on the bone marrow leads to a stress response and enhanced erythropoiesis and levels of HbF. In addition to its effects on SCD via HbF enhancement, hydroxyurea also improves blood flow and reduces vaso‐occlusion via other mechanisms including decrease of adhesion molecules and stimulation of nitric oxide production (Green 2014).
Why it is important to do this review
It is important to examine as a whole, the body of work relating to the use of hydroxyurea in SCD, to evaluate the drug's effectiveness and tolerability in adults and children, and in the different types of SCD, the dosage regimens and whether the setting appears to influence the outcome, i.e. high‐income versus low‐ and middle‐income countries. We aim to review any evidence relating to the impact of hydroxyurea on the natural history of SCD and life expectancy.
Objectives
The aims of this review are to determine whether the use of hydroxyurea in people with SCD:
-
alters the pattern of acute events, including pain;
-
prevents, delays or reverses organ dysfunction;
-
alters mortality and quality of life;
-
is associated with adverse effects.
In addition we hoped to assess whether the response to hydroxyurea in SCD varies with type of SCD, age of the individual, duration and dose of treatment and healthcare setting.
Methods
Criteria for considering studies for this review
Types of studies
All randomised or quasi‐randomised studies, irrespective of language. Studies with quasi‐randomised methods, such as alternation, were included if there was sufficient evidence that the treatment and control groups were similar at baseline.
Types of participants
This review is limited to studies of hydroxyurea in SCD only. In order to fully quantify the potential harm and toxicity of this drug, a further review may need to be undertaken in all patient groups treated with hydroxyurea.
People of any age with SCD (SS, Sβ₀, SC, Sβ+) proven by electrophoresis and sickle solubility test, with family studies or DNA tests as appropriate.
Types of interventions
Hydroxyurea in any formulation at all doses, compared to either placebo or standard treatment (no placebo) for periods of one month or longer.
Types of outcome measures
Primary outcomes
-
Pain alteration
-
frequency, duration, severity measured on self‐reported patient scales
-
health service utilisation (e.g. inpatient days, outpatient or accident and emergency department visits)
-
opioid use
-
-
Life‐threatening illness (e.g. acute chest syndrome, stroke and acute splenic sequestration)*
-
Death during the study
* In the 2017 update of the review, serious adverse events reported in included studies (whether treatment‐related or not) were included under the definition of 'Life‐threatening illness'.
Secondary outcomes
-
Measures of fetal haemoglobin (HbF or F cells) and neutrophil counts
-
Other surrogate markers of response (e.g. haemoglobin, mean cell volume, platelet count and growth)
-
Quality of life, time loss to school or employment, integration into society, scales recording feeling of well‐being and global function (e.g. Karnofsky)
-
Measures of organ damage (e.g. spleen (pitted red cells), chronic sickle lung disease (transfer factor), liver, chronic renal failure (creatinine), priapism, leg ulcer, neurological damage (e.g. intelligence quotient (IQ)))
-
Any reported adverse effects or toxicity
Search methods for identification of studies
We searched for all relevant published and unpublished trials without restrictions on language, year or publication status.
Electronic searches
Relevant studies were identified from the Cochrane Cystic Fibrosis and Genetic Disorders Group's Haemoglobinopathies Trials Register using the terms: sickle cell AND hydroxyurea.
The Haemoglobinopathies Trials Register is compiled from electronic searches of the Cochrane Central Register of Controlled Trials (Clinical Trials) (updated each new issue of the Cochrane Library) and weekly searches of MEDLINE. Unpublished work is identified by searching the abstract books of five major conferences: the European Haematology Association conference; the American Society of Hematology conference; the British Society for Haematology Annual Scientific Meeting; the Caribbean Public Health Agency Annual Scientific Meeting (formerly the Caribbean Health Research Council Meeting); and the National Sickle Cell Disease Program Annual Meeting. For full details of all searching activities for the register, please see the relevant section of the Cochrane Cystic Fibrosis and Genetic Disorders Group's website.
Date of the most recent search of the Group's Haemoglobinopathies Trials Register: 16 January 2017.
We also searched the following trials registries on 20 March 2017.
ClinicalTrials.gov using the following search terms: hydroxyurea AND sickle.
WHO International Clinical Trials Registry Platform (ICTRP) using the following search terms: hydroxyurea AND sickle.
Searching other resources
The bibliographic references of all retrieved studies and reviews were assessed for additional reports of studies.
Data collection and analysis
Selection of studies
For the initial review, two authors (SCD and AO) independently applied inclusion criteria. For the updates to this review, two authors (AJ and SJN) performed this task. There were no discrepancies between the authors' assessments.
Data extraction and management
For the initial review, two authors (SCD and AO) independently extracted the data. For the updates of the review, two authors (AJ and SJN) performed this task. There were no discrepancies between the authors' assessments.
We intended to group outcome data into those measured at three, six, twelve months and annually thereafter. When outcome data were recorded at other time periods, then consideration was given to examining these as well.
Assessment of risk of bias in included studies
For the initial review, two authors (SCD and AO) independently assessed the methodological quality of each trial using the Cochrane Risk of Bias tool (Higgins 2011). For the updates of the review, two authors (AJ and SJN) performed these tasks. The authors assessed methodological quality on the methods of concealment and generation of randomisation sequence, blinding, whether data were available to analyse on intention‐to‐treat basis and whether all randomised participants were included in the analysis. There were no discrepancies between the authors' assessments.
Measures of treatment effect
For binary outcomes, we aimed to calculate a pooled estimate of the treatment effect for each outcome across studies, (the risk of an outcome among treatment allocated participants to the corresponding risk among controls). For each study, we calculated risk ratios (RR) with 95% confidence intervals (CI) for all important, dichotomous outcomes. We present RR in preference to odds ratios (OR), as OR give an inflated impression of the size of effect where event rates are high, as is the case of these studies. For the continuous outcomes, we aimed to calculate a pooled estimate of treatment effect, using the mean difference (MD).
Unit of analysis issues
One study was cross‐over in design (Belgian Study 1996). We planned to analyse data from this study using the approach recommended by Elbourne (Elbourne 2002); extracting and analysing data from paired analyses if possible.
Outcomes were measured at different time points throughout the course of the MSH study. Methods to analyse aggregate longitudinal data if individual patient data are not available are discussed by Jones (Jones 2009); however, data presented did not allow the use of these methods therefore we have carried out analysis at each individual time point reported.
Dealing with missing data
In order to allow an intention‐to‐treat analysis, we collected data by allocated treatment groups, irrespective of compliance, later exclusion (regardless of cause) or loss to follow‐up.
Assessment of heterogeneity
We assessed clinical heterogeneity by reviewing the differences across trials in the characteristics of recruited participants and treatment protocols. We assessed statistical heterogeneity using a Chi² test for heterogeneity. We assessed heterogeneity using the Q test (P < 0.10 for significance) and the I² statistic (greater than 50% indicating considerable heterogeneity (Higgins 2003)) and visually by inspecting forest plots.
Data synthesis
We analysed data using the fixed‐effect model, if we had found considerable heterogeneity (I² statistic > 50%) then we would have examined it using a random‐effects model and subgroup analyses.
Subgroup analysis and investigation of heterogeneity
We intended to perform subgroup analyses according to age (infant, child, adult etc), type of SCD (SS, Sβ₀, SC, Sβ+), dosage regimen (study specific) and setting (community, hospital, outpatient, etc), however, available data did not allow for these analyses.
Sensitivity analysis
We planned a sensitivity analysis based on the methodological quality of the studies, including and excluding quasi‐randomised studies. However, no quasi‐randomised studies were included in the review, therefore, no sensitivity analyses were performed.
Summary of findings and quality of the evidence (GRADE)
In a post hoc change from the protocol, we have presented four summary of findings tables, one for each comparison of the review (summary of findings Table for the main comparison; summary of findings Table 2; summary of findings Table 3; summary of findings Table 4).
-
Hydroxyurea compared to placebo for participants with SCD
-
Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and an increased risk of stroke
-
Hydroxyurea compared to observation for participants with SCD and an increased risk of stroke
-
Hydroxyurea compared to no hydroxyurea for participants with SCD
The following outcomes were reported in all tables (chosen based on relevance to clinicians and consumers): pain alteration; life‐threatening illnesses; deaths during the study; measures of fetal haemoglobin (HbF or F cells) and neutrophil counts, quality of life and adverse events or toxicity.
We determined the quality of the evidence using the GRADE approach; and downgraded evidence in the presence of a high risk of bias in at least one study, indirectness of the evidence, unexplained heterogeneity or inconsistency, imprecision of results, high probability of publication bias. We downgraded evidence by one level if we considered the limitation to be serious and by two levels if very serious.
For clarity in the tables, where outcomes were presented using different measures (e.g. pain alteration) or different domains (e.g. quality of life or adverse events), a general statement is made in the table regarding the summary of findings for these outcomes and the evidence is graded based on all of the measures or sub domains combined.
Results
Description of studies
Results of the search
See Figure 1 for PRISMA study flow diagram.
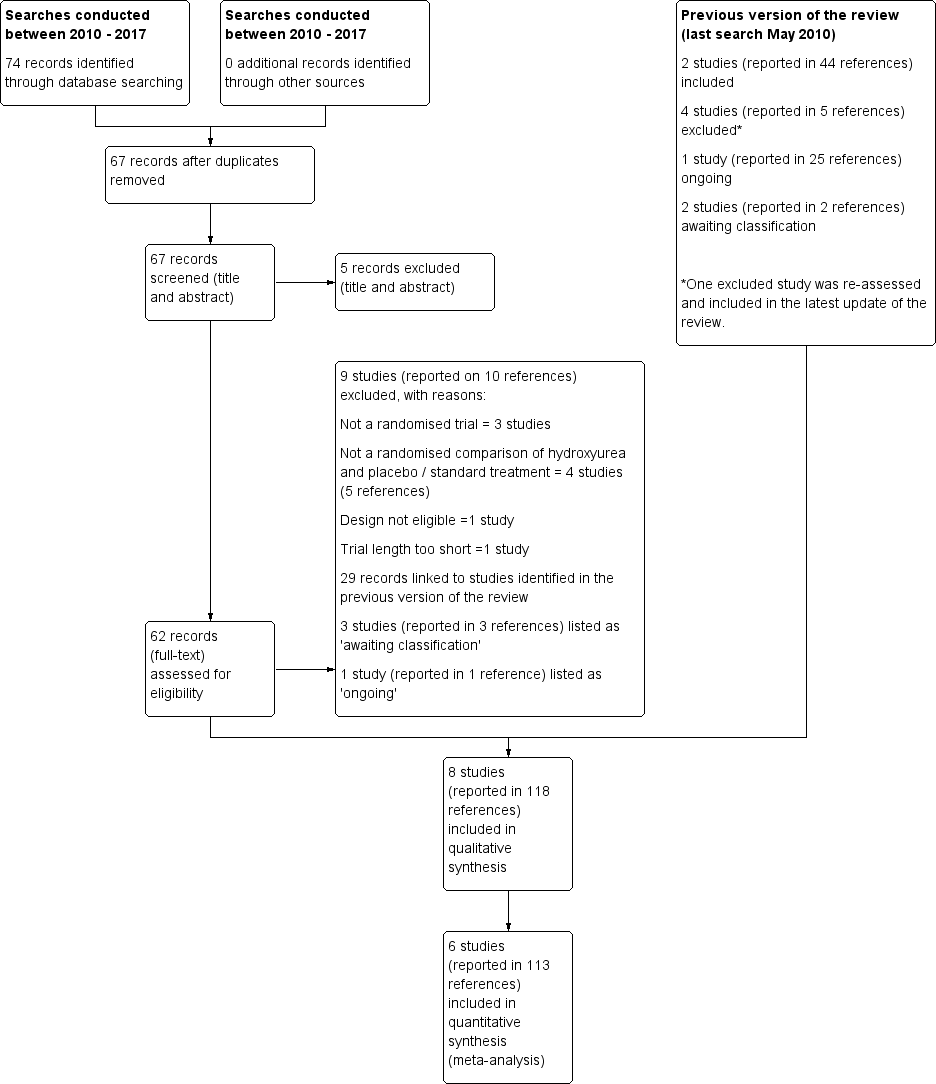
Study flow diagram.
The previous versions of the review (Jones 2001, latest search conducted May 2010) included two studies reported in 44 references (Belgian Study 1996; MSH 1995); additionally, one ongoing study (23 references) was identified (now completed) (BABY HUG 2011). Furthermore, two studies (two references) were listed as awaiting classification (CHAMPS 2011; Jain 2012).
Searches conducted between June 2010 and January 2017 identified 74 records, seven of which were duplicates. Following removal of these, 67 records were screened and five clearly irrelevant records were excluded based on title and abstract. The remaining 62 records were further screened, full texts were accessed where possible. A total of 29 records were linked to studies previously identified (BABY HUG 2011; Belgian Study 1996; CHAMPS 2011; Jain 2012; MSH 1995), nine studies (reported in 10 references) were excluded (see Excluded studies for further details), three studies (reported in three references) were listed as 'awaiting classification' due to uncertainties around the study design and population (see Characteristics of studies awaiting classification for further details) and one study (reported in one reference) was listed as 'ongoing' (see Characteristics of ongoing studies for further details).
The remaining 19 references corresponded to three new studies which were eligible for inclusion (SCATE 2015; SWiTCH 2012; TWiTCH 2016) and one reference previously excluded from the previous version of the review (Ware 2006) was re‐assessed and included under the SWiTCH study (SWiTCH 2012). The three studies previously identified as ongoing or awaiting classification are now also eligible for inclusion in the review (BABY HUG 2011; CHAMPS 2011; Jain 2012)
In total, eight studies (reported in 118 references) are included in the review (BABY HUG 2011; Belgian Study 1996; CHAMPS 2011; Jain 2012; MSH 1995; SCATE 2015; SWiTCH 2012; TWiTCH 2016).
Included studies
Eight studies are included, with a total of 899 children and adults (BABY HUG 2011; Belgian Study 1996; CHAMPS 2011; Jain 2012; MSH 1995; SCATE 2015; SWiTCH 2012; TWiTCH 2016)
The BABY HUG study was a multicentre, randomised, controlled study conducted in 13 centres in the USA (BABY HUG 2011). It was conducted in children aged nine months to 18 months who had haemoglobin SS (HbSS) or haemoglobin Sβºthalassaemia (HbSβºthal). Participants received liquid hydroxyurea (20 mg/kg per day) or matching placebo for two years administered as an oral syrup. A total of 193 children were randomised, 96 were randomised to the hydroxyurea group and 97 were randomised to the placebo group. Participants, caregivers and medical coordinating centre staff were masked to treatment allocation and an unmasked "primary end‐point person" monitored laboratory values and assisted in clinical management.
The Belgian Study was conduced in a single centre in Belgium (Belgian Study 1996). This involved 25 children and young adults with HbSS genotype with the aim of reviewing the impact on pain events, hospitalisation and also on fetal haemoglobin reactivation. This study was also placebo‐controlled, randomised and blinded to the participant but not to the caring physician. In addition, this was a cross‐over study which started at 20 mg/kg per day and, unless cytopenia developed this was raised to a maximum of 25 mg/kg per day. In this study the participants were randomised to either hydroxyurea or placebo for the initial six months and then crossed over to the other arm. There was no statistically significant period or carry‐over effect present for the outcomes of the number of hospitalisations and the number of days in hospital (period and carry‐over effects assessed by the Wilcoxon Rank Sum test).
The CHAMPS study was a randomised multicentre, phase II, double blind placebo‐controlled study with a 2x2 factorial design (CHAMPS 2011). Eligible participants were over the age of five years with HbSC and at least one vaso‐occlusive event in the previous 12 months (but none in the four weeks prior to study entry). A total of 44 participants were randomised equally across four treatment groups for 44 weeks: hydroxyurea (20 mg/kg per day) and magnesium (0.6 mmol/kg per day in two doses), hydroxyurea (20 mg/kg per day) and placebo, placebo and magnesium (0.6 mmol/kg per day in two doses), placebo and placebo. The study was not designed to measure efficacy and measured only laboratory measures.The study was terminated early due to low enrolment after 44 participants had been randomised (target 188).
The Jain study was a double blind (participants, personnel and outcome assessors) randomised controlled study conducted in a tertiary hospital in Nagpur City, India (Jain 2012). The study was conducted in children with sickle cell anaemia (proportion with each genotype not stated) between the ages of five and 18 years with three or more blood transfusions or vaso‐occlusive crises requiring hospitalisation per year despite high HbF. A total of 60 participants were randomised; 30 to hydroxyurea (fixed dose 10 mg/mg per day) and 30 to a matched placebo for 18 months.
The MSH study was a multicentre North American randomised and double‐blind study, which compared hydroxyurea with placebo over two years in adults with sickle cell anemia (SS genotype only) with the objective of reducing the frequency pain crises (MSH 1995). A total of 299 participants were randomised; 152 to hydroxyurea and 147 to matching placebo. Hydroxyurea was started at low dose (15 mg/kg per day) and increased at 12‐weekly intervals by 5 mg/kg per day until mild bone marrow depression, as judged by either neutropenia or thrombocytopenia, at that point the treatment was stopped (as reported for the MSH study) (Handy 1996). Once the blood count had recovered, treatment was restarted at 2.5 mg/kg per day less than the toxic dose. The study was therefore aiming for the maximum tolerated dose (MTD) for each individual within the study. The study was blinded and the study centre recorded and held the mean corpuscular volume (MCV) and HbF levels, which were not looked at by the caring physicians as the MCV and HbF levels rise in most people with SS taking hydroxyurea. As a result of the beneficial effects observed in terms of the primary pain outcome, as reported for the MSH study (Barton 1996), the study was stopped by the National Heart, Lung and Blood Institute of the USA at a mean follow‐up of 21 months, before the planned 24 months of treatment had been completed for all participants (MSH 1995). Long‐term follow‐up continued for the study sample, with all participants offered treatment with hydroxyurea.
The SCATE (Sparing Conversion to Abnormal transcranial doppler (TCD) Elevation) study was a Phase III multicentre, randomised, controlled study conducted in three centres in the USA, Jamaica and Brazil (SCATE 2015). The study was conducted in children with sickle cell anemia (SS, Sβº, HbSOArab, HbSD), haemoglobin SS (HbSS) or haemoglobin Sβº thalassaemia and conditional TCD ultrasound velocities (170 cm to 199 cm per second). A total of 22 participants were randomised; 11 to hydroxyurea at 20 mg/kg with escalation to maximum dose of 35 mg/kg and 11 to standard treatment (observation). The primary aim of the study was to establish whether treatment with hydroxyurea could prevent conversion from conditional to abnormal time averaged mean velocity (TAMV) and subsequent stroke in these children. The planned length of follow‐up was 30 months but the study was terminated after 15 months of follow‐up due to slow participant accrual and the unlikelihood of meeting the trial recruitment target (100) and the primary endpoint.
The SWiTCH study was a non‐inferiority study, comparing hydroxyurea and phlebotomy to standard treatment (transfusion and chelation) using a composite endpoint including secondary stroke prevention and improved management of iron overload. It included children with SCA (HbSS and HbSβºthal, HbSOArab) and previous stroke, who had been receiving chronic transfusions for at least 18 months (SWiTCH 2012). It was conducted in 26 sickle cell centres across the USA and a total of 134 children were randomised (67 to the standard treatment and 67 to the hydroxyurea and phlebotomy group). Participants randomised to hydroxyurea and phlebotomy commenced hydroxyurea at 20 mg/kg with escalation to MTD (defined by dose causing mild myelosuppression). Transfusion continued for four to nine months during hydroxyurea dose escalation. Once MTD was reached and transfusion stopped, phlebotomy of 10 mL/kg monthly was performed, if haemoglobin was sufficient.
The TWiTCH study was a multicentre phase III randomised open label (partially masked) non‐inferiority study conducted at 26 paediatric hospitals and health centres in the USA and Canada (TWiTCH 2016). Eligible participants were children aged four to 16 years with SCA (HbSS, HbSβºthal, HbSOArab) and abnormal TCD ultrasound velocities (≥ 200 cm per second) if they had received 12 months of chronic transfusions. A total of 121 participants were randomised; 60 to hydroxyurea starting at 20 mg/kg per day escalated to the MTD compared to standard treatment (transfusions) for 24 months. Children randomised to the standard treatment group received their usual chelation therapy or deferasirox to manage iron overload. Children randomised to the hydroxyurea group continued to receive transfusions until hydroxyurea was escalated to the MTD and following the discontinuation of transfusions, children received serial phlebotomy to manage iron overload. The primary aim of the study was to establish whether treatment with hydroxyurea could prevent primary stroke in these children. The study was terminated at the first interim analysis when non‐inferiority was demonstrated; the target sample size had been recruited by this point.
Excluded studies
Following the 2010 search for the previous version of the review (Jones 2001), four studies (reported in five references) were excluded from the review (De Montalembert 2006; Silva‐Pinto 2007; Voskaridou 2005; Ware 2006). However, as described above (Results of the search), for the present version of the review, the Ware reference was reassessed and included under the SWiTCH study (SWiTCH 2012).
In total, 12 studies (14 references) were excluded from the current review; five were not randomised (Al‐Nood 2011; Pushi 2000; Silva‐Pinto 2007; Silva‐Pinto 2014; Voskaridou 2005), four did not make a randomised comparison of hydroxyurea and placebo or standard treatment (George 2013; NCT00004492; NCT01960413; Vichinsky 2013), two were of one week of less duration (De Montalembert 2006; NCT01848925) and one was an inappropriate design for measuring the effectiveness of hydroxyurea (NCT02149537).
Risk of bias in included studies
See Figure 2 and Characteristics of included studies for more information.
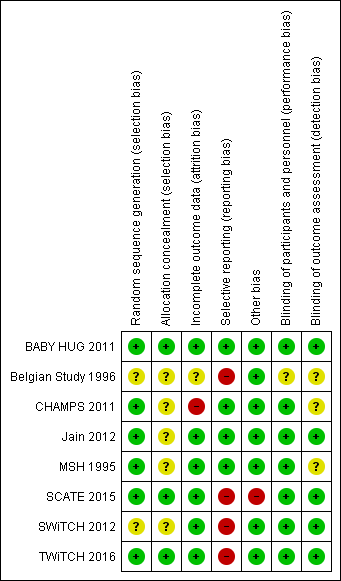
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
One study used an automated telephone response system to randomise participants using lists that had been produced by the medical co‐ordinating centre (BABY HUG 2011). The SCATE and TWiTCH studies used blocked randomisation and central pharmacy allocation (SCATE 2015;TWiTCH 2016 ). All three studies have been assessed as having a low risk of bias.
The MSH study used computerised block randomisation, the Jain trial used random number tables and the CHAMPS study used a sequential allocation algorithm for randomisation (low risk of bias) but none of these studies clearly stated any method of allocation concealment (unclear risk of bias) (CHAMPS 2011; Jain 2012; MSH 1995).
The Belgian study described the randomisation of participants as "drawing sealed envelopes, patients were randomly allocated to one of the following treatment sequences", therefore, the generation and the allocation of the treatment sequence are not clear from this statement (Belgian Study 1996). The hospital pharmacy provided the treatment and placebo for each participant and both were described as "indistinguishable." The SWiTCH trial did not discuss the method for randomisation or allocation concealment and therefore this has been graded as unclear (SWiTCH 2012).
Blinding
The BABY HUG study was described as 'double blind', the study paper stated that "participants, caregivers and medical coordinating centre staff were masked to treatment allocation" (BABY HUG 2011). The hydroxyurea and placebo powders were identical in terms of appearance and packaging and the liquid formulations had the same appearance and taste. In the Jain study, participants, clinicians and outcome assessors including laboratory technicians were blinded to treatment allocation with placebo capsules of identical appearance (Jain 2012). These studies were assessed as low risk of performance and detection bias.
In three studies, the blinding of participants and personnel was also not possible due to the differences between the treatments (hydroxyurea and standard treatment) (SCATE 2015; SWiTCH 2012; TWiTCH 2016). Outcome assessors were partially masked in these studies for assessments around the primary outcomes related to neurological events such as stroke. Given the objective nature of the primary outcomes of the studies judged by the blinded outcome assessors, these studies were assessed as low risk of detection bias.
The MSH study was described as double blind (physician and participant) (MSH 1995) and in the CHAMPS study, treatment was assigned in combinations of identically appearing capsules and blinding was achieved by 'over‐capsulating' tablets (CHAMPS 2011). These two studies were assessed as low risk of performance bias. The Belgian study was single‐blinded (the participant was unaware of the treatment schedule but the physician was aware of the treatment schedule) because of the difficulty of blinding the attending physician to the treatment received (Belgian Study 1996). It was not stated whether outcome assessors were blinded in any of these three studies.
Incomplete outcome data
In four studies, the risk of bias was assessed as low since withdrawals from treatment were documented, an intention‐to‐treat analysis approach in primary analyses was used and all randomised participants were included in the analysis (Jain 2012; MSH 1995; SWiTCH 2012; TWiTCH 2016).
In the BABY HUG study, an intention‐to‐treat analysis was undertaken for primary outcomes (via multiple imputation methods to account for missing data) and for safety outcomes (BABY HUG 2011). Some of the secondary outcomes were reported for only the individuals who completed the study or had data recorded for specific measurements, but given that primary and important safety outcomes were reported using an intention‐to‐treat analysis, this study was judged to be at a low risk of bias.
In the SCATE study, due to the early termination of the study, two randomised participants did not receive their allocated treatment (SCATE 2015). The primary analysis of this study used an intention‐to‐treat approach and a sensitivity analysis considered the actual treatment received so this study was also assessed as having a low risk of bias.
In the Belgian study, three participants were excluded from the analysis due to their failure to attend their monthly evaluation at four to five months (Belgian Study 1996). There was no discussion of whether or not an intention‐to‐treat analysis was used, therefore, the risk of bias was judged to be unclear.
In the CHAMPS study, only participants who completed eight weeks (primary outcome) or 44 weeks (secondary outcomes) of follow‐up were included in the results (CHAMPS 2011). This is not an intention‐to‐treat approach so this trial was judged to be at high risk of bias.
Selective reporting
Three studies defined outcomes in their methods sections, which were reported in the results, and were thus assessed as having a low risk of bias (BABY HUG 2011; Jain 2012; MSH 1995). The CHAMPS study was not designed to measure efficacy and reported only laboratory‐based outcomes; all of these outcomes were well‐defined in the methods and reported in the results, so this study was assessed to be at a low risk of bias (CHAMPS 2011).
In the primary publication of the TWiTCH study, it was stated the the secondary outcomes of neuropsychological status, quality of life and growth would be published at a later date (TWiTCH 2016). For the SWiTCH study, some outcomes (such as growth and development, functional evaluations, neurocognitive evaluations) do not yet seem to have been reported (SWiTCH 2012). As we are not able to include the results at this time, we have judged these studies to be at a high risk of selective reporting bias. If these results can be included at a later date then this judgement will be reconsidered (SWiTCH 2012; TWiTCH 2016). The final two studies planned to measure outcomes which were not reported due to difficulty in collecting the information to inform these outcomes; these studies are also judged to be at a high risk of bias (Belgian Study 1996; SCATE 2015).
Other potential sources of bias
One study was likely to be underpowered due to the early termination of the study with only 22% of the target sample size recruited (SCATE 2015). Another study recruited only 23% of the target sample size (CHAMPS 2011); however; this study was not designed to measure efficacy and analyses were intended to be exploratory, so we did not consider this study to be at high risk of bias. Another study was also terminated early at the first interim analysis, but the target sample size had been recruited at this point so we did not consider this study to be at a high risk of bias (TWiTCH 2016).
No other bias was identified for the remaining studies (BABY HUG 2011; Belgian Study 1996; Jain 2012; MSH 1995; SWiTCH 2012).
Effects of interventions
See: Summary of findings for the main comparison Summary of findings ‐ Hydroxyurea compared with placebo for sickle cell disease; Summary of findings 2 Summary of findings ‐ Hydroxyurea and phlebotomy compared to transfusion and chelation for people with sickle cell disease and an increased risk of stroke; Summary of findings 3 Summary of findings ‐ Hydroxyurea compared with observation for people with sickle cell disease and an increased risk of stroke; Summary of findings 4 Summary of findings ‐ Hydroxyurea compared with no hydroxyurea for people with sickle cell disease
For the 2017 update of the review six new studies were included (BABY HUG 2011; Jain 2012; CHAMPS 2011; SCATE 2015; SWiTCH 2012; TWiTCH 2016). Due to differences in the eligible populations and treatments in these new studies, we have made the following comparisons.
1. Hydroxyurea compared to placebo for participants with SCD
This comparison includes four studies (BABY HUG 2011; Belgian Study 1996; Jain 2012; MSH 1995).
2. Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and an increased risk of stroke
This comparison includes two studies (SWiTCH 2012; TWiTCH 2016).
3. Hydroxyurea compared to observation for participants with SCD and an increased risk of stroke
This comparison includes a single study (SCATE 2015).
4. Hydroxyurea compared to no hydroxyurea for participants with SCD
This comparison includes a single study (CHAMPS 2011). We note that this study recruits only individuals with HbSC; however, this comparison (and other comparisons) are worded to allow for future studies to be included in updates of this review which recruit individuals of all genotypes to contribute to this comparison.
We have conducted meta‐analyses for comparisons 1 and 2 (above) where appropriate and presented results narratively or in additional tables (Table 1; Table 2; Table 3; Table 4). Data are not entered into analysis for the Belgian and CHAMPS studies due to the presentation of results from cross‐over and factorial designs respectively; results are reported narratively (Belgian Study 1996; CHAMPS 2011). Long‐term follow‐up of the participants in MSH study continued for up to 17 years and many publications presented results of long‐term follow‐up (see linked reference list of the MSH study) (MSH 1995). After two years of double‐blind, placebo‐controlled therapy, all participants were offered hydroxyurea therapy, so any results reported after the MSH study period are uncontrolled. The long‐term results are not therefore analysed in this review.
| Hydroxyurea | Placebo | P value | |||
| Baseline | 18 months | Baseline | 18 months | ||
| Clinical events (number of events per participant per year) | |||||
| VOC | 12.13 (8.56) | 0.60 (1.37) | 11.46 (3.01) | 10.2 (3.24) | < 0.001 |
| Blood transfusions | 2.43 (0.69) | 0.13 (0.43) | 2.13 (0.98) | 1.98 (0.82) | < 0.001 |
| Hospitalisations | 10.13 (6.56) | 0.70 (1.28) | 9.56 (2.91) | 9.59 (2.94) | < 0.001 |
| Haematological parameters | |||||
| Hb (g/dL) | 8.1 (0.68) | 9.29 (0.55) | 8.21 (0.68) | 7.90 (0.58) | < 0.001 |
| HbF(%) | 19.8 (0.9) | 24 (5.9) | 19.21 (6.37) | 18.92 (5.77) | < 0.001 |
| Reticulocytes (x10⁵ /mm³) | 1.83 (0.96) | 1.15 (0.1) | 1.73 (0.49) | 1.81 (0.67) | < 0.001 |
| Leucocytes (x10³ /mm³) | 7.36 (6.03) | 6.54 (5.54) | 7.26 (4.91) | 7.38 (2.85) | < 0.001 |
| Platelets (x10³ /mm³) | 1.78 (0.26) | 2.01 (0.18) | 1.91 (0.21) | 2.06 (0.26) | 0.28 |
| RBC (x10⁶ /mm³) | 2.89 (0.57) | 1.98 (0.22) | 1.84 (0.47) | 3.11 (0.20) | 0.05 |
| Total bilirubin (mg/dL) | 2.32 (1.42) | 1.10 (0.42) | 2.27 (1.28) | 2.71 (0.93) | < 0.001 |
Values are mean (standard deviation) P values are calculated using independent t‐test.
Hb: haemoglobin
HbF: fetal haemoglobin
RBC: red blood count
VOC: vaso‐occlusive crises
WBC: white blood count
| Baseline | Hyrdoxyurea | Placebo | P value | ||
| 2 years | Baseline | 2 years | 2 years | ||
| WBC (10⁹/L) | 12.6 (3.4) | 9.9 (3.1) | 12.3 (3.2) | 12.2 (2.8) | 0.0001 |
| Neutrophils (10⁹/L) | 6.9 (2.4) | 4.9 (2.0) | 6.7 (2.3) | 6.4 (2.0) | 0.0001 |
| Platelets (10⁹/L) | 468 (147) | 399 (124) | 457 (130) | 423 (122) | 0.12 |
| Hb (g/dL) | 8.5 (1.4) | 9.1 (1.5) | 8.5 (1.2) | 8.5 (1.3) | 0.0009 |
| PCV (%) | 24.9 (4.4) | 27 (5) | 25.2 (4.0) | 25.1 (4.2) | 0.0007 |
| MCV (fl) | 94 (9) | 103 (14) | 93 (9) | 93 (9) | 0.0001 |
| Reticulocytes (10⁹/L) | 327 (98) | 231 (100) | 325 (94) | 300 (99) | 0.0001 |
| HbF (%) | 5 (3.5) | 8.6 (6.8) | 5.2 (3.4) | 4.7 (3.3) | 0.0001 |
| F cells (%) | 33 (17) | 48 (23) | 33 (17) | 35 (18) | 0.0001 |
| F reticulocytes | 15 (8) | 17 (9) | 15 (8) | 15 (7) | 0.0036 |
| Dense cells (%) | 14 (6) | 11 (6) | 14 (7) | 13 (7) | 0.004 |
| Creatinine (mg/dL) | 0.9 (0.3) | 1.0 (0.5) | 0.9 (0.2) | 1.0 (0.5) | 0.64 |
| Total bilirubin (mg/dL) | 3.7 (2.4) | 2.9 (2.5) | 3.7 (2.5) | 4.2 (4.6) | 0.004 |
| Direct bilirubin (mg/dL) | 0.5 (0.3) | 0.4 (0.3) | 0.5 (0.4) | 0.7 (2.2) | 0.08 |
| Aspartate aminotransferase | 44 (23) | 39 (20) | 41 (21) | 43 (27) | 0.16 |
| Alkaline phosphatase | 120 (59) | 117 (48) | 119 (67) | 119 (71) | 0.71 |
Values are mean (standard deviation) P values are calculated using independent t‐test.
Hb: haemoglobin
HbF: fetal haemoglobin
MCV: mean corpuscular volume
PCV: packed cell volume
WBC: white blood count
| Outcome | Hydroxyurea and phlebotomy group (n = 67) | Transfusions and chelation group (n = 66) | P value |
| HbF (%) | 17.9 (92 to 22.9) | ‐0.2 (‐0.8 to 0.4) | < 0.001 |
| ANC (x10⁹/L) | ‐3.3 (‐5.1 to ‐1.4) | 0.8 (‐1.3 to 2.4) | < 0.001 |
| Hb (g /dL) | 0.0 (‐0.7 to 0.7) | 0.0 (‐0.5 to 0.6) | 0.898 |
| HbA (%) | ‐50.9 (‐66.8 to ‐33.7) | 0.0 (‐12.7 to 6.7) | < 0.001 |
| HbS (%) | 35.0 (21.7 to 46.2) | 0.3 (‐7.5 to 12.3) | < 0.001 |
| MCV (fL) | 19.5 (7.5 to 28.5) | 0.1 (‐2.0 to 2.5) | < 0.001 |
| WBC (x10⁹/L) | ‐5.4 (‐8.1 to ‐2.2) | 0.2 (‐2.0 to 2.3) | < 0.001 |
| ARC (x10⁹/L) | ‐149.1 (‐231.0 to ‐19.0) | ‐11.8 (‐88.2 to 93.2) | < 0.001 |
| Platelets (x10⁹/L) | ‐83.0 (‐171.0 to ‐8.0) | ‐28.0 (‐70.0 to 18.0) | 0.0022 |
| Total bilirubin (mg/dL) | ‐1.1 (‐1.9 to ‐0.6) | 0.4 (‐0.3 to 1.2) | < 0.001 |
| LIC (mg Fe/g) | ‐1.2 (‐2.8 to 7.2) | ‐2.2 (‐5.5 to 4.9) | 0.48888 |
| Serum ferritin (ng/mL) | ‐966.0 (‐1629.0 to 49.0) | 1159.5 (‐662.0 to 2724.0) | < 0.001 |
| LDH (U/L) | ‐67.0 (‐143.0 to 7.0) | ‐8.5 (‐74.0 to 74.0) | 0.0015 |
ANC: absolute neutrophil count
ARC: absolute reticulocyte count
Hb: haemoglobin
HbA: adult haemoglobin
HbF: fetal haemoglobin
HbS: sickle haemoglobin
LDH: lactate dehydrogenase
LIC: liver iron concentration
MCV: mean corpuscular volume
WBC: white blood count
Values are median change from baseline and interquartile range. P values are calculated using Wilcoxon rank sum test.
| Outcome | Hydroxyurea (n = 11) | Observation (n = 11) | P value |
| Hb (g/dL) | 1.6 | ‐0.5 | < 0.0001 |
| MCV (fL) | 8.7 | 1 | 0.0001 |
| ARC ( x10⁹/L) | 22.7 | ‐33.2 | 0.76 |
| WBC ( x10⁹/L) | ‐4.6 | 1.3 | 0.07 |
| ANC ( x10⁹/L) | ‐2.2 | 1.4 | 0.05 |
| Platelets ( x10⁹/L) | ‐76 | ‐35 | 0.56 |
| HbF (%) | 8.9 | 0.3 | 0.002 |
| Weight (kg) | 2.5 | 1.8 | 0.51 |
| Height (cm) | 6.8 | 3.8 | 0.22 |
ANC: absolute neutrophil count
ARC: absolute reticulocyte count
Hb: haemoglobin
HbF: fetal haemoglobin
MCV: mean corpuscular volume
WBC: white blood count.
Values are median change from baseline and P values are calculated using Wilcoxon rank sum test.
Primary outcomes
1. Pain alteration
Hydroxyurea compared to placebo for participants with SCD
The MSH study defined pain crisis as a visit to a medical facility, lasting four or more hours, requiring opiate analgesia (MSH 1995). There was a statistically significant difference between the hydroxyurea group and placebo group in the mean annual crisis rate (all crises), MD ‐2.80 (95% CI ‐4.74 to ‐0.86) (P = 0.005) and for crises requiring hospitalisation, MD ‐1.50 (95% CI ‐2.58 to ‐0.42) (P = 0.007) (Analysis 1.1).
The MSH study also showed a reduction in median time (Kaplan‐Meier life table estimate) from the initiation of treatment to first painful crisis (2.76 months in the hydroxyurea arm compared with 1.35 months on placebo (Cox regression P value = 0.014), second painful crisis (6.58 months in the hydroxyurea group compared with 4.13 months on placebo (Cox regression P value < 0.0024), and third painful crisis (11.9 months in the hydroxyurea group compared with 7.04 months on placebo (Cox regression P value = 0.0002) (reported in Charache 1995). We note that the analysis of time‐to‐first, second and third painful crisis seems to treat crisis events independently which is unlikely to be a realistic assumption. Furthermore, information relating to the analgesia used by participants in this study has been reported, but has not been presented according to the groups to which the participants were randomised (reported in Ballas 1996).
The Jain study presented the number of clinical events (vaso‐occlusive crises) before and after intervention (Jain 2012). We could not calculate change from baseline in the number of clinical events so we have analysed between group data at 18 months and presented the before and after data in an additional table (Table 1). After 18 months of treatment, there was a statistically significant difference between the hydroxyurea group and placebo group, MD ‐9.60 (95% CI ‐10.86 to ‐8.34) (P < 0.00001) (Analysis 1.1).
The BABY HUG study showed a statistically significantly lower proportion of participants experiencing pain in the hydroxyurea group compared to the placebo group, RR 0.68 (95% CI 0.5 to 0.92) (BABY HUG 2011) (Analysis 1.2).
The Belgian study stated that "16 patients out of 22 (73%) did not require any hospitalisation for painful episodes when treated with hydroxyurea as compared with only 3 of 22 (14%) when treated with placebo" (Belgian Study 1996). In addition, it showed as reduction in mean hospital stay, with a stay of 5.3 days in the hydroxyurea group and 15.2 days in the placebo group. A planned outcome of 'number of days in pain' was not reported in the trial publication due to difficulties in collecting this information from participants.
Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and an increased risk of stroke
Both studies reported the number of participants experiencing 'serious' vaso‐occlusive or sickle cell (SCA)‐related pain events (SWiTCH 2012; TWiTCH 2016) and one study also reported the number of participants experiencing any vaso‐occlusive or sickle cell (SCA)‐related pain event (SWiTCH 2012)
There was a statistically significantly higher proportion of participants experiencing serious vaso‐occlusive or sickle cell (SCA)‐related pain in the hydroxyurea and phlebotomy group compared to the transfusion and chelation groups in the SWiTCH and TWiTCH studies, pooled RR 3.37 (95% CI 1.59 to 7.11) (P = 0.001) (SWiTCH 2012; TWiTCH 2016), but there was no significant difference between the groups in terms of all SCA pain events in the SWiTCH study, RR 1.03 (95% CI 0.81 to 1.30) (P = 0.81) (SWiTCH 2012) (Analysis 2.1).
Hydroxyurea compared to observation for participants with SCD and an increased risk of stroke
No information was reported for this outcome in the SCATE study (SCATE 2015).
Hydroxyurea compared to no hydroxyurea for participants with SCD
No information was reported for this outcome in the CHAMPS study (CHAMPS 2011).
2. Life‐threatening illness
Hydroxyurea compared to placebo for participants with SCD
The BABY HUG and the MSH studies provided data on the occurrence of acute chest syndrome, stroke and participants transfused (BABY HUG 2011; MSH 1995). Statistically significant advantages in the hydroxyurea group was the reduction in the occurrence of the acute sickle chest syndrome, pooled RR 0.43 (95% CI 0.29 to 0.63) (P < 0.0001), and also that fewer participants on hydroxyurea underwent transfusions, pooled RR 0.66 (95% CI 0.52 to 0.82) (P = 0.0003). There was no statistically significant difference in terms of stroke, pooled RR 0.54 (95% CI 0.12 to 2.53) (P = 0.44) (Analysis 1.3).
The MSH study reported data on hepatic sequestration and the BABY HUG study reported data on splenic sequestration, the differences between the groups were not statistically significant, RR 0.32 (95% CI 0.03 to 3.06) (P = 0.32) and RR 0.90 (95% CI 0.36 to 2.23) (P = 0.82), respectively (MSH 1995; BABY HUG 2011) (Analysis 1.3).
The Jain study presented the number of clinical events (blood transfusions and hospitalisations) before and after intervention (Jain 2012). We could not calculate change from baseline the number of clinical events so we have analysed between group data at 18 months and presented the before and after data in an additional table (Table 1). After 18 months of treatment, there was a statistically significant difference between the hydroxyurea group and placebo group in the number of blood transfusions, MD ‐1.85 (95% CI ‐2.18 to ‐1.52) (P < 0.00001) and in the number of hospitalisations, MD ‐8.89 (95% CI ‐10.04 to ‐7.74) (P < 0.00001). The duration of hospitalisation was also significantly less in the hydroxyurea group than the placebo group, MD ‐4.00 days (95% CI ‐4.87 to ‐3.13) (P < 0.00001) (Analysis 1.4).
No information was reported for this outcome in the Belgian study (Belgian Study 1996).
Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and an increased risk of stroke
The primary aim of the TWiTCH study was to prevent primary stroke; 29 neurologic events occurred during the study, 17 in the hydroxyurea group and 12 in the standard treatment group; but none were deemed to be stroke or cerebral infarcts (TWiTCH 2016). Three events in each group were deemed to be transient ischaemic attacks and worsened vasculopathy developed in one participant in the standard treatment group.
The aim of the SWiTCH study was to prevent secondary stroke; 91 new‐neurologic events were assessed for stroke and seven participants (all in the hydroxyurea treatment group) has positive stroke adjudication, one of which was fatal (SWiTCH 2012). There were also 20 transient ischaemic attack events in 15 participants (nine on transfusion and chelation and six on hydroxyurea and phlebotomy).
There was no statistically significant difference in life‐threatening neurological events between the treatment groups in either study from the analysis conducted in this review (Analysis 2.2); however, following the seven events in the hydroxyurea and phlebotomy group, the SWiTCH study was terminated following an interim analysis demonstrating the inability of the primary outcome to reduce secondary stroke occurrence while managing iron overload "within the non‐inferiority stroke margin" (SWiTCH 2012).
The SWiTCH and TWiTCH studies reported serious adverse events (including life‐threatening events) and other adverse events or toxicities separately (see Secondary outcomes for Adverse events) (SWiTCH 2012; TWiTCH 2016). Thirty‐eight participants experienced 81 serious adverse events in the SWiTCH study and 15 participants experienced 33 serious adverse events in the TWiTCH study (SWiTCH 2012; TWiTCH 2016). There were significantly more participants experiencing serious adverse events and SCD‐related adverse events in the hydroxyurea treatment groups compared to the transfusions groups; pooled RR 1.93 (95% CI 1.17 to 3.20) (P = 0.01) and RR 3.10 (95% CI 1.42 to 6.75) (P = 0.004), respectively (Analysis 2.2). There was no significant difference between groups in terms of hepatobiliary disease and splenic sequestration but serious acute chest syndrome and infections and infestations were significantly more common on hydroxyurea and phlebotomy treatment than on transfusion and chelation, pooled RR 2.84 (95% CI 1.25 to 6.42) (P = 0.01) and pooled RR 3.65 (95% CI 1.05 to 12.76) (P = 0.04), respectively (Analysis 2.2).
As the control arm of the two studies in this comparison involved blood transfusions, we did not consider the number of participants requiring blood transfusion to be a life‐threatening event for this comparison.
Hydroxyurea compared to observation for participants with SCD and an increased risk of stroke
The primary aim of the SCATE study was to prevent stroke and no strokes or transient ischaemic attacks occurred during the study. Vaso‐occlusive events (pain and acute chest syndrome) occurred more commonly in the observation arm than the hydroxyurea arm, but this was not statistically significant (SCATE 2015). There was also no statistically significant difference in cases of acute splenic sequestration or the number of participants requiring blood transfusion (Analysis 3.1).
Hydroxyurea compared to no hydroxyurea for participants with SCD
No information was reported for this outcome in the CHAMPS study (CHAMPS 2011).
3. Death during the study
Hydroxyurea compared to placebo for participants with SCD
The MSH study reported death and causes of death (MSH 1995); no deaths were reported to be related to hydroxyurea treatment. There were two deaths in the treated group and five in the placebo group including one homicide. There was no statistically significant difference between treatment and control groups for this comparison (Analysis 1.5).
There were no deaths in the remaining three studies (BABY HUG 2011; Belgian Study 1996; Jain 2012).
Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and an increased risk of stroke
In the SWiTCH study, there was one death in the standard treatment arm (pulmonary embolism) and one death in the hydroxyurea treatment arm (fatal haemorrhagic stroke) (SWiTCH 2012). There were no deaths reported in the TWiTCH study (TWiTCH 2016). There was no statistically significant difference between treatment and control groups for this comparison (Analysis 2.3).
Hydroxyurea compared to observation for participants with SCD and an increased risk of stroke
There were no deaths reported in the SCATE study (SCATE 2015).
Hydroxyurea compared to no hydroxyurea for participants with SCD
There were no deaths reported in the CHAMPS study (CHAMPS 2011).
Secondary outcomes
1. Measures of fetal haemoglobin and neutrophil counts
Hydroxyurea compared to placebo for participants with SCD
The BABY HUG study reported the change from baseline in HbF (%) and absolute neutrophil count (ANC); there was a statistically significant increase in HbF in the hydroxyurea group compared to the placebo group, MD 6.70 (95% CI 4.75 to 8.65) (P < 0.00001) (BABY HUG 2011) (Analysis 1.6) and a statistically significant decrease in ANC in the hydroxyurea group compared to the placebo group, MD ‐1.70 (95% CI ‐2.90 to ‐0.50) (P < 0.00001) (Analysis 1.8).
The Jain and MSH studies presented results before and after intervention (Jain 2012; MSH 1995). We could not calculate change from baseline so we have analysed between group data at the end of the study and presented the before and after data in additional tables (Table 1; Table 2). After the intervention, there was a statistically significant increase in HbF in the hydroxyurea group compared to the placebo group in the two studies, pooled MD 4.07 (95% CI 2.95 to 5.18) (P < 0.0001) (Analysis 1.7).
The MSH study also reported the neutrophil response after treatment; at 10 weeks and at two years there was a statistically significant decrease in neutrophil response in the hydroxyurea group compared to the placebo group, MD ‐1.90 (95% CI ‐2.51 to ‐1.29) (P < 0.0001) and MD ‐1.50 (95% CI ‐2.01 to ‐0.99) (P < 0.0001), respectively (MSH 1995) (Analysis 1.9).
One study reported an increase in HbF and a decrease in ANC after six months of hydroxyurea treatment, but did not make a comparison to the placebo group (Belgian Study 1996).
Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and an increased risk of stroke
The SWiTCH study reported the change from baseline in HbF (%) and ANC; there was a statistically significant difference between treatment groups for both of these measures (SWiTCH 2012). The results were presented as median and interquartile ranges and therefore could not be entered into a meta‐analysis; see an additional table for a summary of these results (Table 3).
The TWiTCH study reported the change from baseline in HbF (%) and ANC; there was a statistically significant increase in HbF in the hydroxyurea group compared to the placebo group, MD 15.60 (95% CI 13.41 to 17.79) (P < 0.00001) (Analysis 2.4) and a statistically significant decrease in ANC in the hydroxyurea group compared to the placebo group, MD ‐4.40 (95% CI ‐5.44 to ‐3.36) (P < 0.00001) (TWiTCH 2016) (Analysis 2.5).
Hydroxyurea compared to observation for participants with SCD and an increased risk of stroke
The SCATE study reported a significant increase in HbF and a significant decrease in ANC at last follow‐up in the hydroxyurea group compared to observation (SCATE 2015). Results were reported as median values so could not be included in analysis, see an additional table for a summary of these results (Table 4).
Hydroxyurea compared to no hydroxyurea for participants with SCD
The CHAMPS study, which included participants with HbSC only, reported a statistically significant increase in HbF for hydroxyurea treatment compared to no hydroxyurea treatment at eight weeks and 24 weeks but no statistically significant difference was observed for ANC (CHAMPS 2011). Due to the presentation of results from factorial design of the trial, results cannot be entered into analysis.
2. Other surrogate markers of response
Hydroxyurea compared to placebo for participants with SCD
The BABY HUG study reported change from baseline in haemoglobin (Hb), mean cell volume (MCV), white blood count (WBC), platelet count, absolute reticulocyte count (ARC), reticulocytes and total bilirubin (BABY HUG 2011).
There was a statistically significant increase in Hb (Analysis 1.10), MCV (Analysis 1.11) and a statistically significant decrease in WBC (Analysis 1.12), ARC (Analysis 1.13), reticulocytes (Analysis 1.14) and total bilirubin (Analysis 1.15) in the hydroxyurea group compared to the placebo group. There was no statistically significant difference between groups in platelet count (Analysis 1.16).
The Jain and MSH studies presented results before and after intervention (MSH 1995; Jain 2012). We could not calculate change from baseline so we have analysed between‐group data at the end of the study and presented the before and after data in additional tables (Table 1; Table 2). After the intervention comparing hydroxyurea and placebo groups, there was a statistically significant increase in Hb and MCV at 10 weeks and at the end of the studies (Analysis 1.17, Analysis 1.18), a statistically significant decrease in total bilirubin at the end of the studies (Analysis 1.19) reticulocytes at 10 weeks, 18 months and two years (Analysis 1.20) and a decrease in platelet count at 10 weeks, 18 months and two years which was not statistically significant (Analysis 1.21).
In terms of other laboratory measures comparing hydroxyurea and placebo groups at the end of the studies, there was a statistically significant increase in packed cell volume (Analysis 1.22), F reticulocytes (Analysis 1.23) and F cells (Analysis 1.24), a statistically significant decrease in red blood count (Analysis 1.25), white blood count (Analysis 1.26) and dense cells (Analysis 1.27) and no difference between groups in leucocytes (Analysis 1.28), creatinine (Analysis 1.29), aspartate aminotransferase (Analysis 1.30) and alkaline phosphatase (Analysis 1.31).
One study reported differences in haematologic values after six months of treatment such as Hb, MCV (both significantly increased), platelet count and WBC (both significantly decreased) but only in the hydroxyurea group without comparison to the placebo group (Belgian Study 1996).
The BABY HUG study reported change from baseline in growth, there were no significant differences between the groups in terms of height, weight or head circumference (BABY HUG 2011) (Analysis 1.32). The MSH study reported on weight gain after two years was reported in the MSH study as a mean rise of 3% in the hydroxyurea treated group and 6% in the placebo group, which was not statistically significant (MSH 1995).
Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and an increased risk of stroke
The SWiTCH study reported the change from baseline several laboratory and haematologic measurements such as Hb, MCV, WBC, platelet count and total bilirubin (SWiTCH 2012). There was a statistically significant difference between treatment groups for most of the measurements (increase in HbF, HbS, MCV and decrease in ANC, HbA, WBC, ARC, platelets, serum ferritin and LDH), except for Hb and liver iron concentration; the results were presented as median and interquartile ranges and therefore could not be entered into a meta‐analysis; see an additional table for summary of these results (Table 3).
The TWiTCH study reported the change from baseline in Hb, MCV, WBC, ARC, platelet count, total bilirubin, sickle haemoglobin, liver iron concentration, serum ferritin and lactate dehydrogenase (TWiTCH 2016). There was a statistically significant increase in MCV (Analysis 2.6) and sickle haemoglobin (Analysis 2.7) and a statistically significant decrease in Hb (Analysis 2.8), ARC (Analysis 2.9), WBC (Analysis 2.10), platelets (Analysis 2.11), total bilirubin (Analysis 2.12), liver iron concentration (Analysis 2.13), serum ferritin (Analysis 2.14) and lactate dehydrogenase (Analysis 2.15) in the hydroxyurea and phlebotomy group compared to the transfusion and chelation group,
Hydroxyurea compared to observation for participants with SCD and an increased risk of stroke
The SCATE study reported differences in haematologic values and growth values at last follow‐up (SCATE 2015). There was a statistically significant increase in Hb and MCV in the hydroxyurea group compared to the observation group. Other values were not statistically significantly different (differences the hydroxyurea group and observation group in Hb and MCV were statistically significant and other values were not significant (WBC, ANC, Platelets, ARC, HbF, weight and height)). Results were reported as median values so could not be included in analysis, see an additional table for a summary of these results (Table 4).
Hydroxyurea compared to no hydroxyurea for participants with SCD
The CHAMPS study reported statistically significant increases in MCV and Hb and a statistically significant decrease in WBC and platelets between hydroxyurea treatment and no hydroxyurea treatment at eight weeks and 24 weeks (CHAMPS 2011). No statistically significant difference was observed in red blood cell count (RBC), mean corpuscular haemoglobin concentration (MCHC) and ARC. Due to the presentation of results from factorial design of the study, results cannot be entered into analysis.
3. Quality of life
Hydroxyurea compared to placebo for participants with SCD
The MSH study has published in abstract limited quality of life data collected at six‐monthly intervals (MSH 1995, reported in Terrin 1999 and Ballas 2006). Health‐related quality of life (HQoL) was measured using three measures from the 'Health Status Survey' (nine scales), the 'Profile of Mood States' (four scales) and the 'Ladder of Life'. A lower score for each measure equated to a lower quality of life.
Changes from baseline are presented for only three measures: General Health Perception,' 'Social Function' and 'Changes in Ladder of Life' and four week score was reported for 'Pain Recall'.
There was a statistically significant advantage to hydroxyurea compared to placebo in terms of general health perception at 18 months MD 0.90 (95% CI 0.08, 1.72) (P = 0.03) (Analysis 1.33) and pain recall at 18 months, MD 0.70 (95% CI 0.11 to 1.29) (P = 0.02) (Analysis 1.34) but not at any other measured time point for either measure.
There were no statistically significant differences between the hydroxyurea and placebo groups at six months, one year, 18 months and two years for 'Social Function' and 'Changes in Ladder of Life' (Analysis 1.35, Analysis 1.36).
For the MSH study, it was reported that there were no significant differences between groups in other measures of HQoL (using a P value cut‐off for statistical significance of P < 0.01 to allow for statistical testing of multiple HQoL domains) (MSH 1995 reported in Ballas 2006). Results are presented as final scores rather than change from baseline so are not entered into analysis in this review. We encourage caution when interpreting results of these quality of life scales as not all participants contributed data towards these analyses.
No information was reported for this outcome in the remaining three studies (BABY HUG 2011; Belgian Study 1996; Jain 2012).
Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and an increased risk of stroke
Quality of life was measured in the TWiTCH study, but results have not yet been published; if results are published at a later date, they will be included in an update of this review (TWiTCH 2016). No information was reported for this outcome in the remaining study (SWiTCH 2012).
Hydroxyurea compared to observation for participants with SCD and an increased risk of stroke
Health‐related quality of life was a planned outcome in the SCATE study but was not reported due to difficulties in collecting information from participants at the early study termination date (SCATE 2015).
Hydroxyurea compared to no hydroxyurea for participants with SCD
This outcome was not reported in the CHAMPS study (CHAMPS 2011).
4. Measure of chronic organ damage
Hydroxyurea compared to placebo for participants with SCD
The MSH study reported similar rates of new leg ulcers, RR 0.85 (95% CI 0.44 to 1.64) (P = 0.64) and avascular necrosis of femur and humerus, RR 0.97 (95% CI 0.39 to 2.37) (P = 0.64), in both groups (MSH 1995). The BABY HUG study reported more participants with decreased spleen function at exit in the placebo group than the hydroxyurea group but this was not statistically significant, RR 0.72 (95% CI 0.44 to 1.16) ( P = 0.18) (BABY HUG 2011) (Analysis 1.37).
The BABY HUG study reported several measures of:
-
splenic function: diethylenetriaminepentaacetic acid glomerular filtration rate (Analysis 1.38); Howell‐Jolly body (HJB) (Analysis 1.39); pitted cells (Analysis 1.40); spleen to liver ratio of counts (Analysis 1.41); and spleen volume (Analysis 1.42);
-
renal function: creatinine (Analysis 1.43); Schwartz glomerular filtration rate (GFR) (Analysis 1.44); cystatin C (Analysis 1.45); urine osmolality (Analysis 1.46); urine pH (Analysis 1.47); urine‐specific gravity (Analysis 1.48); and total kidney volume (Analysis 1.49); and
-
central nervous system function: TCD velocity (Analysis 1.50); Bayley mental developmental index (MDI) and Bayley motor performance developmental index (PDI) (Analysis 1.51).
Several of the outcomes showed significantly fewer indications of chronic organ damage on hydroxyurea compared to placebo (Analysis 1.39; Analysis 1.40; Analysis 1.41; Analysis 1.43; Analysis 1.46; Analysis 1.48, Analysis 1.49; Analysis 1.50); however, given the number of outcomes measured and the increased probability of type I statistical error and spurious result, the statistical significance of these secondary endpoint comparisons must be carefully interpreted (BABY HUG 2011).
No information was reported for this outcome in the remaining two studies (Belgian Study 1996; Jain 2012).
Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and an increased risk of stroke
The TWiTCH study reported a measure of central nervous system function (TWiTCH 2016). Eligible participants had abnormal TCD ultrasound velocities (> 200 cm per second). The final TCD velocity was significantly lower in the hydroxyurea and phlebotomy group compared to the transfusion and chelation group, MD ‐5.00 (95% CI ‐9.16 to ‐0.84) (P = 0.02) (Analysis 2.16). This outcome was not reported in the SWiTCH study (SWiTCH 2012).
Hydroxyurea compared to observation for participants with SCD and an increased risk of stroke
The aim of the SCATE study was to prevent conversion from conditional to abnormal time averaged mean velocity (TAMV) and subsequent stroke; one participant in the hydroxyurea group and five participants in the observation group converted, this difference between groups was not statistically significant (Analysis 3.2) but there was a significantly lower TAMV in the hydroxyurea group compared to the observation group, MD ‐25.70 (95% CI ‐45.38 to ‐6.02) (P = 0.01) (SCATE 2015) (Analysis 3.3). No strokes occurred during the study.
Hydroxyurea compared to no hydroxyurea for participants with SCD
This outcome was not reported in the CHAMPS study (CHAMPS 2011).
5. Adverse effects or toxicity
As it is difficult to distinguish between adverse reactions (i.e. adverse events which are definitely drug‐related) and other adverse events which may be sickle‐ or transfusion‐related, we have reported all adverse events (or adverse effects) as they are reported in the study publications. Where possible, we have noted which adverse effects are defined as drug‐related, sickle‐related or transfusion‐related from the study publications.
Hydroxyurea compared to placebo for participants with SCD
The possible adverse effects reported in the MSH study were hair loss, skin rash, fever, gastro‐intestinal disturbance, and 'other' reported events (MSH 1995). There was no statistically significant difference between the groups with these measures (Analysis 1.52). In the MSH study, toxicity relating to the blood count was defined as less than 2500 x 10⁹ neutrophils/L, less than 95,000 x 10⁹ platelets/L, and haemoglobin concentration less than 5.3 g/dL (MSH 1995). Using these definitions 120 of the hydroxyurea‐treated participants (79%) and 54 placebo participants (37%) became 'toxic' at least once, resulting in a dose modification. Importantly, no infections were related to neutropenia and no 'bleeding' episode could be related to thrombocytopenia.
The BABY HUG study reported the proportion of participants experiencing a range of adverse events such as dactylitis, priapism, sepsis or bacteraemia, splenomegaly, ANC below 500, ANC 500 to 1250, thrombocytopaenia, severe anaemia, alanine transaminase over 150, bilirubin, creatinine, skin and subcutaneous disorders and splenic sequestration (BABY HUG 2011). The rates of these specific events were generally quite similar with only dactylitis and gastroenteritis showing any differences between the two treatment groups, with statistically significantly fewer events in the hydroxyurea group (Analysis 1.52); however, given the number of outcomes measured and the increased probability of type I statistical error and spurious group differences, the statistical significance must be carefully interpreted.
No major adverse events occurred in either group in the Jain study (Jain 2012); three participants in the hydroxyurea group experienced skin rash and two experienced nausea, but this was not a statistically significant difference compared to the placebo group (Analysis 1.52). No participants experienced alopecia, leucopenia, neutropenia, renal or hepatic toxicity.
It was stated that two children developed transient mild thrombocytopenia in the Belgian study but the treatment allocation of these children was not stated (Belgian Study 1996).
Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and an increased risk of stroke
Life‐threatening adverse events are presented above in primary outcome 2 (Analysis 2.2).
In the TWiTCH study it was stated that adverse events were balanced between the two groups, in the transfusion and chelation group there were 287 sickle‐related adverse events and 279 sickle‐related adverse events in the hydroxyurea and phlebotomy group (TWiTCH 2016). There were 19 adverse events related to chelation treatment in nine children in the control group (aminotransferases, gastrointestinal symptoms, increased serum creatinine, increased serum bilirubin, rash) and 18 adverse events related to phlebotomy in 14 children in the hydroxyurea treatment group (details not stated). No events related to hydroxyurea were reported. There was insufficient information to enter into the analysis, we hope to include any future information in an update.
In the SWiTCH study, there were a total of 1253 non‐neurological adverse events in 128 individuals, there was no statistically significant difference between groups in the number of participants experiencing any adverse event, RR 0.99 (95% CI 0.92 to 1.05) (P = 0.66) (SWiTCH 2012) (Analysis 2.17). In terms of specific events, there was no statistically significant difference between treatment arms for most events. There was a statistically significant difference in terms of immune disorders (more in the transfusion and chelation group), reticulocytopenia, neutropenia and anaemia (more in the hydroxyurea and phlebotomy group) (Analysis 2.17); however, given the number of outcomes measured and the increased probability of type I statistical error and spurious group differences, the statistical significance must be carefully interpreted.
Hydroxyurea compared to observation for participants with SCD and an increased risk of stroke
Adverse events reported in the SCATE study included transient neutropenia, reticulocytopenia, parasite infestation, headache and dizziness (SCATE 2015). There was no significant difference between treatment arms for any adverse event (Analysis 3.4)
Hydroxyurea compared to no hydroxyurea for participants with SCD
In the CHAMPS study, adverse events and toxicity were only reported for all randomised participants and not by treatment group (CHAMPS 2011). A total of 22 serious adverse events were observed in 10 participants and 293 adverse events in 38 participants. It was reported that vaso‐occlusive pain crises, headache or migraine, upper respiratory infection, skin rash diarrhoea and abdominal pain were the most common adverse events during the trial and these events were evenly distributed across treatment groups. Two individuals, one receiving hydroxyurea and one not receiving hydroxyurea experienced mild neutropenia.
Discussion
Summary of main results
Eight randomised controlled studies were eligible for inclusion in this review, with a total of 899 children and adults with sickle cell disease (SCD) (BABY HUG 2011; Belgian Study 1996; CHAMPS 2011; Jain 2012; MSH 1995; SCATE 2015; SWiTCH 2012; TWiTCH 2016). The studies included in the review made the following comparisons: hydroxyurea compared to placebo (BABY HUG 2011; Belgian Study 1996; Jain 2012; MSH 1995); hydroxyurea compared to no hydroxyurea (CHAMPS 2011); hydroxyurea and phlebotomy compared to transfusion and chelation for the prevention of primary or secondary stroke (SWiTCH 2012, TWiTCH 2016); and hydroxyurea compared to observation for participants at an increased risk of stroke (SCATE 2015).
The randomised studies comparing hydroxyurea with placebo (Belgian Study 1996; Jain 2012; MSH 1995) all showed a decrease in pain crises (albeit with slightly different criteria) in adults and children with sickle cell anaemia. The BABY HUG study also showed decreased rates of pain in the hydroxyurea group compared to placebo. This widening of inclusion criteria has had an important role in increasing indications for and use of hydroxyurea. Two studies comparing transfusion and hydroxyurea showed that transfusion was more effective in preventing 'serious' sickle‐related pain (SWiTCH 2012; TWiTCH 2016), but there was no difference in all pain events between the two groups, as reported by one study (SWiTCH 2012).
Rates of acute chest syndrome (ACS) were decreased in those taking hydroxyurea when compared with those taking placebo and this was true in adults (MSH 1995) and children (BABY HUG 2011; Jain 2012). Similar decreases were seen in transfusion rates, a surrogate for life‐threatening illness (BABY HUG 2011; Jain 2012; MSH 1995). Hydroxyurea did not prevent rates of hepatic or splenic sequestration when compared with placebo (BABY HUG 2011; MSH 1995).
The role of hydroxyurea compared with transfusion in the prevention of stroke has been investigated in two studies (SWiTCH 2012;TWiTCH 2016). The SWiTCH study included people with a previous stroke who had received at least 18 months of transfusion and randomised between ongoing transfusion therapy and hydroxyurea and phlebotomy (SWiTCH 2012). Treatment with hydroxyurea and phlebotomy was not expected to be as effective as transfusion in the reduction of secondary stroke but was expected to improve liver iron loads so a composite primary end point was used including stroke recurrence and liver iron concentration. In the 133 participants there were no strokes in the transfusion and chelation group but seven strokes (10%) in the hydroxyurea and phlebotomy group without concomitant improvement liver iron concentration leading to early trial closure. Hydroxyurea and phlebotomy were not as effective as transfusion for secondary stroke prevention. In the TWiTCH study, hydroxyurea was compared with transfusion in children with abnormal transcranial doppler (TCD) velocities who had received transfusion for at least one year and had no evidence of vasculopathy on magnetic resonance angiography (MRA) (TWiTCH 2016). Hydroxyurea was as effective as transfusion in preventing further stroke and final TCD velocity was lower in the hydroxyurea group. These findings are supported by observational data showing that in a non‐trial situation in children with abnormal TCDs who have normalised with transfusion, hydroxyurea can be used to maintain normal TCDs (Bernaudin 2016).
In the randomised studies included in this analysis there was no statistically significant differences in mortality between any treatment and control group. Follow‐up from cohorts from the MSH study have been published at nine and 17.5 years (MSH 1995), although randomisation ceased after trial closure and participants could choose whether to take hydroxyurea or not (Steinberg 2003; Steinberg 2010). These follow‐up studies both confirmed reduced mortality in the group taking hydroxyurea although the analysis was according to cumulative exposure to hydroxyurea and not the original randomisation. Further supporting evidence for reduced mortality with hydroxyurea comes from a prospective non‐randomized trial (LasHS) from Greece with 17 years of follow‐up which showed improved probability of 10‐year survival in participants who were treated with hydroxyurea (Voskaridou 2010). These results should be treated cautiously as the participants were not randomised and the analysis of mortality in an observational study is more complex.
In terms of chronic organ damage; there were no statistically significant differences in renal and splenic function (the primary outcomes of BABY HUG 2011). Hydroxyurea had no significant effect on glomerular filtration rate over the two years of treatment, but it did improve urine concentrating ability and there was less renal enlargement in the hydroxyurea‐treated groups.
Several of the randomised studies showed a statistically significant increase in HbF levels in the groups treated with hydroxyurea, in keeping with the mechanism of action of the drug. This was seen both in participants treated with the maximum‐tolerated dose (MTD) of hydroxyurea (MSH 1995;SWiTCH 2012; TWiTCH 2016) and those treated with a standard dose (BABY HUG 2011;Jain 2012). A statistically significant increase in Hb level was seen in studies which compared hydroxyurea to placebo (BABY HUG 2011; Belgian Study 1996; CHAMPS 2011; MSH 1995;Jain 2012;SCATE 2015) and a decrease in haemolytic markers with hydroxyurea treatment was seen in some of the studies (BABY HUG 2011;Jain 2012;MSH 1995).
Those studies which used dose escalation to the MTD (MSH 1995; SCATE 2015; SWiTCH 2012; TWiTCH 2016), showed greater rates of cytopenias, which are expected as the dose of the drug is raised. The MSH study showed increased haematological toxicity resulting in a dose reduction in the hydroxyurea group as compared with placebo, but there were no infections related to neutropenia or bleeding episodes due to thrombocytopenia (MSH 1995). Similarly, the SWiTCH study showed significantly increased rates of reticulocytopenia, neutropenia and anaemia in the hydroxyurea group, compared with transfusion (SWiTCH 2012). The BABY HUG study which used a standard dose of 20 mg/kg of hydroxyurea showed an increase in neutropenia (in terms of absolute neurophil count) in the hydroxyurea group but no increase in events of thrombocytopenia and no increase in the number of infections (BABY HUG 2011). There are no randomised studies comparing the effect of using a standard dose versus dose escalation to the MTD. Clearly, with careful laboratory monitoring and appropriate patient education, cytopenia should rarely represent a major issue as demonstrated.
In the randomised studies comparing hydroxyurea with placebo there was no increase in adverse events related to hydroxyurea including hair loss, skin rash, fever and gastro‐intestinal disturbance. In addition, in the MSH study there was no increase in the incidence of leg ulcers and avascular necrosis in those treated with hydroxyurea. This is important as they have both been associated with hydroxyurea use in observational reports and leg ulcers are associated with hydroxyurea use in people with myeloproliferative disease. Furthermore, observational data looking at 15 years of hydroxyurea use from infancy has not shown any concerns about safety (Hankins 2014), although as with the mortality data this is not based on randomised data and should be treated with caution.
Overall completeness and applicability of evidence
Evidence from the eight included studies is extensive and for four of the studies it is reported across many publications (BABY HUG 2011;MSH 1995; SWiTCH 2012; TWiTCH 2016). Furthermore as discussed in the Summary of main results, evidence from these randomised studies is generally supported by longer‐term or observation evidence (or both).
There are still questions about the impact of hydroxyurea on the chronic organ damage associated with SCD. Results from the BABY HUG study showed improved urine concentrating ability and less renal enlargement in the hydroxyurea‐treated groups. These results suggest that hydroxyurea may have some beneficial effect on renal function, but these results do not automatically translate into clinical benefit (BABY HUG 2011). The long‐term effect of hydroxyurea therefore, would benefit from further study, including effects on brain development, IQ, growth and development, as well as the prevention and management of chronic organ damage.
As a chemotherapeutic agent, the cytostatic effects of hydroxyurea are different from those of radiation, alkylating agents and other anti‐cancer drugs, many of which are known to increase the risk of development of either leukaemia or cancer. Long‐term follow‐up of people taking hydroxyurea for other diagnoses, including polycythaemia rubra vera (Berk 1995; Fruchtman 1994; Najean 1997), essential thrombocythaemia (Sterkers 1998) and cyanotic heart disease (Triadou 1994), has shown no increase in malignancies in those with normal bone marrows and no significant increase in the other groups. There has been no evidence of malignancy in those with SCD treated with hydroxyurea in large observational studies (Steinberg 2010; Voskaridou 2010). Small numbers of case reports have reported myelodysplasia or acute leukaemia in people with SCD treated with hydroxyurea and two of these have been associated with 17p deletions. This is of interest as 17p deletions have also been associated with the development of myelodysplasia or acute leukaemia in people with myeloproliferative disease treated with hydroxyurea (Aumont 2015; Baz 2012). In vitro work has not shown increased chromosome breakages or decreased repair in people with SCD on hydroxyurea (McGann 2011).
Concerns have been raised about whether hydroxyurea is associated with abnormal spermatogenesis and teratogenic effects but there are few data to confirm or refute that. There is a theoretical risk of hydroxyurea affecting sperm development and abnormal spermatogenesis has been shown in animals treated with hydroxyurea. Sperm abnormalities, including oligospermia and azoospermia, have been shown in males with SCD taking hydroxyurea, but it is not clear if these are due to the hydroxyurea as similar abnormalities have been described in males with SCD not taking hydroxyurea. One small study compared semen analysis before, during and after hydroxyurea treatment and showed semen parameters were affected whilst on hydroxyurea and did not seem to recover quickly (Berthaut 2008). This included only small numbers of individuals and needs further investigation.
Evidence of adverse outcomes and teratogenic effects in humans exposed to hydroxyurea in utero is limited. There is case report evidence of women with malignant disease taking hydroxyurea through pregnancy with no adverse effects on the fetus and 17‐year follow‐up of the MSH study has shown no adverse fetal outcomes in males or females taking hydroxyurea at conception (Ballas 2009) (Table 5) . An expert panel report evaluating the toxicity of hydroxyurea has led to recommendations that hydroxyurea is stopped in men and women who are trying to conceive and in breastfeeding women (National Toxicology Program 2008). The risks of stopping hydroxyurea whilst attempting conception should be carefully discussed with the individual.
| Pregnancy | Hydroxyurea | Placebo | |
| Patients | Normal full‐term delivery | 1 | 2 |
| Elective termination | 2 | 1 | |
| Partners of patients | Normal full‐term delivery | 2 | 0 |
| Spontaneous abortion | 1 | 0 | |
| Still pregnant | 0 | 1 | |
| TOTAL | 6 | 4 | |
The CHAMPS study was the only study to include participants with HbSC (CHAMPS 2011). It was not powered to measure efficacy and terminated early due to low enrolment so it is not possible to make conclusions about the efficacy of hydroxyurea in prevention of pain episodes in people with HbSC. Observational data suggest it may be safe and effective in selected individuals, but this needs further study with a phase 3 randomised study (Luchtman‐Jones 2016). A total of 165 people with HbS/B+thalassaemia were included in one observational study but only 44 received hydroxyurea and efficacy on this subgroup was not presented separately (Voskaridou 2010).
Quality of the evidence
We judged the quality of the evidence for the comparison 'Hydroxyurea compared to placebo' to be moderate for most outcomes and low for quality of life and adverse events, where data were more limited and imprecise (summary of findings Table for the main comparison).
Similarly, we judged the quality of the evidence for the comparison 'Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke' to be moderate (life‐threatening illness and measures of fetal haemoglobin and neutrophil counts) or low quality (pain alteration, deaths during the study and adverse events) where data were more limited and imprecise (summary of findings Table 2).
The studies contributing the majority of the evidence to these comparison were large, generally well designed and of low risk of bias (BABY HUG 2011; MSH 1995; SWiTCH 2012; TWiTCH 2016). These studies recruited only individuals with haemoglobin SS genotype (HbSS) or haemoglobin Sβº (HbSβº) thalassemia genotypes, therefore, results are not applicable to those with haemoglobin SC genotype (HbSC) genotypes. Furthermore, for the two most recently completed studies, results for secondary outcomes such as neuropsychological status, growth and development, functional evaluations and neurocognitive evaluations have not yet been reported. Any results relevant to this review from further publications will be included in this review.
For the other two comparisons in the review 'Hydroxyurea compared to observation for participants with SCD and risk of stroke' and 'Hydroxyurea compared to no hydroxyurea for participants with SCD,' evidence was limited and of very low quality (summary of findings Table 3; summary of findings Table 4). Only a single study contributed to each outcome and both of these studies are likely underpowered due to early termination after recruiting only around 20% of their target participants. Furthermore, due to the factorial design of one of the studies (CHAMPS 2011), a direct comparison between hydroxyurea and a control treatment was not possible so all results for this comparison must be interpreted as indirect.
Potential biases in the review process
A rigorous methodological approach was applied to the review and a comprehensive search strategy was employed as outlined in Electronic searches, therefore, we do not believe that our methodological approach has introduced any bias into the review.
Given the designs of some of the studies included in this review (e.g. cross‐over, factorial) and differing study‐defined definitions of the outcomes of interest to this review, in many instances we felt it would be more appropriate to summarise results narratively or perform separate analyses rather than attempting to adjust original results in order to perform meta‐analysis.
We encourage particular caution when interpreting results of the outcome 'adverse events or toxicity', as it is difficult to distinguish between adverse reactions (i.e. adverse events which are definitely drug‐related) and other adverse events which may be sickle‐ or transfusion‐related. For completeness, we have reported all "adverse events" or "adverse effects" as they are reported in the study publications, regardless of any noted relationship to treatment.
Agreements and disagreements with other studies or reviews
As described earlier in this section, there have been several studies supporting the findings of this review. In addition to these, numerous reviews and other studies discussing the role of hydroxyurea in SCD are available but this is the only Cochrane Review of the topic. A report from the National Institutes of Health (NIH) reviewed 414 studies reporting on the role of hydroxyurea in SCD (published up until July 2014) included five of the randomised studies included in this review (NIH 2014). In some cases in the NIH review, where a literature search was not conducted or was insufficient, the panel relied on their cumulative expertise and knowledge to make consensus‐panel recommendations as outlined below.
Strong recommendations with high‐quality evidence
-
In adults with sickle cell anaemia who have three or more sickle cell‐associated moderate to severe pain crises in a 12‐month period, treat with hydroxyurea.
-
In infants of nine to 42 months with sickle cell anaemia, offer treatment with hydroxyurea regardless of clinical severity to reduce SCD‐related complications (e.g. pain, dactylitis, ACS, anaemia).
-
To ensure proper use of hydroxyurea and maximize benefits and safety, use an established prescribing and monitoring protocol.
Strong recommendations with moderate quality evidence
-
In adults with sickle cell anaemia who have sickle cell‐associated pain that interferes with daily activities and quality of life, treat with hydroxyurea.
-
In adults with sickle cell anaemia who have a history of severe or recurrent ACS (or both), treat with hydroxyurea.
-
In adults with sickle cell anaemia who have severe symptomatic chronic anaemia that interferes with daily activities or quality of life, treat with hydroxyurea.
The group also made an additional moderate recommendation with moderate‐quality evidence that children over 42 months and adolescents with sickle cell anaemia should be offered treatment with hydroxyurea regardless of clinical severity to reduce SCD‐related complications (e.g. pain, dactylitis, ACS, anaemia). There were additional moderate and weak recommendations with low‐ and very low‐quality evidence and a consensus panel recommendation.
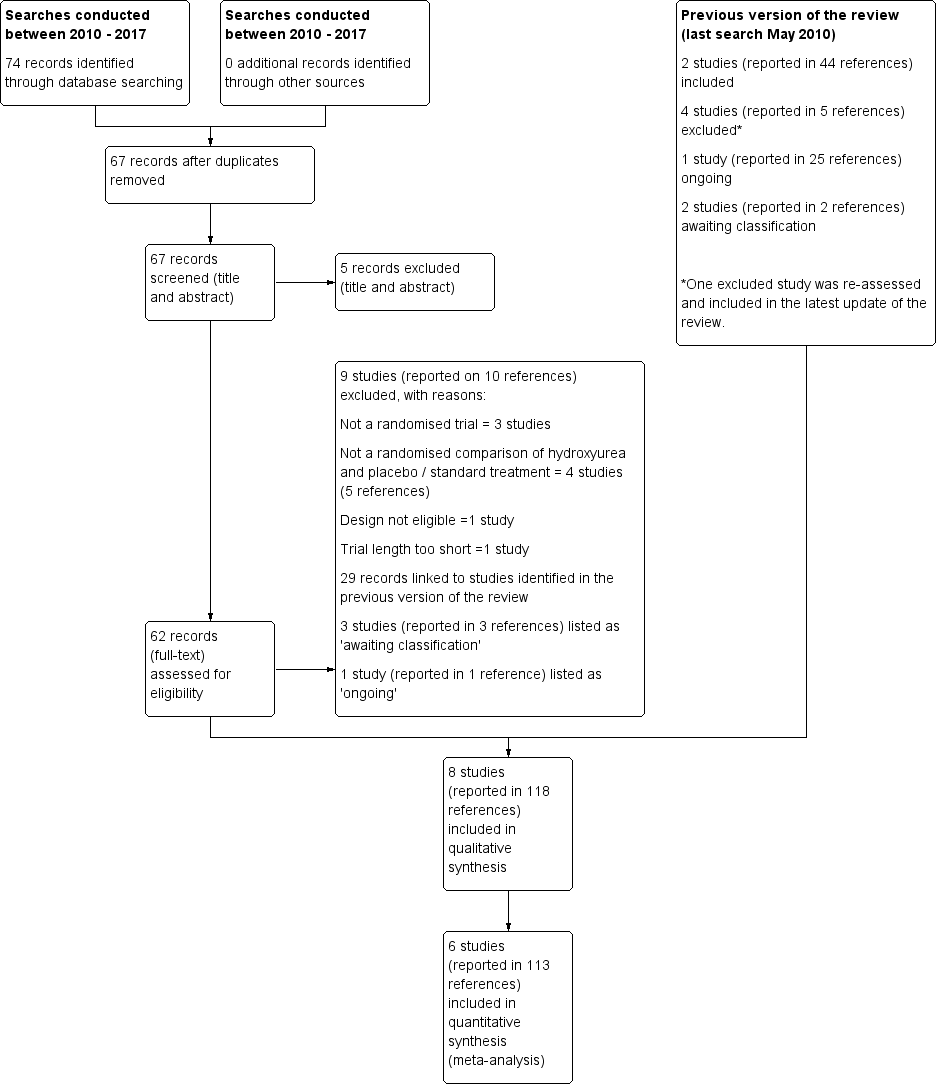
Study flow diagram.
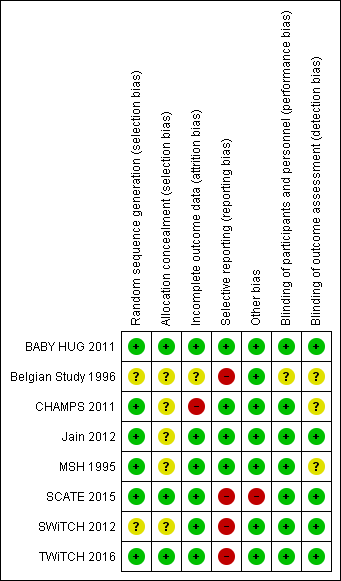
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 1 Pain crises.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 2 Proportion experiencing pain.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 3 Proportion experiencing life threatening events during study.
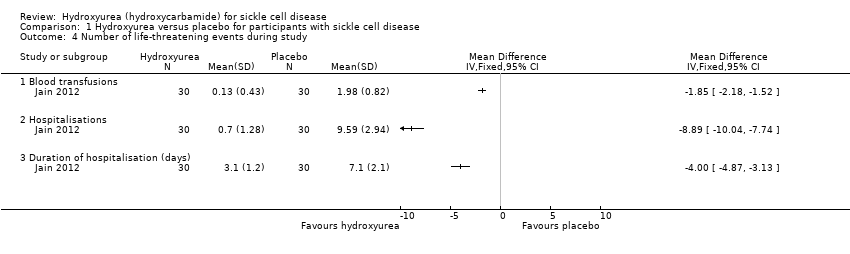
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 4 Number of life‐threatening events during study.
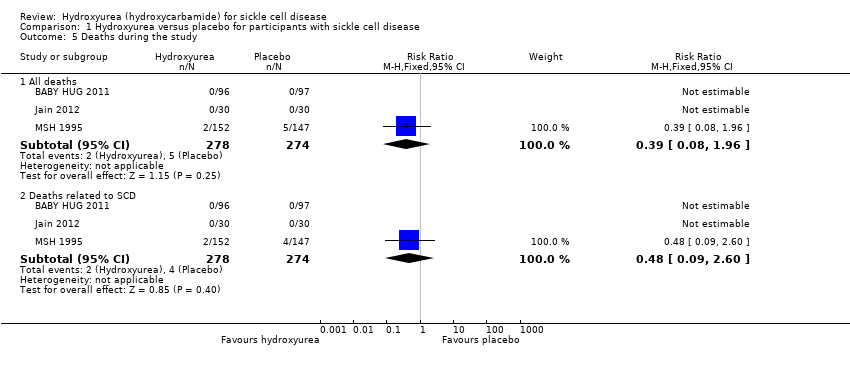
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 5 Deaths during the study.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 6 Change from baseline in fetal haemoglobin (HbF %).
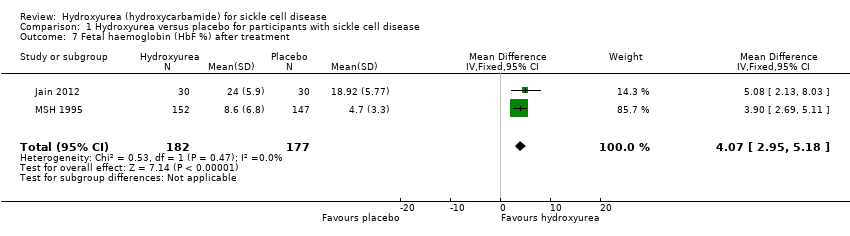
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 7 Fetal haemoglobin (HbF %) after treatment.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 8 Change from baseline in absolute neutrophil count (x10³ per μL).
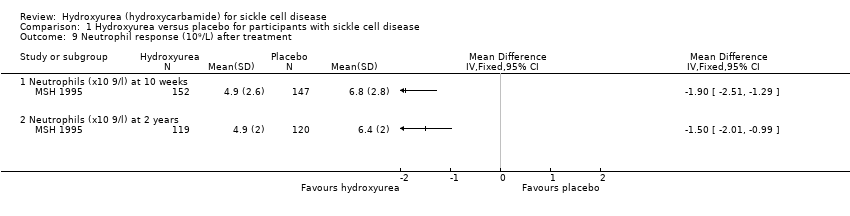
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 9 Neutrophil response (10⁹/L) after treatment.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 10 Change from baseline in haemoglobin (g/L).
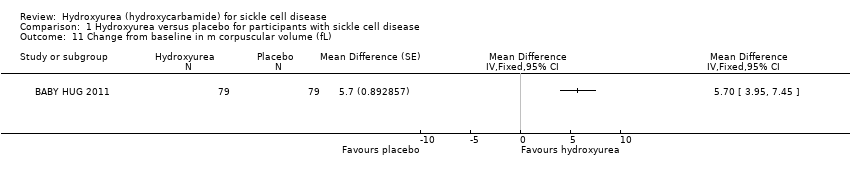
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 11 Change from baseline in m corpuscular volume (fL).
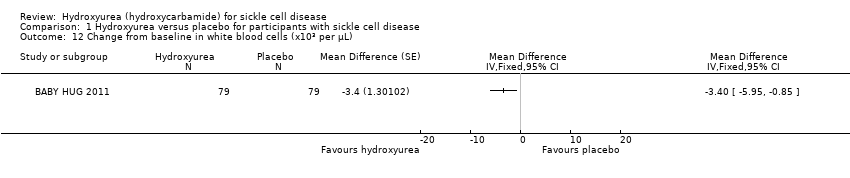
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 12 Change from baseline in white blood cells (x10³ per μL).

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 13 Change from baseline in absolute reticulocyte count (x10³ per μL).
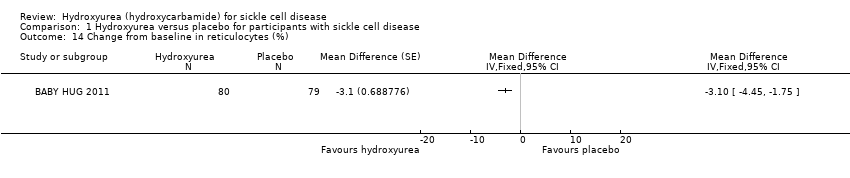
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 14 Change from baseline in reticulocytes (%).

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 15 Change from baseline in total bilirubin (mg/L).
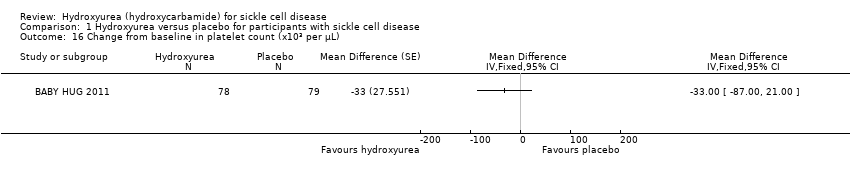
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 16 Change from baseline in platelet count (x10³ per μL).

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 17 Haemoglobin (g/dL).

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 18 Mean corpuscular volume (fL).
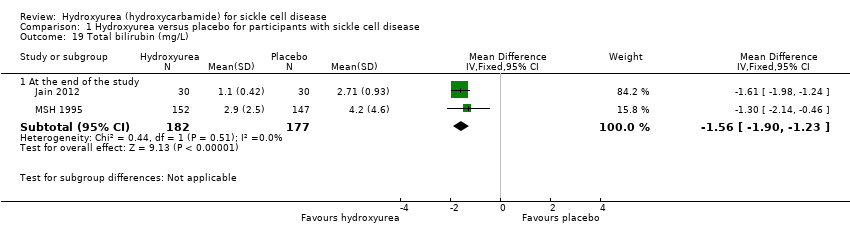
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 19 Total bilirubin (mg/L).

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 20 Reticulocytes.
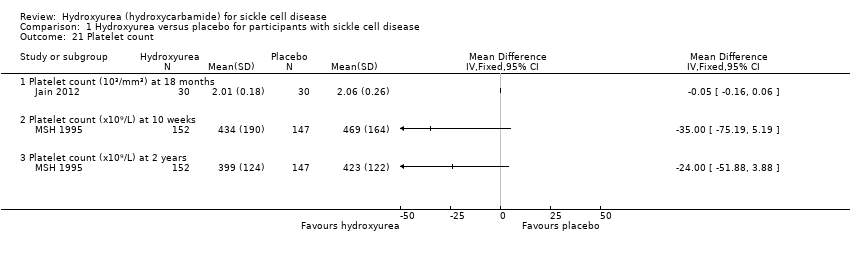
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 21 Platelet count.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 22 Packed cell volume.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 23 F reticulocytes.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 24 F cells.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 25 Red blood count.
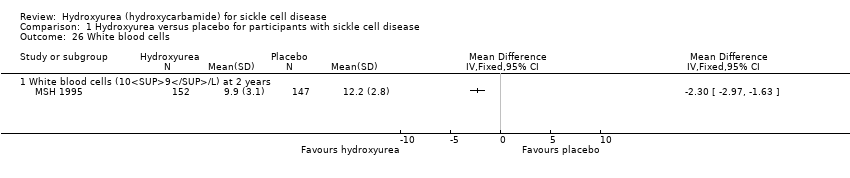
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 26 White blood cells.
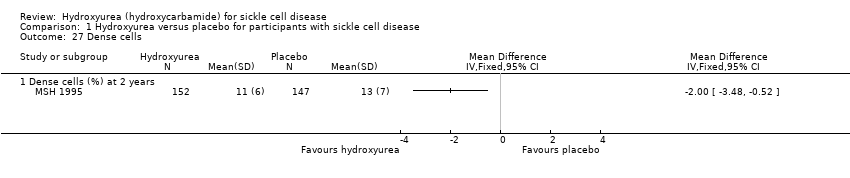
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 27 Dense cells.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 28 Leucocytes.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 29 Creatinine.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 30 Aspartate aminotransferase.
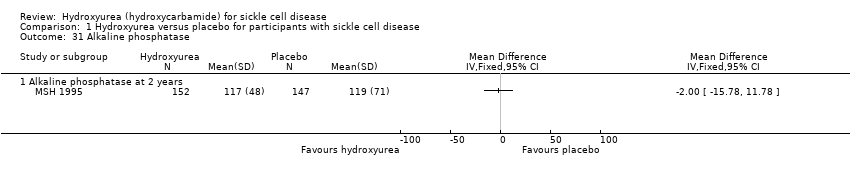
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 31 Alkaline phosphatase.
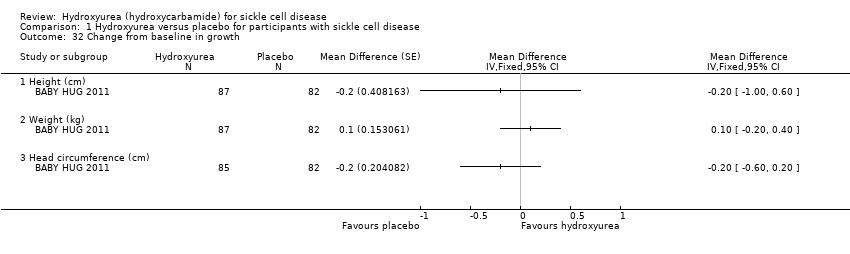
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 32 Change from baseline in growth.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 33 Quality of life: general health perception.
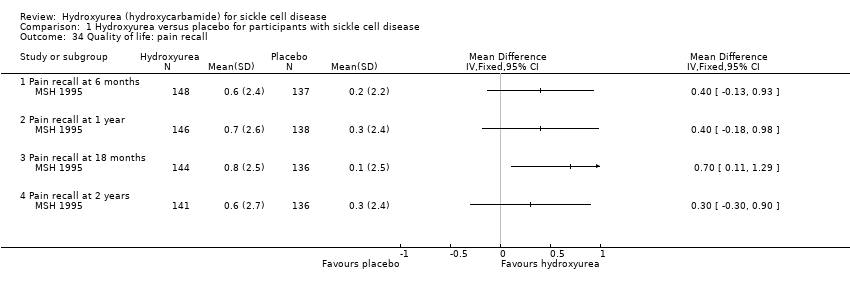
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 34 Quality of life: pain recall.
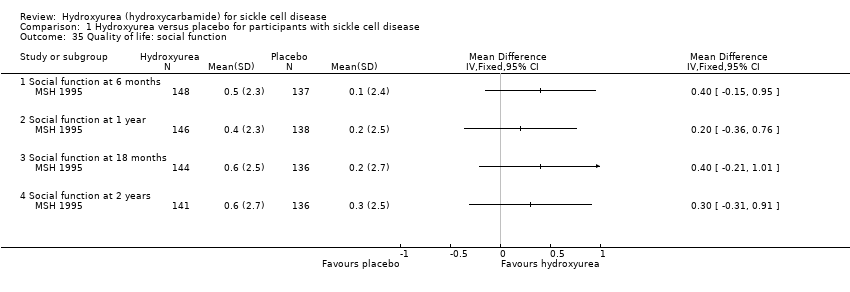
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 35 Quality of life: social function.
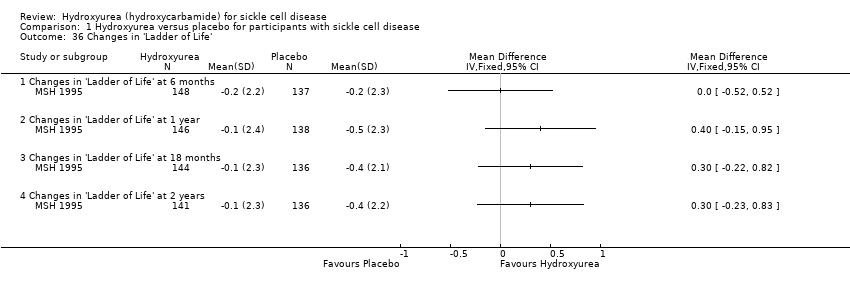
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 36 Changes in 'Ladder of Life'.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 37 Proportion of participants with signs of organ damage.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 38 Signs of organ damage ‐ change from baseline in DTPA GFR.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 39 Signs of organ damage ‐ change from baseline in Howell‐Jolley body (per 106 red blood cells).

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 40 Signs of organ damage ‐ change from baseline in pitted cells (%).
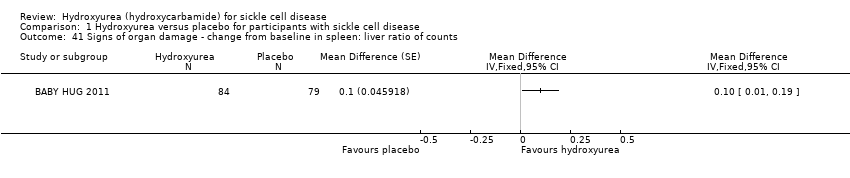
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 41 Signs of organ damage ‐ change from baseline in spleen: liver ratio of counts.
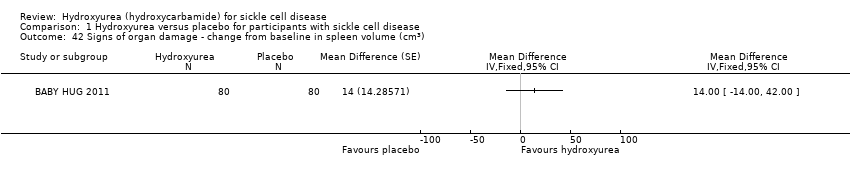
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 42 Signs of organ damage ‐ change from baseline in spleen volume (cm3).
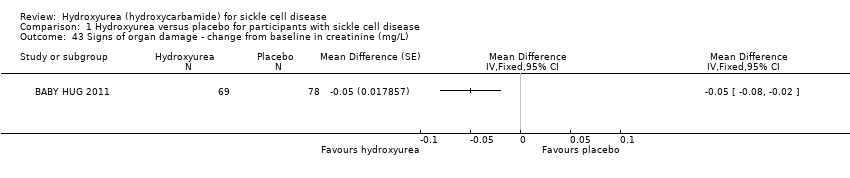
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 43 Signs of organ damage ‐ change from baseline in creatinine (mg/L).
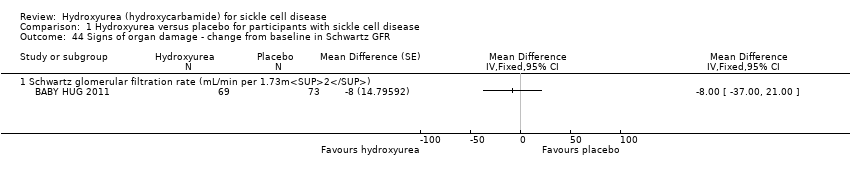
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 44 Signs of organ damage ‐ change from baseline in Schwartz GFR.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 45 Signs of organ damage ‐ change from baseline in cystatin C.
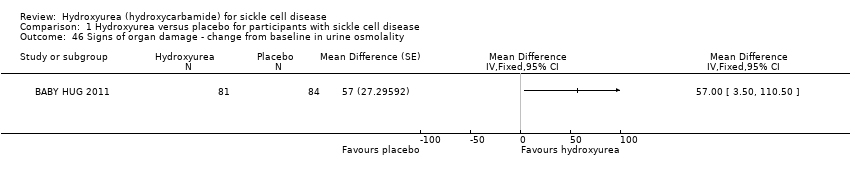
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 46 Signs of organ damage ‐ change from baseline in urine osmolality.
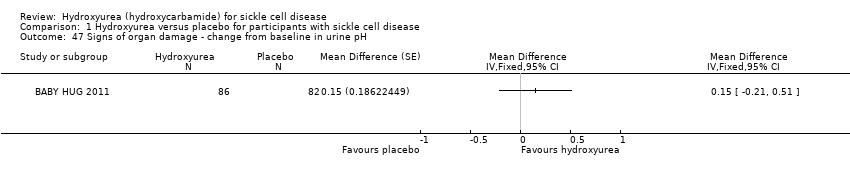
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 47 Signs of organ damage ‐ change from baseline in urine pH.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 48 Signs of organ damage ‐ change from baseline in urine‐specific gravity.
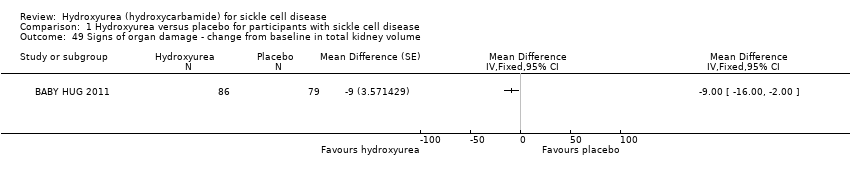
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 49 Signs of organ damage ‐ change from baseline in total kidney volume.
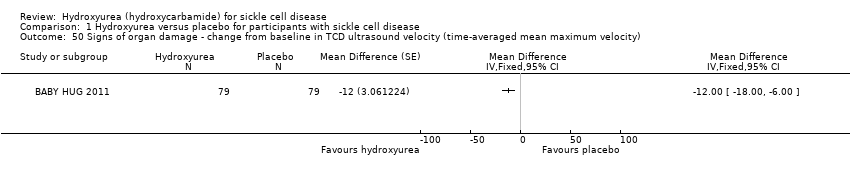
Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 50 Signs of organ damage ‐ change from baseline in TCD ultrasound velocity (time‐averaged mean maximum velocity).

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 51 Signs of organ damage ‐ change from baseline in CNS measures.

Comparison 1 Hydroxyurea versus placebo for participants with sickle cell disease, Outcome 52 Proportion of participants experiencing adverse events and toxicity.

Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 1 Proportion experiencing pain.

Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 2 Proportion experiencing life‐threatening events during study.

Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 3 Deaths during the study.

Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 4 Change from baseline in fetal haemoglobin (HbF %).

Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 5 Change from baseline in absolute neutrophil count (x10⁹/L).

Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 6 Change from baseline in mean corpuscular volume (fL).

Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 7 Change from baseline in sickle haemoglobin (%).

Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 8 Change from baseline in haemoglobin (g/L).

Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 9 Change from baseline in absolute reticulocyte count (10⁹ / L).

Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 10 Change from baseline in white blood count (10⁹ / L).
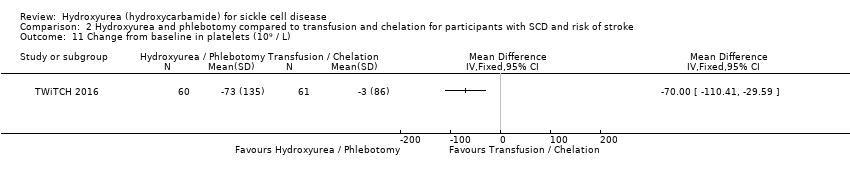
Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 11 Change from baseline in platelets (10⁹ / L).

Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 12 Change from baseline in total bilirubin (mg/L).

Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 13 Change from baseline in liver iron concentration.

Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 14 Change from baseline in serum ferritin (ng/mL).
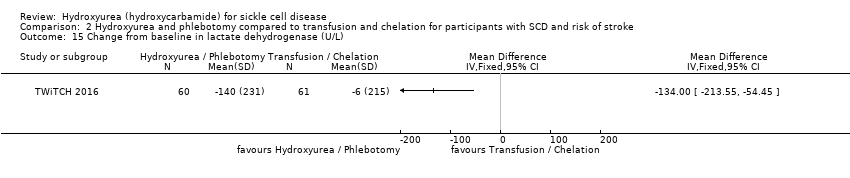
Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 15 Change from baseline in lactate dehydrogenase (U/L).
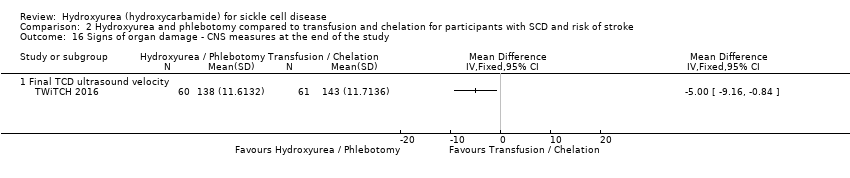
Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 16 Signs of organ damage ‐ CNS measures at the end of the study.
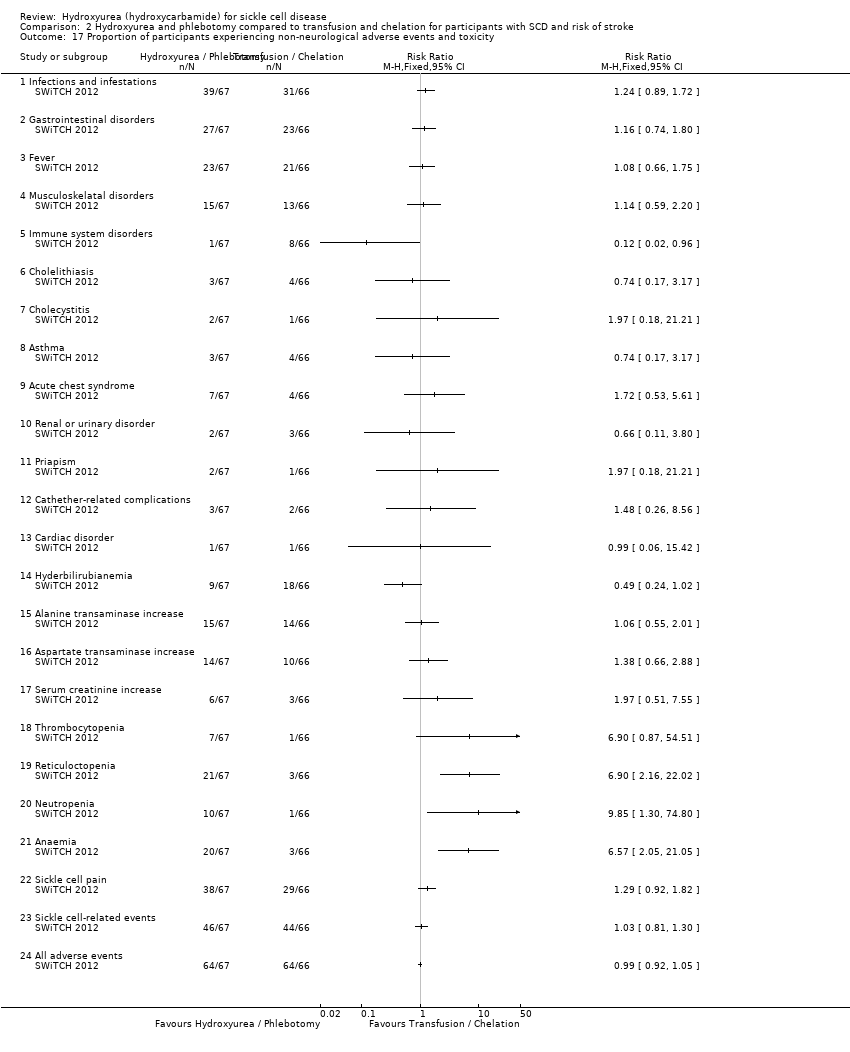
Comparison 2 Hydroxyurea and phlebotomy compared to transfusion and chelation for participants with SCD and risk of stroke, Outcome 17 Proportion of participants experiencing non‐neurological adverse events and toxicity.

Comparison 3 Hydroxyurea compared to observation for participants with SCD and risk of stroke, Outcome 1 Proportion experiencing life‐threatening events during the study.

Comparison 3 Hydroxyurea compared to observation for participants with SCD and risk of stroke, Outcome 2 Signs of organ damage ‐ proportion of participants with a change in CNS measures.

Comparison 3 Hydroxyurea compared to observation for participants with SCD and risk of stroke, Outcome 3 Signs of organ damage ‐ change from baseline in CNS measures.

Comparison 3 Hydroxyurea compared to observation for participants with SCD and risk of stroke, Outcome 4 Adverse events and toxicity.
| Hydroxyurea compared with placebo for sickle cell disease | ||||||
| Patient or population: adults and children with sickle cell disease Settings: outpatients Intervention: hydroxyurea Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Hydroxyurea | |||||
| Pain alteration1 Follow‐up: 6 ‐ 24 months | See comment | See comment | NA | 577 (4 studies)2 | ⊕⊕⊕⊝ | All studies showed a significant advantage to hydroxyurea compared to placebo (different measures of pain alteration presented)1. |
| Life‐threatening illness Follow‐up: 6 ‐ 24 months | See comment | See comment | NA | 552 (3 studies) | ⊕⊕⊕⊝ | Significantly fewer occurrences of ACS (2 studies) and transfusions (3 studies) on hydroxyurea compared to placebo. No significant differences in terms of stroke, hepatic or splenic sequestration (two studies). |
| Death during the study (all deaths) Follow‐up: 6 ‐ 24 months | 26 per 1000 | 10 per 1000 (0 to 51 per 1000) | RR 0.39 (0.08 to 1.96) | 577 (4 studies)2 | ⊕⊕⊕⊝ | There was also no significant difference between groups in terms of deaths related to SCD. |
| Measures of HbF (%) Follow‐up: 6 ‐ 24 months | See comment | See comment | NA | 577 (4 studies)2 | ⊕⊕⊕⊝ | There was a significant increase in HbF(%) in the hydroxyurea group compared to the placebo group in all studies (different measures presented)3. |
| Measures of ANC Follow‐up: 6 ‐ 24 months | See comment | See comment | NA | 517 (3 studies)2 | ⊕⊕⊕⊝ | There was a significant decrease in ANC in the hydroxyurea group compared to the placebo group in all studies (different measures presented)3. |
| Quality of life: 'Health Status Survey' the 'Profile of Mood States' and the 'Ladder of Life' Follow‐up: 24 months | See comment | See comment | NA | up to 277 (1 study) | ⊕⊕⊝⊝ low5,6 | No significant difference in terms of any domain of any scale except for pain recall at 18 months (MD 0.70, 95% CI 0.11 to 1.29, P = 0.02)4. |
| Adverse events or toxicity: differences in rates of specific adverse events Follow‐up: 6 ‐ 24 months | See comment | See comment | NA | 577 (4 studies)2 | ⊕⊕⊝⊝ low5,7 | Significantly fewer events of dactylitis and gastroenteritis on hydroxyurea compared to placebo. No significant differences between groups in terms of all other events. |
| The basis for the assumed risk is the event rate in the control group unless otherwise stated in the comments and footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
|
| ||||||
| Hydroxyurea and phlebotomy compared to transfusion and chelation for people with sickle cell disease and an increased risk of stroke | ||||||
| Patient or population: adults and children with sickle cell disease and an increased risk of stroke Settings: outpatients Intervention: hydroxyurea and phlebotomy Comparison: transfusion and chelation | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Transfusion and chelation | Hydroxyurea and phlebotomy | |||||
| Pain alteration: proportion experiencing serious VOC or sickle‐related pain events Follow‐up: 24 to 30 months | 213 per 1000 | 718 per 1000 (339 to 1000 per 1000) | RR 3.37 (95% CI 1.59 to 7.11) | 254 (2 studies) | ⊕⊕⊝⊝ low4,5 | No significant difference between treatment groups in terms of all pain events (serious and non‐serious) in 1 study (RR 1.03, 95% CI 0.81 to 1.30). |
| Life‐threatening illness Follow‐up: 24 ‐ 30 months | See comment | See comment | NA | 254 (2 studies) | ⊕⊕⊕⊝ | No significant difference between groups in life‐threatening neurological events, hepatobiliary disease and splenic sequestration; significantly more ACS and infections and infestations in the hydroxyurea and phlebotomy compared to the transfusion and chelation group. |
| Death during the study (all deaths) Follow‐up: 24 ‐ 30 months | 1 death occurred in the transfusion and chelation group of 1 study1. | 1 death occurred in the hydroxyurea and phlebotomy group of 1 study1. | RR 0.99 (95% CI 0.06 to 15.42) | 254 (2 studies) | ⊕⊕⊝⊝ low4,5 | |
| Measures of HbF (%) Follow‐up: 24 to 30 months | See comment | See comment | NA | 254 (2 studies) | ⊕⊕⊕⊝ | There was a significant increase in HbF(%) in the hydroxyurea and phlebotomy group compared to the transfusion and chelation group for both studies (different measures presented)2. |
| Measures of ANC Follow‐up: 24 to 30 months | See comment | See comment | NA | 254 (2 studies) | ⊕⊕⊕⊝ | There was a significant decrease in ANC in the hydroxyurea and phlebotomy group compared to the transfusion and chelation group for both studies (different measures presented)2. |
| Quality of life | Outcome not reported3 | NA | ||||
| Adverse events or toxicity: differences in rates of specific adverse events | See comment | See comment | NA | 254 (2 studies) | ⊕⊕⊝⊝ low4,6 | There was a statistically significant difference in terms of immune disorders (more in transfusion and chelation group), reticulocytopenia, neutropenia and anaemia (more in hydroxyurea and phlebotomy group) in 1 study and the rate of adverse events was balanced across groups in the other study. |
| The basis for the assumed risk is the event rate in the control group unless otherwise stated in the comments and footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1. Absolute data presented for number of deaths as the confidence interval of the relative effect very large due to the small number of events. | ||||||
| Hydroxyurea compared with observation for people with sickle cell disease and an increased risk of stroke | ||||||
| Patient or population: adults and children with sickle cell disease and an increased risk of stroke Settings: outpatients Intervention: hydroxyurea Comparison: observation | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| Observation | Hydroxyurea | |||||
| Pain alteration Follow‐up: NA | Outcome not reported | NA | ||||
| Life‐threatening illness Follow‐up: 15 months | See comment | See comment | NA | 22 (1 study) | ⊕⊝⊝⊝ | No significant differences between groups in terms of ACS, blood transfusions required or acute splenic sequestration. |
| Death during the study Follow‐up: 15 months | No deaths occurred | No deaths occurred | NA | 22 (1 study) | ⊕⊝⊝⊝ | |
| Measures of HbF Follow‐up: 15 months | See comment | See comment | NA | 22 (1 study) | ⊕⊝⊝⊝ | There was a significant increase in HbF in the hydroxyurea group compared to the observation group1. |
| Measures of ANC Follow‐up: 15 months | See comment | See comment | NA | 22 (1 study) | ⊕⊝⊝⊝ | There was a significant decrease in ANC in the hydroxyurea group compared to the observation group1. |
| Quality of Life Follow‐up: NA | Outcome not reported2 | NA | ||||
| Adverse events or toxicity: differences in rates of specific adverse events Follow‐up: 15 months | See comment | See comment | NA | 22 (1 study) | ⊕⊝⊝⊝ | No significant differences between groups in terms of transient neutropenia, reticulocytopenia, parasite infestation, headache and dizziness. |
| The basis for the assumed risk is the event rate in the control group unless otherwise stated in the comments and footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| 1. Median values reported so data cannot be entered into analysis. | ||||||
| Hydroxyurea compared with no hydroxyurea for sickle cell disease | ||||||
| Patient or population: adults and children with sickle cell disease Settings: outpatients Intervention: hydroxyurea Comparison: no hydroxyurea | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect | No of Participants | Quality of the evidence | Comments | |
| Assumed risk | Corresponding risk | |||||
| No hydroxyurea | Hydroxyurea | |||||
| Pain alteration Follow‐up: NA | Outcome not reported | NA | ||||
| Life‐threatening illness Follow‐up: NA | Outcome not reported | NA | ||||
| Death during the study Follow‐up: 11 months | No deaths occurred | No deaths occurred | NA | up to 44 (1 study)1 | ⊕⊝⊝⊝ | |
| Measures of HbF Follow‐up: 24 weeks | See comment | See comment | NA | up to 44 (1 study)1 | ⊕⊝⊝⊝ | There was a significant increase in HbF in the hydroxyurea group compared to the no hydroxyurea group1. |
| Measures of ANC Follow‐up: 24 weeks | See comment | See comment | NA | up to 44 (1 study)1 | ⊕⊝⊝⊝ | There was no significant difference in ANC between treatment groups1. |
| Quality of life Follow‐up: NA | Outcome not reported | NA | ||||
| Adverse events or toxicity Follow‐up: 11 months | See comment | See comment | NA | up to 44 (1 study)1 | ⊕⊝⊝⊝ | Vaso‐occlusive pain crises, headache / migraine, upper respiratory infection, skin rash diarrhoea and abdominal pain were the most common adverse events during the trial and these events were evenly distributed across treatment groups (not separated by group). |
| The basis for the assumed risk is the event rate in the control group unless otherwise stated in the comments and footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence. | ||||||
| 1. Due to the factorial design of the study (22 participants randomised to a treatment arm including hydroxyurea and 22 randomised to a treatment arm without hydroxyurea), results are not entered into analysis. All results of this trial are considered exploratory (CHAMPS 2011). | ||||||
| Hydroxyurea | Placebo | P value | |||
| Baseline | 18 months | Baseline | 18 months | ||
| Clinical events (number of events per participant per year) | |||||
| VOC | 12.13 (8.56) | 0.60 (1.37) | 11.46 (3.01) | 10.2 (3.24) | < 0.001 |
| Blood transfusions | 2.43 (0.69) | 0.13 (0.43) | 2.13 (0.98) | 1.98 (0.82) | < 0.001 |
| Hospitalisations | 10.13 (6.56) | 0.70 (1.28) | 9.56 (2.91) | 9.59 (2.94) | < 0.001 |
| Haematological parameters | |||||
| Hb (g/dL) | 8.1 (0.68) | 9.29 (0.55) | 8.21 (0.68) | 7.90 (0.58) | < 0.001 |
| HbF(%) | 19.8 (0.9) | 24 (5.9) | 19.21 (6.37) | 18.92 (5.77) | < 0.001 |
| Reticulocytes (x10⁵ /mm³) | 1.83 (0.96) | 1.15 (0.1) | 1.73 (0.49) | 1.81 (0.67) | < 0.001 |
| Leucocytes (x10³ /mm³) | 7.36 (6.03) | 6.54 (5.54) | 7.26 (4.91) | 7.38 (2.85) | < 0.001 |
| Platelets (x10³ /mm³) | 1.78 (0.26) | 2.01 (0.18) | 1.91 (0.21) | 2.06 (0.26) | 0.28 |
| RBC (x10⁶ /mm³) | 2.89 (0.57) | 1.98 (0.22) | 1.84 (0.47) | 3.11 (0.20) | 0.05 |
| Total bilirubin (mg/dL) | 2.32 (1.42) | 1.10 (0.42) | 2.27 (1.28) | 2.71 (0.93) | < 0.001 |
| Values are mean (standard deviation) P values are calculated using independent t‐test. Hb: haemoglobin | |||||
| Baseline | Hyrdoxyurea | Placebo | P value | ||
| 2 years | Baseline | 2 years | 2 years | ||
| WBC (10⁹/L) | 12.6 (3.4) | 9.9 (3.1) | 12.3 (3.2) | 12.2 (2.8) | 0.0001 |
| Neutrophils (10⁹/L) | 6.9 (2.4) | 4.9 (2.0) | 6.7 (2.3) | 6.4 (2.0) | 0.0001 |
| Platelets (10⁹/L) | 468 (147) | 399 (124) | 457 (130) | 423 (122) | 0.12 |
| Hb (g/dL) | 8.5 (1.4) | 9.1 (1.5) | 8.5 (1.2) | 8.5 (1.3) | 0.0009 |
| PCV (%) | 24.9 (4.4) | 27 (5) | 25.2 (4.0) | 25.1 (4.2) | 0.0007 |
| MCV (fl) | 94 (9) | 103 (14) | 93 (9) | 93 (9) | 0.0001 |
| Reticulocytes (10⁹/L) | 327 (98) | 231 (100) | 325 (94) | 300 (99) | 0.0001 |
| HbF (%) | 5 (3.5) | 8.6 (6.8) | 5.2 (3.4) | 4.7 (3.3) | 0.0001 |
| F cells (%) | 33 (17) | 48 (23) | 33 (17) | 35 (18) | 0.0001 |
| F reticulocytes | 15 (8) | 17 (9) | 15 (8) | 15 (7) | 0.0036 |
| Dense cells (%) | 14 (6) | 11 (6) | 14 (7) | 13 (7) | 0.004 |
| Creatinine (mg/dL) | 0.9 (0.3) | 1.0 (0.5) | 0.9 (0.2) | 1.0 (0.5) | 0.64 |
| Total bilirubin (mg/dL) | 3.7 (2.4) | 2.9 (2.5) | 3.7 (2.5) | 4.2 (4.6) | 0.004 |
| Direct bilirubin (mg/dL) | 0.5 (0.3) | 0.4 (0.3) | 0.5 (0.4) | 0.7 (2.2) | 0.08 |
| Aspartate aminotransferase | 44 (23) | 39 (20) | 41 (21) | 43 (27) | 0.16 |
| Alkaline phosphatase | 120 (59) | 117 (48) | 119 (67) | 119 (71) | 0.71 |
| Values are mean (standard deviation) P values are calculated using independent t‐test. Hb: haemoglobin | |||||
| Outcome | Hydroxyurea and phlebotomy group (n = 67) | Transfusions and chelation group (n = 66) | P value |
| HbF (%) | 17.9 (92 to 22.9) | ‐0.2 (‐0.8 to 0.4) | < 0.001 |
| ANC (x10⁹/L) | ‐3.3 (‐5.1 to ‐1.4) | 0.8 (‐1.3 to 2.4) | < 0.001 |
| Hb (g /dL) | 0.0 (‐0.7 to 0.7) | 0.0 (‐0.5 to 0.6) | 0.898 |
| HbA (%) | ‐50.9 (‐66.8 to ‐33.7) | 0.0 (‐12.7 to 6.7) | < 0.001 |
| HbS (%) | 35.0 (21.7 to 46.2) | 0.3 (‐7.5 to 12.3) | < 0.001 |
| MCV (fL) | 19.5 (7.5 to 28.5) | 0.1 (‐2.0 to 2.5) | < 0.001 |
| WBC (x10⁹/L) | ‐5.4 (‐8.1 to ‐2.2) | 0.2 (‐2.0 to 2.3) | < 0.001 |
| ARC (x10⁹/L) | ‐149.1 (‐231.0 to ‐19.0) | ‐11.8 (‐88.2 to 93.2) | < 0.001 |
| Platelets (x10⁹/L) | ‐83.0 (‐171.0 to ‐8.0) | ‐28.0 (‐70.0 to 18.0) | 0.0022 |
| Total bilirubin (mg/dL) | ‐1.1 (‐1.9 to ‐0.6) | 0.4 (‐0.3 to 1.2) | < 0.001 |
| LIC (mg Fe/g) | ‐1.2 (‐2.8 to 7.2) | ‐2.2 (‐5.5 to 4.9) | 0.48888 |
| Serum ferritin (ng/mL) | ‐966.0 (‐1629.0 to 49.0) | 1159.5 (‐662.0 to 2724.0) | < 0.001 |
| LDH (U/L) | ‐67.0 (‐143.0 to 7.0) | ‐8.5 (‐74.0 to 74.0) | 0.0015 |
| ANC: absolute neutrophil count Values are median change from baseline and interquartile range. P values are calculated using Wilcoxon rank sum test. | |||
| Outcome | Hydroxyurea (n = 11) | Observation (n = 11) | P value |
| Hb (g/dL) | 1.6 | ‐0.5 | < 0.0001 |
| MCV (fL) | 8.7 | 1 | 0.0001 |
| ARC ( x10⁹/L) | 22.7 | ‐33.2 | 0.76 |
| WBC ( x10⁹/L) | ‐4.6 | 1.3 | 0.07 |
| ANC ( x10⁹/L) | ‐2.2 | 1.4 | 0.05 |
| Platelets ( x10⁹/L) | ‐76 | ‐35 | 0.56 |
| HbF (%) | 8.9 | 0.3 | 0.002 |
| Weight (kg) | 2.5 | 1.8 | 0.51 |
| Height (cm) | 6.8 | 3.8 | 0.22 |
| ANC: absolute neutrophil count Values are median change from baseline and P values are calculated using Wilcoxon rank sum test. | |||
| Pregnancy | Hydroxyurea | Placebo | |
| Patients | Normal full‐term delivery | 1 | 2 |
| Elective termination | 2 | 1 | |
| Partners of patients | Normal full‐term delivery | 2 | 0 |
| Spontaneous abortion | 1 | 0 | |
| Still pregnant | 0 | 1 | |
| TOTAL | 6 | 4 | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Pain crises Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.1 Mean annual crisis rate at 2 years (all crises) | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐2.80 [‐4.74, ‐0.86] | |
| 1.2 Mean annual crisis rate at 2 years (all crises requiring hospitalisation) | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐1.50 [‐2.58, ‐0.42] | |
| 1.3 Number of vaso‐occlusive crises after 18 months of treatment | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐9.6 [‐10.86, ‐8.34] | |
| 2 Proportion experiencing pain Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3 Proportion experiencing life threatening events during study Show forest plot | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.1 Acute chest syndrome | 2 | 492 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.43 [0.29, 0.63] |
| 3.2 Hepatic sequestration | 1 | 299 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.32 [0.03, 3.06] |
| 3.3 Stroke | 2 | 492 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.54 [0.12, 2.53] |
| 3.4 Patients transfused | 2 | 492 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.66 [0.52, 0.82] |
| 3.5 Splenic sequestration | 1 | 193 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.36, 2.23] |
| 4 Number of life‐threatening events during study Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4.1 Blood transfusions | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐1.85 [‐2.18, ‐1.52] | |
| 4.2 Hospitalisations | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐8.89 [‐10.04, ‐7.74] | |
| 4.3 Duration of hospitalisation (days) | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐2.00 [‐4.87, ‐3.13] | |
| 5 Deaths during the study Show forest plot | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.1 All deaths | 3 | 552 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.39 [0.08, 1.96] |
| 5.2 Deaths related to SCD | 3 | 552 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.48 [0.09, 2.60] |
| 6 Change from baseline in fetal haemoglobin (HbF %) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 7 Fetal haemoglobin (HbF %) after treatment Show forest plot | 2 | 359 | Mean Difference (IV, Fixed, 95% CI) | 4.07 [2.95, 5.18] |
| 8 Change from baseline in absolute neutrophil count (x10³ per μL) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 9 Neutrophil response (10⁹/L) after treatment Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 9.1 Neutrophils (x10 9/l) at 10 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐1.90 [‐2.51, ‐1.29] | |
| 9.2 Neutrophils (x10 9/l) at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐1.50 [‐2.01, ‐0.99] | |
| 10 Change from baseline in haemoglobin (g/L) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 11 Change from baseline in m corpuscular volume (fL) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 12 Change from baseline in white blood cells (x10³ per μL) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 13 Change from baseline in absolute reticulocyte count (x10³ per μL) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 14 Change from baseline in reticulocytes (%) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 15 Change from baseline in total bilirubin (mg/L) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 16 Change from baseline in platelet count (x10³ per μL) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 17 Haemoglobin (g/dL) Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 17.1 At 10 weeks | 1 | 299 | Mean Difference (IV, Fixed, 95% CI) | 0.5 [0.19, 0.81] |
| 17.2 At the end of the study | 2 | 359 | Mean Difference (IV, Fixed, 95% CI) | 1.04 [0.82, 1.25] |
| 18 Mean corpuscular volume (fL) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 18.1 At 10 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | 12.30 [9.69, 14.91] | |
| 18.2 At 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | 10.0 [7.34, 12.66] | |
| 19 Total bilirubin (mg/L) Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 19.1 At the end of the study | 2 | 359 | Mean Difference (IV, Fixed, 95% CI) | ‐1.56 [‐1.90, ‐1.23] |
| 20 Reticulocytes Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 20.1 Reticulocytes (10⁵/mm³) at 18 months | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐0.66 [‐0.90, ‐0.42] | |
| 20.2 Reticulocytes (10⁹/L) at 10 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐130.0 [‐152.17, ‐107.83] | |
| 20.3 Reticulocytes (10⁹/L) at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐69.0 [‐91.56, ‐46.44] | |
| 21 Platelet count Show forest plot | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 21.1 Platelet count (10³/mm³) at 18 months | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐0.05 [‐0.16, 0.06] | |
| 21.2 Platelet count (x10⁹/L) at 10 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐35.0 [‐75.19, 5.19] | |
| 21.3 Platelet count (x10⁹/L) at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐24.0 [‐51.88, 3.88] | |
| 22 Packed cell volume Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 22.1 Packed cell volume (%) at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | 1.90 [0.85, 2.95] | |
| 23 F reticulocytes Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 23.1 F reticulocytes at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | 2.0 [0.18, 3.82] | |
| 24 F cells Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 24.1 F cells (%) at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | 13.0 [8.33, 17.67] | |
| 25 Red blood count Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 25.1 Red blood count (10⁶/mm³) at 18 months | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐1.13 [‐1.24, ‐1.02] | |
| 26 White blood cells Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 26.1 White blood cells (109/L) at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐2.30 [‐2.97, ‐1.63] | |
| 27 Dense cells Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 27.1 Dense cells (%) at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐2.0 [‐3.48, ‐0.52] | |
| 28 Leucocytes Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 28.1 Leucocytes (10³/mm³) at 18 months | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐0.84 [‐3.07, 1.39] | |
| 29 Creatinine Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 29.1 Creatinine (mg/dL) at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [‐0.11, 0.11] | |
| 30 Aspartate aminotransferase Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 30.1 Aspartate aminotransferase at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐4.0 [‐9.40, 1.40] | |
| 31 Alkaline phosphatase Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 31.1 Alkaline phosphatase at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐2.0 [‐15.78, 11.78] | |
| 32 Change from baseline in growth Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 32.1 Height (cm) | 1 | Mean Difference (Fixed, 95% CI) | ‐0.2 [1.00, 0.60] | |
| 32.2 Weight (kg) | 1 | Mean Difference (Fixed, 95% CI) | 0.10 [‐0.20, 0.40] | |
| 32.3 Head circumference (cm) | 1 | Mean Difference (Fixed, 95% CI) | ‐0.2 [‐0.60, 0.20] | |
| 33 Quality of life: general health perception Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 33.1 General health perception at 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.30 [‐0.54, 1.14] | |
| 33.2 General health perception at 1 year | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.60 [‐0.18, 1.38] | |
| 33.3 General health perception at 18 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.9 [0.08, 1.72] | |
| 33.4 General health perception at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.4 [‐0.51, 1.31] | |
| 34 Quality of life: pain recall Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 34.1 Pain recall at 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.40 [‐0.13, 0.93] | |
| 34.2 Pain recall at 1 year | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.40 [‐0.18, 0.98] | |
| 34.3 Pain recall at 18 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.70 [0.11, 1.29] | |
| 34.4 Pain recall at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.3 [‐0.30, 0.90] | |
| 35 Quality of life: social function Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 35.1 Social function at 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.4 [‐0.15, 0.95] | |
| 35.2 Social function at 1 year | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.2 [‐0.36, 0.76] | |
| 35.3 Social function at 18 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.40 [‐0.21, 1.01] | |
| 35.4 Social function at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.3 [‐0.31, 0.91] | |
| 36 Changes in 'Ladder of Life' Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 36.1 Changes in 'Ladder of Life' at 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [‐0.52, 0.52] | |
| 36.2 Changes in 'Ladder of Life' at 1 year | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.4 [‐0.15, 0.95] | |
| 36.3 Changes in 'Ladder of Life' at 18 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.30 [‐0.22, 0.82] | |
| 36.4 Changes in 'Ladder of Life' at 2 years | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.3 [‐0.23, 0.83] | |
| 37 Proportion of participants with signs of organ damage Show forest plot | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 37.1 New leg ulcers | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.85 [0.44, 1.64] | |
| 37.2 Aseptic necrosis (humerus or femur) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.39, 2.37] | |
| 37.3 Decreased spleen function at exit (compared to baseline) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.44, 1.16] | |
| 38 Signs of organ damage ‐ change from baseline in DTPA GFR Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 39 Signs of organ damage ‐ change from baseline in Howell‐Jolley body (per 106 red blood cells) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 40 Signs of organ damage ‐ change from baseline in pitted cells (%) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 41 Signs of organ damage ‐ change from baseline in spleen: liver ratio of counts Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 42 Signs of organ damage ‐ change from baseline in spleen volume (cm3) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 43 Signs of organ damage ‐ change from baseline in creatinine (mg/L) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 44 Signs of organ damage ‐ change from baseline in Schwartz GFR Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 44.1 Schwartz glomerular filtration rate (mL/min per 1.73m2) | 1 | Mean Difference (Fixed, 95% CI) | ‐8.0 [‐35.00, 21.00] | |
| 45 Signs of organ damage ‐ change from baseline in cystatin C Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 46 Signs of organ damage ‐ change from baseline in urine osmolality Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 47 Signs of organ damage ‐ change from baseline in urine pH Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 48 Signs of organ damage ‐ change from baseline in urine‐specific gravity Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 49 Signs of organ damage ‐ change from baseline in total kidney volume Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 50 Signs of organ damage ‐ change from baseline in TCD ultrasound velocity (time‐averaged mean maximum velocity) Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 51 Signs of organ damage ‐ change from baseline in CNS measures Show forest plot | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 51.1 Bayley Mental Development Index | 1 | Mean Difference (Fixed, 95% CI) | 3.0 [0.00, 8.00] | |
| 51.2 Bayley motor performance development index | 1 | Mean Difference (Fixed, 95% CI) | 2.0 [‐1.00, 7.00] | |
| 52 Proportion of participants experiencing adverse events and toxicity Show forest plot | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 52.1 hair loss at 1 or 2 visits | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.25 [0.69, 2.26] | |
| 52.2 hair loss at 3 or more visits | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.31, 1.21] | |
| 52.3 skin rash at 1 or 2 visits | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.62, 1.51] | |
| 52.4 skin rash at 3 or more visits | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.58, 1.60] | |
| 52.5 fever at 1 or 2 visits | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.55, 1.69] | |
| 52.6 fever at 3 or more visits | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.89 [0.68, 1.17] | |
| 52.7 Gastroinestinal disturbance at 1 or 2 visits | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.50, 1.36] | |
| 52.8 Gastrointestinal disturbance at 3 or more visits | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.74, 1.31] | |
| 52.9 Other abnormalities at 1 or 2 visits | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.60 [0.33, 1.11] | |
| 52.10 Other abnormalities at 3 or more visits | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.83, 1.40] | |
| 52.11 Hospitalisation (for any reason) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.72, 0.96] | |
| 52.12 Dactylitis | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.34 [0.20, 0.58] | |
| 52.13 Priapism | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.52 [0.26, 8.87] | |
| 52.14 Sepsis or bacteraemia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.40 [0.08, 2.03] | |
| 52.15 Splenomegaly | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.61, 1.32] | |
| 52.16 Absolute Neutrophil Count < 500 | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.53 [0.50, 12.71] | |
| 52.17 Absolute Neutrophil 500 ‐ 1250 | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.53 [1.58, 4.03] | |
| 52.18 Thrombocytopaenia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.59 [0.64, 3.92] | |
| 52.19 Alanine transaminase > 150 U/L | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.02 [0.19, 21.92] | |
| 52.20 Severe anaemia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.51 [0.05, 5.48] | |
| 52.21 Bilirubin | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.34 [0.01, 8.17] | |
| 52.22 Creatinine | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 52.23 Skin and subcutaneous disorders | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.91 [0.75, 1.10] | |
| 52.24 Splenic sequestration | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.36, 2.23] | |
| 52.25 Gastroenteritis | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.44 [0.28, 0.71] | |
| 52.26 Nausea | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 5.0 [0.25, 99.95] | |
| 52.27 Skin Rash | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 7.0 [0.38, 129.93] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Proportion experiencing pain Show forest plot | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 Vaso‐occlusive or sickle cell‐related pain (all) | 1 | 133 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.81, 1.30] |
| 1.2 Vaso‐occlusive or sickle cell‐related pain (serious) | 2 | 254 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.37 [1.59, 7.11] |
| 2 Proportion experiencing life‐threatening events during study Show forest plot | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 Stroke (secondary) | 1 | 133 | Risk Ratio (M‐H, Fixed, 95% CI) | 14.78 [0.86, 253.66] |
| 2.2 Transient ischaemic attack (primary) | 1 | 121 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.21, 4.84] |
| 2.3 Transient ischaemic attack (secondary) | 1 | 133 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.66 [0.25, 1.74] |
| 2.4 Other neurological event (primary) | 1 | 121 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.07, 15.88] |
| 2.5 Acute chest syndrome | 2 | 254 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.84 [1.25, 6.42] |
| 2.6 Infections and Infestations | 2 | 254 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.65 [1.05, 12.76] |
| 2.7 Splenic sequestration or splenectomy | 2 | 254 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.34 [0.01, 8.16] |
| 2.8 Hepatobiliary disease | 1 | 121 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.07, 15.88] |
| 2.9 Total with serious adverse events | 2 | 254 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.93 [1.17, 3.20] |
| 2.10 Total with sickle cell related, non‐neurological adverse events | 1 | 133 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.10 [1.42, 6.75] |
| 3 Deaths during the study Show forest plot | 2 | 254 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.06, 15.42] |
| 4 Change from baseline in fetal haemoglobin (HbF %) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5 Change from baseline in absolute neutrophil count (x10⁹/L) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6 Change from baseline in mean corpuscular volume (fL) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7 Change from baseline in sickle haemoglobin (%) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 8 Change from baseline in haemoglobin (g/L) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 9 Change from baseline in absolute reticulocyte count (10⁹ / L) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 10 Change from baseline in white blood count (10⁹ / L) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 11 Change from baseline in platelets (10⁹ / L) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 12 Change from baseline in total bilirubin (mg/L) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 13 Change from baseline in liver iron concentration Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 14 Change from baseline in serum ferritin (ng/mL) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 15 Change from baseline in lactate dehydrogenase (U/L) Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 16 Signs of organ damage ‐ CNS measures at the end of the study Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 16.1 Final TCD ultrasound velocity | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐5.0 [‐9.16, ‐0.84] | |
| 17 Proportion of participants experiencing non‐neurological adverse events and toxicity Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 17.1 Infections and infestations | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.24 [0.89, 1.72] | |
| 17.2 Gastrointestinal disorders | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.16 [0.74, 1.80] | |
| 17.3 Fever | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.66, 1.75] | |
| 17.4 Musculoskelatal disorders | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.59, 2.20] | |
| 17.5 Immune system disorders | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.12 [0.02, 0.96] | |
| 17.6 Cholelithiasis | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.74 [0.17, 3.17] | |
| 17.7 Cholecystitis | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.97 [0.18, 21.21] | |
| 17.8 Asthma | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.74 [0.17, 3.17] | |
| 17.9 Acute chest syndrome | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.72 [0.53, 5.61] | |
| 17.10 Renal or urinary disorder | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.66 [0.11, 3.80] | |
| 17.11 Priapism | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.97 [0.18, 21.21] | |
| 17.12 Cathether‐related complications | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.48 [0.26, 8.56] | |
| 17.13 Cardiac disorder | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.06, 15.42] | |
| 17.14 Hyderbilirubianemia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.49 [0.24, 1.02] | |
| 17.15 Alanine transaminase increase | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.06 [0.55, 2.01] | |
| 17.16 Aspartate transaminase increase | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.38 [0.66, 2.88] | |
| 17.17 Serum creatinine increase | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.97 [0.51, 7.55] | |
| 17.18 Thrombocytopenia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 6.90 [0.87, 54.51] | |
| 17.19 Reticuloctopenia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 6.90 [2.16, 22.02] | |
| 17.20 Neutropenia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 9.85 [1.30, 74.80] | |
| 17.21 Anaemia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 6.57 [2.05, 21.05] | |
| 17.22 Sickle cell pain | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.29 [0.92, 1.82] | |
| 17.23 Sickle cell‐related events | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.81, 1.30] | |
| 17.24 All adverse events | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.92, 1.05] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 Proportion experiencing life‐threatening events during the study Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.1 Vaso‐occlusive events | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.4 [0.10, 1.64] | |
| 1.2 Acute splenic sequestration | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.0 [0.07, 14.05] | |
| 1.3 Blood transfusions required | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.04, 2.73] | |
| 2 Signs of organ damage ‐ proportion of participants with a change in CNS measures Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.1 Participants converting from conditional to abnormal TCD ultrasound velocity | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.2 [0.03, 1.45] | |
| 3 Signs of organ damage ‐ change from baseline in CNS measures Show forest plot | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.1 TCD ultrasound velocity (time‐averaged mean maximum velocity) | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐25.7 [‐45.38, ‐6.02] | |
| 4 Adverse events and toxicity Show forest plot | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.1 Dizziness | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.0 [0.14, 66.53] | |
| 4.2 Headaches | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.0 [0.07, 14.05] | |
| 4.3 Transient neutropenia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.0 [0.14, 66.53] | |
| 4.4 Reticulocytopenia | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.0 [0.07, 14.05] | |
| 4.5 Parasite infection | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.0 [0.07, 14.05] | |