Rehabilitación cardíaca con ejercicios para la cardiopatía coronaria
Referencias
Referencias de los estudios incluidos en esta revisión
Referencias de los estudios excluidos de esta revisión
Referencias de los estudios en espera de evaluación
Referencias de los estudios en curso
Referencias adicionales
Referencias de otras versiones publicadas de esta revisión
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Study characteristics | ||
| Methods | Study design: RCT Country: Denmark Dates participants recruited: NR Maximum follow‐up: 37 months Post MI randomised four weeks after discharge. | |
| Participants | Inclusion criteria: < 66 yrs with 1st MI Exclusion criteria: participants without motivation and participants with impairment of the motorial apparatus that excluded training N randomised: total: 75; intervention: 38; comparator: 37 Diagnosis (% of participants): post MI: 100% Age (mean ±SD): intervention: 52.2 ± 7.5; comparator: 55.6 ± 6.3 Percentage male: intervention: 100%; comparator: 100% | |
| Interventions | Intervention: aerobic activity e.g. running, cycling, skipping + weights for 1 hour x 2 weekly for 2 months, then x 1 week for 10 months. Then continue at home. Components: exercise only Setting: centre‐based initially, followed by home Exercise programme modality: e.g. running, cycling, skipping Total duration: 12 months Co‐interventions: none described Comparator: non‐trained group (although some participants trained on own initiative) Co‐interventions: none described | |
| Outcomes | Total and CHD mortality Non‐fatal MI Outcomes measured at 1, 13, 25 and 37 months post‐discharge | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | 88 participants were randomised, but 13 failed to follow up. Therefore, 75 took part in the study. Several participants in control group trained on own initiative, but were analysed as intention‐to‐treat. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "random numbers" |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 15% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (20 cities) Country: Russia Dates participants recruited: NR Maximum follow‐up: 1 year | |
| Participants | Inclusion criteria: people 3 to 8 weeks after MI, unstable angina or reconstructive coronary arteries intervention. In some cases (at discretion of the researchers), people with stable angina after hospital treatment with unconfirmed diagnosis of MI or unstable angina were included in the study. Exclusion criteria: none reported N Randomised: total: 392; intervention: 197; comparator: 195 Diagnosis (% of participants): Stable angina: intervention: 62.7; comparator: 77.7 Post MI: intervention: 78.4; comparator: 77.3 Unstable angina: intervention: 5.0; comparator: 10.9 (not mutually exclusive) Age (mean ± SD): intervention: 51.9 ± 7.2; comparator: 51.9 ± 7 Percentage male: intervention: 95.5; comparator: 91.7 | |
| Interventions | Intervention: participants of the main group received moderate‐intensity PT (50% to 60% of the performed capacity by bicycle ergometry (BE) test) 3 times per week with duration of exercises from 45 minutes to 1 hour for 1 year Components: exercise only Setting: NR Exercise programme modality: cycling Total duration: 1 year Co‐interventions: participants received standard medical therapy described below. Comparator: participants received standard medical therapy which included beta‐blocker, acetylsalicylic acid or other antithrombotic drug, as well as nitrate, and ACE inhibitor. Some participants took lipid‐lowering drugs. Co‐interventions: none described | |
| Outcomes | Mortality and MI | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of randomisation not described….“patients were randomised into 2 groups….” |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not described |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding of assessments not described |
| Incomplete outcome data (attrition bias) | Low risk | Withdrawals were similar for both groups. |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Russia Dates participants recruited: NR Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: male participants with coronary artery disease that underwent CABG 3 to 8 weeks before enrolment Exclusion criteria: early post‐surgery stenocardia, pericarditis (diagnosed by echocardiography), pericardial effusion with a volume of pericardial fluid exceeding 200 mL, separation of the pericardial layers in diastole more than 1 cm, or moderate pericardial effusion with signs of inflammation), sternal diastasis and other post‐surgery complications (impaired wound healing, suture sinuses or pain), cardiac arrhythmia, heart failure, maximal power output in cycle ergometer test < 50 W, hypertension ( ≥ 180/100 mmHg), history of stroke or transient ischaemia, carotid artery narrowing by ≥ 50%, intermittent claudication syndrome, relapsing thromboembolism complications, severe diabetes mellitus, morbid obesity, pulmonary disorders, concurrent diseases that impede physical training. N randomised: total: 36; intervention: 18; comparator: 18 Diagnosis (% of participants): intervention: received CABG 17 (94%), history of MI 13 (72.2%), history of angina 13 (72.2%); comparator: received CABG 17 (94%), history of MI 10 (55.6%), history of angina 15 (83.3%). Age (mean ±SD): intervention: 58.6 ± 7.0; comparator 55.9 ± 7.0 Percentage male: 100% Ethnicity: NR | |
| Interventions | Intervention: “School for coronary bypass patients” ‐ an integrated cardiac rehabilitation program. Weekly group information sessions (60 to 80 min) under guidance by a cardiologist. Sessions focused on most common topics related to rehabilitation after CABG: cardiac diseases, cardiovascular risk factors, smoking cessation, stress management, anxiety and depression, and “hearthealthy” diet and cooking. Supervised physical training 3 times per week for 4 months. 60‐minute sessions including breathing exercise, physical drill complexes and cycling on a stationary bicycle at moderate intensity (50% to 60% max. power assessed by graded cycle ergometer test). After 4 months centre‐based CR, participants continued home‐based exercise for 6 months. Participants provided with written instructions and a video with recommendations to follow the programme for a year. Participants instructed to perform self‐assessment of their physical well being at home. Exercises included breathing, physical drill and walking. Components: exercise plus education plus individual counselling sessions upon request Setting: centre‐ and then home‐based Exercise programme modality: breathing exercises, physical drills, centre‐based stationary cycling, and home‐based walking Total duration: 10 months Co‐interventions: none described Comparator: control group participants attended the same educational sessions as intervention group. Participants received a recommendation to follow physical training at home on their own. Co‐interventions: none described | |
| Outcomes | Total mortality, revascularisations, hospitalisations, HRQoL | |
| Source of funding | NR | |
| Conflicts of interest | None declared | |
| Notes | Authors contacted for further clinical outcomes and QoL data but no response received | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided regarding methods used to generate allocation sequence |
| Allocation concealment (selection bias) | Unclear risk | No information provided regarding methods used to conceal allocation sequence |
| Blinding of outcome assessment (detection bias) | Unclear risk | No information provided regarding blinding of outcome assessment for any of the main outcomes of interest |
| Incomplete outcome data (attrition bias) | Low risk | Only 1 participant in control group reported as withdrawn for non‐medical reasons |
| Selective reporting (reporting bias) | Unclear risk | No protocol paper or clinical trials registration available |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Sweden Dates participants recruited: 2004 to 2006 Maximum follow‐up: 8 months (6 months following PCI) | |
| Participants | Inclusion criteria: coronary artery stenosis documented by angiography or previous coronary artery bypass grafting, classes I‐III angina pectoris, classified according to Canadian Cardiovascular Society. Exclusion criteria: disabling disease that hindered regular exercise, or if the individual has already engaged in exercise more than 3 days/week N randomised: total: 37; intervention: 21; comparator: 16 Diagnosis (% of participants): stable CAD: 100% Age (years): 63.6 years; intervention: 61.5 (59.8 to 65.5); comparator: 64 (58.5 to 71.0) Percentage male: 86.5%; intervention: 81.0%; comparator: 93.8% Ethnicity: NR | |
| Interventions | Intervention: participants were asked to exercise at home on a bicycle ergometer for 30 min (including a 10‐minute warm‐up and a 5‐minute cool‐down), 5 days a week for 8 months. The training programme was initiated 2 months before the PCI. Twice a week the training participants were allowed to exchange cycling for an equivalent exercise such as jogging or swimming. Components: exercise and education Setting: home Exercise programme modality: bicycle ergometer Total duration: 8 months Co‐interventions: participants in both groups were invited to participate in the CR care consisting of group‐based lifestyle education and aerobic as well as resistance exercise twice a week during months 4 to 6. Comparator: usual care Co‐interventions: as above | |
| Outcomes | PCI at 2 months before PCI and 6 months after PCI | |
| Source of funding | The Swedish Heart Association, the Research and Development Council for Southern Gothenberg and Bohuslan, and Rene Eanders Foundation | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomised" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 8.1% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points (although absolute values not always given) |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Italy Dates participants recruited: NR Maximum follow‐up: 33 (SD 7) months | |
| Participants | Inclusion criteria: successful procedure of coronary angioplasty in 1 or 2 native epicardial coronary arteries and ability to exercise Exclusion criteria: previous coronary artery procedures, cardiogenic shock, unsuccessful angioplasty (defined as residual stenosis > 30% of initial value), complex ventricular arrhythmias, uncontrolled hypertension and diabetes mellitus, creatinine > 2.5 mg/dL, orthopedic or neurological limitations to exercise or unstable angina after procedure and before enrolment N randomised: total:118; intervention: 59; comparator: 59 Diagnosis (% of participants): Myocardial infarction: intervention: 51; comparator: 47 Hypercholesterolemia: intervention: 61; comparator: 54 Diabetes: intervention: 17; comparator: 20 Hypertension: intervention: 42; comparator: 47 LVEF (%): intervention: 52 (SD 16); comparator: 50 (SD 14) Age (mean ± SD): intervention: 53 ± 11; comparator: 59 ± 10 Percentage male: intervention: 83.1%; comparator: 84.8% Percentage white: NR | |
| Interventions | Intervention: exercise sessions were performed at the hospital gym and were supervised by a cardiologist. After a 15‐min phase of stretching and callisthenics, participants pedaled on an electronically‐braked cycle ergometer at the target work rate for 30 min. This working phase was preceded by a 5‐min loadless warm‐up and followed by 3 min of unloaded cool‐down pedaling. Components: exercise only Setting: supervised in hospital gym Exercise programme modality: electronically‐braked cycle ergometer Total duration: six months Co‐interventions: none described Comparator: control participants were recommended to perform basic daily mild physical activities but to avoid any physical training. A list of acceptable physical activities was provided, together with a diary to report daily activities. Co‐interventions: none described | |
| Outcomes | Cardiac mortality; myocardial infarction; coronary angioplasty (percutaneous transluminal coronary angioplasty, coronary stent); coronary artery bypass graft; health‐related quality of life: MOS Short‐Form General Health Survey | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | Cardiac events of 12 participants who were excluded not accounted for |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (5 sites), participants randomised 4 to 6 days post‐event. Two independent 2‐way evaluations: conventional CR versus the Heart Manual (HM) and HM versus usual care Country: UK Dates participants recruited: NR Maximum follow‐up: 1 year | |
| Participants | Inclusion criteria: post MI < 65 years Exclusion criteria: physical infirmity which precludes exercise, inability to speak or read English, dementia or psychosis, age over 75 years, residency more than 20 miles from the coronary care unit (CCU), serious persisting complications which had not been stabilised at time of proposed randomisation including: continuing post‐infarct ischaemia, clinically significant heart failure, important cardiac arrhythmias, conduction disturbances (LBBB > mobitz type 1, 2nd degree AV block), concurrent illnesses (e.g. severe respiratory disease, renal insufficiency, etc.), any other condition which, in the consultant's opinion, would interfere with the individual's successful participation in the programme, or previous participation in the rehabilitation programme N randomised: total: 353; intervention: 251; comparator: 102 Diagnosis (% of participants): MI: 100% Age (mean ±SD): for women: 60.7 ± 7.2 to 64.3 ± 7.3; for men: 57.8 ± 8.9 to 59.4 ± 9.4 Percentage male: 78% Ethnicity: NR | |
| Interventions | Intervention: Heart Manual group: the Heart Manual is a comprehensive home‐based programme which includes an exercise regimen, relaxation and stress management techniques, specific self‐help treatments for psychological problems commonly experienced by MI patients and advice on coronary risk‐related behaviours. Components: exercise, education and psychological Setting: home Exercise programme modality: walking Total duration: up to 6 weeks Co‐interventions: relaxation and stress management techniques, specific self‐help treatments for psychological problems commonly experienced by MI patients and advice on coronary risk‐related behaviours Conventional CR group: 1 to 2 group classes per week, walking etc., other days for 8 to 12 weeks with multidisciplinary team Comparator: usual care Co‐interventions: none described | |
| Outcomes | Total mortality, health‐related quality of life: Nottingham Health Profile | |
| Source of funding | British Heart Foundation | |
| Conflicts of interest | NR | |
| Notes | Hospital readmissions significantly reduced in Heart Manual group compared with conventional CR and control in initial six‐month period | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomisation was achieved by providing each hospital with a series of sealed envelopes containing cards evenly distributed between conditions. The envelopes were taken sequentially and, before opening the envelope, the patient's surname was written diagonally across the sealed flap, in such a way that when the envelope was opened the name was 'torn in two'. Opened envelopes were retained and returned to the trial coordinator. The importance of remaining neutral when advising the patients of the outcome of randomisation was emphasised in the written protocol and was reinforced during the sessions which were held to familiarise facilitators with the protocol." |
| Allocation concealment (selection bias) | Low risk | "Randomisation was achieved by providing each hospital with a series of sealed envelopes containing cards evenly distributed between conditions. The envelopes were taken sequentially and, before opening the envelope, the patient's surname was written diagonally across the sealed flap, in such a way that when the envelope was opened the name was 'torn in two'. Opened envelopes were retained and returned to the trial coordinator. The importance of remaining neutral when advising the patients of the outcome of randomisation was emphasised in the written protocol and was reinforced during the sessions which were held to familiarise facilitators with the protocol." Comment: participants were informed of outcome of randomisation. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | Low risk | 1.5% lost to follow‐up and reported description of withdrawals and/or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Sweden Dates participants recruited: October 1973 to January 1975 Maximum follow‐up: 14 months | |
| Participants | Inclusion criteria: participants > 65 years with MI Exclusion criteria: severe cardiac failure, post myocardial infarction (PMI)‐syndrome, aortic regurgitation, cerebral infarct hemiparesis, disease of hip, status post‐poliomyelitis, amputation of lower extremity, diabetes with retinopathy, hyper/hypo thyroidism, hyperparathyroidism, mental illness N randomised: total: 87; intervention: 44; comparator: 43 Diagnosis (% of participants): AMI: 100% Age (years ± SD): intervention: 55.3 ± 6.6; comparator: 57.1 ± 6.6 Percentage male: 85% Ethnicity: NR | |
| Interventions | Intervention: physical training under the supervision of a specially‐trained physiotherapist attached to the cardiological unit. Exercises consisted of interval training of large muscle groups on a mechanically‐braked ergometer bicycle, callisthenics and jogging for 30 minutes twice weekly over a period of 3 months. The intensity of the exercises was graded individually on the basis of the findings at the exercise tolerance test, and a maximum heart rate at exercise was prescribed. Components: exercise, counselling and social measures Setting: supervised at the cardiological unit Exercise programme modality: ergometer cycling Total duration: 3 months Co‐interventions: Counselling was given, supplying practical information on avoiding weight gain, to stop smoking, to keep on with the physical exercise and to resume leisure activities as much as possible. Comparator: conventional care Co‐interventions: none described | |
| Outcomes | Total mortality, CHD mortality, non‐fatal MI up to average 14 months | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | Most emphasis on social/ psychological aspects. 171 participants were randomised and at discharge, the cardiologist decided whether the participant was fit to take part in the rehabilitation programme ‐ 45 participants were excluded at this point. Seven people in the intervention group declined to take part, but six of these were seen at follow‐up and included in the analysis because "control group probably had a comparable number who would have declined further treatment." | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "allocated at random" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | Description of withdrawals and dropouts: intervention group 29%; control group 33% lost to follow‐up from 126 who took part. 171 were randomised and then 45 excluded by cardiologist. |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT; participants were randomised on day of discharge after MI Country: UK Dates participants recruited: NR Maximum follow‐up: 24 months | |
| Participants | Inclusion criteria: men and women with AMI Exclusion criteria: uncontrolled heart failure; serious rhythm disturbances which persisted and required treatment at time of discharge; another disabling disease N randomised: total: 110; intervention: 57; comparator: 53 Diagnosis (% of participants): AMI: 100% Age (mean ± SD): intervention: 52.1 ± 1.3; comparator: 52.7 ± 1.3 Percentage male: NR Ethnicity: NR | |
| Interventions | Exercise: a formal rehabilitation programme at the hospital started 3 weeks post‐discharge. The programme concentrated mainly on standard pulse‐monitored group exercise, supervised by a physiotherapist. Participants completed a circuit of 12 exercises, and after a five‐minute interval, they repeated the circuit, up to a maximum of four circuits. Components: exercise Setting: supervised group sessions in the hospital gymnasium Exercise programme modality: "group exercises" Total duration: 4 weeks Co‐interventions: health, smoking and dietary advice and a relaxation technique Comparator: standard hospital care Co‐interventions: all participants were asked to stop smoking and given dietary advice either for weight reduction or because of elevated serum cholesterol. To boost confidence, each participant was asked to walk up two flights of stairs under supervision and was given advice on mobilisation on discharge. | |
| Outcomes | Total mortality, non‐fatal MI, revascularisation; assessments at day of discharge, 3rd week after discharge; after rehabilitation (for intervention group); four months after infarct and 12 to 24 months after infarct) | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomised" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 24% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: UK Dates participants recruited: 1 December 1979 to March 1984 Maximum follow‐up: 5 years | |
| Participants | Inclusion criteria: < 65 years post MI; history of chest pain typical of MI, progressive ECG changes, rise and fall in aspartate transaminase concentrations with at least one reading above 40 units/mL Exclusion criteria: medical or orthopaedic problems that precluded their taking part in the exercise course; insulin‐dependent diabetes mellitus; atrial fibrillation; on investigator's personal general practice list N randomised: total: 200; intervention: 99; comparator: 101 Diagnosis (% of participants): MI: 100% Age (mean ± SD): intervention: 54.2 ± 7.2; comparator: 54.2 ± 7.2 Percentage male: intervention: 100%; comparator: 100% Ethnicity: NR | |
| Interventions | Intervention: treatment participants entered a three‐month course of three times a week circuit training. Components: exercise only Setting: centre Exercise programme modality: 8 stage circuit aerobic training Total duration: 3 months Co‐interventions: NR Comparator: participants were given a short talk on the sort of exercise that they might safely take unsupervised Co‐interventions: NR | |
| Outcomes | Total mortality, CHD mortality, non‐fatal MI (11 year follow‐up published in 1999. Five‐year follow‐up data from unpublished material used for meta analysis.) | |
| Source of funding | British Heart Foundation and Wessex Regional Health Authority | |
| Conflicts of interest | NR | |
| Notes | 229 participants were randomised; 14 in the intervention group and 15 in control dropped out before the first exercise test due to death, refusal or other problems. Therefore 200 took part in the study. Cardiac mortality of 3% per annum, once participants survived to be in the trial. Suggests more severely affected participants were not included. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random letter sequence |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 16% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT (1:3 randomisation) Country: Portugal Dates participants recruited: 1 September 2001 to 31 December 2002 Maximum follow‐up: 1 year | |
| Participants | Inclusion criteria: participants without previous cardiological follow‐up, with > 4 years’ education, following hospitalisation for acute coronary syndrome (ACS) Exclusion criteria: none stated N randomised: total: 126; intervention: 31; comparator: 95 Diagnosis (% of participants): Unstable angina: intervention 20; comparator: 27 Non‐Q wave MI: intervention 33; comparator: 31 Anterior MI: intervention 23; comparator: 20 Inferior MI: intervention 24; comparator: 21 MI of undetermined location: intervention 10; comparator 11 Age (years): intervention: 56 (range: 31‐80); comparator: 58 (range: 33‐86) Percentage male: intervention: 84 %; comparator 83% Ethnicity: NR | |
| Interventions | Intervention: the sessions took place in the hospital’s gymnasium under qualified supervision. They consisted of a warm‐up period at the beginning of each session, 20 to 30 minutes on a treadmill or ergometric bicycle and a recovery period with low intensity activities. The exercise programme was initially based on the maximum heart rate reached on the exercise test prior to beginning the programme (performed on average five weeks after the ACS). Components: exercise only Setting: aerobic exercise in supervised group sessions Exercise programme modality: treadmill and bicycle Total duration: 12 weeks, followed by one session a month for the remainder of the year Co‐interventions: none described Comparator: standard follow‐up consisting of a mean of 3.5 consultations per year following the first event Co‐interventions: none described | |
| Outcomes | HRQoL | |
| Source of funding | The Commission to Foster Health Care Research | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "...the patients were randomly allocated to our hospital’s cardiac rehabilitation program or standard cardiological follow‐up." |
| Allocation concealment (selection bias) | High risk | Allocation concealment not described |
| Blinding of outcome assessment (detection bias) | High risk | “nature of the intervention being assessed did not permit blinding” |
| Incomplete outcome data (attrition bias) | Low risk | There was no loss to follow‐up. |
| Selective reporting (reporting bias) | Low risk | All outcomes described in the methods were reported in the results section for both time points. |
| Study characteristics | ||
| Methods | Study design: multicentre open RCT (2 sites) Country: Australia Dates participants recruited: 2‐year period. No dates given. Maximum follow‐up: 1 year | |
| Participants | Inclusion criteria: uncomplicated acute myocardial infarction (AMI) or recovery from unstable angina aged under 75 years, self‐caring, adequately literate in the English language, residing in the geographical area of the health service Exclusion criteria: presentation with uncompensated heart failure, uncontrolled arrhythmias, severe and symptomatic aortic stenosis, or other conditions precluding physical activity N randomised: total: 113; intervention: 57; comparator: 56 Diagnosis (% of participants): AMI: intervention 36.8; comparator 48.2 Unstable angina: intervention 63.2; comparator 51.8 Thrombolytic therapy: intervention 14.0; comparator 25.0 PCI/CAGS: intervention 59.6; comparator 46.4 Prior AMI, PCI, CAGS: intervention 36.8; comparator 50.0 Age (Mean ± SD): intervention: 60.8 ± 8.7; comparator: 61.9 ± 9.4 Percentage male: intervention 72%; comparator 75% Ethnicity: NR | |
| Interventions | Intervention: comprehensive exercise‐based outpatient cardiac rehabilitation Components: exercise plus education plus psychosocial counselling Setting: hospital‐based, supervised exercise Exercise programme modality: aerobic circuit training interspaced with resistance training Total duration: 6 weeks Co‐interventions: 45 minutes of education (12 occasions) and 45 minutes of psychosocial counselling (6 occasions). If necessary, additional one‐on‐one counselling was provided. Comparator: conventional care: participants from both groups received individualised medical treatment including non‐invasive and invasive cardiological procedures, surgical revascularisation, pharmacotherapy, and lifestyle counselling, as determined by their usual doctors. Co‐interventions: none described ("Access to community cardiac rehabilitation programs was limited for the conventional management group") | |
| Outcomes | Costs, HRQoL | |
| Source of funding | University of Sydney, the Cardiac Society of Australia and New Zealand, and the National Heart Foundation of Australia; NHMRC; Department of Cardiology, Royal Prince Alfred Hospital | |
| Conflicts of interest | "None identified" | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "...randomisation using dynamic balancing was performed" |
| Allocation concealment (selection bias) | Low risk | “Central randomisation of participants was performed at the National Health and Medical Research Council Clinical Trials Centre” |
| Blinding of outcome assessment (detection bias) | High risk | “Open” trial so we assume that outcomes were not blinded |
| Incomplete outcome data (attrition bias) | Low risk | One person was lost to follow‐up and 5 participants changed groups; 2 participants were excluded from each group i.e. 4/113 (4%) |
| Selective reporting (reporting bias) | Low risk | All outcomes described in the methods section are reported in results. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Russia Dates participants recruited: NR Maximum follow‐up: 12 months. | |
| Participants | Inclusion criteria: male and female participants of working age (male < 60 years, female < 55 years) with acute MI (3 to 8 weeks prior), signed informed consent to participate, absence of generally accepted contraindications to performing exercise training Exclusion criteria: left ventricular aneurysm with thrombosis, stroke, serious disturbances in the rhythm and conduction of the heart, uncontrolled arterial hypertension with blood pressure ≥ 180/100 mmHg, NYHA class III‐IV heart failure, thromboemboli, aortic aneurysm, history of syncope, thrombophlebitis, phlebothrombosis, musculoskeletal disorders, moderate to severe diabetes, severe concomitant diseases, chronic respiratory, hepatic or renal failure N randomised: total: 300; intervention: 155; comparator: 145. Groups then split into 3 subgroups according to rehabilitation potential (intervention: low n = 32, average n = 55, high n = 68; control: low n = 22, average n = 64, high n = 59) Diagnosis (% of participants): 100% acute MI (68% STEMI) Age (mean ±SD): intervention: 49.9 ± 7.2; comparator 50.9 ± 6.1 Percentage male: intervention: 93.5%, comparator: 92.4% Ethnicity: NR | |
| Interventions | Intervention: physical rehabilitation classes consisting of gymnastics exercises carried out for 60 minutes in groups under supervision of a cardiologist 3 times per week for 1 year. Components: exercise only Setting: centre‐based Exercise programme modality: gymnastic exercises Total duration: 1 year Co‐interventions: none described Comparator: no exercise training Co‐interventions: none described | |
| Outcomes | HRQoL, mortality, MI | |
| Source of funding | Not reported | |
| Conflicts of interest | None declared | |
| Notes | Paper translated from Russian | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Patients were randomized using the envelope method"; no further detail reported |
| Allocation concealment (selection bias) | Unclear risk | "Patients were randomized using the envelope method"; no further detail reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | No detail regarding outcome assessment blinding was reported |
| Incomplete outcome data (attrition bias) | Unclear risk | No PRISMA flow diagram provided, no N in tables and text unclear about attrition, appears that there was no loss to follow‐up |
| Selective reporting (reporting bias) | Unclear risk | No published protocol, outcomes described in methods appear to be reported in the results. Cardiovascular complications unclear |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT (4 arms) Country: Russia Dates participants recruited: NR Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: patients after AMI ( > 3 weeks) and percutaneous coronary interventions (PCI) at the age of < 60 years for men and < 55 years for women Exclusion criteria: inadequately controlled hypertension, aortic or left ventricular (LV) aneurysm with thrombosis, serious arrhythmias, NYHA class III‐IV HF, BMI ≥ 40 kg/m2, moderate/severe diabetes and other severe comorbidities N randomised: total: 312; intervention 1 (BMI < 30 kg/m2) = 78; intervention 2 (BMI ≥ 30 kg/m2) = 78; comparator 1 (BMI < 30 kg/m2) = 78; comparator 2 (BMI ≥ 30 kg/m2) = 78 Diagnosis (% of participants): 100% post MI with PCI Age (mean ±SD): intervention 1 (BMI < 30 kg/m2) = 51.9±7.9; intervention 2 (BMI ≥ 30 kg/m2) = 51.7±6.8; comparator 1 (BMI < 30 kg/m2) = 52.2±7.2; comparator 2 (BMI ≥ 30 kg/m2) = 52.6±6.7 Percentage male: intervention 1 (BMI < 30 kg/m2) = 93.6%; intervention 2 (BMI ≥ 30 kg/m2) = 96.2%; comparator 1 (BMI < 30 kg/m2) = 94.9%; comparator 2 (BMI ≥ 30 kg/m2) = 93.6% Ethnicity: NR | |
| Interventions | Intervention: physical rehabilitation programme included group exercise classes lasting 60 minutes 3 times/week involving a set of gymnastic exercises of moderate intensity Components: exercise only Setting: centre‐based Exercise programme modality: gymnastic exercises Total duration: 1 year Co‐interventions: none described Comparator: control participants did not use exercise training programme Co‐interventions: none described | |
| Outcomes | Mortality, MI, HRQoL | |
| Source of funding | Not reported | |
| Conflicts of interest | None declared | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Patients were randomised into four groups depending on BMI”. Authors provided further information: "randomly assigned to the physical training or to the control group using a computer programme". |
| Allocation concealment (selection bias) | Low risk | Authors provided further information: "The allocation sequence was concealed from enrolling researcher". |
| Blinding of outcome assessment (detection bias) | Unclear risk | No information provided regarding blinding |
| Incomplete outcome data (attrition bias) | Unclear risk | No PRISMA flow diagram or description of attrition |
| Selective reporting (reporting bias) | Unclear risk | No published protocol available, but outcomes described in methods appear to be reported. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Norway Dates participants recruited: August 2010 to March 2012 Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: type 2 diabetes and verified CAD by angiography Exclusion criteria: presence of proliferative retinopathy, end‐stage renal disease, cancer, stroke or acute MI within the last 3 months, unstable angina, uncompensated heart failure, serious arrhythmia, severe valvular disease, severe rheumatologic disease, chronic obstructive pulmonary disease (COPD) stadium Global Initiative for Chronic Obstructive Lung Disease (GOLD) IV, thromboembolic disease, ongoing infections, severe musculoskeletal disorders and other disabilities limiting the ability for physical activity N randomised: total: 137; intervention: 69; comparator: 68 Diagnosis (% of participants): stable angina 51 (37%); previous MI 62 (45%). Age (mean ±SD): intervention: 64.6 ± 7.9; comparator: 63.2 ± 7.2 Percentage male: intervention: 45 (87%); comparator: 50 (81%) Ethnicity: NR | |
| Interventions | Intervention: 12‐month combined aerobic and resistance training programme Components: exercise only Setting: both centre‐ and home‐based Exercise programme modality: circuits containing aerobic and resistance exercises, interval uphill walking/running training, interval step training, spinning on a bike Total duration: 12 months Co‐interventions: none described Comparator: continuation of normal follow‐up with general practitioner Co‐interventions: none described | |
| Outcomes | Serious cardiovascular events (composite outcome ‐ worsening of stable angina pectoris and chronic heart failure, unstable angina pectoris, AMI, stroke, sudden cardiac arrest) | |
| Source of funding | "no specific grant from any funding agency in the public, commercial or not‐for‐profit sectors" | |
| Conflicts of interest | None declared | |
| Notes | Authors contacted to request clinical outcome data, but no response received | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomisation was performed by use of consecutively numbered...in a 1:1 ratio according to tables of random numbers, arranged by the Unit of Epidemiology and Biostatistics." |
| Allocation concealment (selection bias) | Low risk | "Consecutively numbered, non‐translucent envelopes" |
| Blinding of outcome assessment (detection bias) | Unclear risk | “The ventilatory threshold (VT) was calculated by the ventilatory equivalent method and was determined by two blinded, independent investigators.” Presume other outcomes were not blinded |
| Incomplete outcome data (attrition bias) | High risk | 17/69 (24%) participants in the intervention group lost to follow‐up or excluded from analysis due to < 40% adherence to exercise intervention (9/69, 13%) |
| Selective reporting (reporting bias) | Unclear risk | Published protocol paper not available, clinical trials.gov registration gives very vague information about proposed outcomes |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (3 sites) Country: Italy Dates participants recruited: January 2017 to April 2018 Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: age ≥ 70 years, hospital admission for ACS, short physical performance battery (SPPB) score from 4 to 9 at the inclusion visit (30 ± 5 days after discharge) Exclusion criteria: participants with SPPB score ≥ 10 or ≤ 3. Multivessel disease with indication for surgical revascularisation or staged PCI, inability to be discharged to home, congestive HF, LVEF < 30%, severe valvular disease N randomised: total: 235; intervention: 118; comparator: 117 Diagnosis (% of participants): intervention: STEMI 33 (28%), NSTEMI 75 (65%), unstable angina 10 (7%); comparator: STEMI 31 (26%), NSTEMI 77 (66%), unstable angina 9 (8%) Age (median, range): intervention: 76, 72 to 80; comparator: 77, 73 to 80 Percentage male: intervention: 92 (78%); comparator: 89 (76%) Ethnicity (White, %): NR | |
| Interventions | Intervention: 4 supervised sessions (1, 2, 3, 4 months after discharge) combined with an individualised home‐based exercise programme. Centre‐based sessions supervised by sports physician and nurse, and included moderate treadmill walk, strength and balance exercises (30 to 40 min). Participants received a walking programme to perform at home along with a selection of callisthenic exercises based on the Otago Exercise Programme. Participants encouraged to perform exercises 2 times per week for approx 20 mins. After the 4 month supervised session, a long‐term home‐based exercise programme was designed by the sports physician. Components: exercise only Setting: 4 centre‐based sessions, home‐based afterwards Exercise programme modality: walking, callisthenics, strength and balance Total duration: 6 months Co‐interventions: health education Comparator: standard of care Co‐interventions: health education – 15 minute visit with study doctor, who explained the importance of aerobic physical activity (30 to 60 min/day, moderate intensity, e.g. brisk walking for at least 3 days/week). A detailed brochure explaining the benefits of physical exercise provided to all participants. | |
| Outcomes | Total and cardiovascular mortality, ACS, hospitalisations, HRQoL | |
| Source of funding | "Investigator‐driven clinical trial conducted by the University of Ferrara" | |
| Conflicts of interest | None declared | |
| Notes | None | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Randomization is performed….via a dedicated website and stratified according the following three variables: sex, clinical presentation (ST‐segment elevation ACS vs. non ST‐segment elevation ACS) and SPPB score at the inclusion (4–6 vs. 7–9). A dedicated website assigns a unique treatment code" |
| Allocation concealment (selection bias) | Low risk | “Randomization is performed….via a dedicated website and stratified according the following three variables: sex, clinical presentation (ST‐segment elevation ACS vs. non ST‐segment elevation ACS) and SPPB score at the inclusion (4–6 vs. 7–9). A dedicated website assigns a unique treatment code" |
| Blinding of outcome assessment (detection bias) | Low risk | “The assessment staff was blinded to the intervention. Participants were asked not to disclose their assigned group and not to talk about their interventions during the assessment. All events were centrally adjudicated by the clinical events committee whose members were unaware of patient randomisation assignment.” |
| Incomplete outcome data (attrition bias) | Low risk | Low numbers of participants missing from 1 year follow‐up (6 and 7 from each group, < 20%), numbers balanced and reasons provided. |
| Selective reporting (reporting bias) | Low risk | Published protocol paper available, all outcomes listed in protocol paper are reported at 1 year. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Sweden Dates participants recruited: NR Maximum follow‐up: 1 year | |
| Participants | Inclusion criteria: AMI; CABG < 2 weeks prior; PCI < 2 weeks prior Exclusion criteria: signs of unstable angina; signs of ST‐depression at exercise test of more than 3 mm in 2 chest leads or more than 2 mm in two limb leads at four weeks post‐discharge from hospital, signs of CHF, severe, non‐cardiac disease; drinking problems, not a Swedish speaker N randomised: total: 235; intervention: 118; comparator: 117 Diagnosis (% of participants): CABG: 25%; AMI: 75% Age (mean ±SD): AMI patients: intervention: 62.2 ± 5.8; comparator: 61.7 ± 6 CABG patients: intervention: 62.7 ± 4.8; comparator: 59.8 ± 4.8 Percentage male: NR Ethnicity: NR | |
| Interventions | Intervention: continuous physical exercise programme 2 to 3 times weekly for 2 to 3 months. The exercise sessions lasted one hour and were comprised of the following parts: 10 minutes of warm‐up; 40 minutes of interval walking or jogging; 10 minute cool‐down period (consisting of relaxation and light stretching exercises). Individual exercise schedules were provided in order to maintain the effects of the exercise programme beyond the discharge from the hospital training centre. Components: exercise plus education Setting: centre and then home Exercise programme modality: walking or jogging Total duration: 2 to 3 months Co‐interventions: 9 hours of nurse counselling in individual and group sessions over 1 year; smoking cessation 1.5 hours, dietary management 5.5 hours Comparator: usual care, which included two or three visits to their general practitioners during the first year Co‐interventions: all participants were informed about CAD risk factors and the effect of lifestyle changes on the prognosis. | |
| Outcomes | Mortality | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | Groups of 20 participants randomly allocated to intervention and control groups (usual care). Randomised 4 weeks post discharge. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | < 20% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT; participants randomised 6 weeks post‐admission Country: UK Dates participants recruited: NR (recruited over a 3.5 year period) Maximum follow‐up: 3 years | |
| Participants | Inclusion criteria: MI; diagnosis based on ECG changes and/or elevation of serum glutamic oxaloacetic transaminase or lactic dehydrogenase taken on three consecutive days. Exclusion criteria: > 70 years; heart failure at follow‐up clinic; cardio‐thoracic ratio exceeding 59%; severe chronic obstructive lung disease; hypertension requiring treatment; diabetes requiring insulin; disabling angina during convalescence; orthopaedic or medical disorders likely to impede progress in the gym, personality disorders likely to render participant unsuitable for the course. N randomised: total: 303; intervention: 151; comparator: 152 Diagnosis (% of participants): MI: 100% Age (mean ± SE): intervention: 50.3 ± 0.65; comparator: 52.8 ± 0.67 Percentage male: intervention: 100%; comparator: 100% Ethnicity: NR | |
| Interventions | Intervention: participants attended the hospital gym twice weekly for 12 weeks. They were supervised by a doctor and physical educationalist and full resuscitative equipment was available. The exercises were arranged on a circuit basis and pure isometric exercise was avoided. Components: exercise only Setting: centre Exercise programme modality: exercises arranged on a circuit basis Total duration: 12 weeks Co‐interventions: none described Comparator: did not attend gym Co‐interventions: none described | |
| Outcomes | Total mortality, non‐fatal MI at 5 months, 1 year, 2 years and 3 years after MI (mean follow‐up 2.1 years) | |
| Source of funding | Department for Health and Social Security Grant | |
| Conflicts of interest | NR | |
| Notes | There appears to be a reduction in mortality in exercise participants with inferior MI. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly allocated" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 21% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points described in the methods. |
| Study characteristics | ||
| Methods | Study design: superiority RCT with waiting‐list control (single centre) Country: Brazil Dates participants recruited: March 2015 to April 2017 Maximum follow‐up: 12 months ‐ 6 months waiting‐list control | |
| Participants | Inclusion criteria: participants aged > 18 years and living in the Belo Horizonte area, with coronary artery disease: post myocardial infarction undergone percutaneous coronary intervention or coronary artery bypass graft surgery and had been referred to CR Exclusion criteria: cardiac conditions associated with some risk during high‐intensity exercise (e.g. heart failure with EF < 45%, complex ventricular dysrhythmia), any comorbid physical condition (e.g. leg amputation, advanced cancer, disabling stroke, Parkinson’s disease), or serious mental illness that would interfere with the ability to exercise, according to CR clinical practice guidelines, or any visual or cognitive condition that would preclude the participant from completing the questionnaires N randomised: total: 115; intervention 1 (exercise only): 39; intervention 2 (comprehensive CR): 37; comparator: 39 Diagnosis (% of participants): participants with CAD after MI or those undergoing PCI/CABG. MI 107 (93%), angina 69 (60%), PCI 68 (59.1%), CABG 29 (25.5%). Age (mean): intervention 1: 59 ± 9.9; intervention 2: 60.7 ± 8.8; comparator: no CR (n = 16) 55.9± 6.7, exercise only (n = 12) 60.7 ± 13.3, comprehensive CR (n = 11) 60.6 ± 8.4 Percentage male: intervention 1: 28 (71.8%); intervention 2: 27 (73%); comparator: no CR (n = 16) 11 (68.8%), exercise only (n = 12) 12 (100%), comprehensive CR (n = 11) 4 (36.4%) Ethnicity (white, %): NR | |
| Interventions | Intervention: CR program led by a physician and staffed by physiotherapists. Exercise programme 6 months, consisting of 36 1‐hour supervised sessions descending in frequency. Participants provided individualised exercise prescription based on exercise test. Participants requested to exercise in their communities on non‐centre‐based exercise days to accumulated ≥ 30 minutes of MVPA on ≥ 5 days per week. Comprehensive CR participants were offered an additional 24, weekly 30‐minute education sessions, delivered in groups by a health educator, and received a validated education workbook to accompany the sessions. Components: exercise only (group 1); exercise plus education (group 2) Setting: centre‐based (with request to complete home‐based exercise in addition) Exercise programme modality: treadmill/bike/walking Total duration: 6 months Co‐interventions: education sessions provided for comprehensive CR group (group 2). Educational curriculum included: information about the CR program, their aerobic exercise prescription and safety, managing angina, irregular heartbeats, diabetes, exercising in cold and hot weather, the heart (anatomy, pathophysiology, diagnoses, and treatment) and cardiac medications risk factor profile, goal setting and action planning, resistance training, nutrition (fats, fibre, reading food labels, sodium), psychosocial risk, and sexual intimacy, how much physical activity is good, aerobic and resistance training progression, relapse planning, and graduation. Comparator: waiting‐list control – all participants received follow‐up appointments with their physician as deemed medically important. Participants in the control arm received CR after 6‐month mortality ascertained. Participants elected whether they wanted to have exercise only or comprehensive CR, or no CR. Co‐interventions: none | |
| Outcomes | Cardiovascular mortality, MI, revascularisations, hospitalisations | |
| Source of funding | Professor Britto was supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq no. 305786/2014‐8), Fundacao de Amparo a Pesquisa do Estado de Minas Gerais (FAPEMIG no. PPM‐00869‐15 and CS00290‐16) and Coordination for the Improvement of Higher Education Personnel (CAPES) | |
| Conflicts of interest | None declared | |
| Notes | Outcomes at 6 months only used for this review, as waiting‐list control participants elected which arm of the study to go into after this point. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “The randomisation sequence was generated by a professor not involved in the study using the randomization.com website in random blocks of four, with a 1:1:1 allocation ratio.” |
| Allocation concealment (selection bias) | Low risk | “To ensure allocation concealment, the principal investigator (RB) had the allocation sequence in a password‐protected file, and only provided randomisation information to the PhD student once it was confirmed the participant was eligible.” |
| Blinding of outcome assessment (detection bias) | Low risk | “A master’s student blinded to random allocation was responsible for post‐test assessments, outcome ascertainment and data entry.” |
| Incomplete outcome data (attrition bias) | High risk | Loss to follow‐up: control 9/39 (23%), comprehensive CR 5/37 (14%), exercise‐only CR 8/39 (20%) |
| Selective reporting (reporting bias) | Low risk | Outcomes reported in protocol are reported in main paper in addition to event and rate. |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (5 sites); participants were randomised 3rd day post MI Country: USA Dates participants recruited: NR Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: men and women aged 70 years or younger who were hospitalised for AMI. Exclusion criteria: none described N randomised: total: 585; intervention: 293; comparator: 292 Diagnosis (% of participants): MI: 100% Age (mean): intervention: 57 ± 8; comparator: 57 ± 8 Percentage male: intervention: 78.5%; comparator: 79.1% Ethnicity (white, %): intervention: 78.0%; comparator: 75.9% | |
| Interventions | Intervention: the exercise prescription was based on a heart rate range corresponding to 60% to 85% of the peak heart rate achieved during treadmill testing. Participants were instructed to exercise at the prescribed heart rate for 30 minutes per day 5 days per week. Participants walked briskly, jogged, rode a bicycle, or swam. After 4 weeks, the ceiling of the heart‐rate training range was raised to 100% of the peak treadmill exercise heart rate or 85% of the age‐predicted max HR. Components: exercise plus education Setting: nurse‐managed, home‐based Exercise programme modality: walking, jogging, cycling or swimming Total duration: 12 months Co‐interventions: all medically eligible participants received exercise training; all smokers received the smoking cessation intervention; and all participants received dietary counselling and, if needed, lipid‐lowering drug therapy Comparator: usual care including physician counselling on smoking cessation, nutritionist counselling on dietary change during hospitalisation, and physician‐managed, lipid‐lowering drug therapy after hospital discharge Co‐interventions: group outpatient smoking cessation programmes were available for a $50 fee. Group exercise rehabilitation, not generally provided, was available to participants at various community facilities at an average cost of $1800 to $2700 for 3 months' participation. | |
| Outcomes | Total mortality | |
| Source of funding | Grant support: By HL38874 from the National Heart, Lung, and Blood Institute, Bethesda, Maryland and a Shannon Award from the National Institutes of Health, Bethesda, Maryland. Dr. Thomas participated as a Clinical Scholar of the Robert Wood Johnson Foundation. | |
| Conflicts of interest | NR | |
| Notes | Levels of psychological distress dropped significantly for both groups by 12 months. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly allocated" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 33% lost to follow‐up; no description of withdrawals and dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes reported for all time points described. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: China Dates participants recruited: November 2016 to March 2017 Maximum follow‐up: 12 months. | |
| Participants | Inclusion criteria: participants aged 18 or older with documented coronary heart disease (including MI and unstable or stable angina) who were treated with PCI during their index admission. Participants were required to own an operational smartphone, have an active WeChat account or be willing to create one and have sufficient Chinese language proficiency to enable communication with the cardiac rehabilitation and secondary prevention coach via WeChat. Exclusion criteria: contraindications to exercise rehabilitation, an inability to operate a smartphone for the purpose of the trial (e.g. vision, hearing, and cognitive or dexterity impairment), no internet access at their place of residence, or pre‐existing comorbid disease with a life expectancy less than 1 year. N randomised: total: 312; intervention: 156; comparator: 156 Diagnosis (% of participants): post PCI (100%) Age (mean): intervention: 61.9 ± 8.7; comparator: 59.1 ± 9.4 Percentage male: intervention: 126 (81%); comparator: 128 (82%) Ethnicity (white, %): NR | |
| Interventions | Intervention: smartphone‐based home cardiac rehabilitation delivered via WeChat platform. Included a simplified and culturally sensitive WeChat based education programme addressing coronary heart disease knowledge and awareness. Exercise component: individualised walking programme based on baseline 6MWT, with time and intensity of walking increased gradually over the first 8 weeks. Physical activity monitored using WeChat’s inbuilt pedometer function to monitor step counts, along with a WeChat interfaced blood pressure and heart rate monitor. Support provided for medication adherence and risk factor modification (dietary change, lipid control, smoking cessation) provided as required by participants. Data readings automatically transmitted to a secure data portal and reviewed by cardiac rehabilitation coach on a regular basis and provided individualised feedback. Components: exercise plus education Setting: Home‐based Exercise programme modality: walking Total duration: 6 months Co‐interventions: none described Comparator: standard care as provided by their community doctors and cardiologists. Typically involves brief inpatient health education provided by a ward nurse, medication management and ad‐hoc follow‐up visits to a cardiologist or health care provider according to the participant’s self‐assessment of their own cardiovascular health Co‐interventions: none described | |
| Outcomes | HRQoL, adverse cardiac events | |
| Source of funding | Curtin University | |
| Conflicts of interest | None declared | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "The randomisation sequence was computer‐generated by permuted block randomisation (block size of 10), by staff from the study coordinating centre at Curtin University who were not involved with the recruitment of study participants." |
| Allocation concealment (selection bias) | Low risk | "The randomisation sequence was computer generated by staff from the study coordinating centre at Curtin university who were not involved with the recruitment of study participants." |
| Blinding of outcome assessment (detection bias) | Low risk | “To maintain blinding of research personnel involved in follow‐up assessments to group allocation, participants received a WeChat message before each follow‐up visit, to remind them not to reveal their allocation to study personnel. Study personnel who helped participants to set up the SMART‐CR/SP system on their smartphone or provided technology training before the commencement of the trial were not involved in assessments.” |
| Incomplete outcome data (attrition bias) | Low risk | Missing participants balanced across the two groups (intervention: 22/156 (14%); control: 25/156 (16%)) with similar reasons, and maximum‐likelihood estimation methods used in models to account for missing data. |
| Selective reporting (reporting bias) | High risk | Protocol paper (table 1) states that quality of life assessments would be carried out at 12 month follow‐up, but these data have not been reported. All‐cause mortality data not formally reported, just states that no adverse cardiac events occurred – unclear whether this is at 6 or 12 months. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: UK Dates participants recruited: between 1984 and 1988 Maximum follow‐up: 5 years | |
| Participants | Inclusion criteria: MI according to conventional WHO cardiac enzyme and ECG criteria of MI Exclusion criteria: NR N randomised: total: 124; intervention: 62; comparator: 62 Diagnosis (% of participants): MI: 100% Age (years): intervention: 54.8; comparator: 55.7 Percentage male: 98% intervention: NR; comparator: NR Ethnicity: NR | |
| Interventions | Intervention: participants received regular aerobic and local muscular endurance training three times a week for 12 months. This consisted of warm‐up and cool‐down exercises, sit ups, wall bar/bench step ups, cycle ergometry, and a major component centred on the training of aerobic capacity, using walking and jogging. Training programmes were individually designed and based on the results of regular exercise tests and trial exercise prescriptions. Components: exercise only Setting: centre Exercise programme modality: walking, jogging and cycle ergometry Total duration: 12 months Co‐interventions: none described. Comparator: received no formal exercise training throughout the same 12‐month period Co‐interventions: none described | |
| Outcomes | CV mortality; non‐fatal MI; HRQL at 4, 8, 12 months | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | The population was subdivided into groups with good and bad prognoses. There were 36 participants with a good prognosis and 26 with a poor prognosis. Each group were matched with control participants. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly allocated" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | Low risk | All participants accounted for |
| Selective reporting (reporting bias) | Low risk | All outcomes reported for all time points described. |
| Study characteristics | ||
| Methods | Study design: single‐centre open RCT Country: Finland Dates participants recruited: February 1986 to December 1987 Maximum follow‐up: 5 years | |
| Participants | Inclusion criteria: participants who underwent elective CABG Exclusion criteria: any other serious disease; > 65 years of age N randomised: total: 228; intervention: 119; comparator: 109 Diagnosis (% of participants): Previous unstable angina: intervention: 29; comparator: 31 Previous MI: intervention: 42; comparator: 46 Hypertension: intervention: 31; comparator: 23 LVEF: intervention: 70.3; comparator: 71.4 Age (mean ± SD): intervention: 54.1 ± 5.9; comparator: 54.3 ± 6.2 Percentage male: 88% Ethnicity: NR | |
| Interventions | Intervention: 6 to 8 weeks after the CABG, participants followed a 3‐week general CR program, mainly based on exercises, including 24 hours of supervised activities consisting of ergometer cycle training, ball games, outdoor activities, gymnastics and swimming. The participants were also advised to increase their physical activity in leisure time. Components: exercise and education Setting: supervised group sessions at centre Exercise programme modality: ergometer cycle training, ball games, outdoor activities, gymnastics and swimming Total duration: 3 weeks (plus an additional 5 days over a 30‐month period) Co‐interventions: participants participated in a 4‐stage CR programme over 30 months, including dietary counselling and advice about the importance of healthy nutrition and economical cooking. Comparator: all of the participants in both groups received standard postoperative care which consisted of visits to the cardiac outpatient clinic 2, 6, 12, 24, 36 and 60 months after the CABG Co‐interventions: none described | |
| Outcomes | Mortality, CABG, HRQoL: Nottingham Health Profile | |
| Source of funding | Grants from the Sauli Viikari Fund within the Cultural Foundation of Varsinais‐Suomi, Turku, Finland | |
| Conflicts of interest | NR | |
| Notes | Five years after CABG, only 20% of participants were working, despite 90% of participants being in functional classes 1‐2. Almost half of participants had retired pre‐CABG. Many other factors affect return to work post‐CABG ‐ age, education, physical requirements of the job, type of occupation, self‐employed status, non‐work income, personality type, self‐perception of working capacity and mostly length of absence from work pre‐CABG. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 13% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported for all time points described. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: the Netherlands Dates participants recruited: September 1976 to March 1978 Maximum follow‐up: 5 years | |
| Participants | Inclusion criteria: first MI within 6 months before the first psychological investigation; < 65 years; meet three psychological inclusion criteria ‐ one or more symptoms of the anxiety reaction, diminished self‐esteem, positive motivation to take part in the programme Exclusion criteria: severe cardiomyopathy, severe valvular disorders, inadequate performance on exercise, unstable angina pectoris N randomised: total: 80; intervention: 40; comparator: 40 Diagnosis (% of participants): MI: 100 % Age (years): 51 years (range 35 to 60 years); intervention: NR; comparator: NR Percentage male: intervention: 100%; comparator: 100% Ethnicity: NR | |
| Interventions | Intervention: two 1½ hour sessions of fitness training a week in a conventional gymnasium, supervised by a cardiologist. Each session consisted of a 15‐min warm‐up, gymnastics and jogging (both 15 min); sport such as volleyball, soccer and hockey (30 min), and relation exercises (15 min). Components: exercise and education Setting: supervised group sessions in centre Exercise programme modality: gymnastics, jogging and team sports Total duration: 6 months Co‐interventions: in cases of severe psychopathology, a psychologist or a psychiatrist was consulted. Comparator: home rehabilitation ‐ participants received an educational brochure with guidelines and advice about physical fitness training and jogging. Co‐interventions: treatment with either beta blockers or anticoagulants was given upon indication only and not as a prophylactic measure. | |
| Outcomes | Mortality, non‐fatal MI at 5 years | |
| Source of funding | Dutch Heart Foundation | |
| Conflicts of interest | NR | |
| Notes | Complex presentation of results. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "randomly allocated by means of a table for random numbers" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 29% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: USA Dates participants recruited: NR Maximum follow‐up: 6 months | |
| Participants | Inclusion criteria: ≤ 73 years; CAD and physical disability. CAD documented by history of MI, coronary artery bypass surgery, PCI or angiographically demonstrated CAD; have the functional use of more than 2 extremities, 1 being an arm, in order to perform the exercise test and training protocols. Exclusion criteria: uncontrolled hypertension or diabetes mellitus, clinically significant cardiac dysrhythmias, unstable angina pectoris, cognitive deficits, or other problems that would interfere with compliance to the prescribed exercise and diet protocol. N randomised: total: 88; intervention: 41; comparator: 47 Diagnosis (% of participants): CAD and a physical disability Age (mean ±SD): intervention: 62 ± 8; comparator: 63 ± 7 Percentage male: intervention: 100%; comparator: 100% Ethnicity: NR | |
| Interventions | Intervention: participants were provided with a wheelchair ramp with rollers and a telephone electrocardiographic recording device. They were instructed to exercise using the ramp which essentially transformed their wheelchair into a stationary wheelchair ergometer. Specific instructions were to exercise 5 days/week for 20 minutes a day for a total of 100 minutes each week. Components: exercise plus education Setting: home Exercise programme modality: stationary wheelchair ergometer Total duration: 6 months Co‐interventions: both groups received didactic and written dietary instruction from a registered dietitian on the American Heart Association Step I low‐cholesterol, low‐saturated fat diet. Comparator: usual care Co‐interventions: participants in the control group received dietary instruction and were instructed to follow activity guidelines provided by their primary physician and health care team. | |
| Outcomes | Total mortality, non‐fatal MI at 6 months | |
| Source of funding | United States Department of Education | |
| Conflicts of interest | NR | |
| Notes | The treatment programme decreased myocardial oxygen demand. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomized" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Low risk | "The same experienced cardiologist interpreted all echocardiograms and was unaware of randomization procedures" |
| Incomplete outcome data (attrition bias) | High risk | 32% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes reported for all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Sweden Dates participants recruited: September 1985 to March 1988 Maximum follow‐up: 5 years | |
| Participants | Inclusion criteria: 65 years or younger at the time of MI; independent living in the Health Care District after discharge from hospital; meaningful communication and rehabilitation that was not hindered by the MI or other serious illness Exclusion criteria: cerebral or cardiac disorders or serious alcohol abuse N randomised: total: 178; intervention: 87; comparator: 91 Diagnosis (% of participants): MI: 100% Angina: intervention: 32.1%; comparator: 33.3% Age (years): intervention: 55; comparator: 57.6 Percentage male: 87% intervention: 86.8%; comparator: 87.3% Ethnicity: NR | |
| Interventions | Intervention: participants and their spouses visited the hospital for a 2‐hour group session each week for 6 months. These group sessions consisted of a physical and a psychosocial part and were carried out together with a support team consisting of a physiotherapist, a physician and a rehabilitation nurse. The physical part consisted of both exercise and relaxation. Components: exercise plus psychosocial support Setting: centre Exercise programme modality: NR Total duration: 6 months Co‐interventions: the psychosocial part contained eleven themes concerning lifestyle and risks after MI, and psychosocial consequences of MI Comparator: routine cardiac follow‐up Co‐interventions: none described | |
| Outcomes | Total mortality, non‐fatal MI, revascularisations | |
| Source of funding | Swedish Heart Lung Foundation, National Association for Heart and Lung Patients, Sweden, and the County Council, Halland, Sweden | |
| Conflicts of interest | NR | |
| Notes | Positive long‐term effects on physical condition, life habits, cardiac health knowledge. No effects found for cardiac events or psychological condition. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly subdivided" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 32% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points (although absolute values not always given). |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Italy Dates participants recruited: NR Maximum follow‐up: 6 months | |
| Participants | Inclusion criteria: acute ST elevation MI Exclusion criteria: residual myocardial ischaemia, severe ventricular arrhythmias, AV block, valvular disease requiring surgery, pericarditis, severe renal dysfunction (creatinine > 2.5 mg/dL) N randomised: total: 61; intervention: 30; comparator: 31 Diagnosis (% of participants): MI: 100% Age (mean ±SD): intervention: 55.9 ± 3.1; comparator: 55.1 ± 3.7 Percentage male: intervention: 73%; comparator: 71% Ethnicity: NR | |
| Interventions | Intervention: training sessions were supervised under continuous electrocardiography monitoring. Each session was preceded by a 5‐min warm‐up and followed by a 5‐min cool‐down. Exercise was performed for 30 min on a bicycle ergometer with the target of 60% to 70% of VO2 peak achieved at the initial symptom‐limited cardiopulmonary exercise test. Exercise workload was gradually increased until the achievement of the predefined target. Components: exercise only Setting: supervised in centre Exercise programme modality: bicycle ergometer Total duration: 6 months Co‐interventions: none described Comparator: discharged with generic instructions on maintaining physical activity and a correct lifestyle Co‐interventions: none described | |
| Outcomes | Fatal/non‐fatal MI (6 month follow‐up) | |
| Source of funding | "None" | |
| Conflicts of interest | "None" | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomized" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Low risk | "The physician performing all Doppler‐echocardioraphy studies was....blinded to the patient allocation into the study protocol." |
| Incomplete outcome data (attrition bias) | Low risk | All participants were accounted for. |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Germany Dates participants recruited: March 1997 to March 2001 Maximum follow‐up: 1 year | |
| Participants | Inclusion criteria: angina pectoris according to Canadian Cardiovascular Society class I–III, with documented myocardial ischaemia during stress‐electrocardiogram and/or 99mTc scintigraphy and amenable to PCI. Only participants living within a 25 km radius of the host institution were recruited. Exclusion criteria: acute coronary syndromes or recent myocardial infarction ( < 2 months); left main coronary artery stenosis > 25%; reduced left ventricular function (ejection fraction < 40%); significant valvular heart disease; insulin‐dependent diabetes mellitus; previous coronary artery bypass graft or PCI; and conditions excluding regular exercise N randomised: total: 101; intervention: 51; comparator: 50 Diagnosis (% of participants): Stable CAD: 100% (class I to III angina pectoris) Age (years ± SEM): intervention: 62 ± 1; comparator: 60 ± 1 Percentage male: 100 % Ethnicity: NR | |
| Interventions | Intervention: during the first 2 weeks, participants exercised in the hospital 6 times/day for 10 min on a bicycle ergometer at 70% of the symptom‐limited max HR. Before discharge, a maximal symptom‐limited ergospirometry was performed to calculate the target heart rate for home training, which was defined as 70% of the maximal heart rate during symptom‐limited exercise. Participants were asked to exercise on their bicycle ergometer close to the target heart rate for 20 min per day and to participate in one 60 min group training session of aerobic exercise/week. Components: exercise only Setting: supervised exercise in hospital, followed by unsupervised at home plus weekly group training Exercise programme modality: bicycle ergometer Total duration: 2 weeks, followed by 20 min per day unsupervised at 70% plus 60 min aerobic group training per week Co‐interventions: all participants were recommended to receive acetylsalicyl acid, β‐blockers, angiotensin‐converting enzyme inhibitors and statins according to common guidelines. Comparator: stent angioplasty: “the target lesion was treated with PCI after a bolus of 10,000 IU of heparin with a 6F guiding catheter.” Co‐interventions: all participants were given acetylsalicylic acid 100 mg/d and clopidogrel 300 mg/d on the day before the procedure. | |
| Outcomes | Clinical symptoms, angina‐free exercise capacity, myocardial perfusion, cost‐effectiveness, and frequency of a combined clinical end point (death of cardiac cause, stroke, CABG, angioplasty, acute myocardial infarction, and worsening angina with objective evidence resulting in hospitalisation) | |
| Source of funding | “This study was supported by an unconditional scientific grant from Aventis Germany". | |
| Conflicts of interest | NR | |
| Notes | 2 year results of this study are reported by Walther 2008. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Patients were randomly assigned to either stent angioplasty or exercise training by drawing an envelope with the treatment assignment enclosed.” |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not described |
| Blinding of outcome assessment (detection bias) | Low risk | “Initially and after 12 months the angina pectoris status of all patients was classified according to CCS class by a physician blinded for patient assignment.” |
| Incomplete outcome data (attrition bias) | Low risk | Discontinued study, n: intervention 2/51; comparator 2/50 Disabling stroke, n: intervention 1/51; comparator 1/50 Refused angiography, n: intervention 1/51; comparator 0/50 |
| Selective reporting (reporting bias) | Low risk | All outcomes reported. |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (4 sites) Country: USA Dates participants recruited: February 1984 to March 1987 Maximum follow‐up: 4 years | |
| Participants | Inclusion criteria: men and women < 75 years of age with clinically‐indicated coronary arteriography who lived within a 5‐hour drive of Stanford University and considered capable of following the study protocol. After arteriography, participants received PCI or CABG and remained eligible if at least one major coronary artery had a segment with lumen narrowing between 5% and 69% that was unaffected by revascularisation procedures. Exclusion criteria: severe congestive heart failure, pulmonary disease, intermittent claudication, or non‐cardiac life‐threatening illnesses; no qualifying segments, medical complication occurred during angiography, left ventricular ejection fraction of less than 20%, or participant was in another research study N randomised: total: 300; intervention: 145; comparator: 155 Diagnosis (% of participants): CHD: 100% Age (mean ± SD): intervention: 58.3 ± 9.2; comparator: 56.2 ± 8.2 Percentage male: 86% Ethnicity: NR | |
| Interventions | Intervention: a physical activity programme consisting of an increase in daily activities such as walking, climbing stairs and household chores, and a specific endurance exercise training programme* with the exercise intensity based on the subject's treadmill exercise test performance. Components: exercise plus education Setting: home Exercise programme modality: stationary cycling or walking Total duration: NR Co‐interventions: each risk‐reduction participant met with a nurse to design an individualised risk‐reduction programme based on the participant's risk profile, his or her motivation, and resources for making specific changes. Participants were instructed by a dietitian in a low‐fat, low‐cholesterol, and high‐carbohydrate diet with a goal of < 20% of energy intake from fat, < 6% from saturated fat, and < 75 mg of cholesterol per day. Current or recent ex‐smokers were provided with an individualised stop‐smoking or relapse‐prevention programme by a staff psychologist. Comparator: usual care Co‐interventions: none described | |
| Outcomes | Total and CHD mortality, non‐fatal MI, revascularisation at year 1, 2, 3 and 4 | |
| Source of funding | National Heart, Lung, and Blood Institute and a gift from the Claude R. Lambe Charitable Foundation. Lipid drugs for participants in the risk reduction group provided by the Upjohn Company, Merck & Company, and Parke‐Davis, Inc. | |
| Conflicts of interest | NR | |
| Notes | *This exercise programme followed guidelines developed previously for home‐based exercise training of cardiac patients (Miller 1984). The rate of change in the minimal coronary artery diameter was 47% less in intervention than comparator. This was still significant when adjusted for age and baseline segment diameter (P = 0.03). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomization was performed using a random‐numbers table." |
| Allocation concealment (selection bias) | Low risk | "....sequentially numbered, sealed opaque envelopes for each stratification category that were provided by the biostatistician". |
| Blinding of outcome assessment (detection bias) | High risk | "The staff collecting data in the clinic were not blinded to group assignment of subjects". |
| Incomplete outcome data (attrition bias) | High risk | 18% lost to follow‐up; no description of withdrawals or dropouts. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Egypt Dates participants recruited: NR Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: age 40 to 60, within the first year after PCI, mean BMI ≤ 35 kg/m2 Exclusion criteria: people with renal failure, chronic liver disease; people with arrhythmia, chest disease and those who could not fulfil the questionnaire or cooperate through the performed procedures N randomised: total: 60; intervention: 30; comparator: 30 Diagnosis (% of participants): post PCI Age (mean ±SD): intervention: 52.6 ± 5; comparator: 53.8 ± 5 Percentage male: intervention: 70%; comparator: 67% Ethnicity: NR | |
| Interventions | Intervention: participants received mild to moderate exercise training and educational program of secondary prevention. Participants in the CR program were requested to attend their exercise program 3 times per week for 6 months. Components: exercise plus education Setting: centre‐based Exercise programme modality: bicycle ergometer Total duration: 6 months Co‐interventions: none described Comparator: participants received instructions about risk factors after PCI once, and were followed up one year later. Co‐interventions: none described | |
| Outcomes | HRQoL | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “Patients...were selected and assigned to two equal groups in number.” No further information |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of outcome assessment (detection bias) | Unclear risk | No information provided |
| Incomplete outcome data (attrition bias) | Low risk | All participants completed all follow‐up assessments. |
| Selective reporting (reporting bias) | Unclear risk | Study protocol and trial registration unavailable |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Finland Dates participants recruited: February 2011 to May 2014 Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: CAD patients who suffered from acute coronary syndrome, with coronary angiography to confirm the CAD. Exclusion criteria: NYHA class ≥ III, scheduled or emergency procedure for bypass surgery, unstable angina pectoris, severe peripheral atherosclerosis, diabetic retinopathy or neuropathy, or inability to perform regular home‐based exercises, for example, due to severe musculo‐skeletal problems N randomised: total: 204; intervention: 109; comparator: 95 Diagnosis (% of participants): intervention: NSTEMI 47 (48%); STEMI 44(45%); comparator: NSTEMI 45 (58%); STEMI 28 (36%) Age (mean): intervention: 60 ± 11; comparator: 62 ± 9 Percentage male: intervention: 80 (73%); comparator: 67 (71%) Ethnicity (white, %): NR | |
| Interventions | Intervention: the 1‐year exercise training intervention consisted of home‐based aerobic (30 to 40 min) and gym‐based strength exercises (30 to 40 min). A wrist‐worn accelerometer was provided to improve motivation and adherence. Participants instructed to continuously wear the accelerometer and monitor their own daily PA. After 6 months, home‐based exercise continued and checkpoint visits to monitor progression of exercise training were scheduled at 9 and 12 months. Components: exercise plus other components such as dietary counselling or check‐up by a medical doctor when appropriate. Setting: both centre and home (1 centre‐based resistance training session per week for 6 months). Exercise programme modality: walking, running, cycling or cross‐country skiing Total duration: 1 year Co‐interventions: None described Comparator: usual care – participants did not receive any individually‐tailored exercise prescriptions. Co‐interventions: none described | |
| Outcomes | Mortality, hospitalisations, HRQoL, cost effectiveness | |
| Source of funding | NR | |
| Conflicts of interest | JMA is a partner of ESiOR Oy, which provides health economic and outcome research services to pharmaceutical and medical device companies. The other authors report no conflicts of interest. | |
| Notes | Authors provided further data relating to clinical outcomes and HRQoL. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided regarding method used to generate allocation sequence |
| Allocation concealment (selection bias) | Unclear risk | No information provided regarding method used to conceal the allocation sequence |
| Blinding of outcome assessment (detection bias) | Unclear risk | No information provided regarding blinding of outcome assessors |
| Incomplete outcome data (attrition bias) | Unclear risk | Missing data balanced in numbers (intervention 28%, control 26%); missing data were imputed using appropriate methods, but reasons for loss to follow‐up not reported. |
| Selective reporting (reporting bias) | Unclear risk | No published protocol available, clinical trial registry available, but outcome information is limited |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: China Dates participants recruited: August 2014 to October 2016 Maximum follow‐up: 3 years | |
| Participants | Inclusion criteria: (1) fulfilling Third Universal Definition of Myocardial Infarction criteria; (2) a coronary angiography that show no artery stenosis ≥ 50% in any infarct‐related artery; (3) no other clinically overt cause or account for the acute presentation Exclusion criteria: (1) sepsis, cardiac contusion, pulmonary embolism, overlooked obstructive coronary artery disease (CAD), coronary emboli or thrombus, Takotsubo syndrome, and myocarditis; (2) limited exercise tolerance (ejection fraction <35%, chronic obstructive pulmonary disease with FEV1 <50%, severe anaemia); (3) age ≥ 75 years old; (4) physical disability or mental confusion; (5) individuals refused to participate in the trial N randomised: total: 524; intervention: 262; comparator: 262 Diagnosis (% of participants): 100% MI with PCI Age (mean ±SD): intervention: 60.6 ± 12.7; comparator 60.9 ± 12.9 Percentage male: intervention: 45.8%, comparator: 47.7% Ethnicity: NR | |
| Interventions | Intervention: participants exercised 3x per week in the hospital for 20 to 30 min on a treadmill or bicycle at 65% to 75% of symptom limited maximal heart rate. After discharge, moderate continuous training was performed – cycling or treadmill running continuously at a moderate intensity (65% to 75% max HR) for 47 mins 3x per week. Participants used MI electronic band to monitor heart rate and physicians used WeChat software to instruct and supervise individuals each month during the follow‐up period. The home‐based program consisted of 52 exercise sessions (3x per week) each year. Components: exercise only Setting: centre‐ and home‐based Exercise programme modality: treadmill walking/running or cycling Total duration: 3 years Co‐interventions: none described Comparator: control participants did not receive CR Co‐interventions: none described | |
| Outcomes | MACE at 3 years, HRQoL at 1 year | |
| Source of funding | Supported by Zhejiang Provincial Science Foundation of China under Grant No. LY20H020006 and Zhejiang Provincial Basic Public Welfare Research Program of China under Grant No. LGF19H020007 | |
| Conflicts of interest | None declared | |
| Notes | Authors emailed to request further data (mortality, MI, hospitalisation) but no response | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “randomly allocated either to an exercise‐based cardiac rehabilitation group (CR+ group) or a control group (CR− group) on a 1:1 base by drawing an envelope with the assignment enclosed.” |
| Allocation concealment (selection bias) | Unclear risk | “drawing an envelope with the assignment enclosed” |
| Blinding of outcome assessment (detection bias) | Low risk | “Only the members of The Safety and Monitoring Committee knew the group allocation. Data collectors and researchers were blind to the study group assignment.” |
| Incomplete outcome data (attrition bias) | Low risk | Loss to follow‐up balanced across groups and reasons provided. 1 year (SF‐36) intervention: 30/262 = 11%, control: 26/262 = 10% "10.7% dropout reported over the 3 year study period." |
| Selective reporting (reporting bias) | Unclear risk | Protocol paper and trial registration unavailable |
| Study characteristics | ||
| Methods | Study design: cluster‐randomised multicentre RCT Country: Australia Dates participants recruited: 18 September 1990 to 5 December 1991 Maximum follow‐up: 6 months | |
| Participants | Inclusion criteria: < 70 years with a suspected heart attack registered by the Newcastle collaborating centre of the WHO MONICA Project and discharged alive from hospital Exclusion criteria: renal failure or other special dietary requirements and those considered by their physicians to have 'endstage' heart disease N randomised: total: 450; intervention: 213; comparator: 237 Diagnosis (% of participants): MI: 100% Age (mean ± SD): intervention: 59 ± 8; comparator: 58 ± 8 Percentage male: 71% Ethnicity: NR | |
| Interventions | Intervention: a mail‐out programme designed to help participants reduce dietary fat, obtain regular exercise by walking and to quit smoking.
Components: exercise plus education Setting: home Exercise programme modality: walking Total duration: 6 months. Co‐interventions: supplementary telephone contact was also used and a letter was sent to the family doctor regarding the benefit of aspirin and β blockers for secondary prevention. Comparator: usual care Co‐interventions: none described | |
| Outcomes | Total mortality, HRQL Study outcomes assessed at 6 months | |
| Source of funding | National Health and Medical Research Council of Australia | |
| Conflicts of interest | NR | |
| Notes | Low use of preventative services (dietary, anti smoking) by both groups | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Cluster‐randomisation by GP. "All general practices were randomly allocated to intervention or usual care within those strata." Method of randomisation not described. |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 17% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Australia Dates participants recruited: June 1995 to January 1997 Maximum follow‐up: Mean = 51 weeks; range = 36 to 56 weeks post PCI | |
| Participants | Inclusion criteria: participants scheduled for PCI Exclusion criteria: major co‐morbidity such as malignancy, a history of cerebrovascular accident, or other severe, chronic debilitating disease; previous CABG or peri‐PCI complications; unemployment in previous year; MI within 1 month pre‐procedure; surgical management at home time during the 1 year duration of study. N randomised: total: 105; intervention: 54; comparator: 51 Diagnosis (% of participants): Previous MI: intervention: 52%; comparator: 51% Previous PCI: intervention: 10%; comparator: 16% Age (years): intervention: 48 (range 31 to 63); comparator: 47 (range 26 to 63) Percentage male: intervention: 83 %; comparator: 96 % Ethnicity: NR | |
| Interventions | Intervention: individualised comprehensive CR programme based on the principles of social cognitive theory involved a moderate‐intensity walking programme with a graded increase in the frequency and duration of exercise. In the 2 months post‐PCI, the clinician made 3 home visits to each participant and went walking with them as part of this visit. In addition, during home visits, participants were taught to monitor their rate of perceived exertion (RPE) during their walking programme and to document the frequency, duration and RPE of those sessions in an exercise log. Components: exercise plus psychological plus education Setting: home Exercise programme modality: walking Total duration: not specified Co‐interventions: the intervention group received the same education sessions as the control group as well as an individualised, comprehensive CR program based on the principles of social cognitive theory. Strategies used to modify risk factors included (1) goal setting, (2) self‐monitoring and feedback, (3) skills training, (4) reinforcement of target behaviours, and (5) the provision of social support by the clinician. Vocational counselling included specific recommendations regarding return to work. The clinician also made monthly calls when she provided counselling and guidance. Comparator: whilst hospitalised, control participants received two, one‐to‐one bedside education sessions; one 45 min session pre‐PCI and one 60 min session post‐PCI. Teaching media included videotapes of the procedure, photographs of coronary anatomy during the procedure, and equipment. Post‐PCI education included providing information about the pathology and risk factors for CHD and instruction on wound and medication management. Co‐interventions: the clinician made 3 monthly post‐discharge CHD information‐focused telephone calls to each control participant. | |
| Outcomes | Mortality | |
| Source of funding | “Prince Charles Hospital Private Practice Fund supported the research” | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Patients ……were randomly assigned to either control or intervention.” |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not described |
| Blinding of outcome assessment (detection bias) | High risk | Assessments do not appear to be blinded. |
| Incomplete outcome data (attrition bias) | High risk | Although all withdrawals and exclusions were clearly described and the number of withdrawals were similar in the intervention (5) and control (4) groups, 11 (20%) and 5 (10%) participants were lost from the intervention and control groups, respectively. |
| Selective reporting (reporting bias) | Low risk | All outcomes have been reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Sweden Dates participants recruited: February 1993 to December 1995 Maximum follow‐up: 2 years | |
| Participants | Inclusion criteria: (a) at least one significant stenosis suitable for PTCA and at least one additional ‐ although clinically non‐significant ‐ stenosis or plaque, measurable with quantitative computerised angiography (QCA); (b) age < 65 years; (c) employed; (d) absence of other diseases of importance for the programme or with poor prognosis; and (e) able to perform a bicycle ergometer test with a minimum exercise capacity of 70 watts. Exclusion criteria: none described N randomised: total: 87; intervention: 46; comparator: 41 Diagnosis (% of participants): treated with percutaneous transluminal angioplasty Age (mean): intervention: 53; comparator: 53 Percentage male: 83.9% Ethnicity: NR | |
| Interventions | Intervention: started with a 4‐week residential stay at the intervention unit. The programme included intense health education and activities promoting behavioural changes ‐ stress management, diet, exercise and smoking habits. Each subject was assigned a daily individual task including self‐observation, Type A behavioural drills, relaxation training and exercise. Followed by 11‐month structured maintenance programme. Components: exercise plus psychological plus education Setting: centre followed by home Exercise programme modality: NR Total duration: 12 months Co‐interventions: maintenance programme consisted of continuous self‐observation and self‐recording of important everyday lifestyle behaviours, feedback of behaviour changes, and of regular follow‐up contacts between the participant and his/her personal coach for verbal feedback, problem‐solving, and replanning discussions when needed. Comparator: standard care Co‐interventions: none described | |
| Outcomes | Cardiovascular mortality, MI, CABG, PTCA, hospitalisations, health‐related quality of life: Angina Pectoris Quality of Life Questionnaire (APQLQ) recorded during the 2 years' follow‐up. | |
| Source of funding | AMF Insurance Co., the SPP Insurance Co., and The Swedish Heart and Lung Foundation | |
| Conflicts of interest | NR | |
| Notes | 93 participants were randomly assigned to an intervention group or a control group, respectively. Six subjects (two in the intervention group and four in the control group) refused further participation in close connection to randomisation. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly assigned" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 21.8% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Sweden Dates participants recruited: "during a 2‐year period" Maximum follow‐up: 1 year | |
| Participants | Inclusion criteria: acute MI patients under 65 years of age Exclusion criteria: not stated, but individuals have been excluded for being incapable of performing strenuous training due to poor left ventricular function or arrhythmias, orthopaedic disorders, other incapacitating somatic diseases or mental disorders. N randomised: total: 69; intervention: 34; comparator: 35 Diagnosis (% of participants): post‐MI: 100% Age (mean years [range]): intervention: 55 (38 to 65); comparator: 55 (43 to 63) Percentage male: 97% Ethnicity: NR | |
| Interventions | Intervention: started 8 weeks post‐MI and participants trained over a 12‐week period for at least 45 minutes (effective time) twice a week with interval training involving large muscle groups: bicycling (10 min), callisthenics (10 min), jogging (15 min) ending with relaxation (10 min). Components: exercise only Setting: not described, but assumed in a centre Exercise programme modality: bicycling 10 mins, callisthenics 10 min, jogging Total duration: 12 weeks Co‐interventions: none described Comparator: received regular medical care with no emphasis on exercise Co‐interventions: none described | |
| Outcomes | Total mortality, non‐fatal MI & revascularisation Evaluations at 6 weeks and 1 year post‐MI | |
| Source of funding | Research support was given by Malmöhus County Council | |
| Conflicts of interest | NR | |
| Notes | Study authors found no benefit from exercise training. Outcomes were related to self‐rated levels of physical and psychological well being. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomization was performed according to random numbers in sealed envelopes". |
| Allocation concealment (selection bias) | Low risk | "Randomization was performed according to random numbers in sealed envelopes". |
| Blinding of outcome assessment (detection bias) | Low risk | Evaluations were "supervised by independent investigators". |
| Incomplete outcome data (attrition bias) | High risk | 14.5% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes reported for all time points (although absolute values not always given). |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (2 sites) Country: Canada Dates participants recruited: April 2007 to April 2008 Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: participants hospitalised for an ACS (unstable angina, non‐ST–elevation or ST elevation myocardial infarction) and willing to travel to the CR centre every 3 months to meet the clinical nurse specialist and able to read and speak French Exclusion criteria: inability to perform activities of daily living (such as feeding themselves, bathing, dressing, grooming, work, homemaking and leisure); enrolment in another research project or in a heart failure clinic where serial follow‐up creates a bias and contraindication to exercise testing; medical diagnosis of debilitating chronic illness (such as cancer without remission), musculoskeletal or neurological disorder (such as multiple sclerosis, Parkinson's disease, etc.); people with a previous history of stroke could be included if they had no residual effects related to their stroke); serious and unstable mental incapacities or major depression N randomised: total: 65; intervention: 32; comparator: 33 Diagnosis (% of participants): Unstable angina: intervention: 50%; comparator: 52% STeMI: intervention: 28%; comparator: 27% Non STeMI: intervention:22%; comparator: 21% Age (mean ± SD): intervention: 58 ± 8; comparator: 59 ± 9 Percentage male: total: 78%; intervention: 81%; comparator: 76% Ethnicity: NR | |
| Interventions | Intervention: participants received a pedometer‐based programme concomitantly with a socio‐cognitive intervention led by a clinical nurse specialist. Participants used 1 pedometer blinded and used a second one to monitor their daily steps since discharge. Components: exercise plus education plus socio‐cognitive intervention Setting: home Exercise programme modality: walking Total duration: 12 months Co‐interventions: participants received a socio‐cognitive intervention led by a clinical nurse specialist, and a blinded pedometer with instructions about how to wear the pedometer correctly during 7 consecutive days from morning to bedtime. Comparator: participants received the usual advice by the nurse or the physician, or both, at discharge regarding physical activity, diet and medication. They had no restriction to go to a centre‐based cardiac rehabilitation programme or to consult a health care professional such as a nutritionist, an exercise specialist or a psychologist. Participants in both groups received usual medical follow‐up by their own physicians (cardiologist and family physician). Co‐interventions: participants received a blinded pedometer and instructions about how to wear the pedometer correctly during 7 consecutive days from morning to bedtime. | |
| Outcomes | HRQoL | |
| Source of funding | Heart and Stroke Foundation of Canada, Research centre of Institut Universitaire de Cardiologie et Pneumologie de Québec, and Pfizer Canada | |
| Conflicts of interest | "Authors had no conflict of interest to declare". | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "They were randomly allocated to the experimental group or to the usual care group using a randomization table". |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not described |
| Blinding of outcome assessment (detection bias) | Unclear risk | Physical activity recorded by a blinded pedometer. However, blinding of assessors of other tests and measurements not described. |
| Incomplete outcome data (attrition bias) | High risk | Loss to follow‐up was high in both groups: 9/32 (28%) and 11/33 (33%) were lost to follow‐up from the intervention and control groups. |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points described either in the paper or in the supplementary material online. |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (2 sites) Country: Finland Dates participants recruited: May 1973 to October 1975 Maximum follow‐up: 3 years | |
| Participants | Inclusion criteria: participants treated in hospital for acute myocardial infarction based on WHO criteria Exclusion criteria: NR N randomised: total: 375; intervention: 188; comparator: 187 Diagnosis (% of participants): AMI: 100% Age (mean): intervention: 54.4; comparator: 54.1 Percentage male: 80.3% Ethnicity: NR | |
| Interventions | Intervention: the programme was started two weeks after discharge from hospital and consisted of medical examinations by an internist at least monthly for the first six months after AMI, then when necessary or at least 3‐monthly. A physical exercise programme, tailored to the individual’s working capacity determined in a bicycle ergometer test, was recommended, and for most participants, it was done under supervision. The rehabilitation programme was most intensive during the first three months after myocardial infarction. Components: exercise, education and psychological Setting: supervised in a centre Exercise programme modality: NR Total duration: NR Co‐interventions: besides the internist, the team included a social worker, a psychologist, a dietitian, and a physiotherapist. Health education consisted of anti‐smoking and dietary advice, and discussions on psychosocial problems. Comparator: usual care Co‐interventions: none described | |
| Outcomes | Total mortality; cardiovascular mortality (follow‐up 3 years). | |
| Source of funding | Social Insurance Institution | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly allocated" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | Low risk | 1% lost to follow‐up |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points. |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (2 sites) Country: Australia Dates participants recruited: NR Maximum follow‐up: 6 months | |
| Participants | Inclusion criteria: AMI; < 75 years of age; no angina; < 2 mm ST‐segment depression with exercise and if they attained > 7‐METS workload; left ventricular ejection fraction > 40% or no inducible ventricular tachycardia Exclusion criteria: participants were excluded if there was 2 mm ST‐segment depression with exercise or if 7‐METS workload was attained. N randomised: total: 142; intervention: 70; comparator: 72 Diagnosis (% of participants): AMI: 100% Age (mean): intervention: 56.2; comparator: 55.8 Percentage male: intervention: 89%; comparator: 86% Ethnicity: NR | |
| Interventions | Intervention: exercise (conventional treatment group): 5 week rehabilitation program consisted of exercise, education and counselling sessions that were held 2 to 4 times per week, including work at 6 weeks after AMI. Components: exercise, education and psychological Setting: NR Exercise programme modality: NR Total duration: 5 weeks Co‐interventions: the 2 groups of participants were encouraged to exercise at home on a regular basis. Participants were given the telephone numbers of the cardiologist and the nurse co‐ordinator so they could be contacted in case of problems. Comparator: control group (ERNA ‐ early return to normal activities group): return to work at 2 weeks after AMI without a formal CR programme. Co‐interventions: this group of participants was contacted over the telephone by the nurse co‐ordinator once per week for 5 weeks. The 2 groups were encouraged to exercise at home on a regular basis. Participants were given the telephone numbers of the cardiologist and the nurse co‐ordinator so they could be contacted in case of problems. | |
| Outcomes | Total mortality; fatal/non‐fatal mortality; CABG; PCI; HRQoL. Costs reported in Hall 2002. Assessment at 6 weeks and at 6 months | |
| Source of funding | National Health and Medical Research Council, Sydney, Australia | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of randomisation not described |
| Allocation concealment (selection bias) | Low risk | "Randomization schedules were generated by an independent investigator and were kept in opaque sealed envelopes." |
| Blinding of outcome assessment (detection bias) | Unclear risk | "GHPS .... scans being analyzed in a blinded fashion by an independent nuclear medicine specialist." Blinding of other outcome assessments not described |
| Incomplete outcome data (attrition bias) | High risk | 20.4% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Italy Dates participants recruited: 1984 to 1985 Maximum follow‐up: 10 years | |
| Participants | Inclusion criteria: post‐MI patients admitted at Centro Medico di Montescano in 1984 to 1985 Exclusion criteria: atrial fibrillation or abnormal sinus node function, insulin‐dependent diabetes, exercise‐induced myocardial ischaemia, and arterial BP > 160/90 N randomised: total: 95; intervention: 49; comparator: 46 Diagnosis (% of participants): uncomplicated MI: 100% Age (mean): intervention: 51; comparator: 52 Percentage male: 100% Ethnicity: NR | |
| Interventions | Intervention: the exercise sessions (30 minutes, 5 times a week) consisted of callisthenics and stationary bicycle ergometry Components: exercise, education and psychological Setting: supervised in a centre Exercise programme modality: stationary bicycle ergometry Total duration: 4 weeks Co‐interventions: sessions were held by cardiologists and psychologists, dealing with secondary prevention of cardiovascular disease and stressing dietary changes and smoking cessation. Comparator: no training Co‐interventions: all participants attended sessions, held by a cardiologist and a psychologist, dealing with secondary prevention of cardiovascular disease and stressing dietary changes and smoking cessation. | |
| Outcomes | Cardiac mortality; non‐fatal MI; CABG at 3 to 4 month intervals from the time of entry into the study for the first 3 years and contacted periodically by telephone thereafter. | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomized" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | Low risk | All participants accounted for |
| Selective reporting (reporting bias) | High risk | Results not reported for all time points collected |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (2 sites) Country: Canada Dates participants recruited: February 2009 to April 2011 Maximum follow‐up: 16 months | |
| Participants | Inclusion criteria: participants residing in either the region serviced by the Northern Health Authority of British Columbia, or the Coast Garibaldi region, which is inaccessible by road, and residents must travel by either air or ferry to reach the Vancouver area. Participants must have been admitted for either acute coronary syndrome or revascularisation procedure, be at low or moderate risk based on the American Association of Cardiovascular and Pulmonary Rehabilitation guidelines at the time, had regular Internet access (home, work, or other environment), no physical limitations to regular physical activity, and be fluent in English. Exclusion criteria: people with previous experience with cardiac rehabilitation, depression, uncontrolled diabetes mellitus, and other significant comorbidities that may interfere with effective cardiovascular management, pregnant women and those who the attending physician thought were unsuitable for participation. N randomised: total: 78; intervention: 38; comparator: 40 Diagnosis (% of participants): intervention: NSTEMI 47 (48%) STEMI 44(45%); comparator: NSTEMI 45 (58%) STEMI 28 (36%). Age (median, IQR): intervention: 61.7, 51.3‐65.2; comparator: 58.4 (52.8‐64.7). Percentage male: intervention: 34 (90%); comparator: 32 (80%) Ethnicity (white, %): NR | |
| Interventions | Intervention: web‐based virtual cardiac rehabilitation program. 30‐minute in‐person training session on the use of the virtual CR program. Participants supplied with heart rate monitor and blood pressure monitor. Virtual CR program included online intake forms (medical, risk factor and lifestyle), scheduled one on one chat sessions with the program nurse or case manager, exercise specialist and dietician (3 times each during 12 weeks), weekly education sessions with interactive slide presentations, data capture for exercise stress test and blood test results, progress notes and monthly 'ask an expert' group chat sessions. The home‐page displayed the tasks that needed to be completed for each week. Participants were asked to wear heart rate monitor whilst exercising and upload exercise data at least twice per week into the system. Components: exercise plus education Setting: home‐based Exercise programme modality: NR Total duration: 16 weeks Co‐interventions: none described Comparator: usual care (care from primary care physician); participants were given simple guidelines for safe exercising and healthy eating habits and a list of internet‐based resources. Co‐interventions: none described | |
| Outcomes | Cardiovascular‐related emergency room and major events | |
| Source of funding | Heart and Stroke Foundation of BC and Yukon and in part by Canada Health Infoway. Dr Lear holds the Pfizer/Heart and Stroke Foundation Chair in Cardiovascular Prevention Research at St. Paul’s Hospital. | |
| Conflicts of interest | None declared | |
| Notes | Authors contacted for specific clinical outcomes, but no response received. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “The random allocation was computer generated by a statistician unassociated with the trial who was the only one to have access to the list during the study.” |
| Allocation concealment (selection bias) | Low risk | “The list was incorporated into a telephone randomization system to which the randomization research coordinator called for treatment allocation. The randomization research coordinator informed the participants of their group assignment.” |
| Blinding of outcome assessment (detection bias) | Low risk | Outcome assessment reported to be blind – stress test technicians blinded, medical records were adjudicated by the study cardiologist (A.I.) blinded to the participant group assignment and categorized into emergency room visit events only and major cardiovascular events (revascularization, unstable angina requiring hospitalization, stroke, and death of any kind).” “The vCRP was evaluated in a 16‐month randomized controlled trial with blinded outcome assessment”. |
| Incomplete outcome data (attrition bias) | Low risk | Low numbers of missing data in both groups, for similar reasons (intervention 12%, control 8%). |
| Selective reporting (reporting bias) | Low risk | No published protocol, but outcomes listed in trial registration appear to be reported. |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (4 sites) Country: France Dates participants recruited: February 1981 to May 1984 Maximum follow‐up: 2 years | |
| Participants | Inclusion criteria: admitted to participating coronary care units with suspected MI; < 65 years old with typical MI, no major irreversible complication or disability Exclusion criteria: contraindication to exercise testing; i.e. recent stroke, disability of lower limbs, uncontrolled heart failure, severe rhythm disturbances, SBP > 180 mmHg, severe angina pectoris, or abnormalities triggered by baseline exercise test. N randomised: total: 182; intervention: 61; comparator (usual care): 60 counselling programme: 61 (no data analysed in this review) Diagnosis (% of participants): MI: 100% Age (mean): intervention: 51; comparator: 49 Percentage male: 100% Ethnicity: NR | |
| Interventions | Intervention: the programme started within a few days of randomisation and included three training sessions a week on a cycloergometer, walking and gymnastics. Components: exercise and education Setting: centre Exercise programme modality: cycloergometer, walking and gymnastics Total duration: 6 weeks Co‐interventions: also included respiratory physiotherapy, relaxation, recommendations on control of cardiovascular risk factors (smoking habits, diet); recommendations to continue regular physical training at the end of the 6‐week programme. Comparator: participants in the usual care group were referred to their usual private practitioner or cardiologist or both. Co‐interventions: None described | |
| Outcomes | Non‐fatal MI, angina, surgery | |
| Source of funding | Institut National de la Same et de la Recherche Medicale, by the Hospices Civils de Lyon and by the Association pour la Promotion et la Realisation d'Essais Therapeutiques | |
| Conflicts of interest | NR | |
| Notes | Only 14% of all MI patients admitted to the participating hospitals were randomised to the trial. Exclusion of women and patients > 65 accounted for 60% of exclusions. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | Low risk | No losses to follow‐up |
| Selective reporting (reporting bias) | Low risk | All outcomes reported for all time points (although absolute values not always given). |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Scotland, UK Dates participants recruited: March 1988 to March 1991 Maximum follow‐up: 1 year | |
| Participants | Inclusion criteria: confirmed MI (WHO criteria); age less than 80 years; able to speak and read English; resident in the hospital catchment area Exclusion criteria: known history of major psychiatric illness; current psychotic symptoms; evidence of dementia or continuing uncontrolled arrhythmias or heart failure N randomised: total: 176; intervention: 88; comparator: 88 Diagnosis (% of participants): MI: 100% Age (mean ±SD): intervention: 55.3 ± 10.7; comparator: 56.3 ± 10.5 Percentage male: intervention: 70.0%; comparator: 72.7% Ethnicity: NR | |
| Interventions | Intervention: heart manual consisted of six weekly sections that included education, a home‐based exercise programme, and a tape‐based relaxation and stress management programme. Components: exercise, education and psychological Setting: home Exercise programme modality: NR Total duration: 6 weeks. Co‐interventions: specific self‐help treatments were provided for psychological problems commonly experienced by post‐MI patients. Before the participant was discharged from hospital, spouses were given an audiotape that provided information and advice. After discharge, the facilitator made contact with both groups of participants at 1, 3 and 6 weeks, by telephone, at a hospital clinic, or, when neither of these was possible, by brief home visits. Comparator: the control group received an equal amount of the facilitator’s time (approximately 10 min). Co‐interventions: participants were given an extensive package of leaflets from various sources, intended to cover the same information as that presented in the manual. | |
| Outcomes | HRQoL, Hospital Anxiety and Depression Scale (HAD), General Health Questionnaire (GHQ) | |
| Source of funding | This research was supported by a grant from the Chief Scientist Office of the Scottish Home and Health Department. The British Heart Foundation donated additional computer equipment. | |
| Conflicts of interest | NR | |
| Notes | Study terminated (due to expiry of funding) before all participants reached 6‐month or 12‐month stage. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "allocated to the experimental or control group by use of a written pre‐determined randomisation protocol". Method of randomisation not described |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not described |
| Blinding of outcome assessment (detection bias) | Low risk | "Questionnaires were scored and the data entered into the statistical analysis programme by a clerical assistant based at a separate hospital who was blind both to the experimental design and to the patients." |
| Incomplete outcome data (attrition bias) | High risk | 17% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: China Dates participants recruited: January 2014 to December 2015 Maximum follow‐up: 36 months (12 month intervention plus 24 month follow‐up) | |
| Participants | Inclusion criteria: angiographically diagnosed as unprotected left main coronary artery disease (ULMCAD), and the ‘unprotected’ in this context was defined that no perfusion distal to the left main stenosis was supplied by either a patent bypass graft or a collateral vessel; underwent CABG for the first time; age ≥ 18 years; able to independently fulfil the assessment questionnaires used in the study; likely to be followed up regularly, which was evaluated by the investigators. Exclusion criteria: cardiogenic shock; cerebrovascular accident with a persistent neurological deficit before enrolment; complicated with malignancies; pregnant or lactating women. N randomised: total: 300; intervention: 150; comparator: 150. Diagnosis (% of participants): CABG (100%). Age (mean, SD): intervention: 63.1 ± 9.7; comparator: 62.8 ± 10.7. Percentage male: intervention: 121 (80.7%); comparator: 115 (76.7%). Ethnicity (white, %): NR | |
| Interventions | Intervention: Comprehensive rehabilitation and intensive education (CRIE) program consisting of 4 components: 1. CAD‐related health education (1/wk for 2 months) – lectures covering basic knowledge of disease, primary therapeutic strategies, risk factors, antiplatelet and anticoagulant therapy, BP management, lipid, glucose, and uric acid, prevention of upper GI mucosal injury, rehabilitation management about exercise, diet and nutrition, psychological care and good lifestyle formation. 2. Exercise guidance and formation (1/month for 10 months) – formulating an individualised exercise plan covering exercise mode: low intensity walking, moderate intensity aerobics (e.g. jogging, gymnastics, tai chi, bicycling), and moderate to high resistance training (e.g. mountain climbing, mid‐distance sprint); duration 60 to 90 mins each time; frequency 3 to 5 times per week; intensity: RPE 11 to 13. Monthly supervision and guidance by motivational interviewing. 3. Risk factor control (1/month for 10 months): diet control, alcohol and cigarette cessation, management of blood pressure, lipid, glucose and uric acid. Monthly supervision and guidance by motivational interviewing. 4. Psychological nursing (1/month for 10 months): making a holistic assessment of each participants' physical, functional, psychological, social and spiritual status; identifying potential issues in psychological aspects; eliminating negative emotions and improving compliance; providing music therapy. Components: exercise plus education and psychological nursing Setting: centre‐based lectures, with home‐based exercise Exercise programme modality: low‐intensity walking, moderate‐intensity aerobics Total duration: 12 months Co‐interventions: none described Comparator: participants provided discharging guidance and a CAD‐related health education manual (same as distributed to intervention group). Provided rehabilitation recommendations and medication consultation through telephone calls or clinic visits according to need. Co‐interventions: None described | |
| Outcomes | Major adverse cardiac and cerebrovascular events (composite outcome), HRQoL | |
| Source of funding | Supported by National Clinical Key Speciality Construction Project | |
| Conflicts of interest | None declared | |
| Notes | We contacted authors, requesting specific clinical outcome data, but received no response. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "The randomisation sequence was computer‐generated using SAS 9.1" |
| Allocation concealment (selection bias) | Low risk | "The assignment of patients was performed by an independent nurse with the use of sealed envelopes" |
| Blinding of outcome assessment (detection bias) | Unclear risk | No information provided regarding blinding of outcome assessment. |
| Incomplete outcome data (attrition bias) | Unclear risk | Number of participants lost to follow‐up provided ( < 20%) and appear balanced across groups, but no reasons provided |
| Selective reporting (reporting bias) | Unclear risk | No published protocol paper or trial registration |
| Study characteristics | ||
| Methods | Study design: single‐blind multicentre RCT (2 sites) Country: New Zealand Dates participants recruited: 2010 to 2012 Maximum follow‐up: 24 weeks | |
| Participants | Inclusion criteria: aged 18 years or more, with a diagnosis of IHD, defined as angina, myocardial infarction, revascularisation, including angioplasty, stent or coronary artery bypass graft within the previous 3 to 24 months. All participants were clinically stable as outpatients, able to perform exercise, able to understand and write English, and had access to the Internet (e.g. at home, work, library or through friends or relatives). Exclusion criteria: participants were excluded if they had been admitted to hospital with heart disease within the previous 6 weeks; had terminal cancer, or had significant exercise limitations other than IHD N randomised: total: 171; intervention: 85; comparator: 86 Diagnosis (% of participants): IHD: 100% MI: 74% Age (mean ±SD): total: 60.2 ± 9.3; intervention: 61.4 ± 8.9; comparator: 59.0 ± 9.5 Percentage male: total: 81%; intervention: 81%; comparator: 81% Ethnicity: NZ Maori: total: 8%; intervention: 7%; comparator: 8% NZ European/other: total: 76%; intervention: 78%; comparator: 76% | |
| Interventions | Intervention: the HEART programme is a personalised, automated package of text messages via mobile phones aimed at increasing exercise behaviour over 24 weeks. Participants received six messages per week for the first 12 weeks, five messages per week for 6 weeks, and then four messages per week for the remaining 6 weeks. Components: exercise Setting: home Exercise programme modality: moderate to vigorous aerobic‐based exercise (e.g. walking and household chores) Total duration: 24 weeks Co‐interventions: focus on altering the key mediators of behaviour change, including self‐efficacy, social support and motivation. Comparator: usual care, with encouragement to be physically active and attend a cardiac club. Co‐interventions: all participants were free to participate in any other CR service or support that they wished to use (e.g. participating in community‐based CR education sessions on modifying CVD risk factors and psychological support), as well as encouragement to be physically active. | |
| Outcomes | HRQoL, costs | |
| Source of funding | Health Research Council of New Zealand and the Heart Foundation. Dr Maddison was supported by a Heart Foundation Research Fellowship and a Health Research Council Sir Charles Hercus Research Fellowship. | |
| Conflicts of interest | None declared | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "....were randomly allocated..... by means of a central computerized service. Randomization was conducted using the minimization method, stratifying by sex (male and female), ethnicity (Maori – indigenous – and non‐Maori), and exercise history" |
| Allocation concealment (selection bias) | Low risk | "Allocation concealment was maintained up to the point of randomization" |
| Blinding of outcome assessment (detection bias) | Low risk | "This was a single‐blind trial, where outcome assessors were blinded to treatment allocation" |
| Incomplete outcome data (attrition bias) | Low risk | Loss to follow‐up was well reported and was similar in both groups. 10/85 (12%) and 8/86 (9%) were lost to follow‐up from the intervention and control groups, respectively. |
| Selective reporting (reporting bias) | Low risk | All outcomes described in the methods section are reported in results. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: India Dates participants recruited: NR Maximum follow‐up: 1 year | |
| Participants | Inclusion criteria: chronic stable angina and angiographically proven CAD Exclusion criteria: recent (within last six months) MI or unstable angina N randomised: total: 42; intervention: 21; comparator: 21 Diagnosis (% of participants): chronic stable angina and angiographically proven CAD Age (years): intervention: 51; comparator: 52 Percentage male: 100% Ethnicity: NR | |
| Interventions | Intervention: participants and their spouses spent four days at a yoga residential centre where they underwent training in various yogic lifestyle techniques. Subsequently they carried out the yogic exercises at home for an average of 90 min daily. The programme included health rejuvenating exercises, breathing exercises, relaxation, meditation, reflection, stress management, dietary control and moderate aerobic exercises. Components: exercise, education and psychosocial support Setting: centre followed by home Exercise programme modality: yoga and "moderate aerobic exercises" Total duration: 1 year Co‐interventions: relaxation, reflection, stress management, dietary control Comparator: managed by conventional methods i.e. risk factor control and American Heart Association step I diet. Co‐interventions: none described | |
| Outcomes | total mortality; CABG; PCI Assessments are baseline and 1 year | |
| Source of funding | This study was supported in part by a grant from the Central Research Institute of Yoga, Ministry of Health, Government of India. | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomized" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Low risk | "Two independent observers who were blinded to group allocation analysed all arteriograms." |
| Incomplete outcome data (attrition bias) | Low risk | All participants accounted for |
| Selective reporting (reporting bias) | High risk | While participants were given a clinical exam and clinical investigations every month, only the results at 1 year are presented. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Italy Dates participants recruited: NR (48‐month period) Maximum follow‐up: 14 months | |
| Participants | Inclusion criteria: > 56 years; referred to unit for functional evaluation 4 to 6 weeks after MI Exclusion criteria: severe cognitive impairment or physical disability, left ventricular EF < 35%, contraindications to vigorous physical exercise, eligibility for myocardial revascularisation because of low‐effort myocardial ischaemia, refusal, or living too far from the unit N randomised: total: 270; intervention: 90; home: 90; comparator: 90 Diagnosis (% of participants): MI: 100% Age (mean [range]): 69 years [46 to 86] Percentage male: 67.8% Ethnicity: NR | |
| Interventions | Partcipants were randomised to outpatient, hospital‐based CR (Hosp‐CR), home‐based CR (Home‐CR), or no CR within 3 predefined age groups. Intervention: Hospital‐CR: programme consisted of 40 exercise sessions: 24 sessions (3/wk) of endurance training on cycle ergometer (5‐min warm‐up, 20‐min training at constant workload, 5‐min cool‐down, 5‐min post‐exercise monitoring) plus 16 (2/wk) 1‐hr sessions of stretching and flexibility exercises. Home‐CR: 4 to 8 supervised instruction sessions in CR unit, where taught how to perform training at home; then participants received exercise prescription similar to Hosp‐CR group. Setting: centre or home Components: Hospital‐CR: exercise plus psychosocial support Home‐CR: exercise plus psychosocial support Exercise programme modality: cycle ergometer Total duration: 8 weeks Co‐interventions: participants received cardiovascular risk factor management counselling twice per week and were invited to join a monthly support group together with family members. Comparator: participants randomised to no CR were referred back to their family physicians. Co‐interventions: participants received asingle structured education session on cardiovascular risk factor management. | |
| Outcomes | HRQoL at month 2, 8 and 14 Costs over study duration | |
| Source of funding | National Research Council (CNR), the University of Florence, and the Regional Government of Tuscany, Italy | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Low risk | "Testing personnel were blinded to patient assignment." |
| Incomplete outcome data (attrition bias) | High risk | 38 (14.1%) dropped out; clinical event data for these participants not reported per treatment group |
| Selective reporting (reporting bias) | Low risk | Changes in all outcomes reported for all time points (although absolute values not given) |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Spain Dates participants recruited: NR (2‐year enrolment period) Maximum follow‐up: 10 years | |
| Participants | Inclusion criteria: male participants diagnosed with AMI and admitted to the coronary care unit; age < 65 years; low risk (hospital course without complications, absence of signs of myocardial ischaemia, functional capacity > 7 metabolic equivalent time (MET), ejection fraction > 50%, and absence of severe ventricular arrhythmias) Exclusion criteria: none described N randomised: total: 180; intervention: 90; comparator: 90 Diagnosis (% of participants): AMI: 100% Anterior: intervention: 40.0%; comparator: 48.3% Inferior/posterior: intervention: 48.3%; comparator: 46.3% Non‐Q wave: intervention: 11.6%; comparator: 5.3% Age (mean ± SD): intervention: 50.3 ± 6; comparator: 52.6 ± 9 Percentage male: 100% Ethnicity: NR | |
| Interventions | Intervention: Multidisciplinary CR programme, consisting of:
Supervised training was complemented by progressively increasing daily walks of 1 hour in duration, when participants tried to maintain the heart rate achieved during training. Walks were undertaken by participants individually and were unsupervised. Components: exercise plus psychological plus education plus return to work counselling Setting: individualised supervised programme in hospital gym Exercise programme modality: physiotherapy and aerobic training on mats or an exercise bicycle Total duration: 3 months Co‐interventions: participants received a psychological programme including behaviour modification techniques, group therapy, and relaxation sessions, an educational programme on modifying lifestyle and controlling coronary risk factors, and return to work counselling. Comparator: participants received conventional treatment Co‐interventions: none described | |
| Outcomes | Mortality, MI | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "The 180 patients were randomized into 2 groups”. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment is not described. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | Low risk | 7/90 lost to sample in intervention group and 4/90 lost to sample in control group. |
| Selective reporting (reporting bias) | Low risk | All outcomes described in methods section are reported at all time points. |
| Study characteristics | ||
| Methods | Study design: RCT; participants randomised 3 weeks post‐MI Country: USA Dates participants recruited: NR Maximum follow‐up: 6 months | |
| Participants | Inclusion criteria: men < 70 years with MI documented by the combination of characteristic elevation of serum creatine kinase or oxaloacetic transaminase, a history of prolonged chest pain consistent with myocardial infarction, and the appearance of new Q waves or evolutionary ST segment changes. Exclusion criteria: conditions that precluded symptom‐limited treadmill testing 3 weeks after infarction. e.g. congestive heart failure, unstable angina pectoris, valvular heart disease, atrial fibrillation, bundle branch block, stroke, limiting orthopedic abnormalities, peripheral vascular disease, chronic obstructive pulmonary disease and obesity, a history of coronary artery bypass graft (CABG) surgery, reinfarction before testing, and intercurrent noncardiac illness. N randomised: total: 198; group 1: 66; group 2: 61; group 3: 34; comparator: 37 Diagnosis (% of participants): MI: 100% Age (mean ±SD): 52 ± 9 Percentage male: 100% Ethnicity: NR | |
| Interventions | Participants were randomly assigned to one of four exercise protocols:
Regimens of home and group exercise training were designed to provide a similar intensity and duration of exercise training. Intervention: home training Components: exercise only Setting: home Exercise programme modality: stationary cycling or walking Total duration: 8 weeks or 26 weeks. Co‐interventions: none described Intervention: group training Components: exercise Setting: supervised in centre Exercise programme modality: walking or jogging Total duration: 8 weeks or 26 weeks Co‐interventions: none described Comparator: usual care (treadmill testing for the first time at 26 weeks) Co‐interventions: none described | |
| Outcomes | CHD mortality, non‐fatal MI and revascularisation | |
| Source of funding | Supported by grant from the NHLBI, Bethesda, and by a grant from the PepsiCo Foundation, Purchase, NY | |
| Conflicts of interest | NR | |
| Notes | Low rate of cardiac events reflects identification of low risk population | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 5% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes reported for all time points |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Norway Dates participants recruited: NR Maximum follow‐up: 6 months | |
| Participants | Inclusion criteria: successful PCI, defined as a residual diameter stenosis after stent implantation of < 20% of the reference diameter Exclusion criteria: history of myocardial infarction (MI) or CABG; significant valvular heart disease; > 80 years; inability to give informed consent; inability to participate in regular training due to residency, work situation or comorbidity; any known chronic inflammatory disease other than atherosclerosis, or planned surgery within the next 6 months. N randomised: total: 40; intervention: 20; comparator: 20 Diagnosis (% of participants): Stable angina, post PCI: intervention: 85%; comparator: 95% Unstable angina, post PCI: intervention: 15%; comparator: 5% Age (mean ± SD): intervention: 57 ±14; comparator: 61 ± 10 Percentage male: Total: 21%; intervention: 18%; comparator: 25% Ethnicity: NR | |
| Interventions | Intervention: starting 11 ± 4 days after PCI, the training model included 10 min warm‐up at 60% to 70% of max HR, followed by 4 min intervals at 80% to 90% of max HR, when participants were riding an ergometric bicycle or were running. Intervals were interrupted by 3 minutes of active recovery at 60% to 70% of maximal heart rate. Afterwards, there was a 5‐min cool‐down, 10 min of abdominal and spine resistance exercises, and 5 min of stretching and relaxing. The training sessions were monitored with individual pulse watches allowing the participant to achieve the target heart rate. Components: exercise only Setting: centre‐based supervised training in groups of 10 Exercise programme modality: ergometric bicycle or running Total duration: 6 months Co‐interventions: none described Comparator: participants received usual care (not described), including drug therapy of clopidogrel, aspirin and statins Co‐interventions: none described | |
| Outcomes | Mortality, MI, and revascularisations | |
| Source of funding | Norwegian Health Association, Oslo, Norway, and Stavanger University Hospital | |
| Conflicts of interest | NR in this paper, but none declared in Munk 2011 | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “The order of treatments within the block was randomly permuted by a computer‐generated sequence.” |
| Allocation concealment (selection bias) | Low risk | “The investigator, who recruited patients into the trial, was unaware of the group to which a participant was allocated.” |
| Blinding of outcome assessment (detection bias) | Low risk | “All scans were analysed twice with EchoPACtm (GE Vingmed Ultrasound) by two blinded investigators. Two experienced cardiologists independently interpreted the images in a blinded manner.” However, not clear if blinded for clinical events and exercise capacity. |
| Incomplete outcome data (attrition bias) | Low risk | “No patient was lost to follow up.” |
| Selective reporting (reporting bias) | Low risk | All outcomes described in methods were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Kingdom of Saudi Arabia Dates participants recruited: 8 June 2008 to 3 January 2010 Maximum follow‐up: 6 months | |
| Participants | Inclusion criteria: participants admitted for coronary artery bypass graft (CABG) surgery Exclusion criteria: history of ejection fraction less than 30%, poor mobility leading to difficulty in walking, chronic atrial fibrillation, repeat CABG or implantable pacemaker were excluded from the study. N randomised: total: 49; intervention: 28; comparator: 21 Diagnosis (% of participants): post‐CABG: 100% Age (years): intervention: 56.75 (range 53.6 to 59.8); comparator: 57.22 (range 54.4 to 60.2) Percentage male: 100% Ethnicity: NR | |
| Interventions | Intervention: whilst in the cardiac ward, the participants walked daily for 30 minutes. Additionally, before discharge, the participants climbed one flight of stairs and were then asked to walk unaided at a comfortable pace 30 minutes per day until they completed the 6‐month home‐based CR programme. Components: exercise plus education Setting: at home, unsupervised with telephone support Exercise programme modality: walking Total duration: 6 months Co‐interventions: participants received pre‐CABG, immediately post‐CABG, and home‐based CR program, including education, food management education and a one‐hour group workshop which included advice on modifiable and non‐modifiable risk factors, change of lifestyle, active life, stress, and then discussed participant’s problems and feelings during the past 2 months. This group workshop was repeated 4 months and 6 months after hospital discharge. Comparator: the control group received standard hospital care, including regular advice from doctors and followed usual hospital instructions. This did not include a rehabilitation programme or telephone calls by the study authors. Co‐interventions: None described | |
| Outcomes | Mortality, MI, hospitalisation and HRQoL | |
| Source of funding | "Work was not supported or funded by any drug company.” | |
| Conflicts of interest | “Authors have no conflict of interests.” | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “Patients who consented to participate in the study, were randomly assigned....” |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not described |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 7/50 participants (14%) lost to follow‐up: one from control group died (1/22, 5%) and 6 from the intervention group (6/28, 21%) could not complete the study requirements. |
| Selective reporting (reporting bias) | Low risk | All outcomes described in methods are reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Denmark Dates participants recruited: January 2007 to July 2008 Maximum follow‐up: 12 months; mortality data after 5.5 years (mean follow‐up 4½ years) | |
| Participants | Inclusion criteria: participants ≥ 65 years with a recent coronary event defined as acute myocardial infarction (MI), percutaneous transluminal coronary intervention (PCI) or coronary artery bypass graft (CABG) and who declined participation in centre‐based CR Exclusion criteria: mental disorders (dementia), social disorders (severe alcoholism and drug abuse), living in a nursing home, language barriers or use of wheelchair N randomised: total: 40; intervention: 19; comparator: 21 Diagnosis (% of participants): Previous MI: intervention: 31.7; comparator: 38.1 Previous PCI: intervention: 21.1; comparator: 23.8 Previous CABG: intervention: 0; comparator: 9.5 Heart failure LVEF ≤ 45%: intervention: 50.0; comparator: 42.9 Event prior to entry into the study: Post‐MI without invasive procedure: intervention: 0; comparator: 19.1 Post‐PCI: intervention: 84.2; comparator: 66.7 Post‐CABG: intervention: 15.8; comparator: 14.3 Age (mean ± SD): intervention: 77.3 ± 6.0; comparator: 76.5 ± 7.7 Percentage male: intervention: 63.2%; comparator: 52.3% Ethnicity: NR | |
| Interventions | Intervention: individualised exercise programmes followed the international recommendations with 30 min exercise/day including 5‐ to 10‐min warm‐up (e.g. slow walking) and 10‐min cool‐down at a frequency of 6 days/week at an intensity of 11 to 13 on the Borg scale. For very disabled participants, the exercise programmes were of shorter duration but then repeated several times a day. At 4 and 5 months, a telephone call was made by the cardiologist to encourage continuous exercising and to answer any medical questions. Components: exercise plus risk factor management Setting: unsupervised individualised programme at home, with telephone support Exercise programme modality: individualised Total duration: 12 months Co‐interventions: the participants consulted a cardiologist at baseline and after 3, 6 and 12 months, regarding risk factor intervention and medical adjustment. All participants were offered dietary counselling and, if required, smoking cessation. Comparator: participants received usual care. They received consultation with a cardiologist, and telephone calls at 4 and 5 months. They were not offered exercise education or dietary counselling. Co‐interventions: participants were offered risk factor intervention and medical adjustment by a cardiologist at baseline and after 3, 6 and 12 months. | |
| Outcomes | Mortality, HRQoL | |
| Source of funding | Velux Foundations | |
| Conflicts of interest | None | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Patients were randomised in alternated block sizes of 4–6 using computer‐generated randomly permuted blocks”. |
| Allocation concealment (selection bias) | Low risk | “An impartial person, not related to the study, randomised the patients”. |
| Blinding of outcome assessment (detection bias) | Unclear risk | “Because of the nature of the intervention, concealment of randomisation was not feasible with regard to both patients and researcher”. It is not clear if outcome measures are blinded. |
| Incomplete outcome data (attrition bias) | Low risk | “A total of nine patients died during a mean follow‐up of 4.5 years (usual care group n=5 and home group n=4). There was no loss to follow‐up.” |
| Selective reporting (reporting bias) | High risk | Although the methods state that outcomes were measured at 3, 6 and 12 months, only exercise capacity is reported at 6 months. |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (6 sites) Country: Canada Dates participants recruited: NR Maximum follow‐up: 1 year | |
| Participants | Inclusion criteria: diagnosis of AMI and scoring > 5 on the short form of the Beck Depression Inventory or > 43 on the Spielberger State Anxiety Inventory or > 42 on the Spielberger Trait Anxiety Inventory while still in hospital Exclusion criteria: residence > 30 miles from the Health Sciences Centre; inability to exercise due to N randomised: total: 201; intervention: 99; comparator: 102 Diagnosis (% of participants): MI: 100% Age (mean ± SD): intervention: 52.9 ± 9.5; comparator: 52.7 ± 9.5 Percentage male: intervention: 88%; comparator: 90% Ethnicity: NR | |
| Interventions | Intervention: participants attended 50‐min exercise sessions twice a week for 8 consecutive weeks. These sessions were held in a hospital gymnasium under the direct supervision of a cardiologist and qualified exercise specialists. There was a I0‐min group warm‐up at the beginning of each session; stationary cycle ergometry, treadmill walking and arm ergometry followed for 20 to 30 minutes. A cool‐down, involving low‐intensity activities, concluded the exercise session. Components: exercise and behavioural counselling Setting: centre Exercise programme modality: stationary cycle ergometry, treadmill walking and arm ergometry Total duration: 8 weeks Co‐interventions: the cognitive behavioural group intervention, facilitated by group leaders without formal training in counselling, consisted of 8 sessions of 90 minutes complemented by progressive relaxation training at the end of the session. Both participant and spouse were invited to attend the group sessions. Comparator: conventional care Co‐interventions: none described | |
| Outcomes | Mortality. Health‐related quality of life: QOLMI time trade‐off. Cost data reported in Oldridge 1993 | |
| Source of funding | This work was supported by the National Health Research and Development Programme, Health and Welfare, Canada | |
| Conflicts of interest | NR | |
| Notes | Both groups improved over 12 months, with the biggest changes occurring in the first 8 weeks. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomized" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | High risk | "the investigators were not blinded to allocation" |
| Incomplete outcome data (attrition bias) | High risk | For the primary outcome ‐ HRQL ‐ 9% lost to follow‐up; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (2 sites) Country: USA Dates participants recruited: NR Maximum follow‐up: 5 years | |
| Participants | Inclusion criteria: age 35 to 75 years, male or female; residence in the greater San Francisco area; one, two, or three vessel CAD (defined as any measurable coronary atherosclerosis in a non‐dilated or non‐bypassed coronary artery); LVEF > 25% Exclusion criteria: other life‐threatening illnesses; MI during the preceding 6 weeks, history of receiving streptokinase or alteplase; currently receiving lipid‐lowering drugs; scheduled to receive CABG N randomised: total: 48; intervention: 28; comparator: 20 Diagnosis (% of participants): moderate to severe CAD: 100% Age (mean ±SD): Intervention: 56.1 ± 7.5; Comparator: 59.8 ± 9.1 Percentage male: Intervention: 95%; Comparator: 79% Ethnicity: NR | |
| Interventions | Intervention: the intervention began with a week‐long residential retreat at a hotel to teach the lifestyle intervention to the experimental‐group participants. Participants then attended regular group support meetings (4 h twice a week). Participants were individually prescribed exercise levels (typically walking) according to their baseline treadmill test results. Participants were asked to exercise for a minimum of 3 h per week and to spend a minimum of 30 min per session exercising within their target heart rates. Components: exercise plus psychosocial and diet Setting: centre Exercise programme modality: typically walking Total duration: 1 year Co‐interventions: stress management, low fat vegetarian diet, group psychosocial support Comparator: usual care Co‐interventions: none described | |
| Outcomes | CHD mortality, non‐fatal MI, revascularisation Assessment at baseline and after 1 year and 5 years | |
| Source of funding | National Heart, Lung, and Blood Institute of the National Institutes of Health, the Department of Health Services of the State of California, Gerald D. Hines Interests, Houston Endowment Inc, the Henry J. Kaiser Family Foundation. the John E. Fetzer Institute, Continental Airlines, the Enron Foundation, the Nathan Cummings Foundation, the Pritzker Foundation, the First Boston Corporation, Quaker Oats Co., Texas Commerce Bank, Corrine and David Gould, Pacific Presbyterian Medical Center Foundation, General Growth Companies, Arthur Andersen and Co. | |
| Conflicts of interest | NR | |
| Notes | Intervention group had 91% reduction in reported frequency of angina after 1 year and 72% after 5 years; comparator group had 186% increase in reported frequency of angina after 1 year and 36% decrease after 5 years. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly assigned" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Low risk | "Investigators carrying out all medical tests remained unaware of both patient group assignment and the order of the tests". |
| Incomplete outcome data (attrition bias) | High risk | 45/93 (48%) of randomised participants did not participate; no description of withdrawals or dropouts |
| Selective reporting (reporting bias) | High risk | Outcomes are only presented for 1 year, although blood tests were also taken at 6 months. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: India Dates participants recruited: February 2007 to July 2010 Maximum follow‐up: 18 months | |
| Participants | Inclusion criteria: “Patients with proven CAD were recruited. Disease was diagnosed by history of electrocardiograms, echocardiography and treadmill testing. Their willingness to complete the entire span of the project (18 months) was assured.” Exclusion criteria: “Patients who had other co‐morbid conditions (e.g. malignant hypertension, diabetes mellitus, chronic obstructive pulmonary disease, asthma, diseases of the nervous system, endocrinal disorders, congenital heart disease) and patients with known complications of CAD, those on pacemakers, and those who had undergone bypass surgery were excluded from the study” N randomised: total: 258; intervention: 129; comparator: 129 Diagnosis (% of participants): participants with proven CAD (100%) Age (mean ±SD): Intervention: 59.1 ± 9.9; Comparator: 56.4 ± 10.9 Percentage male: intervention: 80%; comparator: 81% Ethnicity: NR | |
| Interventions | Intervention: yogic intervention plus medication performed in the Department of Physiology at Chhatrapati Sahuji Maharah Medical University under the guidance and supervision of yoga experts. 35 to 40 minutes per day, for 5 days per week over 18 months. Components: exercise only Setting: centre Exercise programme modality: yoga Total duration: 18 months Co‐interventions: none described Comparator: medication only Co‐interventions: none described | |
| Outcomes | All‐cause mortality reported in study flow diagram | |
| Source of funding | Department of AYUSH, Ministry of Health and Family Welfare, Government of India | |
| Conflicts of interest | None declared | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Using a random number generator... A professional not associated with this study generated the randomization scheme.” |
| Allocation concealment (selection bias) | Low risk | “A professional not associated with this study generated the randomization scheme.” |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding of yoga instructors, study personnel and outcome assessors was not described |
| Incomplete outcome data (attrition bias) | High risk | 19% in the intervention group and 20% in the control group lost to follow‐up. Reasons were described and "Patients who dropped out of the study did not differ significantly in terms of age and sex". |
| Selective reporting (reporting bias) | Unclear risk | No published protocol or trial registration available. Triallists state that this study is part of “a larger study conducted under the Extra Mural Research Project of the Department of Department of Ayurveda, Yoga & Naturopathy, Unani, Siddha and Homoeopathy (AYUSH), at the Indian Ministry of Health and Family Welfare” but no reference provided. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT with 3 arms (supervised cycling vs home‐based walking vs control) Country: Russia Dates participants recruited: NR Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: male with coronary artery disease, planned myocardial revascularisation surgery (cardiopulmonary bypass) Exclusion criteria: age over 65 years, unstable angina pectoris, recent MI (less than 30 days), changes in ECG making it difficult to interpret the QRS complex and ST segment, atrial fibrillation and other serious cardiac arrhythmias, decreased LVEF ( < 40%), pulmonary hypertension, respiratory and renal failure, metabolic (obesity, decompensated diabetes mellitus) and concomitant diseases that prevent exercise N randomised: total: 114; intervention 1 (cycling): 36; intervention 2 (walking): 36; comparator: 42 Diagnosis (% of participants): CABG (100%) Age (median, IQR): intervention 1 (cycling): 57, 51‐59; intervention: 56, 51‐57; comparator: 56 (51‐57) Percentage male: 100% Ethnicity (white %): NR | |
| Interventions | Intervention: Group 1: controlled aerobic exercise carried out on a stationary bike Group 2: independent dosed walking at home, with training pace controlled by pedometer Components: Exercise only Setting: group 1 ‐ hospital‐based; group 2 ‐ home‐based Exercise programme modality: group 1 ‐ cycling; group 2 ‐ walking Total duration: 3 months Co‐interventions: None described Comparator: Medication plus monthly telephone follow‐up Co‐interventions: None described | |
| Outcomes | HRQoL (results not reported) | |
| Source of funding | Not reported | |
| Conflicts of interest | None declared | |
| Notes | Paper translated from Russian. Authors contacted to request HRQoL data, but no response received | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | By simple randomisation using a table of random numbers |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding of outcome assessment (detection bias) | Unclear risk | No information provided |
| Incomplete outcome data (attrition bias) | Low risk | Number randomised and reported in final outcomes the same, appears to be no dropouts |
| Selective reporting (reporting bias) | High risk | Methods state that at each time point, participants underwent clinical examination, echocardiography, quality of life assessment and determination of exercise tolerance, but these results are not reported. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Russia Dates participants recruited: January 2015 ‐ December 2016 Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: participants with coronary artery disease who underwent CABG with the presence of arterial erectile dysfunction Exclusion criteria: confirmed endocrine causes of erectile dysfunction, acquired primary hypogonadism, anatomical deformities of the external genital organs, drug‐related decrease in secretion testosterone, cancer, history of stroke, radical interventions on the pelvic organs, decompensated somatic diseases, low (< 50 W) exercise tolerance (TFN), arterial hypertension with diastolic blood pressure above 100 mmHg, recent myocardial infarction (< 28 days), complex rhythm and conduction disturbances (paroxysmal tachycardia, atrial fibrillation, polytopic and group ventricular extrasystoles, atrioventricular blockade (II‐III degree), chronic heart failure (class III, IV), subacute course of chronic non‐specific lung diseases, postoperative thrombophlebitis of the lower extremities, diabetes mellitus, a variety of neurological disorders that could interfere with cycling. N randomised: total: 114; intervention: 53; comparator: 61 Diagnosis (% of participants): CABG (100%) Age (mean, SD): intervention: 56.9 ± 4.7; comparator: 57.1 ± 4.8 Percentage male: 100% Ethnicity (white %): NR | |
| Interventions | Intervention: controlled physical training in the form of cycling training Components: exercise only Setting: centre‐based Exercise programme modality: cycling Total duration: NR Co‐interventions: none described Comparator: no physical training Co‐interventions: none described | |
| Outcomes | Methods states: myocardial infarction (MI), episodes of unstable angina pectoris, ischaemic stroke, lethal outcomes. But these are not reported in the results. | |
| Source of funding | Not reported | |
| Conflicts of interest | None declared | |
| Notes | Paper translated from Russian. Authors contacted to request clinical outcome data, but no response received | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information about methods used to generate allocation sequence |
| Allocation concealment (selection bias) | Unclear risk | No information about methods used to conceal allocation sequence |
| Blinding of outcome assessment (detection bias) | Unclear risk | No information provided about blinding of outcome assessors |
| Incomplete outcome data (attrition bias) | Low risk | Appears to be no missing outcome data |
| Selective reporting (reporting bias) | High risk | Methods report collection of myocardial infarction (MI), episodes of unstable angina pectoris, ischaemic stroke, lethal outcome data, but these are not reported in results section |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (24 sites) Country: India Dates participants recruited: August 2014 ‐ March 2018 Maximum follow‐up: median follow‐up 21.6 months | |
| Participants | Inclusion criteria: participants aged 18 to 80 years with acute myocardial infarction within the past 14 days were eligible if they were willing and able to complete the hospital‐based CR programme. Acute MI confirmed by the WHO definition (presence of symptoms of ischaemia and changes in ECG) or the Third Universal definition of MI (elevation of a cardiac biomarker along with the presence of other symptoms of MI or changes in ECG). Exclusion criteria: participants who practised yoga regularly (i.e. > 3hr per week) or were participating in other clinical trials. Those with diseases that limited their life span to < 1 year or considered unlikely to complete the study by the local investigator. N randomised: total: 3959; intervention: 1970; comparator: 1989 Diagnosis (% of participants): MI: 100% Age (mean ± SD): intervention: 53.4 ± 11; comparator: 53.4 ± 10.8 Percentage male: intervention: 86.2%; comparator: 85.9% Ethnicity: NR | |
| Interventions | Intervention: Yoga‐care program. 13 direct contact sessions over 12 weeks. First two sessions delivered individually and the remainder in groups at the hospital. Group sessions lasted ~75 minutes and involved a combination of exercises related to general physical conditioning, stress and relaxation (health rejuvenating exercises ‐ around 10 min, yoga poses ‐ 25 min, breathing exercises ‐ 15 min, meditation and relaxation practices ‐ 15 min; and moderated discussion ‐ 10 min), and some exercises believed to be of particular cardio‐protective benefit in yogic texts. The lifestyle and other educational components were informed by yogic ideas but moderated by established scientific evidence. Sessions led by yoga teachers trained in delivery of yoga‐care program. Participants were also encouraged to practice daily at home following the instructions provided in a DVD and booklet. Components: exercise and education Setting: centre‐based Exercise programme modality: yoga Total duration: 12 weeks Co‐interventions: None described Comparator: Enhanced standard care in the form of educational advice leaflets (once before discharge, at 5 and 12 weeks) along with standard medical care as elsewhere in India but does not include rehabilitation. Co‐interventions: none described | |
| Outcomes | Mortality, MI, hospitalisations, HRQoL (only at 12 weeks), cost effectiveness | |
| Source of funding | Indian Council of Medical Research and the Medical Research Council, United Kingdom | |
| Conflicts of interest | Dr. Chathurvedi has served as a member of the Data Safety and Monitoring Committee for AstraZeneca. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Block randomization, stratified by centers, age (<60 or $60 years), and sex, was carried out by a central computer program” |
| Allocation concealment (selection bias) | Low risk | "...central computer program using an interactive Web response system" |
| Blinding of outcome assessment (detection bias) | Low risk | “Events were adjudicated by an independent committee unaware of trial‐group assignments, using standard definitions specified in the protocol.” Patient‐reported outcomes/quality of life not blinded. |
| Incomplete outcome data (attrition bias) | Low risk | Intervention 61/1979 (3%), Control 49/1989 (2%) participants lost to follow‐up are low in number and < 20%, similar across groups and for similar reasons. Protocol paper states that sensitivity analyses and multiple imputation would be performed, but these are not reported in the main publication. |
| Selective reporting (reporting bias) | Low risk | Protocol paper available. Prespecified economic analyses are not reported in the main report – authors confirmed this will be a separate publication. QoL data at later follow‐up time points also to be included in a later publication. |
| Study characteristics | ||
| Methods | Study design: multicentre RCT (2 sites) Country: Canada Dates participants recruited: December 2004 to December 2007 Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: Admitted for acute coronary syndromes who: underwent successful percutaneous coronary revascularisation; were not planning on enrolling in CR; had Internet access at home or work; and were 20 to 80 years of age. Exclusion criteria: CABG; implantable cardioverter‐defibrillator; NYHA Class III or IV heart failure; inability to speak and read English. N randomised: total: 223 ; intervention: 115; comparator: 108 Diagnosis (% of participants): AMI this admission: 29.1% Age (mean ±SD): intervention: 56.7 ± 9.0; comparator: 56.0 ± 9.0 Percentage male: intervention: 82.6%; comparator: 86.1% Ethnicity: NR | |
| Interventions | Intervention: Participants were visited in hospital by an exercise specialist, who presented a personally tailored physical activity plan and instructions on how to access the CardioFit website. Following discharge, participants were asked to log their daily activity on the CardioFit website and complete a series of five online tutorials (at weeks 2, 4, 8, 14, and 20). Following each tutorial, a new physical activity plan was developed. Between tutorials, participants received emails from the exercise specialist providing motivational feedback on their progress. Components: exercise plus psychological support Setting: home Exercise programme modality: NR Total duration: 20 weeks Co‐interventions: the CardioFit website and tutorials were designed to foster behavioural capability, self‐efficacy, social support, and realistic outcome expectations. Tutorials were organised to engage self‐control processes including exercise planning, goal setting, monitoring and self‐regulation, and relapse prevention. Comparator: physical activity guidance from their attending cardiologist and an education booklet. Co‐interventions: none described | |
| Outcomes | HRQoL | |
| Source of funding | Heart and Stroke Foundation of Ontario. Dr Reid was supported by a New Investigator Award from the Heart and Stroke Foundation of Canada. Dr Blanchard is supported by the Canada Research Chairs programme. | |
| Conflicts of interest | "The authors declare that there is no conflict of interests" | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Participants were randomized ... using a random sequence that was computer generated by a statistical consultant in blocks of 4, 8, and 10." |
| Allocation concealment (selection bias) | Low risk | "Sequences were generated for Ottawa and London and placed in sealed, numbered envelopes to ensure that treatment allocation was concealed until after baseline data collection. Research coordinators allocated the next available number on study entry (while the participant was still hospitalized)" |
| Blinding of outcome assessment (detection bias) | Low risk | "Research assistants, blinded to the participants’ treatment allocation, conducted follow‐up assessments" |
| Incomplete outcome data (attrition bias) | High risk | Loss to follow‐up was well reported but was high in both groups 36/115 [31%] and 33/108 [31%] were lost to follow‐up from the intervention and control groups. |
| Selective reporting (reporting bias) | Low risk | All outcomes described in the methods section are reported in results. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Chile Dates participants recruited: June 1973 to June 1981 Maximum follow‐up: 9 years | |
| Participants | Inclusion criteria: participants with transmural AMI Exclusion criteria: severe arrhythmias persisting after the acute phase of AMI (frequent ventricular premature beats, grade iii‐iv of the Lown classification, atrial flutter, partial or complete AV block); great left‐ventricular enlargement; left ventricular aneurysm; persistent cardiac failure; severe diastolic hypertension post‐myocardial infarction angina. N randomised: total: 193; intervention: 93; comparator: 100 Diagnosis (% of participants): Transmural AMI: 100% Anterior wall infarction: 55% Posteroinferior infarction: 45% Age (mean ± SD): intervention: 56.2 ± 10.3; comparator: 59.1 ± 8.8 Percentage male: intervention: 93.6%; comparator: 87% Ethnicity: NR | |
| Interventions | Intervention: Supervised physical training programme according to the guidelines reported by Zohman and Tobias. It was started with combined ergometric, callisthenic and walk‐jogging exercise lasting 30 min, three times a week. The intensity of the training was graded according to the target heart rate threshold, defined as 70% of maximal heart rate achieved by the participant in the former ergometric work test. Components: exercise only Setting: centre Exercise programme modality: combined ergometric and walk‐jogging exercise Total duration: average 42 months (range 6 to 108 months) Co‐interventions: none described Comparator: Control participants were medically treated according to the guidelines commonly used; namely, short‐ and long‐lasting nitrites, ß‐ blockers or Ca antagonists (nifedipine). Co‐interventions: A small number (8 participants) were also treated with oral anticoagulants. | |
| Outcomes | Mortality, MI and revascularisations | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “Patients were randomly allocated…” |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not described |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | Low risk | 18/93 (19.4%) and 18/100 (18%) withdrew or dropped out from intervention and control groups over the 9‐year period. |
| Selective reporting (reporting bias) | Low risk | Mortality, morbidity and complications were recorded over the duration of the study and are presented as rates. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Sweden Dates participants recruited: NR (recruited over a period of 2½ years) Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: participants > 65 years admitted following an acute coronary event. Participants had to perform a pre‐discharge exercise test with a workload of ≥ 70 watts in men and ≥ 50 watts in women. Exclusion criteria: participants with neurological sequelae, memory dysfunction such as dementia, orthopaedic disability, inability to speak or understand Swedish, or both, and a planned coronary intervention within 3 months. N randomised: total: 101; intervention: 50; comparator: 51 Diagnosis (% of participants): Angina pectoris: intervention: 20%; comparator: 21% Previous AMI: intervention: 18%; comparator: 11% Acute coronary event: intervention: 50%; comparator: 51% Previous PCI: intervention: 7%; comparator: 5% Previous CABG: intervention: 9%; comparator: 9% (Not mutually exclusive numbers.) Age (median): total: 71 years (range 64‐84); intervention: 71 years (range 64‐84); comparator: 71 years (range 65‐83) Percentage male: total 80.2%; intervention: 82%; comparator: 78.4% Ethnicity: NR | |
| Interventions | Intervention: 50 min aerobic group training programme three times a week for 3 months, with a voluntary 50 min step‐down period once a week for another 3 months. The complete programme was supported by music, which guided the intensity of the performance during the session. The training sessions were followed by 10 min of relaxation, also supported by music. Components: exercise only Setting: centre‐based supervised group sessions Exercise programme modality: aerobic exercises to music Total duration: 3 months Co‐interventions: none described Comparator: participants were recommended to take a daily walk at a comfortable speed, and to gradually increase the time, length and speed, and were encouraged to restart their prior physical activity as soon as they felt fit enough for this. Co‐interventions: none described | |
| Outcomes | HRQoL and revascularisation | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "….were randomly allocated into one of two groups:” |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment was not described. |
| Blinding of outcome assessment (detection bias) | Low risk | “patients were evaluated ….. by an independent, blinded to group allocation, researcher.” |
| Incomplete outcome data (attrition bias) | Low risk | There was no attrition ‐ data were reported for all participants randomised. |
| Selective reporting (reporting bias) | Low risk | All outcomes mentioned in methods were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Spain Dates participants recruited: June 2010 ‐ June 2012 Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: Age over 18 years, diagnosis of myocardial ischaemia (MI pre‐infarct angina, angina pectoris, other specific forms of chronic ischaemic heart disease or unspecified ischaemic heart disease) during the current admission, residence in the catchment area of the hospital, absence of cognitive deficit (Pfeiffer test: 0‐2 mistakes), sufficient functional capacity to follow the CRP (Barthel index > 60), and willingness to participate in the study and provide signed informed consent. Exclusion criteria: Symptoms of right heart failure producing pulmonary hypertension or dyspnoea caused by severe pulmonary pathology, additional comorbidities affecting the prognosis of cardiac disease, major comorbidities or limitations that could interfere with the exercise training programme. N randomised: total: 86; intervention: 42; comparator: 44 Diagnosis (% of participants): intervention: myocardial ischaemia (85.4%), pre‐infarct angina (4.9%), cardiac angina (9.8%); comparator: myocardial ischaemia (72.7%), pre‐infarct angina (13.6%), cardiac angina (11.4%), other specific forms of chronic ischaemic heart disease (2.3%). Age (mean ± SD): intervention: 59.4 ± 12; comparator: 59.7 ± 10.4 Percentage male: intervention: 93%; comparator: 77% Ethnicity: NR | |
| Interventions | Intervention: Supervised outpatient exercise training programme based on the results of the exercise stress test and mindful of comorbid conditions and physical limitations. Intervention started within 3 days of exercise test which was performed within 1 month of discharge. Hospital‐based programme of physiotherapist‐supervised exercise (3 hours/week spread over 3 days), for 10 weeks. Classes consisted of 10 minutes of warm‐up and muscle stretching, 30 minutes of aerobic exercises on a cycle ergometer, 15 minutes of isotonic exercises for the upper and lower limbs and 5 minutes of cool‐down. Aerobic exercise intensity was between 75% and 90% of the maximum heart rate obtained in the previous exercise stress test and progressed according to the perceived exertion rate score of 11–15. Resistance training was performed with 10–15 repetitions for three sets, maintaining a perceived exertion rate score of 11–14. Components: exercise only Setting: centre‐based Exercise programme modality: cycle ergometry Total duration: 10 weeks Co‐interventions: None described Comparator: Standard care, given oral and written information about cardiovascular risk factors during hospitalisation. Participants instructed to do exercises to regain mobility and maintain muscle tone and peripheral circulation and taught breathing exercises. Participants provided guidance on how to return to physical activity. Scheduled for follow‐up visits at 3, 6 and 12 months post discharge to control risk factors, reinforce education measures and review adherence to cardiac medication. Co‐interventions: none described | |
| Outcomes | Mortality, hospitalisations, HRQoL | |
| Source of funding | Supported by a grant from the Collegi de Fisioterapeutes de Catalunya (no.: R01/08‐09) | |
| Conflicts of interest | None declared | |
| Notes | Authors contacted to obtain appendices as they were not available online | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "A randomisation list in blocks of 10 was created by a computer random number generator." |
| Allocation concealment (selection bias) | Unclear risk | "The randomisation list and allocation of patients to each group were independently controlled by the Clinical Research Unit" |
| Blinding of outcome assessment (detection bias) | Low risk | "The endpoint committee who assessed the primary outcomes was blinded regarding group assignment." |
| Incomplete outcome data (attrition bias) | Low risk | < 20% missing outcome data and reasons provided |
| Selective reporting (reporting bias) | Low risk | Published protocol paper available; all outcomes reported |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT. Participants randomised after routine angiography for angina. Country: Germany Dates participants recruited: NR Maximum follow‐up: 6 years | |
| Participants | Inclusion criteria: Male, stable symptoms, willingness to participate in the study for at least 12 months, coronary artery stenoses well documented by angiography, and permanent residence within 25 km of the training facilities at Heidelberg. Exclusion criteria: Unstable angina pectoris, left main coronary artery stenosis > 25% luminal diameter reduction, severely depressed left ventricular function (ejection fraction < 35%), significant valvular heart disease, insulin‐dependent diabetes mellitus, primary hypercholesterolaemia (type II hyperlipoproteinaemia, low density lipoprotein [LDL] > 210 mg/dL), and occupational, orthopedic, and other conditions precluding regular participation in exercise sessions. N randomised: total: 113; intervention: 56; comparator: 57 Diagnosis (% of participants): AMI: 66% Age (mean ± SD): intervention: 52.8 ± 5.8; comparator: 54.2 ± 7.7 Percentage male: 100% Ethnicity: NR | |
| Interventions | Intervention: participants stayed on a metabolic ward during the initial 3 weeks, during which they were instructed how to lower the fat content of their regular diet. Participants were asked to exercise daily at home on a cycle ergometer for a minimum of 30 minutes close to their target heart rates, which were determined as 75% of the maximal heart rate during symptom‐limited exercise. In addition, they were expected to participate in at least two group training sessions of 60 minutes each week. Components: exercise and education. Setting: centre (group session) and unsupervised at home. Exercise programme modality: cycle ergometer. Total duration: 12 months. Co‐interventions: participants were on their regular antianginal medication, including β‐blocking agents. Comparator: participants spent 1 week on the metabolic ward, where they received identical instructions about the necessity of regular physical exercise and how to lower fat consumption. "Usual care" was rendered by their private physicians. Co‐interventions: They were asked not to take lipid‐lowering medications. | |
| Outcomes | Total and CHD mortality, non‐fatal MI, revascularisation. | |
| Source of funding | Bundesministerium für Forschung und Technologie, Bonn, FRG. | |
| Conflicts of interest | NR | |
| Notes | Exercise adherence in the first year was 68% (39% to 92%), over the next 5 years 33% (3% to 89%). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported. |
| Allocation concealment (selection bias) | Low risk | "sealed envelopes" |
| Blinding of outcome assessment (detection bias) | Low risk | "Evaluation of coronary angiograms was performed by two technicians blinded to the sequence of films and the patient's identity or group assignment." |
| Incomplete outcome data (attrition bias) | High risk | 20% lost to follow‐up; no description of withdrawals or dropouts. |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Japan Dates participants recruited: NR Maximum follow‐up: 6 months | |
| Participants | Inclusion criteria: Male participants; > 65 years of age; with chronic CAD; referred at least 6 months after a major coronary event, including acute MI, coronary artery bypass grafting or percutaneous balloon angioplasty for acute coronary syndrome. Exclusion criteria: none described. N randomised: total: 38; intervention: 20; comparator: 18 Diagnosis (% of participants): Chronic CAD: 100% MI: 55% Age (mean ± SD): intervention: 69.3±2.9 ; comparator: 70.1±3.7 Percentage male: 100% Ethnicity: NR | |
| Interventions | Intervention: participants participated in an outpatient phase III CR program for 6 months. The weekly supervised exercise session at the clinic consisted of approximately 20 min of warm‐up exercises including stretching and callisthenics, followed by 20–30 min of continuous upright aerobic and dynamic exercise (various combinations of walking, bicycling, jogging, and other activities) and light isometric exercise, such as hand weights, and approximately 20 min of cool‐down stretching and callisthenics. The intensity of exercise was prescribed individually at the anaerobic threshold level measured by a symptom‐limited treadmill exercise test at baseline. In addition to the supervised exercise session, participants were encouraged to exercise twice a week outside of the clinic. Each participant’s exercise prescription was also periodically adjusted on the basis of repeated treadmill exercise test to encourage a gradual increase in overall exercise performance. Components: exercise and education. Setting: supervised in a centre and independent at home. Exercise programme modality: e.g. walking, bicycling, jogging. Total duration: 6 months. Co‐interventions: participants were encouraged and interviewed at the supervised exercise session by physicians, dietitians, nurses, and exercise physiologists to comply with both the exercise and dietary education of the programme throughout its duration. Comparator: participants were followed by an individual physician as a usual outpatient. Co‐interventions: none described. | |
| Outcomes | Health‐related quality of life at 6 months. | |
| Source of funding | Health Sciences Research Grants from Ministry of Health and Welfare (Comprehensive Research on Aging and Health). | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly assigned..by envelope method" |
| Allocation concealment (selection bias) | Unclear risk | "randomly assigned..by envelope method" |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described. |
| Incomplete outcome data (attrition bias) | Low risk | All 38 participants accounted for. |
| Selective reporting (reporting bias) | Low risk | All outcomes are reported for all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Japan Dates participants recruited: NR Maximum follow‐up: 6 months | |
| Participants | Inclusion criteria: > 65 years old with stable CAD Exclusion criteria: Ongoing congestive heart failure, liver dysfunction, renal dysfunction, or systemic diseases, including malignancy and collagen disease. N randomised: total: 39; intervention: 20; comparator: 19 Diagnosis (% of participants): stable CAD: 100% MI: 46% Age (mean ± SD): intervention: 69±3 ; comparator:70±4 Percentage male: 100% Ethnicity: NR | |
| Interventions | Intervention: Weekly outpatient phase III cardiac rehabilitation programme that included an exercise session, exercise prescription, dietary instruction and an educational programme for 6 months. Supervised exercise sessions at the clinic consisted of approximately 15 min of warm‐up exercises including stretching, followed by 20 to 60 min of continuous upright aerobic exercise and light isotonic exercise such as sit‐ups and squatting using the participant's own body weight, followed by approximately 15 min of cool‐down stretching and callisthenics. The intensity of exercise was prescribed individually at the anaerobic threshold (AT) level as measured by a treadmill exercise test using expiratory gas analysis or a rating of 12 to 13 on the standard Borg perceived exertion scale. In addition to the weekly supervised exercise sessions, participants were encouraged to perform aerobic exercise twice weekly (≥ 30 min) at home at an intensity of heart rate of AT or a rating of 12 to 13 on the Borg scale. Components: exercise and education. Setting: centre and home. Exercise programme modality: e.g. walking, bicycling, jogging. Total duration: 6 months. Co‐interventions: participants were instructed about the phase II diet of the American Heart Association at the beginning and every 2 months of the study. An educational programme was also given to each subject by physicians and nurses regarding ischaemic heart disease and risk factors at baseline. Subjects were frequently encouraged by physicians, dietician, nurses, and exercise physiologists to comply with both exercise and dietary instructions throughout the programme. Standard medical care was provided for both groups. Lipid‐lowering drugs and other medications that may affect lipid levels were given at stable doses for at least 4 weeks before entry, and the doses of these medications were not altered during the study period. Comparator: usual outpatient care. Co‐interventions: none described. | |
| Outcomes | Total mortality; non‐fatal/fatal mortality. | |
| Source of funding | Health Sciences Research Grants from Ministry of Health, Labour and Welfare (Comprehensive Research on | |
| Conflicts of interest | NR | |
| Notes | "No subject in either group showed any worsening of symptoms or had clinical events during this study." | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly assigned" |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described. |
| Incomplete outcome data (attrition bias) | Unclear risk | No information reported. |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported for all time points. |
| Study characteristics | ||
| Methods | Study design: Multicentre RCT (5 sites) Country: USA Dates participants recruited: 1976 Maximum follow‐up: 5 years Participants were randomised after completion of a 6‐week, low‐level exercise programme run‐in period. | |
| Participants | Inclusion criteria: documented MI ≥ 8 weeks but ≤ 3 years before being enrolled. Other eligibility criteria included the ability to exercise at an intensity level ≥ 3 metabolic equivalents (METs) and a supine resting diastolic blood pressure < 100 mmHg. Exclusion criteria: participants were considered ineligible if they had any other significant coexisting CVD or other disease likely to be fatal in the near future, uncontrolled diabetes mellitus, complete heart block with or without ventricular pacemaker, or emotional or physical impairments that would make participation and adherence difficult, or if they were already participants in a formal exercise programme. N randomised: total:651; intervention: 323; comparator: 328 Diagnosis (% of participants): MI: 100% Age (mean ± SD): intervention: 51.5 ± 7.4; comparator: 52.1 ± 7.2 Percentage male: 100% Ethnicity % white: intervention: 93.3%; comparator: 94.4% | |
| Interventions | Intervention: An exercise prescription was developed on the basis of each participant’s multistage graded exercise test (MSET) results. An exercise target heart rate guided the prescription and was determined as 85% of the peak heart rate achieved on the test. This group performed brisk physical activity in the laboratory for 8 weeks, exercising 1 hour per day, 3 days per week. The participants were supervised and underwent continuous ECG monitoring. Each individual exercised for 4 minutes on each of 6 stationary machines with a 2‐minute rest interval between machines. Attainment of the target heart rate was the goal for every 4‐minute exercise period. After 8 weeks, participants exercised in a gymnasium or swimming pool without ECG monitoring, although exercise heart rates were periodically checked. Activities consisted of 15 minutes of continuous jogging, cycling, or swimming, followed by 25 minutes of recreational games. The activities were performed at an intensity level enabling each participant to reach his individually prescribed target heart rate. The men were encouraged to attend 3 sessions per week but in some situations were allowed to exercise on their own. Components: exercise only. Setting: group sessions in centre (“but in some situations were allowed to exercise on their own”). Exercise programme modality: “brisk physical activity” on “stationary machines”. Total duration: 8 weeks in the laboratory, followed by regular jogging, cycling, or swimming and recreational games. Co‐interventions: none described. Comparator: Participants in the non‐exercising control group were encouraged to maintain normal routines but not to participate in any regular exercise programme. Co‐interventions: none described. | |
| Outcomes | Total & CHD mortality, non‐fatal MI. | |
| Source of funding | National Heart, Lung, and Blood Institute. | |
| Conflicts of interest | NR | |
| Notes | 90% of ET attended 90% of 24 scheduled sessions post‐randomisation, only 48% attending > 50% of sessions at 18 months. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Sequence generation not described…."the men were randomly assigned.” |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not described. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described. |
| Incomplete outcome data (attrition bias) | High risk | 6.5% lost to follow‐up; no description of withdrawals or dropouts. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported for all time points. |
| Study characteristics | ||
| Methods | Study design: Multicentre RCT (7 sites) Country: USA Dates participants recruited: 1 September 1977 to 2 December 1979 Maximum follow‐up: 6 months Random allocation of individuals to two intervention groups (exercise only (Intervention B1) or exercise plus teaching and counselling (Intervention B2)) and a control group (usual care). | |
| Participants | Inclusion criteria: Previous MI, age < 70 years, living < 50 miles of centre. Exclusion criteria: prolonged complications, physical limitations, noncardiac or cardiac diseases, communication problems, other issues e.g. massive obesity, psychological problems, etc. N randomised: total: 258; Intervention B1: 88; Intervention B2: 86; comparator: 84 Diagnosis (% of participants): AMI: 100% Age (mean ±SD): Intervention B1: 55.6 ± 9.3; Intervention B2: 56.3 ± 8.3; comparator = 57.1 +/‐ 7.3 Percentage male: > 80% Ethnicity: > 80% white | |
| Interventions | Intervention: The outpatient exercise programme was identical for the participants in groups Bl and B2. It consisted of a gradually progressive callisthenic and walking programme prescribed at weekly 30‐minute clinic visits and performed by the participant at home. Participants were instructed to exercise twice a day until they returned to work and once a day thereafter. If the participant was symptom free, the prescription was gradually increased to add callisthenics of increasing intensity and the distance and time (or rate) of walking were gradually advanced. Components: exercise only or exercise plus education and counselling. Setting: centre and home. Exercise programme modality: walking. Total duration: NR Co‐interventions: participants in group B2, in addition to receiving exercise prescriptions as described above, attended a series of eight 1‐hour group sessions during weekly clinic visits. The sessions emphasised the practical aspects of anatomy and physiology of the heart, coronary artery disease, myocardial infarction and medications; risk factors, including smoking, hypercholesterolaemia, hypertension, stress and sedentary living; nutritional Comparator: conventional medical and nursing management throughout all phases of hospitalisation and convalescence at home. Co‐interventions: none described. | |
| Outcomes | Total mortality; health‐related quality of life: Sickness Impact Profile. | |
| Source of funding | Bureau of Health Professions, Division of Nursing, Department of Health and Human Services. | |
| Conflicts of interest | NR | |
| Notes | Several reports of the same trial all with various bits of information. Study authors conclude that multiple intervention trial of this short duration did not change participants' behaviour. MI itself acts as a strong stimulus to alter behaviour with respect to risk factors. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described. |
| Incomplete outcome data (attrition bias) | High risk | 24% lost to follow‐up; no description of withdrawals or dropouts. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points. |
| Study characteristics | ||
| Methods | Study design: Multicentre RCT (6 sites across 5 countries) Country: Europe (the Netherlands, Denmark, Spain, Switzerland, France) Dates participants recruited: November 2015 ‐ January 2018 Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: Participants of 65 years or older who are a candidate for CR and non‐voluntary to participate in the regular CR programme Signed written informed consent One of the following criteria:
Exclusion criteria:
N randomised: total: 179; intervention: 89; comparator: 90. Diagnosis (% of participants): PCI: intervention 63 (71%); control 65 (72%) CABG: intervention 11 (12%); control 8 (9%) Valve replacement: intervention 1 (1%); control 3 (3%) None: intervention 14 (16%); control 14 (16%) Age (mean ±SD): intervention: 72.4 ± 5.4; comparator 73.6 ± 5.5 Percentage male: intervention: 78%, comparator: 84% Ethnicity: intervention: 99%, comparator: 99% white | |
| Interventions | Intervention: 6‐month home‐based CR program equipped with a smartphone and heart rate belt. Participants instructed to exercise at moderate intensity for at least 30 minutes per day, 5 days per week. Motivational interviewing was applied by telephone weekly in the first month, every other week in the second month, and monthly until completion of the program at 6 months Setting: Home‐based Exercise programme modality: Self‐chosen type of activity Total duration: 6 months. Co‐interventions: none described Comparator: participants in the control group did not receive any form of cardiac rehabilitation but received locally defined standard of care. Co‐interventions: none described. | |
| Outcomes | Mortality, MI, PCI, cardiovascular hospitalisation, HRQoL | |
| Source of funding | Study was supported by grant 634439 from the European Union’s Horizon 2020 Research and Innovation Programme and contract 15.0139 from the Swiss State Secretariat for Education, Research and Innovation | |
| Conflicts of interest | Mr Snoek reported receiving grants from European Union’s Horizon 2020 Research and Innovation Programme during the conduct of the study. Dr van der Velde reported receiving grants from the European Union during the conduct of the study. Dr Eijsvogels reported receiving a personal grant from the Dutch Heart Foundation. Dr Prins reported receiving grants from the European Commission during the conduct of the study and outside the submitted work. Dr Bruins reported receiving grants from Isala Heart Centre during the conduct of the study. Dr Meindersma reported receiving grants from the European Commission during the conduct of the study. Dr Peña‐Gil reported receiving grants from European Commission during the conduct of the study. Dr González‐Salvado reported receiving grants from the European Union during the conduct of the study. Dr Iliou reported receiving personal fees and non‐financial support from Servier Laboratories, non‐financial support from Novartis International AG and Sanofi SA, and personal fees from AstraZeneca outside the submitted work. Dr Marcin reported receiving grants from the Swiss National Fond during the conduct of the study. Dr Van’t Hof reported receiving grants from the European Union during the conduct of the study and grants from Medtronic plc, AstraZeneca, and Abbott Laboratories outside the submitted work. Dr de Kluiver reported receiving grants from the European Union during the conduct of the study and having an indirect interest in HC@home/Mobihealth, which provided the hardware and software for this study, outside the submitted work. No other disclosures were reported. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Randomization was performed in fixed blocks of 4, stratified by center, with a 1:1 ratio to the intervention group (MCR) or a control group without cardiac rehabilitation using a centralized computerized allocation system.” |
| Allocation concealment (selection bias) | Low risk | “Randomization was performed in fixed blocks of 4, stratified by center, with a 1:1 ratio to the intervention group (MCR) or a control group without cardiac rehabilitation using a centralized computerized allocation system.” |
| Blinding of outcome assessment (detection bias) | Low risk | “Researchers assessing primary outcomes were blinded for group assignment.” |
| Incomplete outcome data (attrition bias) | Low risk | Intervention group: 16/89 (18%) lost to follow‐up Control group: 12/90 (13%) lost to follow‐up |
| Selective reporting (reporting bias) | Low risk | Trial protocol provided as supplementary file in main publication; outcomes reported in protocol are reported at 6 and 12 months in the results. Costs mentioned in the protocol but likely to be in a future publication. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Italy Dates participants recruited: NR (40‐month period) Maximum follow‐up: mean 34.5 months | |
| Participants | Inclusion criteria: participants < 65 years of age who had not had previous MI, admitted due to chest pain lasting > 30 minutes and because they had a diagnosis of AMI based on evolutionary ECG changes and serum kinase elevation. Exclusion criteria: complicated in‐hospital clinical course e.g. post‐infarction angina requiring urgent revascularisation; evidence of congestive HF; chronic concomitant illnesses or musculoskeletal handicaps that would prevent them from finishing the exercise training period. N randomised: total: 256; intervention: 125; comparator: 131 Diagnosis (% of participants): MI: 100% Prior angina: 42% Age (Mean ± SD): intervention: 51.5 ± 7; comparator: 54.3 ± 8 Percentage male: 91% intervention: 91%; comparator: 91% Ethnicity: NR | |
| Interventions | Intervention: participants underwent a 4‐week physical training period consisting of supervised training sessions of 30 minutes of bicycle ergometry five times a week combined with callisthenics. Training intensity was graded according to 75% of maximal work capacity reached in the previous exercise test. At the end of the 4‐week training period, a second symptom‐limited exercise test was performed. Participants were then discharged with the instructions to continue the callisthenics daily and to walk for ≥ 30 minutes every 2 days. Components: exercise, education and psychology. Setting: centre and then home. Exercise programme modality: bicycle ergometry in centre followed by callisthenics and walking at home. Total duration: 4 weeks supervised and then continued at home. Co‐interventions: All participants went to the Rehabilitation Center for 3 weeks and underwent a symptom‐limited exercise test (28 ± 2 days after myocardial infarction), 24‐hour Holter monitoring, and coronary arteriography (31 ± 3 days after the acute episode). All participants attended colloquial sessions, held by a cardiologist and a psychologist, dealing with secondary prevention of cardiovascular diseases and stressing dietary changes and smoking cessation. Comparator: Discharged after rehab centre and clinically re‐examined 1 month later when they underwent a second symptom‐limited exercise test. Co‐interventions: as above | |
| Outcomes | CHD mortality, revascularisations | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | Ejection fraction (EF) was the only prognostic factor. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomized" |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described. |
| Incomplete outcome data (attrition bias) | Low risk | No losses to follow‐up. |
| Selective reporting (reporting bias) | High risk | While survival data is provided, detailed clinical information was obtained from all participants at 3‐ to 4‐month intervals and these data are not reported. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Sweden Dates participants recruited: October 1994 to June 1997 Maximum follow‐up: 1 year | |
| Participants | Inclusion criteria: participants ≥ 65 years admitted because of an acute coronary event. To be included, the participants had to perform a pre‐discharge exercise test at a workload ≥ 70 W in men and ≥ 50 W in women. For the group with unstable angina pectoris, a ST60 depression of > 1 mm in ≥ two adjacent leads had to be documented at the exercise test. Exclusion criteria: neurological sequelae, memory dysfunction, orthopaedic disability, inability to understand Swedish, coronary intervention planned within 3 months or other complicating diseases. N randomised: total: 109; intervention: 56; comparator: 53 Diagnosis (% of participants): Congestive heart failure: 6% Previous AMI: 27% Age years, (range): intervention: 71 (64‐84); comparator: 68 (65‐83) Percentage male: intervention: 73%; comparator: 75% Ethnicity: NR | |
| Interventions | Intervention: 50 min aerobic outpatient group‐training programme (including warm‐up and cool‐down) 3 times a week for 3 months. Complete programme was supervised by specialised physiotherapist and supported by music which guided intensity of performance during session. Training followed by 10 min of music‐supported relaxation. After 3 months, participants had possibility of participating in programme once a week for another 3 months. Components: exercise. Setting: supervised centre‐based group sessions. Exercise programme modality: NR Total duration: 3 months followed by opportunity to continue once a week for another 3 months. Co‐interventions: none described Comparator: usual care ‐ encouraged to re‐start usual/prior physical activity as soon as they felt fit. Co‐interventions: none described | |
| Outcomes | Total mortality, CABG, PCI, health‐related quality of life; Karolinska Questionnaire at 12‐months. | |
| Source of funding | National Association for Heart and Lung Patients, the Swedish Heart and Lung Foundation, the Swedish Foundation of Health Care Sciences and Allergy Research, and the King Gustaf V and Queen Victoria Foundation. | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described. |
| Incomplete outcome data (attrition bias) | High risk | Clinical event data for 8 (7%) who withdrew before 3 months were not accounted for at 1 yr. |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: USA Dates participants recruited: NR Maximum follow‐up: 1 year. Randomised by blocks of 6 into one of three groups: exercise, group counselling & control. | |
| Participants | Inclusion criteria: Aged 30 to 69 years with documented MI not less than six weeks nor more than one year prior to admission to the study. Work capacity level < 7 MET (men) or < 6 MET (women) or a Taylor Manifest Anxiety Scale raw score of 19 + or Zung Self‐rating Depression Scale raw score of 40 +, or any or all of these. Exclusion criteria: Presence of unstable cardiovascular condition i.e. congestive heart failure, or requirement of treatment for any physical/psychological reason. N randomised: total: 106; intervention: 42; comparator (usual care): 29; group counselling: 35 (no data analysed in this review) Diagnosis (% of participants): MI: 100% Age (mean): 54 Percentage male: intervention: 90%; comparator: 76% Ethnicity: 85% white | |
| Interventions | Intervention: Three one‐hour sessions per week over a 12‐week period. All exercises were dynamic, involving rhythmic movements against resistance. Half were upper limb (rowing machine, arm wheel, and arm ergometer) and half were lower limb (treadmill, cycle, and step ergometer). Participants exercised upper and lower limbs alternately for four minutes with two minutes of rest in between. The intensity of exercise was determined by heart‐rate response, the target level being 85% of the peak exercise heart rate achieved in the first evaluation. If the heart rate was consistently above or below target, the work load was increased or decreased. Components: exercise. Setting: supervised in a centre. Exercise programme modality: e.g. rowing, treadmill, cycle or step ergometer. Total duration: 12 weeks. Co‐interventions: none described. Comparator: followed up by their physicians and given routine post‐MI medical care. Participants were requested to not join a supervised exercise or a formal counselling programme. Co‐interventions: none described. | |
| Outcomes | Mortality, non‐fatal MI. | |
| Source of funding | National Institute of Handicapped Research, Department of Education, Washington, DC. | |
| Conflicts of interest | Not reported | |
| Notes | Minimal differences between groups at one year. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described. |
| Incomplete outcome data (attrition bias) | High risk | 7.7% lost to follow‐up; no description of withdrawals or dropouts. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported for all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: China Dates participants recruited: NR Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: 1) 60 to 75 years old 2) Stable coronary heart disease patients 3) Participants with low or medium risk of coronary heart disease (according to the risk stratification standard) Exclusion criteria: 1) Uncontrolled hypertension; that is, resting systolic blood pressure > 160mm Hg or resting diastolic blood pressure > 100mm Hg 2) Moderate to severe heart valve stenosis 3) Severe left aortic stenosis (stenosis degree ≥ 70%) 4) Osteoarthrosis or vascular disease of the lower extremity 5) Malignant neoplasm N randomised: total: 70; intervention: 35; comparator: 35 Diagnosis (% of participants): intervention: stable angina pectoris (57.1%), asymptomatic post MI (20%), old MI (28.6%), post PCI (25.7%); comparator: stable angina pectoris (51.4%), asymptomatic post MI (5.7%), old MI (22.9%), post PCI (42.9%), post CABG 5.7%. Age (mean, range): intervention: 65, range 61‐72; comparator: 65, range 60‐70. Percentage male: intervention: 54%; comparator: 69% Ethnicity: NR | |
| Interventions | Intervention: 1) Exercise mode: Walk or jog on the exercise board (T2100 exercise board equipped with 12 leads ECG and blood pressure monitoring) 2) Exercise intensity: The heart rate reserve method was used combining self‐perceived fatigue of the participant to reach 50% to 80% of the maximum exercise intensity or Borg rate of perceived exertion at 12 to 16 3) Exercise time: 30 ‐ 60 mins, including 5 ‐ 10 mins warm‐up and relaxation exercises 4) After discharge, participants can choose one or more kinds of aerobic exercise rehabilitation from walking, jogging, walking on the treadmill, cycling, swimming, and playing badminton etc. for 3 to 5 times a week. Components: exercise plus education. Setting: centre‐based (3 months), home‐based (9 months) Exercise programme modality: walking, jogging, walking on the treadmill, cycling, swimming, and playing badminton etc. Total duration: 12 months. Co‐interventions: None described Comparator: “conventional treatment” including “health education and standard medication” Co‐interventions: none described. | |
| Outcomes | No relevant outcomes reported | |
| Source of funding | Military Medicine and Geriatrics of the Headquarters of the General Staff (ZCWS14C25) | |
| Conflicts of interest | Not reported | |
| Notes | Study reports outcomes of BMI, BP, lipids, smoking, and no CONSORT flow diagram reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "random number table used" |
| Allocation concealment (selection bias) | Unclear risk | No details reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | No details of blinding reported |
| Incomplete outcome data (attrition bias) | Low risk | Reasons for lost to follow‐up provided, and equal across groups |
| Selective reporting (reporting bias) | Unclear risk | Protocol paper not available |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: USA Dates participants recruited: NR Maximum follow‐up: 24 months | |
| Participants | Inclusion criteria: Postmenopausal women with coronary heart disease, defined as atherosclerosis, MI, percutaneous transluminal coronary angioplasty, and/or coronary bypass graft surgery. Exclusion criteria: Other life‐threatening illnesses, infarction during the preceding 6 weeks, receiving streptokinase or alteplase, or being scheduled for bypass surgery. N randomised: total: 25; intervention: 14; comparator: 11 Diagnosis (% of participants): CHD: 100% Previous AMI: 52% Age (mean ±SD): intervention: 64 ± 10; comparator: 63 ± 11 Percentage male: 0% Ethnicity: 92% white | |
| Interventions | Intervention: Daily group physical activity sessions included warm‐up, walking or aerobics, and a cool‐down. Participants were individually prescribed exercise intensity based on their treadmill exercise test performance. Following the retreat, the intervention exercise programme required participants to engage in a 1‐hour session per day at least 3 days each week. Components: exercise, education and psychological support. Setting: supervised sessions in a centre followed by home. Exercise programme modality: walking or aerobics. Total duration: 24 months. Co‐interventions:. Participants randomised to the PrimeTime programme began the intervention with a 7‐day retreat. Women were encouraged to bring their partner. As well as physical activity, the daily schedule included cooking classes, instruction in stress‐management techniques including Hatha Yoga stretches, progressive deep relaxation, deep breathing, meditation, group support, smoking cessation and directed or receptive imagery.Twice‐weekly 4‐hour meetings followed the retreat with each meeting following a sequence similar to the retreat schedule. Comparator: usual care. Co‐interventions: none described. | |
| Outcomes | Health‐related quality of life: SF‐36 at 24 months | |
| Source of funding | National Heart, Lung, and Blood Institute | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomized" |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described |
| Incomplete outcome data (attrition bias) | High risk | 3/28 (10.7%) participants lost to follow‐up; no description of withdrawals or dropouts. |
| Selective reporting (reporting bias) | High risk | While most outcomes are reported at all time points, the SF‐36 is poorly reported and it is not stated for which follow‐up the results are reported |
| Study characteristics | ||
| Methods | Study design: Quasi‐RCT (single centre) Country: Bangladesh Dates participants recruited: July 2012 ‐ July 2013 Maximum follow‐up: 12 months | |
| Participants | Inclusion criteria: participants admitted for elective CABG surgery, aged between 25‐65 years and understood Bangla. Exclusion criteria: Admission for emergency CABG surgery or revision CABG surgery, any neurological problems or severe comorbidities, or they were not planning to stay in Bangladesh for ≥ 1 year after CABG surgery. N randomised: total: 142; intervention: 71; comparator: 71 Diagnosis (% of participants): post‐CABG (100%). Age (mean ± SD): intervention: 54 ± 6; comparator: 55 ± 6 Percentage male: intervention: 66 (93%); comparator: 63 (89%) Ethnicity: NR | |
| Interventions | Intervention: participants participated in a 45‐min CR class (groups of 6‐10, 7‐8 days after surgery) in the hospital and were provided with an educational booklet in Bangla. In the class, participants were encouraged to comply with and have knowledge about medical advice, given information about the home exercise program, stress management, smoking cessation, alcohol intake and diet, encouraged to resume everyday activities and social interaction. The booklet described a home exercise training program including upper‐ and lower‐limb exercises, breathing exercises, chest movements and aerobic exercise (walking program). Educational information provided about safe levels of activity, details of personal risk factors, useful telephone numbers, when to seek medical advice, and how to manage recurrent breathlessness or chest pain. Participants received a monthly telephone call for 12 months from a qualified physiotherapist trained by the research team regarding the CR advice booklet and exercise program. The physiotherapist answered any participant questions and reminded them to follow the CR program, and attend their next hospital appointment. Components: exercise plus education. Setting: home‐based (with one initial centre‐based session) Exercise programme modality: Upper and lower limb exercises, breathing and chest exercises, walking. Total duration: 12 months. Co‐interventions: None described Comparator: Usual care – conventional hospital discharge care including drug treatment, post‐surgical information (precautions i.e. do not lift, pull or push heavy objects or weight > 5kg, lie in a supine position in bed), dietary advice from a dietician and routine follow‐up hospital visits. Co‐interventions: none described. | |
| Outcomes | HRQoL | |
| Source of funding | Not reported | |
| Conflicts of interest | None declared | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | “A quasi‐random method was used to allocate patients to either a home‐based CR program in addition to UC or UC alone. Allocation was done according to the week of surgery for patients, with every other week allocating patients to either the CR group or the UC group. Allocation was done by the research team and was not influenced by the preferences of the research team, patients, or relatives.” |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | No information provided about blinding of outcome assessment |
| Incomplete outcome data (attrition bias) | High risk | Intervention 10/71 (14%) Control 31/71 (44%). Missing participant numbers high and uneven across groups, and reasons for loss to follow‐up not provided. Imputation not performed. Demographic characteristics of participants lost to follow‐up were similar to participants with complete data at 12 months. |
| Selective reporting (reporting bias) | Unclear risk | Neither a study protocol nor trial registration available. |
| Study characteristics | ||
| Methods | Study design: RCT Country: Italy Dates participants recruited: NR Maximum follow‐up: 1 year Randomised after exercise tolerance test, 30 days after MI. | |
| Participants | Inclusion criteria: participants aged 40 to 60 years with MI Exclusion criteria: more than one previous MI N randomised: total: 50; intervention: 25; comparator: 25 Diagnosis (% of participants): MI: 100% Age (mean ± SD): intervention: 50.1 ± 5.5; comparator: 50.1 ± 6.3 Percentage male: intervention: 100%; comparator: 100% Ethnicity: 100% Italians | |
| Interventions | Intervention: 6 weeks physical activity programme Components: exercise Setting: NR Exercise programme modality: NR Total duration: 6 weeks Co‐interventions: NR Comparator: after discharge a simple plan of daily exercises (intensity ≤ 3 METs ) to perform at home Co‐interventions: NR | |
| Outcomes | CV mortality | |
| Source of funding | ||
| Conflicts of interest | ||
| Notes | Trained participants showed a better mid‐term prognosis than controls, but this could not be explained by the physical training procedure. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described. |
| Incomplete outcome data (attrition bias) | High risk | 24% lost to follow‐up; no description of withdrawals or dropouts. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Netherlands Dates participants recruited: NR Maximum follow‐up: 5 years Randomised 4 to 6 weeks post‐MI after exercise tolerance test. | |
| Participants | Inclusion criteria: Men (aged 40 to 55 years) who were hospitalised within 6 hours after onset of complaints of first myocardial infarction. Exclusion criteria: Combination of bundle branch block and anterior myocardial infarction N randomised: total: 98; intervention: 47; comparator: 51 Diagnosis (% of participants): MI: 100% Age (mean ± SD): intervention: 49.4 ± 3.7; comparator: 49.1 ± 4.5 Percentage male: intervention: 100%; comparator: 100% Ethnicity: NR | |
| Interventions | Intervention: The rehabilitation consisted of multidisciplinary intervention (physical, social, psychological). Components: exercise, psychological support. Setting: Centre Exercise programme modality: NR Total duration: 6 ‐ 8 weeks. Co‐interventions: none described. Comparator: usual care. Co‐interventions: none described. | |
| Outcomes | Mortality, non‐fatal MI. | |
| Source of funding | Prevention Fund, the Hague. | |
| Conflicts of interest | NR | |
| Notes | Study authors conclude that cardiac rehab benefits participants after MI due to direct effect on myocardial perfusion and to lowering of cholesterol levels. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomized" |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described. |
| Incomplete outcome data (attrition bias) | Low risk | No losses to follow‐up. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points (although absolute values not always given). |
| Study characteristics | ||
| Methods | Study design: Multicentre RCT (3 sites) Country: Norway Dates participants recruited: NR Maximum follow‐up: 2 years | |
| Participants | Inclusion criteria: participants admitted to hospital for acute MI, unstable angina pectoris or after coronary artery bypass grafting. Exclusion criteria: none described. N randomised: total: 197; intervention: 98; comparator: 99 Diagnosis (% of participants): AMI: 37% UAP stabilised: 2% PCI: 20% CABG: 25% Age (mean ± SD): intervention: 54 ± 8; comparator: 55 ± 8 Percentage male: intervention: 91%; comparator: 84% Ethnicity: NR | |
| Interventions | Intervention: The first phase lasted for 6 weeks with supervised physical exercise in addition to a regular group meeting twice a week. Each training session started with 15 min of warm up followed by 20 min of dynamic endurance training, 10 min of active cool‐down activities and finally 10 min of stretching and relaxation. Large muscle groups in the arms and legs were used simultaneously to achieve higher exercise intensity (11‐13 on the Borg scale). No weight lifting took place. This was followed by 9 weeks of supervised physical exercise twice weekly. The intensity level was increased to achieve an exertion rate equal to jogging (13‐15 on the Borg scale). Participants were then encouraged to perform regular training at home. Components: exercise, education and psychological support. Setting: supervised, group sessions in a centre. Exercise programme modality: "dynamic endurance training". Total duration: 15 weeks. Co‐interventions: The multidisciplinary CR of "Heart School" comprised dietary advice, smoking cessation, physical activity counselling, risk factor management, psychosocial management and health education. Comparator: Usual care: participants received usual standardised nurse‐based information on CHD in general and lifestyle measures. Co‐interventions: none described. | |
| Outcomes | Total mortality. | |
| Source of funding | The Norwegian Government Directory for Health and Bristol Myers Squib, Norway. | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomised" |
| Allocation concealment (selection bias) | Low risk | "[Randomization] was performed with pre‐prepared sealed opaque envelopes containing details on group allocation. The patients opened the envelopes themselves so that their allocation to IP or UC was revealed to them without the prior knowledge of the study investigators". |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described. |
| Incomplete outcome data (attrition bias) | High risk | 17.8% lost to follow‐up; no description of withdrawals or dropouts. |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: Multicentre RCT (2 sites) Country: China Dates participants recruited: Oct 2005 to April 2007 Maximum follow‐up: 6 months | |
| Participants | Inclusion criteria: Inclusion criteria comprised a documented diagnosis of acute MI, the ability to speak and read Chinese, a return to living at home after hospital discharge, availability for telephone follow‐up, and availability for meetings after hospital discharge. Exclusion criteria: Exclusion criteria comprised a known history of major psychiatric illness, pre‐existing mobility problems, unstable angina, severe complications such as uncontrolled arrhythmias or heart failure, and other conditions that could be aggravated by exercise, such as a resting systolic blood pressure (BP) > 200 mmHg or a resting diastolic BP > 110 mmHg. N randomised: total: 160; intervention: 80; comparator: 80 Diagnosis (% of participants): AMI: 100% Age (mean± SD): intervention: 57.3 (± 8.6); comparator: 58.3 (± 10.4) Percentage male: intervention: 85.3%; comparator: 81.5% Ethnicity: NR | |
| Interventions | Intervention: A 6‐week, home‐based rehabilitation programme using a self‐help heart manual given to the rehab participants just before discharge from hospital. The manual was similar to the UK Heart Manual but incorporated appropriate sociocultural components such as tai chi, qi gong, and Chinese diet. Section 1 consists of 6 weekly topics on health education. Section 2 answers commonly asked questions about medication, PCI, anxiety and depression etc. Section 3 presents information on normal values of cardiac physiological risk parameters. The rehabilitation group received the manual and the introductory session in addition to usual care. The exercise component of the manual is not described in this paper, and there is no reference to its description elsewhere. Components: exercise plus education. Setting: home. Exercise programme modality: not described. Total duration: not described. Co‐interventions: participants in both groups were telephoned by the principal researcher 3 weeks after discharge. For the rehabilitation group, the researcher checked the participants' progress, encouraged adherence to exercise, and helped solve problems that had arisen using the manual. This consultation lasted approximately 30 minutes, with contact designed to promote participant confidence and self‐management, and minimise dependency and the possibility that the nurse could influence outcomes. Comparator: The usual care group received instructions on taking medications, information leaflets about cardiac risk factors, a healthy diet, and smoking cessation, and a follow‐up appointment. Co‐interventions: The researcher devoted an equal amount of time to telephone contact with the control group, giving general advice on any problems encountered and encouraging and supporting appropriate actions. | |
| Outcomes | Mortality, HRQoL | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | Baseline characteristics only reported for those followed up until 6 months i.e. 68 in intervention group and 65 in usual care group. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “Patients …….were enrolled and assigned to either the experimental or the control group, using a computer‐generated random number”. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment was not described. |
| Blinding of outcome assessment (detection bias) | High risk | “the absence of a blinded condition may threaten its internal validity. In addition, the principal researcher played the role of both intervener and outcome assessor, which may have influenced participants to provide desired answers, and so interviewer bias cannot be excluded” |
| Incomplete outcome data (attrition bias) | Low risk | 12/80 (15%) lost from intervention group. 15/80 (18.8%) lost from the control group. Numbers and reasons were given and were similar for both groups. |
| Selective reporting (reporting bias) | Low risk | All outcomes described were reported for all time points. |
| Study characteristics | ||
| Methods | Study design: Multicentre RCT (14 sites) Country: England and Wales, UK Dates participants recruited: August 1997 to April 2000 Maximum follow‐up: 7 to 9 years | |
| Participants | Inclusion criteria: Admission to hospital with a principal primary diagnosis of acute MI (two of the three standard criteria ‘typical history’, electrocardiographic features and cardiac enzymes), discharged home within 28 days, local resident and able to give informed consent with no age or gender restrictions. Exclusion criteria: Physical frailty, mental confusion, serious co‐existing disease, communication difficulty, previous cardiac rehabilitation and discharged to hospice or another hospital. N randomised: total: 1813; intervention: 903; comparator: 910 Diagnosis (% of participants): Acute MI: 100% Age (mean± SD): intervention: 64.2 ± 11.2; comparator: 64.7 ± 10.9 Percentage male: intervention: 72.6%; comparator: 74.4% Ethnicity: NR | |
| Interventions | Intervention: Exercise training was the largest component, typically occupying half of the available time including warm up and cool down, and used exercise equipment in physiotherapy gyms. Relaxation was primarily physical following ‘cooling down’ from exercise with little or no ‘stress management’ training. Components: exercise plus education plus psych. Setting: centre‐based supervised programmes which varied by centre. Exercise programme modality: varied by centre. Total duration: 6‐8 weeks. Co‐interventions: The programmes comprised exercise training, health education about heart, heart disease, risk factors and treatment, counselling for recovery and advice for long‐term secondary prevention. All involved at least one other discipline (exercise physiologist, dietician, pharmacist, health promotion specialist, psychologist, counsellor, social worker, physician and/or cardiologist). Comparator: All participants in the trial (and in the ‘elective hospitals’ comparison) had similar care in all respects other than referral to cardiac rehabilitation, receiving available explanatory booklets, being advised to see their general practitioner (GP) and attend routine outpatient follow‐up, with referral for further cardiac investigations or interventions as appropriate. Co‐interventions: none described. | |
| Outcomes | Mortality, MI, revascularisations, hospitalisation, HRQoL. | |
| Source of funding | NHS Research and Development Programme (northern region) and the Heart Research Fund for Wales. | |
| Conflicts of interest | None declared. | |
| Notes | An additional 331 participants were entered in two matched pairs of ‘elective rehabilitation’ and ‘elective control’ hospitals; 197 to rehabilitation and 134 to control. These participants did not contribute any data used in the systematic review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “Patients were randomised centrally” – it does not state how. |
| Allocation concealment (selection bias) | Low risk | “Patients were randomised centrally on a preset protocol, daily and blind as to entry characteristics and baseline measures, …..The names of those randomised to rehabilitation were passed to the local programme coordinator”. |
| Blinding of outcome assessment (detection bias) | Low risk | Secondary outcomes were assessed at 1 year….blind to rehabilitation status”. |
| Incomplete outcome data (attrition bias) | Low risk | 5% lost to follow‐up from each group (2 year interviews); “follow‐up interviews were completed in 95% of surviving patients in both groups” |
| Selective reporting (reporting bias) | Low risk | All outcomes reported for all time points. |
| Study characteristics | ||
| Methods | Study design: Multicentre RCT (24 sites; 12 centres accepted for meta analysis.) Country: Multiple European countries Dates participants recruited: 1972 to 1974 Maximum follow‐up: 3 years Participants randomised on discharge from hospital. | |
| Participants | Inclusion criteria: Men < 65 years with first or consecutive MI. Exclusion criteria: NR N randomised: total: 3184; intervention: 1655; comparator: 1529 Diagnosis (% of participants): MI: 100% Age (years): intervention: 52.3; comparator:53.5 Percentage male: intervention: 100%; comparator: 100% Ethnicity: NR | |
| Interventions | Intervention: Comprehensive programme dependent on local provision. Physical training was not compulsory but was strongly recommended. Components: exercise, education and psychosocial support. Setting: centre. Exercise programme modality: NR Total duration: 6 weeks. Co‐interventions: The intervention had to be at the highest possible level available locally. It had to be comprehensive, with the aim of improving health and reducing IHD risk. It comprised treatment of heath failure, arterial hypertension etc, risk factor modification, weight loss and improving physical working capacity. Comparator: usual care. Co‐interventions: none described. | |
| Outcomes | Total mortality, CVD, CHD & sudden death. Fatal & non‐fatal re‐infarction. | |
| Source of funding | WHO Regional Office for Europe and the Ministries of Health of the participating member states. | |
| Conflicts of interest | ||
| Notes | Methodological problems with the execution of the study allowed only death and re‐infarction to be successfully used as end points. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | "Patients were randomised at admission.....by means of random number tables". However, only "12 centres out of the 24 seemed to have achieved proper randomisation in their groups of R and C patients” |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described. |
| Incomplete outcome data (attrition bias) | Unclear risk | No description of withdrawals or dropouts. Varied greatly from site to site. |
| Selective reporting (reporting bias) | Low risk | All clinical endpoints were reported for 12, 24 and 36 month follow‐ups. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Sweden Dates participants recruited: 1968‐1970 Maximum follow‐up: 5 years Participants randomised on discharge. | |
| Participants | Inclusion criteria: All participants born in 1913 or later who suffered a MI during the period 1968‐1970 and were discharged alive from the hospital. Exclusion criteria: none described. N randomised: total: 315; intervention: 158; comparator: 157 Diagnosis (% of participants): MI: 100% Age (years): intervention: 50.6; comparator: 50.6 Percentage male: intervention: 87%; comparator: 90% Ethnicity: NR | |
| Interventions | Intervention: The training programme started 3 months after the MI. The programme at the hospital consisted of three supervised half‐hour training sessions a week. It included dynamic work, such as callisthenics, cycling, and running in an interval programme with individualised intensity. If a participant found it difficult to attend the hospital for training, then individualised programmes were developed for training at home or in the workplace. Components: exercise. Setting: supervised in a centre. Exercise programme modality: e.g. cycling, running. Total duration: NR ‐ see notes below. Co‐interventions: At discharge from hospital, all participants were given general recommendations about gradually increasing physical activity during the convalescence period. Comparator: usual care. Co‐interventions: as above. | |
| Outcomes | Mortality, re‐infarction. | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | 1 year post‐MI, only 39% of those who started training were training at the hospital. A further 21% trained at home or at work. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "By the use of a random number table the patients were allocated..." |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of outcome assessment (detection bias) | Low risk | "The exercise test 1 yr after the MI followed the same protocol but was conducted by another physician, who did not know if the patients belonged to the experimental or the control group". |
| Incomplete outcome data (attrition bias) | Low risk | No losses to follow‐up for clinical events. |
| Selective reporting (reporting bias) | Unclear risk | Outcomes to be collected were not clearly described in the methods. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: China Dates participants recruited: January 2014 ‐ September 2015 Maximum follow‐up: 6 months | |
| Participants | Inclusion criteria: 1) Meet the diagnostic criteria of the coronary heart disease, referring to the 13th edition of the Practice Internal Medicine (a Chinese medical textbook) 2) From 39 to 70 years old 3) Participants who are easy to communicate with 4) Long‐term resident in the local area and completed the informed consent 5) Hemodynamics were stable after PCI Exclusion criteria: 1) People with serious arrhythmia (such as atrioventricular block, atrial fibrillation, ventricular tachycardia, etc.), myocarditis, cardiomyopathy, and the installation of a pacemaker 2) People with serious cardiac insufficiency (NYHA class IV), left ventricular ejection fraction < 30% 3) People with severe cerebrovascular diseases (such as cerebral infarction and cerebral haemorrhage) 4) People with serious pulmonary diseases (such as chronic obstructive pulmonary disease, emphysema, pulmonary heart disease, etc.) 5) People with rheumatoid arthritis, osteoarthritis, muscles and other diseases that seriously affect physical activity 6) People with serious organic diseases and abnormal liver and kidney function N randomised: total: 130; intervention: 65; comparator: 65 Diagnosis (% of participants): post‐PCI patients with unstable angina (100%). Age (mean ± SD): intervention: 56.4 ± 8.1; comparator: 58.6 ± 8 Percentage male: intervention: 46 (79%); comparator: 47 (78%) Ethnicity: NR | |
| Interventions | Intervention: There are 2 stages. The first stage is after patients had PCI until they were discharged, the second is from when they were discharged to the third month after PCI. The first stage: 1) The first day after PCI, advise patients to walk for 200 meters per time for 5 times a day. 2) The second day after PCI, advise patients to walk for 300 meters per time for 5 times a day. 3) The third day after PCI, advise patients to walk for 500 meters per time for 5 times a day. They can also go up and down a flight of stairs depending on their own conditions. The second stage: 1) After the patients discharged in the first month after PCI: Walking 30 to 40 mins with the speed of 65‐75 m/min for 3 times a week; or, walking for 10 to 15 mins 3 times a day with a 5‐min break among them for 3 times a week; or, walking for 15 to 20 mins twice a day with a 5‐min break between them for 3 times a week. After each time of walking, guide patients to do some chest enlargement, slow leg lift and upper limb extension exercise, so that the patients’ heart rate, blood pressure can be back to normal levels before walking. 2) 1 to 2 months after PCI: The exercise mode was repeated in alternations of walking and brisk walking. Walk for 90 seconds, followed by brisk walking for 45 s. Repeat above. The walking speed is at 65‐75 m/min, and the brisk walking speed is at 85‐95 m/min. This exercise was 30~40 min each time for 3 times a week. After each time, patients would have relaxation exercise for 10 to 15 mins. 3) 2 to 3 months after PCI: A set of exercise rehabilitation, includes a combination of upper limb and lower limb exercise, combined with resistance training of elastic band and balance training on yoga mat. The whole process can be divided into the pre‐activity stage (8‐10 min), the exercise march stage (30‐40 min) and the recovery stage (10‐15 min). Components: exercise only. Setting: centre‐based Exercise programme modality: Mostly walking, some upper and lower limb exercise, resistance training and balance exercises. Total duration: 3 months. Co‐interventions: None described Comparator: “All patients received conventional drug therapy and post‐PCI knowledge education” Co‐interventions: none described. | |
| Outcomes | No outcomes reported of relevance, no CONSORT flow diagram | |
| Source of funding | Not reported | |
| Conflicts of interest | Not reported | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “…used random sampling method to divide patients into intervention and control….” |
| Allocation concealment (selection bias) | Unclear risk | No details reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | No details reported |
| Incomplete outcome data (attrition bias) | Unclear risk | Reasons for participants lost to follow‐up not reported |
| Selective reporting (reporting bias) | Unclear risk | No published protocol available |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: China Dates participants recruited: NR Maximum follow‐up: 2 years | |
| Participants | Inclusion criteria: Obese participants with CHD who had either recent AMI or had undergone elective PCI in last 6 weeks. Exclusion criteria: Post‐infarction angina without revascularisation procedures, significant valvular stenosis, active pericarditis or myocarditis, severe uncontrolled hypertension, physical problems that precluded exercise training, cognitive impairment, malignancies that limited life span to 1 year. N randomised: total: 112; intervention: 72; comparator: 40 Diagnosis (% of participants): AMI: 64% Age (mean ±SD): intervention: 62.3 ± 11.2; comparator: 61.2 ± 10.2 Percentage male: intervention: 82%; comparator: 75% Ethnicity: NR | |
| Interventions | Intervention: Phase 1 was an inpatient ambulatory programme that lasted 7 to 14 days. Phase 2 was a 16‐session, twice weekly, outpatient exercise and education programme lasting for 8 weeks. Each session included 1 hour of education class followed by 2 hours of exercise training. The first hour of training focused on aerobic CV training with a target intensity of 65% to 85% of maximal aerobic capacity. This included treadmill, ergometry, rowing, stepper, arm ergometry, and dumbbell and weight training.The next hour was conducted by an occupational therapist in which domiciliary or vocational environment‐focused training was performed. Phase 3 was a community‐based home exercise programme for another 6 months. Components: exercise and education. Setting: centre followed by home. Exercise programme modality: treadmill, ergometry, rowing, stepper, arm ergometry, and dumbbell. Total duration: 8 1/2 months. Co‐interventions: Phase 4 was a long‐term follow‐up programme until the end of 2 years, which included half‐yearly monitoring of lipid profiles, and again stressed the importance of regular exercise and risk factor modification. Comparator: conventional medical therapy. Co‐interventions: The control group attended a 2‐hour talk that explained CHD, the importance of risk factor modification, and potential benefits of physical activity, but without undergoing an outpatient exercise training programme. | |
| Outcomes | HRQoL: 3F‐36 at 8 & 24 months. | |
| Source of funding | NR | |
| Conflicts of interest | NR | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described. |
| Incomplete outcome data (attrition bias) | Low risk | All participants accounted for. |
| Selective reporting (reporting bias) | Low risk | All outcomes were reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: China Dates participants recruited: NR Maximum follow‐up: 2 years | |
| Participants | Inclusion criteria: participants with recent AMI or after elective PCI. Exclusion criteria: Coronary heart disease without revascularisation procedures, significant mitral stenosis (defined as a mitral valve area of 1 cm2) or aortic stenosis (defined as an aortic valve gradient of 50 mmHg), active pericarditis or myocarditis, severe uncontrolled hypertension (systolic blood pressure 200 mmHg and/or diastolic blood pressure 100 mmHg), physical problems that precluded exercise, cognitive impairment or unwillingness to join the programme, malignancies that limited life span to less than 1 year. N randomised: total: 269; intervention: 181; comparator: 88 Diagnosis (% of participants): AMI: 72% Age (mean ±SD): intervention: 64 ± 11; comparator: 64 ± 11 Percentage male: intervention: 76%; comparator: 75% Ethnicity: NR | |
| Interventions | Intervention: Phase 1 was an inpatient ambulatory programme that lasted 7 to 14 days. Phase 2 was a 16‐session, twice weekly, outpatient exercise and education programme lasting for 8 weeks. Each session included 1 hour of education class followed by 2 hours of exercise training. The first hour of training focused on aerobic CV training with a target intensity of 65% to 85% of maximal aerobic capacity. This included treadmill, ergometry, rowing, stepper, arm ergometry, and dumbbell and weight training. The next hour was conducted by an occupational therapist in which domiciliary or vocational environment‐focused training was performed. Phase 3 was a community‐based home exercise programme for another 6 months. Components: exercise and education. Setting: centre followed by home. Exercise programme modality: treadmill, ergometry, rowing, stepper, arm ergometry, and dumbbell. Total duration: 8 1/2 months. Co‐interventions: Phase 4 was a long‐term follow‐up programme until the end of 2 years, which included half‐yearly monitoring of lipid profiles, and again stressed the importance of regular exercise and risk factor modification. Comparator: conventional medical therapy. Co‐interventions: The control group attended a 2‐hour talk that explained CHD, the importance of risk factor modification, and potential benefits of physical activity, but without undergoing an outpatient exercise training programme. | |
| Outcomes | Total mortality, HRQoL, costs. | |
| Source of funding | Health Care & Promotion Fund Committee of Hong Kong. | |
| Conflicts of interest | "No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit upon the authors(s) or upon any organization with which the author(s) is/are associated." | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomized" |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of outcome assessment (detection bias) | Unclear risk | Blinding not described. |
| Incomplete outcome data (attrition bias) | High risk | 24% lost to follow‐up; no description of withdrawals or dropouts. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points. |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: China Dates participants recruited: January 2010 ‐ December 2012 Maximum follow‐up: 6 months | |
| Participants | Inclusion criteria: participants admitted to the outpatient clinic after successful PCI for ST‐segment elevated MI between January 2010 and December 2012. Exclusion criteria: A large area of myocardial infarction, heart failure, acute systemic illness, systolic BP > 180 mmHg at rest, diastolic BP > 110 mmHg at rest, acute metabolic disorders, uncontrolled malignant arrhythmia, and skeletal vascular disease. N randomised: total: 130; intervention: 65; comparator: 65 Diagnosis (% of participants): post‐PCI for STEMI (100%). Age (mean ± SD): intervention: 70.3 ± 10.7; comparator: 69.8 ± 10.4 Percentage male: intervention: 59 (90.8%); comparator: 54 (83.1%) Ethnicity: NR | |
| Interventions | Intervention: GP formulated individual aerobic exercise program that could be performed in the participants' homes or at specialised rehabilitation facilities in the community. Phase II CR optimally initiated within 2 weeks of discharge (lasting 6‐8 weeks). Most available form of exercise was walking, but other forms of aerobic exercise were acceptable. HR < 130 bpm or resting HR plus 30 bpm, or RPE 11‐15. Participants exercised 2‐3 times per week, interval or continuous training for 15‐30 minutes. Phase III started from month 3 to 1 year. Target HR 60‐75% max HR, RPE 12‐16, 30‐45 minutes per session, no less than 3‐5 times per week. Components: exercise only. Setting: home‐ or centre‐based (community), participant choice Exercise programme modality: walking. Total duration: 12 months. Co‐interventions: None described Comparator: Usual care and conventional drug therapy post‐PCI Co‐interventions: none described. | |
| Outcomes | Mortality, MI hospitalisations | |
| Source of funding | Supported by Research Project for practice Development of National TCM Clinical Research Bases (JDZX2015133) | |
| Conflicts of interest | None declared | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information reported |
| Allocation concealment (selection bias) | Unclear risk | No information reported |
| Blinding of outcome assessment (detection bias) | Unclear risk | No information reported |
| Incomplete outcome data (attrition bias) | Low risk | No participants reported missing for outcomes of interest, all participants completed the study |
| Selective reporting (reporting bias) | Unclear risk | No published protocol paper or trial registration, very little description in the methods section about outcome assessment |
| Study characteristics | ||
| Methods | Study design: single‐centre RCT Country: Denmark Dates participants recruited: January 2000 to March 2003 Maximum follow‐up: 1 year | |
| Participants | Inclusion criteria: Participants with congestive heart failure (12%), *ischaemic heart disease (58%) or high risk of ischaemic heart disease (30%). Exclusion criteria: Mental or social problems, severe illness, living in nursing home, unable to speak Danish *Total Randomised (with IHD): total: 446; intervention: 227; comparator: 219 Diagnosis (% of participants): *Ischemic heart disease: 100% Age (years): intervention: 67; comparator: 67 Percentage male: intervention: 64%; comparator: 63% Ethnicity: NR | |
| Interventions | Intervention: A 6‐week intensive CR programme including 12 exercise training sessions. Components: exercise, education and psychosocial support. Setting: centre. Exercise programme modality: NR Total duration: 6 weeks. Co‐interventions: Standardised CR programme which was individually tailored and carried out by a multidisciplinary team, included participant education, dietary counselling, smoking cessation, psychosocial support, risk factor management, and clinical assessment. Comparator: usual care. Co‐interventions: none described. | |
| Outcomes | Total mortality, MI, CABG, PCI, health‐related quality of life: SF‐36 at 1‐yr follow‐up. | |
| Source of funding | Copenhagen Hospital Corporation Research Council, Danish Heart Foundation, Danish Pharmacy Foundation of 1991, Danish Research Council, Danish Center for Evaluation and Health Technology Assessment, Denmark's Ministry of the Interior and Health, Development Fund of Copenhagen County, Villadsen Family Foundation, Eva and Henry Frænkel's Memorial Foundation, Builder LP Christensen's Foundation, Danish Animal Protection Foundation, Bristol Meyers Squibb, Merck Sharp and Dohme, AstraZeneca, The Copenhagen Trial Unit, and Bispebjerg Hospital. | |
| Conflicts of interest | NR | |
| Notes | Outcomes of interest for the IHD population were kindly provided by the authors of this study. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "The Copenhagen Trial Unit computer generated the allocation sequence and provided central secretary‐staffed telephone randomization". |
| Allocation concealment (selection bias) | Low risk | "The essential patient data were registered, and the result of the randomization as delivered to the research nurse, who informed the CCR team and the patient about the allocation". |
| Blinding of outcome assessment (detection bias) | Low risk | "The ... team collected secondary outcome measures blinded to intervention at baseline and without blinding at 12 months. An independent statistician analyzed the primary outcome measure blinded to intervention arm. |
| Incomplete outcome data (attrition bias) | Low risk | All IHD participants accounted for. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported at all time points. |
ACE: acute coronary event
ACS: acute coronary syndrome
AMI: acute myocardial infarction
BMI: body mass index
CABG: coronary artery bypass graft
CAD: coronary artery disease
CAGS: Coronary artery graft surgery
CCU: coronary care unit
CHD: coronary heart disease
CHF: coronary heart failure
CR: cardiac rehabilitation
CV: cardiovascular
CVD: cardiovascular disease
ECG: electrocardiogram
ET: exercise training
FU: follow‐up
GI: gastrointestinal
HR: heart rate
HRQL/HRQoL: health‐related quality of life
IHD: ischaemic heart disease
Kpm/min: kilopond meters per minutes
LVEF: left ventricular ejection fraction
METS: metabolic equivalents
MI: myocardial infarction
MOS: Medical Outcomes Study
MVPA: moderate‐to‐vigorous physical activity
NR: not reported
PCI: percutaneous coronary intervention
PTCA: percutaneous transluminal coronary angioplasty
pts: participants
PWC: physical work capacity
RCT: randomised controlled trial
RPE: rating of perceived exertion
RTW: return to work
SPPB: short physical performance battery
STEMI: ST segment elevation myocardial infarction
V02max: maximum oxygen uptake
WHO: World Health Organisation
W: watts
6MWT: six minute walk test
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
| Ineligible comparator | |
| Ineligible comparator | |
| Improper method of randomisation (based on date of birth) | |
| Systematic review/meta‐analysis | |
| Ineligible study design | |
| Ineligible study design | |
| Not relevant | |
| Systematic review/meta‐analysis | |
| Comparator received exercise | |
| Follow‐up only 16 weeks | |
| Prehabilitation and outcomes of interest not measured or reported | |
| Participants received prior CR | |
| No useful outcome data measured or reported | |
| Method of randomisation was inadequate; of a study population of 265 across 5 centres, only one centre randomised their participants, leaving a control group of 50 and an intervention group of 215 | |
| Ineligible study design | |
| Systematic review/meta‐analysis | |
| Only a small subset of randomised participants responded via questionnaire. Incomplete outcome data | |
| Follow‐up only 6 weeks | |
| Follow‐up only 6 weeks | |
| Not a randomised study ‐ participants divided alternately after admission | |
| Systematic review/meta‐analysis | |
| Control group was not randomised, but selected on geographical basis | |
| Ineligible participant population | |
| Ineligible intervention | |
| Trial terminated early due to poor recruitment | |
| Systematic review/meta‐analysis | |
| Ineligible participant population | |
| Both groups recommended a home exercise training programme | |
| Comparator received exercise | |
| Participants had already received rehabilitation | |
| Systematic review/meta‐analysis | |
| Participants in both groups invited to join an exercise programme prior to randomisation | |
| Non‐RCT | |
| Follow‐up only 3 months | |
| “Our ancillary study was designed to evaluate the probable positive effects of the integrated care team, especially inmodifiable risk‐factor control and exercise capacity.” No outcomes of interest measured or reported | |
| Systematic review/meta‐analysis | |
| Ineligible study design | |
| Ineligible comparator | |
| Ineligible participant population | |
| Ineligible study design | |
| Ineligible study design | |
| Ineligible study design | |
| Ineligible study design | |
| Ineligible comparator | |
| Ineligible intervention | |
| Intervention does not contain exercise | |
| Ineligible study design | |
| Prior CR | |
| Prior CR | |
| Ineligible comparator | |
| Systematic review/meta‐analysis | |
| Ineligible study design | |
| Ineligible study design | |
| Ineligible study design | |
| Ineligible comparator | |
| Ineligible study design | |
| Not relevant | |
| Ineligible study design | |
| Comparator received exercise | |
| Ineligible intervention | |
| Non‐RCT | |
| Ineligible study design | |
| Systematic review/meta‐analysis | |
| Systematic review/meta‐analysis | |
| Systematic review/meta‐analysis | |
| Ineligible comparator | |
| Ineligible comparator | |
| Ineligible comparator | |
| Systematic review/meta‐analysis | |
| Non‐RCT | |
| No outcomes of interest were measured or reported | |
| No outcomes of interest were measured or reported | |
| No outcomes of interest were measured or reported | |
| All participants (treatment and control) participated in 3 to 6 week cardiac rehabilitation programme (including supervised exercise sessions) prior to randomisation. Control group was not "usual care" | |
| No outcomes of interest were measured or reported | |
| Ineligible study design | |
| Ineligible participant population | |
| Ineligible study design | |
| Non‐RCT | |
| Ineligible study design | |
| Follow‐up only 12 weeks | |
| Non‐RCT | |
| Non‐RCT | |
| Intervention does not contain exercise | |
| Intervention does not contain exercise | |
| Systematic review/meta‐analysis | |
| Ineligible study design | |
| No outcomes of interest were measured or reported | |
| Prior CR | |
| Ineligible study design | |
| Ineligible study design | |
| No outcomes of interest were measured or reported | |
| Non‐RCT | |
| Systematic review/meta‐analysis | |
| Prior CR | |
| Not relevant | |
| Ineligible intervention | |
| Prior CR | |
| Ineligible study design | |
| Ineligible study design | |
| Systematic review/meta‐analysis | |
| No useful outcome data were measured or reported | |
| Ineligible intervention | |
| Ineligible study design | |
| Trial terminated | |
| Both groups received cardiac rehabilitation | |
| Systematic review/meta‐analysis | |
| Non‐RCT | |
| No outcomes of interest measured or reported | |
| Non‐RCT | |
| Ineligible intervention | |
| Ineligible study design | |
| Non‐RCT | |
| Non‐RCT | |
| Non‐RCT | |
| Ineligible intervention | |
| Systematic review/meta‐analysis | |
| Ineligible comparator | |
| Not an exercise‐based CR programme | |
| Non‐RCT | |
| Ineligible intervention | |
| Non‐RCT | |
| Follow‐up < 6 months | |
| Follow‐up too short (3 to 4 weeks) and no useful outcome data reported | |
| Intervention does not contain exercise | |
| Systematic review/meta‐analysis | |
| Ineligible study design | |
| Ineligible comparator | |
| Prior CR | |
| Ineligible study design | |
| No outcomes of interest measured or reported | |
| Non‐RCT | |
| Systematic review/meta‐analysis | |
| Ineligible comparator | |
| Systematic review/meta‐analysis | |
| Systematic review/meta‐analysis | |
| Participants in the control group advised to perform home‐based activity | |
| Comparator received exercise | |
| Ineligible intervention | |
| Prior CR | |
| Systematic review/meta‐analysis | |
| Both groups received exercise | |
| Non‐RCT | |
| Ineligible comparator | |
| Ineligible comparator | |
| Comparator received exercise | |
| Comparator received exercise | |
| Participants had already received rehabilitation | |
| Ineligible study design | |
| Partcipants did not have CHD | |
| Systematic review/meta‐analysis | |
| Ineligible study design | |
| Not relevant | |
| Trial terminated | |
| Ineligible study design | |
| Ineligible comparator | |
| Ineligible intervention | |
| Ineligible comparator | |
| Ineligible intervention | |
| Prior CR | |
| Ineligible comparator | |
| Ineligible comparator | |
| Ineligible comparator | |
| Ineligible intervention | |
| Prior CR | |
| Ineligible comparator | |
| Ineligible study design | |
| Prior CR | |
| Ineligible study design | |
| Ineligible study design | |
| Ineligible study design | |
| Ineligible comparator | |
| Ineligible study design | |
| Ineligible intervention | |
| Comparator received exercise | |
| No useful outcome data measured or reported | |
| Ineligible comparator | |
| Both groups received CR | |
| Comparator received exercise | |
| Ineligible study design | |
| Both groups received CR prior to randomisation | |
| Comparator received exercise | |
| Systematic review/meta‐analysis | |
| Ineligible participant population | |
| Prior CR | |
| Ineligible comparator | |
| Ineligible study design | |
| Systematic review/meta‐analysis | |
| Systematic review/meta‐analysis | |
| Follow‐up only 8 weeks | |
| Intervention does not contain exercise | |
| Non‐RCT | |
| Follow‐up only 8 weeks | |
| Comparator received exercise | |
| Systematic review/meta‐analysis | |
| Prior CR | |
| Ineligible comparator | |
| Both groups received CR | |
| Follow‐up only 3 months | |
| Ineligible intervention | |
| Non‐RCT | |
| Ineligible comparator | |
| Follow‐up only 12 weeks | |
| Non‐RCT | |
| Participants did not have CHD | |
| Ineligible study design | |
| No outcomes of interest measured or reported | |
| Ineligible study design | |
| Follow‐up only 3 months | |
| Ineligible study design | |
| Follow‐up only 3 months | |
| Systematic review/meta‐analysis | |
| Systematic review/meta‐analysis | |
| Ineligible study design | |
| Both groups received exercise | |
| Systematic review/meta‐analysis | |
| Ineligible comparator | |
| Systematic review/meta‐analysis | |
| No useful outcome data measured or reported | |
| Ineligible intervention | |
| Intervention does not contain exercise | |
| Comparator received exercise | |
| Ineligible study design | |
| Ineligible comparator | |
| Prior CR | |
| Comparator received exercise | |
| Ineligible intervention | |
| Ineligible intervention | |
| Ineligible participant population | |
| Systematic review/meta‐analysis | |
| Ineligible comparator | |
| Ineligible intervention | |
| Less than 50% participants had CHD | |
| No useful outcome data measured or reported | |
| Systematic review/meta‐analysis | |
| Ineligible comparator | |
| Systematic review/meta‐analysis | |
| Systematic review/meta‐analysis | |
| Non‐RCT | |
| Ineligible study design | |
| Ineligible participant population | |
| Systematic review/meta‐analysis | |
| Systematic review/meta‐analysis | |
| Ineligible study design | |
| No useful outcome data measured or reported | |
| Intervention does not include exercise | |
| Retraction |
CHD: coronary heart disease
CR: cardiac rehabilitation
RCT: randomised controlled trial
NR: not reported
Characteristics of studies awaiting classification [ordered by study ID]
| Methods | Study design: NR Country: Russia Follow‐up: 6 months |
| Participants | Inclusion criteria: Acute coronary event (acute myocardial infarction, unstable angina, CABG) Exclusion criteria: NR N randomised: total: 373; intervention: 188; comparator: 185 |
| Interventions | Intervention: Standard therapy plus exercise programme ‐ moderate exercise for 1 hour, 3 times per week for 1 year Comparator: Standard therapy |
| Outcomes | Not clear if any outcomes of interest were measured or reported |
| Notes | Unable to access full text |
| Methods | Study design: RCT Country: NR Dates participants recruited: January 2002 to November 2004 Planned follow‐up: 5 years |
| Participants | Inclusion criteria: NR Exclusion criteria: NR N randomised: total: 259 Diagnosis (% of participants): people with CAD who underwent PCI or CABG Age (years): Intervention: 56±8 years; comparator: 58±8 years |
| Interventions | Intervention: Group CR combining exercise training 60% peak VO2 3 times a week for 8 weeks with nutrition counselling and standard medication Comparator: No CR |
| Outcomes | MI, PCI, CABG, hospitalisation, cardiac death |
| Notes | Abstract only, with incomplete reporting of study characteristics and outcome data. Full trial report not published. |
| Methods | Study design: RCT Planned follow‐up: 1 year |
| Participants | N randomised: total: 62; intervention: 31; control: 31 Diagnosis (% of participants): PCI (100%) Age (years): Intervention: 56±7 years; comparator: 53±8 years |
| Interventions | Intervention: Program of moderate intensity physical training (60 min per session, 3 times per week for 6 weeks) plus education and standard therapy Comparator: Educational program and standard therapy |
| Outcomes | "Cardiovascular events" (not clear what these include) |
| Notes | Conference abstract; triallists did not respond to repeated requests for further information |
| Methods | Study design: RCT |
| Participants | Inclusion criteria: Participants with a clinical diagnosis of AMI, aged 18 to 80 years, performed PCI, and signed a consent form. Exclusion criteria: Current participation in any other behavioural or pharmacological study or instructor‐led exercise program, cardiogenic shock, severe heart failure (NYHA class IV or LVEF ≤ 35%), malignant arrhythmia (ventricular fibrillation, ventricular tachycardia, and frequent ventricular premature beats), or active bleeding. People with underlying conditions such as bone and joint disease or nervous system disorders that would impede full participation in the study and unavailability during the study period. |
| Interventions | Intervention: Baduanjin sequential therapy (BST) beginning 2 days after surgery (30 min/session, twice per day, 3 days). After discharge, participants did standing Baduanjin exercises 30 min/session, five times per week for 24 weeks. Participants were provided picture‐based educational brochure, and telephone follow‐ups were provided to reinforce participants' adherence to the follow‐up assessments. |
| Outcomes | HRQoL |
| Notes | The authors were contacted to clarify an unclear section within the methods describing the treatment received by the control group, but no response received. |
| Methods | Study design: RCT Country: NR Dates participants recruited: NR Planned follow‐up: 2 years |
| Participants | Inclusion criteria: people with MI who underwent coronary stenting Exclusion criteria: NR N randomised: total: 68; intervention: 30; comparator: 38 Diagnosis (% of participants): post‐coronary stenting after myocardial infraction |
| Interventions | Cardiac rehabilitation programme not described |
| Outcomes | HRQoL |
| Notes | The authors of this conference abstract did not reply to repeated requests for an update on the status of this study. |
| Methods | Study design: RCT Planned follow‐up: 2 years |
| Participants | Inclusion criteria: NR Exclusion criteria: NR N randomised: total: 200; intervention: 92; control: 108 Diagnosis (% of participants): CABG (100%) Mean age: 57.7 years |
| Interventions | Intervention: 2‐year comprehensive rehabilitation programme with cardiologist supervision (1, 3, and every 6 months), intermediate telephone/internet contact (9, 15, 21 months post‐surgery), controlled exercise training (every 6 months) and self‐controlled exercise training (daily morning exercise and walking), psychologist counselling, education programme (60 min every 6 months). Comparator: standard care |
| Outcomes | Treatment costs |
| Notes | Conference abstract; unable to locate full text despite contacting triallists |
| Methods | Study design: RCT Planned follow‐up: 24 weeks |
| Participants | Inclusion criteria: NR Exclusion criteria: NR N randomised: total: 90; intervention: 45; control: 45 Diagnosis (% of participants): ACS (100%) Mean age: intervention: 69.2±4.1 years; comparator: 69.2±5.6 years |
| Interventions | Intervention: Exercise sessions (8 cardiovascular exercises interrupted by 1 minute active breaks), 1 session per week for 2 months Comparator: NR |
| Outcomes | No outcomes of interest reported in either conference abstract |
| Notes | Unable to locate full text |
| Methods | Study design: RCT Follow‐up: 1 year |
| Participants | Inclusion criteria: Clinical diagnosis of ST‐elevated MI, heart function class I‐II (Killip classification), agree to take cardiopulmonary exercise testing before discharge, signature of informed consent document Exclusion criteria: History of MI, acute MI with severe complications (pulmonary edema, severe cardiac arrhythmia or cardiogenic shock), atrial fibrillation, other severe diseases such as HIV infection, malignant tumour or chronic diseases of liver kidney or pulmonary, not capable of exercise training |
| Interventions | Intervention: exercise training Comparator: NR |
| Outcomes | Cardiac mortality, MI, revascularisation, hospitalisation |
| Notes | Triallists contacted for update on status of study, but no response received |
| Methods | Study design: RCT Country: Norway Follow‐up: 3 years |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Intervention: structured secondary prevention programme including patient education, brief counselling, and systematic physical training tailored to each individual. The exercise programme consists of 8 weeks of supervised outpatient physical training. Comparator: conventional care |
| Outcomes | HRQoL |
| Notes | Authors did not respond to repeated requests for study update. |
| Methods | Study design: RCT Follow‐up: 1 year |
| Participants | Inclusion criteria: NR Exclusion criteria: NR N randomised: total: 64; intervention: 29; control: 35 Diagnosis (% of participants): CABG (100%) Mean age: 54.7±4.6 years |
| Interventions | Intervention: Common medical rehabilitation programme with long‐term (3 months) cycling training Comparator: Common medical rehabilitation (medication, lifestyle modifications) |
| Outcomes | Unclear if any outcomes of interest were measured or reported |
| Notes | Triallists did not respond to requests for study updates |
| Methods | Study design: RCT Follow‐up: 12 months |
| Participants | Inclusion criteria: participants with ACS, age > 75 years, after PCI Exclusion criteria: NR N randomised: total: 51; intervention: 25; control: 26 Diagnosis (% of participants): PCI (100%) Mean age: 80 years |
| Interventions | Intervention: training three times per week for 2 months Comparator: received general recommendations for activity |
| Outcomes | HRQoL |
| Notes | Triallists did not respond to repeated requests for study updates |
| Methods | Study design: RCT Follow‐up: NR |
| Participants | Inclusion criteria: participants surviving MI Exclusion criteria: NR N randomised: total: 110; intervention: 53; control: 57 Diagnosis (% of participants): NR Mean age: 58.3 ± 9.8 years |
| Interventions | Intervention: Walking at a speed corresponding to 60% maximal heart rate Comparator: NR |
| Outcomes | Costs |
| Notes | Unable to contact triallists for further information |
| Methods | Study design: RCT Country: NR Dates participants recruited: NR Planned follow‐up: 2 years |
| Participants | Inclusion criteria: participants with CAD and proven exercise‐induced ischaemia Exclusion criteria: NR N randomised: total: 103; intervention: 57; comparator: 46 Age (years): NR Percentage male: NR Ethnicity: NR |
| Interventions | Intervention: regular exercise training Comparator: PCI/stenting |
| Outcomes | Mortality |
| Notes | The authors of this conference abstract did not reply to repeated requests for an update on the status of this study. |
| Methods | Study design: RCT Country: NR Dates participants recruited: NR Planned follow‐up: 2 years |
| Participants | Inclusion criteria: Male participants with indication for elective CABG Exclusion criteria: NR N randomised: total: 47; intervention: 23; comparator: 24 Age (mean ± SD): 64.3 ± 7 years Percentage male: 100% Ethnicity: NR |
| Interventions | Intervention: four‐week pre‐operative endurance training course Comparator: non‐active control |
| Outcomes | HRQoL and clinical outcomes |
| Notes | The authors of this conference abstract did not reply to repeated requests for an update on the status of this study. |
ACS: acute coronary syndrome
CABG: coronary artery bypass graft
CAD: coronary artery disease
CHD: coronary heart disease
CR: cardiac rehabilitation
HRQol: health‐related quality of life
MI: myocardial infarction
N: number
NR: not reported
PCI: percutaneous coronary intervention
PTCA: percutaneous transluminal coronary angioplasty
RCT: randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
| Study name | Tai Chi for stress and cardiovascular function in patients with coronary heart disease and/or hypertension: a randomised controlled trial |
| Methods | RCT with waiting‐list control |
| Participants | Inclusion criteria: (1) Equal to or greater than 40 years of age, regardless of gender; (2) With documented diagnosis of CHD (myocardial infarction, angina or revascularisation) with severity of angina class I to II according to the Canadian Cardiovascular Society functional classification, and/or with established diagnosis of hypertension according to the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; (3) Ability to perform prescribed Tai Chi program; (4) Willing to complete the 24‐week Tai Chi intervention; (5) Not practicing Tai Chi in the past 6 months; (6) Ability to speak and read Chinese or English fluently; (7) Willing to sign a written informed consent. Exclusion criteria: (1) Pregnancy (2) Previous or current psychological disorders not associated with depression or anxiety (3) End‐stage congestive heart failure (4) Permanent bed‐bound status (5) Unstable abdominal, thoracic or cerebral aneurysm (6) Acute myocarditis, pericarditis, pulmonary embolus or pulmonary infarction (7) Significant limitation of physical activity for reasons other than CHD (8) Participation in a clinical trial for an experimental drug within the last 30 days before the study |
| Interventions | Intervention: the intervention group will be offered a standardised Tai Chi intervention over a period of 24 weeks, consisting of a 12‐week intensive Tai Chi intervention and a 12‐week sustained Tai Chi intervention. Comparator: participants assigned to the waiting‐list control group will be instructed to maintain their routine activities and not to begin any new exercise programs during their study participation. These participants will be offered an equivalent 12‐week intensive Tai Chi intervention and 12‐week sustained Tai Chi intervention at the termination of the study, provided the Tai Chi intervention in the treatment is proved to be safe (no severe adverse events directly associated with Tai Chi). |
| Outcomes | HRQoL, adverse events |
| Starting date | 28 August 2015 |
| Contact information | |
| Notes |
| Study name | Efficacy of YOGA in Indian patients with coronary artery disease |
| Methods | RCT |
| Participants | Inclusion criteria: 1. All adults between 30 and 70 years Exclusion criteria: 1. Severe LV dysfunction |
| Interventions | Intervention: participants undergoing PCI with routine advice on discharge and enhanced usual care(physiotherapy, medications and lifestyle modifications) will be taught yoga, based on the module in the first week of each phase. On non‐class days, participants will be motivated to practice yoga sessions at home every day, and their compliance will be ensured telephonically and through a written log. The participants will be encouraged to practice until the end of the follow‐up period (3 years). Comparator: participants will be on enhanced usual care after PCI. |
| Outcomes | MACCE, HRQoL |
| Starting date | 03 July 2017 |
| Contact information | |
| Notes |
| Study name | Efficacy of yoga‐based cardiac rehabilitation on clinical outcomes in post CABG patients: a randomized controlled trial. |
| Methods | RCT |
| Participants | Inclusion criteria: 1. People willing and able to participate Exclusion criteria: a. Emergency CABG d. Acute and chronic renal failure with or without dialysis |
| Interventions | Intervention: yoga plus conventional medical management which includes physiotherapy, lifestyle modifications and medications Comparator: conventional medical management |
| Outcomes | HRQoL, MACCE |
| Starting date | 10/10/2017 |
| Contact information | |
| Notes |
| Study name | Effect of cardiac rehabilitation in patients undergone myocardial infarction and percutaneous coronary intervention |
| Methods | RCT |
| Participants | Inclusion criteria: 1. 18 to 80 years of age Exclusion criteria: 1. Participants with medical conditions which could put them at risk during physical activity testing or training (e.g. angina), or conditions that could limit the participant’s ability to exercise (e.g. severe |
| Interventions | Intervention: adapted phase II and phase III of cardiac rehabilitation programme with components of physical activity, education on coronary artery disease and heart‐healthy living Comparator: participants will not receive any supervised physical activity training. Participants will receive routine care for myocardial infarction after undergoing percutaneous coronary intervention according to current guidelines. |
| Outcomes | HRQoL, cost effectiveness, all‐cause mortality |
| Starting date | 02 July 2019 |
| Contact information | |
| Notes |
| Study name | Century Trial, a randomized lifestyle modification study for management of stable coronary artery disease (Century) |
| Methods | RCT (single centre) |
| Participants | Inclusion Criteria:
Exclusion criteria:
|
| Interventions | Intervention: "P.E.T. guided comprehensive therapy program. The study intervention is comprehensive therapy program for risk factor modification. The comprehensive program of atherosclerotic risk factor modification involves treatment to target lipid levels, blood pressure and diabetes control, smoking cessation, very low fat diet and aerobic exercise program. This is in addition to standard current medical therapy as provided by primary physician. No experimental medications or procedures will be used." "During the 5 year follow‐up they will be educated and guided toward a healthy lifestyle by a dietician, an exercise physiologist/cardiovascular physician specialist." Comparator: "Current standard of care medical management as provided by primary physician." |
| Outcomes | Mortality, non‐fatal MI, revascularisation, total cost |
| Starting date | March 2009 |
| Contact information | K.Lance Gould, Professor, Internal Medicine, Cardiology, University of Texas Health Science Center, Houston |
| Notes |
| Study name | Effects of exercise in patients with coronary artery disease aged 80 years or older |
| Methods | RCT |
| Participants | Inclusion criteria: clinical diagnosis of acute CAD, aged 80 years or older. |
| Interventions | Intervention: exercise Comparator: NR |
| Outcomes | HRQoL |
| Starting date | December 2013 |
| Contact information | Maria Bäck, PhD |
| Notes |
| Study name | efficAcy and Safety of Home‐baSed Cardiac rehabIlitation in ChineSe Revascularized patienTs (ASSIST) |
| Methods | RCT |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Intervention: home‐based cardiac rehabilitation Comparator: no instructed exercise training |
| Outcomes | MACCE, hospitalisation, HRQoL |
| Starting date | 09 November 2017 |
| Contact information | |
| Notes |
| Study name | Utilisation of Telemedicine in Optimal Cardiac Rehabilitation Program in Patients After Myocardial Revascularization (RESTORE) |
| Methods | RCT |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Intervention: Comparator: |
| Outcomes | Mortality, cardiovascular events |
| Starting date | March 2018 |
| Contact information | Krzysztof Milewski; [email protected] |
| Notes |
| Study name | Tele‐Cardiac Rehabilitation Program |
| Methods | RCT |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Intervention: Comparator: |
| Outcomes | hospitalisation, mortality, HRQoL |
| Starting date | July 2018 |
| Contact information | Dr. Robert Klempfner Heart Rehabilitation Institute, Head, Cardiovascular Prevention and Rehabilitation Institute, Sheba Medical Center, Israel, Sheba Medical Center |
| Notes |
| Study name | Stress Management Modified Cardiac Rehabilitation in Patients After Acute Myocardial Infarction or Heart Failure |
| Methods | RCT |
| Participants | Inclusion criteria: Exclusion criteria: |
| Interventions | Intervention 1: Intervention 2: Comparator: |
| Outcomes | HRQoL, rehospitalisation, MACE |
| Starting date | April 2019 |
| Contact information | |
| Notes |
| Study name | Rehabilitation at Home Using Mobile Health in Older Adults after Hospitalization for Ischemic Heart Disease (RESILIENT) |
| Methods | Multicentre RCT |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Intervention: mHealth‐CR: participants receive 3 components for their home activity: (1) communication with exercise therapist (in‐hospital assessment/counselling followed by regular communication post‐discharge), (2) mHealth‐CR software, and (3) wearable activity‐monitoring device. Comparator: usual care |
| Outcomes | HRQoL, hospital readmissions, mortality |
| Starting date | January 2020 |
| Contact information | |
| Notes |
| Study name | Effect of a High Intensity Interval Training in Older Adults With Coronary Artery Disease |
| Methods | RCT |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Intervention: physiotherapy program during two months: interval training at a high intensity, including a warm‐up and a cool‐down. Aerobic exercises, resistance exercises, stretching. Comparator: no physiotherapy. |
| Outcomes | HRQoL (SF‐36) |
| Starting date | October 2012 |
| Contact information | Elena Marques‐Sule, PhD, PT, University of Valencia |
| Notes |
| Study name | M‐Health Care for Patients After AMI on Disease Perception, Self‐Efficacy, Anxiety and Cardio‐Respiratory Fitness |
| Methods | RCT (waiting‐list control) |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Intervention: M‐Health app to remind participants of the walking frequency and time, and use Garmin monitoring bracelet to record daily walking steps. App content also includes knowledge about acute myocardial infarction, self‐care and anxiety. Control: Waiting‐list control for 3 months, then receive the same M‐Health intervention |
| Outcomes | |
| Starting date | 22 July 2020 |
| Contact information | Hui‐Hsun Chiang: [email protected] |
| Notes |
| Study name | Early Individualized‐Exercise Based Cardiac Rehabilitation Programs in Patients With Acute Myocardial Infarction |
| Methods | RCT |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Intervention: exercise intervention group. Participants will receive standard medications plus exercise based CR. Education covering topics related to AMI and exercise for AMI will be implemented and any consultations on exercise prescription and disease management will be explained by a cardiac rehabilitation team consisting of cardiologists, cardiology nurses and physiotherapists. Comparator: participants will receive standard medications according to national guidelines, as well as education and consultations as intervention group. However, no exercise prescription is given. |
| Outcomes | HRQoL (SF‐36), MACE |
| Starting date | 1 February 2021 |
| Contact information | Qin Shao: [email protected] |
| Notes |
| Study name | An Internet‐based Cardiac Rehabilitation Enhancement (i‐CARE) Intervention to Support Self‐care of Patients With Coronary Artery Disease |
| Methods | RCT |
| Participants | Inclusion criteria:
Exclusion criteria:
|
| Interventions | Intervention: Comparator: |
| Outcomes | cardiovascular events, mortality, HRQoL |
| Starting date | May 2021 |
| Contact information | Dr. Polly Wai‐Chi Li, The University of Hong Kong [email protected] |
| Notes |
ACS: acute coronary syndrome
AMI: acute myocardial infarction
APVD: atherosclerotic peripheral vascular disease
CABG: coronary artery bypass graft
COPD: chronic obstructive pulmonary disease
CPET: cardiopulmonary exercise test
CRTD: cardiac resynchronization therapy defibrillator
CTED: chronic pulmonary thromboembolic disease
DBP: diastolic blood pressure
HDL: high‐density lipoprotein
HRQoL: health‐related quality of life
ICD: implantable cardioverter defibrillator
LDL: low‐density lipoprotein
LV: left‐ventricular
LVEF: left ventricular ejection fraction
MACCE: major adverse cardiac and cerebrovascular events
MACE: major adverse coronary event
NYHA: New York Heart Association
PCI: percutaneous coronary intervention
RCT: randomised controlled trial
SBP: systolic blood pressure
Data and analyses
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1.1 All‐cause mortality Show forest plot | 47 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Analysis 1.1  Comparison 1: Exercise‐based rehabilitation versus control, Outcome 1: All‐cause mortality | ||||
| 1.1.1 Follow‐up of 6 to 12 months | 25 | 8823 | Risk Ratio (M‐H, Random, 95% CI) | 0.87 [0.73, 1.04] |
| 1.1.2 Follow‐up of > 12 to 36 months | 16 | 11073 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.80, 1.02] |
| 1.1.3 Follow‐up longer than 3 years | 11 | 3828 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.75, 1.10] |
| 1.2 Cardiovascular mortality Show forest plot | 26 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Analysis 1.2  Comparison 1: Exercise‐based rehabilitation versus control, Outcome 2: Cardiovascular mortality | ||||
| 1.2.1 Follow‐up of 6 to 12 months | 15 | 5360 | Risk Ratio (M‐H, Random, 95% CI) | 0.88 [0.68, 1.14] |
| 1.2.2 Follow‐up of > 12 months to 36 months | 5 | 3614 | Risk Ratio (M‐H, Random, 95% CI) | 0.77 [0.63, 0.93] |
| 1.2.3 Follow‐up of longer than 3 years | 8 | 1392 | Risk Ratio (M‐H, Random, 95% CI) | 0.58 [0.43, 0.78] |
| 1.3 Fatal and/or nonfatal MI Show forest plot | 39 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Analysis 1.3  Comparison 1: Exercise‐based rehabilitation versus control, Outcome 3: Fatal and/or nonfatal MI | ||||
| 1.3.1 Follow‐up of 6 to 12 months | 22 | 7423 | Risk Ratio (M‐H, Random, 95% CI) | 0.72 [0.55, 0.93] |
| 1.3.2 Follow‐up of > 12 to 36 months | 12 | 9565 | Risk Ratio (M‐H, Random, 95% CI) | 1.07 [0.91, 1.27] |
| 1.3.3 Follow‐up of longer than 3 years | 10 | 1560 | Risk Ratio (M‐H, Random, 95% CI) | 0.67 [0.50, 0.90] |
| 1.4 CABG Show forest plot | 29 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Analysis 1.4  Comparison 1: Exercise‐based rehabilitation versus control, Outcome 4: CABG | ||||
| 1.4.1 Follow‐up of 6 to 12 months | 20 | 4473 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.78, 1.27] |
| 1.4.2 Follow‐up of > 12 to 36 months | 9 | 2826 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.77, 1.23] |
| 1.4.3 Follow‐up of longer than 3 years | 4 | 675 | Risk Ratio (M‐H, Random, 95% CI) | 0.66 [0.34, 1.27] |
| 1.5 PCI Show forest plot | 18 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Analysis 1.5  Comparison 1: Exercise‐based rehabilitation versus control, Outcome 5: PCI | ||||
| 1.5.1 Follow‐up of 6 to 12 months | 13 | 3465 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.63, 1.19] |
| 1.5.2 Follow‐up of > 12 to 36 months | 6 | 1983 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.69, 1.35] |
| 1.5.3 Follow‐up of longer than 3 years | 3 | 567 | Risk Ratio (M‐H, Random, 95% CI) | 0.76 [0.48, 1.20] |
| 1.6 All‐cause hospital admissions Show forest plot | 22 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Analysis 1.6  Comparison 1: Exercise‐based rehabilitation versus control, Outcome 6: All‐cause hospital admissions | ||||
| 1.6.1 Follow‐up of 6 to 12 months | 14 | 2030 | Risk Ratio (M‐H, Random, 95% CI) | 0.58 [0.43, 0.77] |
| 1.6.2 Follow‐up of > 12 to 36 months | 9 | 5995 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.82, 1.03] |
| 1.7 Cardiovascular hospital admissions Show forest plot | 8 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| Analysis 1.7  Comparison 1: Exercise‐based rehabilitation versus control, Outcome 7: Cardiovascular hospital admissions | ||||
| 1.7.1 Follow‐up of 6 to 12 months | 6 | 1087 | Risk Ratio (M‐H, Random, 95% CI) | 0.80 [0.41, 1.59] |
| 1.7.2 Follow up of >12 to 36 months | 3 | 943 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.76, 1.12] |
| 1.8 HRQoL SF‐36 summary scores at 6 to 12 months follow up Show forest plot | 6 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 1.8  Comparison 1: Exercise‐based rehabilitation versus control, Outcome 8: HRQoL SF‐36 summary scores at 6 to 12 months follow up | ||||
| 1.8.1 Physical component score | 6 | 1741 | Mean Difference (IV, Random, 95% CI) | 1.70 [‐0.08, 3.47] |
| 1.8.2 Mental component score | 6 | 1741 | Mean Difference (IV, Random, 95% CI) | 2.14 [1.07, 3.22] |
| 1.9 HRQoL SF‐36 8 domains at 6 to 12 months follow up Show forest plot | 8 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| Analysis 1.9  Comparison 1: Exercise‐based rehabilitation versus control, Outcome 9: HRQoL SF‐36 8 domains at 6 to 12 months follow up | ||||
| 1.9.1 Physical functioning | 8 | 2756 | Mean Difference (IV, Random, 95% CI) | 8.47 [3.69, 13.24] |
| 1.9.2 Physical performance | 8 | 2756 | Mean Difference (IV, Random, 95% CI) | 8.08 [2.89, 13.27] |
| 1.9.3 Bodily pain | 8 | 2756 | Mean Difference (IV, Random, 95% CI) | ‐0.06 [‐8.97, 8.84] |
| 1.9.4 General health | 8 | 2756 | Mean Difference (IV, Random, 95% CI) | 5.66 [2.08, 9.25] |
| 1.9.5 Vitality | 7 | 2638 | Mean Difference (IV, Random, 95% CI) | 5.78 [1.89, 9.67] |
| 1.9.6 Social functioning | 8 | 2756 | Mean Difference (IV, Random, 95% CI) | 1.98 [0.26, 3.70] |
| 1.9.7 Emotional performance | 7 | 2638 | Mean Difference (IV, Random, 95% CI) | 0.69 [‐1.33, 2.71] |
| 1.9.8 Mental health | 8 | 2756 | Mean Difference (IV, Random, 95% CI) | 5.60 [1.21, 9.98] |
| 1.10 HRQoL EQ‐5D at 6 to 12 months follow up Show forest plot | 3 | 476 | Mean Difference (IV, Random, 95% CI) | 0.05 [‐0.01, 0.10] |
| Analysis 1.10  Comparison 1: Exercise‐based rehabilitation versus control, Outcome 10: HRQoL EQ‐5D at 6 to 12 months follow up | ||||

PRISMA flow diagram of study selection process

Risk of bias summary: review authors' judgements about each risk of bias item for each included study

Funnel plot of comparison: exercise‐based rehabilitation versus usual care, outcome 1.1: all‐cause mortality at 6 to 12 months' follow‐up

Funnel plot of comparison: exercise‐based rehabilitation versus usual care, outcome 1.1: all‐cause mortality at > 36 months' follow‐up
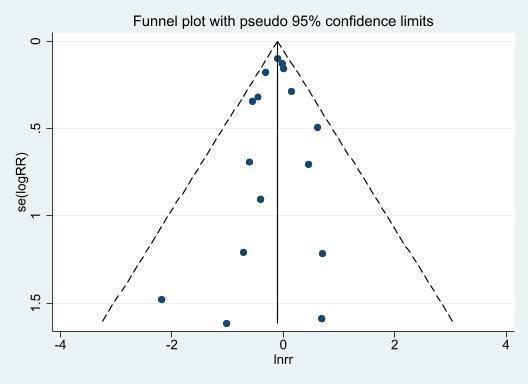
Funnel plot of comparison: exercise‐based rehabilitation versus usual care, outcome 1.1: all‐cause mortality at > 12 to 36 months' follow‐up
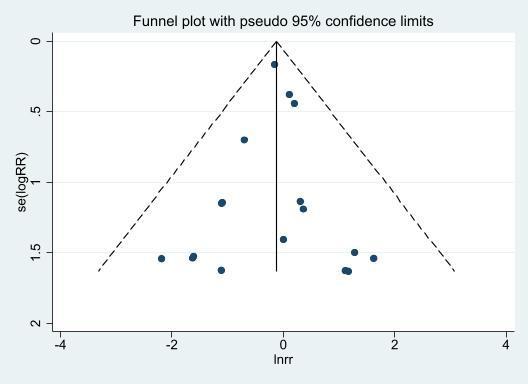
Funnel plot of comparison: exercise‐based rehabilitation versus usual care, outcome 1.2: cardiovascular mortality at 6 to 12 months' follow‐up

Funnel plot of comparison: exercise‐based rehabilitation versus usual care, outcome 1.3: myocardial infarction at 6 to 12 months' follow‐up

Funnel plot of comparison: exercise‐based rehabilitation versus usual care, outcome 1.1: myocardial infarction at > 12 to 36 months' follow‐up

Funnel plot of comparison: exercise‐based rehabilitation versus usual care, outcome 1.1: myocardial infarction at > 36 months' follow‐up

Funnel plot of comparison: exercise‐based rehabilitation versus usual care, outcome 1.1: CABG at 6 to 12 months' follow‐up

Funnel plot of comparison: exercise‐based rehabilitation versus usual care, outcome 1.1: PCI at 6 to 12 months' follow‐up

Funnel plot of comparison: exercise‐based rehabilitation versus usual care, outcome 1.1: all‐cause hospitalisation at 6 to 12 months' follow‐up

Comparison 1: Exercise‐based rehabilitation versus control, Outcome 1: All‐cause mortality

Comparison 1: Exercise‐based rehabilitation versus control, Outcome 2: Cardiovascular mortality

Comparison 1: Exercise‐based rehabilitation versus control, Outcome 3: Fatal and/or nonfatal MI

Comparison 1: Exercise‐based rehabilitation versus control, Outcome 4: CABG

Comparison 1: Exercise‐based rehabilitation versus control, Outcome 5: PCI

Comparison 1: Exercise‐based rehabilitation versus control, Outcome 6: All‐cause hospital admissions

Comparison 1: Exercise‐based rehabilitation versus control, Outcome 7: Cardiovascular hospital admissions

Comparison 1: Exercise‐based rehabilitation versus control, Outcome 8: HRQoL SF‐36 summary scores at 6 to 12 months follow up

Comparison 1: Exercise‐based rehabilitation versus control, Outcome 9: HRQoL SF‐36 8 domains at 6 to 12 months follow up

Comparison 1: Exercise‐based rehabilitation versus control, Outcome 10: HRQoL EQ‐5D at 6 to 12 months follow up
| Exercise‐based cardiac rehabilitation compared to 'no exercise' control for coronary heart disease | ||||||
| Patient or population: people with coronary heart disease | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect | № of participants | Certainty of the evidence | Comments | |
|---|---|---|---|---|---|---|
| Risk with 'no exercise' control | Risk with exercise‐based cardiac rehabilitation | |||||
| All‐cause mortality | Study population | RR 0.87 | 8823 | ⊕⊕⊕⊝ | Exercise‐based cardiac rehabilitation likely results in a slight reduction in all‐cause mortality up to 12 months' follow‐up. 25 RCTs with 26 comparisons. 14 RCTs reported 0 events in both the intervention and control groups. | |
| 57 per 1000 | 50 per 1000 | |||||
| Cardiovascular mortality | Study population | RR 0.88 | 5360 | ⊕⊕⊕⊝ | Exercise‐based cardiac rehabilitation likely results in little to no difference in cardiovascular mortality up to 12 months' follow‐up. 5 RCTs reported 0 events in both the intervention and control groups. | |
| 45 per 1000 | 39 per 1000 | |||||
| Fatal and/or non‐fatal MI | Study population | RR 0.72 | 7423 | ⊕⊕⊕⊕ | Exercise‐based cardiac rehabilitation results in a large reduction in fatal and/or non‐fatal MI up to 12 months' follow‐up. 24 RCTs with 24 comparisons. 3 RCTs reported 0 events in both the intervention and control groups. NNTB 75 (95% CI 47 to 298) | |
| 48 per 1000 | 35 per 1000 | |||||
| Revascularisation ‐ CABG | Study population | RR 0.99 | 4473 | ⊕⊕⊕⊕ | Exercise‐based CR results in little to no difference in CABG revascularisation up to 12 months' follow‐up. 20 RCTs with 22 comparisons. 2 RCTs reported 0 events in both the intervention and control groups. | |
| 56 per 1000 | 56 per 1000 | |||||
| Revascularisation ‐ PCI | Study population | RR 0.86 | 3465 | ⊕⊕⊕⊝ | Exercise‐based CR likely results in little to no difference in risk of PCI revascularisation up to 12 months' follow‐up. 13 RCTs with 14 comparisons. 3 RCTs reported 0 events in both the intervention and control groups. | |
| 60 per 1000 | 52 per 1000 | |||||
| All‐cause hospital admissions | Study population | RR 0.58 | 2030 | ⊕⊕⊕⊝ | Exercise‐based cardiac rehabilitation likely results in a large reduction in all‐cause hospital admissions up to 12 months' follow‐up. 14 RCTs with 16 comparisons. One RCT reported 0 events in both the intervention and control group. NNTB 12 (95% CI 9 to 21) | |
| 214 per 1000 | 124 per 1000 | |||||
| Cardiovascular hospital admissions | Study population | RR 0.80 | 1087 | ⊕⊕⊝⊝ | We are uncertain about the effects of exercise‐based CR on cardiovascular hospitalisation, with a wide confidence interval including considerable benefit as well as harm. | |
| 78 per 1000 | 62 per 1000 | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| GRADE Working Group grades of evidence | ||||||
| a95% CI is wide and overlaps no effect; therefore, downgraded by one level for imprecision. | ||||||
| Measure of HRQoL | Mean (SD) outcome values at follow‐up | P value | Difference between groups | |
|
| Exercise | Control |
|
|
| Aronov 2019 | ||||
| Quality of life questionnaire developed by authors (Aronov 2002) % change of mean score at 6 months | ||||
|
| Δ% | Δ% |
|
|
|
| 30.4 | “no change” | NR |
|
| Bell 1998 | ||||
| Nottingham Health Profile at 10.5 months' follow‐up: | ||||
| Energy | 17.6 (27.1) | 18.3 (29.8) | 0.87** | Exercise = Control |
| Pain | 2.8 (8.8) | 4.82 (11.9) | < 0.05 | Exercise > Control |
| Emotional reactions | 6.4 (17.0) | 12.2 (19.9) | < 0.001 | Exercise > Control |
| Sleep | 7.5 (18.4) | 20.5 (27.8) | < 0.001 | Exercise > Control |
| Social isolation | 2.3 (10.6) | 4.0 (13.3) | 0.37* | Exercise = Control |
| Physical mobility | 8.4 (11.1) | 8.9 (14.5) | 0.82** | Exercise = Control |
| Belardinelli 2001 | ||||
| SF‐36 at 6 months' follow‐up: | ||||
| Physical functioning | 78 (19) | 55 (20) | 0.001 | Exercise > Control |
| Physical performance | 75 (13) | 65 (14) | 0.01 | Exercise > Control |
| Bodily pain | 4 (9) | 22 (10) | 0.001 | Exercise > Control |
| General health | 68 (14) | 50 (19) | 0.001 | Exercise > Control |
| Vitality | NR | NR |
|
|
| Social functioning | 66 (10) | 69 (12) | 0.14* | Exercise = Control |
| Emotional performance | NR | NR |
|
|
| Mental health | 65 (12) | 48 (15) | 0.01 | Exercise > Control |
| SF‐36 at 12 months' follow‐up: | ||||
| Physical functioning | 82 (18) | 54 (20) | 0.001 | Exercise > Control |
| Physical performance | 76 (9) | 58 (14) | 0.01 | Exercise > Control |
| Bodily pain | 4 (9) | 32 (12) | 0.001 | Exercise > Control |
| General health | 70 (14) | 50 (18) | 0.001 | Exercise > Control |
| Vitality | NR | NR |
|
|
| Social functioning | 68 (11) | 68 (12) | 1.00* | Exercise = Control |
| Emotional performance | NR | NR |
|
|
| Mental health | 70 (14) | 45 (15) | 0.001 | Exercise > Control |
| Bettencourt 2005 | ||||
| SF‐36 at 1 year follow‐up: | ||||
| Physical functioning | 70 | 62 | NS* | Exercise = Control |
| Physical performance | 66 | 57 | NS* | Exercise = Control |
| Bodily pain | 73 | 65 | NS* | Exercise = Control |
| General health | 57 | 46 | < 0.02 | Exercise > Control |
| Vitality | 62 | 47 | < 0.02 | Exercise > Control |
| Social functioning | 73 | 66 | NS* | Exercise = Control |
| Emotional performance | 65 | 58 | NS* | Exercise = Control |
| Mental health | 87 | 75 | NS* | Exercise = Control |
| Mental component | 71 | 57 | 0.02 | Exercise > Control |
| Physical component | 63 | 57 | NS* | Exercise = Control |
| Briffa 2005 | ||||
| SF‐36 at 6 months' follow‐up: | ||||
|
| Δ (95% CI) | Δ (95% CI) |
|
|
| Physical functioning | 15.9 (‐8 to 23) | 7.1 (1 to 13) | NS* | Exercise = Control |
| Physical performance | 75 (0 to 100) | 75 (0 to 100) | NS* | Exercise = Control |
| Bodily pain | 26.6 (18 to 35) | 19.2 (11 to 27) | NS* | Exercise = Control |
| General health | 0.1 (‐6 to 6) | ‐0.6 (‐5 to 4) | NS* | Exercise = Control |
| Vitality | 7.1 (1 to 13) | 3.7 (‐2 to 9) | NS* | Exercise = Control |
| Social functioning | 19.6 (10 to 29) | 14.1 (7 to 21) | NS* | Exercise = Control |
| Emotional performance | 33.3 (0 to 100) | 33.3 (33 to 100) | NS* | Exercise = Control |
| Mental health | 0.5 (‐4 to 5) | 1.4 (‐3 to 5) | NS* | Exercise = Control |
| SF‐36 at 1 year follow‐up: | ||||
|
| Δ (95% CI) | Δ (95% CI) |
|
|
| Physical functioning | 17.6 (10 to 25) | 6.8 (‐1 to 14) | 0.04 | Exercise > Control |
| Physical performance | 100 (0 to 100) | 75 (12 to 30) | NS* | Exercise = Control |
| Bodily pain | 30.2 (23 to 37) | 20.9 (‐2 to 7) | NS* | Exercise = Control |
| General health | 2.7 (‐3 to 5) | 2.2 (‐2 to 7) | NS* | Exercise = Control |
| Vitality | 11.9 (6 to 18) | 6.9 (1 to 12) | NS* | Exercise = Control |
| Social functioning | 23.6 (14 to 33) | 16.4 (9 to 23) | NS* | Exercise = Control |
| Emotional performance | 33.3 (33 to 100) | 33.3 (33 to 100) | NS* | Exercise = Control |
| Mental health | 3.6 (‐1 to 9) | 3.9 (0 to 8) | NS* | Exercise = Control |
| Bubnova 2019 | ||||
| Quality of life questionnaire developed by authors (Aronov 2002) mean (SD) score after 12 months: | ||||
| Low rehabilitation potential subgroup | ‐4.9 (4.5) | ‐7.8 (3.1) | < 0.05 | Exercise > Control |
| Average rehabilitation potential subgroup | ‐5 (3.2) | ‐7.4 (4.3) | < 0.05 | Exercise > Control |
| High rehabilitation potential subgroup | ‐4.3 (3.9) | ‐5.6 (4.3) | < 0.05 | Exercise > Control |
| Bubnova 2020 | ||||
| Quality of life questionnaire developed by authors (Aronov 2002) mean (%) score change at 12 months: | ||||
|
| Δ (%) | Δ (%) |
|
|
| BMI < 30 kg/m2 group | 42 (6%) | 10 (2%) | <0.01 | Exercise > Control |
| BMI ≥ 30 kg/m2 group | 27 (5%) | 8 (2%) | <0.001 | Exercise > Control |
| Campo 2020 | ||||
| EuroQol at 6 months' follow‐up: | ||||
|
| Median (IQR) | Median (IQR) |
|
|
| VAS (visual analogue scale) | 80 (70‐90) | 70 (50‐80) | < 0.001 | Exercise > Control |
| 5 domains | N (%) | N (%) |
|
|
| Pain/discomfort: | 103 (89) | 89 (77) | 0.03 | Exercise > Control |
| Anxiety/depression: | 92 (79) | 67 (58) | 0.001 | Exercise > Control |
| Mobility: | 104 (90) | 80 (70) | < 0.001 | Exercise > Control |
| Self‐care: | 114 (98) | 87 (76) | 0.6 | Exercise = Control |
| Usual activities: | 101 (87) | 87 (76) | 0.04 | Exercise > Control |
| EuroQol at 12 months' follow‐up: | ||||
|
| Median (IQR) | Median (IQR) |
|
|
| VAS (visual analogue scale) | 75 (70‐87) | 65 (50‐80) | < 0.001 | Exercise > Control |
| 5 domains | N (%) | N (%) |
|
|
| Pain/discomfort: | 86 (77) | 72 (65) | 0.04 | Exercise > Control |
| Anxiety/depression: | 83 (74) | 58 (53) | 0.03 | Exercise > Control |
| Mobility: | 95 (85) | 74 (67) | 0.008 | Exercise > Control |
| Self‐care: | 101 (91) | 100 (91) | 0.8 | Exercise = Control |
| Usual activities: | 99 (88) | 80 (73) | 0.004 | Exercise > Control |
| Dorje 2019 | ||||
| SF‐12 at 6 months' follow‐up: | ||||
| Physical health score | 46.8 (6.9) | 45.2 (6.5) | 0.22** | Exercise = Control |
| Mental health score | 51.5 (9.3) | 50 (8.6) | 0.28** | Exercise = Control |
| Engblom 1992 | ||||
| Nottingham Health Profile at 5 years' follow‐up: | ||||
| Energy | 18 | 25 | 0.08 | Exercise = Control |
| Pain | 12 | 18 | 0.07 | Exercise = Control |
| Emotional reactions | 14 | 21 | 0.27 | Exercise = Control |
| Sleep | 24 | 29 | 0.42 | Exercise = Control |
| Social isolation | 7 | 9 | 0.42 | Exercise = Control |
| Physical mobility | 6 | 14 | 0.005 | Exercise > Control |
| Hassan 2016 | ||||
| SF‐36 8 domains at 12 months' follow‐up | ||||
| Physical functioning | 83.5 (6.5) | 76.7 (10.6) | 0.01 | Exercise > Control |
| Role limitations physical | 62.5 (23.4) | 50.8 (20.2) | 0.04 | Exercise > Control |
| Role limitations emotional | 61.1 (21.6) | 49.9 (19.1) | 0.04 | Exercise > Control |
| Energy/fatigue | 66 (11.1) | 57.7 (11.7) | 0.01 | Exercise > Control |
| Emotional well being | 69.5 (2.6) | 61.5 (7.5) | 0.000 | Exercise > Control |
| Social functioning | 67.5 (19) | 56.3 (16.3) | 0.02 | Exercise > Control |
| Pain | 79.6 (18.4) | 67.9 (15.9) | 0.01 | Exercise > Control |
| General health | 43 (7.9) | 38.5 (8.8) | 0.04 | Exercise > Control |
| Hautala 2017 | ||||
| 15D Quality of life measure at 6 months' follow‐up: | ||||
|
| 0.915 (0.07) | 0.876 (0.084) | 0.0004* | Exercise > Control |
| 15D Quality of life measure at 12 months' follow‐up: | ||||
|
| 0.922 (0.072) | 0.886 (0.088) | < 0.0015* | Exercise > Control |
| He 2020 | ||||
| SF‐36 at 12 months: | ||||
| Physical functioning | 85 (22) | 74 (19) | < 0.01 | Exercise > Control |
| Role‐physical | 80 (21) | 77 (22) | 0.362 | Exercise = Control |
| Bodily pain | 71 (32) | 68 (30) | 0.348 | Exercise = Control |
| General health | 79 (23) | 72 (19) | < 0.01 | Exercise > Control |
| Vitality | 81 (17) | 73 (25) | < 0.01 | Exercise > Control |
| Social functioning | 75 (22) | 74 (19) | 0.902 | Exercise = Control |
| Role‐emotional | 65 (34) | 65 (33) | 0.976 | Exercise = Control |
| Mental health | 72 (23) | 71 (23) | 0.825 | Exercise = Control |
| Physical health score | 79 (29) | 73 (29) | < 0.01 | Exercise > Control |
| Mental health score | 73 (28) | 71 (27) | 0.102 | Exercise = Control |
| Heller 1993 | ||||
| QLMI at 6 months' follow‐up: | ||||
| Emotional | 5.4 (1.1) | 5.2 (1.2) | 0.04 | Exercise > Control |
| Physical | 5.4 (1.2) | 5.2 (1.3) | 0.17* | Exercise = Control |
| Social | 5.9 (1.1) | 5.8 (1.1) | 0.35* | Exercise = Control |
| Hofman‐Bang 1999 | ||||
| AP‐QLQ at 12 months' follow‐up: | ||||
| Physical activity | 4.9 | 4.3 | < 0.05 | Exercise > Control |
| Somatic symptoms | NR | NR | NS | Exercise = Control |
| Emotional distress | NR | NR | NS | Exercise = Control |
| Life satisfaction | NR | NR | NS | Exercise = Control |
| Houle 2012 | ||||
| Quality of Life Index ‐ cardiac version III at 6 months' follow‐up: | ||||
| Health and functional score | 26 (5.1) | 24.5 (5.3) | 0.048 | Exercise > Control |
| Psychological/spiritual score | 25.6 (5.8) | 25.5 (3.8) | 0.383 | Exercise = Control |
| Social and economic score | 25.7 (3.8) | 25.4 (4.7) | 0.392 | Exercise = Control |
| Family score | 28.1 (2.5) | 26.7 (4.3) | 0.048 | Exercise > Control |
| Overall | 26.2 (4.3) | 25.8 (4.1) | 0.057 | Exercise = Control |
| Quality of Life Index ‐ cardiac version III at 12 months' follow‐up: | ||||
| Health and functional score | 27.8 (2.0) | 25.3 (4.6) | 0.036 | Exercise > Control |
| Psychological/spiritual score | 27.4 (2.5) | 26.2 (4.0) | 0.336 | Exercise = Control |
| Social and economic score | 27.2 (3.0) | 25.9 (5.2) | 0.638 | Exercise = Control |
| Family score | 28 (2.6) | 26.8 (5.0) | 0.092 | Exercise = Control |
| Overall | 27.7 (2.1) | 25.7 (4.2) | 0.048 | Exercise > Control |
| Ma 2020 | ||||
| SF‐12 change at 12 months' follow‐up: | ||||
|
| Δ (SD) | Δ (SD) |
|
|
| Physical component | 13.3 (6) | 9.9 (5.9) | < 0.001 | Exercise > Control |
| Mental component | 12.4 (5.4) | 9 (6.2) | < 0.001 | Exercise > Control |
| Maddison 2014 | ||||
| EQ‐5D at 24 weeks' follow‐up: | ||||
|
| 0.86 | 0.83 | 0.23 | Exercise = Control |
| SF‐36 at 24 weeks' follow‐up: |
|
|
| |
| Physical functioning | 52.9 | 51.9 | 0.20 | Exercise = Control |
| Role physical | 52.6 | 50.8 | 0.08 | Exercise = Control |
| Bodily pain | 52.4 | 51.9 | 0.71 | Exercise = Control |
| General health | 55.3 | 53.2 | 0.03 | Exercise > Control |
| Vitality | 55.7 | 55.9 | 0.79 | Exercise = Control |
| Social Functioning | 53.3 | 52.4 | 0.42 | Exercise = Control |
| Role emotional | 51.4 | 51.6 | 0.81 | Exercise = Control |
| Mental health | 54.6 | 54.0 | 0.61 | Exercise = Control |
| Mutwalli 2012 | ||||
| SF‐36 Health status score at 6 months' follow‐up: | ||||
|
| 90.14 (4.83) | 60.55 (16.21) | 0.000 | Exercise > Control |
| Oerkild 2012 | ||||
| SF‐36 at 12 months' follow‐up: | ||||
|
| Δ (95% CI) | Δ (95% CI) |
|
|
| SF 12 PCS | ‐1.1 (‐5.3 to 3.1) | ‐1.4 (‐5.2 to 2.3) | NS* | Exercise = Control |
| SF 12 MCS | ‐1.4 (‐6.1 to 3.3) | ‐0.3 (‐4.6 to 4.0) | NS* | Exercise = Control |
| Oldridge 1991 | ||||
| QLMI at 4 months' follow‐up: | ||||
| Limitations | 54 | 54 | NS | Exercise = Control |
| Emotions | 103 | 101 | NS | Exercise = Control |
| QLMI at 8 months' follow‐up: | ||||
| Limitations | 54 | 54 | NS | Exercise = Control |
| Emotions | 103 | 103 | NS | Exercise = Control |
| QLMI at 12 months' follow‐up: | ||||
| Limitations | 54 | 55 | NS | Exercise = Control |
| Emotions | 105 | 102 | NS | Exercise = Control |
| Reid 2012 | ||||
| MacNew at 6 months' follow‐up: | ||||
| Global score | 5.8 (0.6) | 5.6 (0.8) | 0.112 | Exercise = Control |
| Emotional subscale | 5.6 (0.6) | 5.4 (0.7) | 0.038 | Exercise > Control |
| Social subscale | 6.3 (0.8) | 6.0 (1.0) | 0.162 | Exercise = Control |
| Physical subscale | 6.0 (0.8) | 5.8 (1.0) | 0.031 | Exercise > Control |
| Sandstrom 2005 | ||||
| Time Trade Off (TTO) at 12 months' follow‐up: | ||||
|
| 0.86 (0.23) | 0.85 (0.21) | NS* | Exercise = Control |
| EuroQol Part one at 12 months' follow‐up: | ||||
|
| 0.87 (0.15) | 0.86 (0.16) | NS* | Exercise = Control |
| EuroQol Part two at 12 months' follow‐up: |
|
| ||
|
| 7.6 (1.46) | 7.43 (1.46) | NS* | Exercise = Control |
| Santaularia 2017 | ||||
| EuroQol‐5D at 12 months' follow‐up: | ||||
|
| N (%) | N(%) |
|
|
| Mobility | 33 (84.6) | 33 (75) | 0.019 | Exercise > Control |
| Self‐care | 38 (97.4) | 43 (97.7) | 0.172 | Exercise = Control |
| Usual activities | 32 (82) | 31 (70.5) | 0.803 | Exercise = Control |
| Pain/discomfort | 28 (71.8) | 26 (59.1) | 0.528 | Exercise = Control |
| Anxiety/depression | 22 (56.4) | 26 (59.1) | 0.429 | Exercise = Control |
| Snoek 2020 | ||||
| SF‐36 summary scores at 6 months: | ||||
| Physical | 50.2 (7.2) | 48.3 (7.5) | 0.086* | Exercise = Control |
| Mental | 54.0 (8.4) | 52.7 (9.1) | 0.322* | Exercise = Control |
| SF‐36 summary scores at 12 months: | ||||
| Physical | 50.6 (7.2) | 49 (8.2) | 0.167* | Exercise = Control |
| Mental | 53.2 (8.8) | 52.5 (9.2) | 0.604* | Exercise = Control |
| Stahle 1999 | ||||
| Karolinska Questionnaire at 12 months' follow‐up: | ||||
| Chest pain | 0.6 (1.2) | 0.4 (1.3) | NS | Exercise = Control |
| Shortness of breath | 0.4 (1.1) | 0.2 (1.0) | NS | Exercise = Control |
| Dizziness | ‐0.1 (1.1) | 0.2 (0.9) | NS | Exercise = Control |
| Palpitation | ‐0.1 (1.0) | 0.1 (0.9) | NS | Exercise = Control |
| Cognitive ability | ‐0.1 (0.6) | 0.0 (0.7) | NS | Exercise = Control |
| Alertness | 0.0 (0.9) | 0.1 (0.8) | NS | Exercise = Control |
| Quality of sleep | 0.0 (0.5) | 0.1 (0.5) | NS | Exercise = Control |
| Physical ability | 0.2 (0.7) | 0.1 (0.4) | NS | Exercise = Control |
| Daily activity | 0.3 (0.5) | 0.1 (0.5) | NS | Exercise = Control |
| Depression | 0.1 (0.3) | 0.1 (0.2) | NS | Exercise = Control |
| Self‐perceived health | 0.5 (1.3) | 0.3 (1.0) | NS | Exercise = Control |
| "Ladder of Life" present | 1.2 (1.2) | 0.9 (1.8) | NS | Exercise = Control |
| "Ladder of Life" future | 0.8 (2.7) | 0.4 (2.3) | NS | Exercise = Control |
| Fitness | 0.6 (1.4) | 0.4 (1.0) | NS | Exercise = Control |
| Physical ability | 0.7 (1.0) | 0.4 (1.1) | NS | Exercise = Control |
| Toobert 2000 | ||||
| SF‐36 at 24 months' follow‐up: | ||||
| Physical functioning | NR | NR | NS | Exercise = Control |
| Physical performance | NR | NR | NS | Exercise = Control |
| Bodily pain | NR | NR | NS | Exercise = Control |
| General health | NR | NR | < 0.05 | Exercise > Control |
| Vitality | NR | NR | NS | Exercise = Control |
| Social functioning | NR | NR | < 0.05 | Exercise > Control |
| Emotional performance | NR | NR | NS | Exercise = Control |
| Mental health | NR | NR | NS | Exercise = Control |
| Uddin 2020 | ||||
| WHOQoL‐BREF at 12 months' follow‐up | ||||
| Overall perception of HRQoL | 4.03 (0.49) | 3.2 (0.82) | < 0.01 | Exercise > Control |
| Overall perception of health | 4.06 (0.4) | 3.17 (0.38) | < 0.01 | Exercise > Control |
| Physical domain | 26.9 (2.88) | 21.17 (3.35) | < 0.01 | Exercise > Control |
| Psychological domain | 23.42 (2.84) | 17.87 (3.19) | < 0.01 | Exercise > Control |
| Social relationship domain | 11.83 (1.5) | 10.75 (0.89) | < 0.01 | Exercise > Control |
| Environmental domain | 28.8 (4.24) | 21.77 (5.31) | 0.03 | Exercise > Control |
| Wang 2012 | ||||
| SF‐36 at 6 months' follow‐up: | ||||
| Physical functioning | 80.8 (13.7) | 73.2 (13.0) | < 0.001 | Exercise > Control |
| Physical performance | 68.2 (17.3) | 56.2 (46.8) | 0.015 | Exercise > Control |
| Bodily pain | 68.2 (17.3) | 63.5 (14.6) | 0.012 | Exercise > Control |
| General health | 57.4 (20.3) | 49.0 (16.2) | 0.017 | Exercise > Control |
| Vitality | 66.3 (17.3) | 56.4 (21.7) | 0.002 | Exercise > Control |
| Social functioning | 71.3 (21.4) | 65.8 (18.0) | 0.031 | Exercise > Control |
| Emotional performance | 80.8 (37.9) | 75.9 (39.7) | 0.12 | Exercise = Control |
| Mental health | 73.5 (17.1) | 65.4 (20.7) | 0.011 | Exercise > Control |
| MIDAS at 6 months' follow‐up: | ||||
| Physical Activity | 37.7 (11.2) | 42.6 (12.3) | < 0.001 | Exercise > Control |
| Insecurity | 28.7 (9.7) | 33.4 (13.8) | < 0.001 | Exercise > Control |
| Emotional reaction | 30.4 (12.8) | 34.8 (14.4) | 0.008 | Exercise > Control |
| Dependency | 27.6 (9.4) | 31.8 (16.6) | 0.001 | Exercise > Control |
| Diet | 36.8 (15.4) | 43.6 (20.7) | 0.40 | Exercise = Control |
| Concerns over meds | 29.4 (12.6) | 37.7 (18.0) | <0.001 | Exercise > Control |
| Side Effects | 28.2 (11.1) | 30.8 (14.3) | 0.30 | Exercise > Control |
| West 2012 | ||||
| SF‐36 at 12 months' follow‐up: | ||||
| Physical function | 65 (29) | 64 (30) | NS* | Exercise = Control |
| Role physical | 69 (31) | 67 (33) | NS* | Exercise = Control |
| Role emotional | 85 (23) | 85 (25) | NS* | Exercise = Control |
| Social function | 81 (28) | 79 (29) | NS* | Exercise = Control |
| Mental health | 76 (13) | 76 (13) | NS* | Exercise = Control |
| Energy /vitality | 65 (24) | 65 (24) | NS* | Exercise = Control |
| Pain | 69 (28) | 68 (29) | NS* | Exercise = Control |
| Health Perception | 58 (25) | 57 (25) | NS* | Exercise = Control |
| Yu 2003 | ||||
| SF‐36 at 8 months' follow‐up: | ||||
| Physical functioning | 88 (12) | 82 (17) | 0.03* | Exercise > Control |
| Physical performance | 75 (33) | 66 (35) | 0.18* | Exercise = Control |
| Bodily pain | 80 (25) | 80 (25) | 1.00* | Exercise = Control |
| General health | 64 (26) | 60 (28) | 0.45* | Exercise = Control |
| Vitality | 79 (18) | 65 (17) | 0.0001 | Exercise > Control |
| Social functioning | 89 (27) | 82 (28) | 0.15 | Exercise = Control |
| Emotional performance | 93 (18) | 83 (35) | 0.05 | Exercise = Control |
| Mental health | 84 (16) | 80 (15) | 0.2 | Exercise = Control |
| SF‐36 at 24 months' follow‐up: | ||||
| Physical functioning | 88 (13) | 87 (9) | 0.67* | Exercise = Control |
| Physical performance | 80 (32) | 79 (30) | 0.87* | Exercise = Control |
| Bodily pain | 81 (21) | 85 (20) | 0.33* | Exercise = Control |
| General health | 64 (20) | 61 (18) | 0.43* | Exercise = Control |
| Vitality | 73 (21) | 73 (17) | 1.00* | Exercise = Control |
| Social functioning | 79 (30) | 90 (18) | 0.04* | Exercise > Control |
| Emotional performance | 89 (25) | 93 (25) | 0.42* | Exercise = Control |
| Mental health | 85 (14) | 85 (12) | 1.00* | Exercise = Control |
| Zwisler 2008 | ||||
| SF‐36 at 12 months' follow‐up: | ||||
| Physical Component Score | 45.2 (9.8) | 46.4 (9.8) | 0.39* | Exercise = Control |
| Mental Component Score | 50.6 (10.8) | 48.4 (11.5) | 0.16* | Exercise = Control |
| AP‐QLQ: Angina Pectoris‐Quality of Life questionnaire | ||||
| Author/ year | Briffa 2005 | Hambrecht 2004 | Hautala 2017 | Kovoor 2006/Hall 2002 | Maddison 2014 | Marchionni 2003 | Oldridge 1991/93 | Yu 2004 |
| Follow‐up (months) | 12 | 12 | 12 | 12 | 6 | 14 | 12 | 24 |
| Year of costs (currency) | 1998 (Australian dollars ‐ AUD) | NR (US dollars ‐ USD) | NR (euros ‐ EUR) | 1999 (Australian dollars ‐ AUD) | NR (euros ‐ EUR) | 2000 (US dollars ‐ USD) | 1991 (US dollars ‐ USD) | 2003 (US dollars ‐ USD) |
| Cost of rehabilitation | ||||||||
| Mean cost/patient | AUD 694 | NR | EUR 299 | AUD 394 | EUR 127 | USD 5246 | USD 670 | NR |
| Costs considered | Details of costed elements not provided | NR | Estimated according to the average monthly fees in Finnish gyms where individual guidance in exercise training is led by a health care professional | staff, assessments, counselling, education, patient travel | NR | NR | space, equipment, staff, literature resources, operating costs, parking, patients costs | NR |
| Total healthcare costs | ||||||||
| Rehabilitation mean cost/patient | AUD 4937 | USD 3708 ± 156 | EUR 1944 | NR | NR | USD 17,272 | NR | USD 15,292 |
| Usual care mean cost/patient | AUD 4541 | USD 6086 ± 370 | EUR 3027 | NR | NR | USD 12,433 | NR | USD 15,707 |
| Absolute difference in mean cost/patient* | AUD 395 | USD ‐2378 | EUR ‐1083 | NR | NR | USD 4839 | USD 480 | USD ‐415 |
| P value for cost difference | 0.74 | P < 0.001 | NR | P > 0.05 (see below) | NR | NR | NR | P > 0.05 |
| Additional healthcare costs considered | Hospitalisations, pharmaceuticals, tests, consultations, rehabilitation, patient expenses, ambulance | Rehospitalisations, revascularisation, cycle ergometers, training facilities, and supervising staff | Primary health care costs, secondary health care costs, occupational health care service costs | Phone calls (P = 0.10); hospital admissions (P = 0.11); gated heart pool scan (P = 0.50); exercise stress test (P = 0.72); other diagnostics (P = 0.37); visits to general practitioner (P = 0.61), specialist doctor (P = 0.35), or health‐care professional (P = 0.31) | NR | NR | Service utilisation, physician costs, emergency costs, in‐patient days, allied health, other rehabilitation visits | Hospitalisations; revascularisations; private clinic visit; cardiac clinic visits; public non‐cardiac visits; casualty visits; drugs |
| Cost‐effectiveness | ||||||||
| Rehabilitation mean health care benefits | Utility‐based quality of life – | NR | Average change in 15D utility: 0.013 | NR | NR | NR | NR | NR |
| Usual care mean health care benefit | Utility 0.010 (95% CI ‐0.001 to 0.022) | NR | Average change in 15D utility: ‐0.012 | NR | NR | NR | NR | NR |
| Incremental mean health care benefit | Utility 0.013 (95% CI, NR) P = 0.38; +0.009 QALYs | NR | 0.045 QALYs (0.023‐0.077) | NR | NR | NR | 0.052 QALYs (95% CI, 0.007 to 0.1) | 0.06 QALYs |
| Incremental cost effectiveness ratio/patient | AUD +42,535 per QALY. Extensive sensitivity analyses reported. | NR | EUR ‐24,511 per QALY | NR | EUR +15,247 per QALY | NR | USD +9200 per QALY | USD ‐650 per QALY |
| NR: not reported * The currency for Hambrecht 2004 is not reported, but healthcare costs are reported within the paper with $ | ||||||||
| Explanatory variable (n trials) | Exp (slope)* | 95% confidence interval, | Proportion of variance explained (adjusted R2) | Interpretation |
| Case mix (% MI patients) (n = 46) | RR = 1.00 | 1.00 to 1.00, P = 0.15 | 56.1% | No evidence that risk ratio is associated with case mix |
| Dose of exercise (number of weeks of exercise training x average number of sessions/week x average min/session) (n = 33) | RR = 1.00 | 1.00 to 1.00, P = 0.11 |
100% | No evidence that risk ratio is associated with type of CR |
| Duration of follow‐up (months) (n = 47) | RR = 1.00 | 1.00 to 1.00, P = 0.07 | 100% | No evidence that risk ratio is associated with length of follow‐up |
| Type of CR (exercise only vs comprehensive CR) (n = 47) | RR = 1.04 | 0.84 to 1.31, P = 0.70 | ‐27.1% | No evidence that risk ratio is associated with type of CR |
| Year of publication (pre‐1995 vs post‐1995) (n = 47) | RR = 0.84 | 0.70 to 0.99, P = 0.04 | 100% | No evidence that risk ratio is associated with publication year |
| CR setting (n = 47) | RR = 0.95 | 0.82 to 1.24, P = 0.95 | ‐11.3% | No evidence that risk ratio is associated with type of CR |
| Risk of bias (low risk in ≤ 3 items vs > 3 items) (n = 47) | RR = 1.02 | 0.94 to 1.09, P = 0.67 | ‐68.55% | No evidence that risk ratio is associated with risk of bias |
| Study location (continent ‐ Europe, North America, Australia/Asia or Other) (n = 47) | RR = 1.01 | 0.86 to 1.19, P = 0.93 | ‐41.24% | No evidence that risk ratio is associated with study location |
| Low‐ and middle‐income country (LMIC) vs high‐income country (n = 47) | RR = 1.02 | 0.70 to 1.48, P = 0.93 | ‐45.10% | No evidence that risk ratio is associated with LMIC |
| Sample size (≤ 150 vs > 150) (n = 47) | RR = 1.19 | 0.73 to 1.93, P = 0.47 | 16.07% | No evidence that risk ratio is associated with study sample size |
| Explanatory variable (n trials) | Exp (slope)* | 95% confidence interval, | Proportion of variance explained (adjusted R2) | Interpretation |
| Case mix (% MI patients) (n = 27) | RR = 1.00 | 0.99 to 1.01, P = 0.76 | ‐8.74% | No evidence that risk ratio is associated with case mix |
| Dose of exercise (number of weeks of exercise training x average number of sessions/week x average min/session) (n = 22) | RR = 1.00 | 1.00 to 1.00, P = 0.62 | 0% | No evidence that risk ratio is associated with dose of exercise |
| Duration of follow‐up (months) (n = 28) | RR = 0.99 | 0.99 to 1.00, P = 0.05 | 90.36% | No evidence that risk ratio is associated with length of follow‐up |
| Type of CR (exercise only vs comprehensive CR) (n = 28) | RR = 0.83 | 0.62 to 1.10, P = 0.18 | 75.69% | No evidence that risk ratio is associated with type of CR |
| Year of publication (pre‐1995 vs post‐1995) (n = 28) | RR = 1.37 | 0.89 to 2.13, P = 0.15 | 63.31% | No evidence that risk ratio is associated with publication year |
| Setting (centre vs home) (n = 28) | RR = 1.05 | 0.88 to 1.24, P = 0.61 | ‐29.66% | No evidence that risk ratio is associated with setting of CR |
| Risk of bias (low risk in ≤ 3 items vs > 3 items) (n = 28) | RR = 0.90 | 0.73 to 1.11, P = 0.30 | 85.73% | No evidence that risk ratio is associated with risk of bias |
| Study location (continent ‐ Europe, North America, Australia/Asia or Other) (n = 28) | RR = 1.02 | 0.75 to 1.39, P = 0.89 | ‐41.75% | No evidence that risk ratio is associated with study location |
| Low‐ and middle‐income country (LMIC) vs high‐income country (n = 28) | RR = 0.69 | 0.22 to 2.19, P = 0.52 | 9.36% | No evidence that risk ratio is associated with LMIC |
| Sample size (≤ 150 vs > 150) (n = 28) | RR = 1.28 | 0.69 to 2.37, P = 0.42 | 28.43% | No evidence that risk ratio is associated with study sample size |
| Explanatory variable (n trials) | Exp (slope)* | 95% confidence interval, | Proportion of variance explained (adjusted R2) | Interpretation |
| Case mix (% MI patients) (n = 41) | RR = 1.00 | 0.99 to 1.01, P = 0.93 | ‐4.57% | No evidence that risk ratio is associated with case mix |
| Dose of exercise (number of weeks of exercise training x average number of sessions/week x average min/session) (n = 33) | RR = 1.00 | 1.00 to 1.00, P = 0.68 | 0% | No evidence that risk ratio is associated with dose of exercise |
| Duration of follow‐up (months) (n = 41) | RR = 1.00 | 0.99 to 1.01, P = 0.97 | ‐12.45% | No evidence that risk ratio is associated with length of follow‐up |
| Type of CR (exercise only vs comprehensive CR) (n = 41) | RR = 0.85 | 0.58 to 1.25, P = 0.39 | 9.68% | No evidence that risk ratio is associated with type of CR |
| Year of publication (pre‐1995 vs post‐1995) (n = 41) | RR = 1.36 | 0.94 to 1.97, P = 0.11 | 25.40% | No evidence that risk ratio is associated with publication year |
| Setting (centre vs home) (n = 39) | RR = 0.80 | 0.67 to 0.95, P = 0.01 | 67.62% | No evidence that risk ratio is associated with setting of CR |
| Risk of bias (low risk in ≤ 3 items vs > 3 items) (n = 41) | RR=1.39 | 0.85 to 2.26, P = 0.18 | ‐16.70% | No evidence that risk ratio is associated with risk of bias |
| Study location (continent ‐ Europe, North America, Australia/Asia or Other) (n = 41) | RR = 0.71 | 0.49 to 1.05, P = 0.09 | 12.94% | No evidence that risk ratio is associated with study location |
| Low‐ and middle‐income country (LMIC) vs high income country (n = 41) | RR = 0.65 | 0.33 to 1.61, P = 0.20 | 0.86% | No evidence that risk ratio is associated with LMIC |
| Sample size (≤ 150 vs > 150) (n = 41) | RR = 1.69 | 1.05 to 2.72, P = 0.03 | 54.95% | No evidence that risk ratio is associated with study sample size |
| Explanatory variable (n trials) | Exp (slope)* | 95% confidence interval, | Proportion of variance explained (adjusted R2) | Interpretation |
| Case mix (% MI patients) (n = 31) | RR = 1.01 | 1.00 to 1.02, P = 0.05 | 0% | No evidence that risk ratio is associated with case mix |
| Dose of exercise (number of weeks of exercise training x average number of sessions/week x average min/session) (n = 25) | RR = 1.00 | 1.00 to 1.00, P = 0.78 | 0% | No evidence that risk ratio is associated with dose of exercise |
| Duration of follow‐up (months) (n = 31) | RR = 1.00 | 0.99 to 1.01, P = 0.75 | 0% | No evidence that risk ratio is associated with length of follow‐up |
| Type of CR (exercise only vs comprehensive CR) (n = 31) | RR = 1.04 | 0.67 to 1.61, P = 0.86 | 0% | No evidence that risk ratio is associated with type of CR |
| Year of publication (pre‐1995 vs post‐1995) (n = 31) | RR = 0.88 | 0.56 to 1.41, P = 0.59 | 0% | No evidence that risk ratio is associated with publication year |
| Setting (centre vs home) (n = 31) | RR = 1.07 | 0.87 to 1.33, P = 0.51 | 0% | No evidence that risk ratio is associated with setting of CR |
| Risk of bias (low risk in ≤ 3 items vs > 3 items) (n = 31) | RR = 0.94 | 0.64 to 1.38, P = 0.73 | 0% | No evidence that risk ratio is associated with risk of bias |
| Study location (continent ‐ Europe, North America, Australia/Asia or Other) (n = 31) | RR = 1.19 | 0.83 to 1.71, P = 0.34 | 0% | No evidence that risk ratio is associated with study location |
| Low‐ and middle‐income country (LMIC) vs high income country (n = 31) | RR = 0.51 | 0.08 to 3.18, P = 0.46 | 0% | No evidence that risk ratio is associated with LMIC |
| Sample size (≤ 150 vs > 150) (n = 31) | RR = 1.31 | 0.82 to 2.09, P = 0.25 | 0% | No evidence that risk ratio is associated with study sample size |
| Explanatory variable (n trials) | Exp (slope)* | 95% confidence interval, | Proportion of variance explained (adjusted R2) | Interpretation |
| Case mix (% MI patients) (n = 18) | RR = 1.00 | 1.00 to 1.01, P = 0.50 | 0% | No evidence that risk ratio is associated with case mix |
| Dose of exercise (number of weeks of exercise training x average number of sessions/week x average min/session) (n = 16) | RR = 1.00 | 1.00 to 1.00, P = 0.50 | 0% | No evidence that risk ratio is associated with dose of exercise |
| Duration of follow‐up (months) (n = 18) | RR = 1.00 | 0.99 to 1.01, P = 0.82 | 0% | No evidence that risk ratio is associated with length of follow‐up |
| Type of CR (exercise only vs comprehensive CR) (n = 18) | RR = 0.78 | 0.38 to 1.59, P = 0.47 | 0% | No evidence that risk ratio is associated with type of CR |
| Year of publication (pre‐1995 vs post‐1995) (n = 18) | RR = 0.95 | 0.46 to 1.95, P = 0.87 | 0% | No evidence that risk ratio is associated with publication year |
| Setting (centre vs home) (n = 18) | RR = 0.91 | 0.72 to 1.15, P = 0.41 | 0% | No evidence that risk ratio is associated with setting of CR |
| Risk of bias (low risk in ≤ 3 items vs > 3 items) (n = 18) | RR = 1.09 | 0.72 to 1.66, P = 0.67 | 0% | No evidence that risk ratio is associated with risk of bias |
| Study location (continent ‐ Europe, North America, Australia/Asia or Other) (n = 18) | RR = 0.81 | 0.53 to 1.23, P = 0.30 | 0% | No evidence that risk ratio is associated with study location |
| Low‐ and middle‐income country (LMIC) vs high income country (n = 18) | RR = 0.29 | 0.05 to 1.63, P = 0.15 | 0% | No evidence that risk ratio is associated with LMIC |
| Sample size (≤ 150 vs > 150) (n = 18) | RR = 1.19 | 0.70 to 2.01, P = 0.49 | 0% | No evidence that risk ratio is associated with study sample size |
| Explanatory variable (n trials) | Exp (slope)* | 95% confidence interval, | Proportion of variance explained (adjusted R2) | Interpretation |
| Case mix (% MI patients) (n = 23) | RR = 1.00 | 1.00 to 1.01, P = 0.71 | ‐20.91% | No evidence that risk ratio is associated with case mix |
| Dose of exercise (number of weeks of exercise training x average number of sessions/week x average min/session) (n = 19) | RR = 1.00 | 1.00 to 1.00, P = 0.44 | ‐69.78% | No evidence that risk ratio is associated with dose of exercise |
| Duration of follow‐up (months) (n = 23) | RR = 1.01 | 1.00 to 1.01, P = 0.07 | 56.52% | No evidence that risk ratio is associated with length of follow‐up |
| Type of CR (exercise only vs comprehensive CR) (n = 23) | RR = 0.93 | 0.65 to 1.33, P = 0.70 | ‐50.20% | No evidence that risk ratio is associated with type of CR |
| Year of publication (pre‐1995 vs post‐1995) (n = 23) | RR = 1.12 | 0.80 to 1.57, P = 0.48 | ‐32.69% | No evidence that risk ratio is associated with publication year |
| Setting (centre vs home) (n = 23) | RR = 0.94 | 0.83 to 1.06, P = 0.28 | ‐36.70% | No evidence that risk ratio is associated with setting of CR |
| Risk of bias (low risk in ≤ 3 items vs > 3 items) (n = 23) | RR = 1.00 | 0.71 to 1.40, P = 0.99 | ‐44.14% | No evidence that risk ratio is associated with risk of bias |
| Study location (continent ‐ Europe, North America, Australia/Asia or Other) (n = 23) | RR = 0.86 | 0.69 to 1.08, P = 0.18 | ‐137.18% | No evidence that risk ratio is associated with study location |
| Low‐ and middle‐income country (LMIC) vs high income country (n = 23) | RR = 1.06 | 0.72 to 1.55, P = 0.76 | ‐49.12% | No evidence that risk ratio is associated with LMIC |
| Sample size (≤ 150 vs > 150) (n = 19) | RR = 1.45 | 1.08 to 1.96, P = 0.02 | 100% | No evidence that risk ratio is associated with study sample size |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1.1 All‐cause mortality Show forest plot | 47 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.1.1 Follow‐up of 6 to 12 months | 25 | 8823 | Risk Ratio (M‐H, Random, 95% CI) | 0.87 [0.73, 1.04] |
| 1.1.2 Follow‐up of > 12 to 36 months | 16 | 11073 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.80, 1.02] |
| 1.1.3 Follow‐up longer than 3 years | 11 | 3828 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.75, 1.10] |
| 1.2 Cardiovascular mortality Show forest plot | 26 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.2.1 Follow‐up of 6 to 12 months | 15 | 5360 | Risk Ratio (M‐H, Random, 95% CI) | 0.88 [0.68, 1.14] |
| 1.2.2 Follow‐up of > 12 months to 36 months | 5 | 3614 | Risk Ratio (M‐H, Random, 95% CI) | 0.77 [0.63, 0.93] |
| 1.2.3 Follow‐up of longer than 3 years | 8 | 1392 | Risk Ratio (M‐H, Random, 95% CI) | 0.58 [0.43, 0.78] |
| 1.3 Fatal and/or nonfatal MI Show forest plot | 39 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.3.1 Follow‐up of 6 to 12 months | 22 | 7423 | Risk Ratio (M‐H, Random, 95% CI) | 0.72 [0.55, 0.93] |
| 1.3.2 Follow‐up of > 12 to 36 months | 12 | 9565 | Risk Ratio (M‐H, Random, 95% CI) | 1.07 [0.91, 1.27] |
| 1.3.3 Follow‐up of longer than 3 years | 10 | 1560 | Risk Ratio (M‐H, Random, 95% CI) | 0.67 [0.50, 0.90] |
| 1.4 CABG Show forest plot | 29 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.4.1 Follow‐up of 6 to 12 months | 20 | 4473 | Risk Ratio (M‐H, Random, 95% CI) | 0.99 [0.78, 1.27] |
| 1.4.2 Follow‐up of > 12 to 36 months | 9 | 2826 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.77, 1.23] |
| 1.4.3 Follow‐up of longer than 3 years | 4 | 675 | Risk Ratio (M‐H, Random, 95% CI) | 0.66 [0.34, 1.27] |
| 1.5 PCI Show forest plot | 18 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.5.1 Follow‐up of 6 to 12 months | 13 | 3465 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.63, 1.19] |
| 1.5.2 Follow‐up of > 12 to 36 months | 6 | 1983 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.69, 1.35] |
| 1.5.3 Follow‐up of longer than 3 years | 3 | 567 | Risk Ratio (M‐H, Random, 95% CI) | 0.76 [0.48, 1.20] |
| 1.6 All‐cause hospital admissions Show forest plot | 22 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.6.1 Follow‐up of 6 to 12 months | 14 | 2030 | Risk Ratio (M‐H, Random, 95% CI) | 0.58 [0.43, 0.77] |
| 1.6.2 Follow‐up of > 12 to 36 months | 9 | 5995 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.82, 1.03] |
| 1.7 Cardiovascular hospital admissions Show forest plot | 8 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.7.1 Follow‐up of 6 to 12 months | 6 | 1087 | Risk Ratio (M‐H, Random, 95% CI) | 0.80 [0.41, 1.59] |
| 1.7.2 Follow up of >12 to 36 months | 3 | 943 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.76, 1.12] |
| 1.8 HRQoL SF‐36 summary scores at 6 to 12 months follow up Show forest plot | 6 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.8.1 Physical component score | 6 | 1741 | Mean Difference (IV, Random, 95% CI) | 1.70 [‐0.08, 3.47] |
| 1.8.2 Mental component score | 6 | 1741 | Mean Difference (IV, Random, 95% CI) | 2.14 [1.07, 3.22] |
| 1.9 HRQoL SF‐36 8 domains at 6 to 12 months follow up Show forest plot | 8 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.9.1 Physical functioning | 8 | 2756 | Mean Difference (IV, Random, 95% CI) | 8.47 [3.69, 13.24] |
| 1.9.2 Physical performance | 8 | 2756 | Mean Difference (IV, Random, 95% CI) | 8.08 [2.89, 13.27] |
| 1.9.3 Bodily pain | 8 | 2756 | Mean Difference (IV, Random, 95% CI) | ‐0.06 [‐8.97, 8.84] |
| 1.9.4 General health | 8 | 2756 | Mean Difference (IV, Random, 95% CI) | 5.66 [2.08, 9.25] |
| 1.9.5 Vitality | 7 | 2638 | Mean Difference (IV, Random, 95% CI) | 5.78 [1.89, 9.67] |
| 1.9.6 Social functioning | 8 | 2756 | Mean Difference (IV, Random, 95% CI) | 1.98 [0.26, 3.70] |
| 1.9.7 Emotional performance | 7 | 2638 | Mean Difference (IV, Random, 95% CI) | 0.69 [‐1.33, 2.71] |
| 1.9.8 Mental health | 8 | 2756 | Mean Difference (IV, Random, 95% CI) | 5.60 [1.21, 9.98] |
| 1.10 HRQoL EQ‐5D at 6 to 12 months follow up Show forest plot | 3 | 476 | Mean Difference (IV, Random, 95% CI) | 0.05 [‐0.01, 0.10] |