Zahvati i pokreti za smanjenje bolova u vratu u usporedbi pristupa bez liječenja i drugim oblicima liječenja
Information
- DOI:
- https://doi.org/10.1002/14651858.CD004249.pub4Copy DOI

- Database:
-
- Cochrane Database of Systematic Reviews
- Version published:
-
- 23 September 2015see what's new
- Type:
-
- Intervention
- Stage:
-
- Review
- Cochrane Editorial Group:
-
Cochrane Back and Neck Group
- Copyright:
-
- Copyright © 2015 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Article metrics
Altmetric:
Cited by:
Authors
Contributions of authors
This is one review of a series conducted by the Cervical Overview Group (COG): Gross AR, Goldsmith CH, Graham N, Santaguida PL, Burnie SJ, Miller J, Peloso P, Kay T, Kroeling P, Trinh K, Langevin P, Santaguida PL, Patel K, Haines T, Haraldsson B, Radylovick Z, Forget M, Szeto G, LeBlanc F, Ezzo J, Morien A, Rice M, Perry L, Fraser M, Cameron I, Wang Z, Lilge L, White R, Bronfort G, Hoving J, Jelley J, Empey B, Lalonde P.
Primary review authors ‐ Gross AR, Langevin P, Burnie SJ, Bédard‐Brochu MS, Empey B, Dugas E, Faber‐Dobrescu M, Andres C, Goldsmith CH, Graham N, Bronfort G, Hoving J, LeBlanc F.
Student members of this review: Bédard‐Brochu MS, Empey B, Dugas E, Faber‐Dobrescu M, Andres C, Boudreau M.
Statistician ‐ Goldsmith C.
Methodological quality assessment ‐ Burnie SJ, Forget M, Goldsmith CH, LeBlanc F, Empey B, Szeto G, Jelley G, Lalonde P.
Study identification and selection ‐ Graham N, Brunarski D, Haines T, Gross AR.
Research librarian ‐ Rice M.
Data abstraction, synthesis, manuscript preparation, public responsibility, grants, administration ‐ Gross AR, Langevin P, Bédard‐Brochu MS, Empey B, Dugas E, Faber‐Dobrescu M, Andres C, Boudreau M.
Final synthesis ‐ Gross AR, Langevine P, Burnie SJ, Bronfort G, Hoving J, Bédard‐Brochu MS, Empey B, Dugas E, Faber‐Dobrescu M, Andres C, Boudreau M.
Grant writing ‐ Santaguida PL, Gross AR, Graham N.
Conference presentation ‐ Empey B, Gross AR, Burnie SJ, Graham N.
Sources of support
Internal sources
-
McMaster University, Department of Clinical Epidemiology and Biostatistics; School of Rehabilitation Sciences; Occupational Health Program, Canada.
-
Centric Health, Lifemark Physiotherapy, Canada.
-
Vrije Universiteit Amsterdam, Academic Medical Centre, Coronel Institute of Occupational Health, Netherlands.
-
Sunnybrook & Women's College Health Sciences Centre, Physiotherapy Department, Canada.
-
LAMP Occupational Health Program, Canada.
-
Northwestern Health Sciences University, Minnesota, USA.
-
Royal Canadian Chiropractic College, Canada.
External sources
-
Problem‐based Research Award; Sunnybrook and Women's College Health Sciences Foundation, Canada.
-
Consortial Center for Chiropractic Research ‐ National Institutes of Health, Bethesda, MD, USA.
-
Hamilton Hospital Association, Canada.
-
University of Saskatchewan, Clinical Teaching and Research Award, Canada.
-
Hamilton Health Sciences Corporation, Chedoke‐McMaster Foundation, Canada.
Declarations of interest
Two of our review authors are authors of included studies. Although Jan Hoving and Gert Bronfort were review authors, they were not involved in decisions about study inclusion, risk of bias assessment or extraction of data from their studies.
Acknowledgements
Funding was provided by the LIfeMark Centric Industry partnership grant. We are indebted to the many authors of primary studies for their support in retrieving original research. We thank our volunteers, translators, students, the Cochrane Back Review Group editors and Lisa Carlesso and Colleen McPhee for granting early access to their research. We would like to thank the members of the Cervical Overview Group for assistance and guidance provided during all phases of this update.
Version history
| Published | Title | Stage | Authors | Version |
| 2015 Sep 23 | Manipulation and mobilisation for neck pain contrasted against an inactive control or another active treatment | Review | Anita Gross, Pierre Langevin, Stephen J Burnie, Marie‐Sophie Bédard‐Brochu, Brian Empey, Estelle Dugas, Michael Faber‐Dobrescu, Cristy Andres, Nadine Graham, Charles H Goldsmith, Gert Brønfort, Jan L Hoving, Francis LeBlanc | |
| 2010 Jan 20 | Manipulation or Mobilisation for Neck Pain | Review | Anita Gross, Jordan Miller, Jonathan D'Sylva, Stephen J Burnie, Charles H Goldsmith, Nadine Graham, Ted Haines, Gert Brønfort, Jan L Hoving | |
| 2004 Jan 26 | Manipulation and mobilisation for mechanical neck disorders | Review | Anita Gross, Jan L Hoving, Ted Haines, Charles H Goldsmith, Theresa M Kay, Peter Aker, Gert Brønfort, Cervical Overview Group | |
| 2002 Jan 03 | Manipulation and Mobilisation for Mechanical Neck Disorders | Protocol | Anita R Gross, Gert Bronfort, Jan L Hoving, Charlie H Goldsmith, Ted A Haines, Peter Aker, G roup Cervical Overview | |
Differences between protocol and review
Our protocol was published in 2002. We have noted some differences from our original protocol.
-
The term for type of participant as 'neck disorder with headache' was changed to 'cervicogenic headache'. Diagnostic criteria remain the same. Mechanical neck disorder was changed to neck pain, but the criteria remained the same.
-
Interventions were subgrouped by region of the body manipulated. Emerging evidence has revealed differences per region. This information was obtained by sensitivity analysis.
-
We added a grey literature search: clinicaltrials.gov.
-
A research librarian was hired and developed sensitive and specific search strategies.
-
Primary outcome categories remain the same, but specific outcomes have evolved over the years.
-
The body of evidence was assessed by the Strength of Evidence assessment, which has been changed to the GRADE system.
-
Original methods used the Jadad Scale. The risk of bias system is now used, as recommended by the Cochrane Handbook for Systematic Reviews of Interventions.
-
The post hoc power analysis for meaningful SMD was discontinued.
Keywords
MeSH
Medical Subject Headings (MeSH) Keywords
Medical Subject Headings Check Words
Humans;
PICOs
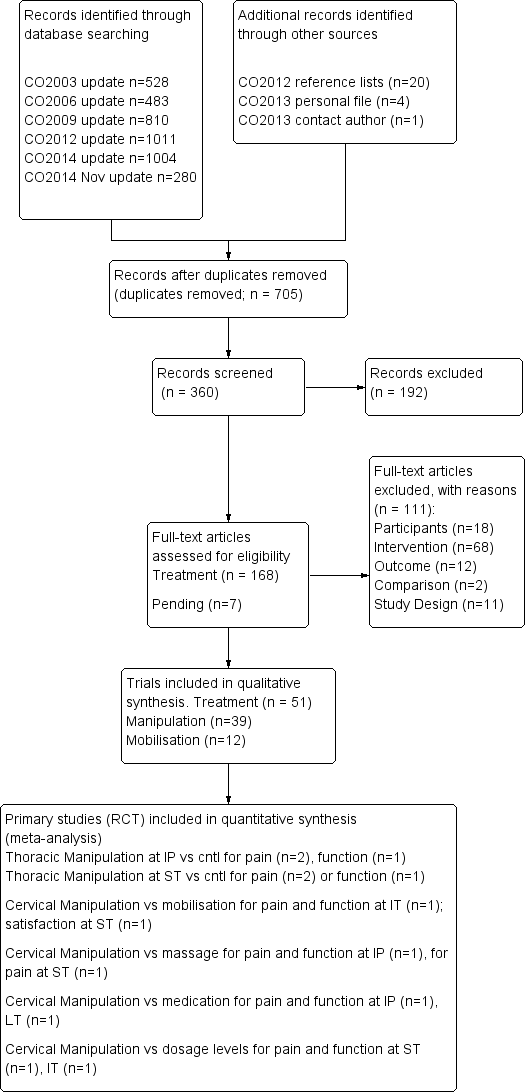
PRISMA diagram for manipulation and mobilisation.

Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
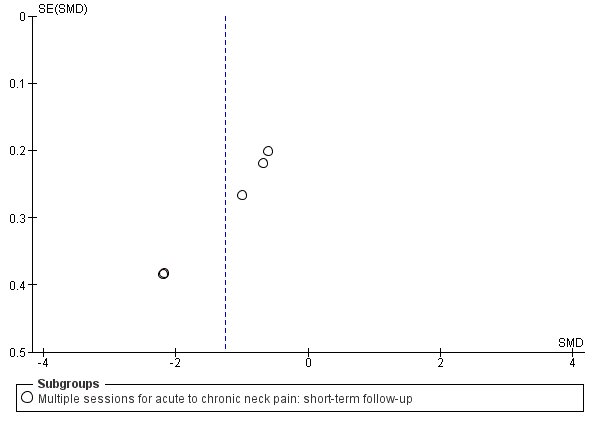
Funnel plot of comparison: manipulation vs control, outcome: FUNNEL PLOT for PAIN: thoracic manipulation vs same treatment in both arms.

Forest plot of comparison: manipulation vs another treatment, outcome: PAIN: cervical manipulation vs medicine.

Forest plot of comparison: manipulation vs another treatment, outcome: PAIN: cervical manipulation vs mobilisation at intermediate‐term follow‐up.

Comparison 1 Manipulation versus placebo, Outcome 1 PAIN: cervical manipulation vs placebo.

Comparison 1 Manipulation versus placebo, Outcome 2 PAIN: thoracic manipulation vs placebo.
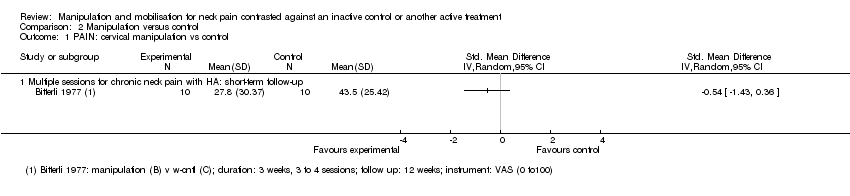
Comparison 2 Manipulation versus control, Outcome 1 PAIN: cervical manipulation vs control.

Comparison 2 Manipulation versus control, Outcome 2 PAIN: cervical manipulation plus treatment vs same treatment in both arms.

Comparison 2 Manipulation versus control, Outcome 3 PAIN: cervical manipulation vs same treatment in both arms.

Comparison 2 Manipulation versus control, Outcome 4 PAIN: thoracic manipulation vs control.

Comparison 2 Manipulation versus control, Outcome 5 PAIN: thoracic manipulation vs same treatment in both arms.
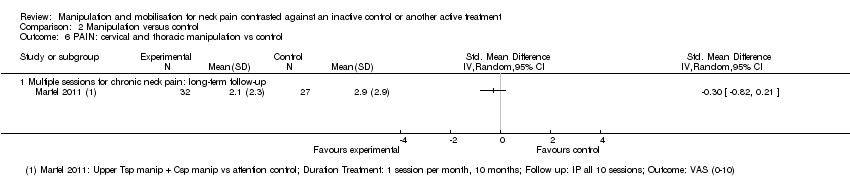
Comparison 2 Manipulation versus control, Outcome 6 PAIN: cervical and thoracic manipulation vs control.

Comparison 2 Manipulation versus control, Outcome 7 FUNCTION: thoracic manipulation vs same treatment in both arms.
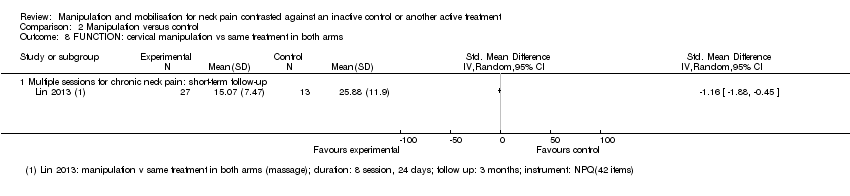
Comparison 2 Manipulation versus control, Outcome 8 FUNCTION: cervical manipulation vs same treatment in both arms.

Comparison 2 Manipulation versus control, Outcome 9 FUNCTION: cervical and thoracic manipulation vs control.

Comparison 2 Manipulation versus control, Outcome 10 QUALITY OF LIFE: thoracic manipulation vs control.

Comparison 2 Manipulation versus control, Outcome 11 FUNNEL PLOT for pain: thoracic manipulation vs same treatment in both arms.
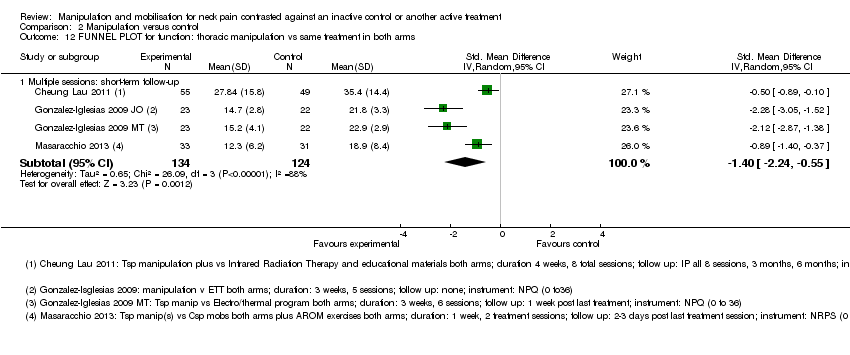
Comparison 2 Manipulation versus control, Outcome 12 FUNNEL PLOT for function: thoracic manipulation vs same treatment in both arms.

Comparison 3 Mobilisation versus control, Outcome 1 PAIN: cervical mobilisation vs control.
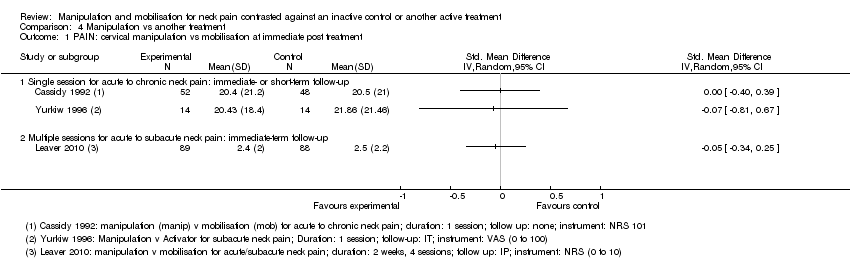
Comparison 4 Manipulation vs another treatment, Outcome 1 PAIN: cervical manipulation vs mobilisation at immediate post treatment.

Comparison 4 Manipulation vs another treatment, Outcome 2 PAIN: cervical manipulation vs mobilisation at intermediate‐term follow‐up.
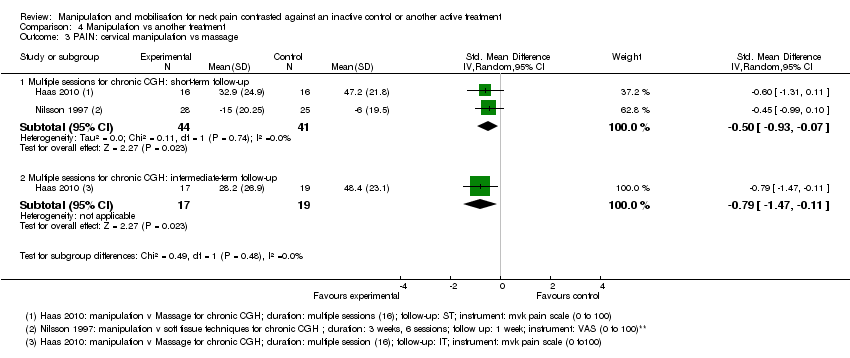
Comparison 4 Manipulation vs another treatment, Outcome 3 PAIN: cervical manipulation vs massage.

Comparison 4 Manipulation vs another treatment, Outcome 4 PAIN: cervical manipulation vs medicine.

Comparison 4 Manipulation vs another treatment, Outcome 5 PAIN: cervical manipulation vs exercise.

Comparison 4 Manipulation vs another treatment, Outcome 6 PAIN: cervical manipulation vs electrotherapy.
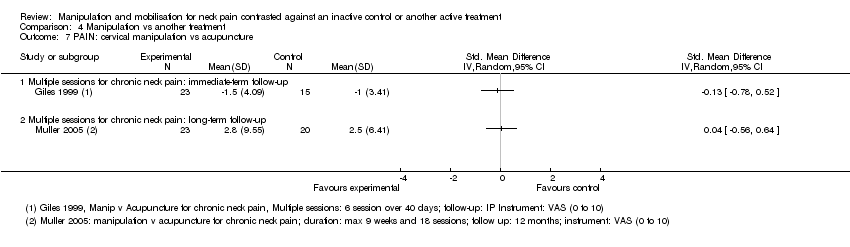
Comparison 4 Manipulation vs another treatment, Outcome 7 PAIN: cervical manipulation vs acupuncture.
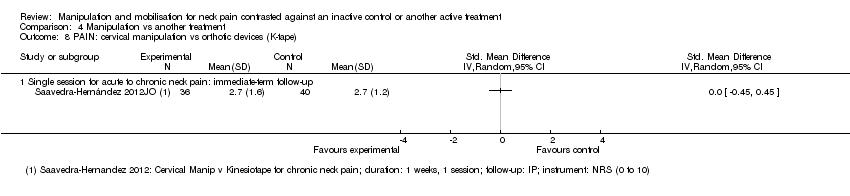
Comparison 4 Manipulation vs another treatment, Outcome 8 PAIN: cervical manipulation vs orthotic devices (K‐tape).
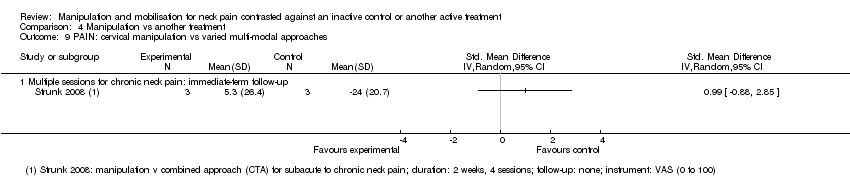
Comparison 4 Manipulation vs another treatment, Outcome 9 PAIN: cervical manipulation vs varied multi‐modal approaches.
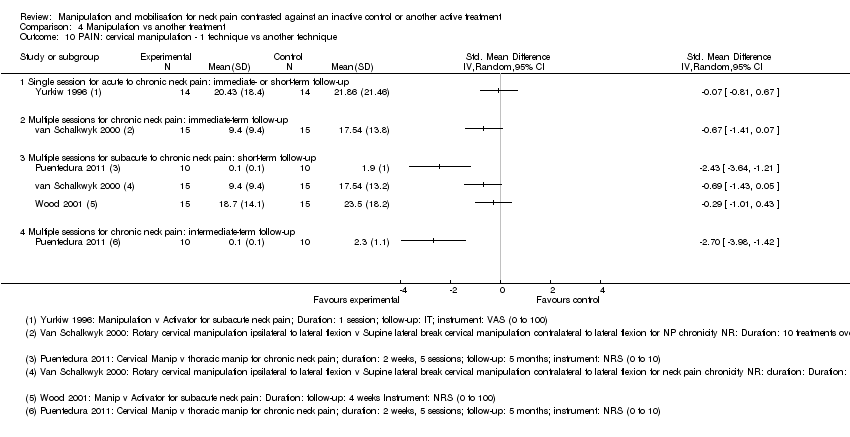
Comparison 4 Manipulation vs another treatment, Outcome 10 PAIN: cervical manipulation ‐ 1 technique vs another technique.
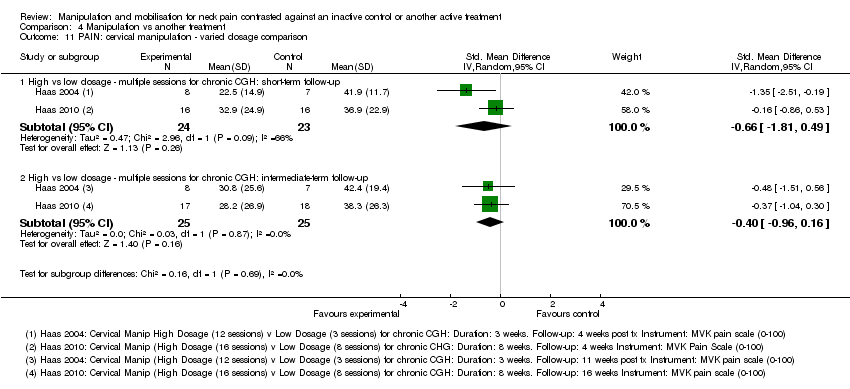
Comparison 4 Manipulation vs another treatment, Outcome 11 PAIN: cervical manipulation ‐ varied dosage comparison.

Comparison 4 Manipulation vs another treatment, Outcome 12 PAIN: thoracic manipulation vs exercise.

Comparison 4 Manipulation vs another treatment, Outcome 13 FUNCTION: cervical manipulation vs mobilisation.
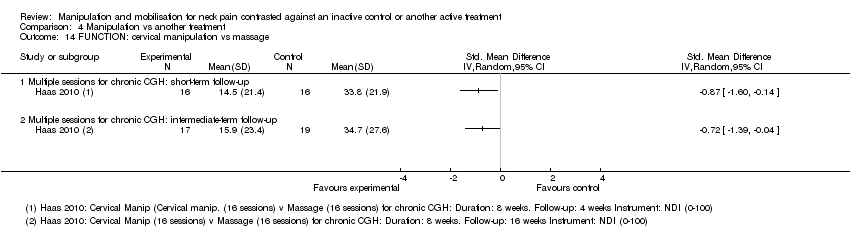
Comparison 4 Manipulation vs another treatment, Outcome 14 FUNCTION: cervical manipulation vs massage.
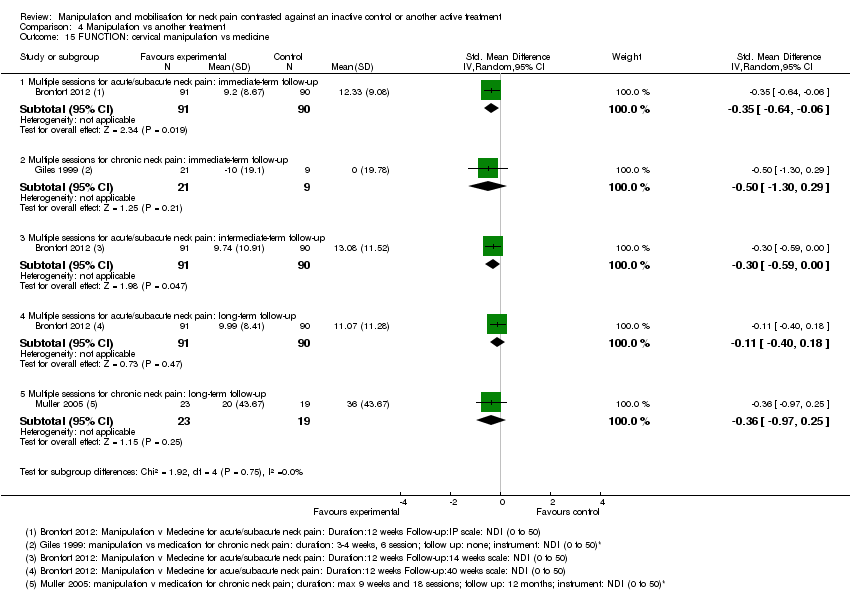
Comparison 4 Manipulation vs another treatment, Outcome 15 FUNCTION: cervical manipulation vs medicine.

Comparison 4 Manipulation vs another treatment, Outcome 16 FUNCTION: cervical manipulation vs exercise.

Comparison 4 Manipulation vs another treatment, Outcome 17 FUNCTION: cervical manipulation vs orthotic devices (K‐taping).

Comparison 4 Manipulation vs another treatment, Outcome 18 FUNCTION: cervical manipulation vs acupuncture.

Comparison 4 Manipulation vs another treatment, Outcome 19 FUNCTION: cervical manipulation vs varied multi‐modal approaches.

Comparison 4 Manipulation vs another treatment, Outcome 20 FUNCTION: cervical manipulation ‐ 1 technique vs another technique.

Comparison 4 Manipulation vs another treatment, Outcome 21 FUNCTION: cervical manipulation ‐ varied dosage comparison.
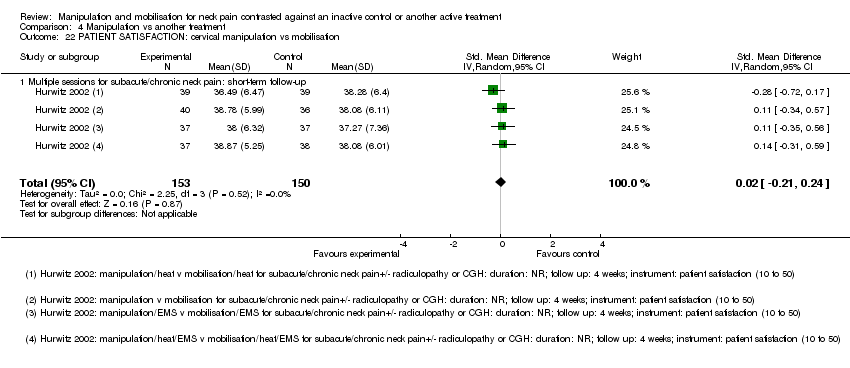
Comparison 4 Manipulation vs another treatment, Outcome 22 PATIENT SATISFACTION: cervical manipulation vs mobilisation.

Comparison 4 Manipulation vs another treatment, Outcome 23 PATIENT SATISFACTION: cervical manipulation vs varied multi‐modal approaches.
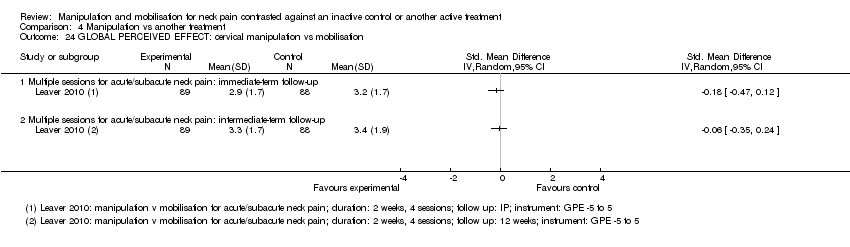
Comparison 4 Manipulation vs another treatment, Outcome 24 GLOBAL PERCEIVED EFFECT: cervical manipulation vs mobilisation.
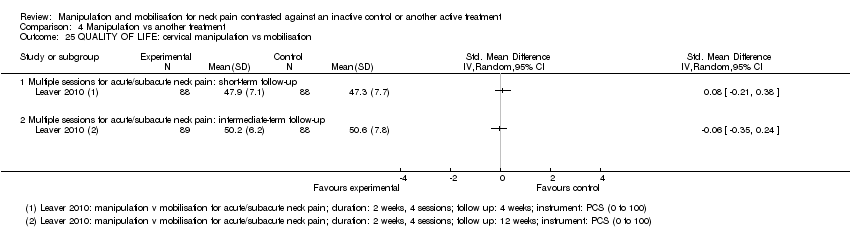
Comparison 4 Manipulation vs another treatment, Outcome 25 QUALITY OF LIFE: cervical manipulation vs mobilisation.

Comparison 4 Manipulation vs another treatment, Outcome 26 QUALITY OF LIFE: cervical manipulation vs medicine.

Comparison 4 Manipulation vs another treatment, Outcome 27 QUALITY OF LIFE: cervical manipulation vs exercise.
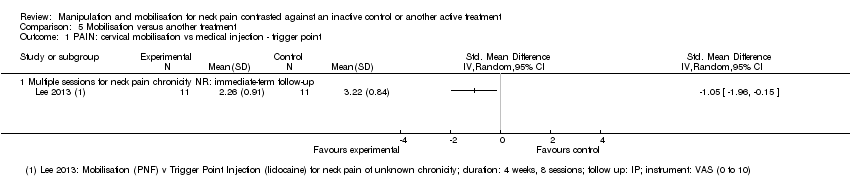
Comparison 5 Mobilisation versus another treatment, Outcome 1 PAIN: cervical mobilisation vs medical injection ‐ trigger point.
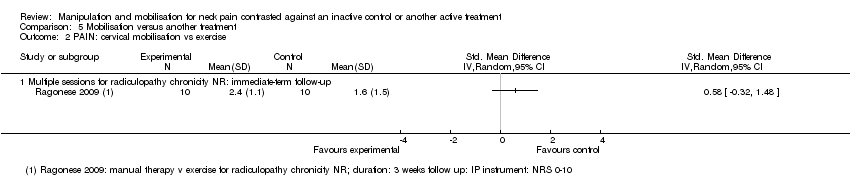
Comparison 5 Mobilisation versus another treatment, Outcome 2 PAIN: cervical mobilisation vs exercise.
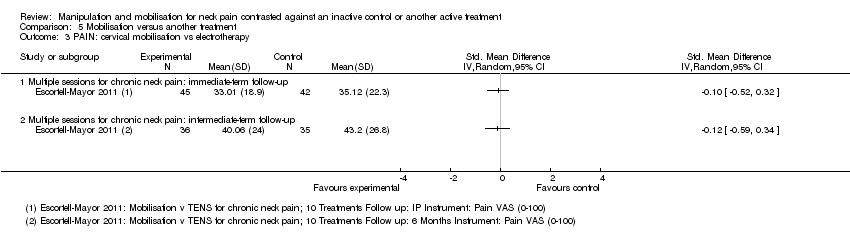
Comparison 5 Mobilisation versus another treatment, Outcome 3 PAIN: cervical mobilisation vs electrotherapy.

Comparison 5 Mobilisation versus another treatment, Outcome 4 PAIN: cervical mobilisation vs sonic devices ‐ ultrasound, shock wave therapy.

Comparison 5 Mobilisation versus another treatment, Outcome 5 PAIN: cervical mobilisation vs mechanical traction.

Comparison 5 Mobilisation versus another treatment, Outcome 6 PAIN: cervical mobilisation vs acupuncture.

Comparison 5 Mobilisation versus another treatment, Outcome 7 PAIN: cervical mobilisation vs varied multi‐modal approaches.

Comparison 5 Mobilisation versus another treatment, Outcome 8 PAIN: cervical mobilisation ‐ 1 technique vs another technique.

Comparison 5 Mobilisation versus another treatment, Outcome 9 PAIN: cervical mobilisation ‐ 1 technique vs another technique.

Comparison 5 Mobilisation versus another treatment, Outcome 10 PAIN: cervical mobilisation vs massage.

Comparison 5 Mobilisation versus another treatment, Outcome 11 FUNCTION: cervical mobilisation vs medical injection ‐ trigger point.

Comparison 5 Mobilisation versus another treatment, Outcome 12 FUNCTION: cervical mobilisation vs exercise.
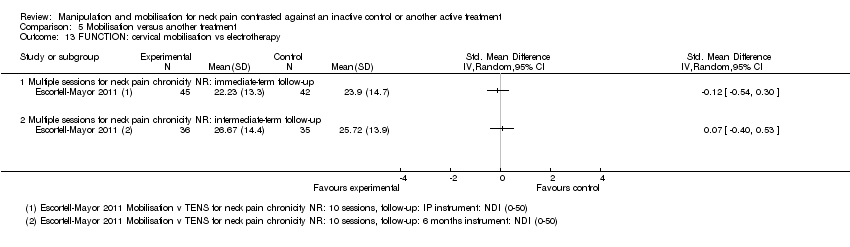
Comparison 5 Mobilisation versus another treatment, Outcome 13 FUNCTION: cervical mobilisation vs electrotherapy.

Comparison 5 Mobilisation versus another treatment, Outcome 14 FUNCTION: cervical mobilisation vs sonic devices ‐ shock wave therapy.

Comparison 5 Mobilisation versus another treatment, Outcome 15 FUNCTION: cervical mobilisation vs acupuncture.

Comparison 5 Mobilisation versus another treatment, Outcome 16 FUNCTION: cervical mobilisation vs varied multi‐modal approaches.

Comparison 5 Mobilisation versus another treatment, Outcome 17 FUNCTION: cervical mobilisation vs massage.

Comparison 5 Mobilisation versus another treatment, Outcome 18 FUNCTION: cervical mobilisation ‐ 1 technique vs another technique.
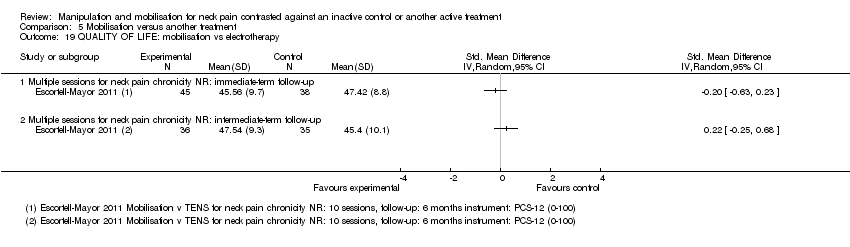
Comparison 5 Mobilisation versus another treatment, Outcome 19 QUALITY OF LIFE: mobilisation vs electrotherapy.

Comparison 5 Mobilisation versus another treatment, Outcome 20 PATIENT SATISFACTION: cervical mobilisation vs varied multi‐modal approaches.
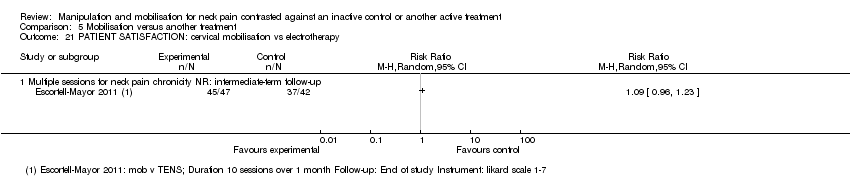
Comparison 5 Mobilisation versus another treatment, Outcome 21 PATIENT SATISFACTION: cervical mobilisation vs electrotherapy.
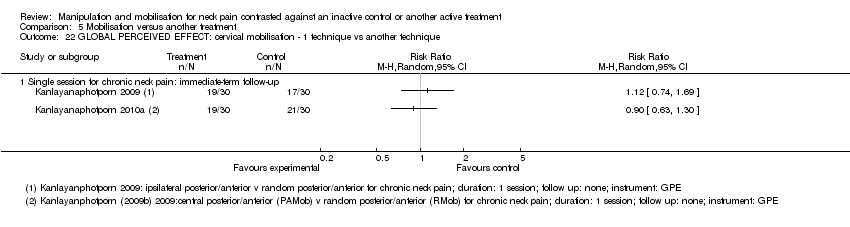
Comparison 5 Mobilisation versus another treatment, Outcome 22 GLOBAL PERCEIVED EFFECT: cervical mobilisation ‐ 1 technique vs another technique.
| Manipulation (cervical) compared with oral medicine for acute/subacute neck pain | ||||
| Patient or population: patients with acute and subacute neck pain Settings: outpatient clinics, ambulatory care services Intervention: manipulation of cervical region ‐ multiple sessions Comparison: oral medicine ‐ varied combinations of non‐steroidal anti‐inflammatory drugs (NSAIDs), analgesics, opioid analgesics and muscle relaxants | ||||
| Outcomes | Relative effect | Number of participants | Quality of the evidence | Comments |
| PAIN | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD ‐0.21 (‐0.5 to 0.08) | 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Acute and subacute neck pain Long‐term follow‐up | SMD ‐0.32 (‐0.61 to ‐0.02) | 181 | ⊕⊕⊕⊝ Moderatea | Pain reduction favouring manipulation over medication |
| FUNCTION | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD ‐0.30 (‐0.59 to ‐0.00) | 182 | ⊕⊕⊕⊝ Moderatea | Functional improvement favouring manipulation over medication |
| Acute and subacute neck pain Long‐term follow‐up | SMD ‐0.11 (‐0.40 to 0.18)
| 181 | ⊕⊕⊕⊝ Moderatea | No significant difference between groups |
| PARTICIPANT SATISFACTION | ||||
| Acute and subacute neck pain Long‐term follow‐up | Not estimable | 182 | ⊕⊕⊕⊝ Moderatea | Manipulation favoured over medication |
| QUALITY OF LIFE | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD 0.22 (‐0.07 to 0.51) | 181 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Acute and subacute neck pain Long‐term follow‐up | SMD: 0.19 (‐0.10 to 0.49) | 181 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Moderate‐quality evidence suggests that multiple sessions of cervical manipulation are more effective than medication (analgesics and non‐steroidal anti‐inflammatory drugs (NSAIDs)) for improving pain at immediate‐term and long‐term follow‐up (1 trial; 181 participants); function at intermediate term and satisfaction over the long term. Quality of life was similar between groups (1 trial, 182 participants) at intermediate‐ and long‐term follow‐up. | ||||
| GRADE Working Group grades of evidence. | ||||
| aIndirectness: ‐1; a second independent trial is needed to clarify emerging data. | ||||
| Manipulation (thoracic) compared with inactive control for neck pain | ||||
| Patient or population: patients with acute, subacute and chronic neck pain Settings: outpatient clinics, ambulatory care services Intervention: manipulation of thoracic region ‐ multiple sessions Comparison: inactive control | ||||
| Outcomes | Relative effect | Number of participants | Quality of the evidence | Comments |
| PAIN | ||||
| Acute and subacute neck pain Short‐term follow‐up | SMD pooled ‐1.46 (‐2.20 to ‐0.71) | 242 Fernandez 2004 JWRD; Fernandez 2009; Gonzalez‐Iglesias 2009 JO; | ⊕⊕⊕⊝ Moderatea | Favoured treatment; NNTB: 4 to 7; magnitude of effect: medium |
| Chronic neck pain Intermediate‐term follow‐up | SMD ‐0.64 (‐1.04 to ‐0.25) | 111 | ⊕⊕⊝⊝ Lowb,c | Favoured treatment; NNTB 4; magnitude of effect: small |
| FUNCTION | ||||
| Acute and subacute neck pain Short‐term follow‐up | SMD pooled ‐1.73 (‐2.68 to ‐0.78) | 258 | ⊕⊕⊕⊝ Moderatea | Favoured treatment; NNTB 4 to 5; magnitude of effect: medium |
| Chronic neck pain Short‐term follow‐up | SMD ‐0.50 (‐0.89 to ‐0.10) | 111 | ⊕⊕⊝⊝ Lowb,c | Favoured treatment; NNTB 5; magnitude of effect: small |
| Chronic neck pain Intermediate‐term follow‐up | SMD ‐0.38 (‐0.77 to 0.01) | 111 (1 trial; Cheung Lau 2011) | ⊕⊕⊝⊝ Lowb,c | Favoured treatment; NNTB 5; magnitude of effect: small |
| QUALITY OF LIFE (QoL) | ||||
| Chronic neck pain Short‐term follow‐up | SMD ‐0.82 (‐1.23 to ‐0.42) | 111 | ⊕⊕⊝⊝ Lowb,c | Favoured treatment |
| Chronic neck pain Intermediate‐term follow‐up | SMD ‐0.61 (‐1.01 to ‐0.22) | 111 | ⊕⊕⊝⊝ Lowc | Favoured treatment |
| Seven trials (428 participants) using multiple sessions of thoracic manipulation for acute to chronic neck pain were assessed at 3 time intervals. At short‐term follow‐up, moderate‐quality evidence favoured thoracic manipulation for pain reduction among participants with acute/subacute neck pain, and with acute to chronic neck pain, it improved function. These findings were consistent but small at intermediate follow‐up for pain, function and quality of life (low‐quality evidence). | ||||
| GRADE Working Group grades of evidence. | ||||
| bIndirectness: ‐1, immediate post‐treatment data have limited clinical relevance; single trials with only immediate‐ and short‐term follow‐up are downgraded (ceiling effect) because future research is likely to have an important impact on the direction of the reported effect, and a second independent trial is needed to clarify emerging short‐term data. cImprecision: ‐1, small sample size. aInconsistency: P value = 0.002; I² = 84%; sensitivity analysis: Statistical differences led us to explore heterogeneity by the following PICO factors: P: about the same; I: about the same; C: about the same; O: for pain, VAS, NPRS; for disability, NPQ, NDI; RoB: most often low RoB but when the trial of high RoB is removed, pooled SMD increases to ‐2.18 (‐2.71 to ‐1.65) for pain, but these data were derived from trials conducted in the same lab. | ||||
| Manipulation compared with mobilisation for neck pain | ||||
| Patient or population: patients with acute, subacute and chronic neck pain Settings: ambulatory care or outpatient clinic Intervention: manipulation of cervical region ‐ multiple sessions Comparison: mobilisation | ||||
| Outcomes | Relative effect | Number of participants | Quality of the evidence | Comments |
| PAIN | ||||
| Acute, subacute and chronic neck pain Intermediate‐term follow‐up | MD pooled ‐0.07 (‐0.72 to 0.59) | 446 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| FUNCTION AND DISABILITY | ||||
| Acute and subacute neck pain Short‐term follow‐up | SMD: ‐0.06 (‐0.35 to 0.24) | 176 | ⊕⊕⊕⊝ Moderateb | No significant differences between groups |
| Acute, subacute and chronic neck pain Intermediate‐term follow‐up | SMD pooled: 0.10 (‐0.18 to 0.37)
| 446 | ⊕⊕⊕⊕ High | No significant differences between groups |
| PARTICIPANT SATISFACTION | ||||
| Subacute and chronic neck pain Short‐term follow‐up | SMD: ‐0.02 (‐0.21 to 0.24) | 269 | ⊕⊕⊕⊝ Moderateb | No significant differences between groups |
| GLOBAL PERCEIVED EFFECT | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD: ‐0.06 | 177 | ⊕⊕⊕⊝ Moderateb | No significant differences between groups |
| QUALITY OF LIFE | ||||
| Acute and subacute neck pain Short‐term follow‐up | SMD: 0.08 (‐0.21 to 0.38) | 176 | ⊕⊕⊕⊝ Moderateb | No significant differences between groups |
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD: ‐0.06 (‐0.35 to 0.24) | 177 | ⊕⊕⊕⊝ Moderateb | No significant differences between groups |
| Moderate‐ to high‐quality evidence (2 trials, 446 participants) suggests that multiple sessions of cervical manipulation produced similar changes in pain, function, quality of life, global perceived effect and patient satisfaction when compared with multiple sessions of cervical mobilisation at immediate‐, short‐ and intermediate‐term follow‐up. | ||||
| GRADE Working Group grades of evidence. | ||||
| aInconsistency: ‐1. bIndirectness: ‐1. | ||||
| Manipulation compared with exercise for neck pain | ||||
| Patient or population: patients with acute and subacute neck pain Settings: ambulatory care or outpatient clinic setting Intervention: manipulation of cervical region Comparison: exercise | ||||
| Outcomes | Relative effect | Number of participants | Quality of the evidence | Comments |
| PAIN | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD: ‐0.16 (‐0.45 to 0.13) | 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Acute and subacute neck pain Long‐term follow‐up | SMD: 0.06 (‐0.23 to 0.35) | 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| FUNCTION | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD: ‐0.01 (‐0.30 to 0.28)
| 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Acute and subacute neck pain Long‐term follow‐up | SMD: ‐0.02 (‐0.31 to 0.27)
| 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| PARTICIPANT SATISFACTION | ||||
| Acute and subacute neck pain Long‐term follow‐up | Not estimable | 182 | ⊕⊕⊕⊝ Moderatea | Improvement in participant satisfaction for manipulation over exercise |
| GLOBAL PERCEIVED EFFECT | ||||
| Acute and subacute neck pain Immediate post‐treatment follow‐up | Not estimable | 182 (1 trial; Bronfort 2012) | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| QUALITY OF LIFE | ||||
| Acute and subacute neck pain Intermediate‐term follow‐up | SMD: ‐0.05 (‐0.35 to 0.24) | 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Acute and subacute neck pain Long‐term follow‐up | SMD: 0.0 (‐0.29 to 0.29) | 182 | ⊕⊕⊕⊝ Moderatea | No significant differences between groups |
| Moderate‐quality evidence suggests no differences in pain, function, global perceived effect and quality of life when multiple sessions of cervical manipulation are compared with exercise at immediate‐, intermediate‐ and long‐term follow‐up. Moderate‐quality evidence indicates that use of cervical manipulation led to greater participant satisfaction when compared with an exercise programme at long‐term follow‐up. | ||||
| GRADE Working Group grades of evidence. | ||||
| aIndirectness: ‐1. | ||||
| High dose of manipulation compared with low dose of manipulation for chronic neck pain | ||||
| Patient or population: patients with chronic neck pain with cervicogenic headache (CGH) Settings: ambulatory care or outpatient clinic setting Intervention: manipulation of cervical region Comparison: high dose vs low dose | ||||
| Outcomes | Relative effect | Number of participants | Quality of the evidence | Comments |
| PAIN | ||||
| Chronic neck pain and CGH Intermediate‐term follow‐up | SMD pooled: ‐0.40 (‐0.96 to 0.16)
| ⊕⊕⊕⊝ Moderatea | Two trials showed no significant differences between groups | |
| FUNCTION | ||||
| Chronic neck pain and CGH Intermediate‐term follow‐up | SMD pooled: ‐0.61 (‐1.38 to 0.17) | ⊕⊕⊕⊝ Moderatea | Two trials showed no significant differences between groups | |
| Moderate‐quality evidence shows that high‐dose (12 to 18 sessions) contrasted against low‐dose (3 to 8 sessions) cervical manipulation produced similar changes in pain and function at intermediate‐term follow‐up for individuals with chronic neck pain with cervicogenic headache. | ||||
| GRADE Working Group grades of evidence. | ||||
| aImprecision: ‐1. | ||||
| Term | Definiton |
| Per cent treatment advantage (%) | Calculation of the clinically important difference or change in a per cent scale was estimated as follows. Karlberg 1996 data are used in this example. % improvement (control) equals the difference between the change in the control group (1) divided by the control baseline (56), which equals 1.8%. Treatment advantage = 42.6% ‐ 1.8% = 40.8% |
| Number needed to treat (NNTB) | For this example, Karlberg 1996 outcomes measured at short‐term follow‐up are used to derive the data. Number needed to treat is the number of patients a clinician needs to treat to achieve a clinically important improvement in 1. If we assume the minimal clinically important difference to be 10% of the baseline mean in the control group, and the control group mean at baseline is 56, then 10% of 56 is 5.6 The effect is baseline ‐ final value; therefore:
Converting these to standard normal values means that:
NNTB = 1 divided by the difference in areas under the normal curve (experimental group ‐ control group):
|
| Author/Comparison | NNTB | Advantage, % |
| PAIN | ||
| Haas 2004: pain | 12 (clinically important pain reduction) at ST | 23 |
| Haas 2010: pain | 4 (clinically important pain reduction) at IT | 29 |
| Cleland 2005 | 5 (clinically important pain reduction) | 29 |
| Cheung Lau 2011: pain | 4 (clinically important pain reduction) | |
| Fernandez 2004a | Unable to calculate because baseline data not reported | |
| Gonzalez‐Iglesias 2009 | 7 (clinically important pain reduction) | 47 |
| Martinez‐Segura 2006, | 2 (clinically important pain reduction) | 54 |
| Massaracchio 2013: pain | 4 (clinically important pain reduction) | |
| von Piekartz 2011: pain | 2 (clinically important pain reduction) at IT | |
| FUNCTION | ||
| Cheung Lau 2011: function | 5 (clinically important functional improvement) at IT | |
| Gonzalez‐Iglesias 2009 | 5 (clinically important functional improvement) | 41 |
| Haas 2010: function | 5 (clinically important functional improvement) at ST and IT | ST: 41 IT: 39 |
| Massaracchio 2013: function | 4 (clinically important functional improvement) | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 PAIN: cervical manipulation vs placebo Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Single session: immediate‐ or short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 PAIN: thoracic manipulation vs placebo Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Single session: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 PAIN: cervical manipulation vs control Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Multiple sessions for chronic neck pain with HA: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 PAIN: cervical manipulation plus treatment vs same treatment in both arms Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Single session for subacute/chronic neck pain: immediate‐ or short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Multiple sessions for subacute/chronic neck pain: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 PAIN: cervical manipulation vs same treatment in both arms Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 3.1 Single session for subacute/chronic neck pain with radicular findings and HA: short‐term follow‐up | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 PAIN: thoracic manipulation vs control Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 Single session for neck pain of not reported duration: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 PAIN: thoracic manipulation vs same treatment in both arms Show forest plot | 8 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 5.1 Multiple sessions for acute neck pain: immediate‐term follow‐up | 2 | 90 | Std. Mean Difference (IV, Random, 95% CI) | ‐3.46 [‐4.13, ‐2.79] |
| 5.2 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 2 | 141 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.23 [‐1.15, 0.69] |
| 5.3 Single session for chronic neck pain: short‐term follow‐up | 1 | 82 | Std. Mean Difference (IV, Random, 95% CI) | 0.08 [‐0.36, 0.51] |
| 5.4 Multiple sessions for acute/subacute neck pain: short‐term follow‐up | 4 | 242 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.46 [‐2.20, ‐0.71] |
| 5.5 Multiple sessions for chronic neck pain: short‐term follow‐up | 1 | 104 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.60 [‐0.99, ‐0.20] |
| 5.6 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | 103 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.64 [‐1.04, ‐0.25] |
| 6 PAIN: cervical and thoracic manipulation vs control Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Multiple sessions for chronic neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 FUNCTION: thoracic manipulation vs same treatment in both arms Show forest plot | 6 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 7.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 2 | 141 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.52 [‐0.85, ‐0.18] |
| 7.2 Single session for chronic neck pain: short‐term follow‐up | 1 | 81 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.61, 0.27] |
| 7.3 Multiple sessions for acute neck pain: short‐term follow‐up | 3 | 154 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.73 [‐2.68, ‐0.78] |
| 7.4 Multiple sessions for chronic neck pain: short‐term follow‐up | 1 | 104 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.50 [‐0.89, ‐0.10] |
| 7.5 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | 103 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.38 [‐0.77, 0.01] |
| 8 FUNCTION: cervical manipulation vs same treatment in both arms Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8.1 Multiple sessions for chronic neck pain: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 FUNCTION: cervical and thoracic manipulation vs control Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 9.1 Multiple sessions for chronic neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 QUALITY OF LIFE: thoracic manipulation vs control Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 10.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 Multiple sessions for chronic neck pain: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.3 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 FUNNEL PLOT for pain: thoracic manipulation vs same treatment in both arms Show forest plot | 5 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 11.1 Multiple sessions for acute to chronic neck pain: short‐term follow‐up | 5 | 346 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.26 [‐1.86, ‐0.66] |
| 12 FUNNEL PLOT for function: thoracic manipulation vs same treatment in both arms Show forest plot | 4 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 12.1 Multiple sessions: short‐term follow‐up | 4 | 258 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.40 [‐2.24, ‐0.55] |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 PAIN: cervical mobilisation vs control Show forest plot | 2 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Single session: intermediate post treatment | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Multiple sessions: short‐term follow‐up | 1 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 PAIN: cervical manipulation vs mobilisation at immediate post treatment Show forest plot | 3 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Single session for acute to chronic neck pain: immediate‐ or short‐term follow‐up | 2 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Multiple sessions for acute to subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 PAIN: cervical manipulation vs mobilisation at intermediate‐term follow‐up Show forest plot | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 Multiple sessions for acute to chronic neck pain: intermediate‐term follow‐up | 2 | 446 | Mean Difference (IV, Random, 95% CI) | ‐0.07 [‐0.72, 0.59] |
| 3 PAIN: cervical manipulation vs massage Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 Multiple sessions for chronic CGH: short‐term follow‐up | 2 | 85 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.50 [‐0.93, ‐0.07] |
| 3.2 Multiple sessions for chronic CGH: intermediate‐term follow‐up | 1 | 36 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.79 [‐1.47, ‐0.11] |
| 4 PAIN: cervical manipulation vs medicine Show forest plot | 3 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 Multiple sessions for acute/subacute neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.4 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.5 Multiple sessions for chronic neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 PAIN: cervical manipulation vs exercise Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.3 Multiple sessions for acute/subacute neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 PAIN: cervical manipulation vs electrotherapy Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Multiple sessions for subacute to chronic CGH: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 Multiple sessions for subacute to chronic neck pain: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 PAIN: cervical manipulation vs acupuncture Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 Multiple sessions for chronic neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 PAIN: cervical manipulation vs orthotic devices (K‐tape) Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8.1 Single session for acute to chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 PAIN: cervical manipulation vs varied multi‐modal approaches Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 9.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 PAIN: cervical manipulation ‐ 1 technique vs another technique Show forest plot | 4 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 10.1 Single session for acute to chronic neck pain: immediate‐ or short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.3 Multiple sessions for subacute to chronic neck pain: short‐term follow‐up | 3 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.4 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 PAIN: cervical manipulation ‐ varied dosage comparison Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 11.1 High vs low dosage ‐ multiple sessions for chronic CGH: short‐term follow‐up | 2 | 47 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.66 [‐1.81, 0.49] |
| 11.2 High vs low dosage ‐ multiple sessions for chronic CGH: intermediate‐term follow‐up | 2 | 50 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.40 [‐0.96, 0.16] |
| 12 PAIN: thoracic manipulation vs exercise Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 12.1 Multiple sessions for neck pain chronicity NR: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13 FUNCTION: cervical manipulation vs mobilisation Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 13.1 Multiple sessions for acute/subacute neck pain: short‐term follow‐up | 1 | 176 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.06 [‐0.35, 0.24] |
| 13.2 Multiple sessions for acute to chronic neck pain: intermediate‐term follow‐up | 2 | 445 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.01 [‐0.21, 0.18] |
| 14 FUNCTION: cervical manipulation vs massage Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 14.1 Multiple sessions for chronic CGH: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.2 Multiple sessions for chronic CGH: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15 FUNCTION: cervical manipulation vs medicine Show forest plot | 3 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 15.1 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | 181 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.35 [‐0.64, ‐0.06] |
| 15.2 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | 30 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.50 [‐1.30, 0.29] |
| 15.3 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | 181 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.30 [‐0.59, ‐0.00] |
| 15.4 Multiple sessions for acute/subacute neck pain: long‐term follow‐up | 1 | 181 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.11 [‐0.40, 0.18] |
| 15.5 Multiple sessions for chronic neck pain: long‐term follow‐up | 1 | 42 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.36 [‐0.97, 0.25] |
| 16 FUNCTION: cervical manipulation vs exercise Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 16.1 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.2 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16.3 Multiple sessions for acute/subacute neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17 FUNCTION: cervical manipulation vs orthotic devices (K‐taping) Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 17.1 Single session for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18 FUNCTION: cervical manipulation vs acupuncture Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 18.1 Multiple sessions for subacute/chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18.2 Multiple sessions for chronic neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19 FUNCTION: cervical manipulation vs varied multi‐modal approaches Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 19.1 Multiple sessions for subacute/chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.2 Multiple sessions for subacute/chronic neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20 FUNCTION: cervical manipulation ‐ 1 technique vs another technique Show forest plot | 3 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 20.1 Multiple sessions for subacute/chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.2 Multiple sessions for acute/subacute neck pain: short‐term follow‐up | 2 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.3 Multiple sessions for neck pain chronicity NR: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20.4 Multiple sessions for acute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21 FUNCTION: cervical manipulation ‐ varied dosage comparison Show forest plot | 2 | 97 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.61 [‐1.09, ‐0.14] |
| 21.1 High vs low dosage ‐ multiple sessions for chronic CGH: short‐term follow‐up | 2 | 47 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.75 [‐1.71, 0.22] |
| 21.2 High vs low dosage ‐ multiple sessions for chronic CGH: intermediate‐term follow‐up | 2 | 50 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.61 [‐1.38, 0.17] |
| 22 PATIENT SATISFACTION: cervical manipulation vs mobilisation Show forest plot | 1 | 303 | Std. Mean Difference (IV, Random, 95% CI) | 0.02 [‐0.21, 0.24] |
| 22.1 Multiple sessions for subacute/chronic neck pain: short‐term follow‐up | 1 | 303 | Std. Mean Difference (IV, Random, 95% CI) | 0.02 [‐0.21, 0.24] |
| 23 PATIENT SATISFACTION: cervical manipulation vs varied multi‐modal approaches Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 23.1 Multiple sessions for subacute/chronic neck pain: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 24 GLOBAL PERCEIVED EFFECT: cervical manipulation vs mobilisation Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 24.1 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 24.2 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 25 QUALITY OF LIFE: cervical manipulation vs mobilisation Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 25.1 Multiple sessions for acute/subacute neck pain: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 25.2 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26 QUALITY OF LIFE: cervical manipulation vs medicine Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 26.1 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 26.2 Multiple sessions for acute/subacute neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 27 QUALITY OF LIFE: cervical manipulation vs exercise Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 27.1 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 27.2 Multiple sessions for acute/subacute neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 27.3 Multiple sessions for acute/subacute neck pain: long‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
| 1 PAIN: cervical mobilisation vs medical injection ‐ trigger point Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 PAIN: cervical mobilisation vs exercise Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Multiple sessions for radiculopathy chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 PAIN: cervical mobilisation vs electrotherapy Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 PAIN: cervical mobilisation vs sonic devices ‐ ultrasound, shock wave therapy Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4.1 Single session for subacute/chronic neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 PAIN: cervical mobilisation vs mechanical traction Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 PAIN: cervical mobilisation vs acupuncture Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 PAIN: cervical mobilisation vs varied multi‐modal approaches Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 Multiple sessions for subacute/chronic neck pain ± radiculopathy or CGH: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 PAIN: cervical mobilisation ‐ 1 technique vs another technique Show forest plot | 5 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 8.1 Single session for chronic neck pain: immediate‐term follow‐up | 2 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 Single session for chronic neck pain ± radiculopathy: immediate‐term follow‐up | 2 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.3 Multiple sessions for chronic CGH: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.4 Multiple sessions for chronic CGH: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 PAIN: cervical mobilisation ‐ 1 technique vs another technique Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 9.1 PA vs other mobilisation for acute/subacute neck pain: multiple sessions: immediate‐term follow‐up | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.2 AP vs other mobilisation: multiple sessions: immediate‐term follow‐up | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 PAIN: cervical mobilisation vs massage Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 10.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 2 | 58 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.56 [‐4.15, 1.03] |
| 10.2 Multiple sessions for chronic CGH: immediate‐term follow‐up | 1 | 36 | Std. Mean Difference (IV, Random, 95% CI) | ‐2.89 [‐3.85, ‐1.93] |
| 11 FUNCTION: cervical mobilisation vs medical injection ‐ trigger point Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 11.1 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 12 FUNCTION: cervical mobilisation vs exercise Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 12.1 Multiple sessions for radiculopathy: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13 FUNCTION: cervical mobilisation vs electrotherapy Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 13.1 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 13.2 Multiple sessions for neck pain chronicity NR: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14 FUNCTION: cervical mobilisation vs sonic devices ‐ shock wave therapy Show forest plot | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 14.1 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 14.2 Multiple sessions for acute/subacute neck pain: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 15 FUNCTION: cervical mobilisation vs acupuncture Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 15.1 Multiple sessions for chronic neck pain: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 16 FUNCTION: cervical mobilisation vs varied multi‐modal approaches Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 16.1 Multiple sessions for subacute/chronic neck pain ± radiculopathy or CGH: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 17 FUNCTION: cervical mobilisation vs massage Show forest plot | 2 | 59 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.03 [‐0.90, 0.84] |
| 17.1 Multiple sessions for chronic neck pain: immediate‐term follow‐up | 1 | 23 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.52 [‐1.35, 0.32] |
| 17.2 Multiple sessions for subacute/chronic CGH: immediate‐term follow‐up | 1 | 36 | Std. Mean Difference (IV, Random, 95% CI) | 0.38 [‐0.28, 1.04] |
| 18 FUNCTION: cervical mobilisation ‐ 1 technique vs another technique Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 18.1 Multiple sessions for chronic CGH: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 18.2 Multiple sessions for chronic CGH: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19 QUALITY OF LIFE: mobilisation vs electrotherapy Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 19.1 Multiple sessions for neck pain chronicity NR: immediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 19.2 Multiple sessions for neck pain chronicity NR: intermediate‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 20 PATIENT SATISFACTION: cervical mobilisation vs varied multi‐modal approaches Show forest plot | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 20.1 Multiple sessions for subacute/chronic neck pain ± radiculopathy or CGH: short‐term follow‐up | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 21 PATIENT SATISFACTION: cervical mobilisation vs electrotherapy Show forest plot | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 21.1 Multiple sessions for neck pain chronicity NR: intermediate‐term follow‐up | 1 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 22 GLOBAL PERCEIVED EFFECT: cervical mobilisation ‐ 1 technique vs another technique Show forest plot | 2 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 22.1 Single session for chronic neck pain: immediate‐term follow‐up | 2 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |